Submitted:
16 January 2024
Posted:
17 January 2024
You are already at the latest version
Abstract
(1) Background: Pseudotumor of the hip is a sterile, non-neoplastic soft tissue mass associated with total hip arthroplasties. Pseudotumors may mimic soft tissue tumors, or infections, so the differential diagnosis is crucial and biopsy is recommended. The purpose of this study was to compare complications and functional results between one-stage and two-stage procedures. (2) Methods: We retrospectively analyzed 21 patients surgically treated at our Institution with “pseudotumor” associated with hip prosthesis (8 male,13 female; mean age 69 years). One-stage revision was performed in 10 cases, two-stage in 10, excision only in one case. Complications were classified as major and minor and functional results assessed using the Harris Hip Score (HHS). (3) Results: Five patients (24%) reported major complications. Survival rate to all com-plications was 75%. Overall survival was 95% at five years. Mean HHS went from 35 pre-operative to 75 post-operative, highlighting improved functional results in all cases. We rec-orded no differences in complications and functional outcome between one and two-stage proce-dures. (4) Conclusions: In our experience, two-stage surgical approach is preferable in cases with major bone defects and larger pseudotumor size. The use of custom-made 3D-printed prostheses is increasing and is a further reason to prefer two-stage revision.
Keywords:
custom-made 3D-printed prostheses
; hip
; pseudotumors
; revision surgery
; total hip arthroplasy
1. Introduction
The introduction Total hip arthroplasty (THA) has become essential in treating disability secondary to degenerative hip joint disease, to improve quality of life. It is constantly growing also due to the increasing age of population. There are currently about 2.5 million people in the United States living with a THA. Over 200,000 THAs are performed in the United States each year, and this number is expected to rise to nearly 570,000 by 2030 [1,2,3].
Over the years several bearing surfaces have been developed: Metal to Polyethylene (MoP), Metal to Metal (MoM) Ceramic to Ceramic (CoC), Ceramic Polyethylene (CoP). Highly cross-linked polyethylene is now commonly used in implants and is considered the "gold standard" [4,5].
MoM THA has decreased from 20% in 2005 to <1% in 2012 [1]. The increased revision rate of MoM THA is thought to be associated with the development of MoM THA unique complications now known as Adverse Metal Debris Reactions (ARMDs), which include elevated serum metal ions, lack of ingrowth in components, aseptic loosening, metallosis, necrosis, pseudotumors, and unexplained pain [1,6].
Tipically, a pseudotumor is a non-neoplastic, sterile, solid and/or cystic lesion of inflammatory origin, fluid accumulation that frequently extends beyond the joint capsule [7].
Pseudotumors are increasingly associated with THA; these pseudotumors are not uncommon: although reported incidences vary with different implants, recent studies report incidences ranging from 0.27% to 5% [7,8] other ranging from 0.6% to 61% [9,10].
The prevalence of pseudotumors in patients with MoM hip implants varies widely in the literature. A meta-analysis reported an estimated incidence of 0.6% [11], however more recent studies have identified asymptomatic pseudotumors in 31% to 60.9%[9]. Asymptomatic pseudotumors are incidental findings in 57-58% of cases[7].
Pseudotumors can be asymptomatic, but they can also cause pain, instability and gait disturbances, leading to excision of the soft tissue mass and/or the need for revision arthroplasty[10].
Clinical symptoms of pseudotumors often include: groin pain, skin changes/rash, instability/spontaneous dislocation, deep vein thrombosis, hip discomfort, paresthesia, antalgic gait, and/or a palpable mass [7,12].
The complexity of treatment of such conditions lies in periprosthetic osteolysis and in extensive damage to the soft tissues, which compromise the stability of the revision implant.
The contribution of a multidisciplinary approach is evident considering the complexity of the type of intervention, specially in explant prostheses and complex prosthesis such as custom made 3 D printed [13,14,15].
Surgery can help to restore joint stability, function and range of motion, allowing patients to regain mobility and participate in activities they could not, due to pseudotumor-related symptoms.
The decision to undertake surgery should be made in close consultation with a multidisciplinary approach [16,17].
In complex revisions, a two-stage surgical procedure is often useful for better management, but there are few studies in the literature on this topic.
The aim of the present study was to report preliminary results of complex revision surgery for hip prostheses in patients suffering from “pseudotumor”, analyzing (1) correct diagnosis, (2) appropriate treatment, one stage or two-stage surgical procedure, (3) incidence of complications and implants survival, (4) functional results. We also performed a literature analysis on diagnostic and management aspects.
2. Materials and Methods
2.1. Patients
This study was designed as a retrospective, single-center, comparative, clinical, and functional study including a consecutive series of Caucasian patients affected by pseudotumor of the hip and treated at our level-I healthcare trauma center (Orthopedics and Orthopedic Oncology Department, University-Hospital of Padova) from January 2016 to December 2022. The following demographical and clinical data was collected for all patients were included in the study considering, sex, age at surgery, comorbidities, tribology, time to implant revision. All patients examined came to our attention for swelling and pain at the hip and functional limitation of day-life activities.
Twenty-one patients (8 male and 13 females) with a median age of 68 years (range 50.4-79.6 years) were included.
Fourteen patients had cardio vascular risk factors as diabetes, hypertension and Hypercholesterolemia, obesity; five patients had history of tumors.
The mean time from the first implant to revision in our department was 9.86 years, with a minimum survival time of the implant of 1 year and a maximum of 20 years.
Bearing of prostheses was MoP in 11 cases while 7 were MoM, 2 CoC, and one CoP.
All patients were preoperatively classified with ASA scores with a mean of 2.6 (range 1 to 4).
They had plain X-rays AP-LL and second level imaging (CT or MRI with contrast); in all patient we performed a biopsy to confirm the diagnosis of pseudotumor (absence of neoplastic cells).
Two further patients out of the 21 analyzed, were not operated due to co-morbidities but only observational follow-up was maintained. These patients were excluded from the statistical analysis.
Excision only was performed in one case, because this patient had recently undergone revision surgery on the prosthetic stem, elsewhere, leaving the pseudotumor in place.
In ten cases a one stage revision was performed while two-stage revision was performed in other 10 patients. Standard prostheses were used in 6 cases, revision prostheses in 6 cases and custom made prostheses in 7 cases. (Table 1)
2.2. Ethics
All subjects participating in this long-term follow-up study received a thorough explanation of the risks and benefits of inclusion and gave their written informed consent to participate to the study. This study has been approved by the local Ethics Committee (CESC Code: 2561 P; 12th March 2012). This study was performed in accordance with the ethical standards of the 1964 Declaration of Helsinki as revised in 2013 and conducted ethically according to the most recent international standards [18].
2.3. Inclusion and Exclusion Criteria
The inclusion criteria were the diagnosis of pseudotumor confirmed by a biopsy, perivascular lymphocytic infiltrate, fibrinous exudate, macrophage accumulation, and tissue necrosis. Patients with revision hips, who had not undergone a biopsy, were excluded. Three of the 24 patients initially considered were excluded from the study: as mentioned before, two patients were very elder with high operative risk, another patient was excluded because significant cognitive impairment.
2.4. Imaging
The first level exams performed were the ultrasound in the suspicion of a mass and the radiography for studying the bone. The radiographic examination is not very sensitive in the diagnosis of pseudotumor but can give important information regarding the quality of bone and prosthesis. The presence of osteolysis can lead to suspicion of a pseudotumor. CT is a useful multiplanar imaging tool for evaluating hip implants; it is advantageous for assessing bone quality, heterotopic ossifications, osteolysis, metallosis. CT allows imaging of radiographically occult cystic and solid pseudotumors, although it is less sensitive than MRI with contrast for evaluating adverse local soft tissue reactions. The administration of iodinated contrast medium is useful for the vascular study, localization and characterization of periarticular cystic pseudotumors [7]. Magnetic resonance imaging (MRI) is an excellent modality to evaluate periarticular soft tissue complications after hip arthroplasty. Pseudotumors have a variable appearance on MRI: alterations shown on T1-T1 signal may mimic soft tissue tumors with no clear margins. Pseudotumors range from discrete thin-walled cystic lesions to ill-defined solid masses, often associated with synovial thickening, surrounding fluid, and/or scattered debris[7,19]. Clinical presentation may be similar to an infection, so the differential diagnosis is crucial. It may be sympthtomatic (more or less) or asympthomatic.
2.5. Biopsy
Histologic evaluation with biopsy is recommended and, in our experience, mandatory for excuding diagnoses of tumors or infection.
When pseudotumor is suspected, biopsy is required for the differential diagnosis with malignant tumors of bone and soft tissue such as liposarcoma, synovial cell sarcoma, malignant peripheral nerve sheath tumor, and non-Hodgkin’s lymphoma, osteosarcoma, chondrosarcoma.
Among the benign masses we find seromas and hematomas, frequent complications of hip arthroplasty. Seroma and hematoma are differentiated from a pseudotumor by their development in the immediate postoperative period and subsequent resolution over time.
An infection is also differentially diagnosed with pseudotumor: but infection often includes local or systemic symptoms and signs such as fever, palpable thermotact positive mass and flushing. Peripheral enhancement of the cystic fluid collection is the typical finding on post-contrast imaging.
2.6. Histology
Pseudotumors are histologically described as aseptic lymphocytic vasculitis-associated lesions [21]. These tissue reactions can manifest as an effusion, local tissue necrosis, periprosthetic osteolysis which may be solid and/or cystic [22]. Histopathologically, pseudotumors are described as cell-mediated (type IV) hypersensitivity reactions characterized by perivascular lymphocytic infiltrate, fibrinous exudate, macrophage accumulation, and tissue necrosis [12,23].
2.7. Surgical Procedure
Surgical procedures performed were: excision of the tumor or excision and revision of the implant and it could be done in different ways: with a standard prosthesis, a revision prosthesis or a custom made. This one is used when the size of bone loss precludes the use of a standard or revision prosthesis.
The excision and revision could also be done in two different ways: one stage or two stage surgery. The choice of which strategy is based on: (1) general condition of patient: one stage surgery requires hemodynamic stability of the patient; (2) size of the pseudotumor: if the tumor is large with bone erosion the two-stage surgery is variable (3) type of implant: with custom made 3D prostheses, which requires a high-resolution CT, the imaging study is better performed after removal of the implant to allow assessment of the bone loss and planning of the implant.
In our study, in 6 cases we used a standard revision prosthesis: in 4 cases total hip prostheses in 2 cases only acetabular component. In 7 cases we used a Custom-Made prosthesis because of the bone loss (Figure 1, Figure S1). We aimed to investigate if there were differences in term of complications and functional result between types of surgery.
2.8. Post-Operative Protocol of Both Procedures
All patients followed the same postoperative protocol and were followed in the same standardized manner. Patients were administered preoperative intravenous antibiotics and continued to receive antibiotics for 7 days. Postoperative menagement included bed rest, analgesia, and mobilisation with a walker or crutches after the second postoperative day when possible. Chemical anti-thrombosis prophylaxis was given until complete weight bearing with low molecular-weight heparin. All patients received physical therapy for a minimum of 6 weeks after discharge from hospital. Immobilization was obtained with a pelvis-thigh brace in all cases of pelvic reconstruction with custom-made prostheses and in all cases of complex revisions: the brace was positioned at 10° of abduction and fixed in extension for 1 month, then unlocked with flexion allowed up to 90° for another month, walking with two crutches, with a progressive load.in the second month.
2.9. Clinical and radiographic evaluation
Patients had plain X-rays (AP-LL) and second level imaging (CT or MRI with contrast imaging) and in all patients, we performed a biopsy to confirm the absence of neoplastic cells and support the diagnosis of pseudotumor. Preoperative radiographic data were obtained from anteroposterior and lateral views of the hip and femur. The bone-implant interface and migration of the acetabular component, in horizontal and vertical directions, were examined on the immediate postoperative and the final follow-up radiographs.
We attempted to stratify our cases according to the severity of bone defects evaluated with Paprosky Classification as well as according to the size of the pseudotumor tissue using an ideal axial diameter [24].
The modified Harris hip score (HHS) was used for the clinical evaluations of all patients at each check. (1969, Harris WH). Every patient was evaluated clinically, with a questionnaire and with Harris Hip Score (HHS), Maximum 100. A result over 70 points indicates a good state of the hip articulation [25]
2.10. Complication
Complications were analyzed according to the classification by Henderson et al. (2011-2013) Endoprosthesis failures were classified as soft-tissue failures (Type I), aseptic loosening (Type 2), structural fracture (Type 3), infection (Type 4). Tumor recurrence (Type 5) was not considered because this was an exclusion criterion from our study.
2.11. Statistical Analysis
Before handling, the data was preprocessed and visually inspected for quality control, missing data and potential outliers. The normality of data distribution was verified by conducting the Shapiro-Wilk test, which was preferred over other tests (including the omnibus test of Kolmogorov-Smirnov or D’Agostino-Pearson) due to the small sample size employed. Continuous variables were expressed as mean and range (min; max), while categorical parameters were calculated as percentages where appropriate. Student’s t-test for paired samples was used to compare pre- and postoperative HHS; Student’s t-test for independent samples was used to compare postoperative HHS between one-stage and two-stage procedures and HHS improvement between one-stage and two-stage. The scatterplot was used to see the correlation between age of pseudotumor onset in relation to age and to assess pre- and postoperative HHS in relation to age and sex.
The survival of the prosthesis to complications was evaluated with Kaplan-Meier curves (1958 Kaplan EL). Finally, Cox proportional hazards regression and the Longrank test were used to compare complications and implant survival between one stage or two stage surgical procedures. Statistical significance was defined as a p ≤ 0.05. Statistical analysis was performed using MedCalc software version (MedCalc Software Broekstraat 52, Mariakerke, Belgium) [28]
3. Results
3.1. Patients Data
From the distribution of data, pseudotumors in our population arose between 8-12 years after implantation of the prosthesis and for most part in subjects above 70 years of age. The scatter plot used to see the correlation between age and pseudotumor onset in relation to age showed that there are no statistically significant differences for age (Figure 2).
There are no significant differences between sex and age in postoperative functional outcomes. Biopsy showed chronic inflammation, giant cell cells, lymphocytic infiltrate, metallosis, necrosis, fibrous tissue.
Our patients were stratified according to Paprosky classification of bony defects. Pseudotumors do not fit perfectly to this classification of bony defects, since we also must consider the extension and location of the pseudotumor itself which have a remarkable role in the choice of indication to surgery. As far as acetabular defects are concerned, we found that 5 cases had a Paprosky type I, 10 cases had a Paprosky type II, while 6 had a Paprosky type III.
As far as the femoral defects is concerned, our series included 10 patients type I, 4 patients type II, 5 patients type III and 2 patients type IV. The acetabular and femoral defects according to Paprosky classification are summarized in Table 4, showing that acetabular and femoral defects are usually combined and that cases with a “major” combined Paprosky (acetabular type III and femoral type III or IV) were mostly treated with two-stage procedure. (Table 2)
Moreover, the entity of bony defect is not the sole factor for deciding between one stage and two-stage procedures, since also the size, extensio, and location of pseudotumor itself concur in this choice. In fact, we stratified our cases in two groups according to size of pseudotumors below and over an average size (ideal axial diameter) of 7 cm: ten cases out of 14 with an axial size of 7 cms and more had a two-stage surgical procedure, while all the 6 cases with a pseudotumor axial size below 7 cm had a one stage. One remaining case only had the pseudotumor excised in our hospital, since the revision of prosthesis had already been done elsewhere previously. (Table 2)
Clinical evaluation of our patients showed that mean preoperative HHS was 35 (range 18- 45), indicating a relevant compromission of the joint in all subjects. The mean postoperative HHS was 75 (range 60- 89). In our study population there is a statistically significant difference between postoperative and preoperative HHS as confirmed by paired sample t test (p<0.0001). Comparing one and two stage procedures there were no statistically significant differences in postoperative HHS (p = n.s.) and in HHS improvement (p = n.s.) (Table 3)
3.2. Complications
The complications in our study at a mean follow-up of 20 months (range 4-65 months), were reported in 8 patients (8/21 patients, 38.1%): 2 were wound dehiscence (type I) within the first 30 days after surgery, treated with wound revision and antibiotic. One case of thigh sensory deficit was found, improving six months after surgery. Five major complications were found: two deaths at 3 months and 1 year after surgery and three patients reported periprosthetic infection (type IV) treated with surgical debridement and antibiotic therapy. In a patient, for the isolation of Proteus mirabilis and E. Coli, surgical cleaning was performed, covering the prosthesis with a rectus abdominis flap. None of our patients had aseptic loosening or implant breakage (type II and III). Survival rate of major complications at an average follow-up of 20 months (range 4-40) was 75% as represented by the Kaplan Maier (Figure 3). Overall survival was 95% at five years. No statistically significant differences in complication rates (p=0.7521) were found between one stage and two stage procedure as demonstrated by comparison of survival curves (Logrank test). The results are summarized in Table 4.
4. Discussion
Pseudotumor of the hip refers to a non-neoplastic soft tissue mass that can develop in the region around the hip joint. The term "pseudotumor" is used because the mass can mimic a tumor in terms of its appearance and growth pattern, but it is not a true tumor. For this reason, biopsy is mandatory. In our study all patients underwent biopsy[29,30].
Pseudotumors around the hip joint are often caused by an inflammatory reaction to wear debris from the components of the hip implant. This condition is most commonly associated with MoM hip joint replacements. In our study 13 (61,9%) women were affected by pseudotumors, 8 (38,1%) were male. Grote et al. in their literature review of pseudotumors, arising in MoM implants point out that women are at increased risk of complications from THA, possibly related to metal hypersensitivity [1].
Hasegawa et al. in their study described more pseudotumor in women after MoM THA, but several case reports on pseudotumor in males or females in MoM implant are described in the literature. Moreover implant type, and implant malposition are most often involved in pseudotumor formation [31]. As reported in the literature by various studies, pseudotumors are recorded in MoM implants, less so in CoC [8,32,33].
In our study in 21 patients with pseudotumor there were 11 (52,3%) MoP implants followed by 7 (33,3%) MoM, 2 (9,5%) CoC, 1(4,7%) CoP. Only 2 cases of pseudotumors were recorded on CoC implants in line with the literature [8,32,33].
The data collected from the various studies are summarized in Supplementary Table 1 [34,35,36,37,38,39,40].
With regard to sex, age of onset and time of symptom onset, the study in accordance in the current literature. Symptoms may present with the appearance of soft tissue mass 3 to 26 years after implantation. In our study, the mean onset of symptoms was 9.8 years.
In a 2016 study, Hasegawa et al. described several types of mixed and solid cystic type pseudotumors [31].
In the literature risk factors for the formation of a pseudotumor are high serum cobalt (Co >5 μg/l) and chromium (Cr) levels (known to cause osteolysis), female gender [7], a high cup inclination angle >55°, a large diameter head in THA>36 mm [1,41,42,43,44]. Despite the observed associations and risk factors, the exact mechanism of THA-induced pseudotumors is still unclear[45].
These data were not taken into consideration by our study, to focus instead on surgical indications.
Our patients were all symptomatic, on the contrary asymptomatic patients with pseudotumor are described in the literature. Hasegawa et al in their study describe how pseudotumors of mixed composition were associated with pain, whereas cystic pseudotumors were mostly asymptomatic [31]. In contrast, a study by Hart et al. found no correlation between type of pseudotumor and presence of symptoms[45].
In a study by Lindsay et al., the Authors show that there is no correlation between pseudotumor size and patients symptoms [9]. In our study, patients had hip pain and swelling, not nerve or vascular deficits. Sagoo et al. describe a symptomatic MoM pseudotumor with extension from the hip joint to the iliopsoas mass in the pelvis, with acute lower abdominal pain and motor deficits[46].
In our study we matched 2 cases of pseudotumor in CoC prosthesis. Few cases are described in the literature. Rodriguez described a pseudotumor in CoC in which ceramic wear debris can lead to an ALTR and nerve complications [47].
In literature the controversy about whether to pursue surgery for pseudotumor treatment revolves around various factors, including patient’s symptoms, severity of the pseudotumor, the potential risks and benefits of surgery, and the overall health of the patient. There is not a one-size-fits-all solution, as treatment decisions should be tailored to each individual’s unique situation. Surgery can provide effective relief from pain, discomfort, and other symptoms associated with pseudotumors, especially if the condition is causing significant impairment in daily activities and quality of life.
Pseudotumors can lead to complications like implant loosening, tissue damage, and joint instability. Surgery can address these issues and prevent further damage, potentially leading to better long-term outcomes. Surgery may help restore joint stability, function, and range of motion, allowing patients to regain mobility and participate in activities they could not due to pseudotumor-related symptoms. Surgery, like any medical procedure, carries risks such as infection, bleeding, anesthesia complication. Surgery often requires a period of recovery and rehabilitation, which can be demanding for patients. Not all pseudotumors cause significant symptoms or complications. In cases where the pseudotumor is asymptomatic or causing only minor discomfort, a "watchful waiting" approach might be considered to avoid unnecessary surgery. Some patients may have medical conditions that make surgery at a higher risk. In such cases, the potential benefits of surgery needs to be carefully weighed against the patient’s overall health[8,10].
Davis et al in their review article stated that pseudotumors without associated pain, disfunction, or elevated metal ion levels are more likely to receive continuous surveillance without surgery[7].
Filer et al. report the case of a hemorrhagic pseudotumor that can be successfully managed conservatively. This patient reported no trauma, was not taking anticoagulants and had no bleeding disorders. The rapid progression in size of the pseudotumor caused significant symptoms and functional impairment. This case presented a significant clinical challenge in decision making regarding appropriate management[10].
In our study we only analyzed operated patients.
The decision to pursue surgery for pseudotumor treatment should be made in close consultation and in multidisciplinary approach[16,48].
Multidisciplinary approach can be analyzed from different points of view and has numerous advantages which can be summarized in: 1) providing different perspectives on the same clinical problem, 2) combined clinical approach, 3) creating comprehensive research ques- tions and 4) developing definitions and guidelines. Effective collaboration between healthcare professionals significantly improves mutual knowledge and trust with improved results for both patients and providers. In recent decades, the collaboration has become wider, especially in surgery, adding plastic and vascular surgeons general surgeons and microsurgeon [16,49].
One stage or two stage surgery is controversial in the treatment of pseudotumors.
In the one-stage approach, both removal of problematic hip implant and pseudotumor and revision implant are performed in a single surgical procedure. This approach is chosen when the pseudotumor is causing significant symptoms or complications and is generally preferred when the extent of tissue damage is limited and the patient’s overall health permits more extensive surgery. The procedure involves removing the problematic implant, cleaning out any inflammatory tissue, and potentially replacing the implant with a different type of implant that is less likely to cause an inflammatory response. The two-step approach involves two separate surgical procedures. In the first stage, the failed hip implant is removed and the pseudotumor and inflammatory tissues are cleared. The joint can be left temporarily without an implant to allow for reduction of the inflammatory response and tissue healing and planning a revision prosthesis. After a period of several months, a second surgery is performed to place a new, more appropriate hip implant. In recent years, 3D printing applications of titanium have become available. This topic is closely related to computer-assisted surgery (CAS) and the optimization of data derived from preoperative imaging studies for improvement of clinical and surgical outcomes such as the accuracy of bone cuts. The use of 3D printing prostheses is increasing specially in musculoskeletal oncology, as well as in cases of complex revisions with extensive bone loss. Improving 3D printing technology allows for the creation of custom implants to face complex reconstructions [14,15].
In our study one stage surgical procedure was performed in ten patients: six patients with standard prosthesis, three revision prosthesis and one with custom made 3D printed. Two stage surgical procedure instead was performed in six patients with revision custom 3D printed and four revision prosthesis. We recorded no differences in terms of complications and functional outcomes between the 2 interventional procedures. Only in one case we performed excision of the pseudotumor without revision of the implant performed, due to a recent revision surgery done elsewhere.
There are few studies in the literature reporting a two-stage procedure.
Cottino et al. reported a case of a 72-year-old woman with a cystic pseudotumor on MoM THA. This case was treated in a two-step procedure, emphasizing the importance of careful planning for the type of surgery to be performed[17]. Moreover, the authors underline how a two-stage revision surgery should be considered in cases of huge cystic pseudotumor to avoid rupture of the cyst and facilitate the revision procedure, reducing surgical times, thus decreasing the risk of infections and bleeding[17].
Instead, in a study by Sagoo et al., the authors describe the excision of the pseudotumor in one stage which led to a marked improvement in symptoms[46].
In our study in cases with large bone loss of substance we preferred a two-stage procedure, reducing surgical time for each surgery and being able to better plan a revision implant.
In our study we had no prosthetic dislocations. In the literature Huang et al in their case report describe a case of dislocation in a 73-year-old woman after removal of a pseudotumor on CoC [39].
The 21 patients analyzed found benefit from the surgery with a functional improvement measured as statistically significant difference between pre- and post-operative HHS statistically significant (p<0.0001). Additionally, we observed no difference in improvement and post-operative HHS between one-stage and two-stage procedure. All enrolled patients were operated in the same Center and followed according to a standardized institutional postoperative protocol, reducing confounding bias. Due to the rarity of the lesion and the small number of patients in related studies, quantitative functional measures were rarely used. As explained below, a possible bias may be due to the fact that two stage procedure has been preferably performed for larger pseudotumors.
In our study, major complications involved 8 patients: 2 of these died three months and one year after surgery and 5 had deep infections There are no statistically significant differences in complications between one stage and two stage (p=0.7521). There are few data in the literature regarding complications of surgery of pseudotumors and all agree on a quite high complication rate [17].
We preferred a two-stage surgical approach in cases with the association of “major” combined Paprosky (acetabular type III and femoral type III or IV) and pseudotumor size of 7 cm or above. The Paprosky classification itself is not sufficient for the indication of treatment since the size and location of pseudotumors must also be considered. A comprehensive classification that can take into account both entity of the bony defects and extension and location of the pseudotumor is still lacking and future studies on broader patient populations will be required to propose such a classification and to define robust treatment recommendations.
5. Conclusions
In suspected pseudotumors, biopsy is always recommended. Given the rarity of the disease, the choice of surgical treatment remains controversial. Surgery is indicated for symptomatic pseudotumors, large pseudotumors, and/or the presence of elevated serum cobalt (Co >5 μg/l) and chromium (Cr) levels. The first two clinical criteria mentioned for surgical indications far outweigh the importance of ion concentration levels, since these are often variable in symptomatic pseudotumors. Prosthetic revision associated with the removal of pseudotumors can be performed in a single or two-stage procedure.
We recorded no differences in complications and functional outcomes between one and two-stage procedures. In our experience, a two-stage surgical approach is preferable in cases with the association of “major” combined Paprosky defects and pseudotumor size of 7 cm or above.
Finally, the use of custom 3D printed implants is increasing in these cases, and this is a further reason to prefer two-stage procedures.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Figure S1. Case of two-stage procedure; Table S1: Published literature on management of pseudotumors of the hip.
Author Contributions
Conceptualization, M.C, G.T, A.A. and P.R.; methodology, M.C., P.R., G.T. and A.A.; formal analysis, A.A. and M.C.; investigation, M.C, G.T, A.A, E.P, A.B, C.B. and P.R.; data curation, M.C., G.T. and A.A.; writing—original draft preparation, M.C., A.A., G.T., and P.R..; writing—review and editing, M.C, G.T, A.A, E.P, A.B, C.B, and P.R.; visualization, M.C. and A.A.; supervision, P.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Local Ethics Committee (CESC Code: 2561 P; 12th March 2012).
Data Availability Statement
The dataset supporting the conclusions of this review is available upon request to the corresponding author.
Conflicts of Interest
Pietro Ruggieri is consultant for Stryker and Exactech. The other authors declare that they have no relation- ships/conditions/circumstances that present a potential conflict of interest with the present manuscript and they have not received benefits or financial funds in support of this study.
References
- Grote, C.W.; Cowan, P.C.; Anderson, D.W.; Templeton, K.J. Pseudotumor from Metal-on-Metal Total Hip Arthroplasty Causing Unilateral Leg Edema: Case Presentation and Literature Review. BioResearch Open Access 2018, 7, 33–38. [Google Scholar] [CrossRef]
- Maradit Kremers, H.; Larson, D.R.; Crowson, C.S.; Kremers, W.K.; Washington, R.E.; Steiner, C.A.; Jiranek, W.A.; Berry, D.J. Prevalence of Total Hip and Knee Replacement in the United States: J. Bone Jt. Surg.-Am. Vol. 2015, 97, 1386–1397. [Google Scholar] [CrossRef]
- Kurtz, S.; Ong, K.; Lau, E.; Mowat, F.; Halpern, M. Projections of Primary and Revision Hip and Knee Arthroplasty in the United States from 2005 to 2030: J. Bone Jt. Surg. 2007, 89, 780–785. [Google Scholar] [CrossRef]
- Kumar, N.; Arora, G.N.C.; Datta, B. Bearing Surfaces in Hip Replacement - Evolution and Likely Future. Med. J. Armed Forces India 2014, 70, 371–376. [Google Scholar] [CrossRef]
- Mp, B.; Ck, L. Metal-on-Metal Total Hip Arthroplasty: Patient Evaluation and Treatment. J. Am. Acad. Orthop. Surg. 2015, 23. [Google Scholar] [CrossRef]
- Pozzuoli, A.; Berizzi, A.; Crimì, A.; Belluzzi, E.; Frigo, A.C.; Conti, G.D.; Nicolli, A.; Trevisan, A.; Biz, C.; Ruggieri, P. Metal Ion Release, Clinical and Radiological Outcomes in Large Diameter Metal-on-Metal Total Hip Arthroplasty at Long-Term Follow-Up. Diagn. Basel Switz. 2020, 10, 941. [Google Scholar] [CrossRef]
- Davis, D.L.; Morrison, J.J. Hip Arthroplasty Pseudotumors: Pathogenesis, Imaging, and Clinical Decision Making. J. Clin. Imaging Sci. 2016, 6, 17. [Google Scholar] [CrossRef]
- Campbell, P.; Shimmin, A.; Walter, L.; Solomon, M. Metal Sensitivity as a Cause of Groin Pain in Metal-on-Metal Hip Resurfacing. J. Arthroplasty 2008, 23, 1080–1085. [Google Scholar] [CrossRef]
- Lt, K.; D, G.; Tm, S.; Jg, M.; De, A.; Ss, W.; Mp, B. Association Between Pseudotumor Formation and Patient Factors in Metal-on-Metal Total Hip Arthroplasty Population. J. Arthroplasty 2018, 33. [Google Scholar] [CrossRef]
- Filer, J.L.; Berstock, J.; Hughes-Roberts, Y.; Foote, J.; Sandhu, H. Haemorrhagic Pseudotumour Following Metal-on-Metal Hip Replacement. Cureus 2021, 13, e15541. [Google Scholar] [CrossRef]
- Wiley, K.F.; Ding, K.; Stoner, J.A.; Teague, D.C.; Yousuf, K.M. Incidence of Pseudotumor and Acute Lymphocytic Vasculitis Associated Lesion (ALVAL) Reactions in Metal-On-Metal Hip Articulations: A Meta-Analysis. J. Arthroplasty 2013, 28, 1238–1245. [Google Scholar] [CrossRef] [PubMed]
- Blau, Y.M.; Meyers, A.J.; Giordani, M.; Meehan, J.P. Pseudotumor in Ceramic-on-Metal Total Hip Arthroplasty. Arthroplasty Today 2017, 3, 220–224. [Google Scholar] [CrossRef]
- Angelini, A.; Trovarelli, G.; Berizzi, A.; Pala, E.; Breda, A.; Ruggieri, P. Three-Dimension-Printed Custom-Made Prosthetic Reconstructions: From Revision Surgery to Oncologic Reconstructions. Int. Orthop. 2019, 43, 123–132. [Google Scholar] [CrossRef] [PubMed]
- A, A.; D, K.; G, T.; A, S.; A, B.; P, R. Analysis of Principles Inspiring Design of Three-Dimensional-Printed Custom-Made Prostheses in Two Referral Centres. Int. Orthop. 2020, 44. [Google Scholar] [CrossRef]
- Kotrych, D.; Angelini, A.; Bohatyrewicz, A.; Ruggieri, P. 3D Printing for Patient-Specific Implants in Musculoskeletal Oncology. EFORT Open Rev. 2023, 8, 331–339. [Google Scholar] [CrossRef] [PubMed]
- Ruggieri, P.; Cerchiaro, M.; Angelini, A. Multidisciplinary Approach in Patients with Metastatic Fractures and Oligometastases. Injury 2023, 54, 268–270. [Google Scholar] [CrossRef] [PubMed]
- Cottino, U.; Dettoni, F.; Risitano, S.; Marmotti, A.; Rossi, R. Two-Stage Treatment of a Large Pelvic Cystic Pseudotumor in a Metal-On-Metal Total Hip Arthroplasty. Joints 2017, 5, 121–124. [Google Scholar] [CrossRef]
- Padulo, J.; Oliva, F.; Frizziero, A.; Maffulli, N. Muscle, Ligaments and Tendons Journal. Basic Principles and Recommendations in Clinical and Field Science Research. Muscles Ligaments Tendons J. 2013, 3, 250–252. [Google Scholar]
- Hauptfleisch, J.; Pandit, H.; Grammatopoulos, G.; Gill, H.S.; Murray, D.W.; Ostlere, S. A MRI Classification of Periprosthetic Soft Tissue Masses (Pseudotumours) Associated with Metal-on-Metal Resurfacing Hip Arthroplasty. Skeletal Radiol. 2012, 41, 149–155. [Google Scholar] [CrossRef]
- Turecki, M.B.; Taljanovic, M.S.; Stubbs, A.Y.; Graham, A.R.; Holden, D.A.; Hunter, T.B.; Rogers, L.F. Imaging of Musculoskeletal Soft Tissue Infections. Skeletal Radiol. 2010, 39, 957–971. [Google Scholar] [CrossRef]
- Carli, A.; Reuven, A.; Zukor, D.J.; Antoniou, J. Adverse Soft-Tissue Reactions around Non-Metal-on-Metal Total Hip Arthroplasty - a Systematic Review of the Literature. Bull. NYU Hosp. Jt. Dis. 2011, 69 Suppl 1, S47-51. [Google Scholar]
- Liow, M.H.L.; Kwon, Y.-M. Metal-on-Metal Total Hip Arthroplasty: Risk Factors for Pseudotumours and Clinical Systematic Evaluation. Int. Orthop. 2017, 41, 885–892. [Google Scholar] [CrossRef]
- Willert, H.-G.; Buchhorn, G.H.; Fayyazi, A.; Flury, R.; Windler, M.; Köster, G.; Lohmann, C.H. Metal-on-Metal Bearings and Hypersensitivity in Patients with Artificial Hip Joints. A Clinical and Histomorphological Study. J. Bone Joint Surg. Am. 2005, 87, 28–36. [Google Scholar] [CrossRef]
- Xiong, L.; Li, H.; Huang, X.; Jie, S.; Zhu, W.; Pan, J.; Wu, X.; Mao, X. Both Acetabular and Femoral Reconstructions With Impaction Bone Grafting in Revision Total Hip Arthroplasty: Case Series and Literature Review. Arthroplasty Today 2023, 24, 101160. [Google Scholar] [CrossRef]
- Mahomed, N.N.; Arndt, D.C.; McGrory, B.J.; Harris, W.H. The Harris Hip Score: Comparison of Patient Self-Report with Surgeon Assessment. J. Arthroplasty 2001, 16, 575–580. [Google Scholar] [CrossRef] [PubMed]
- Pala, E.; Henderson, E.R.; Calabrò, T.; Angelini, A.; Abati, C.N.; Trovarelli, G.; Ruggieri, P. Survival of Current Production Tumor Endoprostheses: Complications, Functional Results, and a Comparative Statistical Analysis. J. Surg. Oncol. 2013, 108, 403–408. [Google Scholar] [CrossRef] [PubMed]
- Henderson, E.R.; Groundland, J.S.; Pala, E.; Dennis, J.A.; Wooten, R.; Cheong, D.; Windhager, R.; Kotz, R.I.; Mercuri, M.; Funovics, P.T.; et al. Failure Mode Classification for Tumor Endoprostheses: Retrospective Review of Five Institutions and a Literature Review. J. Bone Joint Surg. Am. 2011, 93, 418–429. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, E.L.; Meier, P. Nonparametric Estimation from Incomplete Observations. J. Am. Stat. Assoc. 1958, 53, 457–481. [Google Scholar] [CrossRef]
- Mavrogenis, A.F.; Rimondi, E.; Rossi, G.; Calabrò, T.; Ruggieri, P. CT-Guided Biopsy for Musculoskeletal Lesions. Orthopedics 2013, 36, 416–418. [Google Scholar] [CrossRef] [PubMed]
- Angelini, A.; Biz, C.; Cerchiaro, M.; Longhi, V.; Ruggieri, P. Malignant Bone and Soft Tissue Lesions of the Foot. J. Clin. Med. 2023, 12, 3038. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, M.; Iino, T.; Sudo, A. Immune Response in Adverse Reactions to Metal Debris Following Metal-on-Metal Total Hip Arthroplasty. BMC Musculoskelet. Disord. 2016, 17, 221. [Google Scholar] [CrossRef]
- Naik, L.G.; Shon, W.Y.; Clarke, I.C.; Moon, J.-G.; Mukund, P.; Kim, S.-M. Pseudotumor and Subsequent Implant Loosening as a Complication of Revision Total Hip Arthroplasty with Ceramic-on-Metal Bearing: A Case Report. Hip Pelvis 2018, 30, 276–281. [Google Scholar] [CrossRef]
- Isaac, G.H.; Brockett, C.; Breckon, A.; van der Jagt, D.; Williams, S.; Hardaker, C.; Fisher, J.; Schepers, A. Ceramic-on-Metal Bearings in Total Hip Replacement: Whole Blood Metal Ion Levels and Analysis of Retrieved Components. J. Bone Joint Surg. Br. 2009, 91, 1134–1141. [Google Scholar] [CrossRef]
- Maurer-Ertl, W.; Friesenbichler, J.; Liegl-Atzwanger, B.; Kuerzl, G.; Windhager, R.; Leithner, A. Noninflammatory Pseudotumor Simulating Venous Thrombosis after Metal-on-Metal Hip Resurfacing. Orthopedics 2011, 34, e678-681. [Google Scholar] [CrossRef]
- Parfitt, D.J.; Wood, S.N.; Chick, C.M.; Lewis, P.; Rashid, M.H.; Evans, A.R. Common Femoral Vein Thrombosis Caused by a Metal-on-Metal Hip Arthroplasty-Related Pseudotumor. J. Arthroplasty 2012, 27, 1581.e9–1581.e11. [Google Scholar] [CrossRef]
- Algarni, A.D.; Huk, O.L.; Pelmus, M. Metallosis-Induced Iliopsoas Bursal Cyst Causing Venous Obstruction and Lower-Limb Swelling after Metal-on-Metal THA. Orthopedics 2012, 35, e1811-1814. [Google Scholar] [CrossRef]
- Memon, A.R.; Galbraith, J.G.; Harty, J.A.; Gul, R. Inflammatory Pseudotumor Causing Deep Vein Thrombosis after Metal-on-Metal Hip Resurfacing Arthroplasty. J. Arthroplasty 2013, 28, 197.e9-12. [Google Scholar] [CrossRef]
- Kawakita, K.; Shibanuma, N.; Tei, K.; Nishiyama, T.; Kuroda, R.; Kurosaka, M. Leg Edema Due to a Mass in the Pelvis after a Large-Diameter Metal-on-Metal Total Hip Arthroplasty. J. Arthroplasty 2013, 28, 197.e1-4. [Google Scholar] [CrossRef]
- Abdel-Hamid, H.; Miles, J.; Carrington, R.W.J.; Hart, A.; Loh, A.; Skinner, J.A. Combined Vascular and Orthopaedic Approach for a Pseudotumor Causing Deep Vein Thrombosis after Metal-on-Metal Hip Resurfacing Arthroplasty. Case Rep. Orthop. 2015, 2015, 926263. [Google Scholar] [CrossRef]
- Ey, C.; Jl, M.; Jr, V.H.; S, S.; T, W.; A, G.; Cb, C. Metal-on-Metal Total Hip Arthroplasty: Do Symptoms Correlate with MR Imaging Findings? Radiology 2012, 265. [Google Scholar] [CrossRef]
- Bosker, B.H.; Ettema, H.B.; Boomsma, M.F.; Kollen, B.J.; Maas, M.; Verheyen, C.C.P.M. High Incidence of Pseudotumour Formation after Large-Diameter Metal-on-Metal Total Hip Replacement: A Prospective Cohort Study. J. Bone Joint Surg. Br. 2012, 94, 755–761. [Google Scholar] [CrossRef]
- Smeekes, C.; Schouten, B.J.M.; Nix, M.; Ongkiehong, B.F.; Wolterbeek, R.; van der Wal, B.C.H.; Nelissen, R.G.H.H. Pseudotumor in Metal-on-Metal Hip Arthroplasty: A Comparison Study of Three Grading Systems with MRI. Skeletal Radiol. 2018, 47, 1099–1109. [Google Scholar] [CrossRef]
- Moon, J.-K.; Kim, Y.; Hwang, K.-T.; Yang, J.-H.; Ryu, J.-A.; Kim, Y.-H. Prevalence and Natural Course of Pseudotumours after Small-Head Metal-on-Metal Total Hip Arthroplasty: A Minimum 18-Year Follow-up Study of a Previous Report. Bone Jt. J. 2019, 101-B, 317–324. [Google Scholar] [CrossRef]
- Keegan, G.M.; Learmonth, I.D.; Case, C.P. A Systematic Comparison of the Actual, Potential, and Theoretical Health Effects of Cobalt and Chromium Exposures from Industry and Surgical Implants. Crit. Rev. Toxicol. 2008, 38, 645–674. [Google Scholar] [CrossRef]
- Hart, A.J.; Muirhead-Allwood, S.; Porter, M.; Matthies, A.; Ilo, K.; Maggiore, P.; Underwood, R.; Cann, P.; Cobb, J.; Skinner, J.A. Which Factors Determine the Wear Rate of Large-Diameter Metal-on-Metal Hip Replacements? Multivariate Analysis of Two Hundred and Seventy-Six Components. J. Bone Joint Surg. Am. 2013, 95, 678–685. [Google Scholar] [CrossRef]
- Sagoo, N.S.; Sharma, R.; Johnson, C.S.; Stephenson, K.; Aya, K.L. Pseudotumor in the Setting of Metal-on-Metal Total Hip Arthroplasty. Cureus 2020, 12, e8255. [Google Scholar] [CrossRef]
- Carrasco Rodríguez, R.; García Fontán, E.M.; Blanco Ramos, M.; Juaneda Magdalena Benavides, L.; Otero Lozano, D.; Moldes Rodriguez, M.; Cañizares Carretero, M.A. Inflammatory Pseudotumor and Myofibroblastic Inflammatory Tumor. Diagnostic Criteria and Prognostic Differences. Cirugia Espanola 2021, S0009-739X(21)00112-3. [Google Scholar] [CrossRef]
- Angelini, A.; Tiengo, C.; Sonda, R.; Berizzi, A.; Bassetto, F.; Ruggieri, P. One-Stage Soft Tissue Reconstruction Following Sarcoma Excision: A Personalized Multidisciplinary Approach Called “Orthoplasty. ” J. Pers. Med. 2020, 10, 278. [Google Scholar] [CrossRef]
- Angelini, A.; Piazza, M.; Pagliarini, E.; Trovarelli, G.; Spertino, A.; Ruggieri, P. The Orthopedic-Vascular Multidisciplinary Approach Improves Patient Safety in Surgery for Musculoskeletal Tumors: A Large-Volume Center Experience. J. Pers. Med. 2021, 11, 462. [Google Scholar] [CrossRef]
- Huang, S.-H.; Chuang, C.-C.; Huang, C.-C.; Jung, S.-M.; Lee, C.-C. Diagnosis and Treatment of Inflammatory Pseudotumor with Lower Cranial Nerve Neuropathy by Endoscopic Endonasal Approach: A Systematic Review. Diagn. Basel Switz. 2022, 12, 2145. [Google Scholar] [CrossRef]
Figure 1.
Example of two- stage surgical procedure. Preoperative X-ray (a) and CT scan (b) showing pseudotumor. 3D CT scan performed after the first surgery (c) and 3D printed model of the acetabular (d). Post operative X-rays (e,f).
Figure 1.
Example of two- stage surgical procedure. Preoperative X-ray (a) and CT scan (b) showing pseudotumor. 3D CT scan performed after the first surgery (c) and 3D printed model of the acetabular (d). Post operative X-rays (e,f).
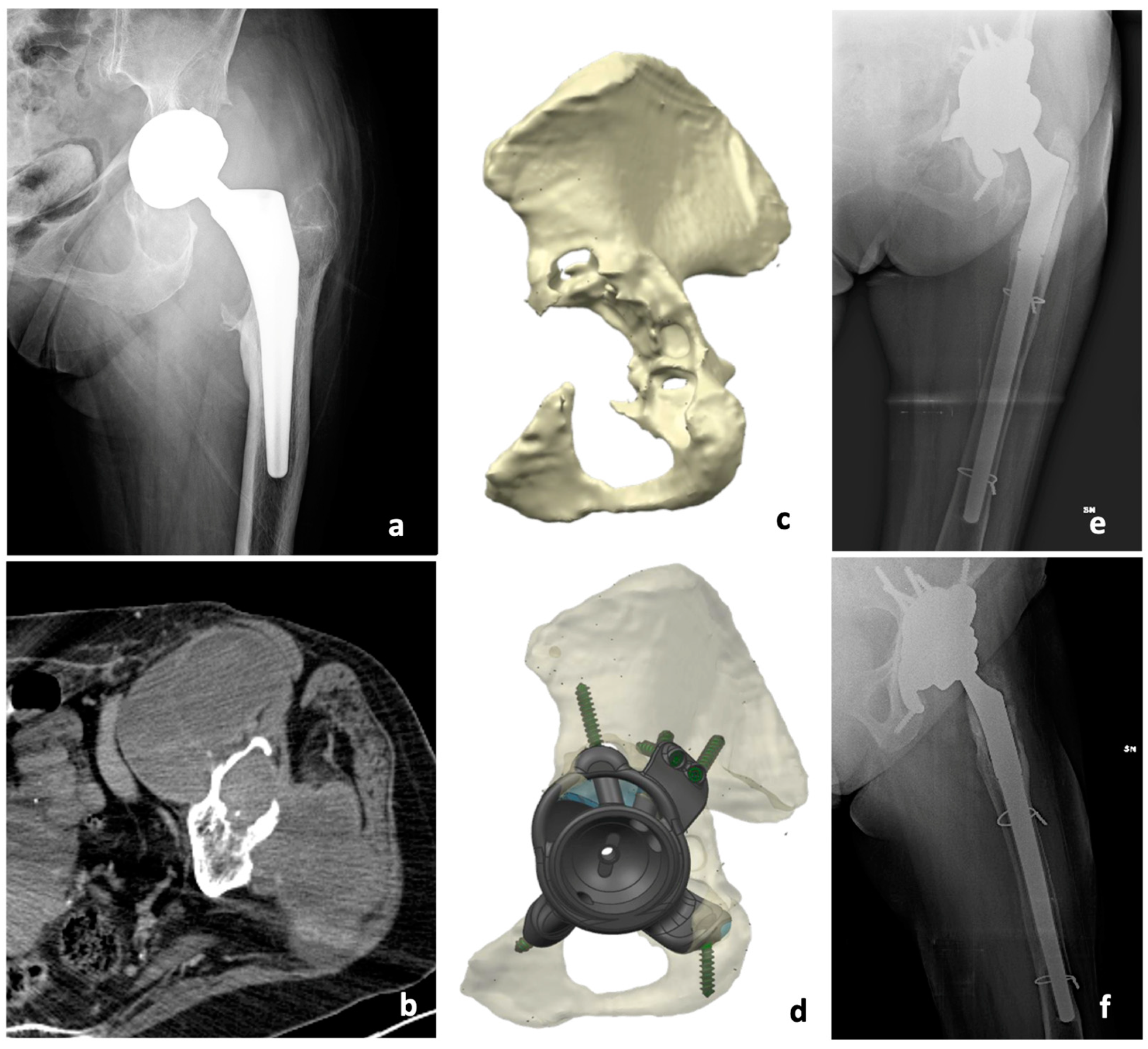
Figure 2.
Scatter plots. Correlation between age at diagnosis of the pseudotumor and years from primary surgery (a) and between age at surgery and postoperative Harry Hip Score (b). In both cases, there were no statistically significant differences.
Figure 2.
Scatter plots. Correlation between age at diagnosis of the pseudotumor and years from primary surgery (a) and between age at surgery and postoperative Harry Hip Score (b). In both cases, there were no statistically significant differences.
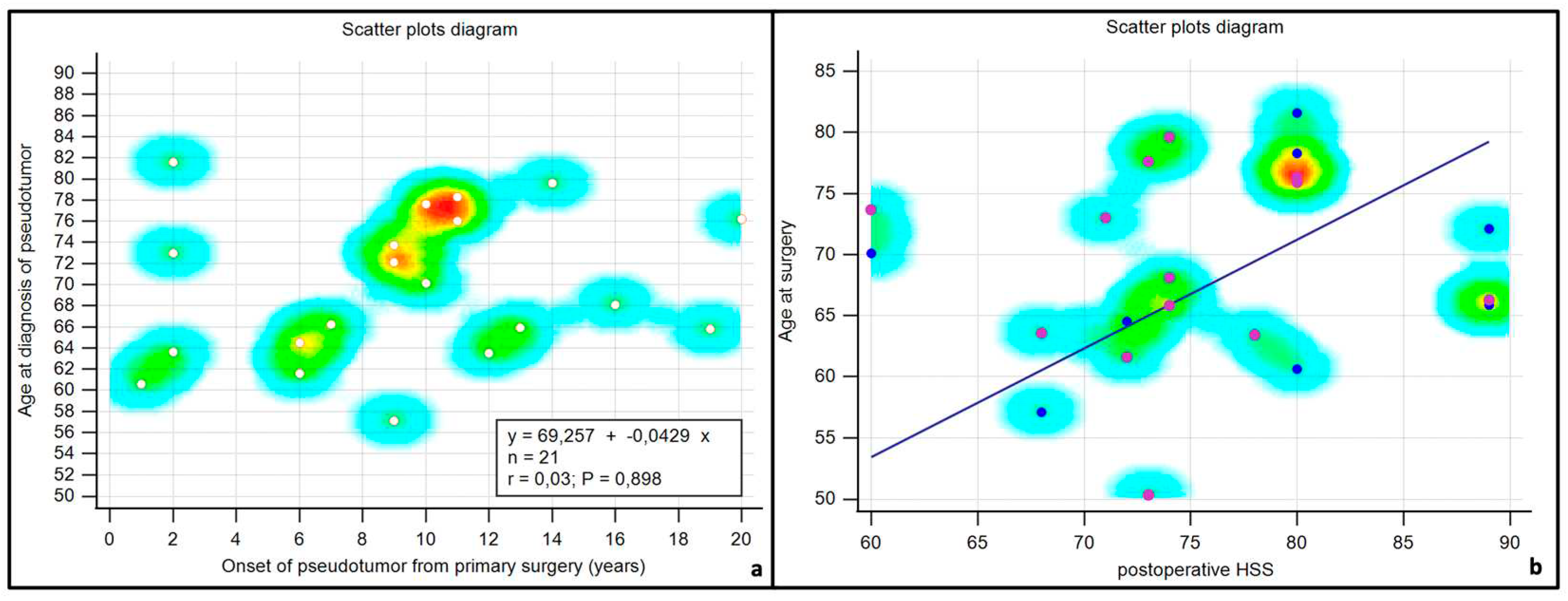
Figure 3.
Kaplan-Maier survival curve. Survival to major complications is compared between one and two-stage procedures.
Figure 3.
Kaplan-Maier survival curve. Survival to major complications is compared between one and two-stage procedures.
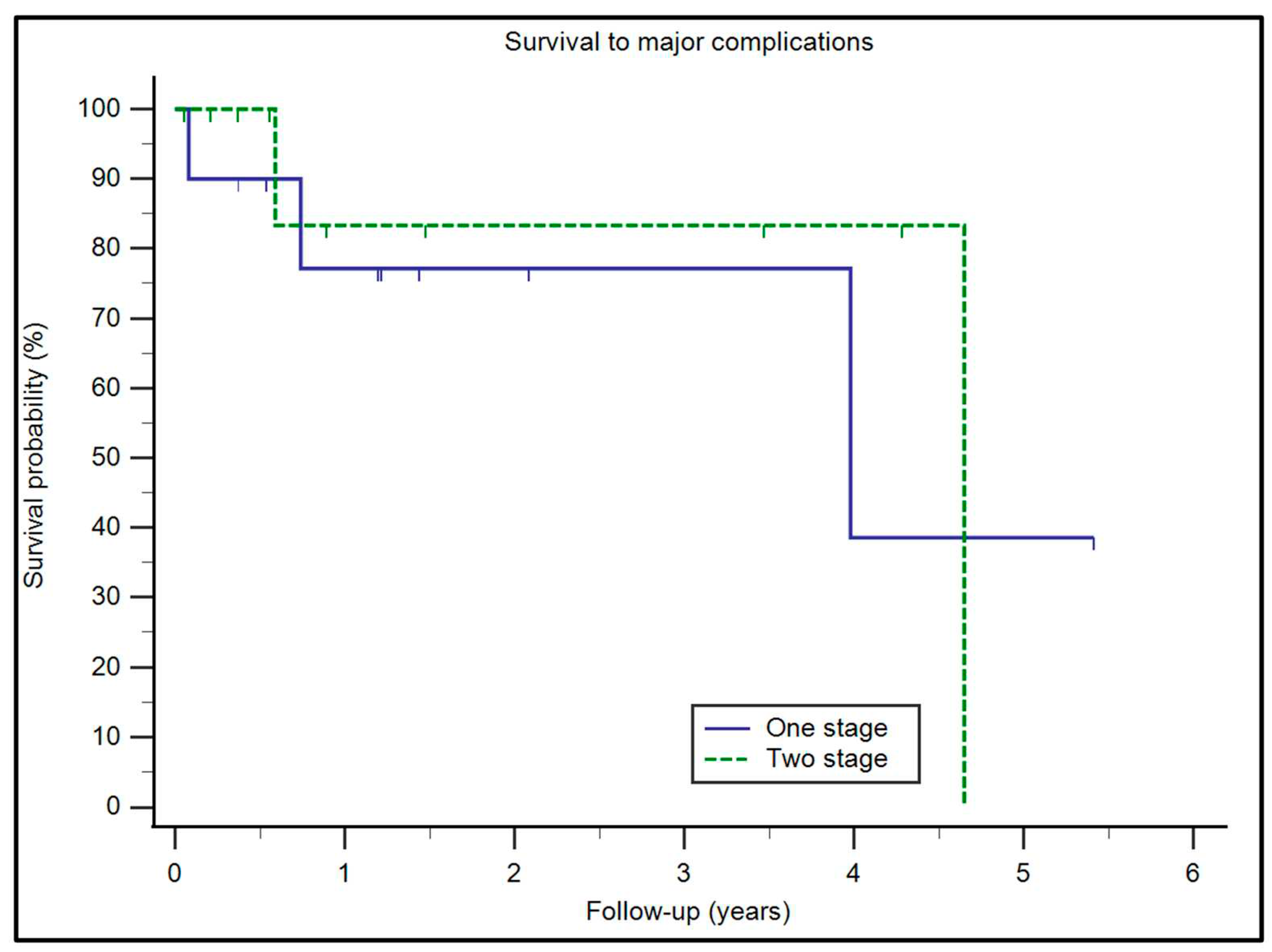

Table 1.
Demographic and clinical characteristics in the cohort of patients.
| Variable | Patients (n=21) |
|---|---|
| Age (at surgery) | 69 range (50-82) |
Sex
|
8 13 |
Tribology
|
7 11 2 1 |
| Time to revision | 10 (yrs) range (1-20) |
Prostheses
|
6 7 7 |
Reconstruction
|
10 10 1 |
Comorbidities
|
4 12 2 3 2 9 |
Abbreviations: MoM=Metal on Meal; MoP=Metal on Polyethylene; CoC=Ceramic on Ceramic; CoP= Ceramic on Polyethylene; Yrs=years.
Table 2.
Paprosky Classification of bony defects and Pseudotumor size.
| Patients | Previous revision surgery | PAPROSKY classification ACETABULAR | PAPROSKY classification FEMUR | Pseudotumor SIZE (Axial-Lateral) cms | Surgery |
|---|---|---|---|---|---|
| 1 (V.G.) | yes | I | IV | 8 x10 | One-stage |
| 2 (A.B.) | no | I | II | 2X2 | One-stage |
| 3 (G.I.) | no | II | I | 4x6 | One-stage |
| 4 (L.C.) | no | II | I | 5x6 | One-stage |
| 5 (M.F.) | yes | I | I | 5x5 | One-stage |
| 6 (L.P.) | no | III | III | 10x9 | Two-stage |
| 7 (L.V.) | yes | III | I | 10x7 | Two-stage |
| 8 (E.S.) | no | III | III | 9x10 | Two-stage |
| 9 (GB.M.) | yes | I | I | 6x7 | Excision only |
| 10 (A.I.) | yes | II | III | 12x15 | Two-stage |
| 11 (KM.V.) | yes | III | IV | 11x20 | One-stage |
| 12 (MA.M.) | no | II | II | 5x5 | One-stage |
| 13 (M.P.) | no | II | II | 10x17 | Two-stage |
| 14 (MG.G.) | yes | III | I | 10x9 | Two-stage |
| 15 (Z.L.) | no | I | III | 7x10 | Two-stage |
| 16(D.G.) | no | II | III | 7x10 | Two-stage |
| 17(F.S.) | no | II | I | 9x6 | One-stage |
| 18(A.F.) | no | II | II | 7x7 | Two-stage |
| 19(M.D.) | yes | III | I | 9x9 | Two-stage |
| 20(G.C.) | no | II | I | 5x8 | One-stage |
| 21(G.L.) | no | II | I | 9x10 | One-stage |
Table 3.
Pre and post operative HHS and improvement.
| Patient | HHS preoperative | HHS postoperative | Improvement HHS | P-value |
|---|---|---|---|---|
| 1 (V.G.) | 41 | 89 | 48 | |
| 2 (A.B.) | 45 | 60 | 15 | |
| 3 (G.I.) | 33 | 74 | 41 | |
| 4 (L.C.) | 25 | 71 | 46 | |
| 5 (M.F.) | 32 | 72 | 40 | |
| 6 (L.P.) | 42 | 80 | 38 | |
| 7 (L.V.) | 39 | 72 | 33 | |
| 8 (E.S.) | 42 | 74 | 32 | |
| 9 (GB.M.) | 43 | 80 | 37 | |
| 10 (A.I.) | 18 | 68 | 50 | |
| 11 (KM.V.) | 36 | 73 | 37 | |
| 12 (MA.M.) | 29 | 78 | 49 | |
| 13 (M.P.) | 27 | 73 | 46 | |
| 14 (MG.G.) | 36 | 80 | 44 | |
| 15 (Z.L.) | 25 | 60 | 35 | |
| 16(D.G.) | 25 | 68 | 43 | |
| 17(F.S.) | 33 | 74 | 41 | |
| 18(A.F.) | 36 | 80 | 44 | |
| 19(M.D.) | 41 | 89 | 48 | |
| 20(G.C.) | 41 | 89 | 48 | |
| 21(G.L.) | 39 | 80 | 41 | |
| Mean | 35 | 75 | 41 | P<0.0001 |
HHS = Harris Hip Score; Comparison between preoperative and postoperative HHS performed using Student t test for paired samples.
Table 4.
Surgical procedure and complications.
| Patient | Surgery | Tribology | Complications (according to Henderson) | Minor | Major |
|---|---|---|---|---|---|
| 1 (V.G.) | One-stage | MoP | IV | Deep infection | |
| 2 (A.B.) | One-stage | MoM | |||
| 3 (G.I.) | One-stage | MoP | |||
| 4 (L.C.) | One-stage | MoP | |||
| 5 (M.F.) | One-stage | MoP | |||
| 6 (L.P.) | Two-stage | MoP | |||
| 7 (L.V.) | Two-stage | MoP | IV | Deep infection | |
| 8 (E.S.) | Two-stage | MoM | |||
| 9 (GB.M.) | Excision only | MoP | |||
| 10 (A.I.) | Two-stage | MoP | I | Superficial infection | Death at 3 months |
| 11 (KM.V.) | One-stage | MoM | IV | Deep infection | |
| 12 (MA.M.) | One-stage | MoM | Death at 1 year | ||
| 13 (M.P.) | Two-stage | MoM | |||
| 14 (MG.G.) | Two-stage | CoP | |||
| 15 (Z.L.) | Two-stage | MoM | |||
| 16(D.G.) | Two-stage | MoM | I | Superficial infection | |
| 17(F.S.) | One-stage | MoP | |||
| 18(A.F.) | Two-stage | MoP | |||
| 19(M.D.) | Two-stage | MoP | I | Femoral nerve injury, sensosy deficit | |
| 20(G.C.) | One-stage | CoC | |||
| 21(G.L.) | One-stage | CoC |
Abbreviations: MoM=Metal on Meal; MoP=Metal on Polyethylene; CoC=Ceramic on Ceramic; CoP= Ceramic on Polyethylene; Yrs=years.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



