
Submitted:
07 February 2024
Posted:
07 February 2024
You are already at the latest version
Abstract
Background
This study aimed to determine the association between immune checkpoint inhibitors (ICIs) and the risk of herpes zoster (HZ) incidence in patients with lung cancer.
Method
We obtained national claims data of 51,021 patients from South Korea with lung cancer between August 2017 and December 2021. The study population was classified into ICIs and non-ICIs groups based on prescription of ICIs at least once during the study period. To estimate the effects of ICIs treatment compared with those without ICIs treatment on HZ incidence, we used the Cox proportional hazards model adjusted for sex, age, comorbidities, and concomitant use of immunosuppressive drugs. Stratified analyses based on sex, age, and comorbidities were conducted to identify corresponding risk factors.
Results
Of the 51,021 study participants, 897 (1.8%) were prescribed ICIs, and 2,262 (4.4%) were diagnosed with HZ. Approximately 75.6% of the patients were male, and the prevalence of diabetes, cardiovascular disease, and chronic lung disease in the ICIs group was significantly lower than that in the non-ICIs group. The Kaplan–Meier plot showed that the probability of incidence of HZ in the ICIs group was lower than that in the non-ICIs group. Additionally, treatment with ICIs was associated with a 31% lower risk of developing HZ when compared to that seen without ICIs treatment (95% confidence interval [CI], 0.48–1.00). This association was stronger in females (hazard ratio [HR], 0.42; 95% CI, 0.19–0.94) and those less than 68 years of age (HR, 0.58; 95% CI, 0.34–0.99).
Conclusion
In these real-world data from an Asian population with lung cancer, ICIs treatment might be associated with a reduced risk of HZ compared to that without ICIs treatment.
Keywords:
herpes zoster
; immune checkpoint inhibitors
; standardized incidence ratio
; cancer patients
INTRODUCTION
Primary infection with varicella-zoster virus (VZV) results in chickenpox. Herpes zoster (HZ) is caused by the reactivation of latent VZV in the cranial nerve or dorsal-root ganglia, with the spread of the virus along the sensory nerve to the dermatome in the form of a painful vesicular rash [1]. In the general population, the incidence of HZ is 2 to 3 per 1,000 patients per year, and the lifetime risk is approximately 30% [2].
Reactivation of VZV is associated with a decline in cell-mediated immunity (CMI) against it [3], either as a natural consequence of aging or due to immunosuppression [4]. The major risk factor for development of HZ is old age, with an odds ratio (OR) of 1.20 (1.10–1.31) per five-year interval in individuals more than 65 years of age [5]. Immunocompromised individuals, including recipients of solid organ or hematopoietic stem cell transplants, those receiving chemotherapy for malignancies, and those with human immunodeficiency virus (HIV) infections are also at an increased risk of HZ. Patients undergoing cancer treatment have been reported to exhibit a higher incidence of HZ and severe symptoms and complications, such as disseminated skin lesions, pneumonia, meningitis, and hepatitis than those seen in the general population [6,7,8].
Cytotoxic chemotherapeutic agents and targeted therapies are commonly used to treat cancers. Over the past decade, however, the emergence of immune checkpoint blocking antibodies targeting cytotoxic T-lymphocyte antigen 4 (CTLA-4), programmed death receptor 1 (PD-1), and programmed death ligand 1 (PD-L1) has revolutionized the field of medical oncology. These monoclonal antibodies, known as immune checkpoint inhibitors (ICIs), are integral to the treatment of numerous cancers [9]. In contrast to the direct approach of targeting cancer cells for death included in conventional chemotherapy, ICIs function by blocking immune checkpoint pathways that serve as mechanisms for immune system regulation [10]. For example, PD-1 and its ligands play negative regulatory roles in the immune response. Consequently, anti-PD-1 antibodies are regarded as immunostimulatory agents that reactivate anergic cytotoxic T cells induced by tumor cells. Therefore, ICIs do not theoretically induce immunosuppression and the potential risk of infectious diseases associated with ICIs has garnered limited attention from physicians.
Limited studies have been performed on the impact of ICIs on reactivation of VZV, which is influenced by decreased CMI, specifically with regard to T-cell immunity. Published studies primarily consist of sporadic case reports [11,12,13] and retrospective analyses with small patient cohorts from a single center [14].
Therefore, in this study, we aimed to evaluate the incidence of HZ in patients with lung cancer receiving ICIs (ICIs group), such as PD-1 antibodies (nivolumab and pembrolizumab) or PD-L1 antibodies (atezolizumab and durvalumab), and compared it with that in patients receiving cytotoxic chemotherapeutic agents and/or targeted therapy (non-ICIs group) using real-world data. To investigate this relationship, we estimated the incidence of HZ in the ICIs and non-ICIs groups using the standardized incidence ratio (SIR) and we used a Cox proportional hazards model for data of patients with total and subgroup lung cancers, which was obtained from a nationwide claims database in South Korea.
2. METHODS
2.1. Study Design, Database, and Population
For this population-based retrospective cohort study, we used data from a nationwide claims database in South Korea (assigned number: Health Insurance Review and Assessment (HIRA) Research Data (M20220920004)). The National Health Insurance (NHI) system is a nonprofit health insurance program in South Korea. It serves as the central authority responsible for assessing and approving medical service fee coverage for the entire population, except for recipients of medical aid (3%), thereby ensuring high-quality healthcare. Healthcare providers are required to submit claims for reimbursement, which are then collected and assessed by the HIRA Service. The HIRA database provides de-identified demographic and clinical information related to submitted medical fees, general details with respect to patient specifications (age, sex, department, date of diagnosis, primary and secondary diagnoses, date of admission, and hospital arrival pathway), healthcare services (service category, drug codes, daily dosages, days and quantity of supply, and unit price), diagnosis information (main and sub-diagnosis), and details of outpatient prescriptions (drug codes, daily dosages, days and quantity of supply, and unit price).
In South Korea, NHI coverage for ICIs has been approved for patients with advanced non-small cell lung cancer (NSCLC) with stage IIIB or higher and who had been previously treated using platinum-containing chemotherapy, including the following: (1) nivolumab and pembrolizumab since August 2017, (2) atezolizumab since January 2018, and (3) durvalumab since April 2020, according to the PD-L1 expression rate. Considering the NHI coverage period, we obtained the national claims data of patients with lung cancer who were older than 18 years between August 2017 and December 2021. Adult patients with lung cancer were identified using the International Classification of Disease-10 (ICD-10) code C34 for primary or secondary diagnoses.
We excluded solid organ transplant patients (ICD-10 code, Z94); concealed data, including mental illness, rare diseases, sexually transmitted infections, and HIV; patients with hematologic malignancy (ICD-10 code, C81–96), patients who were not given chemotherapy; and patients who were prescribed two or more ICIs simultaneously. Additionally, patients treated with a combination of ICIs and untreated individuals were excluded to identify the effects of the ICIs.
2.2. Definitions and Outcomes
The ICIs-treated group included patients who were prescribed ICIs at least once after the diagnosis of lung cancer. Patients without a history of ICIs prescription during the study period were considered as the non-ICIs group. We defined the baseline as the date of first prescription of ICIs or as no prescription; non-ICIs after the diagnosis of lung cancer. The main outcome of interest was the diagnosis of HZ. New cases of HZ were identified by the presence of relevant diagnostic codes for HZ (ICD-10 code B02) in the claims data included in the study after the baseline. Additionally, in the development of HZ, the following potential confounding factors were identified based on claims records between the date of lung cancer diagnosis and the first prescription date of ICIs or non- prescription of ICIs: age; sex; diabetes; cardiovascular disease; chronic lung disease; chronic kidney disease; chronic liver disease; rheumatic disease; and concomitant use of immunosuppressants or steroids. Corticosteroid use was defined as the presence of prescription records for prednisone equivalents ≥ 15 mg/day for at least 14 days, with a prescription history during the study period or the preceding 12 months. All drug codes for ICIs, non-ICIs, corticosteroids, and immunosuppressants and ICD-10 codes for comorbidities are listed in Supplementary Table 1.
2.3. Statistical Analyses
Categorical data for the 10-year age groups, sex, comorbidities, and concomitant use of immunosuppressive drugs were compared using the χ2 test. Additionally, we identified the incidence rates of HZ events per 100,000 person-years (PYs) of follow-up based on the total and subgroups of sex and 10-year age according to ICI treatment. To evaluate the incidence of HZ in patients with lung cancer relative to the general population between August 2017 and December 2021, we obtained sex-, five-year age-, and year-specific HZ incidences in the general population from the Korean Statistical Information Service and estimated the SIR. The SIR was defined as the ratio between the observed and expected numbers of HZ, depending on treatment with ICIs. The expected number was determined by multiplying the PYs in the cohort by the incidence rate of HZ in the cancer population according to sex, age, and calendar year. Additionally, 95% confidence interval (CI) was calculated by assuming the number of HZ events followed a Poisson distribution.
To investigate the effects of ICI treatment compared to those without ICI treatment on the occurrence of HZ, we compared the probability of occurrence of HZ associated with ICIs using Kaplan–Meier plots. Differences were estimated using log-rank tests. Additionally, we presented the hazard ratios (HR) and 95% CI in a Cox-proportional hazards model adjusted for sex, age, comorbidities, concomitant use of immunosuppressants, and corticosteroid use. We also conducted stratified analyses according to sex, age (< 68 years and ≥ 68 years), diabetes, cardiovascular disease, chronic lung diseases, chronic kidney diseases, chronic liver diseases and rheumatic diseases, except for risk factors for which there were insufficient events to estimate the association. All reported p values were two-sided, and a p value of < 0.05 was considered as statistically significant. Data processing and statistical analyses were conducted using the R software version 4.0.3 (R Project for Statistical Computing).
3. RESULTS
3.1. Patient Disposition and Baseline Characteristics
During the study period, data of 88,375 adults (age >18 years) with the ICD code C34 for lung cancer were included. After excluding data of patients based on the exclusion criteria, records of 51,021 individuals who received chemotherapeutic regimens for lung cancer under the coverage of the NHI System were selected. Most patients with cancer included in this study were males and elderly. Of these, 897 (1.8%) patients were included in the ICIs group and the remaining 50,124 (98.2%) in the non-ICIs group (Figure 1). In the ICIs group, 126 (14.0 %), 2 (0.2 %), 309 (34.4 %), and 460 (51.3 %) patients received atezolizumab, durvalumab, nivolumab, and pembrolizumab, respectively. The prevalence of diabetes, cardiovascular disease, and chronic lung disease was significantly lower in the ICIs group than that in the non-ICIs group. The number of patients who received steroids was significantly higher in the non-ICIs group than that in the ICIs group. The baseline characteristics of the study population are presented in Table 1.
3.2. Incidence Rate and Standardized Incidence Ratio of HZ in the ICIs and Non-ICIs Groups
Table 2 presents HZ events, PYs, and incidence of lung cancer according to ICIs treatment. We observed 29 cases of HZ in 2,395.45 PYs in the ICI group and 2,233 cases of HZ for 119,537.78 PYs in the non-ICIs group. In an age-specific classification, the incidence of HZ was highest among individuals between 70–79 years in the ICI group (1,529.44, 95% CI: 882.22–2508.54) and 60–69 years in the non-ICIs group (2,099.38, 95% CI: 1968.17–2237.11). According to sex, male patients exposed to ICIs (1,270.54, 95% CI: 849.45–1839.98) showed higher incidence of HZ than that seen in females (1,025.29, 95% CI: 480.92–1993.90), while the incidence was converse in the non-ICIs group.
We estimated the SIR to compare the incidence of HZ in patients with lung cancer to that in the general population (Table 3). SIR values ranged between 0–5.75 in the ICIs group and 0.77–30.22 in the non-ICIs group. In the ICIs group, male patients between 70–79 years showed the highest incidence of HZ than that seen in the general population (5.75, 95% CI: 3.19–10.39), followed by that in the 60–69 years (5.37, 95% CI: 2.69–10.75) and 50–59 years (4.26, 95% CI: 1.07–17.05) age groups. Individuals more than 80 years of age showed a 1.98-fold higher incidence of HZ; however, the difference was not statistically significant (p = 0.99). We observed significantly greater SIR values among females in the 50–59 years (4.68, 95% CI: 1.17–18.72) and 60–69 years (3.99, 95% CI: 1.29–12.37) age groups. In the non-ICIs group, the highest SIR values were seen in both males and females (19.45, 95% CI: 9.73–38.90) < 40 years. The incidence rates of HZ among patients with lung cancer were higher than those in the general population across all age groups except for the ≥ 80 years group. We observed a 0.77-fold change (95% CI: 0.61–0.98) in HZ incidence for males and 0.91-fold change (0.62–1.35) for that in females. The ICI and non-ICI groups of patients with lung cancer exhibited higher SIR for HZ when compared to that for the general population, with a tendency of decreasing SIR values with increasing age.
3.3. Comparison of HZ Incidence between ICIs and Non-ICIs Groups
The probability of HZ incidence observed in the Kaplan–Meier plot is shown in Figure 2. The cumulative events of HZ 800 and 1,600 days from enrollment were 24 and 29 for the ICIs group, and 1,967 and 2,233 for the non-ICIs group, respectively. The probability of HZ occurrence in patients who were not treated with ICIs was higher than that in patients in the ICIs group; however, the difference between the groups was only slightly significant (p = 0.053).
3.4. Risk Factors for Development of HZ in Patients with Lung Cancer
Table 4 shows the HR values of HZ incidence associated with ICIs treatment compared to those without ICIs treatment in the unadjusted and adjusted Cox model analyses. With respect to satisfaction of the proportional hazards assumption by Schoenfeld residuals (p = 0.36) and graphical evaluation, ICIs were associated with a 31% lower risk of HZ (0–52%, p = 0.05) in the adjusted model. In sex-specific association, female patients in the ICIs group had lower risk of developing HZ than females in the non-ICIs group in both the unadjusted (HR, 0.43; 95% CI: 0.19–0.96, p = 0.04) and adjusted (HR, 0.42; 95% CI: 0.19–0.94, p = 0.04) models, while non-significant associations were observed in male patients. Additionally, ICIs compared to non-ICIs were associated with lower risk of HZ in patients < 68 years (HR, 0.58; 95% CI: 0.34–0.99, p = 0.05). With respect to comorbidity, significant association between ICI treatment and HZ incidence was observed in patients without chronic liver disease (HR, 0.68; 95% CI: 0.47–0.99, p = 0.05) and rheumatic diseases (HR, 0.65; 95% CI: 0.44–0.97, p = 0.03).
4. DISCUSSION
In the present study, we evaluated HZ incidence according to sex and age and the effects of ICIs on HZ events in a lung cancer cohort using a nationwide population-based database. The incidence rate and SIR of HZ in patients with lung cancer receiving cytotoxic chemotherapeutic agents and/or targeted therapy were higher than those in patients treated with ICIs; this disparity was more notable in younger patients. The probability of occurrence of HZ according to–Kaplan–Meier plots was higher in patients from the non-ICIs group than that in patients from the ICIs group, with a marginal degree of statistical significance (p = 0.053). We also confirmed that ICIs treatment was associated with a lower risk of HZ than that with without ICIs treatment (approximately 31%), and this association was stronger in females and in those < 68 years in age.
Previous one study showed that approximately 7% of patients in the United States diagnosed with malignant melanoma and treated with ICIs experience significant infectious complications [15]. Moreover, Pneumocystis pneumonia (PCP) and tuberculosis have been observed in patients treated with the nivolumab (PD-1 antibody) [16,17]. According to our understanding, however, treatment with ICIs does not exhibit elevated susceptibility to infections compared with alternative therapeutic approaches in current large randomized clinical trials [18,19,20,21]. In patients receiving PD-1/PD-L1 inhibitors, randomized trials have not shown an increased risk of infection [20,21]. A systematic review and meta-analysis reported a lower incidence of all-grade infections[22], and a retrospective case series showed that chronic viral reactivation was not observed in patients with HIV, hepatitis B virus (HBV), or hepatitis C virus (HCV) infections treated with ICIs[23].
Normally, VZV reactivation requires disrupted T cell-mediated VZV immunity[24]. Low VZV-specific CD4+ T cell responses correlate with severe HZ and complications such as post-herpetic neuralgia [25], and CD8+ T cell depletion might be associated with increased VZV reactivation.[26] During VZV reactivation, VZV-specific CD4+ T cells acquire elevated levels of T cell inhibitory markers CTLA-4 and PD-1[26,27]. Thus, the function of VZV-specific CD4+ T cells may be enhanced upon ICIs treatment by blocking inhibitory pathways and might protect against VZV reactivation. The induction of the PD-1/PD-L1 pathway during other viral infections has also been documented. Herpes simplex virus-1, another member of the alpha-herpesviridae subfamily, induces PD-1 expression during infection, and the inhibition of PD-L1 in mice enhances primary and secondary CD8+ T cell immune responses [28].
Nevertheless, there are mounting evidences of several mechanisms for the development of infections associated with the administration of ICIs [29]. Immunosuppression associated with immune checkpoint-related leukopenia could result in opportunistic infections [30]. However, mild to severe leukopenia associated with PD-1/PD-L1 blockade only occurred in 0.9% of patients, suggesting that this mechanism is less dominant [30]. Another hypothesis is that ICIs have the potential to trigger immune recovery, thereby facilitating the emergence of the immune reconstitution inflammatory syndrome (IRIS) and the reactivation of latent/chronic infectious diseases with latency. Case reports in which the development of tuberculosis [16,31], VZV induced encephalitis [32] and pulmonary nocardiosis [33] in patients receiving PD-1/PD-L1 inhibitors without immunosuppressive treatment were considered the possibility that IRIS might have been involved. In animal models, PD-1 deficient mice were more susceptible to mycobacterium infection than wild-type mice, and they showed more evidence of fulminant infectious processes [34,35] with tissue damage by excessive production of IFN-gamma in effector T cells[36]. In HIV patients, VZV-IRIS has been associated with an increase in circulating CD8+ T cells after 1 month on ART or 1 month before the onset of HZ [37]. However, whether HZ susceptibility in patients with solid cancer could be clinically increased by the dysregulated immunity due to ICIs has not yet been clarified. The analysis of T cell subsets (CD4+, CD8+, regulatory T cells, etc.) at baseline and at the onset of HZ in patients receiving ICIs treatment may be useful in elucidating the mechanism underlying HZ incidence.
Notably, this observation does not diminish the importance of HZ prevention in lung cancer patients undergoing ICIs monotherapy. Patients undergoing cancer treatment have been reported to have a higher incidence and severe symptoms of HZ than the general population [7,8]. In this study, the group receiving only ICIs also exhibited a high SIR for HZ compared with that seen in the general population across all age groups (Table 3). Additionally, autoimmune phenomena known as immune-related adverse events (irAEs) induced by PD-1/PD-L1 inhibitors may require treatment with immunosuppressive agents such as corticosteroids or antitumor necrosis factor agents, and these could contribute to the development of HZ or other opportunistic infections in this patient population [38]. Currently, there is a consensus recommending prophylaxis against HZ in patients receiving immunosuppressive regimens due to immunotherapy-related toxicities [39]. Moreover, misdiagnosis of infections can lead to delayed diagnosis and treatment, as well as deterioration of the infectious condition due to the administration of corticosteroids and other immunosuppressants used for managing suspected irAEs. Therefore, it is crucial to differentiate between irAEs and infections. Substantial data similar to the findings of this study is required to serve as a foundation for understanding the immunobiology of various infectious diseases.
This is the first study to investigate the effects of ICIs on the risk of HZ in patients with lung cancer in South Korea. We used data on a nationwide population from the HIRA health insurance claims database. A similar study investigating the association between the rate of HZ and ICIs treatment was conducted in Japan; however, it cannot be considered representative because of the small number of participants (n = 436) included in the study [14]. Multivariate analysis was conducted to control potential confounders after adjusting for a range of variables in the risk factor analysis. Finally, the SIR was accurately calculated based on the annual statistics of reported HZ cases and the general population census data published by the Korean government.
However, this study had several limitations that must be considered when interpreting the results. First, owing to the observational nature of the claims database, HZ cases may have been underestimated or misclassified, and the severity of HZ was not assessed. Second, the dosage of ICIs was not considered. Third, there was a large difference in the number of patients in the ICIs and non-ICIs groups, and effects of only a limited number of ICIs (atezolizumab, durvalumab, nivolumab, and pembrolizumab), mostly pembrolizumab, were evaluated. Consequently, it was impossible to ascertain the differential effects of ICIs on the risk of developing HZ. Fourth, our assessment was limited specifically to lung cancer. In South Korea, ICI treatment is covered by insurance for lung cancer, hepatocellular carcinoma, bladder cancer, melanoma, and renal cell cancer. Among these, cancers treated with cytotoxic chemotherapeutic agents only include lung and bladder cancers. Targeted therapies are also used for other diseases, resulting in fewer immunosuppressive side effects and a lower incidence of infectious diseases. Therefore, the target disease groups that aligned with the analytical objectives of this study were lung and bladder cancers. Considering the frequency of the disease, as the rate of lung cancer is significantly high, and this study focused on patients with lung cancer. Further investigations are warranted to elucidate the risk of HZ in patients with different cancer types and those receiving treatment with other types of ICIs such as anti-CTLA-4, anti-LAG-3, and anti-TIM-3 inhibitors. Fifth, HZ vaccination status of patients could not be ascertained in this study. However, during the study period, the only available vaccines for HZ were all live attenuated vaccines (Zostervax®) and the recombinant HZ vaccine (Shingrix®) officially released in December 2022 in South Korea. Therefore, it can be speculated that the HZ vaccination rate among cancer patients may not have been high because of concerns regarding live vaccines. Finally, we were unable to verify HIV infection status of from patient records, which is one of the most significant risk factors for HZ. This is because the HIRA database provides claims data with concealed individual identification of patients with HIV. However, because the data was concealed the overall patient population, we believe that this did not have a significant impact on the findings of this study.
In summary, among patients with lung cancer, the incidence of HZ was lower in the ICIs group than that in the non-ICIs group. As the use of ICIs is expected to gradually increase in treatment of various cancers in the future, it requires resolving of these challenges by large prospective observational studies in order to maximize the clinical benefits of immunotherapy uninterruptedly and safely.
Author Contributions
Jiyun Jung and Sungim Choi wrote the manuscript, performed data curation and evaluation, statistical evaluation, prepared all figures, tables and supplementary materials. Seong Yeon Park, Jae Yoon Park, Dalyong Kim and Kyoungmin Lee participated in study supervision and review and edit for manyscript. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the Dongguk University Research Fund of 2022.
Institutional Review Board Statement
This study was approved by the Institutional Review Board Committee of the Dongguk University Ilsan Medical Center (2022-09-005).
Informed Consent Statement
The requirement for informed consent was waived because this retrospective study was limited to the identification of personal information.
Consent for publication
Not applicable.
Data Availability Statement
In terms of the further use of our data, we ask researchers to cite our paper in their Method section. Data presented in this study are available upon request from the corresponding author.
Conflicts of Interest
The authors declare that they have no conflict of interest.
References
- Cohen JI. Herpes zoster. N Engl J Med. 2013, 369, 1766–7. [CrossRef]
- Gershon AA, Gershon MD, Breuer J, Levin MJ, Oaklander AL, Griffiths PD. Advances in the understanding of the pathogenesis and epidemiology of herpes zoster. J Clin Virol. 2010, 48 (Suppl 1), S2–7. [CrossRef]
- Oxman MN. Immunization to reduce the frequency and severity of herpes zoster and its complications. Neurology. 1995, 45 (Suppl 8), S41–6. [CrossRef]
- Arvin AM, Moffat JF, Redman R. Varicella-zoster virus: aspects of pathogenesis and host response to natural infection and varicella vaccine. Adv Virus Res. 1996, 46, 263–309. [CrossRef]
- Donahue JG, Choo PW, Manson JE, Platt R. The incidence of herpes zoster. Arch Intern Med. 1995, 155, 1605–9.
- McKay SL, Guo A, Pergam SA, Dooling K. Herpes Zoster Risk in Immunocompromised Adults in the United States: A Systematic Review. Clin Infect Dis. 2020, 71, e125–e134. [CrossRef]
- Lin YH, Huang LM, Chang IS, et al. Disease burden and epidemiology of herpes zoster in pre-vaccine Taiwan. Vaccine. 2010, 28, 1217–20. [CrossRef]
- 8. Yenikomshian MA, Guignard AP, Haguinet F, et al. The epidemiology of herpes zoster and its complications in Medicare cancer patients. BMC Infect Dis. 2015, 15, 106. [CrossRef]
- Ribas A, Wolchok JD. Cancer immunotherapy using checkpoint blockade. Science. 2018, 359, 1350–1355. [CrossRef] [PubMed]
- Dine J, Gordon R, Shames Y, Kasler MK, Barton-Burke M. Immune Checkpoint Inhibitors: An Innovation in Immunotherapy for the Treatment and Management of Patients with Cancer. Asia Pac J Oncol Nurs. 2017, 4, 127–135. [CrossRef] [PubMed]
- Watanabe Y, Kikuchi R, Iwai Y, et al. Varicella zoster virus encephalitis mimicking nivolumab-induced autoimmune neuropathy in a patient with lung cancer. Journal of Thoracic Oncology. 2019, 14, e163–e165. [CrossRef]
- Sakoh T, Kanzaki M, Miyamoto A, et al. Ramsay-Hunt syndrome and subsequent sensory neuropathy as potential immune-related adverse events of nivolumab: a case report. BMC Cancer. 2019, 19, 1220. [CrossRef]
- Gozzi E, Rossi L, Angelini F, et al. Herpes zoster granulomatous dermatitis in metastatic lung cancer treated with nivolumab: A case report. Thorac Cancer. 2020, 11, 1330–1333. [CrossRef]
- Taoka M, Ochi N, Yamane H, et al. Herpes zoster in lung cancer patients treated with PD-1/PD-L1 inhibitors. Transl Cancer Res. 2022, 11, 456–462. [CrossRef]
- Del Castillo M, Romero FA, Argüello E, Kyi C, Postow MA, Redelman-Sidi G. The spectrum of serious infections among patients receiving immune checkpoint blockade for the treatment of melanoma. Clinical Infectious Diseases. 2016, 63, 1490–1493. [CrossRef] [PubMed]
- Fujita K, Terashima T, Mio T. Anti-PD1 Antibody Treatment and the Development of Acute Pulmonary Tuberculosis. J Thorac Oncol. 2016, 11, 2238–2240. [CrossRef] [PubMed]
- Kim HR, Keam B, Park YS, et al. Pneumocystis Pneumonia Developing during Treatment of Recurrent Renal Cell Cancer with Nivolumab. The Korean Journal of Medicine. 2018, 93, 571–574. [CrossRef]
- Topalian SL, Hodi FS, Brahmer JR, et al. Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N Engl J Med. 2012, 366, 2443–54. [CrossRef] [PubMed]
- Brahmer JR, Tykodi SS, Chow LQ, et al. Safety and activity of anti-PD-L1 antibody in patients with advanced cancer. N Engl J Med. 2012, 366, 2455–65. [CrossRef] [PubMed]
- Eigentler TK, Hassel JC, Berking C, et al. Diagnosis, monitoring and management of immune-related adverse drug reactions of anti-PD-1 antibody therapy. Cancer Treat Rev. 2016, 45, 7–18. [CrossRef] [PubMed]
- Fehrenbacher L, Spira A, Ballinger M, et al. Atezolizumab versus docetaxel for patients with previously treated non-small-cell lung cancer (POPLAR): a multicentre, open-label, phase 2 randomised controlled trial. Lancet. 2016, 387, 1837–46. [CrossRef]
- Petrelli F, Morelli AM, Luciani A, Ghidini A, Solinas C. Risk of Infection with Immune Checkpoint Inhibitors: A Systematic Review and Meta-analysis. Target Oncol. 2021, 16, 553–568. [CrossRef] [PubMed]
- Shah NJ, Al-Shbool G, Blackburn M, et al. Safety and efficacy of immune checkpoint inhibitors (ICIs) in cancer patients with HIV, hepatitis B, or hepatitis C viral infection. J Immunother Cancer. 2019, 7, 353. [CrossRef]
- Weinberg A, Levin MJ. VZV T cell-mediated immunity. Curr Top Microbiol Immunol. 2010, 342, 341–57. [CrossRef]
- Abendroth A, Lin I, Slobedman B, Ploegh H, Arvin AM. Varicella-zoster virus retains major histocompatibility complex class I proteins in the Golgi compartment of infected cells. J Virol. 2001, 75, 4878–88. [CrossRef]
- Laing KJ, Ouwendijk WJD, Koelle DM, Verjans G. Immunobiology of Varicella-Zoster Virus Infection. J Infect Dis. 2018, 218 (suppl_2), S68–S74. [CrossRef] [PubMed]
- Zangeneh Z, Golmoghaddam H, Emad M, Erfani N, Doroudchi M. Elevated PD-1 expression and decreased telomerase activity in memory T cells of patients with symptomatic Herpes Zoster infection. Cell Mol Biol (Noisy-le-grand). 2014, 60, 13–21.
- Channappanavar R, Twardy BS, Suvas S. Blocking of PDL-1 interaction enhances primary and secondary CD8 T cell response to herpes simplex virus-1 infection. PLoS One. 2012, 7, e39757. [CrossRef]
- Hamashima R, Uchino J, Morimoto Y, et al. Association of immune checkpoint inhibitors with respiratory infections: A review. Cancer Treat Rev. 2020, 90, 102109. [CrossRef]
- Delanoy N, Michot JM, Comont T, et al. Haematological immune-related adverse events induced by anti-PD-1 or anti-PD-L1 immunotherapy: a descriptive observational study. Lancet Haematol. 2019, 6, e48–e57. [CrossRef]
- Anastasopoulou A, Ziogas DC, Samarkos M, Kirkwood JM, Gogas H. Reactivation of tuberculosis in cancer patients following administration of immune checkpoint inhibitors: current evidence and clinical practice recommendations. J Immunother Cancer. 2019, 7, 239. [CrossRef]
- Watanabe Y, Kikuchi R, Iwai Y, et al. Varicella Zoster Virus Encephalitis Mimicking Nivolumab-Induced Autoimmune Neuropathy in a Patient with Lung Cancer. J Thorac Oncol. 2019, 14, e163–e165. [CrossRef]
- Lasagna A, Arlunno B, Imarisio I. A case report of pulmonary nocardiosis during pembrolizumab: the emerging challenge of the infections on immunotherapy. Immunotherapy. 2022, 14, 1369–1375. [CrossRef] [PubMed]
- Lazar-Molnar E, Chen B, Sweeney KA, et al. Programmed death-1 (PD-1)-deficient mice are extraordinarily sensitive to tuberculosis. Proc Natl Acad Sci U S A. 2010, 107, 13402–7. [CrossRef] [PubMed]
- Tousif S, Singh Y, Prasad DV, Sharma P, Van Kaer L, Das G. T cells from Programmed Death-1 deficient mice respond poorly to Mycobacterium tuberculosis infection. PLoS One. 2011, 6, e19864. [CrossRef]
- Sakai S, Kauffman KD, Sallin MA, et al. CD4 T Cell-Derived IFN-gamma Plays a Minimal Role in Control of Pulmonary Mycobacterium tuberculosis Infection and Must Be Actively Repressed by PD-1 to Prevent Lethal Disease. PLoS Pathog. 2016, 12, e1005667. [CrossRef]
- Price P, Murdoch DM, Agarwal U, Lewin SR, Elliott JH, French MA. Immune restoration diseases reflect diverse immunopathological mechanisms. Clin Microbiol Rev. 2009, 22, 651–63. [CrossRef] [PubMed]
- Liu Z, Liu T, Zhang X, et al. Opportunistic infections complicating immunotherapy for non-small cell lung cancer. Thorac Cancer. 2020, 11, 1689–1694. [CrossRef]
- Thompson JA, Schneider BJ, Brahmer J, et al. Management of Immunotherapy-Related Toxicities, Version 1.2019. J Natl Compr Canc Netw. 2019, 17, 255–289. [CrossRef]
Figure 1.
Flow chart showing details of the study population. ICD-10, International Classification of Diseases-10; HIV, human immunodeficiency virus; ICIs, immune checkpoint inhibitors.
Figure 1.
Flow chart showing details of the study population. ICD-10, International Classification of Diseases-10; HIV, human immunodeficiency virus; ICIs, immune checkpoint inhibitors.
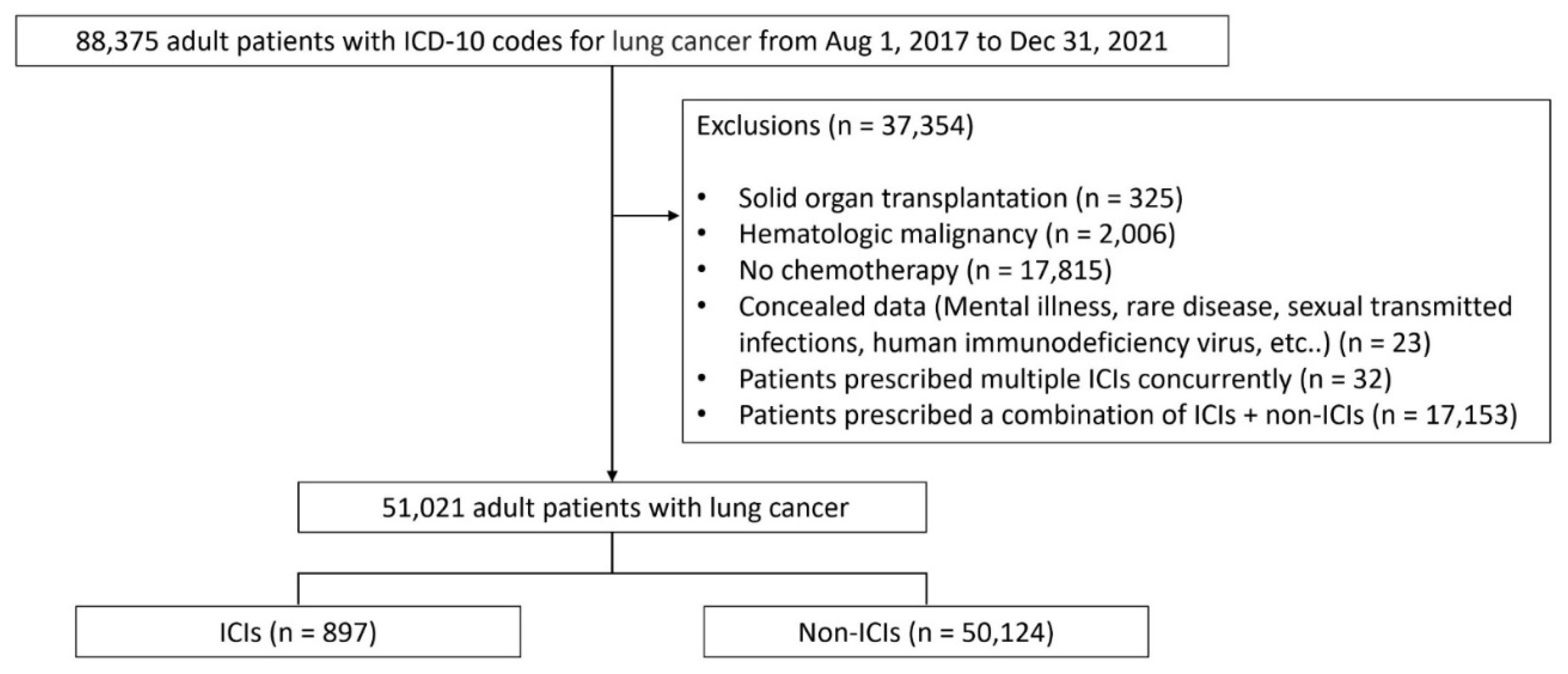
Figure 2.
Kaplan–Meier curves showing the timeframe (in days) from study enrollment to events of herpes zoster (HZ) in the study population upon cancer treatment.
Figure 2.
Kaplan–Meier curves showing the timeframe (in days) from study enrollment to events of herpes zoster (HZ) in the study population upon cancer treatment.
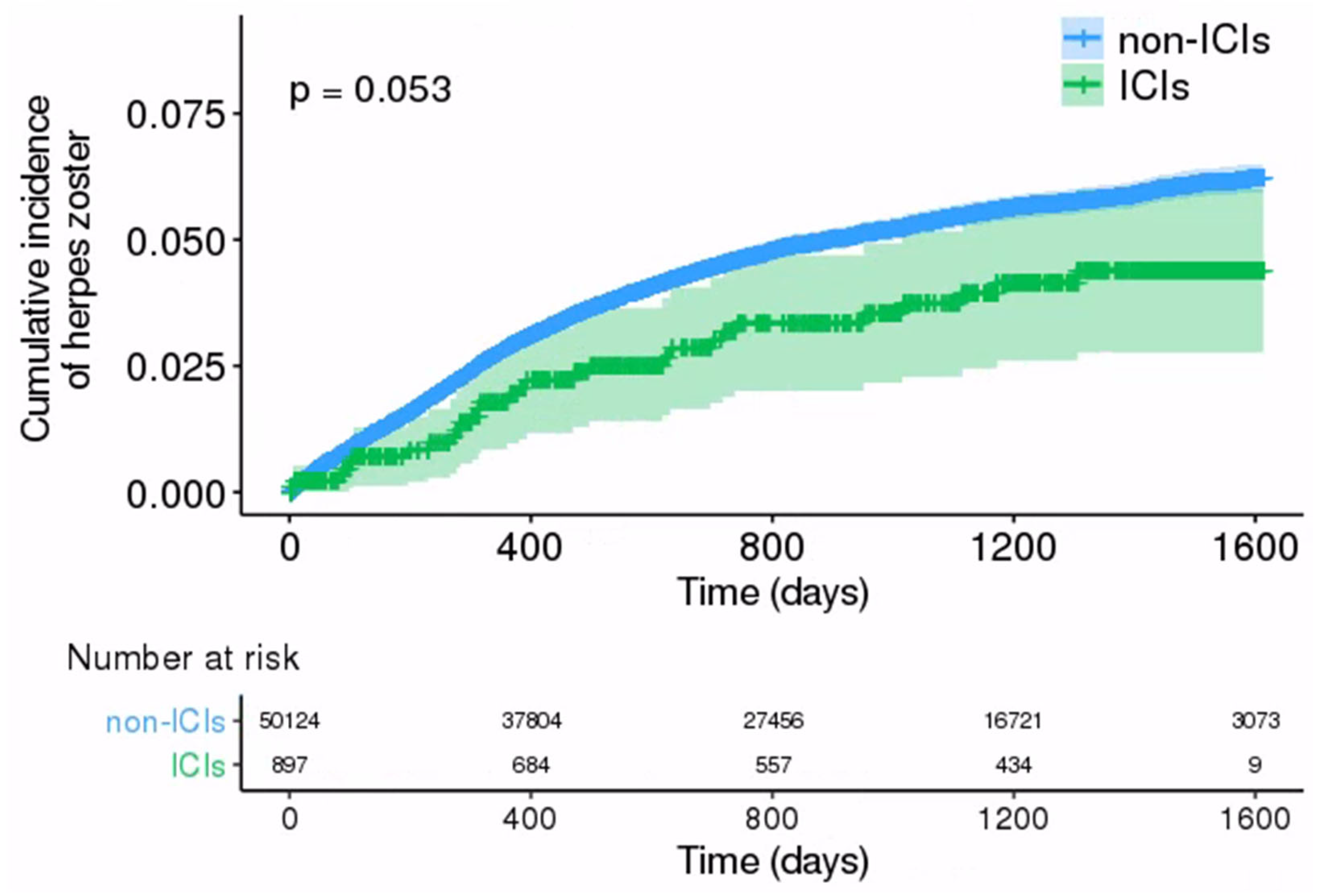

Table 1.
Baseline characteristics of patients with lung cancer treated with immune checkpoint inhibitors (ICIs) or comparator non-ICIs.
Table 1.
Baseline characteristics of patients with lung cancer treated with immune checkpoint inhibitors (ICIs) or comparator non-ICIs.
| ICIs | Non-ICIs (n = 50,124) |
p-value | |||||
|---|---|---|---|---|---|---|---|
| Atezolizumab (n = 126) |
Durvalumab (n = 2) |
Nivolumab (n = 309) |
Pembrolizumab (n = 460) |
Total (n = 897) |
|||
| Age (year), n (%) | 0.008 | ||||||
| < 40 (%) | 1 (0.8) | 0 (0) | 1 (0.3) | 4 (0.9) | 6 (0.7) | 475 (0.9) | |
| 40–50 (%) | 10 (7.9) | 0 (0) | 18 (5.8) | 16 (3.5) | 44 (4.9) | 2,019 (4.0) | |
| 50–60 (%) | 22 (17.5) | 0 (0) | 55 (17.8) | 79 (17.2) | 156 (17.4) | 8,040 (16.0) | |
| 60–70 (%) | 42 (33.3) | 2 (100) | 116 (37.5) | 143 (31.1) | 303 (33.8) | 18,395 (36.7) | |
| 70–80 (%) | 43 (34.1) | 0 (0) | 96 (31.1) | 159 (34.6) | 298 (33.2) | 17,555 (35.0) | |
| ≥ 80 (%) | 8 (6.3) | 0 (0) | 23 (7.4) | 59 (12.8) | 90 (10.0) | 3,640 (7.3) | |
| Sex, n (%) | 0.3112 | ||||||
| Male | 89 (70.6) | 2 (100) | 253 (81.9) | 334 (72.6) | 678 (75.6) | 37,109 (74.0) | |
| Female | 37 (29.4) | 0 (0) | 56 (18.1) | 126 (27.4) | 219 (24.4) | 13,015 (26.0) | |
| Comorbidity, n (%) | |||||||
| Diabetes | 51 (40.5) | 0 (0) | 106 (34.3) | 193 (42.0) | 350 (39.0) | 21,708 (43.3) | 0.011 |
| Cardiovascular disease* | 51 (40.5) | 0 (0) | 81 (26.2) | 169 (36.7) | 301 (33.6) | 20,791 (41.5) | <0.001 |
| Chronic lung diseases | 94 (74.6) | 1 (50) | 199 (64.4) | 307 (66.7) | 601 (67.0) | 36,234 (72.3) | 0.001 |
| Chronic kidney diseases | 12 (9.5) | 0 (0) | 18 (5.8) | 29 (6.3) | 59 (6.6) | 2,751 (5.5) | 0.179 |
| Chronic liver diseases | 6 (4.8) | 0 (0) | 10 (3.2) | 9 (2.0) | 25 (2.8) | 1,404 (2.8) | 1.000 |
| Rheumatic diseases | 9 (7.1) | 0 (0) | 7 (2.3) | 32 (7.0) | 48 (5.4) | 3,221(6.4) | 0.217 |
|
Concomitant use of immunosuppressive drugs, n (%) |
|||||||
| Immunosuppressant | 10 (7.9) | 0 (0) | 6 (1.9) | 15 (3.3) | 31 (3.5) | 2,428 (4.8) | 0.065 |
| Steroid** | 4 (3.2) | 0 (0) | 12 (3.9) | 18 (3.9) | 34 (3.8) | 3,386 (6.8) | 0.001 |
* Includes ischemic heart disease, cerebrovascular disease, and diseases of the arteries, arterioles, and capillaries. ** includes the use of corticosteroids defined as the presence of prescription records for prednisone equivalents ≥15 mg/day for at least 14 days.
Table 2.
Incidence of herpes zoster corresponding to treatment with immune checkpoint inhibitors (ICIs).
Table 2.
Incidence of herpes zoster corresponding to treatment with immune checkpoint inhibitors (ICIs).
| ICIs | Non-ICIs | |||||
|---|---|---|---|---|---|---|
| Event (n) | Person-years | Incidence* (95% CI) | Event (n) | Person-years | Incidence* (95% CI) | |
| Total | 29 | 2,395.45 | 1,210.63 (844.97–1689.36) | 2,233 | 119,537.78 | 1,868.03 (1791.34–1945.44) |
| Age, n (%) | ||||||
| < 40 | 0 | 13.92 | 0 (0–0) | 19 | 1,166.73 | 1,628.48 (1047.07–2438.24) |
| 40–49 | 0 | 131.22 | 0 (0–0) | 74 | 5,042.06 | 1,467.65 (1170.00–1820.42) |
| 50–59 | 4 | 446.80 | 895.25 (363.36–1962.22) | 410 | 20,084.68 | 2,041.36 (1853.26–2243.62) |
| 60–69 | 11 | 849.69 | 1,294.60 (729.75–2164.36) | 921 | 43,870.17 | 2,099.38 (1968.17–2237.11) |
| 70–79 | 12 | 784.60 | 1,529.44 (882.22–2508.54) | 716 | 41,251.46 | 1,735.70 (1610.87–1862.60) |
| ≥ 80 | 2 | 169.22 | 1,181.90 (365.61–3292.58) | 93 | 8,122.67 | 1,144.94 (935.18–1389.07) |
| Sex, n (%) | ||||||
| Male | 23 | 1,810.25 | 1,270.54 (849.45–1839.98) | 1,471 | 89,520.82 | 1,643.19 (1561.37–1728.22) |
| Female | 6 | 585.20 | 1,025.29 (480.92–1993.90) | 762 | 30,016.96 | 2,538.56 (2364.71–2721.94) |
* Incidence per 100,000 person-years (PYs). CI, confidence interval.
Table 3.
Standardized incidence ratio (SIR) of herpes zoster for the general population with 95% confidence interval (CI), according to treatment, age, and sex.
Table 3.
Standardized incidence ratio (SIR) of herpes zoster for the general population with 95% confidence interval (CI), according to treatment, age, and sex.
| ICIs | Non-ICIs | |||||||
|---|---|---|---|---|---|---|---|---|
| Observed event (n) | Expected event (n) | SIR (95% CI) | p-value | Observed event (n) | Expected event (n) | SIR (95% CI) | p-value | |
| Male | ||||||||
| < 40 | 0 | 0.01 | 0 (0–0) | 1.00 | 11 | 0.36 | 30.22 (16.74–54.57) | < 0.01 |
| 40–49 | 0 | 0.10 | 0 (0–0) | 1.00 | 37 | 3.16 | 11.69 (8.47–16.13) | < 0.01 |
| 50–59 | 2 | 0.47 | 4.26 (1.07–17.05) | 0.04 | 224 | 21.01 | 10.66 (9.35–12.15) | < 0.01 |
| 60–69 | 18 | 1.49 | 5.37 (2.69–10.75) | < 0.01 | 609 | 78.64 | 7.74 (7.15–8.38) | < 0.01 |
| 70–79 | 11 | 1.91 | 5.75 (3.19–10.39) | < 0.01 | 521 | 98.19 | 5.32 (4.88–5.79) | < 0.01 |
| ≥ 80 | 2 | 1.98 | 1.01 (0.25–4.04) | 0.99 | 68 | 88.02 | 0.77 (0.61–0.98) | 0.03 |
| Female | ||||||||
| < 40 | 0 | 0 | 0 (0–0) | 1.00 | 8 | 0.41 | 19.45 (9.73–38.90) | < 0.01 |
| 40–49 | 0 | 0.08 | 0 (0–0) | 1.00 | 37 | 4.12 | 8.99 (6.51–12.40) | < 0.01 |
| 50–59 | 2 | 0.43 | 4.68 (1.17–18.72) | 0.03 | 186 | 19.34 | 9.62 (8.33–11.10) | < 0.01 |
| 60–69 | 3 | 0.75 | 3.99 (1.29–12.37) | 0.02 | 312 | 36.09 | 8.65 (7.74–9.66) | < 0.01 |
| 70–79 | 1 | 0.51 | 1.96 (0.28–13.9) | 0.50 | 194 | 29.60 | 6.55 (5.69–7.54) | < 0.01 |
| ≥ 80 | 0 | 0.43 | 0 (0–0) | 1.00 | 25 | 27.43 | 0.91 (0.62–1.35) | 0.64 |
Table 4.
Hazard ratio (HR) values of herpes zoster incidence associated with immune checkpoint inhibitors (ICIs) compared to that for non-ICIs.
Table 4.
Hazard ratio (HR) values of herpes zoster incidence associated with immune checkpoint inhibitors (ICIs) compared to that for non-ICIs.
| Unadjusted | Adjusted | |||
|---|---|---|---|---|
| HR (95% CI) | P-value | HR (95% CI) | p-value | |
| Total | 0.70 (0.48–1.01) | 0.05 | 0.69 (0.48–1.00) | 0.05 |
| Sex | ||||
| Male | 0.84 (0.55–1.26) | 0.39 | 0.84 (0.55–1.26) | 0.40 |
| Female | 0.43 (0.19–0.96) | 0.04 | 0.42 (0.19–0.94) | 0.04 |
| Age | ||||
| < 68 years | 0.59 (0.35–0.99) | 0.05 | 0.58 (0.34–0.99) | 0.05 |
| ≥ 68 years | 0.84 (0.51–1.40) | 0.51 | 0.84 (0.50–1.40) | 0.50 |
| Diabetes | ||||
| No | 0.81 (0.53–1.23) | 0.32 | 0.84 (0.55–1.28) | 0.41 |
| Yes | 0.49 (0.23–1.03) | 0.06 | 0.48 (0.23–1.01) | 0.05 |
| Cardiovascular disease | ||||
| No | 0.65 (0.42–1.01) | 0.06 | 0.65 (0.41–1.01) | 0.05 |
| Yes | 0.80 (0.42–1.55) | 0.52 | 0.85 (0.44–1.64) | 0.63 |
| Chronic lung diseases | ||||
| No | 0.59 (0.32–1.11) | 0.10 | 0.58 (0.31–1.09) | 0.09 |
| Yes | 0.76 (0.48–1.19) | 0.23 | 0.76 (0.48–1.20) | 0.24 |
| Chronic kidney diseases | ||||
| No | 0.71 (0.49–1.03) | 0.07 | 0.70 (0.48–1.02) | 0.07 |
| Yes | 0.52 (0.07–3.74) | 0.52 | 0.52 (0.07–3.89) | 0.53 |
| Chronic liver diseases | ||||
| No | 0.68 (0.47–0.99) | 0.05 | 0.68 (0.47–0.99) | 0.05 |
| Yes | 1.57 (0.22–11.41) | 0.65 | 1.18 (0.13–10.91) | 0.88 |
| Rheumatic diseases | ||||
| No | 0.66 (0.45–0.97) | 0.03 | 0.65 (0.44–0.97) | 0.03 |
| Yes | 1.52 (0.48–4.78) | 0.47 | 1.76 (0.52–5.93) | 0.36 |
CI, confidence interval.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



