
Submitted:
22 February 2024
Posted:
22 February 2024
You are already at the latest version
Abstract
Dental pulp chamber volume is a fundamental measurement in the field of endodontics, but also in forensic sciences, teaching and training, or tissue engineering. This study evaluates the precision of cone beam computed tomography (CBCT) in comparison with computed micro-tomography (micro-CT) in evaluating pulp chamber volume of upper central incisors ex vivo. The intra-operator and inter-operator error were evaluated, and the results for the two techniques were compared with a T-test for paired samples. Intra-operator and inter-operator errors were >0.05, indicating an adequate reproducibility in each operator and no significant differences between their meas-urements. On the other hand, no significant differences between the two measurement techniques. The present results demonstrate that CBCT is a precise, feasible and reproducible technique for evaluation of dental pulp chamber volume ex vivo. Results provided with this method are suitable for different medical branches but also for teaching and training of undergraduate and post-graduate students. Furthermore, the findings of this study carry significant clinical implications, as accurate assessment of pulp chamber volume is critical in the diagnosis and treatment of various endodontic conditions. The ability of CBCT to provide reliable 3D dental anatomy measurements can enhance the planning of endodontic treatments by allowing for a better understanding of internal tooth morphology. Additionally, the precision and reproducibility of CBCT in assessing pulp chamber volume can contribute to improved clinical outcomes and reduced complications during endodontic procedures. These findings further support the increasingly vital role of CBCT in modern clinical practice and underscore its value as an indispensable tool in the field of dentistry.
Keywords:
Cone beam computed tomography
; Computed micro-tomography
; Dental pulp chamber volume.
1. Introduction
Determining dental pulp chamber anatomy and volume is an important goal in dentistry, as they provide information that consent correct diagnosis, treatment-planning for several dental pathologies, and helps to monitor cases over time [1]. In this context, computed micro-tomography (micro-CT) is currently regarded as the gold standard technique for studying root canal anatomy and apical foramens, evaluate volumetric pulp space, and follow-up interventions [2,3,4,5]. However, several factors limit the use of micro-CT in dentistry daily practice. They include the high price of the device and equipment as well as data analysis software. Also, the use of micro-CT is not possible in medical practice because the long time needed for scanning and digital reconstruction. Moreover, due to volume limitations, micro-CT do not consent to scan the full head of a living person but is restricted to extracted teeth or jaw segments containing teeth, and any case is only used in studies ex vivo [3,6,7].
Recently, it has been reported that small field cone-beam computed tomography (CBCT) consent to obtain good quality teeth three-dimensional images adequately at low levels of radiation without superimposing neighbouring anatomical structures. CBCT has been incorporated into clinical practice in a variety of clinical disciplines including Periodontics, Oral and Maxillofacial Surgery, Implantology, and Forensic Dentistry [7,8,9]. Importantly, in Endodontics, it has been used to identify the number of root canals with great accuracy [10], and its use is particularly relevant in the diagnosis of dental fracture and resorption [6]. In fact, the numbers of images captured by CBCT now surpass the use of classical digital radiology in dentistry diagnosis and treatment planning [7].Although the images obtained with CBCT would appear to offer high precision in all spatial planes, assessments of their reliability and accuracy have been few [3]. The variables studied have included measurements of the areas and diameters of root canals [6], linear measurements on digital models [11], linear measurements in the field of implant dentistry [8], calculations of dental volumes [1] or assessment of volumetric distortion artifact in endodontically treated teeth [12], CBCT is also used to made measurements of pulp chamber volumes and to estimate age. In fact, dental-age estimation in living individuals as well as in cadavers is one of the most frequent requests undertaken by forensic odontologists. It is well known that ageing is accomplished of formation of secondary dentine and consistently the reduction in tubular lumen diameter leading to a reduction in the volume of the pulp chamber [13,14,15,16,17]. Indeed, measurements of the pulp chamber are necessary in preparing 3D models to be used as scaffolds for in vitro pulp reconstruction [18,19,20]. Importantly, CBCT is also a good tool to create realistic tooth models for preclinical teaching and training to endodontic postgraduates [21,22,23,24]. Nevertheless, although CBCT images have a high precision in all spatial planes, studies analysing their reliability and accuracy are scarce, and when used to evaluate dental pulp chamber underestimation or overestimation of measurements were identified [8,12,25].
In the last years, it has been reported the use CBCT to determine the volume of the dental pulp chamber but, as far as we know, studies corroborating its accuracy and reproducibility are not available. Thus, this study was designed to validate the precision CBCT by comparing pulp chamber volume measurements ex vivo obtained with Promax® 3D Max CBCT and those obtained with micro-CT. A recent study by Maddalone et al. [26] concluded that CBCT is suitable for pulp chamber morphology evaluation with limitations in detecting the anatomical variability of small branches in root canal system.
The present study aimed to assess the dimensions of the pulp chamber of the upper central incisors using CBTC images from ex vivo teeth, evaluating the precision and reproducibility of this method in assessing pulp chamber volume.
2. Materials and Methods
2.1. Sample Selection
Thirty upper central incisors were used in this study. The material was collected from the Dental Clinic of the Universidad CEU Cardenal Herrera in Valencia (Spain) and was extracted for periodontal reasons. Patient informed consent was obtained prior to sample collection. The pieces showed closed apices and no major destructions. Teeth presenting any anatomical abnormality, internal or external resorption, prosthetic or orthodontic restoration, or endodontic treatment were excluded [11,27]. After extraction, the pieces were disinfected with 5% sodium hypochlorite for 2 hours, and then stored at 40 C in distilled water until use. The study was approved by the Ethical Committee at Cardenal Herrera University (Valencia, Spain; Reg. No. CEI19/089).
2.2. CBCT Study
For image acquisition the teeth were placed on a silicone impression putty base (Express 2 Putty Quick, 3M ESPE), in groups of ten, and were scanned using the Promax® 3D Max CBCT unit (Planmeca Inc, Roselle, IL, USA). The images generated were captured applying the following parameters: a field of view of 8 x 5 cm, 120KV, 8 mA and voxel size of 0.2mm, according [28]. The imaging time was 8.03 seconds, and data were reconstructed at a slice interval of 1mm. CBCT images were stored in Digital Imaging and Communication in Medicine format (DICOM). Then, two researchers (dentists with over 10 years of experience), independently took measurements of pulp chamber volume using Planmeca Romexis software (version 5.3.4.39).
The process was carried out twice, separated by an interval of 15 days. Intra- and inter-examiner errors were calculated since pulp chamber volume measurement is subject to an element of subjectivity, as the operator must select the area to be measured. Pulp camber volume was obtained using the grid tool to measure volumes automatically using the grayscale threshold as previous studies [29]. For each tooth, a start point was selected from which the 3D region growing tool was set to the option “root cavity.” A 3D model was generated, and the pulp volume measured in cm3 (Figure 1).
2.3. Micro-CT Study
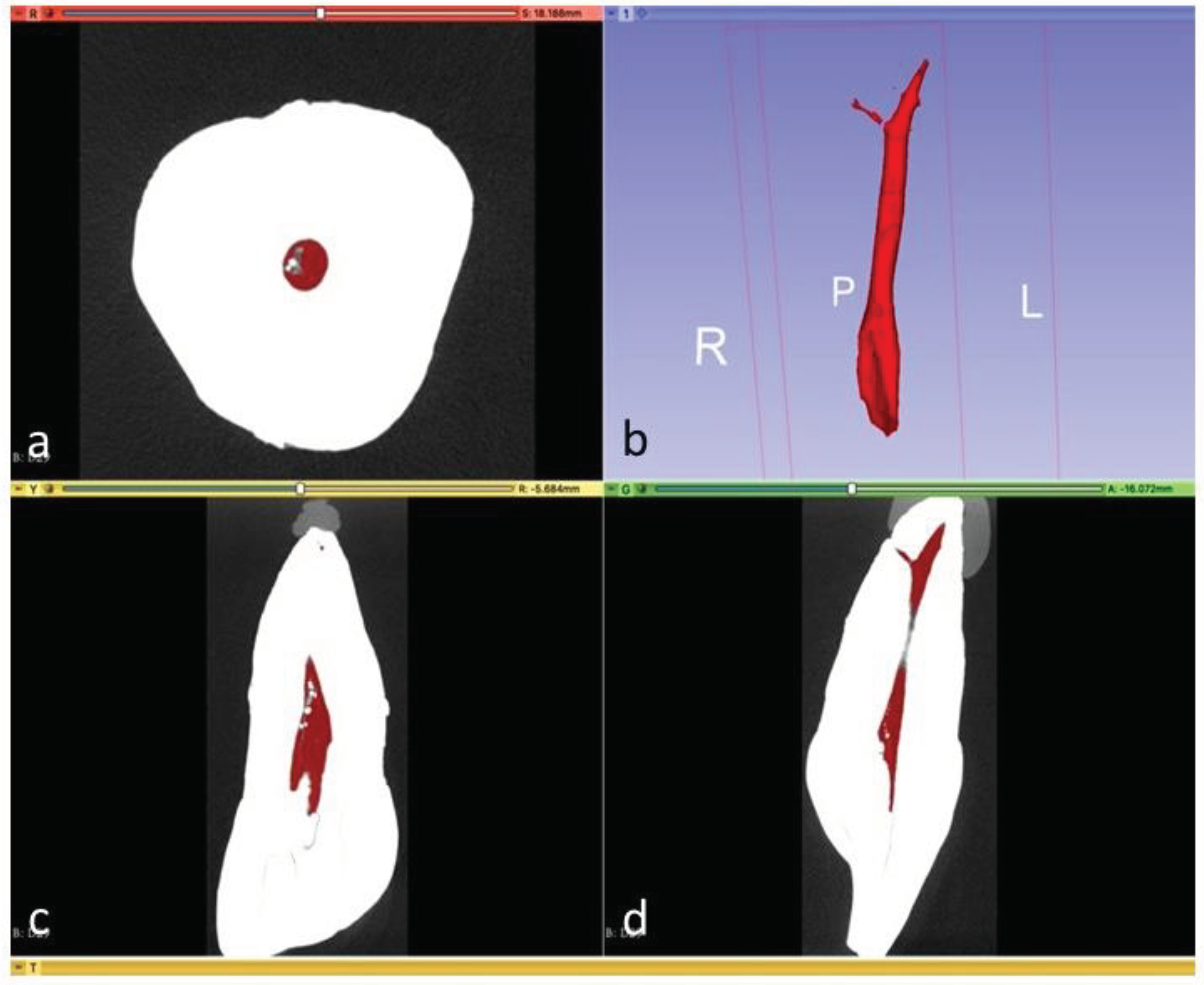
The same pieces were then analysed with micro-CT. The study was carried out at Centro Nacional de Investigación sobre la Evolución Humana (CENIEH; National Center for Human Evolution) Burgos, Spain, using a micro-CT (Phoenix VltomelXs240, GE Sensing & Inspection Technologies Phoenix X Ray, Wunstorf, Germany). The scanning conditions were set at 120 kV, 120 µA, 0.2-mm Cu filter, 19 µm voxel size, and 0.2 step rotation. To minimize ring artifacts, air calibration of the detector was performed before scanning. Each sample was rotated 360º within an integration time of 2 seconds. Mean scanning time was approximately 1 hour. Thereafter, data were exported in DICOM format and pulp volumes were calculated with 3D Slicer software (version 4.10.2). Segmentation was performed using the grayscale threshold tool, differentiating coronal dentin from root cementum. An examiner trained in the software was blinded for segmentation, evaluating the three planes simultaneously (axial, sagittal and coronal), eliminating all calcifications found throughout the pulp from coronal to apical areas. The process took between 45 min to 3 hours per tooth. 3D models were generated, measuring pulp volume in mm3 automatically. Phoenix datos/x 2 reconstruction and 3D Slicer software were used for root canal visualization and reconstruction. For reconstruction, a median filter was applied, and the beam-hardening correction was set at 80%. Contrast limits were applied automatically following the GE micro-CT manufacturer’s instructions. 3D Slicer software was used to visualize 3D volumes and to measure root canal volume (Figure 2).
2.4. Statistical Analysis
The consistency and reliability of the measurements was evaluated by the two investigating dentists to reduce bias and improve the validity of the results.
Firstly, the mean (average) of measurements taken by two different operators was calculated to reduce the potential for bias that might be associated with individual operator measurements. Statistical Package for the Social Sciences (SPSS) version 22.0 for Windows (IBM, Chicago, IL, USA) was used for the analysis, and descriptive analyses involved calculating means and standard deviations of the measurements.
Normal distribution was assessed for both micro-CT and CBCT volume measurement using the Kolmogorov-Smirnov (KS) test. This is a type of statistical test used to assess whether a dataset follows a specific probability distribution, such as a normal or Gaussian distribution. The test compares the empirical distribution of the observed data with the theoretical distribution expected under the null hypothesis that the data follow the specified distribution. If the p-value associated with the test is greater than a predefined threshold (commonly 0.05), there is not enough evidence to reject the null hypothesis, suggesting that the data may follow the specified distribution.
The test compares the empirical cumulative distribution of the data with the expected cumulative distribution under the null hypothesis. The p-values reported for both tests were 0.20, suggesting that the data did not deviate significantly from a normal distribution, i.e. they do not provide sufficient evidence to reject the null hypothesis at the 0.05 significance level (commonly used threshold). The significance level represents the probability of making a type I error of incorrectly rejecting a true null hypothesis. A lower significance level reduces the probability of making Type I errors, but may increase the probability of making Type II errors, of failing to reject a false null hypothesis. Therefore, the significance level should consider the nature of the problem, the practical implications, and the risk tolerance for statistical errors.
The KS test is used as a goodness-of-fit test, assessing the extent to which the sample data fit a specified theoretical distribution. It is also particularly effective in detecting differences between the observed data and the expected distribution in the tails of the data set, providing a comprehensive assessment of the entire distribution.
Student's t-test was performed to compare the means of the two groups. In the context of paired data, such as data before and after a treatment, or data from two matched groups like those obtained by two different operators, the t-test is used to determine if there is a significant difference between the means of the two groups or simply the result of chance. The p-value associated with the test indicates the probability of obtaining results as extreme as those observed if the true difference between the group means is zero. If the p-value is less than a predefined threshold (usually 0.05), there is considered to be a statistically significant difference between the means of the two groups.
This comparation was possible because the data follow a normal distribution and the variances of the two groups are approximately equal (homoscedasticity). The p-value associated with Fisher's test is 0.586, suggesting that there is no significant evidence to reject the null hypothesis of equal variances. In addition, the paired samples t-test has been performed to compare the means of the two related data sets and to assess whether there is a significant difference between the two measurement conditions, assuming normality of the differences and homogeneity of the variances. A significance level for the t-test of 0.05 has been chosen.
3. Results
The pulp volume of the 30 teeth ex vivo was obtained using CBCT and micro-CT images. Next the measurements were compared to verify whether the CBCT was an accurate tool in determining dental pulp volume.
As during the procedure, the operator had to select the area to be measured and this is subject to an element of subjectivity, intra- and inter-examiner errors were calculated.
The intra-operator error calculated reached a value of 0.183 for the first operator and 0.632 for the second operator. In this case, low values suggest adequate reproducibility or consistency in the measurements made by each operator, that is, measurements can be repeated consistently, even when performed by different operators.
Furthermore, Student’s t-test for paired samples obtained p-values higher than 0.05 (0.375 for operator 1 and 0.330 for operator 2), meaning there are no significant differences between the measurement values in either of the operators (Table A1).

Table 1.
Differences in operators’ measurements and comparison between measurements taken with CBCT and micro-CT.
Table 1.
Differences in operators’ measurements and comparison between measurements taken with CBCT and micro-CT.
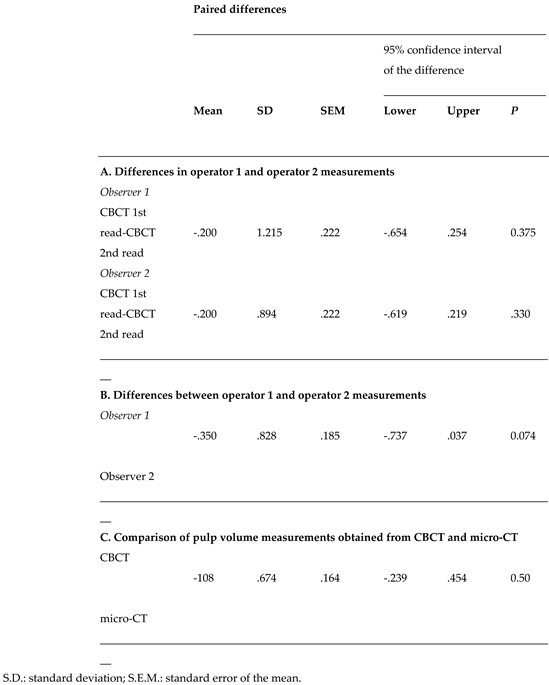
The inter-operator error between operators 1 and 2 is 0.883, and the Student’s t-test for paired samples obtained a p-value of 0.074>0.05. Based on the results of this test, it is concluded that there are no statistically significant differences between the measurements made by operators 1 and 2. Although there is an error between them (0.883), this error is not large enough to consider that the measurements differ significantly. The consistency between operators is supported by the non-significant t-test result (Table B1).
When comparing the measurements taken with CBCT and micro-CT, the error between instruments is 1.0061. This was calculated by taking the averages of the measurements obtained with CBCT by both operators and comparing them with the micro-CT measurements. Student’s t-test for paired samples obtained a p-value of 0.520>0.05, meaning that no statistically significant differences were identified between CBCT and micro-CT pulp volume measurements (Table C1).
According to the results of the Student's t-test, no statistically significant differences were found between the pulp volume measurements obtained by CBCT and micro-CT. This suggests that both methods are comparable in terms of measuring pulp volume and that there is no significant difference in the measurements between the two methods evaluated.
4. Discussion
The present study was designed to validate de use of CBCT for measurement of the human teeth pulp chamber volume using upper central incisors as a model. We compared the results of CBCT images with obtained with micro-CT, which is regarded as the gold standard to study the pulp chamber. We choose upper central incisors, as previously Porto et al. [27], since they are shorter than canines, have wider pulp chambers than lower incisors and their root anatomy is simpler than that of molars and premolars. Furthermore, volumetric measurements in multirooted teeth are less precise. Our results demonstrate that CBCT is superimposable to micro-CT to evaluate dental pulp chamber when evaluators have an appropriate training. Also, we support the idea that micro-CT is crucial in studies that evaluate the precision of measurements obtained with CBCT [30]. So, it may be assumed that CBCT achieves high precision and reproducibility for evaluation of pulp camber volume ex vivo. Nevertheless, measurements made on CBCT images have some troubles and it was observed that CBCT generated larger measurements that micro-CT, and different values can be obtained with different CBCT devices [25,31]. To the best of our knowledge, this is the first study that compare both techniques in the evaluation of pulp chamber volume. It was used earlier to evaluate root canals [6,10].
To know the anatomy and dimensions of the root canals and pulp chamber has interest for several branches of dentistry. First, for diagnostic and treatment in the field of endodontics [32] facilitating operative sequences when it comes to choosing the most appropriate type of obturation, or in guided root canal treatment [33]. Furthermore, CBCT is also useful to estimate age calculating pulp chamber volumes since there is an age-related reduction of the pulp chamber due to deposition of secondary dentin [17]. The measurement of pulp volume is of particular interest as it can be used to estimate the chronological age of a living or deceased human. Various ways of determining the age of an individual are available depending on the subjects’ age group. In individuals aged up to 24 years, age can be estimated on the basis of dental eruption and the extent of dental development. But once third molar maturation has taken place in adulthood, this becomes much more complex [16]. One of the characteristics that can be investigated to determine age is the decreasing size of the pulp cavity. Secondary dentin is deposited on the pulp cavity walls throughout an individual’s life, reducing its size; so, pulp volume is indicative of age in adults [28].
The precise knowledge of the pulp chamber volume is also a key factor in preparing 3D scaffolds tissue engineering for regeneration of the dental pulp [18,19,20,34]. But another important application of the CBCT generated images in dentistry is in preclinical teaching and training of endodontic postgraduates. A need for realistic tooth models for education has often been expressed by dental students. 3D-printed replicas of teeth have been proposed for creation of realistic macro-models to study anatomical details for use in preclinical dental education as alternatives to the study of extracted human teeth [23,35]. 3D printing technology offers new possibilities to dental schools by creating their own customized teaching models according to the specific curricula [36]. On the other hand, 3D models are optimal to study in detail root canal anatomy and the ideal access cavity, therefore for endodontic education both during preclinical courses before and during training [21,22,24,36]. So, based on present results of CBCT models of the different teeth could be made to study the morphology and dimensions of the dental cavities for educational and training purposes.
The objective of this study was to compare pulp volume measurements obtained by means of CBCT and micro-CT in order to confirm the precision of cone beam computed tomography for measuring this variable. The results did not present statistically significant differences between the two measurement techniques, so it may be assumed that CBCT achieves high precision and reproducibility when calculating pulp volume ex vivo. To the best of our knowledge, the literature does not include any study that has made this comparison.
Micro-CT was the reference standard for the study. Its precision when studying small volume structures, such as reduced pulp chambers and mineralized pulp tissue has already been satisfactorily assessed in literature [29]. Currently the use of micro-CT is considered crucial in studies that evaluate the precision of measurements obtained with CBCT [30].
Although recent studies have recommended the use of CBCT to assess root canals [6,10] the literature also describes imprecisions in its measurements. Among the researchers who have set out to validate CBCT as a measurement tool, Celikten et al. studied volumetric distortion in 30 endodontically treated lower incisors, comparing measurements taken from micro-CT and CBCTs with a voxel size of 200 microns. It was concluded that there were differences between the two sets of measurements whereby CBCT generated larger measurements. Differences were also found between different types of CBCT, with greater variations found with Promax 3D Max (PlanmecaInc, Roselle, IL, USA) than NewTom VGi evo (NewTom, Verona, Italy) [25]. This could be due to the presence of intracanal high density materials which could decrease the quality of the image. This is observed in the study by Møller et al. when comparing CBCT and micro-CT images in the search of voids within the guttapercha-filled canals. False-positives where found in the CBCT images, so the authors do not recommend CBCT for the assessment of the quality of the obturation of root canals [31]. In the present work the root canals analysed are intact, thus reducing the number of artefacts that could affect the precision of the measurements.
Our study has some limitations, including the size of the sample although it was similar to the studies of Grande et al. [37] or Domark et al. [7]. Furthermore, our study was performed ex vivo, which could make CBCT volumetric measurements more imprecise due to superimposed structures [8]. It must be added that measurements have only been taken with one type of CBCT, Promax 3D Max CBCT unit, and that the results could be different when using other brands. Voxel size is another parameter that is modifiable, and which influences measurement accuracy [28,38]. Maret et al. (2012) scanned 70 teeth, taking volume measurements by means of CBCT set at different voxel sizes (200, 300 and 74 microns) and micro-CT (at 41 microns). It was found that with a voxel size of 300 microns, measurements were significantly smaller [28]. In 2014, Maret et al. also compared geometric measurements between 37 dental reconstructions using CBCT with different voxel sizes and micro-CT. Images were placed on the same plane, and differences were identified using a color map; it was found that maximum differences occurred at cervical margins, cusp tips, and incisal edges. It was concluded that a voxel size of 200 microns or smaller should be used for studying dental anatomy [38]. This was the size used in the present study.
In conclusion, CBCT Promax 3D Max CBCT unit has proven to be a precise and reproducible tool in the ex vivo measurement of the pulp volume of root canals in nonendodontically treated incisors. Furthers studies are necessary to using other brands of CBCT and other dental groups. Studies are in progress in our laboratory to definitively validate CBCT for volume measurements in different teeth and using different CBCT devices.
5. Conclusion
This study demonstrated that cone-beam computed tomography (CBCT) is a precise and reproducible tool for the ex vivo evaluation of dental pulp chamber volume. The results showed no statistically significant differences between volume measurements obtained by CBCT and micro-CT. Additionally, it was found that the measurements can be consistently replicated, even when performed by different operators.
The significance of the study lies in the validation of CBCT for measuring pulp chamber volume, which has significant implications in various branches of dentistry. This includes diagnosis and treatment in endodontics, age estimation through pulp chamber volume calculation, or the preparation of 3D models for creating realistic dental models for teaching and preclinical training. Furthermore, this study lays the groundwork for future research utilizing different CBCT brands and different dental groups.
An interesting fact that emerges from the present study is that dental students should be trained in the management of CBTC and the interpretation of images obtained with this method. The possibility of obtaining three-dimensional images with CBTC facilitates the knowledge of the anatomy of the pulp chamber and consequently will facilitate clinical actions on it in the future.
Funding
This study was supported by a grant from Cardenal Herrera University for clinical research development (ICLINIC19/05).
Institutional Review Board Statement
This study was approved by the Ethical Committee for Biomedical Research of the Cardenal Herrera University, Valencia, Spain (Reg. No. CEI19/089).
Informed Consent Statement
This study was approved by the Ethical Committee for Biomedical Research of the Cardenal Herrera University, Valencia, Spain (Reg. No. CEI19/089).
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
The authors thank D. José Joaquín Alcaina Acosta for his valuable assistance in micro-CT images analysis and Prof. Elisabet Palazón Radford for valuable assistance in language revision.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Liu, Y., Olszewski, R., Alexandroni, E.S., Enciso, R., Xu, T., Mah, J.K., 2010. The validity of in vivo tooth volume determinations from cone-beam computed tomography. Angle Orthod. 80, 160-6. [CrossRef]
- Nielsen, R.B., Alyassin, A.M., Peters, D.D., Carnes, D.L., Lancaster, J., 1995. Microcomputed tomography: an advanced system for detailed endodontic research. J. Endod. 21: 561-8. [CrossRef]
- Rhodes, J.S., Ford, T.R., Lynch, J.A., Liepins, P.J., Curtis, R.V., 1999. Micro-computed tomography: a new tool for experimental endodontology. Int. Endo. J. 32, 165-70. [CrossRef]
- Park, J.W., Lee, J.K., Ha, B.H., Choi, J.H., Perinpanayagam, H., 2009. Three-dimensional analysis of maxillary first molar mesiobuccal root canal configuration and curvature using microcomputed tomography. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 108, 437-42. [CrossRef]
- Liang, X., Zhang, Z., Gu, J., Wang, Z., Vandenberghe, B., Jacobs, R., Yang, J., Ma, G., Ling, H., Ma, X., 2017. Comparison of micro-CT and cone beam CT on the feasibility of assessing trabecular structures in mandibular condyle. Dentomaxillofac. Radiol. 46: 20160435. [CrossRef]
- Michetti, J., Maret, D., Mallet, J.P., Diemer, F., 2010. Validation of cone beam computed tomography as a tool to explore root canal anatomy. J. Endod. 36, 1187-1190. [CrossRef]
- Domark, J.D., Hatton, J.F., Benison, R.P., Hildebolt, C.F., 2013. An ex vivo comparison of digital radiography and cone-beam and micro computed tomography in the detection of the number of canals in the mesiobuccal roots of maxillary molars. J. Endod. 39, 901-905. [CrossRef]
- Fokas, G., Vaughn, V.M., Scarfe, W.C., Bornstein, M.M., 2018. Accuracy of linear measurements on CBCT images related to presurgical implant treatment planning: A systematic review. Clin Oral Implants Res. 29, 393-415.
- Asif, M.K., Nambiar, P., Mani S.A., Ibrahim, N.B., Khan, I.M., Lokman, N.B., 2019. Dental age estimation in Malaysian adults based on volumetric analysis of pulp/tooth ratio using CBCT data. Leg. Med. 36, 50-8. [CrossRef]
- Zhang, D., Chen, J., Lan, G., Li, M., An, J., Wen, X., Liu, L., Deng, M., 2017. The root canal morphology in mandibular first premolars: a comparative evaluation of cone-beam computed tomography and micro-computed tomography. Clin Oral Investig. 21, 1007-1012. [CrossRef]
- Creed, B., Kau, C.H., English, J.D., Xia, J.J., Lee, R.P., 2011. A Comparison of the Accuracy of Linear Measurements Obtained from Cone Beam Computerized Tomography Images and Digital Models. Semin Orthod. 17, 49-56. [CrossRef]
- Gulsahi, A., Kulah, C.K., Bakirarar, B., Gulen, O., Kamburoglu, K., 2018. Age estimation based on pulp/tooth volume ratio measured on cone-beam CT images. Dentomaxillofac. Radiol. 47, 20170239. [CrossRef]
- Ge, Z.P., Yang, P., Li, G., Zhang, J.Z., Ma, X.C., 2016. Age estimation based on pulp cavity/chamber volume of 13 types of teeth from cone beam computed tomography images. Int. J. Legal Med. 130, 1159-67. [CrossRef]
- Orhan, A.I., Orhan, K., Ozgul, B.M., Öz, F.T., 2015. Analysis of pulp chamber of primary maxillary second molars using 3D micro-CT system: an in vitro study. Eur. J. Paediatr. Dent. 16: 305-10. [CrossRef]
- Pinchi, V., Pradella, F., Buti, J., Baldinotti, C., Focardi, M., Norelli, G.A., 2015. A new age estimation procedure based on the 3D CBCT study of the pulp cavity and hard tissues of the teeth for forensic purposes: A pilot study. J. Forensic. Leg. Med. 36,150-7. [CrossRef]
- Biuki, N., Razi, T., Faramarzi, M., 2017. Relationship between pulp-tooth volume ratios and chronological age in different anterior teeth on CBCT. J. Clin. Exp. Dent. 9, E688-693. [CrossRef]
- Zheng, Q., Ge, Z., Du, H., Li G., 2021. Age estimation based on 3D pulp chamber segmentation of first molars from cone-beam-computed tomography by integrated deep learning and level set. Int. J. Legal. Med. 135, 365-373. [CrossRef]
- Itoh, Y., Sasaki, J.I., Hashimoto, M., Katata, C., Hayashi, M., Imazato, S., 2018. Pulp Regeneration by 3-dimensional Dental Pulp Stem Cell Constructs. J Dent Res. 97,1137-43. [CrossRef]
- Ma, Y., Xie, L., Yang, B., Tian, W., 2019. Three-dimensional printing biotechnology for the regeneration of the tooth and tooth-supporting tissues. Biotechnol Bioeng. 116, 452-68. [CrossRef]
- Hadjichristou, C., About, I., Koidis, P., Bakopoulou, A., 2021. Advanced in Vitro Experimental Models for Tissue Engineering-based Reconstruction of a 3D Dentin/pulp Complex: A Literature Review. Stem Cell Rev. Rep. 17, 785-802. [CrossRef]
- Zehnder, M.S., Connert, T., Weiger, R., Krastl, G., Kühl, S., 2016. Guided endodontics: accuracy of a novel method for guided access cavity preparation and root canal location. Int. Endod. J. 49, 966-92. [CrossRef]
- Anderson, J., Wealleans, J., Ray. J., 2018. Endodontic applications of 3D printing. Int. Endod. J. 51: 1005-18. [CrossRef]
- Höhne, C., Schmitter, M., 2019. 3D Printed Teeth for the Preclinical Education of Dental Students. J. Dent. Educ. 83,1100-6. [CrossRef]
- Hanafi, A., Donnermeyer, D., Schäfer, E., Bürklein, S., 2020. Perception of a modular 3D print model in undergraduate endodontic education. Int. Endod. J. 53, 1007-16. [CrossRef]
- Celikten, B., Jacobs, R., deFaria Vasconcelos, K., Huang, Y., Nicolielo, L.F.P., Orhan, K., 2017. Assessment of Volumetric Distortion Artifact in Filled Root Canals Using Different Cone-beam Computed Tomographic Devices. J. Endod. 43, 1517-1521. [CrossRef]
- Maddalone, M., Citterio, C., Pellegatta, A., Gagliani, M., Karanxha, L., Del Fabbro, M., 2020. Cone-beam computed tomography accuracy in pulp chamber size evaluation: An ex vivo study. Aust. Endod. J. 46, 88-93. [CrossRef]
- Porto, L.V., Celestino da Silva Neto, J., Anjos Pontual, A.D., Catunda, R.Q., 2015. Evaluation of volumetric changes of teeth in a Brazilian population by using cone beam computed tomography. J Forensic Leg Med. 36, 4-9. [CrossRef]
- Maret, D., Telmon, N., Peters, O.A., Lepage, B., Treil, J., Inglèse, J.M., Peyre, A., Kahn, J.L., Sixou, M., 2012. Effect of voxel size on the accuracy of 3D reconstructions with cone beam CT. Dentomaxillofac Radiol. 41, 649-655. [CrossRef]
- Chen, B., Szabo, D., Shen, Y., Zhang, D., Li, X., Ma, J., Haapasalo, M., 2020. Removal of calcifications from distal canals of mandibular molars by a non-instrumentational cleaning system: A micro-CT study. Aust Endod J. 46, 11-16. [CrossRef]
- Johnsen, G.F., Sundnes, J., Wengenroth, J., Haugen, H.J., 2016. Methodology for morphometric analysis of modern human contralateral premolars. J Comput Assist Tomogr. 40, 617-625. [CrossRef]
- Møller, L., Wenzel, A., Wegge-Larsen, A.M. Ding, M., Væth, M., Hirsch, E., Kirkevang, L.L., 2013. Comparison of images from digital intraoral receptors and cone beam computed tomography scanning for detection of voids in root canal fillings: an in vitro study using micro-computed tomography as validation. Oral Surg, Oral Med, Oral Pathol, Oral Radiol, Endod. 115, 810-818. [CrossRef]
- Van der Meer, W.J., Vissink, A., Ng, Y.L., Gulabivala, K., 2016. 3D Computer aided treatment planning in endodontics. J. Dent. 45, 67-72. [CrossRef]
- Ahmed, H.M.A., Ibrahim, N., Mohamad, N.S., Nambiar, P., Muhammad, R.F., Yusoff, M., Dummer, P.M.H., 2021. Application of a new system for classifying root and canal anatomy in studies involving micro-computed tomography and cone beam computed tomography: Explanation and elaboration. Int Endod J. 54:1056-1082. [CrossRef]
- Kim, S.G., Malek, M., Sigurdsson, A., Lin, L.M., Kahler, B, 2018. Regenerative endodontics: a comprehensive review. Int Endod J. 51, 1367-1388. [CrossRef]
- Höhne, C., Schwarzbauer, R., Schmitter, M., 2020. Introduction of a new teaching concept for crown preparation with 3D printed teeth. Eur J Dent Educ. 24, 526-534. [CrossRef]
- Pouhaër, M., Picart, G., Baya, D., Michelutti, P., Dautel, A., Pérard, M., Le Clerc, J., 2021. Design of 3D-printed macro-models for undergraduates' preclinical practice of endodontic access cavities. Eur J Dent Educ. [CrossRef]
- Grande, N.M., Plotino, G., Pecci, R., Bedini, R., Pameijer, C.H., Somma, F., 2008. Micro-computerized tomographic analysis of radicular and canal morphology of premolars with long oval canals. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 106, E70-E76. [CrossRef]
- Maret, D., Peters, O.A., Galibourg, A. Dumoncel, J., Esclassan, R., Kahn, J.L., Sixou, M., Telmon, N., 2014. Comparison of the accuracy of 3-dimensional cone-beam computed tomography and micro-computed tomography reconstructions by using different voxel sizes. J Endod. 40, 1321-1326. [CrossRef]
Figure 1.
CBCT image of a specimen showing pulp volume measurement in three planes: (a): coronal plane; (b): sagittal plane; (c): axial plane; (d): 3D reproduction of pulp volume.
Figure 1.
CBCT image of a specimen showing pulp volume measurement in three planes: (a): coronal plane; (b): sagittal plane; (c): axial plane; (d): 3D reproduction of pulp volume.
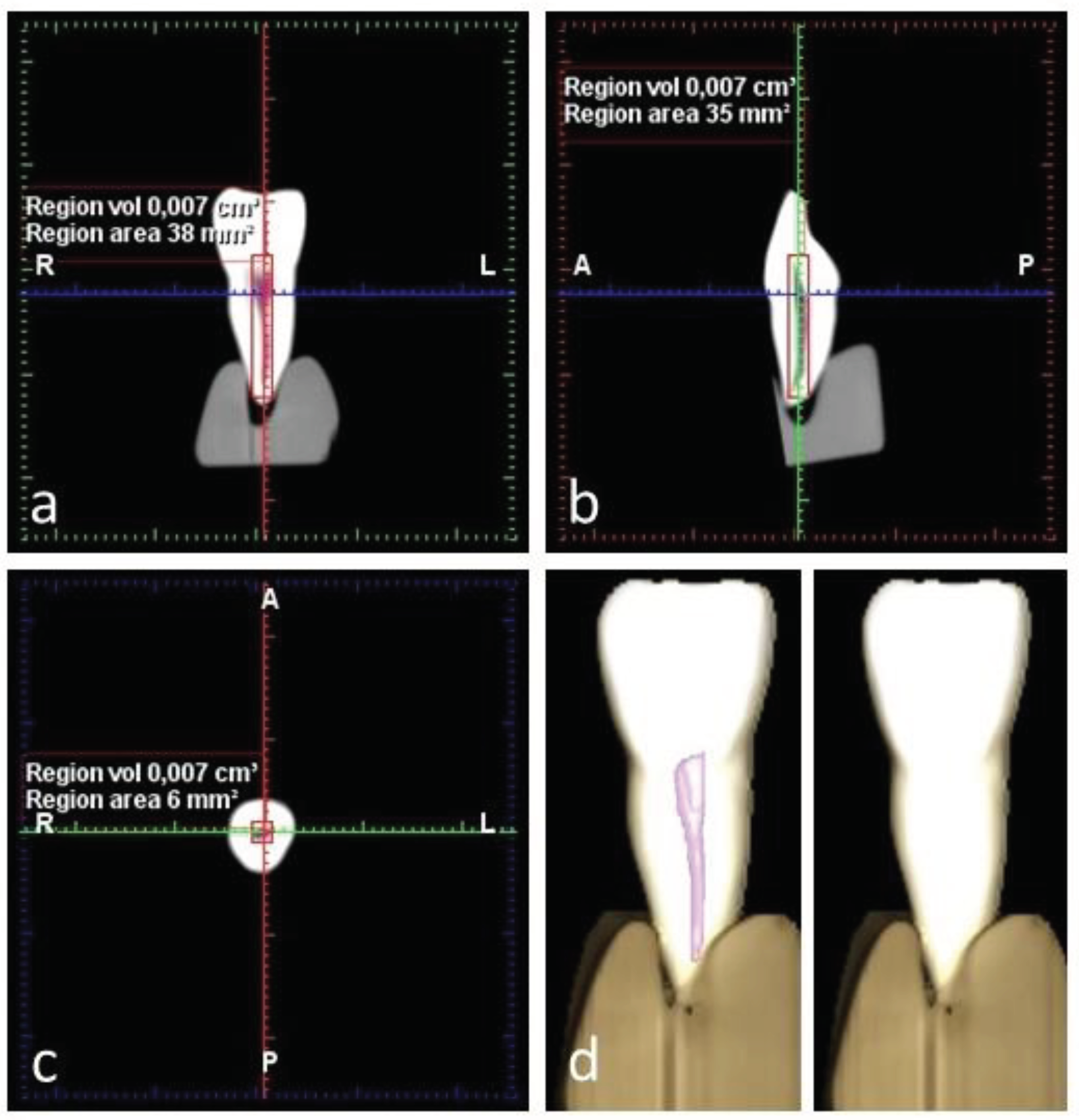
Figure 2.
Micro-CT image of a specimen showing pulp volume measurement in three planes: (a): axial plane; (c): coronal plane; (d): sagittal plane; (b): 3D reconstruction of pulp volume.
Figure 2.
Micro-CT image of a specimen showing pulp volume measurement in three planes: (a): axial plane; (c): coronal plane; (d): sagittal plane; (b): 3D reconstruction of pulp volume.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



