
Submitted:
23 January 2024
Posted:
24 January 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Coronavirus disease 2019 (COVID-19), the global pandemic caused by severe acute respiratory syndrome 2 virus (SARS-CoV-2) infection, has caused millions of infections and fatalities worldwide. Extensive SARS-CoV-2 research has been conducted to develop therapeutic drugs and prophylactic vaccines, and even though some drugs have been approved to treat SARS-CoV-2 infection, treatment efficacy remains limited. Therefore, preventive vaccination has been implemented on a global scale and represents the primary approach to combat the COVID-19 pandemic. Approved vaccines vary in composition, although vaccine design has been based on either the key viral structural (spike) protein or viral components carrying this protein. Therefore, mutations of the virus, particularly mutations in the S protein, severely compromise effectiveness of current vaccines and the ability to control COVID-19 infection. This review begins by describing the SARS-CoV-2 viral composition, mechanism of infection, role of angiotensin-converting enzyme 2, host defense responses against infection and the most common vaccine designs. Next, this review summarizes the common mutations of SARS-CoV-2 and how these mutations change viral properties, confer immune escape and influence vaccine efficacy. Finally, this review discusses global strategies that have been employed to mitigate the decreases in vaccine efficacy encountered against new variants.
Keywords:
COVID-19
; SARS-CoV-2
; Mutations
; Variants
; Vaccination
; Vaccine effectiveness
1. Introduction
Coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome 2 virus (SARS-CoV-2), is an ongoing global pandemic that has threatened public health over the past 3 years. Quickly spreading throughout the world since 2019, the COVID-19 virus has infected over 760 million individuals and caused more than 6.9 million deaths worldwide. SARS-CoV-2 is a betacoronavirus from the family of Coronaviridae that contains a central core consisting of positive-sense, single-stranded RNA (+ssRNA) shielded by envelop proteins. The Coronaviridae family is classified into four genera: alpha-, beta-, gamma- and delta-coronaviruses, but only the alpha- and beta-coronaviruses are capable of infecting humans.[1] Prior to the COVID-19 pandemic, there were two other pandemics caused by beta-coronaviruses: severe acute respiratory syndrome (SARS) in 2003, caused by severe acute respiratory syndrome coronavirus (SARS-CoV), and Middle East respiratory syndrome (MERS) in 2012, caused by Middle East respiratory syndrome coronavirus MERS-CoV. All three viruses exhibit high genetic similarity with SARS-CoV-2 sharing 79% and 50% genetic similarity with SARS-CoV and MERS-CoV, respectively.[2]
A variety of mild to severe symptoms have been associated with COVID-19. Typical mild symptoms of COVID-19 include flu-like fever, cough and muscle aches that often resolve without medical care, while severe COVID-19 symptoms include coma, difficulty breathing and severe chest pain that require intensive medical care. Asymptomatic infection and some rare symptoms have also been associated with COVID-19.[3] Like influenza, the primary modes of airborne transmission for SARS-CoV-2 are contact and droplet transmission;[4] therefore, infection can spread through particles and droplets of respiratory fluids expelled when an infected person coughs, sneezes or talks. These infected respiratory fluids are inhaled by people in close contact (i.e., typically within 1 meter) or fall into the mouth, nose, or eyes of close contacts causing infection.[5]
Early in 2023, the World Health Organization (WHO) renewed recommendations for therapeutics in the Therapeutics and COVID-19 Living Guideline.[6] Among the three approved drugs for non-severe COVID-19, only Nirmatrelvir-ritonavir (Paxlovid) is recommended by WHO. In addition, WHO recommends corticosteroid, interleukin-6 inhibitors and baricitinib for severe and critical COVID-19. However, all of these recommended drugs have limited applicability and efficacy.[7,8] Vaccination against COVID-19 has been widely recommended as a preventive method and proven safe and effective. The primary aim of vaccination is to induce antibody production, although the importance of cellular immunity is often overlooked. Early in the pandemic, mRNA, DNA and whole virus-based vaccines were approved by WHO for emergency use and widely applied globally; however, there are now more than 300 vaccine candidates in different stages of pre-clinical or clinical trials.
During vaccine development, the whole or specific parts of a pathogen are selected as antigens and used to stimulate production of antibodies that can identify and neutralize the virus once infection accurs.[9] The antigen-coding gene of the SARS-CoV-2 spike (S) protein was selected as the main component of the developed mRNA and DNA-based viral vector vaccines. The mutation sites on S proteins can prevent antigen recognition and evade the immune system, reducing the effectiveness of vaccines. Therefore, the continuous emergence of new variants with more mutation sites on the S protein poses a significant threat to vaccine effectiveness. The numbers of COVID-19 infections are still increasing as there are ongoing COVID-19 outbreaks in multiple countries, despite the majority of these populations being vaccinated. Thankfully, the current COVID-19 fatality rate is lower than it was during the early stages of the pandemic.[10].
2. SARS-CoV-2 composition
The SARS-CoV-2 virus is composed of a core containing genetic material (i.e., positive-sense single-strand RNA (+ssRNA)) covered by a protein-based capsid. The genome of SARS-CoV-2 is approximately 30 kb with 10 functional open reading frames (ORFs).[11] ORF1a and ORF1b occupy almost two-thirds of the whole genome sequence (about 20 kb) and are located near the 5'-cap end, while the other ORFs are close to 3'- poly(A) tail and code structural and accessory proteins.[12] All proteins encoded by the +ssRNA can be divided into three groups according to their functions: 16 non-structural proteins (NSPs), four structural proteins and nine accessory proteins (Figure 1).
2.1. Structural proteins
The complete SARS-CoV-2 virion contains RNA and four structural proteins: spike (S), envelope (E), membrane (M) and nucleocapsid (N) proteins (Figure 2). Trimeric S protein mainly consists of subunit 1 (S1) and 2 (S2) with the furin cleavage site located between the two subunits. The whole protein structure begins with a signal peptide and ends with a transmembrane domain and cytoplasmic tail. Subunit 1, consisting of an N-terminal domain (NTD) and a receptor binding domain (RBD), mainly facilitates host cell recognition and receptor binding. Prior to viral entry into cells, the receptor binding motif (RBM) in the RBD interacts with angiotensin-converting enzyme 2 (ACE2) on the host cell surface.[13] The main function of S2 is membrane fusion facilitated by three functional domains that include the fusion peptide and heptad repeat 1 and 2 (HR1 and HR2) domains. The E protein has 75 amino acid residues, making it the smallest viral structural protein. Its overall structure consists of a five-helix bundle with a stick-shaped, dehydrated, narrow pore that contains a bipartite channel. Longitudinally, the structure is composed of a short hydrophilic N-terminal transmembrane (TM) domain linked with a large hydrophobic region, followed by a hydrophilic C-terminal domain. The protein functions include assembly and release of new virions, and the specific homopentameric structure plays major role in viral pathogenicity.[14,15,16]
The most abundant and conserved structural protein in SARS-CoV-2 is the M protein. Composed of 222 amino acids, the M protein consists of an 19 amino acid ecto-domain at N-terminal domain, a long C-terminal endo-domain with 123 amino acid residues and three transmembrane helices (TMH1, TMH2, and TMH3) with 19, 25, and 25 amino acid residues, respectively.[17] With the help of N protein, the M protein is primarily responsible for virus assembly and membrane budding.[18,19,20,21,22] In addition, interactions between M protein dimers induce conformational changes that influence virus assembly.[22] The N protein (419 amino acids) contains three conserved domains. The N- and C-terminal domains are predicted to be the β-strand, although the C-terminal domain also contains short helices. The link region between the two folded domains is known as the RNA-binding domain that is responsible for binding to the viral RNA genome.[23,24] In addition to being involved in viral RNA packaging as the structural protein, the N protein also promotes virion assembly and improves viral transcription efficiency.
2.2. Non-structural proteins
Non-structural SARS-CoV-2 proteins are produced following cleavage of the replicase polyprotein, which is generated from ORF 1a and ORF 1b. Some SARS-CoV-2 non-structural protein functions have been predicted based on the functions of analogous conserved proteins in SARS-CoV. In addition to functioning as enzymes, some non-structural SARS-CoV-2 proteins interact with other non-structural proteins and are involved in membrane remodeling, RNA replication and transcription (Table 1).[25,26,27,28,29,30,31,32,33,34,35,36,37]
2.3. Accessory factors
Eleven SARS-CoV-2 proteins have been designated as accessory factors involved in a variety of functions, including inhibition of host immune responses, regulation of apoptosis and early evolution of the virus. Similar to predicting non-structural protein functions, the functions of accessory SARS-CoV-2 proteins have also been predicted based on their functions in SARS-CoV and other relevant coronaviruses, such as MERS-CoV. Compared with non-structural proteins, accessory factors are more variable between coronaviruses. The mutations of some accessory proteins have been associated with pathogenesis and increasing viral transmissibility.[12,38]
3. Angiotensin-converting enzyme 2
Angiotensin-converting enzyme 2 (ACE2) is a receptor for the SARS-CoV-2 S protein and widely expressed in multiple human tissues and organs, allowing the virus to enter and replicate in the lungs, intestines, kidney, gallbladder and heart.[39] The S protein has another target receptor on human host cell surfaces – the leucine rich repeat containing 15 (LRRC15) receptor which was identified as an inhibitory attachment factor for viral entry.[40] During infection, the S protein binds to ACE2 during the first stage of viral entry into the host cell.[41] Notably, the binding affinity of the SARS-CoV-2 S protein to ACE2 is 10 - 20 times stronger than SARS-CoV S protein to ACE2 and considered the key factor for increasing viral infectivity.[42] Prior to being discovered as a cellular receptor for the SARS coronavirus, ACE2 was identified as the primary enzyme in the renin-angiotensin system[43] – the complex regulatory system responsible for controlling the cardiovascular system and hydroelectrolyte balance.[44] SARS-CoV-2 infection disrupts the renin-angiotensin system by downregulating expression of ACE2,[45] weakening anti-inflammatory protection and leading to multiple organ injury.[46,47,48,49]
4. Mechanism of SARS-CoV-2 infection
Infection begins when the SARS-CoV-2 S protein binds to the ACE2 receptor on host cells and initiates viral entry. The mechanism of infection can be divided into nine steps (Figure 3) beginning with the virus binding to host cells and ending with release of new viral cells. Following recognition of the ACE2 receptor by the S protein, endocytosis and viral membrane fusion within the host cell are the next steps. The viral protein coat is then proteolyzed inducing release of viral RNAs that serve as templates for RNA replication. The +ssRNAs promote translation of the viral replicase protein, known as RNA-dependent RNA polymerase (RdRp). The replicase proteins facilitate synthesis of the negative strand by using the positive strand as a template. The synthesized negative strand enables synthesis of complete RNA. After complete RNA replication, the host cell ribosome is used to express structural and accessory viral proteins – essential components of new viruses.[50] Structural viral proteins synthesized in the cytoplasm accumulate in the endoplasmic reticulum-Golgi compartment and are packed with replicated RNA to form a new virus. The newly formed virus is released by the cell through exocytosis to infect other surrounding host cells. The high demands of viral protein production cause destruction of the host cell endoplasmic reticulum and eventually cell death.[51,52,53] The whole process is repeated in newly infected host cells, causing SARS-CoV-2 infection in the host and COVID-19.
5. Host defence mechanisms against infections
The immune system is a complex network that helps defend the human body against pathogens. This defence system is based on innate and adaptive immunity. Non-pathogen specific innate immunity is composed of physical and chemical barriers that act as the first line of defence to prevent pathogens from entering the human body. Physical barriers include skin, cilia, mucosa and their secretions; however, some pathogens evade these physical barriers and enter the human body, activating the second line of defence that involves release of chemical defence signals and mobilisation of protective functional cells. Natural killer (NK) cells and phagocytic cells play major roles in chemical defence mechanisms. Complement proteins also participate in these defence systems. Unfortunately, non-pathogen specific innate immunity is unable to prevent and resolve infection in many cases. In contrast, adaptive immunity is highly pathogen specific and effective, although response time is longer compared to innate immunity. After pathogen recognition by the innate system, adaptive immune responses targeted to the specific pathogen antigens are triggered, initiating pathogen clearance and activating immunologic memory that can rapidly initiate strong humoral (antibody-based) and cellular (cytotoxic T lymphocyte-based) responses when the body encounters the same antigen again.[54,55,56] Adaptive immunity involves a complex network of immune cells and signalling molecules.
5.1. Host defence against SARS-CoV-2
Innate immunity plays an important role in controlling SARS-CoV-2 infection by limiting viral entry, translation, replication and assembly, facilitating recognition and clearance of infected cells and promoting adaptive immunity. Antigen-presenting cells (APCs), such as dendritic cells and macrophages, recognise the SARS-CoV-2 virus or pathogen-associated molecular patterns through pattern recognition receptors on the cell surface. Following recognition, antigens or pathogens enter APCs thorough endocytosis[57,58] and are presented to naive CD8+ T cells by corresponding major histocompatibility complex class I (MHC I) or to naive CD4+ T cells by MHC II.[59] There are two subsets of CD4+ T cells: T helper cells type 1 (Th1) and T helper cells type 2 (Th2) that release Th1 and Th2 cytokines, respectively. Th1 cytokines mainly stimulate CD8+ T cells to promote cellular immune responses and Th2 cytokines act on B cells to enhance humoral immune responses.[60-62] CD8+ cytotoxic T lymphocytes (CTLs) are responsible for killing and clearing infected cells, while B cells differentiate into memory B cells and plasma cells. Plasma cells produce antibodies that recognize specific antigens to prevent the infection and memory B cells can differentiate into plasma cells following future stimulation by the same antigens (Figure 4).
6. Vaccines
Vaccines play a crucial role in preventing infection and transmission of diseases. Vaccines typically consist of a pathogen or its fragments that stimulate adaptive immune responses, induce antibody production and activate cellular immunity, including cytotoxic T lymphocytes (CTLs).
6.1. Whole pathogen vaccines
Traditional whole pathogen vaccines contain inactivated or attenuated pathogens. Attenuation greatly reduces the capacity of pathogens to reproduce and lowers the risk of reversion to a virulent stage.[63] However, attenuated whole pathogen vaccines can produce infection under certain circumstances and exhibit some toxicity, inducing undesired immune responses (e.g., excessive inflammation). Inactivated vaccines contain whole pathogens that have been killed and cannot replicate. While there is no risk of reversion to a virulent stage, inactivated whole pathogen vaccines exhibit similar disadvantageous to attenuated vaccines by being less immunogenic than weakened microorganism-based vaccines.[64] Therefore, to achieve desired immune response, whole pathogen vaccines typically require more than one dose.
6.2. Subunit vaccines
Subunit vaccines contain antigenic fragments of pathogens, such as proteins,[65] peptides[62] or polysaccharides,[66,67]that can elicit protective immune responses. Compared to traditional whole pathogen vaccines, subunit vaccines decrease the risks of side-effects and are safer to use in immunosuppressed patients.[68,69] In addition, subunit vaccines do not require cultivation, making them more suitable for large-scale production than whole pathogen vaccines and reducing risks associated with biohazardous materials.[68,69] However, reducing the size of antigenic components can lead to decreased immunogenicity. Therefore, adjuvants and delivery systems are needed to enhance immune responses elicited by subunit vaccines.[70] As a result, a wide range of adjuvants and delivery systems have been developed, each with their own advantages and limitations.[71,72,73]
6.3. Genetic vaccines
Genetic vaccines are third generation vaccines where the core antigenic components are genetic material (i.e., mRNA or DNA)[74] capable of expressing antigens. The genetic material is delivered to human cells that produce target proteins as antigens to stimulate an immune response.[75] The mRNA vaccine is a new type of genetic vaccine that has been developed in recent years and often uses both non-replicating mRNA and self-amplifying RNA in the vaccine design. Non-replicating and self-amplifying RNA produce pathogen proteins using host cells. In addition, self-amplifying RNA encodes viral replication machinery that facilitates amplification of intracellular RNA and more robust protein production.[76] Initial development of mRNA vaccines was hindered by technical obstacles, including inherent structural instability of mRNA, low mRNA delivery efficiency and the potential of mRNA vaccines to induce severe inflammation in the human body. Several strategies have been employed to overcome these obstacles, such as genetically engineering mRNA to optimise the coding sequence, modifying purification methods to efficiently remove contaminating double-stranded RNA (dsRNA) and employing new materials that can efficiently deliver mRNAs and protect them from decomposition.[77,78] Modifying mRNA structure increases mRNA stability and translation efficiency while reducing immunogenicity.[79] In addition, lipidic, polymeric and peptide delivery systems can protect and deliver encapsulated mRNA into cells.[80,81]
DNA vaccines contain DNA that encodes target proteins and delivery vectors that enable vaccine components to enter the cell nucleus where DNA is transcribed into mRNA for protein biosynthesis.[74,82] Compared with RNA vaccines that require specific cold storage conditions, DNA vaccines are more stable for transportation and can be stored at 2-8 Celsius degree.[83] DNA vaccines can also induce both B and T cell immune responses; however, transportation of DNA to the nucleus presents a significantly greater challenge compared to delivery of RNA to the cytoplasm. To improve the effectiveness and safety of DNA vaccines, several improvements have included optimizing the structure of DNA constructs and delivery vectors.[84] Various DNA structures, including circular, linear and closed minimalistic forms, have been employed for vaccine development.[85] A typical circular DNA vaccine construct is plasmid DNA containing a gene encoding an antigen along with a promoter and terminator. Viral vectors have been widely used for genetic vaccine delivery and consist of a fragment of the target pathogen gene and a deactivated virus, unrelated to the targeted pathogen, as a carrier.[86] These carriers have disadvantages, like toxicity and propensity to induce immunological reactions, that may lead to premature elimination of the vaccine before reaching its target. For example, adenovirus is a typical vector with a highly immunogenic capsid that can trigger strong immune responses and severe inflammatory reactions,[87] particularly following systemic administration of large doses.[88,89] However, severity of these reactions can be reduced by genomic modification of the vector.[88]
7. Vaccines against SARS-CoV-2
A wide variety of SARS-CoV-2 vaccines have been approved worldwide to either prevent COVID-19 infection or at least reduce disease severity. WHO lists four types of COVID-19 vaccines approved for human use: mRNA vaccines, DNA-based viral vector vaccines, inactivated whole pathogen vaccines and protein subunit vaccines (Table 2).
7.1. mRNA vaccines
The two most widely utilized mRNA vaccines are Pfizer-BioNTech (Comirnaty) and Moderna (Spikevax) COVID-19 vaccines. These vaccines are administered through a two-dose regimen and designed to prevent the SARS-CoV-2 S protein from binding to ACE2 receptors on host cells, blocking viral entry. These vaccines consist of nucleoside-modified mRNA encoding the SARS-CoV-2 S protein packaged within synthetic, cationic lipid nanoparticles (containing polyethylene glycol (PEG)) (Table S1).[90,91,92] Notably, PEG-lipids enhance delivery efficacy and improve nanoparticle stability.[91,93,94]
7.2. DNA-based viral vector vaccines
Three DNA-based viral vector vaccines have been approved by WHO: Janssen COVID-19, CONVIDECIA COVID-19 and Vaxzevria. Janssen COVID-19 vaccine is a single-dose vaccine that utilizes the recombinant non-replicating vector adenovirus type 26. CONVIDECIA COVID-19 is another single-dose vaccine that utilizes a modified, non-replicating adenovirus type 5 as its viral vector, while Vaxzevria consists of the non-replicating chimpanzee adenovirus ChAdOx and requires a booster dose. These viral vectors deliver genetic material encoding a stabilized version of the S protein to trigger an immune response against SARS-CoV-2.
7.3. Inactivated whole pathogen vaccines
Four traditional inactivated whole pathogen vaccines have been approved by WHO and are produced by purification of chemically inactivated SARS-CoV-2 cultured in a susceptible cell line.[64,95] However, production of inactivated vaccines requires high biosafety level facilities, as cultivation of live infectious viruses and incomplete inactivation pose a risk of infection to personnel and the virus escaping from the facility. [95] These inactivated vaccines are usually adjuvanted with alum to improve immunogenicity (for example in CoronaVac, BBIBP-CorV and VLA2001 vaccines).[96]
7.4. Protein subunit vaccines
Two protein-based subunit COVID-19 vaccines has been approved by WHO: Nuvaxovid and Corbevax. Notably, Nuvaxovid is the first certified protein-based subunit vaccine that can confer protection against the different S proteins of SARS-CoV-2 variants. Novaxovid contains recombinant SARS-CoV-2 S protein nanoparticles, Matrix-M as the adjuvant and 40-nm cage-like nanoparticles composed of saponins, cholesterol and phospholipids.[97]
8. Mutations and SARS-CoV-2 variants
Viral mutations are found in a wide variety of viruses and caused by substitutions, deletions or insertions of non-synonymous nucleotides in protein-coding genome sequences. Deleterious mutations do not strongly influence virulency as mutated viruses are often quickly eliminated. Neutral mutations are relatively safe for virus and host as they do not change viral properties; however, certain mutations induce adaptive changes that increase viral infectivity and toxicity. Genetic mutations, and resulting variants, have been reported in SARS-CoV-2 since the beginning of pandemic in 2020. Variants have been classified by WHO into three categories: variant of interest (VOI), variant of concern (VOC) and variant under monitoring (VUM). Variant classifications differ between organizations, for example the Centers for Disease Control and Prevention classify variants based on global impact.
8.1. Variants of concern
Variants of concern (VOCs) exhibit increased transmissibility or virulence and negatively impact COVID-19 epidemiology and clinical presentation of disease, limiting the efficacy of public health measures or available diagnostics, vaccines and therapeutics (Table 3). The WHO has implemented various measures to address possible VOCs, including comparative assessments, laboratory investigations and sharing of virus isolates. For identified VOCs, primary actions include metadata sharing of complete genome sequences, field investigations and laboratory assessments. Since March 2023, Omicron parent lineages (i.e., BA.1, BA.2, BA.4/BA.5) and descendent lineages (XBB.1.5) were classified separately by WHO as VOCs and VOIs to better identify different Omicron sub lineages.
8.2. Variants of interest
Variants of interest (VOIs) contain mutations known or predicted to cause significant transmission in multiple countries and epidemiological impacts on global public health. To respond to potential VOIs, WHO has described several primary actions including comparative assessment of variants, sharing virus isolates and information on relevant cases and monitoring and tracking the global spread. Previously circulating VOIs known to pose a reduced risk to global public health are listed and continuously monitored and evaluated. As of September 2023, circulating VOIs include EG.5, XBB.1.5 and XBB.1.16 from the XBB.1sub-lineages with S protein mutations.
8.3. Variants under monitoring
Variants under monitoring (VUMs) are SARS-CoV-2 variants with unclear phenotypic or epidemiological impacts that may be associated with future risks to global public health. All VUMs currently circulating are from the BA.2 sub-lineage with S protein mutations.
8.4. Variants and mutation trends
The frequency of amino acid mutations in SARS-CoV-2, particularly in RBD, is consistently increasing over time[109,110] causing newer variants to mutate faster. The main changes in viral phenotype are pathogenicity, infectivity, transmissibility and antigenicity.[111] Notably, mutations that increase viral infectivity exhibit greater dissemination and supplant less infectious viral phenotypes. Recombination has also been recently reported in newly emerging Omicron variants. Genetic recombination is the exchange of genetic material between objects that originate from distinct lineages. For example, XD – also designated as “Deltacron”, contains genomes from Delta (AY.4) and Omicron (BA.1).[112] Recombination events can also occur within the same lineages, as exemplified by recombination of the Omicron XE variant through sibling lineages of Omicron (BA.1 and BA.2). In general, mutations are prevalent among viruses as they evolve and are subjected to natural selection. During this progression, detrimental changes are eliminated and adaptive mutations are preserved. However, when mutations accumulate, variants deviate more noticeably from original and previously prevalent strains, creating unexpected challenges in the development of viral drugs and amplifying the complexity of infection management.
9. Impacts of mutations
Mutations can alter the fitness and enhance the infectivity and pathogenicity of the SARS-CoV-2 virus. The SARS-CoV-2 S protein plays a crucial role in facilitating viral entry into the host cell, making the S protein a primary target of mutations that can directly impact viral characteristics. Several S protein mutation sites have been identified and found to be associated with the significant viral feature changes that increase infectivity and transmissibility of SARS-CoV-2.
9.1. Mutations and viral characteristic changes
The RBD, particularly the RBM, is the core part of the S protein that directly binds to ACE2 on host cells. Some mutations in the RBM can induce significant changes in SARS-CoV-2 phenotype. For example, the S protein N439K mutation within the RBM was investigated early in the pandemic as this mutation enhances binding affinity of the S protein to the ACE2 receptor and also reduces the neutralizing activity of some antibodies, including polyclonal and some neutralizing monoclonal antibodies, in sera from recovered patients. Diminished neutralization capacity of antibodies is considered an early manifestation of immune escape (described later in 9.2).[113,114] Another mutation in the RBM, V483A, replaces a critical amino acid residue slightly changing the secondary S protein structure.[115,116] By changing the RBM of the S protein loop region, V483A indirectly affects receptor binding of SARS-CoV-2[115] and increases affinity of the S protein for ACE2, making this variant more infectious.[117]
Some mutation sites outside of the RBD also changes variant characteristics. For example, the D614G mutation replaces the 614th aspartic acid (SD614) of the S protein with glycine (SG614),[118,119,120] decreasing S1 release, increasing S protein incorporation into pseudovirions and increasing viral stability.[121,122] The D614G mutation also creates a new serine protease cleavage site in the S protein, significantly increasing viral infectivity of ACE2-expressing cells.[118] In addition to viral transmissibility and infectivity being impacted by mutations, some mutations can also impact other properties of the virus. For example, the Y453F mutation not only enhances infectivity and transmissibility, but is also resistant to convalescent sera, reducing the effectiveness of vaccines.[123] Mutations also occur in other structural proteins (Table 4), non-structural proteins and accessory factors. These mutations also alter viral properties with some associated with changes in variant nature. For example, I76F and L84S mutations in ORF8 directly impact protein–protein interactions with MHC-I[124] and disrupt antigen presentation and replication of the host interferon pathway, enhancing viral pathogenicity.[125] There are over 4000 mutations in the S protein;[126] however, only representative mutations are described in this review (and shown in Table 4). In general, mutations in viral proteins, particularly in the S protein, can strongly impact viral infectivity, virulence and immunogenicity and therefore require continuous monitoring.
9.2. Mutations cause immune escape
The phenomenon known as immune escape, also referred to as immune evasion or antigenic escape, occurs when the host immune system fails to identify foreign antigens, preventing the immune system from initiating a response. This phenomenon directly correlates with pathogen (e.g., virus) evolution and survival. The RBM in the RBD is a key part of the S protein that directly binds to ACE2; therefore, more mutations in the RBM enhance immune evasion properties of these variants (Table 4). [128,132,133,134,135,136,137,138] For instance, it has been proposed that the D614G mutation can evade antibody neutralisation.[111,149] Mutations in the E484 S protein residue can also evade antibody neutralization, including E484K mutations present in Beta and Gamma lineages, [150,151,152] E484A mutations present in Omicron variants,[153,154] and E484Q widely distributed in the Delta lineages.[155] However, the E484D mutation exhibits a relatively diminished capacity for immune evasion, showing resistance to only particular antibodies.[156]
Mutations in proteins other than the S protein also cause immune evasion. Mutations in SARS-CoV-2 accessory proteins, such as mutations in ORF3 and ORF6, can perturb host innate immune responses and are therefore implicated in immune evasion.[157] Non-structural Nsp1 protein is considered as a major immune evasion factor of SARS-CoV-2 as it blocks host antiviral defence proteins by interfering with cellular translation machinery.[158] Notably, a deletion in the coding region (Δ500-532) of Nsp1 reportedly triggers even stronger immune escape of the variant.[159]
9.3. Immune escape reduces vaccine effectiveness
To date, vaccination has been the most effective medical intervention against COVID-19; however, mutations can impact antibody neutralization and reduce vaccine effectiveness.[134] A recent meta-analysis compared the impact of VOCs on effectiveness of the most widely used vaccines targeted to the original SARS-CoV-2, including Pfizer, Moderna, AstraZeneca, Johnson, Sinovac, Sinopharm and Novavax (Figure 5).[160] Decreased vaccine effectiveness weakens protection and creates greater public health challenges through the persistence and recurrence of COVID-19 outbreaks. To evaluate changes in vaccine effectiveness related to immune escape of variants, several comparative assessments of antibody neutralization in the sera from vaccinated individuals have been conducted.[134]
9.3.1. Impact of immune escape on inactivated vaccine efficacy
The Sinovac COVID-19 vaccine is discussed here as a representative of inactivated vaccines. In a 2021 study, sera were collected 14 days after two doses of Sinovac and used to measure antibody neutralizing activity against wild-type SARS-CoV-2 and variant forms. Compared with the antibody neutralizing activity against the wild-type virus, antibody neutralizing activity against Beta and Gamma variants was 5.3-, and 3.9-fold less, respectively.[161] Similarly, a more extensive study evaluated Sinovac vaccine effectiveness against VOCs and also showed reductions in sera antibody neutralizing activity by 2.9-, 5.5-, 4.3-, 3.4- and 12.5-fold against Alpha, Beta, Gamma, Delta and Omicron variants, respectively.[162,163] Another inactivated vaccine, the Sinopharm COVID-19 vaccine, has also exhibited reduced neutralization capacity against VOCs including Beta, Delta and Omicron variants with 6,1.9 and 11.2-fold reductions observed compared to the original virus.[164]
9.3.2. Impact of immune escape on subunit vaccine efficacy
Novavax COVID-19 vaccine is the only protein-based subunit vaccine certified by WHO. To evaluate effectiveness of Novavax against immune-escape related variants, sera was collected from individuals 14 days after vaccination with two doses of Novavax and used in antibody neutralization assays. Findings showed 8.1-, 41- and 30-fold reductions in neutralization capacity against Beta, Omicron BA.1, and Omicron BA.4/BA.5 variants compared to the strain with the D614G mutation.[165]
9.3.3. Impact of immune escape on genetic vaccine efficacy
SARS-CoV-2 variants containing immune-escape related mutations also reduce the effectiveness of genetic vaccines such as Moderna and Pfizer. Effectiveness of the Moderna vaccine against VOIs and VOCs, except Omicron, was evaluated in a test negative case-control study. The comparison was based on vaccine effectiveness against infection 14 days after the second dose. Results showed that effectiveness against infection with the delta variant was 86.7% (95% confidence interval (CI): 84.3% to 88.7%), significantly lower than effectiveness against infection with the Alpha variant (98.4%, 95% CI: 96.9% to 99.1%).[166] Compared with other variants, Delta variants with more immune escape related mutations further reduced vaccine effectiveness.[166] Another study also explored Moderna vaccine effectiveness against Delta and Omicron variants 14–90 days after the second vaccination. Findings showed that vaccine effectiveness against infection with Omicron variants (44.0%,95% CI: 35.1 to 51.6%) was lower than vaccine effectiveness against infection with Delta variants (80.2%, 95% CI: 68.2 to 87.7%).[167]
Effectiveness of the Pfizer COVID-19 vaccine, another widely used mRNA vaccine, has also been tested by determining the neutralizing titers against the original virus and VOCs (except the Omicron variant) in sera collected 14 days after the second dose. Compared to the original virus, results showed the following fold reductions in neutralizing titers for different variants: Alpha 1.7 (95% CI: 1.2–2.1), Gamma 2.3 (95% CI: 1.6–3), Beta 10.4 (95% CI: 6.4–14.4) and Delta 2.1 (95% CI: 1.7–2.5).[168] Effectiveness of two doses of the vaccine in preventing hospitalizations for variants was 85% (95% CI: 82% to 88%) against the Alpha variant, 85% (95% CI: 83% to 87%) against the Delta variant and 65% (95% CI: 51% to 75%) against the Omicron variant.[169]
Another problem associated with immune escape by variants is the decreased duration of protection provided by vaccines. A comprehensive literature review comparing the duration of effectiveness provided by Pfizer, Moderna and AstraZeneca demonstrated the impact of two variants with immune escape mutations, Delta and Omicron, on the quick decline in vaccine efficacy.[170] Vaccine efficacy was evaluated against Delta (B.1.617.2) and Omicron (B.1.1.529) variants in the short- (i.e., less 28 days after the second dose) and long-term (i.e., over 91 days after the second dose) and showed that vaccination protection over longer periods was significantly weaker (Figure 6).
9.4. Booster
Most marketed vaccines, except the Johnson single-dose vaccine, were originally designed to be two-dose regimes. However, due to declined efficacy against variants, especially Omicron, a COVID-19 vaccine booster doses were recommended by WHO and other government institutes. A booster is an extra dose administered after the vaccination regime (i.e., one or two doses) has been provided. Booster doses proved to be effective, at least to a certain extent, against Omicron variants.[171] There are two types of boosters: homologous and heterologous. Homologous boosters utilize the same vaccine administered as an additional dose, while heterologous boosters use a different vaccine for the additional immunization. Notably, as more sub-lineages of the Omicron variant emerge, updated bivalent vaccines are also being used as boosters.
9.4.1. Homologous booster
In a test-negative case–control study involving 2,663,549 participants, effectiveness of the Pfizer booster against symptomatic disease caused by the Omicron (B.1.1.529) was explored. Vaccine effectiveness was 67.2% (95% CI: 66.5 to 67.8) at 2 to 4 weeks after the Pfizer booster, compared with primary vaccination effectiveness of 65.5% (95% CI: 63.9 to 67.0); therefore, the booster vaccination helped maintain short-term vaccine effectiveness similar to the primary vaccine. However, like the primary vaccination strategy, effectiveness of the booster also decreased to 45.7% (95% CI: 44.7 to 46.7) over 10 weeks.[172] The Moderna mRNA vaccine booster efficacy was assessed by measuring neutralization antibody titers. Results showed that neutralization was enhanced by approximately 3.6-fold by a 100 μg booster after 2 weeks, compared to the neutralization titer measured 4 weeks after the second dose of the vaccine.[173]
During the period of the pandemic when the Omicron variant predominated, effectiveness of the Johnson vaccine against laboratory-confirmed COVID-19–associated emergency department or urgent care cases were 24% with one dose and 54% following administration of a homologous booster.[174] In the same study, vaccine effectiveness of single and booster strategies against laboratory-confirmed COVID-19–associated hospitalizations were 31% and 67%, again proving that homologous boosters provide higher protection than a single dose.[174] A regional study in Turkey among healthcare workers evaluated RBD immunoglobulin G (IgG) levels after homologous Sinovac booster administration and showed an 8.7-fold increase in antibody levels 4 months after the second dose.[175] Evidence shows that homologous booster administrations help confer protection against SARS-CoV-2, benefitting public health.[176] However, a persistent issue remains as efficacy of vaccinations diminishes steadily over time.
9.3.2. Heterologous booster
Another strategy to reduce the effect of immune evasion involves heterologous boosters. After primary immunization with two doses of Sinovac vaccine, homologous (i.e., Sinovac vaccine) and heterologous boosters (i.e., original monovalent Pfizer and AstraZeneca vaccines) were administered. Effectiveness of the homologous booster against hospitalisation and death was 59·3% (95% CI: 51·5%–65·9%) and 62·7% (95% CI: 44·9%–74·7%), respectively. However, heterologous boosters enhanced vaccine effectiveness more than homologous boosters with the Pfizer booster being 86·6% (95% CI: 83·6%–89·1%) effective against hospitalisation and 90·7% (95% CI: 82·2%–95·1%) effective against death. The heterologous AstraZeneca booster was slightly more effective than the Pfizer booster producing 93·0% (95% CI: 91·9%–93·9%) and 94·7% (95% CI: 92·5%–96·3%) effectiveness against hospitalisation and death, respectivly.[177] A similar comparative study evaluated anti-RBD IgG levels after a 2-dose Sinovac vaccination regimen with a homologous booster (i.e., Sinovac) and a heterologous booster (i.e., original monovalent Pfizer vaccine) and showed that anti-RBD IgG levels increased 8.7-fold and 104.8-fold respectively.[175]
Another study investigated booster effectiveness against Omicron variants in a population immunized with primary two-doses of AstraZeneca vaccine. Effectiveness of the primary vaccines was lost 25 weeks following the second dose. A Pfizer booster restored protection to 62.4% (95% CI: 61.8%–63.0%) while a Moderna booster restored protection to 70.1% (95% CI: 69.5%–70.7%) 2–4 weeks following immunization. In addition, effectiveness of the booster vaccines in the same population increased from 8.8% (95% CI, 7.0 to 10.5) over 25 weeks to 67.2% (95% CI: 66.5%–67.8%) after the monovalent Pfizer booster and 73.9% (95% CI: 73.1%–74.6%) after the monovalent Moderna booster (2–4 weeks following the booster).[172] To determine effectiveness of a heterologous fourth dose (i.e., one dose of the original monovalent Moderna vaccine after three doses of original monovalent Pfizer vaccine), the level of Omicron specific neutralizing antibodies was measured. Peak antibody titers after the fourth dose were similar to the peak antibody response following the third dose, suggesting that a heterologous fourth dose only restores immunity to peak levels, rather than boost immunity.[178]
9.3.3. Bivalent vaccines against Omicron variants
Effectiveness of homologous and heterologous boosters has decreased as new Omicron sub-variants continue to emerge.[179] To mitigate the threat of new variants, new bivalent vaccines are developed. Compared to the original monovalent vaccines, bivalent vaccines are based on both the original SARS-CoV-2 strain and Omicron variants. Bivalent omicron-containing boosters have been recommended as new heterologous boosters by multiple health institutions, including European Medicines Agency, Therapeutic Goods Administration and U.S. Food and Drug Administration. Initial bivalent vaccines were designed against BA.1 subvariant; however, as BA.4/BA.5 gradually replaced BA.1 and became the main circulating variants worldwide, the bivalent BA.4/5 vaccine was updated (Table S2).[180,181,182]
10. The future of COVID-19 vaccines
The major limitation of existing COVID-19 vaccines is poor efficacy against SARS-CoV-2 variants. Several approaches have been utilized to overcome this challenge including boosters, seasonal vaccination and novel vaccines utilising conserved antigen or antigens. The booster strategy for COVID-19 vaccination evolved from an initial monovalent immunisation to a bivalent approach where a different vaccine is used for the subsequent immunisation. However, boosters typically involved vaccines against old variants and only a small portion of produced antibodies could recognize new virus strains, making this strategy poorly and only temporarily effective.
An alternative approach involves cyclic production of new vaccines based on “updated” antigens that allow for continual viral mutation – an identical strategy to the current approach for controlling the spread of flu viruses. It is important to note that seasonal flu vaccines often exhibit moderate efficacy as their design is largely based on predicting what the predominant strain will be in the next flu season. Given the apparent seasonality of COVID-19 transmission, this approach is also the most feasible, albeit imperfect.
In theory, the most promising approach to overcome vaccination inefficacy against variants with immune escape mutations is substituting current non-conserved antigens with highly conserved alternatives. As previously stated, COVID-19 vaccine development mostly focuses on the SARS-CoV-2 S protein which exhibits a high propensity for mutation. However, other SARS-CoV-2 proteins may also be valid targets for vaccine development. The N protein sequence of SARS-CoV-2 has a 90.5% identity with SARS-CoV N protein, suggesting conservation.[183] Notably, the SARS-CoV N protein is also antigenic,[184] making this protein a promising antigen for vaccine developemnt.[185] Combining N and S proteins within a single vaccine has been suggested to reduce the impact of mutations on vaccine effectiveness.[185] With the help of immunoinformatic methods, a multi-epitope-based peptide vaccine was designed based on S and N proteins.[186] However, these vaccine candidates have not yet been tested in vitro or in vivo. Similarly, the bioinformatics analysis employed to design an N protein-based multi-epitope vaccine that can generate both humoral and cellular immune responses,[187] has not been confirmed in vitro or in vivo. Furthermore, Crooke, S. N., et, al. developed a computational workflow to identify and analyse the T- and B-cell epitopes derived from M, S and N proteins.[188] To date, this antigen replacement strategy has only been confirmed by bioinformatics analysis and still requires further experimental verification. Finally, it is worth noting that influenza A virus infection promotes SARS-CoV-2 infection and is associated with increased expression levels of ACE2 receptors.[189] This mechanism could also be explored to produced more effective COVID-19 vaccines.[190]
11. Conclusion
The COVID-19 pandemic has caused a significant number of illnesses and fatalities on a global scale. Interactions between the spike protein of SARS-CoV-2 and ACE2 receptors are the fundamental basis for viral infection and vaccine development. Current vaccines confer some protection, although vaccine effectiveness against variants has decreased due to immune escape mutations. Among the variants, Omicron and its most recent variant Kraken, exhibit the strongest capacity for immune escape, significantly reducing vaccine effectiveness. The efficacy of several techniques is currently being investigated to combat SARS-CoV-2, including booster strategies, the development of refreshed or seasonal COVID-19 vaccines and the substitution of antigenic components in vaccines with conserved antigens. However, all current strategies have limitations and are unable to overcome immune evasion exhibited by SARS-CoV-2 variants, so further innovative research is needed to mitigate these ongoing challenges.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Funding
This work was supported by the Australian Research Council grant (Discovery Project DP21010280).
References
- Cascella, M.; Rajnik, M.; Aleem, A.; Dulebohn, S.C.; Di Napoli, R. Features, evaluation, and treatment of coronavirus (COVID-19). 2020.
- Zhu, Z.; Lian, X.; Su, X.; Wu, W.; Marraro, G.A.; Zeng, Y. From SARS and MERS to COVID-19: a brief summary and comparison of severe acute respiratory infections caused by three highly pathogenic human coronaviruses. Respiratory Research 2020, 21, 224. [CrossRef]
- Pascarella, G.; Strumia, A.; Piliego, C.; Bruno, F.; Del Buono, R.; Costa, F.; Scarlata, S.; Agrò, F.E. COVID-19 diagnosis and management: a comprehensive review. Journal of internal medicine 2020, 288, 192-206. [CrossRef]
- World Health Organization. Transmission of SARS-CoV-2: implications for infection prevention precautions: scientific brief, 09 July 2020; World Health Organization: 2020.
- Organization, W.H. Mask use in the context of COVID-19: interim guidance, 1 December 2020; World Health Organization: 2020.
- Organization, W.H. Therapeutics and COVID-19: living guideline, 13 January 2023; World Health Organization: 2023.
- Vegivinti, C.T.R.; Evanson, K.W.; Lyons, H.; Akosman, I.; Barrett, A.; Hardy, N.; Kane, B.; Keesari, P.R.; Pulakurthi, Y.S.; Sheffels, E. Efficacy of antiviral therapies for COVID-19: a systematic review of randomized controlled trials. BMC Infectious Diseases 2022, 22, 107. [CrossRef]
- Siemieniuk, R.; Rochwerg, B.; Agoritsas, T.; Lamontagne, F.; Leo, Y.-S.; Macdonald, H.; Agarwal, A.; Zeng, L.; Lytvyn, L.; Appiah, J.A. A living WHO guideline on drugs for covid-19. Bmj 2020 (Last updated 10 Nov 2023), 370, m3379.
- Jeyanathan, M.; Afkhami, S.; Smaill, F.; Miller, M.S.; Lichty, B.D.; Xing, Z. Immunological considerations for COVID-19 vaccine strategies. Nature Reviews Immunology 2020, 20, 615-632. [CrossRef]
- Zhou, C.-M.; Qin, X.-R.; Yan, L.-N.; Jiang, Y.; Yu, X.-J. Global trends in COVID-19. Infectious Medicine 2022, 1, 31-39. [CrossRef]
- Naqvi, A.A.T.; Fatima, K.; Mohammad, T.; Fatima, U.; Singh, I.K.; Singh, A.; Atif, S.M.; Hariprasad, G.; Hasan, G.M.; Hassan, M.I. Insights into SARS-CoV-2 genome, structure, evolution, pathogenesis and therapies: Structural genomics approach. Biochim Biophys Acta Mol Basis Dis 2020, 1866, 165878. [CrossRef]
- Yadav, R.; Chaudhary, J.K.; Jain, N.; Chaudhary, P.K.; Khanra, S.; Dhamija, P.; Sharma, A.; Kumar, A.; Handu, S. Role of Structural and Non-Structural Proteins and Therapeutic Targets of SARS-CoV-2 for COVID-19. Cells 2021, 10. [CrossRef]
- Lan, J.; Ge, J.; Yu, J.; Shan, S.; Zhou, H.; Fan, S.; Zhang, Q.; Shi, X.; Wang, Q.; Zhang, L. Structure of the SARS-CoV-2 spike receptor-binding domain bound to the ACE2 receptor. nature 2020, 581, 215-220.
- Mandala, V.S.; McKay, M.J.; Shcherbakov, A.A.; Dregni, A.J.; Kolocouris, A.; Hong, M. Structure and drug binding of the SARS-CoV-2 envelope protein transmembrane domain in lipid bilayers. Nat Struct Mol Biol 2020, 27, 1202-1208. [CrossRef]
- Schoeman, D.; Fielding, B.C. Coronavirus envelope protein: current knowledge. Virol J 2019, 16, 69. [CrossRef]
- EA, J.A.; Jones, I.M. Membrane binding proteins of coronaviruses. Future Virol 2019, 14, 275-286. [CrossRef]
- Thomas, S. The Structure of the Membrane Protein of SARS-CoV-2 Resembles the Sugar Transporter SemiSWEET. Pathog Immun 2020, 5, 342-363. [CrossRef]
- Opstelten, D.J.; Raamsman, M.J.; Wolfs, K.; Horzinek, M.C.; Rottier, P.J. Envelope glycoprotein interactions in coronavirus assembly. J Cell Biol 1995, 131, 339-349. [CrossRef]
- Fehr, A.R.; Perlman, S. Coronaviruses: an overview of their replication and pathogenesis. Methods Mol Biol 2015, 1282, 1-23. [CrossRef]
- Escors, D.; Ortego, J.; Laude, H.; Enjuanes, L. The membrane M protein carboxy terminus binds to transmissible gastroenteritis coronavirus core and contributes to core stability. J Virol 2001, 75, 1312-1324. [CrossRef]
- Narayanan, K.; Maeda, A.; Maeda, J.; Makino, S. Characterization of the coronavirus M protein and nucleocapsid interaction in infected cells. J Virol 2000, 74, 8127-8134. [CrossRef]
- Zhang, Z.; Nomura, N.; Muramoto, Y.; Ekimoto, T.; Uemura, T.; Liu, K.; Yui, M.; Kono, N.; Aoki, J.; Ikeguchi, M. Structure of SARS-CoV-2 membrane protein essential for virus assembly. Nature communications 2022, 13, 4399.
- Gao, T.; Gao, Y.; Liu, X.; Nie, Z.; Sun, H.; Lin, K.; Peng, H.; Wang, S. Identification and functional analysis of the SARS-COV-2 nucleocapsid protein. BMC Microbiol 2021, 21, 58. [CrossRef]
- Satarker, S.; Nampoothiri, M. Structural Proteins in Severe Acute Respiratory Syndrome Coronavirus-2. Arch Med Res 2020, 51, 482-491. [CrossRef]
- Huang, C.; Lokugamage, K.G.; Rozovics, J.M.; Narayanan, K.; Semler, B.L.; Makino, S. SARS coronavirus nsp1 protein induces template-dependent endonucleolytic cleavage of mRNAs: viral mRNAs are resistant to nsp1-induced RNA cleavage. PLoS Pathog 2011, 7, e1002433. [CrossRef]
- Cornillez-Ty, C.T.; Liao, L.; Yates, J.R., 3rd; Kuhn, P.; Buchmeier, M.J. Severe acute respiratory syndrome coronavirus nonstructural protein 2 interacts with a host protein complex involved in mitochondrial biogenesis and intracellular signaling. J Virol 2009, 83, 10314-10318. [CrossRef]
- Lei, J.; Kusov, Y.; Hilgenfeld, R. Nsp3 of coronaviruses: Structures and functions of a large multi-domain protein. Antiviral Res 2018, 149, 58-74. [CrossRef]
- Moustaqil, M.; Ollivier, E.; Chiu, H.P.; Van Tol, S.; Rudolffi-Soto, P.; Stevens, C.; Bhumkar, A.; Hunter, D.J.B.; Freiberg, A.N.; Jacques, D.; et al. SARS-CoV-2 proteases PLpro and 3CLpro cleave IRF3 and critical modulators of inflammatory pathways (NLRP12 and TAB1): implications for disease presentation across species. Emerg Microbes Infect 2021, 10, 178-195. [CrossRef]
- Sun, X.; Liu, Y.; Huang, Z.; Xu, W.; Hu, W.; Yi, L.; Liu, Z.; Chan, H.; Zeng, J.; Liu, X.; et al. SARS-CoV-2 non-structural protein 6 triggers NLRP3-dependent pyroptosis by targeting ATP6AP1. Cell Death Differ 2022, 29, 1240-1254. [CrossRef]
- Ricciardi, S.; Guarino, A.M.; Giaquinto, L.; Polishchuk, E.V.; Santoro, M.; Di Tullio, G.; Wilson, C.; Panariello, F.; Soares, V.C.; Dias, S.S.G.; et al. The role of NSP6 in the biogenesis of the SARS-CoV-2 replication organelle. Nature 2022, 606, 761-768. [CrossRef]
- Reshamwala, S.M.S.; Likhite, V.; Degani, M.S.; Deb, S.S.; Noronha, S.B. Mutations in SARS-CoV-2 nsp7 and nsp8 proteins and their predicted impact on replication/transcription complex structure. J Med Virol 2021, 93, 4616-4619. [CrossRef]
- Peng, Q.; Peng, R.; Yuan, B.; Zhao, J.; Wang, M.; Wang, X.; Wang, Q.; Sun, Y.; Fan, Z.; Qi, J.; et al. Structural and Biochemical Characterization of the nsp12-nsp7-nsp8 Core Polymerase Complex from SARS-CoV-2. Cell Rep 2020, 31, 107774. [CrossRef]
- de, O.A.J.; Pinheiro, S.; Zamora, W.J.; Alves, C.N.; Lameira, J.; Lima, A.H. Structural, energetic and lipophilic analysis of SARS-CoV-2 non-structural protein 9 (NSP9). Sci Rep 2021, 11, 23003. [CrossRef]
- Bouvet, M.; Lugari, A.; Posthuma, C.C.; Zevenhoven, J.C.; Bernard, S.; Betzi, S.; Imbert, I.; Canard, B.; Guillemot, J.C.; Lécine, P.; et al. Coronavirus Nsp10, a critical co-factor for activation of multiple replicative enzymes. J Biol Chem 2014, 289, 25783-25796. [CrossRef]
- Wang, W.; Zhou, Z.; Xiao, X.; Tian, Z.; Dong, X.; Wang, C.; Li, L.; Ren, L.; Lei, X.; Xiang, Z.; et al. SARS-CoV-2 nsp12 attenuates type I interferon production by inhibiting IRF3 nuclear translocation. Cell Mol Immunol 2021, 18, 945-953. [CrossRef]
- Yuen, C.K.; Lam, J.Y.; Wong, W.M.; Mak, L.F.; Wang, X.; Chu, H.; Cai, J.P.; Jin, D.Y.; To, K.K.; Chan, J.F.; et al. SARS-CoV-2 nsp13, nsp14, nsp15 and orf6 function as potent interferon antagonists. Emerg Microbes Infect 2020, 9, 1418-1428. [CrossRef]
- Vithani, N.; Ward, M.D.; Zimmerman, M.I.; Novak, B.; Borowsky, J.H.; Singh, S.; Bowman, G.R. SARS-CoV-2 Nsp16 activation mechanism and a cryptic pocket with pan-coronavirus antiviral potential. Biophys J 2021, 120, 2880-2889. [CrossRef]
- Redondo, N.; Zaldívar-López, S.; Garrido, J.J.; Montoya, M. SARS-CoV-2 accessory proteins in viral pathogenesis: knowns and unknowns. Frontiers in Immunology 2021, 2698.
- Bourgonje, A.R.; Abdulle, A.E.; Timens, W.; Hillebrands, J.L.; Navis, G.J.; Gordijn, S.J.; Bolling, M.C.; Dijkstra, G.; Voors, A.A.; Osterhaus, A.D.; et al. Angiotensin-converting enzyme 2 (ACE2), SARS-CoV-2 and the pathophysiology of coronavirus disease 2019 (COVID-19). J Pathol 2020, 251, 228-248. [CrossRef]
- Song, J.; Chow, R.D.; Peña-Hernández, M.A.; Zhang, L.; Loeb, S.A.; So, E.-Y.; Liang, O.D.; Ren, P.; Chen, S.; Wilen, C.B. LRRC15 inhibits SARS-CoV-2 cellular entry in trans. Plos Biology 2022, 20, e3001805.
- Zhou, P.; Yang, X.L.; Wang, X.G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.R.; Zhu, Y.; Li, B.; Huang, C.L.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270-273. [CrossRef]
- Wrapp, D.; Wang, N.; Corbett, K.S.; Goldsmith, J.A.; Hsieh, C.L.; Abiona, O.; Graham, B.S.; McLellan, J.S. Cryo-EM structure of the 2019-nCoV spike in the prefusion conformation. Science 2020, 367, 1260-1263. [CrossRef]
- Tipnis, S.R.; Hooper, N.M.; Hyde, R.; Karran, E.; Christie, G.; Turner, A.J. A human homolog of angiotensin-converting enzyme: cloning and functional expression as a captopril-insensitive carboxypeptidase. Journal of Biological Chemistry 2000, 275, 33238-33243.
- Santos, R.A.S.; Sampaio, W.O.; Alzamora, A.C.; Motta-Santos, D.; Alenina, N.; Bader, M.; Campagnole-Santos, M.J. The ACE2/Angiotensin-(1-7)/MAS Axis of the Renin-Angiotensin System: Focus on Angiotensin-(1-7). Physiol Rev 2018, 98, 505-553. [CrossRef]
- Datta, P.K.; Liu, F.; Fischer, T.; Rappaport, J.; Qin, X. SARS-CoV-2 pandemic and research gaps: Understanding SARS-CoV-2 interaction with the ACE2 receptor and implications for therapy. Theranostics 2020, 10, 7448.
- Oudit, G.Y.; Kassiri, Z.; Jiang, C.; Liu, P.P.; Poutanen, S.M.; Penninger, J.M.; Butany, J. SARS-coronavirus modulation of myocardial ACE2 expression and inflammation in patients with SARS. Eur J Clin Invest 2009, 39, 618-625. [CrossRef]
- Glowacka, I.; Bertram, S.; Herzog, P.; Pfefferle, S.; Steffen, I.; Muench, M.O.; Simmons, G.; Hofmann, H.; Kuri, T.; Weber, F.; et al. Differential downregulation of ACE2 by the spike proteins of severe acute respiratory syndrome coronavirus and human coronavirus NL63. J Virol 2010, 84, 1198-1205. [CrossRef]
- Ni, W.; Yang, X.; Yang, D.; Bao, J.; Li, R.; Xiao, Y.; Hou, C.; Wang, H.; Liu, J.; Yang, D.; et al. Role of angiotensin-converting enzyme 2 (ACE2) in COVID-19. Crit Care 2020, 24, 422. [CrossRef]
- Tang, Q.; Wang, Y.; Ou, L.; Li, J.; Zheng, K.; Zhan, H.; Gu, J.; Zhou, G.; Xie, S.; Zhang, J. Downregulation of ACE2 expression by SARS-CoV-2 worsens the prognosis of KIRC and KIRP patients via metabolism and immunoregulation. International journal of biological sciences 2021, 17, 1925.
- Poduri, R.; Joshi, G.; Jagadeesh, G. Drugs targeting various stages of the SARS-CoV-2 life cycle: Exploring promising drugs for the treatment of Covid-19. Cell Signal 2020, 74, 109721. [CrossRef]
- Boopathi, S.; Poma, A.B.; Kolandaivel, P. Novel 2019 coronavirus structure, mechanism of action, antiviral drug promises and rule out against its treatment. J Biomol Struct Dyn 2021, 39, 3409-3418. [CrossRef]
- Masters, P.S. The molecular biology of coronaviruses. Adv Virus Res 2006, 66, 193-292. [CrossRef]
- van Hemert, M.J.; van den Worm, S.H.; Knoops, K.; Mommaas, A.M.; Gorbalenya, A.E.; Snijder, E.J. SARS-coronavirus replication/transcription complexes are membrane-protected and need a host factor for activity in vitro. PLoS Pathog 2008, 4, e1000054. [CrossRef]
- Kurtz, J. Memory in the innate and adaptive immune systems. Microbes Infect 2004, 6, 1410-1417. [CrossRef]
- Sun, J.C.; Beilke, J.N.; Lanier, L.L. Adaptive immune features of natural killer cells. Nature 2009, 457, 557-561. [CrossRef]
- Braciale, T.J.; Sun, J.; Kim, T.S. Regulating the adaptive immune response to respiratory virus infection. Nat Rev Immunol 2012, 12, 295-305. [CrossRef]
- Diamond, M.S.; Kanneganti, T.D. Innate immunity: the first line of defense against SARS-CoV-2. Nat Immunol 2022, 23, 165-176. [CrossRef]
- Tay, M.Z.; Poh, C.M.; Rénia, L.; MacAry, P.A.; Ng, L.F.P. The trinity of COVID-19: immunity, inflammation and intervention. Nat Rev Immunol 2020, 20, 363-374. [CrossRef]
- Wieczorek, M.; Abualrous, E.T.; Sticht, J.; Álvaro-Benito, M.; Stolzenberg, S.; Noé, F.; Freund, C. Major Histocompatibility Complex (MHC) Class I and MHC Class II Proteins: Conformational Plasticity in Antigen Presentation. Front Immunol 2017, 8, 292. [CrossRef]
- Sette, A.; Crotty, S. Adaptive immunity to SARS-CoV-2 and COVID-19. Cell 2021, 184, 861-880. [CrossRef]
- Romagnani, S. Th1 and Th2 in human diseases. Clin Immunol Immunopathol 1996, 80, 225-235. [CrossRef]
- Skwarczynski, M.; Toth, I. Peptide-based synthetic vaccines. Chem Sci 2016, 7, 842-854. [CrossRef]
- Belete, T.M. Review on up-to-date status of candidate vaccines for COVID-19 disease. Infection and drug resistance 2021, 151-161. [CrossRef]
- Gao, Q.; Bao, L.; Mao, H.; Wang, L.; Xu, K.; Yang, M.; Li, Y.; Zhu, L.; Wang, N.; Lv, Z. Development of an inactivated vaccine candidate for SARS-CoV-2. Science 2020, 369, 77-81.
- Chappell, K.J.; Mordant, F.L.; Li, Z.; Wijesundara, D.K.; Ellenberg, P.; Lackenby, J.A.; Cheung, S.T.; Modhiran, N.; Avumegah, M.S.; Henderson, C.L. Safety and immunogenicity of an MF59-adjuvanted spike glycoprotein-clamp vaccine for SARS-CoV-2: a randomised, double-blind, placebo-controlled, phase 1 trial. The Lancet Infectious Diseases 2021, 21, 1383-1394.
- Hansson, M.; Nygren, P.A.k.; Sta˚ hl, S. Design and production of recombinant subunit vaccines. Biotechnology and applied biochemistry 2000, 32, 95-107.
- Xu, Z.; Moyle, P.M. Bioconjugation approaches to producing subunit vaccines composed of protein or peptide antigens and covalently attached toll-like receptor ligands. Bioconjugate chemistry 2017, 29, 572-586.
- Vartak, A.; Sucheck, S.J. Recent advances in subunit vaccine carriers. Vaccines 2016, 4, 12.
- Skwarczynski, M.; Toth, I. Non-invasive mucosal vaccine delivery: Advantages, challenges and the future. Expert Opinion on Drug Delivery 2020, 17, 435-437.
- Nahar, U.J.; Toth, I.; Skwarczynski, M. Mannose in vaccine delivery. Journal of Controlled Release 2022, 351, 284-300. [CrossRef]
- Foged, C. Subunit vaccines of the future: the need for safe, customized and optimized particulate delivery systems. Therapeutic delivery 2011, 2, 1057-1077. [CrossRef]
- Alharbi, N.; Skwarczynski, M.; Toth, I. The influence of component structural arrangement on peptide vaccine immunogenicity. Biotechnology Advances 2022, 108029. [CrossRef]
- Firdaus, F.Z.; Skwarczynski, M.; Toth, I. Developments in vaccine adjuvants. Vaccine Design: Methods and Protocols, Volume 3. Resources for Vaccine Development 2022, 145-178.
- Acosta-Coley, I.; Cervantes-Ceballos, L.; Tejeda-Benítez, L.; Sierra-Márquez, L.; Cabarcas-Montalvo, M.; García-Espiñeira, M.; Coronell-Rodríguez, W.; Arroyo-Salgado, B. Vaccines platforms and COVID-19: what you need to know. Tropical Diseases, Travel Medicine and Vaccines 2022, 8, 20. [CrossRef]
- Ura, T.; Okuda, K.; Shimada, M. Developments in viral vector-based vaccines. Vaccines 2014, 2, 624-641. [CrossRef]
- Pardi, N.; Hogan, M.J.; Porter, F.W.; Weissman, D. mRNA vaccines — a new era in vaccinology. Nature Reviews Drug Discovery 2018, 17, 261-279. [CrossRef]
- Kariko, K.; Muramatsu, H.; Welsh, F.A.; Ludwig, J.; Kato, H.; Akira, S.; Weissman, D. Incorporation of pseudouridine into mRNA yields superior nonimmunogenic vector with increased translational capacity and biological stability. Mol Ther 2008, 16, 1833-1840. [CrossRef]
- Sahin, U.; Kariko, K.; Tureci, O. mRNA-based therapeutics--developing a new class of drugs. Nat Rev Drug Discov 2014, 13, 759-780. [CrossRef]
- Kim, S.C.; Sekhon, S.S.; Shin, W.R.; Ahn, G.; Cho, B.K.; Ahn, J.Y.; Kim, Y.H. Modifications of mRNA vaccine structural elements for improving mRNA stability and translation efficiency. Mol Cell Toxicol 2022, 18, 1-8. [CrossRef]
- Yi Xue, H.; Guo, P.; Wen, W.-C.; Lun Wong, H. Lipid-based nanocarriers for RNA delivery. Current pharmaceutical design 2015, 21, 3140-3147. [CrossRef]
- Chahal, J.S.; Khan, O.F.; Cooper, C.L.; McPartlan, J.S.; Tsosie, J.K.; Tilley, L.D.; Sidik, S.M.; Lourido, S.; Langer, R.; Bavari, S. Dendrimer-RNA nanoparticles generate protective immunity against lethal Ebola, H1N1 influenza, and Toxoplasma gondii challenges with a single dose. Proceedings of the National Academy of Sciences 2016, 113, E4133-E4142.
- Liu, M.A. A comparison of plasmid DNA and mRNA as vaccine technologies. Vaccines 2019, 7, 37.
- Crommelin, D.J.; Volkin, D.B.; Hoogendoorn, K.H.; Lubiniecki, A.S.; Jiskoot, W. The science is there: key considerations for stabilizing viral vector-based Covid-19 vaccines. Journal of pharmaceutical sciences 2021, 110, 627-634. [CrossRef]
- Narayanan, D.; Djearamane, S.; Fuloria, S.; Kayarohanam, S.; Subramaniyan, V.; Sekar, M.; Fuloria, N.K. A Review on DNA Vaccines in Pre-Clinical Trials Against SARS-CoV-2. Journal of Experimental Biology and Agricultural Sciences 2022, 10, 487-493.
- Shafaati, M.; Saidijam, M.; Soleimani, M.; Hazrati, F.; Mirzaei, R.; Amirheidari, B.; Tanzadehpanah, H.; Karampoor, S.; Kazemi, S.; Yavari, B. A brief review on DNA vaccines in the era of COVID-19. Future Virology 2022, 17, 49-66. [CrossRef]
- Deng, S.; Liang, H.; Chen, P.; Li, Y.; Li, Z.; Fan, S.; Wu, K.; Li, X.; Chen, W.; Qin, Y.; et al. Viral Vector Vaccine Development and Application during the COVID-19 Pandemic. Microorganisms 2022, 10, 1450. [CrossRef]
- SM Wold, W.; Toth, K. Adenovirus vectors for gene therapy, vaccination and cancer gene therapy. Current gene therapy 2013, 13, 421-433.
- Butt, M.H.; Zaman, M.; Ahmad, A.; Khan, R.; Mallhi, T.H.; Hasan, M.M.; Khan, Y.H.; Hafeez, S.; Massoud, E.E.S.; Rahman, M.H.; et al. Appraisal for the Potential of Viral and Nonviral Vectors in Gene Therapy: A Review. Genes (Basel) 2022, 13. [CrossRef]
- Gregory, S.M.; Nazir, S.A.; Metcalf, J.P. Implications of the innate immune response to adenovirus and adenoviral vectors. Future virology 2011, 6, 357-374. [CrossRef]
- Bavli, Y.; Chen, B.-M.; Gross, G.; Hershko, A.; Turjeman, K.; Roffler, S.; Barenholz, Y. Anti-PEG antibodies before and after a first dose of Comirnaty®(mRNA-LNP-based SARS-CoV-2 vaccine). Journal of Controlled Release 2023, 354, 316-322.
- Mabrouk, M.T.; Huang, W.C.; Martinez-Sobrido, L.; Lovell, J.F. Advanced materials for SARS-CoV-2 vaccines. Advanced Materials 2022, 34, 2107781.
- FDA. Overview of COVID-19 Vaccines. Availabe online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/different-vaccines/overview-COVID-19-vaccines.html (accessed on.
- Hou, X.; Zaks, T.; Langer, R.; Dong, Y. Lipid nanoparticles for mRNA delivery. Nature Reviews Materials 2021, 6, 1078-1094. [CrossRef]
- Tenchov, R.; Bird, R.; Curtze, A.E.; Zhou, Q. Lipid nanoparticles─ from liposomes to mRNA vaccine delivery, a landscape of research diversity and advancement. ACS nano 2021, 15, 16982-17015.
- Krammer, F. SARS-CoV-2 vaccines in development. Nature 2020, 586, 516-527.
- Nagy, A.; Alhatlani, B. An overview of current COVID-19 vaccine platforms. Computational and structural biotechnology journal 2021, 19, 2508-2517.
- Keech, C.; Albert, G.; Cho, I.; Robertson, A.; Reed, P.; Neal, S.; Plested, J.S.; Zhu, M.; Cloney-Clark, S.; Zhou, H. Phase 1–2 trial of a SARS-CoV-2 recombinant spike protein nanoparticle vaccine. New England Journal of Medicine 2020, 383, 2320-2332.
- Shalash, A.O.; Azuar, A.; Madge, H.Y.R.; Modhiran, N.; Amarilla, A.A.; Liang, B.; Khromykh, A.A.; Hussein, W.M.; Chappell, K.J.; Watterson, D.; et al. Peptide-Based Vaccine against SARS-CoV-2: Peptide Antigen Discovery and Screening of Adjuvant Systems. Pharmaceutics 2022, 14. [CrossRef]
- Shalash, A.O.; Toth, I.; Skwarczynski, M. The potential of developing a protective peptide-based vaccines against SARS-CoV-2. Drug Dev Res 2022, 83, 1251-1256. [CrossRef]
- Pandey, M.; Ozberk, V.; Eskandari, S.; Shalash, A.O.; Joyce, M.A.; Saffran, H.A.; Day, C.J.; Lepletier, A.; Spillings, B.L.; Mills, J.L. Antibodies to neutralising epitopes synergistically block the interaction of the receptor-binding domain of SARS-CoV-2 to ACE 2. Clinical & Translational Immunology 2021, 10, e1260.
- Shalash, A.O.; Hussein, W.M.; Skwarczynski, M.; Toth, I. Key considerations for the development of safe and effective SARS-CoV-2 subunit vaccine: A peptide-based vaccine alternative. Advanced Science 2021, 8, 2100985.
- Shalash, A.O.; Azuar, A.; Madge, H.Y.; Modhiran, N.; Amarilla, A.A.; Liang, B.; Khromykh, A.A.; Watterson, D.; Young, P.R.; Toth, I. Detection and quantification of SARS-CoV-2 receptor binding domain neutralization by a sensitive competitive ELISA assay. Vaccines 2021, 9, 1493.
- Sanchez-Felipe, L.; Vercruysse, T.; Sharma, S.; Ma, J.; Lemmens, V.; Van Looveren, D.; Arkalagud Javarappa, M.P.; Boudewijns, R.; Malengier-Devlies, B.; Liesenborghs, L. A single-dose live-attenuated YF17D-vectored SARS-CoV-2 vaccine candidate. Nature 2021, 590, 320-325.
- Liu, Y.; Zhang, X.; Liu, J.; Xia, H.; Zou, J.; Muruato, A.E.; Periasamy, S.; Kurhade, C.; Plante, J.A.; Bopp, N.E. A live-attenuated SARS-CoV-2 vaccine candidate with accessory protein deletions. Nature communications 2022, 13, 4337.
- Yoon, W.; Park, Y.; Kim, S.; Bang, I.S. Development of an oral Salmonella-based vaccine platform against SARS-CoV-2. Vaccines 2022, 10, 67.
- Geng, Q.; Tai, W.; Baxter, V.K.; Shi, J.; Wan, Y.; Zhang, X.; Montgomery, S.A.; Taft-Benz, S.A.; Anderson, E.J.; Knight, A.C. Novel virus-like nanoparticle vaccine effectively protects animal model from SARS-CoV-2 infection. PLoS pathogens 2021, 17, e1009897.
- van Riel, D.; de Wit, E. Next-generation vaccine platforms for COVID-19. Nature Materials 2020, 19, 810-812. [CrossRef]
- Rezaei, M.; Nazari, M. New Generation Vaccines for COVID-19 Based on Peptide, Viral Vector, Artificial Antigen Presenting Cell, DNA or mRNA. Avicenna J Med Biotechnol 2022, 14, 30-36. [CrossRef]
- Chavda, V.P.; Bezbaruah, R.; Deka, K.; Nongrang, L.; Kalita, T. The Delta and Omicron variants of SARS-CoV-2: what we know so far. Vaccines 2022, 10, 1926.
- Chugh, A.; Khurana, N.; Verma, K.; Sehgal, I.; Rolta, R.; Vats, P.; Phartyal, R.; Salaria, D.; Kaushik, N.; Choi, E.H. Changing dynamics of SARS-CoV-2: a global challenge. Applied Sciences 2022, 12, 5546.
- Harvey, W.T.; Carabelli, A.M.; Jackson, B.; Gupta, R.K.; Thomson, E.C.; Harrison, E.M.; Ludden, C.; Reeve, R.; Rambaut, A.; Consortium, C.-G.U. SARS-CoV-2 variants, spike mutations and immune escape. Nature Reviews Microbiology 2021, 19, 409-424.
- Chakraborty, C.; Bhattacharya, M.; Sharma, A.R.; Dhama, K. Recombinant SARS-CoV-2 variants XD, XE, and XF: The emergence of recombinant variants requires an urgent call for research–Correspondence. International journal of surgery (London, England) 2022, 102, 106670.
- Thomson, E.C.; Rosen, L.E.; Shepherd, J.G.; Spreafico, R.; da Silva Filipe, A.; Wojcechowskyj, J.A.; Davis, C.; Piccoli, L.; Pascall, D.J.; Dillen, J. The circulating SARS-CoV-2 spike variant N439K maintains fitness while evading antibody-mediated immunity. BioRxiv 2020, 2020.2011. 2004.355842.
- Zhou, W.; Xu, C.; Wang, P.; Luo, M.; Xu, Z.; Cheng, R.; Jin, X.; Guo, Y.; Xue, G.; Juan, L. N439K variant in spike protein alter the infection efficiency and antigenicity of SARS-CoV-2 based on molecular dynamics simulation. Frontiers in cell and developmental biology 2021, 9, 697035.
- Guan, Q.; Sadykov, M.; Nugmanova, R.; Carr, M.J.; Arold, S.T.; Pain, A. The genomic variation landscape of globally-circulating clades of SARS-CoV-2 defines a genetic barcoding scheme. biorxiv 2020, 2020.2004. 2021.054221.
- Ashwaq, O.; Manickavasagam, P.; Haque, S.M. V483A: An emerging mutation hotspot of SARS-CoV-2. Future Virology 2021, 16, 419-429.
- Chen, J.; Wang, R.; Wang, M.; Wei, G.-W. Mutations strengthened SARS-CoV-2 infectivity. Journal of molecular biology 2020, 432, 5212-5226.
- Hu, J.; He, C.-L.; Gao, Q.-Z.; Zhang, G.-J.; Cao, X.-X.; Long, Q.-X.; Deng, H.-J.; Huang, L.-Y.; Chen, J.; Wang, K. D614G mutation of SARS-CoV-2 spike protein enhances viral infectivity. BioRxiv 2020, 2020.2006. 2020.161323.
- Hou, Y.J.; Chiba, S.; Halfmann, P.; Ehre, C.; Kuroda, M.; Dinnon III, K.H.; Leist, S.R.; Schäfer, A.; Nakajima, N.; Takahashi, K. SARS-CoV-2 D614G variant exhibits efficient replication ex vivo and transmission in vivo. Science 2020, 370, 1464-1468.
- Sixto-López, Y.; Correa-Basurto, J.; Bello, M.; Landeros-Rivera, B.; Garzón-Tiznado, J.A.; Montaño, S. Structural insights into SARS-CoV-2 spike protein and its natural mutants found in Mexican population. Scientific Reports 2021, 11, 4659.
- Zhang, L.; Jackson, C.B.; Mou, H.; Ojha, A.; Rangarajan, E.S.; Izard, T.; Farzan, M.; Choe, H. The D614G mutation in the SARS-CoV-2 spike protein reduces S1 shedding and increases infectivity. BioRxiv 2020.
- Zhang, L.; Jackson, C.B.; Mou, H.; Ojha, A.; Peng, H.; Quinlan, B.D.; Rangarajan, E.S.; Pan, A.; Vanderheiden, A.; Suthar, M.S. SARS-CoV-2 spike-protein D614G mutation increases virion spike density and infectivity. Nature communications 2020, 11, 6013.
- Ren, W.; Lan, J.; Ju, X.; Gong, M.; Long, Q.; Zhu, Z.; Yu, Y.; Wu, J.; Zhong, J.; Zhang, R. Mutation Y453F in the spike protein of SARS-CoV-2 enhances interaction with the mink ACE2 receptor for host adaption. PLoS Pathogens 2021, 17, e1010053.
- Zhang, Y.; Chen, Y.; Li, Y.; Huang, F.; Luo, B.; Yuan, Y.; Xia, B.; Ma, X.; Yang, T.; Yu, F. The ORF8 protein of SARS-CoV-2 mediates immune evasion through down-regulating MHC-Ι. Proceedings of the National Academy of Sciences 2021, 118, e2024202118.
- Zhang, Y.; Zhang, J.; Chen, Y.; Luo, B.; Yuan, Y.; Huang, F.; Yang, T.; Yu, F.; Liu, J.; Liu, B. The ORF8 protein of SARS-CoV-2 mediates immune evasion through potently downregulating MHC-I. biorxiv 2020, 2020.2005. 2024.111823.
- Cosar, B.; Karagulleoglu, Z.Y.; Unal, S.; Ince, A.T.; Uncuoglu, D.B.; Tuncer, G.; Kilinc, B.R.; Ozkan, Y.E.; Ozkoc, H.C.; Demir, I.N. SARS-CoV-2 mutations and their viral variants. Cytokine & growth factor reviews 2022, 63, 10-22.
- Ou, J.; Zhou, Z.; Dai, R.; Zhang, J.; Zhao, S.; Wu, X.; Lan, W.; Ren, Y.; Cui, L.; Lan, Q. V367F mutation in SARS-CoV-2 spike RBD emerging during the early transmission phase enhances viral infectivity through increased human ACE2 receptor binding affinity. Journal of virology 2021, 95. [CrossRef]
- Hirabara, S.M.; Serdan, T.D.; Gorjao, R.; Masi, L.N.; Pithon-Curi, T.C.; Covas, D.T.; Curi, R.; Durigon, E.L. SARS-COV-2 variants: differences and potential of immune evasion. Frontiers in cellular and infection microbiology 2022, 11, 1401. [CrossRef]
- Tandel, D.; Gupta, D.; Sah, V.; Harinivas Harshan, K. N440K variant of SARS-CoV-2 has higher infectious fitness. BioRxiv 2021, 2021.2004. 2030.441434.
- Gan, H.H.; Twaddle, A.; Marchand, B.; Gunsalus, K.C. Structural modeling of the SARS-CoV-2 spike/human ACE2 complex interface can identify high-affinity variants associated with increased transmissibility. Journal of Molecular Biology 2021, 433, 167051.
- Sobitan, A.; Mahase, V.; Rhoades, R.; Williams, D.; Liu, D.; Xie, Y.; Li, L.; Tang, Q.; Teng, S. Computational saturation mutagenesis of SARS-CoV-1 spike glycoprotein: Stability, binding affinity, and comparison with SARS-CoV-2. Frontiers in Molecular Biosciences 2021, 8, 784303.
- Weisblum, Y.; Schmidt, F.; Zhang, F.; DaSilva, J.; Poston, D.; Lorenzi, J.C.; Muecksch, F.; Rutkowska, M.; Hoffmann, H.-H.; Michailidis, E. Escape from neutralizing antibodies by SARS-CoV-2 spike protein variants. elife 2020, 9, e61312.
- Deng, X.; Garcia-Knight, M.A.; Khalid, M.M.; Servellita, V.; Wang, C.; Morris, M.K.; Sotomayor-González, A.; Glasner, D.R.; Reyes, K.R.; Gliwa, A.S. Transmission, infectivity, and neutralization of a spike L452R SARS-CoV-2 variant. Cell 2021, 184, 3426-3437. e3428.
- Chakraborty, C.; Sharma, A.R.; Bhattacharya, M.; Lee, S.-S. A detailed overview of immune escape, antibody escape, partial vaccine escape of SARS-CoV-2 and their emerging variants with escape mutations. Frontiers in Immunology 2022, 13, 801522.
- Baum, A.; Fulton, B.O.; Wloga, E.; Copin, R.; Pascal, K.E.; Russo, V.; Giordano, S.; Lanza, K.; Negron, N.; Ni, M. Antibody cocktail to SARS-CoV-2 spike protein prevents rapid mutational escape seen with individual antibodies. Science 2020, 369, 1014-1018.
- Planas, D.; Veyer, D.; Baidaliuk, A.; Staropoli, I.; Guivel-Benhassine, F.; Rajah, M.M.; Planchais, C.; Porrot, F.; Robillard, N.; Puech, J. Reduced sensitivity of SARS-CoV-2 variant Delta to antibody neutralization. Nature 2021, 596, 276-280.
- Alenquer, M.; Ferreira, F.; Lousa, D.; Valério, M.; Medina-Lopes, M.; Bergman, M.-L.; Gonçalves, J.; Demengeot, J.; Leite, R.B.; Lilue, J. Signatures in SARS-CoV-2 spike protein conferring escape to neutralizing antibodies. PLoS pathogens 2021, 17, e1009772.
- Lu, L.; Chu, A.W.-H.; Zhang, R.R.; Chan, W.-M.; Ip, J.D.; Tsoi, H.-W.; Chen, L.-l.; Cai, J.-P.; Lung, D.C.; Tam, A.R. The impact of spike N501Y mutation on neutralizing activity and RBD binding of SARS-CoV-2 convalescent serum. EBioMedicine 2021, 71.
- Borges, V.; Isidro, J.; Cortes-Martins, H.; Duarte, S.; Vieira, L.; Leite, R.; Gordo, I.; Caetano, C.P.; Nunes, B.; Sá, R. On the track of the D839Y mutation in the SARS-CoV-2 Spike fusion peptide: emergence and geotemporal spread of a highly prevalent variant in Portugal. medRxiv 2020, 2020.2008. 2010.20171884.
- Cavallo, L.; Oliva, R. D936Y and other mutations in the fusion core of the SARS-Cov-2 spike protein heptad repeat 1 undermine the Post-Fusion assembly. BioRxiv 2020, 2020.2006. 2008.140152.
- Barrett, C.T.; Neal, H.E.; Edmonds, K.; Moncman, C.L.; Thompson, R.; Branttie, J.M.; Boggs, K.B.; Wu, C.-Y.; Leung, D.W.; Dutch, R.E. Effect of clinical isolate or cleavage site mutations in the SARS-CoV-2 spike protein on protein stability, cleavage, and cell–cell fusion. Journal of Biological Chemistry 2021, 297.
- Rahman, M.S.; Hoque, M.N.; Islam, M.R.; Islam, I.; Mishu, I.D.; Rahaman, M.M.; Sultana, M.; Hossain, M.A. Mutational insights into the envelope protein of SARS-CoV-2. Gene reports 2021, 22, 100997.
- Timmers, L.F.S.M.; Peixoto, J.V.; Ducati, R.G.; Bachega, J.F.R.; de Mattos Pereira, L.; Caceres, R.A.; Majolo, F.; da Silva, G.L.; Anton, D.B.; Dellagostin, O.A. SARS-CoV-2 mutations in Brazil: from genomics to putative clinical conditions. Scientific reports 2021, 11, 11998.
- Mou, K.; Abdalla, M.; Wei, D.Q.; Khan, M.T.; Lodhi, M.S.; Darwish, D.B.; Sharaf, M.; Tu, X. Emerging mutations in envelope protein of SARS-CoV-2 and their effect on thermodynamic properties. Informatics in medicine unlocked 2021, 25, 100675.
- Wu, H.; Xing, N.; Meng, K.; Fu, B.; Xue, W.; Dong, P.; Tang, W.; Xiao, Y.; Liu, G.; Luo, H. Nucleocapsid mutations R203K/G204R increase the infectivity, fitness, and virulence of SARS-CoV-2. Cell host & microbe 2021, 29, 1788-1801. e1786. [CrossRef]
- Rahman, M.S.; Islam, M.R.; Alam, A.R.U.; Islam, I.; Hoque, M.N.; Akter, S.; Rahaman, M.M.; Sultana, M.; Hossain, M.A. Evolutionary dynamics of SARS-CoV-2 nucleocapsid protein and its consequences. Journal of medical virology 2021, 93, 2177-2195.
- Bartolini, B.; Rueca, M.; Gruber, C.E.M.; Messina, F.; Carletti, F.; Giombini, E.; Lalle, E.; Bordi, L.; Matusali, G.; Colavita, F. SARS-CoV-2 phylogenetic analysis, Lazio region, Italy, February–march 2020. Emerging infectious diseases 2020, 26, 1842.
- Troyano-Hernáez, P.; Reinosa, R.; Holguín, Á. Evolution of SARS-CoV-2 envelope, membrane, nucleocapsid, and spike structural proteins from the beginning of the pandemic to September 2020: a global and regional approach by epidemiological week. Viruses 2021, 13, 243. [CrossRef]
- Hu, J.; Peng, P.; Cao, X.; Wu, K.; Chen, J.; Wang, K.; Tang, N.; Huang, A.-l. Increased immune escape of the new SARS-CoV-2 variant of concern Omicron. Cellular & Molecular Immunology 2022, 19, 293-295.
- Lohr, B.; Niemann, D.; Verheyen, J. Bamlanivimab treatment leads to rapid selection of immune escape variant carrying the E484K mutation in a B. 1.1. 7-infected and immunosuppressed patient. Clinical Infectious Diseases 2021, 73, 2144-2145. [CrossRef]
- Jangra, S.; Ye, C.; Rathnasinghe, R.; Stadlbauer, D.; Alshammary, H.; Amoako, A.A.; Awawda, M.H.; Beach, K.F.; Bermúdez-González, M.C.; Chernet, R.L. SARS-CoV-2 spike E484K mutation reduces antibody neutralisation. The Lancet Microbe 2021, 2, e283-e284.
- Jangra, S.; Ye, C.; Rathnasinghe, R.; Stadlbauer, D.; Krammer, F.; Simon, V.; Martinez-Sobrido, L.; Garcia-Sastre, A.; Schotsaert, M.; Group, P.S. The E484K mutation in the SARS-CoV-2 spike protein reduces but does not abolish neutralizing activity of human convalescent and post-vaccination sera. MedRxiv 2021.
- Cui, Z.; Liu, P.; Wang, N.; Wang, L.; Fan, K.; Zhu, Q.; Wang, K.; Chen, R.; Feng, R.; Jia, Z. Structural and functional characterizations of infectivity and immune evasion of SARS-CoV-2 Omicron. Cell 2022, 185, 860-871. e813.
- Vogt, A.-C.S.; Augusto, G.; Martina, B.; Chang, X.; Nasrallah, G.; Speiser, D.E.; Vogel, M.; Bachmann, M.F.; Mohsen, M.O. Increased receptor affinity and reduced recognition by specific antibodies contribute to immune escape of SARS-CoV-2 variant omicron. Vaccines 2022, 10, 743.
- Li, G.; Zhou, Z.; Du, P.; Yu, M.; Li, N.; Xiong, X.; Huang, H.; Liu, Z.; Dai, Q.; Zhu, J. The SARS-CoV-2 spike L452R-E484Q variant in the Indian B. 1.617 strain showed significant reduction in the neutralization activity of immune sera. Precision Clinical Medicine 2021, 4, 149-154. [CrossRef]
- Liu, Z.; VanBlargan, L.A.; Bloyet, L.-M.; Rothlauf, P.W.; Chen, R.E.; Stumpf, S.; Zhao, H.; Errico, J.M.; Theel, E.S.; Liebeskind, M.J. Landscape analysis of escape variants identifies SARS-CoV-2 spike mutations that attenuate monoclonal and serum antibody neutralization. BioRxiv 2020, 2020.2011. 2006.372037.
- Lei, X.; Dong, X.; Ma, R.; Wang, W.; Xiao, X.; Tian, Z.; Wang, C.; Wang, Y.; Li, L.; Ren, L. Activation and evasion of type I interferon responses by SARS-CoV-2. Nature communications 2020, 11, 3810.
- Thoms, M.; Buschauer, R.; Ameismeier, M.; Koepke, L.; Denk, T.; Hirschenberger, M.; Kratzat, H.; Hayn, M.; Mackens-Kiani, T.; Cheng, J. Structural basis for translational shutdown and immune evasion by the Nsp1 protein of SARS-CoV-2. Science 2020, 369, 1249-1255.
- Lin, J.-w.; Tang, C.; Wei, H.-c.; Du, B.; Chen, C.; Wang, M.; Zhou, Y.; Yu, M.-x.; Cheng, L.; Kuivanen, S. Genomic monitoring of SARS-CoV-2 uncovers an Nsp1 deletion variant that modulates type I interferon response. Cell host & microbe 2021, 29, 489-502. e488.
- Zeng, B.; Gao, L.; Zhou, Q.; Yu, K.; Sun, F. Effectiveness of COVID-19 vaccines against SARS-CoV-2 variants of concern: a systematic review and meta-analysis. BMC medicine 2022, 20, 1-15.
- Chen, Y.; Shen, H.; Huang, R.; Tong, X.; Wu, C. Serum neutralising activity against SARS-CoV-2 variants elicited by CoronaVac. The Lancet Infectious Diseases 2021, 21, 1071-1072.
- Wang, Y.; Ma, Y.; Xu, Y.; Liu, J.; Li, X.; Chen, Y.; Chen, Y.; Xie, J.; Xiao, L.; Xiang, Z. Resistance of SARS-CoV-2 Omicron variant to convalescent and CoronaVac vaccine plasma. Emerging Microbes & Infections 2022, 11, 425-428.
- Jin, L.; Li, Z.; Zhang, X.; Li, J.; Zhu, F. CoronaVac: A review of efficacy, safety, and immunogenicity of the inactivated vaccine against SARS-CoV-2. Human Vaccines & Immunotherapeutics 2022, 18, 2096970.
- Ai, J.; Zhang, H.; Zhang, Y.; Lin, K.; Zhang, Y.; Wu, J.; Wan, Y.; Huang, Y.; Song, J.; Fu, Z. Omicron variant showed lower neutralizing sensitivity than other SARS-CoV-2 variants to immune sera elicited by vaccines after boost. Emerging microbes & infections 2022, 11, 337-343.
- Bhiman, J.N.; Richardson, S.I.; Lambson, B.E.; Kgagudi, P.; Mzindle, N.; Kaldine, H.; Crowther, C.; Gray, G.; Bekker, L.-G. Novavax NVX-COV2373 triggers neutralization of Omicron sub-lineages. Scientific Reports 2023, 13, 1222. [CrossRef]
- Bruxvoort, K.J.; Sy, L.S.; Qian, L.; Ackerson, B.K.; Luo, Y.; Lee, G.S.; Tian, Y.; Florea, A.; Aragones, M.; Tubert, J.E. Effectiveness of mRNA-1273 against delta, mu, and other emerging variants of SARS-CoV-2: test negative case-control study. bmj 2021, 375.
- Tseng, H.F.; Ackerson, B.K.; Luo, Y.; Sy, L.S.; Talarico, C.A.; Tian, Y.; Bruxvoort, K.J.; Tubert, J.E.; Florea, A.; Ku, J.H. Effectiveness of mRNA-1273 against SARS-CoV-2 Omicron and Delta variants. Nature medicine 2022, 28, 1063-1071.
- Lustig, Y.; Zuckerman, N.; Nemet, I.; Atari, N.; Kliker, L.; Regev-Yochay, G.; Sapir, E.; Mor, O.; Alroy-Preis, S.; Mendelson, E. Neutralising capacity against Delta (B. 1.617. 2) and other variants of concern following Comirnaty (BNT162b2, BioNTech/Pfizer) vaccination in health care workers, Israel. Eurosurveillance 2021, 26, 2100557. [CrossRef]
- Lauring, A.S.; Tenforde, M.W.; Chappell, J.D.; Gaglani, M.; Ginde, A.A.; McNeal, T.; Ghamande, S.; Douin, D.J.; Talbot, H.K.; Casey, J.D. Clinical severity of, and effectiveness of mRNA vaccines against, covid-19 from omicron, delta, and alpha SARS-CoV-2 variants in the United States: prospective observational study. Bmj 2022, 376.
- Paul, P.; El-Naas, A.; Hamad, O.; Salameh, M.A.; Mhaimeed, N.; Laswi, I.; Abdelati, A.A.; AlAnni, J.; Khanjar, B.; Al-Ali, D. Effectiveness of the pre-Omicron COVID-19 vaccines against Omicron in reducing infection, hospitalization, severity, and mortality compared to Delta and other variants: A systematic review. Human Vaccines & Immunotherapeutics 2023, 19, 2167410. [CrossRef]
- Chenchula, S.; Karunakaran, P.; Sharma, S.; Chavan, M. Current evidence on efficacy of COVID-19 booster dose vaccination against the Omicron variant: A systematic review. Journal of Medical Virology 2022, 94, 2969-2976.
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Rickeard, T.; Gallagher, E.; Gower, C.; Kall, M.; Groves, N.; O’Connell, A.-M. Covid-19 vaccine effectiveness against the Omicron (B. 1.1. 529) variant. New England Journal of Medicine 2022, 386, 1532-1546.
- Atmar, R.L.; Lyke, K.E.; Deming, M.E.; Jackson, L.A.; Branche, A.R.; El Sahly, H.M.; Rostad, C.A.; Martin, J.M.; Johnston, C.; Rupp, R.E. Homologous and heterologous Covid-19 booster vaccinations. New England Journal of Medicine 2022, 386, 1046-1057. [CrossRef]
- Natarajan, K.; Prasad, N.; Dascomb, K.; Irving, S.A.; Yang, D.-H.; Gaglani, M.; Klein, N.P.; DeSilva, M.B.; Ong, T.C.; Grannis, S.J. Effectiveness of homologous and heterologous COVID-19 booster doses following 1 Ad. 26. COV2. S (Janssen [Johnson & Johnson]) vaccine dose against COVID-19–associated emergency department and urgent care encounters and hospitalizations among adults—VISION Network, 10 states, December 2021–March 2022. Morbidity and Mortality Weekly Report 2022, 71, 495.
- Çağlayan, D.; Süner, A.F.; Şiyve, N.; Güzel, I.; Irmak, Ç.; Işik, E.; Appak, Ö.; Çelik, M.; Öztürk, G.; Alp Çavuş, S.; et al. An analysis of antibody response following the second dose of CoronaVac and humoral response after booster dose with BNT162b2 or CoronaVac among healthcare workers in Turkey. J Med Virol 2022, 94, 2212-2221. [CrossRef]
- Thye, A.Y.-K.; Tan, L.T.-H.; Law, J.W.F.; Letchumanan, V. COVID-19 Booster Vaccines Administration in Different Countries. Progress In Microbes & Molecular Biology 2021, 4. [CrossRef]
- Jara, A.; Undurraga, E.A.; Zubizarreta, J.R.; González, C.; Pizarro, A.; Acevedo, J.; Leo, K.; Paredes, F.; Bralic, T.; Vergara, V. Effectiveness of homologous and heterologous booster doses for an inactivated SARS-CoV-2 vaccine: a large-scale prospective cohort study. The Lancet Global Health 2022, 10, e798-e806.
- Regev-Yochay, G.; Gonen, T.; Gilboa, M.; Mandelboim, M.; Indenbaum, V.; Amit, S.; Meltzer, L.; Asraf, K.; Cohen, C.; Fluss, R. 4th dose COVID mRNA vaccines’ immunogenicity & efficacy against omicron VOC. MedRxiv 2022, 2022.2002. 2015.22270948.
- Bowen, J.E.; Addetia, A.; Dang, H.V.; Stewart, C.; Brown, J.T.; Sharkey, W.K.; Sprouse, K.R.; Walls, A.C.; Mazzitelli, I.G.; Logue, J.K.; et al. Omicron spike function and neutralizing activity elicited by a comprehensive panel of vaccines. Science 2022, 377, 890-894. [CrossRef]
- Kawasuji, H.; Morinaga, Y.; Tani, H.; Saga, Y.; Yamada, H.; Yoshida, Y.; Takegoshi, Y.; Kaneda, M.; Murai, Y.; Kimoto, K. Efficacy of the wild-type/Omicron BA. 1 bivalent vaccine as the second booster dose against Omicron BA. 2 and BA. 5. medRxiv 2022, 2022.2011. 2015.22282328. [CrossRef]
- Zou, J.; Kurhade, C.; Patel, S.; Kitchin, N.; Tompkins, K.; Cutler, M.; Cooper, D.; Yang, Q.; Cai, H.; Muik, A. Improved neutralization of Omicron BA. 4/5, BA. 4.6, BA. 2.75. 2, BQ. 1.1, and XBB. 1 with bivalent BA. 4/5 vaccine. BioRxiv 2022, 2022.2011. 2017.516898.
- Scheaffer, S.M.; Lee, D.; Whitener, B.; Ying, B.; Wu, K.; Liang, C.-Y.; Jani, H.; Martin, P.; Amato, N.J.; Avena, L.E. Bivalent SARS-CoV-2 mRNA vaccines increase breadth of neutralization and protect against the BA. 5 Omicron variant in mice. Nature medicine 2023, 29, 247-257.
- Zeng, W.; Liu, G.; Ma, H.; Zhao, D.; Yang, Y.; Liu, M.; Mohammed, A.; Zhao, C.; Yang, Y.; Xie, J. Biochemical characterization of SARS-CoV-2 nucleocapsid protein. Biochemical and biophysical research communications 2020, 527, 618-623.
- Chow, S.C.; Ho, C.Y.; Tam, T.T.; Wu, C.; Cheung, T.; Chan, P.K.; Ng, M.H.; Hui, P.; Ng, H.-K.; Au, D.M. Specific epitopes of the structural and hypothetical proteins elicit variable humoral responses in SARS patients. Journal of clinical pathology 2006, 59, 468-476. [CrossRef]
- Grifoni, A.; Sidney, J.; Zhang, Y.; Scheuermann, R.H.; Peters, B.; Sette, A. A sequence homology and bioinformatic approach can predict candidate targets for immune responses to SARS-CoV-2. Cell host & microbe 2020, 27, 671-680. e672.
- Rouzbahani, A.K.; Kheirandish, F.; Hosseini, S.Z. Design of a multi-epitope-based peptide vaccine against the S and N proteins of SARS-COV-2 using immunoinformatics approach. Egypt J Med Hum Genet 2022, 23, 16. [CrossRef]
- Kumar, J.; Qureshi, R.; Sagurthi, S.R.; Qureshi, I.A. Designing of nucleocapsid protein based novel multi-epitope vaccine against SARS-COV-2 using immunoinformatics approach. International journal of peptide research and therapeutics 2021, 27, 941-956. [CrossRef]
- Crooke, S.N.; Ovsyannikova, I.G.; Kennedy, R.B.; Poland, G.A. Immunoinformatic identification of B cell and T cell epitopes in the SARS-CoV-2 proteome. Scientific reports 2020, 10, 14179.
- Bai, L.; Zhao, Y.; Dong, J.; Liang, S.; Guo, M.; Liu, X.; Wang, X.; Huang, Z.; Sun, X.; Zhang, Z. Coinfection with influenza A virus enhances SARS-CoV-2 infectivity. Cell research 2021, 31, 395-403.
- Zhang, L.; Jiang, Y.; He, J.; Chen, J.; Qi, R.; Yuan, L.; Shao, T.; Zhao, H.; Chen, C.; Chen, Y. Intranasal influenza-vectored COVID-19 vaccine restrains the SARS-CoV-2 inflammatory response in hamsters. Nature Communications 2023, 14, 4117.
Figure 1.
Genomic structure of SARS-CoV-2.
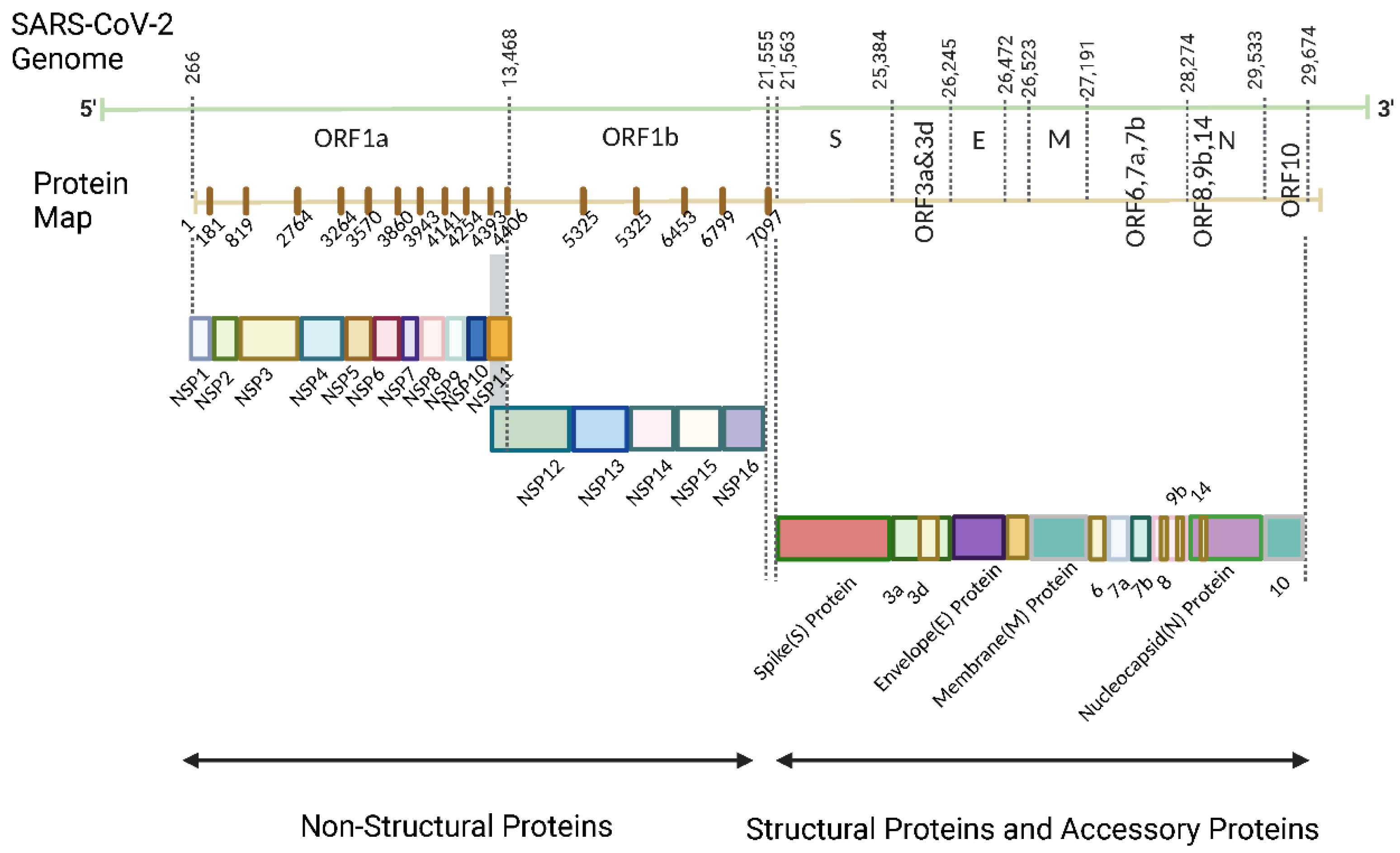
Figure 2.
Structure of SARS-CoV-2.
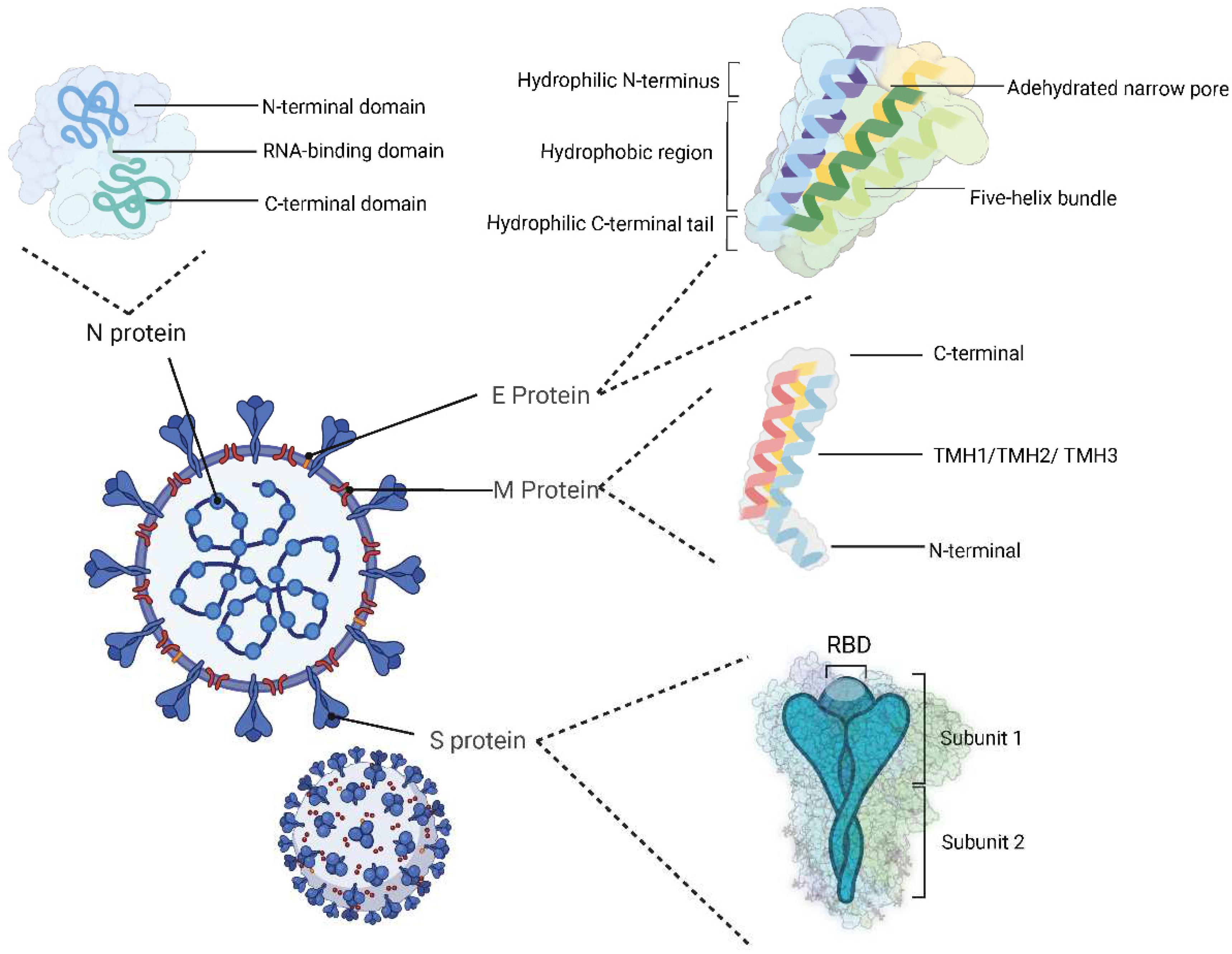
Figure 3.
Mechanism of SARS-CoV-2 infection in the host cells. The SARS-CoV-2 S protein binds to the ACE2 receptor on the surface of host cells, the S1/S2 subunits are cleaved by the proprotein convertase furin. The S2’ cleavage site is exposed and further cleaved by the host cell protease transmembrane serine protease 2. Then, the viral cell entry via membrane fusion or endocytosis occurs, and RNA is released to the cytoplasm. Then ribosomes from host cells are employed for the translation of RNA-dependent RNA polymerase before the viral RNA replication. RNA genome coding structural proteins are obtained. The structural proteins are translated in the host endoplasmic reticulum. Together with the new viral RNA and N proteins, the new virions are assembled in the ER-Golgi intermediate compartment (ERGIC) of host cells, finally the new SARS-CoV-2 viruses are released outside the host cells through exocytosis. .
Figure 3.
Mechanism of SARS-CoV-2 infection in the host cells. The SARS-CoV-2 S protein binds to the ACE2 receptor on the surface of host cells, the S1/S2 subunits are cleaved by the proprotein convertase furin. The S2’ cleavage site is exposed and further cleaved by the host cell protease transmembrane serine protease 2. Then, the viral cell entry via membrane fusion or endocytosis occurs, and RNA is released to the cytoplasm. Then ribosomes from host cells are employed for the translation of RNA-dependent RNA polymerase before the viral RNA replication. RNA genome coding structural proteins are obtained. The structural proteins are translated in the host endoplasmic reticulum. Together with the new viral RNA and N proteins, the new virions are assembled in the ER-Golgi intermediate compartment (ERGIC) of host cells, finally the new SARS-CoV-2 viruses are released outside the host cells through exocytosis. .
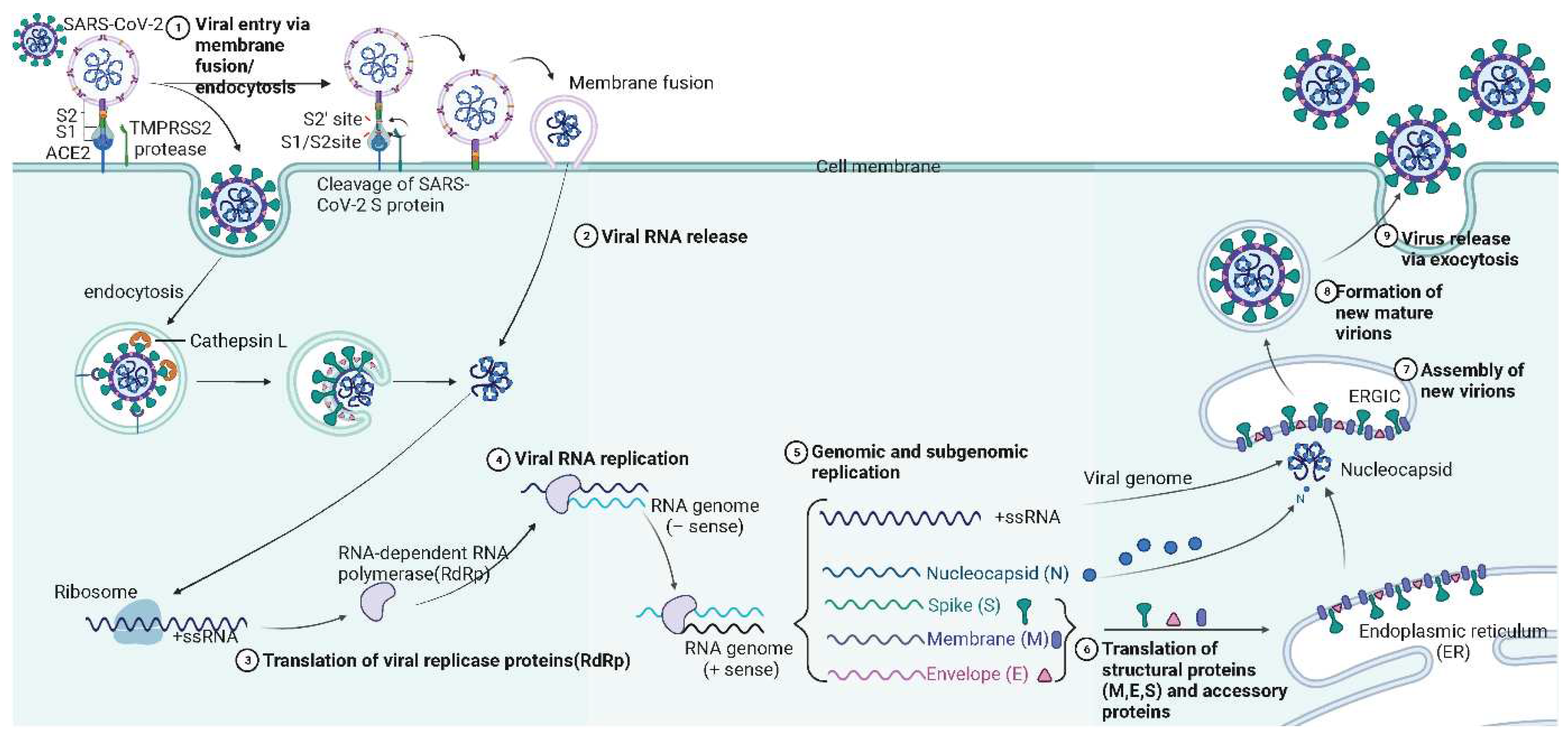
Figure 4.
The simplified schematic representation of antiviral immunity.
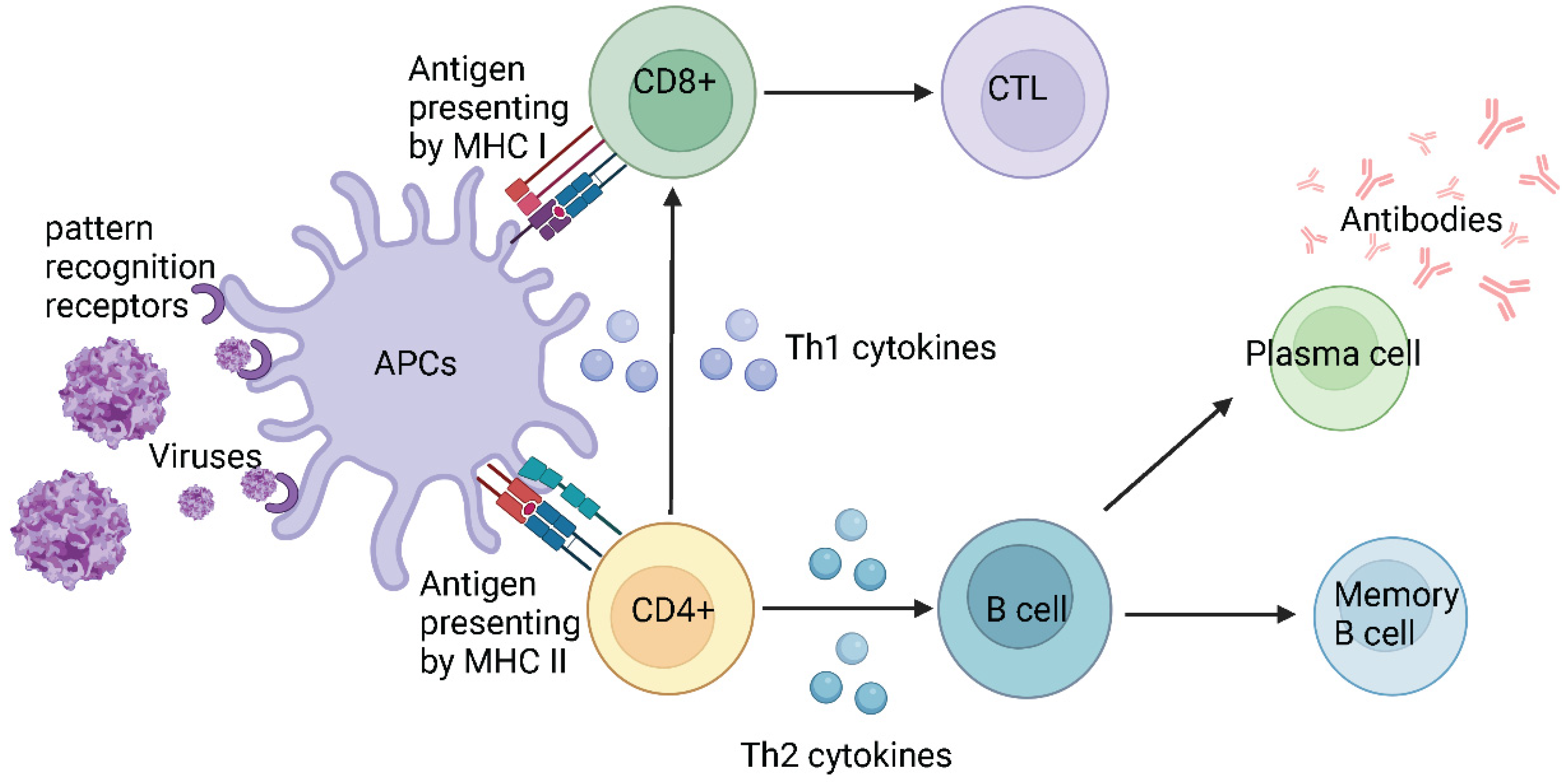
Figure 5.
The impact of VOCs on summary vaccine effectiveness. The summary vaccine effectiveness is based on the Meta-analysis, the analysis (20 cohort studies with 52,782,321 participants, and 26 case-control studies with 2,584,732 cases) involves 11 vaccines (8 WHO certified vaccines: Moderna, Pfizer, AstraZenac, Johnson, Novavax, Sinopharm, Sinovac, Covaxin; 3 vaccines in development: SCB-2019, CVnCoV and HB02).
Figure 5.
The impact of VOCs on summary vaccine effectiveness. The summary vaccine effectiveness is based on the Meta-analysis, the analysis (20 cohort studies with 52,782,321 participants, and 26 case-control studies with 2,584,732 cases) involves 11 vaccines (8 WHO certified vaccines: Moderna, Pfizer, AstraZenac, Johnson, Novavax, Sinopharm, Sinovac, Covaxin; 3 vaccines in development: SCB-2019, CVnCoV and HB02).
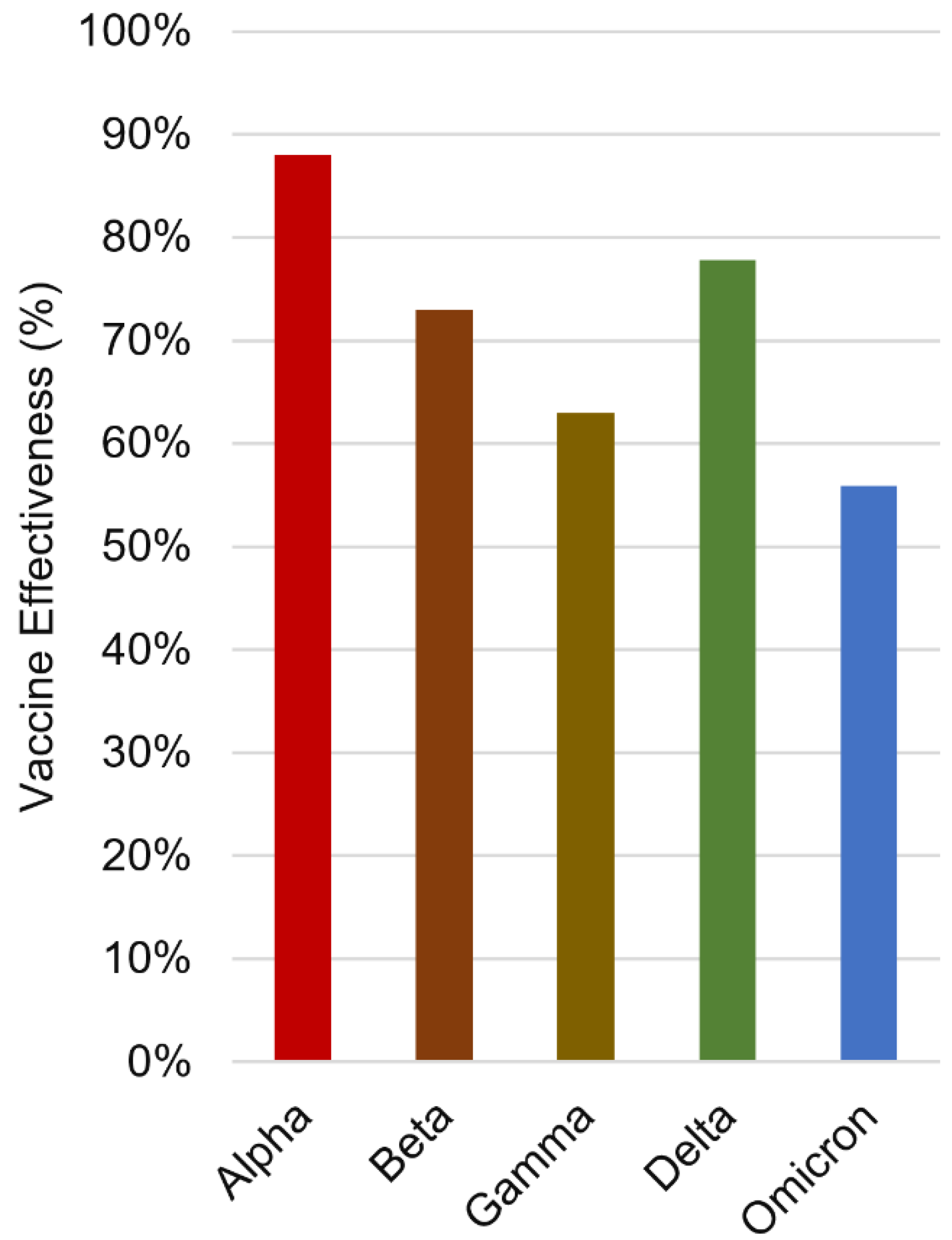
Figure 6.
Pfizer, Moderna and AstraZeneca vaccine effectiveness against Delta (green bars) and Omicron (blue bars) variants. Short term vaccine efficacy is marked in green/blue colour, while long-term efficacy in light green/blue colour.
Figure 6.
Pfizer, Moderna and AstraZeneca vaccine effectiveness against Delta (green bars) and Omicron (blue bars) variants. Short term vaccine efficacy is marked in green/blue colour, while long-term efficacy in light green/blue colour.
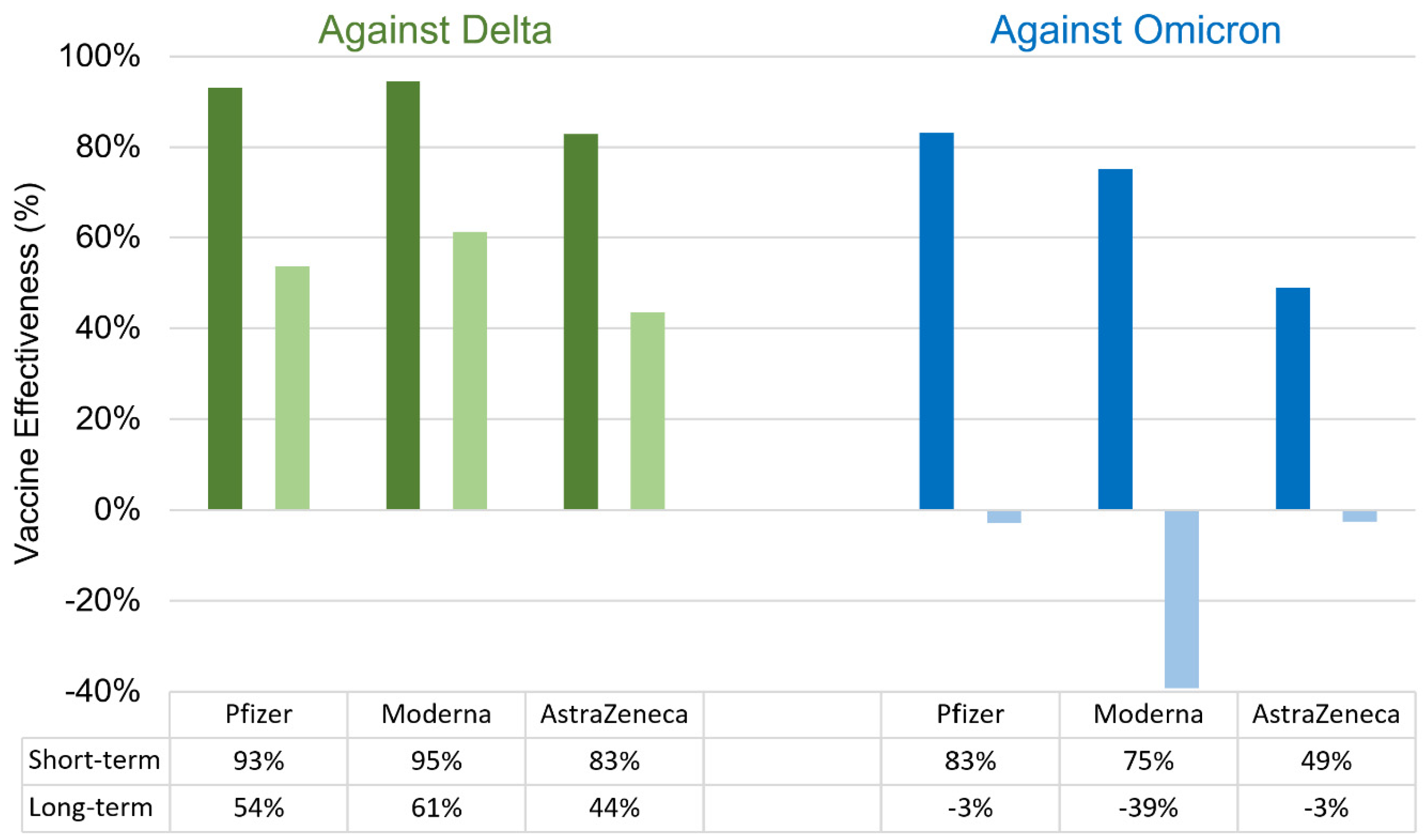

Table 1.
Non-structural proteins of SARS-CoV-2.
| Name | Range on genome | Function | Sequence Reference Number |
|---|---|---|---|
| Nsp1 | 1-180 | Leader protein host RNA inhibitor (degrade the host RNA)[25] |
YP_009725297.1 |
| Nsp2 | 181-818 | Disruption of signaling in host cells (predicted based on SARS-CoV)[26] | YP_009725298.1 |
| Nsp3 | 819-2763 | Papain-like protease Promotion of RNA replication and transcription[27] Cleavage of proteins involved in the host innate immune immunity[28] |
YP_009725299.1 |
| Nsp4 | 2764-3263 | Membrane remodeling (Binding to nsp3) | YP_009725300.1 |
| Nsp5 | 3264-3569 | 3C-like proteinase Mediates cleavages downstream of nsp4 Cleavage of proteins related to the host innate immune response[28] |
YP_009725301.1 |
| Nsp6 | 3570-3859 | Limitation of autophagic flux[29,30] Transmembrane domain |
YP_009725302.1 |
| Nsp7 | 3860-3942 | Forms a complex with RdRp for genome replication[31] | YP_009725303.1 |
| Nsp8 | 3943-4140 | Combine with RdRp[31] Subunit of SARS-CoV-2 polymerase complex[32] |
YP_009725304.1 |
| Nsp9 | 4141-4253 | RNA binding subunit[33] | YP_009725305.1 |
| Nsp10 | 4254-4392 | Regulator of viral replicase function Activation of methyltransferase activity as a co-factor[34] |
YP_009725306.1 |
| Nsp11 | 4393-4405 | Unknown | YP_009725312.1 |
| Nsp12 | 4393-5324 | RNA-dependent RNA polymerase (RdRp)[35] | YP_009725307.1 |
| Nsp13 | 5325-5925 | Helicase[36] | YP_009725308.1 |
| Nsp14 | 5926-6452 | Exonuclease[36] | YP_009725309.1 |
| Nsp15 | 6453-6798 | Endoribonuclease[36] | YP_009725310.1 |
| Nsp16 | 6799-7096 | 2′-O-methyltransferase Immune evasion related[37] |
YP_009725311.1 |
Table 2.
WHO certified vaccines against COVID-19.
| Vaccine | Developers & (Country) | Vaccine Type | Doses | Injection Interval* | Vaccination Restrictions** |
|---|---|---|---|---|---|
| Comirnaty | Pfizer-BioNTech (USA & Germany) |
mRNA | 2 | 21 days | All individuals aged 6 months and above |
| Spikevax | Moderna, NIAID (USA) | mRNA | 2 | 28 days | All individuals aged 6 months and above |
| Johnson & Johnson vaccine | Janssen Pharmaceuticals Johnson & Johnson (USA) | Viral vector | 1 | - | 18 and above |
| Vaxzevria | AstraZeneca, University of Oxford (UK) | Viral vector | 2 | 28 days | 18 and above |
| CONVIDECIA | CanSino Biologics Inc. (China) |
Viral vector | 1 | - | 18 and above |
| CoronaVac | Sinovac (China) |
Inactivated (Vero Cells) | 2 | 14 days | 18 and above; Further assessment for pregnant women is needed |
| BBIBP-CorV (Vero Cells) | Sinopharm (China) |
Inactivated (Vero Cells) | 2 | 21 days | 18 and above; Further assessment for pregnant women is needed |
| BBV152/COVAXIN | Bharat Biotech (India) |
Inactivated | 2 | 28 days | 18 and above; recommended for pregnant woman only when the benefits of vaccination outweigh the potential risks |
| VLA2001 | Valneva SE (France) |
Inactivated | 2 | 28 days | 18 to 50 years |
| Nuvaxovid | Novavax (U.S) |
Protein Subunit vaccine | 2 | 21 days | 12 and above; recommended for pregnant woman only when the benefits of vaccination outweigh the potential risks |
* This interval was required for the vaccines that were originally designed as primary - booster model. ** Individuals with the allergic history of any component of the vaccine shouldn’t take the vaccines; Vaccination restrictions for pregnant women may be updated based on more data.
Table 3.
VOCs circulating in 2020-2023.
| WHO label* | Pango lineage** | GISAID Clade*** | Mutations in binding sites | First reported (Date/Country) |
Designation /Date |
|---|---|---|---|---|---|
| Alpha | B.1.1.7 | GRY | S:N501Y | Sep/2020 UK |
VOC: 18/Dec/2020 Previous VOC: 09/Mar/2022 |
| Beta | B.1.351 | GH/501Y.V2 | S:K417N,S:E484K,S:N501Y | May/2020 South Africa |
VOC: 18/Dec/2020 Previous VOC: 09/Mar/2022 |
| Gamma | P.1 | GH/501Y.V3 | S:K417T,S:E484K,S:N501Y | Nov/2020 Brazil |
VOC: 11/Jan/2021 Previous VOC: 09/Mar/2022 |
| Delta | B.1.617.2 | G/478K.V1 | S:L452R,S:T478K,S:E484Q | Oct/2020 India |
VOI: 4/Apr/2021 VOC: 11/May/2021 Previous VOC: 07/Jul/2022 |
| Omicron | B.1.1.529 | GR/484A | S:G339D,S:S371L,S:S373P,S:S375F,S:K417N, S:N440K,S:G446S,S:S477N,S:T478K,S:E484A, S:Q493R,S:G496S,S:Q498R,S:N501Y,S:Y505H |
Nov/2021 Multiple countries |
VUM: 24/Nov/2021 VOC: 26/Nov/2021 Previous VOC: 14/Mar/2023 |
* The Greek Alphabet were recommended for non-scientific discussions by WHO convened expert group. ** Pango lineage is a classifying and naming system based on the virus genomes analysis, it is for genetically distinct lineages of SARS-CoV-2 and variants. Only the genomic sequence identified from the first cases are listed; Variety of lineage under the same label and the variations are not entirely consistent. *** GISAID is a nomenclature system for major clades to understand the patterns and determinants of SARS-CoV-2 variant strains, which are based on Pango lineage, the system contains 8 high-level phylogenetic groupings: the early split of S and L, the further evolution of L are V and G, the further evolution of G are GH, GR and GV, and the further evolution of GR are GRY.
Table 4.
Table 4. Representative mutations of S protein and impact on viral characteristics.
| Mutations | Location | Impact |
|---|---|---|
| H49Y | NTD | Slight structural changes on the HR1 region; Increased cell entry[120] |
| V367F | RBD | Enhanced infectivity; Increased affinity to ACE2[127] |
| K417N | RBD | Immune escape[128] |
| N440K | RBD (RBM) | Higher infectious fitness; Increased affinity to ACE2[129,130] |
| S443A | RBD (RBM) | Stabilized SARS-CoV-2 S protein; Increased affinity to ACE2[130,131] |
| K444R/Q/N* | RBD (RBM) | Immune escape[132] |
| L452R | RBD (RBM) | Immune escape[133,134] |
| Y453F | RBD (RBM) | Immune escape[135] |
| G476S | RBD (RBM) | Conformational changes in the S protein; Increased affinity to ACE2[130] |
| T478K | RBD (RBM) | Immune escape[136] |
| S494P | RBD (RBM) | Immune escape[137] |
| N501Y | RBD (RBM) | Immune escape[138] |
| D839Y | S2 subunit | Structural changes on the S protein Enhanced infectivity (Prediction)[139] |
| D936Y | HR1 | Conformational stability adjustment of the pre- and/or post-fusion S protein[140] |
| S943P | HR1 | Conformational stability adjustment of the pre- and/or post-fusion S protein[140] |
| P1263L | Cytoplasmic tail | A significant increase in fusion (compared with WT)[141] |
| T9I | E protein | Destabilizing[142] |
| V62F | E protein | Highly destabilizing[142] |
| S68F | E protein | Slightly stabilizing[142,143,144] |
| R203K | N protein | Destabilized and decreased overall structural flexibility; Increased transmission and virulence of select SARS-CoV-2 variants[145,146] |
| G204R | N protein | Destabilized and decreased overall structural flexibility; Increased transmission and virulence of select SARS-CoV-2 variants[145,146] |
| D3G | M protein | A nonsynonymous substitution[147,148] |
| T175M | M protein | High antigenicity values[147,148] |
* The substitutions are different in the sub-lineages of BA.2.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



