Submitted:
15 December 2023
Posted:
18 December 2023
You are already at the latest version
Abstract
Objective: To determine if higher weight-to-length z-scores after 32 weeks of gestation are associated with higher Pulmonary Scores (PS) in preterm infants requiring respiratory support using a prospective observational study.
Methods: Infants born <30 weeks, with a post-menstrual age (PMA) of 30-33 weeks were enrolled. Weight, infant’s length, and head circumference were measured weekly. Data on calories/kg/d, protein g/kg/d, weight for length percentiles, z-scores, and BMI at 33 through 40 weeks PMA were collected. PS was calculated.
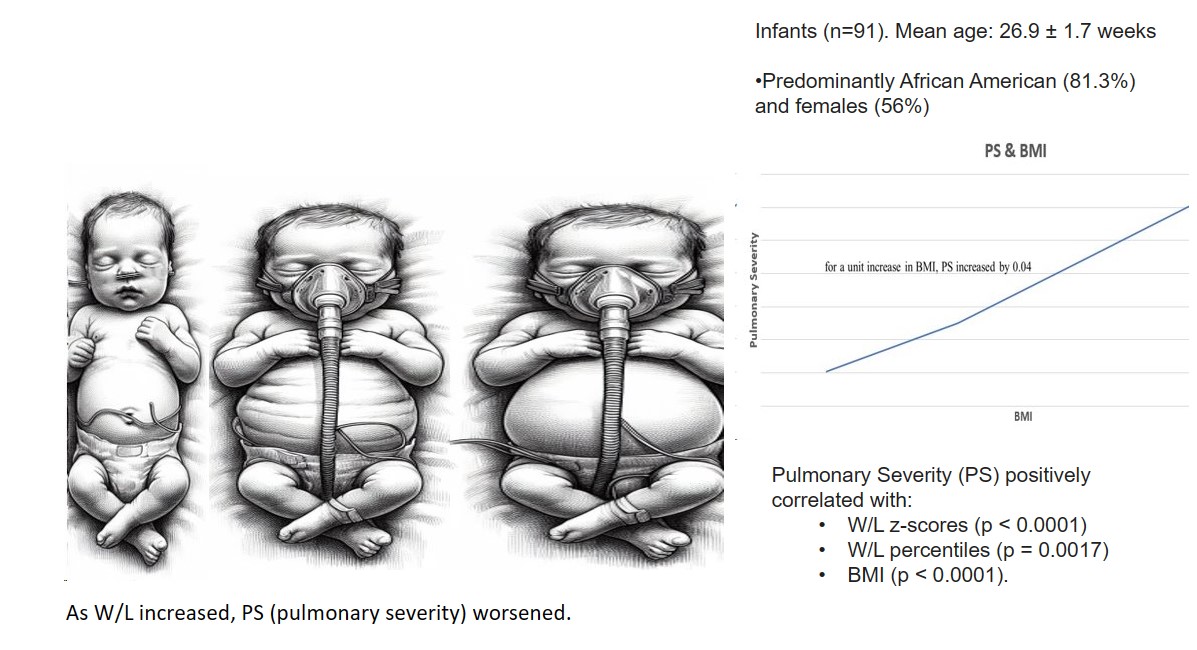
Results: We analyzed 91 infants. The mean gestational age was 26.9 ± 1.7 weeks. There was a significant association between PS and W/L z scores(p<0.0001). For every one-unit increase in W/L z-scores, PS increased by 0.063. There was a significant association between PS and W/L percentiles (p = 0.0017) as well as BMI (p = <0.0001). For every unit increase in W/L percentiles, PS increased by 0.002, and for a unit increase in BMI, PS increased by 0.04. The association remained significant after postnatal steroids, sex, corrected, and birth gestational ages were included in the regression analysis. Nutrition did not affect anthropometric measurements.
Conclusion: Our study is the first to demonstrate that higher BMI and W/L may adversely affect respiratory severity in infants.
Keywords:
weight for length
; BMI
; BPD
; respiratory severity
; preterm
Introduction
Very low birth weight premature infants are at high risk for bronchopulmonary dysplasia (BPD) 1,2, which is a significant contributor to long-term respiratory morbidity in preterm infants. The incidence of BPD decreases as gestational age at birth increases. Severely affected lungs may not be able to keep up with the increased metabolic demands of the body. This may be further complicated if the body weight outgrows the linear growth, as severely affected lungs may not be able to keep up with the increased metabolic demands of the body.
The BPD collaborative suggests 3 that the weight for length should be maintained at the 50th percentile. Hence, it is a common practice among clinicians to restrict the calories when the weight-for-length ratio is high. However, no studies indicate if a higher weight for length is detrimental in preterm infants with respiratory morbidity. Miller et al. found that infants whose growth of the length was deteriorating were more likely to require increased oxygen during a respiratory wean and were at a higher risk of developing pulmonary hypertension 4.
The large multinational Intergrowth 21st study has published normative values for the weight for length in preterm infants. The study also concluded that weight for length is more accurate than the body mass index (BMI) in predicting fat-free mass (FFM) and fat mass (FM) as measured by air displacement plethysmography in premature infants 5. Thus, weight for length in preterm infants can be a helpful non-invasive tool to assess the perturbations in body composition. However, there is no current evidence associating anthropometric measurements in preterm infants with BPD and their respiratory outcomes.
DEXA (dual-energy x-ray absorptiometry) and air displacement plethysmography accurately estimated fat mass and fat-free mass in preterm and term infants. However, these methods are impractical in sick neonates, and air displacement plethysmography cannot be used on infants requiring supplemental oxygen. Several experts recommend assessing the weight status by monitoring the weight for length in children <2 years of age 6,7.
This study investigated the association between weight-for-length (W/L) percentiles and respiratory morbidity in preterm infants. We, therefore, explored our hypothesis that higher percentiles and z scores for weight for length in preterm infants could increase the severity of pulmonary morbidity. We used the Pulmonary Score (PS) to assess the severity of pulmonary morbidity in preterm infants. Our goal was to determine if higher weight-to-length z-scores after 32 weeks of gestation are associated with higher PS before term-corrected gestational age in preterm infants requiring respiratory support in a prospective observational study.
Methods
This project was supported by the Pilot Project Grant Program of the Mississippi Center for Clinical and Translational Research (MCCTR) and the NIH: Award #1U54GM115428. University of Mississippi Medical Center’s Institutional Review Board approved this prospective study in February 2019, and the approval number is IRB File #2018-0204. We enrolled preterm infants born at less than 30 weeks of gestation, with a post-menstrual age (PMA) of 30-33 weeks, and requiring oxygen at enrollment for at least three days at the time of enrollment. We excluded babies with congenital anomalies such as abdominal wall defects, skeletal dysplasia affecting the chest wall or lung, congenital diaphragmatic hernia, babies with myopathies, confirmed surfactant protein-B deficiency, or congenital prostaglandin-dependent heart lesions from the study.
The institutional review board at the University of Mississippi Medical Center approved the study, and informed consent was obtained from each participant. The study was performed per the Declaration of Helsinki.
Data collection
A dedicated research nurse measured the weight (in grams) using the certified electronic weighing scale, length using an infant length board (in centimeters), and head circumference (in centimeters) using paper-based measuring tape once a week on all the recruited infants. Each parameter was measured twice for accuracy, and we calculated a mean for each parameter. The weight for length percentiles and z-scores for the corresponding week were obtained using Intergrowth 21st study data. We collected data on calories/kilogram/day, protein grams/kilogram/day, protein to calorie ratio, weight for length percentiles, z-scores, and BMI from 33 through 40 weeks PMA. The definition of BPD used in the current study was per the NICHD BPD workshop published in February 2018 8.
Pulmonary Score (PS)
The PS is a standardized score that assesses the severity of pulmonary morbidity in premature infants with bronchopulmonary dysplasia (BPD) developed by Ashima Madan et al. for the STOP-ROP study 9. PS scores for the current study were computed weekly from 33 weeks until 40 weeks of PMA or discharge, whichever occurred early, for stratification and subsequent comparison purposes. The formula to calculate the score was: (Fio2)(support) + (medications), where Fio2 is expressed as a fraction (room air: 0.21) for the ventilator, CPAP, or hood and as effective Fio2 for nasal cannula; support is 2.5 for ventilator or tracheostomy, 1.5 for CPAP (nasal or endotracheal), and 1.0 for the nasal cannula, hood oxygen, or no oxygen; and the medications score is 0.20 for systemic steroids for chronic lung disease, 0.10 each for regular diuretics (daily or every other day) or inhaled steroids, and 0.05 each for methylxanthines or intermittent diuretics. PS has a range from 0.21 to a maximum of 2.7.
Statistical analysis
We compared the mean weight for length percentiles and z-scores with PS.
Sample size calculation:
No previous studies compared the PS scores with weight for length percentiles. Therefore, to calculate the sample size, we assumed that the mean PS score would be 0.59±0.22 in the high-weight for length group vs. 0.44± 0.14 in the normal-weight for length group. This assumption was based on the study that used PS to differentiate infants with BPD who passed the room-air challenge versus those who failed to wean to room air from a nasal cannula 10. For the study, we classified the weight for length centiles as high if centiles are 50 or higher and normal if the weight for length centiles is <50. Based on our assumptions of an 80% probability of rejecting the null hypothesis (OR=1) when it is false, a 5% probability of obtaining a false positive with the (two-sided) statistical test, and assuming that mean PS in high weight for the length group is 0.59 +/-0.22 vs. 0.44 +/-0.14 in the normal weight for the length group, we would need a sample size of 46 in each group.
Data were analyzed using both descriptive and inferential statistical techniques. Summary statistics were computed as mean (standard deviation) for continuous variables and frequency (percentage) for categorical variables. A linear mixed model that accounts for the correlation due to the repeated measurements for each baby was employed to assess the association between response and independent variables of interest, adjusting for covariates. Statistical significance is for P-value <0.05 based on two-tailed tests.
Results
We analyzed 91 infants for our study. We excluded one infant after he was too sick to obtain further anthropometric measurements. The mean gestational age was 26.9 ± 1.7 weeks. The mean birth weight was 0.898 ± 0.238 kgs. They were predominantly African American (81.3%) and girls (56%). Postnatal steroids were administered in 26.4% of the infants. The mean duration of invasive ventilation was 19.23 days ± 28.30 days. The mean duration of non-invasive ventilation was 44.03 ± 22.60 days. The mean PS at 36 PMA was 0.36 ± 0.41. Table 1 shows maternal and neonatal characteristics.
Anthropometric measures and Post MenstrualAge
The mean PS was significantly higher in grade 3 BPD (1.04 ± 0.4) compared to grade 1 BPD (0.29 ± 0.05), p = <0.0001 (Figure 1), showing that PS correlated with pulmonary morbidity. One hundred and thirteen infant measurements between 33 to 40 weeks PMA had W/L measurements above the 50th percentile. Of these 113 infants’ measurements, 92 (82.4%) had a normal length for PMA. This suggests that high Weight/Length is due to higher weight for age and not due to growth restriction in length in most cases. Similarly, at 36 PMA, 84.6% of those with W/L percentiles >50 also had normal length for PMA.
Correlation between anthropometric measures and Pulmonary Severity (PS):
Overall, there was a significant positive association between PS and W/L z scores (p<0.0001). For every one-unit increase in W/L z-scores, PS increased by 0.063. This is illustrated in Figure 2.
Similarly, there was a significant positive association between PS and W/L percentiles (p = 0.0017) as well as BMI (p = <0.0001). For every one-unit increase in W/L percentile, PS increased by 0.002, and for a unit increase in BMI, PS increased by 0.04.
Effect of regression analysis:
The association between PS and W/L z-scores, W/L percentiles, and BMI remained significant (p = <0.0001) after postnatal steroids, sex, post-menstrual, and birth gestational ages were included in the regression analysis, which suggests that the association between PS and anthropometric measurements is natural.
Effect of postnatal steroids:
Since postnatal steroids may affect growth in general, we analyzed the results after excluding the infants exposed to postnatal steroids to evaluate if the W/L and PS association is true. The association between PS and W/L z-score remained significant after the infants receiving postnatal steroids were excluded from the regression analysis. After excluding infants exposed to postnatal steroids, for every unit increase in W/L z score, PS increased by 0.03 with a p-value of 0.003.
Effect of nutrition and sex:
There were no sex differences observed in the mean PS. Likewise, no association was noted between the anthropometric measurements and the nutrition provided to the infants in the study. The mean calories provided at 36 weeks PMA was 121.39 ± 18.28 Kcal/kg/d. The mean protein provided at 36 weeks PMA was 3.78 ± 0.59 g/kg/d. The mean calories did not correlate with BMI (P= 0.78). Similarly, mean protein did not correlate with BMI (P = 0.83). Likewise, mean calories or mean protein did not correlate with W/L percentiles (P= 0.07 and 0.48, respectively), indicating that nutrition did not play a role in higher W/L or BMI in the current study.
Discussion
Our prospective observational study investigated the relationship between pulmonary scores (PS) and anthropometric indicators, such as weight-for-length (W/L) z-scores, W/L percentiles, and body mass index (BMI), in preterm infants. We found a significant positive correlation between the PS and these indicators. Specifically, the PS was found to be higher in grade 3 BPD compared to grade 1 BPD. The study’s findings suggest that as the W/L z-scores or percentiles increased, the PS worsened, indicating an increased risk of pulmonary complications in preterm infants with higher W/L ratios. This information can help identify those infants who are at a higher risk of developing pulmonary complications and in developing interventions to reduce the risk of such complications.
It is widely accepted that improved growth in very low birth weight (VLBW) infants with bronchopulmonary dysplasia (BPD) is linked to better lung function.11,12. However, there is little research on how abnormal growth affects lung function in premature babies. This paper is the first prospective study that focused on the association between altered body proportionality and the severity of respiratory status. A recent retrospective study investigated whether changes in BMI from birth to 36 weeks of post-menstrual age were associated with the likelihood of developing BPD in preterm infants 13. These researchers also noted that increases in BMI z score from birth to 36 weeks PMA were associated with higher odds of BPD and an increase in the severity of BPD. In the adjusted analysis, higher ΔBMI z score quartiles were associated with higher odds of BPD (Q3 vs Q2, AOR [95% CI], 2.02 [1.23; 3.31] and Q4 vs Q2, AOR [95% CI], 2.00 [1.20; 3.34]). Our study associated pulmonary severity with increasing BMI, W/L Z-scores, and percentiles from 33 weeks PMA Our study has revealed that preterm infants with a higher body mass index (BMI) or a larger weight-to-length ratio are at a greater risk of developing respiratory health issues, even before they are diagnosed with bronchopulmonary dysplasia (BPD). These respiratory issues can lead to serious complications that can affect the infant’s overall health and development. Therefore, it is important to closely monitor and maintain appropriate anthropometry in preterm infants who are at risk of developing BPD. Proper nutrition, feeding practices, and weight management can help reduce the risk of respiratory illness and improve the long-term health outcomes in preterm infants. The results of our study indicate that all three anthropometric measurements, namely W/L percentiles, W/L z-scores, and BMI, were found to be significantly associated with respiratory morbidity. These findings underline the importance of considering these anthropometric measures while assessing respiratory health. However, it is worth noting that our study was not designed to predict the development of BPD, and further research is needed in this area.
Recent studies have shown that administering postnatal steroids, either single or multiple courses, has no effect on the growth of premature infants with bronchopulmonary dysplasia (BPD)14,15,16. However, to ensure that the use of postnatal steroids did not influence the observed results, we analyzed the data after eliminating the infants exposed to postnatal steroids. In our study, approximately 26% of the infants had received postnatal steroids. We therefore conducted a regression analysis after removing all infants who received postnatal steroids. The results showed that the relationship between PS and weight/length z-score remained significant (with a point estimate of 0.03 and a p-value of 0.003). This confirms that there is a genuine link between PS and anthropometric measurements adding strength to our findings.
Our study found no association between calorie and protein intake and BMI or weight/length (W/L) percentiles in infants with severe lung disease. This means there was no correlation between the infants’ calorie or protein intake and their BMI or W/L percentiles. Our findings do not support the hypothesis that excessive nutrition intake is responsible for higher BMI or W/L percentile in our study infants. Therefore, we conclude that the association between PS and anthropometric measures is natural.
Our research has confirmed the belief among clinicians that infants with pulmonary morbidity may be adversely affected by higher weight-to-length ratios or body mass index. The BPD collaborative suggests3 that maintaining weight for length at the 50th percentile is beneficial, and our study supports the current recommendation. The strengths of our study are that it is prospective, includes preterm infants at increased risk for BPD. We have assessed pulmonary severity in relation to anthropometric data. A dedicated research nurse was responsible for measuring the anthropometric data, ensuring high consistency in the results.
Our study has a few limitations. We did not investigate whether improving the body mass index or weight-to-length ratio would reduce respiratory severity. A higher W/L percentile could be due to having a higher weight or a lower length for age, while other variables remain normal. Though it is possible that higher pulmonary morbidity in our study group could have stunted their length growth, resulting in normal weight for age, lower length for age, and deceptively higher W/L percentiles. However, we noticed that most of those with weight-to-length percentiles greater than 50 at 36 weeks of PMA also had normal length for PMA. Hence, stunting of length is not the cause higher W/L percentiles in the study group. This observation supports our hypothesis that a true association exists between higher weight-to-length percentiles and pulmonary severity.
Recent scientific research has demonstrated that optimizing the nutrition of premature infants between 31 and 34 weeks of corrected gestational age can have a positive impact on their body mass index (BMI) proportionality at the time of their discharge from hospital17. The study found that infants who received treatment according to targeted nutrition guidelines had a statistically significant reduction in disproportionately low BMI (8.6% vs 2.5%; P = .0380), which suggests that providing optimal nutrition during this period is crucial for their healthy development. Our study’s findings add to the increasing body of evidence that emphasizes the need for more research on the impact of body proportionality indices on respiratory morbidity in preterm infants. It is crucial to comprehend the underlying mechanisms and create focused interventions to alleviate the burden of respiratory morbidity in this vulnerable population.
Conclusion
Our study is the first to demonstrate that higher BMI and W/L may adversely affect respiratory severity in preterm infants. Our findings suggest that maintaining the ideal anthropometry in preterm infants with severe respiratory conditions may prevent further respiratory morbidity in this subset of infants. Larger studies are needed to confirm our findings.
Author Contributions
PA conceptualized and designed the study. RK assisted with study design and execution. PA wrote the first draft of the manuscript along with RK. PA, RK, along with KH and Kr Hy collected the data for analysis. WY did the statistical analysis. PA obtained the NIH grant.
Funding
This project was supported by the Pilot Project Grant Program of the Mississippi Center for Clinical and Translational Research (MCCTR) and the NIH: Award #1U54GM115428.
Data Availability Statement
The materials described in the manuscript, including all relevant raw data, will be freely available to any researcher wishing to use them for noncommercial purposes without breaching participant confidentiality. The data is available on the University of Mississippi Medical center IRB approved red cap.
Acknowledgments
We acknowledge the contribution of our research nurses, Trenton Hughes and Heather Williams, in collecting the anthropometric data on the included infants.
Conflicts of Interest
Authors have no potential conflicts of interests.
Category of study
Prospective observational clinical study.
Impact Statement
Our study is the first to demonstrate that higher BMI and W/L z-scores may adversely affect respiratory severity in preterm infants. Hence, attention should be paid to avoiding preterm overweight in infants with respiratory morbidity such as BPD..
Ethics approval and consent to participate
The institutional review board at University of Mississippi medical center approved the study and an informed consent was obtained on each participant. The study was performed in accordance with the Declaration of Helsinki.
References
- Martin, R.J.; Jobe, A.H.; Bancalari, E. What is BPD today and in the next 50 years? Am. J. Physiol. Lung Cell Mol. Physiol. 2021, 321, L974–L977. [Google Scholar] [CrossRef] [PubMed]
- Jensen, E.A.; Edwards, E.M.; Greenberg, L.T.; Soll, R.F.; Ehret, D.E.Y.; Horbar, J.D. Severity of Bronchopulmonary Dysplasia Among Very Preterm Infants in the United States. Pediatrics 2021, 148. [Google Scholar] [CrossRef] [PubMed]
- Abman, S.H.; Collaco, J.M.; Shepherd, E.G.; et al. Interdisciplinary Care of Children with Severe Bronchopulmonary Dysplasia. J. Pediatr. 2017, 181, 12–28. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.N.; Moise, A.A.; Cottrell, L.; Loomis, K.; Polak, M.; Gest, A. Linear growth is associated with successful respiratory support weaning in infants with bronchopulmonary dysplasia. J. Perinatol. 2022, 42, 544–545. [Google Scholar] [CrossRef] [PubMed]
- Villar, J.; Puglia, F.A.; Fenton, T.R.; et al. Body composition at birth and its relationship with neonatal anthropometric ratios: the newborn body composition study of the INTERGROWTH-21(st) project. Pediatr. Res. 2017, 82, 305–316. [Google Scholar] [CrossRef] [PubMed]
- Furlong, K.R.; Anderson, L.N.; Kang, H.; et al. BMI-for-Age and Weight-for-Length in Children 0 to 2 Years. Pediatrics 2016, 138. [Google Scholar] [CrossRef] [PubMed]
- Secker, D. Promoting optimal monitoring of child growth in Canada: using the new WHO growth charts. Can. J. Diet Pract. Res. 2010, 71, e1–e3. [Google Scholar] [CrossRef] [PubMed]
- Higgins, R.D.; Jobe, A.H.; Koso-Thomas, M.; et al. Bronchopulmonary Dysplasia: Executive Summary of a Workshop. J. Pediatr. 2018, 197, 300–308. [Google Scholar] [CrossRef] [PubMed]
- Madan, A.; Brozanski, B.S.; Cole, C.H.; Oden, N.L.; Cohen, G.; Phelps, D.L. A pulmonary score for assessing the severity of neonatal chronic lung disease. Pediatrics 2005, 115, e450–e457. [Google Scholar] [CrossRef] [PubMed]
- Trzaski, J.M.; Hagadorn, J.I.; Hussain, N.; Schwenn, J.; Wittenzellner, C. Predictors of successful discontinuation of supplemental oxygen in very low-birth-weight infants with bronchopulmonary dysplasia approaching neonatal intensive care unit discharge. Am. J. Perinatol. 2012, 29, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Filbrun, A.G.; Popova, A.P.; Linn, M.J.; McIntosh, N.A.; Hershenson, M.B. Longitudinal measures of lung function in infants with bronchopulmonary dysplasia. Pediatr. Pulmonol. 2011, 46, 369–75. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Solis, M.; Perez-Fernandez, V.; Bosch-Gimenez, V.; Quesada, J.J.; Garcia-Marcos, L. Lung function gain in preterm infants with and without bronchopulmonary dysplasia. Pediatr. Pulmonol. 2016, 51, 936–42. [Google Scholar] [CrossRef] [PubMed]
- Li Ching Ng, L.; Patel, S.; Plourde, H.; et al. The association between BMI trajectories and bronchopulmonary dysplasia among very preterm infants. Pediatr. Res. 2022. [Google Scholar] [CrossRef] [PubMed]
- Williams, E.E.; Dassios, T.; Mann, M.; Greenough, A. The effect of postnatal corticosteroids on growth parameters in infants with bronchopulmonary dysplasia. J. Perinat. Med. 2021, 49, 1141–1144. [Google Scholar] [CrossRef] [PubMed]
- LeFlore, J.L.; Engle, W.D. Growth and neurodevelopment in extremely low-birth-weight neonates exposed to postnatal steroid therapy. Am. J. Perinatol. 2011, 28, 635–42. [Google Scholar] [CrossRef] [PubMed]
- Zozaya, C.; Avila-Alvarez, A.; García-Muñoz Rodrigo, F.; et al. The Impact of Postnatal Systemic Steroids on the Growth of Preterm Infants: A Multicenter Cohort Study. Nutrients 2019, 11. [Google Scholar] [CrossRef] [PubMed]
- Philip, S.S.; Davenport, S.E.; Mannan, J.; White, H.O.; Lee, A.F.; Rhein, L.M. Impact of a targeted volume-increase nutrition guideline on growth and body mass index in premature infants: A retrospective review. JPEN J. Parenter. Enteral Nutr. 2022, 46, 561–571. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Correlation between BPD severity and respiratory severity scores.
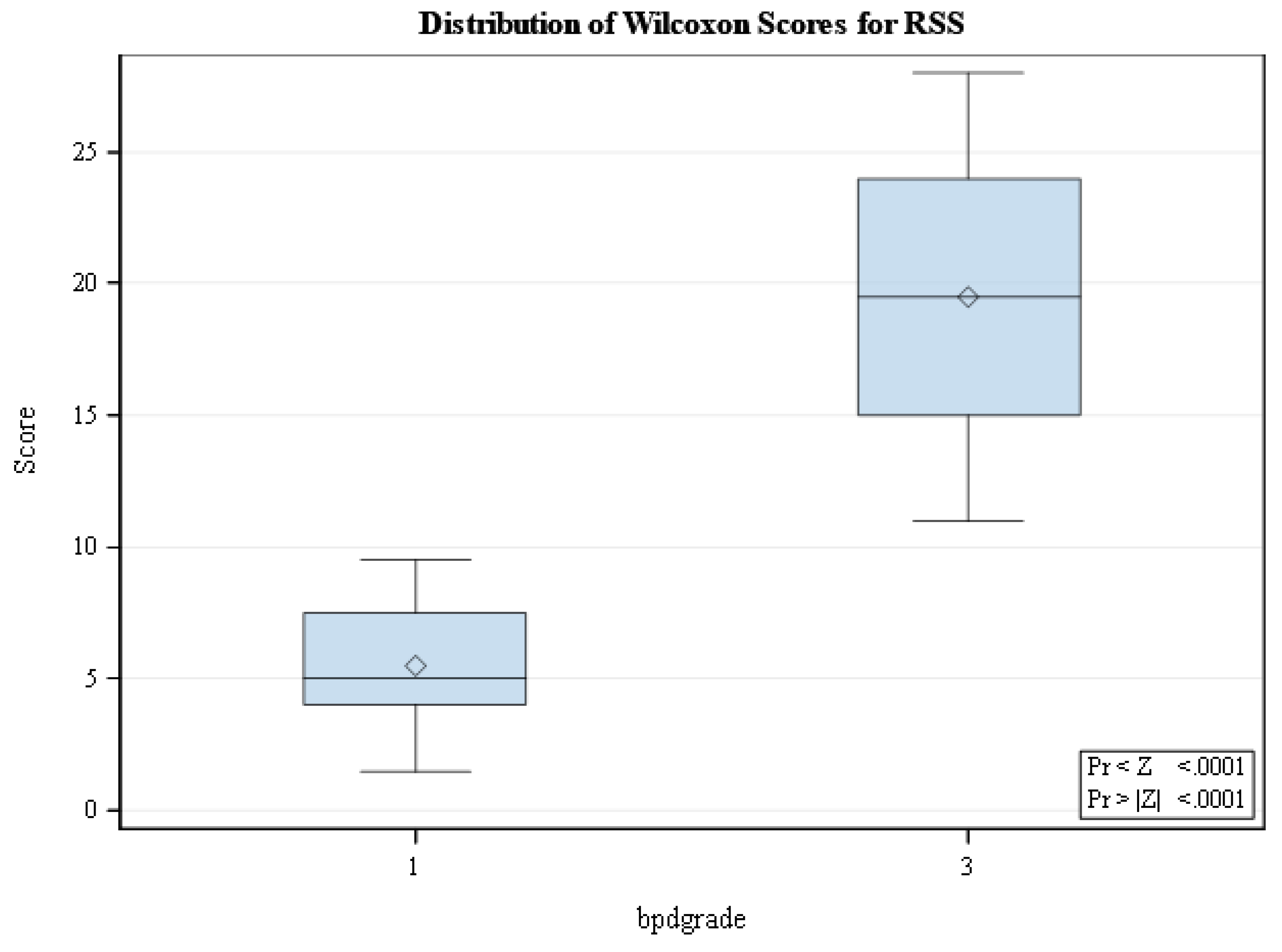
Figure 2.
Association between RSS and W/L z-scores.
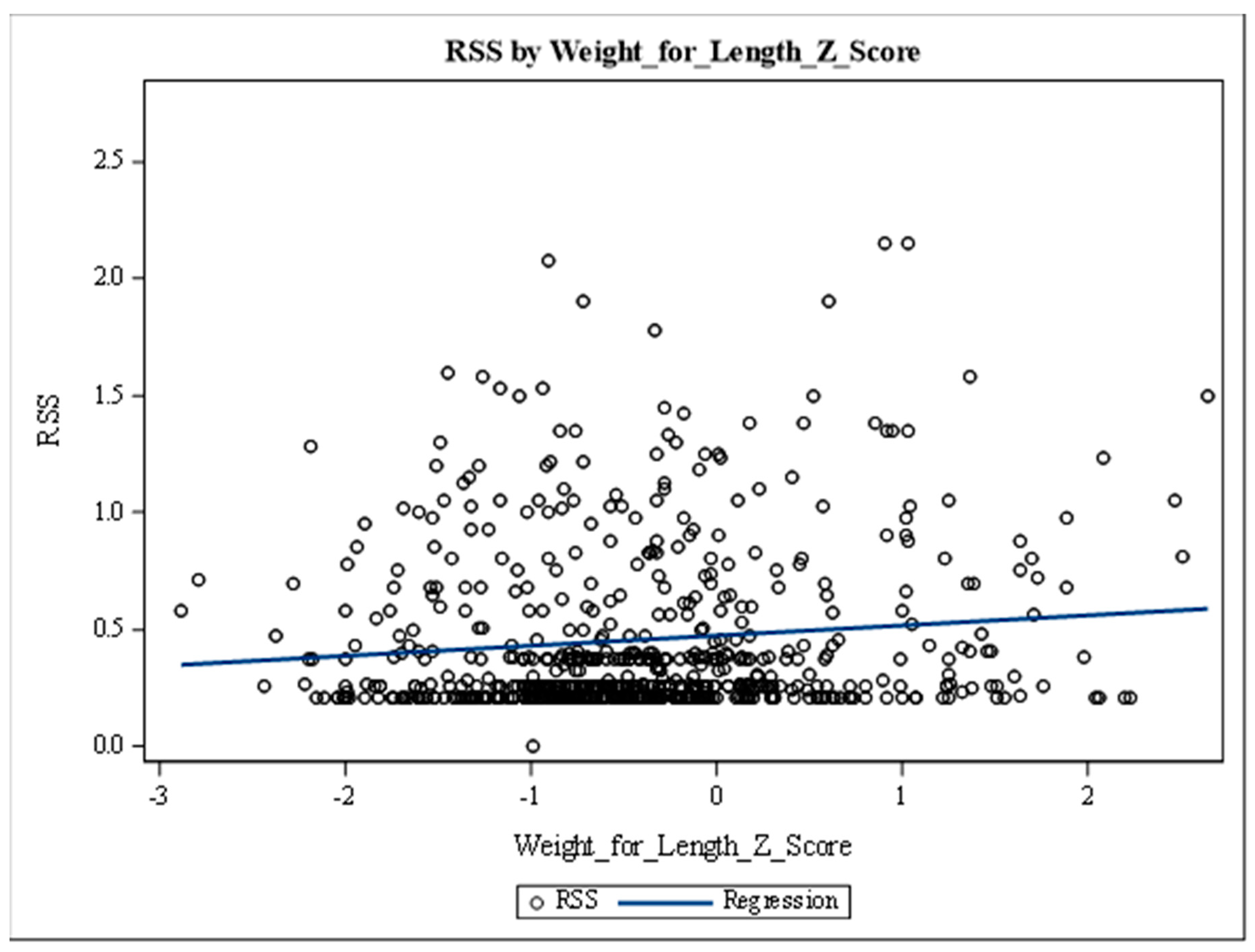

Table 1.
Maternal and newborn characteristics.
| Maternal characteristics | Number (Percentage) |
|---|---|
| Maternal diabetes | 13 (15.5%) |
| Pre eclampsia | 41 (47.7%) |
| Ante natal steroid use | 67 (74.4%) |
| Chorioamnionitis | 11 (12.6%) |
| Newborn characteristics | |
| Male | 40 (44%) |
| Black | 74 (81.3%) |
| Methyl xanthine use | 91 (100%) |
| Postnatal steroid use | 24 (26.4%) |
| Pulmonary HTN | 18 (19.7%) |
| Nitric oxide use | 8 (8.8%) |
| Sildenafil use | 1(1.1%) |
| Diuretic use | 30 (33%) |
| Any IVH | 29 (31.9%) |
| Any ROP | 22 (24.2%) |
| PDA present after 30 weeks | 37 (40.6%) |
| PDA treatment | 19 (20.9%) |
| Any BPD at 36 weeks | 31 (34%) |
| Grade 3 BPD | 18 (19.7%) |
| Ventilated babies at 36 weeks | 14 (15.4%) |
| Ventilated babies at 40 weeks | 5(5.5%) |
| Culture positive infection | 24 (26.4%) |
| NEC | 9 (9.9%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



