
Submitted:
26 December 2023
Posted:
27 December 2023
You are already at the latest version
Abstract
Feline sporotrichosis is an endemic disease with high occurrence in Brazil. Itraconazole (ITZ), remains the drug of choice for treating this disease in cats, despite the increasing reports of therapeutic failure. A controlled, randomized clinical trial was performed on 166 naive cats with sporotrichosis to assess the effectiveness and safety of the combination therapy (ITZ+KI) com-pared with ITZ monotherapy. Cats were randomly allocated in two treatment groups: G1 - ITZ 100 mg/cat/day and G2 - ITZ 100mg/cat/day + KI 2.5-20 mg/kg/day. Cats treated in G2 presented 77% more risk of reaching clinical cure (a positive effect) than those treated in G1, even when controlled by negative predictors. The survival curves of the two treatment protocols indicates that clinical cure was achieved faster in G2. An increase in the KI dose was necessary in 28 cats due to persistence of clinical signs. Adverse reactions were equally frequent in both groups and manageable with a temporary drug suspension and/or a hepatoprotective therapy. The combination therapy was associated with a higher cure rate and a shorter treatment time, suggesting that ITZ+KI arises as a better option for treating feline sporotrichosis and should be considered as the first-line treatment in the presence of negative predictors.
Keywords:
sporotrichosis
; Sporothrix
; cats
; itraconazole
; potassium iodide
; treatment
; combination therapy
1. Introduction
Sporothrix brasiliensis and Sporothrix schenckii are the main causative agents of feline sporotrichosis [1,2,3,4,5,6], with cases mostly reported in South America, Asia and the United States [1,7,8,9,10]. S. brasiliensis is the main etiological agent of sporotrichosis in Brazil, where epizootic as well as zoonotic transmission related to cats have been reported reported over the last twenty-five years [2,11,12,13,14,15,16], although the isolation of this species from the environment suggests that the sapronotic transmission can also occur [17].
Sporothrix brasiliensis is the most virulent species [11] and related to atypical and severe clinical manifestations in cats and humans with increasing virulence over time [18,19,20]. Recently, new cases involving S. brasiliensis are being reported in Argentina, Chile, Paraguay, the United States and the United Kingdom [21,22,23,24,25], indicating a propagation of this species.
Cats are the most susceptible animal species to Sporothrix infection, often developing severe forms of the disease [2,26,27]. Clinical manifestations range from a single to multiple skin lesions, which can progress to disseminated systemic forms [28]. Nodules and ulcers are the most common lesion types followed by respiratory signs (dyspnea, sneezing, nasal discharge) and mucosal involvement (nasal, ocular) [29,30]. The presence of lesions on the nasal bridge, nasal mucosa, respiratory signs and lesions in multiples sites are considered negative predictors that may hinder a complete cure [29,31,32].
The early diagnosis of the disease combined with a fast initiation of treatment represents an important disease control measure as it may induces a quick reduction of the fungal burden [33]. On the other hand, the increased virulence of S. brasiliensis, unrestricted access of cats to outdoors and an inappropriate treatment protocol could lead to longer treatment times, therapeutic failure or even abandonment, which seems to be an issue for the epidemiological control [30].
Many potential drug candidates showed in vitro activity against Sporothrix [15,34,35,36,37,38], but in spite of that, there are few antifungal agents available that are effective in vivo against feline sporotrichosis [30].
The therapeutic options for feline sporotrichosis are most often used as monotherapy regimens, and itraconazole (ITZ) remains the drug of choice for treating the disease [30]. Due the increasing number of cases refractory to ITZ [36,39,40], the combination of antifungal agents should be considered to achieve synergy [30]. In addition, alternative therapies as intralesional amphotericin B, cryosurgery, intranasal clotrimazole spray, local laser therapy and photodynamic therapy were associated with an oral antifungal agent [41,42,43,44,45] , but there are some limitations due to its clinical indication.
The combination therapy with KI has been described as the best therapeutic option for treating feline sporotrichosis, however, this is based on case series studies [40,46]. Randomized clinical trials (RCT) provide the highest level of evidence for evaluating the effectiveness of a treatment since they are designed to reduce bias and systematic errors [47,48], which is essential for the evidence-based veterinary medicine (EBVM) [49].
Thus, the aim of this study was to assess whether ITZ+KI is more effective and safer than the conventional treatment (ITZ) through a controlled randomized clinical trial.
2. Materials and Methods
This was a prospective, non-blinded, randomized, controlled clinical trial comparing monotherapy with ITZ and the combination therapy with ITZ+KI in owned cats with sporotrichosis. The study was conducted at the Laboratory of Clinical Research on Dermatozoonoses in Domestic Animals (Lapclin-Dermzoo), INI, Fiocruz and the cats were enrolled from 2013 to 2016.
The protocol and the informed consent were reviewed and approved by the Ethics Commission on the Use of Animals (CEUA/Fiocruz), license number LW37/2012.
2.1. Inclusion, Exclusion and Elimination criteria
Cats seen at Lapclin-Dermzoo/INI/Fiocruz and suspected of having sporotrichosis were assessed by two veterinarians at day 0 to determine eligibility for the study. Inclusion criteria comprised cats of any breed, older than 6 months, weight >3 kg and a clinical and cytopathological diagnostic of sporotrichosis. The exclusion criteria were previous systemic antifungal therapy, owners that did not signed informed consent and concurrent pregnancy at day 0.
Cats that fulfilled eligibility criteria were randomized into a treatment group, but they were subsequently removed from the study if Sporothrix sp. could not be isolated in culture from cutaneous lesion or nasal swabs or if the owners did not return to the second visit (declined treatment). This data was not computed and analyzed in the trial.
2.2. Study Procedure
Cats enrolled in the study underwent clinical examination, collection of clinical specimens and photographic data. Anamnesis was carried out in every follow-up visit.
The clinical examination consisted of the following procedures: evaluation of health condition (good, fair, and poor), inspection of the skin and mucous membranes (conjunctive, nasal, oral, genital, and anal), palpation of lymph nodes (mandibular, parotid, axillary and popliteal) and body weigh assessment. The veterinarians also inspected the nasal cavity and checked for the presence of respiratory signs. The time elapsed between the onset of clinical signs and the first appointment was based on the information provided by the owners.
To estimate the level of dissemination of cutaneous lesions, the cats were divided into three groups: L1 (skin lesions at one site), L2 (skin lesions at two non-adjacent sites), and L3 (skin lesions at three or more non-adjacent sites) [29].
Exudate from ulcerated lesions or secretion from nasal cavities were collected using sterile swabs and seeded on to Sabouraud dextrose agar and Mycobiotic agar (Difco, ™; Becton, Dickinson and Company, Sparks, MD, USA), incubated at 25°C and observed during four weeks for fungal growth. Suspected isolates were subcultivated on potato dextrose agar medium (Difco) at 25°C for macroscopic and microscopic morphological studies. Dimorphism was demonstrated by conversion to the yeast-like form on brain heart infusion agar medium (Difco) at 37°C.
Blood samples were collected for a complete blood count and biochemistry analysis (urea, creatinine, alanine aminotransferase [ALT], aspartate aminotransferase [AST]). In addition, serum samples from all cats were tested for the presence of antibodies against feline immunodeficiency virus (FIV) and antigen of feline leukemia virus (FeLV) by ELISA® Snap-Combo FIV-FeLV (IDEXX Laboratories Inc., EUA), according to manufacturer instructions.
2.3. Sample size and Randomization
An estimated sample of 74 cats in each group was established to detect a difference of 25% in clinical cure between treatments, considering a dropout rate of 20%, an alpha (α) of 0.05 and a power of 0.8.
Each cat was assigned a number based on admission order. According to this number, they were randomly allocated (1:1 ratio) to group G1 (ITZ) or G2 (ITZ +KI), using the random function of the software Statistical Package for the Social Sciences v16.0.
Cat-owners and the veterinary staff were non-blinded to the allocated treatment.
2.4. Treatment
Cats randomized to G1 received only ITZ 100 mg (Prati-Donaduzzi®) in a blister pack. Owners were instructed to administer one capsule per day, directly into the oral cavity or mixed with canned cat food.
Cats randomized to G2 received ITZ 100 mg (Prati-Donaduzzi®) plus compounded KI (about 2.5 mg/kg) in a different capsule pack. Owners were advised to administer one capsule of ITZ 100 mg per day and the KI every other day for the first 7 days. After that, KI should be administered per day. They were also instructed to provide the drugs at the same time, directly into the oral cavity or mixed with canned cat food. The proposed dose for KI in cats should never be managed all at once, but gradually increased as previously reported [46,50].
Drugs were dispensed according to each treatment and in the required amount to last until the next appointment. Owners were guided to call the veterinary staff in case of clinical adverse reaction (CAR) and hepatotoxicity, such as loss of appetite, lethargy, vomiting, diarrhea, jaundice or if they had any doubt about the treatment. Furthermore, they were requested to return with patients to the scheduled follow-up visit within 30 days until treatment outcome.
All procedures, laboratorial tests and drugs were supplied free-of-charge. Owners had to provide informed consent prior to enrolment and were free to withdraw at any point without any loss to the cats’ treatment and care.
2.5. Follow-Up Procedures
The follow-up appointments were carried out monthly for anamnesis, clinical and photographic documentation. During these visits, questions about adverse reactions were asked. Clinical signs were recorded and compared with the previous appointment.
Cats presenting hyporexia or anorexia combined with body loss of >10% or the association of CAR and elevated serum aminotransferase (ESA) had a temporary suspension of the drug(s). Drug suspension was for a minimum of seven days for G1. In G2, both drugs were suspended at the same time, but the reintroduction of ITZ occurred on the eighth day and the KI on the eleventh, in the attempt to detect which drug was causing the unwanted effect. The maximum period for the temporary interruption of the drug (s) was set as 30 days. A hepatoprotective therapy with oral silymarin 30 mg/kg/day was prescribed for persistence of CAR and ESA.
In cases of persistence of the initial skin/mucosal lesion(s), persistence of respiratory signs or worsening of the lesion(s), cats from G2 had the dose of KI increased by increments of about 2.5 mg/kg at the follow-up visit up to a satisfactory clinical response or until the dose reached 20 mg/kg maximum.
Clinical cure was defined as a complete healing of the skin/mucosal lesions and/or remission of respiratory signs. After clinical cure, the therapy was maintained for about a month, which corresponded to the discharge assessment. Cats that did not present any improvement in two consecutives follow-up visits were considered treatment failure as well as cats that were incapable to tolerate KI 2.5mg/kg and/or ITZ 100 mg.
2.6. Statistical analysis
For exploratory analysis of the data, we calculated the frequency distribution for categorical variables and summary measures (median -MD, interquartile range-IQR) for quantitative variables.
We performed the Kaplan-Meier survival analysis to estimate median time to achieve clinical cure in each treatment group.
The Cox semiparametric regression model was used to identify factors associated with clinical cure. Time was measured in weeks from inclusion to the event (clinical cure or censoring). The cure was the event of interest, while censorship occurred due to other outcomes (therapeutic failure, loss to follow up and death). The treatment groups were monotherapy (G1) and combination therapy (G2). In the multivariate regression, significant predictors from univariate regression were chosen as adjustment variables. Non-significant variables were sequentially removed from the model. Hazard Ratios (HR) with 95% confidence intervals were provided for interpretation. An HR=1 suggests no survival difference, HR > 1 implies increased cure rate (positive effect), and HR < 1 indicates a smaller cure rate (negative effect). The Cox proportionality assumption was not rejected by the Schoenfeld test.
The log-rank test was used to compare the distribution of time up to the occurrence of a drug adverse reaction (CAR or ESA). A p-value < 0.05 was considered statistically significant.
All analyses were performed using the R v4.2.1 software.
3. Results
One hundred and seventy-nine cats were evaluated. The recruitment process of the eligible cats is illustrated in Figure 1.
3.1. Exploratory analysis
All cats were residents from Rio de Janeiro state. Most of them were male (73.4%), mixed breed (91.5%), had access outdoors (78.3%) and were in good overall condition (88.5%). Twenty-one isolates were recovered from cultures of clinical samples, and all of them were identified as S. brasiliensis. T3B PCR fingerprinting was used for molecular identification of the Sporothrix species [51].
The clinical characteristics of the cats is shown in Table 1. The groups were equivalent in terms of age and weight, and they had the same median interval between the onset of clinical signs (information provided by the owner) and the first appointment. Skin lesions were detected in all cases, respiratory signs in 31.9%, and mucosal lesions in 29.5%.
The overall median dose of ITZ in the trial was 24.4 mg/kg (IQR= 21.2-27.7 mg/kg), while the KI was 2.6 mg/kg (IQR= 2.3-2.9 mg/kg).
Twenty-eight cats in G2 had the dose of KI increased (Table 2) and two cats required dose reduction due to persistent clinical adverse effects at the proposed dose. The maximum dose of KI reached in this trial was 12.5 mg/kg. A borderline effect was noted when evaluating the influence of a 10-unit increment in the KI dosage on the cure rate (HR (95%CI) = 0.14 (0.02-1.11), p-value = 0.06).
One hundred and fifteen cats achieved clinical cure (67.2%) and were discharged from the therapeutic protocol (Figure 2). The cure rate was 50.6% in G1 and 88 % in G2. Figure 3 shows the frequency of outcome of the 166 cats included in the trial.
Twenty-five G1 cats were censored due to therapeutic failure assigned to disease stagnation (n=16), worsening of clinical signs (n=7) and severe adverse drug reaction (n=2).
The FIV and/or FeLV co-infection has seemingly not affected the treatment response in this sample. Of the 31 co-infected cats, 23 were clinically cured (G1: n=8/13; G2: n=15/18), five were lost to follow-up (G1: n=2/13; G2: n=3/18) and three failed treatment (G1: n=3/13; 10%).
The comparison between the curves (Figure 4) of the two protocols indicates that clinical cure was achieved faster in cats treated with the combination therapy (G2) than in those who were treated with ITZ monotherapy (G1) [HR (95%CI) = 1.768 (1.207,2.588), p-value <0.01]. After cure, the therapy was maintained for about a month.
3.2. Cox regression model
The following clinical-epidemiological variables were entered into the univariate cox model to investigate independent risk factors for clinical cure: treatment group, general condition, sex, age, respiratory signs, temporarily drug suspension, lymphangitis, lymphadenomegaly, mucosal lesion, access to outdoors, distribution of skin lesions, neutering and FIV/FeLV infection.
The exposure variable - treatment group - showed significance in univariate and multivariate cox models (Table 3).
Cats in G2 (ITZ+KI) presented 77% more risk of reaching the event of clinical cure (a positive effect) than cats in G1 (ITZ), even when controlled by other factors, including negative predictors as presence of “respiratory signs” and “mucosal lesions”. In addition, the cox model shows that the absence of lymphangitis is a negative predictor in time to achieve clinical cure.

Table 3.
Univariate and multivariate Cox models analysis of 166 cats with sporotrichosis, Rio de Janeiro, Brazil.
Table 3.
Univariate and multivariate Cox models analysis of 166 cats with sporotrichosis, Rio de Janeiro, Brazil.
| Predictors | Category | Clinical Cure | Crude HR (95% CI) | Adjusted HR (95% CI | |
|---|---|---|---|---|---|
| Yes, n (%) | No, n (%) | ||||
| Treatment group | ITZ | 42 (50.6) | 41 (49.4) | 1 | 1 |
| ITZ + KI | 73 (88) | 10 (12) | 1.77 (1.21-2.59) | 1.77 (1.2-2.62) | |
| Respiratory signs | Yes | 31 (58.5) | 22 (41.5) | 1 | 1 |
| No | 84 (74.3) | 29 (25.7) | 3 (1.74-5.17) | 2.09 (1.14-3.83) | |
| Mucosal lesions | Yes | 32 (54.2) | 27 (45.8) | 1 | 1 |
| No | 83 (77.6) | 24 (22.4) | 2.36 (1.56-3.58) | 1.74 (1.09-2.78) | |
| Distribution of skin lesions | L3 | 41 (59.4) | 28 (40.6) | 1 | 1 |
| L2 | 35 (79.5) | 9 (20.5) | 1.76 (1.12-2.78) | 2.08 (1.3-3.32) | |
| L1 | 39 (73.6) | 14 (26.4) | 1.79 (1.15-2.81) | 2.24 (1.39-3.61) | |
| Lymphangitis | Yes | 23 (79.3) | 6 (20.7) | 1 | 1 |
| No | 92 (67.2) | 45 (32.8) | 0.55 (0.34-0.87) | 0.46 (0.28-0.76) | |
| Neutering | No | 48 (58.5) | 34 (41.5) | 1 | 1 |
| Yes | 67 (82.7) | 14 (17.3) | 1.78 (1.22-2.58) | 1.61 (1.09-2.37) | |
Abbreviations: HR= Hazard Ratio, CI= Confidence interval.
3.3. Safety
The frequency of an adverse drug reaction (ADR) was similar in both groups regarding CAR and ESA.
Clinical adverse reaction was noted in 35 cats (42.2%) from G1 and in 39 cats (47.0%) from G2, being hyporexia the most frequent one (G1: n=23/35; G2: n=27/39). Serum transaminases were elevated in 50 cats from G1 (60.2%) and in 43 (51.8%) from G2 (Table 4).
In this study, the distribution of time up to the occurrence of CAR (p=0.493) or ESA (p=0.096) did not differ between groups.
Table 4.
Evaluation of serum aminotransferase in 166 cats treated for sporotrichosis, according to treatment group, Rio de Janeiro, Brazil.
Table 4.
Evaluation of serum aminotransferase in 166 cats treated for sporotrichosis, according to treatment group, Rio de Janeiro, Brazil.
| Aminotransferase levels | G1-ITZ (N=83) |
G2-ITZ+KI (N=83) |
Unit | Reference Value |
|---|---|---|---|---|
| Normal | 33 | 40 | U/L | AST (6-83) [52] ALT (26-43) [52] |
| Mild elevation (ALT and/or AST) | 43 |
39 | U/L | <5 times the upper reference range [53] |
| Moderate elevation (ALT) | 5 | 4 | U/L | 5–10 times the upper reference range [53] |
| Marked elevation (ALT) | 2 | 0 | U/L | >10 times the upper reference range [53] |
Abbreviations: ALT: Alanine aminotransferase; AST: Aspartate aminotransferase.
Thirty-seven cats had the therapy temporarily suspended (G1: n=15, 18.0%; G2: n=22, 26.5%) due to clinical signs of hepatotoxicity (G1: n=4; G2: n=9) or these signs combined with an elevation of serum transaminases (G1: n=12; G2: n= 12). Signs of CAR were reversible within 7 to 20 days (MD=7 days) of temporary drug suspension and the transaminases alterations returned to pre-treatment levels after drug suspension and/or oral hepatoprotective therapy.
Two cats from G1 were censured due to severe CAR (anorexia, weight loss, apathy, jaundice) and marked elevation of ALT. They were indexed as treatment failure given to inability to tolerate the drug.
4. Discussion
In the hyperendemic scenario of Rio de Janeiro, the lack of public health polices to curb sporotrichosis combined with the absence of free-of-charge antifungal medications, the cat's high zoonotic potential to transmit S. brasiliensis, the challenging of treating cats orally and keeping them indoors, may be some of the reasons for having an increased number of human and feline sporotrichosis cases [30,33]. Furthermore, educational measures to ensure responsible ownership, mass neutering, early diagnosis and mass treatment can slow the spread of the disease [20,30,54].
The combination of ITZ and KI has been considered an important option for the treatment of refractory cases [40] as well as for naïve cats [46] , especially for those presenting multiple cutaneous lesions, nasal mucosa lesions and/or respiratory signs [30,46]. To evaluate the efficacy and safety of this treatment protocol and consider it as first-line treatment for feline sporotrichosis, we carried out a clinical trial comparing it with the conventional protocol (ITZ monotherapy).
In this trial, the combined therapy with ITZ+KI increased up 77 times the rate of clinical cure. This finding is consistent to previous studies that noted an increased likelihood of recovery in sporotrichosis with the use of the combination therapy for both naïve [46] and cats that did not respond to ITZ monotherapy [40]. Respiratory signs, mucosal lesions, skin lesions on 3 or more sites (L3) and not being neutered, are in fact, obstacles to achieve clinical cure, as previously reported [29,31,32]. Interestingly, lymphangitis seems to be a positive predictor in cats, which has not been reported so far, differing from human sporotrichosis cases [55,56]. In addition, ITZ+KI therapy has also been shown to be effective in the healing and in the prompt control of fungal burden in skin lesions from cats with sporotrichosis [33]. In human sporotrichosis, ITZ combined with KI is used in cases with severe or ITZ-refractory sporotrichosis [57], as well as for the treatment of other fungal infections [58,59].
Although this trial was controlled and randomized, we did not blind the groups as the prescribed KI dose must be escalated to avoid toxicity [46,50]. An increase in the KI dose was expected in case of non-response to the initial dose. The overall KI dose in the present study was lower than that reported in a study conducted with refractory cats [40], which is somehow expected, considering the shorter time elapsed between the onset of clinical signs and the start of treatment in naïve cats (m=8 weeks). The higher rate of nasal lesions and respiratory signs in refractory cats could have contributed to the higher KI dose, since nasal lesions, respiratory signs, and lesions in multiples sites (group L3) are predictors of severity in feline sporotrichosis and are linked to increased risk of negative outcomes. Although Retrovirus/Sporothrix co-infection can lead to important changes in immunological balance of cats [60], in this study, the co-infection did not represent an obstacle to clinical cure, which is consistent with other findings [31,32,46,60].
Both therapeutic regimens were reasonably tolerated by cats in this study. The CAR of ITZ monotherapy (42.2%) was higher than those observed in a retrospective study of feline sporotrichosis using this azolic (30.9%) [32]. However, it is important to emphasize that the dose range of ITZ in this trial was higher (21.2-27.7 mg/kg) than the previously reported (8.3–27.7 mg/kg) [32]. CAR and increased ALT are considered a dose-dependent effect to ITZ administration and have also been reported in cats with sporotrichosis under KI therapy [40,46,50].
Regarding KI, the tolerance threshold for the drug in cats may range from 2.5 to 20 mg/kg [50], even though in this study the maximum dose reached was 12.5mg/kg. The frequency of CAR in this study (47%) was lower than reported for refractory cats (76.3%) [40], which could be explained by the higher dose of KI and the previous treatment with ITZ (MD=16 weeks) in those cats when compared to the present study. In this trial, the ADR were successfully managed with a temporary drug suspension and/or oral hepatoprotective therapy as previously reported [46]. There was no statistical difference between CAR and ESA in both treatment groups, demonstrating that the combined therapy is as safe as ITZ monotherapy.
The criterion for cure of feline sporotrichosis is clinical and determined by the complete remission of all clinical signs [30]. It is important to continue the treatment for at least 1 month after that to minimize the risk of recurrence [30,46]. Although the median time up to clinical cure differed between G1 and G2, it was consistent with the medians already reported in studies involving treatment with ITZ [31,61] and ITZ+KI [46]. In cats treated with ITZ monotherapy, a shorter treatment might be tied to the early intervention with the use of an approved generic capsule of the drug. Compounded formulations of ITZ, on the other hand, are absorbed poorly and inconsistently [62], so we do not recommend their use in cats. While branded ITZ may be cost-prohibitive in low socioeconomic endemic areas such as in Brazil, the generic drug is a satisfactory alternative [30] as demonstrated in this trial.
Although these results endorse the previous reports on the beneficial use of KI for the treatment of feline sporotrichosis, the mechanism of action of KI is still to be determined. While a direct antimicrobial effect seems unlikely, immune-related effects are more well-accepted but still controversial [63,64]. A shorten time to remission of all clinical signs in cats treated with the combined therapy may be related to the anti-inflammatory effect of KI linked to cytokine regulation [65], and/or to a beneficial interaction between ITZ and KI that has not been fully elucidated yet. In addition, excessive iodine supplementation in humans as well as in cats may affect the thyroid function, which might have an impact in the host immune response, but this has not been explored with the use of KI in the treatment of sporotrichosis [66,67,68,69,70,71].
Cats receiving the combined therapy had shown increased cure rates, a lower rate of drop-out and a fast onset of action, suggesting this treatment regimen (ITZ+KI) should be considered as the first-line treatment, notably in the presence of negative predictors. Further studies are still encouraged to investigate the mechanisms behind the successful use of KI in the treatment of feline sporotrichosis. We believe this can provide valuable information on the use of KI and boost the confidence of veterinarians at prescribing this drug for cats.
Author Contributions
Conceptualization: EGR, SAP, TMPS and IDFG; Methodology: EGR, LHMM, SAP, JNS, MSBQ, TMPS and IDFG; Sample collection and clinical follow-up: EGR, JNS, PGV and LHMM; Data checking: CCSH, GRPO, ABFF; Statistical analysis: MSBQ and RVCO; Writing: EGR, SAP, LHMM, MDSBQ, RVCO, JNS, PGV, ABFF, CCDSH, GRPO, TMPS and IDFG; Supervision TMPS and IDFG.
Funding
This work was supported by grants from the Brazilian funding agencies: Conselho Nacional de Desenvolvimento Científico e Tecnológico - CNPq [Gremião IDF, Universal: 478262/2013-2; Schubach TMP: 305669/2012-5], Fundação de Amparo à Pesquisa do Estado do Rio de Janeiro [Pereira SA, Jovem Cientista do Nosso Estado: E23/102.255/2013; Schubach TMP, Cientista do Nosso Estado: E26/102251/2009]; Programa Jovens Pesquisadores (INI/Fiocruz): [Gremião IDF: 25029.100173/2019-58] and Coordenação de Aperfeiçoamento da Pessoal de Nível Superior (CAPES). Pereira SA is recipient of CNPq productivity fellowship.
Institutional Review Board Statement
The study protocol and the informed consent were reviewed and approved by the Animal Ethics Committee (CEUA) of Oswaldo Cruz Foundation (Fiocruz). License number: LW37/12 (P-84/11.2).
Informed Consent Statement
Informed consent was obtained from all cat owners included in the study.
Acknowledgments
The authors are grateful to the staff of the Laboratório de Pesquisa Clínica em Dermatozoonoses em Animais Domésticos (INI/Fiocruz), Noemi Lorenzi (Sefarm/INI/Fiocruz), the staff of Lab-Micol/INI/Fiocruz and Dra Valdiléa Gonçalves Veloso dos Santos (Director of INI/Fiocruz).
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; and in the decision to publish the results.
References
- Han, H.S.; Kano, R. Feline Sporotrichosis in Asia. Braz J Microbiol 2021, 52, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, A.M.; Goncalves, S.S.; de Carvalho, J.A.; Borba-Santos, L.P.; Rozental, S.; Camargo, Z.P. Current Progress on Epidemiology, Diagnosis, and Treatment of Sporotrichosis and Their Future Trends. J Fungi 2022, 8. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, S.S.; da Cruz Bahiense Rocha, I.; Rediguieri, B.C.; de Carvalho, J.A.; Maifrede, S.B.; Kruschewsky, W.L.L.; Falqueto, A.; Rodrigues, A.M. Human and Feline Sporotrichosis in a Reference Center of Southeastern Brazil: Genetic Differentiation, Diversity, and Antifungal Susceptibility of Sporothrix Species. JoF 2023, 9, 831. [Google Scholar] [CrossRef] [PubMed]
- Gallo, S.; Arias-Rodriguez, C.; Sánchez-Cifuentes, E.A.; Santa-Vélez, C.; Larrañaga-Piñeres, I.; Gaviria-Barrera, M.E.; Vásquez-Ochoa, L.A.; Montoya, D.; Jiménez-Alzate, M. del P. First Three Cases of Cat-associated Zoonotic Cutaneous Sporotrichosis in Colombia. Int J Dermatology 2022, 61, 1276–1279. [Google Scholar] [CrossRef] [PubMed]
- Santos, A.F.; Azevedo, M.I.; Amaral, C.I.; Grom, N.A.; Marinho, F.; de Oliveira, C.S.F.; de M. Soares, D.F.; Morais, M.H.F.; Brandão, S.T.; Menezes, R.C.; et al. Feline Sporotrichosis: Characterization of Cutaneous and Extracutaneous Lesions Using Different Diagnostic Methods. Feline Sporotrichosis: Characterization of Cutaneous and Extracutaneous Lesions Using Different Diagnostic Methods 2023, 61, 221–231. [Google Scholar] [CrossRef] [PubMed]
- Zúñiga-Valencia, M.S.; Ordoñez, A.R.; Cunha, F.R.; Guerrero-López, A.E. Esporotricosis en un gato doméstico. Reporte del primer caso en Ecuador. RC FCV-LUZ 2022, 32, 1–7. [Google Scholar] [CrossRef]
- Etchecopaz, A.; Toscanini, M.A.; Gisbert, A.; Mas, J.; Scarpa, M.; Iovannitti, C.A.; Bendezu, K.; Nusblat, A.D.; Iachini, R.; Cuestas, M.L. Sporothrix Brasiliensis: A Review of an Emerging South American Fungal Pathogen, Its Related Disease, Presentation and Spread in Argentina. J Fungi (Basel) 2021, 7. [Google Scholar] [CrossRef] [PubMed]
- Singer, J.I.; Muncie, J.E. Sporotrichosis; Etiologic Considerations and Report of Additional Cases from New York. N Y State J Med 1952, 52, 2147–2153. [Google Scholar] [PubMed]
- Rees, R.K.; Swartzberg, J.E. Feline-Transmitted Sporotrichosis: A Case Study from California. Dermatol Online J 2011, 17, 2. [Google Scholar] [CrossRef]
- Reed, K.D.; Moore, F.M.; Geiger, G.E.; Stemper, M.E. Zoonotic Transmission of Sporotrichosis: Case Report and Review. Clinical Infectious Diseases 1993, 16, 384–387. [Google Scholar] [CrossRef]
- Della Terra, P.P.; Rodrigues, A.M.; Fernandes, G.F.; Nishikaku, A.S.; Burger, E.; de Camargo, Z.P. Exploring Virulence and Immunogenicity in the Emerging Pathogen Sporothrix Brasiliensis. PLoS Negl Trop Dis 2017, 11, e0005903. [Google Scholar] [CrossRef] [PubMed]
- Falcão, E.M.M.; Romão, A.R.; Magalhães, M.d.A.F.M.; de Lima Filho, J.B.; do Valle, A.C.F.; Bastos, F.I.; Gutierrez-Galhardo, M.C.; Freitas, D.F.S. A Spatial Analysis of the Spread of Hyperendemic Sporotrichosis in the State of Rio de Janeiro, Brazil. JoF 2022, 8, 434. [Google Scholar] [CrossRef] [PubMed]
- Freitas, D.F.S.; do Valle, A.C.F.; de Almeida Paes, R.; Bastos, F.I.; Galhardo, M.C.G. Zoonotic Sporotrichosis in Rio de Janeiro, Brazil: A Protracted Epidemic yet to Be Curbed. CLIN INFECT DIS 2010, 50, 453–453. [Google Scholar] [CrossRef] [PubMed]
- Angelo, D.F.D.S.; Rabello, V.B.D.S.; Maciel, M.A.S.; Atanázio, S.S.D.L.A.; Costa, M.C.L.D.; Silva, S.R.; Almeida-Paes, R.; Bernardes-Engemann, A.R.; Zancopé-Oliveira, R.M.; Clementino, I.J. Sporothrix Brasiliensis Infecting Cats in Northeastern Brazil: New Emerging Areas in Paraíba State. Cienc. Rural 2023, 53, e20220351. [Google Scholar] [CrossRef]
- Maschio-Lima, T.; Marques, M.D.R.; Lemes, T.H.; Brizzotti-Mazuchi, N.S.; Caetano, M.H.; de Almeida, B.G.; Bianco, L.M.; Monteiro, R.C.; Rodrigues, A.M.; de Camargo, Z.P.; et al. Clinical and Epidemiological Aspects of Feline Sporotrichosis Caused by Sporothrix Brasiliensis and in Vitro Antifungal Susceptibility. Vet Res Commun 2021, 45, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, M.M.E.; Maifrede, S.B.; Ribeiro, M.A.; Zancope-Oliveira, R.M. Molecular Identification of Sporothrix Species Involved in the First Familial Outbreak of Sporotrichosis in the State of Espírito Santo, Southeastern Brazil. Mem. Inst. Oswaldo Cruz 2013, 108, 936–938. [Google Scholar] [CrossRef] [PubMed]
- Rabello, V.B.S.; Almeida-Silva, F.; Scramignon-Costa, B.d.S.; Motta, B. da S.; de Macedo, P.M.; Teixeira, M. de M.; Almeida-Paes, R.; Irinyi, L.; Meyer, W.; Zancopé-Oliveira, R.M. Environmental Isolation of Sporothrix Brasiliensis in an Area With Recurrent Feline Sporotrichosis Cases. Front. Cell. Infect. Microbiol. 2022, 12, 894297. [Google Scholar] [CrossRef]
- Almeida-Paes, R.; de Oliveira, M.M.; Freitas, D.F.; do Valle, A.C.; Zancope-Oliveira, R.M.; Gutierrez-Galhardo, M.C. Sporotrichosis in Rio de Janeiro, Brazil: Sporothrix Brasiliensis Is Associated with Atypical Clinical Presentations. PLoS Negl Trop Dis 2014, 8, e3094. [Google Scholar] [CrossRef] [PubMed]
- Freitas, D.F.; Santos, S.S.; Almeida-Paes, R.; de Oliveira, M.M.; do Valle, A.C.; Gutierrez-Galhardo, M.C.; Zancope-Oliveira, R.M.; Nosanchuk, J.D. Increase in Virulence of Sporothrix Brasiliensis over Five Years in a Patient with Chronic Disseminated Sporotrichosis. Virulence 2015, 6, 112–120. [Google Scholar] [CrossRef]
- Schechtman, R.C.; Falcão, E.M.M.; Carard, M.; García, M.S.C.; Mercado, D.S.; Hay, R.J. Sporotrichosis: Hyperendemic by Zoonotic Transmission, with Atypical Presentations, Hypersensitivity Reactions and Greater Severity. Anais Brasileiros de Dermatologia 2022, 97, 1–13. [Google Scholar] [CrossRef]
- Etchecopaz, A.N.; Lanza, N.; Toscanini, M.A.; Devoto, T.B.; Pola, S.J.; Daneri, G.L.; Iovannitti, C.A.; Cuestas, M.L. Sporotrichosis Caused by Sporothrix Brasiliensis in Argentina: Case Report, Molecular Identification and in Vitro Susceptibility Pattern to Antifungal Drugs. Journal de Mycologie Médicale 2020, 30, 100908. [Google Scholar] [CrossRef] [PubMed]
- Thomson, P.; González, C.; Blank, O.; Ramírez, V.; Río, C.D.; Santibáñez, S.; Pena, P. Sporotrichosis Outbreak Due to Sporothrix Brasiliensis in Domestic Cats in Magallanes, Chile: A One-Health-Approach Study. JoF 2023, 9, 226. [Google Scholar] [CrossRef]
- do Prado, C.M.; Razzolini, E.; Santacruz, G.; Ojeda, L.; Geraldo, M.R.; Segovia, N.; Pereira Brunelli, J.; Vicente, V.A.; Svoboda, W.K.; Queiroz-Telles, F. First Cases of Feline Sporotrichosis Caused by Sporothrix Brasiliensis in Paraguay. JoF 2023, 9, 972. [Google Scholar] [CrossRef] [PubMed]
- Kaadan, M.I.; Dennis, M.; Desai, N.; Yadavalli, G.; Lederer, P. One Health Education for Future Physicians: A Case Report of Cat-Transmitted Sporotrichosis. Open Forum Infectious Diseases 2020, 7, ofaa049. [Google Scholar] [CrossRef] [PubMed]
- Barnacle, J.R.; Chow, Y.J.; Borman, A.M.; Wyllie, S.; Dominguez, V.; Russell, K.; Roberts, H.; Armstrong-James, D.; Whittington, A.M. The First Three Reported Cases of Sporothrix Brasiliensis Cat-Transmitted Sporotrichosis Outside South America. Medical Mycology Case Reports 2023, 39, 14–17. [Google Scholar] [CrossRef] [PubMed]
- Montenegro, H.; Rodrigues, A.M.; Dias, M.A.G.; da Silva, E.A.; Bernardi, F.; de Camargo, Z.P. Feline Sporotrichosis Due to Sporothrix Brasiliensis: An Emerging Animal Infection in São Paulo, Brazil. BMC Vet Res 2014, 10, 269. [Google Scholar] [CrossRef] [PubMed]
- Xavier, M.O.; Poester, V.R.; Trápaga, M.R.; Stevens, D.A. Sporothrix Brasiliensis: Epidemiology, Therapy, and Recent Developments. JoF 2023, 9, 921. [Google Scholar] [CrossRef] [PubMed]
- Macêdo-Sales, P.A.; Souto, S.R.L.S.; Destefani, C.A.; Lucena, R.P.; Machado, R.L.D.; Pinto, M.R.; Rodrigues, A.M.; Lopes-Bezerra, L.M.; Rocha, E.M.S.; Baptista, A.R.S. Domestic Feline Contribution in the Transmission of Sporothrix in Rio de Janeiro State, Brazil: A Comparison between Infected and Non-Infected Populations. BMC Vet Res 2018, 14, 19. [Google Scholar] [CrossRef] [PubMed]
- Schubach, T.M.; Schubach, A.; Okamoto, T.; Barros, M.B.; Figueiredo, F.B.; Cuzzi, T.; Fialho-Monteiro, P.C.; Reis, R.S.; Perez, M.A.; Wanke, B. Evaluation of an Epidemic of Sporotrichosis in Cats: 347 Cases (1998-2001). J Am Vet Med Assoc 2004, 224, 1623–1629. [Google Scholar] [CrossRef] [PubMed]
- Gremiao, I.D.F.; Martins da Silva da Rocha, E.; Montenegro, H.; Carneiro, A.J.B.; Xavier, M.O.; de Farias, M.R.; Monti, F.; Mansho, W.; de Macedo Assuncao Pereira, R.H.; Pereira, S.A.; et al. Guideline for the Management of Feline Sporotrichosis Caused by Sporothrix Brasiliensis and Literature Revision. Braz J Microbiol 2021, 52, 107–124. [Google Scholar] [CrossRef]
- Souza, E.W.; Borba, C.M.; Pereira, S.A.; Gremiao, I.D.F.; Langohr, I.M.; Oliveira, M.M.E.; de Oliveira, R.V.C.; da Cunha, C.R.; Zancope-Oliveira, R.M.; de Miranda, L.H.M.; et al. Clinical Features, Fungal Load, Coinfections, Histological Skin Changes, and Itraconazole Treatment Response of Cats with Sporotrichosis Caused by Sporothrix Brasiliensis. Sci Rep 2018, 8, 9074. [Google Scholar] [CrossRef] [PubMed]
- Pereira, S.A.; Passos, S.R.; Silva, J.N.; Gremiao, I.D.; Figueiredo, F.B.; Teixeira, J.L.; Monteiro, P.C.; Schubach, T.M. Response to Azolic Antifungal Agents for Treating Feline Sporotrichosis. Vet Rec 2010, 166, 290–294. [Google Scholar] [CrossRef] [PubMed]
- Miranda, L.H.M.; Silva, J.N.; Gremiao, I.D.F.; Menezes, R.C.; Almeida-Paes, R.; Dos Reis, E.G.; de Oliveira, R.V.C.; de Araujo, D.; Ferreiro, L.; Pereira, S.A. Monitoring Fungal Burden and Viability of Sporothrix Spp. in Skin Lesions of Cats for Predicting Antifungal Treatment Response. J Fungi (Basel) 2018, 4. [Google Scholar] [CrossRef] [PubMed]
- Marimon, R.; Serena, C.; Gené, J.; Cano, J.; Guarro, J. In Vitro Antifungal Susceptibilities of Five Species of Sporothrix. Antimicrob Agents Chemother 2008, 52, 732–734. [Google Scholar] [CrossRef] [PubMed]
- Koehler, A.; Pagani, D.M.; da Silva Hellwig, A.H.; Scroferneker, M.L. In-Vitro Antifungal Susceptibility of the Genus Sporothrix and Correlation with Treatment Options for Sporotrichosis: A Systematic Review. Reviews in Medical Microbiology 2021, 32, 219–227. [Google Scholar] [CrossRef]
- Nakasu, C.C.T.; Waller, S.B.; Ripoll, M.K.; Ferreira, M.R.A.; Conceição, F.R.; Gomes, A.d.R.; Osório, L.d.G.; de Faria, R.O.; Cleff, M.B. Feline Sporotrichosis: A Case Series of Itraconazole-Resistant Sporothrix Brasiliensis Infection. Braz J Microbiol 2021, 52, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Borba-Santos, L.P.; Gagini, T.; Ishida, K.; De Souza, W.; Rozental, S. Miltefosine Is Active against Sporothrix Brasiliensis Isolates with in Vitro Low Susceptibility to Amphotericin B or Itraconazole. Journal of Medical Microbiology 2015, 64, 415–422. [Google Scholar] [CrossRef] [PubMed]
- Borba-Santos, L.P.; Rodrigues, A.M.; Gagini, T.B.; Fernandes, G.F.; Castro, R.; De Camargo, Z.P.; Nucci, M.; Lopes-Bezerra, L.M.; Ishida, K.; Rozental, S. Susceptibility of Sporothrix Brasiliensis Isolates to Amphotericin B, Azoles, and Terbinafine. Medical Mycology 2015, 53, 178–188. [Google Scholar] [CrossRef] [PubMed]
- Silva, F.S.; Cunha, S.C.; Moraes, V.A.; Leite, J.S.; Ferreira, A.M. Refractory Feline Sporotrichosis: A Comparative Analysis on the Clinical, Histopathological, and Cytopathological Aspects. Braz J Vet Res 2022, 42. [Google Scholar] [CrossRef]
- Rocha, R.F.D.B.; Schubach, T.M.P.; Pereira, S.A.; Dos Reis, E.G.; Carvalho, B.W.; Gremiao, I.D.F. Refractory Feline Sporotrichosis Treated with Itraconazole Combined with Potassium Iodide. J Small Anim Pract 2018, 59, 720–721. [Google Scholar] [CrossRef]
- de Souza, C.P.; Lucas, R.; Ramadinha, R.H.; Pires, T.B. Cryosurgery in Association with Itraconazole for the Treatment of Feline Sporotrichosis. Journal of Feline Medicine and Surgery 2016, 18, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Santi, J.P.; Santos, C.R.G.R.; Santos, A.S.d.; Souza, H.J.M. Intranasal Clotrimazole Spray 1% Associated with Oral Itraconazole for Nasal Feline Sporotrichosis: A Case Series. Braz. J. Vet. Med. 2022, 44, e004821. [Google Scholar] [CrossRef]
- Ribeiro, D.S.C.; Machado, L.J.; Pereira, J.G.; de Souza Baptista, A.R.; da Rocha, E.M.D.S. Laser Therapy in the Treatment of Feline Sporotrichosis: A Case Series. Braz. J. Vet. Med. 2023, 45, e005822. [Google Scholar] [CrossRef]
- Cabral, F.V.; Sellera, F.P.; Ribeiro, M.S. Feline Sporotrichosis Successfully Treated with Methylene Blue-Mediated Antimicrobial Photodynamic Therapy and Low Doses of Itraconazole. Photodiagnosis and Photodynamic Therapy 2022, 40, 103154. [Google Scholar] [CrossRef] [PubMed]
- Gremiao, I.; Schubach, T.; Pereira, S.; Rodrigues, A.; Honse, C.; Barros, M. Treatment of Refractory Feline Sporotrichosis with a Combination of Intralesional Amphotericin B and Oral Itraconazole. Aust Vet J 2011, 89, 346–351. [Google Scholar] [CrossRef]
- Reis, E.G.; Schubach, T.M.; Pereira, S.A.; Silva, J.N.; Carvalho, B.W.; Quintana, M.S.; Gremiao, I.D. Association of Itraconazole and Potassium Iodide in the Treatment of Feline Sporotrichosis: A Prospective Study. Med Mycol 2016, 54, 684–690. [Google Scholar] [CrossRef]
- Sargeant, J.M.; Plishka, M.; Ruple, A.; Selmic, L.E.; Totton, S.C.; Vriezen, E.R. Quality of Reporting of Clinical Trials in Dogs and Cats: An Update. J Vet Intern Med 2021, 35, 1957–1971. [Google Scholar] [CrossRef]
- Burns, P.B.; Rohrich, R.J.; Chung, K.C. The Levels of Evidence and Their Role in Evidence-Based Medicine: Plastic and Reconstructive Surgery 2011, 128, 305–310. 128. [CrossRef]
- Lloret, A. The Process of Evidence-Based Medicine. Journal of Feline Medicine and Surgery 2009, 11, 529–529. [Google Scholar] [CrossRef] [PubMed]
- Reis, E.G.; Gremiao, I.D.; Kitada, A.A.; Rocha, R.F.; Castro, V.S.; Barros, M.B.; Menezes, R.C.; Pereira, S.A.; Schubach, T.M. Potassium Iodide Capsule Treatment of Feline Sporotrichosis. J Feline Med Surg 2012, 14, 399–404. [Google Scholar] [CrossRef]
- Boechat, J.S.; Oliveira, M.M.E.; Gremião, I.D.F.; Almeida-Paes, R.; Machado, A.C.d.S.; Zancopé-Oliveira, R.M.; Oliveira, R.d.V.C.; Morgado, D.S.; Corrêa, M.L.; Figueiredo, A.B.F.; et al. Sporothrix Brasiliensis and Feline Sporotrichosis in the Metropolitan Region of Rio de Janeiro, Brazil (1998–2018). JoF 2022, 8, 749. [Google Scholar] [CrossRef]
- Kaneko, J.J.; Harvey, J.W. Appendixes. In Clinical Biochemistry of Domestic Animals; Elsevier, 2008; pp. 873–904 ISBN 978-0-12-370491-7.
- Center, S.A. Interpretation of Liver Enzymes. Vet Clin North Am Small Anim Pract 2007, 37, 297–333. [Google Scholar] [CrossRef] [PubMed]
- Araújo, A.A.; Codeço, C.; Freitas, D.F.S.; De Macedo, P.M.; Pereira, S.A.; Gremião, I.D.F.; Coelho, F.C. Mathematical Model of the Dynamics of Transmission and Control of Sporotrichosis in Domestic Cats. PLoS ONE 2023, 18, e0272672. [Google Scholar] [CrossRef] [PubMed]
- Morgado, F.N.; Schubach, A.O.; Barros, M.B.L.; Conceição-Silva, F. The in Situ Inflammatory Profile of Lymphocutaneous and Fixed Forms of Human Sporotrichosis. Med Mycol 2011, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Conceição-Silva, F.; Morgado, F. Immunopathogenesis of Human Sporotrichosis: What We Already Know. JoF 2018, 4, 89. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Li, S.S.; Zhong, S.X.; Liu, Y.Y.; Yao, L.; Huo, S.S. Report of 457 Sporotrichosis Cases from Jilin Province, Northeast China, a Serious Endemic Region. J Eur Acad Dermatol Venereol 2013, 27, 313–318. [Google Scholar] [CrossRef]
- Gupta, M.; Narang, T.; Kaur, R.J.; Manhas, A.; Saikia, U.N.; Dogra, S. A Prospective Case Series Evaluating Efficacy and Safety of Combination of Itraconazole and Potassium Iodide in Rhinofacial Conidiobolomycosis. Int J Dermatol 2016, 55, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Mendiratta, V.; Karmakar, S.; Jain, A.; Jabeen, M. Severe Cutaneous Zygomycosis Due to Basidiobolus Ranarum in a Young Infant. Pediatr Dermatol 2012, 29, 121–123. [Google Scholar] [CrossRef] [PubMed]
- Miranda, L.H.M.; Meli, M.; Conceicao-Silva, F.; Novacco, M.; Menezes, R.C.; Pereira, S.A.; Sugiarto, S.; Dos Reis, E.G.; Gremiao, I.D.F.; Hofmann-Lehmann, R. Co-Infection with Feline Retrovirus Is Related to Changes in Immunological Parameters of Cats with Sporotrichosis. PLoS One 2018, 13, e0207644. [Google Scholar] [CrossRef]
- Rossi, C.N.; Odaguiri, J.; Larsson, C.E. Retrospective Assessment of the Treatment of Sporotrichosis in Cats and Dogs Using Itraconazole. Acta Scientiae Veterinariae 2013, 41. [Google Scholar]
- Mawby, D.I.; Whittemore, J.C.; Fowler, L.E.; Papich, M.G. Comparison of Absorption Characteristics of Oral Reference and Compounded Itraconazole Formulations in Healthy Cats. J Am Vet Med Assoc 2018, 252, 195–200. [Google Scholar] [CrossRef]
- Aceves, C.; Mendieta, I.; Anguiano, B.; Delgado-Gonzalez, E. Molecular Iodine Has Extrathyroidal Effects as an Antioxidant, Differentiator, and Immunomodulator. Int J Mol Sci 2021, 22. [Google Scholar] [CrossRef] [PubMed]
- Costa, R.O.; Macedo, P.M.; Carvalhal, A.; Bernardes-Engemann, A.R. Use of Potassium Iodide in Dermatology: Updates on an Old Drug. An Bras Dermatol 2013, 88, 396–402. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, S.; Ishikawa, S.; Ishii, E.; Koike, M.; Kaminaga, T.; Hamasaki, Y.; Sairenchi, T.; Kobashi, G.; Igawa, K. Anti-Inflammatory Effects of Potassium Iodide on SDS-Induced Murine Skin Inflammation. Journal of Investigative Dermatology 2020, 140, 2001–2008. [Google Scholar] [CrossRef] [PubMed]
- Duan, J.; Kang, J.; Deng, T.; Yang, X.; Chen, M. Exposure to DBP and High Iodine Aggravates Autoimmune Thyroid Disease Through Increasing the Levels of IL-17 and Thyroid-Binding Globulin in Wistar Rats. Toxicol Sci 2018, 163, 196–205. [Google Scholar] [CrossRef] [PubMed]
- Edinboro, C.H.; Scott-Moncrieff, J.C.; Glickman, L.T. Feline Hyperthyroidism: Potential Relationship with Iodine Supplement Requirements of Commercial Cat Foods. J Feline Med Surg 2010, 12, 672–679. [Google Scholar] [CrossRef] [PubMed]
- Kalarani, I.B.; Veerabathiran, R. Impact of Iodine Intake on the Pathogenesis of Autoimmune Thyroid Disease in Children and Adults. Ann Pediatr Endocrinol Metab 2022, 27, 256–264. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.; Kawashima, A.; Ishido, Y.; Yoshihara, A.; Oda, K.; Hiroi, N.; Ito, T.; Ishii, N.; Suzuki, K. Iodine Excess as an Environmental Risk Factor for Autoimmune Thyroid Disease. Int J Mol Sci 2014, 15, 12895–12912. [Google Scholar] [CrossRef] [PubMed]
- Taylor, P.N.; Albrecht, D.; Scholz, A.; Gutierrez-Buey, G.; Lazarus, J.H.; Dayan, C.M.; Okosieme, O.E. Global Epidemiology of Hyperthyroidism and Hypothyroidism. Nat Rev Endocrinol 2018, 14, 301–316. [Google Scholar] [CrossRef]
- Teng, W.; Shan, Z.; Teng, X.; Guan, H.; Li, Y.; Teng, D.; Jin, Y.; Yu, X.; Fan, C.; Chong, W.; et al. Effect of Iodine Intake on Thyroid Diseases in China. N Engl J Med 2006, 354, 2783–2793. [Google Scholar] [CrossRef]
Figure 1.
Inclusion flow chart illustrating the recruitment process of the cats, Rio de Janeiro, Brazil.
Figure 1.
Inclusion flow chart illustrating the recruitment process of the cats, Rio de Janeiro, Brazil.
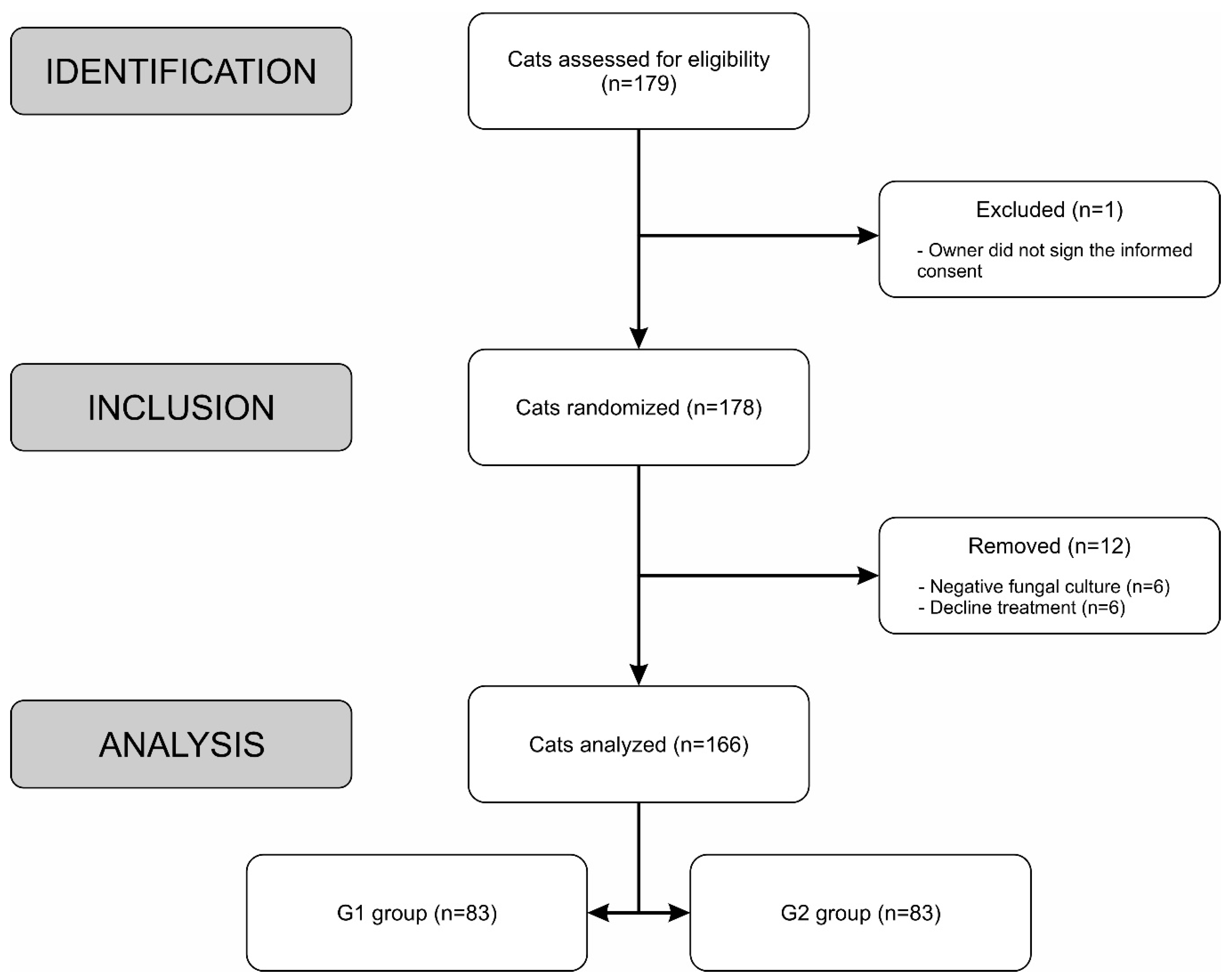
Figure 2.
(a) Cat with sporotrichosis with an extensive ulcer with hematic crust on the right lateral face and erosions on the nose and in the nasal philtrum before treatment. (b) The skin lesions have resolved after ITZ monotherapy. (c) Cat with spo- rotrichosis with an ulcerated nodule with presence of hematic crust on the nasal bridge and nasal planum. (d) The lesion has resolved, and the nasal bridge returned to normal after ITZ+KI treatment.
Figure 2.
(a) Cat with sporotrichosis with an extensive ulcer with hematic crust on the right lateral face and erosions on the nose and in the nasal philtrum before treatment. (b) The skin lesions have resolved after ITZ monotherapy. (c) Cat with spo- rotrichosis with an ulcerated nodule with presence of hematic crust on the nasal bridge and nasal planum. (d) The lesion has resolved, and the nasal bridge returned to normal after ITZ+KI treatment.

Figure 3.
Frequency of outcome of the 166 cats with sporotrichosis, according to treatment group, Rio de Janeiro, Brazil.
Figure 3.
Frequency of outcome of the 166 cats with sporotrichosis, according to treatment group, Rio de Janeiro, Brazil.
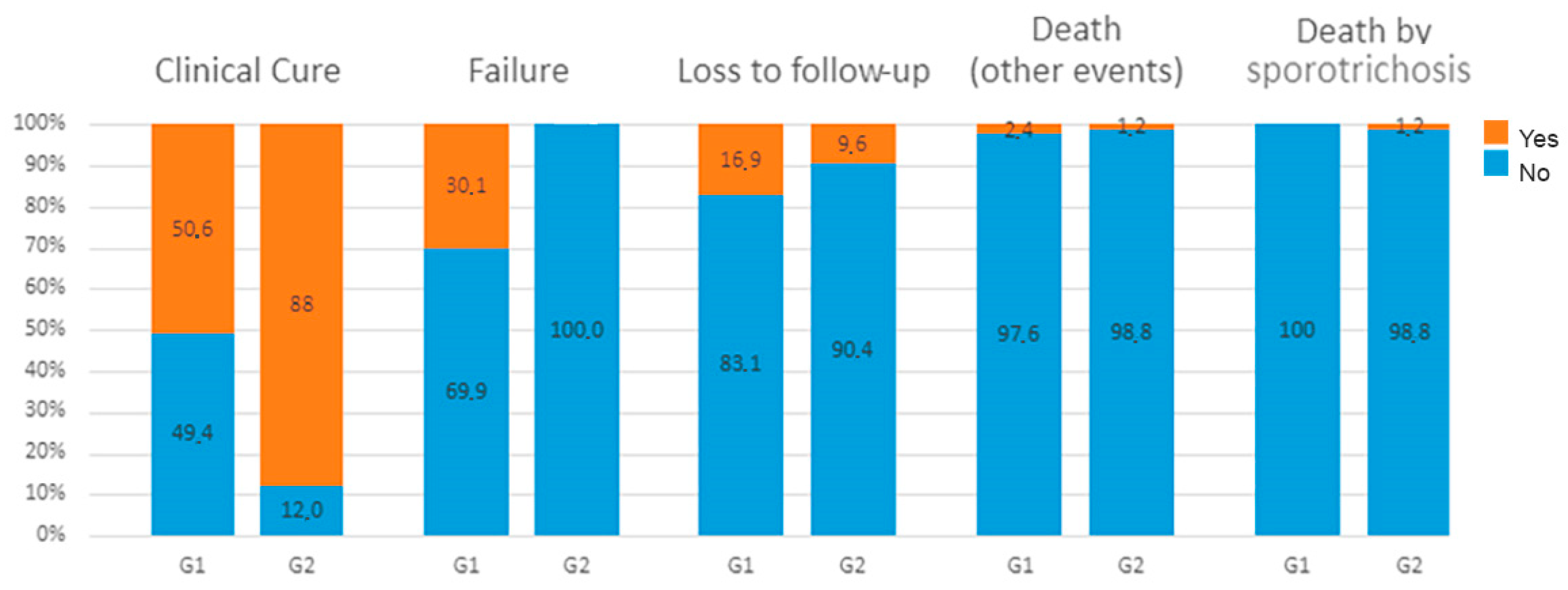
Figure 4.
Kaplan-Meier survival curves comparing treatment time between cats treated with ITZ (G1) and ITZ+KI (G2). The median time until cure was 14.9 weeks for G1 and 10 weeks for G2 cats. The tick marks indicate censured data.
Figure 4.
Kaplan-Meier survival curves comparing treatment time between cats treated with ITZ (G1) and ITZ+KI (G2). The median time until cure was 14.9 weeks for G1 and 10 weeks for G2 cats. The tick marks indicate censured data.
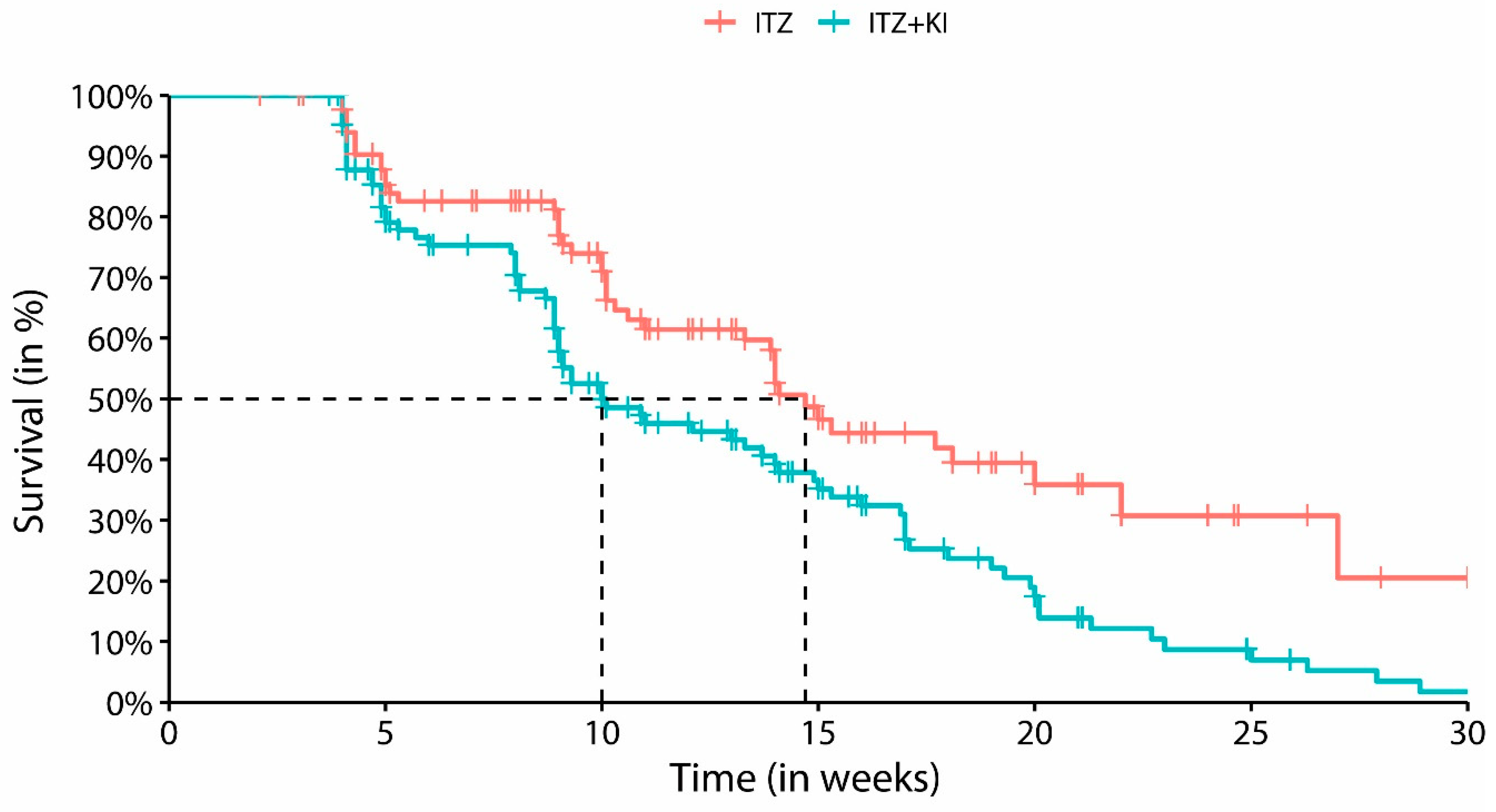
Table 1.
Clinical characteristics of the 166 cats with sporotrichosis, according to treatment group, Rio de Janeiro, Brazil.
Table 1.
Clinical characteristics of the 166 cats with sporotrichosis, according to treatment group, Rio de Janeiro, Brazil.
| Variables | G1-ITZ (N=83) |
G2-ITZ+KI (N=83) |
|---|---|---|
| Sex, n (%) | ||
| Male | 58 (69.9%) | 64 (77.1%) |
| Female | 25 (30.1%) | 19 (22.9%) |
| Clinical form, n (%) | ||
| Cutaneous | 51 (61.4%) | 56 (67.5%) |
| Cutaneous/Mucosal | 32 (38.6%) | 27 (32.5%) |
| Distribution of skin lesions, n (%) | ||
| L1 | 27 (32.5%) | 26 (31.3%) |
| L2 | 22 (26.5%) | 22 (26.5%) |
| L3 | 34 (41.0%) | 35 (42.2%) |
| Respiratory signs, n (%) | 30 (36.1%) | 23 (27.7%) |
| Lymphadenomegaly, n (%) | 69 (83.1%) | 67 (80.7%) |
| Lymphangitis, n (%) | 16 (19.3%) | 13 (15.7%) |
| Access outdoors, n (%) | 68 (81.9%) | 62 (74.1%) |
| Neutering, n (%) | 36 (43.4%) | 45 (54.2%) |
| FIV Ab and FeLV Ag *, n (%) | 13 (8.07%) | 18 (11.18%) |
| Age in months, MD (IQR) ** | 24 (24-48) | 24 (15-36) |
| Weight in Kg, MD (IQR) ** | 4 (3.5-4.7) | 4 (3.6-4.5) |
| Time interval between the onset ofclinical signs in weeks, MD (IQR) ** | 8 (4-12) | 8 (4-12) |
| Variables | G1-ITZ (N=83) |
G2-ITZ+KI (N=83) |
| Sex, n (%) | ||
| Male | 58 (69.9%) | 64 (77.1%) |
| Female | 25 (30.1%) | 19 (22.9%) |
| Clinical form, n (%) | ||
| Cutaneous | 51 (61.4%) | 56 (67.5%) |
| Cutaneous/Mucosal | 32 (38.6%) | 27 (32.5%) |
| Distribution of skin lesions, n (%) | ||
| L1 | 27 (32.5%) | 26 (31.3%) |
| L2 | 22 (26.5%) | 22 (26.5%) |
| L3 | 34 (41.0%) | 35 (42.2%) |
| Respiratory signs, n (%) | 30 (36.1%) | 23 (27.7%) |
| Lymphadenomegaly, n (%) | 69 (83.1%) | 67 (80.7%) |
| Lymphangitis, n (%) | 16 (19.3%) | 13 (15.7%) |
| Access outdoors, n (%) | 68 (81.9%) | 62 (74.1%) |
| Neutering, n (%) | 36 (43.4%) | 45 (54.2%) |
| FIV Ab and FeLV Ag *, n (%) | 13 (8.07%) | 18 (11.18%) |
| Age in months, MD (IQR) ** | 24 (24-48) | 24 (15-36) |
| Weight in Kg, MD (IQR) ** | 4 (3.5-4.7) | 4 (3.6-4.5) |
| Time interval between the onset of clinical signs in weeks, MD (IQR) ** |
8 (4-12) | 8 (4-12) |
* FIV = Feline immunodeficiency virus antibody; FeLV= Feline leukemia virus antigen. ** MD = Median, IQR= Interquartile range.
Table 2.
Potassium iodide dose adjustment in 28 cats from G2 group, Rio de Janeiro, Brazil.
| Variable | Cats with increasing dose | KI mg/kg | |||
|---|---|---|---|---|---|
| n | % | range | |||
| Persistent Lesion | Skin | 15 | 53.6 | 2.5-9.5 | |
| Mucosal | 2 | 7.1 | 3.1-8.1 | ||
| Skin and mucosal | 11 | 39.3 | 2.5-12.5 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



