
Submitted:
22 February 2024
Posted:
23 February 2024
You are already at the latest version
Abstract
Background: Limited data exist on postoperative acute kidney injury (AKI) in patients underwent esophageal cancer surgery. The purpose of the study was to evaluate the incidence, risk factors and consequences of postoperative acute kidney after esophagectomy. Methods: This was a retrospective cohort study. The study was conducted in a tertiary specialized cancer center in Italy. All patients undergoing elective esophageal cancer surgery between 2016 and 2021 were included in the study. AKI was defined according to Kidney Disease: Improving Global Outcomes criteria (both serum creatinine and urine output), within 48 hours after surgery. Preoperative and intraoperative data were registered. We also collected data concerning progression of AKI, need for kidney replacement therapy, mortality, medical (pulmonary, cardiovascular, septic) and surgical complications within 30 days from surgery, as well as length of hospital stay. Results: Incidence of postoperative AKI was 32%. The independent risk factors were body mass index and the invasive surgical approach. Persistent AKI accounted for 15% of the cases and it was associated with increased risk of major cardiovascular events (odds ratio 4.14, 95% CI 1.05-15.8, p-value 0.036), pulmonary complications (OR 3.67, 95% CI 1.04-14.9, p-value 0.050) and increased length of hospital stay (AME 7.2, 0.5-13.9, p-value 0.035). Conclusions: Postoperative AKI is common after esophageal cancer surgery. BMI and totally invasive surgical approach are independent risk factors. Persistent AKI lasting more than 48 hours increased the risk for cardiovascular and pulmonary complications, with prolonged length of hospital stay.
Keywords:
postoperative acute kidney injury
; esophageal cancer surgery
; outcome
1. Introduction
Esophagectomy is considered to be the cornerstone treatment for locally advanced esophageal cancer [1]. Esophagectomy is a complex major intervention, with well-known risk of pulmonary, cardiac, anastomotic, and septic complications. The presence of postoperative complications after esophagectomies for cancer is associated with a reduced long-term survival [2]. There is a paucity of data in the literature concerning postoperative renal outcomes after esophageal surgery, with a wide range of incidence[3,4,5,6,7]. Perioperative acute kidney injury (AKI) and the ways in which it develops is multifaceted and complex. Hypoperfusion, inflammation, and neuroendocrine response to surgery are common mechanisms affecting renal function and structure[8]. Moreover, AKI may be considered a sentinel complication which engenders distant organ’s dysfunctions, resulting in more postoperative complications with increased length of hospital stay[9].
The primary aim of this study was to evaluate the incidence of postoperative AKI in patients undergoing elective esophageal cancer surgery. As secondary aim, we assessed the progression of the acute kidney injury and the association with adverse pulmonary, cardiovascular, anastomotic, and septic events, as well as mortality. We also identified the risk factors associated with AKI occurrence.
2. Materials and Methods
2.1. Study Population
This is a retrospective observational study conducted at the University Hospital of Padua in patients who underwent elective esophagectomy from January 2016 to January 2021. Exclusion criteria were age< 18 years, end-stage renal disease, missing data for AKI definition, second surgery (for patients having multiple surgeries performed during a 30-day period, only the first in each period was included).
2.2. Endpoints
Our primary endpoint was to evaluate the incidence of postoperative AKI according KDIGO criteria within 48 hours after surgery. Our secondary endpoints were the distinction between transient and persistent AKI, occurrence of recovery of AKI or progression at 7, 30 days and 3 months, the association between AKI and pulmonary complications, major adverse cardiovascular events, surgical or septic complications, or death; the identification of risk factors associated with AKI occurrence.
2.3. Statistical Analysis
Descriptive statistics were reported as median (I quartile-III quartile) for continuous variables and as absolute numbers (percentages) for categorical variables. Univariable and multivariable logistic regression models were employed to identify factors associated with postoperative AKI. Results were reported as Odds Ratio, 95% Confidence Interval (CI), and p-value. Univariable logistic models were employed to evaluate the association between AKI and postoperative binary outcomes. Univariable Gamma models were employed for continuous outcomes, given the non-normal distribution of all the continuous outcomes considered. For what concerns Gamma models, the marginal effect was computed considering the partial derivatives of the marginal expectation. Results were reported as average marginal effect (AME), 95% CI, and p-value. Analyses were performed using the R software.
2.4. Data Collection
A team properly instructed collected patient’s data in a CRF (Case Report Form). An electronic copy of CRF was retained in Microsoft Excel format. We collected data on preoperative (age, gender, body mass index (BMI), level of dependency, American Society of Anesthesiology (ASA) status, comorbidities, medications, laboratory tests, such as serum creatinine (SCr), urea, blood cells count, estimation of glomerular filtration rate (eGFR) and length of hospital stay according National Surgical Quality Improvement Program (NSQIP)), intraoperative (type of surgery, type of anesthesia, duration of anesthesia, type of ventilation, lower systolic arterial pressure, lower ratio of oxygen saturation and fractional inspired oxygen content, amount of fluids, use of colloids or blood, use of vasopressors, inotropes or antiarrhythmics, blood loss, hemoglobin and lactate at the end of surgery, diuresis at the end of surgery and use of non-steroidal anti-inflammatory drugs), postoperative (serum creatinine, diuresis, fluid balance, medical and surgical complications) data. All collected data were identified and stored in such a way as to protect patient confidentiality. The staff involved in the collection and management of data didn’t use or disseminate such information for purposes other than those provided for the realization of the study. All data were collected and processed in a completely anonymous way, in compliance with the guaranteed terms of privacy and as approved by Comitato Etico per la Sperimentazione Clinica della Provincia di Padova.
2.5. Assessment of Renal Function
AKI was defined according to Kidney Disease Improving Global Outcomes (KDIGO) 2012 consensus guidelines[10] as an increase in SCr by ≥ 0.3 mg/dl), or an increase in SCr level 1.5-1.9 times the baseline value or urine volume < 0.5ml/Kg/h for 6-12 hours. AKI was staged as followed: stage 1 as an increase in SCr level by ≥ 0.3 mg/dl), or an increase in SCr level 1.5-1.9 times the baseline value or urine volume < 0.5ml/Kg/h for 6-12 hours; stage 2 as an increase in SCr level 2.0-2.9 times the baseline value or urine volume < 0.5 ml/kg/h for ≥ 12 hours; stage 3 as an increase in SCr level 3.0 times baseline or ≥ 4.0 mg/dl, or initiation of kidney replacement therapy. For those who did not have available baseline SCr levels, we expanded the screening criteria to an increase or decrease in SCr by 0.3 mg/dl during hospital stay. Every patient with suspected AKI was reviewed on a case-by-case basis to confirm or to rule out the diagnosis. Positive fluid balance and hemodilution were considered in the diagnosis and staging of AKI using the following formula [11]:
Adjusted SCr level = SCr × correction factor,
where the correction factor = (weight (kg) upon hospital admission × 0.6 + Σ (daily cumulative fluid balance (L))/hospital admission weight × 0.6. The eGFR was determined using SCr [12]. The following definitions according to Acute Dialysis Quality Initiative Consensus12 were applied:
Persistent AKI: the protraction of AKI by serum creatinine or urine output criteria (according KDIGO criteria) beyond 48 h from AKI onset. Transient AKI: complete reversal of AKI by KDIGO criteria within 48 h of AKI onset. Acute kidney disease (AKD): a condition wherein criteria for AKI stage 1 or greater persists ≥7 days after surgery.
2.6. Assessment of Complications and Mortality
Postoperative pulmonary complications were identified and classified based on European Perioperative Clinical Outcome definitions from the European Society of Anesthesiology-European Society of Intensive Care Medicine taskforce on perioperative outcome measures [14]. These include respiratory infection, respiratory failure, pleural effusion, atelectasis, pneumothorax, bronchospasm, aspiration pneumonitis. Major adverse cardiac and cerebrovascular events (MACCE) were a composite outcome of non-fatal cardiac arrest, acute myocardial infarction, congestive heart failure, new cardiac arrhythmia, angina, ischemic stroke [14]. Sepsis was defined according to Sepsis-3 definition [15]. We performed analyses of complications apparently related to surgical technique (classified according Esophagectomy Complications Consensus Group[16]) and medical complications.
All complications were evaluated at 30 days after surgery. In-hospital mortality was only considered. This was more reliably quantified than 30-day mortality.
3. Results
3.1. Participants
A total of 263 patients underwent elective esophagectomy during the 60-month study period. According to study protocol, nine patients were excluded, while 254 patients were eligible for analysis, as shown in Figure 1.
The baseline perioperative characteristics of these 254 patients are shown in Table 1.
3.2. Incidence and Risk Factors of Postoperative AKI
The incidence of postoperative AKI within 48 hours from esophageal cancer surgery was 32%. Figure 2 shows the distribution of AKI KDIGO criteria within different stages of postoperative AKI.
Only 2 patients required kidney replacement therapy after surgery, for a median time of 8 ± 1 days. In univariable model regression eight factors were associated with postoperative AKI: BMI; history of hypertension, smoking habit, NSQIP calculated length of hospital stay, angiotensin-receptor blocker use, preoperative eGFR, totally invasive surgery and intraoperative urinary output. In multivariable model regression the only independent predictors for postoperative AKI were BMI (OR 1.1, 95% CI 1.03-1.18, p-value <0.01) and totally invasive surgery (OR 3.5, 95% CI 1.3-9.2, p-value <0.05). The complete analysis is presented in Supplementary file 1.
3.3. Difference between Transient and Persistent Postoperative AKI
The vast majority of AKI patients (85%) had transient postoperative AKI, while only twelve AKI patients (15%) had persistent postoperative AKI lasting more than 48 hours. Within AKI group, eight patients (9.8%) didn’t recover within 7 days from surgery, therefore diagnosed as having acute kidney disease. When comparing patients with transient AKI, patients with persistent AKI had less preoperative eGFR (86 ± 18 vs 77 ± 18, p-value 0.02; OR 0.97, 95% CI 0.94-0.99, p-value 0.024), had greater AKI stage (stage 1 74% vs 67%, stage 2 26% vs 8%, stage 3 0% vs 25%, p-value <0.001; OR 5.7, 95% CI 2.7-11.9, p-value <0.001) and were more likely to be diagnosed according to both serum creatinine and diuresis KDIGO criteria (10% vs 33%, p-value 0.02; OR 2.9, 95% CI 1.3-6.7, p-value 0.009).
3.4. Postoperative Complications and Association with Kidney-Related Adverse Events
The most frequent postoperative complications were pulmonary (37%), followed by renal (32%), septic (18%), surgical (14%, with second surgery in 6%) and cardiovascular (11%). We had data on renal function at 3 months from surgery only in 47 patients: 2 patients (0.8% of the overall cohort and 2.4% of the AKI patients) were classified as having chronic kidney disease. The median lengths of stay were 1 day (IQR 1-2) and 12 days (IQR10-14) in ICU and in hospital, respectively. Intra-hospital mortality accounted for 0.8% of the overall population (2 patients), 1 patient (0.4%) died during ICU stay. Patients with postoperative AKI had greater risk of postoperative MACCE within 30 days from surgery (OR 2.51, 95%CI 1.14-5.56, p-value 0.021). No significant association was found between postoperative AKI and other medical or surgical complications. Although patients who developed AKI didn’t stay longer in hospital, patients who experienced persistent AKI were more likely to have increased length hospital stay (p-value 0.035).
Interestingly, patients who had persistent postoperative AKI had a higher risk of medical complications, such as MACCE (OR 4.14, 95% CI 1.05-15.8, p-value 0.036) and pulmonary complications (OR 3.67, 95% CI 1.04-14.9, p-value 0.050), with a significant effect on hospital length of stay (AME 7.2, 0.5-13.9, p-value 0.035). The complete analysis is presented in Supplementary file 1.
4. Discussion
4.1. Major Findings
In this monocentric retrospective study, the incidence of postoperative AKI after esophageal cancer surgery, as defined by serum creatinine and diuresis KDIGO criteria, was 32%. The only independent risk factor associated with postoperative AKI was BMI. The AKI episode was transient in the majority of the cases and did not affect length of hospital stay; nonetheless it was associated with 2-fold risk increase for MACCE within 30 days from surgery. Moreover, an AKI episode lasting more than 48 hours was not only associated with 4-fold risk increase for MACCE and 3-fold risk increase for pulmonary complications within 30 days from surgery, but it did increase the length of hospital stay by an average of 7 days.
4.2. Comparison with Previous Studies
There are few studies investigating the incidence of renal dysfunction exquisitely in patients undergoing elective esophageal cancer surgery. The incidence reported was variable, ranging from 1.3% to 35.3% [2,3,4,5,6,7]; with some studies, however, lacking the definition of renal dysfunction [2,4], and others using Acute Kidney Injury Network SCr criterion[3,5,7], or Risk, Injury, Failure, Loss and End-Stage kidney disease SCr criterion[6]. The population analysed in our study is similar to former studies[3,4,5,6,7] in terms of preoperative characteristics. Our study differs from the previous[3,4,5,6,7] by using KDIGO criteria, urine output and SCr for AKI diagnosis, and not only SCr. We also conducted the adjustment for SCr according to fluid balance (which reduced the possible underestimation of AKI incidence due to perioperative change in body water). Considering urine output as diagnostic criterion, we certainly increased the estimated incidence of AKI, including also those patients (substantially AKI stage 1 by urine output criterion only) who may have responded to multiple physiological perioperative factors, including volume status, relative or absolute hypotension and neurohormonal response to surgery. Similar to other previous studies[3,4,5,6,7], we found that BMI was a modifiable factor that was found to be associated with increased risk for AKI occurrence[3,7]. Unlike we found in our study, previous studies also showed that older age and elevated ASA status were associated with AKI development[3,6], as well as some intraoperative factors, like colloid use[3], fluid management[5], or duration of surgery[2]. Interestingly the choice of a totally invasive surgery was associated with increased risk for AKI, possibly because of more traumatic body injury with more inflammation or more difficult management of perioperative status, including fluid or pain management. We investigated the relevance of duration of renal insult, by distinguishing in transient and persistent postoperative AKI event. In line with Murphy et al study[7], in our population AKI was mostly transient and did not increase length of hospital stay, even though it was associated with 2-fold risk increase for major cardiovascular events within 30 days from surgery. Persistent AKI was a less frequent but frightening postoperative complication, which appeared to be associated with increased risk for MACCE, increased incidence of pulmonary complications with significant impact on length of hospital stay. It is now well-established that AKI is associated with increased morbidity and mortality, but in the perioperative settings data on short- and long-term outcomes are still limited. Few studies have shown a strong relation between AKI and cardiovascular, pulmonary complications or mortality in abdominal surgery [17,18,19], but none of them pointed out the relation between these complications and the duration of AKI event. From a pathophysiological perspective, in the perioperative period, the factors determining kidney dysfunction may be multiple and simultaneous, sustaining the perpetuation of AKI event. We should also keep in mind that major thoraco-abdominal surgery, like esophagectomy, stresses many organs at the same time. In this scenario, the renal insult may initiate or result from another organ dysfunction. The link between the kidney dysfunction and other organs’ dysfunction is conceptualized as organ crosstalk and may be at the basis of persistent postoperative AKI, this for example explains the relationship found between kidney dysfunction and cardio-pulmonary complications.
4.3. Limitations
Our results should be generalized carefully because the study was conducted in a single tertiary specialized cancer hospital. The retrospective nature of the study is the major limitation: the study lacks information on several variables of clinical relevance (notably neoadjuvant treatment, preoperative dysphagia, strategies to mitigate AKI). The study shows an association between persistent AKI and other postoperative complications, but the cause-effect relationship cannot be determined due to the retrospective analysis. Moreover, the limited number of events for mortality, limit the evaluation of association between AKI and in-hospital death from surgery. Unfortunately, the follow-up at 90 days for determining CKD association wasn’t available. We used the timeframe of 48 hours from surgery to diagnose postoperative AKI, instead of 7 days as suggested by the more recent Acute Dialysis Quality Initiative consensus published by Prowle et al[20]; on the other hand, the authors believed that using such a time limitation could also limit the error of including AKI events not necessarily associated with surgery.
5. Conclusions
In our study 32% of patients who underwent esophagectomy experienced postoperative AKI, which was transitory in the majority of them. However, postoperative AKI event lasting more than 48 hours was associated with increased risk of MACCE and pulmonary complications and increased the length of hospital stay. The factors found to be associated with increased risk for AKI development were BMI and totally invasive surgical approach.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. file S1.
Author Contributions
IG contributed to the design of the work, analysis and interpretation of data. PF and MV contributed to the design of the work and interpretation of data. AA, LM, GC, ESP, GZ and RS contributed to data collection. GL and DG contributed to the analysis of data. All authors substantially revised the study and approved the final manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was approved by Comitato Etico per la Sperimentazione Clinica della Provincia di Padova (protocol number 3073). The study is identified with the registration number NCT04773080.
Informed Consent Statement
Patient consent was waived due to the retrospective nature of the study.
Data Availability Statement
The datasets analyzed during the study are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- van Hagen, P.; Hulshof, M.C.; van Lanschot, J.J.; et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. The New England journal of medicine. 2012, 366, 2074–2084. [Google Scholar] [CrossRef] [PubMed]
- McCulloch, P.; Ward, J.; Tekkis, P.P.; et al. Mortality and morbidity in gastrooesophageal cancer surgery: initial results of ASCOT multicentre prospective cohort study. BMJ. 2003, 327, 1192–1197. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.H.; Kim, H.R.; Baek, S.H.; et al. Risk factors of postoperative acute kidney injury in patients undergoing esophageal cancer surgery. J Cardiothorac Vasc Anesth. 2014, 28, 936–942. [Google Scholar] [CrossRef] [PubMed]
- Moore, J.M.; Hooker, C.M.; Molena, D.; et al. Complex Esophageal Reconstruction Procedures Have Acceptable Outcomes Compared With Routine Esophagectomy. Ann Thorac Surg. 2016. [CrossRef] [PubMed]
- Konda, P.; Ai, D.; Guerra, C.E.; et al. Identification of Risk Factors Associated With Postoperative Acute Kidney Injury After Esophagectomy for Esophageal Cancer. J Cardiothorac Vasc Anesth. 2017, 31, 474–481. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Wang, T.; Feng, X.; Sun, L. Incidence and risk factors of acute kidney injury after esophageal cancer surgery: A nested case-control study. Int J Surg. 2017, 39, 11–15. [Google Scholar] [CrossRef] [PubMed]
- Murphy, C.F.; Dunne, T.; Elliott, J.A.; et al. Acute Kidney Injury After Esophageal Cancer Surgery: Incidence, Risk Factors, and Impact on Oncologic Outcomes [published online ahead of print, 2020 Jul 24]. Ann Surg. 2020. [CrossRef]
- Sam D. Gumbert, Felix Kork, Maisie L. Jackson, Naveen Vanga, Semhar J. Ghebremichael, Christy Y. Wang, Holger K. Eltzschig; Perioperative Acute Kidney Injury. Anesthesiology 2020, 132, 180–204. [CrossRef]
- Bihorac, A.; Yavas, S.; Subbiah, S.; Hobson, C.E.; Schold, J.D.; Gabrielli, A.; Layon, A.J.; Segal, M.S. Long-term risk of mortality and acute kidney injury during hospitalization after major surgery. Ann Surg. 2009, 249, 851–8. [Google Scholar] [CrossRef] [PubMed]
- Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int Suppl 2012, 1–138. [Google Scholar]
- Macedo, E.; Bouchard, J.; Soroko, S.H.; et al. Fluid accumulation, recognition and staging of acute kidney injury in critically-ill patients. Crit Care 2010, 14, R82. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; et al. A new equation to estimate glomerular filtration rate. Ann Intern Med 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Chawla, L.; Bellomo, R.; Bihorac, A.; et al. Acute kidney disease and renal recovery: consensus report of the Acute Disease Quality Initiative (ADQI) 16 Workgroup. Nat Rev Nephrol 2017, 13, 241–257. [Google Scholar] [CrossRef] [PubMed]
- 14 Jammer, I.; Wickboldt, N.; Sander, M.; Smith, A.; Schultz, M.J.; Pelosi, P.; Leva, B.; Rhodes, A.; Hoeft, A.; Walder, B.; Chew, M.S.; Pearse, R.M.; European Society of Anaesthesiology (ESA) and the European Society of Intensive Care Medicine (ESICM); European Society of Anaesthesiology; European Society of Intensive Care Medicine. Standards for definitions and use of outcome measures for clinical effectiveness research in perioperative medicine: European Perioperative Clinical Outcome (EPCO) definitions: a statement from the ESA-ESICM joint taskforce on perioperative outcome measures. Eur J Anaesthesiol. 2015, 32, 88–105. [Google Scholar]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Low, D.E.; Alderson, D.; Cecconello, I.; Chang, A.C.; Darling, G.E.; DʼJourno, X.B.; Griffin, S.M.; Hölscher, A.H.; Hofstetter, W.L.; Jobe, B.A.; Kitagawa, Y.; Kucharczuk, J.C.; Law, S.Y.; Lerut, T.E.; Maynard, N.; Pera, M.; Peters, J.H.; Pramesh, C.S.; Reynolds, J.V.; Smithers, B.M.; van Lanschot, J.J. International Consensus on Standardization of Data Collection for Complications Associated With Esophagectomy: Esophagectomy Complications Consensus Group (ECCG). Ann Surg. 2015, 262, 286–94. [Google Scholar] [CrossRef] [PubMed]
- Long, T.E.; Helgason, D.; Helgadottir, S.; Palsson, R.; Gudbjartsson, T.; Sigurdsson, G.H.; Indridason, O.S.; Sigurdsson, M.I. Acute Kidney Injury After Abdominal Surgery: Incidence, Risk Factors, and Outcome. Anesth Analg. 2016, 122, 1912–20. [Google Scholar] [CrossRef] [PubMed]
- Biteker, M.; Dayan, A.; Tekkeşin, A.İ.; Can, M.M.; Taycı, İ.; İlhan, E.; Şahin, G. Incidence, risk factors, and outcomes of perioperative acute kidney injury in noncardiac and nonvascular surgery. Am J Surg. 2014, 207, 53–9. [Google Scholar] [CrossRef] [PubMed]
- Gameiro, J.; Neves, J.B.; Rodrigues, N.; Bekerman, C.; Melo, M.J.; Pereira, M.; Teixeira, C.; Mendes, I.; Jorge, S.; Rosa, R.; Lopes, J.A. Acute kidney injury, long-term renal function and mortality in patients undergoing major abdominal surgery: a cohort analysis. Clin Kidney J. 2016, 9, 192–200. [Google Scholar] [CrossRef] [PubMed]
- Prowle, J.R.; Forni, L.G.; Bell, M.; et al. Postoperative acute kidney injury in adult non-cardiac surgery: joint consensus report of the Acute Disease Quality Initiative and PeriOperative Quality Initiative. Nat Rev Nephrol 2021, 17, 605–618. [Google Scholar] [CrossRef]
Figure 1.
Flowchart. AKI, acute kidney injury.
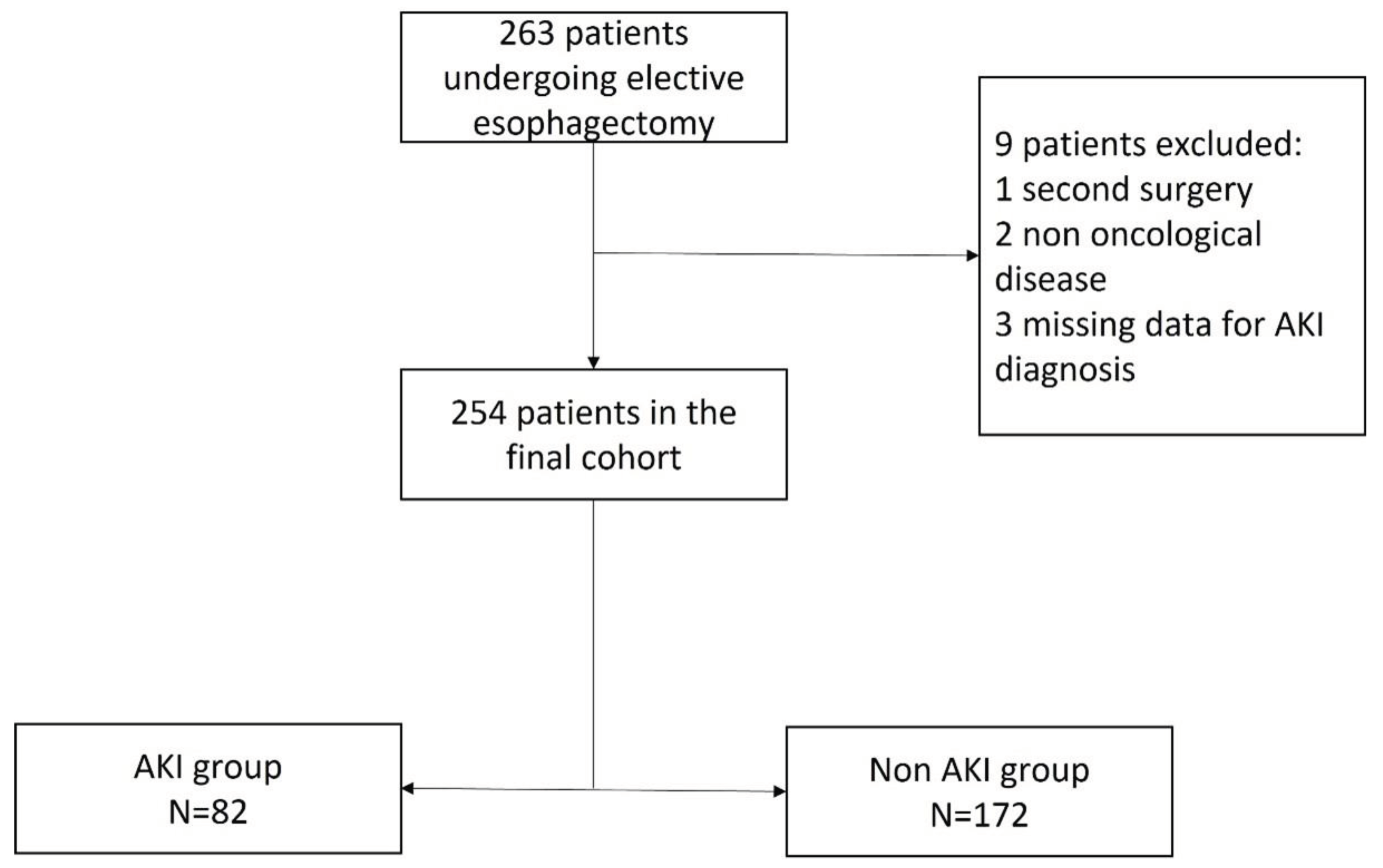
Figure 2.
Distribution of AKI according to Kidney Disease Improving Global Outcomes criteria and stages. AKI, acute kidney injury, AKI-KRT, acute kidney injury requiring kidney replacement therapy.
Figure 2.
Distribution of AKI according to Kidney Disease Improving Global Outcomes criteria and stages. AKI, acute kidney injury, AKI-KRT, acute kidney injury requiring kidney replacement therapy.
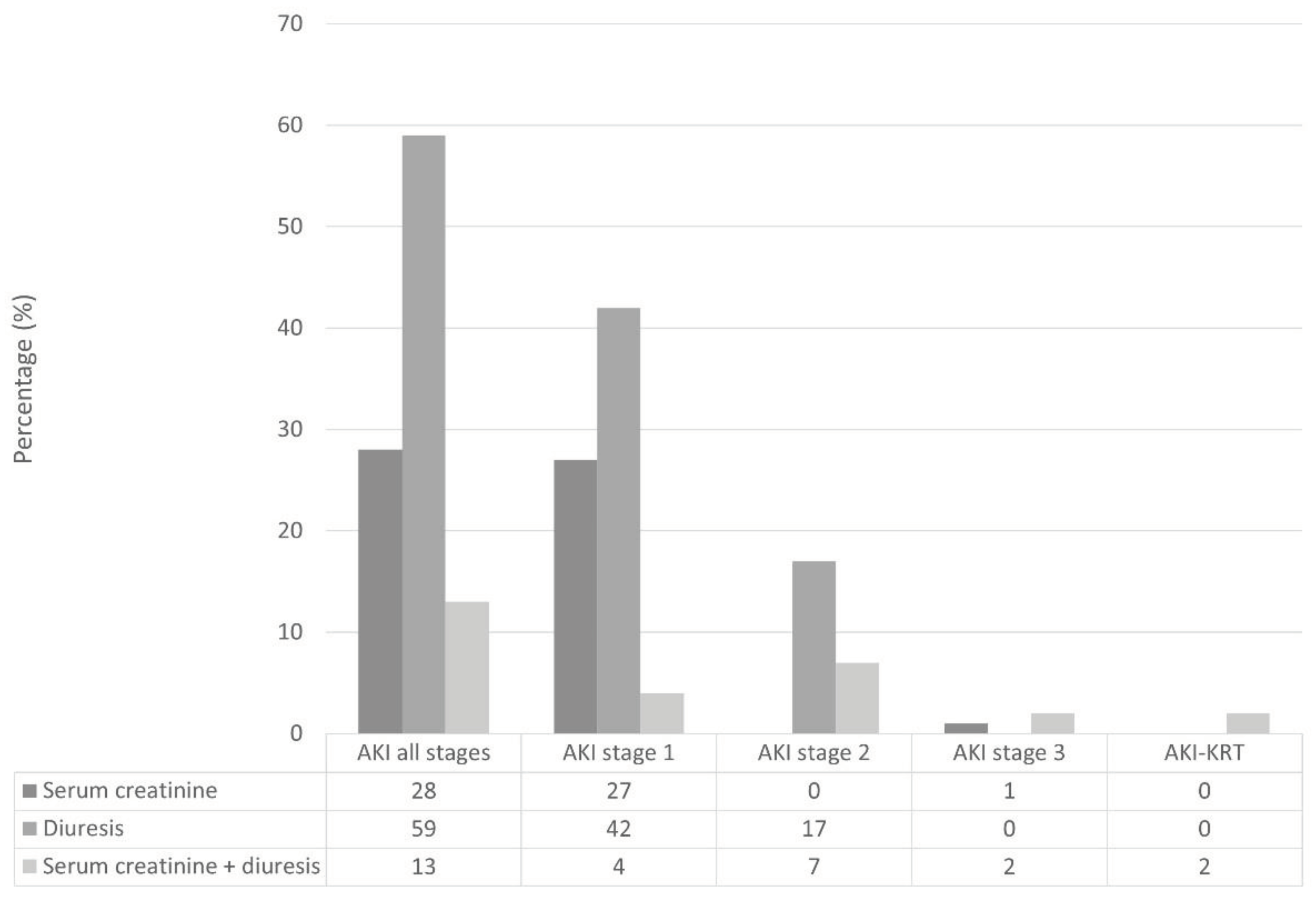

Table 1.
Preoperative and intraoperative characteristics. BMI, body mass index, ASA, American Society of Anesthesiology, COPD, chronic obstructive pulmonary disease, NSQIP, National Surgical Quality Improvement Program, SpO2/FiO2, ratio between peripheral saturation of oxygen and fractional inspired oxygen content.
Table 1.
Preoperative and intraoperative characteristics. BMI, body mass index, ASA, American Society of Anesthesiology, COPD, chronic obstructive pulmonary disease, NSQIP, National Surgical Quality Improvement Program, SpO2/FiO2, ratio between peripheral saturation of oxygen and fractional inspired oxygen content.
| Characteristic | N | Overall, N = 2541 |
Non-AKI, N = 1721 |
AKI, N = 821 |
| Age (years) | 254 | 66 (56, 72) | 65 (56, 71) | 66 (58, 73) |
| Gender | 254 | |||
| Male | 206 (81%) | 140 (81%) | 66 (80%) | |
| Female | 48 (19%) | 32 (19%) | 16 (20%) | |
| BMI (kg/h2) | 254 | 24.3 (22.4, 27.7) | 24.0 (22.0, 26.9) | 26.2 (23.1, 29.4) |
| Level of dependency | 254 | |||
| Independent | 247 (97%) | 168 (98%) | 79 (96%) | |
| Partially dependent | 7 (2.8%) | 4 (2.3%) | 3 (3.7%) | |
| ASA status | 254 | |||
| 1 | 1 (0.4%) | 1 (0.6%) | 0 (0%) | |
| 2 | 144 (57%) | 105 (61%) | 39 (48%) | |
| 3 | 106 (42%) | 64 (37%) | 42 (51%) | |
| 4 | 3 (1.2%) | 2 (1.2%) | 1 (1.2%) | |
| Chronic steroid use | 254 | |||
| No | 242 (95%) | 164 (95%) | 78 (95%) | |
| Yes | 12 (4.7%) | 8 (4.7%) | 4 (4.9%) | |
| Diabetes mellitus | 254 | |||
| No | 209 (82%) | 145 (84%) | 64 (78%) | |
| Yes | 45 (18%) | 27 (16%) | 18 (22%) | |
| Hypertension | 254 | |||
| No | 153 (60%) | 112 (65%) | 41 (50%) | |
| Yes | 101 (40%) | 60 (35%) | 41 (50%) | |
| Current smoker within 1 year | 254 | |||
| No | 206 (81%) | 133 (77%) | 73 (89%) | |
| Yes | 48 (19%) | 39 (23%) | 9 (11%) | |
| Severe COPD | 254 | |||
| No | 226 (89%) | 156 (91%) | 70 (85%) | |
| Yes | 28 (11%) | 16 (9.3%) | 12 (15%) | |
| NSQIP | 254 | 9.00 (8.00, 11.50) | 9.00 (8.00, 11.50) | 10.50 (8.00, 11.50) |
| Alohol use | 254 | |||
| No | 244 (96%) | 166 (97%) | 78 (95%) | |
| Yes | 10 (3.9%) | 6 (3.5%) | 4 (4.9%) | |
| Statins use | 254 | |||
| No | 208 (82%) | 142 (83%) | 66 (80%) | |
| Yes | 46 (18%) | 30 (17%) | 16 (20%) | |
| Angiotensin-converting-enzyme inhibitors use | 254 | |||
| No | 208 (82%) | 146 (85%) | 62 (76%) | |
| Yes | 46 (18%) | 26 (15%) | 20 (24%) | |
| Angiotensin-receptors blockers use | 254 | |||
| No | 223 (88%) | 156 (91%) | 67 (82%) | |
| Yes | 31 (12%) | 16 (9.3%) | 15 (18%) | |
| Beta blockers | 254 | |||
| No | 204 (80%) | 137 (80%) | 67 (82%) | |
| Yes | 50 (20%) | 35 (20%) | 15 (18%) | |
| Insulin use | 254 | |||
| No | 245 (96%) | 166 (97%) | 79 (96%) | |
| Yes | 9 (3.5%) | 6 (3.5%) | 3 (3.7%) | |
| Proton pump inhibitor use | 254 | |||
| No | 116 (46%) | 84 (49%) | 32 (39%) | |
| Yes | 138 (54%) | 88 (51%) | 50 (61%) | |
| Non-sterois-antinflammatory drugs use | 254 | |||
| No | 219 (86%) | 151 (88%) | 68 (83%) | |
| Yes | 35 (14%) | 21 (12%) | 14 (17%) | |
| Baseline serum creatinine (µmol/L) | 254 | 77 (67, 87) | 77 (66, 87) | 78 (69, 92) |
| Preoperative urea (mmol/L) | 230 | 5.55 (4.31, 7.00) | 5.60 (4.36, 6.88) | 5.50 (4.07, 7.53) |
| Estimated glomerular filtration rate (ml/min/1.73m2) | 254 | 90 (79, 100) | 92 (81, 101) | 88 (72, 98) |
| Preoperative hemoglobin (g/dL) | 248 | 12.90 (11.70, 13.80) | 12.80 (11.70, 13.80) | 12.90 (11.80, 13.70) |
| Preoperative white blood cell count (x109/L) | 210 | 5.71 (4.48, 7.30) | 5.66 (4.50, 6.98) | 6.03 (4.46, 7.60) |
| Preoperative platelet count (x104/µL) | 244 | 207 (165, 252) | 205 (168, 247) | 216 (164, 258) |
| Preoperative atrial fibrillation | 254 | |||
| No | 244 (96%) | 166 (97%) | 78 (95%) | |
| Yes | 10 (3.9%) | 6 (3.5%) | 4 (4.9%) | |
| Preoperative ejection fraction < 45% | 254 | |||
| No | 247 (97%) | 168 (98%) | 79 (96%) | |
| Yes | 7 (2.8%) | 4 (2.3%) | 3 (3.7%) | |
| Surgical technique | 254 | |||
| Mini-invasive | 39 (15%) | 33 (19%) | 6 (7.3%) | |
| Partially-invasive | 9 (3.5%) | 4 (2.3%) | 5 (6.1%) | |
| Totally-invasive | 206 (81%) | 135 (78%) | 71 (87%) | |
| Tri-incisional surgery | 254 | |||
| No | 241 (95%) | 161 (94%) | 80 (98%) | |
| Yes | 13 (5.1%) | 11 (6.4%) | 2 (2.4%) | |
| Type of anesthesia | 248 | |||
| Inhaled | 2 (0.8%) | 0 (0%) | 2 (2.5%) | |
| Totally intravenous | 23 (9.3%) | 16 (9.5%) | 7 (8.9%) | |
| Inhaled + epidural | 18 (7.3%) | 9 (5.3%) | 9 (11%) | |
| Totally intravenous + epidural | 205 (83%) | 144 (85%) | 61 (77%) | |
| Anesthesia duration (hours) | 251 | 6.00 (5.20, 7.20) | 6.00 (5.20, 7.20) | 6.05 (5.95, 7.00) |
| Intraoperative minimal SpO2/FiO2 | 248 | 120 (98, 155) | 120 (96, 158) | 120 (107, 155) |
| Intraoperative minimal systolic blood pressure (mmHg) | 247 | 100 (90, 100) | 100 (90, 100) | 100 (90, 110) |
| Intraoperative colloid use | 247 | |||
| No | 233 (94%) | 159 (95%) | 74 (94%) | |
| Yes | 14 (5.7%) | 9 (5.4%) | 5 (6.3%) | |
| Intraoperative blood loss (ml) | 246 | 150 (100, 200) | 100 (100, 200) | 200 (100, 215) |
| Intraoperative blood transfusion | 247 | |||
| No | 233 (94%) | 161 (96%) | 72 (91%) | |
| Yes | 14 (5.7%) | 7 (4.2%) | 7 (8.9%) | |
| Intraoperative volume infused (ml/kg/h) | 247 | 9.26 (7.68, 10.72) | 9.50 (7.67, 11.13) | 8.70 (7.74, 10.15) |
| End of surgery hemoglobin level (mg/dL) | 241 | 12.00 (11.00, 13.10) | 12.00 (11.10, 13.20) | 12.00 (10.90, 12.80) |
| End of surgery lactate level (mmol/L) | 74 | 1.16 (0.99, 1.78) | 1.10 (0.88, 2.03) | 1.25 (1.06, 1.65) |
| Intraoperative vasopressor use | 247 | |||
| No | 231 (94%) | 158 (94%) | 73 (92%) | |
| Yes | 16 (6.5%) | 10 (6.0%) | 6 (7.6%) | |
| Intraoperative inotrope use | 247 | |||
| No | 230 (93%) | 157 (93%) | 73 (92%) | |
| Yes | 17 (6.9%) | 11 (6.5%) | 6 (7.6%) | |
| Intraoperative arrhytmya | 248 | |||
| No | 242 (98%) | 166 (98%) | 76 (96%) | |
| Yes | 6 (2.4%) | 3 (1.8%) | 3 (3.8%) | |
| End of surgery diuresis (ml/kg/h) | 246 | 1.14 (0.76, 1.75) | 1.20 (0.81, 1.77) | 1.01 (0.63, 1.65) |
| Intraoperative use of diuretics | 248 | |||
| No | 223 (90%) | 154 (91%) | 69 (87%) | |
| Yes | 25 (10%) | 15 (8.9%) | 10 (13%) | |
| Intraoperative use of non-steroid-anti inflammatory drugs | 248 | |||
| No | 129 (52%) | 95 (56%) | 34 (43%) | |
| Yes | 119 (48%) | 74 (44%) | 45 (57%) | |
| End of surgery extubation | 253 | |||
| No | 117 (46%) | 80 (47%) | 37 (46%) | |
| Yes | 136 (54%) | 92 (53%) | 44 (54%) | |
| Intraoperative acute kidney injury | 246 | |||
| No | 219 (89%) | 153 (92%) | 66 (84%) | |
| Yes | 27 (11%) | 14 (8.4%) | 13 (16%) | |
| 1Median (IQR); n (%) | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



