Submitted:
10 January 2024
Posted:
10 January 2024
You are already at the latest version
Abstract
Synthetic bone made of calcium phosphate is widely used for the clinical treatment of bone defects caused by trauma and bone tumors. Although synthetic bone is easy to use, its effects are only partial depending on the size and location of the bone defect, and there are many treatment options other than the use of synthetic bone. Various biodegradable polymers that are being considered for use as scaffolds for regenerative medicine are also being considered for use as synthetic bones; however, commercial synthetic bone products with performance comparable to that of calcium phosphate bioceramics have not yet been clinically applied. This review introduces the practice of bone regeneration therapy with synthetic bone and recent research on bone regeneration therapy with biodegradable polymers.
Keywords:
bone defect
; bone regeneration
; scaffold
; calcium phosphate
; biodegradable polymer
1. Introduction
The discovery of pluripotent cells such as induced pluripotent stem cells (iPS cells) has led to extensive research in regenerative medicine [1,2]. However, organs do not comprise of only one type of cell. For example, in the case of the heart, tissues such as myocardia, blood vessels, cardiac membranes, nerves, valves, and tendinous cords exhibit complex structures and functions that present many obstacles before heart regeneration can be applied to clinical practice. Regenerative medicine cannot simply be realized by increasing the number of cells in the target organ or tissue but requires the proliferation of these cells to form organs and tissues for which scaffolding plays an important role [3].
When a bone defect occurs due to trauma or treatment of a bone tumor, there are various treatment options that include joint arthroplasty, autologous bone grafting, allogeneic bone grafting, synthetic bone grafting, and the induced membrane technique [4,5,6,7,8,9,10,11,12,13,14,15]. The appropriate treatment strategy depends on the size and location of the bone defect and the type of bone [16].
Joint arthroplasty such as endoprosthetic replacement surgery is performed when the bone defect is relatively large or occurs near the joint. Osteosarcoma is the most common malignant bone tumor among adolescent patients and typically occurs near the joint [17], and tumor endoprostheses are usually used to reconstruct the bone defect created by tumor resection. Although joint arthroplasty can fill large defects, when artificial joint replacement is performed on younger patients, there is a high risk for complications such as loosening or implant failure due to its long-term postoperative course, potentially requiring an invasive revision procedure [18].
Autologous bone grafting is a method of using one's own bone to fill a defect. Since the graft uses bone obtained from the same patient receiving the graft, the graft material can be harvested relatively safely from a site with low donor-site morbidity, even if there is a certain amount of bone defect that occurs at the donor site. The iliac crest and fibula are often used as donor sites. There are no biocompatibility issues, as the graft uses bone from the patient’s own body. However, there is a finite supply of bone that can be harvested from the patient, and the donor site is damaged in order to harvest the bone for grafting, which may cause problems such as bleeding, infection, and pain at the donor site [19,20,21,22].
Allogeneic bone grafting is a treatment method wherein the bones of a donor are heat-treated, cryopreserved, and filled in the bone defect. The bones used are obtained from cadavers and surplus bone tissues that are no longer needed in surgery such as artificial joint replacement. Although there is an ample supply of bone in countries with well-developed bone bank services for the preservation and utilization of cadaver bones [23,24,25,26,27], in countries like Japan where human remains after cremation are buried, cultural and religious practices often prevent the collection of donor bone from cadavers. Thus, the donation of allogeneic bone can be in short supply at bone banks in these countries [28]. The resorptive and regenerative properties of allogeneic bone is not as effective as that of autologous bone; however, it not only serves as a scaffold, but also contains growth factors such as bone morphogenetic protein (BMP) that remain after heat treatment and enable osteoinduction [29,30,31]. In recent years, the human demineralized bone matrix (DBM) has been commercialized, and scaffolds that retain the ability to induce bone by growth factors has become widely available [32,33,34,35].
Bone regeneration with synthetic bone is performed using synthetic bone made of calcium phosphates such as hydroxyapatite and β-tricalcium phosphate (βTCP). These synthetic bones form a porous body and act as a scaffold for bone regeneration. Although the synthetic bone itself functions as a scaffold, it is incapable of osteoinduction and is unsuitable for the treatment of large bone defects.
The induced membrane technique can be used to treat relatively large bone defects by mixing synthetic bone with autologous bone [15,36]. However, because a membrane must be induced for bone regeneration, a separate operation is required prior to the grafting of synthetic and autologous bone. Since autologous bone is used, there is a limit to the number of defects that can be regenerated.
As described above, there are numerous treatment methods for bone defects. Each method presents advantages and disadvantages, and there is still room for development and research. In particular, treatment with synthetic bone is less invasive to patients, and improvement in efficiency and expansion of indications for bone regeneration by synthetic bone are strongly desired in bone regeneration treatment. In this review, we will introduce the clinical use of synthetic bone made of calcium phosphate bioceramics and the recent research and development involving synthetic bone made of biodegradable polymers.
2. Clinical Application of Bone Regeneration Therapy Using Synthetic Bone
Currently available synthetic bones used in clinical practice are mainly made of calcium phosphate such as hydroxyapatite and βTCP. Granular and block-type synthetic bones are porous [37] (Figure 1a). Osteoblasts and osteoclasts invade the pores and proliferate, promote the resorption of the synthetic bone and subsequent osteogenesis, and allow a gradual replacement with the patient's own bone. The bone defect caused by a bone tumor is initially filled with synthetic bone, and the regeneration of autologous bone can ultimately be expected. The treatment is mainly used for cancellous bone defects when the cortical bone remains intact. Autologous bone may be used in combination for large defects and bone defects near the articular surface.
Figure 2 is an image of a patient with a large aneurysmal bone cyst (ABC) in the tibia. Since the bone defect is close to the articular surface, a layer of autologous iliac cortical bone graft is placed under the subchondral bone in the deep layer of the articular surface after curettage of the tumor, and block-shaped and granular βTCP synthetic bones are filled underneath the autologous graft. The defect is fixated using a titanium alloy plate and screws for reinforcement (Figure 2b-d). Five years after the operation, the autologous iliac bone graft demonstrates osseous integration with the subchondral bone, and the synthetic bone is replaced with the autologous bone; however, residual synthetic bone is still visible in the center (Figure 2e).
The HA/collagen sponge composite is marketed as a synthetic bone for the treatment of bone defects. The composite combines both the osteoconductivity of HA and rapid degradation of collagen to enable a quick replacement by autologous bone [12,38]. However, its initial strength as a synthetic bone is mechanically weak, and inflammatory reactions including swelling, exudation, and redness of surgical wounds may occur in bones near the superficial layer such as finger bones. Therefore, the implantation site is limited, and careful monitoring is required for postoperative recovery. When the scaffold is infiltrated by blood or tissue fluid in the body, the scaffold becomes soft enough to fill the void tightly according to the shape of the bone defect (Figure 1a).
Figure 3 shows a patient with ABC of the humerus that recurred after two surgeries (curettage, βTCP synthetic bone grafting). For the third surgery, synthetic bone made of a HA/collagen composite was filled after curettage (Figure 3a-e). Five years after the operation, no tumor recurrence was observed, and regeneration of the autologous bone was observed; however, a growth disorder of the humerus occurred due to the effects of surgery during childhood, and the affected humerus became shorter compared to the unaffected side (Figure 3g, h). Although synthetic bone made of a HA/collagen composite provides good intraoperative handling, its high radiolucency is a disadvantage that makes postoperative radiologic confirmation difficult with plain radiography.
In the treatment of bone defects with synthetic bones, the presence of residual cortical bone is desirable. However, if the induced membrane technique is used, even a circumferential defect can be regenerated. The surgical procedure of the induced membrane technique is carried out in two steps. In the first step, the bone defect is filled with bone cement that acts as a spacer to close the wound. A periosteal-like tissue is subsequently formed around the spacer. A second surgery is performed 1-2 months later, in which the spacer is removed, and a mixture of autologous and granular synthetic bone are mixed and filled into the bone defect in its place [15]. The treatment of large bone defects is made possible by forming an induced membrane and mixing autologous and synthetic bone. Although we performed extracorporeal irradiation to kill malignant tumor cells in the femur and re-implanted the bone for cases with malignant femoral tumors [39], the irradiated bone showed a poor bony union rate, and bony union was sometimes not achieved. Following bone reconstruction with the extracorporeal irradiation and re-implantation technique for patients who exhibit nonunion or intramedullary nail failure, the femur was regenerated by the induced membrane technique. The spacer was removed during the second operation, filled with synthetic and iliac bone graft, and new bone was regenerated in the femoral bone defect and fixated with an intramedullary nail and an osteosynthesis plate. In addition, good bone formation was achieved with the induced membrane technique even in cases with a large bone defect that occurred due to a benign bone tumor of the tibia and extensive damage to the cortical bone that resulted from tumor curettage (Figure 4).
Synthetic bone made of calcium phosphate, which has already been used in clinical applications, is a convenient and powerful scaffold for bone regeneration therapy. However, there is still room for improvement, as there are limitations in terms of the site and size of bone defects that are suitable for treatment, a potential need for the combined use of autologous bone grafts, a possible need for multiple surgeries, and delay in weight-bearing ambulation for cases of the lower extremities.
3. Research and Development of Biodegradable Polymers
In the field of regenerative medicine, biodegradable polymers are used as scaffolds that are gradually replaced by the patient's own tissues, in addition to their roles as carriers of growth factors and cells. Langer and Vacanti succeeded in seeding bovine articular chondrocytes onto a scaffold made of polyglycolic acid-polylactic acid in the shape of a human auricle and transplanting it subcutaneously into the back of an immunocompromised mouse [40,41]. The scaffold is envisaged to play a role in regenerative medicine that is as important as pluripotent cells that can be engrafted in tissues [42]. Factors that influence the performance of a scaffold in regenerative medicine include its material (bio/tissue affinity, chemical properties), three-dimensional structure, added cells, and signaling molecules. The following sections will describe each factor.
3.1. Material of the Polymer
Bio-derivative polymers exhibit excellent biosafety and are being studied as potential biomaterials [43]. Collagen is abundantly present in the living body as a component of bone and soft tissues that include bone, cartilage, ligament, and tendon. In bone, more than 90% of the matrix proteins are composed of collagen. When bone is formed, calcium phosphate is deposited on collagen fibers that are produced by osteoblasts to create a tough bone matrix. [44]. Since collagen natively plays an important role as an extracellular matrix for hard and fibrous tissues of the human body, extensive research has been conducted for its use as a scaffold in regenerative medicine, including evaluative studies for the myocardium [45], bladder [46], and ligament [47]. Bone tissue regeneration is being studied clinically in animal models. Carstens et al. used collagen as a scaffold to regenerate bone in non-weight-bearing bones such as the maxilla and mandible [48]. Venugopal et al. created a composite of type I collagen and HA, on which human fetal osteoblast cells were cultured [49]. In Alizarin Red S staining for assessing calcification [50], cultures on this HA-collagen composite scaffold showed more vivid staining compared to the HA-free collagen fiber scaffold [49]. Yeo et al. created a porous, three-dimensional composite of βTCP and polycaprolactone (PCL), which was filled with collagen nanofibers to form scaffolds [51]. The MTT (3- (4,5-dimethylthiazol-2-yl) -2, 5-diphenyl tetrazolium bromide) assay [52] to evaluate the cell proliferation of human MG-63 osteoblast-like cell demonstrated a higher cell proliferation in this scaffold compared to the βTCP/PCL composite scaffold without collagen nanofibers.
Gelatin is a triple helix structure derived from denatured and decomposed polypeptide chains of collagen fibers. Gelatin is widely used in foods and cosmetics. In the medical field, it is commonly used as capsules for pharmaceuticals, as well as a hemostatic agent [53] and an embolic substance for arterial embolization [54,55]. Gelatin is also being studied as a scaffold in regenerative medicine. Yokota et al. created a scaffold from a gelatin sponge coated in poly(D,L-lactic-co-glycolic acid) as a carrier for recombinant human bone morphogenetic protein (rhBMP)-2 and implanted the scaffold in the dorsal subcutaneous tissue of a rat to induce ectopic bone formation [56]. Ramin et al. examined the possibility of using gelatin sponge, which is commercially available as a hemostatic agent, as a scaffold. They cultured MG-63 cells on a gelatin sponge and observed their cell number, alkaline phosphatase (ALP) activity, and cell invasion into the pores of the sponge [57].
Although collagen is a gold standard for scaffolds made of animal-based polymers in regenerative medicine, various other materials have been considered for use as a scaffold, such as cellulose obtained from plant polysaccharides [58], chitosan derived from the exoskeleton of crustaceans such as shrimp and crab [59,60], and hyaluronic acid [61,62], which is also a component of articular cartilage and articular fluid.
Natural polymers are used in foods and cosmetics, and are considered to be biomaterials with high biocompatibility. In basic research, there are many reports that describe their excellent properties such as high biocompatibility and rapid degradability, and they are expected to be used as a scaffold in bone regenerative medicine. However, there are concerns about risks such as immune reactions due to disease transfer and xenogenicity [63,64]. Clinical applications of natural polymers should warrant caution, as there have been reports of allergies due to injections and foods, inflammation, and pulmonary complications [65,66,67].
A biodegradable synthetic polymer is capable of being hydrolyzed and absorbed in vivo. The use of synthetic polymers as scaffolds for bone regeneration is being investigated. We developed and evaluated the performance of a scaffold using polylactic acid-p-dioxanone-polyethylene glycol block copolymer (PLA-DX-PEG), which is a biodegradable polymer, as a carrier of rhBMP-2 [68] (Figure 5a). We succeeded in inducing the formation of ectopic bone under the dorsal fascia of mice using this scaffold (Figure 5a-d). This scaffold was also able to repair a critical-sized bone defect in the rabbit ulna [42] (Figure 5e). Other common synthetic polymers that have been evaluated as materials for scaffolds include poly-L-lactic acid (PLA), polycaprolactone (PCL), polylactic-co-glycolic acid (PLGA), and poly (vinyl alcohol) (PVA).
Although the PLA-DX-PEG we previously studied is a copolymer of PLA and PEG, PLA itself is also being evaluated as scaffold. PLA is a biodegradable polymer widely used in food trays and agricultural films. Zhang et al. created a collagen/PLA scaffold in which collagen was combined with the layer of nanofiber of PLA [70]. From the bone marrow-derived mesenchymal stem cells (BMSCs) cultured onto this scaffold, a gene expression of osteocalcin (OCN), which is a bone formation marker, was observed stronger than that of BMSCs cultured onto collagen scaffolds. They also filled the osteochondral defects created in the femur of rabbits with the collagen/PLA scaffold, and an evaluation of the scaffold using the Visual Histological Assessment Scale of the International Cartilage Repair Society [71] demonstrated better regeneration of subchondral bone than the group filled with a scaffold made of collagen alone.
PCL is a thermoplastic with a low melting point and a polymer of ε-polycaprolactone [72] with excellent biocompatibility [73]. Wang et al. added nanosilicates to PCL to prepare scaffolds comprising of nanofibers and cultured MC3T3-E1 cells, which are osteoblast cell lines [74]. On this scaffold, the cell viability and ALP activity of MC3T3-E1 cells increased according to the amount of nanosilicates.
Yang et al. created and evaluated a scaffold consisting of nanofibers in which nanosilicates were combined with PLGA [75]. They cultured osteoblast-like cells (SaOS-2 cells) on this scaffold and evaluated their differentiation into bone using Alizarin Red S staining and ALP activity. As a result, it was shown that nanosilicate/PLGA scaffold promoted the better differentiation of SaOS-2 cells into bone compared to a scaffold made of PLGA alone.
PVA is highly hydrophilic and easily dissolves in vivo [76]. Enayati et al developed a PVA/HA scaffold that combines PVA with nanoparticles of HA [77]. They cultured MG63 cells on a PVA/HA scaffold and evaluated their effect on bone formation using Alizarin Red S staining and ALP activity. As a result, the PVA/HA scaffold promoted better differentiation of MG63 cells into osteoblasts than the scaffold with scaffold with alone. Although PVA is a substance with excellent biocompatibility, PVA itself is bio-inert [78], and it is speculated that the additional effect of HA nanoparticles promoted differentiation into osteoblasts.
Biodegradable polymer is not limited to one type of material, and by combining multiple materials, it is possible to create scaffolds that incorporate the advantages of each material. Many combinations of scaffolds have been studied, such as combining different biodegradable polymers with each other and combining biodegradable polymers with inorganic materials. Both the collagen/PLA composite described by Zhang et al. [70] and the PVA/HA composite described by Enayati et al. [77] can be expected to demonstrate better bone regeneration than a scaffold made of a single material. In polymer composites, the type of material, method of creating the composite, and its three-dimensional structure are factors related to bone regeneration, but there are innumerable combinations of materials, and the optimum composite for bone formation have not yet been clarified.
3.2. Three-Dimensional Structure of Synthetic Bonessc
For bone regeneration scaffolds, not only the material but also the three-dimensional structure is an important factor, and various forms of scaffolds are being investigated.
Like the PLA-DX-PEG scaffold we used, there are other hydrogel scaffolds. We were able to combine rhBMP-2 with a PLA-DX-PEG scaffold to form ectopic bone on the dorsum of mice and regenerate bone in critical-sized bone defects of rabbit ulna [42]. Other scaffolds reported in the literature include a gelatin hydrogel [79] and gelatin and chitosan composite hydrogel [80].
A sponge-like scaffold can be made by freeze-drying the hydrogel material (Figure 6a). Takeda et al created a sponge-like implant from a collagen/rhBMP-2 composite and reconstructed rat collagenellae (ossicles) [81]. Takahashi et al. cultivated rat mesenchymal stem cells (MSCs) on a gelatin/β-TCP composite sponge and demonstrated using scanning electron microscopy (SEM) that MSCs invaded and adhered to the pores of the sponge [82] (Figure 6b). By making the scaffold a porous body, cells are more likely to enter, and a superior tissue regeneration is observed compared to those in the form of a dense, compacted body.
Fiber-shaped implants can also serve as good scaffolds by controlling their three-dimensional structures [69]. Electrospinning is a method of fiber production that charges and ejects a polymer solution through a nozzle under a high-voltage electric field to produce nano-sized fibers [83]. Lee et al. created a collagen fiber and PCL composite with a diameter of approximately 350 nm [84]. By hardening collagen nanofiber with excellent cell adhesion and proliferation using PCL, it was possible to increase the mechanical strength of the scaffold. They cultured MG63 cells on this scaffold and demonstrated better cell proliferation by MTT assay compared to a scaffold made of PCL alone. Both the collagen/PLA composite scaffold described by Zhang et al. [70] and the PVA/HA composite scaffold described by Enayati et al. are fibrous scaffolds produced by electrospinning [76] (Figure 6c).
By creating a scaffold by 3D-printing, it has become possible to control its fine structure. The PLGA/HA /chitosan scaffolds described by Deng et al. were made by 3D printing, and their pore size was approximately 430 μm. Zhang et al. made a PTG implant in which graphene oxide (GO) was combined with PLGA and βTCP using 3D printing technology. This scaffold was a lattice-structure implant with a pore size of 400 ± 50 μm (Figure 6d,e). MSC of rat was cultured onto this scaffold, and increases in gene expression of bone formation markers ALP, OCN, and osteopontin (OPN) were observed. They also used this scaffold to repair critical-sized cranial defects in rats [85].
3.3. Cells and Signaling Molecules
Calcium phosphate bioceramic scaffolds (TCP, HA) are osteoconductive and are currently used clinically in the treatment of bone defects. Relatively small bone defects can be repaired by simply filling voids with this scaffold. However, there is a limit to the size of bone defects that can be treated with this scaffold alone.
Unlike calcium phosphate-based scaffolds that are osteoconductive, biodegradable polymers are not osteoconductive. Therefore, it is necessary to improve the efficiency of bone regeneration by adding signaling molecules and cells to these scaffolds in order to increase their osteoconductivity.
Among the signaling molecules that promote bone formation, BMP-2 is the most commonly used. BMP-2 induces bone formation and has been put to practical use in the treatment of fractures and bone defects. In order for BMP-2 to act efficiently in fractures and bone defects, it is important for scaffolds to act as a carrier and drug delivery system (DDS) for BMP-2. In the in vitro test of the PLGA/HA/chitosan scaffold reported by Deng et al. described in the previous section, when BMP-2 is added to PLGA/HA/chitosan scaffold and immersed in a culture medium, the scaffold takes more than 2 weeks to disintegrate and to gradually release the BMP-2 over a month period or more. In an in vivo study, Deng et al. reported that this scaffold successfully repaired a bone defect created in a rabbit mandible [86].
Other signaling molecules such as BMP-6 and BMP-7, which are part of the BMP family, and vascular endothelial growth factor (VEGF), which is an angiogenesis factor/tissue growth factor, are expected to be used in clinical applications [87,88].
In the body, when scaffolds are placed on the affected area, bone-forming cells from surrounding tissues enter the scaffold and proliferate to form bone. However, in order to repair a large bone defect, it can be expected that replacement with new bone will be accelerated by engrafting cells in scaffold in advance. The cells combined with scaffolds are expected to produce the aforementioned signaling molecules and to differentiate into target organs/tissues to be regenerated. In recent years, many studies have been conducted using iPS cells. iPS cells can be produced by introducing several types of genes called Yamanaka factors into somatic cells collected from the skin and demonstrate pluripotency that allows them to differentiate into any cell. Since it can be differentiated into various cells, it is expected to be applied clinically in regenerative medicine, treatment of intractable diseases, and cancer treatment. In bone regeneration, iPS cells are also being investigated as cells to be added to scaffolds.
The cells seeded on scaffolds for bone regeneration do not need to have pluripotency like iPS cells, and it is sufficient if they differentiate into bone tissue. Therefore, considerable research on BMSC, which is a progenitor cell of osteoblasts, has been conducted [89,90]. BMSC from a patient can be relatively easily obtained in abundance from the iliac bone marrow of the patient with minimal invasiveness. BMSC can be differentiated into osteoblast progenitor cells by culturing in a bone-forming medium containing β-glycerophosphate and dexamethasone. Studies are being conducted to promote bone formation by culturing BMSC on scaffolds and differentiating it into osteoblast progenitor cells. One research report has recently described the addition of BMSC to a scaffold made of chitosan/HA and PCL/PLA composites.
A therapeutic method of adding platelet-rich plasma (PRP) to scaffolds is also being investigated. PRP can be easily obtained by centrifuging the patient's peripheral blood. PRP contains growth factors such as VEGF, insulin-like growth factor (IGF), platelet-derived growth factor (PDGF), and transforming growth factor beta (TGF-β). These growth factors are not expected to act as cells that differentiate into tissues but are rather expected to be used as a DDS for patient-derived signaling molecules [91,92]. Cheng et al. treated critical-sized cranial bone defects in rats with a silk fibroin/PCL composite scaffold augmented with PRP [93].
4. Conclusions
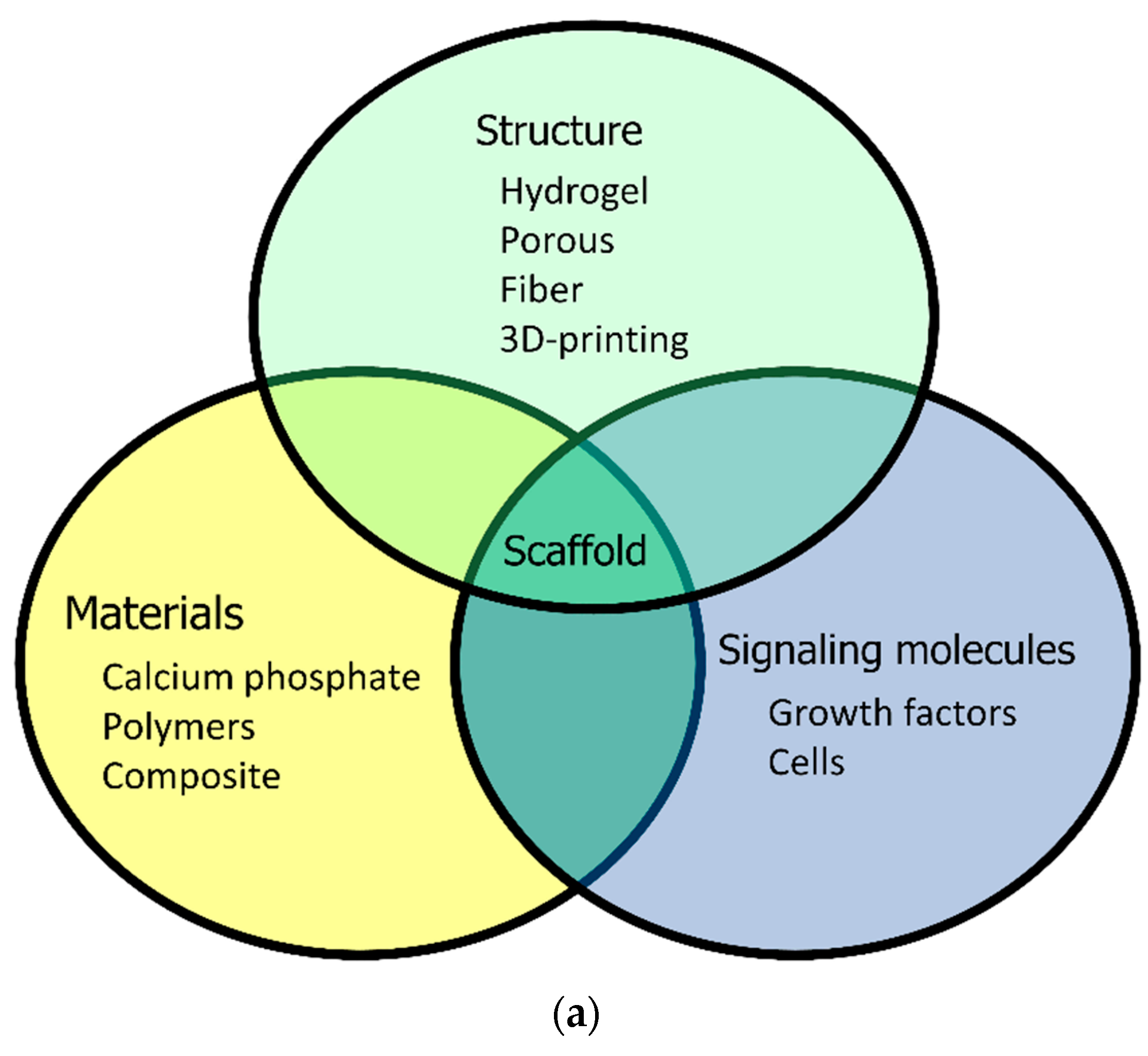
The performance of biodegradable scaffold in bone regeneration is associated with its material, three-dimensional structure, and added cells and signaling molecules; however, there are innumerable combinations that can yield varying results (Figure 7). Synthetic bone made of calcium phosphate bioceramics has already been used clinically in human patients. Although synthetic bone made of calcium phosphate bioceramics is a convenient therapeutic device, there are some disadvantages such as the time it takes to be replaced with bone, the inability to perform early loading in weight-bearing bone, limitation to the size of bone defects that can be treated, and the need to harvest autologous bone when the defect is large.
Various research on synthetic bones made of biodegradable polymers have been conducted, but their performance is still inferior to that of calcium phosphate bioceramic material, which has osteoconductivity. Synthetic bone made of a HA/collagen composite—a composite of collagen, a biodegradable polymer, and HA, a calcium phosphate bioceramic—is one successful example. By clarifying the optimum combination of material properties, structural characteristics, and cells and signaling molecules, the development of an ideal scaffold with high bone regeneration efficiency can be expected in future studies.
Author Contributions
Conceptualization, K.A., N.S.; methodology, K.A. and N.S.; validation, K.A. and S.N.; investigation, K.A. and S.N.; resources, K.A., H.I., Y.K., A.T., M.K., M.O., J.T. and S.S.; data curation, K.A.; writing—original draft preparation, K.A. and N.S.; writing—review and editing, K.A.; visualization, K.A., H.I., Y.K., A.T., M.K., M.O., and S.S.; supervision, J.T.; project administration, N.S.
Funding
This research received no external funding.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
We would like to thank Sho Steven Sugita (OrthoTranslations) for English language editing.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Takahashi, K.; Okita, K.; Nakagawa, M.; Yamanaka, S. Induction of pluripotent stem cells from fibroblast cultures. Nat. Protoc. 2007, 2, 3081–3089. [Google Scholar] [CrossRef]
- Okita, K.; Ichisaka, T.; Yamanaka, S. Generation of germline-competent induced pluripotent stem cells. Nature. 2007, 448, 313–U1. [Google Scholar] [CrossRef] [PubMed]
- Kwon, S.G.; Kwon, Y.W.; Lee, T.W.; Park, G.T.; Kim, J.H. Recent advances in stem cell therapeutics and tissue engineering strategies. Biomater. Res. 2018, 22, 36. [Google Scholar] [CrossRef]
- Ayoub, M.A.; El-Rosasy, M.A. Hybrid grafting of post-traumatic bone defects using beta-tricalcium phosphate and demineralized bone matrix. Eur. J. Orthop. Surg. Traumatol. 2014, 24, 663–670. [Google Scholar] [CrossRef]
- Dimitriou, R.; Mataliotakis, G.I.; Angoules, A.G.; Kanakaris, N.K.; Giannoudis, P.V. Complications following autologous bone graft harvesting from the iliac crest and using the RIA: a systematic review. Injury. 2011, 42 Suppl 2, S3–15. [Google Scholar] [CrossRef]
- Goulet, J.A.; Senunas, L.E.; DeSilva, G.L.; Greenfield, M.L. Autogenous iliac crest bone graft. Complications and functional assessment. Clin. Orthop. Relat. Res. 1997, 339, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Kong, C.B.; Lee, S.Y.; Jeon, D.G. Staged lengthening arthroplasty for pediatric osteosarcoma around the knee. Clin. Orthop. Relat. Res. 2010, 468, 1660–1668. [Google Scholar] [CrossRef]
- Manfrini, M.; Bindiganavile, S.; Say, F.; Colangeli, M.; Campanacci, L.; Depaolis, M.; Ceruso, M.; Donati, D. Is There Benefit to Free Over Pedicled Vascularized Grafts in Augmenting Tibial Intercalary Allograft Constructs? Clin. Orthop. Relat. Res. 2017, 475, 1322–1337. [Google Scholar] [CrossRef] [PubMed]
- Muscolo, D.L.; Ayerza, M.A.; Aponte-Tinao, L.A. Massive allograft use in orthopedic oncology. Orthop. Clin. North Am. 2006, 37, 65–74. [Google Scholar] [CrossRef]
- Rabitsch, K.; Maurer-Ertl, W.; Pirker-Fruhauf, U.; Wibmer, C.; Leithner, A. Intercalary reconstructions with vascularised fibula and allograft after tumour resection in the lower limb. Sarcoma, 2013; 160295. [Google Scholar] [CrossRef]
- Sotome, S.; Ae, K.; Okawa, A.; Ishizuki, M.; Morioka, H.; Matsumoto, S.; Nakamura, T.; Abe, S.; Beppu, Y.; Shinomiya, K. Efficacy and safety of porous hydroxyapatite/type 1 collagen composite implantation for bone regeneration: A randomized controlled study. J. Orthop. Sci. 2016, 21, 373–380. [Google Scholar] [CrossRef]
- Tamai, N.; Myoui, A.; Tomita, T.; Nakase, T.; Tanaka, J.; Ochi, T.; Yoshikawa, H. Novel hydroxyapatite ceramics with an interconnective porous structure exhibit superior osteoconduction in vivo. J. Biomed. Mater. Res. 2002, 59, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.; Kumagae, Y.; Saito, M.; Chazono, M.; Komaki, H.; Kikuchi, T.; Kitasato, S.; Marumo, K. Bone formation and resorption in patients after implantation of beta-tricalcium phosphate blocks with 60% and 75% porosity in opening-wedge high tibial osteotomy. J. Biomed. Mater. Res. B Appl. Biomater. 2008, 86, 453–459. [Google Scholar] [CrossRef] [PubMed]
- Taylor, B.C.; French, B.G.; Fowler, T.T.; Russell, J.; Poka, A. Induced membrane technique for reconstruction to manage bone loss. J. Am. Acad. Orthop. Surg. 2012, 20, 142–150. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Hu, J.; Zhu, K.; Cai, T.; Ma, X. Survival, complications and functional outcomes of cemented megaprostheses for high-grade osteosarcoma around the knee. Int. Orthop. 2018, 42, 927–938. [Google Scholar] [CrossRef] [PubMed]
- Roddy, E.; DeBaun, M.R.; Daoud-Gray, A.; Yang, Y. P.; Gardner, M.J. Treatment of critical-sized bone defects: clinical and tissue engineering perspectives. Eur. J. Orthop. Surg. Traumatol. 2018, 28, 351–362. [Google Scholar] [CrossRef] [PubMed]
- Mirabello, L.; Pfeiffer, R.; Murphy, G.; Daw, N.C.; Patiño-Garcia, A.; Troisi, R.J.; Hoover, R.N.; Douglass, C.; Schüz, J.; Craft, A.W.; Savage, S.A. Height at diagnosis and birth-weight as risk factors for osteosarcoma. Cancer Causes Control. 2011, 22, 899–908. [Google Scholar] [CrossRef] [PubMed]
- Tsagozis, P.; Parry, M.; Grimer, R. High complication rate after extendible endoprosthetic replacement of the proximal tibia: a retrospective study of 42 consecutive children. Acta. Orthop. 2018, 89, 678–682. [Google Scholar] [CrossRef] [PubMed]
- Dimar, J.R. 2nd; Glassman, S.D.; Burkus, J.K.; Pryor, P.W.; Hardacker, J.W.; Carreon, L.Y. Two-year fusion and clinical outcomes in 224 patients treated with a single-level instrumented posterolateral fusion with iliac crest bone graft. Spine J. 2009, 9, 880–885. [Google Scholar] [CrossRef] [PubMed]
- Gore, D.R. The arthrodesis rate in multilevel anterior cervical fusions using autogenous fibula. Spine. 2001, 26, 1259–1263. [Google Scholar] [CrossRef]
- Jakoi, A.M.; Iorio, J.A. Iorio; Cahill, P.J. Autologous bone graft harvesting: a review of grafts and surgical techniques. Musculoskelet. Surg. 2015, 99, 171–178. [Google Scholar] [CrossRef]
- Schwartz, C.E.; Martha, J.F.; Kowalski, P.; Wang, D.A.; Bode, R.; Li, L.; Kim, D.H. Prospective evaluation of chronic pain associated with posterior autologous iliac crest bone graft harvest and its effect on postoperative outcome. Health Qual. Life Outcomes. 2009, 7, 49. [Google Scholar] [CrossRef] [PubMed]
- de Alencar, P.G; Vieira, I.F. BONE BANKS. Rev. Bras. Ortop. 2010, 45, 524–528. [Google Scholar] [CrossRef]
- Mishra, A.K.; Vikas, R.; Agrawal, H.S. Allogenic bone grafts in post-traumatic juxta-articular defects: Need for allogenic bone banking. Med. J. Armed Forces India. 2017, 73, 282–286. [Google Scholar] [CrossRef] [PubMed]
- Mohr, J.; Germain, M.; Winters, M.; Fraser, S.; Duong, A.; Garibaldi, A.; Simunovic, N.; Alsop, D.; Dao, D.; Bessemer, R.; Ayeni, O.R.; Bioburden Steering Committee and Musculoskeletal Tissue Working group. Disinfection of human musculoskeletal allografts in tissue banking: a systematic review. Cell Tissue Bank. 2016, 17, 573-584. [CrossRef] [PubMed]
- Warnock, J.M.; Rowan, C.H.; Davidson, H.; Millar, C.; McAlinden, M.G. Improving efficiency of a regional stand alone bone bank. Cell Tissue Bank, 2016, 17, 85–90. [Google Scholar] [CrossRef]
- Zwitser, E.W.; Jiya, T.U.; Licher, H.G.; van Royen, B.J. Design and management of an orthopaedic bone bank in The Netherlands. Cell Tissue Bank. 2012, 13, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Uchiyama, K.; Inoue, G.; Takahira, N.; Takaso, M. Revision total hip arthroplasty - Salvage procedures using bone allografts in Japan. J. Orthop. Sci. 2017, 22, 593–600. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, G.; Moghaddam, A. Allograft bone matrix versus synthetic bone graft substitutes. Injury. 2011, 42, S16–S21. [Google Scholar] [CrossRef] [PubMed]
- Kowalczewski, C.J.; Saul, J.M. Biomaterials for the Delivery of Growth Factors and Other Therapeutic Agents in Tissue Engineering Approaches to Bone Regeneration. Front Pharmacol. 2018, 9, 15. [Google Scholar] [CrossRef]
- Smith, C.A.; Board, T.N.; Rooney, P.; Eagle, M.J.; Richardson, S.M; Hoyland, J.A. Human decellularized bone scaffolds from aged donors show improved osteoinductive capacity compared to young donor bone. Plos One. 2017, 12, 15. [Google Scholar] [CrossRef]
- Gitelis, S.; Virkus, W.; Anderson, D.; Piasecki, P.; Yao, T.K. Functional outcomes of bone graft substitutes for benign bone tumors. Orthopedics. 2004, 27 Suppl 1, S141–S144. [Google Scholar] [CrossRef]
- Kwok, T.Y.; Wong, H.K. Evolving Treatment Modality of Hand Enchondroma in a Local Hospital: From Autograft to Artificial Bone Substitutes. J. Orthop. Traumatol. Rehabil. 2016, 20, 19–23. [Google Scholar] [CrossRef]
- Urist, MR. Bone: formation by autoinduction. Science. 1965, 150, 893–899. [Google Scholar] [CrossRef] [PubMed]
- van der Stok, J.; Hartholt, K.A.; Schoenmakers, D.A.L.; Arts, J.J.C. The available evidence on demineralised bone matrix in trauma and orthopaedic surgery: A systematic review. Bone Joint Res. 2017, 6, 423–432. [Google Scholar] [CrossRef] [PubMed]
- Kombate, N.K.; Walla, A.; Ayouba, G.; Bakriga, B.M.; Dellanh, Y.Y.; Abalo, A.G.; Dossim, A.M. Reconstruction of traumatic bone loss using the induced membrane technique: preliminary results about 11 cases. J. Orthop. 2017, 14, 489–494. [Google Scholar] [CrossRef] [PubMed]
- Yoshikawa, H.; Tamai, N.; Murase, T.; Myoui, A. Interconnected porous hydroxyapatite ceramics for bone tissue engineering. J. R. Soc. Interface. 2009, 6 Suppl 3, S341–S348. [Google Scholar] [CrossRef]
- Masaoka, T.; Yamada, T.; Yuasa, M.; Yoshii, T.; Okawa, A.; Morita, S.; Kozaka, Y.; Hirano, M.; Sotome, S. Biomechanical evaluation of the rabbit tibia after implantation of porous hydroxyapatite/collagen in a rabbit model. J. Orthop. Sci. 2016, 21, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Pruksakorn, D.; Kongthavonskul, J.; Teeyakasem, P.; Phanphaisarn, A.; Chaiyawat, P.; Klangjorhor, J.; Arpornchayanon, O. Surgical outcomes of extracorporeal irradiation and re-implantation in extremities for high grade osteosarcoma: A retrospective cohort study and a systematic review of the literature. J. Bone Oncol. 2019, 14, 8. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.L.; Vacanti, J.P.; Paige, K.T.; Upton, J.; Vacanti, C.A. Transplantation of chondrocytes utilizing a polymer-cell construct to produce tissue-engineered cartilage in the shape of a human ear. Plast. Reconstr. Surg. 1997, 100, 297–302. [Google Scholar] [CrossRef]
- Langer, R.; Vacanti, J.P. Tissue engineering. Science. 1993, 260, 920–926. [Google Scholar] [CrossRef]
- Aoki, K.; Saito, N. Biodegradable Polymers as Drug Delivery Systems for Bone Regeneration. Pharmaceutics. 2020, 12, 20. [Google Scholar] [CrossRef] [PubMed]
- Ko, H.F.; Sfeir, C.; Kumta, P.N. Novel synthesis strategies for natural polymer and composite biomaterials as potential scaffolds for tissue engineering. Philos. Trans. A Math Phys. Eng. Sci. 2010, 368, 1981–1997. [Google Scholar] [CrossRef] [PubMed]
- Long, F. Building strong bones: molecular regulation of the osteoblast lineage. Nat. Rev. Mol. Cell Biol. 2012, 13, 27–38. [Google Scholar] [CrossRef] [PubMed]
- Rashedi, I.; Talele, N.; Wang, X.H.; Hinz, B.; Radisic, M.; Keating, A. Collagen scaffold enhances the regenerative properties of mesenchymal stromal cells. PloS One. 2017, 12, e0187348. [Google Scholar] [CrossRef] [PubMed]
- Hoogenkamp, H.R.; Pot, M.W.; Hafmans, T.G.; Tiemessen, D.M.; Sun, Y.; Oosterwijk, E.; Feitz, W.F.; Daamen, W.F.; van Kuppevelt, T.H. Scaffolds for whole organ tissue engineering: Construction and in vitro evaluation of a seamless, spherical and hollow collagen bladder construct with appendices. Acta Biomater. 2016, 43, 112–121. [Google Scholar] [CrossRef]
- Ashworth, J.C.; Mehr, M.; Buxton, P.G.; Best, S.M.; Cameron, R.E. Optimising collagen scaffold architecture for enhanced periodontal ligament fibroblast migration. J. Mater. Sci. Mater. Med. 2018, 29, 166. [Google Scholar] [CrossRef] [PubMed]
- Carstens, M.H.; Chin, M.; Li, X.J. In situ osteogenesis: Regeneration of 10-cm mandibular defect in porcine model using recombinant human bone morphogenetic protein-2 (rhBMP-2) and helistat absorbable collagen sponge. J. Craniofac. Surg. 2005, 16, 1033–1042. [Google Scholar] [CrossRef] [PubMed]
- Venugopal, J.; Low, S.; Choon, A.T.; Sampath Kumar, T.S.; Ramakrishna, S. Mineralization of osteoblasts with electrospun collagen/hydroxyapatite nanofibers. J. Mater. Sci. Mater. Med. 2008, 19, 2039–46. [Google Scholar] [CrossRef]
- Gregory, C.A.; Gunn, W.G.; Peister, A.; Prockop, D.J. An Alizarin red-based assay of mineralization by adherent cells in culture: comparison with cetylpyridinium chloride extraction. Anal. Biochem. 2004, 329, 77–84. [Google Scholar] [CrossRef]
- Yeo, M.; Lee, H.; Kim, G. Three-dimensional hierarchical composite scaffolds consisting of polycaprolactone, beta-tricalcium phosphate, and collagen nanofibers: fabrication, physical properties, and in vitro cell activity for bone tissue regeneration. Biomacromolecules. 2011, 12, 502–10. [Google Scholar] [CrossRef]
- Mosmann, T. Rapid colorimetric assay for cellular growth and survival: application to proliferation and cytotoxicity assays. J. Immunol. Methods. 1983, 65, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, H.P.; Janda, R.; Clarke, J. Clinical and experimental observations on the use of gelatin sponge or foam. Surgery. 1946, 20, 124–132. [Google Scholar] [PubMed]
- Abada, H.T.; Golzarian, J. Gelatine sponge particles: handling characteristics for endovascular use. Tech. Vasc. Interv. Radiol. 2007, 10, 257–260. [Google Scholar] [CrossRef] [PubMed]
- Sangro, B.; Bilbao, I.; Herrero, I.; Corella, C.; Longo, J.; Beloqui, O.; Ruiz, J.; Zozaya, J.M.; Quiroga, J.; Prieto, J. Partial splenic embolization for the treatment of hypersplenism in cirrhosis. Hepatology. 1993, 18, 309–314. [Google Scholar] [CrossRef] [PubMed]
- Yokota, S.; Sonohara, S.; Yoshida, M.; Murai, M.; Shimokawa, S.; Fujimoto, R.; Fukushima, S.; Kokubo, S.; Nozaki, K.; Takahashi, K.; Uchida, T.; Yokohama, S.; Sonobe, T. A new recombinant human bone morphogenetic protein-2 carrier for bone regeneration. Int. J. Pharm. 2001, 223, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Rohanizadeh, R.; Swain, M.V.; Mason, R.S. Gelatin sponges (Gelfoam) as a scaffold for osteoblasts. J. Mater. Sci. Mater. Med. 2008, 19, 1173–1182. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, P.K.; Adhikari, J.; Saha, P. Facile fabrication of electrospun regenerated cellulose nanofiber scaffold for potential bone-tissue engineering application. Int J Biol Macromol. 2019, 122, 644–652. [Google Scholar] [CrossRef] [PubMed]
- Sharifi, F.; Atyabi, S.M.; Norouzian, D.; Zandi, M.; Irani, S.; Bakhshi, H. . Polycaprolactone/carboxymethyl chitosan nanofibrous scaffolds for bone tissue engineering application. Int J Biol Macromol. 2018, 115, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Peng, H.; Wu, Y.; Zhang, C.; Cai, Y.; Xu, G.; Li, Q.; Chen, X.; Ji, J.; Zhang, Y.; OuYang, H.W. The promotion of bone regeneration by nanofibrous hydroxyapatite/chitosan scaffolds by effects on integrin-BMP/Smad signaling pathway in BMSCs. Biomaterials. 2013, 34, 4404–4417. [Google Scholar] [CrossRef]
- Yan, H.J.; Casalini, T.; Hulsart-Billström, G.; Wang, S.; Oommen, O.P.; Salvalaglio, M.; Larsson, S.; Hilborn, J.; Varghese, O.P. Synthetic design of growth factor sequestering extracellular matrix mimetic hydrogel for promoting in vivo bone formation. Biomaterials. 2018, 161, 190–202. [Google Scholar] [CrossRef]
- Paidikondala, M.; Wang, S.J.; Hilborn, J.; Larsson, S.; Varghese, O.P. Impact of Hydrogel Cross-Linking Chemistry on the in Vitro and in Vivo Bioactivity of Recombinant Human Bone Morphogenetic Protein-2. ACS Appl. Bio Mater. 2019, 2, 2006–2012. [Google Scholar] [CrossRef] [PubMed]
- Bach, F.H.; Fishman, J.A.; Daniels, N.; Proimos, J.; Anderson, B.; Carpenter, C.B.; Forrow, L.; Robson, S.C.; Fineberg, H.V. Uncertainty in xenotransplantation: Individual benefit versus collective risk. Nat. Med. 1998, 4, 141–144. [Google Scholar] [CrossRef] [PubMed]
- Butler, D. Last chance to stop acid think on risks of xenotransplants. Nature. 1998, 391, 320–324. [Google Scholar] [CrossRef] [PubMed]
- Bhojani-Lynch, T. Late-Onset Inflammatory Response to Hyaluronic Acid Dermal Fillers. Plast. Reconstr. Surg. Glob. Open. 2017, 5, e1532. [Google Scholar] [CrossRef] [PubMed]
- Han, S.W.; Park, M.J.; Lee, S.H. Hyaluronic acid-induced diffuse alveolar hemorrhage: unknown complication induced by a well-known injectable agent. Ann Transl Med, 2019, 7, 13. [Google Scholar] [CrossRef]
- Mullins, R.J.; Richards, C.; Walker, T. Allergic reactions to oral, surgical and topical bovine collagen. Anaphylactic risk for surgeons. Aust. N. Z. J. Ophthalmol. 1996, 24, 257–60. [Google Scholar] [CrossRef] [PubMed]
- Saito, N.; Okada, T.; Horiuchi, H.; Murakami, N.; Takahashi, J.; Nawata, M.; Ota, H.; Nozaki, K.; Takaoka, K. A biodegradable polymer as a cytokine delivery system for inducing bone formation. Nat. Biotechnol. 2001, 19, 332–335. [Google Scholar] [CrossRef] [PubMed]
- Aoki, K.; Haniu, H.; Kim, Y.A.; Saito, N. The Use of Electrospun Organic and Carbon Nanofibers in Bone Regeneration. Nanomaterials (Basel). 2020, 10. [Google Scholar] [CrossRef]
- Zhang, S.; Chen, L.; Jiang, Y.; Cai, Y.; Xu, G.; Tong, T.; Zhang, W.; Wang, L.; Ji, J.; Shi, P.; Ouyang, H.W. Bi-layer collagen/microporous electrospun nanofiber scaffold improves the osteochondral regeneration. Acta Biomater. 2013, 9, 7236–47. [Google Scholar] [CrossRef]
- van den Borne, M.P.; Raijmakers, N.J.; Vanlauwe, J.; Victor, J.; de Jong, S.N.; Bellemans, J.; Saris, D.B.; International Cartilage Repair Society. International Cartilage Repair Society (ICRS) and Oswestry macroscopic cartilage evaluation scores validated for use in Autologous Chondrocyte Implantation (ACI) and microfracture. Osteoarthritis Cartilage. 2007, 15, 1397–402. [Google Scholar] [CrossRef]
- Song, Z.; Zhu, W.; Song, J.; Wei, P.; Yang, F.; Liu, N.; Feng, R. Linear-dendrimer type methoxy-poly (ethylene glycol)-b-poly (epsilon-caprolactone) copolymer micelles for the delivery of curcumin. Drug Deliv. 2015, 22, 58–68. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Yang, Z. Short-peptide-based molecular hydrogels: novel gelation strategies and applications for tissue engineering and drug delivery. Nanoscale. 2012, 4, 5259–5267. [Google Scholar] [CrossRef]
- Wang, Y.; Cui, W.; Chou, J.; Wen, S.; Sun, Y.; Zhang, H. Electrospun nanosilicates-based organic/inorganic nanofibers for potential bone tissue engineering. Colloids Surf. B Biointerfaces. 2018, 172, 90–97. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Li, Y.; Liu, X.; Huang, Q.; Zhang, R.; Feng, Q. Incorporation of silica nanoparticles to PLGA electrospun fibers for osteogenic differentiation of human osteoblast-like cells. Regen Biomater. 2018, 5, 229–238. [Google Scholar] [CrossRef]
- Timofejeva, A.; D'Este, M.; Loca, D. Calcium phosphate/polyvinyl alcohol composite hydrogels: A review on the freeze-thawing synthesis approach and applications in regenerative medicine. Eur. Polym. J. 2017, 95, 547–565. [Google Scholar] [CrossRef]
- Enayati, M.S.; Behzad, T.; Sajkiewicz, P.; Rafienia, M.; Bagheri, R.; Ghasemi-Mobarakeh, L.; Kolbuk, D.; Pahlevanneshan, Z.; Bonakdar, S.H. Development of electrospun poly (vinyl alcohol)-based bionanocomposite scaffolds for bone tissue engineering. J. Biomed. Mater. Res. A. 2018, 106, 1111–1120. [Google Scholar] [CrossRef]
- Gonzalez, J.S.; Alvarez, V.A. Mechanical properties of polyvinylalcohol/hydroxyapatite cryogel as potential artificial cartilage. J. Mech. Behav. Biomed. Mater. 2014, 34, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Hokugo, A.; Ozeki, M.; Kawakami, O.; Sugimoto, K.; Mushimoto, K.; Morita, S.; Tabata, Y. Augmented bone regeneration activity of platelet-rich plasma by biodegradable gelatin hydrogel. Tissue Eng. 2005, 11, 1224–1233. [Google Scholar] [CrossRef] [PubMed]
- Re, F.; Sartore, L.; Moulisova, V.; Cantini, M.; Almici, C.; Bianchetti, A.; Chinello, C.; Dey, K.; Agnelli, S.; Manferdini, C.; Bernardi, S.; Lopomo, N.F.; Sardini, E.; Borsani, E.; Rodella, L.F.; Savoldi, F.; Paganelli, C.; Guizzi, P.; Lisignoli, G.; Magni, F.; Salmeron-Sanchez, M.; Russo, D. 3D gelatin-chitosan hybrid hydrogels combined with human platelet lysate highly support human mesenchymal stem cell proliferation and osteogenic differentiation. J. Tissue Eng. 2019, 10, 2041731419845852. [Google Scholar] [CrossRef]
- Takeda, Y.; Tsujigiwa, H.; Nagatsuka, H.; Nagai, N.; Yoshinobu, J.; Okano, M.; Fukushima, K.; Takeuchi, A.; Yoshino, T.; Nishizaki, K. Regeneration of rat auditory ossicles using recombinant human BMP-2/collagen composites. J. Biomed. Mater. Res. A. 2005, 73, 133–41. [Google Scholar] [CrossRef]
- Takahashi, Y.; Yamamoto, M.; Tabata, Y. Osteogenic differentiation of mesenchymal stem cells in biodegradable sponges composed of gelatin and beta-tricalcium phosphate. Biomaterials. 2005, 26, 3587–3596. [Google Scholar] [CrossRef] [PubMed]
- Reneker, D.H.; Chun, I. Nanometre diameter fibres of polymer, produced by electrospinning. Nanotechnology. 1996, 7, 216–223. [Google Scholar] [CrossRef]
- Lee, H.; Yeo, M.; Ahn, S.; Kang, D.O.; Jang, C.H.; Lee, H.; Park, G.M.; Kim, G.H. Designed hybrid scaffolds consisting of polycaprolactone microstrands and electrospun collagen-nanofibers for bone tissue regeneration. J. Biomed. Mater. Res. B Appl. Biomater. 2011, 97, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Wang, C.; Fu, L.; Ye, S.; Wang, M.; Zhou, Y. Fabrication and Application of Novel Porous Scaffold in Situ-Loaded Graphene Oxide and Osteogenic Peptide by Cryogenic 3D Printing for Repairing Critical-Sized Bone Defect. Molecules. 2019, 24, 1669. [Google Scholar] [CrossRef] [PubMed]
- Deng, N.; Sun, J.; Li, Y.; Chen, L.; Chen, C.; Wu, Y.; Wang, Z.; Li, L. Experimental study of rhBMP-2 chitosan nano-sustained release carrier-loaded PLGA/nHA scaffolds to construct mandibular tissue-engineered bone. Arch. Oral. Biol. 2019, 102, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Das, A.; Fishero, B.A.; Christophel, J.J.; Li, C.J.; Kohli, N.; Lin, Y.; Dighe, A.S.; Cui, Q. Poly(lactic-co-glycolide) polymer constructs cross-linked with human BMP-6 and VEGF protein significantly enhance rat mandible defect repair. Cell and Tissue Research,. [CrossRef]
- Berner, A.; Boerckel, J.D.; Saifzadeh, S.; Steck, R.; Ren, J.; Vaquette, C.; Zhang, J.Q.; Nerlich, M.; Guldberg, R.E.; Hutmacher, D.W.; Woodruff, M.A. Biomimetic tubular nanofiber mesh and platelet rich plasma-mediated delivery of BMP-7 for large bone defect regeneration. Cell Tissue Res. 2012, 347, 603–612. [Google Scholar] [CrossRef] [PubMed]
- Asatrian, G.; Pham, D.; Hardy, W.R.; James, A.W.; Peault, B. Stem cell technology for bone regeneration: current status and potential applications. Stem Cells Cloning. 2015, 8, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.Z.; Lee, J.H. Mesenchymal Stem Cell Therapy for Bone Regeneration. Clin. Orthop. Surg. 2018, 10, 271–278. [Google Scholar] [CrossRef]
- Del Rosario, C.; Rodriguez-Evora, M.; Reyes, R.; Delgado, A.; Evora, C. BMP-2, PDGF-BB, and bone marrow mesenchymal cells in a macroporous beta-TCP scaffold for critical-size bone defect repair in rats. Biomed. Mater. 2015, 10, 045008. [Google Scholar] [CrossRef]
- Roussy, Y.; Bertrand Duchesne, M.P.; Gagnon, G. Activation of human platelet-rich plasmas: effect on growth factors release, cell division and in vivo bone formation. Clin. Oral Implants Res. 2007, 18, 639–648. [Google Scholar] [CrossRef]
- Cheng, G.; Ma, X.; Li, J.; Cheng, Y.; Cao, Y.; Wang, Z.; Shi, X.; Du, Y.; Deng, H.; Li, Z. Incorporating platelet-rich plasma into coaxial electrospun nanofibers for bone tissue engineering. Int J Pharm. 2018, 547, 656–666. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Synthetic bone made of hydroxyapatite (HA). (a) Photograph of synthetic bone made of HA. There are block-shaped, cylindrical, and granular products, which are used according to the size and shape of the bone defect. (b) Scanning electron microscopy (SEM) image of synthetic bone made of HA. The synthetic bone forms a porous body with micrometer-sized pores. Images are modified from a study by Yoshikawa et al. Reproduced with permission from The Royal Society, 2008 [37]. (c) Photograph of synthetic bone made of a HA/collagen composite (left). The synthetic bone becomes soft when it contains water. Images are modified from a study by Sotome et al [12].
Figure 1.
Synthetic bone made of hydroxyapatite (HA). (a) Photograph of synthetic bone made of HA. There are block-shaped, cylindrical, and granular products, which are used according to the size and shape of the bone defect. (b) Scanning electron microscopy (SEM) image of synthetic bone made of HA. The synthetic bone forms a porous body with micrometer-sized pores. Images are modified from a study by Yoshikawa et al. Reproduced with permission from The Royal Society, 2008 [37]. (c) Photograph of synthetic bone made of a HA/collagen composite (left). The synthetic bone becomes soft when it contains water. Images are modified from a study by Sotome et al [12].
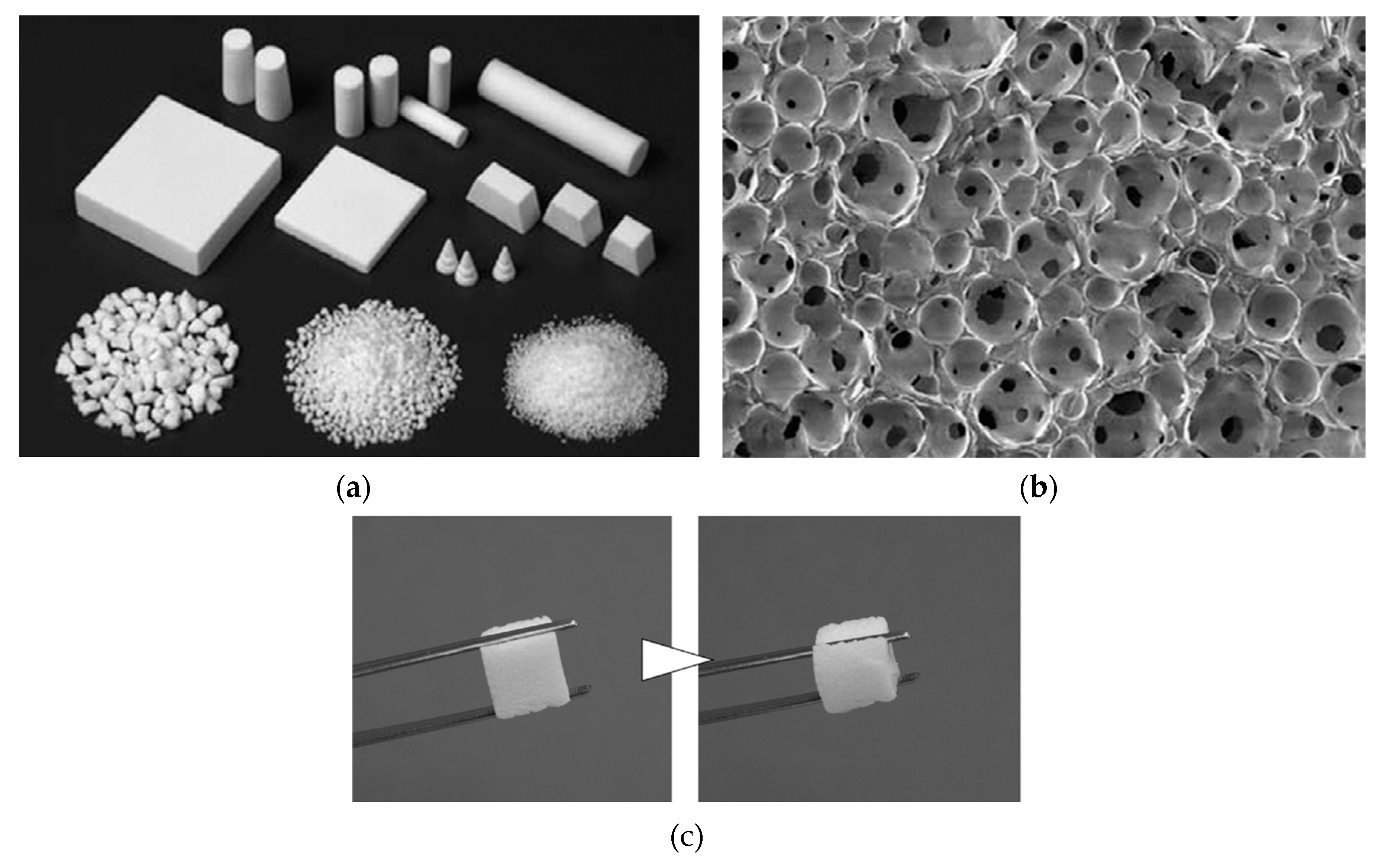
Figure 2.
A case with a tibial aneurysmal bone cyst (ABC). (a) Preoperative plain radiography image. Radiotransparency is observed from the epiphysis to the epiphysis of the tibia. There is a pathological fracture at the tumor site, and the fixation is performed with a cast. (b) Intraoperative photograph following tumor curettage. After curettage of the tumor, autologous iliac bone is grafted just below the articular surface, and most of the remaining space is filled with synthetic bone made of βTCP and reinforced with plates and screws. (c) Plain radiography immediately after surgery. It is observed that the bone defect where the tumor curettage was performed is filled with block-shaped and granular synthetic bones. (d) Plain radiography at 5 years after surgery. The autologous iliac graft just below the articular surface shows bony union. The synthetic bone has been replaced with autologous bone, but some of the large block-shaped synthetic bone remains. No tumor recurrence is observed.
Figure 2.
A case with a tibial aneurysmal bone cyst (ABC). (a) Preoperative plain radiography image. Radiotransparency is observed from the epiphysis to the epiphysis of the tibia. There is a pathological fracture at the tumor site, and the fixation is performed with a cast. (b) Intraoperative photograph following tumor curettage. After curettage of the tumor, autologous iliac bone is grafted just below the articular surface, and most of the remaining space is filled with synthetic bone made of βTCP and reinforced with plates and screws. (c) Plain radiography immediately after surgery. It is observed that the bone defect where the tumor curettage was performed is filled with block-shaped and granular synthetic bones. (d) Plain radiography at 5 years after surgery. The autologous iliac graft just below the articular surface shows bony union. The synthetic bone has been replaced with autologous bone, but some of the large block-shaped synthetic bone remains. No tumor recurrence is observed.
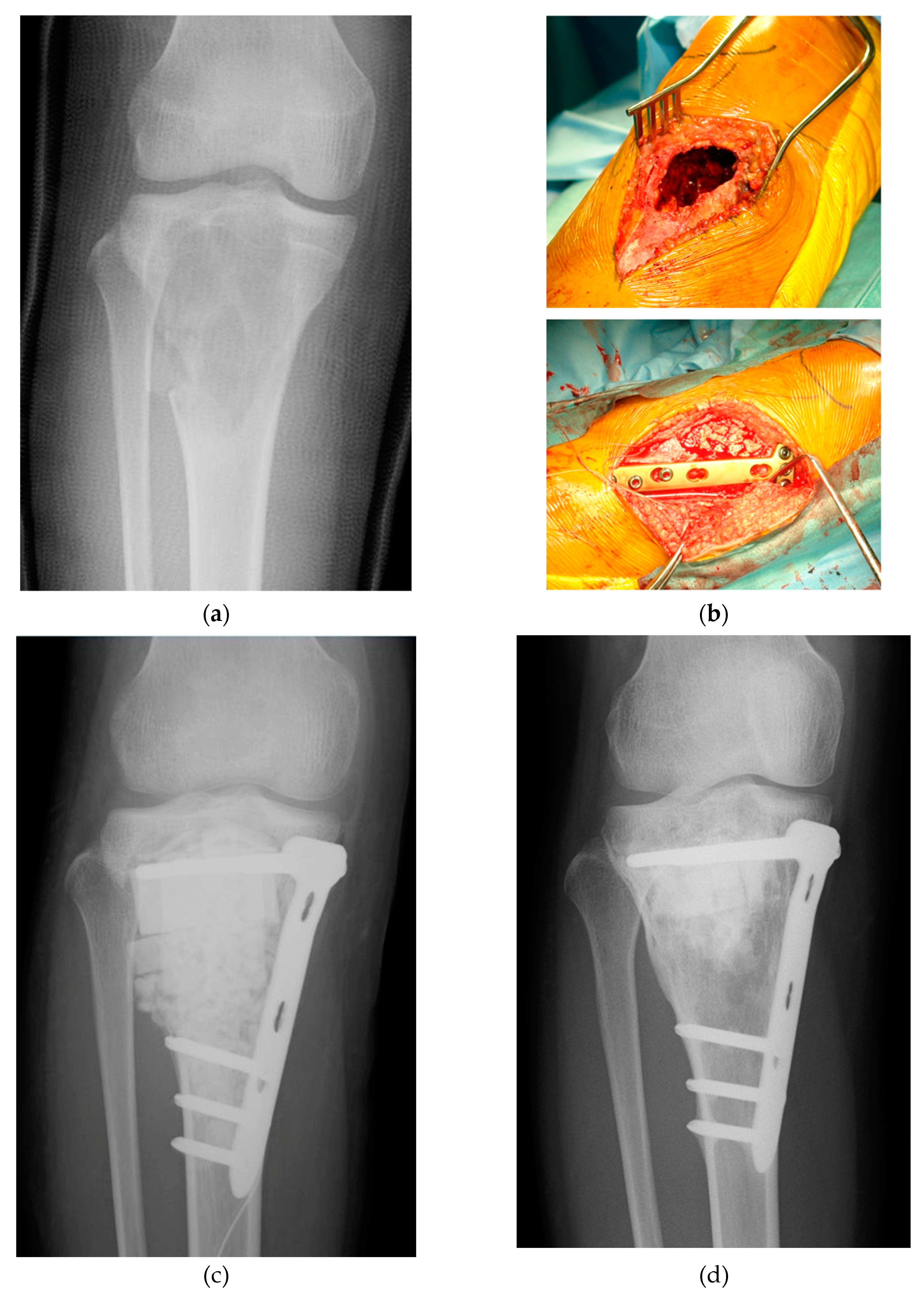
Figure 3.
A case of ABC of the humerus. (a) A diagnosis of a simple bone cyst was made by a previous doctor, and decompression was performed with a cannulated screw made of hydroxyapatite, but the tumor did not shrink and a radiotransparency was observed. (b) The tumor was curattaged at our hospital and filled with granular βTCP synthetic bone. (c) Plain radiography at 1 year after synthetic bone filled by βTCP. The synthetic bone has been resorbed and the tumor has recurred. (d) CT image at the time of tumor recurrence. Two recurrent tumors are found at the metaphysis and at the diaphysis. (e) Plain radiography after reoperation at our hospital. After tumor curettage, the synthetic bone made of the collagen/HA composite was filled. The synthetic bone made of the collagen-HA composite has high radiotransparency and is less visible compared to the βTCP synthetic bone. (f) Plain radiography at 1 year after reoperation. The autologous bone is regenerating. (g) Plain radiography at 5 years after reoperation. No recurrence is observed. (h) CT image at 5 years after reoperation. A shadow of regenerated cancellous bone is observed at the site where there was a bone defect due to the tumor. Deformity remains at the metaphyseal end of the humerus.
Figure 3.
A case of ABC of the humerus. (a) A diagnosis of a simple bone cyst was made by a previous doctor, and decompression was performed with a cannulated screw made of hydroxyapatite, but the tumor did not shrink and a radiotransparency was observed. (b) The tumor was curattaged at our hospital and filled with granular βTCP synthetic bone. (c) Plain radiography at 1 year after synthetic bone filled by βTCP. The synthetic bone has been resorbed and the tumor has recurred. (d) CT image at the time of tumor recurrence. Two recurrent tumors are found at the metaphysis and at the diaphysis. (e) Plain radiography after reoperation at our hospital. After tumor curettage, the synthetic bone made of the collagen/HA composite was filled. The synthetic bone made of the collagen-HA composite has high radiotransparency and is less visible compared to the βTCP synthetic bone. (f) Plain radiography at 1 year after reoperation. The autologous bone is regenerating. (g) Plain radiography at 5 years after reoperation. No recurrence is observed. (h) CT image at 5 years after reoperation. A shadow of regenerated cancellous bone is observed at the site where there was a bone defect due to the tumor. Deformity remains at the metaphyseal end of the humerus.
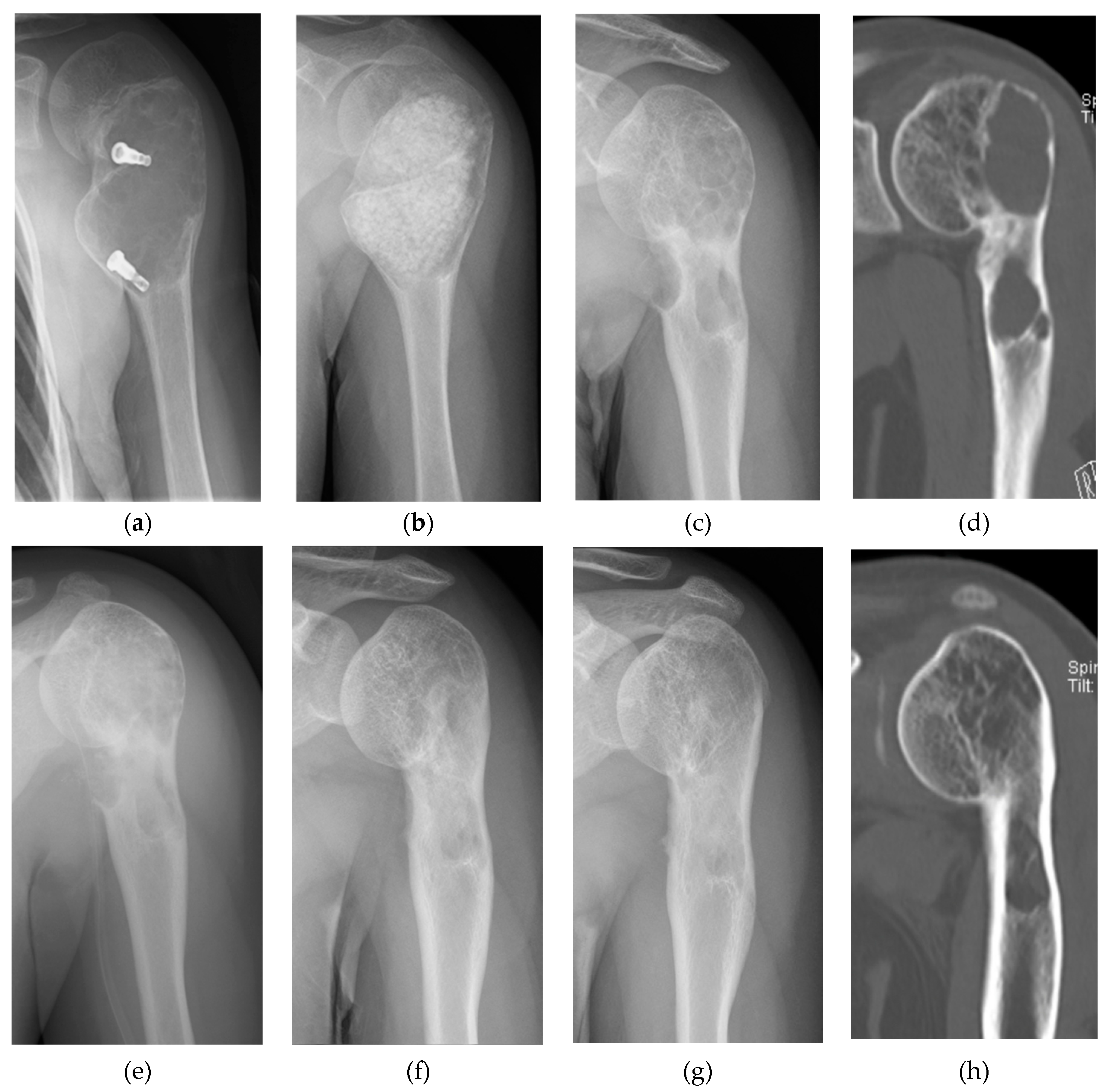
Figure 4.
A case with chondromyxoid fibroma. (a) Preoperative plain radiography. A bone defect has occurred at the tumor site proximal to the lateral tibia. (b) Preoperative CT image. Due to the tumor, bone defects including the outer cortical bone are observed. (c) Preoperative 3D-CT image. Bone defects at the tumor site are observed as depressions. (d) Simple X-ray image immediately after the 1st stage operation by induced membrane technique. The bone defect is filled with bone cement. (e) CT image immediately after the 1st stage operation. (f) Six weeks after the first surgery, the second surgery is performed. Plain radiography after second surgery. Bone cement is removed and filled with a mixture of granular βTCP synthetic bone and autologous iliac cancellous bone. (g) Plain radiography at 3 years after surgery. Resorption of synthetic bone is progressing, and autologous bone is being regenerated. (h) CT image at 3 years after surgery. Autologous bone, including the cortical bone, is regenerating. Some synthetic bone remains inside.
Figure 4.
A case with chondromyxoid fibroma. (a) Preoperative plain radiography. A bone defect has occurred at the tumor site proximal to the lateral tibia. (b) Preoperative CT image. Due to the tumor, bone defects including the outer cortical bone are observed. (c) Preoperative 3D-CT image. Bone defects at the tumor site are observed as depressions. (d) Simple X-ray image immediately after the 1st stage operation by induced membrane technique. The bone defect is filled with bone cement. (e) CT image immediately after the 1st stage operation. (f) Six weeks after the first surgery, the second surgery is performed. Plain radiography after second surgery. Bone cement is removed and filled with a mixture of granular βTCP synthetic bone and autologous iliac cancellous bone. (g) Plain radiography at 3 years after surgery. Resorption of synthetic bone is progressing, and autologous bone is being regenerated. (h) CT image at 3 years after surgery. Autologous bone, including the cortical bone, is regenerating. Some synthetic bone remains inside.
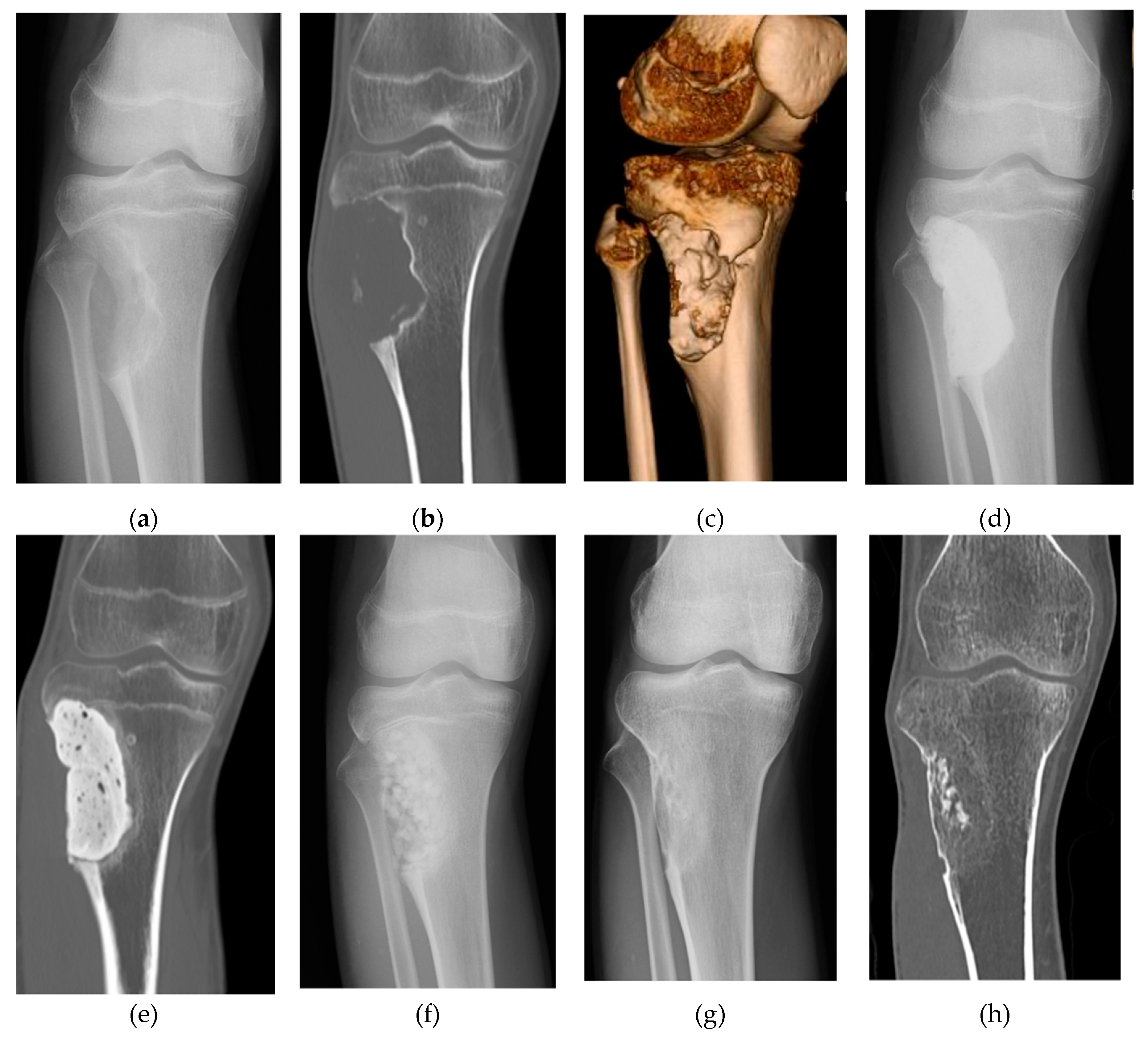
Figure 5.
(a) Structural formula of polylactic acid-p-dioxanone-polyethylene glycol block copolymer (PLA-DX-PEG). (b) Photograph of PLA-DX-PEG hydrogel. (c) Ectopic bone formed under the dorsal fascia of mice by adding rhBMP-2 to the PLA-DX-PEG scaffold. (d) Dissolution curve of PLA-DX-PEG polymer. The polymer was immersed in PBS at 37 °C and weighed. The weight was gradually reduced over 10 days and completely dissolved within 20 days. Images are modified from a study by Saito et al. [68]. (e) rhBMP-2 was added to the PLA-DX-PEG scaffold to treat a critical-sized bone defect in the rabbit ulna. Approximately 3 months after the operation, the bone defect was repaired. Images are modified from a study by Aoki et al. [69].
Figure 5.
(a) Structural formula of polylactic acid-p-dioxanone-polyethylene glycol block copolymer (PLA-DX-PEG). (b) Photograph of PLA-DX-PEG hydrogel. (c) Ectopic bone formed under the dorsal fascia of mice by adding rhBMP-2 to the PLA-DX-PEG scaffold. (d) Dissolution curve of PLA-DX-PEG polymer. The polymer was immersed in PBS at 37 °C and weighed. The weight was gradually reduced over 10 days and completely dissolved within 20 days. Images are modified from a study by Saito et al. [68]. (e) rhBMP-2 was added to the PLA-DX-PEG scaffold to treat a critical-sized bone defect in the rabbit ulna. Approximately 3 months after the operation, the bone defect was repaired. Images are modified from a study by Aoki et al. [69].
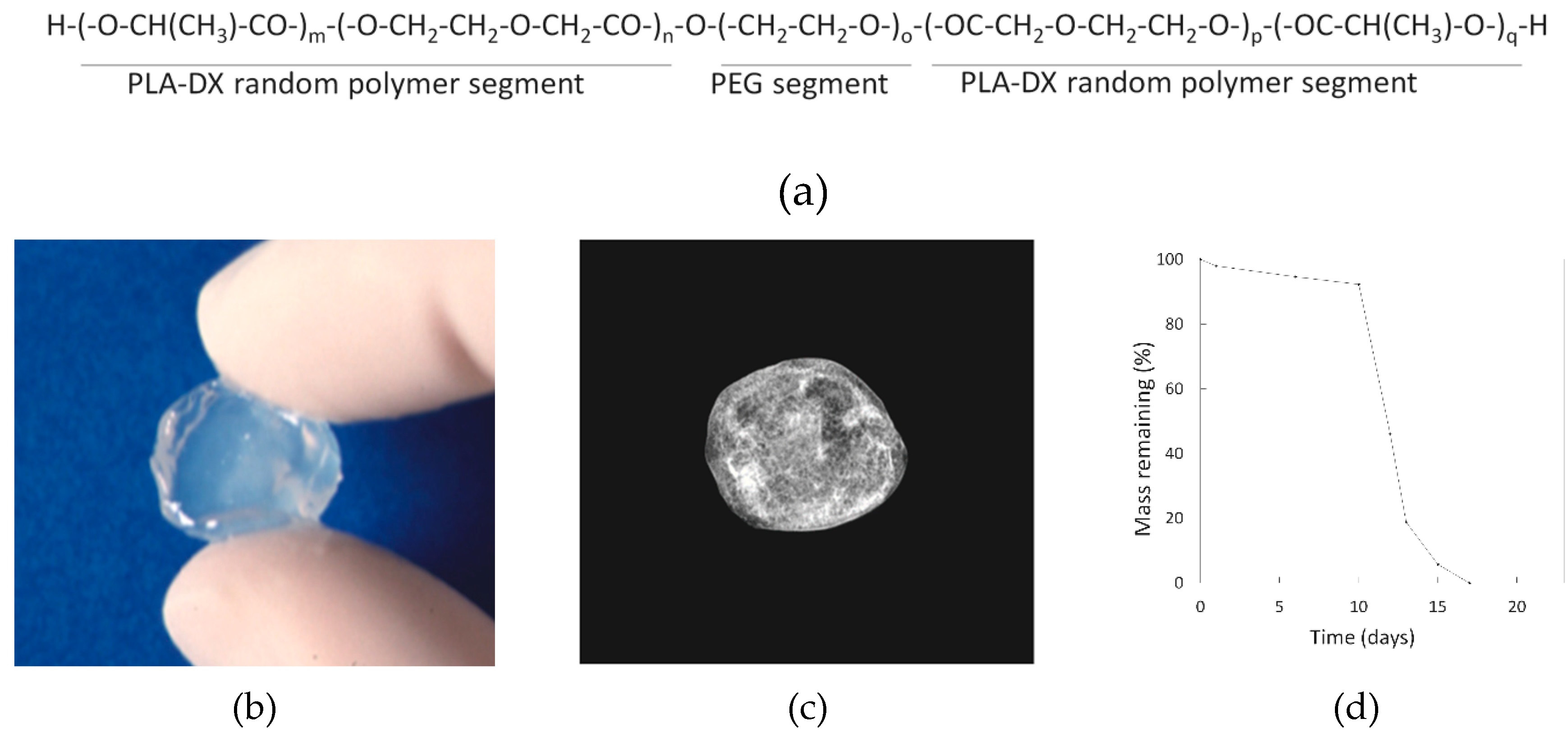
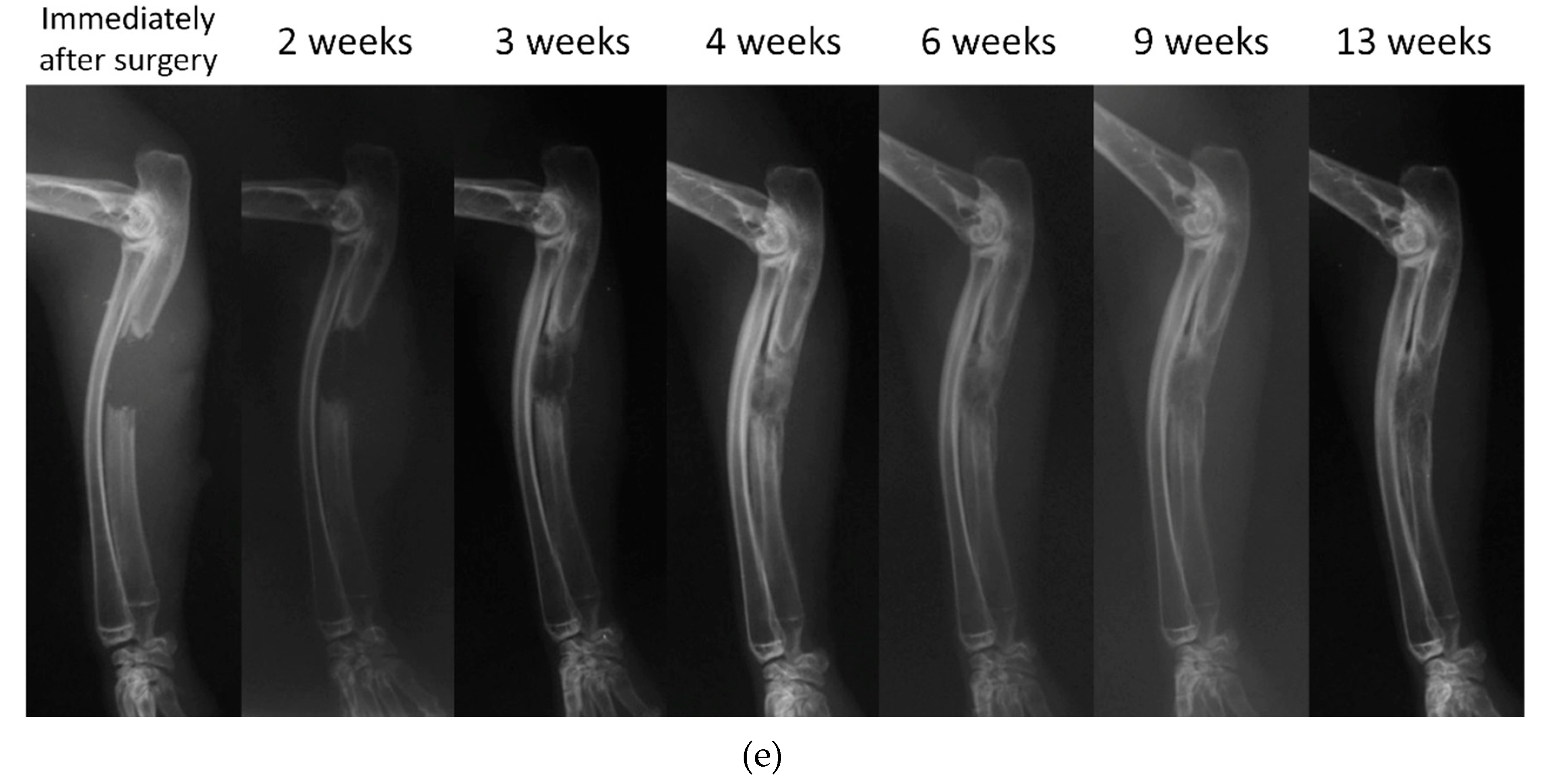
Figure 6.
Three-dimensional structure of biodegradable polymer: (a) Scanning electron microscopy (SEM) image of a scaffold prepared by freeze-drying Type I collagen; (b) SEM image of a gelatin/β-TCP composite scaffold. Image is modified from a study by Takahashi et al. Reproduced with permission from Elsevier, 2005 [82]; (c) SEM image of a PVA/HA composite scaffold created by the electrospinning method. Image is modified from a study by Enayati et al. Reproduced with permission from John Wiley and Sons, 2018 [77]; (d) Photograph of a PLGA/βTCP/GO (PTG) composite scaffold created by 3D-printing; (e) SEM image of a PTG composite scaffold. Images are modified from a study by Zhang et al. [85].
Figure 6.
Three-dimensional structure of biodegradable polymer: (a) Scanning electron microscopy (SEM) image of a scaffold prepared by freeze-drying Type I collagen; (b) SEM image of a gelatin/β-TCP composite scaffold. Image is modified from a study by Takahashi et al. Reproduced with permission from Elsevier, 2005 [82]; (c) SEM image of a PVA/HA composite scaffold created by the electrospinning method. Image is modified from a study by Enayati et al. Reproduced with permission from John Wiley and Sons, 2018 [77]; (d) Photograph of a PLGA/βTCP/GO (PTG) composite scaffold created by 3D-printing; (e) SEM image of a PTG composite scaffold. Images are modified from a study by Zhang et al. [85].
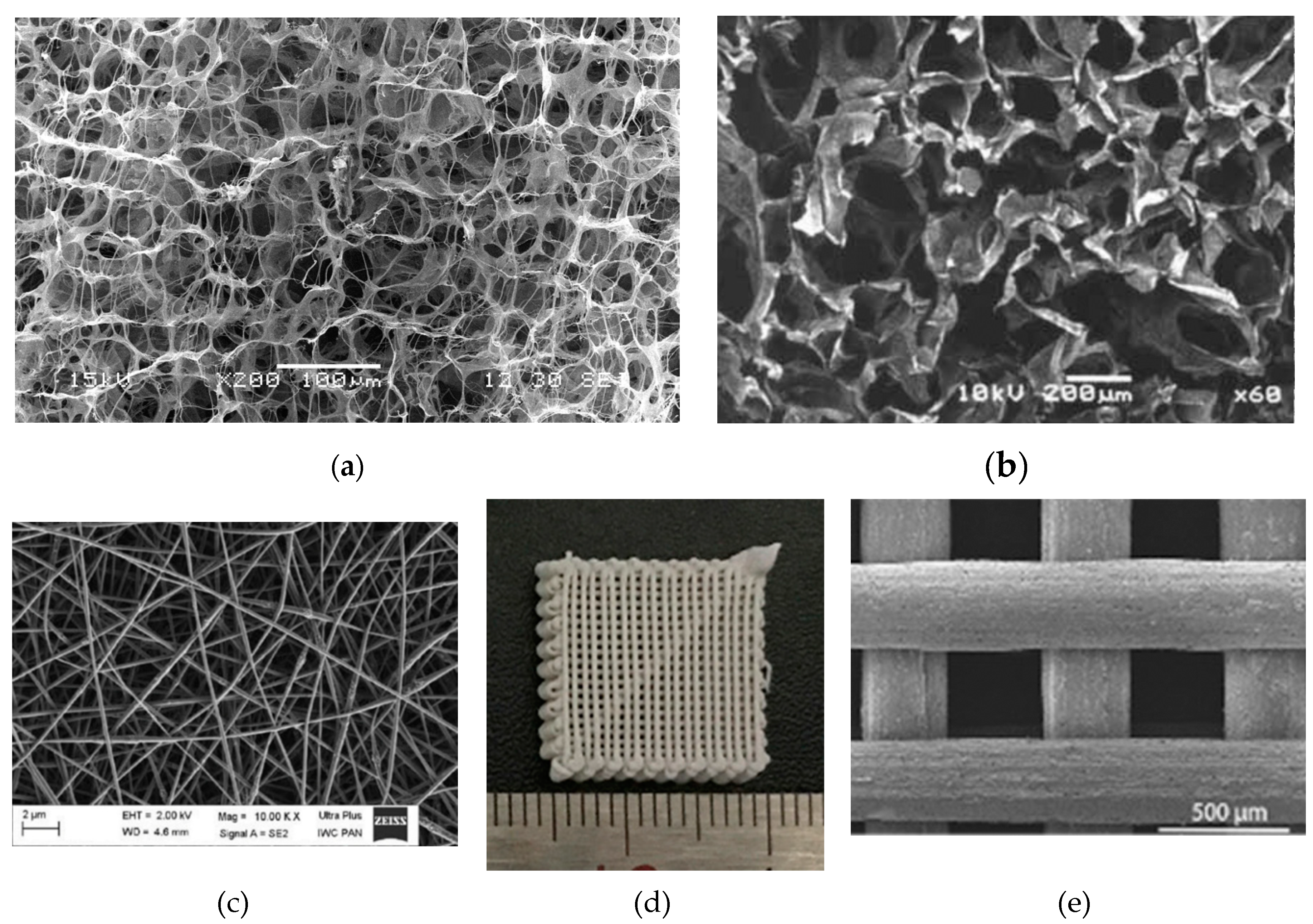
Figure 7.
Factors that affect the performance of biodegradable scaffolds.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



