Submitted:
09 January 2024
Posted:
10 January 2024
You are already at the latest version
Abstract
The goal was to assess dental students' perception of digital technologies after participating in a CAD/CAM exercise for scanning, designing, and manufacturing computer-aided provisional fixed dental restorations. A survey was conducted among second-year dental students (pre-D2 and post-D2), first- (D1, negative control), third-, and fourth-year dental students (D3 and D4, positive controls). Only OSU College of Dentistry students who completed the activity and completed the surveys were included. Seven questions were rated, which evaluated changes in knowledge, skill, interest, the importance of technology availability in an office, patients' perception of technology, the importance of having the technology, and the expected frequency of clinics utilizing the technology. Statistical analysis was performed with a significance level of 0.05. A total of 74 pre-D2 and 77 post-D2 questionnaires were completed. Additionally, 63 D1, 43 D3, and 39 D4 responded to the survey. Significant differences were found for "knowledge" and "skill" between pre-D2 and post-D2, and pre-D2 and control groups (p<0.001). There was a significant difference between post-D2 and all controls for “interest” (p=0.0127) and on practice preference for technology availability (p<0.05). There were significant results between post-D2 and all controls regarding the importance of technology availability in an office (p<0.001) and the expected frequency of clinics utilizing the technology (p=0.01). No significance was found for "patient's value of technology" and "the importance of having the technology". The presence of technology in the practice and educational academic environments significantly improved students’ interest and perception of knowledge and skill.
Keywords:
Digital Dentistry
; CAD/CAM
; Technology
; Dental studentds
; Practice management
1. Introduction
The emergence of digital dentistry and dental Computer-Aided Design/Computer-Aided Manufacturing (CAD/CAM) technologies have prompted dental schools to revise their curriculum and integrate dental technologies into the education of dental students.1,2 CAD/CAM composite restorative materials are now accessible for subtractive fabrication procedures, utilizing milling machines and uniformly manufactured blocks. These blocks exhibit enhanced properties compared to direct composite materials, consisting of a resin polymer matrix and ceramic-based filler particles.5 The composition, proportions, properties, and distribution of compartments vary greatly among different CAD/CAM materials, resulting in diverse material characteristics.3,6-9
Digital impression acquisition (scanning) and CAD/CAM technology, including machine milling and three-dimensional (3D) printing, have significantly advanced modern restorative and prosthetic procedures. These technological advancements have gained widespread acceptance and are extensively utilized in private dental offices, resulting in positive feedback and transforming clinicians’ perceptions and practice models.3,10-12 However, limited clinical studies that specifically investigate composite-based CAD/CAM materials are available. Most existing studies are in vitro and primarily focus on mechanical tests, such as fatigue and fracture behavior, predominantly pertaining to veneer restorations.13-18
Incorporating digital technologies into dental education is necessary to keep pace with advancements in materials and technology. However, there is limited literature on how students perceive this integration and how it affects their professional aspirations in private practice. This study assessed dental students’ perceptions of digital technologies by exposing them to a pre-clinical simulation exercise of scanning, designing, and manufacturing a computer-aided provisional fixed dental restoration. It was proposed here that comprehensive digital dentistry teaching and exposure will influence students to incorporate dental technologies in their future clinical practice. The null hypothesis is that there will be no difference in student perception after exposure to this learning experience.
2. Materials and Methods
This study was submitted and approved by the University’s Ethical Committee (#20220799).
2.1. Sample selection and grouping
Second-year students typically receive pre-clinical education in Fixed Prosthodontics and Operative Dentistry as part of the dental curriculum at the College of Dentistry. Previously, these students were introduced to digital impression acquisition (intraoral scanning) on typodonts and were exposed to computer-aided design (CAD) without computer-aided manufacturing (CAM) during this pre-clinical training. However, as part of the curriculum re-engineering process, a comprehensive CAD/CAM exercise was developed and implemented in the fourth course of the operative curriculum during the fall semester of the second year. A survey was conducted among the intervention group per Suppl to evaluate any changes in perception regarding digital dentistry. Table 1 shows the inclusion criteria, which consisted of second-year dental students, both before and after completing the comprehensive CAD/CAM exercise. The same survey was also administered to the first-year dental students (who had not yet been exposed to digital dentistry) and the third and fourth-year dental students (who had limited exposure to intraoral scanning and CAD exercises during their pre-clinical training) as control groups. All students from the first, second, third, and fourth years were recruited, and participants who did not complete all the required surveys for each respective group were excluded from the analysis.
2.2. Eligibility criteria
All included students agreed to participate before starting the survey. For inclusion, it was considered only students from the OSU College of Dentistry (Ohio, U.S.A.) who accepted to be part of the study, completed the activity, and filled out the surveys (initial and after the activity); students from the first year, who did not learn about Digital Dentistry, to fill the survey out as negative control; and as a positive control, students of the third and fourth years. It excluded participants who did not complete the activity proposed at the correct time or did not fill out the survey.
2.3. Activity proposed
The exercise conducted in the pre-clinical simulation laboratory involved a clinical scenario on a typodont, specifically preparing an ivorine molar tooth #46 (Nissin Dental Products - Kilgore, Japan) for a CAD/CAM onlay restoration. The process began by acquiring a digital impression of the tooth preparation using the 3Shape TRIOS® intraoral scanner (3Shape, Denmark). Subsequently, the students proceeded with the CAD step, designing their own onlay with the assistance of a tutorial video created by the course faculty. Faculty members within the laboratory provided support during the CAD process using the 3Shape TRIOS® software (3Shape, Denmark). The designed onlay was then exported in the Standard Tessellation Language (STL) format, allowing its import into the AnyCubic Workshop (Anycubic, China) software for 3D printing. In the 3D printing software, students were able to rotate the model, add support beams, and include an identifying key tag with their name before slicing the model for printing.
The dental students used the Photon M2 3D printers (Anycubic, China) to successfully perform a CAM exercise by printing unique dental restorations that fit their prepared teeth. The simulation concluded with students seating and adjusting the 3D-printed provisional prosthesis, which was cemented using a provisional cement (TempBond NE [non-eugenol], KaVo Kerr, USA). It’s important to note that the hands-on exercise was supplemented with a series of CAD/CAM lectures to provide students with theoretical knowledge alongside practical application. During the 3D printing exercise, an additional lecture was conducted in collaboration with the College of Engineering, offering a multidisciplinary teaching approach. A practice management lecture was also delivered to educate students about clinical considerations when implementing digital dentistry in practice. Following these lectures, an active learning exercise was conducted, where students formed groups to discuss fictional office scenarios and make decisions regarding the acquisition of CAD/CAM technology based on each practice’s profile.
2.4. Survey (Questionnaire)
Considering the extent of this exercise and the importance of the exposure to CAD/CAM Dentistry in a predoctoral academic environment, the principal investigator raised questions about how this exercise would impact students’ perception of digital dentistry value and their aspiration for their professional careers. The survey was anonymous, and the gathered results were organized into a spreadsheet for statistical analysis (Excel, Microsoft Office, CA, U.S.A.).
Seven questions were developed, ranging between the scores 1 (lowest) and 10 (highest) or 1 (I strongly disagree) and 10 (I strongly agree), aiming to assess the following areas of interest: (i) change in knowledge, (ii) skill, (iii) interest, (iv) importance given to technology availability in an office, (v) patient’s value of technology, (vi) importance of having the technology, and (vii) the expected relative frequency of clinics having the technology (Table 2).
2.5. Studies limitation
To ensure the anonymity of respondents, no identification was recorded from any of the applied questionnaires. Consequently, we could not pair repeated measures from second-year participants before and after the intervention, needing to assume independence instead.
2.6. Statistical analysis
The Kolmogorov-Smirnov test evaluated the normality of the data. Sequentially, the Kruskal-Wallis test was used to assess if control D1, control D3, control D4, and post-D2 were similar. Since D2 may not be comparable with control D1, D3, and D4 for skill and knowledge, those two categories are not tested. However, Pre-D2 will be analyzed separately since it is not independent of post-D2. Moreover, the Kruskal-Wallis test was applied to compare the difference between post-D2, control D1, control D3, and control D4. To compare second-year dental students before the exercise (pre-D2) to all controls combined (negative control [D1] and positive controls [D3 and D4]), Wilcoxon’s test with Bonferroni correction for multiple comparisons was used. Statistical analysis was conducted using the software R (R v3.6.1; R Core Team 2021), and a significant level of 0.05 was assumed.
3. Results
3.1. Sample
118 enrolled second-year dental students printed 118 unique dental restorations fitting to their prepared typodont teeth. Therefore, of the 118 students surveyed, 74 responded (62.71%) to the pre-intervention (pre-D2) and 77 (65.25%) to the post-intervention (post-D2) questionnaire. 120 first-year dental students (D1) were surveyed as negative controls, and 63 responded and participated in this survey (52.5%). Another 240 students were invited (3rd and 4th years) as the positive control (120 students from each year), and 43 (D3) responded (35.83%), and 39 (D4) responded (32.5%). The class composition is shown in Table 3.
3.2. Knowledge and skill
Analyzing the “knowledge” and “skill” (Figure 1), it was noted there was a significant difference between pre-D2 and all controls (p<0.001 for both). This means that pre-D2 is not comparable with the other controls except knowledge and skill. Thus, it does not seem appropriate to compare D2 posts with the other controls for knowledge and skill questions since the difference could not be linked to the intervention.
Multiple comparisons were made to compare the measures between pre-D2 and post-D2 (same students). It was observed there was a significant difference between pre-D2 and post-D2 for “knowledge” (p<0.001) and “skill” (p<0.001) (Figure 2 and Suppl. Figure 1). In addition, multiple comparisons were made for post-D2 and all control groups (controlD1, controlD3, and controlD4). There was a significant difference between post-D2 and all controls for “knowledge” (p<0.001) and “skill” (p<0.001). A correction for multiple comparisons was also used to compare post-D2 with control-D3 and control-D4 combined. A significant difference between post-D2 with control-D3 and control-D4 combined was found for “knowledge” (p<0.001) and “skill” (p<0.0001).
3.3. Interest
The evaluated interest question had a statistically significant result (p<0.05), demonstrating that pre-D2 students were comparable with all controls for their interest in digital dentistry. Also, there was a significant difference between post-D2, control D1, control D3, and control D4 for the subject “interest” (p=0.02). For outcome “interest”, there was a significant difference between postD2/controlD1 (p=0.0362). Multiple comparisons were made to compare the measures between pre-D2 and post-D2 (same students). It was observed there was a significant difference between pre-D2 and post-D2 for “interest” (p=0.0102) (Figure 2 and Suppl. Figure 1). In addition, multiple comparisons were made for post-D2 and all control groups (controlD1, controlD3, and controlD4). There was a significant difference between post-D2 and all controls for “interest” (p=0.0127).
Multiple comparisons were made to compare post-D2 with control-D3 and control-D4 combined. A significant difference between post-D2 with control-D3 and control-D4 combined was found for “interest” (p=0.0065). No significant difference was noted between control-D1 with control-D3 and control-D4 combined for all questions (Figure 3).
3.4. Practice aspiration
The practice aspiration question evaluated had significant results (p<0.05), demonstrating that pre-D2 students were comparable with all controls for the availability of dental technology on their practice preference. Also, there was a significant difference between post-D2, control D1, control D3, and control D4 for the subject “importance given to technology availability in an office” (p<0.001) and “the relative frequency of clinics having the technology” (p=0.01).
For the outcome “importance given to technology availability in an office”, there was a significant difference between postD2/controlD1 (p=0.00284) and postD2/controlD4 (p=0.0399). No significant difference was between any groups for “the importance of having the technology” (p<0.05). Otherwise, “the relative frequency of clinics having the technology” had a significant difference between postD2/controlD4 (p=0.01213) (Table 4).
Multiple comparisons were made to compare the measures between pre-D2 and post-D2 (same students). It was observed there was a significant difference between pre-D2 and post-D2 for “importance given to technology availability in an office” (p=0.0024) (Figure 2 and Suppl. Figure 1). In addition, multiple comparisons were made for post-D2 and all control groups (controlD1, controlD3, and controlD4). There was a significant difference between post-D2 and all controls for “importance given to technology availability in an office” (p<0.002).
Multiple comparisons were also used to compare post-D2 with control-D3 and control-D4 combined. A significant difference between post-D2 with control-D3 and control-D4 combined was found for “importance given to technology availability in an office” (p =0.0043) and “the relative frequency of clinics having the technology” (p=0.0203). No significant difference was noted between control-D1 with control-D3 and control-D4 combined for all questions (Figure 3).
3.5. Value of technology
All value parameters evaluated had statistically significant results (p<0.05), demonstrating that pre-D2 students were comparable with all controls for those. There was no significant difference between any groups for “patient’s value of technology” and “the importance of having the technology” (p<0.05). Multiple comparisons were made to compare the measures between pre-D2 and post-D2 (same students). It was observed there was no significant difference between pre-D2 and post-D2 for “patient’s value of technology” and “the importance of having the technology” (Figure 2 and Suppl. Figure 1). In addition, multiple comparisons were made for post-D2 and all control groups (controlD1, controlD3, and controlD4). There was no significant difference between post-D2 and all controls for “patient’s value of technology” and “the importance of having the technology”.
Multiple comparisons were also used to compare post-D2 with control-D3 and control-D4 combined. The result for “patient’s value of technology” and “the importance of having the technology” was not significant, as well as between control-D1 with control-D3 and control-D4 combined for all questions noted (Figure 3).
4. Discussion
The aim of this study was to assess dental students’ perception of digital technologies. The research strategy was to understand if students’ exposition in the pre-clinical simulation environment with the simulated exercise, scanning, designing, and manufacturing a computer-aided provisional fixed dental restoration, would produce more impact on the dental student’s future aspiration to incorporating dental technologies in their clinical practice (positive hypothesis). The results highlighted significant changes in students’ knowledge, skill, interest, and technology (importance given to technology availability in an office, patient’s value, importance of technology, and the relative frequency of clinics having the technology).
The clinical curriculum has undergone modifications appropriate for novice dentists (or the clinic curriculum has undergone appropriate modifications for novice dentists). It is based on new technologies and high-quality evidence of efficacy. CAD/CAM is one of the most impacting technological advances in Dentistry, and its implementation in clinical activities has occurred slowly, mainly when the subject is the insertion into the dental curriculum.19 Since the 2010s, studies have been developed to report this introduction in academic behavior. Dehghan et al. (2012)20 considered the introduction of CEREC (an acronym for “ceramic reconstruction"), which is a CAD/CAM system, at the University of Tennessee College of Dentistry, which was the first university in the US to embrace this technology and integrate it into the four-year curriculum. The authors concluded this technology was an educational tool for dental students, providing a cost-effective improvement and exceptional patient service. Browning et al.21 evaluated undergraduate dental students over one year who provided 125 all-ceramic crowns to patients; they designed, milled, sintered, and stained the CAD/CAM restorations and concluded a significant reduction in lab costs. Also, the authors reported the faculty’s appreciation of the marginal fit and esthetic obtained. The same group published an article in the following year22 on the same subject to present the incorporation of CAD/CAM system into the predoctoral curriculum at the Indiana University School of Dentistry. These articles aimed to present data regarding students’ opinions after one year of the implementation. 88 out of 105 D1 students (84% response rate) participated and completed the form. The overall learning was considered good or excellent by 80% of the students, and 43% judged themselves prepared to fabricate a crown independently.
In comparison, the authors of the present study expanded the questionnaire intervention to all students, focusing on the intervention group of second-year students. 118 second-year dental students scanned, designed, and 3D-printed 118 unique dental restorations. The entire group was surveyed, but 74 responded (62.71%) in the pre-intervention (pre-D2) and 77 (65.25%) in the post-intervention (post-D2) questionnaire. Positive results were found between pre-D2 and post-D2/all control groups (D1, D3, and D4) for “knowledge” (p<0.001) and “skill” (p < 0.001). Significant differences were also found among post-D2, controls D1, D3, and D4 for “technology availability in an office” (p<0.001) and “relative frequency of clinics having the technology” (p=0.01).
Another study,2 published in 2017, presented the implementation of a CAD/CAM system in the University of Illinois at Chicago College of Dentistry’s predoctoral implant program. The preliminary data showed an increased proportion of implant restorations made digitally compared to the traditional way. In 2018, Schweyen et al.23 evaluated technology implementation in the prosthetic education curriculum at a German dental school. 94% of all students participated in the CAD/CAM curriculum, indicating considerable interest, a number superior to the findings in our study. The restorations fabricated by the students had a good clinical performance. The authors concluded that there is a tendency for the use of CAD/CAM systems by the students who prepared digitally more teeth than other students without knowledge of CAD/CAM technology.
In the current study, changes were perceptible in the intervention group (2nd-year dental students) relative to the negative control (first year) and the positive control (third and fourth year). Similar to a previous study1, implementing digital technology was linked to positive student perceptions and attitudes toward future clinical applications. The same study1 showed that over 90% of students were comfortable and willing to use intraoral scanners in their practice. This intervention improved second-year students’ skills and knowledge in digital dentistry. The skills and knowledge of the control groups are lower than those of the intervention group. In the negative control (1st-year students), this may be explained by the fact that those students have not been exposed to or taught digital dentistry yet. For positive controls in the third and fourth years, this may be due to the limited nature of their digital dentistry exposure one or two years ago. Appropriate and timely digital integration into predoctoral education is essential in optimizing the learning environment.2 The negative control (1st-year students) and intervention group (second years) displayed a higher valuation of digital technology in the clinical setting compared to positive controls (third and fourth year), which may be explained by the lack of digital dentistry in the clinical setting at the time of the survey. This may reflect clinical practice teaching.
The second-year students indicated an increased interest in joining a clinic utilizing dental technology following the intervention exercise. This suggests a change in professional career practice aspiration thanks to this comprehensive exercise. Similar responses were noted in the first-year students, and to a lesser extent, for the third- and fourth-year students. The reduced interest of the positive control group may once again reflect the scarcity of digital technology in the student clinic. All groups expressed high interest in digital dentistry. In the intervention group, this interest was increased. These results are similar to dental students’ positive and enthusiastic attitude towards digital dentistry technology.24
Towers et al.25 similarly studied students’ perception of virtual reality (VR) and 3D-printing combination for operative teaching. Their results complemented this study, highlighting students’ value of technology and innovative teaching methods that are translatable to clinical settings. The study also highlighted the importance of educator support, which was not assessed in this survey. The impact of the teaching on the clinical procedure and the patient are notable in this study, mainly to provide a valuable contribution to increasing students’ confidence and preparedness.
Finally, one study published in 2023 26 aimed to evaluate the predoctoral dental students’ CAD/CAM-related education, knowledge, attitudes, and professional behavior; moreover, the relationships between the year in dental school and variables were contrasted. 358 dental students from 17 of the 68 US dental schools (25%) participated in a web-based anonymous survey. Similar to the present study, questions asking about the subject and percentual obtained were: simulated exercises (86.9%), video demonstrations (81.8%), demonstrations during a lecture (76.4%) or for smaller groups of students (69.2%), hands-on (65.6%), and individual instruction (50.4%). There was a significant improvement in the knowledge and attitude to using CAD/CAM technology (p<0.001 and p<0.05, respectively); otherwise, student satisfaction was non-significant. The authors concluded that most students in the US dental schools considered CAD/CAM the future of dentistry and made them better dentists.
There were limitations to be considered. Limited and concentrated students’ opinions were obtained, which might not translate into students’ skills. Moreover, students’ perceptions of concepts, such as skills and knowledge, can inflate responses to questions. Only one institution was involved, although similar experiences were conducted in other institutions during analog-to-digital transfer. The focus could be amplified to all years, not only 2nd year, to observe the maintenance of the learning and knowledge reached in the superior years (3rd and 4th).
5. Conclusions
Within the limitations of this study, it was possible to conclude that: (i) around 60% of the 2nd year students (experimental group) responded to the questionnaire, with statistically significant results for the subject “interest”; (ii) significative improvement was observed for “knowledge” and “skill” when compared pre-D2 and post-D2/all control groups (controlD1, controlD3, and controlD4); (iii) significative impact was found for the presence of technology in the practice and educational academic environment. Further research (prospective cohort study) is suggested to follow up a greater number of students in the long term, indicating a multicentric design.
Supplementary Materials
Suppl. Figure 1. Box plot for the areas of interest studied, comparing pre-D2 and post-D2.
Author Contributions
Conceptualization, LMN, SB; methodology, LMN, SB, FS; software, LMN, FS, RR, GVOF; validation, LMN, SB, FS, W-EL, RR, GVOF; formal analysis, LMN, SB, FS, W-EL, RR, GVOF; investigation, LMN, SB, FS, W-EL, RR, GVOF; resources, X.X.; data curation, LMN, SB, FS, W-EL; writing—original draft preparation, LMN, SB, FS, W-EL, RR, GVOF; writing—review and editing, LMN, SB, FS, W-EL, RR, GVOF; visualization, LMN, SB, FS, W-EL, RR, GVOF; supervision, LMN, GVOF; project administration, LMN. All authors have read and agreed to the published version of the manuscript.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of the Ohio State University’s Ethical Committee (#20220799) on 9/6/2022.
Informed Consent Statement
“Informed consent was obtained from all subjects involved in the study.”
Data Availability Statement
All data were inserted in the article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Schlenz M.A., Michel K, Wegner K, Schmidt A, Rehmann P, Wöstmann B. Undergraduate dental students’ perspective on the implementation of digital dentistry in the preclinical curriculum: a questionnaire survey. BMC Oral Health 2020;20:1-10. [CrossRef]
- Afshari FS, Sukotjo C, Alfaro MF, McCombs J, Campbell SD, Knoernschild KL, Yuan JC-C. Integration of digital dentistry into a predoctoral implant program: program description, rationale, and utilization trends. J Dent Educ 2017;81:986-994. [CrossRef]
- Blatz MB, Conejo J. The current state of chairside digital dentistry and materials. Dent Clin 2019;63:175-197. [CrossRef]
- Alharbi A, Ardu S, Bortolotto T, Krejci I. Stain susceptibility of composite and ceramic CAD/CAM blocks versus direct resin composites with different resinous matrices. Odontology 2017;105:162-169. [CrossRef]
- Kamonwanon P, Hirose N, Yamaguchi S, Sasaki JI, Kitagawa H, Kitagawa R, Thaweboon S, Srikhirin T, Imazato S. SiO2-nanocomposite film coating of CAD/CAM composite resin blocks improves surface hardness and reduces susceptibility to bacterial adhesion. Dent Mater J 2017;36:88-94. [CrossRef]
- Sulaiman, Taiseer A. "Materials in digital dentistry - A review." J Esthet Rest Dent 2020;32,171-181. [CrossRef]
- Zimmermann M, Mehl A, Reich S. New CAD/CAM materials and blocks for chairside procedures. Int J Comput Dent 2013;16:173-181.
- Goujat A, Abouelleil H, Colon P, Jeannin C, Pradelle N, Seux D, Grosgogeat B. Mechanical properties and internal fit of 4 CAD-CAM block materials. J Prosthet Dent 2018;119:384-389. [CrossRef]
- Ruse ND, Sadoun MJ. Resin-composite blocks for dental CAD/CAM applications. J Dent Res 2014;93:1232-1234. [CrossRef]
- Nassani MZ, Ibraheem S, Shamsy E, Darwish M, Faden A, Kujan O. A survey of dentists’ perception of chair-side CAD/CAM technology. Healthcare (Basel, Switzerland) 2021;9:68. [CrossRef]
- Matthews DC, McNeil K, Brillant M, Tax C, Maillet P, McCulloch CA, Glogauer M. Factors influencing adoption of new technologies into dental practice: A qualitative study: A qualitative study. JDR Clin Translat Res 2016;1:77-85. [CrossRef]
- Fung L, Brisebois P. Implementing digital dentistry into your esthetic dental practice. Dent Clin North Am 2020;64:645-657. [CrossRef]
- Zimmerman M, Koller C, Reymus M, Mehl A, Hickel R. Clinical evaluation of indirect particle-filled composite resin CAD/CAM partial crowns after 24 months. J Prosthodont 2017;27:694-699. [CrossRef]
- Shembish FA, Tong H, Kaizer M, Janal MN, Thompson VP, Opdam NJ, Zhang Y. Fatigue resistance of CAD/CAM resin composite molar crowns. Dent Mater 2016;32:499-509. [CrossRef]
- Schlichting LH, Maia HP, Baratien LN, Magne P. Novel design ultra-thin CAD/CAM composite resin and ceramic occlusal veneers for the treatment of severe dental erosion. J Prosthet Dent 2011;105:217-226. [CrossRef]
- Magne P, Schlichting CH, Maia HP, Barattieri LN. In vitro fatigue resistance of CAD/CAM composite resin and ceramic posterior occlusal veneers. J Prosthet Dent 2010;104:149-157. [CrossRef]
- Magne P, Stanley K, Schlichting LH. Modeling of ultrathin occlusal veneers. Dent Mater 2012;28:777-782. [CrossRef]
- El-Damanhoury HM, Haj-Ali RN, Plat JA. Fracture resistance and microleakage of endocrowns utilizing three CAD-CAM blocks. Oper Dent 2015;40:201-210. [CrossRef]
- Fernandes GVO, Nassani LM. The Implementation of CAD/CAM Technology at Schools of Dentistry: A Short Communication. Env Dental J 2023;5:1-3. [CrossRef]
- Dehghan M, Simon JF, Harrison J. Integrating the CEREC technology at UT College of Dentistry. J Tenn Dent Assoc 2012;92:19-21; quiz 21-22.
- Browning WD, Reifeis P, Willis L, Kirkup ML. Including CAD/CAM dentistry in a dental school curriculum. J Indiana Dent Assoc 2013;92:40-45,47.
- Reifeis PE, Kirkup ML, Willis LH, Browning WD. Introducing CAD/CAM into a predoctoral dental curriculum: a case study. Dent Educ 2014;78:1432-1441. [CrossRef]
- Schweyen R, Beuer F, Bochskanl M, Hey J: Implementing a new curriculum for computer-assisted restorations in prosthetic dentistry. Eur J Dent Educ 2018;22:e237-e247. [CrossRef]
- Sharab L, Adel M, Abualsoud R, Hall B, Albaree S, de Leeuw R, Kutkut A. Perception, awareness, and attitude toward digital dentistry among pre-dental students: an observational survey. Bullet Nat Res Centre 2022;46:1-7. [CrossRef]
- Towers A, Dixon J, Field J, Martin R, Martin N. Combining virtual reality and 3D-printed models to simulate patient-specific dental operative procedures - A study exploring student perceptions. Eur J Dent Educ 2022;26:393-403. [CrossRef]
- Alhamed FJ, Neiva GF, Bak S-Y, Karl E, Inglehart MR. Pre-doctoral dental students’ computer-aided design/computer-aided manufacturing-related education, knowledge, attitudes and behavior: A national survey. J Dent Educ 2023;87:562-571. [CrossRef]
Figure 1.
The empirical density of the self-reported knowledge (left) and skill (right) among all students enrolled.
Figure 1.
The empirical density of the self-reported knowledge (left) and skill (right) among all students enrolled.
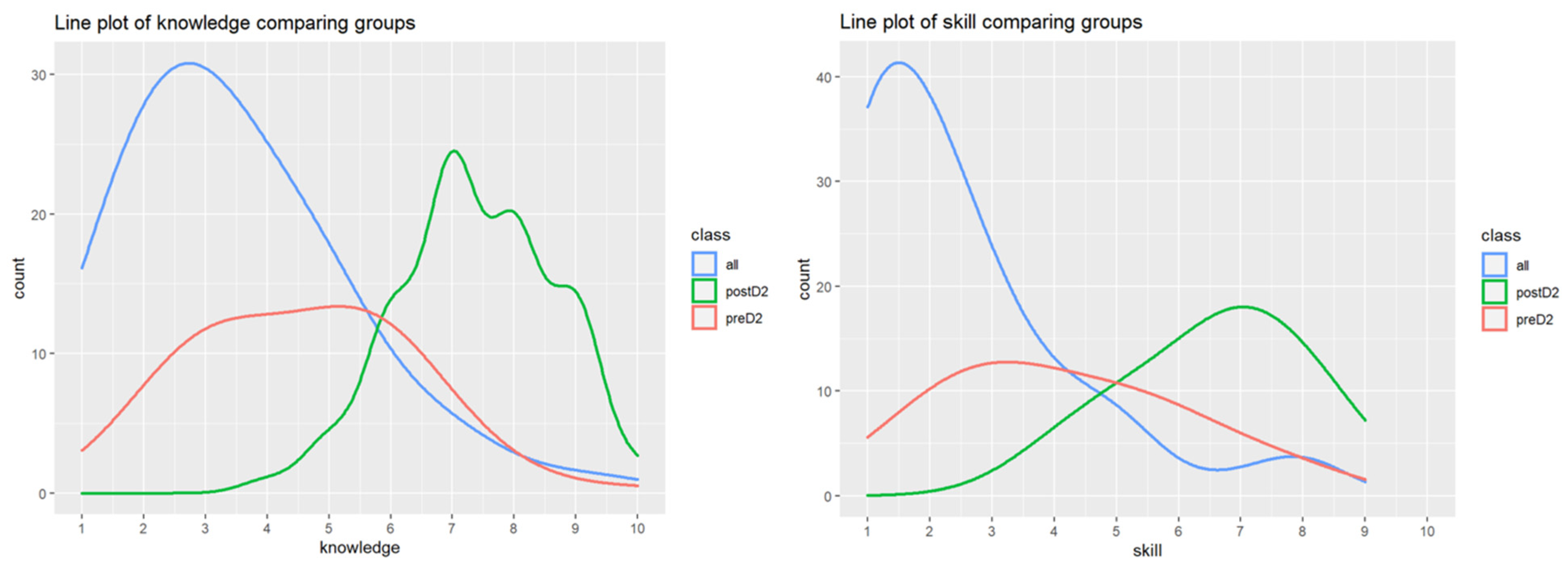
Figure 2.
The mean difference for the areas of interest studied, comparing pre-D2 and post-D2.
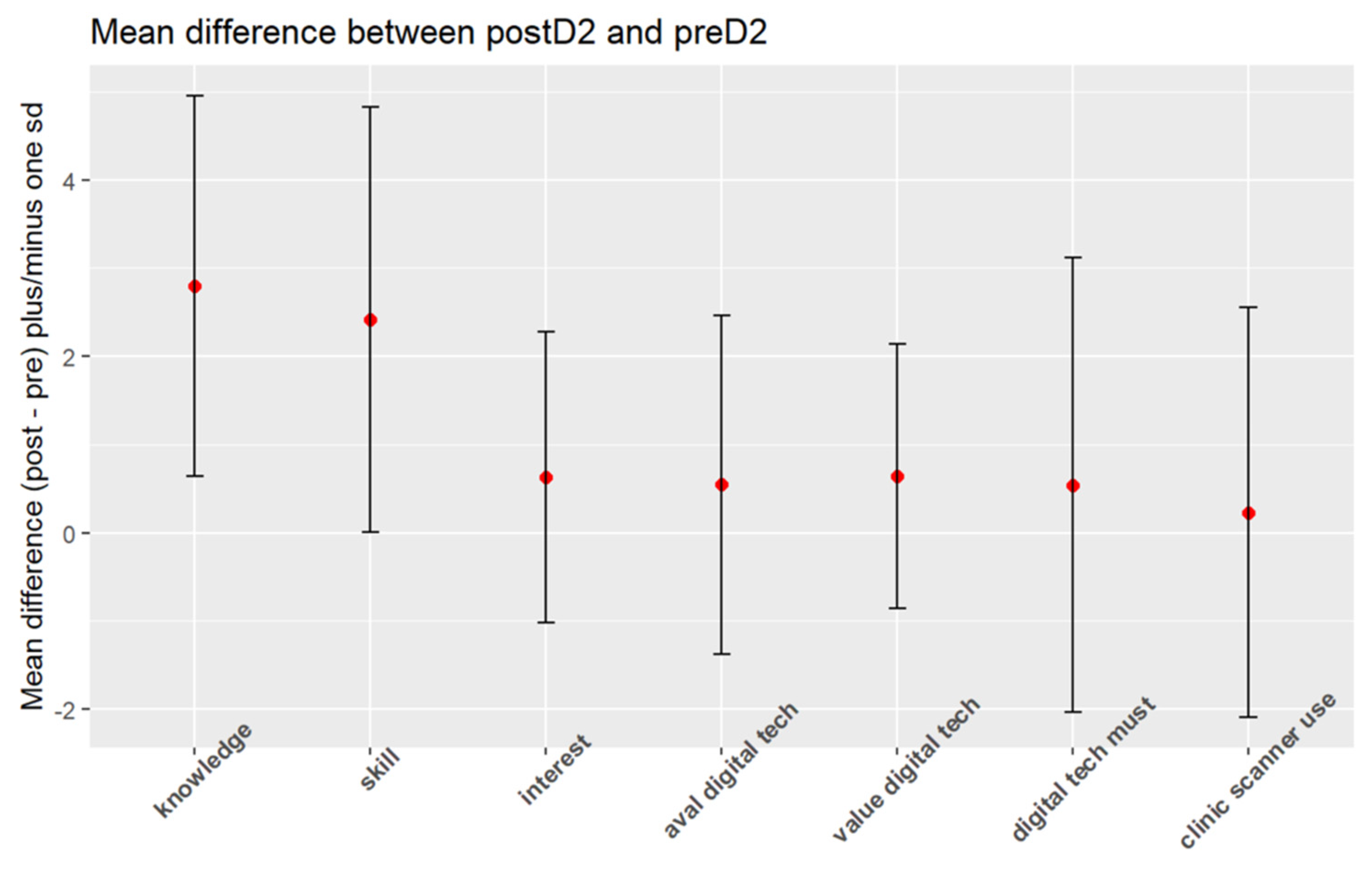
Figure 3.
The empirical density of students’ consideration about the “importance of having the technology” for pre-D2/post-D2 and all control groups.
Figure 3.
The empirical density of students’ consideration about the “importance of having the technology” for pre-D2/post-D2 and all control groups.
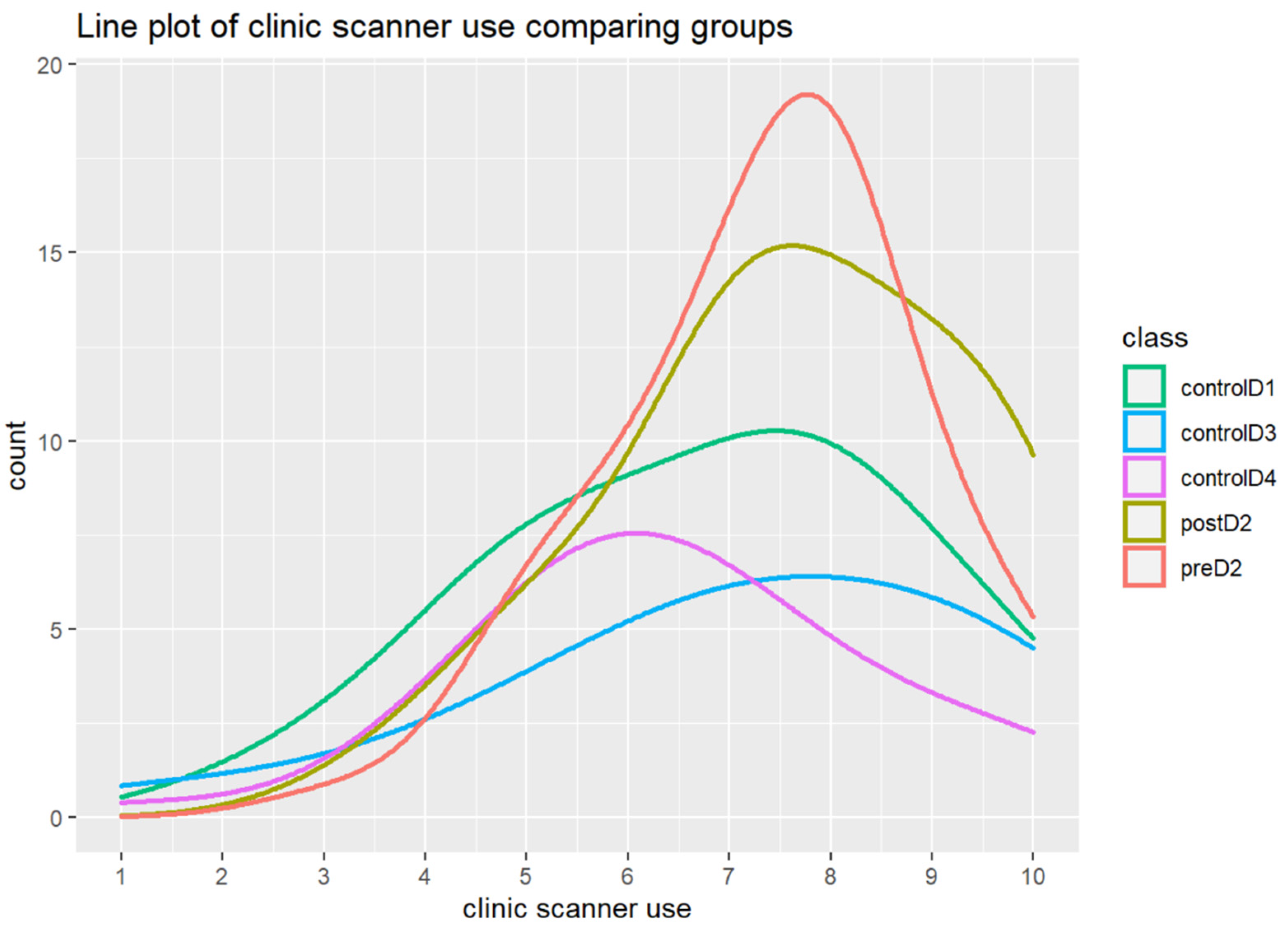

Table 1.
Eligibility criteria summarized.
| Inclusion criteria | Exclusion criteria |
|---|---|
| - Students at the OSU College of Dentistry - Completed the activity - Filled out the surveys - Students: 1st year (negative control) 2nd year (test group) 3rd and 4th years (positive control) |
- Students of other areas (different of Dentistry) - Non-students at the OSU College of Dentistry - Rejected to fill out - Did not complete the activity |
Table 2.
The questionnaire applied to the students (1 lowest, 10 highest; or 1 I strongly disagree, 10 I strongly agree).
Table 2.
The questionnaire applied to the students (1 lowest, 10 highest; or 1 I strongly disagree, 10 I strongly agree).
|
Table 3.
Classes compositions.
| Class | Class size | Age range/average | Gender | Underrepresented minority | ||
| Male | Female | Other | ||||
| 2023 | 120 | 21-34 / 24 | 65 | 55 | 1 | 8 |
| 2024 | 120 | 19-50 / 23 | 54 | 66 | 0 | 13 |
| 2025 | 118 | 20-38 / 22 | 55 | 63 | 0 | 14 |
| 2026 | 120 | 19-41 / 22 | 55 | 65 | 0 | 5 |
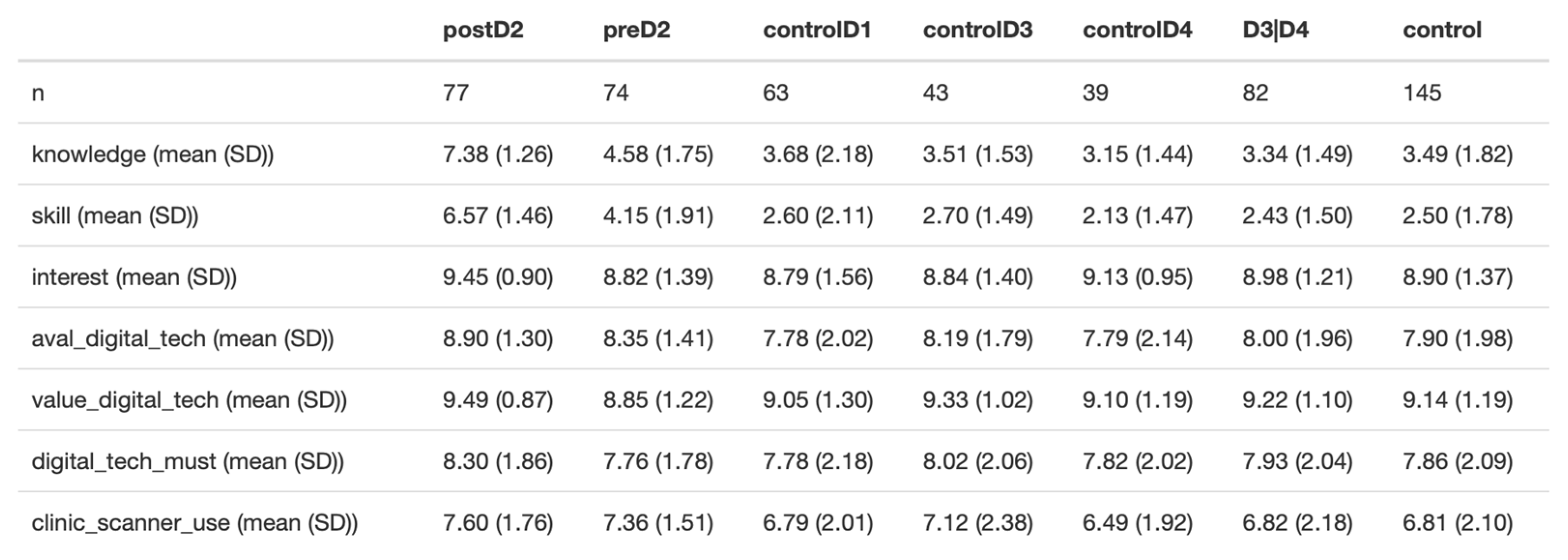
Table 4.
Summary statistics.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



