Submitted:
19 December 2023
Posted:
20 December 2023
You are already at the latest version
Abstract
The movement toward prevention trials in people at-risk for Parkinson’s is rapidly becoming a reality. The authors of this article include a genetically at-risk advocate with the LRRK2 G2019S variant and two patients with rapid eye movement sleep behavior disorder (RBD), one of whom has now been diagnosed with Parkinson’s disease (PD). These authors participated as speakers, panelists, and moderators in the “Planning for Prevention of Parkinson’s: A Trial Design Forum” hosted by Massachusetts General Hospital in 2021 and 2022. Other authors include a young onset person with Parkinson’s (PwP) and retired family physician, an expert in patient engagement in Parkinson’s, and early career and veteran movement disorders clinician researchers. Several themes emerged from the at-risk participant voice concerning the importance of early intervention, the legitimacy of their input in decision-making, and the desire for transparent communication and feedback throughout the entire research study process. Challenges and opportunities in the current environment include lack of awareness among primary care physicians and general neurologists about PD risk, legal and psychological implications of risk disclosure, limited return of individual research study results, and undefined engagement and integration of individuals at-risk into the broader Parkinson’s community. Incorporating the perspectives of individuals at-risk as well as those living with PD at this early stage of prevention trial development is crucial to success.
Keywords:
Parkinson's Disease
; Prevention
; Risk
; Patient Advocacy
; Patient Engagement
; REM Sleep Behavior Disorder
; Hyposmia
; LRRK2
; GBA
INTRODUCTION
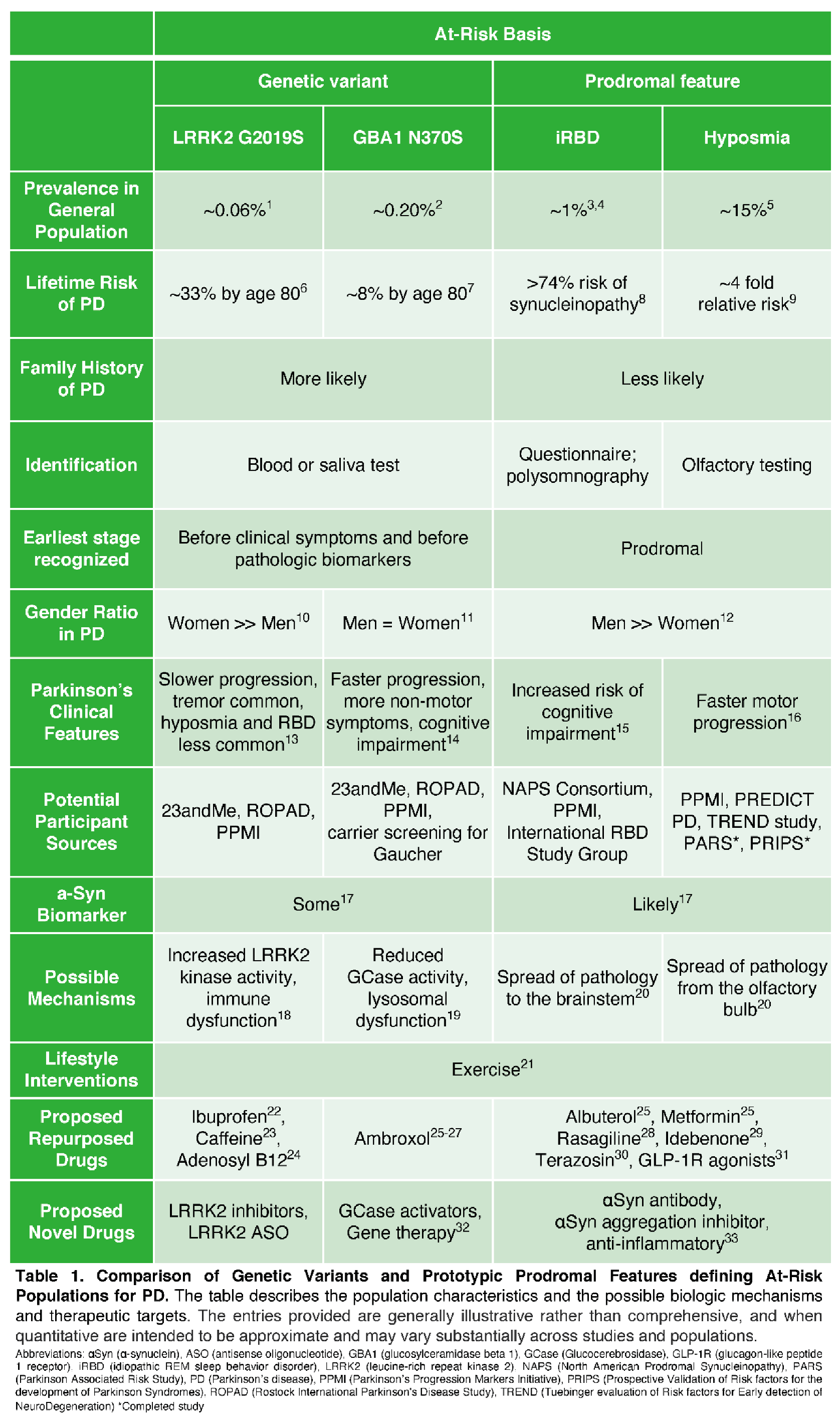
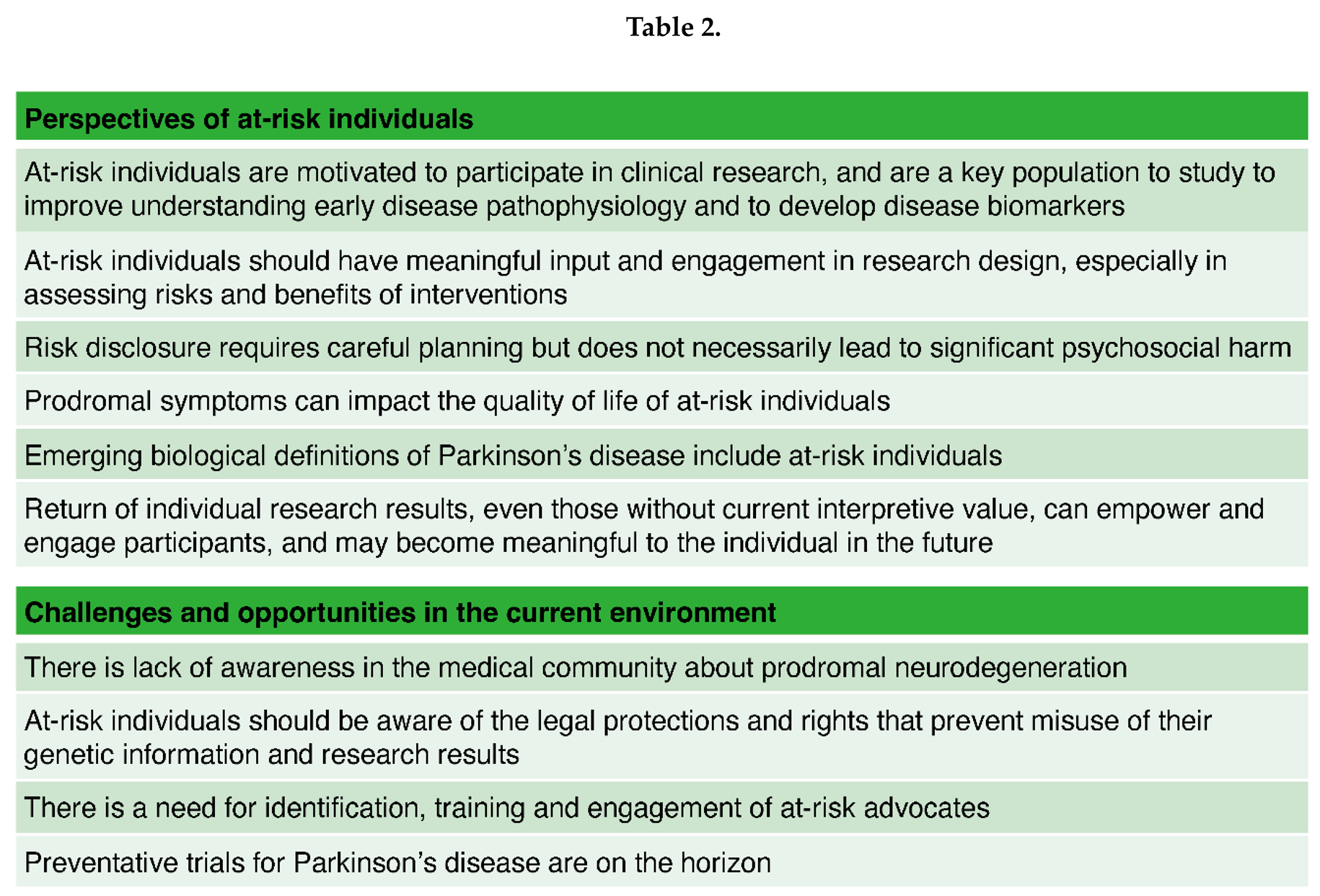
The cascade of events that leads to neurodegeneration takes decades to manifest into overt cardinal motor symptoms of Parkinson’s disease (PD). As a result, there are millions of people living across the globe who are unaware they have an underlying biological predisposition that may eventually lead to PD. Prevention can be a particularly important and urgent concern for the genetically at-risk population and those diagnosed with rapid eye movement sleep behavior disorder (RBD) or other prodromal features that substantially increase the risk of developing PD and other synucleinopathies. [Table 1] [1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33] There is a growing consensus within the PD community that these at-risk individuals represent a unique population to participate in clinical trials to delay or prevent the phenoconversion to manifest Parkinson’s and to address early symptoms. Arguably, one of the most imperative future directions for PD preventative trials is prioritizing an effective participant engagement culture. Gaining the perspective of this group should never be an afterthought. Since at-risk individuals may have early PD or the potential to have parkinsonism, but do not yet have a formal diagnosis of PD or a related neurodegenerative synucleinopathy, several considerations are unique to this participant group that are different from those of traditional advocates comprising people with Parkinson’s (PwP) and care partners. Additionally, the research landscape is rapidly evolving, with the emergence of participant-driven and precision medicine models, the systematic validation through the Michael J. Fox Foundation’s Parkinson’s Progression Markers Initiative (PPMI) study of an alpha-synuclein seed amplification assay that can detect abnormal biology even before dopamine transporter (DaT) scans,[17] and the proposal of a flexible new biologic definition and staging system in Parkinson’s.[34,35,36,37] Thus, it is paramount that identified at-risk individuals are meaningfully involved in the clinical research decision-making process throughout trial design, implementation, and dissemination of findings. [Table 2]
PERSPECTIVES OF AT-RISK INDIVIDUALS
Preventing Parkinson’s is an Important Objective
In June of 2019, the Michael J. Fox Foundation released a report with critical findings about the annual economic burden of Parkinson’s disease. The total cost of PD to individuals, families, and the United States government is $51.9 billion every year, with $25.4 billion attributable to direct medical costs (e.g., hospitalizations, medication) and $26.5 billion in non-medical costs like missed work, lost wages, early forced retirement, and family caregiver time.[38] These staggering figures are estimated to increase as the prevalence of PD is growing.[39] By 2030, it is estimated that 1.2 million Americans will be living with PD,[40,41] with 90,000 new cases of PD per year.[42]
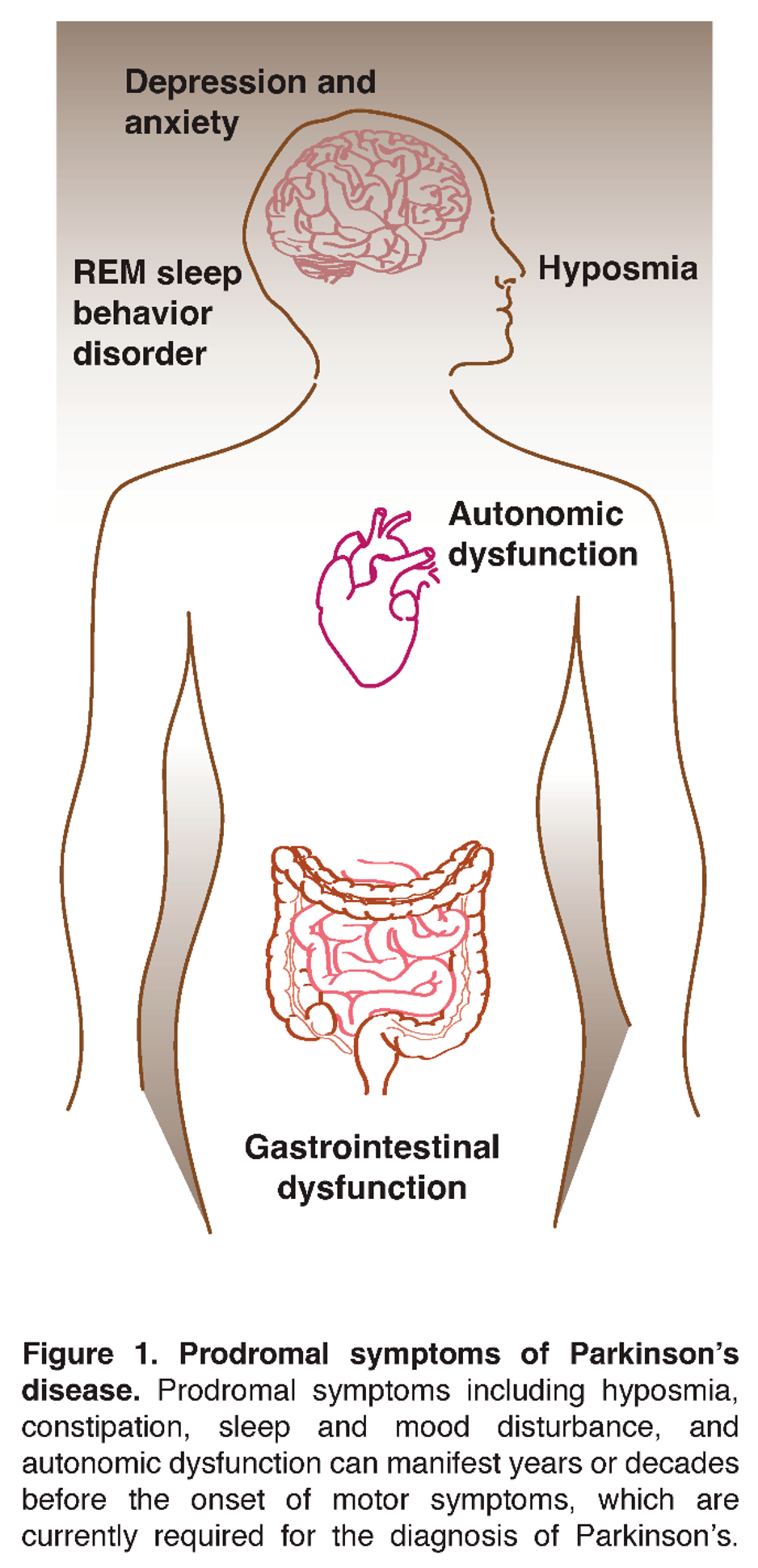
Aside from the large economic cost of Parkinson’s, the physical and emotional burden over a long period of time on individuals and families can be unbearable. PD is not limited to changes in movement. It negatively affects many other body systems such as gastrointestinal, urological, dermal, visual, speech, and autonomic functions.[Figure 1] In addition to lack of mobility and falls, depression, anxiety, sleep disruptions, mood changes, apathy, and cognitive impairment are common.[43,44] There is no doubt that Parkinson’s has a devastating impact on overall quality of life as the condition progresses. Thus, preventing Parkinson’s from ever manifesting in the first place or slowing its progression in at-risk individuals and the population at large is an important objective.
As aging remains the largest risk factor for PD,[45] presumably earlier intervention has a greater chance of preventing the degeneration of dopaminergic neurons in the brain, which is thought to play a key role in the development and progression of Parkinson’s disease. Estimates vary, but it is widely accepted that a significant portion of neurons have died by the time a person begins showing motor signs of Parkinson’s. Plus, the importance of early Parkinson’s prevention initiatives is critical if one considers the penetrance and conversion rate of certain prodromal groups.[Table 1] Studies have indicated that the overall conversion rate from RBD to an overt neurodegenerative synucleinopathy such as PD, dementia with Lewy bodies (DLB), or multiple system atrophy (MSA) is 6.3% per year with nearly all converting within 15 years.[46,47] Individuals diagnosed with polysomnography-proven RBD are not “healthy”. Even though prodromal individuals do not yet have a formal PD, DLB, or MSA diagnosis, they deserve significant research urgency and public attention since it is highly likely that neurodegeneration is already underway. There is no time to waste. With the recent breakthrough development of the alpha-synuclein seed amplification assay, which can identify Parkinson’s with high sensitivity and specificity early,[17] robust participant stratification for prevention trials in this prodromal population is now a reality.[48]
Moreover, lower penetrance rates in genetically at-risk individuals such as carriers of pathogenic LRRK2 or GBA variants complicate trial design and statistical power in the absence of established validated biomarkers for these targets. However, low-risk prevention interventions in genetically at-risk individuals remain promising because the underlying biological and pathological mechanisms are more elucidated, biomarker research is progressing quickly, and at-risk individuals can be identified very early.[49] In addition, direct-to-consumer genetic testing companies such as 23andMe as well as research initiatives such as PPMI and the Rostock International Parkinson’s Disease Study (ROPAD) have already identified over 4,000 contactable, non-manifesting carriers of the LRRK2 G2019S variant and even more with pathologic GBA variants.[50] According to a survey of over 200 non-manifesting carriers of the LRRK2 G2019S variant in the VALOR-PD study, 94% responded that they would be willing to participate in a clinical trial aimed at preventing the development of Parkinson’s.[50] And, the proportion interested was even higher if they had a family member who had been diagnosed with PD, as they are personally impacted and have seen firsthand the toll that Parkinson’s can take. Genetically at-risk individuals are incredibly motivated to act, not only for themselves, but for their children and siblings. Similarly, in an Alzheimer’s study, it was found that those with a family history of dementia were more than twice as likely to join a drug intervention trial.[51] While a large portion of clinical trial costs are spent on recruiting potential participants for studies,[52] the genetic revolution in recent years has allowed a significant head start on identifying a participant pool for intervention trials in genetically at-risk individuals.
Because the prevalence of neurodegenerative disease like Parkinson’s is increasing, clinical trials of candidate treatments to slow or reverse neurodegeneration should receive the same focus as wellness and preventative measures for other chronic diseases. Health plans and self-insured employers understand that they cannot reduce long term medical costs without managing and controlling chronic diseases through prevention and better outcomes. There is much to learn about pathologic causes and progression of Parkinson’s by studying at-risk individuals. Preventing, halting, or delaying disease progression in prodromal individuals will eventually enable the healthcare system to direct more resources to the treatment and management of those already suffering from manifest neurodegenerative diseases. If researchers are successful in testing treatments to fight against early neurodegenerative disease, such progress should attract more overall attention from government and industry for other Parkinson’s research. Therefore, engagement of at-risk individuals in prevention and biomarker research is essential.
Meaningful Input from At-Risk Individuals is Beneficial to Research
While community engagement in research is now implemented and endorsed by major research organizations such as the National Institutes of Health (NIH), Food and Drug Administration (FDA), and major pharmaceutical companies,[53,54,55] some advocates believe that not enough tangible progress has been made. However, with the new focus on prevention, there is the opportunity to design meaningful engagement with at-risk individuals from the start. Meaningful input from at-risk individuals is mutually beneficial to all stakeholders and has a foundation in medical ethics.
Meaningful input or engagement is defined as, “The active, meaningful, and collaborative interaction between patients and researchers across all stages of the research process, where research decision making is guided by patients’ contributions as partners, recognizing their specific experiences, values, and expertise.”[56] Two essential ethical principles that are of particular importance to patient engagement are (i) respect for persons and (ii) autonomy, an individual’s right to be involved in his or her own medical decisions. While these ethical principles have gained acceptance in the culture of generalized health care, they are still not fully embraced in the clinical research process.[57,58] Yet, these ethical foundations maintain that the public has a right to have a say in how research is conducted on conditions in which they are impacted.[58,59] For example, decisions regarding which interventions have the most appropriate balance of risk and benefit should not be made by researchers and regulators in isolation without strong participant representation regarding risk tolerance.[60] The level of transparency and public trust in research greatly improves when at-risk individuals are involved in all aspects of clinical research.[58]
At-risk individuals are eager to participate when barriers to involvement are removed and they feel respected for their contribution.[57] Engagement in research allows those with Parkinson’s risk factors an opportunity to channel their energy in a positive and productive way. For many, action cures fear. At-risk individuals often feel empowered when they are educated and active in research.[61] On the other side, while clinicians frequently interact directly with people with Parkinson’s, many lab researchers and academics remain largely disconnected and have never built relationships with people directly impacted by their research. This lack of association substantially limits researchers’ intimate understanding and appreciation for the condition. As a result, these researchers often miss out on the chance to develop the strong relationships with patients that result in a deeper sense of purpose in their work. Establishing collaborative partnerships among researchers and participants has an added advantage of ameliorating this gap.[62]
The importance of unique perspectives that at-risk individuals may offer to researchers should not be overlooked. They are a highly diverse group and possess unique knowledge and skills to contribute towards shared objectives. There are connections that people in the prodromal stage can illuminate that may lead to novel ideas – correlations that are easily missed by researchers when only looking at aggregate data or relying on standard questionnaires. As recently demonstrated by Morel et al., PwP who are newly diagnosed have subtle symptom changes that have not previously been well-elucidated,[63] and measuring these changes may be critical to successful early disease intervention. It is likely that at-risk patients, one step back from newly diagnosed, may also have subtle symptoms and changes that are not well understood and potentially the key to prevention.
From a financial standpoint, not involving potential participants in planning, development, and implementation of clinical trials contributes to wasted resources and delays.[64,65] Most notably, participant input achieves cost efficiencies by boosting recruitment and retention.[66] Prior research demonstrates that individuals being studied who have shared responsibility in developing research protocols and informed consent forms may increase the credibility of the study to other potential participants, which translates into better outreach.[67] In addition, actively listening to the community throughout the research continuum has long-term benefits since costly mistakes can be avoided upfront. For example, if certain therapeutic indications are not especially meaningful, specific trade-offs are not tolerated, or other more important quality of life outcomes are not measured, the tested interventions might falsely indicate negative results or may not be particularly useful to society.
People identified as at-risk for Parkinson’s have a different kind of motivation. Individuals directly impacted by diseases have the most to gain or lose from the success of translational research.[59] There is also a strong desire to help others with similar risk factors, as well as children and other family members in the case of those genetically at-risk. A balance of perspectives, and an opportunity for at-risk individuals to have the ability to make decisions that have real consequences, are necessary for accountability in achieving optimal research outcomes.[58] Well-informed at-risk individuals can provide greater exposure and attention to the problem by helping to disseminate understandable information and results to the wider community.[67]
Psychology of Risk Disclosure
Despite concerns regarding adverse implications of risk disclosure,[68] a study by Kim et al. showed that blinded enrollment to a participant’s risk marker status may be unnecessary from an ethical standpoint in prevention trials for other neurodegenerative diseases (NDD) like Alzheimer's disease (AD). This study demonstrated that significant psychosocial harm does not necessarily occur if risk of NDD is disclosed.[69] When PD risk disclosure included recommendations about lifestyle changes such as diet or exercise, Schaeffer et al. found that 85% of patients thought in retrospect it would have been a good idea to understand the relationship between their at-risk status and developing a neurodegenerative disorder.[70] While a healthy diet, sleep schedule, and physical activity are generally recommended for all individuals regardless of risk, the reality is that behavioral adherence to healthy lifestyle factors is higher with personalized education, support, and understanding of the physical benefits of lifestyle changes.[71]
Risk disclosure may also motivate at-risk individuals to participate in research studies. For example, individuals with RBD often feel embarrassed or confused about their symptoms, and the negative emotional toll can be real when a person goes to bed not knowing if he or she will cause harm to himself or herself or a bed partner. However, we should not underestimate the positive psychological impact that study participation has on at-risk individuals. Patients often report that they feel better just knowing that they are contributing to research that can lead to meaningful advances to help others. The larger the pool of patients who understand their at-risk status, the easier it should be to find and recruit at-risk individuals to participate in research that will lead to novel treatments and therapies for PD and other related neurological diseases.
Importantly, 92.5% of patients with idiopathic RBD (iRBD) enrolled in the Mayo Clinic iRBD Patient Registry responded in a recent survey that they felt knowledge concerning personal risk of neurodegenerative diseases was important, while only 4.3% desired less information about their NDD risk.[72] Similarly, a 2023 exploratory study by the PREDICT-PD team found that 90% of iRBD patients indicated that they wished that information regarding the increased risk of neurodegenerative diseases was offered by their treating clinician, and 60% indicated that it should happen at the time of diagnosis.[73] New guidelines published in 2023 by the American Academy of Sleep Medicine recommend that patients with RBD should be compassionately counseled about prognosis according to the individual patient’s desires.[74] In addition to learning about research opportunities, many patients and families wish to know more details for advanced care, financial, and retirement planning purposes and to be monitored more closely for development of additional symptoms so treatment can begin early.
Although patient input and attitudes regarding clinical and genetic disclosure should be at the heart of a strong patient – physician relationship, many physicians only discuss the risk of neurological disease when it is medically actionable. However, patients are often more resilient and capable of understanding than doctors assume. In the same way that physicians approach decision-making with patients who have other risk factors, there is good reason to consider such joint decision-making with patients at risk for neurological disease. Some individuals may not want to wait until they are on the verge of diagnosis to learn about their risk. Instead, patients should be given the opportunity and autonomy to provide meaningful input and feedback about what information is shared with them. This is not only an ethical imperative, but also a potential driver of better health outcomes. Studies demonstrate that patient access to clinical notes allows them to, “feel more involved in and knowledgeable about their care, feel better prepared for visits, and report being more likely to follow their clinicians’ advice.”[75]
In addition, clinicians are also reminded that when patients first learn of their RBD diagnosis, they are likely to take to the internet where they will quickly learn of the future risk of PD or other synucleinopathies. These patients may become acutely anxious about the information they find on various websites or even become angry with their physician for not sharing more information.[76] By taking the time to get to know patients, and by explaining that having one or more risk factors doesn’t mean that eventual disease will result, physicians can help to better guide patients. The timing and content of these discussions are dependent on the circumstances of the situation, who is making the diagnosis, and whether longitudinal follow up care is planned.[76]
Early Symptoms
The at-risk population phenoconverts to manifest Parkinson’s or another α-synucleinopathy over many years, if not decades.[46] Because α-synucleinopathy diseases like Parkinson's can have a long prodromal stage, many people exhibit various non-motor and subclinical motor manifestations for several years, adding to the challenge of diagnosing this complex disease during its insidious onset.[77] A recent case-control study using random sampled survey data from the National Health and Aging Trends Study (NHATS) found that unrecognized, prodromal Parkinson’s is connected to significant problems with mobility and strength compared to the general population up to three years prior to diagnosis.[78]
Encouraging the at-risk population to participate in clinical studies during the prodromal stage to monitor the onset of symptom development is critical to identifying interventions that can slow, stop, or reverse disease progression prior to a traditional diagnosis of PD. Yet, many at-risk individuals do not feel supported when communicating their concerns. It is human nature for family, friends, and doctors to want to comfort and reassure someone who may be experiencing mental or physical changes, so too often the first reaction is to downplay early symptoms. The intention may be well-meaning but could make at-risk people feel worse because their concerns and symptoms are not validated.
Many early signs might be masked because of the brain and body’s efforts to compensate. Even though a patient may not meet conventional criteria to establish a clinical diagnosis of PD, this person may still be experiencing a degenerative process with damaging consequences. Sometimes genetically at-risk individuals are labeled as “asymptomatic” or “non-manifesting” carriers because they are not experiencing or displaying classical motor features of PD, but they may indeed be symptomatic of and manifesting the disease at an early stage. Holistic and lifestyle interventions such as diet, exercise, and supplements as well as repurposed drugs with a reasonable safety profile may fit the risk tolerance for participation in research trials in these individuals. Longer trials in at-risk individuals then become more of a practical consideration and not really related to long trials in “healthy” people. If the research community waits until there is one hundred percent certainty that at-risk individuals have PD before intervening, we won’t make progress quickly enough. The modest success of a recent, long-term, randomized controlled trial of a multivitamin for preserved brain function by Yeung et al.[79] highlights the potential utility and practicality of moving quickly into such trials. Testing of biologically compelling interventions that are lower risk, less invasive, and less expensive than those generally pursued by the biopharmaceutical industry, could provide an invaluable early experience for improving the design and success of subsequent trials toward this emerging indication of prevention.
How Do At-Risk Individuals Fit into the Broader Parkinson’s Community?
At present, at-risk individuals are a distinct category from PwP and caregivers, and have not been prominently recognized separately at conferences or events in the broader Parkinson’s community, though their voice is beginning to be heard and sought as reflected in the recent Parkinson’s prevention symposium that the authors participated in. Part of the reason for this might be related to the novel nature of this prevention initiative in PD, the lack of desire amongst at-risk individuals to publicly disclose their at-risk status, or the lack of motivation to become involved in advocacy with no PD diagnosis or strong personal connection to PwP. However, this is not always the case, particularly in genetically at-risk individuals, where they might be current or former care partners to a PwP and therefore feel connected to the broader Parkinson’s community in other ways. For some at-risk individuals with a family history, there might be a long continuum of Parkinson’s advocacy that spans caregiving, being at-risk, and later potentially living with PD. For some individuals with RBD, who are neither a PwP nor a caregiver, it may be difficult to engage in Parkinson’s prevention research and advocacy without more targeted organization and rallying of the at-risk population. The North American Prodromal Synucleinopathy (NAPS) consortium and other initiatives recruiting RBD cohorts through sleep centers may help in that effort.
Further complicating the situation, there is perceived competition between at-risk individuals and those already diagnosed with PD for funding and other resources. Likewise, there may also be competition among at-risk categories for resources as well. The resulting tension might discourage open involvement and discussion in the community. However, the greater the spotlight that is placed on Parkinson’s by increasing collaboration with at-risk individuals, and the more educated society is about the sequelae of PD, the greater the potential benefit to the entire Parkinson’s research community. Also, the emerging effort to redefine PD biologically [34,35,36,37] means that people with RBD and/or other prodromal features might be considered to be in an early stage of PD, and therefore already PwP. It is important for the wider PD community to embrace and support one another. At-risk individuals can positively influence the community by helping researchers secure additional resources to accelerate progress towards collective goals. Thus, prevention trials incorporating at-risk individuals should be viewed as complementary and not in competition with trials for PwP. A diversification strategy that includes trials with participants from earlier stages and various subtypes will have different risk tolerances, length, target intervention, sample size, and outcome measures. Nonetheless, knowledge has a way of building, and discovery and advancements in one group can directly or indirectly benefit people in another stage and category.
Lastly, there is much to learn from those at-risk individuals who never develop enough symptoms to be diagnosed with PD, and studying these individuals might provide the key to both prevention and disease modification. And if a trial of a candidate neuroprotectant in a prodromal population were to demonstrate efficacy for preventing classically manifest PD, then there is a good chance that the intervention would similarly benefit those with more advanced disease. Therefore, studying at-risk people may help everyone in the PD community.
Return of Individual Information
The 21st Century Cures Act (Cures Act) was signed into United States law on December 13, 2016. Congress passed the Cures Act with the intent to begin to unravel the web of medical information in the healthcare system that patients and caregivers find difficult to access and understand. As advocates for the at-risk population, the lay authors believe that the same underlying public policy considerations that led to the passage of the Cures Act support providing research participants with the same seamless access to research data. One of the fundamental benefits of the Cures Act is to provide ease of access to an individual’s medical record to better motivate and engage patients in their healthcare decision making. The same rationale for data sharing in the clinical setting also applies to the research setting. Motivating and recruiting individuals to participate in research studies can be challenging. However, designing clinical studies around the same information sharing approach of the Cures Act promises to increase interest and willingness to participate in research studies.
A Committee on the Return of Individual-Specific Research Results Generated in Research Laboratories concluded in a consensus report that the risks of harms have historically been overstated and the potential benefits of returning information to participants have been understated. Instead the Committee recommended that the balance should actually lean more towards personal disclosure with references and support.[80] Especially given that science is at the dawn of precision medicine, the research paradigm is evolving towards a participant-driven and open access model, which inevitably includes increased communication of individual as well as composite results.[61,80] Participants are naturally curious, and as a matter of respect and reciprocity, the return of information should be widely considered according to personal choice.[58,61,80,81] Directly communicating results back to participants makes a difference in engagement, can improve recruitment and retention, and is a way for researchers to express their appreciation for the value that participants provide.[81]
There is often an overlap between exams and testing in the clinical setting and the research setting. If research information is shared with a participant’s treating provider, this may avoid costly repetitive testing and help reduce healthcare burden. Alternatively, sharing research data such as sleep study results, DaT scan imaging, neurocognitive testing, a-syn skin biopsy results, a-syn CSF results, and olfactory testing may allow the treating provider to gain earlier insight into signs and symptoms to facilitate earlier diagnosis of Parkinson’s. Just as the use of mobile devices, wearable devices, and biosensors promises to better engage people in their healthcare as a result of the interoperability provisions of the Cures Act, this same technology can do the same with individuals who participate in clinical studies if researchers are willing to challenge the status quo by applying the information sharing principles of the Cures Act to the research setting.
While even clinically available and CLIA-certified test results are rarely returned to participants in the setting of research studies, a more nuanced issue often arises over sharing results of experimental, unvalidated tests. At present many potential PD biomarkers like alpha-synuclein seed amplification assay (aSyn-SAA), neurofilament light chain (Nfl), genetic variants of unknown significance (VUS), digital trackers, etc. are not shared in part for this reason. Some argue all results even if unclear or 'not meaningful' should be shared, whereas others argue that it's irresponsible to share results that the researcher may not be able to appropriately interpret or offer counseling on. However, it is a misconception that research participants are incapable of understanding data with an appropriate level of context and involvement of a researcher or treating physician. What is meaningful to participants as individuals can be vastly different to what researchers or clinicians consider meaningful to society. Individuals are not averages. Scientific knowledge changes over time, so biomarker levels captured preclinically or prodromally might be personally informative for prognosis or subtyping for an individual later on. That benefit is lost if individual information is not returned. Likewise, test results captured at a point in time for a parent or grandparent might be very useful information to know for children or grandchildren in the future - particularly in genetic cases. What is deemed unclear or not meaningful now might be highly valuable later.
There are existing cohorts of at-risk individuals who have already participated in observational and biomarker studies either longitudinally or cross-sectionally and across disciplines and targets. Participants give their time, biological samples, observational data and tolerate unknown risks in an effort to contribute to scientific discovery. There is a wealth of information that is left untapped unless infrastructure and systems are developed to support the preservation and consolidation of data at the individual level. By linking studies and curating the data over generations by connecting relevant family members and communities, synergistic cost savings result.[82] We may not know how things are connected now, but rich datasets might be very helpful later once scientific understanding has advanced.
CHALLENGES AND OPPORTUNITIES IN THE CURRENT ENVIRONMENT
Lack of Awareness Among Primary Care Physicians & General Neurologists
The ability to accurately identify those at risk for developing Parkinson’s is a critical variable in order to conduct much needed prevention trials. Even after a traditional clinical diagnosis of PD, when symptoms are responsive to dopaminergic therapy, diagnostic accuracy is relatively poor.[83] Studies have shown that while neurologists with expertise in movement disorders are very good diagnosticians, with low false-positive rates for the diagnosis of idiopathic PD, PD diagnoses in general practice clinics are usually significantly less accurate.[84]
However, the first potential point of contact about Parkinson’s risk in an individual’s clinical care is their primary care physician or general practitioner. Given the breadth of issues that must be managed in a primary care setting and the rapid evolution of medical knowledge, it is difficult for primary care physicians to be well versed and updated in all areas. This may be reflected in their variable knowledge of neurodegenerative illness like PD, its clinical presentation, and its management. The challenge is highlighted by a substantial gap in practical clinical knowledge of PD genetics, which can define a major at-risk group, even among movement disorders specialists and by the relative discomfort of a high proportion of them in discussing it with their patients.[85] However, with the appropriate educational updates, their knowledge base improves, and this hopefully translates to clinical practice.[86] Therefore, to help ensure that patients who meet the inclusion criteria for enrollment in prevention trials are aware of their eligibility, investment in an appropriate educational update for both first line and specialist physicians, would be crucial.
In preparation for prevention trials, we need to spend time and resources educating clinicians about Parkinson’s risk. For example, screening for hyposmia or the RBD1Q are potentially high yield tests used in research that could be applied to the general clinic. Concurrent advocacy and health literacy programs for the general public along with training programs for care providers are needed to empower individuals to gain confidence in communicating with each other. In parallel to engaging clinicians, it will be equally important to educate and mobilize the emerging advocacy community of those at-risk for PD and those who are committed to its prevention through their lived experience with the disease. They will in turn play a critical role in educating and motivating not only clinicians but also academic, industry, philanthropic, and regulatory partners.
Earlier diagnosis can translate to feelings of relief in some individuals because they feel validated regarding their concerns. It prevents gaslighting and leads to more understanding and compassion from family members. In retrospect, PwP often report frustration with the length of time it took to get diagnosed and many had to endure initial misdiagnoses. With earlier diagnosis, people have a chance to implement lifestyle changes such as increased exercise, have an opportunity to join clinical research studies and can better plan for the future.
Legal Implications
Some individuals may rightfully wonder if participating in clinical research or undergoing genetic testing will impact their employment or ability to obtain insurance. However, fear of discrimination should not discourage volunteers from participating in research. There are many important legal protections to limit intentional or unintentional misuse of genetic or other research information, and there are steps that patients and physicians can take together to share research information but yet limit the scope of who can access this information.
The Genetic Information Nondiscrimination Act of 2008 (GINA) is a federal law that was passed by the United States Congress to provide important protections to individuals because of the rapidly accumulating information about a person’s genetic information. GINA, together with already existing nondiscrimination provisions of the Health Insurance Portability and Accountability Act (HIPAA), generally prohibits health insurers from using such information for decisions regarding coverage, rates, or preexisting conditions. GINA also prohibits employers from using genetic information for hiring, firing, or promotion decisions (See Genetic Information Nondiscrimination Act (GINA): OHRP Guidance (2009)). Even if workers voluntarily disclose genetic risks, their employer is still prohibited from taking unlawful discriminatory action based on that information.
GINA has helped to clarify the legal landscape and protect patients from misuse of genetic information, and it fundamentally recognizes that genetic predisposition to develop a disease does not mean actual disease is a certainty. As defined in the law, protected genetic information includes family medical history, manifest disease in family members, and information regarding individuals' and family members' genetic tests. See 29 CFR 1635.3. Nonetheless, it is important to note that GINA’s health insurance protections do not cover long-term care insurance, life insurance or disability insurance. Many people advise to obtain these specific types of insurance prior to genetic testing, with the option to cancel their policies later if they are not found to have any genetic risk and do not wish to pay the premiums. Despite the loophole, most insurers still do not use genetic testing in eligibility criteria for these types of insurance policies.[87] And, the whole premise of purchasing insurance is to mitigate potential future risk. However, one is less likely to purchase long term care and disability insurance when they are young and healthy and are not aware of their higher risk for disease.
In the context of at-risk individuals, GINA protects individuals who carry LRRK2 or GBA genetic variants, for example, but it does not provide protection to individuals with a known diagnosis of RBD. However, even if the express provisions of GINA do not apply to individuals with RBD, the Americans with Disabilities Act (ADA) provides other important protections to individuals with physical or mental impairment or record of such impairment like RBD. 29 CFR Section 1630.2(g). As a result, it is extremely risky for an employer to take adverse action against an employee or applicant with RBD based on the potential to develop medical problems in the future.
Despite legal protections and rights, at-risk individuals can be understandably wary about being public about their risk of PD. If adverse action is taken against an at-risk individual, it can be difficult and expensive for a person claiming discrimination to prevail in a lawsuit. It is for these reasons that the Office for Human Research Protections (OHRRP) within HHS recommends integrating GINA into clinical research. Research participants should carefully read and understand informed consent forms and be clear with the study coordinator on what research information the participant authorizes the principal investigator to share. Most research records are not mingled with the participant’s formal clinical record. The risks are manageable if there is clear communication and careful coordination between the participant, treating physician and research team.
Identification, Training, and Engagement of At-Risk Advocates
At present, many programs exist that train and support individual advocates in driving research decision- making, and train researchers to work with advocates. These include pan-disease trainings such as the European Patients’ Academy on Therapeutic Innovation (EUPATI), pan-collaborator trainings such as the Patient Engagement Management Suite of Patient Focused Medicines Development, and disease- or collaborator-specific trainings such as the Parkinson’s Foundation Research Advocacy program for people with Parkinson’s, care partners and researchers or the TransCelerate Patient Protocol Engagement Toolkit (P-PET).[55,88] These programs are part of the full spectrum of community engagement that includes both the work of individual grassroot advocates, those trained by patient advocacy organizations and professional patient advocates with roles at organizations such as the FDA. However, there are no programs that the authors are aware of that specifically target and train at-risk advocates. There is an opportunity for an established program to use their resources to start a targeted outreach initiative with that purpose. Each of these groups of advocates bring a unique perspective. What knits all these advocates together is their lived experience expertise that only they have and the expertise they bring from their personal and professional lives. This experience is complementary to the scientific expertise brought by research and is invaluable in making research more efficient and effective.
There is currently a plethora of online training, tools, and resources for patient engagement. As previously noted, however, despite the existence of this supportive infrastructure, patient engagement is often still tokenistic or not done at all. The newness of the presently formed community of at-risk individuals, their loved ones, researchers, advocacy organizations, and consortiums allows for the chance to begin with best practices of engagement in place. Through co-creation, the roles and responsibilities of partners should be clearly defined, goals and methods of engagement should be outlined and followed, and evaluation and assessment of the quality and impact of engagement should be done to ensure that the process does not slip into tokenism, and allow the team to celebrate achieving goals of true collaboration. At-risk individuals should be engaged in setting research questions, prioritizing research, defining study outcomes and endpoints, determining how many study visits occur and what types of tests are done and how often, monitoring safety data, educating their community about research participation, analyzing data, and disseminating results.
CONCLUSION
While unprecedented until recently, preventative trials in Parkinson’s symbolize a fresh canvas and allow an opportunity to engage with at-risk individuals as true active partners. In order to fully leverage the benefits of participant integration in the research process, influencers are beginning to make a concerted effort to equalize the authority structure as evidenced by the format of the recent “Planning for Prevention of Parkinson’s: A Trial Design Forum” in which the authors participated. Working together in parallel with researchers, regulators, funders, industry members, and clinicians, individuals identified as at-risk are a powerful contribution to the research planning team in the bold quest to prevent Parkinson’s.
Funding
The Michael J. Fox Foundation for Parkinson’s Research Award MJFF-022854.
Acknowledgments
Massachusetts General Hospital, The Michael J. Fox Foundation for Parkinson’s Research Katherine Callahan at MGH “Planning for Prevention of Parkinson’s: A Trial Design Forum” was supported by The ABY Fund, the American Parkinson Disease Association, the Carol T. Barrett Fund for Parkinson’s Disease Research, Cure Parkinson’s, GE Healthcare, the National Institute of Neurological Disorders And Stroke of the National Institutes of Health under Award Number R13NS129235 (the content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health), the Parkinson’s Foundation via Grant No.PF-CA-946319, the Parkinson Study Group, Sanofi US Services, Inc., and The Sergey Brin Family Foundation.
Conflicts of interest
The authors have no conflict of interest to report.
References
- Reference SNP (rs) Report rs34637584 LRRK2 [Internet],National Library of Medicine (US), National Center for Biotechnology Information, Available from: https://www.ncbi.nlm.nih.gov/snp/rs34637584, September 21, 2022,Accessed September 27, 2023.
- Reference SNP (rs) Report rs76763715 (GBA) [Internet],National Library of Medicine (US), National Center for Biotechnology Information, Available from: https://www.ncbi.nlm.nih.gov/snp/rs76763715, September 21, 2022,Accessed September 27, 2023.
- Cicero, C.E.; Giuliano, L.; Luna, J.; Zappia, M.; Preux, P.M.; Nicoletti, A. Prevalence of idiopathic REM behavior disorder: a systematic review and meta-analysis. Sleep 2021, 44, zsaa294. [Google Scholar] [CrossRef] [PubMed]
- Haba-Rubio, J.; Frauscher, B.; Marques-Vidal, P.; Toriel, J.; Tobback, N.; Andries, D.; Preisig, M.; Vollenweider, P.; Postuma, R.; Heinzer, R. Prevalence and determinants of rapid eye movement sleep behavior disorder in the general population. Sleep 2018, 41, zsx197. [Google Scholar] [CrossRef]
- Desiato, V.M.; Levy, D.A.; Byun, Y.J.; Nguyen, S.A.; Soler, Z.M.; Schlosser, R.J. The Prevalence of Olfactory Dysfunction in the General Population: A Systematic Review and Meta-analysis. Am J Rhinol Allergy 2021, 35, 195–205. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.J.; Wang, Y.; Alcalay, R.N.; Mejia-Santana, H.; Saunders-Pullman, R.; Bressman, S.; Corvol, J.C.; Brice, A.; Lesage, S.; Mangone, G.; Tolosa, E.; Pont-Sunyer, C.; Vilas, D.; Schule, B.; Kausar, F.; Foroud, T.; Berg, D.; Brockmann, K.; Goldwurm, S.; Siri, C.; Asselta, R.; Ruiz-Martinez, J.; Mondragon, E.; Marras, C.; Ghate, T.; Giladi, N.; Mirelman, A.; Marder, K.; Michael, J.F.L.C.C. Penetrance estimate of LRRK2 p.G2019S mutation in individuals of non-Ashkenazi Jewish ancestry. Mov Disord 2017, 32, 1432–1438. [Google Scholar] [CrossRef] [PubMed]
- Alcalay, R.N.; Dinur, T.; Quinn, T.; Sakanaka, K.; Levy, O.; Waters, C.; Fahn, S.; Dorovski, T.; Chung, W.K.; Pauciulo, M.; Nichols, W.; Rana, H.Q.; Balwani, M.; Bier, L.; Elstein, D.; Zimran, A. Comparison of Parkinson risk in Ashkenazi Jewish patients with Gaucher disease and GBA heterozygotes. JAMA Neurol 2014, 71, 752–757. [Google Scholar] [CrossRef] [PubMed]
- Dauvilliers, Y.; Schenck, C.H.; Postuma, R.B.; Iranzo, A.; Luppi, P.H.; Plazzi, G.; Montplaisir, J.; Boeve, B. REM sleep behaviour disorder. Nat Rev Dis Primers 2018, 4, 19. [Google Scholar] [CrossRef] [PubMed]
- Sui, X.; Zhou, C.; Li, J.; Chen, L.; Yang, X.; Li, F. Hyposmia as a Predictive Marker of Parkinson's Disease: A Systematic Review and Meta-Analysis. Biomed Res Int 2019, 2019, 3753786. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Yan, X.; Lv, H.; Liu, Y.; He, Z.; Luo, X. Gender differences in prevalence of LRRK2-associated Parkinson disease: A meta-analysis of observational studies. Neurosci Lett 2020, 715, 134609. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Jing, Y.; Lun, P.; Liu, X.; Sun, P. Association of gender and age at onset with glucocerebrosidase associated Parkinson's disease: a systematic review and meta-analysis. Neurol Sci 2021, 42, 2261–2271. [Google Scholar] [CrossRef]
- Cerri, S.; Mus, L.; Blandini, F. Parkinson's Disease in Women and Men: What's the Difference? J Parkinsons Dis 2019, 9, 501–515. [Google Scholar] [CrossRef]
- Kestenbaum M, Alcalay RN (2017) Clinical Features of LRRK2 Carriers with Parkinson’s Disease In Leucine-Rich Repeat Kinase 2 (LRRK2), Rideout HJ, ed. Springer International Publishing, Cham, pp. 31-48.
- Ren, J.; Zhan, X.; Zhou, H.; Guo, Z.; Xing, Y.; Yin, H.; Xue, C.; Wu, J.; Liu, W. Comparing the effects of GBA variants and onset age on clinical features and progression in Parkinson's disease. CNS Neurosci Ther 2024, 30, e14387. [Google Scholar] [CrossRef] [PubMed]
- St Louis, E.K.; Boeve, B.F. REM Sleep Behavior Disorder: Diagnosis, Clinical Implications, and Future Directions. Mayo Clin Proc 2017, 92, 1723–1736. [Google Scholar] [CrossRef] [PubMed]
- He, R.; Zhao, Y.; He, Y.; Zhou, Y.; Yang, J.; Zhou, X.; Zhu, L.; Zhou, X.; Liu, Z.; Xu, Q.; Sun, Q.; Tan, J.; Yan, X.; Tang, B.; Guo, J. Olfactory Dysfunction Predicts Disease Progression in Parkinson's Disease: A Longitudinal Study. Front Neurosci 2020, 14, 569777. [Google Scholar] [CrossRef]
- Siderowf, A.; Concha-Marambio, L.; Lafontant, D.E.; Farris, C.M.; Ma, Y.; Urenia, P.A.; Nguyen, H.; Alcalay, R.N.; Chahine, L.M.; Foroud, T.; Galasko, D.; Kieburtz, K.; Merchant, K.; Mollenhauer, B.; Poston, K.L.; Seibyl, J.; Simuni, T.; Tanner, C.M.; Weintraub, D.; Videnovic, A.; Choi, S.H.; Kurth, R.; Caspell-Garcia, C.; Coffey, C.S.; Frasier, M.; Oliveira, L.M.A.; Hutten, S.J.; Sherer, T.; Marek, K.; Soto, C.; Parkinson's Progression Markers Initiative. Assessment of heterogeneity among participants in the Parkinson's Progression Markers Initiative cohort using alpha-synuclein seed amplification: a cross-sectional study. Lancet Neurol 2023, 22, 407–417. [Google Scholar] [CrossRef] [PubMed]
- Paisan-Ruiz, C.; Lewis, P.A.; Singleton, A.B. LRRK2: cause, risk, and mechanism. J Parkinsons Dis 2013, 3, 85–103. [Google Scholar] [CrossRef]
- Gan-Or, Z.; Liong, C.; Alcalay, R.N. GBA-Associated Parkinson's Disease and Other Synucleinopathies. Curr Neurol Neurosci Rep 2018, 18, 44. [Google Scholar] [CrossRef] [PubMed]
- Del Tredici, K.; Braak, H. Review: Sporadic Parkinson's disease: development and distribution of alpha-synuclein pathology. Neuropathol Appl Neurobiol 2016, 42, 33–50. [Google Scholar] [CrossRef] [PubMed]
- Schootemeijer, S.; van der Kolk, N.M.; Bloem, B.R.; de Vries, N.M. Current Perspectives on Aerobic Exercise in People with Parkinson's Disease. Neurotherapeutics 2020, 17, 1418–1433. [Google Scholar] [CrossRef] [PubMed]
- San Luciano, M.; Tanner, C.M.; Meng, C.; Marras, C.; Goldman, S.M.; Lang, A.E.; Tolosa, E.; Schule, B.; Langston, J.W.; Brice, A.; Corvol, J.C.; Goldwurm, S.; Klein, C.; Brockman, S.; Berg, D.; Brockmann, K.; Ferreira, J.J.; Tazir, M.; Mellick, G.D.; Sue, C.M.; Hasegawa, K.; Tan, E.K.; Bressman, S.; Saunders-Pullman, R.; Michael, J.F.F.L.C.C. Nonsteroidal Anti-inflammatory Use and LRRK2 Parkinson's Disease Penetrance. Mov Disord 2020, 35, 1755–1764. [Google Scholar] [CrossRef]
- Crotty, G.F.; Maciuca, R.; Macklin, E.A.; Wang, J.; Montalban, M.; Davis, S.S.; Alkabsh, J.I.; Bakshi, R.; Chen, X.; Ascherio, A.; Astarita, G.; Huntwork-Rodriguez, S.; Schwarzschild, M.A. Association of caffeine and related analytes with resistance to Parkinson disease among LRRK2 mutation carriers: A metabolomic study. Neurology 2020, 95, e3428–e3437. [Google Scholar] [CrossRef]
- Schaffner, A.; Li, X.; Gomez-Llorente, Y.; Leandrou, E.; Memou, A.; Clemente, N.; Yao, C.; Afsari, F.; Zhi, L.; Pan, N.; Morohashi, K.; Hua, X.; Zhou, M.M.; Wang, C.; Zhang, H.; Chen, S.G.; Elliott, C.J.; Rideout, H.; Ubarretxena-Belandia, I.; Yue, Z. Vitamin B(12) modulates Parkinson's disease LRRK2 kinase activity through allosteric regulation and confers neuroprotection. Cell Res 2019, 29, 313–329. [Google Scholar] [CrossRef] [PubMed]
- Crotty, G.F.; Schwarzschild, M.A. What to Test in Parkinson Disease Prevention Trials? Repurposed, Low-Risk, and Gene-Targeted Drugs. Neurology 2022, 99, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Krohn, L.; Ruskey, J.A.; Rudakou, U.; Leveille, E.; Asayesh, F.; Hu, M.T.M.; Arnulf, I.; Dauvilliers, Y.; Hogl, B.; Stefani, A.; Monaca, C.C.; Abril, B.; Plazzi, G.; Antelmi, E.; Ferini-Strambi, L.; Heidbreder, A.; Boeve, B.F.; Espay, A.J.; De Cock, V.C.; Mollenhauer, B.; Sixel-Doring, F.; Trenkwalder, C.; Sonka, K.; Kemlink, D.; Figorilli, M.; Puligheddu, M.; Dijkstra, F.; Viaene, M.; Oertel, W.; Toffoli, M.; Gigli, G.L.; Valente, M.; Gagnon, J.F.; Desautels, A.; Montplaisir, J.Y.; Postuma, R.B.; Rouleau, G.A.; Gan-Or, Z. GBA variants in REM sleep behavior disorder: A multicenter study. Neurology 2020, 95, e1008–e1016. [Google Scholar] [CrossRef] [PubMed]
- Mullin, S.; Smith, L.; Lee, K.; D'Souza, G.; Woodgate, P.; Elflein, J.; Hallqvist, J.; Toffoli, M.; Streeter, A.; Hosking, J.; Heywood, W.E.; Khengar, R.; Campbell, P.; Hehir, J.; Cable, S.; Mills, K.; Zetterberg, H.; Limousin, P.; Libri, V.; Foltynie, T.; Schapira, A.H.V. Ambroxol for the Treatment of Patients With Parkinson Disease With and Without Glucocerebrosidase Gene Mutations: A Nonrandomized, Noncontrolled Trial. JAMA Neurol 2020, 77, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Mandel, S.; Weinreb, O.; Amit, T.; Youdim, M.B. Mechanism of neuroprotective action of the anti-Parkinson drug rasagiline and its derivatives. Brain Res Brain Res Rev 2005, 48, 379–387. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Wang, C.; Luo, N.; Chen, F.; Zhou, L.; Niu, M.; Kang, W.; Liu, J. Efficacy of idebenone in the Treatment of iRBD into Synucleinopathies (EITRS): rationale, design, and methodology of a randomized, double-blind, multi-center clinical study. Front Neurol 2022, 13, 981249. [Google Scholar] [CrossRef] [PubMed]
- Simmering, J.E.; Welsh, M.J.; Schultz, J.; Narayanan, N.S. Use of Glycolysis-Enhancing Drugs and Risk of Parkinson's Disease. Mov Disord 2022, 37, 2210–2216. [Google Scholar] [CrossRef]
- Kim, D.S.; Choi, H.I.; Wang, Y.; Luo, Y.; Hoffer, B.J.; Greig, N.H. A New Treatment Strategy for Parkinson's Disease through the Gut-Brain Axis: The Glucagon-Like Peptide-1 Receptor Pathway. Cell Transplant 2017, 26, 1560–1571. [Google Scholar] [CrossRef] [PubMed]
- Abeliovich, A.; Hefti, F.; Sevigny, J. Gene Therapy for Parkinson's Disease Associated with GBA1 Mutations. J Parkinsons Dis 2021, 11, S183–S188. [Google Scholar] [CrossRef]
- Schilter, H.C.; Collison, A.; Russo, R.C.; Foot, J.S.; Yow, T.T.; Vieira, A.T.; Tavares, L.D.; Mattes, J.; Teixeira, M.M.; Jarolimek, W. Effects of an anti-inflammatory VAP-1/SSAO inhibitor, PXS-4728A, on pulmonary neutrophil migration. Respir Res 2015, 16, 42. [Google Scholar] [CrossRef]
- Chahine, L.M.; Merchant, K.; Siderowf, A.; Sherer, T.; Tanner, C.; Marek, K.; Simuni, T. Proposal for a Biologic Staging System of Parkinson's Disease. J Parkinsons Dis 2023, 13, 297–309. [Google Scholar] [CrossRef] [PubMed]
- Höglinger GU, Adler CH, Berg D, Klein C, Outeiro TF, Poewe W, Postuma R, Stoessl J, Lang AE (2023) in Preprints Preprints.
- Cardoso, F.; Goetz, C.G.; Mestre, T.A.; Sampaio, C.; Adler, C.H.; Berg, D.; Bloem, B.R.; Burn, D.J.; Fitts, M.S.; Gasser, T.; Klein, C.; de Tijssen, M.A.J.; Lang, A.E.; Lim, S.Y.; Litvan, I.; Meissner, W.G.; Mollenhauer, B.; Okubadejo, N.; Okun, M.S.; Postuma, R.B.; Svenningsson, P.; Tan, L.C.S.; Tsunemi, T.; Wahlstrom-Helgren, S.; Gershanik, O.S.; Fung, V.S.C.; Trenkwalder, C. A Statement of the MDS on Biological Definition, Staging, and Classification of Parkinson's Disease. Mov Disord. 2024, 39, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Wood, H. A new biological classification for Parkinson disease. Nat Rev Neurol 2023, 19, 711. [Google Scholar] [CrossRef]
- Yang, W.; Hamilton, J.L.; Kopil, C.; Beck, J.C.; Tanner, C.M.; Albin, R.L.; Ray Dorsey, E.; Dahodwala, N.; Cintina, I.; Hogan, P.; Thompson, T. Current and projected future economic burden of Parkinson's disease in the U.S. NPJ Parkinsons Dis 2020, 6, 15. [Google Scholar] [CrossRef] [PubMed]
- Dorsey, E.R.; Sherer, T.; Okun, M.S.; Bloem, B.R. The Emerging Evidence of the Parkinson Pandemic. J Parkinsons Dis 2018, 8, S3–S8. [Google Scholar] [CrossRef] [PubMed]
- GBD 2016 Parkinson's Disease Collaborators. Global, regional, and national burden of Parkinson's disease, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol 2018, 17, 939–953. [Google Scholar] [CrossRef]
- Marras, C.; Beck, J.C.; Bower, J.H.; Roberts, E.; Ritz, B.; Ross, G.W.; Abbott, R.D.; Savica, R.; Van Den Eeden, S.K.; Willis, A.W.; Tanner, C.M.; Parkinson's Foundation, P.G. Prevalence of Parkinson's disease across North America. NPJ Parkinsons Dis 2018, 4, 21. [Google Scholar] [CrossRef] [PubMed]
- Willis, A.W.; Roberts, E.; Beck, J.C.; Fiske, B.; Ross, W.; Savica, R.; Van Den Eeden, S.K.; Tanner, C.M.; Marras, C.; Parkinson's Foundation, P.G. Incidence of Parkinson disease in North America. NPJ Parkinsons Dis 2022, 8, 170. [Google Scholar] [CrossRef]
- Hermanowicz, N.; Jones, S.A.; Hauser, R.A. Impact of non-motor symptoms in Parkinson's disease: a PMDAlliance survey. Neuropsychiatr Dis Treat 2019, 15, 2205–2212. [Google Scholar] [CrossRef]
- Lageman, S.K.; Cash, T.V.; Mickens, M.N. Patient-reported Needs, Non-motor Symptoms, and Quality of Life in Essential Tremor and Parkinson's Disease. Tremor Other Hyperkinet Mov (N Y) 2014, 4, 240. [Google Scholar] [CrossRef]
- Hou, Y.; Dan, X.; Babbar, M.; Wei, Y.; Hasselbalch, S.G.; Croteau, D.L.; Bohr, V.A. Ageing as a risk factor for neurodegenerative disease. Nat Rev Neurol 2019, 15, 565–581. [Google Scholar] [CrossRef] [PubMed]
- Postuma, R.B.; Berg, D. Advances in markers of prodromal Parkinson disease. Nat Rev Neurol 2016, 12, 622–634. [Google Scholar] [CrossRef] [PubMed]
- Yao, C.; Fereshtehnejad, S.M.; Dawson, B.K.; Pelletier, A.; Gan-Or, Z.; Gagnon, J.F.; Montplaisir, J.Y.; Postuma, R.B. Longstanding disease-free survival in idiopathic REM sleep behavior disorder: Is neurodegeneration inevitable? Parkinsonism Relat Disord 2018, 54, 99–102. [Google Scholar] [CrossRef] [PubMed]
- Berg, D.; Klein, C. alpha-synuclein seed amplification and its uses in Parkinson's disease. Lancet Neurol 2023, 22, 369–371. [Google Scholar] [CrossRef] [PubMed]
- Niotis, K.; West, A.B.; Saunders-Pullman, R. Who to Enroll in Parkinson Disease Prevention Trials? The Case for Genetically At-Risk Cohorts. Neurology 2022, 99, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Schneider, R.B.; Myers, T.L.; Rowbotham, H.M.; Luff, M.K.; Amodeo, K.; Sharma, S.; Wilson, R.; Jensen-Roberts, S.; Auinger, P.; McDermott, M.P.; Alcalay, R.N.; Biglan, K.; Kinel, D.; Tanner, C.; Winter-Evans, R.; Augustine, E.F.; Cannon, P.; Me Research, T.; Holloway, R.G.; Dorsey, E.R. A Virtual Cohort Study of Individuals at Genetic Risk for Parkinson's Disease: Study Protocol and Design. J Parkinsons Dis 2020, 10, 1195–1207. [Google Scholar] [CrossRef] [PubMed]
- Cox, C.G.; Davis, M.A.; Grill, J.D.; Roberts, J.S. US Adults' Likelihood to Participate in Dementia Prevention Drug Trials: Results from the National Poll on Healthy Aging. J Prev Alzheimers Dis 2023, 10, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Sertkaya A, AnnaBerlind, Ayesha Eyraud, John (2014) ASPE Reports, Washington, DC, p. 92.
- (2020).
- (2021), Bethesda, MD.
- TransCelerate Biopharma Toolkits Core Team; Elmer, M.; Florek, C.; Gabryelski, L.; Greene, A.; Inglis, A.M.; Johnson, K.L.; Keiper, T.; Ludlam, S.; Sharpe, T.J.; Shay, K.; Somers, F.; Sutherland, C.; Teufel, M.; Yates, S. Amplifying the Voice of the Patient in Clinical Research: Development of Toolkits for Use in Designing and Conducting Patient-Centered Clinical Studies. Ther Innov Regul Sci 2020, 54, 1489–1500. [Google Scholar] [PubMed]
- Harrington, R.L.; Hanna, M.L.; Oehrlein, E.M.; Camp, R.; Wheeler, R.; Cooblall, C.; Tesoro, T.; Scott, A.M.; von Gizycki, R.; Nguyen, F.; Hareendran, A.; Patrick, D.L.; Perfetto, E.M. Defining Patient Engagement in Research: Results of a Systematic Review and Analysis: Report of the ISPOR Patient-Centered Special Interest Group. Value Health 2020, 23, 677–688. [Google Scholar] [CrossRef]
- Lowe, M.M.; Blaser, D.A.; Cone, L.; Arcona, S.; Ko, J.; Sasane, R.; Wicks, P. Increasing Patient Involvement in Drug Development. Value Health 2016, 19, 869–878. [Google Scholar] [CrossRef]
- Sacristan, J.A.; Aguaron, A.; Avendano-Sola, C.; Garrido, P.; Carrion, J.; Gutierrez, A.; Kroes, R.; Flores, A. Patient involvement in clinical research: why, when, and how. Patient Prefer Adherence 2016, 10, 631–640. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, K.; White, J. Democratizing clinical research. Nature 2011, 474, 277–278. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury K, Christopher S, Foley J, Grossman C, Haas KL, Hemphill R, Massoud A, McCarty M, Nguyen M, Otlewski M, Rhim C, Saha A, Selig W, Tarver M, Rincon-Gonzalez L, Steele D (2021) Maximizing Patient Input in the Design and Development of Medical Device Clinical Trials. A Report of the Science of Patient Input Program of the Medical Device Innovation Consortium (MDIC). Arlington, VA.
- Johns H, Chowdhury S, Simon G, Corrigan P (2014) Presidential Commission for the Study of Bioethical Issues, Transcript, Meeting 17, Session 4. Atlanta, GA.
- Hewlett, S.; Wit, M.; Richards, P.; Quest, E.; Hughes, R.; Heiberg, T.; Kirwan, J. Patients and professionals as research partners: challenges, practicalities, and benefits. Arthritis Rheum 2006, 55, 676–680. [Google Scholar] [CrossRef]
- Morel, T.; Cleanthous, S.; Andrejack, J.; Barker, R.A.; Blavat, G.; Brooks, W.; Burns, P.; Cano, S.; Gallagher, C.; Gosden, L.; Siu, C.; Slagle, A.F.; Trenam, K.; Boroojerdi, B.; Ratcliffe, N.; Schroeder, K. Patient Experience in Early-Stage Parkinson's Disease: Using a Mixed Methods Analysis to Identify Which Concepts Are Cardinal for Clinical Trial Outcome Assessment. Neurol Ther 2022, 11, 1319–1340. [Google Scholar] [CrossRef]
- Chalmers, I.; Glasziou, P. Avoidable waste in the production and reporting of research evidence. Obstet Gynecol 2009, 114, 1341–1345. [Google Scholar] [CrossRef]
- Stergiopoulos, S.; Michaels, D.L.; Kunz, B.L.; Getz, K.A. Measuring the Impact of Patient Engagement and Patient Centricity in Clinical Research and Development. Ther Innov Regul Sci 2020, 54, 103–116. [Google Scholar] [CrossRef] [PubMed]
- Crocker, J.C.; Ricci-Cabello, I.; Parker, A.; Hirst, J.A.; Chant, A.; Petit-Zeman, S.; Evans, D.; Rees, S. Impact of patient and public involvement on enrolment and retention in clinical trials: systematic review and meta-analysis. BMJ 2018, 363, k4738. [Google Scholar] [CrossRef]
- Domecq, J.P.; Prutsky, G.; Elraiyah, T.; Wang, Z.; Nabhan, M.; Shippee, N.; Brito, J.P.; Boehmer, K.; Hasan, R.; Firwana, B.; Erwin, P.; Eton, D.; Sloan, J.; Montori, V.; Asi, N.; Dabrh, A.M.; Murad, M.H. Patient engagement in research: a systematic review. BMC Health Serv Res 2014, 14, 89. [Google Scholar] [CrossRef]
- Malkani, R.G.; Wenger, N.S. REM Sleep Behavior Disorder as a Pathway to Dementia: If, When, How, What, and Why Should Physicians Disclose the Diagnosis and Risk for Dementia. Curr Sleep Med Rep 2021, 7, 57–64. [Google Scholar] [CrossRef]
- Kim, S.Y.; Karlawish, J.; Berkman, B.E. Ethics of genetic and biomarker test disclosures in neurodegenerative disease prevention trials. Neurology 2015, 84, 1488–1494. [Google Scholar] [CrossRef]
- Schaeffer, E.; Rogge, A.; Nieding, K.; Helmker, V.; Letsch, C.; Hauptmann, B.; Berg, D. Patients' views on the ethical challenges of early Parkinson disease detection. Neurology 2020, 94, e2037–e2044. [Google Scholar] [CrossRef] [PubMed]
- Deslippe, A.L.; Soanes, A.; Bouchaud, C.C.; Beckenstein, H.; Slim, M.; Plourde, H.; Cohen, T.R. Barriers and facilitators to diet, physical activity and lifestyle behavior intervention adherence: a qualitative systematic review of the literature. Int J Behav Nutr Phys Act 2023, 20, 14. [Google Scholar] [CrossRef] [PubMed]
- Gossard, T.R.; Teigen, L.N.; Yoo, S.; Timm, P.C.; Jagielski, J.; Bibi, N.; Feemster, J.C.; Steele, T.; Carvalho, D.Z.; Junna, M.R.; Lipford, M.C.; Tippmann Peikert, M.; LeClair-Visonneau, L.; McCarter, S.J.; Boeve, B.F.; Silber, M.H.; Hirsch, J.; Sharp, R.R.; St Louis, E.K. Patient values and preferences regarding prognostic counseling in isolated REM sleep behavior disorder. Sleep 2023, 46, zsac244. [Google Scholar] [CrossRef] [PubMed]
- Perez-Carbonell, L.; Simonet, C.; Chohan, H.; Gill, A.; Leschziner, G.; Schrag, A.; Noyce, A.J. The Views of Patients with Isolated Rapid Eye Movement Sleep Behavior Disorder on Risk Disclosure. Mov Disord 2023, 38, 1089–1093. [Google Scholar] [CrossRef] [PubMed]
- Howell, M.; Avidan, A.Y.; Foldvary-Schaefer, N.; Malkani, R.G.; During, E.H.; Roland, J.P.; McCarter, S.J.; Zak, R.S.; Carandang, G.; Kazmi, U.; Ramar, K. Management of REM sleep behavior disorder: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med 2023, 19, 759–768. [Google Scholar] [CrossRef] [PubMed]
- Salmi, L.; Blease, C.; Hagglund, M.; Walker, J.; DesRoches, C.M. US policy requires immediate release of records to patients. BMJ 2021, 372, n426. [Google Scholar] [CrossRef] [PubMed]
- Boeve, B.F. REM sleep behavior disorder: Updated review of the core features, the REM sleep behavior disorder-neurodegenerative disease association, evolving concepts, controversies, and future directions. Ann N Y Acad Sci 2010, 1184, 15–54. [Google Scholar] [CrossRef] [PubMed]
- Fereshtehnejad, S.M.; Yao, C.; Pelletier, A.; Montplaisir, J.Y.; Gagnon, J.F.; Postuma, R.B. Evolution of prodromal Parkinson's disease and dementia with Lewy bodies: a prospective study. Brain 2019, 142, 2051–2067. [Google Scholar] [CrossRef] [PubMed]
- Miller-Patterson, C.; Hsu, J.Y.; Willis, A.W.; Hamedani, A.G. Functional Impairment in Individuals With Prodromal or Unrecognized Parkinson Disease. JAMA Neurol 2023, 80, 200–204. [Google Scholar] [CrossRef]
- Yeung, L.K.; Alschuler, D.M.; Wall, M.; Luttmann-Gibson, H.; Copeland, T.; Hale, C.; Sloan, R.P.; Sesso, H.D.; Manson, J.E.; Brickman, A.M. Multivitamin Supplementation Improves Memory in Older Adults: A Randomized Clinical Trial. Am J Clin Nutr 2023, 118, 273–282. [Google Scholar] [CrossRef]
- National Academies of Sciences, Engineering, and Medicine, Health and Medicine Division, Board on Health Sciences Policy, Committee on the Return of Individual-Specific Research Results Generated in Research Laboratories (2018) In Returning Individual Research Results to Participants: Guidance for a New Research Paradigm, Downey AS, Busta ER, Mancher M, Botkin JR, eds., Washington (DC).
- Secretary's Advisory Committee on Human Research Protections (2016) Attachment B: Return of Individual Research Results. Sharing Study Data and Results: Return of Individual Results. U.S. Department of Health and Human Services.
- Schroeder, K.; Bertelsen, N.; Scott, J.; Deane, K.; Dormer, L.; Nair, D.; Elliott, J.; Krug, S.; Sargeant, I.; Chapman, H.; Brooke, N. Building from Patient Experiences to Deliver Patient-Focused Healthcare Systems in Collaboration with Patients: A Call to Action. Ther Innov Regul Sci 2022, 56, 848–858. [Google Scholar] [CrossRef] [PubMed]
- Adler, C.H.; Beach, T.G.; Hentz, J.G.; Shill, H.A.; Caviness, J.N.; Driver-Dunckley, E.; Sabbagh, M.N.; Sue, L.I.; Jacobson, S.A.; Belden, C.M.; Dugger, B.N. Low clinical diagnostic accuracy of early vs advanced Parkinson disease: clinicopathologic study. Neurology 2014, 83, 406–412. [Google Scholar] [CrossRef] [PubMed]
- Swarztrauber, K.; Graf, E. Nonphysicians' and physicians' knowledge and care preferences for Parkinson's disease. Mov Disord 2007, 22, 704–707. [Google Scholar] [CrossRef] [PubMed]
- Alcalay, R.N.; Kehoe, C.; Shorr, E.; Battista, R.; Hall, A.; Simuni, T.; Marder, K.; Wills, A.M.; Naito, A.; Beck, J.C.; Schwarzschild, M.A.; Nance, M. Genetic testing for Parkinson disease: current practice, knowledge, and attitudes among US and Canadian movement disorders specialists. Genet Med 2020, 22, 574–580. [Google Scholar] [CrossRef]
- Thompson, M.R.; Stone, R.F.; Dan Ochs, V.; Litvan, I. Primary health care providers' knowledge gaps on Parkinson's disease. Educ Gerontol 2013, 39, 856–862. [Google Scholar] [CrossRef]
- Taylor, D.H., Jr.; Cook-Deegan, R.M.; Hiraki, S.; Roberts, J.S.; Blazer, D.G.; Green, R.C. Genetic testing for Alzheimer's and long-term care insurance. Health Aff (Millwood) 2010, 29, 102–108. [Google Scholar] [CrossRef]
- Patient Protocol Engagement Toolkit,TransCelerate Biopharma Inc, https://www.transceleratebiopharmainc.com/ppet/planning-for-patient-engagement/, November 20, 2023.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



