
Submitted:
24 January 2024
Posted:
25 January 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Coronavirus disease 2019 (COVID-19), can manifest with ocular symptoms. These symptoms can be divided into isolated events attributed to COVID-19 and those occurring in multisystem inflammatory syndrome in children (MIS-C), a newly diagnosed disease entity associated with COVID-19 infection. Currently, the literature lacks specific guidelines and treatment regimens for COVID-19 ocular symptoms, especially in children.
Keywords:
panuveitis
; treatment of Covid uveitis
; Depomedrol under Tenon's capsule in the treatment of Covid uveitis
; ophthalmic complications after Covid infection
; COVID-19 thromboembolic (clotting) complications
1. Introduction
According to epidemiological data provided by the WHO from 2019, when the first case of SARS-CoV-2 coronavirus infection was described, through December 6th, 2023, more than 772 million cases of COVID-19 have been confirmed worldwide. Among them, more than 6.98 million have resulted in death [WHO]. To date, 12 different variants of the SARS-CoV-2 virus have been identified: B.1.1.7 (Alpha), B.1.351 (Beta), B.1.525 (Eta), B.1.427/B.1.429 (Epsilon), B.1.526 (Iota), B.1.617.1 (Kappa), B.1.617.2 (Delta), C.37 (Lambda), P.1 (Gamma), P.2 (Zeta), P.3 (Theta) and B.1.1.529 (Omicron) [1]. In addition to B.1.1.529, there are other Omicron variant lines: lines BA.2, BA.3, BA.4, BA.5, XBB and BQ.1. On January 21, 2023, it was announced that the XBB.1.5 (Kraken) subvariant had been identified as the cause of 49.1% of COVID-19 cases in the US, but it did not dominate for long, as new Omicron subvariants have emerged since January 2023 [2]. As of August 19, 2023, the most common SARS-CoV-2 Omicron virus variants include: EG.5 (Eris — 20.6% of cases); FL.1.5.1 (Fornax — 13.3% of cases); and XBB.1.16 (Arcturus — 10.7% of cases) [3]. To date, variants of the virus that cause ocular symptoms have been described in the literature, but the severity of clinical presentations between specific viral variants in children remains poorly understood. To date, most analyses of the clinical complications of SARS-CoV-2 variants have been conducted on adults or without a direct link between a specific viral variant and a patient's clinical phenotype [4]. A study described in 2022 in the U.S. showed a high affinity of the beta variant for receptors found on the surface of the eye and an omicron strain that more often manifests as ocular pruritus than conjunctival congestion [5]. Children may be at risk of severe infection, and a Kawasaki-like disease associated with the clinical manifestations of SARS-CoV-2 has been described in the literature, referred to as the new multisystem inflammatory syndrome in children (MIS-C) [6]. There are reports that during the period of the Delta and Omicron virus infection, patients with MIS-C were younger compared to those when the Alpha variant predominated, which may be related to differences in the pathogenicity of the variants [4]. The virus is transmitted by the droplet route [7] but the genetic material of the virus is also detectable within the eye in tears and conjunctival secretions [7,8,9,10]. Ocular manifestations of COVID-19 infection in children are variable, and the prevalence ranges from 0.7% to 31.6% in children worldwide [11,12,13,14]. They may resolve spontaneously or be the first signs of a severe infection, especially in MIS-C, where accelerated treatment may improve prognosis [15]. Ocular manifestations so far reported and documented in the course of COVID-19 in children include conjunctivitis, chorioretinitis and/or retinal vasculitis, epitheliitis, corneal epitheliopathy, orbital cellulitis, orbital inflammatory disease, lacrimal gland inflammation, retinal vascular obstruction, retinopathy, maculopathy, intraocular inflammation, cranial nerve palsy and optic neuritis [6,16,17].
It should be noted that in all of the aforementioned cases of ocular infections, treatment is dominated by the use of topical steroids in drops and/or their systemic administration.
After analyzing the available literature from 2020-2023 with the PubMed and Google Scholar search engines, it was observed that the authors' description of covid panuveitis in a child is the first in which a beneficial effect of steroid therapy by injection under the Tenon capsule, with local drip therapy and general multi-month therapy with acetylsalicylic acid and pentoxifylline and without the need for systemic steroid therapy, was demonstrated.
2. Materials and Methods
The authors reviewed the current literature covering the years 2020-2023 in the PubMed and Google Scholar search engines, using the following keywords in various combinations: COVID-19, SARS-CoV-2, COVID-19 ocular manifestations, pentoxifylline, COVID-19 thrombotic complications, pediatric ocular cases of COVID-19, panuveitis, treatment of covid uveitis, Depomedrol under Tenon's pouch in the treatment of covid uveitis, ophthalmic complications after covid infection, posteroid complications. In addition, references cited in the identified articles were reviewed to find additional reports. This paper describes a postcovid case of pediatric panuveitis, in the treatment of which, for the first time, the beneficial effect of steroid therapy by injection under the Tenon capsule was demonstrated with local drip therapy and general multi-month therapy with acetylsalicylic acid and pentoxifylline, without the need for systemic steroid therapy, and analyzes other cases of pediatric panuveitis described in the literature as well as the latest information on the ocular manifestations of SARS-CoV-2 infection in children.
3. Results
According to epidemiological data provided by the WHO from 2019, when the first case of SARS-CoV-2 coronavirus infection was described, through December 6th, 2023, more than 772 million cases of COVID-19 have been confirmed worldwide. Among them, more than 6.98 million have resulted in death [WHO]. To date, 12 different variants of the SARS-CoV-2 virus have been identified: B.1.1.7 (Alpha), B.1.351 (Beta), B.1.525 (Eta), B.1.427/B.1.429 (Epsilon), B.1.526 (Iota), B.1.617.1 (Kappa), B.1.617.2 (Delta), C.37 (Lambda), P.1 (Gamma), P.2 (Zeta), P.3 (Theta) and B.1.1.529 (Omicron) [1]. In addition to B.1.1.529, there are other Omicron variant lines: lines BA.2, BA.3, BA.4, BA.5, XBB and BQ.1. On January 21, 2023, it was announced that the XBB.1.5 (Kraken) subvariant had been identified as the cause of 49.1% of COVID-19 cases in the US, but it did not dominate for long, as new Omicron subvariants have emerged since January 2023 [2]. As of August 19, 2023, the most common SARS-CoV-2 Omicron virus variants include: EG.5 (Eris — 20.6% of cases); FL.1.5.1 (Fornax — 13.3% of cases); and XBB.1.16 (Arcturus — 10.7% of cases) [3]. To date, variants of the virus that cause ocular symptoms have been described in the literature, but the severity of clinical presentations between specific viral variants in children remains poorly understood. To date, most analyses of the clinical complications of SARS-CoV-2 variants have been conducted on adults or without a direct link between a specific viral variant and a patient's clinical phenotype [4]. A study described in 2022 in the U.S. showed a high affinity of the beta variant for receptors found on the surface of the eye and an omicron strain that more often manifests as ocular pruritus than conjunctival congestion [5]. Children may be at risk of severe infection, and a Kawasaki-like disease associated with the clinical manifestations of SARS-CoV-2 has been described in the literature, referred to as the new multisystem inflammatory syndrome in children (MIS-C) [6]. There are reports that during the period of the Delta and Omicron virus infection, patients with MIS-C were younger compared to those when the Alpha variant predominated, which may be related to differences in the pathogenicity of the variants [4]. The virus is transmitted by the droplet route [7] but the genetic material of the virus is also detectable within the eye in tears and conjunctival secretions [7,8,9,10]. Ocular manifestations of COVID-19 infection in children are variable, and the prevalence ranges from 0.7% to 31.6% in children worldwide [11,12,13,14]. They may resolve spontaneously or be the first signs of a severe infection, especially in MIS-C, where accelerated treatment may improve prognosis [15]. Ocular manifestations so far reported and documented in the course of COVID-19 in children include conjunctivitis, chorioretinitis and/or retinal vasculitis, epitheliitis, corneal epitheliopathy, orbital cellulitis, orbital inflammatory disease, lacrimal gland inflammation, retinal vascular obstruction, retinopathy, maculopathy, intraocular inflammation, cranial nerve palsy and optic neuritis [6,16,17].
It should be noted that in all of the aforementioned cases of ocular infections, treatment is dominated by the use of topical steroids in drops and/or their systemic administration.
After analyzing the available literature from 2020-2023 with the PubMed and Google Scholar search engines, it was observed that the authors' description of covid panuveitis in a child is the first in which a beneficial effect of steroid therapy by injection under the Tenon capsule, with local drip therapy and general multi-month therapy with acetylsalicylic acid and pentoxifylline and without the need for systemic steroid therapy, was demonstrated.
CASE DESCRIPTION
A 14.5-year-old patient presented to the ophthalmological emergency room with congestion, tearing and markedly increased photophobia of the right eye with symptoms of general infection: malaise, subfebrile state, chills and vomiting. The COVID-19 antigen test performed on admission was negative. Upon ophthalmologic examination, visual acuity (VA) assessed on a Snellen chart with best spectacle correction was: right eye — 0.5 sc, left eye — 1.0 sc; binocular intraocular pressure (IOP) 17.6 mmHg (I-care tonometer). Conjunctivitis, of possible COVID-19 etiology, was initially diagnosed in the right eye (RE). Hence, a topical antiviral and antimicrobial treatment was implemented, achieving a mediocre improvement (Viru-POS eye ointment and Vigamox). After 4 weeks, re-exacerbation of ophthalmic symptoms appeared in the left eye, hitherto healthy, resulting in significant visual impairment; VA RE 0.9 sc; VA LE 2.5/50 sc; IOP RE/LE 15.0 and 12.0 mmHg, respectively. The following accompanying ocular symptoms were found under the slit lamp in both eyes: mixed ciliary nastema, corneal edema and multiple inflammatory deposits of the corneal endothelium, tyndalization of the ventricular fluid ++/+++; posterior circular adhesion of the iris, fibrin in the pupillary aperture, constriction and irregular shape of the pupil. Figure 1. In the posterior segment in both eyes: features of intraocular inflammation of the optic nerve with swelling, obliteration of borders and elevation of the optic disc, streaky hemorrhages on the surface of the disc, retinal vessels mainly venous dilated and tortuous, uneven caliber, constrictions visible in places. An image indicating a prothrombotic condition in the retinal vessels. In the left eye, an image similar to the RE with visible inflammatory vascular sheaths along the retinal vessels in the periocular area. Figure 2. In the chamber of the vitreous body, hyperechoic exudate confirmed by ultrasound B. Panuveitis of the left eye and post-uveitis condition of the right eye were diagnosed.
Additional examinations: OCT (optical coherence tomography) of the macula indicated thickening of the central part of the retina in the RE — 317 um, in the LE — 300 um; OCT of the optic disc (CN II) — binocular elevation of the optic nerve disc; crowding of CN II fibers on the disc (more significantly on the left side) with RNFL RE 244 um; LE 299 um. Figure 3. Kinetic perimetry, VER RE/LE and MRI (magnetic resonance imaging) of the brain and orbits within normal limits.
Treatment included Depo-Medrol 40 mg/ml injection under the Tenon capsule and subconjunctival injection of epinephrine into the RE and LE to disrupt posterior adhesions.
Fluorescein angiography (AF) confirmed obliteration of the borders of the optic disc with a widened network of natal vessels and accumulation of pigment, fluorescence block in the projection of hemorrhages at the LE disc and dilated and tortuous retinal vessels in both eyes. In the far periphery from the temples, retinal-vascular leaks as a sign of blood-retinal barrier dissection. Figure 4.
Indocyanine angiography. Late-phase, scattered foci of hypofluorescence in both eyes. In the peripheral part of the retina and in the LE macula, possibly corresponding to the presence of inflammatory foci in the course of uveitis. Figure 5.
Abnormal biochemical test results included: elevated levels of IgG antibodies to Sars-CoV-2 (161 AU/ml; norm less than 12 AU/ml); D-Dimers (501 ng/ml; norm 0-500 ng/ml); and platelets (415,000/mm3; norm 150-400,000/mm3). IgM p/Sars-CoV- 2 antibody levels were within normal limits. Computerized tomography (CT) of the lungs — a ground glass opacity image and multinodular inflammatory lesions in various segments of the lungs were described, indicating a history of COVID-19 infection. In the multispecialty consultations performed, the following was excluded: JIA (rheumatologist), lymphoproliferative diseases (hematologist), multiple sclerosis (neurologist), upper respiratory tract infections and sinusitis (otolaryngologist), inflammatory foci in the oral cavity (dentist), hypertension and renal failure (hypertensiologist and nephrologist); tuberculosis and sarcoidosis (pulmonologist).
Detailed laboratory diagnosis of uveitis did not confirm infection for Lyme disease, bartonellosis, toxocariasis, HSV-1, HSV-2, toxoplasmosis, syphilis, cytomegalovirus, leptospirosis, VZV, brucellosis, HIV 1/2, antinuclear antibodies (ANA), anti-neutrophil cytoplasmic antibodies (ANCA), rheumatoid factor, fecal parasites. ACE (angiotensin-converting enzyme) and lysozyme levels were also determined, ruling out sarcoidosis, and HLA-B (human leukocyte antigen) was determined, confirming the presence of HLA B*07 and HLA B*15.
Treatment was administered in the form of: steroidal and non-steroidal anti-inflammatory eye drops: dexamethasone 0.1%; diclofenac; mydriatic-atropine 1%. Acetylsalicylic acid (150 mg) and pentoxifylline (100 mg) were administered orally, which resulted in a reduction in photophobia and a significant improvement in visual acuity — VRE 1.0; VLE 0.9 — as well as binocular partial disruption of posterior adhesions. Follow-up systematic ophthalmologic examinations conducted initially every 2 weeks for about six months, then every 4 weeks, and then every 2 months for up to 1 year after the end of hospitalization, indicated a reduction in the features of intraocular inflammation of the optic disc, absorption of hemorrhages, upright course of retinal vessels, absence of choroidal sheaths and reduction of exudate in the vitreous. Figure 6 and Figure 7.
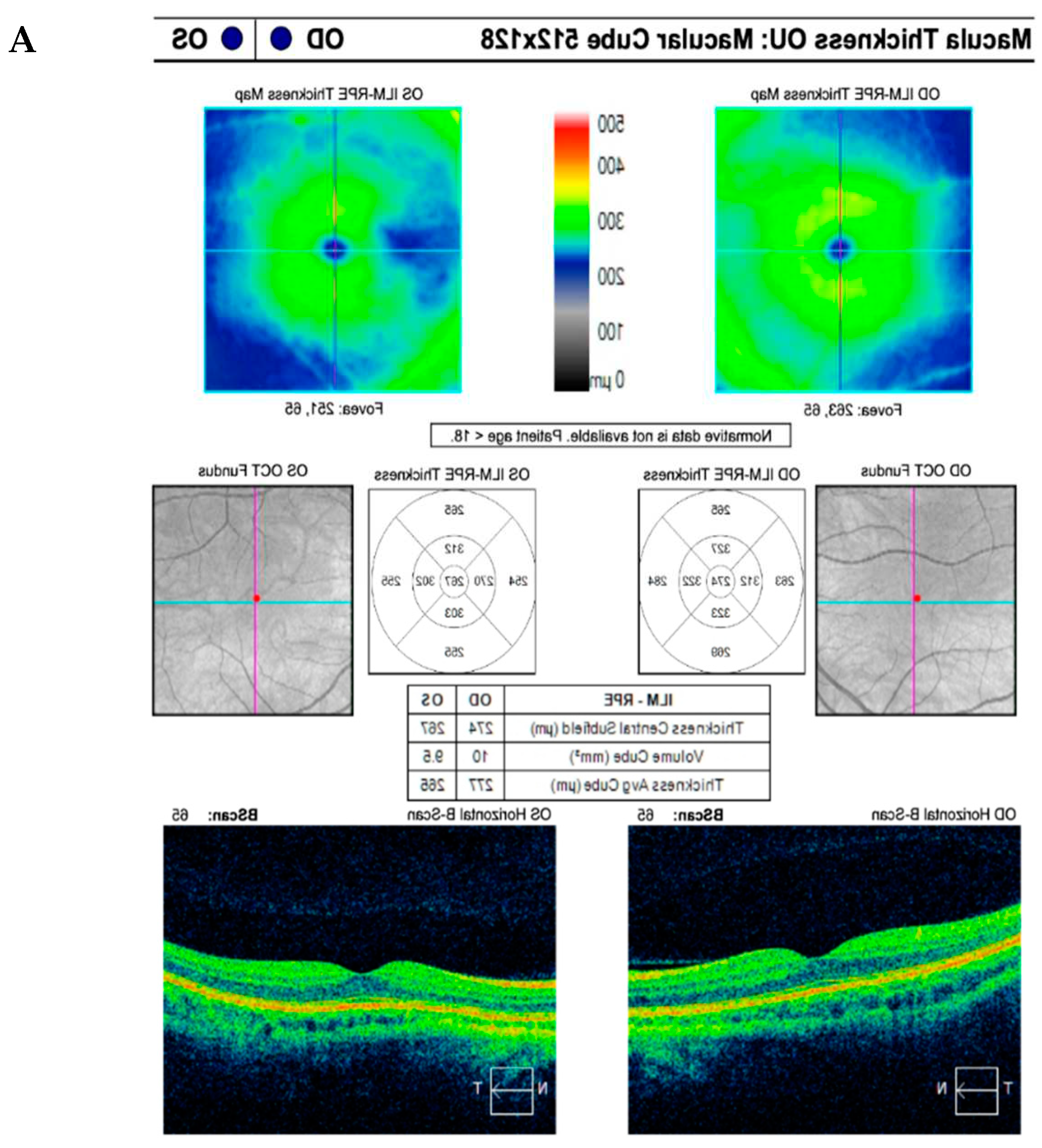
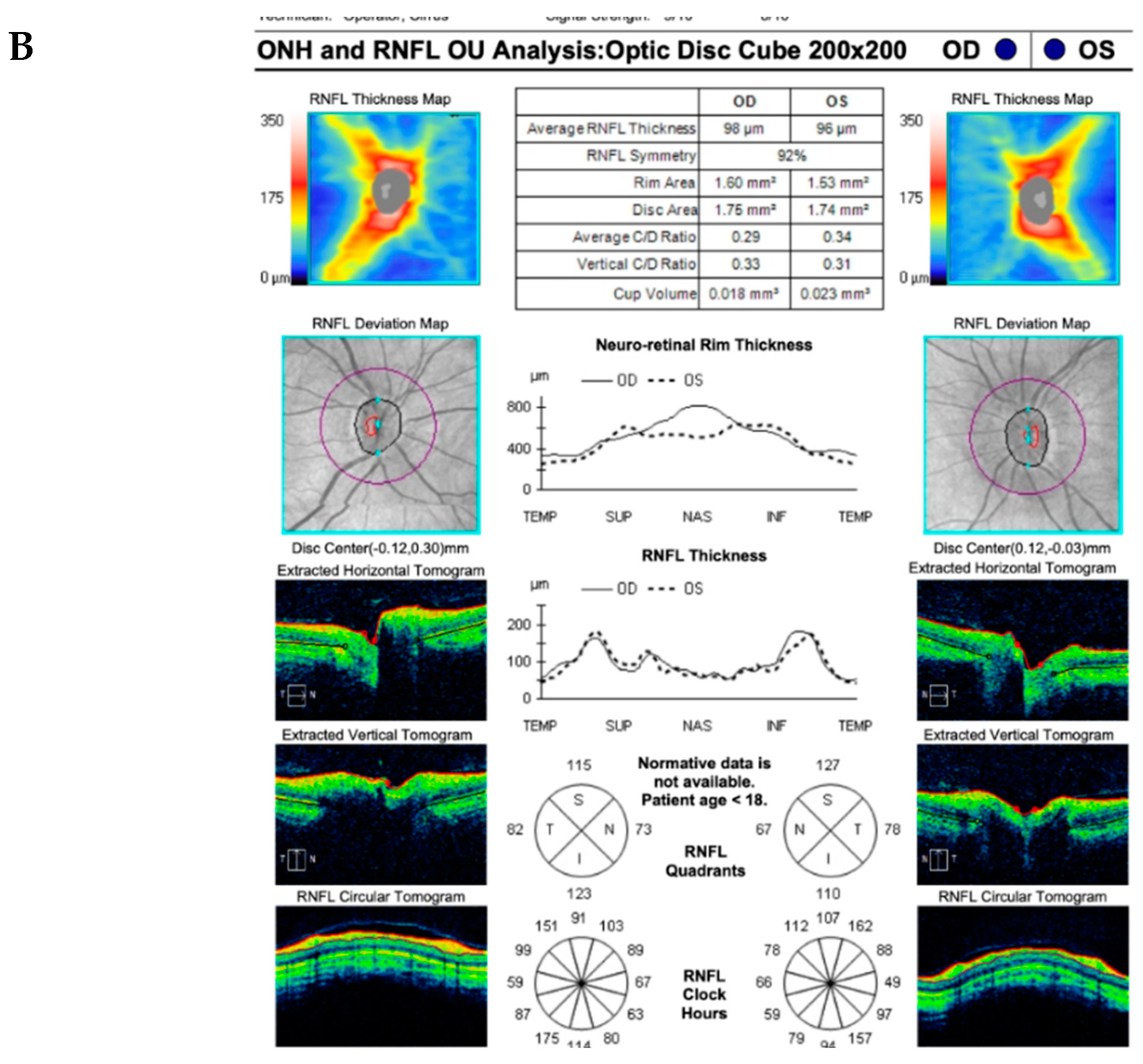
Diagnostic ophthalmologic examinations after topical steroid and Tenon capsule treatment indicated improvement in inflammation: in OCT of the macula, a reduction in central retinal thickness (CRT) was obtained in RE 274 um, in LE 267 um. In OCT of the optic disc, a reduction in the thickness of the RNFL was observed in the RE — 98 um; in the LE — 96 um, with swelling of the optic disc area still visible. Figure 8. On B-scan ultrasound, a reduction in vitreous exudate was noted and laboratory tests showed normalization of previously elevated or abnormal results.
Topical treatment with Dexamethasone once a day and oral administration of acetylsalicylic acid (150 mg) and pentoxifylline (100 mg) was carried out for up to 12 consecutive months, until complete local improvement was achieved in both eyes.
4. Discussion
In SARS-CoV-2 infection, the angiotensin-converting enzyme 2 (ACE2) is involved in the virus attachment to the host cell. This is a receptor that is a component of the renin-angiotensin system. It is expressed in endothelial cells as well as in corneal and conjunctival cells, and perhaps more internal layers of the ocular epithelium, particularly in fibroblasts and dendritic cells [18]. Expression of the ACE2 gene has been shown to be higher in older children and young adults than in younger children, a likely reason for the lower rate of SARS-CoV-2 transmission through tears in younger children [16]. The ACE2 enzyme is stimulated by the transepithelial serine protease type II TMPRSS2 or cathepsin L. Other additional receptors involved in the infection process have also been described thusfar: CD147/EMMPRIN/Basigin, Axl and Neuropilin-1 (NRP1) [19]. The conjunctiva, corneal and stroma epithelium as well as the corneal endothelium all show expression of SARS-CoV-2 receptors such as ACE2, TMPRSS2, CD147 and NRP1 [20]. The conjunctiva is, therefore, the most commonly infected inflammatory structure of the eye and, according to the literature, conjunctivitis occurs in up to 31% of severe COVID-19 cases [6]. According to a June 2021 meta-analysis where a total of 30 studies were identified, the most common ocular symptoms in children and adolescents were conjunctival congestion (7.6%), discharge in the eye (4.8%), tearing (6.9%) and foreign body sensation (6.9%) [16,21]. In January 2021, statistics compiled by Nasiri et al. were published, according to which the most common ocular symptoms included conjunctivitis, dry eye or foreign body sensation, redness, tearing and itching among 88.8%, 16%, 13.3%, 12.8% and 12.6% of COVID-19-infected patients respectively, regardless of age and gender [22].
Ocular manifestations of coronavirus in pediatric age groups are divided in the literature into two categories: symptoms associated with MIS-C, which include conjunctivitis and anterior uveitis, optic neuritis, retinitis, and corneal epitheliopathy; and symptoms associated with COVID-19 such as conjunctivitis, neonatal conjunctivitis (ophthalmia neonatorum), optic neuritis, paralysis of the retrobulbar nerve, oculomotor nerve, opsoclonus, neuromyelitis optica, orbital inflammatory disease (orbital cellulitis, orbital myositis), retinal vasculitis and central retinal vein obstruction [6,17,23]. In addition, other unusual pediatric ocular manifestations of COVID-19 have been described in the literature, such as a case of widespread peripheral necrotizing retinitis in a 5-year-old child, described in 2021. Aniruddh Soni et al. described the association of SARS-CoV2 virus infection with herpes virus reactivation [24]. In February 2021. Pérez-Chimal et al. produced a report on ophthalmic manifestations associated with SARS-CoV-2 in newborns, where the most common symptoms included periorbital edema (100%), chemosis and hemorrhagic conjunctivitis (73%) and ciliary injection (53%). Cases of infants with corneal edema (40%), posterior segment symptoms, including retinopathy of prematurity (in 20%) of infants, retinal exudate similar to "cotton wool spots" (13.3%) and vitreous hemorrhage (6.6%) have also been described [25]. In December 2021, Diwakara et al. published the first report of COVID-19-associated rhinocerebral mucormycosis in children and adolescents with type 1 diabetes during treatment for diabetic ketoacidosis [26].
The literature lacks a uniform treatment regimen for uveitis, including panuveitis caused by COVID-19. According to our internet search (Pubmed and Google Scholar search engines) conducted up until December 2023, only three (3) pediatric cases of panuveitis associated with coronavirus infection in the pediatric population (7, 9 and 12 years old) between 2021 and 2023 have been described in which treatment was successful, but none of the described cases received isolated treatment with steroid injections under the Tenon capsule. All cases were treated with systemic steroids and methotrexate [27], a cycle of intravenous methylprednisolone (IVMP) followed by oral and topical steroids [27] and dexamethasone intravenously (0.4 mg/kg/day) followed by oral steroids, gradually reducing the dose, until the desired effect was achieved [28].
In addition, up until the time of writing this article, no pediatric case of COVID-19-induced intraocular inflammation has been published with treatment consiting of extraocular steroid therapy combined with prophylaxis of retinal vascular thrombotic complications. Precisely such a treatment was applied successfully in our patient, giving him aspirin and pentoxifylline to improve vascular flow, with prothrombotic readiness observed on the fundus (elevation of D-dimers and retinal vasculature on the fundus and AF).
The literature reports a correlation of COVID-19 infection with progression of procoagulation mechanisms, leading to severe thrombotic complications. The increased affinity of the SARS-CoV-2 virus for the ACE2 receptor in host cells indirectly affects the release of pro-inflammatory cytokines in the vascular endothelium [29]. The body's excessive inflammatory response, endothelial dysfunction and platelet activation result in an increased predisposition of patients infected with COVID-19 to thromboembolic events, both in the arterial and venous circulation. Due to the abundant vascularization of the retina, this is a structure of the eye particularly vulnerable to thromboembolic complications [30].
In view of the above, it is vital that ophthalmologists pay special attention to the effects of the SARS-CoV-2 virus, which include the increased coagulation caused by the infection. In 2020, F. Seirafianpour et al. described the potential antiviral properties of pentoxifylline and the benefits of its use under many of the circumstances present in COVID-19, particularly in controlling inflammation and related complications [31]. There are also reports of the efficacy of pentoxifylline treatment in retinal vein thrombosis in patients with sudden loss of vision [32,33]. Pentoxifylline decreases blood viscosity, so it can alleviate the increased blood rheology induced by COVID-19 and the hyperaggregation of red blood cells that is associated with the development of coagulopathy. Therefore, it is reasonable to assess further observations in order to confirm the beneficial effects of treatment with isolated steroid therapy under the Tenon capsule in combination with anti-aggregation treatment, thus improving retinal-vascular circulation without exposing the child to post-steroid complications in general use.
5. Conclusions
Analyzing the aforementioned cases leads to the general conclusion that the most commonly used therapies for the treatment of simultaneous inflammation of all sections of the uvea — panuveitis — in the course of COVID-19 include systemic and topical steroids. Medications from the group of glucocorticosteroids in ocular injections and topical drops are definitely less burdensome for children and help to avoid complications such as growth and development retardation, psychosis, osteoporosis, cataracts, gastrointestinal complaints (peptic ulcers, candidiasis), dermatological lesions (hirsutism, striae, difficulties in wound healing) and hormonal changes (weight gain, adrenal inhibition, hypertension, hyperglycemia) [34]. In the case described by the authors, the treatment used Depo-Medrol (40 mg/ml) injected under the Tenon capsule with two subconjunctival injections of epinephrine, local steroid therapy and non-steroidal anti-inflammatory drugs — dexamethasone (0.1%) and diclofenac drops. In addition, acetylsalicylic acid (150 mg) and pentoxifylline (100 mg) were administered orally throughout the course of the disease as well as up to 12 months after its termination until complete improvement in visual acuity and withdrawal of ophthalmic lesions was achieved. It can be assumed that this type of treatment is clearly more beneficial for pediatric patients, with an effect comparable to systemic steroid administration, achieving improvement in retinal-vascular circulation without exposing the child to systemic posteroid complications.
Author Contributions
Conceptualization, M.M.; software and validation M.M.; O.Z. formal analysis, M.M.; resources, M.M.; writing-original draft preparation M.M.; O.Z; J.C.; W.B.; review and editing, M.M.; visualization, O.Z.; J.C.; W. B.; supervision, M.M.; project administration, M.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare that there are no conflicts of interest regarding the publication of this paper.
References
- Ghosh N, Nandi S, Saha I. A review on evolution of emerging SARS-CoV-2 variants based on spike glycoprotein. Int Immunopharmacol. 2022;105:108565. [CrossRef]
- Parums, DV. Editorial: The XBB.1.5 ('Kraken') Subvariant of Omicron SARS-CoV-2 and its Rapid Global Spread. Med Sci Monit. 2023;29:e939580. Published 2023 Feb 1. [CrossRef]
- Parums, DV. Editorial: A Rapid Global Increase in COVID-19 is Due to the Emergence of the EG.5 (Eris) Subvariant of Omicron SARS-CoV-2. Med Sci Monit. 2023;29:e942244. Published 2023 Sep 1. [CrossRef]
- Sperotto F, Gutiérrez-Sacristán A, Makwana S, et al. Clinical phenotypes and outcomes in children with multisystem inflammatory syndrome across SARS-CoV-2 variant eras: a multinational study from the 4CE consortium. EClinicalMedicine. 2023;64:102212. Published 2023 Sep 14. [CrossRef]
- Mostafavi E, Dubey AK, Teodori L, Ramakrishna S, Kaushik A. SARS-CoV-2 Omicron variant: A next phase of the COVID-19 pandemic and a call to arms for system sciences and precision medicine. MedComm (2020). 2022;3(1):e119. Published 2022 Feb 11. [CrossRef]
- Alnahdi MA, Alkharashi M. Ocular manifestations of COVID-19 in the pediatric age group. Eur J Ophthalmol. 2023;33(1):21-28. [CrossRef]
- Worldmeter. COVID-19 Coronavirus Pandemic. Available from: https://www.worldometers.info/coronavirus/. Accessed September 22, 2022.
- Akbari M, Dourandeesh M. Update on overview of ocular manifestations of COVID-19. Front Med (Lausanne). 2022;9:877023. Published 2022 Sep 13. [CrossRef]
- Hosseini SM, Abrishami M, Zamani G, et al. Acute Bilateral Neuroretinitis and Panuveitis in A Patient with Coronavirus Disease 2019: A Case Report. Ocul Immunol Inflamm. 2021; 29(4):677-680. [CrossRef]
- Braceros KK, Asahi MG, Gallemore RP. Visual Snow-Like Symptoms and Posterior Uveitis following COVID-19 Infection. Case Rep Ophthalmol Med. 2021; 2021:6668552. [CrossRef]
- Ichhpujani P, Singh RB, Dhillon HK, Kumar S. Ocular manifestations of COVID-19 in pediatric patients. Ther Adv Ophthalmol. 2023;15:25158414221149916. Published 2023 Mar 14. [CrossRef]
- Guo CX, He L, Yin JY, et al. Epidemiological and clinical features of pediatric COVID-19. BMC Med. 2020;18(1):250. Published 2020 Aug 6. [CrossRef]
- Valente P, Iarossi G, Federici M, et al. Ocular manifestations and viral shedding in tears of pediatric patients with coronavirus disease 2019: a preliminary report. J AAPOS. 2020;24(4):212-215. [CrossRef]
- Mandal, A., Kumari, E., Roy, A., & Bandyopadhyay, M. (2021). Ocular manifestations and clinical profile of multisystemic inflammatory syndrome in children during COVID-19 pandemic. Int J Res Med Sci, 10(1), 173. [CrossRef]
- Madani, S. Acute and sub-acute ocular manifestations in pediatric patients with COVID-19: A systematic review. Med Hypothesis Discov Innov Ophthalmol. 2022;11(1):11-18. Published 2022 Apr 1. [CrossRef]
- Ichhpujani P, Singh RB, Dhillon HK, Kumar S. Ocular manifestations of COVID-19 in pediatric patients. Ther Adv Ophthalmol. 2023;15:25158414221149916. Published 2023 Mar 14. [CrossRef]
- Singh S, Garcia G Jr, Shah R, et al. SARS-CoV-2 and its beta variant of concern infect human conjunctival epithelial cells and induce differential antiviral innate immune response. Ocul Surf. 2022;23:184-194. [CrossRef]
- Willcox MD, Walsh K, Nichols JJ, Morgan PB, Jones LW. The ocular surface, coronaviruses and COVID-19. Clin Exp Optom. 2020;103(4):418-424. [CrossRef]
- Kyrou I, Randeva HS, Spandidos DA, Karteris E. Not only ACE2-the quest for additional host cell mediators of SARS-CoV-2 infection: Neuropilin-1 (NRP1) as a novel SARS-CoV-2 host cell entry mediator implicated in COVID-19. Signal Transduct Target Ther. 2021;6(1):21. Published 2021 Jan 18. [CrossRef]
- Collin J, Queen R, Zerti D, et al. Co-expression of SARS-CoV-2 entry genes in the superficial adult human conjunctival, limbal and corneal epithelium suggests an additional route of entry via the ocular surface. Ocul Surf. 2021;19:190-200. [CrossRef]
- Zhong Y, Wang K, Zhu Y, et al. Ocular manifestations in COVID-19 patients: A systematic review and meta-analysis. Travel Med Infect Dis. 2021;44:102191. [CrossRef]
- Eissa M, Abdelrazek NA, Saady M. Covid-19 and its relation to the human eye: transmission, infection, and ocular manifestations. Graefes Arch Clin Exp Ophthalmol. 2023;261(7):1771-1780. [CrossRef]
- Hu K, Patel J, Swiston C, Patel BC. Ophthalmic Manifestations of Coronavirus (COVID-19). In: StatPearls. Treasure Island (FL): StatPearls Publishing; May 24, 2022.
- Soni A, Narayanan R, Tyagi M, Belenje A, Basu S. Acute Retinal Necrosis as a presenting ophthalmic manifestation in COVID 19 recovered patients. Ocul Immunol Inflamm. 2021;29(4):722-725. [CrossRef]
- Pérez-Chimal LG, Cuevas GG, Di-Luciano A, Chamartín P, Amadeo G, Martínez-Castellanos MA. Ophthalmic manifestations associated with SARS-CoV-2 in newborn infants: a preliminary report. J AAPOS. 2021;25(2):102-104. [CrossRef]
- Diwakar J, Samaddar A, Konar SK, et al. First report of COVID-19-associated rhino-orbito-cerebral mucormycosis in pediatric patients with type 1 diabetes mellitus. J Mycol Med. 2021;31(4):101203. [CrossRef]
- Ganesh SK, Mohanan-Earatt A. An analysis of the clinical profile of patients with uveitis following COVID-19 infection. Indian J Ophthalmol. 2022;70(3):1000-1006. [CrossRef]
- Merticariu CI, Merticariu M, Cobzariu C, Mihai MM, Dragomir MS. Pediatric inflammatory multisystem syndrome induced Panuveitis associated with SARS-CoV- 2 infection: What the Ophthalmologists need to know. Rom J Ophthalmol. 2022;66(2):198-208. [CrossRef]
- Yeo S, Kim H, Lee J, Yi J, Chung YR. Retinal vascular occlusions in COVID-19 infection and vaccination: a literature review. Graefes Arch Clin Exp Ophthalmol. 2023;261(7):1793-1808. [CrossRef]
- Shiroma HF, Lima LH, Shiroma YB, et al. Retinal vascular occlusion in patients with the Covid-19 virus. Int J Retina Vitreous. 2022;8(1):45. Published 2022 Jun 23. [CrossRef]
- Seirafianpour F, Mozafarpoor S, Fattahi N, Sadeghzadeh-Bazargan A, Hanifiha M, Goodarzi A. Treatment of COVID-19 with pentoxifylline: Could it be a potential adjuvant therapy?. Dermatol Ther. 2020;33(4):e13733. [CrossRef]
- De Sanctis MT, Cesarone MR, Belcaro G, Incandela L, Steigerwalt R, Nicolaides AN, Griffin M, Geroulakos G. Treatment of retinal vein thrombosis with pentoxifylline: a controlled, randomized trial. Angiology. 2002 Jan-Feb;53 Suppl 1:S35-8. PMID: 11865834.
- Mostafa-Hedeab G, Al-Kuraishy HM, Al-Gareeb AI, Jeandet P, Saad HM, Batiha GE. A raising dawn of pentoxifylline in management of inflammatory disorders in Covid-19. Inflammopharmacology. 2022;30(3):799-809. [CrossRef]
- Shivpuri A, Turtsevich I, Solebo AL, Compeyrot-Lacassagne S. Pediatric uveitis: Role of the pediatrician. Front Pediatr. 2022;10:874711. Published 2022 Aug 1. [CrossRef]
Figure 1.
Anterior segment of the right and left eyes (RE and LE). Irregular pupils and posterior synechiae, shallow anterior chamber in the right eye.
Figure 1.
Anterior segment of the right and left eyes (RE and LE). Irregular pupils and posterior synechiae, shallow anterior chamber in the right eye.
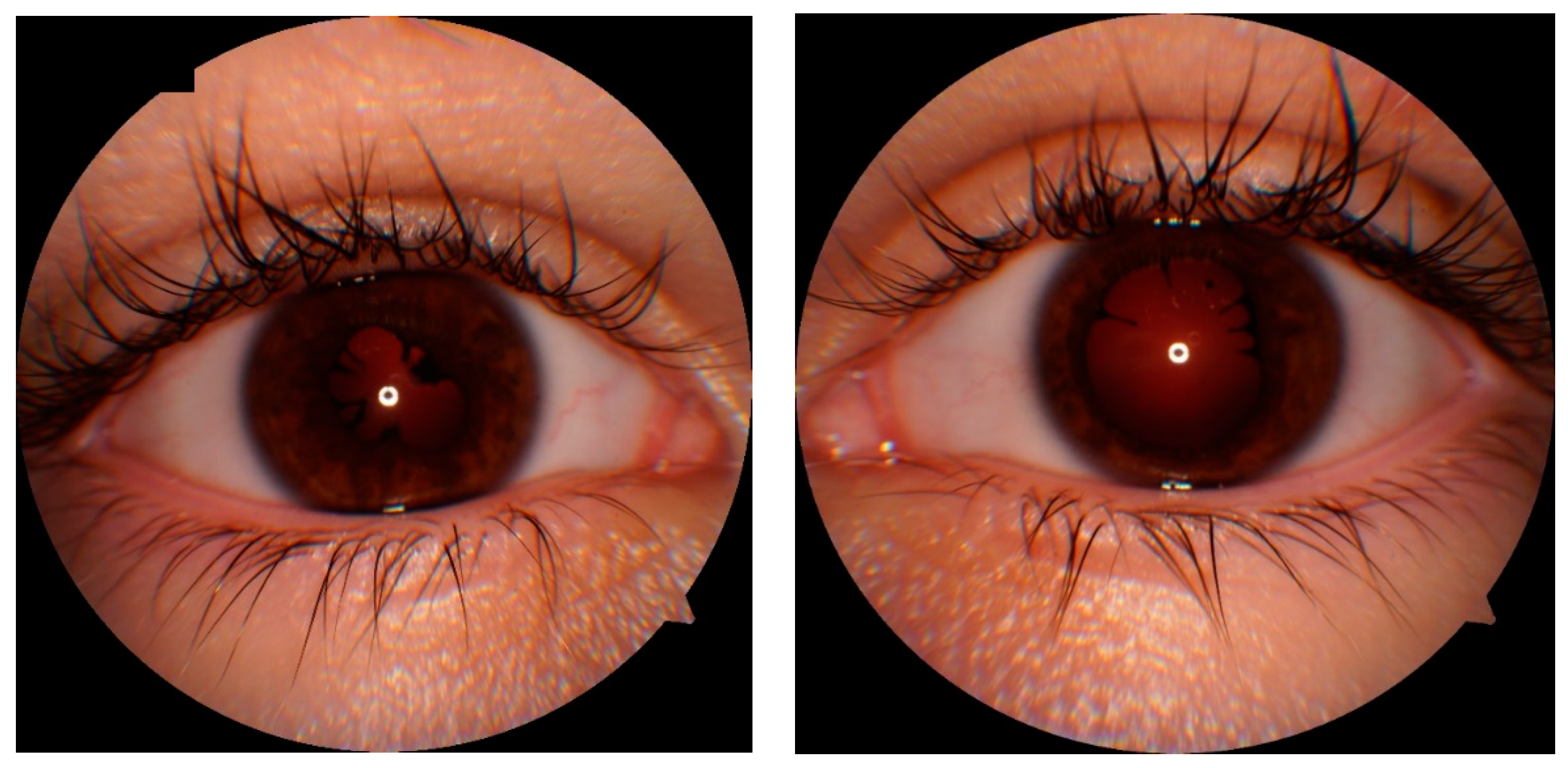
Figure 2.
Fundus of the both eye: optic disc swollen, partially blurred boundaries of the optic disc, hemorrhages on the surface and around of the optic disc, tortuous, irregular and dilated retinal vessels, in vitreous posterior vitreous opacification. The fundus of the left eye with signs of intraocular inflammation of the optic nerve disc and retinal vessels.
Figure 2.
Fundus of the both eye: optic disc swollen, partially blurred boundaries of the optic disc, hemorrhages on the surface and around of the optic disc, tortuous, irregular and dilated retinal vessels, in vitreous posterior vitreous opacification. The fundus of the left eye with signs of intraocular inflammation of the optic nerve disc and retinal vessels.
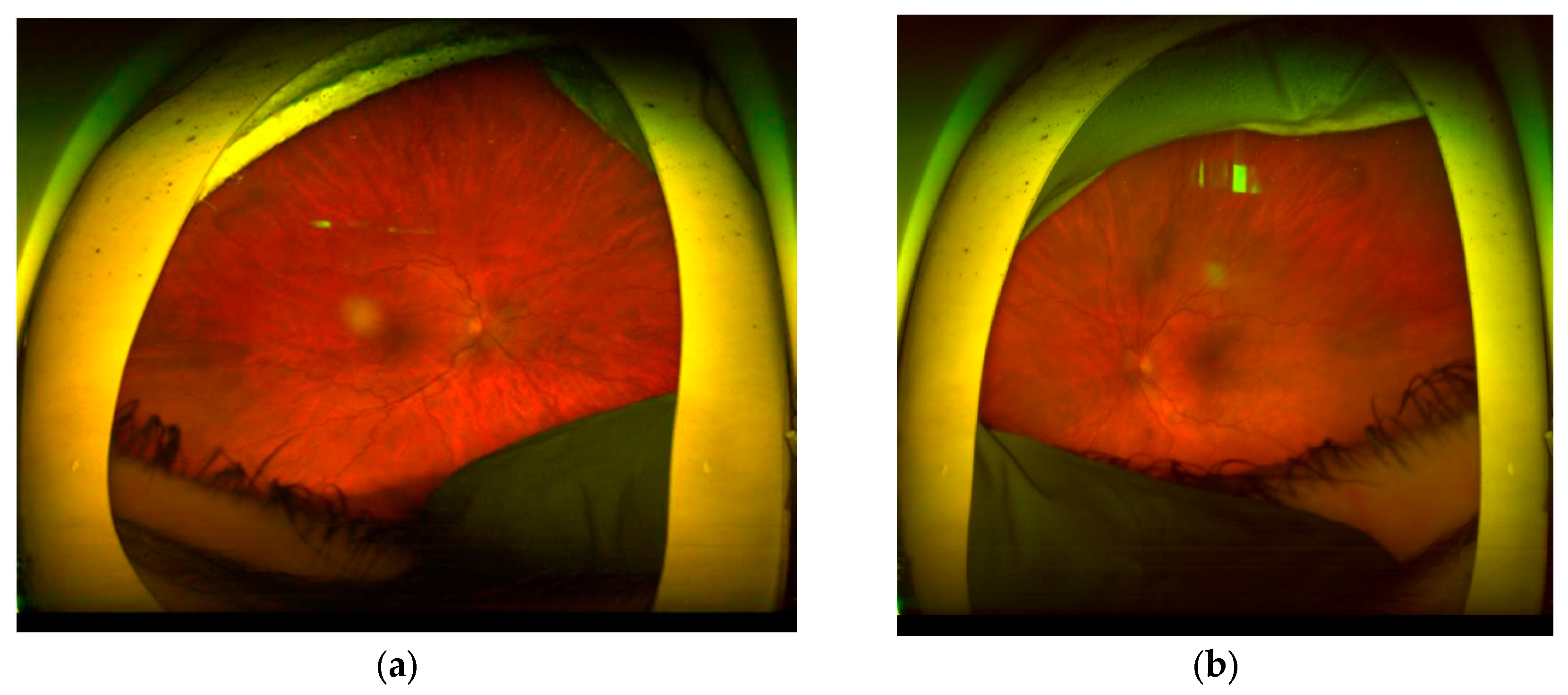
Figure 3.
On the left side- OCT- macular tests for Right and Left eyes, without lesions. On the right side- OCT optic disc test- significant elevation of the optic nerve; crowding and increase number of the of optic nerve fibers.
Figure 3.
On the left side- OCT- macular tests for Right and Left eyes, without lesions. On the right side- OCT optic disc test- significant elevation of the optic nerve; crowding and increase number of the of optic nerve fibers.
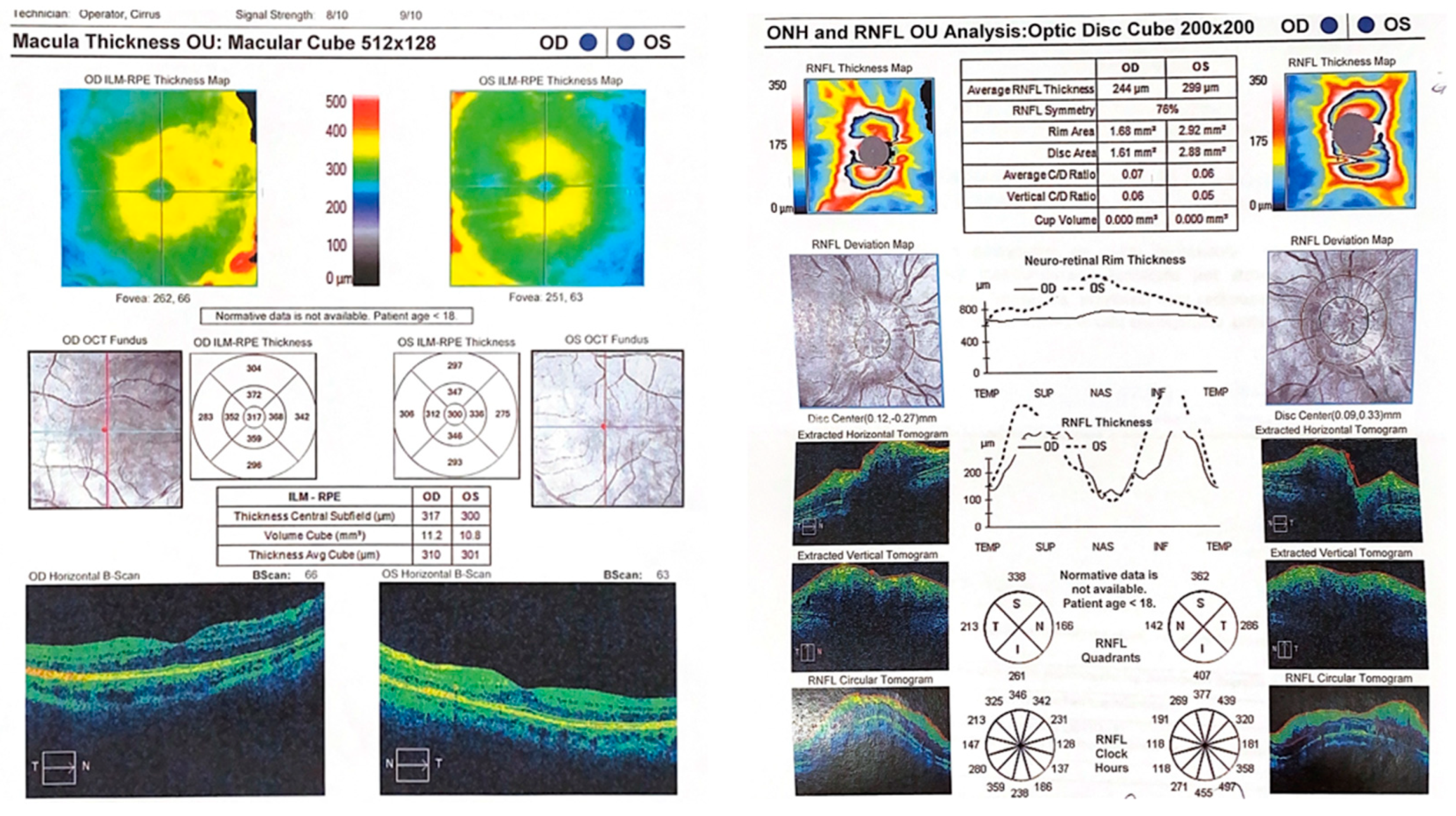
Figure 4.
In Fluorescein- Angiography confirmed: blurring of the boundaries of the disc II with a dilated network of epiphyseal vessels and accumulation of dye, blocking of fluorescence in the projection of hemorrhages near the disc LE, and dilated and tortuous retinal vessels in both eyes. On the periphery far from the temple, there are retinochoroidal leaks as a symptom of a breakdown of the blood-retinal barrier.
Figure 4.
In Fluorescein- Angiography confirmed: blurring of the boundaries of the disc II with a dilated network of epiphyseal vessels and accumulation of dye, blocking of fluorescence in the projection of hemorrhages near the disc LE, and dilated and tortuous retinal vessels in both eyes. On the periphery far from the temple, there are retinochoroidal leaks as a symptom of a breakdown of the blood-retinal barrier.
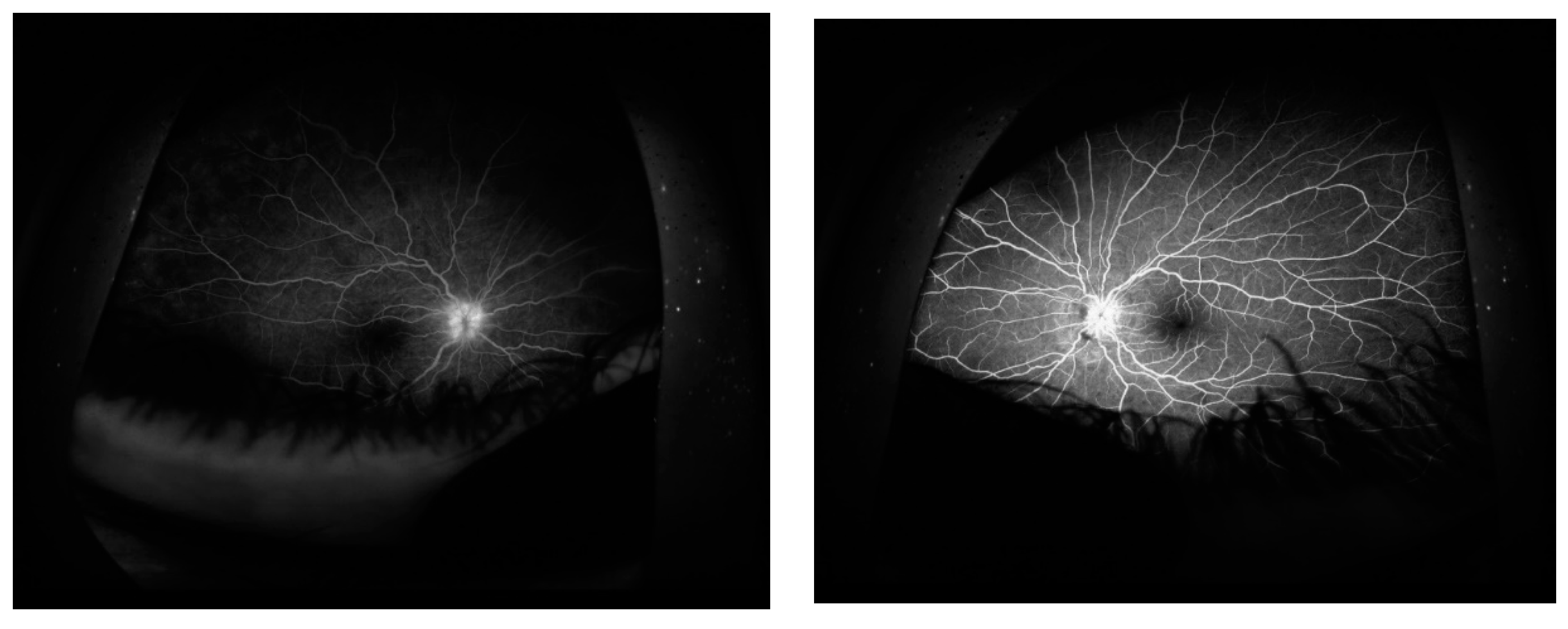
Figure 5.
Indocyanine angiography: in both eyes there were scattered foci of hypofluorescence in the late phase of contrast in the peripheral part of the retina and in the macula LE, which may correspond to the presence of inflammatory foci in the course of uveitis.
Figure 5.
Indocyanine angiography: in both eyes there were scattered foci of hypofluorescence in the late phase of contrast in the peripheral part of the retina and in the macula LE, which may correspond to the presence of inflammatory foci in the course of uveitis.
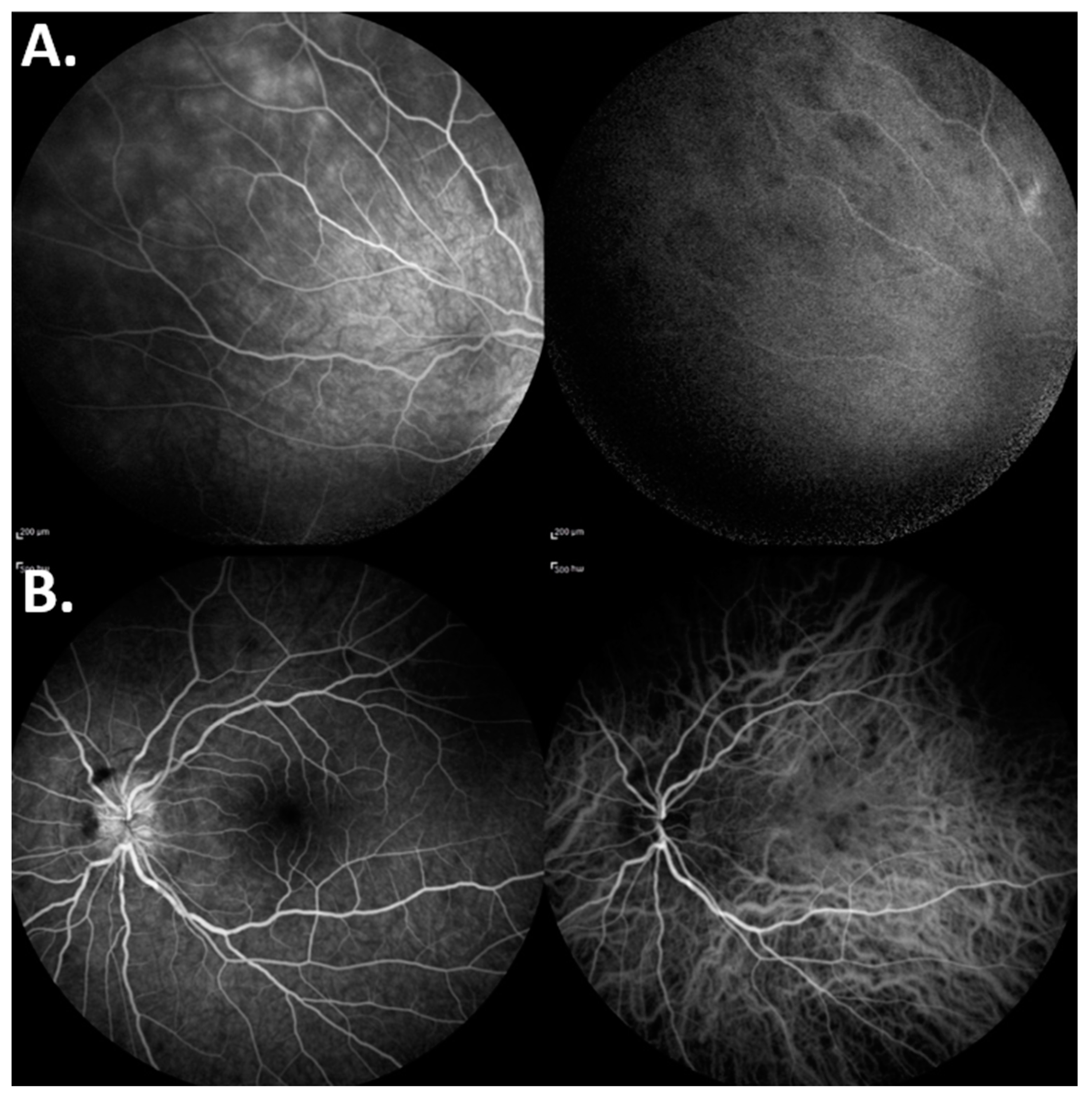
Figure 6.
Fundus of the right and left eye after treatment.
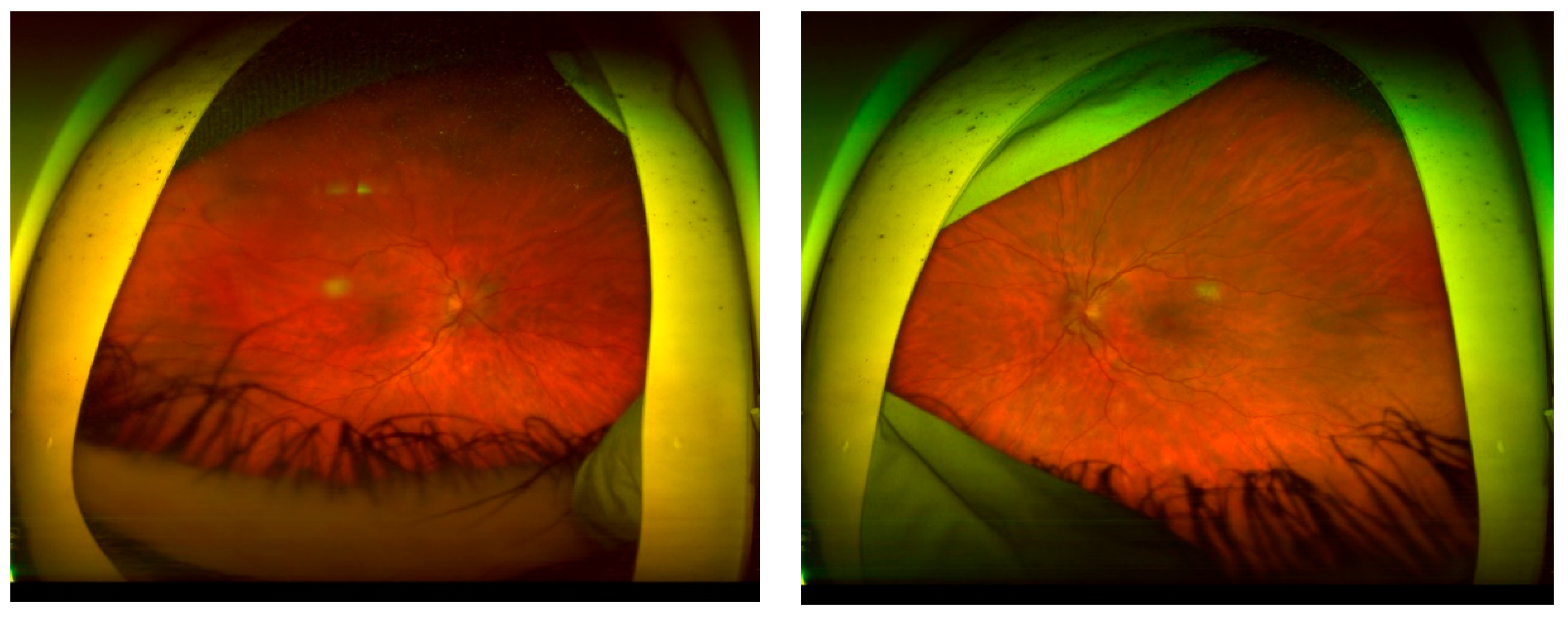
Figure 7.
Fundus right and left eye. (A) Evolution of changes on the fundus of the eye, (B) Fundus of the right eye: disc II with borders traceable from the nose, vessels with a tortuous course in places, well filled. White focus in the vitreous - much smaller compared to previous examinations, less saturated, less dense, Fundus of the left eye: disc no. II, borders traceable from the nose, vessels with a tortuous course in places, properly filled. The focus in the vitreous was not visible, (C) Right and left eyes, evolution of changes on the fundus of the eye.
Figure 7.
Fundus right and left eye. (A) Evolution of changes on the fundus of the eye, (B) Fundus of the right eye: disc II with borders traceable from the nose, vessels with a tortuous course in places, well filled. White focus in the vitreous - much smaller compared to previous examinations, less saturated, less dense, Fundus of the left eye: disc no. II, borders traceable from the nose, vessels with a tortuous course in places, properly filled. The focus in the vitreous was not visible, (C) Right and left eyes, evolution of changes on the fundus of the eye.
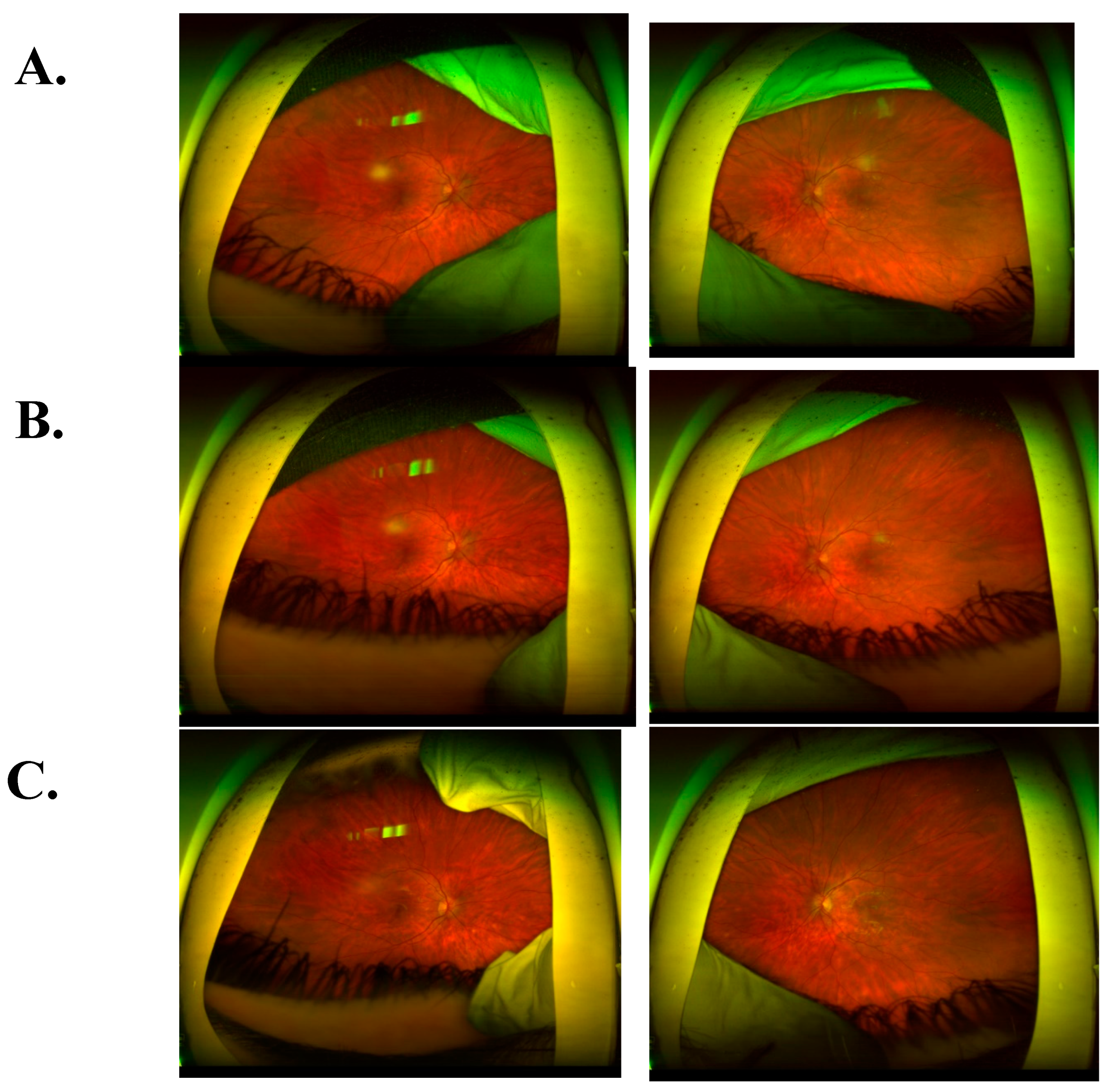
Figure 8.
Regression of lesions on the fundus of the eye expressed in the form of improvement in numerical values in OCT examinations (A) Macular OCT – right eye 274 μm; left eye 267 μm, (B) OCT disc II right/left eye - RNFL right eye 98 μm; left eye 96 um.
Figure 8.
Regression of lesions on the fundus of the eye expressed in the form of improvement in numerical values in OCT examinations (A) Macular OCT – right eye 274 μm; left eye 267 μm, (B) OCT disc II right/left eye - RNFL right eye 98 μm; left eye 96 um.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



