Submitted:
29 January 2024
Posted:
30 January 2024
You are already at the latest version
Abstract
The 2022-2023 Mpox multi-country outbreak, identified in over 110 WHO Member States, revealed a predominant impact on cisgender men, particularly those engaging in sex with men, while less frequently affecting women. This disparity prompted a focused investigation into the gender-specific characteristics of Mpox infections, particularly among women, to address a notable knowledge gap. This review systematically gathers and analyzes scientific literature and case reports concerning Mpox infections in women, covering a broad geographical spectrum including regions such as Buenos Aires, Brazil, Northern California, Colombia, Nigeria, Europe, Vietnam, Spain, Switzerland, and the United States. The analysis delves into various aspects of Mpox in women, including clinical features, epidemiology, psychological impacts, preparedness strategies, and case studies, with particular attention to pregnant women and those with underlying health conditions. Empirical data from multiple studies underscore the unique epidemiological and clinical patterns of Mpox in women. In the United States, a small percentage of Mpox cases were reported among cisgender women, with a notable portion involving non-Hispanic Black or African American, non-Hispanic White, and Hispanic or Latino ethnicities. The primary transmission route was identified as sexual or close intimate contact, with the virus predominantly manifesting on the legs, arms, and genital areas. Further, a study in Spain highlighted significant disparities in diagnosis delays, transmission modes, and clinical manifestations between genders, indicating a different risk profile and disease progression in women. Additionally, a case from Vietnam linked to a new Mpox sublineage in women emphasizes the role of women in the transmission dynamics and the importance of genomic monitoring. This review emphasizes the necessity for inclusive surveillance and research to fully understand Mpox dynamics across diverse population groups, including women. Highlighting gender and sexual orientation in public health responses is crucial for an effective approach to managing the spread and impact of the disease. The findings advocate for a gender-diverse assessment in health services and further research to explore the nuances of Mpox transmission, behavior, and progression among different groups, thereby enhancing the global response to Mpox and similar public health challenges.
Keywords:
Mpox
; cisgender
; transgender women
; and non-binary individuals assigned to female sex at birth
; gender-specific differences
; gender medicine
Introduction
Mpox (formerly known as Monkeypox) is a rare zoonotic disease caused by a double-stranded DNA viral agent from the Orthopoxvirus genus, belonging to the same family of viruses that cause smallpox and smallpox-like infections (Poxviridae) [1]. The disease was first identified in humans in 1970 in the Democratic Republic of the Congo in a region where smallpox had been eliminated in 1968 and had been declared as successfully eradicated in the whole country in 1971, after the completion of a mass vaccination campaign, conducted amidst dramatic challenges, including extreme poverty, a weak, deteriorating health system, and civil strife [2].
Since then, Mpox has been reported in people in several other central and western African countries [3,4]. Characterized by flu-like symptoms, such as fever, fatigue, lymphadenopathy, and rash, it generally spans 2-4 weeks, often resolving itself, though severe cases occur in immunocompromised individuals [5]. A distinctive feature of Mpox is the rash that develops, often beginning on the face and then spreading to other parts of the body, including the palms of the hands and soles of the feet. The rash goes through different stages, including macules, papules, vesicles, pustules, and crusts, before healing [6]. Mpox is primarily transmitted to humans through close contact with infected animals, such as rodents and primates, or their bodily fluids. Human-to-human transmission can occur through close physical contact with infected individuals or their contaminated materials, such as bedding or clothing. Respiratory droplets can also spread the virus, but this requires prolonged face-to-face interaction [7].
In early April-May 2022, Mpox cases were detected and described also in countries without direct or immediate epidemiological links to West or Central Africa. Given the emerging epidemiological and clinical features, on 23 June 2022, the “World Health Organization” (WHO) declared Mpox an evolving threat of moderate public health concern [8], and, then, on 23 July 2022, a “Public Health Emergency of International Concern” (PHEIC) [9,10].
In countries within Africa where Mpox is endemic, the disease is transmitted through two closely related genetic groups: Clade I (previously known as Congo Basin) and Clade IIa (previously known as West Africa). Both types can lead to infections that pose a serious risk to life. However, the molecular signature of the 2022-2023 Mpox multi-country outbreak appears to significantly differ [11,12]. Also, from an epidemiological standpoint, during this outbreak, the majority of cases were observed in cisgender men having sex with men (cMSM), with women being less frequently affected [13,14,15]. According to the available data, 3,141 out of 87,036 confirmed Mpox cases (3.6%) involved women, mostly from the WHO Region of the Americas (2,336 out of 3,141, 74%) and exposed to the virus via sexual encounters (260 out of 507 cases for which the transmission route was documented, 51%) [16]. However, to the best of our knowledge, the sex- and gender-specific characteristics of Mpox infections in terms of differential epidemiological trends, impacts, and clinical features have not been comprehensively appraised, despite the importance and necessity of integrating sex and gender considerations into emerging infectious disease management to mitigate the magnification of existing inequities and violation of principles of fairness and human rights [17].
Therefore, to fill in this gap of knowledge, we have systematically collected all references to scientific articles, cohort studies, and clinical reports concerning Mpox infection, particularly focusing on the female population, encompassing cases from specific populations, like pregnant or breastfeeding women, female sex workers, or female patients with underlying comorbidities, from various geographical locations. The present review covers various aspects such as distinctive clinical characteristics and epidemiological features that warrant enhanced surveillance and tailored management policies. We also discuss the infection's psychological impacts on women, country-specific preparedness strategies, and implications for female sexual, reproductive, and overall health [18,19], as well as the importance of global initiatives addressing Mpox in particular generally overlooked groups, such as pregnant women [20,21,22], and gender-diverse individuals, including transgender women [23].
Material and Methods
Study Protocol and Ethical Considerations
Before commencing the literature search, an a priori study protocol was drafted, consulting an expert librarian, in accordance with the “Preferred reporting items for systematic review and meta-analysis protocols” (PRISMA-P) checklist [24]. A multidisciplinary team was established, consisting of experts in research methodology (N.L.B., L.S.), mathematical modeling of communicable diseases (W.A.W., J.W.), queer/LGBT-medicine (M.C., A.C.), internal medicine and infectious diseases (R.F.), gynecology and obstetrics (M.O., R.K.-F.), and gender-medicine (R.K.-F.). The study was designed to ensure inclusivity and consideration for diversity within gender categories, particularly emphasizing the inclusion of transgender and non-binary individuals.
Study Aims and Objectives
The main objective was to delve into the symptoms and clinical progressions of Mpox in women and compare these findings to those observed in men, paying special attention to any differences in severity, presentation, and potential complications. An in-depth look into the epidemiology of Mpox among women was also undertaken to understand incidence/prevalence rates, identify risk factors, and explore any disparities in access to care or outcomes that may exist. An important aspect of this study involved analyzing the predominant routes of Mpox transmission among women and contrasting these with the trends observed in men, highlighting any gender-specific behaviors or trends that may influence transmission dynamics. Moreover, the study aimed to evaluate the effectiveness and outcomes of Mpox treatments in women compared to men, taking into account aspects such as side effects, recovery durations, and the necessity for gender-specific treatment adaptations.
Search Strategy
To conduct a systematic literature review focusing on the impact of Mpox on women, we employed a comprehensive search strategy using specific keywords to ensure the inclusion of relevant studies. The search was performed across multiple electronic scholarly databases, including MEDLINE via its publicly accessible interface PubMed, Scopus, Web of Science, and EMBASE, to capture a wide range of scientific literature. The keywords used for the search were a combination of terms related to the disease (“monkeypox” OR “Mpox”) and those specifying the population of interest by including them in the title/abstract of the articles (“female”, “females”, “woman”, “women”, “transwoman”, “transwomen”, “male-to-female”, “lactation”, “pregnant”, “pregnancy”, and “breastfeeding”). This approach was designed to specifically target studies that focus on women or females, thus allowing for a focused review of the gender-specific aspects of Mpox infections. We embraced an expanded, inclusive definition of women, incorporating transgender women and non-binary individuals assigned to female sex at birth. The search was supplemented by manual searches of the reference lists of identified articles and of target journals to ensure comprehensive coverage.
Inclusion and Exclusion Criteria
Inclusion/exclusion criteria were devised according to the “Population/patients – Exposure – Comparator/comparison – Outcome(s) – Study design” (PECOS) mnemonic. In studying the impact of Mpox on different genders, the focus was on women affected by the virus, including cisgender and transgender women, as well as non-binary individuals assigned female at birth (P, population/patients). Exposure (E) to the Mpox virus had to be laboratory-confirmed. The examination extends to comparing their experiences with those of men, encompassing cisgender, transgender, and non-binary individuals assigned male at birth (C, comparator/comparison). The key areas of investigation include the clinical manifestations of Mpox, its epidemiological features, the routes through which it is transmitted, and the responses to various treatment options (O, outcomes). In terms of study design (S), eligible studies included peer-reviewed articles, case reports, and observational studies that provided data on clinical characteristics, epidemiological features, and outcomes of Mpox infections in women.
Selection and Identification Process of Eligible Studies
The selection process involved screening titles and abstracts for relevance, followed by a thorough full-text review to confirm eligibility, ensuring a methodical and exhaustive review of the literature on the subject.
Further details are reported in Table 1.
Data Synthesis and Finding Reporting
Data were synthesized and findings were reported in accordance with the “Preferred reporting items for systematic review and meta-analysis” (PRISMA) checklist [25].
Gray Literature
Besides peer-reviewed literature, some major institutional websites of national/international public health authorities and organisms have been searched, including the sites of the WHO, the “Public Health Agency of Canada” (PHAC), the USA “Centers for Disease Control and Prevention” (CDC), the “European Centre for Disease Prevention and Control” (ECDC), and the “UK Health Security Agency” (UKHSA).
Expected Study Outcomes
The expected outcomes include gaining nuanced insights into the gender-specific impacts of Mpox, which can inform the development of tailored public health strategies and clinical guidelines. By enhancing our understanding of Mpox's effects on women, particularly those from marginalized gender identities, this research aims to contribute significantly to the global response to the disease, ensuring that interventions and public health measures are responsive to the specific needs and risks faced by women.
Results
Literature Search
The initial literature search yielded a pool of 4,490 items; 3,533 items were removed, being duplicates. Out of 957 unique items, 928 were discarded, based on title and/or abstract screening. Out of twenty-nine studies screened in full-text, thirteen studies were excluded with reason while the remaining sixteen studies [26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41] from various locations including Buenos Aires, Brazil, Northern California, Colombia, Nigeria, Europe, Vietnam, Spain, Switzerland, and the USA were retained and overviewed. More in detail, six cohort studies [26,27,28,29,30,31] were retrieved and synthesized, along with seven clinical case reports [32,33,34,35,36,37,38], two case series [39,40], and one case series review [41] (Figure 1). The major features of these studies are presented in Table 2.
Cohort Studies
In the USA, Oakley et al. [26] gathered all cases reported between May 11 and November 7, 2022, by the CDC and health departments. A total of 769 Mpox cases affected cisgender women aged 15 and older, making up 2.7% of all cases reported during this period. Based on the data collected, the median age was 32 years (interquartile range: 25–40 years; range: 15–89 years), and a significant portion of these cases involved cisgender women of non-Hispanic Black or African American (44%), non-Hispanic White (25%), and Hispanic or Latino ethnicity (23%). Most of these women (71%) reported sexual activity or close intimate contact as their likely exposure to Mpox. More specifically, the majority had recent sexual contact with cisgender men and a smaller number with cisgender women. From a clinical standpoint, the virus manifested with symptoms including rash, headache, pruritis, malaise, fever, and chills. The rash was mainly located on the legs, arms, genital areas, and trunk. The distribution of rash locations was consistent regardless of whether recent sexual exposure was reported. Among those with available data on immunocompromising conditions, 9% reported having such a condition other than HIV. Among the subset with known HIV status, 8% were HIV-positive, none of whom were pregnant. Of note, there were 23 cases (3%) of Mpox among pregnant (n = 21) or recently pregnant individuals (n = 2, within 3 weeks postpartum), all of whom were identified as cisgender women. Among those with known exposure data, sexual contact was the most reported mode of transmission, followed by household contact. The cases were fairly evenly distributed across all trimesters of pregnancy. Rash was a universal symptom, and genital lesions were reported in some cases. However, there were no reports of genital lesions at the time of delivery. Out of 23 cases, four required hospitalization due to symptoms, but none required intensive care or unplanned delivery, and eleven were treated with tecovirimat without any reported adverse effects. Three main types of outcomes were reported: two full-term deliveries without complications and one spontaneous abortion. Two newborns developed lesions shortly after birth but responded well to treatment with tecovirimat, and one also received intravenous vaccinia immune globulin. There was a case of a breastfeeding individual developing lesions postpartum, with the newborn also showing symptoms later. Two other breastfeeding women diagnosed with Mpox had no transmission through breast milk, confirmed by negative PCR tests for Mpox virus DNA, underscoring the importance of monitoring and managing Mpox cases in pregnant and recently pregnant individuals, considering the potential risks to both the mother and the newborn. The effective response to newborn infections and the absence of adverse events from tecovirimat treatment are particularly noteworthy.
In Argentina, Sánchez Doncell et al. [27] conducted a study specifically focusing on women from June 2022 to February 2023, exploring Mpox's epidemiology, clinical manifestations, and post-infection complications. Utilizing retrospective analysis at a Febrile Emergency Unit, based in Buenos Aires, the authors examined RT-PCR confirmed cases among women, investigating sexual health impacts. Of 214 positive cases from 340 consultations, only 3 were female (two cisgender women and one transgender woman). Details are provided by the authors only for the two cisgender women, who are aged 31 years, one with an obstetric history of pregnancy and childbirth, both apparently healthy, immunocompetent and with a negative serology report for HIV, syphilis, or hepatitis B and C. Concerning contraception, one denies current use, the other reports previous tubal ligation. Both are heterosexual, one with a partner positive for Mpox. One patient reports headache, myalgias, and asthenia, while the other denies headache and muscle aches, describing complaints of weakness, fever, perianal pain, and lymphadenopathy. Lesions are located in the upper and lower limbs, back, and abdomen in the first case, while in the second case, they affect the upper and lower limbs, abdomen, perianal area, and face. Both deny allergies, diseases, and surgeries, reporting sexual relations in the last 21 days. No complications are reported in either case.
In Brazil, Coutinho et al. [28] obtained surveillance data of Mpox cases notified to Rio de Janeiro State Health Department in the period from June 12 to December 15, 2022, and compared women (cisgender or transgender) to men (cisgender or transgender) using chi-squared, Fisher's exact, and Mood's median tests. A total of 1,306 Mpox cases were reported; 1,188 (91.0%) men (99.8% cisgender, 0.2% transgender), 108 (8.3%) women (87.0% cisgender, 13.0% transgender), and 10 (0.8%) non-binary persons. Compared to men, women were more frequently older (concerning the category of 40 years and older: 34.3% versus 25.1%; p < 0.001), reported more frequent non-sexual contact with a potential Mpox case (21.4% versus 9.8%; p = 0.004), fewer sexual partnerships (10.9 vs. 54.8%; p < 0.001), less sexual contact with a potential Mpox case (18.5% versus 43.0%; p < 0.001), fewer genital lesions (31.8% versus 57.9%; p < 0.001), fewer systemic Mpox signs/symptoms (38.0% versus 50.1%; p = 0.015) and had a lower HIV prevalence rate (8.3% versus 46.3%; p < 0.001), with all cases among transgender women. Eight women aged 13-69 years were hospitalized (with a median hospitalization time of five days, interquartile range 3.5–7 days), with the frequency of skin rashes and hospital admissions being similar across genders. However, no deaths occurred among women, with all reported Mpox fatalities (totaling 5) being among men. In terms of epidemiological temporal trends, the highest number of cases among women was notified in epidemiological week 34, when the number of cases among men started to decrease. Specifically concerning transgender women and non-binary individuals assigned to female sex at birth, the majority of Mpox cases among transgender women (14 cases) and non-binary individuals (10 cases) were observed in those aged 25–29 years or older, with 12 out of 14 and 9 out of 10 cases respectively falling into this age group. The predominant racial self-identification was Pardo for transgender women (10 out of 14) and non-binary individuals (3 out of 10), with Black being the next most common (2 out of 14 for transgender women and 3 out of 10 for non-binary individuals). Half of the individuals in each group had completed secondary education (9 out of 13 transgender women and 5 out of 10 non-binary individuals). Approximately half of both groups reported having sexual relationships exclusively with men (7 out of 8 transgender women and 4 out of 7 non-binary individuals). The majority had engaged in sexual activities with someone who could potentially have Mpox (10 out of 14 transgender women and 5 out of 6 non-binary individuals). All HIV cases among the women in the study were found in transgender women (8 out of 14), while non-binary individuals accounted for three HIV cases. There were no hospitalizations recorded for either transgender women or non-binary individuals.
In Europe, an online survey was conducted under the VACCELERATE Consortium [29], focusing on the evaluation and confirmation of Mpox cases among women across countries. The survey revealed that Spain and Belgium had the highest numbers evaluated, with Spain reporting 226 cases and Belgium 60 cases. Among those evaluated, women residing in Spain and Portugal showed the highest likelihood of infection, with ratios of 0.08 and 0.06, respectively.
Specifically concerning Spain, analyzing surveillance data, Vallejo-Plaza et al. [30] found similar temporal trends but noted disparities in diagnosis delays, sexual transmission, and clinical manifestations between genders. In terms of prevalence and age distribution, women constituted a small fraction (2.1%) of the total Mpox cases reported in Spain during the study period, with a younger median age compared to men. Concerning the transmission mechanisms, the primary mode of transmission was close contact during sexual relations for both men and women, though a significant proportion of women had different transmission routes compared to men. Regarding the HIV infection rates, a notable disparity was observed in HIV infection rates between men and women with Mpox, suggesting differing risk profiles. In terms of symptomatology, women exhibited certain signs and symptoms at different rates than men, such as less frequent anogenital rash but more frequent rashes in other locations. As far as diagnosis and complications were concerned, women experienced a longer delay from symptom onset to diagnosis and had higher complication rates compared to men, although no deaths were reported among women.
Globally, Thornhill et al. [31] collected data on 136 cisgender and transgender women and non-binary individuals assigned to female sex at birth and diagnosed with Mpox virus from May 11 to October 4, 2022, across 15 countries. The median age was 34 years, with a range from 19 to 84 years. The group included 62 transwomen, 69 cis-women, and five non-binary individuals, with the latter two categories combined for analysis. In terms of sexual orientation, 108/136 (79%) were heterosexual, while 10/136 (7%), 2/136 (1%), and 16/136 (12%) were bisexual, lesbian, and unknown, respectively. A significant majority, consisting of 121 participants, had sexual contact with men. HIV prevalence was notable, especially among transwomen (50% of transwomen compared to 8% of cis-women and non-binary individuals). The majority of transwomen (89%) and a lesser proportion of cisgender women and non-binary individuals assigned female at birth (61%) were suspected of contracting the virus through sexual contact, while cisgender women and non-binary individuals assigned female at birth also reported non-sexual transmission routes. Misdiagnosis occurred in 34% of cisgender women and non-binary individuals assigned female at birth. The data showed that 93% had a rash, predominantly anogenital (74%) and vesiculopustular (87%). Lesions were common, with a median count of ten. Over half of the participants had mucosal lesions, which were correlated with vaginal and anal sexual activities. PCR tests confirmed monkeypox virus DNA in all vaginal swabs taken. Hospitalization was necessary for 13% of cases, mainly for bacterial superinfection treatment and pain management. Tecovirimat was administered to 24% of the individuals, and 4% received post-exposure vaccinations. Finally, there were no fatalities reported.
Pooling all data together, analyzing them, and sourcing from the WHO [16], some interesting sex- and gender-specific differences in Mpox symptom prevalence can be found (Figure 2). There are noticeable differences between genders in the rate of certain symptoms like “genital rash” and “any lymphadenopathy”, which show a higher prevalence in males compared to females, indicating possible variations in disease manifestation or reporting between genders. Some symptoms are, instead, common across genders, such as “any rash” and “fever”, even if slightly higher in males, suggesting that, while certain symptoms are universally common among Mpox patients, the extent to which they are experienced can still vary by gender. Some symptoms appear to be sex-/gender-specific with significant disparities, like “genital rash”, which is much more prevalent in males than in females, or “headache” and “muscle ache”, which, on the contrary, show a relatively higher prevalence in females. This could reflect differences in biological response, exposure, or even healthcare-seeking behaviors between males and females. Finally, symptoms, such as “conjunctivitis”, “diarrhea”, and “genital oedema”, are relatively rare in both genders, even though a few of them still present notable differences in prevalence between males and females.
Case Reports and Case Series
Nine studies [32,33,34,35,36,37,38,39,40] reporting eleven cases were found and synthesized. The average age of patients was 32 years, ranging from 20 to 57 years. Transmission route was sexual contact in five cases, with close contact being reported in two cases and non-sexual routes being reported in the remaining cases. Antivirals (including treatments like tecovirimat and cidofovir) were employed in one case, while symptomatic care was administered in four cases (including symptomatic relief measures and topical treatments). In the remaining four cases, no detailed treatment information was provided. Overall, these clinical case reports and case series highlight the variability in transmission routes and treatment approaches for Mpox, as well as the broad age range of affected individuals (Table 3).
Mancha et al. [32] reported the unusual case of a 30-year-old female (Fitzpatrick phototype III), highlighting not only the disease's potential to affect a broader population but also, and especially, a rather rare, previously undocumented transmission route, namely oro-mammary sex with a partner who had symptoms suggestive of tonsillitis (which was later confirmed to be Mpox). This emphasizes the viability of the virus in saliva and the potential for transmission through intimate, non-genital contact. From a clinical standpoint, the case started as an erythematous papule on the left nipple and evolved into a flat ulceration with a hemorrhagic crust surrounded by umbilicated pustules, along with systemic symptoms like fever and lymphadenopathy, underscoring the diverse manifestations and transmission routes of Mpox in female individuals. The patient was treated with symptomatic care and topical fusidic acid, and finally recovered from the infection.
Cole et al. [33] highlighted a complex, multi-faceted case involving a 35-year-old White, apparently healthy woman from the UK, who developed encephalitis and longitudinally extensive transverse myelitis due to Mpox but showed remarkable neurological recovery following treatment with antivirals (tecovirimat and cidofovir), analgesia, antibiotics for secondary infections, and ultimately, immunosuppressive therapy with steroids (methylprednisolone), and plasma exchange to manage the post-infectious autoimmune complications. Initially presenting with symptoms typical of a sexually transmitted infection after unprotected sex, the patient's condition escalated to include severe genital lesions, systemic symptoms, and eventually significant neurological complications. The initial differential diagnosis included common causes of genital lesions like herpes simplex virus and varicella-zoster virus, but tests for these were negative. The diagnosis of Mpox was confirmed through PCR testing of the genital lesions, and the patient's condition was complicated by severe pain, difficulty in urination, systemic spread of the lesions, and lymphadenopathy. The situation became more critical with the development of neurological symptoms, leading to the suspicion and subsequent confirmation of Mpox encephalitis and later, longitudinally extensive transverse myelitis. With the treatment, the patient's condition, including the neurological deficits, showed improvement, highlighting the importance of multidisciplinary care in managing complex infectious disease presentations.
Ezzat et al. [34] described a 31-year-old female patient residing in Switzerland who presented to the gynecologic emergency department for painful vulvar lesions after an episode of upper respiratory tract infection. Shortly after, the patient developed generalized and typical Mpox lesions on her whole body. She was initially misdiagnosed with a mycotic infection and later with genital herpes, before being correctly diagnosed with Mpox following the worsening of her symptoms and the appearance of additional lesions. The patient's symptoms did not respond to antiviral or antifungal treatments, leading to further investigation and the eventual diagnosis of Mpox through PCR testing.
van Hennik and Petrignani [35] reported the case of a 57-year-old female, the partner of a bisexual man tested positive for Mpox, presented at the Centre of Sexual Health at Den Haag, The Netherlands. During the physical examination, lesions characteristic of Mpox were observed at the vaginal opening. The patient reported experiencing symptoms for a period of eight days, beginning with itchiness and progressing to pain, which decreased after three days.
Napoli et al. [36] described a 28-year-old woman suffering from gastroesophageal reflux disease and untreated atopic dermatitis, who had just gotten a tattoo, who presented with intense pain in her right ear and multiple vesiculopustular lesions. Within a week, she had developed around 80 lesions spread across her body. Lab tests confirmed an infection with the Mpox virus, and after starting treatment with oral tecovirimat, no new lesions appeared. Complications and Management: The patient experienced severe pain, gastrointestinal distress, bacterial superinfection, acute kidney injury (AKI), and anemia as complications of Mpox. The use of tecovirimat, an antiviral approved for the treatment of orthopoxvirus infections, was considered but posed challenges due to the patient's AKI. This highlights the need for careful consideration of treatment options in Mpox patients, especially those with comorbidities that may limit the use of certain medications. Public Health Implications: The case emphasizes the importance of considering Mpox in differential diagnoses, even in the absence of known exposure or classic risk factors. It also highlights the need for heightened surveillance and preventive measures in settings where the virus may be present in the environment, such as tattoo and piercing establishments. Research and Knowledge Gaps: The case illustrates the ongoing need for research into Mpox, particularly regarding its transmission dynamics, clinical manifestations in diverse patient populations, and effective treatment options. The limited efficacy data for Mpox treatments and the challenges posed by comorbid conditions in affected individuals underline the importance of continued investigation and data collection.
Ogoina and James [37] presented a case involving a 24-year-old Nigerian female sex worker who tested positive for Mpox, underscores the significance for public health in understanding the spread and management of Mpox within Africa and worldwide, especially in a socially vulnerable, highly stigmatized population, namely the community of sex workers. The patient began experiencing fever and, four days after her last sexual encounter with a client in a brothel, developed vesiculopustular lesions on her groin and genital area.
Sampson et al. [38] presented a case of a 20-year-old pregnant woman at 31 weeks of gestation, with a history of sexually transmitted infections but no chronic conditions. She sought medical attention due to vaginal discharge, bleeding, painful urination, and decreased fetal movements for two weeks. At the genital exam, she presented with a new painful vaginal lesion (a 1-cm labial ulcer, affecting her left labia majora) and subsequent herpes-like papular rash on her abdomen and leg at 31 weeks of gestation, along with tender lymph nodes in her left groin. She was admitted for a suspected urinary tract infection and fetal observation. Previously, she had been treated for gonorrhea, chlamydia, and pyelonephritis during her pregnancy. Initial screenings for HIV and syphilis were negative. Upon admission, she showed signs of tachycardia but no fever or high blood pressure, and fetal monitoring was normal. During the hospital stay, the vaginal lesion grew, accompanied by new, itchy, red lesions on her body. Six days after, she mentioned her partner had recently tested positive for Mpox and, on the seventh day, PCR tests confirmed her vaginal lesion was positive for orthopoxvirus, while also indicating herpes simplex virus-1, suggesting viral shedding rather than the cause of the ulcer. After being diagnosed with Mpox infection and herpes co-infection, she was treated with tecovirimat and acyclovir. Her condition stabilized, with no new lesions, allowing her discharge to complete tecovirimat treatment at home. Her lesions resolved 10 days after starting treatment. She had an uncomplicated induction of labor at 39 and 2/7 weeks of gestation and delivered a healthy neonate, who, despite reporting a temporary lesion on the scalp and having a positive immunoglobulin G test result for orthopoxvirus, did not have skin lesions or positive molecular test results on cord blood, fetal serum, maternal vaginal fluid, and the placenta's surface suggestive of infection. The baby remained healthy and developed normally at the three-month follow-up.
Renfro et al. [39] reported two cases of Mpox infection in pregnant, heterosexual cisgender women, focusing on their pregnancy and childbirth outcomes. Both women underwent labor induction and encountered complications from chorioamnionitis during childbirth. The first case is a 19-year-old female, in her first pregnancy, who experienced vaginal itching at 24 weeks of gestation. She tested negative for Chlamydia trachomatis and Neisseria gonorrhoeae, but positive for Mpox from a vaginal swab. At 36 weeks, labor was induced due to intrahepatic cholestasis: during labor, she developed chorioamnionitis. Initial treatment for the presumed vaginitis included topical metronidazole, and labor was induced using a Cook balloon and an oxytocin infusion. Chorioamnionitis was treated aggressively with intravenous ampicillin and gentamicin. The second case is a 22-year-old female, also in her first pregnancy, who underwent routine sexually transmitted infections screening at 36 weeks, testing negative for C. trachomatis and N. gonorrhoeae, but positive for Mpox from a vaginal swab. At 38 weeks and 4 days, labor was induced due to oligohydramnios, which followed 48 hours of fluid leakage. Similar to the first case, she developed chorioamnionitis during labor, which was induced with an oxytocin infusion. The treatment for chorioamnionitis mirrored that of the first case, with a regimen of intravenous ampicillin and gentamicin. Both cases illustrate the complexities of managing pregnant individuals with Mpox, especially when coupled with obstetric complications like intrahepatic cholestasis, oligohydramnios, and chorioamnionitis. The management strategies involved not only addressing the Mpox infection but also carefully navigating pregnancy complications to ensure the health and safety of both the mother and the fetus. Indeed, the use of antivirals like tecovirimat and vaccinia immune globulin in pregnant women may give rise to obstetric issues, such as the potential for prolonged QT-interval when corrected for heart rate, errors in measuring blood glucose levels, and an increased risk of venous thromboembolism caused by medical interventions.
Finally, Dung et al. [40] reported two women who traveled from the United Arab Emirates to Vietnam diagnosed with Mpox, hospitalized, and linked to a newer, emerging sublineage, A.2.1 (clade IIb), differing from the B.1 lineage associated with the widespread outbreak. Patient 1, a 35-year-old woman, exhibited symptoms after sexual contact in Dubai, including fever and a maculopapular rash. She tested positive for Mpox and varicella-zoster virus. Patient 2, a 38-year-old woman and friend of patient 1, also showed symptoms following a sexual encounter in Dubai and tested positive for Mpox upon her return to Vietnam. Both patients were afebrile upon admission and had stable conditions throughout their hospitalization. They were isolated according to local health regulations. Patient 1 was treated with oral acyclovir due to varicella-zoster virus co-infection. No specific treatments were mentioned for patient 2. This interesting case series suggests women may also play a role in transmitting Mpox, underscoring the importance of advanced genomic monitoring to understand the virus's evolution. More in detail, the phylogenetic analysis of the Mpox viral strains from the patients detected a novel nonsynonymous substitution from threonine to isoleucine in amino 717 (T717I mutation) in the polymerase protein, which was identified in patient 1's virus sequence, indicating potential genetic diversity within the strains. This case series has major epidemiological and public health implications, highlighting the role of women in Mpox transmission networks and the need for enhanced genomic surveillance to understand and monitor the epidemiology and evolution of the Mpox virus.
Case Series Review
Finally, Schwartz and Pittman [41] have reviewed 58 cases of pregnant women positive to Mpox infection that have been reported during the 2022–2023 outbreak. These cases include the 23 cases reported by Oakley et al. [26]. There have been no documented cases of negative outcomes related to pregnancy or childbirth, such as stillbirths. The lack of complications during pregnancy or at birth linked to Clade IIb is consistent with the overall mortality rate of less than 0.1% among non-pregnant women, as infections from this clade tend to be milder compared to those caused by Clade I or IIa variants of Mpox. Therefore, the two researchers have formulated the hypothesis according to which Mpox viral clade differences may be associated with varying obstetrical and fetal outcomes.
Discussion
During the 2022 outbreak, Mpox has primarily affected cisgender men, especially those having sex with men, with fewer cases in women [42]. This review aimed to address the knowledge gap regarding gender-specific characteristics of Mpox by reviewing scientific literature on infections in women, including diverse cases and geographical locations. Despite lesser involvement of women, we could note specific trends and outcomes in the female cases studied. Women diagnosed with Mpox presented differences in epidemiological, behavioral, and clinical characteristics compared to men.
For instance, the patient described by Napoli et al. [36] exhibited rather unusual clinical features, including erythema multiforme and lesions within a tattoo, which are not commonly associated with Mpox, underscoring the variability in Mpox presentations, especially in individuals with underlying skin conditions like atopic dermatitis, which may alter the typical progression and appearance of the disease. Also, the case raises questions about the transmission dynamics of Mpox, as the patient had no known direct contact with Mpox cases, suggesting the possibility of indirect transmission or acquisition from environmental sources. This appears to be supported by a few reports [43,44,45,46,47], which found Mpox transmission in tattooes and piercing establishments/parlors, indicating that the virus can persist in the environment and infect individuals through less direct routes.
Health services should provide a comprehensive assessment that accounts for gender diversity and should promote international collaborations in monitoring and managing infectious diseases. Our findings underscore, indeed, the necessity of inclusive, tailored surveillance and research to understand the dynamics of Mpox across different population groups, including women and those who are pregnant.
Specifically concerning pregnancy, this topic has been particularly underexplored in the currently available body of scholarly literature. Only a few cases have been reported, including those from previous outbreaks. For instance, Mbala et al. [48] documented the pregnancy outcomes of four expectant mothers included in a study conducted at the General Hospital of Kole (Sankuru Province), Democratic Republic of Congo. This study observed 222 individuals presenting symptoms between 2007 and 2011. Among these four pregnant participants, one delivered a healthy baby, two experienced first-trimester miscarriages, and one reported a fetal demise. The deceased fetus, which was macerated, exhibited widespread maculopapular skin lesions covering the head, body, and limbs, extending to the palms and soles. Schwartz et al. [49] described the autopsy findings of a stillborn fetus at 21 weeks, diagnosed with congenital Mpox syndrome in the Democratic Republic of the Congo in 2008. The infection was transmitted from the mother to the fetus via the placenta and Mpox virus presence in the mother, fetus, and placenta was confirmed through Mpox virus-specific quantitative PCR, even if the virus subtype could not be identified.
Given the paucity of information, experts [50,51,52,53,54] recommend that pregnant, postpartum, and lactating women should wear masks, particularly when in the vicinity of potentially infected individuals, and should avoid contact with anyone displaying symptoms like fever or skin lesions on mucous membranes. Moreover, they should practice safe sex using condoms during oral, vaginal, and anal intercourse due to the high risk of transmission through intimate contact. They should be vigilant for any genital lesions in their sexual partner, and seek medical consultation immediately upon noticing any concerning symptoms to facilitate timely clinical and laboratory diagnosis. Healthcare professionals should advise pregnant women with mild illness to isolate at home with regular monitoring by their healthcare team, and ensure that cases with severe symptoms receive in-hospital care. The absence of a specific antiviral treatment protocol for the pregnancy-puerperal cycle should be noted. Close attention should be paid to monitoring fetal well-being in patients with moderate to severe illness due to increased risks of fetal complications. Healthcare professionals should make obstetric decisions regarding delivery on a case-by-case basis, with cesarean sections not routinely recommended, and should advise delaying breastfeeding during isolation, providing support for relactation afterwards.
Even less data are available on Mpox among transgender women and non-binary individuals assigned to female sex at birth. This lack of data presents challenges in understanding the full scope and impact of the disease within these groups, who may have unique health needs and risk factors compared to the broader population. Transgender women and non-binary individuals often face barriers in accessing healthcare, including discrimination, lack of provider knowledge on gender-diverse health needs, and economic constraints. These challenges can lead to underreporting of health issues and decreased participation in health studies, further contributing to the scarcity of data. Additionally, the social and behavioral factors that affect the risk of Mpox transmission in these communities might differ from those in the general population. For instance, the networks and dynamics of sexual partnerships, the prevalence of other sexually transmitted infections which may facilitate Mpox transmission, and the use of gender-affirming medical interventions that might impact immune function, are all areas that require targeted research. Given these complexities, there is a critical need for more inclusive and comprehensive research efforts. Studies should be designed to explicitly include and address the health concerns of transgender women and non-binary individuals, taking into account the diverse experiences and challenges they face. Improving data collection and research methodologies to be more inclusive of gender diversity will not only help in understanding the epidemiology of Mpox in these groups but also inform more effective public health strategies and interventions tailored to their needs.
The present review emphasizes the importance of considering gender and sexual orientation in public health responses to effectively address the spread and impact of the disease. For this purpose, inclusively collecting data on sex, gender identity and expression, and sexual orientation on a routine basis would be essential. Further research is encouraged to explore the nuances of transmission, behavior, and disease progression among diverse groups, enhancing the overall response to Mpox and similar public health challenges (Table 4).
Future Directions
In-depth studies on Mpox transmission dynamics in women, particularly focusing on non-sexual routes and environmental factors, are warranted to better understand the full spectrum of transmission risks. Exploration of the unique clinical manifestations of Mpox in women, especially in those with underlying health conditions is necessary, to tailor clinical management and public health interventions. Enhanced surveillance and research on Mpox in pregnant women is highly needed, in order to systematically document outcomes and provide evidence-based guidelines for management during pregnancy. Investigation into Mpox's impact on transgender women and non-binary individuals assigned female at birth should address the lack of data and the specific health needs and risk factors of these populations. Finally, genomic monitoring and analysis should be implemented to track the evolution of the Mpox virus, particularly in light of cases linked to new sublineages, which could have implications for vaccine and treatment efficacy, especially among cisgender and transgender women and non-binary individuals assigned to female sex at birth.
Conclusions
The comprehensive review of Mpox's impact on women, across various global contexts, underlines the disease's distinct epidemiological and clinical manifestations in female populations, including pregnant women. Despite the predominance of cases among cisgender men, particularly those having sex with men, the findings from cohort studies, case reports, and systematic literature review highlight the necessity for gender-inclusive surveillance and research. This approach is crucial to understand and address the unique risks and outcomes associated with Mpox in women, advocating for tailored public health strategies and interventions that consider gender diversity and the specific needs of women and pregnant individuals in managing infectious diseases.
Acknowledgements
W.A.W., J.W., and N.L.B. acknowledge financial support from the CIHR under the Mpox and other zoonotic threats Team Grant (FRN. 187246).
References
- Bunge EM, Hoet B, Chen L, Lienert F, Weidenthaler H, Baer LR, Steffen R. The changing epidemiology of human monkeypox-A potential threat? A systematic review. PLoS Negl Trop Dis. 2022 Feb 11;16(2):e0010141. [CrossRef]
- Muyembe-Tamfum JJ, Mulembakani P, Lekie RB, Szczeniowski M, Ježek Z, Doshi R, Hoff N, Rimoin AW. Smallpox and its eradication in the Democratic Republic of Congo: lessons learned. Vaccine. 2011 Dec 30;29 Suppl 4:D13-8. [CrossRef]
- Rimoin AW, Mulembakani PM, Johnston SC, Lloyd Smith JO, Kisalu NK, Kinkela TL, Blumberg S, Thomassen HA, Pike BL, Fair JN, Wolfe ND, Shongo RL, Graham BS, Formenty P, Okitolonda E, Hensley LE, Meyer H, Wright LL, Muyembe JJ. Major increase in human monkeypox incidence 30 years after smallpox vaccination campaigns cease in the Democratic Republic of Congo. Proc Natl Acad Sci U S A. 2010 Sep 14;107(37):16262-7. [CrossRef]
- Thornhill JP, Gandhi M, Orkin C. Mpox: The Reemergence of an Old Disease and Inequities. Annu Rev Med. 2023 Oct 3. [CrossRef] [PubMed]
- Ahmed SK, Mohamed MG, Dabou EA, Abuijlan I, Chandran D, El-Shall NA, Chopra H, Dhama K. Monkeypox (Mpox) in immunosuppressed patients. F1000Res. 2023 Feb 2;12:127. [CrossRef]
- Ogoina D, Damon I, Nakoune E. Clinical review of human Mpox. Clin Microbiol Infect. 2023 Dec;29(12):1493-1501. [CrossRef] [PubMed]
- Islam MM, Dutta P, Rashid R, Jaffery SS, Islam A, Farag E, Zughaier SM, Bansal D, Hassan MM. Pathogenicity and virulence of monkeypox at the human-animal-ecology interface. Virulence. 2023 Dec;14(1):2186357. [CrossRef]
- Zebardast A, Latifi T, Shafiei-Jandaghi NZ, Gholami Barzoki M, Shatizadeh Malekshahi S. Plausible reasons for the resurgence of Mpox (formerly Monkeypox): an overview. Trop Dis Travel Med Vaccines. 2023 Dec 25;9(1):23. [CrossRef]
- World Health Organization (WHO). WHO Director-General declares the ongoing monkeypox outbreak a Public Health Emergency of International Concern. 23 July 2022. Accessible at: https://www.who.int/europe/news/item/23-07-2022-who-director-general-declares-the-ongoing-monkeypox-outbreak-a-public-health-event-of-international-concern.
- Karagoz A, Tombuloglu H, Alsaeed M, Tombuloglu G, AlRubaish AA, Mahmoud A, Smajlović S, Ćordić S, Rabaan AA, Alsuhaimi E. Monkeypox (Mpox) virus: Classification, origin, transmission, genome organization, antiviral drugs, and molecular diagnosis. J Infect Public Health. 2023 Apr;16(4):531-541. [CrossRef]
- Borges V, Duque MP, Martins JV, Vasconcelos P, Ferreira R, Sobral D, Pelerito A, de Carvalho IL, Núncio MS, Borrego MJ, Roemer C, Neher RA, O'Driscoll M, Rocha R, Lopo S, Neves R, Palminha P, Coelho L, Nunes A, Isidro J, Pinto M, Santos JD, Mixão V, Santos D, Duarte S, Vieira L, Martins F, Machado J, Veríssimo VC, Grau B, Peralta-Santos A, Neves J, Caldeira M, Pestana M, Fernandes C, Caria J, Pinto R, Póvoas D, Maltez F, Sá AI, Salvador MB, Teófilo E, Rocha M, Moneti V, Duque LM, E Silva FF, Baptista T, Vasconcelos J, Casanova S, Mansinho K, Alves JV, Alves J, Silva A, Alpalhão M, Brazão C, Sousa D, Filipe P, Pacheco P, Peruzzu F, de Jesus RP, Ferreira L, Mendez J, Jordão S, Duarte F, Gonçalves MJ, Pena E, Silva CN, Guimarães AR, Tavares M, Freitas G, Cordeiro R, Gomes JP. Viral genetic clustering and transmission dynamics of the 2022 Mpox outbreak in Portugal. Nat Med. 2023 Oct;29(10):2509-2517. [CrossRef]
- Bragazzi NL, Kong JD, Wu J. Integrated epidemiological, clinical, and molecular evidence points to an earlier origin of the current monkeypox outbreak and a complex route of exposure. J Med Virol. 2023 Jan;95(1):e28244. [CrossRef] [PubMed]
- Limonta S, Lapadula G, Mezzadri L, Corsico L, Rovida F, Ranzani A, Baldanti F, Bonfanti P. Mpox Virus in the Pharynx of Men Having Sex with Men: A Case Series. Pathogens. 2024 Jan 20;13(1):92. [CrossRef] [PubMed]
- Thornhill JP, Barkati S, Walmsley S, Rockstroh J, Antinori A, Harrison LB, Palich R, Nori A, Reeves I, Habibi MS, Apea V, Boesecke C, Vandekerckhove L, Yakubovsky M, Sendagorta E, Blanco JL, Florence E, Moschese D, Maltez FM, Goorhuis A, Pourcher V, Migaud P, Noe S, Pintado C, Maggi F, Hansen AE, Hoffmann C, Lezama JI, Mussini C, Cattelan A, Makofane K, Tan D, Nozza S, Nemeth J, Klein MB, Orkin CM; SHARE-net Clinical Group. Monkeypox Virus Infection in Humans across 16 Countries - April-June 2022. N Engl J Med. 2022 Aug 25;387(8):679-691. 20 June. [CrossRef] [PubMed]
- Bragazzi NL, Kong JD, Mahroum N, Tsigalou C, Khamisy-Farah R, Converti M, Wu J. Epidemiological trends and clinical features of the ongoing monkeypox epidemic: A preliminary pooled data analysis and literature review. J Med Virol. 2023 Jan;95(1):e27931. [CrossRef] [PubMed]
- World Health Organization (WHO). 2022 Mpox (Monkeypox) outbreak: global trends. December 2023. Accessible at: https://worldhealthorg.shinyapps.io/mpx_global. Accessed on 28 January 2024.
- Lawry LL, Lugo-Robles R, McIver V. Overlooked sex and gender aspects of emerging infectious disease outbreaks: Lessons learned from COVID-19 to move towards health equity in pandemic response. Front Glob Womens Health. 2023 Feb 20;4:1141064. [CrossRef]
- Alvarez-Gómez AM, Vélez-Cuervo SM, Cardona-Maya WD. Monkey pox: importance in female sexual health. Rev Colomb Obstet Ginecol. 2023 Mar 30;74(1):87-89. English, Spanish. [CrossRef]
- Ghebreyesus TA, Allotey P, Narasimhan M. Advancing the "sexual" in sexual and reproductive health and rights: a global health, gender equality and human rights imperative. Bull World Health Organ. 2024 Jan 1;102(1):77-78. [CrossRef]
- Hoenig, LJ. Hoenig LJ. The Monkeypox Outbreak 2022: Women and Children Patients. Skinmed. 2022 Oct 31;20(5):334-335. [PubMed]
- Khalil A, Samara A, Ladhani S, O'Brien P. Monkeypox and pregnancy: time for global surveillance and prevention strategies. Lancet. 2022 Oct 8;400(10359):1193. [CrossRef]
- Pomar L, Favre G, Baud D. Monkeypox infection during pregnancy: European registry to quantify maternal and fetal risks. Ultrasound Obstet Gynecol. 2022 Sep;60(3):431. [CrossRef] [PubMed]
- Rodriguez-Morales AJ, Amer FA. Monkeypox virus infection in women and non-binary people: uncommon or neglected? Lancet. 2022 Dec 3;400(10367):1903-1905. [CrossRef]
- Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, Shekelle P, Stewart LA; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015 Jan 1;4(1):1. [CrossRef]
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hróbjartsson A, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S, McGuinness LA, Stewart LA, Thomas J, Tricco AC, Welch VA, Whiting P, Moher D. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021 Mar 29;372:n71. [CrossRef]
- Oakley LP, Hufstetler K, O'Shea J, Sharpe JD, McArdle C, Neelam V, Roth NM, Olsen EO, Wolf M, Pao LZ, Gold JAW, Davis KM, Perella D, Epstein S, Lash MK, Samson O, Pavlick J, Feldpausch A, Wallace J, Nambiar A, Ngo V, Halai UA, Richardson CW, Fowler T, Taylor BP, Chou J, Brandon L, Devasia R, Ricketts EK, Stockdale C, Roskosky M, Ostadkar R, Vang Y, Galang RR, Perkins K, Taylor M, Choi MJ, Weidle PJ, Dawson P, Ellington S; CDC Mpox Analytics Team. Mpox Cases Among Cisgender Women and Pregnant Persons - United States, May 11-November 7, 2022. MMWR Morb Mortal Wkly Rep. 2023 Jan 6;72(1):9-14. [CrossRef]
- Sánchez Doncell J, Lemos M, Francos J JL, González Montaner P. Viruela símica: características en población femenina, Buenos Aires, Argentina [Monkeypox: characteristics in female population, Buenos Aires, Argentina]. Medicina (B Aires). 2024;84(1):143-147. Spanish. [PubMed]
- Coutinho C, Secco Torres Silva M, Torres TS, Peixoto E, Avelar Magalhães M, Wagner Cardoso S, Nazário G, Mendonça M, Menezes M, Almeida PM, Dias de Brito de Carvalho PR, Bia Bedin S, Almeida AM, Carvalho S, Gonçalves Veloso V, Grinsztejn B, Velasque L; INI-Fiocruz Mpox Study Group. Characteristics of women diagnosed with Mpox infection compared to men: A case series from Brazil. Travel Med Infect Dis. 2023 Nov-Dec;56:102663. [CrossRef] [PubMed]
- Grothe JH, Cornely OA, Salmanton-García J; VACCELERATE consortium. Monkeypox in children and adult women in Europe: Results from a flash VACCELERATE pilot survey. Enferm Infecc Microbiol Clin (Engl Ed). 2023 May;41(5):309-311. [CrossRef]
- Vallejo-Plaza A, Rodríguez-Cabrera F, Hernando Sebastián V, Guzmán Herrador BR, Santágueda Balader P, García San Miguel Rodríguez-Alarcón L, Díaz Franco A, Garzón Sánchez A, Sierra Moros MJ; Spanish Monkeypox Response Network; Simón Soria F, Suárez Rodríguez B. Mpox (formerly monkeypox) in women: epidemiological features and clinical characteristics of Mpox cases in Spain, April to November 2022. Euro Surveill. 2022 Dec;27(48):2200867. [CrossRef]
- Thornhill JP, Palich R, Ghosn J, Walmsley S, Moschese D, Cortes CP, Galliez RM, Garlin AB, Nozza S, Mitja O, Radix AE, Blanco JL, Crabtree-Ramirez B, Thompson M, Wiese L, Schulbin H, Levcovich A, Falcone M, Lucchini A, Sendagorta E, Treutiger CJ, Byrne R, Coyne K, Meyerowitz EA, Grahn AM, Hansen AE, Pourcher V, DellaPiazza M, Lee R, Stoeckle M, Hazra A, Apea V, Rubenstein E, Jones J, Wilkin A, Ganesan A, Henao-Martínez AF, Chow EJ, Titanji BK, Zucker JE, Ogoina D, Orkin CM; Share-Net writing group. Human monkeypox virus infection in women and non-binary individuals during the 2022 outbreaks: a global case series. Lancet. 2022 Dec 3;400(10367):1953-1965. [CrossRef]
- Mancha D, Brazão C, Filipe P. Oro-mammary inoculation pathway of monkeypox in a female patient. J Eur Acad Dermatol Venereol. 2023 May;37(5):e636-e637. [CrossRef] [PubMed]
- Cole J, Choudry S, Kular S, Payne T, Akili S, Callaby H, Gordon NC, Ankcorn M, Martin A, Hobson E, Tunbridge AJ. Monkeypox encephalitis with transverse myelitis in a female patient. Lancet Infect Dis. 2023 Mar;23(3):e115-e120. [CrossRef]
- Ezzat D, Barcellini B, Meier J, Duc-Ha E, Mathis J. Ulcerating vulvar lesions revealing a rare female case of monkeypox in Switzerland. AJOG Glob Rep. 2023 Feb;3(1):100155. [CrossRef]
- van Hennik MM, Petrignani MWF. Klinische presentatie van monkeypox bij de vrouw [Clinical presentation of monkeypox in women]. Ned Tijdschr Geneeskd. 2022 Nov 15;166:D7082. Dutch. [PubMed]
- Napoli E, Frizzell M, Gravell C, Vallejo S, Theodore S, Chen K, Siddiqui H, Dunn J, Marrufo D, Cadena J, Danaher PJ. Eczema Monkeypoxicum in a Female Patient With Atopic Dermatitis. Open Forum Infect Dis. 2023 Feb 10;10(3):ofad072. [CrossRef]
- Ogoina D, James IH. Mpox in a female sex worker in Nigeria: A case report. IJID Reg. 2022 Dec 14;7:143-145. [CrossRef]
- Sampson MM, Magee G, Schrader EA, Dantuluri KL, Bukhari A, Passaretti C, Temming L, Leonard M, Philips JB, Weinrib D. Mpox (Monkeypox) Infection During Pregnancy. Obstet Gynecol. 2023 May 1;141(5):1007-1010. [CrossRef] [PubMed]
- Renfro ZT, Contag CA, Lu J, Solis D, Huang C, Sahoo MK, Yamamoto F, Mah J, Jones MS, Lin J, Levy V, Pinsky BA. Two cases of MPXV infection during pregnancy in heterosexual cisgender women without classic cutaneous lesions, Northern California, 2022. IDCases. 2023 Aug 21;33:e01881. [CrossRef]
- Dung NT, Hung LM, Hoa HTT, Nga LH, Hong NTT, Thuong TC, Ngoc NM, Ny NTH, Quy VT, Thoa VTK, Thanh NT, Tho PV, Toan LM, Quang VM, Man DNH, Phat NT, Phuong TTL, Tam TTT, Thoa PTN, Tam NH, Lan TTT, Thanh TT, Maurer-Stroh S, Khanh LTT, Yen LM, Hung NH, Thwaites G, Tung NLN, Thwaites L, Chau NVV, Anh NT, Van Tan L. Monkeypox Virus Infection in 2 Female Travelers Returning to Vietnam from Dubai, United Arab Emirates, 2022. Emerg Infect Dis. 2023 Apr;29(4):778-781. [CrossRef]
- Schwartz DA, Pittman PR. Mpox (Monkeypox) in Pregnancy: Viral Clade Differences and Their Associations with Varying Obstetrical and Fetal Outcomes. Viruses. 2023 Jul 28;15(8):1649. [CrossRef]
- Bragazzi NL, Khamisy-Farah R, Tsigalou C, Mahroum N, Converti M. Attaching a stigma to the LGBTQI+ community should be avoided during the monkeypox epidemic. J Med Virol. 2023 Jan;95(1):e27913. [CrossRef] [PubMed]
- Tascini C, Geminiani M, Sbrana F, Pagotto A, Martini L. Possible tattoo-transmitted monkeypox viral infection. Intern Emerg Med. 2022 Nov;17(8):2421-2422. [CrossRef]
- Del Río García V, Palacios JG, Morcillo AM, Duran-Pla E, Rodríguez BS, Lorusso N. Monkeypox outbreak in a piercing and tattoo establishment in Spain. Lancet Infect Dis. 2022 Nov;22(11):1526-1528. [CrossRef]
- Viedma-Martinez M, Dominguez-Tosso FR, Jimenez-Gallo D, Garcia-Palacios J, Riera-Tur L, Montiel-Quezel N, Linares-Barrios M. MPXV Transmission at a Tattoo Parlor. N Engl J Med. 2023 Jan 5;388(1):92-94. [CrossRef] [PubMed]
- Beaumont AL, Raphaël E, Bertin C, Lariven S, Peiffer-Smadja N. Mpox lesions on a tattoo. Lancet Infect Dis. 2023 Jun;23(6):762. [CrossRef] [PubMed]
- Tascini C, Sbrana F, Giuliano S, Geminiani M, Pagotto A. Monkeypox virus transmission in tattoo parlor. New Microbiol. 2023 Sep;46(3):315-316. [PubMed]
- Mbala PK, Huggins JW, Riu-Rovira T, Ahuka SM, Mulembakani P, Rimoin AW, Martin JW, Muyembe JT. Maternal and Fetal Outcomes Among Pregnant Women With Human Monkeypox Infection in the Democratic Republic of Congo. J Infect Dis. 2017 Oct 17;216(7):824-82. [CrossRef] [PubMed]
- Schwartz DA, Mbala-Kingebeni P, Patterson K, Huggins JW, Pittman PR. Congenital Mpox Syndrome (Clade I) in Stillborn Fetus after Placental Infection and Intrauterine Transmission, Democratic Republic of the Congo, 2008. Emerg Infect Dis. 2023 Nov;29(11):2198-2022. [CrossRef]
- Cono J, Cragan JD, Jamieson DJ, Rasmussen SA. Prophylaxis and treatment of pregnant women for emerging infections and bioterrorism emergencies. Emerg Infect Dis. 2006 Nov;12(11):1631-7. [CrossRef]
- Kopanou Taliaka P, Tsantes AG, Konstantinidi A, Liakou P, Tavoulari EF, Piovani D, Bonovas S, Iacovidou N, Tsantes AE, Sokou R. Monkeypox disease and pregnancy. Where are we today? A review of literature. J Perinatol. 2023 Apr;43(4):417-423. [CrossRef] [PubMed]
- Mattar R, Neto ARB, Luz AG, Hatanaka A, Zaconeta A, Guazzelli CAF, Traina E, Baptista FS, Osanan G, Duarte G, Ramos JGL, Oppermann ML, Francisco RPV, Cardoso SMLQ, Quintana SM, Sun SY, Borges VTM. Expert Recommendations on Monkeypox (MPX) in Pregnancy, Postpartum and Lactating Women. Rev Bras Ginecol Obstet. 2022 Dec;44(12):1122-1125. [CrossRef]
- Dashraath P, Nielsen-Saines K, Mattar C, Musso D, Tambyah P, Baud D. Guidelines for pregnant individuals with monkeypox virus exposure. Lancet. 2022 Jul 2;400(10345):21-22. [CrossRef]
- Dashraath P, Nielsen-Saines K, Rimoin A, Mattar CNZ, Panchaud A, Baud D. Monkeypox in pregnancy: virology, clinical presentation, and obstetric management. Am J Obstet Gynecol. 2022 Dec;227(6):849-861.e7. [CrossRef]
Figure 1.
The PRISMA 2020 flow diagram depicting the search strategy adopted in the present systematic review.
Figure 1.
The PRISMA 2020 flow diagram depicting the search strategy adopted in the present systematic review.
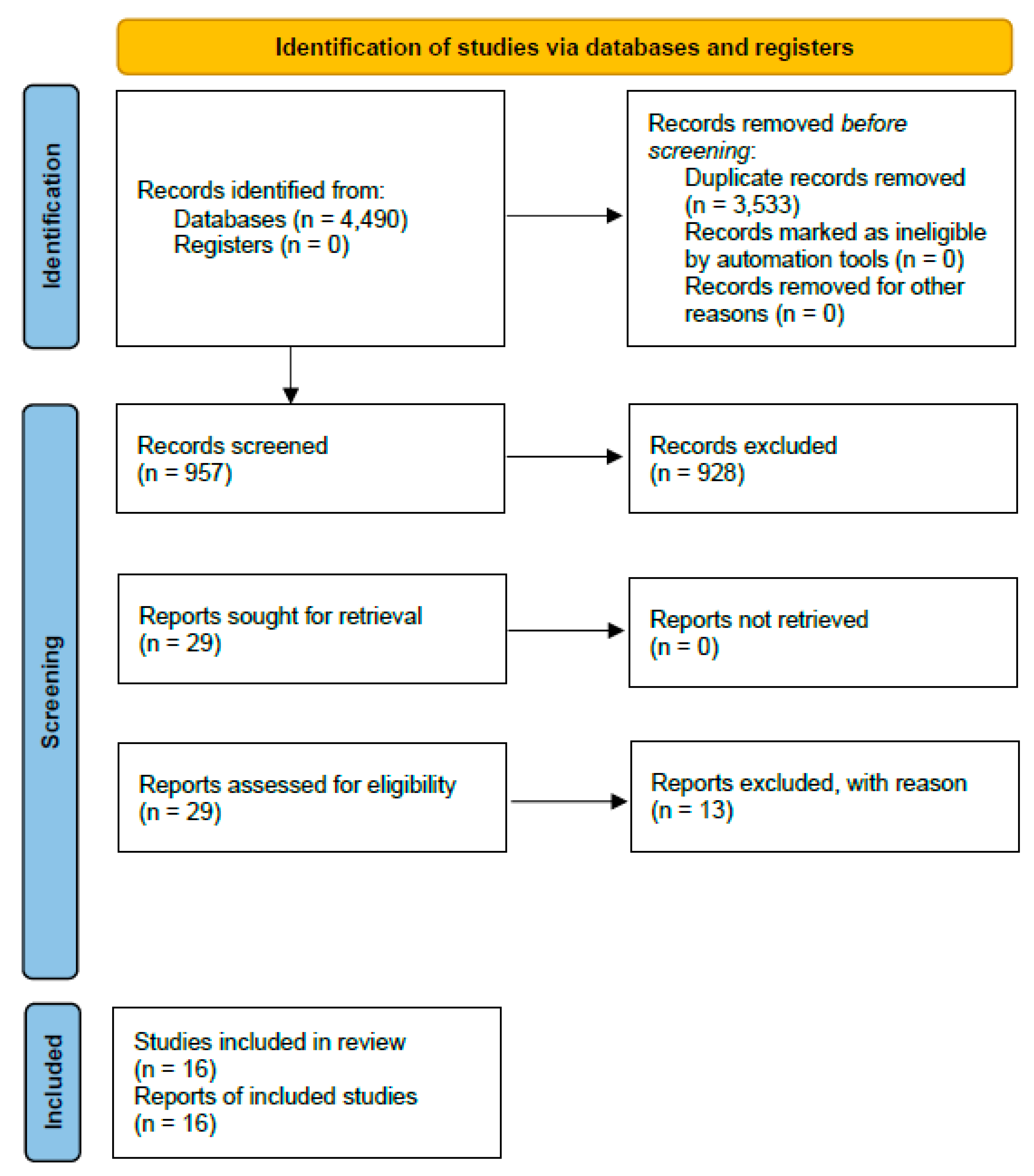
Figure 2.
Comparative Prevalence of Mpox Symptoms in Male and Female Patients.
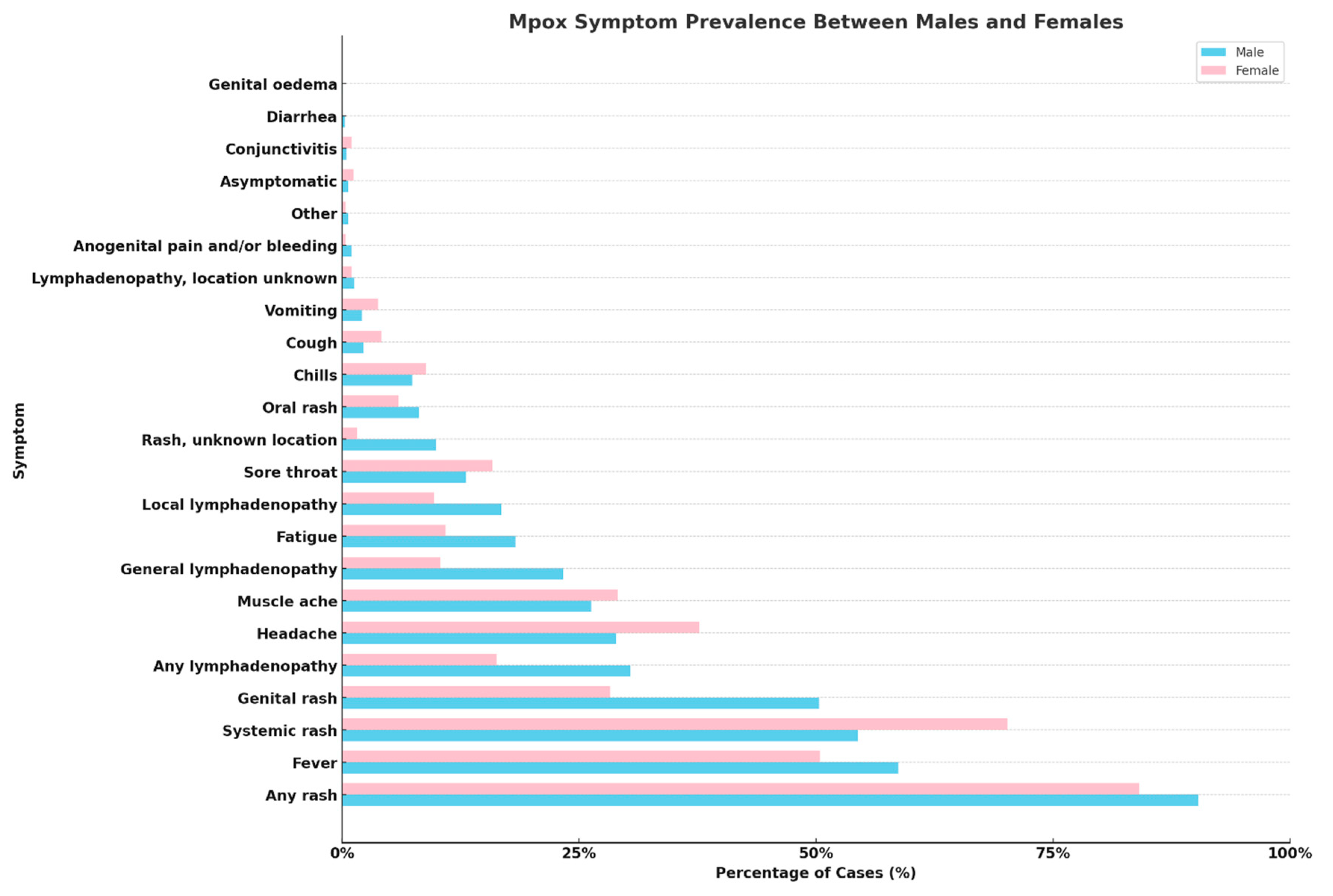

Table 1.
Systematic Review Criteria for Investigating Mpox in Women: A PECOS-Based Framework with Search Methodology Overview.
Table 1.
Systematic Review Criteria for Investigating Mpox in Women: A PECOS-Based Framework with Search Methodology Overview.
| Search criteria | Brief description |
|---|---|
| Population | Women affected by Mpox, including cisgender and transgender women, and non-binary individuals assigned female at birth |
| Exposure | Infection with Mpox virus |
| Comparator | Men (either cisgender or transgender, and non-binary individuals assigned male at birth) |
| Outcome | Clinical manifestations of Mpox, epidemiological features, transmission routes, treatment responses |
| Study Design | Cohort studies, case reports, cross-sectional studies, online surveys focusing on Mpox in the specified population |
| Keywords | (Monkeypox OR Mpox) AND (women OR woman OR female* OR male-to-female OR transwoman OR transwomen OR pregnant OR pregnancy OR lactation OR breastfeeding OR postpartum) |
| Databases Searched | MEDLINE/PubMed, Scopus, Web of Science, EMBASE |
| Hand-searched target journals | AJOG Glob Rep: Emerg Infect Dis; Enferm Infecc Microbiol Clin; Euro Surveill; IDCases; IJID Reg; J Eur Acad Dermatol Venereol; Lancet; Lancet Infect Dis; MMWR Morb Mortal Wkly Rep; Medicina (B Aires); Ned Tijdschr Geneeskd; Obstet Gynecol; Open Forum Infect Dis; Travel Med Infect Dis; Viruses |
| Gray literature | WHO, PHAC, CDC, ECDC, UKHSA |
Table 2.
Comparative Analysis of Mpox's Clinical and Epidemiological Patterns in Women: A Global Perspective.
Table 2.
Comparative Analysis of Mpox's Clinical and Epidemiological Patterns in Women: A Global Perspective.
| Study | Study location | Study type | Participant details | Main findings | Specific observations |
|---|---|---|---|---|---|
| Oakley et al. [26] | USA | Cohort Study | 769 cisgender women, including 23 pregnant individuals (21 cases of Mpox during pregnancy and 2 within 3 weeks of pregnancy) | Predominant impact on specific ethnic groups; sexual or intimate contact as primary transmission route | Cases among pregnant women; some required hospitalization |
| Sánchez Doncell et al. [27] | Argentina | Retrospective Analysis | 3 women, including 2 cisgender women, and 1 transgender woman | Low incidence among women; focus on sexual health impacts | No complications reported; symptoms included headache, myalgias, fever |
| Coutinho et al. [28] | Brazil | Surveillance Data | 108 women (cisgender and transgender), 10 non-binary persons | Older women, more non-sexual contact, fewer genital lesions, lower HIV prevalence compared to men | Hospitalizations but no deaths among women |
| Grothe et al. [29] | Europe | Online Survey | Women across Spain and Belgium, among others | Higher likelihood of infection in Spain and Portugal | Disparities in diagnosis delays and clinical manifestations between genders |
| Vallejo-Plaza et al. [30] | Spain | Surveillance data analysis | Both men and women with Mpox cases reported in Spain | Women constituted 2.1% of total Mpox cases, showing a younger median age compared to men The primary route of transmission was close contact during sexual relations for both genders, but women also had significant other transmission routes |
Women experienced longer diagnosis delays Women showed different symptom patterns and risk profiles |
| Thornhill et al., [31] | Global (15 countries) | Data Collection | 136 cisgender and transgender women, non-binary individuals | High HIV prevalence among trans women; many contracted virus through sexual contact | Misdiagnosis in a significant portion; majority presented with anogenital rash |
| Mancha et al. [32]; Cole et al. [33]; Ezzat et al. [34]; van Hennik and Petrignani [35]; Napoli et al. [36]; Ogoina and James [37]; Sampson et al. [38]; Renfro et al. [39]; Dung et al. [40] | Globally (various case Reports) | Case Reports | Individual women cases | Unusual transmission routes; severe complications in some cases | Diversity in clinical manifestations and transmission routes highlighted |
| Schwartz and Pittman [41] | Globally (various case reports) | Review of 58 cases | Cases of pregnant women positive for Mpox infection during the 2022–2023 outbreak | No documented cases of negative outcomes Absence of complications linked to Mpox Clade IIb |
Mpox clade could influence the severity of the infection and its impact on pregnancy and fetal health |
Table 3.
Comprehensive Overview of Diverse Mpox Cases Among Women: Transmission, Clinical Presentation, and Treatment Outcomes.
Table 3.
Comprehensive Overview of Diverse Mpox Cases Among Women: Transmission, Clinical Presentation, and Treatment Outcomes.
| Study | Patient Profile | Transmission Route | Clinical Presentation | Treatment and Outcome |
|---|---|---|---|---|
| Mancha et al. [29] | 30-year-old female, Fitzpatrick phototype III | Oro-mammary sex | Erythematous papule on left nipple evolving into flat ulceration with hemorrhagic crust and umbilicated pustules; fever, lymphadenopathy | Symptomatic care, topical fusidic acid; recovered |
| Cole et al. [30] | 35-year-old White, apparently healthy woman from the UK | Unprotected sex | Severe genital lesions, systemic symptoms, encephalitis, longitudinally extensive transverse myelitis | Antivirals (tecovirimat, cidofovir), analgesia, antibiotics, steroids, plasma exchange; remarkable neurological recovery |
| Ezzat et al. [31] | 31-year-old female in Switzerland | Not specified | Painful vulvar lesions, generalized Mpox lesions | Initial misdiagnosis; confirmed Mpox through PCR; treatment details not specified |
| van Hennik and Petrignani [32] | 57-year-old female, partner of a bisexual man | Close contact | Lesions at vaginal opening | Symptom duration and treatment not detailed |
| Napoli et al. [33] | 28-year-old woman with gastroesophageal reflux, untreated atopic dermatitis | Not specified, recent tattoo | Intense ear pain, multiple vesiculopustular lesions | Oral tecovirimat; complications included pain, GI distress, bacterial superinfection, AKI, anemia |
| Ogoina and James [34] | 24-year-old Nigerian female sex worker | Sexual contact | Fever, vesiculopustular lesions on groin and genital area | Not specified |
| Sampson et al. [35] | 20-year-old pregnant woman at 31 weeks of gestation | Sexual contact | Vaginal discharge, bleeding, painful urination, labial ulcer, herpes-like rash | Tecovirimat and acyclovir; stable condition, discharged, lesions resolved |
| Renfro et al. [36] | Two pregnant, heterosexual cisgender women | Not specified | Vaginal itching, chorioamnionitis during childbirth | Induced labor, antibiotics for chorioamnionitis; details of Mpox treatment not specified |
| Dung et al. [37] | Two women, 35 and 38 years old, traveled from UAE to Vietnam | Sexual contact | Fever, maculopapular rash | Isolation, oral acyclovir for co-infection in Patient 1; treatment for Patient 2 not specified |
Table 4.
Strategic Directions for Advancing Mpox Research and Public Health Interventions in Women and Gender-Diverse Populations.
Table 4.
Strategic Directions for Advancing Mpox Research and Public Health Interventions in Women and Gender-Diverse Populations.
| Research area | Recommendations | Suggestions |
|---|---|---|
| Transmission Dynamics.. | Conduct studies focusing on non-sexual transmission routes and environmental factors | Collaborate with community organizations to reach diverse populations |
| Clinical Manifestations. | Investigate unique clinical manifestations in women, especially those with underlying health conditions | Develop specialized training for healthcare providers on recognizing and managing Mpox in women |
| Mpox in Pregnancy | Systematically document Mpox outcomes in pregnant women to inform management guidelines | Engage obstetric and gynecological associations to develop and disseminate guidelines |
| Impact on Transgender Women and Non-Binary Individuals | Address the lack of data for transgender women and non-binary individuals, focusing on their specific health needs | Include transgender and non-binary individuals in research and public health campaigns |
| Genomic Monitoring | Implement genomic analysis to track virus evolution and its implications for treatment and vaccine efficacy | Coordinate with international health organizations for data sharing and joint research initiatives |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



