
Submitted:
14 December 2023
Posted:
29 January 2024
You are already at the latest version
Abstract
Background: Neuromuscular electrical stimulation (NMES) has beneficial effects on physical functions in Multiple Sclerosis (MS) patients. However, the neurophysiological mechanisms underlying these functional improvements are still unclear. This study aims at comparing acute responses in spinal excitability, as measured by soleus Hoffmann reflex (H-reflex), between MS patients and healthy individuals, following three experimental conditions involving the ankle planta flexor muscles: 1) passive NMES (pNMES); 2) NMES superimposed to isometric voluntary contraction (NMES+); and 3) isometric voluntary contraction (ISO). Methods: 20 MS patients (MSp) and 20 healthy individuals as control group (CG) took part in a single experimental session. During each condition, participants performed 15 repetitions of 6 seconds at 20% of maximal voluntary isometric contraction, with 6 seconds of recovery between repetitions. Before and after each condition, H-reflex amplitudes were recorded. Results: In MSp, H-reflex amplitude did not change following any experimental condition (ISO: p = 0.506; pNMES: p = 0.068; NMES+: p = 0.126). In CG, H-reflex amplitude significantly increased following NMES+ (p = 0.01), decreased after pNMES (p = 0.000) and was unaltered following ISO (p = 0.829). Conclusion: the different H-reflex responses between MS and CG might reflect a reduced ability of MS patients in modulating spinal excitability.
Keywords:
electric stimulation
; H-reflex
; spinal excitability
; multiple sclerosis
; soleus
; GABA
; presynaptic inhibition
; rehabilitation
1. Introduction
Multiple sclerosis (MS) is the most common immune-mediated disorder that affects the central nervous system (CNS) [1], involving approximately 2.8 million people worldwide [2]. MS is characterized by axonal damages in the brain and the spinal cord, which lead to conduction block or delay of electrical potentials along neuronal pathways throughout the CNS [3,4]. Consequently, people with MS (pwMS) experience a wide range of disabilities [5,6], which lead to a progressive limitation of functioning in daily activities, thus reducing the health-related quality of life (HRQOL) [7,8].
In MS rehabilitation, physical activity is an important non-pharmacological tool for countering the multifaceted symptoms of the disease. [9,10,11]. The benefits of exercise for the MS population include improving or maintaining walking ability and balance, cardiovascular and neuromuscular fitness, physical and psychological fatigue, HRQOL, depression, and chronic disease risk profiles [12,13,14,15,16,17,18,19,20]. Unfortunately, despite the benefits of physical activity, 78% of pwMS are physically inactive [11,21,22]. Particularly, patients with advanced MS, or wheelchair users, may find exercise very difficult due to significant fatigue, leg muscle paresis, and poor flexibility [23]. For these reasons, several rehabilitative techniques have been developed in recent years to improve motor function using technological devices, such as neuromuscular electrical stimulation (NMES). NMES is a Food and Drug Administration–approved treatment for reducing muscle pain and spasm, as well as disuse-associated muscle atrophy [24]. NMES induces visible muscle contractions by depolarizing local motor nerves via intermittent electrical stimuli that are transcutaneously applied to superficial skeletal muscles [25,26]. This training technique has been widely employed in rehabilitation clinics to treat several pathological conditions of the neuromuscular system [27,28,29] and other neurological diseases [30,31]. Furthermore, many researchers have reported a broad range of positive effects of NMES on motor and brain functions [29,31,32,33]. Specifically, in relation to MS, some evidence suggests that individuals with greater levels of disability can experience gains in physical function and perceived physical health when exercise training is combined with NMES [34,35]. Some authors found that supplementing a traditional training program with NMES improves muscle strength, force steadiness, gait speed, walking endurance, self-reported levels of walking disability, and balance [36,37,38], as well as reduces fatigue level in pwMS, even in those who use walking aids [38]. Furthermore, other studies reported that NMES applied during cycling enhances muscle strength and cardiorespiratory metabolism, improves walking, and increases the ability to transfer independently for individuals who rely on manual wheelchairs for daily mobility [34,35]. Altogether, these findings suggest that NMES could be considered a promising treatment option for persons with primary or advanced MS, who often have very limited capacity for strength and aerobic exercise. However, although these clinical results have been recognized by researchers and clinicians, the neurophysiological mechanisms behind NMES training benefits are still unclear.
The Hoffmann reflex (H-reflex), which represents a measure of reflex response elicited by percutaneous electrical stimulation over a peripheral mixed nerve, has been extensively used to investigate some of the neurophysiological mechanisms underlying NMES intervention in both healthy young and elderly individuals [39,40,41,42,43]. As a monosynaptic spinal reflex, the H-reflex could be an effective tool for studying the modulation of spinal excitability under certain conditions [44]. Several research works revealed that NMES stimulation modulates H-reflex responses in healthy individuals [39,41,42,43,45,46]. Some authors demonstrated an acute potentiation of soleus H-reflex amplitude following a single session of NMES superimposed onto voluntary isometric contractions of the ankle plantar flexor muscles [39,40,41]. On the contrary, an acute depression of H-reflex amplitude was reported when NMES was passively applied over muscles [39,41,43,47,48,49]. Based on these results, several authors stated that NMES modulates spinal excitability in healthy individuals by acting on some presynaptic mechanisms which are mainly involved in the facilitation/inhibition of the H-reflex [39,41,42,43,47,50]. However, to the best of our knowledge, the spinal mechanisms underlying NMES training have not been investigated in neurological populations and, particularly, in pwMS.
Therefore, the aim of this study was to compare the acute modulation of spinal excitability, measured by means of H-reflex in the Soleus (SOL) muscle, between MS patients and healthy individuals, following a single intervention consisting of three experimental conditions: 1) NMES superimposed onto voluntary contraction (NMES+) of the plantar flexor muscles of the ankle; 2) passive NMES (pNMES) applied to the plantar flexor muscles of the ankle; 3) voluntary isometric contractions (ISO) of the plantar flexor muscles of the ankle. Based on the results reported from previous studies that have applied this protocol on healthy individuals [39,41], the first hypothesis is that the H-reflex would increase after NMES+ in MS patients and healthy individuals; the second hypothesis is that the H-reflex would decrease after pNMES in MS patients and healthy individuals; and, the third hypothesis is that the H-reflex would remain unchanged after ISO condition in MS patients and healthy individuals.
2. Materials and Methods
2.1. Participants
Forty volunteers participated in the study and were divided into 2 groups: ‘MSp’, which involved 20 patients with MS (mean ± SD, age: 38.8 ± 10.9 years, mass: 68.8 ± 13.1 kg, height: 1.72 ± 0.8 m; EDSS < 5 ); ‘CG’, which involved 20 healthy individuals as control group (mean ± SD, age: 39.2 ± 11.9 years, mass: 67.8 ± 12,26 kg, height: 1.71 ± 0.7 m). The sample size was determined a priori based on a statistical power analysis (G*Power software v.3.1.9.4) for a mixed-model ANOVA (within-between factors) (α=0.05, statistical power=0.95, effect size = 0.26), as described by Cohen (1992).
MSp participants were recruited according to the following inclusion criteria [36,51]: relapsing-remitting MS, EDSS score ≤ 5, aged between 20 and 60 years, able to walk independently at household distances, never had experience with NMES before. On the other hand, they were excluded from the study according to the following exclusion criteria [36,51]: MS relapse in the past three months, history of cardiovascular disease, seizures, implanted pacemaker, unstable long bone fractures, allergies to surface electrode gel, ongoing pregnancy, neural lesions at or below the lumbar enlargement, implanted biomedical devices or metal, contra-indications to electrical stimulation, lung problems, epilepsy, uncontrolled hypertension, orthopedic problems in the lower limbs. CG participants were recruited by matching them with the MS patients for age, gender, height, and body mass. They were excluded from the study if they presented any neurological or orthopedic disorders. In addition, both MSp and CG volunteers did not engage in regular physical activity or sport practice more than three times a week, for more than 40–60 min each time.
MSp participants were recruited at the Multiple Sclerosis Centers of 'Santa Maria Goretti' Latina hospital and ‘San Pietro, Fatebenefratelli’ Rome hospital, and were identified from initial screening questionnaire that was administered by the clinicians. CG participants were recruited at the University of Rome - Foro Italico and were identified, by the research assistant, using an initial screening questionnaire. During a first appointment, participants of both groups received the participant information sheet and were verbally informed of the study procedures. They were shown the equipment and were given 15 minutes to familiarize with NMES. During a second appointment (2-4 days later) they were asked to sign an informed consent that was approved by the institutional ethics review board of the University of Rome - Foro Italico” (CAR 96/2021). Participants who gave informed consent and met the inclusion/exclusion criteria were assigned a trial code number by which all their test data were subsequently named and stored. The main investigator held a paper list of the subjects’ name, age, trial code number and group allocation in a locked filing cabinet.
2.2. Instrumentation
2.2.1. Maximum voluntary isometric contraction (MVIC)
An ankle dynamometer v1.0 (OT Bioelettronica, Turin, Italy) was used to measure maximal voluntary isometric contractions (MVIC) of the ankle plantar flexor muscles. Participants were seated with their hips at 90° (0° = neutral hip position), their knees at 60° (0° = full knee extension) and their ankles at 0° of ankle plantar-dorsi flexion (0° = foot orthogonal to the shank axis), the lateral malleolus aligned with the dynamometer's axis and the foot tightly fastened to the device’s footplate [39,41], as described in Figure 1. Warm-up and familiarisation exercises consisted of 15 - 20 submaximal isometric contractions. MVIC testing involved a rapid increase in ankle plantar flexor force to a maximum. A computer screen provided visual feedback to participants during the test. Participants were instructed and verbally encouraged to maintain their maximal isometric contraction for three seconds before relaxing. The best result was selected after a minimum of three attempts, separated by 3 min rest intervals to minimize muscle fatigue. MVIC was then used to establish a target isometric plantarflexion force of 20% of MVIC. This represents the constant force that participants were required to reach during the three experimental conditions. This force level was chosen based on previous research investigating changes in spinal activation following acute non-fatigue NMES protocols [39,40,41,42,48,52]. In addition, at the end of the entire protocol, MVIC was evaluated again to determine whether muscle fatigue had developed.
2.2.2. Surface electromyography (sEMG)
Surface electromyography (sEMG) measurements were conducted with a 64-channel EMG device with Wi-Fi communication (OT Bioelettronica, Turin, Italy) at a sampling of 2000 Hz. In accordance with the SENIAM guidelines for soleus muscle [53], two pre-gelled, self-adhesive electrodes (36 × 40 mm, FIAB, Florence, Italy) were placed on the soleus muscle (SOL), approximately 2-3 cm below the gastrocnemius musculotendinous junction with Achilles tendon, with an inter electrode distance of 20 mm (centre-to-centre). An additional reference electrode (36 mm x 40 mm, FIAB, Florence, Italy) was placed on the lateral malleolus, as shown in Figure 2. Before attaching the surface electrodes, the participants' skin was shaved, gently abraded with sandpaper, and cleaned with ethyl alcohol to keep the impedance below 5 kΩ. sEMG was used to record H-reflexes and motor waves.
2.2.3. Soleus H-reflex
Single rectangular biphasic pulses of 1 ms duration were delivered to the posterior tibial nerve using a constant voltage electrical stimulator (Digitimer DS7A, Hertfordshire, AL7 3BE, England, UK). As a first step, participants were asked to lie down on a physiotherapy bed in a prone position to find the optimal stimulation site in the popliteal fossa, which was identified using a cathode ball electrode, as illustrated in Figure 3. Therefore, two self-adhesive electrodes were placed in a bipolar configuration to elicit the H-reflex: the cathode (diameter 24 mm, Spes Medica, Genova, Italy) was applied to the posterior tibial nerve, while the anode (diameter 50 × 50 mm, Compex Dura-Stick® Plus a Snap, DJO Global, Vista, CA, USA) was applied anteriorly to the knee, above the patella [39,41,54]. Afterwards, participants were asked to sit in the dynamometer chair, as described in the MVIC section (Figure 1), with a band secured around the distal thigh and the ankle to prevent the legs from falling into external rotation and abduction. In this position, the H-reflex recruitment curve was assessed by using sEMG to record the involuntary muscle activity of the triceps surae muscle in response to the stimulation. The recruitment curve was obtained by plotting the amplitude of the recorded H-reflexes over the amplitude of the corresponding motor waves (M-waves). Based on previously established procedures [39,41,54], a series of single electrical stimulations, with a gradual increase in current intensity, were applied to the tibial nerve in the popliteal fossa. A stimulation interval of 4-10 seconds was chosen to prevent fatigue [55], with stimulus intervals unevenly spaced to prevent anticipation and reduce post-activation depression [55]. The stimulus intensity was gradually increased with steps of 1 mA until the maximum H-reflex (Hmax) and motor wave (Mmax) amplitudes were reached; to confirm no further increase in Mmax amplitude, stimulus intensity was increased slightly beyond this point. A peak-to-peak analysis of the sEMG recordings was used to measure the amplitude of H-reflexes and M-waves. According to previous studies [39,41,54], the test reflex stimulus intensity was determined to obtain an H-reflex (Htest) on the ascending limb of the recruitment curve with an amplitude between 80 and 85% of the Hmax, as illustrated in Figure 4. To ensure stimulus consistency and repeatability, a small M-wave (Mtest) corresponding to the Htest was selected and monitored throughout the entire experiment [39,40]. The evoked H-reflexes were accepted if the M-wave amplitude was within 5% of the selected Mtest. Twenty H-reflexes were recorded before and after each neuromechanical assessment. Additionally, all H-reflex and M-wave amplitudes were normalized to Mmax amplitudes, averaged within each trial, and analyzed off-line. Furthermore, the Hmax/Mmax ratio of both MSp and CG was calculated, using the amplitudes measured during the recruitment curve, to determine the overall level of reflex excitability of the motor pool at rest.
For this study, the H-reflex of the SOL muscle was chosen given the accessibility of the posterior tibial nerve which could be easily identified and stimulated to evoke the reflex responses. Moreover, as the SOL muscle has stronger spinal connections compared to other limb muscles [42,56], the SOL H-reflex has been one of the most studied reflexes to assess spinal excitability [39,40,41,54]
2.2.4. Neuromuscular electrical stimulation (NMES)
A muscle stimulator (Chattanooga Wireless Professional, DJO Global, Vista, CA, USA), which produces rectangular, balanced biphasic pulses, was used to electrically stimulate the ankle plantar flexor muscles. The NMES stimulator was always accurately and safely managed by the investigator. At the beginning of the experimental session, motor points were determined using a hand-held cathode ball electrode, as described in the electrical stimulator user’s guide. Therefore, 3 self-adhesive electrodes (diameter 50 × 50 mm, Compex Dura-Stick® Plus a Snap, DJO Global, Vista, CA, USA) with positive polarity were applied over the motor points of gastrocnemius lateralis, gastrocnemius medialis, and soleus muscles, while 3 three self-adhesive electrodes with negative polarity were applied to the same muscles about 3 cm above the positive electrodes (Figure 2). NMES was administered using a pulse frequency between 20 and 50 Hz, and a pulse duration of 400 μs for successfully stimulating both slow- and fast-twitch muscle fibers and minimizing discomfort during the simulation [25]. The stimulation intensity was progressively increased (according to each participant’s tolerance) to achieve the target force of 20% of MVIC, either with NMES passively applied to the target muscles or NMES superimposed on voluntary contractions. According to Wiest et al. (2017) [57], the intensity of NMES used to generate 20% of MVIC force does not induce pain or discomfort.
2.3. Experimental procedure
All assessments were performed in the “Laboratory of Bioengineering and Neuromechanics of Movement” at the University of Rome “Foro Italico” between November 2022 and May 2023. Each participant took part in a single experimental session lasting around 150 minutes. First, participants were asked to lie down in a prone position on a physiotherapy bed to find the correct point of electrical stimulation in the popliteal fossa to elicit the H-reflex and the corresponding M-wave (Figure 3). Participants were then introduced to the NMES and familiarized with the stimulation of the ankle plantar flexor muscles for about 10 minutes. After that, they were asked to sit in the dynamometric chair, as previously described (Figure 1), and maintain this position for the entire experimental session. They had a computer screen in front of them for visual feedback. In this position, the MVIC of the triceps surae muscles was assessed [39,41], and the H-reflex recruitment curve was obtained. Subsequently, participants were administered three experimental conditions involving the contraction of the ankle plantar flexor muscles: 1) Passive NMES (pNMES); 2) NMES superimposed on voluntary isometric contraction (NMES+); 3) Voluntary isometric contraction only (ISO).
The order of conditions was randomly administered to each participant. During each condition, which lasted around 3 min, participants were asked to perform 15 intermittent contractions (6 s contraction/6 s rest). To prevent long-lasting effects caused by the previous condition, recovery periods of 15 minutes were provided between the conditions [39,40,58]. The entire experimental protocol, illustrated in Figure 5, was designed to modulate spinal excitability, and to prevent muscle fatigue, as reported in previous investigations [39,41,49]. During ISO condition, participants were asked to achieve the target force of 20% of MVIC by voluntarily contracting their plantar flexor muscles. During pNMES condition, current pulse intensity was progressively increased until the target force of 20% of MVIC was reached by passively stimulating plantar flexor muscles. Participants were instructed not to voluntarily contract their ankle plantar flexor muscles during the passive NMES to isolate the effects of NMES intervention. To the best of our knowledge, none of the participants voluntarily contracted their muscles during pNMES. During NMES+ condition, current pulse intensity was set to produce half of the target force (10% of MVIC), while participants voluntarily contracted their plantar flexor muscles at 10% of MVIC to reach the full target force (20% of MVIC). The investigator adjusted the intensity of the simulation by asking participants to relax their calf muscles before and after the first and the tenth contractions. Whenever participants reported pain or discomfort, NMES conditions were immediately stopped. Each experimental condition was preceded by a pre-treatment assessment of baseline (PRE) H-reflex and immediately followed by a post-treatment (POST) H-reflex assessment. To exclude the contribution of fatigue, the MVIC was repeated at the end of the entire experiment. For MSp, all the procedures were performed on the participant’s weaker or more affected leg (based on self-report), as described by Almuklass et al (2018) [36]. For CG, all experimental procedures were performed on the dominant leg of each participant, as described by Botter et al. (2011) [26]. Leg dominance was established by asking to the participants the preferred limb for hopping or kicking a ball [59].
2.4. Data analysis
All data were analyzed using a custom Matlab code (Matlab 2018b, Mathworks Inc., Natick, MA, USA). The sEMG recordings were checked for possible pre-activation of SOL muscle before reflex assessment. If pre-activation occurred, the sEMG trace and the associated H-reflex measure were removed from the analysis.
2.5. Statistical analysis
Statistical analysis was performed using IBM SPSS 24.0 (IBM Corp., Armonk, NY, USA). A two-way mixed ANOVA was used to investigate statistical differences in H-reflex and M-wave measures between the two groups, the three experimental conditions, and over time. “Condition” and “Time” represented the two within-subjects factors with “Condition” having three levels (ISO, pNMES and NMES+), and “Time” having two levels (PRE and POST). ‘Group’ represented the between-subjects factor, with ‘MSp’ referred to MS patients, and ‘CG’ referred to healthy individuals of the control group. When a significant main effect or interaction was found, paired t tests were used for post hoc analyses. In addition, a t test was performed to compare MVIC values at the beginning (Pre-test) and at the end (Post-test) of the entire experimental protocol in both MSp and CG as well as to compare the baseline level of Hmax/Mmax ratio between the two groups. The alpha level for statistical significance was set to p < 0.05, with a Bonferroni correction for multiple post hoc comparisons. Normality and sphericity of the data were checked using the Shapiro–Wilk Test and the Mauchly Test, respectively. Data are reported as group mean ± standard deviation (SD).
3. Results
All recorded data showed a normal distribution and the Mauchly test confirmed that the assumption of sphericity was not violated for any of the variables analyzed.
The mixed ANOVA on the normalized H-reflex amplitude showed a main effect of Condition (F = 3.292, ηp2 = 0.017, p = 0.043) and a Condition*Group interaction (F = 4.909, ηp2 = 0.025, p = 0.010), a Condition*Time interaction (F = 16.137, ηp2 = 0.036, p < 0.000), and a Condition*Time*Group interaction (F = 9.569, ηp2 = 0.022, p < 0.000). Post hoc analysis showed no significant differences in H-reflex amplitude between PRE and POST measures for all experimental conditions (ISO: p = 0.506; pNMES: p = 0.068; NMES+: p = 0.126) in MSp. Conversely, H-reflex amplitude significantly increased following NMES+ (+12.6%; p = 0.010), decreased after pNMES (− 17.8%; p < 0.000) and was unaltered following ISO (p = 0.829) in CG. Moreover, post hoc analysis showed no significant differences in the amplitude of H-reflex measured before (PRE) all the three experimental conditions, in both MSp (PRE ISO vs POST ISO: p = 0.306; PRE pNMES vs POST pNMES: p = 0.656; PRE NMES+ vs POST NMES+; p = 0.339) and CG (PRE ISO vs POST ISO: p = 0.342; PRE pNMES vs POST pNMES: p = 0.076; PRE NMES+ vs POST NMES+; p = 0.168). PRE and POST values of all conditions are reported in Table 1 as mean ± standard deviation (SD).
The mixed ANOVA on the normalized M-wave amplitude showed no effect of Time (F = 0.071, ηp2 = 0.002, p = 0.791) and Condition (F = 0.121, ηp2 = 0.003, p = 0.886) as well as no Condition*Group interaction (F = 0.119, ηp2 = 0.003, p = 0.888), no Time*Group interaction (F = 0.560, ηp2 = 0.015, p = 0.459), no Condition*Time interaction (F = 1.514, ηp2 = 0.038, p = 0.229) and no Condition*Time*Group interaction (F = 2.276, ηp2 = 0.057, p = 0.110).
Figure 6 (a, b) describes a typical example of SOL H-reflex and M-wave sEMG response to a series of 20 electrical stimuli that were averaged within the same trial before (PRE) and after (POST) each experimental condition (ISO, NMES, NMES+) in one healthy participant of the CG (Figure 6a) and in one MS participant of the MSp (Figure 6b). Figure 7 (a, b) reports the mean values of SOL H-reflex amplitude and associated M-waves that were both normalized to Mmax before (PRE) and after (POST) the three experimental conditions (ISO, pNMES, NMES+) in MSp (Figure 7a) and in CG (Figure 7b).
The paired t-test analysis on the Hmax/Mmax ratio showed no significant differences between MSp and CG (p = 0,901), as illustrated in Figure 8.
The t-test analysis on the Pre-test and Post-test MVIC values showed no significant differences in both MSp (p = 0.655) and CG (p = 0.267), as illustrated in Table 2.
4. Discussion
The main result of this study was the different H-reflex response between healthy individuals and MS patients following a single NMES session. According to our hypotheses, in healthy individuals the amplitude of H-reflex decreased after pNMES, increased after NMES+, and did not change after ISO, confirming that NMES modulates spinal excitability. However, in contrast with our hypotheses, in MS patients there were no significant differences in H-reflex amplitude following both pNMES and NMES+, thus suggesting an alteration in the control of some presynaptic mechanisms related to the modulation of spinal reflexes. Finally, as hypothesized, no significant differences were found in MS patients after ISO. Therefore, of clinical significance, it appears that in MS patients a single session of NMES, either passive or superimposed to voluntary movement, has the same effect as voluntary isometric exercise and does not affect spinal excitability.
In our study, healthy individuals showed an acute attenuation of SOL H-reflex amplitude, which is consistent with the results of previous studies reporting that NMES inhibits spinal reflexes when it is passively applied [39,41,43,47,48,49]. These studies suggested that pNMES may induce specific neuroplasticity of inhibitory pathway at spinal cord level, leading to a decreased spinal excitability [43]. Indeed, several authors stated that NMES directly acts on some presynaptic mechanisms that are primarily involved in the modulation of the H-reflex [47,54], such as presynaptic inhibition (PSI). PSI, which is one of the most important spinal regulatory networks [60], is mediated by the action of an inhibitory interneuron which acts on the Ia-afferent terminals, leading to a reduction in the number of neurotransmitters released in the synapse between Ia-afferent fiber and alpha-motoneuron. The decrease in neurotransmitter’s release results in a concomitant reduction in depolarization of the alpha-motoneuron, which is induced by Ia-afferent activity. Therefore, it was proposed that increased PSI in Ia-afferent terminals could be considered as the main responsible for the substantial attenuation soleus H-reflex amplitudes that are induced by passive NMES in healthy individuals [39,41,47,49,50]. A possible neurophysiological mechanism that may be associated to this phenomenon is primary afferent depolarization (PAD) [61], which induces a reduction in neurotransmitter’s release by prior depolarizing Ia-afferent terminals. Consequently, the neurotransmission between Ia-afferents and α-motoneurons is compromised. Pierrot-Deseilligny and Mazevet (2000) [50] suggested that since PAD interneurons have lower threshold than α-motoneurons, they might be more sensitive to repetitive electrical stimuli, thus resulting in decreased spinal excitability.
Regarding the effects of NMES+ on the healthy participants of our study, the increased SOL H-reflex amplitude was consistent with previous studies that were carried out in healthy individuals. Scalia et al. (2023) [41] and Borzuola et al. [39,40] reported an acute increase in H-reflex amplitude between 5 and 20% after a single experimental session during which participants performed voluntary isometric contractions of the ankle planta-flexor muscles together with NMES superimposed on the triceps surae muscles. Moreover, Lagerquist et al. (2012) [42] reported similar results in response to a protocol that consisted in voluntary isometric contractions of the ankle plantar flexor muscles paired with tibial nerve stimulation. Therefore, our results suggest that NMES+ may enhance spinal excitability, which might be associated with an increased force generation capacity in healthy individuals [42,54]. A reduced PSI in Ia-afferent terminals may be responsible for the significant increase in the H-reflex amplitude following NMES+ in healthy adults [39,41,47,54].
In contrast with our hypothesis, MS patients did not show any changes in the H-reflex responses immediately after both pNMES and NMES+. This is similar to recent results by Scalia et al. (2023) [41], who investigated the effects of pNMES and NMES+ in older individuals. The authors attributed the lack of modulation of the H-reflex to a different ability of older adults to modulate PSI with respect to young individuals [62,63,64,65,66].Therefore, the results of our study suggest that also in patients with MS there may be a change in PSI mechanisms. PSI occurs when an inhibitory neurotransmitter, like gamma-aminobutyric acid (GABA), acts on the GABA receptors of sensory afferent axons, resulting in a reduction in neurotransmitter release. Wang and colleagues (2006a, 2009) [67,68] suggested that changes in GABAergic function may play a key role in producing the motoneuron plasticity which directly underlies the modulation of H-reflex after conditioning NMES interventions in healthy individuals. However, it has been demonstrated that the synthesis, release, and reuptake of GABA are altered in MS patients, with GABAergic synapses being more vulnerable to phagocytosis [69,70]. Several findings from transcriptomic, proteomic, neurophysiological, and histological studies indicate that MS is characterized by pathological alteration of synaptic structure and function, also known as synaptopathy [70]. Particularly, it has been shown that neuroinflammation perturbates both inhibitory (mediated by GABA) and excitatory (mediated by glutamate) neurotransmission, which are significantly involved in the correct functioning of the CNS. The release of proinflammatory cytokines during acute MS attack increases glutamate-mediated synaptic transmission and reduces γ-aminobutyric acid-mediated synaptic signaling, altering the balance between the GABAergic and glutamatergic systems in the brain and spinal cord. When the alteration of synaptic homeostasis is maintained over time, it can become detrimental, leading to neurodegeneration of CNS. These observations may be highly relevant for explaining our results as inhibitory synapses are crucial for healthy neurotransmission [71,72]. However, further investigation is required to elucidate whether and how NMES alter synaptic neurotransmission in pwMS.
Another factor that may affect the lack of H-reflex response to NMES in MS patients is represented by spinal cord abnormalities. Several studies reported extensive demyelination and neuronal loss of both white and grey matter in the spinal cord [73,74,75,76,77,78]. MS patients show a reduction of synaptic spine density in both myelinated and demyelinated neurons, which leads to irreversible spinal symptoms, including alterations in spinal reflexes [75]. Interestingly, the results of our study showed no differences in the Hmax/Mmax ratio between MS patients and healthy individuals at baseline. Therefore, the different H-reflex responses between MS and CG could be exclusively attributed to the direct effects of passive and superimposed NMES on inhibitory and regulatory mechanisms that are involved in the synaptic neurotransmission at spinal cord level. Likely, the MS-induced neuronal damage was not severe enough to alter the H-reflex at rest, as we recruited MS patients with a low level of disability (EDSS ≤ 5). However, when the spinal reflex pathway was overloaded with external stimuli, such as NMES, the damage to the CNS could have impaired the inhibitory/excitatory mechanisms involved in the modulation of the H-reflex, potentially explaining the unaltered H-reflex responses that were found in MS patients after the NMES interventions. However, there is a gap in the literature related to the comparison of the Hmax/Mmax ratio between MS patients and healthy individuals, as the H-reflex has been only investigated as a measure of spasticity [56,79,80,81,82]. Only one study by Cantrell et al. (2022) [83] investigated the H-reflex in pwMS without spasticity with the aim of comparing its amplitude between limbs and correlate reflex asymmetry with postural control. This highlights the importance of future studies which should be focused on understanding the mechanisms underlying H-reflex modulation in MS patients who do not present spasticity symptoms.
Lastly, according to our hypothesis, no significant differences were found in H-reflex response after ISO both in healthy individuals and MS patients. This result is consistent with previous studies [39,41,42], showing unaltered H-reflexes after a protocol of isometric voluntary contractions of the ankle plantar flexor muscles. The lack of modulation in spinal excitability could be attributed to the short duration of our 3-min exercise protocol, as previously discussed [39,41,42].
There are some limitations in our study. First, we did not assess PSI, even though it has been indicated as a primary mechanism responsible for spinal changes in spinal excitability [42,49,54]. Therefore, it is necessary to conduct further experiments to examine the potential implication of PSI, which may explain the different acute responses in spinal excitability between healthy individuals and MS patients after the NMES intervention of the present study. Second, it could be hypothesized that a longer training protocol may be needed to observe changes in the H-reflex amplitude in pwMS after passive or superimposed NMES. Indeed, MS induces an alteration in some CNS structures and mechanisms that are mainly involved in the modulation of the spinal reflex. Therefore, our 3-min training protocol, which involved 15 intermittent isometric contractions at 20% of MVIC with NMES, may not be long enough to induce significant acute modulation of spinal circuitry function in MS patients compared to healthy individuals. However, with longer intervention protocols the effect of muscle fatigue on H-reflex responses should be considered since muscle fatigue affects H-reflex by reducing excitation of Ia-afferents or increasing excitability threshold of nerve fibers [84]. In this regard, our study revealed that MVIC baseline values did not decrease following the three experimental conditions in both CG and MSp, suggesting that fatigue did not arise at the end of the entire protocol and, therefore, H-reflex responses were not affected by muscle fatigue [39,49,54].
5. Conclusions
The present study demonstrated that MS patients and healthy individuals had different acute modulations of soleus H-reflex responses after passive and superimposed NMES. While healthy participants showed an acute potentiation of the H-reflex after NMES+ and an attenuation after pNMES, MS patients did not show any changes in the H-reflex amplitudes after both NMES+ and pNMES. This result could be explained by an alteration in the control of some presynaptic mechanisms, involving PSI and GABA release, which are compromised in MS as well as by spinal cord abnormalities that could alter the modulation of spinal reflex pathway. Moreover, in both MS patients and healthy individuals, the lack of H-reflex responses after ISO indicates that voluntary isometric contractions do not acutely affects spinal excitability compared to pNMES and NMES+. Of practical importance, in MS patients this result suggests that NMES acts similarly to voluntary isometric exercise and does not affect spinal excitability. Future studies are warranted to explore specific spinal, and potentially supraspinal, adaptations related to NMES interventions in MS.
Author Contributions
Conceptualization, M.S., R.B. and A.M.; Data curation, M.S., R.B. and M.P.; Formal analysis, M.S. and R.B.; Investigation, M.S., M.P., G.B., F.S., F.M. and E.M.; Methodology, M.S., R.B., M.P., G.B., F.S., F.B., E.M. and A.M.; Project administration, M.S. and A.M.; Resources, M.S., G.B., F.S. and F.M.; Software, R.B.; Supervision, A.M.; Validation, M.S., R.B. and A.M.; Visualization, M.S.; Writing – original draft, M.S., R.B., M.P. and A.M.; Writing – review & editing, M.S., R.B., M.P., G.B., F.S., F.B., E.M. and A.M.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the institutional ethics review board of the University of Rome - Foro Italico” (CAR 96/2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patients to publish this paper.
Data Availability Statement
The raw data supporting the conclusion of this article will be made available by the authors, without undue reservation.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Berer, K.; Krishnamoorthy, G. Microbial View of Central Nervous System Autoimmunity. FEBS Lett 2014, 588, 4207–4213. [Google Scholar] [CrossRef]
- Lane, J.; Ng, H.S.; Poyser, C.; Lucas, R.M.; Tremlett, H. Multiple Sclerosis Incidence: A Systematic Review of Change over Time by Geographical Region. Mult Scler Relat Disord 2022, 63, 103932. [Google Scholar] [CrossRef]
- Milo, R.; Kahana, E. Multiple Sclerosis: Geoepidemiology, Genetics and the Environment. Autoimmun Rev 2010, 9, A387–A394. [Google Scholar] [CrossRef]
- Bjartmar, C.; Trapp, B.D. Axonal and Neuronal Degeneration in Multiple Sclerosis: Mechanisms and Functional Consequences. Curr Opin Neurol 2001, 14, 271–278. [Google Scholar] [CrossRef]
- Coles, A.J.; Cox, A.; Le Page, E.; Jones, J.; Trip, S.A.; Deans, J.; Seaman, S.; Miller, D.H.; Hale, G.; Waldmann, H.; et al. The Window of Therapeutic Opportunity in Multiple Sclerosis: Evidence from Monoclonal Antibody Therapy. J Neurol 2006, 253, 98–108. [Google Scholar] [CrossRef]
- Rizzo, M.A.; Hadjimichael, O.C.; Preiningerova, J.; Vollmer, T.L. Prevalence and Treatment of Spasticity Reported by Multiple Sclerosis Patients. Multiple Sclerosis 2004, 10, 589–595. [Google Scholar] [CrossRef]
- Benito-León, J.; Manuel Morales, J.; Rivera-Navarro, J.; Mitchell, A.J. A Review about the Impact of Multiple Sclerosis on Health-Related Quality of Life. Disabil Rehabil 2003, 25, 1291–1303. [Google Scholar] [CrossRef] [PubMed]
- Motl, R.W.; McAuley, E. Symptom Cluster and Quality of Life: Preliminary Evidence in Multiple Sclerosis. J Neurosci Nurs 2010, 42, 212–216. [Google Scholar] [CrossRef] [PubMed]
- Dalgas, U.; Stenager, E.; Ingemann-Hansen, T. Review: Multiple Sclerosis and Physical Exercise: Recommendations for the Application of Resistance-, Endurance- and Combined Training. Multiple Sclerosis Journal 2008, 14, 35–53. [Google Scholar] [CrossRef]
- Motl, R.W.; Arnett, P.A.; Smith, M.M.; Barwick, F.H.; Ahlstrom, B.; Stover, E.J. Worsening of Symptoms Is Associated with Lower Physical Activity Levels in Individuals with Multiple Sclerosis. Multiple Sclerosis 2008, 14, 140–142. [Google Scholar] [CrossRef] [PubMed]
- Latimer-Cheung, A.E.; Martin Ginis, K.A.; Hicks, A.L.; Motl, R.W.; Pilutti, L.A.; Duggan, M.; Wheeler, G.; Persad, R.; Smith, K.M. Development of Evidence-Informed Physical Activity Guidelines for Adults With Multiple Sclerosis. Arch Phys Med Rehabil 2013, 94, 1829–1836.e7. [Google Scholar] [CrossRef] [PubMed]
- Pearson, M.; Dieberg, G.; Smart, N. Exercise as a Therapy for Improvement of Walking Ability in Adults With Multiple Sclerosis: A Meta-Analysis. Arch Phys Med Rehabil 2015, 96, 1339–1348.e7. [Google Scholar] [CrossRef] [PubMed]
- Latimer-Cheung, A.E.; Pilutti, L.A.; Hicks, A.L.; Martin Ginis, K.A.; Fenuta, A.M.; MacKibbon, K.A.; Motl, R.W. Effects of Exercise Training on Fitness, Mobility, Fatigue, and Health-Related Quality of Life Among Adults With Multiple Sclerosis: A Systematic Review to Inform Guideline Development. Arch Phys Med Rehabil 2013, 94, 1800–1828.e3. [Google Scholar] [CrossRef]
- Gunn, H.; Markevics, S.; Haas, B.; Marsden, J.; Freeman, J. Systematic Review: The Effectiveness of Interventions to Reduce Falls and Improve Balance in Adults With Multiple Sclerosis. Arch Phys Med Rehabil 2015, 96, 1898–1912. [Google Scholar] [CrossRef]
- Pilutti, L.A.; Dlugonski, D.; Sandroff, B.M.; Klaren, R.; Motl, R.W. Randomized Controlled Trial of a Behavioral Intervention Targeting Symptoms and Physical Activity in Multiple Sclerosis. Multiple Sclerosis Journal 2014, 20, 594–601. [Google Scholar] [CrossRef]
- Kuspinar, A.; Rodriguez, A.M.; Mayo, N.E. The Effects of Clinical Interventions on Health-Related Quality of Life in Multiple Sclerosis: A Meta-Analysis. Multiple Sclerosis Journal 2012, 18, 1686–1704. [Google Scholar] [CrossRef]
- Dalgas, U.; Stenager, E.; Sloth, M.; Stenager, E. The Effect of Exercise on Depressive Symptoms in Multiple Sclerosis Based on a Meta-analysis and Critical Review of the Literature. Eur J Neurol 2015, 22, 443. [Google Scholar] [CrossRef]
- Charron, S.; McKay, K.A.; Tremlett, H. Physical Activity and Disability Outcomes in Multiple Sclerosis: A Systematic Review (2011–2016). Mult Scler Relat Disord 2018, 20, 169–177. [Google Scholar] [CrossRef]
- Edwards, T.; Pilutti, L.A. The Effect of Exercise Training in Adults with Multiple Sclerosis with Severe Mobility Disability: A Systematic Review and Future Research Directions. Mult Scler Relat Disord 2017, 16, 31–39. [Google Scholar] [CrossRef]
- Motl, R.W.; McAuley, E.; Snook, E.M. Physical Activity and Multiple Sclerosis: A Meta-Analysis. Multiple Sclerosis 2005, 11, 459–463. [Google Scholar] [CrossRef] [PubMed]
- Marrie, R.A.; Horwitz, R.; Cutter, G.; Tyry, T.; Campagnolo, D.; Vollmer, T. High Frequency of Adverse Health Behaviors in Multiple Sclerosis. Multiple Sclerosis 2009, 15, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Beckerman, H.; De Groot, V.; Scholten, M.A.; Kempen, J.C.E.; Lankhorst, G.J. Physical Activity Behavior of People with Multiple Sclerosis: Understanding How They Can Become More Physically Active. Phys Ther 2010, 90, 1001–1013. [Google Scholar] [CrossRef] [PubMed]
- Silveira, S.L.; Jeng, B.; Cutter, G.; Motl, R.W. Perceptions of Physical Activity Guidelines among Wheelchair Users with Multiple Sclerosis. Mult Scler J Exp Transl Clin 2022, 8. [Google Scholar] [CrossRef]
- Wahls, T.L.; Reese, D.; Kaplan, D.; Darling, W.G. Rehabilitation with Neuromuscular Electrical Stimulation Leads to Functional Gains in Ambulation in Patients with Secondary Progressive and Primary Progressive Multiple Sclerosis: A Case Series Report. Journal of Alternative and Complementary Medicine 2010, 16, 1343–1349. [Google Scholar] [CrossRef]
- Maffiuletti, N.A. Physiological and Methodological Considerations for the Use of Neuromuscular Electrical Stimulation. Eur J Appl Physiol 2010, 110, 223–234. [Google Scholar] [CrossRef] [PubMed]
- Botter, A.; Oprandi, G.; Lanfranco, F.; Allasia, S.; Maffiuletti, N.A.; Minetto, M.A. Atlas of the Muscle Motor Points for the Lower Limb: Implications for Electrical Stimulation Procedures and Electrode Positioning. Eur J Appl Physiol 2011, 111, 2461–2471. [Google Scholar] [CrossRef]
- Bickel, C.S.; Gregory, C.M.; Dean, J.C. Motor Unit Recruitment during Neuromuscular Electrical Stimulation: A Critical Appraisal. Eur J Appl Physiol 2011, 111, 2399–2407. [Google Scholar] [CrossRef]
- Fuentes, J.P.; Armijo Olivo, S.; Magee, D.J.; Gross, D.P. Effectiveness of Interferential Current Therapy in the Management of Musculoskeletal Pain: A Systematic Review and Meta-Analysis. Phys Ther 2010, 90, 1219–1238. [Google Scholar] [CrossRef]
- Paillard, T.; Noé, F.; Passelergue, P.; Dupui, P. Electrical Stimulation Superimposed onto Voluntary Muscular Contraction. Sports Med 2005, 35, 951–966. [Google Scholar] [CrossRef]
- Houghton, P.E.; Campbell, K.E.; Fraser, C.H.; Harris, C.; Keast, D.H.; Potter, P.J.; Hayes, K.C.; Woodbury, M.G. Electrical Stimulation Therapy Increases Rate of Healing of Pressure Ulcers in Community-Dwelling People With Spinal Cord Injury. Arch Phys Med Rehabil 2010, 91, 669–678. [Google Scholar] [CrossRef]
- Kimberley, T.J.; Lewis, S.M.; Auerbach, E.J.; Dorsey, L.L.; Lojovich, J.M.; Carey, J.R. Electrical Stimulation Driving Functional Improvements and Cortical Changes in Subjects with Stroke. Exp Brain Res 2004, 154, 450–460. [Google Scholar] [CrossRef] [PubMed]
- Adams, G.R.; Harris, R.T.; Woodard, D.; Dudley, G.A. Mapping of Electrical Muscle Stimulation Using MRI. J Appl Physiol (1985) 1993, 74, 532–537. [Google Scholar] [CrossRef] [PubMed]
- Bergquist, A.J.; Clair, J.M.; Lagerquist, O.; Mang, C.S.; Okuma, Y.; Collins, D.F. Neuromuscular Electrical Stimulation: Implications of the Electrically Evoked Sensory Volley. Eur J Appl Physiol 2011, 111, 2409–2426. [Google Scholar] [CrossRef] [PubMed]
- Ratchford, J.N.; Shore, W.; Hammond, E.R.; Rose, J.G.; Rifkin, R.; Nie, P.; Tan, K.; Quigg, M.E.; De Lateur, B.J.; Kerr, D.A. A Pilot Study of Functional Electrical Stimulation Cycling in Progressive Multiple Sclerosis. NeuroRehabilitation 2010, 27, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Fornusek, C.; Hoang, P. Neuromuscular Electrical Stimulation Cycling Exercise for Persons with Advanced Multiple Sclerosis. J Rehabil Med 2014, 46, 698–702. [Google Scholar] [CrossRef]
- Almuklass, A.M.; Davis, L.; Hamilton, L.D.; Hebert, J.R.; Alvarez, E.; Enoka, R.M. Pulse Width Does Not Influence the Gains Achieved With Neuromuscular Electrical Stimulation in People With Multiple Sclerosis: Double-Blind, Randomized Trial. Neurorehabil Neural Repair 2018, 32, 84–93. [Google Scholar] [CrossRef] [PubMed]
- Broekmans, T.; Roelants, M.; Feys, P.; Alders, G.; Gijbels, D.; Hanssen, I.; Stinissen, P.; Eijnde, B.O. Effects of Long-Term Resistance Training and Simultaneous Electro-Stimulation on Muscle Strength and Functional Mobility in Multiple Sclerosis. Multiple Sclerosis Journal 2011, 17, 468–477. [Google Scholar] [CrossRef] [PubMed]
- Coote, S.; Hughes, L.; Rainsford, G.; Minogue, C.; Donnelly, A. Pilot Randomized Trial of Progressive Resistance Exercise Augmented by Neuromuscular Electrical Stimulation for People with Multiple Sclerosis Who Use Walking Aids. Arch Phys Med Rehabil 2015, 96, 197–204. [Google Scholar] [CrossRef]
- Borzuola, R.; Labanca, L.; Macaluso, A.; Laudani, L. Modulation of Spinal Excitability Following Neuromuscular Electrical Stimulation Superimposed to Voluntary Contraction. Eur J Appl Physiol 2020, 120, 2105–2113. [Google Scholar] [CrossRef]
- Borzuola, R.; Quinzi, F.; Scalia, M.; Pitzalis, S.; Di Russo, F.; MacAluso, A. Acute Effects of Neuromuscular Electrical Stimulation on Cortical Dynamics and Reflex Activation. J Neurophysiol 2023, 129, 1310–1321. [Google Scholar] [CrossRef]
- Scalia, M.; Parrella, M.; Borzuola, R.; Macaluso, A. Comparison of Acute Responses in Spinal Excitability between Older and Young People after Neuromuscular Electrical Stimulation. Eur J Appl Physiol 2023. [Google Scholar] [CrossRef]
- Lagerquist, O.; Mang, C.S.; Collins, D.F. Changes in Spinal but Not Cortical Excitability Following Combined Electrical Stimulation of the Tibial Nerve and Voluntary Plantar-Flexion. Exp Brain Res 2012, 222, 41–53. [Google Scholar] [CrossRef]
- Milosevic, M.; Masugi, Y.; Obata, H.; Sasaki, A.; Popovic, M.R.; Nakazawa, K. Short-Term Inhibition of Spinal Reflexes in Multiple Lower Limb Muscles after Neuromuscular Electrical Stimulation of Ankle Plantar Flexors. Exp Brain Res 2019, 237, 467–476. [Google Scholar] [CrossRef] [PubMed]
- Laudani, L.; Mira, J.; Carlucci, F.; Orlando, G.; Menotti, F.; Sacchetti, M.; Giombini, A.; Pigozzi, F.; Macaluso, A. Whole Body Vibration of Different Frequencies Inhibits H-Reflex but Does Not Affect Voluntary Activation. Hum Mov Sci 2018, 62, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Jimenez, S.; Mordillo-Mateos, L.; Dileone, M.; Campolo, M.; Carrasco-Lopez, C.; Moitinho-Ferreira, F.; Gallego-Izquierdo, T.; Siebner, H.R.; Valls-Solé, J.; Aguilar, J.; et al. Effects of Patterned Peripheral Nerve Stimulation on Soleus Spinal Motor Neuron Excitability. PLoS One 2018, 13. [Google Scholar] [CrossRef]
- Kato, T.; Sasaki, A.; Yokoyama, H.; Milosevic, M.; Nakazawa, K. Effects of Neuromuscular Electrical Stimulation and Voluntary Commands on the Spinal Reflex Excitability of Remote Limb Muscles. Exp Brain Res 2019, 237, 3195–3205. [Google Scholar] [CrossRef]
- Wegrzyk, J.; Fouré, A.; Vilmen, C.; Ghattas, B.; Maffiuletti, N.A.; Mattei, J.P.; Place, N.; Bendahan, D.; Gondin, J. Extra Forces Induced by Wide-Pulse, High-Frequency Electrical Stimulation: Occurrence, Magnitude, Variability and Underlying Mechanisms. Clinical Neurophysiology 2015, 126, 1400–1412. [Google Scholar] [CrossRef] [PubMed]
- Gueugneau, N.; Grosprêtre, S.; Stapley, P.; Lepers, R. High-Frequency Neuromuscular Electrical Stimulation Modulates Interhemispheric Inhibition in Healthy Humans. J Neurophysiol 2017, 117, 467–475. [Google Scholar] [CrossRef]
- Grosprêtre, S.; Gueugneau, N.; Martin, A.; Lepers, R. Presynaptic Inhibition Mechanisms May Subserve the Spinal Excitability Modulation Induced by Neuromuscular Electrical Stimulation. Journal of Electromyography and Kinesiology 2018, 40, 95–101. [Google Scholar] [CrossRef]
- Pierrot-Deseilligny, E.; Mazevet, D. The Monosynaptic Reflex: A Tool to Investigate Motor Control in Humans. Interest and Limits. Neurophysiol Clin 2000, 30, 67–80. [Google Scholar] [CrossRef]
- Hoque, M.; Borich, M.; Sabatier, M.; Backus, D.; Kesar, T. Effects of Downslope Walking on Soleus H-Reflexes and Walking Function in Individuals with Multiple Sclerosis: A Preliminary Study. NeuroRehabilitation 2019, 44, 587–597. [Google Scholar] [CrossRef]
- Borzuola, R.; Nuccio, S.; Scalia, M.; Parrella, M.; Del Vecchio, A.; Bazzucchi, I.; Felici, F.; Macaluso, A. Adjustments in the Motor Unit Discharge Behavior Following Neuromuscular Electrical Stimulation Compared to Voluntary Contractions. Front Physiol 2023, 14. [Google Scholar] [CrossRef]
- SENIAM. Available online: http://seniam.org/ (accessed on 30 November 2023).
- Zehr, E.P. Considerations for Use of the Hoffmann Reflex in Exercise Studies. Eur J Appl Physiol 2002, 86, 455–468. [Google Scholar] [CrossRef]
- Stein, R.B.; Estabrooks, K.L.; McGie, S.; Roth, M.J.; Jones, K.E. Quantifying the Effects of Voluntary Contraction and Inter-Stimulus Interval on the Human Soleus H-Reflex. Exp Brain Res 2007, 182, 309–319. [Google Scholar] [CrossRef] [PubMed]
- Morita, H.; Crone, C.; Christenhuis, D.; Petersen, N.T.; Nielsen, J.B. Modulation of Presynaptic Inhibition and Disynaptic Reciprocal Ia Inhibition during Voluntary Movement in Spasticity. Brain 2001, 124, 826–837. [Google Scholar] [CrossRef] [PubMed]
- Wiest, M.J.; Bergquist, A.J.; Collins, D.F. Torque, Current, and Discomfort During 3 Types of Neuromuscular Electrical Stimulation of Tibialis Anterior. Phys Ther 2017, 97, 790–789. [Google Scholar] [CrossRef] [PubMed]
- Gondin, J.; Giannesini, B.; Vilmen, C.; Dalmasso, C.; Le Fur, Y.; Cozzone, P.J.; Bendahan, D. Effects of Stimulation Frequency and Pulse Duration on Fatigue and Metabolic Cost during a Single Bout of Neuromuscular Electrical Stimulation. Muscle Nerve 2010, 41, 667–678. [Google Scholar] [CrossRef] [PubMed]
- Holmback, A.M.; Porter, M.M.; Downham, D.; Andersen, J.L.; Lexell, J.; Ck, H.; Maria, A. Structure and Function of the Ankle Dorsiflexor Muscles in Young and Moderately Active Men and Women. J Appl Physiol 2003, 95, 2416–2424. [Google Scholar] [CrossRef] [PubMed]
- Pinar, S.; Kitano, K.; Koceja, D.M. Role of Vision and Task Complexity on Soleus H-Reflex Gain. Journal of Electromyography and Kinesiology 2010, 20, 354–358. [Google Scholar] [CrossRef] [PubMed]
- Baudry, S.; Maerz, A.H.; Enoka, R.M. Presynaptic Modulation of Ia Afferents in Young and Old Adults When Performing Force and Position Control. J Neurophysiol 2010, 103, 623–631. [Google Scholar] [CrossRef] [PubMed]
- Koceja, D.M.; Markus, C.A.; Trimble, M.H. Postural Modulation of the Soleus H Reflex in Young and Old Subjects. Electroencephalogr Clin Neurophysiol 1995, 97, 387–393. [Google Scholar] [CrossRef]
- Koceja, D.M.; Mynark, R.G. Comparison of Heteronymous Monosynaptic Ia Facilitation in Young and Elderly Subjects in Supine and Standing Positions. Int J Neurosci 2000, 103, 1–17. [Google Scholar] [CrossRef]
- Morita, H.; Shindo, M.; Yanagawa, S.; Yoshida, T.; Momoi, H.; Yanagisawa, N. Progressive Decrease in Heteronymous Monosynaptic Ia Facilitation with Human Ageing. Exp Brain Res 1995, 104, 167–170. [Google Scholar] [CrossRef]
- Papegaaij, S.; Taube, W.; Baudry, S.; Otten, E.; Hortobágyi, T. Aging Causes a Reorganization of Cortical and Spinal Control of Posture. Front Aging Neurosci 2014, 6. [Google Scholar] [CrossRef]
- Baudry, S.; Penzer, F.; Duchateau, J. Input-Output Characteristics of Soleus Homonymous Ia Afferents and Corticospinal Pathways during Upright Standing Differ between Young and Elderly Adults. Acta Physiologica 2014, 210, 667–677. [Google Scholar] [CrossRef]
- Huang, C.Y.; Wang, C.H.; Hwang, I.S. Characterization of the Mechanical and Neural Components of Spastic Hypertonia with Modified H Reflex. Journal of Electromyography and Kinesiology 2006, 16, 384–391. [Google Scholar] [CrossRef]
- Wang, Y.; Pillai, S.; Wolpaw, J.R.; Chen, X.Y. H-Reflex down-Conditioning Greatly Increases the Number of Identifiable GABAergic Interneurons in Rat Ventral Horn. Neurosci Lett 2009, 452, 124–129. [Google Scholar] [CrossRef]
- Mandolesi, G.; Gentile, A.; Musella, A.; Fresegna, D.; De Vito, F.; Bullitta, S.; Sepman, H.; Marfia, G.A.; Centonze, D. Synaptopathy Connects Inflammation and Neurodegeneration in Multiple Sclerosis. Nat Rev Neurol 2015, 11, 711–724. [Google Scholar] [CrossRef]
- Huiskamp, M.; Yaqub, M.; van Lingen, M.R.; Pouwels, P.J.W.; de Ruiter, L.R.J.; Killestein, J.; Schwarte, L.A.; Golla, S.S.V.; van Berckel, B.N.M.; Boellaard, R.; et al. Cognitive Performance in Multiple Sclerosis: What Is the Role of the Gamma-Aminobutyric Acid System? Brain Commun 2023, 5. [Google Scholar] [CrossRef]
- Isaacson, J.S.; Scanziani, M. How Inhibition Shapes Cortical Activity. Neuron 2011, 72, 231–243. [Google Scholar] [CrossRef]
- Kim, R.; Sejnowski, T.J. Strong Inhibitory Signaling Underlies Stable Temporal Dynamics and Working Memory in Spiking Neural Networks. Nat Neurosci 2021, 24, 129–139. [Google Scholar] [CrossRef]
- Eden, D.; Gros, C.; Badji, A.; Dupont, S.M.; De Leener, B.; Maranzano, J.; Zhuoquiong, R.; Liu, Y.; Granberg, T.; Ouellette, R.; et al. Spatial Distribution of Multiple Sclerosis Lesions in the Cervical Spinal Cord. Brain 2019, 142, 633–646. [Google Scholar] [CrossRef]
- Lycklama, G.; Thompson, A.; Filippi, M.; Miller, D.; Polman, C.; Fazekas, F.; Barkhof, F. Spinal-Cord MRI in Multiple Sclerosis. Lancet Neurol 2003, 2, 555–562. [Google Scholar] [CrossRef]
- Petrova, N.; Nutma, E.; Carassiti, D.; RS Newman, J.; Amor, S.; Altmann, D.R.; Baker, D.; Schmierer, K. Synaptic Loss in Multiple Sclerosis Spinal Cord. Ann Neurol 2020, 88, 619–625. [Google Scholar] [CrossRef]
- Friese, M.A. Widespread Synaptic Loss in Multiple Sclerosis. Brain 2016, 139, 2–4. [Google Scholar] [CrossRef]
- Petrova, N.; Carassiti, D.; Altmann, D.R.; Baker, D.; Schmierer, K. Axonal Loss in the Multiple Sclerosis Spinal Cord Revisited. Brain Pathology 2018, 28, 334–348. [Google Scholar] [CrossRef]
- DeLuca, G.C.; Ebers, G.C.; Esiri, M.M. Axonal Loss in Multiple Sclerosis: A Pathological Survey of the Corticospinal and Sensory Tracts. Brain 2004, 127, 1009–1018. [Google Scholar] [CrossRef]
- Sinkjaer, T.; Toft, E.; Hansen, H.J. H-Reflex Modulation during Gait in Multiple Sclerosis Patients with Spasticity. Acta Neurol Scand 1995, 91, 239–246. [Google Scholar] [CrossRef]
- Sosnoff, J.J.; Motl, R.W. Effect of Acute Unloaded Arm versus Leg Cycling Exercise on the Soleus H-Reflex in Adults with Multiple Sclerosis. Neurosci Lett 2010, 479, 307–311. [Google Scholar] [CrossRef]
- Sosnoff, J.J.; Shin, S.; Motl, R.W. Multiple Sclerosis and Postural Control: The Role of Spasticity. Arch Phys Med Rehabil 2010, 91, 93–99. [Google Scholar] [CrossRef]
- Motl, R.W.; Snook, E.M.; Hinkle, M.L.; McAuley, E. Effect of Acute Leg Cycling on the Soleus H-Reflex and Modified Ashworth Scale Scores in Individuals with Multiple Sclerosis. Neurosci Lett 2006, 406, 289–292. [Google Scholar] [CrossRef] [PubMed]
- Cantrell, G.S.; Lantis, D.J.; Bemben, M.G.; Black, C.D.; Larson, D.J.; Pardo, G.; Fjeldstad-Pardo, C.; Larson, R.D. Relationship between Soleus H-Reflex Asymmetry and Postural Control in Multiple Sclerosis. Disabil Rehabil 2022, 44, 542–548. [Google Scholar] [CrossRef] [PubMed]
- Sammali, F.; Xu, L.; Rabotti, C.; Cardinale, M.; Xu, Y.; van Dijk, J.P.; Zwarts, M.J.; Del Prete, Z.; Mischi, M. Effects of Vibration-Induced Fatigue on the H-Reflex. Journal of Electromyography and Kinesiology 2018, 39, 134–141. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Participant’s position. Participant’s position on the dynamometer chair during the MVIC, the H-reflex recruitment curve and the three experimental conditions (pNMES, NMES+, ISO).
Figure 1.
Participant’s position. Participant’s position on the dynamometer chair during the MVIC, the H-reflex recruitment curve and the three experimental conditions (pNMES, NMES+, ISO).

Figure 2.
Electrodes positioning. The neuromuscular stimulator active wireless electrodes (white pods) are placed in a bipolar configuration on the soleus, gastrocnemius medialis and gastrocnemius lateralis muscles. sEMG electrodes are placed on the Soleus muscle and the reference electrode on the lateral malleolus. The electrode of the H-reflex stimulation is positioned on the posterior tibial nerve.
Figure 2.
Electrodes positioning. The neuromuscular stimulator active wireless electrodes (white pods) are placed in a bipolar configuration on the soleus, gastrocnemius medialis and gastrocnemius lateralis muscles. sEMG electrodes are placed on the Soleus muscle and the reference electrode on the lateral malleolus. The electrode of the H-reflex stimulation is positioned on the posterior tibial nerve.
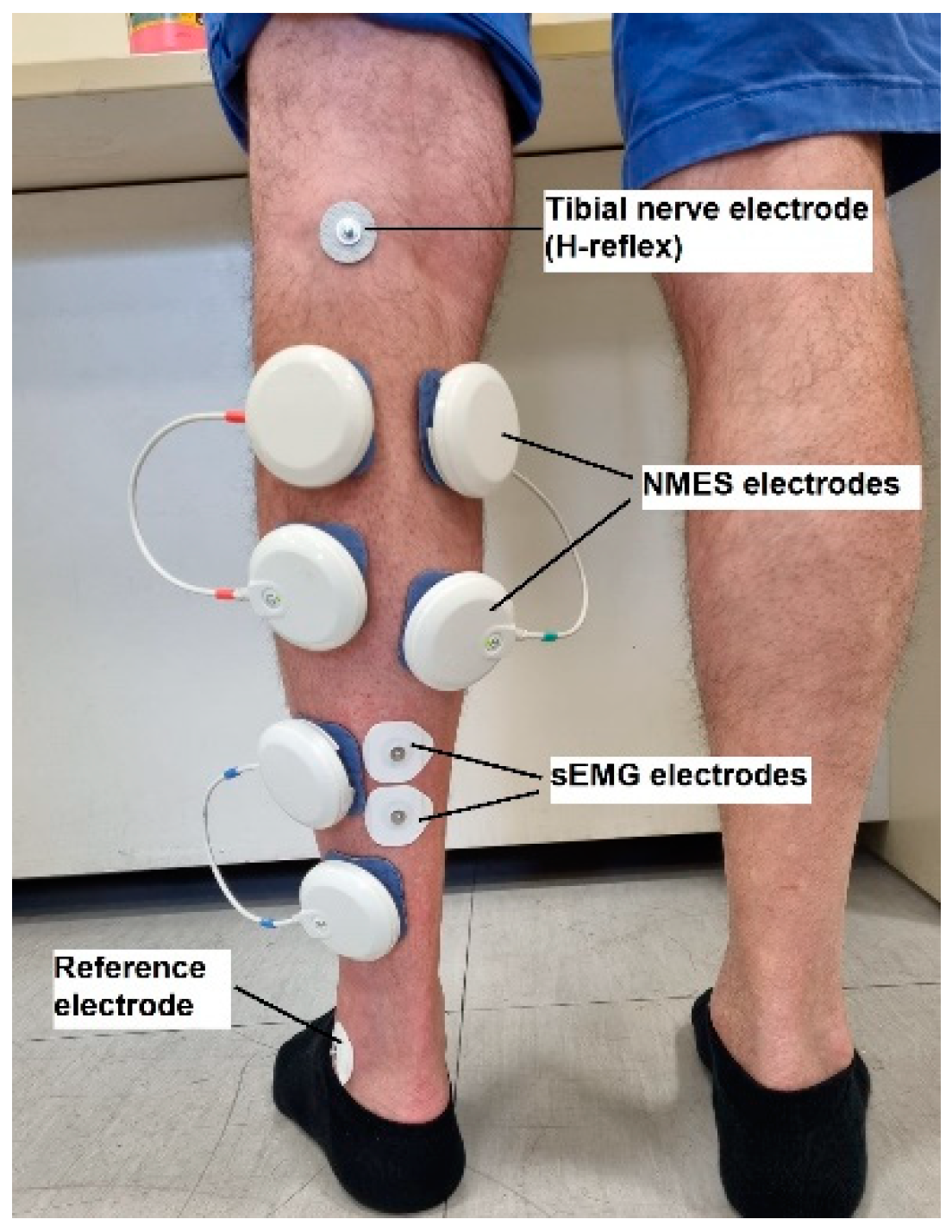
Figure 3.
Participant’s position during the H-reflex assessment. Participant’s prone position on the physiotherapy bed while the investigator located the optimal stimulation site in the popliteal fossa by using a cathode ball electrode to evoke the H-reflex of SOL muscle.
Figure 3.
Participant’s position during the H-reflex assessment. Participant’s prone position on the physiotherapy bed while the investigator located the optimal stimulation site in the popliteal fossa by using a cathode ball electrode to evoke the H-reflex of SOL muscle.
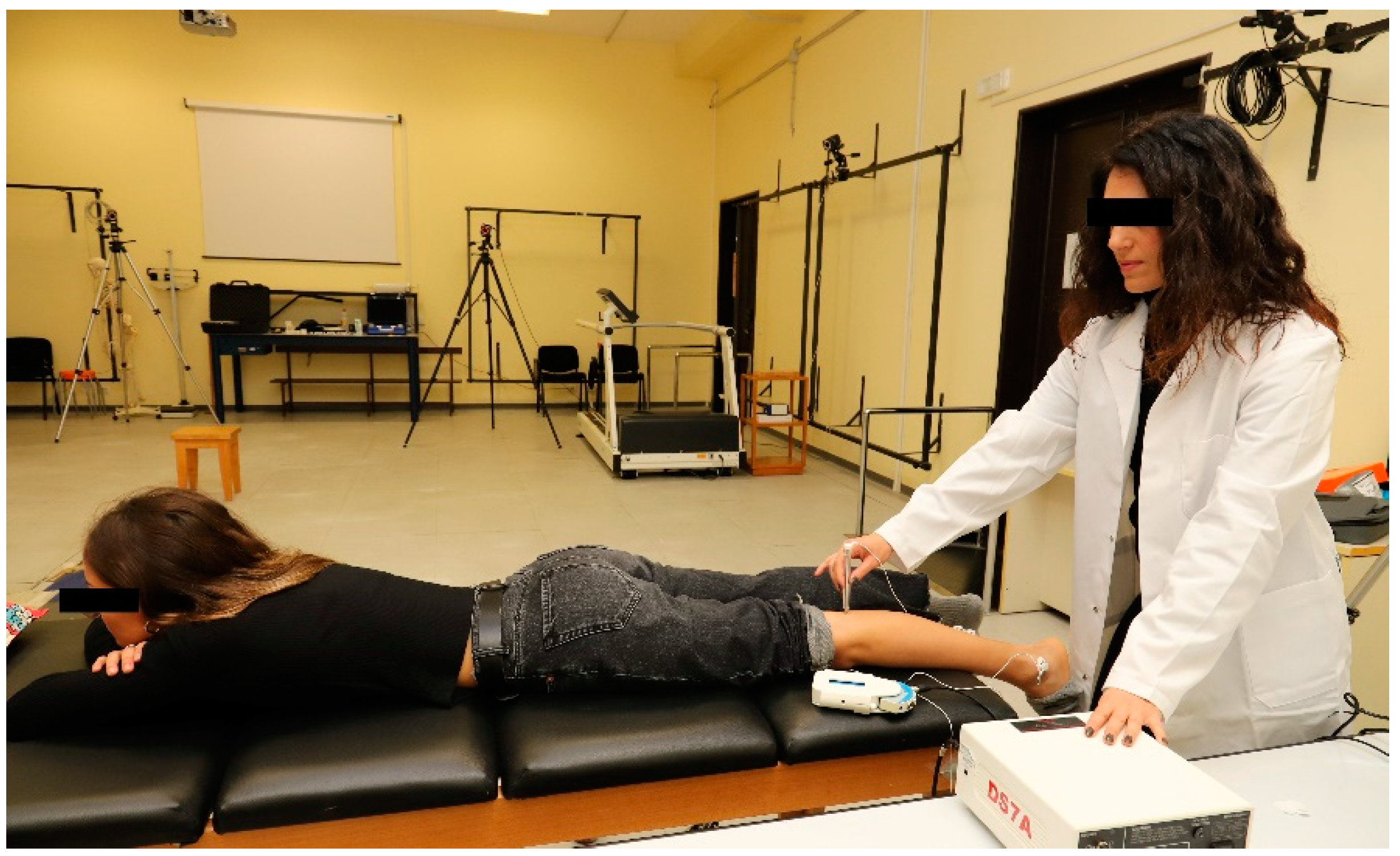
Figure 4.
Test H-reflex selection. Test H-reflex sEMG data (black solid line) with the small M-wave (Mtest) and the corresponding test H-reflex (Htest) (80–85% of Hmax). Maximal H-reflex sEMG data (grey dashed line) with corresponding Hmax.
Figure 4.
Test H-reflex selection. Test H-reflex sEMG data (black solid line) with the small M-wave (Mtest) and the corresponding test H-reflex (Htest) (80–85% of Hmax). Maximal H-reflex sEMG data (grey dashed line) with corresponding Hmax.
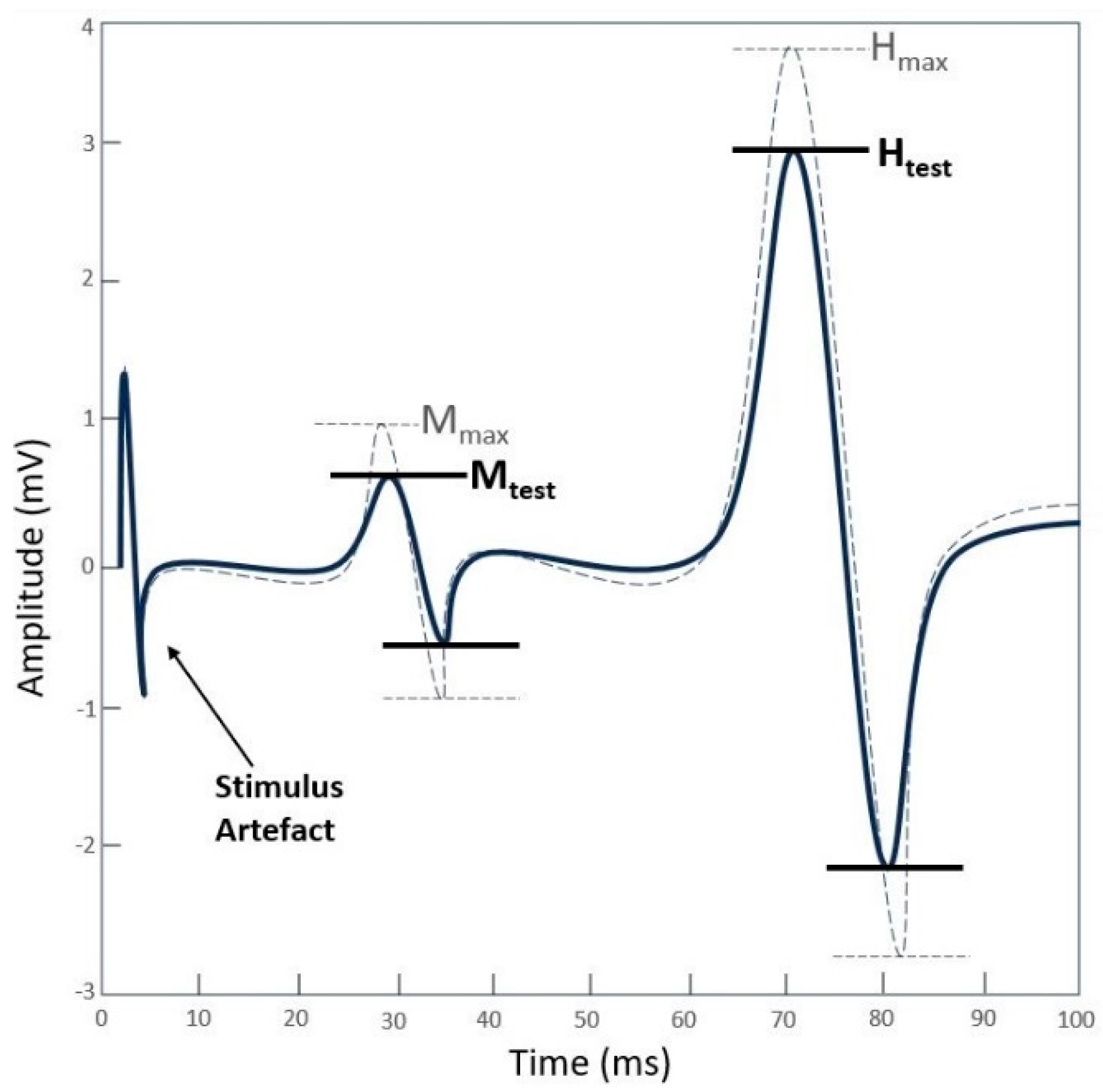
Figure 5.
Diagram of the experimental protocol. Preliminary phase and experimental conditions.
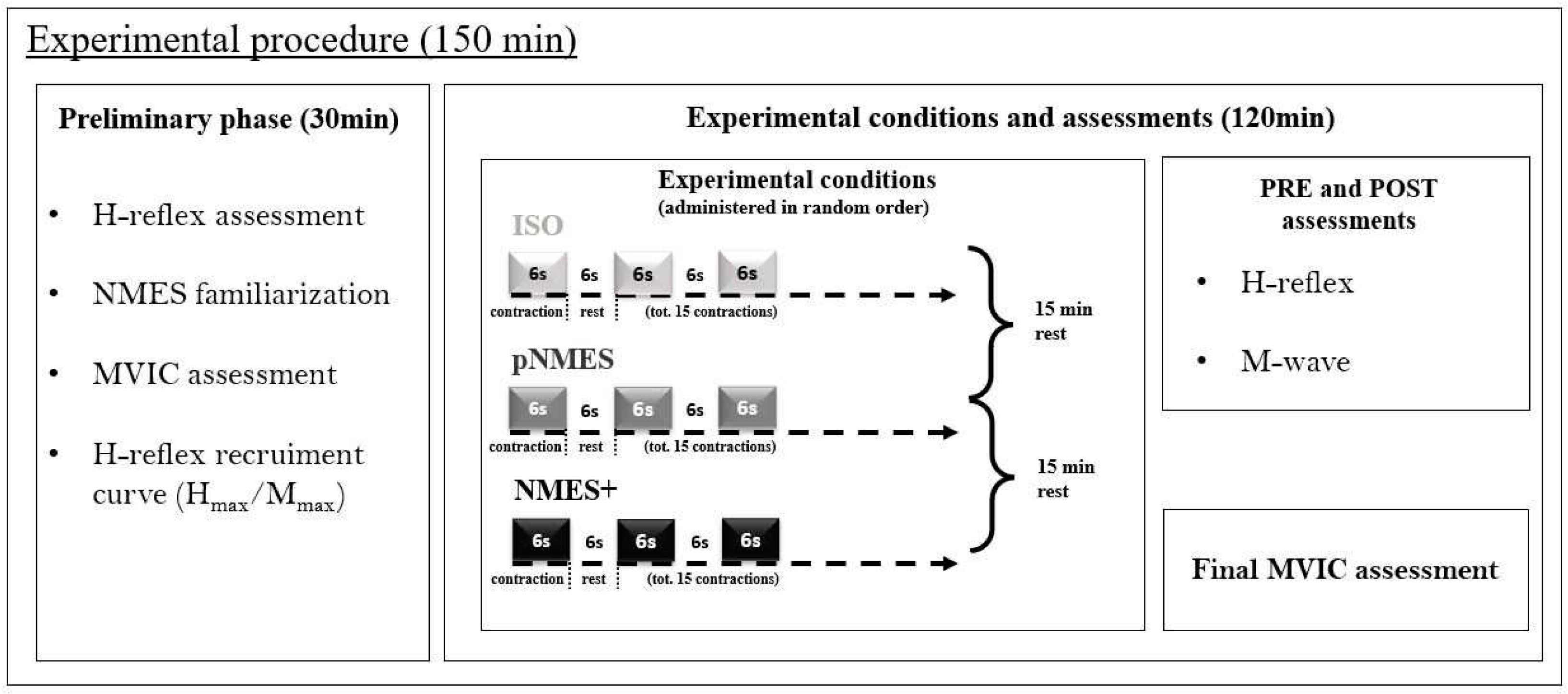
Figure 6.
H-reflex and M-wave before and after the three experimental conditions. (a) The H-reflex and M-wave average sEMG responses of one healthy participant of the CG to a series of 20 electrical stimuli applied to the posterior tibial nerve in the popliteal fossa before (red line) and after (black line) each experimental condition (ISO, pNMES, NMES+). (b) The H-reflex and M-wave average sEMG responses of one MS participant of the MSp to a series of 20 electrical stimuli applied to the posterior tibial nerve in the popliteal fossa before (red line) and after (black line) each experimental condition (ISO, pNMES, NMES+).
Figure 6.
H-reflex and M-wave before and after the three experimental conditions. (a) The H-reflex and M-wave average sEMG responses of one healthy participant of the CG to a series of 20 electrical stimuli applied to the posterior tibial nerve in the popliteal fossa before (red line) and after (black line) each experimental condition (ISO, pNMES, NMES+). (b) The H-reflex and M-wave average sEMG responses of one MS participant of the MSp to a series of 20 electrical stimuli applied to the posterior tibial nerve in the popliteal fossa before (red line) and after (black line) each experimental condition (ISO, pNMES, NMES+).
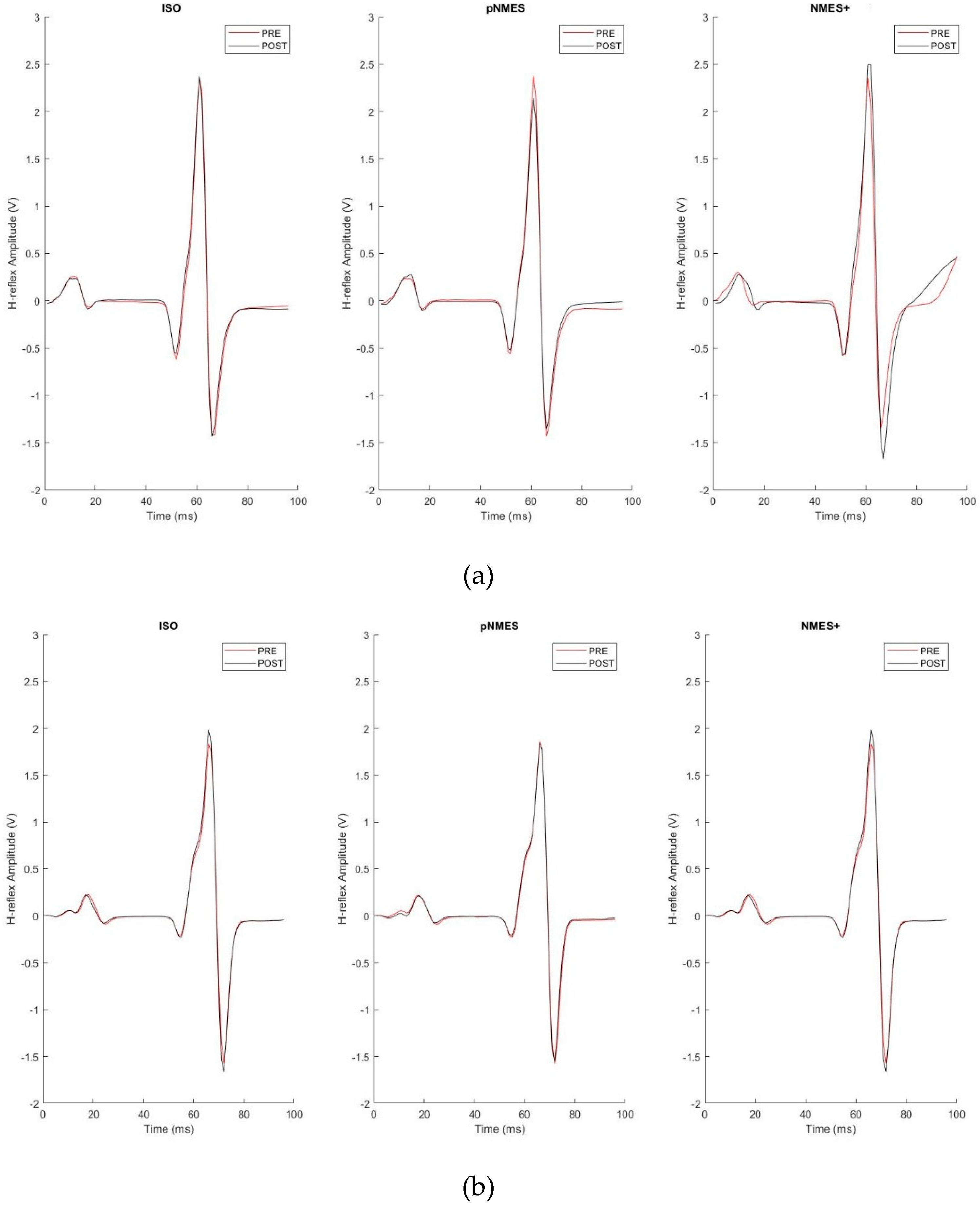
Figure 7.
H-reflex and M-wave normalized by Mmax. (a) Amplitude of soleus H-reflexes and corresponding M-waves normalized to Mmax before (PRE) and after (POST) the three experimental conditions (ISO, pNMES and NMES+), in CG. Data are reported as group means ± standard deviation (*p = 0.010; **p < 0.000). (b) Amplitude of soleus H-reflexes and corresponding M-waves normalized to Mmax before (PRE) and after (POST) the three experimental conditions (ISO, pNMES and NMES+), in MSp. H-reflex and M-wave amplitudes average did not change in ISO, pNMES and NMES+. Data are reported as group means ± standard deviation.
Figure 7.
H-reflex and M-wave normalized by Mmax. (a) Amplitude of soleus H-reflexes and corresponding M-waves normalized to Mmax before (PRE) and after (POST) the three experimental conditions (ISO, pNMES and NMES+), in CG. Data are reported as group means ± standard deviation (*p = 0.010; **p < 0.000). (b) Amplitude of soleus H-reflexes and corresponding M-waves normalized to Mmax before (PRE) and after (POST) the three experimental conditions (ISO, pNMES and NMES+), in MSp. H-reflex and M-wave amplitudes average did not change in ISO, pNMES and NMES+. Data are reported as group means ± standard deviation.
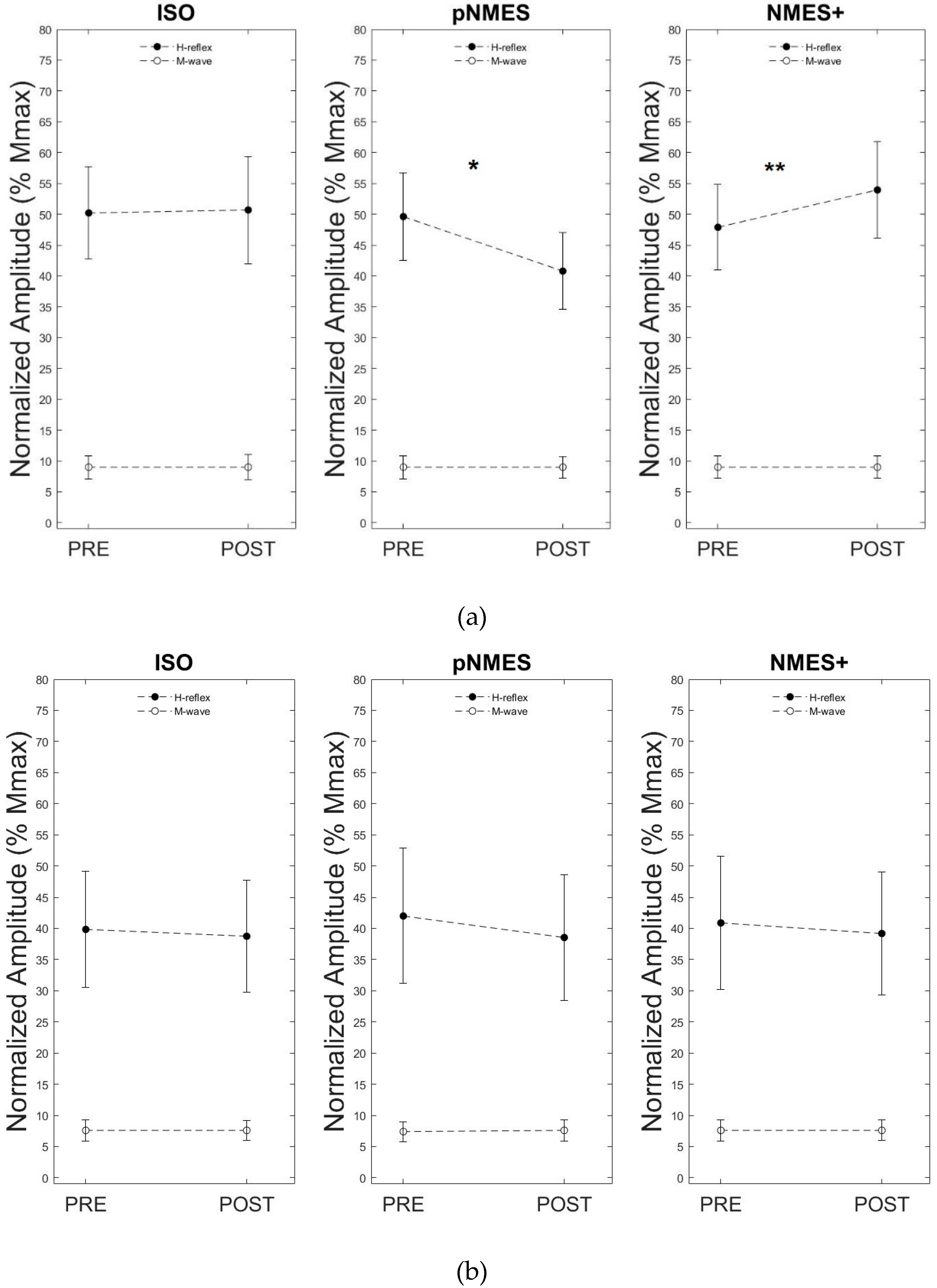
Figure 8.
Hmax/Mmax ratio. MSp and CG showed no differences in the Hmax/Mmax ratio values at rest.
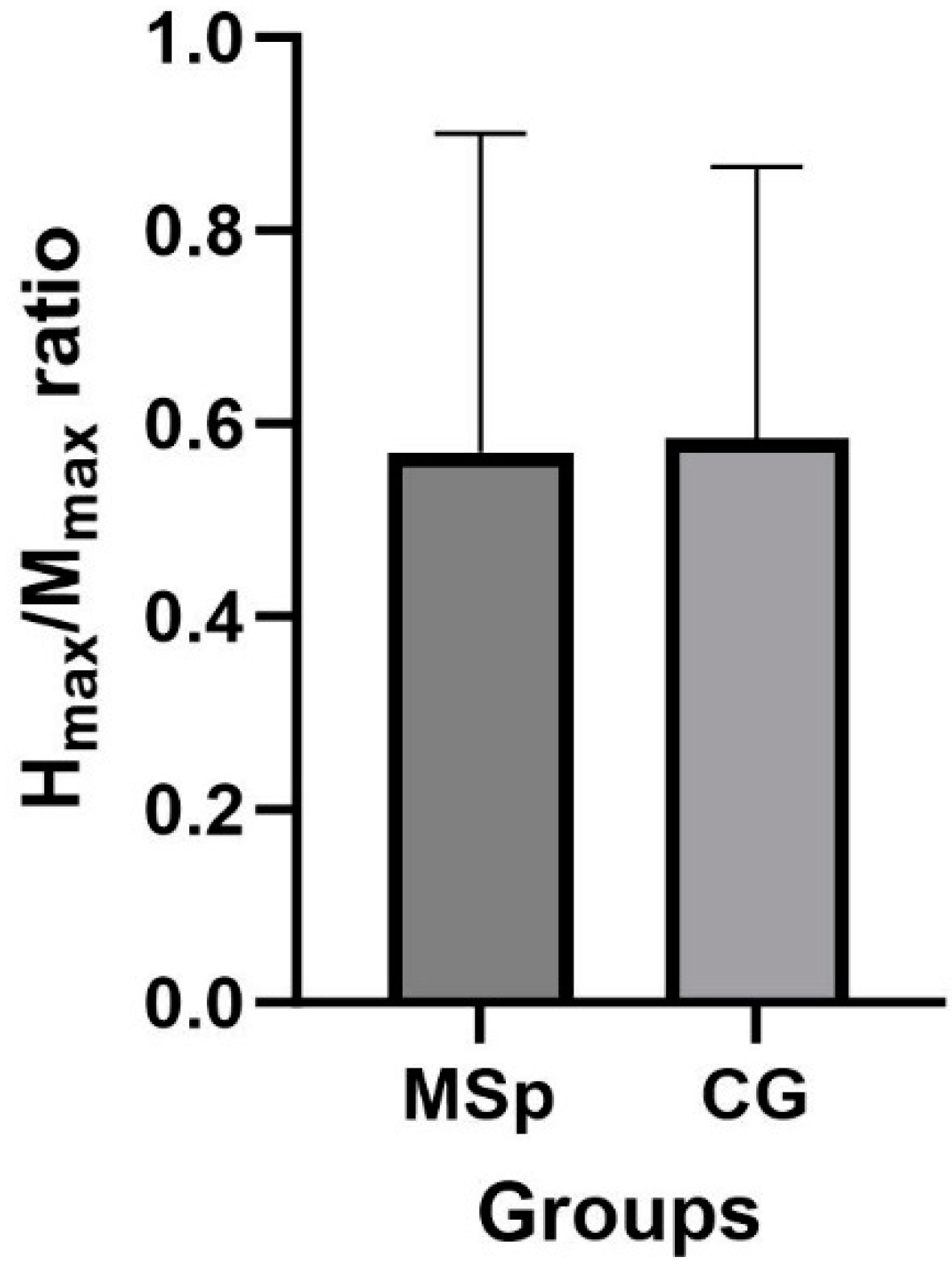

Table 1.
PRE and POST H-reflex values. The amplitudes of the H-reflex before (PRE) and after (POST) all three experimental conditions (ISO, pNMES, NMES+) are reported as a mean ± standard deviation. The corresponding p values of each condition are illustrated in the table. *Significantly different from PRE.
Table 1.
PRE and POST H-reflex values. The amplitudes of the H-reflex before (PRE) and after (POST) all three experimental conditions (ISO, pNMES, NMES+) are reported as a mean ± standard deviation. The corresponding p values of each condition are illustrated in the table. *Significantly different from PRE.
| PRE | POST | p value | ||
|---|---|---|---|---|
| ISO | MSp | 0.39 ± 0.29 | 0.38 ± 0.28 | 0.506 |
| CG | 0.50 ± 0.24 | 0.50 ± 0.27 | 0.829 | |
| pNMES | MSp | 0.42 ± 0.34 | 0.39 ± 0.32 | 0.068 |
| CG | 0.49 ± 0.22 | 0.40 ± 0.20* | 0.000 | |
| NMES+ | MSp | 0.40 ± 0.34 | 0.39 ± 0.31 | 0.126 |
| CG | 0.48 ± 0.22 | 0.54 ± 0.25* | 0.010 |
Table 2.
Maximal voluntary isometric contraction (MVIC) (Nm). Maximal voluntary isometric contraction (MVIC) of the ankle plantar flexor muscles before starting the experimental conditions (Pre-test) and at the end of the entire protocol (Post-test), in MSp and CG. Data are illustrated as group means ± standard deviation.
Table 2.
Maximal voluntary isometric contraction (MVIC) (Nm). Maximal voluntary isometric contraction (MVIC) of the ankle plantar flexor muscles before starting the experimental conditions (Pre-test) and at the end of the entire protocol (Post-test), in MSp and CG. Data are illustrated as group means ± standard deviation.
| Pre-test | Post-test | |
|---|---|---|
| MSp | 43.12 ± 15.1 | 40.86 ± 15.48 |
| CG | 53.43 ± 27.29 | 54.2 ± 26.45 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



