Submitted:
15 January 2024
Posted:
16 January 2024
You are already at the latest version
Abstract
Background: A careful work-up before Transcatheter aortic valve replacement (TAVR) consists not only of measuring anatomical conditions but also assessment of frailty. Previous studies have evaluated body composition parameters, primarily fat and muscle mass. Few data are available on other frailty parameters, which, however, can be easily determined by pre-TAVR computed tomography (CT).
Objectives: The primary objective was to investigate the impact of total muscle area (TMA) and visceral adipose tissue (VAT), as frailty parameters, on 5-year all-cause mortality in patients undergoing TAVR.
Methods: Between 01/2017 and 12/2018, consecutive TAVR patients undergoing CT-angiography scan enabling TMA and VAT measurement were included. A single axial image was acquired at the level of the middle third lumbar vertebra to perform TMA and VAT measurements using dedicated slicing software (Sliceomatic, TomoVision).
Results: A total of 500 patients qualified for TMA analysis. Age was not associated with a higher risk of 5-year mortality HR 1.02 (95% CI: 0.998 - 1.049; p=0.069). Body surface area normalized TMA (nTMA) was significantly associated with 5-year all-cause mortality (HR 0.927, 95% CI: 0.927-0.997; p= 0.033), while VAT had no effect (HR 1.002, 95% CI: 0.99-1.015; p= 0.7). The effect of nTMA on 5- year all-cause mortality was gender-dependent: the protective effect of higher nTMA was found in male patients (pinteraction: sex * nTMA = 0.007). The combination of normalized TMA and VAT was not associated with higher mortality rates.
Conclusion: Normalized TMA derived from routine CT before TAVR complements frailty assessment in patients undergoing TAVR.
Keywords:
aortic valve stenosis
; body composition parameters
; CT scan
; sarcopenia
; frailty
Introduction
Due to significant advancements in TAVR safety, efficacy and noninferiority to surgical aortic valve re-placement (SAVR) the number of TAVR procedures is rising.1-6
A meaningful examination prior to TAVR consists not only of measuring anatomic features such as femoral access size, valve type and size to be implanted, or determining the coronary status, but also obtaining parameters of general medical condition and frailty. While measuring anatomical structures is standardized and precise by using TAVR CT scan, assessment of frailty may be more difficult to objectify, and there is no consensus on its assessment. Although Society of Thoracic Surgeons (STS) and European System for Cardiac Operative Risk Evaluation (EuroSCORE)-2 scores are an integral part of any heart team evaluation to predict outcomes after TAVR, a comprehensive frailty assessment should be performed.7 Previous studies have analysed factors such as age, cognitive impairment, physical weakness, and also laboratory values such as anaemia and hypoalbuminemia.8 There is a great heterogeneity in clinical vulnerability, including nutritional status, physical and cognitive impairment, and psychosocial risk factors.9
As an objective frailty parameter, body composition parameters have been analysed in previous studies. In particular, two tissues were measured for risk assessment, namely muscle mass and fat mass. These parameters were evaluated not only for cardiac risk but also for noncardiac risk assessment. 10-16 With respect to muscle mass, studies have shown that sarcopenia is associated with frailty in the elderly population.17 For example, quadriceps depth measured by ultrasound was a predictor of adverse postoperative outcomes, including discharge to a skilled nursing facility and delirium.18 Measurement of sarcopenia using the psoas muscle area (PMA) has also been evaluated.19,20 Studies have been performed with regard to subcutaneous and visceral adipose tissue fat mass, analyzing the effects on noncardiac and cardiac perioperative outcomes and survival.21,22
In summary, data are available for both muscle mass and visceral adipose tissue (VAT) to support them as predictors of poor outcome after surgery. However, regarding muscle mass primarily PMA was measured and only spare data is available on the effects of total muscle area (TMA) which includes the total muscle mass of a given segment. Consequently also the impact of TMA and VAT interaction on the outcome after TAVR is unclear.
We aimed to identify an objective marker of frailty. We hypothesized that low TMA is associated with poor survival and, second, that the combination of low TMA and low VAT may be a stronger predictor of poor outcome in patients after TAVR.
Methods
Study design and population
All patients undergoing TAVR at our university-based tertiary referral center are consecutively recorded in a prospective institutional database as part of the Swiss TAVI registry, which is mandated by the national health authorities (registered at clinicaltrials.gov with NCT01368250).23 The present analysis included all patients with severe aortic valve stenosis who underwent transfemoral (TF)-TAVR with contemporary balloon-expandable (SAPIEN 3, SAPIEN 3 Ultra [Edwards Lifesciences]) or self-expanding devices (Evolut R/PRO [Medtronic]) between January 2017 and December 2018. The registry was approved by the local ethics committee. All patients provided written informed consent for participation.
CT assessment
All patients who had a CT scan before TAVR were included. A volumetric assessment of each CT scan was performed. Here, a single axial image was acquired at the level of the middle third lumbar vertebra (L3) and analysed with dedicated software (Sliceomatic, TomoVision, 3280 chemin Milletta, Magog, J1X 0R4, Canada) by measuring visceral adipose tissue (VAT) area (cm2) and total muscle area (TMA). (Figure 1) TMA was normalized by division with BSA. VAT was measured in cm2.
Data collection
Baseline clinical, procedural, and follow-up data were prospectively recorded in a web-based database held at the Clinical Trials Unit of the University of Bern. Clinical follow-up was obtained from standardized telephone interviews, medical reports, and hospital discharge summaries. All adverse events were independently adjudicated by a clinical event committee according to Valve Academic Research Consortium (VARC) criteria applicable at the time of the procedure of the university of Bern.24
Endpoints
The primary objective endpoint of this analysis was to assess the impact of normalized total muscle area (TMA) and visceral adipose tissue (VAT) on 5-year all-cause mortality.
Statistical analysis
Categorical variables are presented as frequencies and percentages. Continuous variables are presented as mean and standard deviation if they are normally distributed variables and with median and interquartile range (IQR) otherwise. Univariable and multivariable logistic regression and Cox proportional hazard models were used to calculate hazard ratios (HRs), respectively. The Youden index was used to calculate cutoff values for normalized TMA and VAT in relation to 5-year all-cause mortality. A p value < 0.05 was considered statistically significant, and all calculations were performed using R version 4.0.2.25
Results
604 patients underwent TAVR between 01/2017 and 12/2018. Due to image cropping TMA and VAT measurements could be performed in 500 patients (82.8% of the overall patient number in the study period).
The mean age of this cohort was 82.8 years (IQR: 79.0-86.5), and 304 (52.1%) patients were female (Table 1). Age was not associated with a higher risk of 5-year mortality with HR 1.023 (95% CI: 0.998 - 1.049; p=0.069).
Body mass index (kg/m2) was also not associated with higher 5-year mortality with a HR of 1.005 (95% CI: 0.97-1.05; p= 0.8).
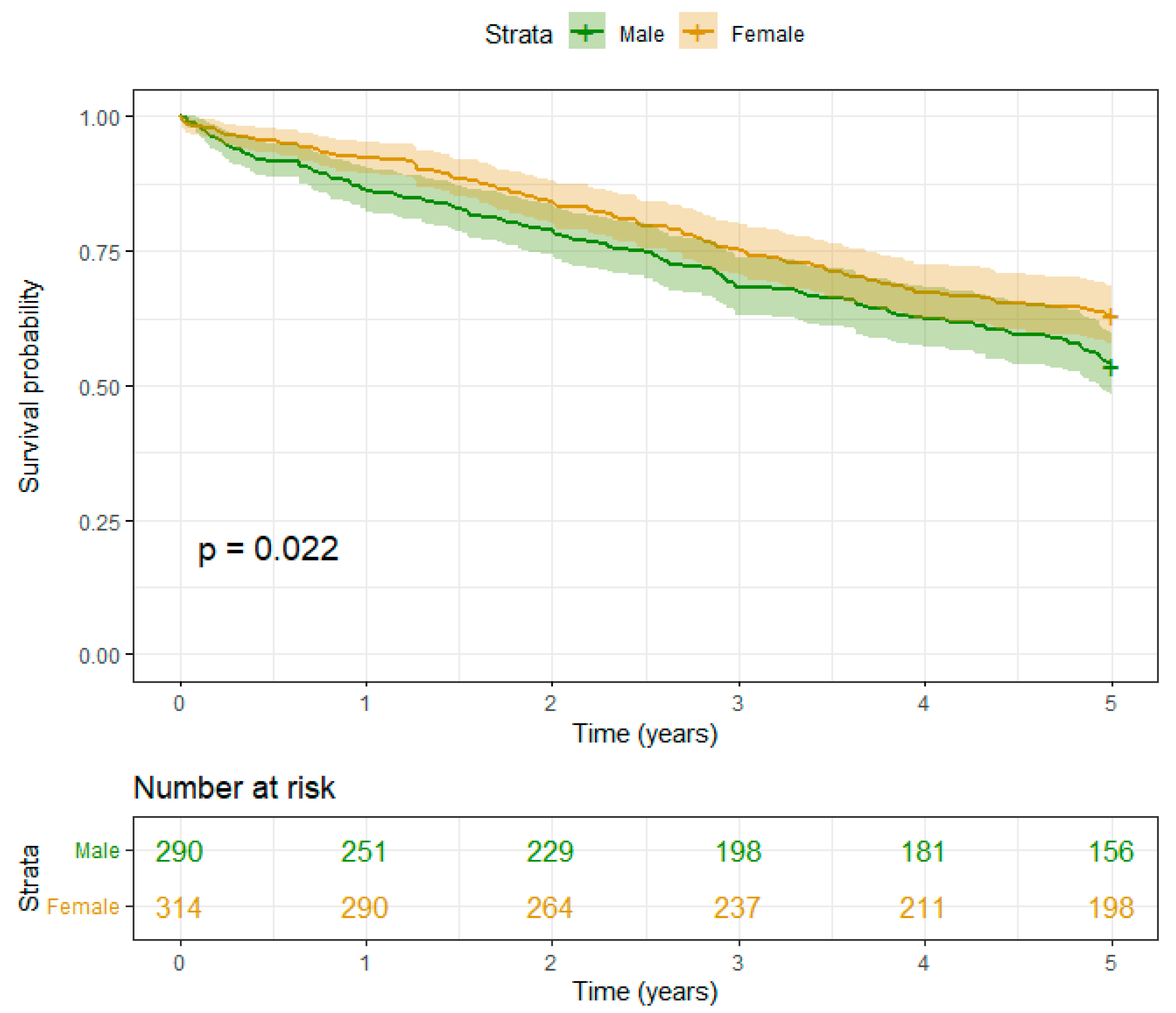
However, female patients had better survival compared to male patients with a HR of 0.036, 95% CI: 0.003-0.39, p=0.007) in the 5 year follow up period. (Table 2, Figure 3 A)
Further,a significant interaction between female and nTMA was observed (HR: 1.048, 95%-CI: 1.013 - 1.084; p=0.007) (Table 2).
Regarding the individual CT tissue parameters, the following results were observed:
- I) Muscle mass:
PMA was not associated with higher 5-years mortality with HR 0.970 (95% CI: 0.921- 1.026; p=0.3).
nTMA was significantly associated with higher 5-year all-cause mortality with HR 0.96 (95% CI: 0.927-0.997; p= 0.033).
When analyzing sex-specific outcomes, we observed a higher survival probability for the whole 5 year period with p=0.022 in female patients compared to male patients. (Table2) (Figure 3A). A protective effect of higher nTMA levels was observed in male patients (pinteraction: sex * TMA (normalized) = 0.007) (Figure 2, Table 3).
- II) Fat mass:
Regarding VAT, no significant difference was observed HR 1.002 (95% CI: 0.99-1.015; p= 0.7). No gender difference was also observed with HR 0.99 (95% CI: 0.99-1.001; p= 0.2) (Table2).
- III) Interaction of Muscle and Fat mass:
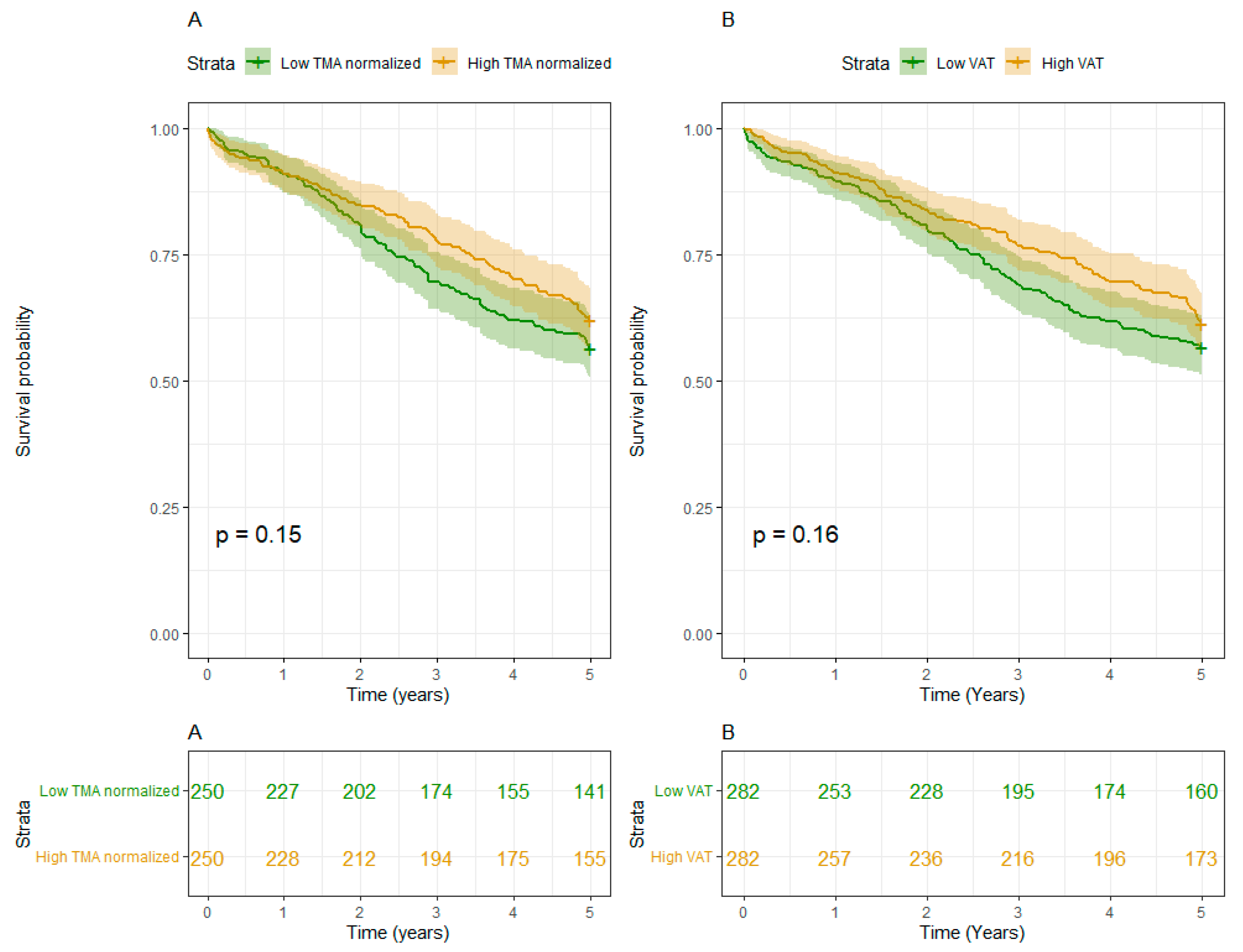
The combination of nTMA with VAT (cm2) was not associated with higher mortality and HR 1.00 (95% CI:1.00- 1.00; p = 0.5) (Table2). Low TMA and low VAT were rather associated with mortality than high TMA and high VAT in both sexes. (Figure 3B)
Figure 3.
A. 5 years Survival curves, associated p-values from the log rank test and number at risk stratified according to gender (A). B. 5 years Survival curves, associated p-values from the log rank test and number at risk stratified according normalized TMA values (A) and VAT values (B). Legend: TMA means total muscle area; VAT means visceral adipose tissue.
Figure 3.
A. 5 years Survival curves, associated p-values from the log rank test and number at risk stratified according to gender (A). B. 5 years Survival curves, associated p-values from the log rank test and number at risk stratified according normalized TMA values (A) and VAT values (B). Legend: TMA means total muscle area; VAT means visceral adipose tissue.
Discussion
In the present study, we investigated various body composition parameters for the purpose of a comprehensive assessment of frailty using the obligatory CT scan before TAVR. Our study showed that low TMA, i.e., sarcopenia, was associated with higher 5-year all-cause mortality and was an additional tool for comprehensive assessment of frailty. The effect of nTMA on 5-year all-cause mortality was gender-dependent. Here the protective effect of higher nTMA levels was found in male patients (pinteraction: sex *nTMA = 0.007). But PMA and VAT were not associated with higher 5-year mortality. Also, the combination of TMA and VAT was not a stronger parameter for lower survival.
In the existing body of literature, risk assessment predominantly revolves around the investigation of two primary tissues, namely muscle mass and fat mass. Additionally, comprehensive frailty assessments often incorporate further parameters, such as low bone mineral density. However, although low BMD is significantly associated with increased cardiovascular risk regarding the interaction of low bone mineral density and TAVR outcome only spare data is available. 26,27
Regarding fat mass, subcutaneous fat and visceral adipose tissue have been investigated in several previous studies analyzing the effects on noncardiac and cardiac perioperative outcomes and survival.21,22 For TAVR, a previous study demonstrated that VAT was not associated with significant differences, but patients with higher subcutaneous adipose tissue (SAT) had a significantly lower incidence of composite outcome and all-cause death compared with patients with lower SAT.22 In another study, it was observed that low volume of subcutaneous and visceral adipose tissue was associated with worse clinical outcomes than high volume in patients undergoing TAVR.28 Thus, with regard to VAT, there are conflicting data in the literature. Previous studies have also analysed adipose tissue in non-cardiac procedures. Thus, in patients with locally advanced rectal cancer, a high visceral to subcutaneous adipose tissue ratio is the body composition parameter most strongly associated with poor early postoperative outcomes.29 The ratio of visceral to subcutaneous fat also has a significant impact on postoperative complications in colorectal cancer.30
In our cohort, VAT was not significantly associated with higher mortality. Even after a sex-specific analysis, no significant difference was found between a low and a high VAT value. Whether adipose tissue has different effects on outcome depending on cardiac or noncardiac interventions needs to be investigated in further studies.
Regarding muscle mass, valuable studies have evaluated PMA for the diagnosis of sarcopenia, as it is one of the key components of the frailty syndrome. In noncardiac surgery such as elective spine surgery, PMA was a predictor of the need for intensive care and postoperative blood transfusion.31 Moreover, in patients with acute mesenteric ischemia, postoperative complications and 30-day mortality were lower in patients with low PMA.32 Sarcopenia, defined by psoas muscle mass, was also an independent predictor of 2-year mortality, major complications, and severity of complications after major colorectal surgery.33 PMA was an objective frailty assessment tool predicting early morbidity and mortality following spine surgery.21 Also in cardiac surgery low PMA was associated with worse outcome.34,35 Low PMA was also associated with increased length of stay in older adults undergoing cardiac surgical procedures.36 In cardiac procedures, PMA was described as a relevant predictor of poor outcome. In patients undergoing TAVR, the PMA index significantly predicted 1-year risk-adjusted mortality and long-term mortality, as well as risk-adjusted severe morbidity, prolonged ventilation, length of stay, hospital discharge, and hospital costs.37 But in the present study low PMA was not associated with higher 5-year mortality. Nevertheless nTMA, which includes the total muscle mass of a given segment was significantly associated with higher 5y mortality. This shows the importance of nTMA measurement since it could be a stronger predictor for frailty assessment compared to PMA and should performed regularly
Further In the present study the protective effect of higher nTMA levels was found in male patients. Gender differences in this regard need to be investigated in further studies.
In summary, normalized Total Muscle Area (nTMA) has proven to be a robust predictor of all-cause mortality. This parameter emerges as a novel, valuable, and supplementary tool, complementing well-established frailty prediction tools. Furthermore, its relevance extends to long-term survival post-Transcatheter Aortic Valve Replacement (TAVR), reinforcing its utility in predicting outcomes beyond frailty assessment alone.
Study Limitations
The principal constraint in this study is rooted in the intricate nature of the frailty syndrome. Notably, body composition parameters, being inherently imaging-related, constitute only a partial scope of the comprehensive frailty assessment. It is imperative to recognize that the evaluation of frailty should transcend the sole consideration of imaging parameters. Nevertheless, we posit that these objective parameters can significantly contribute to a holistic understanding of frailty when opportunistically integrated with CT scans, supplementing conventional factors such as age, cognitive impairment, physical weakness, and occupational values.
Moreover, the gender-specific disparities remain ambiguous. The rationale behind the impact of total muscle area on outcomes in males, while not evident in females, lacks clarity. This disparity necessitates further scrutiny in subsequent investigations to elucidate the underlying mechanisms and discern any potential gender-specific nuances impacting the observed outcomes.
Data Availability Statements
The data underlying this article is available in the TAVI Register of Bern and will be shared on reasonable request to the corresponding author.
Acknowledgments
Sources of funding: None.
Disclosures
Thomas Pilgrim reports research, travel or educational grant to the institution without personal remuneration from Biotronik, Boston Scientific, Edwards Lifesciences, and ATSens; speaker fees and consultancy fees to the institution from Biotronik, Boston Scientific, Edwards Lifesciences, Abbott, Medtronic, Biosensors, and Highlife. Dr. Windecker reports research and educational grants to the institution from Abbott, Amgen, Astra Zeneca, BMS, Bayer, Biotronik, Boston Scientific, Cardinal Health, CardioValve, CSL Behring, Daiichi Sankyo, Edwards Lifesciences, Guerbet, InfraRedx, Johnson & Johnson, Medicure, Medtronic, Novartis, Polares, OrPha Suisse, Pfizer, Regeneron, Sanofi-Aventis, Sinomed, Terumo, V-Wave. Dr. Windecker serves as unpaid advisory board member and/or unpaid member of the steering/executive group of trials funded by Abbott, Abiomed, Amgen, Astra Zeneca, BMS, Boston Scientific, Biotronik, Cardiovalve, Edwards Lifesciences, MedAlliance, Medtronic, Novartis, Polares, Sinomed, V-Wave and Xeltis, but has not received personal payments by pharmaceutical companies or device manufacturers. He is also member of the steering/executive committee group of several investigator-initiated trials that receive funding by industry without impact on his personal remuneration. Dr. Windecker is an unpaid member of the Pfizer Research Award selection committee in Switzerland and of the Women as One Awards Committee. The authors have no relationships relevant to the contents of this article to disclose.
Abbreviations
| TAVR | Transcatheter aortic valve replacement |
| AS | Aortic valve stenosis |
| TMA | Total muscle area |
| nTMA | normalized total muscle area |
| PMA | Psoas muscle area |
| VAT | Visceral adipose tissue |
References
- Mack, M.J.; Leon, M.B.; Thourani, V.H.; Makkar, R.; Kodali, S.K.; Russo, M.; Kapadia, S.R.; Malaisrie, S.C.; Cohen, D.J.; Pibarot, P.; et al. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1695–1705. [Google Scholar] [CrossRef]
- Popma, J.J.; Deeb, G.M.; Yakubov, S.J.; Mumtaz, M.; Gada, H.; O’Hair, D.; Bajwa, T.; Heiser, J.C.; Merhi, W.; Kleiman, N.S.; et al. Transcatheter Aortic-Valve Replacement with a Self-Expanding Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1706–1715. [Google Scholar] [CrossRef]
- Reardon, M.J.; Van Mieghem, N.M.; Popma, J.J.; Kleiman, N.S.; Søndergaard, L.; Mumtaz, M.; Adams, D.H.; Deeb, G.M.; Maini, B.; Gada, H.; et al. Surgical or Transcatheter Aortic-Valve Replacement in Intermediate-Risk Patients. N. Engl. J. Med. 2017, 376, 1321–1331. [Google Scholar] [CrossRef]
- Leon, M.B.; Smith, C.R.; Mack, M.J.; Makkar, R.R.; Svensson, L.G.; Kodali, S.K.; Thourani, V.H.; Tuzcu, E.M.; Miller, D.C.; Herrmann, H.C.; et al. Transcatheter or Surgical Aortic-Valve Replacement in Intermediate-Risk Patients. N. Engl. J. Med. 2016, 374, 1609–1620. [Google Scholar] [CrossRef]
- Dowling, C.; Kondapally Seshasai, S.R.; Firoozi, S.; Brecker, S.J. Transcatheter aortic valve replacement versus surgery for symptomatic severe aortic stenosis: A reconstructed individual patient data meta-analysis. Catheter. Cardiovasc. Interv. 2020, 96, 158–166. [Google Scholar] [CrossRef]
- Makkar, R.R.; Thourani, V.H.; Mack, M.J.; Kodali, S.K.; Kapadia, S.; Webb, J.G.; Yoon, S.H.; Trento, A.; Svensson, L.G.; Herrmann, H.C.; et al. Five-Year Outcomes of Transcatheter or Surgical Aortic-Valve Replacement. N. Engl. J. Med. 2020, 382, 799–809. [Google Scholar] [CrossRef]
- Grossman, Y.; Barbash, I.M.; Fefer, P.; Goldenberg, I.; Berkovitch, A.; Regev, E.; Fink, N.; Ben-Zekry, S.; Brodov, Y.; Kogan, A.; et al. Addition of albumin to Traditional Risk Score Improved Prediction of Mortality in Individuals Undergoing Transcatheter Aortic Valve Replacement. J. Am. Geriatr. Soc. 2017, 65, 2413–2417. [Google Scholar] [CrossRef]
- Afilalo, J.; Lauck, S.; Kim, D.H.; Lefèvre, T.; Piazza, N.; Lachapelle, K.; Martucci, G.; Lamy, A.; Labinaz, M.; Peterson, M.D.; et al. Frailty in Older Adults Undergoing Aortic Valve Replacement: The FRAILTY-AVR Study. J. Am. Coll. Cardiol. 2017, 70, 689–700. [Google Scholar] [CrossRef] [PubMed]
- Søndergaard, L.; Kirk, B.H.; Jørgensen, T.H. Frailty: An Important Measure in Patients Considered for Transcatheter Aortic Valve Replacement. JACC Cardiovasc. Interv. 2018, 11, 404–406. [Google Scholar] [CrossRef] [PubMed]
- Ilic, I.; Faron, A.; Heimann, M.; Potthoff, A.L.; Schäfer, N.; Bode, C.; Borger, V.; Eichhorn, L.; Giordano, F.A.; Güresir, E.; et al. Combined Assessment of Preoperative Frailty and Sarcopenia Allows the Prediction of Overall Survival in Patients with Lung Cancer (NSCLC) and Surgically Treated Brain Metastasis. Cancers 2021, 13. [Google Scholar] [CrossRef] [PubMed]
- Bentov, I.; Kaplan, S.J.; Pham, T.N.; Reed, M.J. Frailty assessment: from clinical to radiological tools. Br. J. Anaesth. 2019, 123, 37–50. [Google Scholar] [CrossRef]
- Flexman, A.M.; Street, J.; Charest-Morin, R. The impact of frailty and sarcopenia on patient outcomes after complex spine surgery. Curr. Opin. Anaesthesiol. 2019, 32, 609–615. [Google Scholar] [CrossRef]
- Kołodziejska, K.; Witowski, J.; Tylec, P.; Grochowska, A.; Przytuła, N.; Lis, M.; Pędziwiatr, M.; Rubinkiewicz, M. Radiological Features for Frailty Assessment in Patients Requiring Emergency Laparotomy. J. Clin. Med. 2022, 11. [Google Scholar] [CrossRef]
- de Bree, R.; Meerkerk, C.D.A.; Halmos, G.B.; Mäkitie, A.A.; Homma, A.; Rodrigo, J.P.; López, F.; Takes, R.P.; Vermorken, J.B.; Ferlito, A. Measurement of Sarcopenia in Head and Neck Cancer Patients and Its Association With Frailty. Front. Oncol. 2022, 12, 884988. [Google Scholar] [CrossRef]
- Okamura, H.; Kimura, N.; Mieno, M.; Yuri, K.; Yamaguchi, A. Preoperative sarcopenia is associated with late mortality after off-pump coronary artery bypass grafting. Eur. J. Cardiothorac. Surg. 2020, 58, 121–129. [Google Scholar] [CrossRef]
- Canales, C.; Mazor, E.; Coy, H.; Grogan, T.R.; Duval, V.; Raman, S.; Cannesson, M.; Singh, S.P. Preoperative Point-of-Care Ultrasound to Identify Frailty and Predict Postoperative Outcomes: A Diagnostic Accuracy Study. Anesthesiology 2022, 136, 268–278. [Google Scholar] [CrossRef]
- Meng, N.H.; Li, C.I.; Liu, C.S.; Lin, W.Y.; Lin, C.H.; Chang, C.K.; Li, T.C.; Lin, C.C. Sarcopenia Defined by Combining Height- and Weight-Adjusted Skeletal Muscle Indices is Closely Associated With Poor Physical Performance. J. Aging Phys. Act. 2015, 23, 597–606. [Google Scholar] [CrossRef]
- McIsaac, D.I. Preoperative Frailty Assessment: An Opportunity to Add Value to Perioperative Care. Anesthesiology 2022, 136, 255–257. [Google Scholar] [CrossRef]
- Mamane, S.; Mullie, L.; Piazza, N.; Martucci, G.; Morais, J.; Vigano, A.; Levental, M.; Nelson, K.; Lange, R.; Afilalo, J. Psoas Muscle Area and All-Cause Mortality After Transcatheter Aortic Valve Replacement: The Montreal-Munich Study. Can. J. Cardiol. 2016, 32, 177–182. [Google Scholar] [CrossRef]
- Saji, M.; Lim, D.S.; Ragosta, M.; LaPar, D.J.; Downs, E.; Ghanta, R.K.; Kern, J.A.; Dent, J.M.; Ailawadi, G. Usefulness of Psoas Muscle Area to Predict Mortality in Patients Undergoing Transcatheter Aortic Valve Replacement. Am. J. Cardiol. 2016, 118, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Mok, M.; Allende, R.; Leipsic, J.; Altisent, O.A.; Del Trigo, M.; Campelo-Parada, F.; DeLarochellière, R.; Dumont, E.; Doyle, D.; Côté, M.; et al. Prognostic Value of Fat Mass and Skeletal Muscle Mass Determined by Computed Tomography in Patients Who Underwent Transcatheter Aortic Valve Implantation. Am. J. Cardiol. 2016, 117, 828–833. [Google Scholar] [CrossRef]
- Okuno, T.; Koseki, K.; Nakanishi, T.; Ninomiya, K.; Tomii, D.; Tanaka, T.; Sato, Y.; Osanai, A.; Sato, K.; Koike, H.; et al. Prognostic Impact of Computed Tomography-Derived Abdominal Fat Area on Transcatheter Aortic Valve Implantation. Circ. J. 2018, 82, 3082–3089. [Google Scholar] [CrossRef] [PubMed]
- Stortecky, S.; Franzone, A.; Heg, D.; Tueller, D.; Noble, S.; Pilgrim, T.; Jeger, R.; Toggweiler, S.; Ferrari, E.; Nietlispach, F.; et al. Temporal trends in adoption and outcomes of transcatheter aortic valve implantation: a SwissTAVI Registry analysis. European heart journal. Qual. Care Clin. Outcomes 2019, 5, 242–251. [Google Scholar] [CrossRef]
- Tomii, D.; Okuno, T.; Heg, D.; Lanz, J.; Praz, F.; Stortecky, S.; Windecker, S.; Pilgrim, T. Validation of the VARC-3 Technical Success Definition in Patients Undergoing TAVR. JACC Cardiovasc. Interv. 2022, 15, 353–364. [Google Scholar] [CrossRef]
- R Core Team. R: A language and environment for statistical computing. R. Foundation for Statistical; Computing: Vienna, Austria,, 2020; https://www.R-project.org/.
- Rodríguez, A.J.; Scott, D.; Hodge, A.; English, D.R.; Giles, G.G.; Ebeling, P.R. Associations between hip bone mineral density, aortic calcification and cardiac workload in community-dwelling older Australians. Osteoporos. Int. 2017, 28, 2239–2245. [Google Scholar] [CrossRef]
- Shi, L.; Yu, X.; Pang, Q.; Chen, X.; Wang, C. The associations between bone mineral density and long-term risks of cardiovascular disease, cancer, and all-cause mortality. Front. Endocrinol. 2022, 13, 938399. [Google Scholar] [CrossRef]
- Shibata, K.; Yamamoto, M.; Yamada, S.; Kobayashi, T.; Morita, S.; Kagase, A.; Tokuda, T.; Shimura, T.; Tsunaki, T.; Tada, N.; et al. Clinical Outcomes of Subcutaneous and Visceral Adipose Tissue Characteristics Assessed in Patients Underwent Transcatheter Aortic Valve Replacement. CJC Open 2021, 3, 142–151. [Google Scholar] [CrossRef]
- Bocca, G.; Mastoridis, S.; Yeung, T.; James, D.R.C.; Cunningham, C. Visceral-to-subcutaneous fat ratio exhibits strongest association with early post-operative outcomes in patients undergoing surgery for advanced rectal cancer. Int. J. Colorectal Dis. 2022, 37, 1893–1900. [Google Scholar] [CrossRef]
- He, A.Q.; Li, C.Q.; Zhang, Q.; Liu, T.; Liu, J.; Liu, G. Visceral-to-Subcutaneous Fat Ratio Is a Potential Predictor of Postoperative Complications in Colorectal Cancer. Med. Sci. Monit. 2021, 27, e930329. [Google Scholar] [CrossRef]
- Pernik, M.N.; Hicks, W.H.; Akbik, O.S.; Nguyen, M.L.; Luu, I.; Traylor, J.I.; Deme, P.R.; Dosselman, L.J.; Hall, K.; Wingfield, S.A.; et al. Psoas Muscle Index as a Predictor of Perioperative Outcomes in Geriatric Patients Undergoing Spine Surgery. Global Spine J. 2023, 13, 2016–2024. [Google Scholar] [CrossRef]
- Miao, S.L.; Ye, X.N.; Lin, T.T.; Qiu, Y.H.; Huang, J.Y.; Zheng, X.W.; Chen, F.F. The psoas muscle density as a predictor of postoperative complications and 30-day mortality for acute mesenteric ischemia patients. Abdom. Radiol. 2022, 47, 1644–1653. [Google Scholar] [CrossRef]
- Batista, A.F.R.; Petty, D.; Fairhurst, C.; Davies, S. Psoas muscle mass index as a predictor of long-term mortality and severity of complications after major intra-abdominal colorectal surgery - A retrospective analysis. J. Clin. Anesth. 2023, 84, 110995. [Google Scholar] [CrossRef]
- Balsam, L.B. Psoas muscle area: a new standard for frailty assessment in cardiac surgery? J. Thorac. Dis. 2018, 10 (Suppl. 33), S3846–S3849. [Google Scholar] [CrossRef]
- Paknikar, R.; Friedman, J.; Cron, D.; Deeb, G.M.; Chetcuti, S.; Grossman, P.M.; Wang, S.; Englesbe, M.; Patel, H.J. Psoas muscle size as a frailty measure for open and transcatheter aortic valve replacement. J. Thorac. Cardiovasc. Surg. 2016, 151, 745–751. [Google Scholar] [CrossRef]
- Zuckerman, J.; Ades, M.; Mullie, L.; Trnkus, A.; Morin, J.F.; Langlois, Y.; Ma, F.; Levental, M.; Morais, J.A.; Afilalo, J. Psoas Muscle Area and Length of Stay in Older Adults Undergoing Cardiac Operations. Ann. Thorac. Surg. 2017, 103, 1498–1504. [Google Scholar] [CrossRef]
- Hawkins, R.B.; Mehaffey, J.H.; Charles, E.J.; Kern, J.A.; Lim, D.S.; Teman, N.R.; Ailawadi, G. Psoas Muscle Size Predicts Risk-Adjusted Outcomes After Surgical Aortic Valve Replacement. Ann. Thorac. Surg. 2018, 106, 39–45. [Google Scholar] [CrossRef]
Figure 1.
Measurement of each body composition parameter, total muscle area (TMA) and visceral adipose tissue (VAT). Legend: PMA means psoas muscle area; VAT means visceral adipose tissue; SAT means Subcutaneous adipose tissue.
Figure 1.
Measurement of each body composition parameter, total muscle area (TMA) and visceral adipose tissue (VAT). Legend: PMA means psoas muscle area; VAT means visceral adipose tissue; SAT means Subcutaneous adipose tissue.
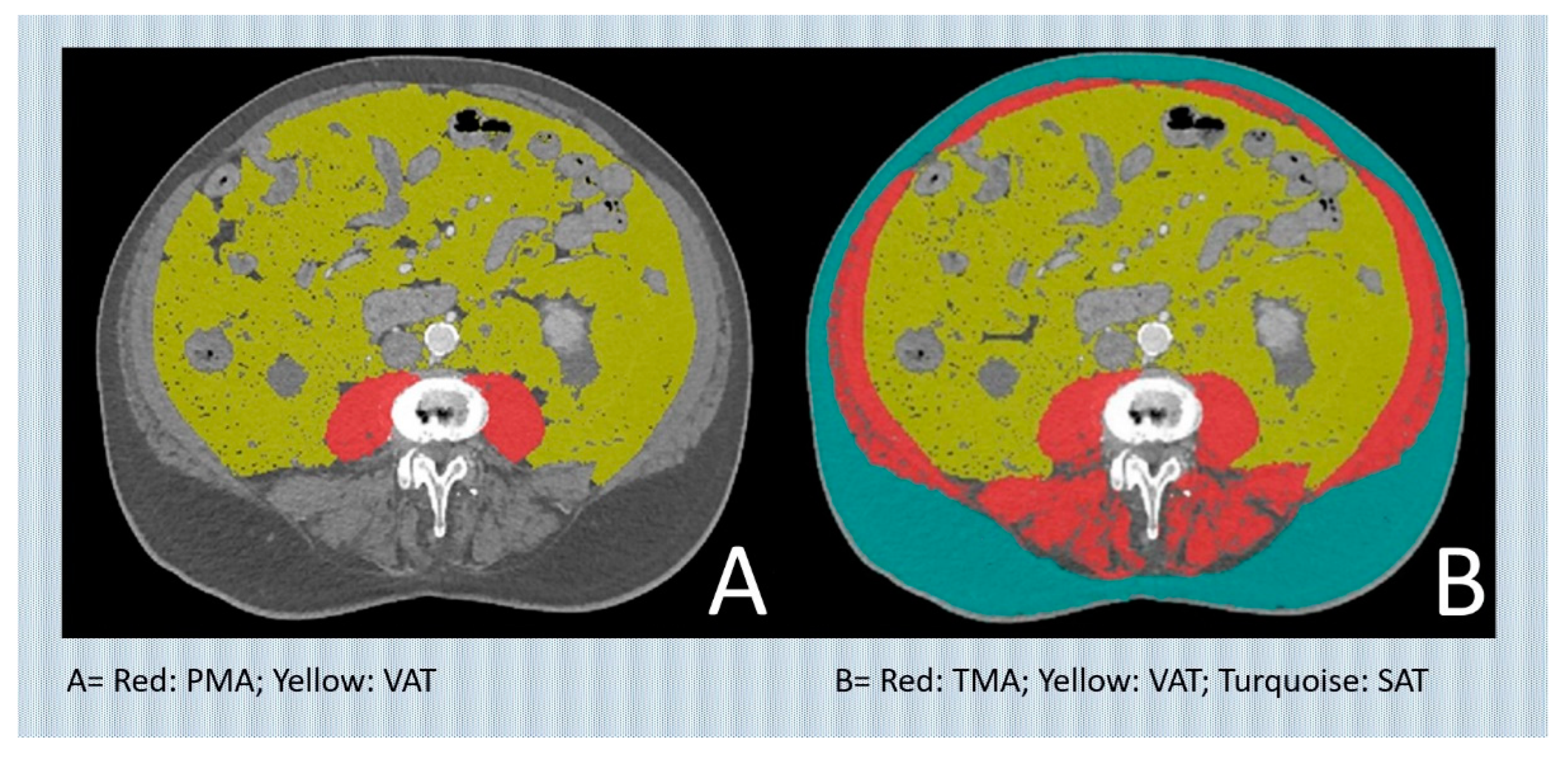
Figure 2.
(A) Marginal distributions of total muscle area (TMA) and visceral adipose tissue (VAT) in surviving and deceased patients for the entire cohort and stratified according to gender. (B) Predicted 5-yr mortality risk when considering TMA and VAT jointly.
Figure 2.
(A) Marginal distributions of total muscle area (TMA) and visceral adipose tissue (VAT) in surviving and deceased patients for the entire cohort and stratified according to gender. (B) Predicted 5-yr mortality risk when considering TMA and VAT jointly.
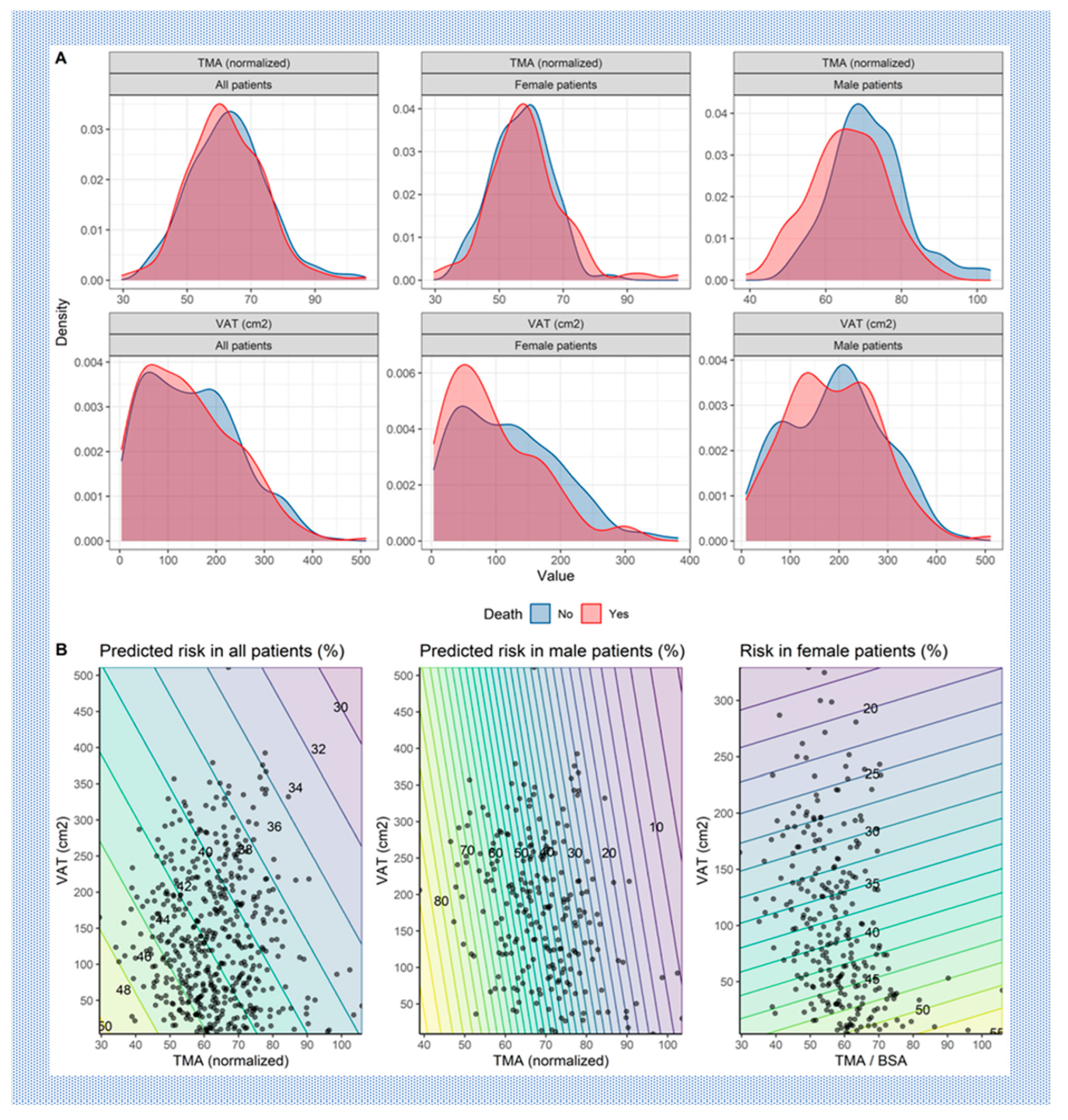

Table 1.
Baseline Characteristics.
| All patients N=584 | |
|---|---|
| Gender: | |
| Male | 280 (47.9%) |
| Female | 304 (52.1%) |
| Age (years) | 82.8 [79.0;86.5] |
| Height (cm) | 165 [158;172] |
| Weight (kg) | 71.0 [62.0;83.0] |
| Body mass index (kg/m2) | 25.6 [22.7;29.7] |
| Diabetes mellitus [Yes] | 156 (26.7%) |
| Arterial hypertension [Yes] | 506 (86.6%) |
| Dyslipidemia [Yes] | 391 (67.0%) |
| Chronic obstructive pulmonary disease [Yes] | 61 (10.4%) |
| History of cerebrovascular accident [Yes] | 71 (12.2%) |
| Transient ischemic attack [Yes] | 31 (5.31%) |
| Coronary artery disease [Yes] | 346 (59.2%) |
| History of myocardial infarction [Yes] | 87 (14.9%) |
| Atrial fibrillation [Yes] | 203 (34.8%) |
| Peripheral artery disease [Yes] | 69 (11.8%) |
| History of cardiac surgery [Yes] | 59 (10.1%) |
| Dyspnea [Yes] | 578 (99.1%) |
| Body surface area (m2, Haycock) | 1.81 [1.67;1.99] |
| Visceral adipose tissue (cm2) | 134 [68.5;216] |
| Total muscle area (cm2) | 110 [93.4;131] |
| Total muscle Area normalized by body surface area (-) | 62.3 [54.5;70.1] |
| Subcutaneous adipose tissue (cm2) | 148 [106;207] |
| Creatinine (µmol/l) | 95.5 [77.0;120] |
| Brain natriuretic peptide (pg/ml) | 257 [108;625] |
| Albumin (g/L) | 34.0 [32.0;36.0] |
| Mean Gradient (mmHg) | 39.0 [28.0;47.0] |
| Peak Gradient (mmHg) | 63.0 [45.0;78.0] |
| Aortic Valve Area (cm2) | 0.70 [0.60;0.90] |
| Indexed Aortic Valve Area (cm2) | 0.27 [0.21;0.32] |
| Left ventricular ejection fractionLVEF (%) | 60.0 [50.0;65.0] |
| Logistic Euro Score | 9.18 [5.83;17.7] |
| Linear Euro Score | 8.00 [6.00;10.0] |
| Euro Score II | 3.67 [2.24;6.66] |
| STS predicted risk of mortality | 4.12 [2.90;6.31] |
Table 2.
Regression coefficient and associated 95%-confidence intervals and p-values for a multivariable logistic regression model and multivariable survival cox regression model.
Table 2.
Regression coefficient and associated 95%-confidence intervals and p-values for a multivariable logistic regression model and multivariable survival cox regression model.
| Cox regression | |||
|---|---|---|---|
| Characteristic | HR | 95% CI | p |
| Age (years) | 1.023 | 0.998, 1.049 | 0.069 |
| BMI (kg/m2) | 1.005 | 0.97, 1.046 | 0.8 |
| Sex: | |||
| Female | 0.036 | 0.003, 0.396 | 0.007 |
| TMA (normalized) | 0.96 | 0.927, 0.997 | 0.033 |
| VAT (cm2) | 1.002 | 0.99, 1.015 | 0.7 |
| Sex * TMA (normalized) | |||
| Female * TMA (normalized) | 1.048 | 1.013, 1.084 | 0.007 |
| Sex * VAT | |||
| Female * VAT (cm2) | 0.997 | 0.99, 1.001 | 0.2 |
| TMA (normalized) * VAT (cm2) | 0.9999 | 0.9998, 1.00011 | 0.5 |
Table 3.
Gender-specific regression coefficient and associated 95%-confidence intervals and p-values for multivariable survival cox regression model.
Table 3.
Gender-specific regression coefficient and associated 95%-confidence intervals and p-values for multivariable survival cox regression model.
| Female patients | Male patients | |||||
|---|---|---|---|---|---|---|
| Characteristic | HR1 | 95% CI1 | p | HR1 | 95% CI1 | p |
| Age (years) | 1.029 | 0.99, 1.070 | 0.14 | 1.018 | 0.99, 1.052 | 0.3 |
| BMI (kg/m2) | 1.003 | 0.948, 1.061 | >0.9 | 1.006 | 0.95, 1.065 | 0.8 |
| TMA (normalized) | 1.009 | 0.98, 1.038 | 0.6 | 0.96 | 0.917, 0.999 | 0.044 |
| VAT (cm2) | 1.001 | 0.98, 1.019 | >0.9 | 1.001 | 0.99, 1.017 | 0.9 |
| TMA (normalized) * VAT (cm2) | 0.9999 | 0.9996, 1.00022 | 0.6 | 0.99995 | 0.9997, 1.00017 | 0.7 |
| 1HR = Hazard Ratio, CI = Confidence Interval | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



