
Submitted:
03 January 2024
Posted:
04 January 2024
You are already at the latest version
Abstract
Background: A decline in the prevalence of Helicobacter pylori infection has been claimed to increase the probability of developing atopic diseases. Aims: To evaluate the prevalence of atopic disorders in a pediatric population according to seropositivity against H. pylori. Methods: Children referred to the local Pediatric Hospital were investigated to identify risk factors, especially H. pylori infection, associated with atopic disorders. A questionnaire, including demographics, house size, history of breastfeeding, residence, school or daycare center attendance, exposure to animals, and a diagnosis of atopy, was filled out by a trained pediatrician according to parents’ answers. A blood sample was collected from each participant. Results: Seroprevalence of H. pylori infection was 11.7% among 492 children (240 females); 32 of them had a diagnosis of asthma and 12 of allergy. No one child showed both conditions. Statistically significant differences in H. pylori seropositivity were not detected between children with or without atopy (8.4 vs. 12.6; p=0.233). Although atopic disorders were more frequent in children exposed to traditional risk factors none showed to be significant after adjusting for all covariates. Conclusions: H. pylori infection, serologically assessed, was not significantly associated with a reduced risk of atopic diseases in children.
Keywords:
asthma
; allergy
; atopy
; Helicobacter pylori
; inflammation
1. Introduction
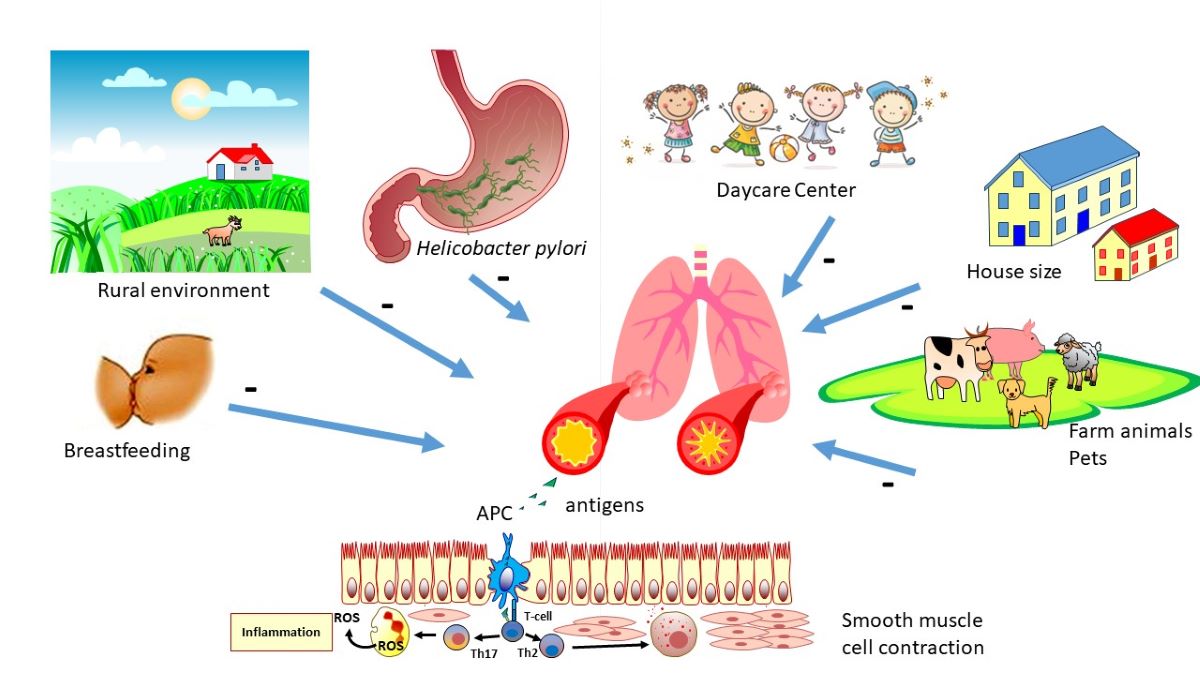
The term “hygiene hypothesis”, postulated back in 1989 by David Strachan [1], refers to the observation that exposure to a reduced quantity of microbes in the excessively hygienic environments of modern times may raise the risk of developing atopic diseases including asthma. Although the original version of the hypothesis has been subject to serious criticism [2,3], more or less modified versions of it are still supported by some epidemiologists and considered capable of explaining peculiar aspects observed, especially in developing societies [4,5]. Although the precise mechanisms underpinning the ability of the microbic infection to protect against immune-mediated diseases have not yet been clearly elucidated, it is usually assumed that early exposure to microorganisms naturally colonizing an unsanitary environment might induce a maturation of the human immune system, making it resistant to the loss of immune tolerance later in life, thus triggering atopic, or more generally, immune-mediated diseases [6]. The role of specific environmental bacterial or parasitic species in the development of immune tolerance has been widely debated in the literature, and it is believed that it may extend to cover soil-transmitted helminthic [7,8], fungal [9] and even viral infections [10].
Among the various microorganisms, the bacterial load of which has progressively decreased in the environment due to the improved hygienic conditions, and whose infection has been advocated to explain the rise in allergic diseases, there is also the microaerophile Helicobacter pylori able to colonize the gastric mucosa [11,12,13,14,15,16,17]. The spread of this microorganism mainly occurs in environments characterized by poor hygienic conditions, such as those present in developing countries and in rural regions [18]. In such circumstances, children are infected at an early age, whereby their innate immune system is shunted in a way that maintains immune tolerance. If not pharmacologically eradicated, the infection persists for life in the stomach, owing to the establishment of a peculiar host-bacterial relationship based on a blunting of the host immune reaction, which becomes less efficient in clearing the invader. For this reason, it has been conjectured that the rapid improvement of the hygienic and sanitation conditions of several populations in the past decades may have drastically reduced the prevalence of H. pylori infection and, at least partially, decreased the alleged protection of the infection itself against immune-mediated diseases [1,19]. This hypothesis has been tested in numerous epidemiological studies, however, with conflicting results. Some studies found a significant protective effect [20,21,22,23,24] while a few others did not provide any evidence of such an effect [25,26]. Overall, the meta-analysis by Lionetti et al. in 2014 concluded that the weight of evidence is in favor of a protective effect [14]. Yet, in light of the criticisms recently addressed to the hygiene hypothesis in general, and the fact that the H. pylori-host relationship is not entirely coincident with that of other commensal microorganisms, a re-examination of the issue with the contribution of new data seems warranted.
Based on these premises, we aimed to evaluate the impact of H. pylori infection, assessed by serology, on the prevalence of atopic diseases in a cohort of children from Northern Sardinia, Italy.
2. Materials and Methods
2.1. Study design
Consecutive children referred for a visit to the Children's Hospital (University of Sassari, Italy) for any reason were screened for H. pylori infection by serology. A validated questionnaire [27] was completed by the pediatrician for each child in collaboration with their parents. The questionnaire was designed to collect information regarding age, sex, place of residence, number of persons living in the household, home size, history of breastfeeding, and attendance at daycare centers or school. In addition, data regarding exposure to animals, more specifically pets (dogs, cats, and parrots) or farm animals (pigs, goats, horses, ducks, donkeys, and chickens), were collected. At the enrollment, a sample of venous blood was collected, and the separated serum was stored at -20° C until processed. The main reason for an eligible child to be excluded from the study was the denial by the parents to give the informed consent.
2.2. H. pylori status
H. pylori status was assessed by using an ELISA test, as previously reported [28]. The test possesses a high specificity and positive and negative predictive value and was validated in children from the same geographic area. IgG titer above 0.21 was considered positive.
2.3. Allergy and Asthma
For the purpose of the study, information on the presence of asthma or allergic disease was recorded according to the parents’ interview and double-checked by matching the treatment (antihistamine drugs, corticosteroids, β2-agonists).
2.4. Ethical considerations
Children were enrolled in the study after informed consent was obtained from their parents. The study protocol was approved by the Ethics Committee of the Faculty of Medicine at the University of Sassari (Sassari, Italy).
2.5. Statistical analysis
Continuous variables were expressed as the mean ± SD, while categorical variables were presented as the absolute and percent frequencies. An urban area was defined as a population center with more than 20,000 inhabitants, according to the local environmental administration. The house size was categorized according to the threshold of 100 m². Breastfeeding was stratified based on its duration reported by the mother, i.e., less than 6 months, between 6 and 11 months, and greater than or equal to 12 months. The ownership of animals took into account the distinction between pets and farm animals. School and daycare center attendance were considered separately. Body weight was divided into normal or reduced based on comparison with growth percentiles. A multivariable regression model was fitted, using atopic disease occurrence as a dependent variable and H. pylori status as an independent variable, adjusting for age, sex, residence, house size, breastfeeding, body weight, and animal ownership as covariates. The Hosmer-Lemeshow goodness-of-fit test was used to evaluate whether the regression assumptions were satisfied. Data were analyzed by the SPSS statistical software package version 20.0 (Chicago, IL, USA). Statistical significance was taken as p < 0.05.
3. Results
Characteristics of children participating in the study are illustrated in Table 1. Overall, a total of 492 children were recruited, aged from 7 months to ≥37 months, and 48.8% were female. Among the overall cohort, the seroprevalence of H. pylori was 11.8%, without any significant difference in the two sexes (9.2% vs. 14.3%). More specifically, the highest significant prevalence was detected among children older than 37 months (19.4%), living in rural areas (25.3%) and smaller houses (<100 mt2) (16.1%), breastfed for 6 to 11 months (26.7%), owners of animals, especially farms animals (33.3%) and attending daycare or school (15.3%). There were no significant differences in the body weight of the children with seropositivity for H. pylori infection compared with those without (Table 1). Among the studied children, atopic disorders, including asthma, were reported by their parents in 44 of them, corresponding to 8.9% of the total study cohort. Allergies were more common in children negative for H. pylori infection, according to serology, while the prevalence of asthma was slightly higher in seropositive children (12.5% vs. 87.5%) but without statistically significant difference (Table 1).
The Figure 1 reports the rates of atopic disorders according to the age ranges, showing that, especially asthma, occurred beyond 13 months of age. Although asthma has been reported to be more commonly present in individuals with other atopic diseases, such as atopic dermatitis and allergic rhinitis [29], no one studied participant displayed a double condition in our study (Table 1).
Table 2 listed the atopy rates in relation to the covariates included in the study. Although atopy was more frequent in oldest and male children living in urban areas, small houses, exposed to animals, and attending school, statistically significant differences were observed only for the oldest age and breastfeeding practice. More importantly, significant differences in the frequency of atopy between H. pylori seropositive and seronegative children were not observed.
After adjusting for all covariates (Table 3), not one traditional risk factor was found to be statistically associated with asthma or atopy, including H. pylori infection.
4. Discussion
The results obtained in this study do not either confirm an inverse or a positive relation between atopic disorders, including asthma and H. pylori infection in children. These findings are consistent with our previous study conducted in the same geographic area [30]. In children aged 10 months to six years, screened for H. pylori infection using IgG serology and followed up for the occurrence of asthma and or allergic disease for seven years. 17.2% developed asthma, according to the Global Initiative on Asthma (GINA) [31], before the age of five years. Among them, 85.9% were H. pylori negative and 14.1% Hp positive [30]. By multiple logistic regression analysis H. pylori infection did not result significantly associated with childhood asthma.
Interestingly, we observed an overall reduction in the prevalence of H. pylori infection compared to previously reported data in a cohort of school children (22% vs. 11.7%) [27]. A decline in H. pylori infection has been observed in the last decades across most high-resource countries [32]. However, it cannot be ruled out that the increased use of antibiotics in the pediatric age [33], for which Italy holds the record in Europe, and the ensuing accidental eradication of the bacterium have contributed, at least in part, to the reduction in prevalence.
The traditional risk factors implicated in the acquisition of H. pylori infection were also confirmed in this study. Previously, in the same geographic area, the prevalence of H. pylori infection in 2810 school children was significantly higher among children living in rural areas compared with those living in urban areas (OR 3.8; 95%CI 3.2–4.7), and the risk was even greater for children who had dogs (OR, 1.8; 95%CI, 1.3–2.6) [27]. Ownership of animals, especially farm animals, and crowding (living in small-sized apartments/houses) were confirmed as risk factors significantly associated with H. pylori seropositivity also in the present study. Attendance at daycare centers and breastfeeding did not show a lower association with seropositivity [27,34,35].
Asthma is a chronic inflammatory disease of the airways, characterized by obstruction of the bronchial tree caused by inflammation of the lower airways and its consequences, generally reversible. The condition is the result of complex interactions between multiple risk factors and genetic influences that vary according to age, sex, breastfeeding, residence, exposure to animals, and school attendance, among others. Asthma represents the most frequent chronic respiratory disease in childhood, with a general prevalence in Italy estimated at around 10% (https://www.salute.gov.it/), not different from the prevalence found in our cohort (8.9%) with a tendency to be higher after 18 months of age.
Although childhood asthma has been reported to predominate in male children for a number of reasons, overall explained by sexual dimorphism in lung physiology [36,37], in our study, a statistically significant difference was not detected between sexes. However, similarly to our findings, some studies concluded that there are no sex differences in asthma severity [38,39]. Breastfeeding was repeatedly reported as a protective factor against asthma by several researchers [40,41,42,43,44]. This is understandable; breastfeeding helps to prevent respiratory tract infections [41]. Furthermore, some oligosaccharides contained in human milk, involved in specific (secretory immunoglobulin A, immunoglobulin M, and G) and nonspecific immunity (lactoferrin) and glycolipids [42], are able to reduce the virulence of pathogens and to modulate the immune response, thus attenuating the damage to the bronchial tree [42]. In addition, evidence has indicated that breastfeeding may help protect lung function in individuals exposed to high levels of air pollution, including secondhand smoke [43,44], suggesting the role of human milk in lung development. According to the literature, a lower prevalence of asthma was also found in our breastfed children.
In agreement with our results, early exposure in life to pets and or farm animals has been reported to be protective against the development of asthma and allergic disease [45,46]. Based on the rationale of greater allergen exposure, in adjusted analyses, the risk of asthma and allergen sensitization were increased in children living in urban areas compared to children living in rural areas [47]. The authors were able to demonstrate that the composition of airway and gut microbiotas differed between children living in urban and rural areas and suggested that changes in the child microbiota associated with the urban environment may increase the risk of asthma and atopic disorders, probably via cross-talk with the developing immune system [47]. However, although age, female sex, urban residence, breastfeeding, animal ownership, and no school attendance showed an inverse association with asthma and atopic disorders, as expected, none of these risk factors showed to be statistically significant predictors after adjusting for all covariates. More importantly, H. pylori infection was not found to be significantly associated with pediatric asthma.
H. pylori infection is considered a proxy of poor hygiene condition, and it has been supposed that, in the past century, improvements in household amenities, higher standards of personal hygiene, and reduced family size have decreased the opportunity for cross-infection in young families, and exposure to different antigens favoring earlier expression of atopic disease. However, in countries such as Malaysia and Zanzibar, with poor hygiene conditions and a very low prevalence of H. pylori infection, an increase in childhood asthma was not observed [48,49,50,51]. Several reports confirm an increase in asthma and atopic disorders, especially in high-income countries [52]. According to that, some studies have reported a lower prevalence of H. pylori infection in asthmatic patients, confirmed by a meta-analysis including 106 articles for a total of 28,283 patients [53] (OR= 0.84, 95%CI: 0.73–0.96, P = 0.013). However, a subgroup analysis indicated a similar prevalence in the asthmatic group and the control group of CagA-positive H. pylori infection [53]. However, other studies have reported neutral results or even a positive association between infection and asthma [30,54]. These contrasting results may be attributed to the different H. pylori detection methods used in the studies.
Some molecular aspects of the H. pylori-host interaction may help explain our results. Unlike other microorganisms, the bacterium does not favor the proper maturation of the immune system but, on the contrary, induces a tolerogenic phenotype in the dendritic cells, able to facilitate the persistence of the infection [55]. These tolerogenic cells, through interleukin-10 release, could inhibit the development of effector T cells, thereby creating an imbalance that induces later the appearance of exaggerated responses in the host [56].
The present study has several limitations that deserve discussion. Most data were self-reported by parents who may have exaggerated the importance of some environmental factors. Given that the study was limited to a pediatric population in Northern Sardinia, it may in some way have limited the generalizability of the results obtained, and finally, the cross-sectional design made us unable to establish causality.
5. Conclusions
In conclusion, in our study, the H. pylori infection, assessed through serological tests, did not significantly reduce the risk of allergy and atopy in children, suggesting that this bacterium—unlike other microorganisms—does not protect against atopic diseases by altering the host immune response.
Author Contributions
Conceptualization, M.P.D.; methodology, G.M.P.; software, G.M.P.; validation, M.P.D, and G.M.P.; formal analysis, G.M.P.; investigation, G.M.; resources, M.P.D.; data curation, M.P.D.; writing—original draft preparation, M.P.D.; writing—review and editing, M.P.D., G.M., and G.M.P.; visualization, G.M.P.; supervision, M.P.D.; project administration, M.P.D.; funding acquisition, M.P.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the Faculty of Medicine at the University of Sassari (Sassari, Italy).
Informed Consent Statement
Informed consent was obtained from the legal tutors of all subjects involved in the study.
Data Availability Statement
Data supporting reported results can be available upon reasonable request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Strachan, D.P. Hay fever, hygiene, and household size. BMJ 1989, 299, 1259–1260. [Google Scholar] [CrossRef] [PubMed]
- Bloomfield, S.F.; Rook, G.A.; Scott, E.A.; Shanahan, F.; Stanwell-Smith, R.; Turner, P. Time to abandon the hygiene hypothesis: new perspectives on allergic disease, the human microbiome, infectious disease prevention and the role of targeted hygiene. Perspect Public Health 2016, 136, 213–224. [Google Scholar] [CrossRef] [PubMed]
- Bach, J.F. Revisiting the Hygiene Hypothesis in the Context of Autoimmunity. Front Immunol 2020, 11, 615192. [Google Scholar] [CrossRef]
- Guarner, F.; Bourdet-Sicard, R.; Brandtzaeg, P.; Gill, H.S.; McGuirk, P.; van Eden, W.; Versalovic, J.; Weinstock, J.V.; Rook, G.A. Mechanisms of disease: the hygiene hypothesis revisited. Nat Clin Pract Gastroenterol Hepatol 2006, 3, 275–284. [Google Scholar] [CrossRef] [PubMed]
- Caraballo, L. The tropics, helminth infections and hygiene hypotheses. Expert Rev Clin Immunol 2018, 14, 99–102. [Google Scholar] [CrossRef] [PubMed]
- Vercelli, D. Mechanisms of the hygiene hypothesis--molecular and otherwise. Curr Opin Immunol 2006, 18, 733–737. [Google Scholar] [CrossRef]
- Weinstock, J.V.; Elliott, D.E. Helminths and the IBD hygiene hypothesis. Inflamm Bowel Dis 2009, 15, 128–133. [Google Scholar] [CrossRef]
- Maizels, R.M.; Smits, H.H.; McSorley, H.J. Modulation of Host Immunity by Helminths: The Expanding Repertoire of Parasite Effector Molecules. Immunity 2018, 49, 801–818. [Google Scholar] [CrossRef]
- Panelli, S.; Epis, S.; Cococcioni, L.; Perini, M.; Paroni, M.; Bandi, C.; Drago, L.; Zuccotti, G.V. Inflammatory bowel diseases, the hygiene hypothesis and the other side of the microbiota: Parasites and fungi. Pharmacol Res 2020, 159, 104962. [Google Scholar] [CrossRef]
- Alvarez, C.S.; Aviles-Santa, M.L.; Freedman, N.D.; Perreira, K.M.; Garcia-Bedoya, O.; Kaplan, R.C.; Daviglus, M.L.; Graubard, B.I.; Talavera, G.A.; Thyagarajan, B.; et al. Associations of Helicobacter pylori and hepatitis A seropositivity with asthma in the Hispanic Community Health Study/Study of Latinos (HCHS/SOL): addressing the hygiene hypothesis. Allergy Asthma Clin Immunol 2021, 17, 120. [Google Scholar] [CrossRef]
- Pfefferle, P.I.; Kramer, A. Helicobacter pylori-infection status and childhood living conditions are associated with signs of allergic diseases in an occupational population. Eur J Epidemiol 2008, 23, 635–640. [Google Scholar] [CrossRef] [PubMed]
- Blaser, M.J.; Chen, Y.; Reibman, J. Does Helicobacter pylori protect against asthma and allergy? Gut 2008, 57, 561–567. [Google Scholar] [CrossRef] [PubMed]
- Arnold, I.C.; Dehzad, N.; Reuter, S.; Martin, H.; Becher, B.; Taube, C.; Muller, A. Helicobacter pylori infection prevents allergic asthma in mouse models through the induction of regulatory T cells. J Clin Invest 2011, 121, 3088–3093. [Google Scholar] [CrossRef] [PubMed]
- Lionetti, E.; Leonardi, S.; Lanzafame, A.; Garozzo, M.T.; Filippelli, M.; Tomarchio, S.; Ferrara, V.; Salpietro, C.; Pulvirenti, A.; Francavilla, R.; et al. Helicobacter pylori infection and atopic diseases: is there a relationship? A systematic review and meta-analysis. World J Gastroenterol 2014, 20, 17635–17647. [Google Scholar] [CrossRef] [PubMed]
- Daugule, I.; Karklina, D.; Remberga, S.; Rumba-Rozenfelde, I. Helicobacter pylori Infection and Risk Factors in Relation to Allergy in Children. Pediatr Gastroenterol Hepatol Nutr 2017, 20, 216–221. [Google Scholar] [CrossRef]
- Ness-Jensen, E.; Langhammer, A.; Hveem, K.; Lu, Y. Helicobacter pylori in relation to asthma and allergy modified by abdominal obesity: The HUNT study in Norway. World Allergy Organ J 2019, 12, 100035. [Google Scholar] [CrossRef]
- Zuo, Z.T.; Ma, Y.; Sun, Y.; Bai, C.Q.; Ling, C.H.; Yuan, F.L. The Protective Effects of Helicobacter pylori Infection on Allergic Asthma. Int Arch Allergy Immunol 2021, 182, 53–64. [Google Scholar] [CrossRef]
- Dore, M.P.; Bilotta, M.; Vaira, D.; Manca, A.; Massarelli, G.; Leandro, G.; Atzei, A.; Pisanu, G.; Graham, D.Y.; Realdi, G. High prevalence of Helicobacter pylori infection in shepherds. Dig Dis Sci 1999, 44, 1161–1164. [Google Scholar] [CrossRef] [PubMed]
- Palmas, C.; Gabriele, F.; Conchedda, M.; Bortoletti, G.; Ecca, A.R. Causality or coincidence: may the slow disappearance of helminths be responsible for the imbalances in immune control mechanisms? J Helminthol 2003, 77, 147–153. [Google Scholar] [CrossRef]
- Matricardi, P.M. 99th Dahlem conference on infection, inflammation and chronic inflammatory disorders: controversial aspects of the 'hygiene hypothesis'. Clin Exp Immunol 2010, 160, 98–105. [Google Scholar] [CrossRef]
- Shiotani, A.; Miyanishi, T.; Kamada, T.; Haruma, K. Helicobacter pylori infection and allergic diseases: epidemiological study in Japanese university students. J Gastroenterol Hepatol 2008, 23, e29–33. [Google Scholar] [CrossRef]
- Janson, C.; Asbjornsdottir, H.; Birgisdottir, A.; Sigurjonsdottir, R.B.; Gunnbjornsdottir, M.; Gislason, D.; Olafsson, I.; Cook, E.; Jogi, R.; Gislason, T.; et al. The effect of infectious burden on the prevalence of atopy and respiratory allergies in Iceland, Estonia, and Sweden. J Allergy Clin Immunol 2007, 120, 673–679. [Google Scholar] [CrossRef]
- Reibman, J.; Marmor, M.; Filner, J.; Fernandez-Beros, M.E.; Rogers, L.; Perez-Perez, G.I.; Blaser, M.J. Asthma is inversely associated with Helicobacter pylori status in an urban population. PLoS One 2008, 3, e4060. [Google Scholar] [CrossRef]
- Holster, I.L.; Vila, A.M.; Caudri, D.; den Hoed, C.M.; Perez-Perez, G.I.; Blaser, M.J.; de Jongste, J.C.; Kuipers, E.J. The impact of Helicobacter pylori on atopic disorders in childhood. Helicobacter 2012, 17, 232–237. [Google Scholar] [CrossRef]
- Bodner, C.; Anderson, W.J.; Reid, T.S.; Godden, D.J. Childhood exposure to infection and risk of adult onset wheeze and atopy. Thorax 2000, 55, 383–387. [Google Scholar] [CrossRef]
- Radon, K.; Windstetter, D.; Eckart, J.; Dressel, H.; Leitritz, L.; Reichert, J.; Schmid, M.; Praml, G.; Schosser, M.; von Mutius, E.; et al. Farming exposure in childhood, exposure to markers of infections and the development of atopy in rural subjects. Clin Exp Allergy 2004, 34, 1178–1183. [Google Scholar] [CrossRef]
- Dore, M.P.; Malaty, H.M.; Graham, D.Y.; Fanciulli, G.; Delitala, G.; Realdi, G. Risk Factors Associated with Helicobacter pylori Infection among Children in a Defined Geographic Area. Clin Infect Dis 2002, 35, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Dore, M.P.; Fanciulli, G.; Tomasi, P.A.; Realdi, G.; Delitala, G.; Graham, D.Y.; Malaty, H.M. Gastrointestinal symptoms and Helicobacter pylori infection in school-age children residing in Porto Torres, Sardinia, Italy. Helicobacter 2012, 17, 369–373. [Google Scholar] [CrossRef] [PubMed]
- Yaneva, M.; Darlenski, R. The link between atopic dermatitis and asthma- immunological imbalance and beyond. Asthma Res Pract 2021, 7, 16. [Google Scholar] [CrossRef] [PubMed]
- Dore, M.P.; Massidda, M.; Meloni, G.F.; Soro, S.; Pes, G.M.; Graham, D.Y. The Association of Childhood Asthma and Helicobacter pylori Infection in Sardinia. Archives of Pediatric Infectious Diseases 2014, 2. [Google Scholar] [CrossRef]
- Global Initiative for Asthma. Asthma management and prevention for adults and children older than 5 years. A pocket guide for health professionals. ; 2019.
- Yuan, C.; Adeloye, D.; Luk, T.T.; Huang, L.; He, Y.; Xu, Y.; Ye, X.; Yi, Q.; Song, P.; Rudan, I.; et al. The global prevalence of and factors associated with Helicobacter pylori infection in children: a systematic review and meta-analysis. Lancet Child Adolesc Health 2022, 6, 185–194. [Google Scholar] [CrossRef]
- Duong, Q.A.; Pittet, L.F.; Curtis, N.; Zimmermann, P. Antibiotic exposure and adverse long-term health outcomes in children: A systematic review and meta-analysis. J Infect 2022, 85, 213–300. [Google Scholar] [CrossRef]
- Shah, S.C.; Tarassishin, L.; Eisele, C.; Rendon, A.; Debebe, A.; Hawkins, K.; Hillenbrand, C.; Agrawal, M.; Torres, J.; Peek, R.M., Jr.; et al. Breastfeeding Is Associated with Lower Likelihood of Helicobacter Pylori Colonization in Babies, Based on a Prospective USA Maternal-Infant Cohort. Dig Dis Sci 2022, 67, 5149–5157. [Google Scholar] [CrossRef]
- Lunet, N.; Peleteiro, B.; Bastos, J.; Correia, S.; Marinho, A.; Guimaraes, J.T.; La Vecchia, C.; Barros, H. Child day-care attendance and Helicobacter pylori infection in the Portuguese birth cohort Geracao XXI. Eur J Cancer Prev 2014, 23, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Reddy, K.D.; Oliver, B.G.G. Sexual dimorphism in chronic respiratory diseases. Cell Biosci 2023, 13, 47. [Google Scholar] [CrossRef] [PubMed]
- Ekpruke, C.D.; Silveyra, P. Sex Differences in Airway Remodeling and Inflammation: Clinical and Biological Factors. Front Allergy 2022, 3, 875295. [Google Scholar] [CrossRef]
- Raherison, C.; Hamzaoui, A.; Nocent-Ejnaini, C.; Essari, L.A.; Ouksel, H.; Zysman, M.; Prudhomme, A.; groupe de travail 'Femmes et poumons' de la, S. [Woman's asthma throughout life: Towards a personalized management?]. Rev Mal Respir 2020, 37, 144–160. [Google Scholar] [CrossRef] [PubMed]
- Ricciardolo, F.L.M.; Levra, S.; Sprio, A.E.; Bertolini, F.; Carriero, V.; Gallo, F.; Ciprandi, G. Asthma in the Real-World: The Relevance of Gender. Int Arch Allergy Immunol 2020, 181, 462–466. [Google Scholar] [CrossRef]
- Waidyatillake, N.T.; Allen, K.J.; Lodge, C.J.; Dharmage, S.C.; Abramson, M.J.; Simpson, J.A.; Lowe, A.J. The impact of breastfeeding on lung development and function: a systematic review. Expert Rev Clin Immunol 2013, 9, 1253–1265. [Google Scholar] [CrossRef]
- Waidyatillake, N.T.; Dharmage, S.C.; Allen, K.J.; Lodge, C.J.; Simpson, J.A.; Bowatte, G.; Abramson, M.J.; Lowe, A.J. Association of breast milk fatty acids with allergic disease outcomes-A systematic review. Allergy 2018, 73, 295–312. [Google Scholar] [CrossRef]
- Orczyk-Pawilowicz, M.; Lis-Kuberka, J. The Impact of Dietary Fucosylated Oligosaccharides and Glycoproteins of Human Milk on Infant Well-Being. Nutrients 2020, 12. [Google Scholar] [CrossRef]
- Zhang, C.; Guo, Y.; Xiao, X.; Bloom, M.S.; Qian, Z.; Rolling, C.A.; Xian, H.; Lin, S.; Li, S.; Chen, G.; et al. Association of Breastfeeding and Air Pollution Exposure With Lung Function in Chinese Children. JAMA Netw Open 2019, 2, e194186. [Google Scholar] [CrossRef]
- Moshammer, H.; Hutter, H.P. Breast-Feeding Protects Children from Adverse Effects of Environmental Tobacco Smoke. Int J Environ Res Public Health 2019, 16. [Google Scholar] [CrossRef]
- Kerkhof, M.; Wijga, A.H.; Brunekreef, B.; Smit, H.A.; de Jongste, J.C.; Aalberse, R.C.; Hoekstra, M.O.; Gerritsen, J.; Postma, D.S. Effects of pets on asthma development up to 8 years of age: the PIAMA study. Allergy 2009, 64, 1202–1208. [Google Scholar] [CrossRef]
- Genuneit, J.; Seibold, A.M.; Apfelbacher, C.J.; Konstantinou, G.N.; Koplin, J.J.; La Grutta, S.; Logan, K.; Flohr, C.; Perkin, M.R.; Task Force "Overview of Systematic Reviews in Allergy Epidemiology " of the, E.I.G.o.E. The state of asthma epidemiology: an overview of systematic reviews and their quality. Clin Transl Allergy 2017, 7, 12. [Google Scholar] [CrossRef]
- Lehtimäki, J.; Thorsen, J.; Rasmussen, M.A.; Hjelmso, M.; Shah, S.; Mortensen, M.S.; Trivedi, U.; Vestergaard, G.; Bonnelykke, K.; Chawes, B.L.; et al. Urbanized microbiota in infants, immune constitution, and later risk of atopic diseases. J Allergy Clin Immunol 2021, 148, 234–243. [Google Scholar] [CrossRef]
- Raj, S.M.; Choo, K.E.; Noorizan, A.M.; Lee, Y.Y.; Graham, D.Y. Evidence against Helicobacter pylori Being Related to Childhood Asthma. J Infect Dis 2009, 199, 914–915. [Google Scholar] [CrossRef] [PubMed]
- Farag, T.H.; Stoltzfus, R.J.; Khalfan, S.S.; Tielsch, J.M. Unexpectedly low prevalence of Helicobacter pylori infection among pregnant women on Pemba Island, Zanzibar. Trans R Soc Trop Med Hyg 2007, 101, 915–922. [Google Scholar] [CrossRef] [PubMed]
- Farag, T.H.; Fahey, J.W.; Khalfan, S.S.; Tielsch, J.M. Diet as a factor in unexpectedly low prevalence of Helicobacter pylori infection. Trans R Soc Trop Med Hyg 2008, 102, 1164–1165. [Google Scholar] [CrossRef] [PubMed]
- Graham, D.Y.; Yamaoka, Y.; Malaty, H.M. Contemplating the future without Helicobacter pylori and the dire consequences hypothesis. Helicobacter 2007, 12 Suppl 2, 64–68. [Google Scholar] [CrossRef]
- Eder, W.; Ege, M.J.; von Mutius, E. The asthma epidemic. N Engl J Med 2006, 355, 2226–2235. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Wu, J.; Zhang, G. Association between Helicobacter pylori and asthma: a meta-analysis. Eur J Gastroenterol Hepatol 2013, 25, 460–468. [Google Scholar] [CrossRef] [PubMed]
- Tsang, K.W.; Lam, W.K.; Chan, K.N.; Hu, W.; Wu, A.; Kwok, E.; Zheng, L.; Wong, B.C.; Lam, S.K. Helicobacter pylori sero-prevalence in asthma. Respir Med 2000, 94, 756–759. [Google Scholar] [CrossRef] [PubMed]
- Soloski, M.J.; Poulain, M.; Pes, G.M. Does the trained immune system play an important role in the extreme longevity that is seen in the Sardinian blue zone? Front Aging 2022, 3, 1069415. [Google Scholar] [CrossRef]
- Rizzuti, D.; Ang, M.; Sokollik, C.; Wu, T.; Abdullah, M.; Greenfield, L.; Fattouh, R.; Reardon, C.; Tang, M.; Diao, J.; et al. Helicobacter pylori inhibits dendritic cell maturation via interleukin-10-mediated activation of the signal transducer and activator of transcription 3 pathway. J Innate Immun 2015, 7, 199–211. [Google Scholar] [CrossRef]
Figure 1.
Prevalence distribution of seropositivity for H. pylori infection and atopy disorders in 492 children according to age ranges.
Figure 1.
Prevalence distribution of seropositivity for H. pylori infection and atopy disorders in 492 children according to age ranges.
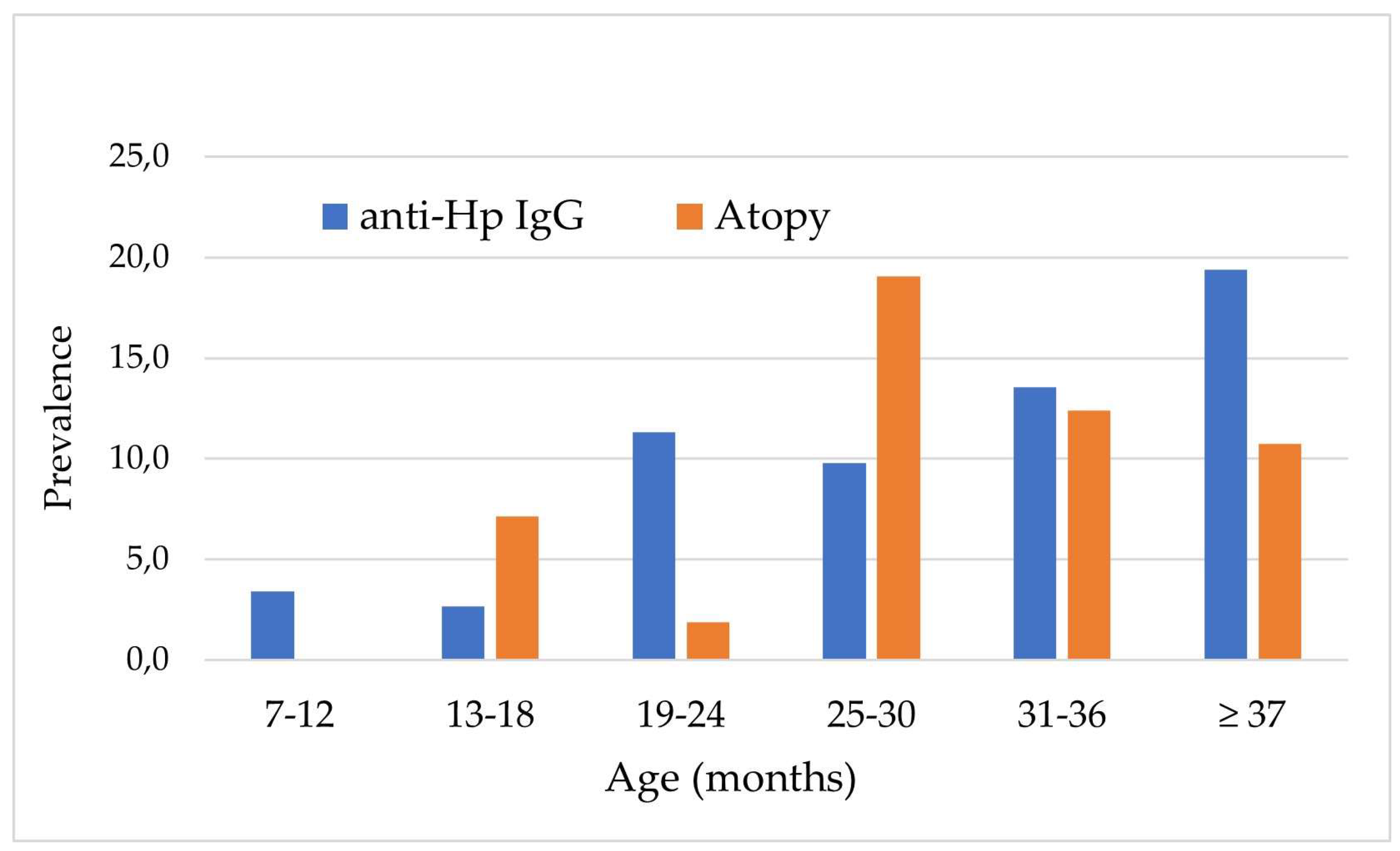

Table 1.
Characteristics of 492 children according to Helicobacter pylori status assessed by serology.
Table 1.
Characteristics of 492 children according to Helicobacter pylori status assessed by serology.
| Variables | Hp 1 IgG < 0.21 (n=434) |
Hp IgG ≥ 0.21 (n=58) |
P-value 2 |
|---|---|---|---|
| Age (months), n (%) 7 ‒ 12 13 ‒ 18 19 ‒ 24 25 ‒ 30 31 ‒ 36 ≥ 37 |
58 (96.5) 73 (97.3) 47 (88.7) 46 (90.2) 102 (86.4) 108 (80.6) |
3 (4.9) 2 (2.7) 6 (11.3) 5 (9.8) 16 (13.6) 26 (19.4) |
0.002 |
| Sex, n (%) Female Male |
218 (90.8) 216 (85.7) |
22 (9.2) 36 (14.3) |
0.078 |
| Residence, n (%) Urban Rural |
369 (91.1) 65 (74.7) |
36 (8.9) 22 (25.3) |
<0.0001 |
| House size in m2, n (%) ≥ 100 < 100 |
226 (92.6) 208 (83.9) |
18 (7.4) 40 (16.1) |
0.003 |
| Breastfeeding, n (%) No < 6 months 6‒11 months ≥ 12 months |
197 (89.5) 188 (90.8) 33 (73.3) 16 (80.0) |
23 (10.5) 19 (9.2) 12 (26.7) 4 (20.0) |
0.409 |
| Ownership of animals, n (%) No Pets Farm animals |
358 (90.2) 76 (80.0) 16 (66.7) |
39 (9.8) 19 (20.0) 8 (33.3) |
0.006 |
| School, n (%) No Day care center School |
271 (93.2) 96 (84.7) 67 (97.1) |
49 (6.8) 7 (15.3) 2 (2.9) |
0.011 |
| Weight, n (%) Normal Reduced |
343 (87.1) 91 (92.9) |
51 (12.9) 7 (7.1) |
0.111 |
| Allergy and/or asthma, n (%) No Allergy Asthma Allergy and asthma |
397 (88.6) 9 (75.0) 28 (87.5) 0 (0.0) |
51 (11.4) 3 (25.0) 4 (12.5) 0 (0.0) |
0.374 |
1 Helicobacter pylori; 2 Values in bold are statistically significant.
Table 2.
Baseline characteristics of 492 children according to atopy.
| Variables | No atopy (n=448) | Atopy (n=44) | p-value * |
|---|---|---|---|
| Age (months), n (%) 7 ‒ 12 13 ‒ 18 19 ‒ 24 25 ‒ 30 31 ‒ 36 ≥ 37 |
59 (100.0) 70 (93.3) 51 (96.2) 42 (82.4) 105 (89.0) 121 (89.0) |
2 (3.3) 5 (6.7) 2 (3.8) 9 (17.6) 13 (11.0) 13 (9.7) |
0.001 |
|
Sex, n (%) Female Male |
222 (92.5) 226 (89.7) |
18 (7.5) 26 (10.3) |
0.420 |
|
Residence, n (%) Urban Rural |
368 (90.9) 80 (92.0) |
37 (9.1) 7 (8.0) |
0.482 |
|
House size, n (%) < 100 ≥ 100 |
215 (90.0) 233 (92.1) |
29 (11.9) 15 (6.0) |
0.406 |
|
Breastfeeding, n (%) No Yes |
197 (89.5) 251 (92.3) |
23 (10.5) 21 (7.7) |
0.025 |
|
Ownership of animals, n (%) No Yes |
361 (90.9) 87 (91.6) |
36 (9.1) 8 (8.4) |
0.827 |
|
School, n (%) No Yes |
297 (92.8) 151 (87.8) |
23 (7.2) 21 (12.2) |
0.063 |
|
H. pylori IgG < 0.21 ≥ 0.21 |
398 (91.7) 50 (86.2) |
36 (8.3) 8 (13.8) |
0.233 |
* Values in bold are statistically significant.
Table 3.
Odds ratios (ORs) and their 95% Confidence Interval (CI) for atopic disease in 492 children older than 6 months.
Table 3.
Odds ratios (ORs) and their 95% Confidence Interval (CI) for atopic disease in 492 children older than 6 months.
| Variables, n (%) | Unadjusted OR (95%CI) | Adjusted OR (95%CI) |
|---|---|---|
|
Age < 24 months ≥ 24 months |
reference 1.70 (0.88‒3.30) |
reference 1.10 (0.41‒2.94) |
|
Sex Female Male |
reference 1.29 (0.69‒2.41) |
reference 2.17 (0.95‒4.44) |
|
Residence, n (%) Urban Rural |
reference 0.73 (0.30‒1.78) |
reference 1.46 (0.64‒3.35) |
|
Breastfeeding, n (%) No Yes |
reference 1.07 (1.57‒2.00) * |
reference 1.91 (0.75‒4.84) |
|
Ownership of animals No Yes |
reference 2.29 (1.26‒4.19) |
reference 0.65 (0.23‒1.86) |
|
School, n (%) No Yes |
reference 1.80 (0.96‒3.35) |
reference 1.58 (0.57‒4.39) |
|
Helicobacter pylori status negative positive |
reference 1.81 (0.80‒4.11) |
reference (0.22‒2.84) |
* p-value statistically significant.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



