Submitted:
23 December 2023
Posted:
25 December 2023
You are already at the latest version
Abstract
Different nutraceuticals are often considered by parents of infants and children with abdominal pain and disorders of the gut-brain interaction. Herb extracts and natural compounds have long been used in traditional medicine, but clinical pediatric trials are very limited. This narrative review based on relevant studies identified through Pubmed-Medline literature search updated to October 2023, focused on the effect of nutraceuticals in infantile colic, functional abdominal pain and irritable bowel syndrome in children and adolescents. Significant reduction of colic episodes and crying time was reported in two studies on fennel (seeds oil or tea), in three studies on different multiple herbal extracts (all including fennel), in one study on Mentha piperita, and in at least two double-blind randomized controlled studies on Lactobacillus reuteri DSM 17938 and Bifidobacterium lactis BB-12 (108 CFU/day for at least 21 days) in breast-fed infants. Compared to placebo, in children with functional abdominal pain or irritable bowel syndrome a significant reduction of pain was reported in two studies supplementing peppermint oil capsules or psyllium fibers, in one study on corn fiber cookies or partial hydrolysed guar gum or a specific multiple herbal extract (STW-5) or vitamin D supplementation. To date, there is a moderate certainty of evidence with a weak grade of recommendation for Lactobacillus reuteri DSM 17938 (108 CFU/day) for reducing pain intensity in children with functional abdominal pain and for Lactobacillus rhamnosus GG (1-3 x109 CFU twice daily) for reducing pain frequency and intensity in children with IBS. Further large and well-designed pediatric studies are needed to prove efficacy and safety of different herbal extracts and prolonged use of studied products in infants and children with pain disorders of the gut-brain interaction.
Keywords:
Nutraceutical
; Complementary therapies
; herbs
; fibers
; prebiotics
; probiotics
; abdominal pain
; irritable bowel syndrome
; infantile colic
; FGIDs
; FAPs
; disorders of the gut-brain interaction
INTRODUCTION
“Nutraceutical’ is a term introduced by Stephen Defelice in 1989 and identifies ‘a food or part of a food or a dietary supplement, that has a medical or health benefit, including the prevention and treatment of disease’.1
The medicinal and spiritual applications of plants, herbs and other natural compounds date back to many centuries earlier and was already reported in Egyptians, Romans, Mesopotamian and Greek civilizations and depicted some ancient artworks.2
In ancient Indian literature, Susruta and Charaka mention the use of cardamom, turmeric, ginger, cinnamon, and pepper for their medicinal properties. Some of these spices continue to be used for the treatment of multiple conditions including abdominal pain disorders throughout the world.3 The concept of nutraceuticals has evolved over time but still does not have a well-established definition worldwide.4 Nutraceuticals have been recently classified into traditional and non-traditional nutraceuticals. Traditional nutraceuticals include three subcategories: chemical constituents (nutrients, herbals, phytochemicals, polynsaturated fatty acids); probiotics and prebiotics; nutraceutical enzymes. The non-traditional nutraceuticals are fortified nutraceuticals and recombinant nutraceuticals.5 Nutraceutical compounds are generally considered as products, including minerals, vitamins, amino acids, vegetables or herbs that confer benefit to human health by improving functional, mental and physical activities.6
Despite their wide and long-term use, scientific information about nutraceuticals is limited, there are very few studies evaluating safety7 and efficacy8,9,10,11 and no international regulation regarding their marketing and dosing.5,12
Functional abdominal pain (FAP) disorders are disorders of the gut brain interaction (DGBI) and according to Rome IV criteria, include infantile colic, irritable bowel syndrome, functional dyspepsia and functional abdominal pain not otherwise specified.13,14, 8
They affect more than 20% of infants and children15 throughout the world, with a significant economic impact, decreased quality of life and long-term adverse outcomes.16
According to data published in 2015 from a multicenter trial in The Netherlands total annual costs per patient with FAPs calculated as the sum of medical and nonmedical costs were estimated to be more than 2500 euro, excluded initial diagnostic investigations.17
Despite an increasing recognition of multiple underlying factors, treatment is still challenging and symptoms often persist despite multiple non-pharmacological and pharmacological interventions, including probiotics, diets, spasmolitics, anti-depressants and cognitive-behavior approach. 18 Because of frequent lack of benefit of conventional treatment, almost 40% of parents of pediatric gastroenterology patients search for complementary and alternative medicine (CAM) for their child. More than 90% of these parents also considered important that paediatricians acquired knowledge and initiate CAM research.19
Likewise, a large number of adult patients with functional gastrointestinal disorders use CAMs. 20
The scope of this narrative review is to summarize current evidence of the nutraceuticals effects on abdominal pain disorders in infants and children and to provide health care professionals a practical guide for their possible clinical application.
LITERATURE SEARCH STRATEGY
Medline-PubMed was searched up to 31 October 2023 using the following MESH and Bolean terms: “herbs” OR “herbal supplements” OR “nutraceuticals” OR “ginger” OR “iberogast” OR “STW-5” OR “peppermint” OR “mentha piperita” OR “licorice” OR “liquorice” OR “fennel” OR “vitamins” OR “antioxidants” OR “polyphenols” AND (“functional gastrointestinal disorders” OR “abdominal pain” OR “infantile colic”), limited to English language and children (0-18 years). References of selected studies and reviews were also used to retrieve additional original studies.
NUTRACEUTICALS AND FAP/DGBI IN PEDIATRIC AGE
Only a very limited number of nutraceuticals have been assessed in clinical trials in infants and children with FAP/DGBI disorders.
Recent reviews have extensively covered studies evaluating fibers21,22 probiotics, prebiotics and synbiotics in different pediatric gastrointestinal disorders 23, 24, 8
This review focuses on nutraceuticals other than biotics and fibers in infants and children with infantile colic, functional dyspepsia, functional abdominal pain and irritable bowel syndrome. A summary of studies evaluating these included nutraceuticals in the above disorders in pediatric patients are reported in Table 1.
FENNEL
The fennel taxonomically identified as Foeniculum vulgare is a perennial plant used, in various forms, in traditional medicine for ages. The main component of fennel is the anethole, also known as estragole, that is extracted from its seeds and has a chemical structure similar to dopamine, with a reported relaxing effect on the intestinal smooth muscles.25
Two studies reported a beneficial effect of fennel on crying in colicky infants.
In 2003 a randomized placebo-controlled trial tested the effect of fennel seed oil emulsion in 125 infants (2 to 12 weeks of age) with infantile colic.26
Colic, as defined according to Wessel’s criteria, disappeared in 65% (40/62) of infants in the fennel group compared to 23% (14/59) of the placebo group (P < 0.01). A significant reduction of weekly crying time was also found in the treatment group compared with the placebo group [Absolute Risk Reduction (ARR) = 41% (95% CI 25 to 57), Number Needed to Treat (NNT) = 2 (95% CI 2 to 4)]. No side effects were reported in the two groups of infants. 26
A prospective randomised-controlled study involved 35 colicky infants who were treated with herbal (fenel) tea (35 ml three times a day for 7 days). Crying time significantly decreased from 5.11 ± 1.43 hours/day at baseline to 3.20 ± 1.23 hours/day after one week of intervention ( -1.51 hours/day vs. -0.09 hours/day in the control group, p < 0.001)27
GINGER
Ginger is the rhizome of the Zingiber officinale commonly used as food and in Asian traditional medicine for gastrointestinal symptoms.28
Ginger contains many different compounds, carbohydrates, lipids, terpenes, phenolic components, 6-gingerol,8-gingerol,10-gingerol and 6-shogaol which may act through cholinergic and calcium antagonist mechanisms, M3 and 5-HT3 receptors and synthesis of prostaglandins. 29,30
Ginger has been studied mostly for nausea, in pregnancy31, in adults and children on chemotherapy32,33 or post-surgery.34
Wu et al. showed that ginger accelerates gastric emptying and stimulates antral contractions in healthy adult individuals. 35
One study reported an antiemetic effect in children with gastroenteritis 36 but we did not find studies evaluating ginger in FAPs or DGBI in children.
Nonetheless, a survey about the use of complementary and alternative therapies in 100 children with abdominal pain disorders found that 11% of IBS children used ginger as treatment. 37
Ginger is generally considered as safe. The most common adverse effects, at the dosage above 5 g per day, are mouth and throat irritation, abdominal discomfort, heartburn, burping, and diarrhea. These symptoms may be avoided or reduced by taking ginger in capsule form.38
LICORICE
Licorice root (Glycyrrhiza glabra) is an ancient herb mostly used in Chinese medicine. It contains triterpentoid saponin glycyrrhizin, flavonoids, isoflavonoids, chalcones, cumarins, triterpenoids and sterols which have anti-inflammatory, immune, metabolic, endocrine and possible gastric activities. 39
After more than 2 weeks of intake, not deglycyrrhizinated licorice can cause hypertension and hypokalemia via mineralcorticoid effect (sodium and water retention). 40
There are currently no pediatric studies evaluating licorice as single supplementation in abdominal pain disorders.
PEPPERMINT
Peppermint is a species of mint, a perennial herb of the Lamiaceae family, used for ages for its presumed anti-inflammatory, analgesic and antispasmodic effects.41,42,43
Peppermint oil, obtained by steam distillation from the fresh leaves, is reported to induce smooth muscle relaxation (by blocking calcium channel44 or direct enteric nervous system effects); modulate visceral sensitivity (via transient receptor potential cation channels) and psychosocial distress; exert anti-microbial and anti-inflammatory effects. 45
Among the main compounds of peppermint are flavonoids and phenolic acids.
Moreover, menthol may act on Cajal interstitial cells, stimulate the production of prostaglandins and have a nociceptive action in the brain by the activation of GABA receptors type A. 46
A double-blind randomized crossover study enrolling 30 colicky infants showed that episodes of colic decreased in infants treated with Mentha piperita and with simethicone (from 3.9 per day at baseline to 1.6 per day after one week of intervention), duration of crying was similar between the two groups of treatment and colic disappeared in 40% of infants treated with Mentha piperita vs. 43% of infants on simethicone.47
In one pediatric randomized, double-blind, placebo-controlled study43, peppermint oil enteric coated capsules (1-2 capsules containing 187 mg, three times per day) were administered to 42 children (aged 8-12 years) with IBS for two weeks. The intervention group reported more frequently reduced symptoms (71% vs. 43%) and severity (79% vs. 16%) but not significant changes in Gastrointestinal Symptom Rating Scale.
Another randomized placebo-controlled trial compared the effects of peppermint oil (1-2 capsules of 187 mg, three times per day) (34 children), a symbiotic (Bacillus coagulans and fructooligosaccharide) (29 patients), and placebo (folic acid) (25 patients) for one month in children with FAPs (30 with IBS). The group who received peppermint oil had a significant reduction in severity of pain (as assessed on a one to ten scale), duration (minutes per day) and frequency of abdominal pain (episodes per week) compared to placebo and compared to symbiotic.48
No adverse events were noted. Two other studies performed in children with abdominal pain disorders pointed out that peppermint oil has no effect on microbiome composition49 or small bowel/colonic transit time.50
MULTIPLE HERBAL EXTRACTS
A prospective double-blind randomized controlled study including 68 colicky infants showed that colic disappeared in 19/33 (57%) infants taking herbal tea (up to 150 ml three times per day during episodes of colic, for 7 days) vs. 9/35 (26%) infants in the placebo group (p < 0.01). The tea contained extracts of chamomile (Matricaria chamomilla), vervain (Verbena officinalis), licorice (Glycyrrhiza glabra), fennel (Foenieulum vulgare), and balm-mint (Melissa officinalis) plus glucose and the placebo was made by glucose and natural flavors.51
A randomized, double-blind, placebo-controlled trial investigated the effect of a phytotherapeutic agent (combination of Matricariae recutita, Foeniculum vulgare and Melissa officinalis) in 88 colicky breastfed infants. After one week of intervention crying time was significantly reduced in more infants treated with the combination of herbs than in infants of the placebo group (85% vs, 49%, p < 0.005). The daily average crying time also decreased significantly more in the intervention group than in the placebo group (-124.3 min vs. -28.8 min, (p < 0.005) and these results were maintained fifteen days after the end of therapy (average crying time 82.1 min/day vs. 165.3 min/day, p<0.005), No side effects were reported.52
A recent open-label single-group study was conducted in 30 colicky infants (age 3-16 weeks) evaluating the effect of a product containing Carbo vegetabilis (vegetable charcoal), Prunus spinosa (Blackthorne), Carum carvi (Caraway), Matricaria chamomilla (Chamomile), Foeniculum vulgare (Fennel), Zingiber officinale (Ginger), Melissa officinalis (Lemon Balm), and Mentha piperita (Peppermint). The product was administered 1.25 ml orally during a colic episode and repeated after 120 minutes, if needed, Average daily crying time was recorded using a modified Barr’s diary and analysed after 7 and 14 days from recruitment. Daily crying time and flatulence significantly decreased (P < .05) with a reduction of ≥50% in 73% of infants by day 7 and in 80% by day 14. After stopping the intervention 40% of infants had a relapse of colic. 53
STW 5 (IBEROGAST)
STW-5 is a herbal combination of nine alcoholic extracts from Iberis amara, Angelicae radix, Cardui mariae fructus, Chelidonii herba, Liquiritiae radix, Matricariae flos, Melissae folium, Carvi fructus, and Menthae piperitae.54
This combination is supposed to have a synergic action on reducing gastrointestinal contraction and inflammation and stimulating gastric secretion.55
STW-5 was introduced to the market in the 1960s and in the last 30 years clinical trials have been conducted.56. 57
Among the nine herbal extracts, Iberis amara selectively inhibits muscarinic M3 receptors, while chelandine herb and chamomile flowers act on 5-HT4 and liquorice root on 5-HT3 receptors.
In the esophagus, it acts as a mucosal protector by increasing mucin and prostaglandin E2 secretion and increase the pressure of the LES (lower esophageal sphincter). 58
In the stomach, STW5 relaxes the fundus and corpus and increases antral region contractions. 59. 60
A prospective observational study included 980 children (age 3-14 years) with FGID (IBS in 43 %, FD in 26 %). STW-5 was administered 10-20 drops three times a day for 1 week. During the treatment period, an adapted gastrointestinal symptom score (GIS) decreased 76% from baseline score and 39% percent of children reported complete relief of their symptoms, with similar effect among different patients’ groups. Seven patients (0.7 %) reported adverse events (skin rash, nausea, vomiting, abdominal pain, and increased gastrointestinal complaints).54
In a retrospective study on 154 children (aged 4-18 years) affected by functional dyspepsia, STW5 showed significant benefit only in boys.61
FIBERS AND PREBIOTICS
In the last decades many dairy companies have added fibers/prebiotics, such as short-chain galactoligosaccharides and long-chain fructooligosaccharides in infant formulas to improve infant gut microbiota composition and possibly ameliorate digestive disturbs. However, since these formulas also present hydrolyzed proteins, reduced lactose content, modified fat and, eventually, probiotics, the clinical benefit in reducing crying and colic, reported in some studies, cannot be clearly correlated to the fibers. 21
We identified only two studies evaluating the effect of fibers in infantile colic 62, 63
Soy-polysaccharide was supplemented in a specific infant formula and assessed in 27 colicky infants (aged 2-8 weeks) in a placebo-controlled crossover trial for 9 days. No significant difference in daily crying time and fussing was found between the two groups.62
In the other randomized double-blind controlled study, 94 infants received galactoligosaccharides and polydextrose or a specific strain of probiotic (Lactobacillus GG) or placebo for the first two months of life. The group receiving prebiotics and probiotics reported significantly less frequent excessive crying compared to the placebo group (19% and 19% vs. 47%, p=0.02).63
We refer to three recent reviews15,21,22 for a detailed analysis of the role of fibers in children with abdominal pain and gastrointestinal disorders.
In brief, in children with FAPs, corn fiber cookies for two weeks 64 significantly reduced the frequency of abdominal pain compared to placebo. Likewise, partial hydrolysed guar gum supplementation in 60 children with chronic abdominal pain or IBS significantly decreased an IBS score, while improving stool consistency, compared to the placebo group. 65
Conversely, glucomannan did not show any significant benefit on abdominal pain. 66
In another randomized controlled trial on 71 children with IBS, inulin for 4 weeks was less effective than probiotics and synbiotics. 67
Psyllium fiber (6–12 g/day for 6 weeks) 68 reduced the mean number of abdominal pain episodes but not pain intensity.
More recently, the same dosage of psyllium supplementation significantly improved the IBS severity scoring scale and showed a higher remission rate, compared to placebo. 69
PROBIOTICS
As reported by the 2023 ESPGHAN position paper on probiotics for the management of pediatric gastrointestinal disorders 23, in infantile colic there is a moderate certainty of evidence and a weak grade of recommendation for Lactobacillus reuteri DSM 17938 and Bifidobacterium lactis BB-12 (108 CFU/day for at least 21 days) in breastfed infants. No recommendation can currently be made for or against probiotics in formula-fed infants or for preventing infantile colic. There is also a moderate certainty of evidence and a weak grade of recommendation for Lactobacillus reuteri DSM 17938 (108 CFU/day) for reducing pain intensity in children with FAPs and for L. rhamnosus GG (1-3 x109 CFU twice daily) for reducing pain frequency and intensity in children with IBS. 23
SYNBIOTICS
The recent ESPGHAN position paper on the use of synbiotics for the management of children with gastrointestinal disorders 70 concluded that currently no recommendation can be formulated on the use of any specific symbiotic preparation in the treatment of infant colic, FAP or IBS.
VITAMINS AND ANTI-OXIDANTS
We identified only one pediatric study assessing the effect of vitamin on abdominal pain in children. A randomized controlled trail in 112 adolescents with IBS and vitamin D deficiency showed that oral vitamin D3 2000IU/day for 6 months normalized the vitamin D level and significantly improved different IBS symptom score systems (IBS-SSS, IBS-QoL and total score) compared to the group receiving placebo. 71
Vitamin D may act by reducing inflammation by immune modulation and by regulating the synthesis of serotonin. 72
LIMITATIONS OF THIS REVIEW
We are aware of some limitations of this review. First, we did not perform a systematic review and we limited the literature search to Medline and English language. However, we retrieve additional studies by references of selected articles and recent reviews to reduce the chance to miss original studies. Second, many herbal extracts have long been used in traditional medicine but data are not reported in clinical trials. Third, we aimed to help health care professionals orienting in the nutraceutical field for children who are affected from pain disorder of the gut-brain interaction but we did not provide any clear recommendation. Likewise, the European Medicine Agency currently does not recommend any herbal product for gastrointestinal disorders in the pediatric population because of lack of adequate data on efficacy and safety.73
Caution and medical supervision on the use of nutraceuticals in pediatric subjects have also been advocated in other recent reviews. 15, 10, 8, 22
CONCLUSIONS
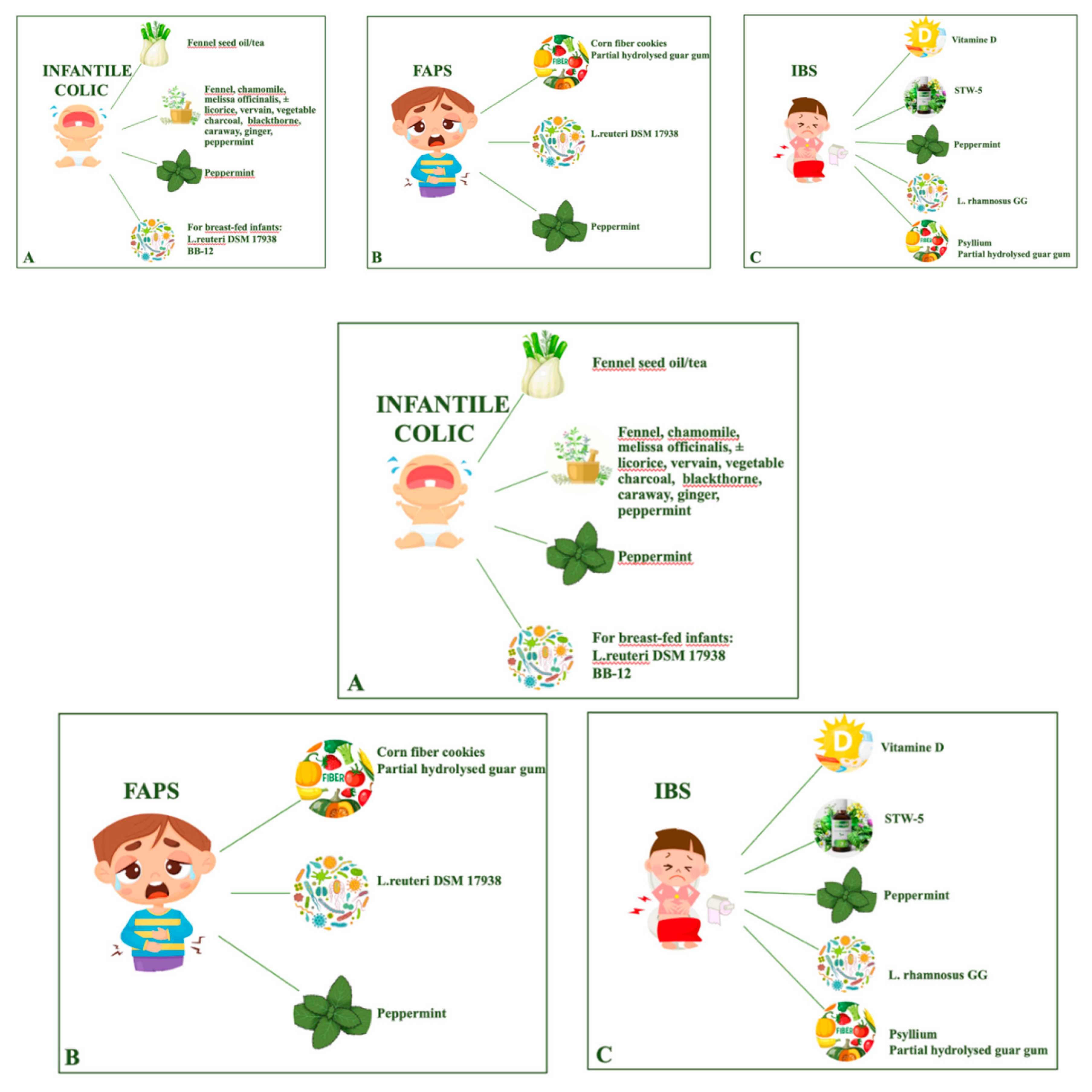
Nutraceuticals are often considered by parents to treat their child with infantile colic and abdominal pain disorders. However, there is a very limited number of studies assessing efficacy and tolerance of herbs, spices and nutritional supplements in children with these conditions. A growing evidence of efficacy in reducing infant colic episodes and crying time is emerging for fennel (seeds oil or tea or in different multiple herbal extracts), for Lactobacillus reuteri DSM 17938 and Bifidobacterium lactis BB-12, in breast-fed infants. In children and adolescents with functional abdominal pain or irritable bowel syndrome, reduction of pain was reported in patients supplemented with Lactobacillus reuteri DSM 17938 or Lactobacillus rhamnosus GG and in two studies using peppermint oil capsules or psyllium fibers; the benefit of corn fiber cookies or partial hydrolysed guar gum or a specific multiple herbal extract (STW-5) or vitamin D supplementation was demonstrated only in one study for each product (Figure 1). No recommendation can currently be provided for other nutraceuticals and possible adverse effects should always be considered. Moreover, current pediatric studies present small sample size, heterogeneity in the population recruited, product and dosage used, outcome measures, lack of long-term assessment of efficacy and safety.
Author Contributions
S.S., M.C., M.A and L.P. contributed to conception and design of the review, collection and interpretation of data, drafting the article and approval of the manuscript; S.S. and D.C. contributed to the literature search, interpretation of data, drafting the article and approval of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This review received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors have no conflict of interest to declare.
References
- DeFelice SL. The nutraceutical revolution: its impact on food industry R&D. Trends Food Sci Technol. 1995;6(2):59-61. [CrossRef]
- Ruchi S, Amanjot K, Sourav T, Keerti B, Sujit B. Role of nutraceuticals in health care: A review. International Journal of Green Pharmacy. Jul-Sep 2017 (Suppl);11 (3): S385. [CrossRef]
- Fifi A, Axelrod C, Chakraborty P, Saps M. Herbs and Spices in the Treatment of Functional Gastrointestinal Disorders: A Review of Clinical Trials. Nutrients. 2018;10(11):1715. [CrossRef]
- Kalra EK. Nutraceutical-definition and introduction. AAPS PharmSci. 2003;5(3):27-28. [CrossRef]
- Helal NA, Eassa HA, Amer AM, Eltokhy MA, Edafiogho I, Nounou MI. Nutraceuticals’ Novel Formulations: The Good, the Bad, the Unknown and Patents Involved. Recent Pat Drug Deliv Formul. 2019;13(2):105-156. [CrossRef]
- Dickinson A. History and overview of DSHEA. Fitoterapia. 2011;82(1):5-10. [CrossRef]
- Ronis MJJ, Pedersen KB, Watt J. Adverse Effects of Nutraceuticals and Dietary Supplements. Annu Rev Pharmacol Toxicol. 2018;58:583-601. [CrossRef]
- Corsello A, Scatigno L, Fiore G, et al. Nutraceuticals and biotics in pediatric gastrointestinal disorders. Eur J Clin Nutr. Published online October 24, 2023. [CrossRef]
- Puri V, Nagpal M, Singh I, et al. A Comprehensive Review on Nutraceuticals: Therapy Support and Formulation Challenges. Nutrients. 2022;14(21):4637. Published 2022 Nov 3. [CrossRef]
- Chopra AS, Lordan R, Horbańczuk OK, et al. The current use and evolving landscape of nutraceuticals. Pharmacol Res. 2022;175:106001. [CrossRef]
- Chakraborty PS, Daniel R, Navarro FA. Non-pharmacologic approaches to treatment of pediatric functional abdominal pain disorders. Front Pediatr. 2023;11:1118874. Published 2023 Jun 15. [CrossRef]
- Vettorazzi A, López de Cerain A, Sanz-Serrano J, Gil AG, Azqueta A. European Regulatory Framework and Safety Assessment of Food-Related Bioactive Compounds. Nutrients. 2020;12(3):613. Published 2020 Feb 26. [CrossRef]
- Benninga MA, Faure C, Hyman PE, St James Roberts I, Schechter NL, Nurko S. Childhood Functional Gastrointestinal Disorders: Neonate/Toddler. Gastroenterology. Published online February 15, 2016. [CrossRef]
- Hyams JS, Di Lorenzo C, Saps M, Shulman RJ, Staiano A, van Tilburg M. Functional Disorders: Children and Adolescents. Gastroenterology. Published online February 15, 2016. [CrossRef]
- de Bruijn CM, Rexwinkel R, Gordon M, Sinopoulou V, Benninga MA, Tabbers MM. Dietary interventions for functional abdominal pain disorders in children: a systematic review and meta-analysis. Expert Rev Gastroenterol Hepatol. 2022;16(4):359-371. [CrossRef]
- Saps M, Velasco-Benitez CA, Langshaw AH, Ramírez-Hernández CR. Prevalence of Functional Gastrointestinal Disorders in Children and Adolescents: Comparison Between Rome III and Rome IV Criteria. J Pediatr. 2018;199:212-216. [CrossRef]
- Hoekman DR, Rutten JM, Vlieger AM, Benninga MA, Dijkgraaf MG. Annual Costs of Care for Pediatric Irritable Bowel Syndrome, Functional Abdominal Pain, and Functional Abdominal Pain Syndrome. J Pediatr. 2015;167(5):1103-8.e2. [CrossRef]
- Rexwinkel R, Vlieger AM, Saps M, Tabbers MM, Benninga MA. A therapeutic guide on pediatric irritable bowel syndrome and functional abdominal pain-not otherwise specified. Eur J Pediatr. 2022;181(7):2603-2617. [CrossRef]
- Vlieger AM, Blink M, Tromp E, Benninga MA. Use of complementary and alternative medicine by pediatric patients with functional and organic gastrointestinal diseases: results from a multicenter survey. Pediatrics. 2008;122(2):e446-e451. [CrossRef]
- Deutsch JK, Levitt J, Hass DJ. Complementary and Alternative Medicine for Functional Gastrointestinal Disorders. Am J Gastroenterol. 2020;115(3):350-364. [CrossRef]
- Salvatore S, Battigaglia MS, Murone E, Dozio E, Pensabene L, Agosti M. Dietary Fibers in Healthy Children and in Pediatric Gastrointestinal Disorders: A Practical Guide. Nutrients. 2023;15(9):2208. Published 2023 May 6. [CrossRef]
- Pop D, Pop RS, Farcău D. The Use of Fibers, Herbal Medicines and Spices in Children with Irritable Bowel Syndrome: A Narrative Review. Nutrients. 2023;15(20):4351. Published 2023 Oct 12. [CrossRef]
- Szajewska H, Berni Canani R, Domellöf M, et al. Probiotics for the Management of Pediatric Gastrointestinal Disorders: Position Paper of the ESPGHAN Special Interest Group on Gut Microbiota and Modifications. J Pediatr Gastroenterol Nutr. 2023;76(2):232-247. [CrossRef]
- Gordon M, Wallace C, Sinopoulou V, et al. Probiotics for management of functional abdominal pain disorders in children. Cochrane Database of Systematic Reviews 2023, Issue 2. Art. No.: CD012849. [CrossRef]
- Portincasa P, Bonfrate L, Scribano ML, et al. Curcumin and Fennel Essential Oil Improve Symptoms and Quality of Life in Patients with Irritable Bowel Syndrome. J Gastrointestin Liver Dis. 2016;25(2):151-157. [CrossRef]
- Alexandrovich I, Rakovitskaya O, Kolmo E, Sidorova T, Shushunov S. The effect of fennel (Foeniculum Vulgare) seed oil emulsion in infantile colic: a randomized, placebo-controlled study. Altern Ther Health Med. 2003;9(4):58-61.
- Arikan D, Alp H, Gözüm S, Orbak Z, Cifçi EK. Effectiveness of massage, sucrose solution, herbal tea or hydrolysed formula in the treatment of infantile colic. J Clin Nurs. 2008;17(13):1754-1761. [CrossRef]
- van Tilburg MAL, Palsson OS, Ringel Y, Whitehead WE. Is ginger effective for the treatment of irritable bowel syndrome? A double blind randomized controlled pilot trial. Complement Ther Med. 2014;22(1):17-20. [CrossRef]
- Zehsaz F, Farhangi N, Mirheidari L. Clinical immunology The effect of Zingiber officinale R. rhizomes (ginger) on plasma pro-inflammatory cytokine levels in well-trained male endurance runners. Cent Eur J Immunol. 2014;2:174-180. [CrossRef]
- Pertz H, Lehmann J, Roth-Ehrang R, Elz S. Effects of Ginger Constituents on the Gastrointestinal Tract: Role of Cholinergic M 3 and Serotonergic 5-HT 3 and 5-HT 4 Receptors. Planta Med. 2011;77(10):973-978. [CrossRef]
- Viljoen E, Visser J, Koen N, Musekiwa A. A systematic review and meta-analysis of the effect and safety of ginger in the treatment of pregnancy-associated nausea and vomiting. Nutr J. 2014;13(1):20. [CrossRef]
- Choi J, Lee J, Kim K, Choi HK, Lee SA, Lee HJ. Effects of Ginger Intake on Chemotherapy-Induced Nausea and Vomiting: A Systematic Review of Randomized Clinical Trials. Nutrients. 2022;14(23):4982. [CrossRef]
- Pillai AK, Sharma KK, Gupta YK, Bakhshi S. Anti-emetic effect of ginger powder versus placebo as an add-on therapy in children and young adults receiving high emetogenic chemotherapy: Ginger as Antiemetic. Pediatr Blood Cancer. 2011;56(2):234-238. [CrossRef]
- Soltani E, Jangjoo A, Afzal Aghaei M, Dalili A. Effects of preoperative administration of ginger (Zingiber officinale Roscoe) on postoperative nausea and vomiting after laparoscopic cholecystectomy. J Tradit Complement Med. 2018;8(3):387-390. [CrossRef]
- Wu KL, Rayner CK, Chuah SK, et al. Effects of ginger on gastric emptying and motility in healthy humans: Eur J Gastroenterol Hepatol. 2008;20(5):436-440. [CrossRef]
- Nocerino R, Cecere G, Micillo M, et al. Efficacy of ginger as antiemetic in children with acute gastroenteritis: a randomised controlled trial. Aliment Pharmacol Ther. 2021;54(1):24-31. [CrossRef]
- Ciciora SL, Yildiz VO, Jin WY, Zhao B, Saps M. Complementary and Alternative Medicine Use in Pediatric Functional Abdominal Pain Disorders at a Large Academic Center. J Pediatr. 2020;227:53-59.e1. [CrossRef]
- Cherry RN, Blanchard SS, Chogle A, Santucci NR, Mehta K, Russell AC. Herbal Approaches to Pediatric Functional Abdominal Pain. Children. 2022;9(8):1266. [CrossRef]
- Yang R, Yuan BC, Ma YS, Zhou S, Liu Y. The anti-inflammatory activity of licorice, a widely used Chinese herb. Pharm Biol. 2017;55(1):5-18. [CrossRef]
- Nazari S, Rameshrad M, Hosseinzadeh H. Toxicological Effects of Glycyrrhiza glabra (Licorice): A Review. Phytother Res. 2017;31(11):1635-1650. [CrossRef]
- Anwar F, Abbas A, Mehmood T, Gilani A, Rehman N. Mentha: A genus rich in vital nutra-pharmaceuticals—A review. Phytother Res. 2019;33(10):2548-2570. [CrossRef]
- Ulbricht C, Costa D, M Grimes Serrano J, et al. An Evidence-Based Systematic Review of Spearmint by the Natural Standard Research Collaboration. J Diet Suppl. 2010;7(2):179-215. [CrossRef]
- Kline RM, Kline JJ, Di Palma J, Barbero GJ. Enteric-coated, pH-dependent peppermint oil capsules for the treatment of irritable bowel syndrome in children. J Pediatr. 2001;138(1):125-128. [CrossRef]
- Amato A, Liotta R, Mulè F. Effects of menthol on circular smooth muscle of human colon: Analysis of the mechanism of action. Eur J Pharmacol. 2014;740:295-301. [CrossRef]
- Mahendran G, Rahman L. Ethnomedicinal, phytochemical and pharmacological updates on Peppermint ( Mentha × piperita L.)—A review. Phytother Res. 2020;34(9):2088-2139. [CrossRef]
- Saps M, Miranda A. Gastrointestinal Pharmacology. In: Greenwood-Van Meerveld B, ed. Gastrointestinal Pharmacology. Vol 239. Handbook of Experimental Pharmacology. Springer International Publishing; 2017:147-176. [CrossRef]
- Alves JG, de Brito Rde C, Cavalcanti TS. Effectiveness of Mentha piperita in the Treatment of Infantile Colic: A Crossover Study. Evid Based Complement Alternat Med. 2012;2012:981352. [CrossRef]
- Asgarshirazi M, Shariat M, Dalili H. Comparison of the Effects of pH-Dependent Peppermint Oil and Synbiotic Lactol (Bacillus coagulans + Fructooligosaccharides) on Childhood Functional Abdominal Pain: A Randomized Placebo-Controlled Study. Iran Red Crescent Med J. 2015;17(4). [CrossRef]
- Thapa S, Luna RA, Chumpitazi BP, et al. Peppermint oil effects on the gut microbiome in children with functional abdominal pain. Clin Transl Sci. 2022;15(4):1036-1049. [CrossRef]
- Shulman RJ, Chumpitazi BP, Abdel-Rahman SM, Garg U, Musaad S, Kearns GL. Randomised trial: Peppermint oil (menthol) pharmacokinetics in children and effects on gut motility in children with functional abdominal pain [published correction appears in Br J Clin Pharmacol. 2022 Dec;88(12):5436]. Br J Clin Pharmacol. 2022;88(3):1321-1333. [CrossRef]
- Weizman Z, Alkrinawi S, Goldfarb D, Bitran C. Efficacy of herbal tea preparation in infantile colic. J Pediatr. 1993;122(4):650-652. [CrossRef]
- Savino F, Cresi F, Castagno E, Silvestro L, Oggero R. A randomized double-blind placebo-controlled trial of a standardized extract of Matricariae recutita, Foeniculum vulgare and Melissa officinalis (ColiMil®) in the treatment of breastfed colicky infants. Phytother Res. 2005;19(4):335-340. [CrossRef]
- Evans C, Lorentz WP. Efficacy and Safety of a Colic Relief Remedy in Infantile Colic. Glob Pediatr Health. 2022;9:2333794X221100810. Published 2022 Aug 1. [CrossRef]
- Michael R, Bettina V, Eckehard L. Functional gastrointestinal disorders in children: Effectivity, safety, and tolerability of the herbal preparation STW-5 (Iberogast®) in general practice. Complement Ther Med. 2022;71:102873. [CrossRef]
- Ulrich-Merzenich G, Welslau L, Aziz-Kalbhenn H, Kelber O, Shcherbakova A. Synergy quantifications to identify individual contributions of combination partners to the overall activity – The example of STW 5. Phytomedicine. 2019;60:153013. [CrossRef]
- Ottillinger B, Storr M, Malfertheiner P, Allescher HD. STW 5 (Iberogast®)—a safe and effective standard in the treatment of functional gastrointestinal disorders. Wien Med Wochenschr. 2013;163(3-4):65-72. [CrossRef]
- Abdel-Aziz H, Kelber O, Lorkowski G, Storr M. Evaluating the Multitarget Effects of Combinations through Multistep Clustering of Pharmacological Data: the Example of the Commercial Preparation Iberogast. Planta Med. 2017;83(14/15):1130-1140. [CrossRef]
- Khayyal M, El-Ghazaly M, Kenawy S, et al. Antiulcerogenic Effect of Some Gastrointestinally Acting Plant Extracts and their Combination. Arzneimittelforschung. 2011;51(07):545-553. [CrossRef]
- Hohenester B, Rühl A, Kelber O, Schemann M. The herbal preparation STW5 (lberogast) has potent and region-specific effects on gastric motility. Neurogastroenterol Motil. 2004;16(6):765-773. [CrossRef]
- Schemann M, Michel K, Zeller F, Hohenester B, Rühl A. Region-specific effects of STW 5 (Iberogast) and its components in gastric fundus, corpus and antrum. Phytomedicine. 2006;13 Suppl 5:90-99. [CrossRef]
- Légeret C, Stienen Y, Furlano R, Köhler H. Effectivity of treatment for children with functional dyspepsia. Sci Rep. 2022;12(1):1467. [CrossRef]
- Treem WR, Hyams JS, Blankschen E, Etienne N, Paule CL, Borschel MW. Evaluation of the effect of a fiber-enriched formula on infant colic. J Pediatr. 1991;119(5):695-701. [CrossRef]
- Pärtty A, Luoto R, Kalliomäki M, Salminen S, Isolauri E. Effects of early prebiotic and probiotic supplementation on development of gut microbiota and fussing and crying in preterm infants: a randomized, double-blind, placebo-controlled trial. J Pediatr. 2013;163(5):1272-7.e72. [CrossRef]
- Feldman W, McGrath P, Hodgson C, Ritter H, Shipman RT. The use of dietary fiber in the management of simple, childhood, idiopathic, recurrent, abdominal pain. Results in a prospective, double-blind, randomized, controlled trial. Am J Dis Child. 1985;139(12):1216-1218. [CrossRef]
- Romano C, Comito D, Famiani A, Calamarà S, Loddo I. Partially hydrolyzed guar gum in pediatric functional abdominal pain. World J Gastroenterol. 2013;19(2):235-240. [CrossRef]
- Horvath A, Dziechciarz P, Szajewska H. Glucomannan for abdominal pain-related functional gastrointestinal disorders in children: a randomized trial. World J Gastroenterol. 2013;19(20):3062-3068. [CrossRef]
- Baştürk A, Artan R, Yılmaz A. Efficacy of synbiotic, probiotic, and prebiotic treatments for irritable bowel syndrome in children: A randomized controlled trial. Turk J Gastroenterol. 2016;27(5):439-443. [CrossRef]
- Shulman RJ, Hollister EB, Cain K, et al. Psyllium Fiber Reduces Abdominal Pain in Children With Irritable Bowel Syndrome in a Randomized, Double-Blind Trial. Clin Gastroenterol Hepatol. 2017;15(5):712-719.e4. [CrossRef]
- Menon J, Thapa BR, Kumari R, Puttaiah Kadyada S, Rana S, Lal SB. Efficacy of Oral Psyllium in Pediatric Irritable Bowel Syndrome: A Double-Blind Randomized Control Trial. J Pediatr Gastroenterol Nutr. 2023;76(1):14-19. [CrossRef]
- Hojsak I, Kolaček S, Mihatsch W, et al. Synbiotics in the Management of Pediatric Gastrointestinal Disorders: Position Paper of the ESPGHAN Special Interest Group on Gut Microbiota and Modifications. J Pediatr Gastroenterol Nutr. 2023;76(1):102-108. [CrossRef]
- El Amrousy D, Hassan S, El Ashry H, Yousef M, Hodeib H. Vitamin D supplementation in adolescents with irritable bowel syndrome: Is it useful? A randomized controlled trial. Saudi J Gastroenterol. 2018;24(2):109-114. [CrossRef]
- Yu XL, Li CP, He LP. Vitamin D may alleviate irritable bowel syndrome by modulating serotonin synthesis: a hypothesis based on recent literature. Front Physiol. 2023;14:1152958. Published 2023 Jul 27. [CrossRef]
- European Medicine Agency. European Union herbal monographs: Overview of recommendations for the uses of herbal medicinal products in the paediatric population. Last updated: 15 March 2023. EMA/HMPC/228356/2012, Rev. 2. Committee on Herbal Medicinal Products (HMPC).
Figure 1.
Evidence of nutraceuticals efficacy in Infantile Colic (A), Functional Abdominal Pain (B), Irritable Bowel Syndrome (C).
Figure 1.
Evidence of nutraceuticals efficacy in Infantile Colic (A), Functional Abdominal Pain (B), Irritable Bowel Syndrome (C).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



