
Submitted:
18 February 2024
Posted:
19 February 2024
You are already at the latest version
Abstract
Daridorexant, as the first Dual Orexin Receptor Antagonist (DORA) marketed in Europe, offers a novel therapeutic approach to insomnia. However, data regarding its real-world safety are scarce. Thus, the aim of this study was to assess its safety profile using a large-scale pharma-covigilance database. Daridorexant-related Adverse Drug Reaction (ADR) reports from the FDA Adverse Event Reporting System were scrutinized, and ADRs were selected using reporting odds ratio (ROR) as a measure of disproportionality. Frequencies of events related to daridorexant were compared to all other drugs (reference group, RG1) and only to other DORAs (RG2). Only significant disproportionalities to both RGs were evaluated in-depth. A total of 845 dari-dorexant-related reports were selected; nightmares (n = 146; Dari vs. RG1: ROR = 113.74; 95%CI[95.13, 136]; Dari vs. RG2: ROR = 2.35; 95CI%[1.93, 2.85]), depression (n = 22; Dari vs. RG1: 2.13; [1.39, 3.25]; Dari vs. RG2: ROR = 2.31; 95CI%[1.45, 3.67]), and hangover (n = 20; Dari vs. RG1: ROR = 127.92; 95CI%[81.98, 199.62]; Dari vs. RG2: 3.38; [2.04, 5.61]) were considered as safety signals. These data provide valuable insights into the real-world safety profile of dari-dorexant, supporting the existence of safety signals related to nightmares, depression, and hang-over.
Keywords:
Daridorexant
; Insomnia
; Orexin
; Pharmacovigilance databases
1. Introduction
The Fifth edition of the Diagnostic and Statistical Manual of Mental Disorders defines insomnia as a condition characterized by a predominant dissatisfaction with sleep quantity or quality. In terms of primary symptoms, this condition can be characterized by difficulties in initiating or maintaining sleep, as well as by early-morning awakenings with an inability to return to sleep. These symptoms must be present for at least three nights per week and persist for a period of at least three months despite the presence of adequate opportunities to sleep to meet the diagnostic criteria for Insomnia Disorder (ID) [1]. ID appears to be among the most widespread and enduring medical conditions as it is estimated to afflict approximately 10% of the global demographic [2]. An important consequence of ID is the impairment of daytime functioning [3]. It, in fact, could substantially compromise various aspects of a patient’s life, including social interactions, occupational performance, educational achievement, and behavioural outcomes [4]. In addition to that, ID was also correlated with an increased risk of chronic non-communicable diseases such as hypertension, diabetes, and depression [5]. Current treatment guidelines for ID recommend as a first-line option the so-called Cognitive Behavioural Therapy for Insomnia (CBT-I) [6,7]. However, maintaining adherence to this type of intervention can be challenging. Thus, it is frequently necessary to support patients with pharmacological interventions [8].
Currently available treatment options for treating ID, include benzodiazepines (BDZs), agonists of the benzodiazepine receptor (Z-drugs), some antidepressants (i.e., mirtazapine and trazodone), and melatonin agonists [9]. However, BDZs, Z-drugs and other hypnotic medications are acknowledged for their propensity to induce physical dependency in patients undergoing extended treatments. In addition to that therapy discontinuation can often lead to protracted withdrawal symptoms that persist for several months [10,11]. The Dual Orexin receptor antagonists (DORAs) represent an innovative treatment strategy that could help to treat ID symptoms while reducing the burden of tolerability problems [12]. Orexins are two neuropeptides (orexin A and orexin B) secreted from neurons originating from the lateral hypothalamus that project to various brain regions. Orexin neurotransmission is mediated through two types of postsynaptic G-protein-coupled receptors: orexin 1 (Ox1R) and orexin 2 (Ox2R). Orexins play a key role in the regulation of numerous physiological functions, including arousal, cognition, stress responses, appetite regulation, and metabolism [13]. DORAs act by exercising a blockade of both types of Ox receptors, reducing the intensity of wakefulness stimuli and promoting sleep onset [12,14]. This mechanism of action prevents the broader inhibition of neuronal pathways and should help to reduce associated side effects (such as next-morning residual sleepiness, falls, motor incoordination, tolerance, and physical dependence) that are inherent to GABA-A modulators such as BDZs and Z-Drugs. Currently, there are three market-approved DORAs, suvorexant, lemborexant, and daridorexant, that primarily differ in their pharmacokinetic (PK) properties [15].
Daridorexant is the latest DORA introduced on the market and the only one to be authorized for the treatment of insomnia by the European Medicines Agency (EMA). It is characterized by a pharmacokinetic profile presenting fast absorption and a shorter half-life (8 hours) compared to the other DORAs. This should enable further reduction of next-morning sleepiness while maintaining the same level of control over nighttime sleep [16]. Daridorexant showed in its pre-marketing phase an overall encouraging safety profile, with the most frequently observed Adverse Drug Reactions (ADRs) being relative to headache, somnolence, and dizziness [17]. However, some concerns regarding tolerability aspects that are challenging to evaluate in randomized controlled trials, such as the increased frequency of suicidal ideation related ADRs, are currently being investigated [17,18,19,20]. Pharmacovigilance evaluations based on disproportionality analyses have proven to be valid tools for providing insightful safety data regarding newly marketed drugs or formulations [21,22]. However, to our knowledge, studies conducted using spontaneous reporting data regarding the safety of daridorexant, especially those comparing it to the other DORAs are still limited. Considering this, our aim was to investigate the overall safety profile of this new therapeutic option. This evaluation was realized using individual case safety reports (ICSRs) collected in the US Food and Drug Administration (FDA) Adverse Event Reporting System (FAERS).
2. Results
Initial FAERS dataset, covering from the database inception to 31/03/2023, contained 19,514,139 records. After the removal of obsolete versions of ICSRs, duplicates and undescriptive (i.e. presenting only generic terms such as “unevaluable event” or “no adverse drug reaction”) ICSRs, 15,676,304 ICSRs were left. Among those, the ones in which daridorexant was considered as a primary suspect drug were 845, while 8,986 had other DORAs as a suspected drug (Figure 1).
Descriptive analysis
Most daridorexant-related ICSRs were found to be issued by consumers (n = 712; 84.3%). When comparing these ICSRs to those relative to the other DORAs a significant difference in the proportion of consumer-reported ICSRs (n = 712; 84.6% vs. n = 3426; 38.1%; p < 0.001) over those reported by healthcare professionals (n = 131; 15.5% vs. n = 5549; 61.8%; p < 0.001) was observed.
Regarding demographical characteristics, daridorexant-related ICSRs showed a woman-to-man patient ratio of 1.9 (n = 533; 62.3% vs. n = 279; 32.6). Patient age data were available in 42.3% of the examined ICSRs. Our analysis showed that ICSRs relative to daridorexant had a lower median age value when compared to those relative to the other DORAs (60 years, interquartile range, IQR [51- 60] vs. 64 years, [50 -74]; p = 0.003). Furthermore, a significantly higher frequency of patients in the 50 to 64 years age group was observed in daridorexant-related ICSRs (n = 101; 38.7% of ICSRs with age information vs. n = 1065; 27.3% of ICSRs with age information; p < 0.001). As far as the reported ADR characteristics were concerned, most of daridorexant-related ICSRs described not serious ADRs (n = 805; 95.3%). The percentage of serious ADR cases in daridorexant-related ICSRs was lower than the one observed in other DORAs related ICSRs (n = 40; 4.7% vs. n = 1559; 17.4%; p < 0.001). Among serious ADRs, those categorized as “other serious important medical events” (n = 26; 65.0%) were the most represented, followed by ICSRs in which the death of the patient was reported (n = 9; 22.5%) and ICSRs that described an ADR causing or prolonging a hospitalization (n = 3; 7.5%). See Table 1 for further details.
In terms of ADR categories at the Medical Dictionary for Regulatory Activities (MedDRA®) High Level Group Terms (HLGTs), those observed with the higher frequency have been sleep disorders and disturbances (n = 326, 38%) with the most frequently associated preferred Terms (PTs) being nightmare (n = 146, 17.3%), insomnia (n = 80; 9.5%), abnormal dreams (n = 64; 7.6%), somnambulism (n = 18, 2.1%), and middle insomnia (n = 15; 1.8%). These ADRs were followed by those relative to therapeutic and nontherapeutic effects (n = 311; 36.8%), namely drug ineffective (n = 233; 27.6%), therapeutic product effect incomplete (n = 33; 3.9%), therapeutic product effect delayed (n = 18; 2.1%), therapeutic product effect variable (n = 8; 0.9%), and therapeutic product effect decreased (n = 8; 0.9%). The third class of frequently observed ADRs were those relative to general system disorders (n = 194; 23%), specifically feeling abnormal (n = 64; 7.6%), fatigue (n = 45; 5.3%), hangover (n = 20; 2.4%), illness (n = 17; 2%), and malaise (n = 12; 1.4%). Full details regarding the observed HLGTs distribution for daridorexant-related ICSRs are available in Supplementary Table S1. Data concerning the full distribution of ADRs at the PT level for each HLGT are available in Supplementary Table S2.
Disproportionality analyses
MedDRA® High Level Group Terms Analysis
The Reporting Odds Ratio (ROR) with a 95% confidence interval (CI) was used as a disproportionality measure to select ADRs of potential interest.
ADRs were firstly considered at MedDRA® HLGTs. HLGTs in daridorexant-related ICSRs were compared to both ICSRs relative to all other drugs (Reference Group 1; RG1) or to those related to another DORA (suvorexant, lemborexant) as a suspected drug (Reference Group 2; RG2). HLGTs related to significant ROR for both RGs were further investigated.
Significantly higher odds of reporting were observed when in relation to the HLGTs: sleep disorders and disturbances (n = 326; Dari vs. RG1: ROR = 26.42; 95%CI [23.01, 30.35]; Dari vs. RG2: 1.84; [1.59, 2.13]), product quality, supply, distribution, manufacturing and quality system issues (n = 69; Dari vs. RG1: 3.98; [3.11, 5.08]; Dari vs. RG2: 4.12; [3.1, 5.47]) and salivary gland conditions (n = 14 Dari vs. RG1: 3.38; [1.99, 5.73]; Dari vs. RG2: 2.21; [1.24, 3.94]). See Table 2 for further details.
Disproportional HLGTs were then examined at a more detailed level, the MedDRA® PT one (e.g., the headache HLGT contained the headache PT as well as migraine). Also, their expectedness was evaluated using the US FDA or European Summary of Product Characteristics (SmPCs). Data on co-reported PTs, dechallenge, rechallenge, and time-to-onset (TTO) for each double disproportionality signal were obtained using a case-by-case assessment methodology.
Disproportionally reported PTs in the HLGT sleep disorders and disturbances included: nightmare (n = 146 Dari vs. RG1: ROR 113.74; 95%CI[95.13, 136]; Dari vs. RG2: 2.35; [1.93, 2.85]), insomnia (n = 80; Dari vs. RG1: 7.41; [5.88, 9.33]; Dari vs. RG2: 1.94; [1.51, 2.49], and hypnagogic hallucination (n = 3 Dari vs. RG1: 267.22; [85.32, 836.95]; Dari vs. RG2: 4; [1.06, 15.1]). See Table 3 for further details.
The case-by-case assessment for these ADRs showed, as frequently co-reported PTs with nightmare: drug ineffective (n = 32; 21.9%), hallucination (n = 10; 6.8%), and hangover (n = 8; 5.5%). A positive dechallenge was observed in 20.5% of nightmare ICSRs (n = 30), and negative dechallenge in 3.4% (n = 5). TTO data was available in 20 nightmare ICSRs (13.7%) and showed a median of 1 day IQR[1-1]. Considering insomnia, frequently co-reported PTs included: product availability issues (n = 46; 57.5%), drug ineffective (n = 7; 8.8%), and feeling abnormal (n = 7; 8.8%). A positive dechallenge was reported in 20.5% of insomnia ICSRs (n = 30), and a negative dechallenge in 3.4% (n = 5). TTO data were present in 6 ICSRs (7.5%) with an observed median of 1 day IQR[1-13]. As far as hypnagogic hallucination was concerned, co-reported PTs included confusional state, auditory hallucination, and nightmare (all with n = 1; 33.3%). A positive dechallenge was observed in 2 cases (66.7%), while no rechallenge and TTO data were available for these ICSRs.
In the HLGT salivary gland conditions, the only observed PT was dry mouth (n = 14 Dari vs. RG1: ROR = 4.17; 95%CI [2.46, 7.07]; Dari vs. RG2: 2.31; [1.29, 4.14]. This ADR is not currently reported neither in the European or FDA SmPCs. The case-by-case assessment showed that frequently co-reported PTs included: drug ineffective (n = 5; 35.7%), nocturia (n = 2; 14.3%), and nightmare (n = 2; 14.3%). A positive dechallenge was reported in 6 ICSRs (42.8%). No TTO data was available.
As far the HLGT Product quality, supply, distribution, manufacturing and quality system issues was concerned, the disproportional PTs were: product packaging difficult to open (n = 7; Dari vs. RG1: ROR = 104.91 95%CI[49.76, 221.20] Dari vs. RG2: 5.35; [2.15, 13.3]), and product availability issue (n = 51; Dari vs. RG1 97.47; [73.39, 129.45] Dari vs. RG2: 32; [18.61, 55.04]). See Table S3 for more information. Both ADRs were not reported in either the daridorexant European or FDA SmPCs. The case-by-case assessment data showed that frequently co-reported PTs with product packaging difficult to open included drug ineffective (n = 3; 42.9%), headache (n = 2; 28.6%), and yawning (n = 1; 14.3%). PTs frequently co-reported with product availability issue were: insomnia (n = 46; 90.2%), drug ineffective (n = 5; 9.8%), and nightmare (n = 3; 58.8%).
The Disproportional PTs reported in the HLGT headaches were: headache (n = 59; Dari vs. RG1: ROR = 2.27; 95%CI[1.74, 2.95]; Dari vs. RG2: 1.52; [1.15, 2.01]) and Migraine (n = 8; Dari vs. RG1: 2.05; [1.02, 4.12]; Dari vs. RG2: 2.25; [1.05, 4.84]). See Table S3 for more information. These ADRs are already listed in European or FDA SmPCs. Frequently co-reported PTs that emerged from the case-by-case assessment of headache ICSRs included: drug ineffective (n = 16; 27.1%), somnolence (n = 9; 15.2%), and fatigue (n = 8; 13.6%). A positive dechallenge was observed in 49.2% of these cases (n = 29), and a negative one in 3.4% (n = 2). TTO data were available in 17 ICSRs (28.8%) with a median observed value of 1 day IQR[1-1]. Considering migraine frequently co-reported PTs included: tremor, somnolence, and product prescribing error (all with n = 1; 12.5%). A positive dechallenge was observed in 37.5% of cases (n = 3). TTO data were available in only two reports both showing an interval of 2 days between treatment initiation and ADR onset. No rechallenge data were available for both headache and migraine.
As far as PTs belonging to the HLGT depressed mood disorders and disturbances those were: depression (n = 22; Dari vs. RG1: ROR = 2.13; 95%CI[1.39, 3.25]; Dari vs. RG2: 2.31; [1.45, 3.67]) and depressed mood (n = 3; Dari vs. RG1: 1.36; [0.44, 4.24]; Dari vs. RG2: 1.45; [0.43, 4.86]). Both ADRs are acknowledged in European or FDA SmPCs. Frequently co-reported PTs with depression were drug ineffective (n = 7; 31.8%), suicidal ideation (n= 5; 22.7%), and insomnia (n = 4; 18.2%). A positive dechallenge was observed in 45.5% of depression cases (n = 10) and a negative one in 9.1% (n = 2). No rechallenge data were available. TTO data was available in 6 ICSRs (27.3%), with a median value of 5 days IQR[1-11].
Considering the HLGT general system disorders NEC, disproportional PTs were feeling abnormal (n = 64 Dari vs. RG1: 6.19; [4.8, 7.99]; Dari vs. RG2: 1.75; [1.33, 2.29]), followed by fatigue (n= 45 Dari vs. RG1: 1.41; [1.05, 1.91]; Dari vs. RG2: 2.28; [1.64, 3.17]), hangover (n = 20; Dari vs. RG1: ROR = 127.92; 95%CI[81.98, 199.62]; Dari vs. RG2: 3.38, [2.04, 5.61]), and energy increased (n = 5; Dari vs. RG1: 18.7; [7.76, 45.06]; Dari vs. RG2: 6.68; [2.18, 20.47]). See Table 4 for further details.
The case-by-case assessment for feeling abnormal ICSRs highlighted frequently co-reported PTs such as drug ineffective (n = 17; 26.6%), fatigue (n = 14; 21.9%), and headache (n = 8; 12.5%). These ICSRs were characterized by a positive dechallenge in 25 cases (39.1%) and a negative dechallenge in 2 cases (3.1%). TTO data were available in 16 of these ICSRs (25%) with an observed median value of 1 day IQR[1-1]. Considering fatigue frequently co-reported PTs included somnolence (n = 22; 48.9%), drug ineffective (n = 18; 40%), and feeling abnormal (n = 14; 31.1%). A positive dechallenge was observed in 57.8% of fatigue-related ICSRs (n = 26). In terms of rechallenge, 1 ICSR (2.2%) showed a positive rechallenge and another ICSR a negative one. Twelve fatigue-related ICSRs (26.7%) presented TTO data with a median value of 1 day IQR[1-1]. Focusing on hangover the frequently co-reported PTs were nightmare (n = 8; 40%), drug ineffective (n = 5; 25%), and somnolence (n = 3; 15%). A positive dechallenge was observed in 20% of hangover ICSRs (n = 4). TTO data were available in only 2 hangover-related ICSRs with intervals of one or 2 days. The evaluation of energy increases ICSRs showed as frequently co-reported PTs insomnia, drug ineffective (both with n = 2; 40%), and therapeutic response unexpected (n = 1; 20%). A positive dechallenge was observed in 3 cases (60%), while TTO data were available in 2 cases with a 1-day onset time.
Full data regarding disproportionality evaluations of observed PTs for each HLGT is available in Supplementary Table S3.
3. Discussion
This study analyzed the currently available real-world safety data for daridorexant reported in the FAERS database and compared them to the ones relative to the other DORAs. This new targeted drug class represents an important step forward in ID pharmacological treatment. DORAs promise, in fact, to offer a therapeutic alternative that could improve critical tolerability aspects of commonly used medications in this setting. Furthermore, daridorexant, being the only DORA authorized from both the FDA and EMA, could represent a new therapeutic alternative for a portion of patients who previously did not have access to these treatments. Our analysis points out increased odds of reporting for potentially important ADRs such as nightmares and worsening of depression. Considering this and given the current lack of real-world safety studies regarding this drug, the result of our analysis could represent a useful tool to help clinicians.
Descriptive analysis
A significantly higher frequency of ICSRs reported by patients was observed when comparing daridorexant-related ICSRs to those relative to the other DORAs. This can be viewed as a consequence of the high level of attention that daridorexant has received in its first year of market presence. Furthermore, daridorexant is currently being actively promoted, especially in the US, which could incentivize consumer-driven reporting. Multiple studies have highlighted how the media could strongly influence ADR reporting by the consumers [23].
A significantly higher proportion of daridorexant-related ICSRs involved patients in the 50 to 64 years age group when compared to those relative to the other DORAs. These data are in line with the common clinical practice in which consolidated therapeutic options are always preferred for the treatment of older, thus more fragile, patients [24,25].
A significantly lower frequency of serious ADRs was observed when comparing daridorexant-related ICSRs to those relative to the other DORAs. This data could be intended as confirmation of pre-marketing studies depicting an overall good safety profile. However, the shorter market permanence of daridorexant should be taken into account. Indeed, as the market permanence of a drug increases, the propensity for reporting non-serious ADRs diminishes due to their increasing recognition and familiarity among prescribers [24]. Therefore, the ratio between ADRs classified as serious and those classified as non-serious can undergo significant variations. As far as the seriousness characteristics of ADRs are concerned, even if differences were observed compared to the other DORAs, the extremely limited number of ICSRs presenting serious ADRs makes an unbiassed evaluation of these data difficult.
The relatively high frequency of observation for terms regarding drug ineffectiveness represents an interesting occurrence. Several reasons, such as patient skepticism and initial administration errors, could contribute to reporting this kind of ADRs. Furthermore, literature sources highlight that patient-reported ICSRs, which represent the majority of daridorexant-related ICSRs, have a higher ratio of drug ineffectiveness when compared to those reported by healthcare professionals [25,26]. These considerations can also be applied to the high number of ICSRs reporting insomnia observed, pointing towards the existence of an indication bias. The previously discussed ADRs are, thus, more likely to be attributed to ineffective control of preexisting ID conditions rather than being a direct result of drug administration.
Disproportional ADRs
When compared to the rest of the FAERS database, disproportionalities concerned mostly ADRs already known for other DORAs. This data depicts a globally comparable safety profile for all DORAs. However, some differences seem to be present and merit further attention.
Hangover manifestations
Hangover and fatigue were found to be disproportionally reported in daridorexant-related ICSRs when compared to both RGs. This data should be viewed in light of some considerations. Daridorexant, was selected among several drug candidates thanks an expected effect duration of around 8 hours with a dose of 25mg. This choice was made in order to minimize “next morning” residual effects [27]. However, some people may still experience “next morning” residual effects, such as somnolence, when treated with daridorexant [17,28]. In addition to that, in 1/4th of ICSRs hangover also reported ineffectiveness or effectiveness reduction. Moreover, because daridorexant was designed to minimize such ADRs, their occurrence is more likely to garner increased attention than other DORAs. Considering this, we cannot rule out the presence of a notoriety bias regarding this ADR.
Dry mouth
Dry mouth was also disproportional for daridorexant compared to both RGs. Currently this ADR is not reported neither in the European nor in the US FDA SmPCs. Only the FDA documentation relative to suvorexant reported dry mouth as an ADR observed in premarketing studies [29]. Although apparently mild, the impact of this ADR on patients’ quality of life has to be carefully considered. Indeed, literature sources point out that xerostomia or self-reported sensations of dry mouth can be correlated with insufficient quality of sleep [30,31]. Furthermore, from a case-by-case analysis, we were able to observe that 35.7% of ICSRs presenting dry mouth as an ADR also highlighted an ineffectiveness of the drug. Thus, the reporting by patients of a feeling of dry mouth should be, in our opinion, carefully considered by the clinicians as it might be related to a sub-optimal control of the quality of sleep.
Nightmares
Nightmares were found to be disproportional for daridorexant both when considering the rest of the database and to ICSRs relative to the other DORAs. The possibility of the onset of this type of ADR is currently not reported in the EMA SmPC of daridorexant, but just in the FDA one. Furthermore, data associating these ADRs to other DORAs is limited to the results of two clinical trials conducted for lemborexant [32]. The onset of nightmares was deemed as an uncommon occurrence in both studies. Indeed, in the SUNRISE-1 trial, only 0.6% (3 out of 534) of patients treated with lemborexant developed nightmares [33]. While considering the SUNRISE-2 trial, 1.8% of patients treated with lemborexant (11 out of 628) presented nightmares [34]. These ADRs should not be underestimated as the onset of nightmares in patients with sleep disorders has been linked to increased distress levels and, in some cases, to the development of secondary forms of ID [35]. The mechanism behind the onset of nightmares might be linked to the actions that DORAs as a class have on patients' global sleep architecture. Indeed, one of the supposed effects of DORAs is promoting the REM phase of sleep [36]. This increase in REM sleep time could facilitate the recalling of dream content and its remembering by the patient [37]. Furthermore, other ADRs like headaches or migraine, are possible risk factors for nightmares [38]. However, after an in-depth evaluation of nightmares cases (n = 146), we observed that 21.9% of those also reported an ineffectiveness of the drug. Thus, the impact of inadequate control or worsening preexisting conditions cannot be excluded. In addition to that, we observed that were available TTO data (13.7%) indicated short onset median time (1 day). These data even if limited, surely remark the need to monitor the initial stages of ID pharmacological treatments closely. Furthermore, a need to further investigate these issues with focused studies emerges from our analysis. An initial step in this direction should involve epidemiological studies based on large-scale databases. These studies might be particularly fitting considering the low incidence rates noted in clinical trials for lemborexant and the limited availability of real-world data. Once a deeper understanding of the problem is achieved, the next step should involve short- and long-term prospective studies to obtain first-hand clinical practice data.
Worsening of Depression
Depression was found to be disproportional for daridorexant both when considering the rest of the database and to ICSRs relative to the other DORAs. The risk of worsening pre-existing depression condition might represent an important safety aspect of daridorexant. Previously, another DORA, suvorexant, has been associated with seemingly dose-dependent worsening depression ad suicidal ideation [39]. Also, general warnings regarding these ADRs are present in the SmPCs [17,28]. Furthermore, previous studies showed that suicidal patients affected by major depressive disorder (MDD) present lower orexin levels than those without a diagnosis of MDD [40]. However, the results of a recently published real-world study seem to underline a certain coherency between DORAs and Z-drugs in terms of suicidal ideation ADRs [41]. Furthermore, sleep disorders are renowned among the core symptoms of depression [42]. Thus, the possibility of the depression worsening as a consequence of the insufficient control of these disturbances cannot be ruled out. As far as suicidal ideation is concerned, the intricate nature of these clinical presentations makes drawing unbiased conclusions a task beyond the capability of a disproportionality analysis-based study. In this context, the employment of techniques like network analyses could aid in the assessment of these manifestations. Indeed, the potential to provide quantifiable data on relationships among ADRs, which these techniques seem to possess, could allow the achievement of a more holistic comprehension of these phenomena.
Strengths and Limitations
The study is based on real-world data collected from the FAERS database, providing a practical insight into the safety of daridorexant. The fact that daridorexant is the only drug in its class to be authorized by the FDA and EMA makes it particularly interesting to healthcare professionals. To the best of our knowledge, this is the first study evaluating real-world safety data for this drug in comparison to those relative to the other DORAs using a large-scale pharmacovigilance database. Although our findings provide a comprehensive perspective in the evaluation of daridorexant-related ADRs, the results of the present study should be interpreted in the light of some limitations.
FAERS data are based on spontaneous ICSRs; thus, the presence of duplicate ICSRs, reporting errors and high variability in the general quality and completeness of reported data should be considered. We acknowledge these factors and we adopted a cautious approach in ICSRs where data were insufficient, often resulting in the exclusion of cases. Other FAERS-specific limitations regarded the TTO, dechallenge and rechallenge data. These data were present in a limited number of reports and provided on a “drug-event” basis rather than a “drug-single ADR” basis. However, the type of ADRs examined usually present themselves without large time between the various symptoms. Thus, the impact of these limitations on our analysis should be limited.
Disproportionality analyses are commonly affected by biases such as the notoriety bias and confounding by indication [43]. As far as notoriety bias is concerned, its impact on our analysis cannot be underestimated. We acknowledge this, and in order to minimize this influence, we adopted an extremely cautious approach in the evaluation of ADRs more prone to this phenomenon. Concerning the confounding by indication bias, the implementation of two RGs in our study, the second of which constituted drugs with the same mechanism of action of daridorexant and approved for the same indication, should allow for the mitigation of this issue. However also, in this case, given the complexity of the conditions underlying ID, caution was applied in the interpretation of the results.
Furthermore, it is crucial to approach pharmacovigilance data with consideration of certain technical issues, including under-reporting compared to the global clinical population and the challenge of identifying confounding factors. This suggests that the reported ADRs may only represent a partial, and possibly underrepresented, percentage of all ADRs occurring in routine clinical practice. Additionally, the absence of data on the number of patients effectively treated with these drugs during the specified period (i.e., the denominator for calculating incidence fractions) precludes the calculation of incidence rates.
4. Materials and Methods
Data Source and extraction criteria
A retrospective observational study was conducted by using ICSRs collected in the FAERS database. FAERS is a widely utilized publicly accessible database comprising over 19 million ICSRs from patients, healthcare professionals, and pharmaceutical companies across the United States, Europe, and Asia. These ICSRs, aside from unique identification numbers, can include information, dates of ICSR submission and ADR occurrences, reporting country, primary source qualifications, patient characteristics (such as gender, age, and weight), suspected and concurrent medications along with their prescribed uses, ADR descriptions, and their seriousness.
Data relative to ICSRs were extracted from the ASCII files made publicly available each quarter by the FDA (https://fis.fda.gov/extensions/FPD-QDE-FAERS/FPD-QDE-FAERS.html, accessed on May 15th 2023). Files corresponding to a time interval ranging from Q1 2004 to Q1 2023, have been downloaded and preprocessed. In case of the presence of multiple versions of a single ICSR, only the latest one was considered for the analyses. Duplicate ICSRs were recognized through the presence of overlapping data in crucial fields such as: event dates, gender, age, reporting country, body weight, reported ADRs, and suspected active substances. In addition to that, ICSRs linked to literature sources were also excluded. Furthermore, ICSRs not providing a description of an ADR (i.e presenting only terms such as unevaluable event or no adverse event) were excluded.
ICSRs presenting a unique case identifier code and having as a primary suspect drug daridorexant were extracted and considered for the analyses. In addition to those, uniquely identifiable ICSRs presenting as primary suspect drugs the other currently approved DORAs (suvorexant and lemborexant) were also extracted to compare their characteristics with the daridorexant related ones. No restrictions based on gender or age group reported in the ICSRs were applied for the extraction.
All the observed ADRs have been categorized in accordance with the MedDRA®. MedDRA® provides a multiaxial hierarchical classification articulated in 5 levels. The terms range from the more specific Lowest Level Term to the more encompassing System Organ Class. For this analysis ADRs were at first regrouped in HLGTs and then examined at the PT level.
Data Analyses
Descriptive analysis
A descriptive statistical analysis was carried out to examine the demographic and clinical attributes of FAERS ICSRs related to daridorexant in comparison to those related to other DORAs. This analysis encompassed patient characteristics (such as gender and age), primary sources of information, year of reporting, reporting countries, as well as ADR characteristics, including seriousness. Continuous variables were presented as medians (IQR), while categorical variables were expressed as absolute values (percentages). Differences in frequencies of the categorical variables were assessed using Pearson's chi-square test on a 2x2 contingency table with Yates' continuity correction. Continuous variables were evaluated using the Mann-Whitney U test. A statistically significant threshold was set at a p value of < 0.001 for all analyses.
Disproportionality analysis
The ROR with the corresponding 95%CI was used as a disproportionality measure. The statistical significance threshold was set at values > 1 of the lower limit of the ROR 95% CI, with a minimum of 3 ICSRs for each drug-event pair.
To evaluate significant disproportionalities in the odds of ADR reporting a two-step process was implemented: at first, a disproportionality analysis was conducted with ADRs regrouped at the HLGT. Daridorexant-related ICSRs were compared to the rest of the database (RG1). In addition, to minimize the impact of possible confounding factors, daridorexant-related ICSRs were compared to RG2 constituted by ICSRs presenting suvorexant and lemborexant as suspected drugs. Disproportionally reported HLGTs were further investigated only if significant results emerged from the comparison with both the reference groups. As a second step, for each disproportional HLGT, disproportional ADRs were investigated at the PT Level. As for the previous step disproportional ADRs were further analyzed only if significant differences were observed in comparison to both reference groups.
Case-by-case assessments, TTO calculation and ADRs expectedness evaluation
Qualitative case-by-case assessments were conducted to further characterize the observed double disproportionality signals. These evaluations were performed by examining ADRs reported concomitantly to the disproportional ones. The presence of dechallenge and rechallenge data in ICSRs presenting disproportional ADRs to both RGs was also evaluated in this context. In addition to that, the TTO of the ADR cases was calculated as the difference in days between the event date and the starting date of the therapy [44]. The expectedness evaluation of the observed ADRs for daridorexant was performed on the basis of the data contained in the European or US FDA SmPCs.
All statistical analyses were performed using SPSS version 28. The present study is reported in accordance with the "Reporting of A Disproportionality analysis for drUg Safety" (READ-US) statement [45].
5. Conclusions
This study analyzed real-world safety data for daridorexant as reported in the FAERS database, with a particular focus on comparing it to other drugs of the same class. Daridorexant, as the only drug of its class to be authorized by both the FDA and EMA, could represent a new treatment option for many patients. Our data, seem to point towards a safety profile overall in line with literature data and previous studies on other DORAs. However, the possible presence of still not entirely acknowledged safety signals like nightmares and dry mouth emerges from our analysis. Given the complex nature of some ADRs, like nightmares and worsening of depression, further studies are required to better understand their implications for patient safety.
Supplementary Materials
The following supporting information can be downloaded at: Preprints.org, Table S1. ADRs Observed in Daridorexant and other DORAs related ICSRs regrouped by MedDRA High Level Group Terms; Table S2. ADRs Observed in Daridorexant and other DORAs related ICSRs by MedDRA High Level Group Terms and Preferred Terms; Table S3. Disproportionality analysis at Preferred Terms level for each High-Level Group Term observed in daridorexant-related ICSRs
Author Contributions
Conceptualization, G.C. and E.S.; methodology, F.S. and E.S.; software, G.C.; validation, M.A.B., F.S., and E.S.; formal analysis, G.C; investigation, G.C. and M.A.B; data curation, G.C.; writing—original draft preparation, G.C.; writing—review and editing, G.C., M.A.B., and F.S.; visualization, G.R.; supervision, F.S. and E.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study used publicly available safety ICSR data that were provided in an anonymous form and were already compliant with ethical standards. Therefore, no further ethical evaluation was necessary.
Data Availability Statement
This study was entirely based on publicly anonymized data made available by the Food and Drug Administration. The raw data can be downloaded at the following link https://fis.fda.gov/extensions/FPD-QDE-FAERS/FPD-QDE-FAERS.html
Conflicts of Interest
The authors declare no conflicts of interest.
References
- American Psychiatric Association Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Association Publishing, 2022; ISBN 0-89042-575-2.
- Morin, C.M.; Jarrin, D.C. Epidemiology of Insomnia. Sleep. Med. Clin. 2022, 17, 173–191. [Google Scholar] [CrossRef] [PubMed]
- Brownlow, J.A.; Miller, K.E.; Gehrman, P.R. Insomnia and Cognitive Performance. Sleep. Med. Clin. 2020, 15, 71–76. [Google Scholar] [CrossRef]
- Hudgens, S.; Phillips-Beyer, A.; Newton, L.; Seboek Kinter, D.; Benes, H. Development and Validation of the Insomnia Daytime Symptoms and Impacts Questionnaire (IDSIQ). Patient-Patient-Centered Outcomes Res. 2021, 14, 249–268. [Google Scholar] [CrossRef] [PubMed]
- Wilson, S.; Anderson, K.; Baldwin, D.; Dijk, D.-J.; Espie, A.; Espie, C.; Gringras, P.; Krystal, A.; Nutt, D.; Selsick, H.; et al. British Association for Psychopharmacology Consensus Statement on Evidence-Based Treatment of Insomnia, Parasomnias and Circadian Rhythm Disorders: An Update. J. Psychopharmacol. 2019, 33, 923–947. [Google Scholar] [CrossRef]
- Riemann, D.; Baglioni, C.; Bassetti, C.; Bjorvatn, B.; Dolenc Groselj, L.; Ellis, J.G.; Espie, C.A.; Garcia-Borreguero, D.; Gjerstad, M.; Gonçalves, M.; et al. European Guideline for the Diagnosis and Treatment of Insomnia. J. Sleep. Res. 2017, 26, 675–700. [Google Scholar] [CrossRef] [PubMed]
- Qaseem, A.; Kansagara, D.; Forciea, M.A.; Cooke, M.; Denberg, T.D. Management of Chronic Insomnia Disorder in Adults: A Clinical Practice Guideline From the American College of Physicians. Ann. Intern. Med. 2016, 165, 125. [Google Scholar] [CrossRef] [PubMed]
- Agnew, S.; Vallières, A.; Hamilton, A.; McCrory, S.; Nikolic, M.; Kyle, S.D.; Fleming, L.; Crawford, M.R. Adherence to Cognitive Behavior Therapy for Insomnia. Sleep Med. Clin. 2021, 16, 155–202. [Google Scholar] [CrossRef]
- Madari, S.; Golebiowski, R.; Mansukhani, M.P.; Kolla, B.P. Pharmacological Management of Insomnia. Neurotherapeutics 2021, 18, 44–52. [Google Scholar] [CrossRef]
- Fluyau, D.; Revadigar, N.; Manobianco, B.E. Challenges of the Pharmacological Management of Benzodiazepine Withdrawal, Dependence, and Discontinuation. Ther. Adv. Psychopharmacol. 2018, 8, 147–168. [Google Scholar] [CrossRef]
- Schifano, F.; Chiappini, S.; Corkery, J.M.; Guirguis, A. An Insight into Z-Drug Abuse and Dependence: An Examination of Reports to the European Medicines Agency Database of Suspected Adverse Drug Reactions. Int. J. Neuropsychopharmacol. 2019, 22, 270–277. [Google Scholar] [CrossRef]
- Muehlan, C.; Roch, C.; Vaillant, C.; Dingemanse, J. The Orexin Story and Orexin Receptor Antagonists for the Treatment of Insomnia. J. Sleep. Res. 2023. [Google Scholar] [CrossRef]
- Saper, C.B.; Scammell, T.E.; Lu, J. Hypothalamic Regulation of Sleep and Circadian Rhythms. Nature 2005, 437, 1257–1263. [Google Scholar] [CrossRef]
- Stahl, S.M. Mechanism of Action of Suvorexant. CNS Spectr. 2016, 21, 215–218. [Google Scholar] [CrossRef]
- Xue, T.; Wu, X.; Chen, S.; Yang, Y.; Yan, Z.; Song, Z.; Zhang, W.; Zhang, J.; Chen, Z.; Wang, Z. The Efficacy and Safety of Dual Orexin Receptor Antagonists in Primary Insomnia: A Systematic Review and Network Meta-Analysis. Sleep Med. Rev. 2022, 61, 101573. [Google Scholar] [CrossRef]
- Kunz, D.; Dauvilliers, Y.; Benes, H.; García-Borreguero, D.; Plazzi, G.; Seboek Kinter, D.; Coloma, P.; Rausch, M.; Sassi-Sayadi, M.; Thein, S. Long-Term Safety and Tolerability of Daridorexant in Patients with Insomnia Disorder. CNS Drugs 2023, 37, 93–106. [Google Scholar] [CrossRef]
- European Medicines Agency Summary Of Product Characteristics - Qviviq. Human. medicine European public assessment reports Database 2022.
- Palagini, L.; Geoffroy, P.A.; Micoulaud-Franchi, J.A.; Gemignani, A.; Riemann, D. Potential Aggravation of Suicide Risk With Daridorexant. J. Clin. Psychiatry 2023, 84. [Google Scholar] [CrossRef] [PubMed]
- Nobile, B.; Olié, E.; Courtet, P. Possible Suicidal Risk With Daridorexant, a New Treatment for Insomnia. J. Clin. Psychiatry 2022, 84, 44433. [Google Scholar] [CrossRef]
- Salvo, F.; Micoulaud-Franchi, J.-A.; Palagini, L.; Geoffroy, P.A. Dual Orexin Receptor Antagonists and Suicide Risk. J. Clin. Psychiatry 2023, 84. [Google Scholar] [CrossRef]
- Montastruc, J.; Sommet, A.; Bagheri, H.; Lapeyre-Mestre, M. Benefits and Strengths of the Disproportionality Analysis for Identification of Adverse Drug Reactions in a Pharmacovigilance Database. Br. J. Clin. Pharmacol. 2011, 72, 905–908. [Google Scholar] [CrossRef]
- Cicala, G.; de Filippis, R.; Barbieri, M.A.; Cutroneo, P.M.; De Fazio, P.; Schoretsanitis, G.; Spina, E. Tolerability Profile of Paliperidone Palmitate Formulations: A Pharmacovigilance Analysis of the EUDRAVigilance Database. Front. Psychiatry 2023, 14. [Google Scholar] [CrossRef]
- Inácio, P.; Cavaco, A.; Airaksinen, M. The Value of Patient Reporting to the Pharmacovigilance System: A Systematic Review. Br. J. Clin. Pharmacol. 2017, 83, 227–246. [Google Scholar] [CrossRef]
- Weber, J.C.P. Epidemiology in the United Kingdom of Adverse Drug Reactions from Non-Steroidal Anti-Inflammatory Drugs. In; 1987; pp. 27–35.
- Kim, H.-J.; Jeong, H.E.; Bae, J.-H.; Baek, Y.-H.; Shin, J.-Y. Characteristics and Trends of Spontaneous Reporting of Therapeutic Ineffectiveness in South Korea from 2000 to 2016. PLoS ONE 2019, 14, e0212905. [Google Scholar] [CrossRef]
- Blenkinsopp, A.; Wilkie, P.; Wang, M.; Routledge, P.A. Patient Reporting of Suspected Adverse Drug Reactions: A Review of Published Literature and International Experience. Br. J. Clin. Pharmacol. 2007, 63, 148–156. [Google Scholar] [CrossRef]
- Markham, A. Daridorexant: First Approval. Drugs 2022, 82, 601–607. [Google Scholar] [CrossRef]
- Food and Drug Administration QUVIVIQ Full Prescribing Information. Available online: https://www.accessdata.fda.gov/drugsatfda_ docs/label/2022/214985s000lbl.pdf (accessed on 3 May 2023).
- Food and Drug Administration BELSOMRA Full Prescribing Information. Available online: https://www.accessdata.fda.gov/drugsatfda_ docs/label/2014/204569s000lbledt.pdf (accessed on 3 May 2023).
- Apessos, I.; Andreadis, D.; Steiropoulos, P.; Tortopidis, D.; Angelis, L. Investigation of the Relationship between Sleep Disorders and Xerostomia. Clin. Oral. Investig. 2020, 24, 1709–1716. [Google Scholar] [CrossRef]
- Lopez -Jornet, P.; Lucero Berdugo, M.; Fernandez-Pujante, A.; C, C.F.; Lavella C, Z.; A, P.-F.; J, S.R.; Silvestre, F.J. Sleep Quality in Patients with Xerostomia: A Prospective and Randomized Case-Control Study. Acta Odontol. Scand. 2016, 74, 224–228. [Google Scholar] [CrossRef]
- Roth, T.; Yardley, J.; Pinner, K.; Kumar, D.; Cheng, J.; Moline, M. P097 Incidence of Abnormal Dreams and Nightmares with Lemborexant in Adults with Insomnia: Results from Two Phase 3 Studies. Sleep Adv. 2021, 2, A52. [Google Scholar] [CrossRef]
- Rosenberg, R.; Murphy, P.; Zammit, G.; Mayleben, D.; Kumar, D.; Dhadda, S.; Filippov, G.; LoPresti, A.; Moline, M. Comparison of Lemborexant With Placebo and Zolpidem Tartrate Extended Release for the Treatment of Older Adults With Insomnia Disorder. JAMA Netw. Open 2019, 2, e1918254. [Google Scholar] [CrossRef]
- Kärppä, M.; Yardley, J.; Pinner, K.; Filippov, G.; Zammit, G.; Moline, M.; Perdomo, C.; Inoue, Y.; Ishikawa, K.; Kubota, N. Long-Term Efficacy and Tolerability of Lemborexant Compared with Placebo in Adults with Insomnia Disorder: Results from the Phase 3 Randomized Clinical Trial SUNRISE 2. Sleep 2020, 43. [Google Scholar] [CrossRef]
- Paul, F.; Schredl, M.; Alpers, G.W. Nightmares Affect the Experience of Sleep Quality but Not Sleep Architecture: An Ambulatory Polysomnographic Study. Borderline Pers. Disord. Emot. Dysregul 2015, 2, 3. [Google Scholar] [CrossRef]
- Clark, J.W.; Brian, M.L.; Drummond, S.P.A.; Hoyer, D.; Jacobson, L.H. Effects of Orexin Receptor Antagonism on Human Sleep Architecture: A Systematic Review. Sleep. Med. Rev. 2020, 53, 101332. [Google Scholar] [CrossRef]
- Dal Sacco, D. Dream Recall Frequency and Psychosomatics. Acta Biomed. 2022, 93, e2022046. [Google Scholar] [CrossRef]
- Stefani, A.; Högl, B. Nightmare Disorder and Isolated Sleep Paralysis. Neurotherapeutics 2021, 18, 100–106. [Google Scholar] [CrossRef]
- Petrous, J.; Furmaga, K. Adverse Reaction with Suvorexant for Insomnia: Acute Worsening of Depression with Emergence of Suicidal Thoughts. BMJ Case Rep. 2017, bcr-20. [Google Scholar] [CrossRef]
- Brundin, L.; Björkqvist, M.; Petersén, Å.; Träskman-Bendz, L. Reduced Orexin Levels in the Cerebrospinal Fluid of Suicidal Patients with Major Depressive Disorder. Eur. Neuropsychopharmacol. 2007, 17, 573–579. [Google Scholar] [CrossRef]
- Salvo, F.; Micoulaud-Franchi, J.-A.; Palagini, L.; Geoffroy, P.A. Dual Orexin Receptor Antagonists and Suicide Risk. J. Clin. Psychiatry 2023, 84. [Google Scholar] [CrossRef]
- Nutt, D.; Wilson, S.; Paterson, L. Sleep Disorders as Core Symptoms of Depression. Dialogues Clin. Neurosci. 2008, 10, 329–336. [Google Scholar] [CrossRef]
- Cutroneo, P.M.; Sartori, D.; Tuccori, M.; Crisafulli, S.; Battini, V.; Carnovale, C.; Rafaniello, C.; Capuano, A.; Poluzzi, E.; Moretti, U.; et al. Conducting and Interpreting Disproportionality Analyses Derived from Spontaneous Reporting Systems. Front. Drug Saf. Regul. 2024, 3. [Google Scholar] [CrossRef]
- Barbieri, M.A.; Sorbara, E.E.; Cicala, G.; Santoro, V.; Cutroneo, P.M.; Franchina, T.; Spina, E. Adverse Drug Reactions with HER2-Positive Breast Cancer Treatment: An Analysis from the Italian Pharmacovigilance Database. Drugs Real. World Outcomes 2022, 9, 91–107. [Google Scholar] [CrossRef]
- Khouri, C.; Salvo, F.; Raschi, E.; Fusaroli, M. Reporting of A Disproportionality Analysis for DrUg Safety - READUS. Available online: https://readus-statement.org/ (accessed on 15 January 2024).
Figure 1.
Database Pre-processing and Individual Case Safety Reports (ICSRs) Selection. ASCII: American standard code for information interchange; DORAs: Dual Orexin Receptor Antagonists; ICSRs: Individual Case Safety Reports; FAERS: Food and Drug Administration Adverse Event Reporting System.
Figure 1.
Database Pre-processing and Individual Case Safety Reports (ICSRs) Selection. ASCII: American standard code for information interchange; DORAs: Dual Orexin Receptor Antagonists; ICSRs: Individual Case Safety Reports; FAERS: Food and Drug Administration Adverse Event Reporting System.
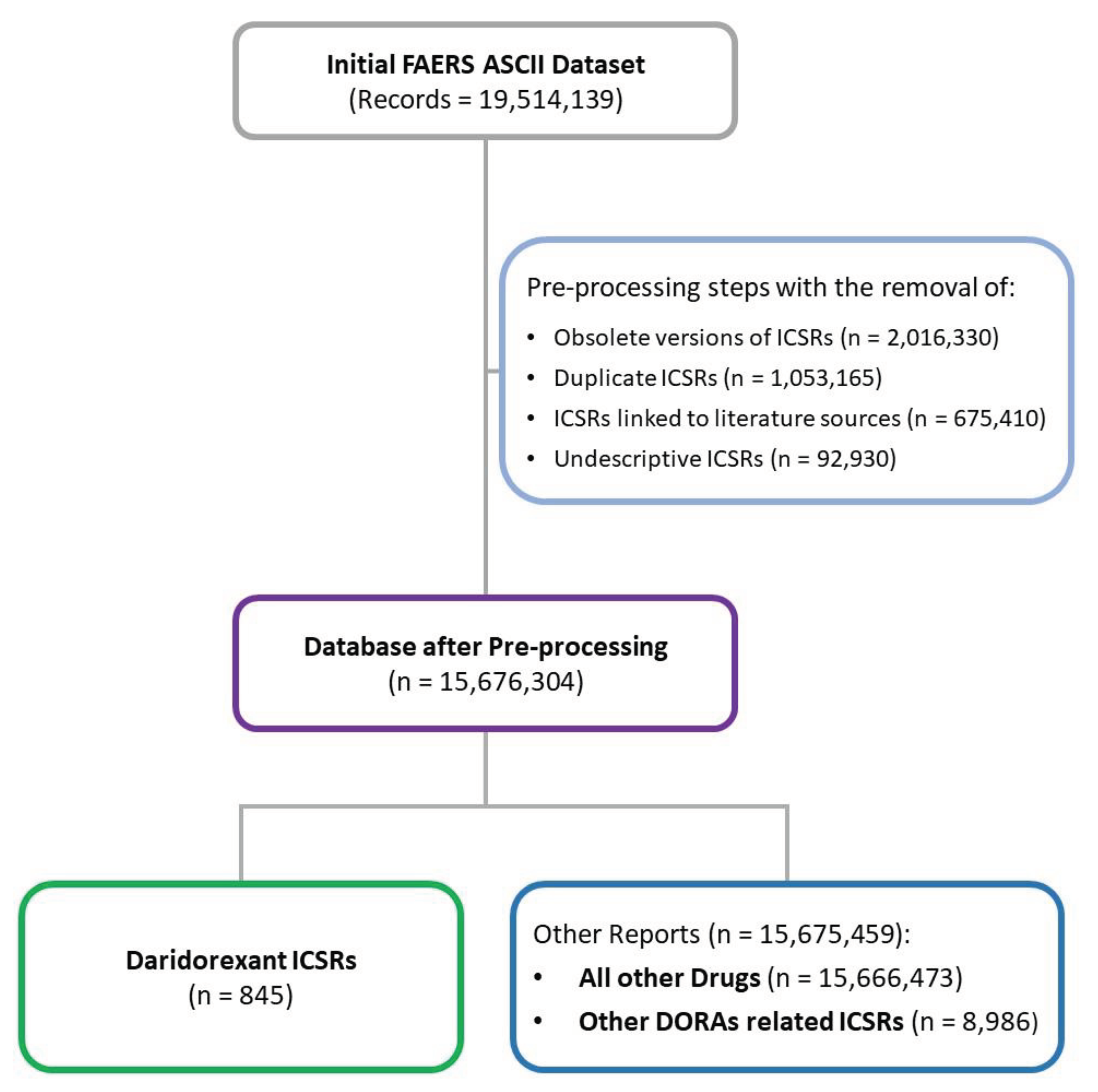

Table 1.
Demographic Characteristics in Daridorexant and Other DORAs related ICSRs.
| Characteristic | Daridorexant-related ICSRs (n = 845) |
Other DORAs related ICSRs (n = 8,986) |
|---|---|---|
| Sex, n° (%) | ||
| Women | 527 (62.4) | 4,914 (54.7) |
| Men | 275 (32.5) | 3,012 (33.5) |
| Not Available | 43 (5.9) | 1,060 (11.8) |
| Age Group, n° (%) | ||
| 0-17 | - | 25 (0.3) |
| 18-34 | 16 (1.9) | 288 (3.2) |
| 35-49 | 45 (5.3) | 591 (6.6) |
| 50-64 | 101 (12) | 1,065 (11.9) |
| 65-79 | 77 (9.1) | 1,254 (14.0) |
| 80+ | 22 (2.6) | 675 (7.5) |
| Not available | 584 (69.1) | 5,088 (56.6) |
| Reporter type, n° (%) | ||
| Consumer | 712 (84.3) | 3,426 (38.1) |
| Healthcare professional | 131 (15.5) | 5,549 (61.8) |
| Not specified | 2 (0.2) | 11 (0.1) |
| Seriousness, n° (%) | ||
| Not serious | 805 (95.3) | 7,427 (82.7) |
| Serious | 40 (4.7) | 1,559 (17.4) |
| Seriousness Criteria, n° (%) | ||
| Death | 9 (1.1) | 159 (1.8) |
| Disability | - | 73 (0.8) |
| Hospitalization | 3 (0.4) | 443 (4.9) |
| Life-Threatening | 1 (0.1) | 85 (0.9) |
| Other Serious Important Medical Event | 26 (3.1) | 797 (8.9) |
| Required Intervention | 1 (0.1) | 2 (0.0) |
| Not Available | 805 (95.3) | 7,427 (82.7) |
ICSRs: Individual Case Safety Reports.
Table 2.
Disproportionality analysis with daridorexant-related ADRs regrouped by MedDRA High-Level Group Terms.
Table 2.
Disproportionality analysis with daridorexant-related ADRs regrouped by MedDRA High-Level Group Terms.
| MedDRA HLGTs | ICSRsa |
Daridorexant vs. RG1 ROR [95%CI] |
Daridorexant vs. RG2 ROR [95%CI] |
| Sleep disorders and disturbances | 326 | 26.42 [23.01, 30.35] | 1.84 [1.59, 2.13] |
| Sleep disturbances (incl subtypes) | 32 | 20.63 [14.49, 29.37] | 0.91 [0.63, 1.31] |
| Disturbances in thinking and perception | 44 | 7.15 [5.28, 9.68] | 1.13 [0.82, 1.55] |
| Therapeutic and nontherapeutic effects (excl toxicity) | 311 | 4.74 [4.12, 5.46] | 1.05 [0.91, 1.21] |
| Changes in physical activity | 10 | 4.36 [2.34, 8.14] | 1.88 [0.95, 3.69] |
| Product quality, supply, distribution, manufacturing and quality system issues | 69 | 3.98 [3.11, 5.08] | 4.12 [3.1, 5.47] |
| Salivary gland conditions | 14 | 3.38 [1.99, 5.73] | 2.21 [1.24, 3.94] |
| Headaches | 69 | 2.34 [1.83, 3] | 1.66 [1.27, 2.15] |
| Anxiety disorders and symptoms | 40 | 1.79 [1.31, 2.46] | 1.01 [0.73, 1.41] |
| Depressed mood disorders and disturbances | 25 | 1.73 [1.16, 2.57] | 1.98 [1.29, 3.06] |
| Suicidal and self-injurious behaviours NEC | 16 | 1.63 [0.99, 2.67] | 0.96 [0.57, 1.61] |
| Neurological disorders NEC | 114 | 1.61 [1.32, 1.96] | 1 [0.81, 1.23] |
| Movement disorders (incl parkinsonism) | 26 | 1.48 [0.96, 2.18] | 1.16 [0.77, 1.75] |
| Cardiac disorders, signs and symptoms NEC | 16 | 1.46 [0.89, 2.39] | 1.56 [0.92, 2.64] |
| Overdoses and underdoses NEC | 23 | 1.45 [0.96, 2.19] | 0.85 [0.55, 1.3] |
| Allergic conditions | 30 | 1.43 [0.94, 2.07] | 6.71 [4.24, 10.63] |
| General system disorders NEC | 194 | 1.31 [1.12, 1.54] | 2.11 [1.77, 2.5] |
| Lifestyle issues | 10 | 1.2 [0.64, 2.23] | 3.25 [1.6, 6.62] |
| Deliria (incl confusion) | 11 | 1.19 [0.66, 2.16] | 0.6 [0.33, 1.11] |
| Medication errors and other product use errors and issues | 102 | 1.18 [0.96, 1.45] | 1.21 [0.97, 1.51] |
| Skin appendage conditions | 21 | 0.94 [0.61, 1.44] | 2.49 [1.54, 4.03] |
| Mood disorders and disturbances NEC | 11 | 0.7 [0.39, 1.27] | 0.98 [0.53, 1.83] |
| Muscle disorders | 14 | 0.56 [0.33, 0.95] | 0.95 [0.55, 1.64] |
| Cardiac and vascular investigations (excl enzyme tests) | 11 | 0.54 [0.3, 0.98] | 1.23 [0.66, 2.31] |
| Gastrointestinal signs and symptoms | 41 | 0.54 [0.39, 0.73] | 1.25 [0.9, 1.74] |
| Gastrointestinal motility and defaecation conditions | 21 | 0.52 [0.34, 0.81] | 1.65 [1.03, 2.62] |
| Epidermal and dermal conditions | 34 | 0.49 [0.35, 0.69] | 2.03 [1.4, 2.95] |
| HRespiratory disorders NEC | 22 | 0.45 [0.29, 0.69] | 1.33 [0.85, 2.08] |
HLGT: High Level Group Term; NEC: Not Elsewhere Classified; RG1: Reference Group 1; RG2: Reference Group 2. aHLGTs with less than 10 associated ICSRs were excluded from the table. MedDRA® Preferred Term disproportionality analysis and case-by-case assessment.
Table 3.
ADRs belonging to the MedDRA HLGT sleep disorders and disturbances classified by preferred terms.
Table 3.
ADRs belonging to the MedDRA HLGT sleep disorders and disturbances classified by preferred terms.
| MedDRA PTs | ICSRsa | Daridorexant vs. RG1 ROR [95%CI] |
Daridorexant vs. RG2 ROR [95%CI] |
Expb |
|---|---|---|---|---|
| Nightmare | 146 | 113.74 [95.13, 136] | 2.35 [1.93, 2.85] | Yes |
| Insomnia | 80 | 7.41 [5.88, 9.33] | 1.94 [1.51, 2.49] | No |
| Abnormal dreams | 64 | 52.79 [40.9, 68.13] | 1.16 [0.89, 1.52] | Yes |
| Somnambulism | 18 | 56.94 [35.67, 90.9] | 1.51 [0.91, 2.48] | Yes |
| Middle insomnia | 15 | 19.82 [11.89, 33.03] | 0.98 [0.58, 1.68] | No |
| Poor quality sleep | 10 | 11.51 [6.17, 21.48] | 0.55 [0.29, 1.04] | No |
| Sleep terror | 9 | 61.64 [31.93, 119.02] | 1.85 [0.91, 3.77] | No |
| Sleep-related eating disorder | 4 | 113.13 [42.23, 303.02] | 2.67 [0.89, 7.99] | Yes |
| Initial insomnia | 4 | 9.91 [3.71, 26.46] | 0.6 [0.22, 1.64] | No |
| Hypnagogic hallucination | 3 | 267.22 [85.32, 836.95] | 4 [1.06, 15.1] | Yes |
Exp: Expected; PT: Preferred Term; aPTs with less than 3 associated ICSRs were excluded from the table. bADR expectedness evaluated in accordance with US Food and Drug Administration (FDA) and European Medicine Agency Summary of Product Characteristics (SmPCs).
Table 4.
ADRs belonging to the MedDRA HLGT General system disorders NEC classified by preferred terms.
Table 4.
ADRs belonging to the MedDRA HLGT General system disorders NEC classified by preferred terms.
| MedDRA PTs | ICSRsa | Daridorexant vs. RG1 ROR [95%CI] |
Daridorexant vs. RG2 ROR [95%CI] |
Exp.b |
|---|---|---|---|---|
| Feeling abnormal | 64 | 6.19 [4.8, 7.99] | 1.75 [1.33, 2.29] | No |
| Fatigue | 45 | 1.41 [1.05, 1.91] | 2.28 [1.64, 3.17] | Yes |
| Hangover | 20 | 127.92 [81.98, 199.62] | 3.38 [2.04, 5.61] | Yes |
| Illness | 17 | 7.19 [4.44, 11.62] | 18.43 [8.41, 40.38] | No |
| Malaise | 12 | 0.61 [0.34, 1.07] | 1.07 [0.59, 1.95] | No |
| Feeling jittery | 6 | 6.89 [3.08, 15.37] | 1.25 [0.54, 2.93] | No |
| Asthenia | 6 | 0.37 [0.17, 0.83] | 1.16 [0.5, 2.71] | No |
| Energy increased | 5 | 18.7 [7.76, 45.06] | 6.68 [2.18, 20.47] | No |
| Crying | 5 | 2.95 [1.22, 7.1] | 2.67 [0.99, 7.13] | No |
| Concomitant disease aggravated | 4 | 15.43 [5.78, 41.23] | - | No |
| Sluggishness | 4 | 9.02 [3.38, 24.09] | 3.05 [0.99, 9.28] | Yes |
| Chest pain | 4 | 0.48 [0.18, 1.28] | 1.29 [0.46, 3.65] | No |
| Pain | 4 | 0.14 [0.05, 0.38] | 0.82 [0.29, 2.26] | No |
| Screaming | 3 | 10.74 [3.46, 33.39] | 2.66 [0.75, 9.46] | No |
| Discomfort | 3 | 1.16 [0.37, 3.6] | 2.91 [0.81, 10.44] | No |
| Swelling face | 3 | 1.06 [0.34, 3.3] | 2.91 [0.81, 10.44] | No |
| Condition aggravated | 3 | 0.27 [0.09, 0.83] | 1.88 [0.55, 6.43] | No |
aIndividual Case Safety Report; PTs with less than 3 associated ICSRs were excluded from the table. bExpected; ADR expectedness evaluated in accordance to USA Food and Drug Administration (FDA) and European Medicine Agency Summary of Product Characteristics (SmPCs).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



