
Submitted:
18 December 2023
Posted:
19 December 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background: The COVID-19 pandemic has presented numerous challenges to global healthcare system and emerging evidence suggests a potential link between COVID-19 treatment, specifically steroid therapy, and the development of avascular necrosis (AVN) of the hip. This review aims to provide a comprehensive overview of recent studies and case reports investigating the relationship between COVID-19, corticosteroid therapy, and the development of AVN. Understanding the nuances of AVN in the context of COVID-19 is crucial for healthcare professionals to navigate treatment decisions and mitigate potential complications. Materials and Methods: The Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) was used in the systematic review until September 1st, 2023. The full-texts of the remaining twenty-three (n=23) articles were independently reviewed by the authors of this review. Conclusions: The association between steroid therapy for COVID-19 and the development of hip AVN is a noteworthy concern even though, no relationship is evident between the duration of treatment, cumulative dosage of medication, maximum daily dosage received, and the presence of AVN. Further research with larger cohorts and long-term follow-up is needed to better understand the causative relationship and optimal management strategies for hip AVN in the context of COVID-19 and steroid therapy
Keywords:
COVID-19
; AVN
; bone avascular necrosis
; osteonecrosis
; hip pain
; steroids
1. Introduction
The COVID-19 pandemic has presented numerous challenges to global healthcare system, and as healthcare professionals continue to explore the long-term consequences of the infection, emerging evidence suggests a potential link between COVID-19 infection and treatment, specifically steroid therapy, and the development of avascular necrosis (AVN) of the hip.
COVID-19 infection is tethered to endothelial damage and with the combination of steroid therapy, microthrombi begin to form and can cause osteonecrosis. COVID-19 triggers systemic inflammation leading to an influx of cytokines that prevent the osteoblast from proliferating and differentiating. Moreover, pro-inflammatory proteins cause vasculitis, hypercoagulability and bone necrosis, and the result can be avascular necrosis (AVN) (1). While various factors contribute to AVN, emerging evidence suggests a potential association between osteonecrosis and COVID-19, the disease originated by the novel coronavirus. The interplay between viral infections, the immune response, and the use of corticosteroids, a common therapeutic intervention for severe COVID-19 cases, has raised concerns about its impact on joint health.
AVN is a debilitating condition characterized by the death of bone tissue due to lack of blood supply, often leading to joint destruction and significant morbidity. Studies report 12% of joint pain following the infection and 9% of patients complain about mobility difficulties (2). AVN can be found mainly after prolonged therapies with high dose of steroid treatment, probably due to a combination of fat embolism, lipid abnormalities and coagulation defects (3). The altered lipid metabolism can result in fat accumulation in bone marrow which will increase the intramedullary pressure and decrease the blood supply of the bones. The estimated cumulative dose, which was measured at 2000mg of prednisolone, is a risk of osteonecrosis (ONC) and depends on the type of steroid, the daily dosage and the duration of treatment (4). In addition to this, the COVID-19 antiviral treatments, like ritonavir and lopinavir, are incriminated for ONC (5).
The incidence of hip AVN in patients recovering from COVID-19 and receiving steroid therapy varies among the studies and there is no report till know, establishing the incidence of femoral head osteonecrosis (FHOn). Even though the exact cumulative steroid dose and the duration of COVID-19 treatment, that can lead to AVN is not yet established, it is known that the longer treatment duration, the severity of infection, admission in the ICU and the personal history count as potential risk factors (6). Close follow-up with MRI of the major joints is suggested for the first 3 months after a SARS infection, in order to treat the damage and save the joint, especially in young active patients. Symptoms of hip AVN typically manifested several weeks to months after COVID-19 infection and steroid treatment. The literature illustrates the importance of MRI in diagnosis of AVN, and more specifically as an early-stage diagnosis (7), as it may aid in choosing between surgical or nonsurgical type of treatment (8). Femoral head is the most common location for ONC and quite often is bilaterally(9), but signs of necrosis can be found in other parts like the shoulder, knee and ankle(10). Appears to be a correlation between the use of steroids, particularly methylprednisolone and dexamethasone, in the treatment of moderate to severe COVID-19 and the subsequent development of hip AVN (11). Further research with larger cohorts and long-term follow-ups is needed, to better understand the causative relationship and optimal management strategies for hip AVN in the context of COVID-19 and steroid therapy.
This review aims to provide a comprehensive overview of recent studies and case reports, investigating the relationship between COVID-19, corticosteroid therapy, and the development of AVN. The presented cases span diverse demographics and severity levels, shedding light on the clinical outcomes and management strategies employed. Understanding the nuances of AVN in the context of COVID-19 is crucial for healthcare professionals to navigate treatment decisions and mitigate potential complications.
2. Materials and Methods
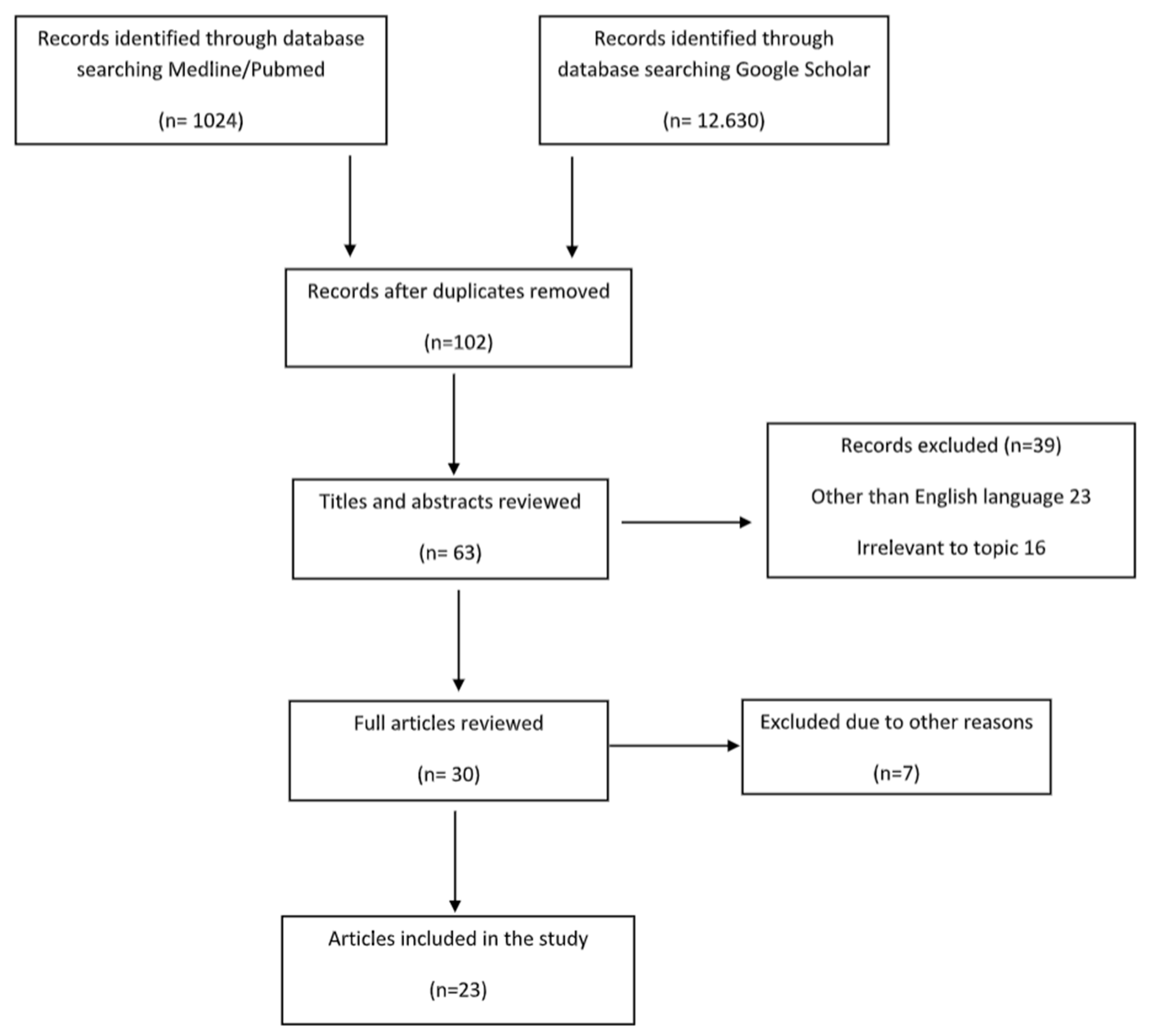
The Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) was used in the systematic review and no ethical approval was needed, because the information was from published literature. The studies that were identified and included, were written in the English language and designed to illustrate the appearance of bone avascular necrosis after COVID 19 infection or vaccination. A comprehensive and systematic search for articles published in computerized literature databases (MEDLINE/Pubmed and Google Scholar) from 2022 to September 2023, containing the keyword terms COVID 19 and joint pain and bone avascular necrosis and bone osteonecrosis was performed. Reference lists from articles that met the inclusion criteria were further investigated.
Relevant studies were selected for inclusion based on the following predetermined eligibility criteria:
- Articles in English
- COVID-19 infection or vaccination
- No joint pain prior to the infection
- Musculoskeletal symptoms after COVID-19
- Patients over 18 years old
The search using the aforementioned keywords yielded 13.654 articles, until September 1st, 2023. The studies were analysed for duplication with resulting number of studies to 102. The authors independently reviewed the titles and abstract of each result, and those that were clearly irrelevant and/or failed to pertain to the pre-determined inclusion criteria (n=39) were eliminated. The remaining seventy-five (n=30) articles were further scrutinized for clearly relevant trials that indisputably met the inclusion criteria, eliminating a further 7 trials. The full-texts of the remaining twenty-three (n=23) articles were independently reviewed by the authors of this review, who agreed upon all twenty-three remaining articles to be objectively relevant to this summary in discussion.
3. Results
3.1. Demographics
Twenty-three articles are included in the study and 613 patients in total. 62% of them are males and the rest are females. The estimated mean age is 42,9 years old, ranging from 19 to 63 years old. It is important to be noted, that a lot of patients had bilateral joint pain and signs of AVN after the COVID-19 infection. The majority of the articles are case reports, illustrating mostly one patient and some of them reference up to 5 different patients (21). The prospective study by Veizi et al (7) is the biggest study so far, concerning the number of patients, with 472 people. All of the patients show symptoms of hip osteonecrosis, except for the study by Kashkosh et al (24), in which, the patient had humeral head pain, only two days after the second dose of Pfizer COVID-19 vaccine.
3.2. Course of COVID-19 infection
The infection's severity varied, with mild, moderate, and severe cases being observed. Mild infections in the studies were scarce with only 11 patients, while the majority of the patients had mostly moderate and some moderate to severe symptoms. 18 out of 23 articles are related to severe COVID-19 infection.
Clinical signs of musculoskeletal symptoms typically manifested within a range of days to a few months after the COVID-19 infection, with an average of 85 days. The shortest period is 14 days (31) and the longer duration for the AVN symptoms to appear is 300 days (20). Generally, joint discomfort occurred after the resolution of acute respiratory symptoms and elevated body temperature.
3.3. COVID-19 treatment
The treatment for moderate to severe cases is consisted of antiviral therapy and corticosteroids, which could be administered either intravenously, either oraly. Three studies combined the antiviral medication with steroids (12)(17)(22), while at the same time three other studied, did not use any corticosteroid (18)(19)(25). However, Veizi et al (7), divided the patients into two groups and half of them were treated with steroid and the rest, without. Corticosteroids, commonly used in COVID-19 treatment are dexamethasone, methylprednisolone and prednisolone and are associated with potential complications such as femoral head osteonecrosis (FHOn). Their doses varied widely, ranging from 40 mg to 20,675 mg prednisolone equivalents, while the treatment duration differed, from a few days to several weeks. A cumulative dose of 2000 mg of prednisolone or equivalent is linked to an increased risk for AVN. While corticosteroids have shown benefits in treating severe COVID-19 cases, the text raises concerns about potential long-term complications. It emphasizes the need for a balance between the benefits of treatment and the risks of complications.
3.4. AVN treatment approaches and outcome measures
In six studies, the patients initially undergone conservative treatment, which constituted by NSAIDS, physical therapy(12)(19), intra-articular (IA) steroid injections, oral or IV steroid medication and bisphosphonates(16)(18). Concerning the mobility, patients modified their activities and had protected bare weight. In one study, the patients received and IA hydrodilatation injection (24). Out of those articles, the conservative treatment succeeded only in 2 studies, with clinical improvement (12) and a mean VAS score 2.7 (16), while in the rest, the patients had surgical intervention, like core decompression, total hip arthroplasty (THA), and bone marrow aspirate concentrate (BMAC) injection. As for core decompression, it was combined with BMAC in three studies (17)(27)(29) out of the ten that it was used. Furthermore, total hip arthroplasty was paired with decompression of the necrosis foci, in the study by Annam et al (22) for the younger patient. For the rest of the patients, that were treated with THA, the results indicated improvement in motor activity, decrease in pain intensity, without though having significant improvement in MRI. The mean VAS score lessened from 9.4 to 2.8 in the first postoperative week (21). Some cases did not receive specific treatment for AVN and in general the response to treatment varied, while some patients improved with conservative measures, while others required surgical intervention. Only one case involved infection post-THA and needed a two-stage THA (21). As for the radiological outcomes, in some cases, there was improvement seen in imaging studies, but not in all. However, Veizi et al (7) highlighted that there is no relationship between the treatment duration, cumulative dosage of medication and ONC.
3.5. Follow-up period
The text highlights persistent symptoms, including fatigue, shortness of breath, anxiety, depression, joint pain, and stiffness, in COVID-19 survivors at one-year follow-up. Joint pain and stiffness are underreported in long-term studies. The majority of the studies have followed-up their patients for an average of 3-4 months and only one study had long term outcomes at 25 months (28). The impact of SARS-CoV-2 infection and therapeutic interventions on the skeletal system, especially AVN, is not thoroughly investigated. The text emphasizes the need for further studies to identify risk factors, determine the incidence of FHOn, and establish protocols for early diagnosis and intervention. The study also highlights gaps in existing studies, such as inconsistent reporting of musculoskeletal symptoms and a lack of emphasis on FHOn incidence. It suggests that future research should include comprehensive musculoskeletal evaluations in the post-acute phase of COVID-19.

| Scheme . | Study Design | No of Patients and Gender | Mean age (years) | COVID Symptoms | Treatment COVID | Days till AVN | AVN TREATMENT | Results |
|---|---|---|---|---|---|---|---|---|
| 1.Sulewski et al (2021)(3) | Cohort study | 10(6 F +4M) | 58.8 | Moderately severe | Steroids | Initially conservatively (NSAIDs, IA steroid inj) with no improvement Oral Dexamethasone 2x8 mg daily for 2 weeks |
30% THA with good clinical outcome 10% chronic pain without joint destruction in the control tests |
|
| 2.Alkindi et al (2021)/(12) | Case report | 1 M | 29 | Combination of experimental anti-COVID-19 therapies (favipiravir, hydroxychloroquine, tocilizumab) Methylprednisolone IV 40mg/d for 5 days |
IV corticosteroids for 5 days (cumulative dose: 200 mg) |
Clinical improvement with NSAIDs and PT | ||
| 3.Daltro et al (2021)/ (13) | Follow up | 14 M + 9 F | 43.5 | 33 % Mild 66% Moderate/Severe |
Mild infection: no hospitalization/ corticosteroid Dexamethasone: min dose 40mg/day for a mean time of 14.6 days (min 15-max 21) |
33% osteonecrosis of the femoral head | ||
| 4.Chacko et al (2021)/ (14) | Case report | 1 M (bilateral) | 23 | IV dexamethasone 6 mg/d for 9 days and IV methylprednisolone 40mg X2/d for 5 days Cumulative dose is equivalent to 860 mg of prednisolone |
56 | Core decompression of femoral heads Bone marrow aspirate concentrate injection |
||
| 5.Joshi et al (2021)/(15) | Case report | 1 F (bilateral) | 31 | Moderate/Severe | Methylprednisolone 32 mg/d for 7 days with minimal improvement Continued for 10 days more Total dose 544 mg |
30 | N/G | |
| 6.Agarwala et al (2021)/ (16) | Case report | 3M (bilateral) | 37 | Moderate/Severe | Mean equivalent to 758mg of prednisolone | 58 | Oral alendronate 70mg/w IV zoledronic acid 5 mg /annually |
Mean VAS: 2.7 No surgery |
| 7.Panin et al(2022)/ (17) | Case report | 4 (2M/2F) (bilateral) | 34 | Moderate/Severe | Mean total dose of dexamethasone/prednisolone 264 (80-600mg)/1759 (533-4000mg) 1patient: iv favipiravir, tocilizumab 2nd: iv triazaverin |
96.6 | 2 Decompression of the necrosis foci Administration of a bone marrow concentrate 1THA Statins Bisphosphonates Anticoagulants |
Improvement in motor activity Decrease in pain intensity No significant improvement in MRI |
| 8.Uyshal et al (2022) / (18) | Case report | 1 M | 63 | Mild/moderate | No steroid usage | Protected weight bearing Oral alendronate 70mg/w (no improvement) THA |
||
| 9.Ergün et al (2022) / (19) | Case Report | 1 F (bilateral) | 51 | No prior use of steroid Favipiravir LMWH |
60 | Core decompression PT No weight bearing for 6weeks |
Improved clinical scores No femoral head subchondral bone collapse |
|
| 10.Kingma et al (2022)/ (20) | Case report | 1 M (bilateral) | 60 | Severe | Total dose of prednisone equivalent 1,327.5 mg | 300 | Bilateral THA | No complications |
| 11. Ardakani et al (2022)/ (21) | Case series | 5 (2M/3F) | 38,4 | Moderate/Severe | Mean dose of prednisolone was 1695.2 mg | 41.6 | All patients underwent surgery with direct anterior approach 1 did two-stage THA due to Serratia marcescens infection in both hips |
Clinical and laboratory symptoms improved significantly Mean VAS decreased from 9.4 to 2.8 1week post-operation |
| 12. Annam et al (2022)/ (22) | Case report | 2 M (bilateral) | 48 (27/69) | Moderate | Oseltamivir, Doxycycline, and Methylprednisolone Mean total dose of methylprednisolone 588 mg, equivalent to 735 mg of prednisolone |
The younger had bilateral THA and hip core decompression The older left THA and Right hip decompression |
||
| 13. Kamani et al (2022)/ (23) | Case report | 1 M (bilateral) | 40 | Severe | Steroid injection | Bilateral Core decompression hip surgery PT |
||
| 14. Kashkosh et al (2022)/ (24) | Case report | 1 M | 40 | Second dose of the Pfizer COVID-19 vaccine | AVN of the Humeral head |
2 | Analgesics Activity modification IA hydrodilatation inj |
Improved ROM Severe shoulder pain Surgical intervention |
| 15. Jyothiprasanth et al (2023)/ (25) | Cohort study | 17 (10 M/ 7F)/ 4bilateral | 37 | 82.4% COVID19 Inf | No steroid therapy | 66 | N/G | |
| 16. Baimukhamedov (2023)/ (8) | Cohort study | 8 M | N/G | N/G | Range of cumulative corticosteroid doses 50–20,675 mg prednisolone |
N/G | N/G | |
| 17. Karpur et al (2023)/ (26) | Follow-up | 20 (14M/6F) | N/G | N/G | N/G | N/G | N/G | Stage I: 45% Stage II: 40% M/F: 70/30 % |
| 18. Shershahet al (2023)/ (27) | Case reports | 3 (2M/1F) bilateral | 29.3 | Severe | 560mg IV methylprednisolone | 240 | Conservative without results 2 Bilateral THA 1 core decompression with bone marrow aspirate infiltration |
|
| 19. Velchov et al (2023)/ (28) | Follow-up | 24 (17M/7F) 4 bilateral |
55.6 | 8 Moderate/ 16 Severe | Moderate: mean 120mg Dexamethasone Severe: also, 3600mg Methylprednisolone |
56.3 | 23 THAs 5 Core decompression |
|
| 20. Jayapalan et al (2023)/ (29) | Case report | 1M (bilateral) | 31 | Moderate | IV methylprednisolone (600 mg) followed by an oral dose 8 mg | 65 | Bilateral core decompression and BMAC | |
| 21. Parikh et al (2023)/ (30) | Case reports | 3 (2M/1F) |
55.6 | Moderate | Steroid treatment | N/G | Core decompression (1bilateral) | |
| 22. Sinha et al (2023)/ (31) | Cohort study | 10 (4M/6F) | 53.9 | 7Moderate/3 Severe | 4 steroid therapies | 14 | 4 core decompression | |
| 23. Veizi et al (2023)/ (7) | Prospective study | 472 (289 M/183F) | 42 | Group 2: (236) received steroid treatment | Increased % of AVN in Group 2 Joint pain: 5.1% Group 1 11.9% in Group 2 AVN: 8pts from Group 2 |
No relationship between the treatment duration, cumulative dosage of medication and ONC |
Figure 1.
MRI of bilateral avascular necrosis of the hip after Covid-19 infection and treatment in ICU unit of our department.
Figure 1.
MRI of bilateral avascular necrosis of the hip after Covid-19 infection and treatment in ICU unit of our department.
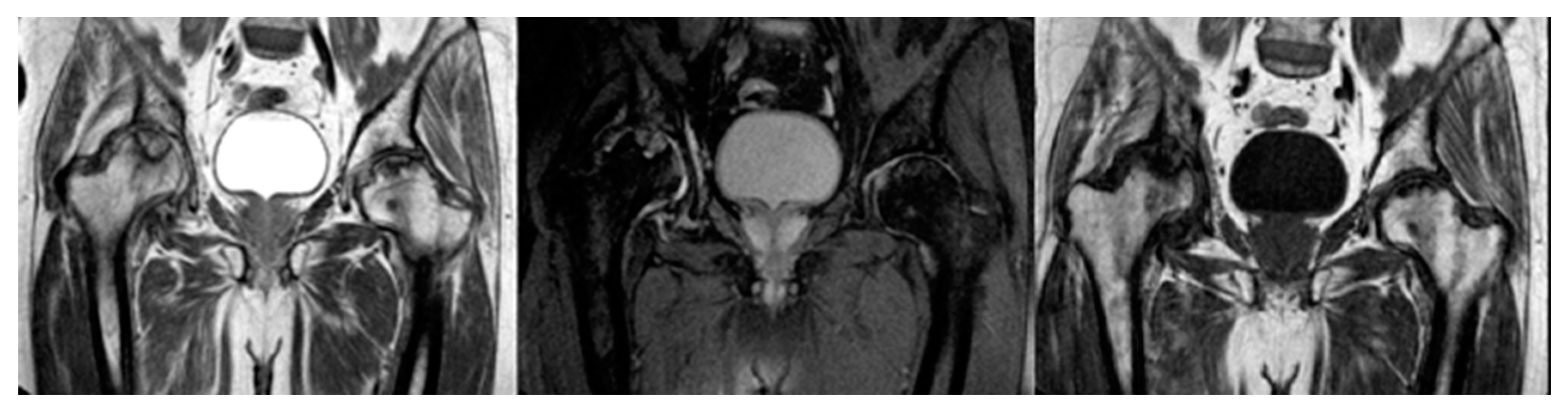
Figure 2.
Treatment of AVN with Total Hip Arthroplasty.
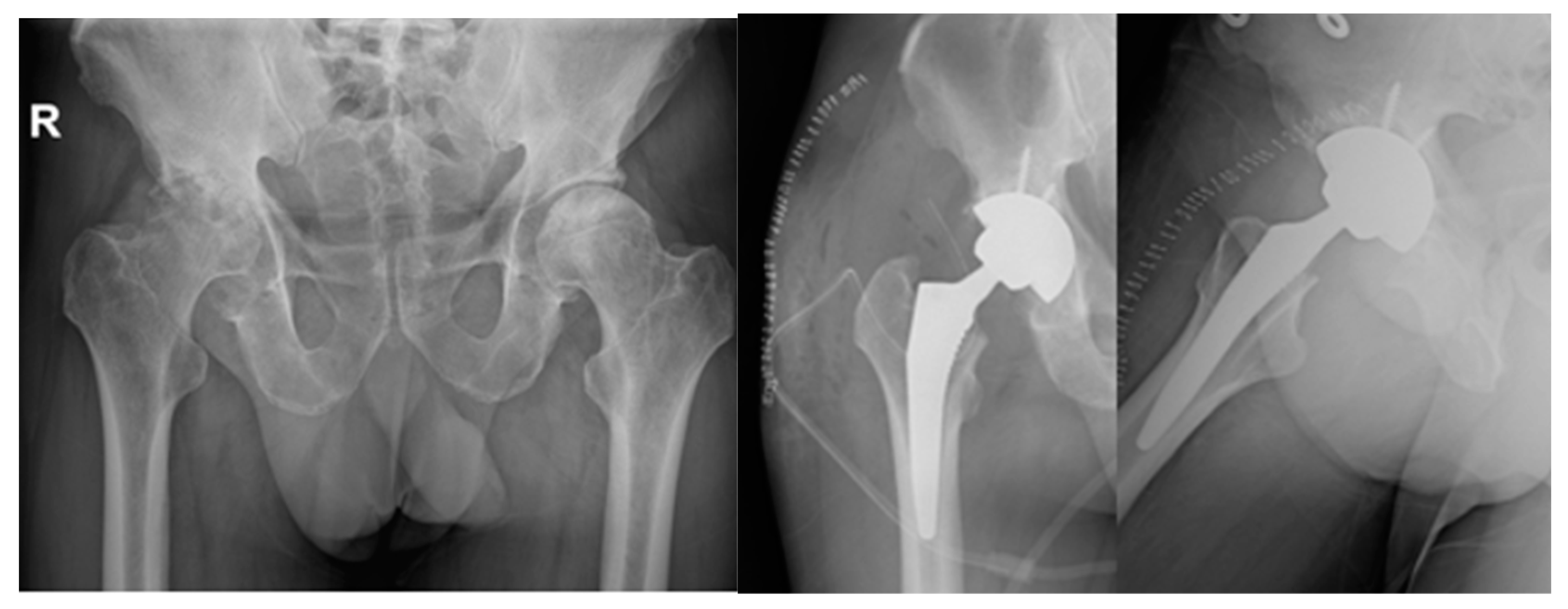
Figure 3.
MRI of bilateral AVN of humerus head (left).
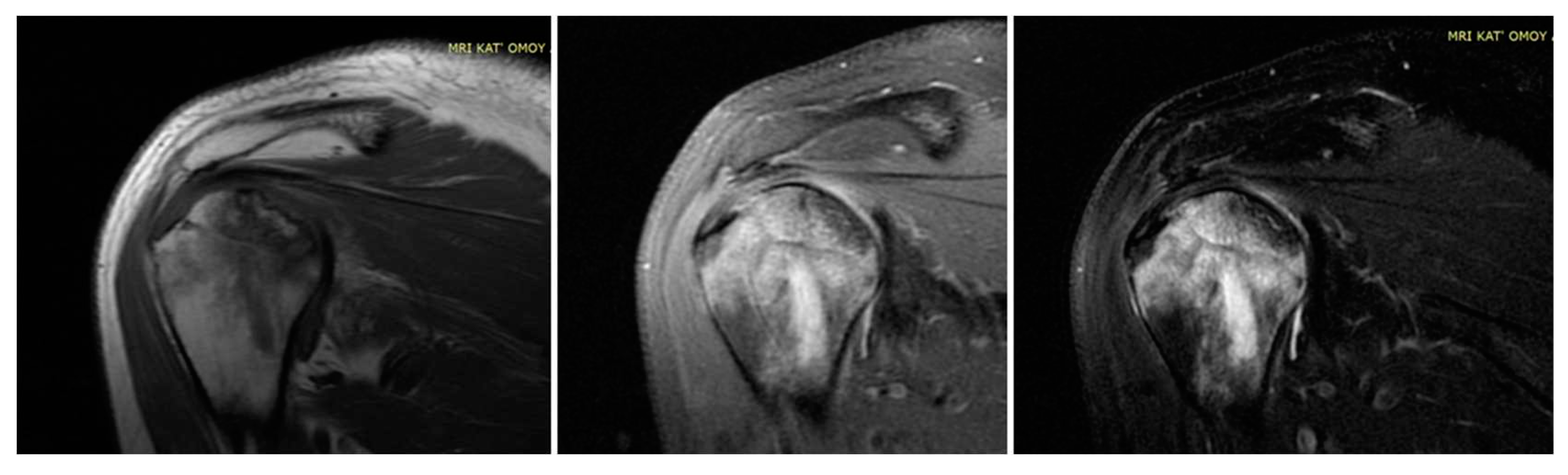
Figure 4.
MRI of bilateral AVN of humerus head (Right).
4. Discussion
As the medical community strives to comprehend the multifaceted implications of COVID-19 and its treatments, this review contributes to the ongoing dialogue surrounding the intricate relationship between steroid therapy and the risk of hip AVN. Understanding these associations is crucial for forming clinical decision-making and developing targeted interventions to optimize patient outcomes in the aftermath of COVID-19 infection. This review article aims to provide a comprehensive analysis of avascular necrosis (AVN) cases in orthopaedic department, associated with steroid use in the context of COVID-19 treatment. The included studies present a diverse range of cases, encompassing various patient demographics, severity of COVID-19, steroid regimens, and outcomes. The objective is to synthesize the existing literature, identify common trends, and draw insights into the management and potential preventive strategies for steroid-induced AVN.
Several factors may contribute to the development of AVN in individuals with a history of COVID-19 infection and steroid therapy. It is important to mention the vascular effects, as COVID-19 has been associated with vascular complications, including thrombosis and damage to blood vessels, but also disruption of blood supply to the bones that can contribute to AVN. Next, the body's immune response to the viral infection, as well as the anti-inflammatory effects of steroid therapy, may play a role in disrupting the normal bone repair and maintenance processes. The steroid treatment each self, particularly at higher doses and for prolonged duration, can have negative effects on bone health. They may affect bone remodelling and decrease bone density, potentially contributing to AVN. Moreover, some individuals may be more predisposed to developing AVN due to genetic or other factors, as Karpur et al (26) demonstrated that males are affected more than females, with a ratio of 7/3, and the combination of COVID-19 infection and steroid therapy may exacerbate this susceptibility. Varius treatments exist for COVID-19 depending on the severity of the infection. Corticosteroid and antiviral medication are the most effective so far and commonly used. One of the most important complications of the steroids, linked to the orthopaedic world is the avascular necrosis and usually in the femoral head (FHOn), through disrupting the balance between bone formation and resorption, leading to decreased bone density and compromising blood supply to the bones. Veizi et al (7), in a cohort study of 472 patients, showed increased percentage of hip AVN in patients who received steroid treatment, as also the percentage of joint pain was more than double in this group. However, no relationship was evident between the duration of treatment, cumulative dosage of medication and the presence of osteonecrosis.
The text underscores the importance of healthcare workers' awareness of potential musculoskeletal complications, especially FHOn, in COVID-19 survivors treated with corticosteroids. Early detection through screening and close follow-up is crucial for timely intervention. The incidence of hip AVN in patients recovering from COVID-19 and receiving steroid therapy varies among the studies. Symptoms of hip AVN typically manifested several weeks to months after COVID-19 infection and steroid treatment. The shortest time for the symptoms to develop, was illustrated by Kashkosh et al (24), who published a case report of a 40 years old male patient with symptoms of left humeral head AVN, 2 days after the second dose of the Pfizer COVID-19 vaccine on the same shoulder. Next, Sinha et al (31) in a cohort study of 10 patients, with a mean age of 53.9 years old, who suffered from moderate to severe COVID19 infection, gathered data of hip AVN at around 14 days later and 4 of them needed core decompression surgery. The majority of articles indicate that the FHOn manifests at 30-60 days after the infection, and in some cases can take up to 8-10 months (20)(27).
In our review 613 patients suffered from moderate to severe SARS infection and 255 of them were not treated with steroids. The following studies, highlight the importance of corticosteroid treatment in the development of AVN. Uysal et al (18) reports a case study of a 63 years old male patient, who suffered from moderate to severe COVID-19 infection without steroid treatment. Some days later had symptoms of hip AVN. Treatment was conservatively first with protected weight bearing and oral alendronate. Due to no improvement, THA followed. Next, Ergun et al (19) also treated a 51 years old female patient for COVID-19 infection, without steroids, and 60 days later, had symptoms of bilateral hip AVN that was improved clinically with core decompression, PT and no weight bearing for 6weeks. She did not present femoral head subchondral bone collapse. Jyothiprasanth et al (25), in a cohort study of 17 patients, the majority of whom had COVID-19 infection in the past and were not administered any steroid, presented 2months later with symptoms of hip AVN and 4 of them were bilaterally.
A range of steroid doses and treatment durations was observed across the studies. Even in the corticosteroid department there was a big variance, with the scientists using mostly methylprednisolone, prednisolone and dexamethasone either intravascularly, either orally or in combination. Even in one study ,like the one conducted by Baimukhamedov et al (8), the amount of steroid had a wide range, with a cumulative corticosteroid dose at 50–20.675 mg prednisolone. The biggest portion of steroid was given by Velchov et al (28) who treated the patients with severe infection by administering 120mg dexamethasone with 3600mg methylprednisolone in total. 56 days later, the patients had signs of hip AVN and 4 of them had on both hips. All of them except one undergone THA, and 5 of them had core decompression. Also Panin et al (17), medicated the patients with a mean total dose of dexamethasone/prednisolone 264 (80-600mg)/1759 (533-4000mg) and 96,6 days later had signs of bilateral hip AVN, that was encountered successfully surgically, with improvement in motor activity, decrease in pain intensity but no significant improvement in MRI. In the same area worked Ardakani et al (21) who administered the patients with severe infection with 1695.2 mg mean dose of prednisolone and 40 days later they presented with hip ONC. Generally the most preferred dosage is around 500 and 800 mg methylprednisolone (14)(15), as Jayapalan et al (29) presents a young woman with bilateral hip AVN after a combination of oral and IV methylprednisolone and Daltro et al (32), illustrates a 33% of osteonecrosis of the femoral head, in patients with severe SARS infection. However, Alkindi et al (12) combined experimental anti-COVID-19 therapies (favipiravir, hydroxychloroquine, tocilizumab) and 200 mg methylprednisolone and the patient experienced mild signs of hip AVN, that was improved with NSAIDs and PT.
Another concern after the presentation of the AVN, is the course of treatment, which can be nonoperative with NSAIDS, physical therapy(12)(19), intra-articular (IA) steroid injections, oral or IV steroid medication and bisphosphonates(16)(18) or operative with core decompression, total hip arthroplasty (THA), and bone marrow aspirate concentrate (BMAC) injection. Concerning the conservative treatment Sulewski et al (3), in 70% of patients, after having no positive effect with NSAIDs and IA injection, proceeded to oral steroids with 10% of them experiencing chronic pain without though joint destruction in the control tests. Also Alkindi et al (12) had clinical improvement and Agarwala et al (16) used oral alendronate and IV zoledronic acid in patients with bilateral hip AVN, that led to improvement to a mean VAS score 2.7. As for the surgical intervention, the option that was favoured is core decompression often in combination with BMAC and next the THA. Seems that the first type of treatments was chosen mostly for the younger and more active patients (22)(23)(30) and when THA was chosen, the direct approach is the preferred one (21). Only one case by Ardakani et al (21)involved infection post-THA due to Serratia marcescens in both hips and needed a two-stage THA with laboratory and clinically improvement postoperatively.
The text has implications for public health, urging healthcare providers to be vigilant in monitoring and managing post-acute complications in COVID-19 survivors and emphasizes the need for further studies to identify risk factors, determine the incidence of FHOn, and establish protocols for early diagnosis and intervention.
5. Conclusions
The association between steroid therapy for COVID-19 and the development of hip AVN is a noteworthy concern even though, no relationship is evident between the duration of treatment, cumulative dose of medication, maximum daily dosage received, and the presence of AVN. So far, patients with COVID-19 express more pathogenetic factors in developing AVN and especially those treated with corticosteroids. Close monitoring of patients who receive steroids, especially in higher cumulative doses, is crucial for early detection and intervention. Further research with larger cohorts and long-term follow-up is needed, to better understand the causative relationship and optimal management strategies for hip AVN, in the context of COVID-19 and steroid therapy.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
Limitations
The limited sample sizes in some studies may affect the generalizability of the findings. Variability in treatment protocols and patient characteristics makes it challenging to draw definitive conclusions.
References
- Griffith JF. Musculoskeletal complications of severe acute respiratory syndrome. Semin Musculoskelet Radiol. 2011 Nov;15(5):554–60. [CrossRef]
- Huang L, Yao Q, Gu X, Wang Q, Ren L, Wang Y, et al. 1-year outcomes in hospital survivors with COVID-19: a longitudinal cohort study. Lancet (London, England). 2021 Aug;398(10302):747–58. [CrossRef]
- Sulewski A, Sieroń D, Szyluk K, Lukoszek D, Christe A, Dabrowski M, et al. Avascular necrosis bone complication after active COVID-19 infection: Preliminary results. Med. 2021;57(12):1–8. [CrossRef]
- Powell C, Chang C, Naguwa SM, Cheema G, Gershwin ME. Steroid induced osteonecrosis: An analysis of steroid dosing risk. Autoimmun Rev. 2010 Sep;9(11):721–43. [CrossRef]
- Patel TK, Patel PB, Barvaliya M, Saurabh MK, Bhalla HL, Khosla PP. Efficacy and safety of lopinavir-ritonavir in COVID-19: A systematic review of randomized controlled trials. J Infect Public Health. 2021 Jun;14(6):740–8. [CrossRef]
- Shetty GM. Double Trouble-COVID-19 and the Widespread Use of Corticosteroids: Are We Staring at an Osteonecrosis Epidemic? Indian J Orthop. 2022 Feb;56(2):226–36. [CrossRef]
- Veizi E, Erdoğan Y, Sezgin BS, Karaman Y, Kılıçarslan K, Fırat A. The painful joint after COVID-19 treatment: A study on joint osteonecrosis following COVID-19-related corticosteroid use. Jt Dis Relat Surg. 2022;34(1):75–83. [CrossRef]
- Baimukhamedov C, Botabekova A, Lessova Z, Abshenov B, Kurmanali N. Osteonecrosis amid the COVID-19 pandemic. Rheumatol Int [Internet]. 2023;43(7):1377–8. Available from. [CrossRef]
- Freund, E. BILATERAL ASEPTIC NECROSIS OF THE FEMORAL HEAD: PROBLEMS ARISING IN A COMPENSATION CASE. Ann Surg. 1936 Jul;104(1):100–6. [CrossRef]
- Guo KJ, Zhao FC, Guo Y, Li FL, Zhu L, Zheng W. The influence of age, gender and treatment with steroids on the incidence of osteonecrosis of the femoral head during the management of severe acute respiratory syndrome: a retrospective study. Bone Joint J. 2014 Feb;96-B(2):259–62. [CrossRef]
- Koutalos AA, Stefanou N, Malizos KN. Postacute sequelae of SARS-CoV-2 infection. Osteonecrosis must not be overlooked. Int J Infect Dis [Internet]. 2022;121:11–3. Available from. [CrossRef]
- Alkindi F, Al Nokhatha S, Alseiari K, Alnaqb KA. Reactive Hip Arthritis and Avascular Necrosis After Severe COVID-19 Infection: A Case Report and Comprehensive Review of Literature. EMJ Rheumatol. 2022;(March 2022):48–55. [CrossRef]
- Slater G|;, Elliott M, Slater G. Journal of Regenerative Biology and Medicine. J Regen Biol Med [Internet]. 2019;2(1):1–15. Available online: https://www.maplespub.com/webroot/files/Growth-Factors-and-Articular-Cartilage-Rejuvenation-Where-are-we-up-to-with-reversing-OA-_1577100292.
- Chacko A, Babu M, Thomas DK. Osteonecrosis of bilateral femoral head in a post COVID-19 patient: case report. Int J Res Orthop. 2021;7(3):674. [CrossRef]
- Joshi SR, Mahmud CI, Selimullah A, Sidny DNZ. Post COVID-19 osteoporosis and avascular necrosis of femoral head: A case report. Int J Orthop Sci. 2021;7(4):177–9. [CrossRef]
- Agarwala SR, Vijayvargiya M, Pandey P. Avascular necrosis as a part of a € long COVID-19’. BMJ Case Rep. 2021;14(7):1–3. [CrossRef]
- Panin MA, Petrosyan AS, Hadjicharalambous KK, Boiko A V. Avascular Necrosis of the Femoral Head After COVID-19: A Case Series. Travmatol i Ortop Ross [Internet]. 2022;28(1):110–7. [CrossRef]
- UYSAL A, ERDEM UYSAL M. Bilateral Avascular Necrosis of the Femoral Head After COVID-19 Infection: A Case Report. Batı Karadeniz Tıp Derg. 2022;6(2):235–8. [CrossRef]
- Ergün S, Adiyaman C, Sensöz E, Eceviz E. Avascular Necrosis of the Hip Triggered by COVID-19 Infection in a Patient with Sickle Cell Disease: A Case Report. J Orthop Case Reports. 2022;12(6):10–2. [CrossRef]
- Kingma TJ, Hoch V, Johnson C, Chaudhry B. Avascular Necrosis of the Hip: A Post COVID-19 Sequela. Cureus. 2022;14(10). [CrossRef]
- Ardakani MV, Parviz S, Ghadimi E, Zamani Z, Salehi M, Firoozabadi MA, et al. Concomitant septic arthritis of the hip joint and femoral head avascular necrosis in patients with recent COVID-19 infection: a cautionary report. J Orthop Surg Res [Internet]. 2022;17(1):1–11. Available from. [CrossRef]
- Annam P, Manda A, Myneni UK, Sahar AN, Prasad N, Sam KK, et al. Corticosteroids induced avascular necrosis of hip, a “long COVID-19” complication: Case report. Ann Med Surg [Internet]. 2022;82(September):104753. Available from. [CrossRef]
- Kamani S, Lakhwani MG, Phansopkar P. Undiagnosed Bilateral Avascular Necrosis of the Femur in a Young Male Caused by COVID-19 Steroid Injections. Cureus. 2022;14(10). [CrossRef]
- Kashkosh A, Peake CM, Narvani AA, Imam MA. Spontaneous Avascular Necrosis of the Humeral Head Following COVID-19 Vaccination. Arch bone Jt Surg. 2023;11(2):140–3. [CrossRef]
- Jyothiprasanth M, Jithin CR, Vincent A, Thomas AK, Pratheesh CB, Sarang P. A case series on Covid-19 infection and avascular necrosis of hip. J Orthop Reports [Internet]. 2023;2(1):100104. Available from. [CrossRef]
- Karpur S, Baja N, Malikireddy P, Pokuri D. Avascular necrosis of hip joints in post - COVID - 19 patients : A case series. 2023;98–101.
- Shershah K, Chandrashekar M, Ramanand M, Akash K. Bilateral avascular necrosis of femoral head following COVID-19 infection: Case series. Sanamed. 2023;18(1):53–7. [CrossRef]
- Velchov V, Georgiev P, Tserovski S, Tsenkov T, Alexiev V. Corticosteroid-Associated Avascular Necrosis of the Femoral Head in Patients with Severe COVID-19: A Single-Center Study. Med Sci Monit. 2023;29:1–6. [CrossRef]
- Jayapalan Y, Baskar A, Mohan JP, Maheshwaran SMP. Osteonecrosis-An Emerging Challenge of Post COVID-19 Sequalae. Eur J Clin Med. 2023;4(3):4–6. [CrossRef]
- Parikh S, Gomez O, Davis T, Lyon Z, Corces A. Avascular Necrosis as a Sequela of COVID-19: A Case Series. Cureus. 2023;15(2). [CrossRef]
- Sinha PR, Mallick N, Sahu RL. Avascular Necrosis of the Hip after the COVID-19 Pandemic. J Pharm Bioallied Sci. 2023 Jul;15(Suppl 1):S661–4. [CrossRef]
- Daltro G, Franco B, Rosário D, Faleiro T, Lima V, Vitório F, et al. Osteonecrosis Development Post Covid-19 Infection. J Regen Biol Med. 2021 Aug 4;1–8.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



