Submitted:
14 December 2023
Posted:
14 December 2023
You are already at the latest version
Abstract
Sarcomas are a group of malignancies of mesenchymal origin with plethora of subtypes. Given the sheer heterogeneity of various subtypes and rarity of the disease, management of sarcomas has been challenging with poor patient outcomes. Surgery, radiation therapy and chemotherapy have remained the backbone of treatment in patients with sarcoma. The introduction of immunotherapy has rev-olutionized the treatment of various solid and hematological malignancies. In this review, we discuss basics of immunotherapy and immune microenvironment in sarcomas, various modalities of im-munotherapy such as immune checkpoint blockade, oncolytic viruses, cancer targeted antibodies, vaccine therapy and adoptive cell therapies like CAR T-cell therapy, T cell therapy, TCR therapy.
Keywords:
Immunotherapy
; sarcomas
; adoptive cell therapy
; CAR T-cell therapy
; oncolytic viruses
; TCR therapy
; immune microenvironment.
1. Introduction
Sarcomas are a group of heterogeneous malignancies of mesenchymal origin with more than 100 histologic subtypes. They have diverse molecular, genetic, and clinical features and comprise 1% of adult malignancies [1,2,3]. They can be generally classified into two major types: soft tissue sarcomas (STS), which include more than 50 subtypes (with the most common being liposarcoma, leiomyosarcoma and undifferentiated pleomorphic sarcoma), and bone sarcomas (BS) (osteosarcoma, chondrosarcoma, and Ewing’s sarcoma) [4,5] (Refer to Table 1 and Table 2 for WHO classifications). Some of the sarcoma subtypes are extremely rare with limited current knowledge of their pathophysiology and treatment responses, and they are underrepresented in clinical trials.
Recently, incorporation of immunotherapies to treatment regimens has been heavily investigated and has revolutionized the treatment of solid tumors. Immune check point inhibitors (ICIs) have limited efficacy in sarcomas compared to other solid tumors, however it has shown some activity in certain subtypes. Moreover, clinical trials are heterogenous, as most have been basket trials with a variety of different sarcoma subtypes despite their unique biological characteristics, thus making it difficult to utilize ICIs in rare subtypes. There are several challenges with immunotherapy use in sarcoma due to tumor heterogeneity, the paucity of targetable antigens in sarcoma subtypes by therapeutic antibodies, vaccines, chimeric antigen receptors, and the lack of individualized trials for rare subtypes. However, combination of ICIs with other agents appears to have synergistic effects, and potential treatment options such as adoptive cell therapy and oncolytic viruses are emerging. In this review, we discuss the biological basis, current clinical trials, and future challenges of immunotherapy in advanced sarcomas.
2. Current Sarcoma Treatment Landscape
Treatment of STS can be based on the given subtype, such as STS of extremity, superficial/trunk or head and neck; retroperitoneal or intra-abdominal STS, desmoid tumors and rhabdomyosarcomas [6]. Patients should be evaluated and managed by a multidisciplinary team, including experienced pathologists, radiologists, medical oncologists, surgical oncologists, and radiation oncologists for consideration of systemic therapy, surgery, and/or radiation [6]. Conventional chemotherapy, including anthracycline-based regimens, is the standard treatment for most advanced and metastatic STS and non-anthracycline based regimens are preferred in angiosarcomas (AS) and perivascular epithelioid cell neoplasms [7,8,9]. A number of tyrosine kinase inhibitors (TKIs) have shown promising results in patients with certain histologic subtypes of advanced and metastatic STS. Pazopanib, a multitargeted tyrosine kinase inhibitor (multi-TKI), can be used as a single agent in metastatic nonlipogenic STS patients previously treated with anthracycline-based chemotherapy, or as a front line in advanced/metastatic STS patients who are not candidates for anthracycline-based regimens [10,11]. Other TKIs used in advanced STS include regorafinib (nonadiopocytic sarcoma and AS), sorafenib (desmoid tumors) and imatinib (dermatofibrosarcoma protuberans and gastrointestinal stromal tumors (GIST)) [12,13,14,15].
Treatment of BS can be vastly different depending on subtypes. Osteosarcomas (OS) are usually radiation resistant, and treatment involves wide excision with perioperative chemotherapy including doxorubicin, cisplatin, and high dose methotrexate [16]. On the other hand, Ewing’s sarcomas (ES) are sensitive to radiation, and treatment usually involves perioperative chemotherapy with vincristine, doxorubicin, cyclophosphamide, ifosfamide and etoposide with surgery with or without radiation [17]. Chondrosarcomas (CS) are chemotherapy and radiation resistant, and primary treatment is surgical resection [18]. Recently, TKIs like regorafenib, cabozantinib and apatinib have also been shown to be effective in OS [19]. The investigation of TKIs for other BS has not been well developed but it has shown some promising results in preclinical and early trials in ES and chondrosarcomas [19]. Currently, atezolizumab is the only immunotherapy drug approved by the Food and Drug Administration (FDA) for sarcomas and it is approved for unresectable or metastatic alveolar soft part sarcoma (ASPS) on December 9th, 2022 [20]. Pembrolizumab can be considered as a second line treatment for patients with certain subtypes of advanced or metastatic STS, including myxofibrosarcoma (MFS), undifferentiated pleomorphic sarcoma (UPS), cutaneous AS and undifferentiated sarcomas [6].
3. Cancer immunotherapy
Clinical benefits of immune enhancement in cancers have been well proven since the 1800s. Immunotherapy is the fifth pillar of cancer treatment after surgery, chemotherapy, radiation therapy and targeted therapy. In some cases, it has become the first line of treatment [21]. Cancer immunotherapies can be categorized based on the mechanism of action: (i) checkpoint blockade which removes the natural inhibitory signals of the immune system; CTLA-4 inhibitor (e.g., ipilimumab), PD-1 inhibitor (e.g., pembrolizumab, nivolumab), PD-L1 inhibitor (e.g., atezolizumab, avelumab, durvalumab) (ii) adoptive cell therapies including infusion of modified immune effector cells (T cells, Chimeric Antigen Receptor T cells (CAR T-cells), NK cells or TCR based therapy; (iii) cancer vaccines; (iv) oncolytic viruses; and (v) cancer targeted antibodies. The success of immunotherapy is significantly affected by the immunogenicity of tumor, tumor mutation burden and tumor microenvironment.
4. Immune Microenvironment and Biomarkers in Sarcoma
The tumor microenvironment (TME) is a primary location for cell-to-cell interactions around the tumor, signal transfer or delivery, and cytokine production. It plays an important role in tumor cells escaping the natural immune system and can similarly affect the efficacy of some immunotherapies. The components of the TME are tumor-associated macrophages (TAMs), pro-inflammatory cytokines, other immune checkpoint modulators, regulatory T-cells (Treg), immunosuppressive cytokines; for example, transforming growth factor-beta (TGF-beta), pro-angiogenic cytokine like fibroblast growth factor (FBGF), or vascular endothelial growth factor (VEGF). They are functioning through a complex pathway to maintain the tumor growth and to overcome the anti-cancer immune system.
Being a heterogeneous disease with multiple subtypes, sarcoma has a variety of genetic profiles and characteristics of tumor cells in each individual subtype [22]. The tumor mutational burden (TMB) and microsatellite instability (MSI) status have commonly been used to predict tumor response to immunotherapy. There is high variability of TMB among different subtypes of sarcoma. For example, a few sarcoma subtypes such as soft tissue rhabdomyosarcoma, alveolar, liposarcoma and synovial sarcoma have low TMB, whereas soft tissue angiosarcoma has high TMB with a median mutational burden of 3.8 mutations/Mb and 13.4% of cases having more than 20 mutations/Mb [22].
Another potential predictive factor used to evaluate utility of immunotherapy in sarcoma treatment are tertiary lymphoid structures (TLS), which refer to the organized aggregates of lymphoid cells forming around the tumor cells. Usually observed via use of immunohistochemistry (IHC), the aggregation of-B cell follicles, dendritic cells, helper T cells (CD4+) and cytotoxic T cells (CD8+) represents the TLS phenotype, which is frequently found in high immune sarcoma types and can predict better outcomes with immune checkpoint inhibitors (ICI) [23,24]. This hypothesis is supported in the PEMBROSARC trial, a multicohort phase II trial, which showed that the presence of TLS features in the TME was associated with a higher pembrolizumab treatment response [25]. Interestingly, a high infiltration of regulatory T (Treg) cells, which modulate the immune function, was found in TLS positive non-responder groups, and decreased the effect of pembrolizumab [25]. As such, the clinical impact of TLS is still controversial with limited known predictive value currently.
By analyzing bulk RNA transcriptome data from tumor infiltrating lymphocytes (TILs) in 85 osteosarcoma patients, researchers identified five different TIL marker genes. These genes were used to create a risk model with both prognostic and predictive value. In this model, varying levels of expression of these five genes were used to classify patients based on higher survival (“low risk”) or lower survival (“high risk”). Additionally, it was found that high risk tumors had a lower abundance of immune cell infiltration, whereas low risk tumors had a higher expression of immune checkpoint genes such as CTLA4 and LAG3, which could provide a positive predictive value in the response to immunotherapy for low risk patients [26]. The combination of IHC for TLS phenotype and the TIL molecular RNA signature could potentially be used together to provide enhanced prognostic and predictive models.
PD-L1 expression varies in different types of tumors. High PD-L1 expression is found in high grade dedifferentiated leiomyosarcoma [27]. However, there is no sufficient data to support PD-1 or PD-L1 as a predictive biomarker for ICI treatment. The efficacy of pembrolizumab was not related to the level of PD-L1 expression in the SARC028 trial [28]. In endometrial sarcoma, PD-L2 expression was associated with mismatch repair (MMR) proficient tumors and lower OS rates when compared to PD-L1 expression [29]. Similar findings were reported in uterine adenosarcoma, which also showed that PD-L1 expression did not correlate with density of TILs, but PD-L2 expression is positively correlated with TP53 mutation, which is associated with worse clinical outcomes [30].
5. Immune Checkpoint Blockade
ICIs target tumor cells’ known inhibitory signals to T cells and have demonstrated response in solid tumors. Immune checkpoint receptors including CTLA-4, PD-1, PD-L1, LAG-3 are inhibitory molecules present on the surface of immune cells, cancer cells and other supporting cells in the tumor microenvironment (TME) [31]. Sarcomas usually have low tumor mutational burden (TMB) and immunosuppressive TME, low PD-L1 expression, and only a few percent of these tumors are mismatch repair deficient; they are not considered immune sensitive tumors [1]. Even though response to ICIs in sarcomas is not high in general, there is some benefit in specific histological subtypes [1]. In addition, the role of PD-L1 expression in STS is unclear, as responses are seen even in the absence of PD-L1 expression [32].
Earlier trials with single-agent immunotherapy (anti PD-1 nivolumab, anti-CTLA-4 ipilimumab) failed to demonstrate significant anti-tumor activity [33,34]. One of the first ICI trials with positive results was the prospective single arm phase II trial SARC028, evaluating the anti-PD1 antibody pembrolizumab as a second line in 80 patients with either STS or BS [32]. This study demonstrated an objective response rate (ORR) of 18% in patients with STS with median progression free survival (PFS) and overall survival (OS) of 18 and 49 weeks, respectively [32]. One patient with UPS had a complete response (CR), but the benefit was limited to the patients with UPS and dedifferentiated liposarcoma (DDLPS), with minimal benefit in synovial sarcoma (SS), leiomyosarcoma (LMS) or BS [32]. However, this trial excluded rare STS subtypes, thus the efficacy of anti-PD1 in rare STS subtypes was not evaluated. The response of UPS to pembrolizumab was further confirmed in an expansion cohort of SARC028 with two CR and seven partial responses (PR) in the UPS cohort, but the response was not confirmed in the liposarcoma (LPS) cohort [35].
A phase II French AcSé trial evaluating the efficacy of pembrolizumab in different cohorts of patients with rare cancers, including the rarest sarcoma subtypes, showed an ORR of 15.3% with disease control rate (DCR) of 52.5% [36]. It demonstrated the highest response rates in ASPS with 50% ORR and in SMARCA4-deficient malignant rhabdoid tumor (SMRT) with 27% ORR. Other response rates were 8.8% in chordoma, 12.5% in desmoplastic small round cell tumors (DSCRT) and 3.2% in other histotypes [36].
A pooled analysis of clinical trials investigating anti PD-1/PD-L1 immunotherapy in patients with advanced STS including UPS, LPS, LMS, ASPS, reported that among 384 patients, 39.8% received anti-PD1/PD-L1 immunotherapy and had ORR of 15.1% and median PFS of 58.5% [26]. ASPS and UPS were among the highest responders (48.4% and 15.7%, respectively) and LPS and LMS among the lowest (7.3% and 6.9%, respectively) [37]. In the first line setting, a retrospective study of nivolumab with or without ipilimumab was evaluated in PD-L1 positive STS, demonstrating an ORR of 13% in the combination group vs 7% in the nivolumab group [38].
Targeting different immune checkpoints including PD-1, CTLA-4 and LAG-3 simultaneously is a promising approach to improve the effectiveness of immunotherapy. Lussier et al. showed that CTLA-4 expression was upregulated in T cells infiltrating PD-L1 antibody-resistant tumors in mice with metastatic OS, suggesting a potential synergic effect of anti CTLA-4 and PD-L1 blockade [39]. Combination checkpoint inhibition with nivolumab and ipilimumab was evaluated in previously treated patients with advanced STS in the phase II Alliance A091401trial with an ORR of 16%, and a median PFS and OS of 4.1 and 14.3 months, respectively, and better responses are seen with combination therapy and the best responses in UPS (33%), LMS (14.2), and AS (33%) [40].
Dual blockade of PD-1 and LAG-3 has also shown synergistic antitumor activity in preclinical models. A phase II basket trial of anti-PD1 spartalizumab plus anti-LAG3 LAG525 with a cohort of 10 sarcoma patients reported 40% DCR at 24 weeks [41]. Expansion criterion was not met, but the sarcoma cohort was not found to be futile [41]. Currently, the combination of nivolumab plus anti-LAG3 relatimab vs nivolumab alone is being investigated in advanced STS in ongoing phase II trial NCT04095208 (CONGRATS trial).
Tumor biomarker analysis of ASPS affirms the presence of PD-1/PD-L1 immune check point components, suggesting that immune check point inhibition could be beneficial in advanced ASPS [42]. A phase II trial of 43 evaluable patients with ASPS using anti-PD-L1 atezolizumab showed an ORR of 37.2% with median duration of response (DOR) of 16.5 months [42]. Recently updated results with 52 patients confirmed the ORR of 37% with DOR of 24.7 months, and PFS of 20.8 months [43]. The FDA approved atezolizumab for unresectable or metastatic ASPS on December 9th, 2022 [20].
Given the lack of randomized phase III trials and limited therapeutic alternatives for patients who progressed on chemotherapy, ICI could be considered especially in patients with UPS, DDLPS as well as ASPS. Dual immune blockades appear to show higher response rates and may be considered in selected patients. Further details and summary of ICI trials are listed in Table 3.
6. Combination of ICI with Tyrosine Kinase Inhibitors
The quest to find the optimal response of ICI in sarcomas has led to the combination of ICI with targeted therapies, mainly anti-angiogenic and multi TKIs. Preclinically, the normalization of abnormal tumor vessels and increased infiltration of immune effector cells into tumors by anti-angiogenic TKIs has shown to enhance the efficacy of ICI [44]. In addition to blocking the immune-suppressive effect of vascular epidermal growth factors (VEGF), multi TKIs seem to make favorable immune modulating effect by decreasing the arrival of myeloid derived suppressor cells and tumor associated macrophages, as well as increasing the infiltration of dendritic cells, natural killer cells and CD8+ lymphocytes, potentially making multi-TKIs a reasonable combination with ICIs [45].
The combination of nivolumab and sunitinib in advanced BS was evaluated in the phase I/II trial IMMUNOSARC, with ORR of 5% with 1 CR in dedifferentiated chondrosarcoma (DDCS), 1 PR and 22 SD and PFS of 3.7 months [46]. In this same trial, an advanced STS cohort was also evaluated and found to have an ORR of 21% with 1 CR in AS, 5 PR, and 33 SD among 46 patients and a median PFS of 5.6 months [47]. On the other hand, pembrolizumab in combination with axitinib demonstrated promising responses in a phase II trial of 33 advanced sarcoma patients among which 51% were previously treated [48]. It showed an ORR of 25% (8 PR) and PFS of 4.7 months, with the most benefit seen in ASPS who had 50% ORR with PFS of 12.4 months [48]. The benefit was thought to be due to high tumor infiltrating lymphocytes and PD-L1 expression in ASPS tumors [48]. Another anti-PD1 camrelizumab was evaluated with apatinib in the phase II APFAO trial of 43 patients with chemotherapy-refractory OS and showed an ORR of 20.9% and PFS of 6.2 months with the most PFS observed in patients with lung metastasis and with PD-L1 tumor proportion score of 5% [49].
The combination of durvalumab with pazopanib in previously treated patients with advanced STS showed an ORR of 28.3% and median PFS of 7.7 months with objective responses in ASPS, AS, UPS, and dedifferentiated chondrosarcoma (DSRCT) [50,51]. Upon further analysis, tumors with high CD20+B cell infiltration and vessel density were reported to have a longer PFS and a better response than those with low B cell infiltration and vessel density [51].
Combinations of ICI and TKIs could be considered in patients with advanced STS after progression on standard chemotherapy. On the other hand, the effectiveness of this combination in BS is not very promising. Further investigations are needed to compare the clinical benefits of these combinations with single ICI or TKI monotherapy, including the utility in BS. Also, they can be potentially considered to be used as a front-line treatment in selected patients unfit for anthracycline based chemotherapy. Further details and summary of trials for combination of ICI and TKIs is listed in Table 3.
7. Combination of ICI with Conventional Chemotherapy
The rationale for combination of chemotherapy with ICI is that the induction of cell death by chemotherapy could synergize with immunotherapy and make ICI more effective [52]. Cytotoxic drugs can result in DNA damage leading to cell death, release of immunostimulatory signals known as damage-associated molecular patterns (DAMPs) and proteins that work as “danger signals”, with eventual upregulation of PD1 and enhancement of effector lymphocytes’ activity [19].
In the phase II PEMBROSARC trial of pembrolizumab with metronomic cyclophosphamide in 50 patients with locally advanced or metastatic sarcomas (both treatment naive and pretreated patients), including LMS, UPS and GIST showed limited activity, with just one PR in a patient with solitary fibrous tumor (SFT) with PD-L1 expression greater than 10% in immune cells [53]. This trial demonstrated that the clinical benefit of ICI with chemotherapy is very limited in an unselected population. An amended study of PEMBROSARC, which included 35 patients with TLS-positive advanced STS showed a 6-month non-progression rate and ORR of 40% and 30%, respectively, compared with 4.9% and 2.4% respectively in the previous cohort of PEMBROSARC study [25]. Thus, TLS presence in the advanced STS could be a potential predictive biomarker to improve the selection of patients for the treatment of ICI with chemotherapy.
The first combination phase I/II trial of pembrolizumab with doxorubicin in 37 anthracycline-naive patients with advanced STS demonstrated an ORR of 19% (7 PR), PFS of 8.1 months and OS of 27.6 months, with more prominent results in UPS and DDLPS subtypes [54]. Even though it failed to meet its primary endpoint with response rate of 29%, combination therapy was associated with longer PFS than doxorubicin alone (8.1 months vs. 4.1 months) [54]. Another trial of pembrolizumab and doxorubicin in advanced STS showed that patients with PD-L1 ≥ 5% had a 3 times greater ORR (63.6%) than those with PD-L1 <5% [55]. PD-L1 expression was not found to be associated with improved PFS or OS but was associated with improved ORR [55].
LMS and LPS are usually resistant to PD-1/PD-L1 inhibition, likely due to the infiltration of high levels of immunosuppressive tumor-associated macrophages (TAMs) [56]. Trabectedin could influence TME and reduce TAMs, thus improving antitumor adaptive immunity to anti-PD1 therapy [57]. Trabectedin in combination with anti-PD-L1 avelumab in a phase I/II study of patients with advanced LPS and LMS showed 2 PR and 11 SD, with 6 month PFS of 50.1% [56]. In the phase II NiTraSarc trial, nivolumab with trabectedin are evaluated as a second line treatment in anthracycline pretreated advanced STS patients (Group A with advanced LPS or LMS and Group B with other sarcomas including pleomorphic, spindle cell, fibromyxoid, synovial and epithelial sarcoma) [57]. In the late combination cohort (LCC), patients are treated with 3 cycles of trabectedin followed by trabectedin plus nivolumab whereas early combination cohort (ECC) started combination treatment at cycle 2 [57]. After a median follow up of 16.6 months, PFS in group A was 47.6% (60% in LCC vs 36.4% in ECC), and 14.6% in group B. Median PFS was higher in group A compared to group B (5.5 vs 2.3 months) and longer in LCC vs ECC (9.8 vs 4.4 months) [57]. OS was much higher in group A vs group B (18.7 vs 5.6 months), and longer in LCC vs ECC (24.6 vs 13.9 months) [57]. It confirmed the activity of trabectedin followed by combination with nivolumab in LPS and LMS [57].
Results of a phase II trial of doxorubicin with anti-CTLA-4 zalifrelimab and anti-PD1 balstilimab as first and second line treatment in 28 patients without prior doxorubicin or ICI were recently reported [58]. The study had a two-stage design, with stage 1 giving a priming dose of zalifrelimab and balstilimab in cycle 1 prior to adding doxorubicin at cycle 2, and stage 2 giving all drugs at cycle 1. ORR was 36% and DCR was 86%, with DOR of 12.8 weeks in overall population [58]. Patients who received ICI priming at cycle 1 prior to chemotherapy had a better 6-month PFS (56.3 vs 25%), ORR (56% vs 8.3%) and DCR (94% vs 75%) compared to stage 2 [58].
The combination of ICI and chemotherapy seems to respond better in specific histologic subtypes such as LPS, LMS and UPS. However, it is difficult to obtain meaningful results given the heterogeneity in the selections of patients and difficulty confirming therapeutic benefit of immunotherapy to chemotherapy without randomized trials. Moreover, further investigations are needed to evaluate the sequence of priming with either ICI or chemotherapy to find the most effective treatments. Phase III trials comparing these regimens to the standard treatment would be needed to confirm these findings and the utilization of ICI and chemotherapy as a front-line systemic treatment in advanced sarcomas, especially STS. Moreover, this combination is not very well investigated in BS. Further details and summary of trials for combination of ICI and chemotherapy is listed in Table 3.
8. Combination of Immunotherapy with Local Radioation Therapy
Radiation may produce neoantigens that enhance the immunogenicity of tumors with low TMB, making them sensitive to ICI in a T-cell dependent manner [1]. A randomized phase II non-comparative trial evaluating neoadjuvant radiation with nivolumab alone or nivolumab with ipilimumab in 24 surgically resectable patients with DDLPS or UPS, showed significant clinical activity in UPS with a median pathological response of 95%, while it was 22.5% in the DDLPS cohort; with responses being similar irrespective of the addition of ipilimumab [59]. It was found that radiation therapy in UPS increased tumor infiltrating immune cells and tumor PD-L1 expression [59,60]. Combination of ICI with radiation therapy is currently being investigated in several trials (see Table 4).

Table 4.
Currently Ongoing Selected Clinical Trials for Immunotherapy in Sarcomas.
| Phase | NCT number/trial name | Status | Conditions | Interventions |
|---|---|---|---|---|
| ICI | ||||
| Phase I/II | NCT03138161 SAINT |
Recruiting | Unresectable or metastatic STS as first line treatment | trabectedin + ipilimumab + nivolumab |
| Phase II | NCT04095208 | Recruiting | Advanced or Metastatic STS (TLS +) | nivolumab + relatimab vs nivolumab |
| Phase II | NCT04802876 ACROPOLI (SOLTI-1904) |
Recruiting | Across multiple cancer types with PD1-high mRNA Expressing Tumors - Include Sarcoma Cohort | spartalizumab + tislelizumab |
|
ICI with TKIs |
||||
| Phase II | NCT04784247 | Recruiting | Advanced STS | lenvatinib + pembrolizumab |
| Phase II | NCT05182164 | Recruiting | Advance sarcomas: ES, OS, UPS | pembrolizumab + carbozantinib |
| Phase II | NCT04551430 | Active, not recruiting | Metastatic STS | cabozantinib + nivolumab + ipilimumab |
|
ICI with Chemotherapy | ||||
| Phase II | NCT03899805 | Active, not recruiting | STS (LPS, LMS, UPS) |
eribulin + pembrolizumab |
| Phase II | NCT04535713 GALLANT |
Recruiting | Advanced sarcoma | metronomic gemcitabine + doxorubicin + docetaxel + nivolumab |
| Phase I/II | NCT05876715 LINNOVATE |
Recruiting | Advanced STS | lurbinectedin + nivolumab + ipilimumab |
| Phase I/II | NCT04577014 | Recruiting | Advanced STS |
retifanlimab + gemcitabine + docetaxel |
| Phase II | NCT04028063 | Recruiting | Advanced STS | doxorubicin + zalifrelimab -AGEN1884 + balstilimab – AGEN2034 |
|
ICI with Radiation Therapy | ||||
| Phase I | NCT05488366 | Recruiting | Metastatic STS | pembrolizumab + Radiation Therapy |
| Phase II | NCT03307616 | Active, no recruiting | Recurrent or resectable DDLPS and UPS before surgery | nivolumab +/- ipilimumab + Radiation Therapy |
| Phase I/II | NCT03116529 | Active, not recruiting | High risk STS | durvalumab + tremelimumab + Radiation + Surgery |
Retrieved from www.clinicaltrials.gov on October 6, 2023.
Table 4.
Ongoing clinical trials for CAR T-cell therapy in Sarcoma:.
| Trial Number | Phase | Intervention | Disease |
|---|---|---|---|
| NCT01953900 | Phase I | Anti-GD2 T-cells in combination with a varicella zoster vaccine and lymphodepleting chemotherapy | GD2 positive sarcoma and neuroblastoma in relapsed or refractory setting |
| NCT04995003 | Phase I | Anti-HER2 CAR T-cells in combination with an immune checkpoint inhibitor drug (pembrolizumab or nivolumab) | HER 2 positive Sarcoma in patients disease progression or recurrence after at least one prior systemic therapy |
| NCT02107963 | Phase I | Administering escalating doses of autologous anti-GD2-CAR T-cells | Osteosarcoma, GD2+ solid tumors that recurred or progressed on treatment |
| NCT00902044 | Phase I | Anti-HER2 CAR T-cells with fludarabine and cyclophosphamide | Refractory HER2-positive sarcoma or metastatic HER2-positive sarcoma with disease progression after receiving at least one prior systemic therapy |
| NCT03721068 | Phase I | Anti GD2 CAR T-cells, fludarabine and cyclophosphamide | Relapsed refractory osteosarcoma and neuroblastoma |
Table 4.
Ongoing Trial for Cancer Vaccine Therapy in Sarcoma.
| NCT | Phase | Intervention | Disease |
|---|---|---|---|
| NCT01241162 | Phase I | Mature DC pulsed with peptides derived from NY-ESO-1, MAGE-A1, and MAGE-A3 for vaccine production. | Relapsed refractory Ewings sarcoma, osteogenic sarcoma, rhabdomyosarcoma or synovial sarcoma |
It is difficult to determine the most immune sensitive sarcoma subtypes given the heterogeneity of sarcomas, the limited numbers of patients enrolled, the inconsistencies in the designs and results of various trials, lack of phase III randomized clinical trials, lack of representatives of rare histology subtypes, and the lack of validated biomarkers for ICIs. Currently there is a need for trials with better designs and individualized studies investigating each group of sarcomas that share common biological characteristics.
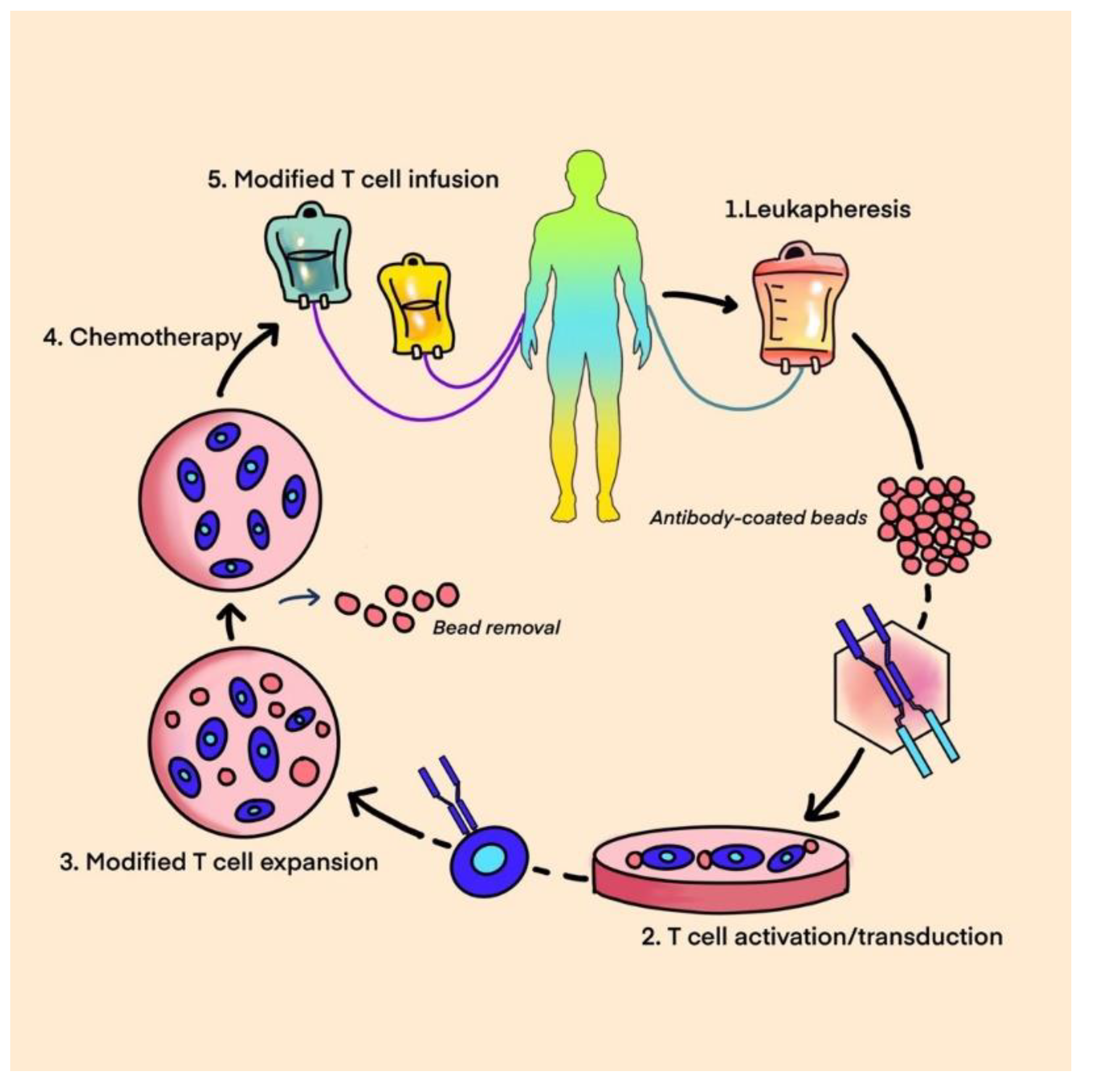
9. Adoptive Cell Therapy
Adoptive cell therapy (ACT) is a new and innovative strategy that uses the immune system to target cancer cells. It has the potential to induce a durable response in tumors, and promising results have been seen in hematological malignancies and some solid tumors. ACT involves extraction of immune cells from a patient’s blood, tumor tissue or healthy donor via leukapheresis. The cells are then genetically engineered ex-vivo to make them targeted towards specific tumor cells, and then expanded prior to reinfusion in the patient. T-cells have the ability to both kill tumor cells directly and activate additional immune cells, subsequently eliciting an endogenous immune response. Three classic examples of ACTs used for cancer immunotherapy are:
- A.
- T-cell therapy
- B.
- Chimeric antigen receptor T-cell therapy (CAR-T)
- C.
- T-cell receptor-based therapy (TCR)
A. T-Cell Therapy
T-cell based therapy is comprised of tumor infiltrating lymphocytes (TILs), which are extracted from the tumor, activated ex-vivo, expanded and reinfused in the patient in combination with immune enhancing adjuvants, such as interleukin-2 (IL-2), to induce a durable immunological response against the tumor cells. Prior to reinfusion of these TILs, the patient receives a lymphodepleting chemotherapy regimen, such as cyclophosphamide and fludarabine, to deplete the innate T-cells that may suppress the proliferation of the infused T-cells in the body [79]. In contrast to engineered TCRs and CAR-T cells, this is the only ACT technique with multiple T-cell receptor clones able to target the antigenic heterogeneity of sarcoma[80]. The role of TILs in cancer immunotherapy has been studied in various cancers, such as renal cell carcinoma, breast cancer, colon cancer, melanoma amongst various others [81]. Earliest studies dating back to three decades ago by Balch et al. reported TILs were present in about 35% of patients with sarcoma particularly gastrointestinal stromal tumor (GIST), STS, Ewing’s sarcoma (ES), osteosarcoma and uterine sarcomas however their potential consideration as predictive markers is unclear based on the current data [81]. This approach of infusing ex-vivo expanded TILs was found to have striking efficacy in melanoma, with durable response rates and long-term survival benefits [82].
Mullinax at al. conducted a study on 70 patients with soft tissue sarcoma (STS) and demonstrated the feasibility of creating TIL cultures using a rapid expansion protocol. The study showed that TILs demonstrated tumor-specific reactivity by IFNγ release assay in 51 samples. The tumor-specific activity was noted in 56.3% of patients (9/16) using the fragment method (tumor fragments were minced into pieces ~1 mm3 in size) and in 40% (14/35) using the digest method (tumor tissue was processed into a single cell suspension using both mechanical and enzymatic disruption) (P = 0.37 comparing fragment vs. digest methods)[83]. In a retrospective study conducted by Zhou et al., 60 patients with chemotherapy-resistant metastatic osteosarcoma were enrolled, and a combined approach with adoptive TIL and anti-PD1 therapy was investigated. The results were encouraging with an ORR of 36.7%, a DCR of 80%, and a median PFS of 5.8 months. Overall, OS was 23.7 months in responders versus 8.7 months in non-responders (p < 0.0001) [84].
However, despite interesting and promising preclinical and retrospective data, further research is required to understand and navigate the challenges still faced by the TIL therapy, especially in sarcomas, given the substantial heterogeneity between different subtypes.
A. CAR T-cell Therapy
CAR (chimeric antigen receptor) T-cell therapy is a type of adoptive cell therapy that aims to modify the DNA of a patient’s T-lymphocytes in order to enable them to selectively target and eliminate cancer cells. The identification of tumor specific antigens for CAR T-cell targeting is challenging in solid tumors, given intense antigenic heterogeneity due to their polyclonal expansion and accumulative mutations, which makes it hard to find homogeneously expressed targets, particularly without unacceptable toxicity.
Figure 1.
CAR T-cell- Leukapheresis, T cell modification, expansion, and CAR T-cell infusion.
Chimeric antigen receptor structure consists of: (Figure 2)
- An antigen-recognition domain- a single-chain variable fragment (scFv) as a part of a genetically engineered monoclonal antibody that targets the selected tumor antigen.
- A hinge that links a recognition site to the transmembrane domain bridging the membrane.
- An intracellular domain that is critical for T-cell receptor signaling [85].
The positive results obtained in clinical trials using CAR T-cell therapy for treatment of B-cell lymphomas and acute lymphoblastic leukemias led to the extension of study of CAR T-cells in treatment of various types of sarcomas. GD2 (diasialoganglioside) has been considered an attractive target for cancer immunotherapy given it is over-expressed on various tumors, including neuroblastoma, melanoma, osteosarcoma, ES, and rhabdomyosarcoma, while it is poorly expressed in normal tissue. T-cells expressing the first generation anti-GD2 chimeric antigen receptors (CARs) were safe and mediated modest antitumor activity in some patients with refractory neuroblastoma[86]. Clinical trials testing the use of anti-GD2 CAR T-cells in patients with sarcomas and other GD-2 positive solid tumors are currently ongoing (See Table 1).
Another important phase I/II trial tested escalating doses of T-cells expressing a HER2-specific chimeric antigen receptor in patients with recurrent/refractory HER2 positive sarcoma[87]. This study demonstrated that the CAR T-cells could persist for 6 weeks without major toxicities, setting the stage for ongoing studies that combine anti-HER2 CAR T-cells with other immunomodulatory approaches to enhance their expansion and persistence [88]. Another important Phase I clinical trial in sarcoma is aimed at testing the combination of anti-HER2 CAR T-cell therapy in combination with immune checkpoint blocking agents such as pembrolizumab or nivolumab (NCT04995003). These patients are typically pretreated with lymphodepleting agents such as cyclophosphamide and fludarabine prior to infusion of CAR T-cells targeting the HER2 receptor. One week after the patient receives the HER2 CAR T-cells, they will begin pembrolizumab every three weeks or nivolumab every two weeks. This study is currently active and recruiting.
A. TCR therapy
T-cell receptor-based therapy utilizes engineered T lymphocytes specifically targeted towards surface tumor antigens. T-cell receptor (TCR)-engineered effector cells use a naturally occurring (or minimally modified) TCR, in contrast to CAR T-cell technology which uses an artificial receptor introduced into the immune effector cells to recognize tumor cell surface proteins[89]. In this strategy, the patient’s autologous T-cells are extracted through leukapheresis or from tumor tissue, modified ex-vivo through a lentivirus or retrovirus vector encoding a specific TCR gene, and expanded prior to reinfusion of cells into the patient. TCR recognizes fragments of tumor specific antigens which are presented by MHC molecules on tumor cell surface. The binding of TCR to the MHC-antigen complex, in combination with other co-stimulator signals, leads to the activation of T lymphocytes. T-cells can kill tumor directly and attract additional immune cells, thereby eliciting an endogenous immune response. It is prudent to identify tumor specific antigens that are overexpressed in the solid tumors with absent or limited expression in normal tissues. Expression of cancer testis antigens (CTAs), including melanoma antigen gene (MAGE), New York esophageal squamous cell carcinoma gene-1 (NY-ESO-1) and synovial sarcoma X (SSX), is restricted to the germline in normal tissue, but these molecules are broadly upregulated in various tumors. Expression of either NY-ESO-1 and/or MAGE-A4 has been observed in greater than 50% of primary synovial sarcoma specimens. It has also been observed in myxoid liposarcoma, osteosarcomas, pleomorphic liposarcoma and chondrosarcomas, making them appealing targets for TCR based therapies [90,91,92].
In an interesting phase I/II study by Ramachandran et al. patients with advanced synovial sarcoma were injected with genetically modified autologous T-cells expressing NY-ESO1-1c259, an anti-NY-ESO specific receptor. Engineered T-cell persistence was determined by qPCR. Serum cytokines were evaluated by immunoassay. Transcriptomic analyses and immunohistochemistry were performed on tumor biopsies from patients before and after T-cell infusion. Responses across cohorts were affected by preconditioning and intra-tumoral NY-ESO-1 expression. Of the 42 patients that were evaluated, 1 patient achieved a complete response, 14 achieved partial responses, 24 showed stable disease (SD), and progressive disease (PD) was observed in only 3 patients. The study concluded that a lymphodepletion regimen containing high doses of fludarabine and cyclophosphamide is necessary for genetically modified autologous T-cell persistence and efficacy[93]. Another important pilot trial by Robbins et al. tested autologous TCR-transduced T-cells following lymphodepleting chemotherapy on patients with metastatic synovial cell sarcoma or melanoma expressing NY-ESO-1 that were refractory to standard. Out of 18 patients with NY-ESO-1 positive synovial cell sarcomas, 11 demonstrated objective clinical responses. The estimated overall 3- and 5-year survival rates for patients with synovial cell sarcoma were 38% and 14% respectively [94].
In a phase 2 open label trial called SPEARHEAD 1, D’Angelo et al. aimed to evaluate the efficacy, safety, and tolerability of afamitresgene autoleucel in patients with advanced/metastatic synovial sarcoma (SS) or Myxoid/Round Cell Liposarcoma (MLS). Afamitresgene autoleucel is a genetically engineered autologous specific peptide enhanced affinity receptor (SPEAR) targeting MAGE-A4. Patients with MAGE-A4-expressing tumors underwent leukapheresis for collection of autologous T-cells for processing and manufacture into afamitresgene autoleucel cells, which were infused back into the patients after lymphodepleting chemotherapy. Among 25 evaluable subjects (23 SS and 2 MLS), there were 2 CR, 8 PR and 11 SD (DCR 84%). Side-effects were manageable with mainly low-grade cytokine release syndrome (CRS) and reversible hematologic toxicities due to lymphodepleting chemotherapy[95]. Unlike TCRs, which can only recognize Major Histocompatibility complex (MHC1) restricted peptides, CAR T-cells can target any protein expressed on the surface of tumor cells.
Figure 4.
ONCOLYTIC VIRUSES.
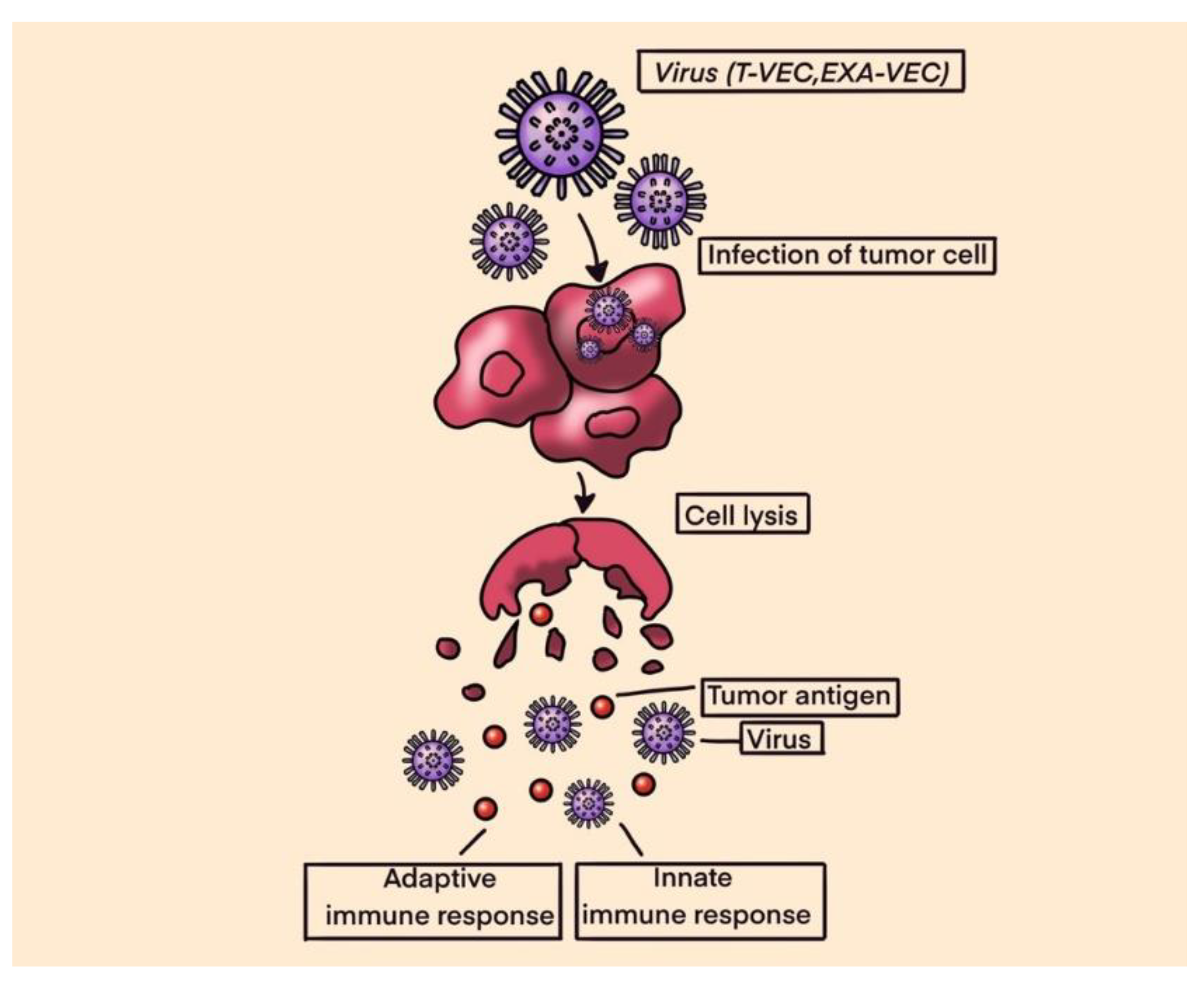
Oncolytic viruses are thought to mediate antitumor activity through two distinct mechanisms of action: selective replication within neoplastic cells, resulting in a direct lytic effect on tumor cells; and induction of systemic antitumor immunity. Lysis of tumor cells releases tumor-specific antigens that trigger both the innate and adaptive immune systems [96]. Tumor antigens released by destroyed cancer cells are processed by antigen presenting cells (APC) and presented to the CD4+ and CD8+ lymphocytes, triggering the immune response that enhance tumor destruction. OVs can be divided into two major categories: natural viruses and genetically modified virus strains. Natural viruses include wild type and naturally variant strains of weak viruses[97]. With the development of molecular biology techniques, genetic editing technology is used to optimize these wild virus strains, to weaken viral pathogenicity and improve immunogenicity. Insertion of an exogenous therapeutic gene into the OV genome, to increase its expression in the tumor, makes it is possible to avoid the occurrence of a systemic immune response and enhances the lethality of the virus[98].
In a study by Le Boeuf et al. four oncolytic viruses, reovirus, vaccinia virus, herpes-simplex virus and two rhabdoviruses (vesicular stomatitis virus and maraba virus MG1) were screened for their ability to infect and kill sarcoma cell lines in-vitro. In the in-vitro setting, both rhabdoviruses demonstrated a high potency in their ability to kill sarcoma cells, with - MG1 showing productive viral replication in 18 of 21 tumor samples (86%) and inducing >50% cell death at lower concentrations. Ex vivo, the efficacy of MG1 was tested on murine models infected with tumor cells that were seeded subcutaneously in mice. MG1 was then administered intra-tumorally. Results showed that MG1 effectively replicates in murine sarcoma tumors, leading to eradication of 80% of tumors. Additionally, MG1 also induced the generation of a memory immune response that provided protection against a subsequent tumor challenge[99].
The modified herpes simplex virus known as Talimogene laherparepvec (T-VEC) was approved by the FDA for the treatment of melanoma in 2015. The success of TVEC in melanoma has led to its evaluation in other solid malignancies. In a phase IB/II trial, Monga et al. explored a novel combination of TVEC with external beam radiation therapy (EBRT) administered preoperatively in patients with locally advanced STS of the extremities and trunk. The combination was safe and well-tolerated, however only 5 of the 23 evaluable achieved the primary endpoint of pathological complete response (pCR defined as ≥95% tumor necrosis)[100]. In another phase 2 clinical trial by Kelly et al., treatment with T-VEC plus pembrolizumab was associated with antitumor activity in advanced sarcoma across a range of sarcoma histologic subtypes, with a manageable safety profile. The study met its primary end point, with an ORR at 24 weeks of 35% (95% CI, 15%-59%; n = 7)[101].
Overall, the aforementioned studies suggest OVs could be promising immunotherapies for the treatment of sarcoma. So far, OVs have had limited success as monotherapies suggesting that OVs will likely require use in combination with other modalities that can overcome known resistance mechanisms, including innate antiviral responses and immunological resistance.
Figure 5.
CANCER VACCINES.
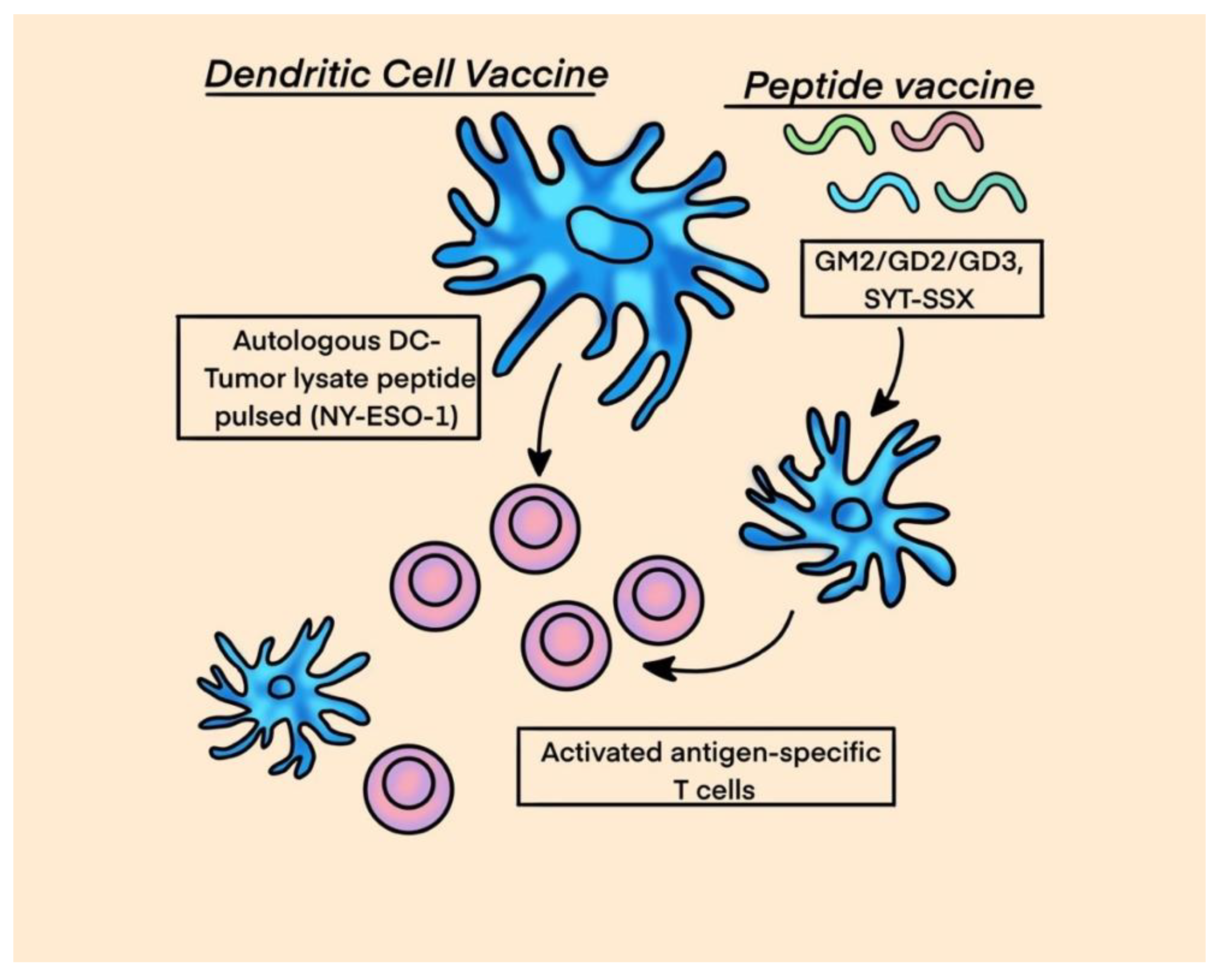
Cancer vaccines is a realm of immunotherapy where selected tumor antigens are exogenously administered along with adjuvants/immunostimulants, such as granulocyte-macrophage colony-stimulating factor (GM-CSF) or interferon-gamma a to induce the activity of APCs, mainly dendritic cells, aiming to stimulate the adaptive immune system against cancer cells. Antigens for vaccines can be procured from: 1. killed tumor cells, 2. antigens purified from patients with tumor, 3. antigens produced in vitro. The main over-expressed CTAs in sarcomas are NY-ESO-1, MAGE, PRAME (preferentially expressed antigen of Melanoma), BAGE (B melanoma antigen), CAGE (Cancer associated antigen gene); all of them may be excellent candidates for vaccines and as targets for genetically modified adoptive T cells.
In a randomized phase II study by Carvajal et al. immunological adjuvant with a conjugated ganglioside vaccine targeting ganglioside monosialic (GM2), diasialoganglioside (GD2), GD3 and control was tested in patients with metastatic sarcoma following complete metastasectomy. Patients received total of ten injections and imaging was performed to evaluate response. The primary endpoint was progression-free survival (PFS). Secondary endpoints included overall survival (OS) and serologic response. Median PFS and 1-year PFS rate were 6.4 months and 35%, respectively, with no difference between arms. The 1-year OS rate was >90%. Serologic responses (IgM and/or IgG) to GM2 and GD2 were observed in 98% and 21% of pts treated with complete vaccine and control, respectively. At weeks 40-68, induction of high (>160) IgM and IgG titers was observed in 52% and 24% of pts receiving vaccine and 0% and 2% of pts receiving control. No difference in PFS was observed between arms [102].
Unique chromosomal translocation events are ubiquitous within certain sarcoma subtypes such as the t(X;18)(p11;q11) translocation in synovial sarcoma or the t(12;16)(q13;p11) translocation in myxoid/round cell liposarcoma, and are attractive vaccine targets as the newly-formed peptide will potentially represent a tumor-specific neoantigen. A fragment of the SYT-SSX fusion peptide that results from the characteristic synovial sarcoma translocation was studied by Kawaguchi et al. as a vaccine in 21 patients with advanced synovial sarcoma that were deemed unresectable and previously failed first line of treatment. One out of nine patients administered with the peptide fragment alone did not have disease progression within the study period, and 6 out of 12 patients who received the peptide with an adjuvant and interferon-α had stable disease, one patient exhibited transient shrinkage of a metastatic lesion [103].
In addition to vaccines based on specific peptides, a potential approach to induce tumor recognition is the production of vaccines derived from whole tumor cells combined with immune-enhancing adjuvants (such as IFN-γ and GM-CSF). In a phase II study, Chawla et al. studied CMB305 and atezolizumab compared with atezolizumab alone in soft tissue sarcomas expressing NY-ESO-1[104]. CMB305 is a heterologous prime-boost vaccination regimen created to prime NY-ESO-1-specific CD8 T-cell populations and then activate the immune response with a potent toll-like receptor 4(TLR-4) agonist. Patients with locally advanced, relapsed, or metastatic synovial sarcoma or myxoid liposarcoma were randomly assigned to receive CMB305 with atezolizumab or atezolizumab alone. PFS was 2.6 months and 1.6 months in the combination and control arms, respectively (hazard ratio, 0.9; 95% CI, 0.6 to 1.3). Median OS was 18 months in both treatment arms. The combination of CMB305 and atezolizumab did not result in significant increases in PFS or OS compared with atezolizumab alone. Some patients demonstrated evidence of an anti-NY-ESO-1 immune response and appeared to fare better by imaging than those without such an immune response, however this combination approach merits further evaluation.
Although cancer vaccines for sarcoma appear to be safe and result in an immunological response in most of the patients, limited improvement in clinical outcome of patients suggests that many modifications need to be made to attain better therapeutic outcomes. Further research in this field is warranted.
10. Cancer targeted antibodies
Gangliosides are plasma membrane-bound glycosphingolipids which interact with membrane proteins to regulate the cell signaling pathway [105,106,107]. The monosaccharide component protruding outside of the cell membrane has antigenic properties and participates in intercellular communication and adhesion [107,108,109]. Multiple subtypes of gangliosides such as GM3, GM2, GM1 are found on normal cells and regulate the function of membrane bound signaling proteins [109,110]. However, disialoganglioside (GD2) is expressed mostly on tumor cells, with limited expression on normal central and peripheral nerve fibers, mesenchymal stem cells, melanocytes, and lymphocytes [111,112]. This specific tumor antigenic quality of GD2 becomes not only an interesting target in cancer immunotherapy but also a biomarker to predict prognosis and a cancer imaging modality via radioimmunodetection [113,114].
GD2 expression is notable in Ewing sarcoma, usually confirmed by immunostaining [115,116]. In osteosarcoma, the higher intensity of IHC staining was observed in recurrent or relapsed disease tissue section compared to the initial tissue resection [117]. Combination therapy of an anti-GD2 mAb (14G2a) and cisplatin has synergistic effect on apoptosis of the osteosarcoma cells in vitro [118]. In the study, 70-85% of cells apoptosis was observed in osteosarcoma cells treated with cisplatin and 14G2a combination. In soft tissue sarcoma, the expression of GD2 varies from 25% to 93% among different subtypes [119,120].
Another interesting target is CD47, a transmembrane bound protein highly expressed on some tumor cells including angiosarcomas. By producing CD47, tumor cells resist phagocytosis by macrophages; as such, inhibiting CD47 could result in increased tumor cell death [121]. In one of the vitro studies, anti-CD47 therapy increased the production of pro-inflammatory cytokines in the TME of soft tissue sarcomas [122]. In an vivo study using a murine model, the combination of the anti-GD2 antibody dinutuximab and an anti-CD47 antibody (B6H12) was shown to have synergistic activity [123]. In this study, mice with osteosarcoma with pulmonary metastases were treated with a control antibody, anti-GD2, anti-CD47, or a combination of both anti-GD2 and anti-CD47. It was found that anti-GD2 antibody alone did not alter the burden of pulmonary metastases, the anti-CD47 antibody alone reduced the burden of metastases, and the combination treatment eradicated nearly all pulmonary metastatic disease [123]. This is in keeping with a previous trial where dinutuximab (anti-GD2) was used as a single agent in relapsed osteosarcoma in children and young adults, in which disease control rate did not improve [124]. The reasoning for the combination being more potent is a synergism where anti-GD2 primes tumor cells for phagocytosis via upregulation of surface proteins, while anti-CD47 prevents the tumor’s “don’t eat me” signals [123]. The ongoing phase I clinical trial (NCT04751383) is testing the combination therapy of magrolimab (anti-CD47) and dinutuximab (anti-GD2) in patients with relapsed or refractory neuroblastoma or relapsed osteosarcoma.
11. Conclusions
The impact of modern immunotherapeutic modalities across various cancer types presents an exciting opportunity for further studies in treatment of sarcomas. An accumulating understanding of the immune microenvironment and antigenic signatures of various sarcoma subtypes has generated promising new targets for immunotherapy. Despite of unrivaled progress in the field of immune oncology over the last decade, early experiences of immunotherapy with sarcomas has been disappointing due to antigenic heterogeneity and rarity of the disease. Although it is difficult to adequately capture the complexity of sarcomas, it appears combination therapies involving ICBs is likely the path forward. When it comes to sarcomas, there is no “one size fits all” strategy and each subtype will require stringent characterization of its immune components and antigenic signatures to select an optimal treatment modality. Further studies are encouraged to develop effective immunotherapy-based regimens for treatment of sarcomas to have better responses and clinical outcomes with manageable toxicity profiles.
Author Contributions
First author (Shivani Dalal) contributed to this manuscript’s conceptualization, original draft preparation; Writing- Shivani Dalal, Khine Shan, Nyein Nyein Thaw Dar, Misha Dalal, Alejandra Ergle; Review and editing- Shivani Dalal, , Khine Shan, Nyein Nyein Thaw Dar, Atif Hussein, Alejandra Ergle; Tables- Shivani Dalal and Khine Shan; Figures/Diagrams: Misha Dalal. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not Applicable.
Informed Consent Statement
Not Applicable.
Data Availability Statement
Not Applicable.
Acknowledgments
We would like to thank Misha Dalal from Government Medical College, India. In this paper, Misha Dalal has worked on some sections of the adoptive cell therapy, such as Oncolytic viruses and Cancer Vaccines. She has also created all the medical illustrations for the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Banks, L.B.; D’Angelo, S.P. The Role of Immunotherapy in the Management of Soft Tissue Sarcomas: Current Landscape and Future Outlook. J. Natl. Compr. Canc Netw. 2022, 20, 834–844. [Google Scholar] [CrossRef] [PubMed]
- Sbaraglia, M.; Bellan, E.; Dei Tos, A.P. The 2020 WHO Classification of Soft Tissue Tumours: news and perspectives. Pathol. J. Ital. Soc. Anat. Pathol. Diagn. Cytopathol. 2020, 113, 70–84. [Google Scholar] [CrossRef] [PubMed]
- Savina, M.; Le Cesne, A.; Blay, J.Y.; Ray-Coquard, I.; Mir, O.; Toulmonde, M.; Cousin, S.; Terrier, P.; Ranchere-Vince, D.; Meeus, P.; et al. Patterns of care and outcomes of patients with METAstatic soft tissue SARComa in a real-life setting: the METASARC observational study. BMC Med. 2017, 15, 78. [Google Scholar] [CrossRef] [PubMed]
- Albarrán, V.; Villamayor, M.L.; Pozas, J.; Chamorro, J.; Rosero, D.I.; San Román, M.; Guerrero, P.; Pérez de Aguado, P.; Calvo, J.C.; García de Quevedo, C.; et al. Current Landscape of Immunotherapy for Advanced Sarcoma. Cancers 2023, 15, 2287. [Google Scholar] [CrossRef]
- Clemente, O.; Ottaiano, A.; Di Lorenzo, G.; Bracigliano, A.; Lamia, S.; Cannella, L.; Pizzolorusso, A.; Di Marzo, M.; Santorsola, M.; De Chiara, A.; et al. Is immunotherapy in the future of therapeutic management of sarcomas? J. Transl. Med. 2021, 19, 173. [Google Scholar] [CrossRef]
- Von Mehren, M.; Kane, J.M.; Agulnik, M.; Bui, M.M.; Carr-Ascher, J.; Choy, E.; Connelly, M.; Dry, S.; Ganjoo, K.N.; Gonzalez, R.J.; et al. Soft Tissue Sarcoma, Version 2.2022, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2022, 20, 815–833. [Google Scholar] [CrossRef]
- Penel, N.; Bui, B.N.; Bay, J.-O.; Cupissol, D.; Ray-Coquard, I.; Piperno-Neumann, S.; Kerbrat, P.; Fournier, C.; Taieb, S.; Jimenez, M.; et al. Phase II Trial of Weekly Paclitaxel for Unresectable Angiosarcoma: The ANGIOTAX Study. J. Clin. Oncol. 2008, 26, 5269–5274. [Google Scholar] [CrossRef] [PubMed]
- Wagner, A.J.; Ravi, V.; Riedel, R.F.; Ganjoo, K.; Tine, B.A.V.; Chugh, R.; Cranmer, L.; Gordon, E.M.; Hornick, J.L.; Du, H.; et al. nab-Sirolimus for Patients With Malignant Perivascular Epithelioid Cell Tumors. J. Clin. Oncol. 2021, 39, 3660–3670. [Google Scholar] [CrossRef] [PubMed]
- Seddon, B.; Strauss, S.J.; Whelan, J.; Leahy, M.; Woll, P.J.; Cowie, F.; Rothermundt, C.; Wood, Z.; Benson, C.; Ali, N.; et al. Gemcitabine and docetaxel versus doxorubicin as first-line treatment in previously untreated advanced unresectable or metastatic soft-tissue sarcomas (GeDDiS): a randomised controlled phase 3 trial. Lancet Oncol. 2017, 18, 1397–1410. [Google Scholar] [CrossRef] [PubMed]
- Grünwald, V.; Karch, A.; Schuler, M.; Schöffski, P.; Kopp, H.-G.; Bauer, S.; Kasper, B.; Lindner, L.H.; Chemnitz, J.-M.; Crysandt, M.; et al. Randomized Comparison of Pazopanib and Doxorubicin as First-Line Treatment in Patients With Metastatic Soft Tissue Sarcoma Age 60 Years or Older: Results of a German Intergroup Study. J. Clin. Oncol. 2020, 38, 3555–3564. [Google Scholar] [CrossRef] [PubMed]
- van der Graaf, W.T.; Blay, J.Y.; Chawla, S.P.; Kim, D.W.; Bui-Nguyen, B.; Casali, P.G.; Schoffski, P.; Aglietta, M.; Staddon, A.P.; Beppu, Y.; et al. Pazopanib for metastatic soft-tissue sarcoma (PALETTE): a randomised, double-blind, placebo-controlled phase 3 trial. Lancet 2012, 379, 1879–1886. [Google Scholar] [CrossRef]
- Mir, O.; Brodowicz, T.; Italiano, A.; Wallet, J.; Blay, J.Y.; Bertucci, F.; Chevreau, C.; Piperno-Neumann, S.; Bompas, E.; Salas, S.; et al. Safety and efficacy of regorafenib in patients with advanced soft tissue sarcoma (REGOSARC): a randomised, double-blind, placebo-controlled, phase 2 trial. Lancet Oncol. 2016, 17, 1732–1742. [Google Scholar] [CrossRef] [PubMed]
- Gounder, M.M.; Mahoney, M.R.; Van Tine, B.A.; Ravi, V.; Attia, S.; Deshpande, H.A.; Gupta, A.A.; Milhem, M.M.; Conry, R.M.; Movva, S.; et al. Sorafenib for Advanced and Refractory Desmoid Tumors. N. Engl. J. Med. 2018, 379, 2417–2428. [Google Scholar] [CrossRef] [PubMed]
- Rutkowski, P.; Klimczak, A.; Ługowska, I.; Jagielska, B.; Wągrodzki, M.; Dębiec-Rychter, M.; Pieńkowska-Grela, B.; Świtaj, T. Long-term results of treatment of advanced dermatofibrosarcoma protuberans (DFSP) with imatinib mesylate – The impact of fibrosarcomatous transformation. Eur. J. Surg. Oncol. (EJSO) 2017, 43, 1134–1141. [Google Scholar] [CrossRef] [PubMed]
- Demetri, G.D.; Von Mehren, M.; Blanke, C.D.; Van Den Abbeele, A.D.; Eisenberg, B.; Roberts, P.J.; Heinrich, M.C.; Tuveson, D.A.; Singer, S.; Janicek, M.; et al. Efficacy and Safety of Imatinib Mesylate in Advanced Gastrointestinal Stromal Tumors. N. Engl. J. Med. 2002, 347, 472–480. [Google Scholar] [CrossRef]
- Misaghi, A.; Goldin, A.; Awad, M.; Kulidjian, A.A. Osteosarcoma: a comprehensive review. SICOT-J. 2018, 4, 12. [Google Scholar] [CrossRef]
- Zöllner, S.K.; Amatruda, J.F.; Bauer, S.; Collaud, S.; de Álava, E.; DuBois, S.G.; Hardes, J.; Hartmann, W.; Kovar, H.; Metzler, M.; et al. Ewing Sarcoma-Diagnosis, Treatment, Clinical Challenges and Future Perspectives. J. Clin. Med. 2021, 10, 1685. [Google Scholar] [CrossRef] [PubMed]
- Gazendam, A.; Popovic, S.; Parasu, N.; Ghert, M. Chondrosarcoma: A Clinical Review. J. Clin. Med. 2023, 12, 2506. [Google Scholar] [CrossRef]
- Albarran, V.; Villamayor, M.L.; Chamorro, J.; Rosero, D.I.; Pozas, J.; San Roman, M.; Calvo, J.C.; Perez de Aguado, P.; Moreno, J.; Guerrero, P.; et al. Receptor Tyrosine Kinase Inhibitors for the Treatment of Recurrent and Unresectable Bone Sarcomas. Int. J. Mol. Sci. 2022, 23, 13784. [Google Scholar] [CrossRef] [PubMed]
- FDA.gov. FDA grants approval to atezolizumab for alveolar soft part sarcoma. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-grants-approval-atezolizumab-alveolar-soft-part-sarcoma#:~:text=On%20December%209%2C%202022%2C%20the%20Food%20and%20Drug,unresectable%20or%20metastatic%20alveolar%20soft%20part%20sarcoma%20%28ASPS%29. (accessed on October 5, 2023).
- Groisberg, R.; Hong, D.S.; Behrang, A.; Hess, K.; Janku, F.; Piha-Paul, S.; Naing, A.; Fu, S.; Benjamin, R.; Patel, S.; et al. Characteristics and outcomes of patients with advanced sarcoma enrolled in early phase immunotherapy trials. J. Immunother. Cancer 2017, 5, 100. [Google Scholar] [CrossRef]
- Chalmers, Z.R.; Connelly, C.F.; Fabrizio, D.; Gay, L.; Ali, S.M.; Ennis, R.; Schrock, A.; Campbell, B.; Shlien, A.; Chmielecki, J.; et al. Analysis of 100,000 human cancer genomes reveals the landscape of tumor mutational burden. Genome Med. 2017, 9, 34. [Google Scholar] [CrossRef] [PubMed]
- Petitprez, F.; de Reyniès, A.; Keung, E.Z.; Chen, T.W.; Sun, C.M.; Calderaro, J.; Jeng, Y.M.; Hsiao, L.P.; Lacroix, L.; Bougoüin, A.; et al. B cells are associated with survival and immunotherapy response in sarcoma. Nature 2020, 577, 556–560. [Google Scholar] [CrossRef] [PubMed]
- Sautès-Fridman, C.; Petitprez, F.; Calderaro, J.; Fridman, W.H. Tertiary lymphoid structures in the era of cancer immunotherapy. Nat. Rev. Cancer 2019, 19, 307–325. [Google Scholar] [CrossRef] [PubMed]
- Italiano, A.; Bessede, A.; Pulido, M.; Bompas, E.; Piperno-Neumann, S.; Chevreau, C.; Penel, N.; Bertucci, F.; Toulmonde, M.; Bellera, C.; et al. Pembrolizumab in soft-tissue sarcomas with tertiary lymphoid structures: a phase 2 PEMBROSARC trial cohort. Nat. Med. 2022, 28, 1199–1206. [Google Scholar] [CrossRef] [PubMed]
- Tang, H.; Liu, S.; Luo, X.; Sun, Y.; Li, X.; Luo, K.; Liao, S.; Li, F.; Liang, J.; Zhan, X.; et al. A novel molecular signature for predicting prognosis and immunotherapy response in osteosarcoma based on tumor-infiltrating cell marker genes. Front. Immunol. 2023, 14, 1150588. [Google Scholar] [CrossRef] [PubMed]
- Kostine, M.; Briaire-de Bruijn, I.H.; Cleven, A.H.G.; Vervat, C.; Corver, W.E.; Schilham, M.W.; Van Beelen, E.; van Boven, H.; Haas, R.L.; Italiano, A.; et al. Increased infiltration of M2-macrophages, T-cells and PD-L1 expression in high grade leiomyosarcomas supports immunotherapeutic strategies. Oncoimmunology 2018, 7, e1386828. [Google Scholar] [CrossRef] [PubMed]
- Keung, E.Z.; Burgess, M.; Salazar, R.; Parra, E.R.; Rodrigues-Canales, J.; Bolejack, V.; Van Tine, B.A.; Schuetze, S.M.; Attia, S.; Riedel, R.F.; et al. Correlative Analyses of the SARC028 Trial Reveal an Association Between Sarcoma-Associated Immune Infiltrate and Response to Pembrolizumab. Clin. Cancer Res. 2020, 26, 1258–1266. [Google Scholar] [CrossRef] [PubMed]
- Atılgan, A.O.; Tepeoğlu, M.; Özen, Ö.; Reyhan, A.N.H.; Ayhan, A. The expression of programmed death-ligand 1 and programmed death-ligand 2 in endometrial carcinosarcoma: Correlation with mismatch repair protein expression status, tumor-infiltrating lymphocyte infiltration, and clinical outcomes. Ann. Diagn. Pathol. 2023, 65, 152137. [Google Scholar] [CrossRef] [PubMed]
- Ok Atılgan, A.; Yılmaz Akçay, E.; Özen, Ö.; Haberal Reyhan, A.N.; Ayhan, A. The Overexpression of Programmed Death-Ligand 2 in Uterine Adenosarcoma: Correlation with High-Grade Morphology, Mutant Type TP53 Expression and Clinical Outcomes. Int. J. Surg. Pathol. 2023, 31, 352–364. [Google Scholar] [CrossRef] [PubMed]
- Qin, S.; Xu, L.; Yi, M.; Yu, S.; Wu, K.; Luo, S. Novel immune checkpoint targets: moving beyond PD-1 and CTLA-4. Molecular Cancer 2019, 18. [Google Scholar] [CrossRef]
- Tawbi, H.A.; Burgess, M.; Bolejack, V.; Van Tine, B.A.; Schuetze, S.M.; Hu, J.; D’Angelo, S.; Attia, S.; Riedel, R.F.; Priebat, D.A.; et al. Pembrolizumab in advanced soft-tissue sarcoma and bone sarcoma (SARC028): a multicentre, two-cohort, single-arm, open-label, phase 2 trial. Lancet Oncol. 2017, 18, 1493–1501. [Google Scholar] [CrossRef] [PubMed]
- Maki, R.G.; Jungbluth, A.A.; Gnjatic, S.; Schwartz, G.K.; D’Adamo, D.R.; Keohan, M.L.; Wagner, M.J.; Scheu, K.; Chiu, R.; Ritter, E.; et al. A Pilot Study of Anti-CTLA4 Antibody Ipilimumab in Patients with Synovial Sarcoma. Sarcoma 2013, 2013, 168145. [Google Scholar] [CrossRef] [PubMed]
- Ben-Ami, E.; Barysauskas, C.M.; Solomon, S.; Tahlil, K.; Malley, R.; Hohos, M.; Polson, K.; Loucks, M.; Severgnini, M.; Patel, T.; et al. Immunotherapy with single agent nivolumab for advanced leiomyosarcoma of the uterus: Results of a phase 2 study. Cancer 2017, 123, 3285–3290. [Google Scholar] [CrossRef] [PubMed]
- Burgess, M.A.; Bolejack, V.; Schuetze, S.; Tine, B.A.V.; Attia, S.; Riedel, R.F.; Hu, J.S.; Davis, L.E.; Okuno, S.H.; Priebat, D.A.; et al. Clinical activity of pembrolizumab (P) in undifferentiated pleomorphic sarcoma (UPS) and dedifferentiated/pleomorphic liposarcoma (LPS): Final results of SARC028 expansion cohorts. J. Clin. Oncol. 2019, 37, 11015–11015. [Google Scholar] [CrossRef]
- Blay, J.-Y.; Penel, N.; Ray-Coquard, I.L.; Cousin, S.; Bertucci, F.; Bompas, E.; Eymard, J.-C.; Saada-Bouzid, E.; Soulie, P.; Boudou-Rouquette, P.; et al. High clinical activity of pembrolizumab in chordoma, alveolar soft part sarcoma (ASPS) and other rare sarcoma histotypes: The French AcSé pembrolizumab study from Unicancer. J. Clin. Oncol. 2021, 39, 11520–11520. [Google Scholar] [CrossRef]
- Italiano, A.; Bellera, C.; D’Angelo, S. PD1/PD-L1 targeting in advanced soft-tissue sarcomas: a pooled analysis of phase II trials. J. Hematol. Oncol. 2020, 13, 55. [Google Scholar] [CrossRef]
- Chen, Y.; Liu, X.; Liu, J.; Liang, D.; Zhao, M.; Yu, W.; Chen, P. Nivolumab plus ipilimumab versus nivolumab in individuals with treatment-naive programmed death-ligand 1 positive metastatic soft tissue sarcomas: a multicentre retrospective study. BMC Cancer 2021, 21, 108. [Google Scholar] [CrossRef]
- Lussier, D.M.; Johnson, J.L.; Hingorani, P.; Blattman, J.N. Combination immunotherapy with α-CTLA-4 and α-PD-L1 antibody blockade prevents immune escape and leads to complete control of metastatic osteosarcoma. J. Immunother. Cancer 2015, 3, 21. [Google Scholar] [CrossRef] [PubMed]
- D’Angelo, S.P.; Mahoney, M.R.; Van Tine, B.A.; Atkins, J.; Milhem, M.M.; Jahagirdar, B.N.; Antonescu, C.R.; Horvath, E.; Tap, W.D.; Schwartz, G.K.; et al. Nivolumab with or without ipilimumab treatment for metastatic sarcoma (Alliance A091401): two open-label, non-comparative, randomised, phase 2 trials. Lancet Oncol. 2018, 19, 416–426. [Google Scholar] [CrossRef] [PubMed]
- Uboha, N.V.; Milhem, M.M.; Kovacs, C.; Amin, A.; Magley, A.; Purkayastha, D.D.; Piha-Paul, S.A. Phase II study of spartalizumab (PDR001) and LAG525 in advanced solid tumors and hematologic malignancies. J. Clin. Oncol. 2019, 37, 2553–2553. [Google Scholar] [CrossRef]
- Naqash, A.R.; Coyne, G.H.O.S.; Moore, N.; Sharon, E.; Takebe, N.; Fino, K.K.; Ferry-Galow, K.V.; Hu, J.S.; Tine, B.A.V.; Burgess, M.A.; et al. Phase II study of atezolizumab in advanced alveolar soft part sarcoma (ASPS). J. Clin. Oncol. 2021, 39, 11519–11519. [Google Scholar] [CrossRef]
- Chen, A.P.; Sharon, E.; O’Sullivan-Coyne, G.; Moore, N.; Foster, J.C.; Hu, J.S.; Van Tine, B.A.; Conley, A.P.; Read, W.L.; Riedel, R.F.; et al. Atezolizumab for Advanced Alveolar Soft Part Sarcoma. N. Engl. J. Med. 2023, 389, 911–921. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.S.; Yang, H.; Chon, H.J.; Kim, C. Combination of anti-angiogenic therapy and immune checkpoint blockade normalizes vascular-immune crosstalk to potentiate cancer immunity. Exp. Mol. Med. 2020, 52, 1475–1485. [Google Scholar] [CrossRef] [PubMed]
- Fleuren, E.D.G.; Terry, R.L.; Meyran, D.; Omer, N.; Trapani, J.A.; Haber, M.; Neeson, P.J.; Ekert, P.G. Enhancing the Potential of Immunotherapy in Paediatric Sarcomas: Breaking the Immunosuppressive Barrier with Receptor Tyrosine Kinase Inhibitors. Biomedicines 2021, 9, 1798. [Google Scholar] [CrossRef] [PubMed]
- Palmerini, E.; Lopez-Pousa, A.; Grignani, G.; Redondo, A.; Hindi, N.; Stacchiotti, S.; Sebio, A.; Lopez-Martin, J.A.; Morales, C.M.V.; Martinez-Trufero, J.; et al. IMMUNOSARC: a collaborative Spanish (GEIS) and Italian (ISG) sarcoma groups phase I/II trial of sunitinib and nivolumab in advanced soft tissue and bone sarcoma: Results from the phase II part, bone sarcoma cohort. J. Clin. Oncol. 2020, 38, 11522–11522. [Google Scholar] [CrossRef]
- Martin-Broto, J.; Hindi, N.; Grignani, G.; Martinez-Trufero, J.; Redondo, A.; Valverde, C.; Stacchiotti, S.; Lopez-Pousa, A.; D’Ambrosio, L.; Gutierrez, A.; et al. Nivolumab and sunitinib combination in advanced soft tissue sarcomas: a multicenter, single-arm, phase Ib/II trial. J. ImmunoTherapy Cancer 2020, 8, e001561. [Google Scholar] [CrossRef] [PubMed]
- Wilky, B.A.; Trucco, M.M.; Subhawong, T.K.; Florou, V.; Park, W.; Kwon, D.; Wieder, E.D.; Kolonias, D.; Rosenberg, A.E.; Kerr, D.A.; et al. Axitinib plus pembrolizumab in patients with advanced sarcomas including alveolar soft-part sarcoma: a single-centre, single-arm, phase 2 trial. Lancet Oncol. 2019, 20, 837–848. [Google Scholar] [CrossRef]
- Xie, L.; Xu, J.; Sun, X.; Guo, W.; Gu, J.; Liu, K.; Zheng, B.; Ren, T.; Huang, Y.; Tang, X.; et al. Apatinib plus camrelizumab (anti-PD1 therapy, SHR-1210) for advanced osteosarcoma (APFAO) progressing after chemotherapy: a single-arm, open-label, phase 2 trial. J. ImmunoTherapy Cancer 2020, 8, e000798. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Cho, H.J.; Yun, K.-H.; Lee, Y.H.; Kim, S.H.; Baek, W.; Jeon, M.K. Durvalumab and pazopanib in patients with advanced soft tissue sarcoma: A single-center, single-arm, phase 2 trial. J. Clin. Oncol. 2021, 39, 11551–11551. [Google Scholar] [CrossRef]
- Cho, H.J.; Yun, K.-H.; Shin, S.-J.; Lee, Y.H.; Kim, S.H.; Baek, W.; Han, Y.D.; Kim, S.K.; Lee, J.; Cho, I.; et al. Abstract CT038: Comprehensive molecular characterization of clinical response to durvalumab plus pazopanib combination in patients with advanced soft tissue sarcomas: A phase 2 clinical trial. Cancer Res. 2023, 83, CT038–CT038. [Google Scholar] [CrossRef]
- Roulleaux Dugage, M.; Nassif, E.F.; Italiano, A.; Bahleda, R. Improving Immunotherapy Efficacy in Soft-Tissue Sarcomas: A Biomarker Driven and Histotype Tailored Review. Front. Immunol. 2021, 12, 775761. [Google Scholar] [CrossRef] [PubMed]
- Toulmonde, M.; Penel, N.; Adam, J.; Chevreau, C.; Blay, J.Y.; Le Cesne, A.; Bompas, E.; Piperno-Neumann, S.; Cousin, S.; Grellety, T.; et al. Use of PD-1 Targeting, Macrophage Infiltration, and IDO Pathway Activation in Sarcomas: A Phase 2 Clinical Trial. JAMA Oncol. 2018, 4, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Pollack, S.M.; Redman, M.W.; Baker, K.K.; Wagner, M.J.; Schroeder, B.A.; Loggers, E.T.; Trieselmann, K.; Copeland, V.C.; Zhang, S.; Black, G.; et al. Assessment of Doxorubicin and Pembrolizumab in Patients With Advanced Anthracycline-Naive Sarcoma: A Phase 1/2 Nonrandomized Clinical Trial. JAMA Oncol. 2020, 6, 1778–1782. [Google Scholar] [CrossRef] [PubMed]
- Livingston, M.B.; Jagosky, M.H.; Robinson, M.M.; Ahrens, W.A.; Benbow, J.H.; Farhangfar, C.J.; Foureau, D.M.; Maxwell, D.M.; Baldrige, E.A.; Begic, X.; et al. Phase II Study of Pembrolizumab in Combination with Doxorubicin in Metastatic and Unresectable Soft-Tissue Sarcoma. Clin. Cancer Res. 2021, 27, 6424–6431. [Google Scholar] [CrossRef]
- Wagner, M.; He, Q.; Zhang, Y.; Cranmer, L.; Loggers, E.; McDonnell, S.; Maxwell, S.; Pollack, S. 796 A phase I/II trial combining avelumab and trabectedin for advanced liposarcoma and leiomyosarcoma. J. ImmunoTherapy Cancer 2020, 8, A476–A476. [Google Scholar] [CrossRef]
- Andreou, D.; Flörcken, A.; Groß, T.; Richter, S.; Kessler, T.; Kortüm, M.; Schmidt, C.A.; Kasper, B.; Wardelmann, E.; Benedict, A.; et al. Efficacy and safety of nivolumab and trabectedin in pretreated patients with advanced soft tissue sarcomas (STS): Results of a phase II trial of the German Interdisciplinary Sarcoma Group (GISG-15, NitraSarc). J. Clin. Oncol. 2023, 41, 11500–11500. [Google Scholar] [CrossRef]
- Maleddu, A.; Mailhot, A.; Cartwright, C.; Gao, D.; Tellez, C.M.; Powers, K.; Kemp, L.; Therrien, N.; Patel, J.M.; Grossman, J.E.; et al. A single-arm, open-label phase 2 trial of doxorubicin plus zalifrelimab, a CTLA-4 inhibitor, with balstilimab, a PD-1 inhibitor, in patients with advanced/metastatic soft tissue sarcomas. J. Clin. Oncol. 2023, 41, 11501–11501. [Google Scholar] [CrossRef]
- Roland, C.L.; Keung, E.Z.-Y.; Lazar, A.J.; Torres, K.E.; Wang, W.-L.; Guadagnolo, A.; Bishop, A.J.; Lin, H.Y.; Hunt, K.; Feig, B.W.; et al. Preliminary results of a phase II study of neoadjuvant checkpoint blockade for surgically resectable undifferentiated pleomorphic sarcoma (UPS) and dedifferentiated liposarcoma (DDLPS). J. Clin. Oncol. 2020, 38, 11505–11505. [Google Scholar] [CrossRef]
- Keung, E.Z.; Tsai, J.-W.; Ali, A.M.; Cormier, J.N.; Bishop, A.J.; Guadagnolo, B.A.; Torres, K.E.; Somaiah, N.; Hunt, K.K.; Wargo, J.A.; et al. Analysis of the immune infiltrate in undifferentiated pleomorphic sarcoma of the extremity and trunk in response to radiotherapy: Rationale for combination neoadjuvant immune checkpoint inhibition and radiotherapy. OncoImmunology 2018, 7, e1385689. [Google Scholar] [CrossRef] [PubMed]
- Ahlawat, S.; M. Fayad, L. Revisiting the WHO classification system of bone tumours: emphasis on advanced magnetic resonance imaging sequences. Part 2. Polish Journal of Radiology 2020, 85, 409–419. [CrossRef] [PubMed]
- Zhou, M.; Bui, N.; Bolleddu, S.; Lohman, M.; Becker, H.-C.; Ganjoo, K. Nivolumab plus ipilimumab for soft tissue sarcoma: a single institution retrospective review. Immunotherapy 2020, 12, 1303–1312. [Google Scholar] [CrossRef] [PubMed]
- Delyon, J.; Biard, L.; Renaud, M.; Resche-Rigon, M.; Le Goff, J.; Dalle, S.; Heidelberger, V.; Da Meda, L.; Toullec, L.; Carcelain, G.; et al. PD-1 blockade with pembrolizumab in classic or endemic Kaposi’s sarcoma: a multicentre, single-arm, phase 2 study. Lancet Oncol. 2022, 23, 491–500. [Google Scholar] [CrossRef]
- Zer, A.I.O.; Yosef, L.; Avram, D.; Jacobi, O.; Fenig, E.; Kurman, N.; Peretz, I.; Shamai, S.; Merimsky, O.; Ben-Ami, E.; et al. Phase II single-arm study of nivolumab and ipilimumab (Nivo/Ipi) in previously treated classical Kaposi sarcoma (cKS). Ann. Oncol. 2022, 33, 720–727. [Google Scholar] [CrossRef] [PubMed]
- Somaiah, N.; Conley, A.P.; Parra, E.R.; Lin, H.; Amini, B.; Solis Soto, L.; Salazar, R.; Barreto, C.; Chen, H.; Gite, S.; et al. Durvalumab plus tremelimumab in advanced or metastatic soft tissue and bone sarcomas: a single-centre phase 2 trial. Lancet Oncol. 2022, 23, 1156–1166. [Google Scholar] [CrossRef]
- Schöffski, P.; Bahleda, R.; Wagner, A.J.; Burgess, M.A.; Junker, N.; Chisamore, M.; Peterson, P.; Szpurka, A.M.; Ceccarelli, M.; Tap, W.D. Results of an Open-label, Phase Ia/b Study of Pembrolizumab plus Olaratumab in Patients with Unresectable, Locally Advanced, or Metastatic Soft-Tissue Sarcoma. Clinical Cancer Research 2023, OF1–OF9. [Google Scholar] [CrossRef] [PubMed]
- Paoluzzi, L.; Cacavio, A.; Ghesani, M.; Karambelkar, A.; Rapkiewicz, A.; Weber, J.; Rosen, G. Response to anti-PD1 therapy with nivolumab in metastatic sarcomas. Clin. Sarcoma Res. 2016, 6, 24. [Google Scholar] [CrossRef]
- Martin-Broto, J.; Hindi, N.; Grignani, G.; Martinez-Trufero, J.; Redondo, A.; Valverde, C.; Stacchiotti, S.; Lopez-Pousa, A.; D’Ambrosio, L.; Gutierrez, A.; et al. Nivolumab and sunitinib combination in advanced soft tissue sarcomas: a multicenter, single-arm, phase Ib/II trial. J. Immunother. Cancer 2020, 8. [Google Scholar] [CrossRef] [PubMed]
- Cousin, S.; Bellera, C.; Guegan, J.P.; Valentin, T.; Bahleda, R.; Metges, J.P.; Cassier, P.A.; Cantarel, C.; Spalato Ceruso, M.; Kind, M.; et al. 1494P Regomune - a phase II study of regorafenib + avelumab in solid tumors: Results of the soft tissue sarcoma (STS) cohort. Ann. Oncol. 2022, 33, S1230. [Google Scholar] [CrossRef]
- Grilley-Olson, J.E.; Allred, J.B.; Schuetze, S.; Davis, E.J.; Wagner, M.J.; Poklepovic, A.S.; Waechter, B.; Riedel, R.F.; Welliver, M.X.; Berg, S.A.; et al. A multicenter phase II study of cabozantinib + nivolumab for patients (pts) with advanced angiosarcoma (AS) previously treated with a taxane (Alliance A091902). J. Clin. Oncol. 2023, 41, 11503–11503. [Google Scholar] [CrossRef]
- Eulo, V.; Toeniskoetter, J.; Ruff, T.; Luo, J.; Kemp, L.; Tellez, C.M.; Weiss, M.C.; Hirbe, A.C.; Meyer, C.F.; Elias, A.D.; et al. Randomized phase II trial of cabozantinib combined with PD-1 and CTLA-4 inhibition versus cabozantinib in metastatic soft tissue sarcoma. Journal of Clinical Oncology 2023, 41, LBA11504–LBA11504. [Google Scholar] [CrossRef]
- Nathenson, M.; Choy, E.; Carr, N.D.; Hibbard, H.D.; Mazzola, E.; Catalano, P.J.; Thornton, K.A.; Morgan, J.A.; Cote, G.M.; Merriam, P.; et al. Phase II study of eribulin and pembrolizumab in patients (pts) with metastatic soft tissue sarcomas (STS): Report of LMS cohort. J. Clin. Oncol. 2020, 38, 11559–11559. [Google Scholar] [CrossRef]
- Smrke, A.; Ostler, A.; Napolitano, A.; Vergnano, M.; Asare, B.; Fotiadis, N.; Thway, K.; Zaidi, S.; Miah, A.B.; Van Der Graaf, W.; et al. 1526MO GEMMK: A phase I study of gemcitabine (gem) and pembrolizumab (pem) in patients (pts) with leiomyosarcoma (LMS) and undifferentiated pleomorphic sarcoma UPS). Ann. Oncol. 2021, 32, S1114. [Google Scholar] [CrossRef]
- Wagner, M.J.; Zhang, Y.; Cranmer, L.D.; Loggers, E.T.; Black, G.; McDonnell, S.; Maxwell, S.; Johnson, R.; Moore, R.; Hermida de Viveiros, P.; et al. A Phase 1/2 Trial Combining Avelumab and Trabectedin for Advanced Liposarcoma and Leiomyosarcoma. Clin. Cancer Res. 2022, 28, 2306–2312. [Google Scholar] [CrossRef]
- Toulmonde, M.; Brahmi, M.; Giraud, A.; Chakiba, C.; Bessede, A.; Kind, M.; Toulza, E.; Pulido, M.; Albert, S.; Guégan, J.-P.; et al. Trabectedin plus Durvalumab in Patients with Advanced Pretreated Soft Tissue Sarcoma and Ovarian Carcinoma (TRAMUNE): An Open-Label, Multicenter Phase Ib Study. Clin. Cancer Res. 2022, 28, 1765–1772. [Google Scholar] [CrossRef] [PubMed]
- Adnan, N.; Sekhon, S.; Chawla, S.P.; Kim, T.T.; Chua-Alcala, V.S.; Fernando, M.; Ahari, A.; Feske, W.; Quon, D.V.; Gordon, E.M. GALLANT: A phase 2 study using metronomic gemcitabine, doxorubicin, nivolumab, and docetaxel as second/third-line therapy for advanced sarcoma (NCT04535713). Journal of Clinical Oncology 2022, 40, 11518–11518. [Google Scholar] [CrossRef]
- Beveridge, R.D.; Moura, D.; Ramos, R.; Martinez-Trufero, J.; Carrasco-Garcia, I.; Lopez-Pousa, A.; -Billalabeitia, E.G.; Gutierrez, A.; Jurado, J.C.; Sebio, A.; et al. ImmunoSarc2: A Spanish Sarcoma Group (GEIS) phase Ib trial of doxorubicin and dacarbazine plus nivolumab in first line treatment of advanced leiomyosarcoma. J. Clin. Oncol. 2023, 41, 11502–11502. [Google Scholar] [CrossRef]
- Gordon, E.M.; Chawla, S.P.; Tellez, W.A.; Younesi, E.; Thomas, S.; Chua-Alcala, V.S.; Chomoyan, H.; Valencia, C.; Brigham, D.A.; Moradkhani, A.; et al. SAINT: A Phase I/Expanded Phase II Study Using Safe Amounts of Ipilimumab, Nivolumab and Trabectedin as First-Line Treatment of Advanced Soft Tissue Sarcoma. Cancers (Basel) 2023, 15. [Google Scholar] [CrossRef] [PubMed]
- Chandran, S.S.; Somerville, R.P.T.; Yang, J.C.; Sherry, R.M.; Klebanoff, C.A.; Goff, S.L.; Wunderlich, J.R.; Danforth, D.N.; Zlott, D.; Paria, B.C.; et al. Treatment of metastatic uveal melanoma with adoptive transfer of tumour-infiltrating lymphocytes: a single-centre, two-stage, single-arm, phase 2 study. Lancet Oncol. 2017, 18, 792–802. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Deng, J.; Rao, S.; Guo, S.; Shen, J.; Du, F.; Wu, X.; Chen, Y.; Li, M.; Chen, M.; et al. Tumor Infiltrating Lymphocyte (TIL) Therapy for Solid Tumor Treatment: Progressions and Challenges. Cancers (Basel) 2022, 14. [Google Scholar] [CrossRef] [PubMed]
- Balch, C.M.; Riley, L.B.; Bae, Y.J.; Salmeron, M.A.; Platsoucas, C.D.; von Eschenbach, A.; Itoh, K. Patterns of human tumor-infiltrating lymphocytes in 120 human cancers. Arch. Surg. 1990, 125, 200–205. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, S.A.; Yang, J.C.; Sherry, R.M.; Kammula, U.S.; Hughes, M.S.; Phan, G.Q.; Citrin, D.E.; Restifo, N.P.; Robbins, P.F.; Wunderlich, J.R.; et al. Durable complete responses in heavily pretreated patients with metastatic melanoma using T-cell transfer immunotherapy. Clin. Cancer Res. 2011, 17, 4550–4557. [Google Scholar] [CrossRef] [PubMed]
- Mullinax, J.E.; Hall, M.; Beatty, M.; Weber, A.M.; Sannasardo, Z.; Svrdlin, T.; Hensel, J.; Bui, M.; Richards, A.; Gonzalez, R.J.; et al. Expanded Tumor-infiltrating Lymphocytes From Soft Tissue Sarcoma Have Tumor-specific Function. J. Immunother. 2021, 44, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Wu, J.; Duan, C.; Liu, Y. Retrospective Analysis of Adoptive TIL Therapy plus Anti-PD1 Therapy in Patients with Chemotherapy-Resistant Metastatic Osteosarcoma. J. Immunol. Res. 2020, 2020, 7890985. [Google Scholar] [CrossRef]
- Thanindratarn, P.; Dean, D.C.; Nelson, S.D.; Hornicek, F.J.; Duan, Z. Chimeric antigen receptor T (CAR-T) cell immunotherapy for sarcomas: From mechanisms to potential clinical applications. Cancer Treat. Rev. 2020, 82, 101934. [Google Scholar] [CrossRef] [PubMed]
- Richards, R.M.; Sotillo, E.; Majzner, R.G. CAR T Cell Therapy for Neuroblastoma. Front. Immunol. 2018, 9, 2380. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, N.; Brawley, V.S.; Hegde, M.; Robertson, C.; Ghazi, A.; Gerken, C.; Liu, E.; Dakhova, O.; Ashoori, A.; Corder, A.; et al. Human Epidermal Growth Factor Receptor 2 (HER2) –Specific Chimeric Antigen Receptor–Modified T Cells for the Immunotherapy of HER2-Positive Sarcoma. J. Clin. Oncol. 2015, 33, 1688–1696. [Google Scholar] [CrossRef] [PubMed]
- Hegde, M.; DeRenzo, C.C.; Zhang, H.; Mata, M.; Gerken, C.; Shree, A.; Yi, Z.; Brawley, V.; Dakhova, O.; Wu, M.-F.; et al. Expansion of HER2-CAR T cells after lymphodepletion and clinical responses in patients with advanced sarcoma. J. Clin. Oncol. 2017, 35, 10508–10508. [Google Scholar] [CrossRef]
- Tsimberidou, A.M.; Van Morris, K.; Vo, H.H.; Eck, S.; Lin, Y.F.; Rivas, J.M.; Andersson, B.S. T-cell receptor-based therapy: an innovative therapeutic approach for solid tumors. J. Hematol. Oncol. 2021, 14, 102. [Google Scholar] [CrossRef] [PubMed]
- Akers, S.N.; Odunsi, K.; Karpf, A.R. Regulation of cancer germline antigen gene expression: implications for cancer immunotherapy. Future Oncol. 2010, 6, 717–732. [Google Scholar] [CrossRef] [PubMed]
- Kakimoto, T.; Matsumine, A.; Kageyama, S.; Asanuma, K.; Matsubara, T.; Nakamura, T.; Iino, T.; Ikeda, H.; Shiku, H.; Sudo, A. Immunohistochemical expression and clinicopathological assessment of the cancer testis antigens NY-ESO-1 and MAGE-A4 in high-grade soft-tissue sarcoma. Oncol. Lett. 2019, 17, 3937–3943. [Google Scholar] [CrossRef] [PubMed]
- Iura, K.; Kohashi, K.; Ishii, T.; Maekawa, A.; Bekki, H.; Otsuka, H.; Yamada, Y.; Yamamoto, H.; Matsumoto, Y.; Iwamoto, Y.; et al. MAGEA4 expression in bone and soft tissue tumors: its utility as a target for immunotherapy and diagnostic marker combined with NY-ESO-1. Virchows Arch. 2017, 471, 383–392. [Google Scholar] [CrossRef] [PubMed]
- Ramachandran, I.; Lowther, D.E.; Dryer-Minnerly, R.; Wang, R.; Fayngerts, S.; Nunez, D.; Betts, G.; Bath, N.; Tipping, A.J.; Melchiori, L.; et al. Systemic and local immunity following adoptive transfer of NY-ESO-1 SPEAR T cells in synovial sarcoma. J. Immunother. Cancer 2019, 7, 276. [Google Scholar] [CrossRef] [PubMed]
- Robbins, P.F.; Kassim, S.H.; Tran, T.L.; Crystal, J.S.; Morgan, R.A.; Feldman, S.A.; Yang, J.C.; Dudley, M.E.; Wunderlich, J.R.; Sherry, R.M.; et al. A pilot trial using lymphocytes genetically engineered with an NY-ESO-1-reactive T-cell receptor: long-term follow-up and correlates with response. Clin. Cancer Res. 2015, 21, 1019–1027. [Google Scholar] [CrossRef] [PubMed]
- D’Angelo, S.P.; Tine, B.A.V.; Attia, S.; Blay, J.-Y.; Strauss, S.J.; Morales, C.M.V.; Razak, A.R.A.; Winkle, E.V.; Trivedi, T.; Biswas, S.; et al. SPEARHEAD-1: A phase 2 trial of afamitresgene autoleucel (Formerly ADP-A2M4) in patients with advanced synovial sarcoma or myxoid/round cell liposarcoma. J. Clin. Oncol. 2021, 39, 11504–11504. [Google Scholar] [CrossRef]
- Harrington, K.; Freeman, D.J.; Kelly, B.; Harper, J.; Soria, J.C. Optimizing oncolytic virotherapy in cancer treatment. Nat. Rev. Drug Discov. 2019, 18, 689–706. [Google Scholar] [CrossRef] [PubMed]
- Bai, Y.; Hui, P.; Du, X.; Su, X. Updates to the antitumor mechanism of oncolytic virus. Thorac. Cancer 2019, 10, 1031–1035. [Google Scholar] [CrossRef]
- Turnbull, S.; West, E.J.; Scott, K.J.; Appleton, E.; Melcher, A.; Ralph, C. Evid. Oncolytic Virotherapy: Where Have We Got Where Are We Going? Viruses 2015, 7, 6291–6312. [Google Scholar] [CrossRef] [PubMed]
- Le Boeuf, F.; Selman, M.; Son, H.H.; Bergeron, A.; Chen, A.; Tsang, J.; Butterwick, D.; Arulanandam, R.; Forbes, N.E.; Tzelepis, F.; et al. Oncolytic Maraba Virus MG1 as a Treatment for Sarcoma. Int. J. Cancer 2017, 141, 1257–1264. [Google Scholar] [CrossRef]
- Monga, V.; Miller, B.J.; Tanas, M.; Boukhar, S.; Allen, B.; Anderson, C.; Stephens, L.; Hartwig, S.; Varga, S.; Houtman, J.; et al. Intratumoral talimogene laherparepvec injection with concurrent preoperative radiation in patients with locally advanced soft-tissue sarcoma of the trunk and extremities: phase IB/II trial. J. Immunother. Cancer 2021, 9. [Google Scholar] [CrossRef]
- Kelly, C.M.; Antonescu, C.R.; Bowler, T.; Munhoz, R.; Chi, P.; Dickson, M.A.; Gounder, M.M.; Keohan, M.L.; Movva, S.; Dholakia, R.; et al. Objective Response Rate Among Patients With Locally Advanced or Metastatic Sarcoma Treated With Talimogene Laherparepvec in Combination With Pembrolizumab: A Phase 2 Clinical Trial. JAMA Oncol. 2020, 6, 402–408. [Google Scholar] [CrossRef] [PubMed]
- Carvajal, R.D.; Agulnik, M.; Ryan, C.W.; Milhem, M.M.; George, S.; Jones, R.L.; Chmielowski, B.; Tine, B.A.V.; Tawbi, H.A.-H.; Elias, A.D.; et al. Trivalent ganglioside vaccine and immunologic adjuvant versus adjuvant alone in metastatic sarcoma patients rendered disease-free by surgery: A randomized phase 2 trial. J. Clin. Oncol. 2014, 32, 10520–10520. [Google Scholar] [CrossRef]
- Kawaguchi, S.; Tsukahara, T.; Ida, K.; Kimura, S.; Murase, M.; Kano, M.; Emori, M.; Nagoya, S.; Kaya, M.; Torigoe, T.; et al. SYT-SSX breakpoint peptide vaccines in patients with synovial sarcoma: a study from the Japanese Musculoskeletal Oncology Group. Cancer Sci. 2012, 103, 1625–1630. [Google Scholar] [CrossRef] [PubMed]
- Chawla, S.P.; Van Tine, B.A.; Pollack, S.M.; Ganjoo, K.N.; Elias, A.D.; Riedel, R.F.; Attia, S.; Choy, E.; Okuno, S.H.; Agulnik, M.; et al. Phase II Randomized Study of CMB305 and Atezolizumab Compared With Atezolizumab Alone in Soft-Tissue Sarcomas Expressing NY-ESO-1. J. Clin. Oncol. 2022, 40, 1291–1300. [Google Scholar] [CrossRef]
- Yu, R.K.; Tsai, Y.T.; Ariga, T.; Yanagisawa, M. Structures, biosynthesis, and functions of gangliosides--an overview. J. Oleo Sci. 2011, 60, 537–544. [Google Scholar] [CrossRef] [PubMed]
- Berois, N.; Osinaga, E. Glycobiology of neuroblastoma: impact on tumor behavior, prognosis, and therapeutic strategies. Front. Oncol. 2014, 4, 114. [Google Scholar] [CrossRef] [PubMed]
- Lopez, P.H.; Schnaar, R.L. Gangliosides in cell recognition and membrane protein regulation. Curr. Opin. Struct. Biol. 2009, 19, 549–557. [Google Scholar] [CrossRef]
- Battula, V.L.; Shi, Y.; Evans, K.W.; Wang, R.Y.; Spaeth, E.L.; Jacamo, R.O.; Guerra, R.; Sahin, A.A.; Marini, F.C.; Hortobagyi, G.; et al. Ganglioside GD2 identifies breast cancer stem cells and promotes tumorigenesis. J. Clin. Invest. 2012, 122, 2066–2078. [Google Scholar] [CrossRef] [PubMed]
- Krengel, U.; Bousquet, P.A. Molecular recognition of gangliosides and their potential for cancer immunotherapies. Front. Immunol. 2014, 5, 325. [Google Scholar] [CrossRef]
- Brodeur, G.M. Neuroblastoma: biological insights into a clinical enigma. Nat. Rev. Cancer 2003, 3, 203–216. [Google Scholar] [CrossRef]
- Cavdarli, S.; Groux-Degroote, S.; Delannoy, P. Gangliosides: The Double-Edge Sword of Neuro-Ectodermal Derived Tumors. Biomolecules 2019, 9. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, S.; Fukumoto, S.; Kawaguchi, H.; Sato, S.; Ueda, R.; Furukawa, K. Ganglioside G(D2) in small cell lung cancer cell lines: enhancement of cell proliferation and mediation of apoptosis. Cancer Res. 2001, 61, 4244–4252. [Google Scholar] [PubMed]
- Valentino, L.; Moss, T.; Olson, E.; Wang, H.J.; Elashoff, R.; Ladisch, S. Shed tumor gangliosides and progression of human neuroblastoma. Blood 1990, 75, 1564–1567. [Google Scholar] [CrossRef]
- Yeh, S.D.; Larson, S.M.; Burch, L.; Kushner, B.H.; Laquaglia, M.; Finn, R.; Cheung, N.K. Radioimmunodetection of neuroblastoma with iodine-131-3F8: correlation with biopsy, iodine-131-metaiodobenzylguanidine and standard diagnostic modalities. J. Nucl. Med. 1991, 32, 769–776. [Google Scholar]
- Bailey, K.; Cost, C.; Davis, I.; Glade-Bender, J.; Grohar, P.; Houghton, P.; Isakoff, M.; Stewart, E.; Laack, N.; Yustein, J. Emerging novel agents for patients with advanced Ewing sarcoma: a report from the Children’s Oncology Group (COG) New Agents for Ewing Sarcoma Task Force. F1000Res 2019, 8. [Google Scholar] [CrossRef]
- Kailayangiri, S.; Altvater, B.; Meltzer, J.; Pscherer, S.; Luecke, A.; Dierkes, C.; Titze, U.; Leuchte, K.; Landmeier, S.; Hotfilder, M.; et al. The ganglioside antigen G(D2) is surface-expressed in Ewing sarcoma and allows for MHC-independent immune targeting. Br. J. Cancer 2012, 106, 1123–1133. [Google Scholar] [CrossRef] [PubMed]
- Roth, M.; Linkowski, M.; Tarim, J.; Piperdi, S.; Sowers, R.; Geller, D.; Gill, J.; Gorlick, R. Ganglioside GD2 as a therapeutic target for antibody-mediated therapy in patients with osteosarcoma. Cancer 2014, 120, 548–554. [Google Scholar] [CrossRef]
- Zhu, W.; Mao, X.; Wang, W.; Chen, Y.; Li, D.; Li, H.; Dou, P. Anti-ganglioside GD2 monoclonal antibody synergizes with cisplatin to induce endoplasmic reticulum-associated apoptosis in osteosarcoma cells. Pharmazie 2018, 73, 80–86. [Google Scholar] [CrossRef]
- Chang, H.R.; Cordon-Cardo, C.; Houghton, A.N.; Cheung, N.K.; Brennan, M.F. Expression of disialogangliosides GD2 and GD3 on human soft tissue sarcomas. Cancer 1992, 70, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Saraf, A.J.; Dickman, P.S.; Hingorani, P. Disialoganglioside GD2 Expression in Pediatric Rhabdomyosarcoma: A Case Series and Review of the Literature. J. Pediatr. Hematol. Oncol. 2019, 41, 118–120. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.Y.; Ye, Z.H.; Huang, M.Y.; Lu, J.J. Regulation of CD47 expression in cancer cells. Transl. Oncol. 2020, 13, 100862. [Google Scholar] [CrossRef] [PubMed]
- Ozaniak, A.; Smetanova, J.; Bartolini, R.; Rataj, M.; Capkova, L.; Hacek, J.; Fialova, M.; Krupickova, L.; Striz, I.; Lischke, R.; et al. A novel anti-CD47-targeted blockade promotes immune activation in human soft tissue sarcoma but does not potentiate anti-PD-1 blockade. J. Cancer Res. Clin. Oncol. 2023, 149, 3789–3801. [Google Scholar] [CrossRef] [PubMed]
- Theruvath, J.; Menard, M.; Smith, B.A.H.; Linde, M.H.; Coles, G.L.; Dalton, G.N.; Wu, W.; Kiru, L.; Delaidelli, A.; Sotillo, E.; et al. Anti-GD2 synergizes with CD47 blockade to mediate tumor eradication. Nat. Med. 2022, 28, 333–344. [Google Scholar] [CrossRef] [PubMed]
- Hingorani, P.; Krailo, M.; Buxton, A.; Hutson, P.; Sondel, P.M.; Diccianni, M.; Yu, A.; Morris, C.D.; Womer, R.B.; Crompton, B.; et al. Phase 2 study of anti-disialoganglioside antibody, dinutuximab, in combination with GM-CSF in patients with recurrent osteosarcoma: A report from the Children’s Oncology Group. Eur. J. Cancer 2022, 172, 264–275. [Google Scholar] [CrossRef] [PubMed]
Figure 2.
CAR T-cell structure.
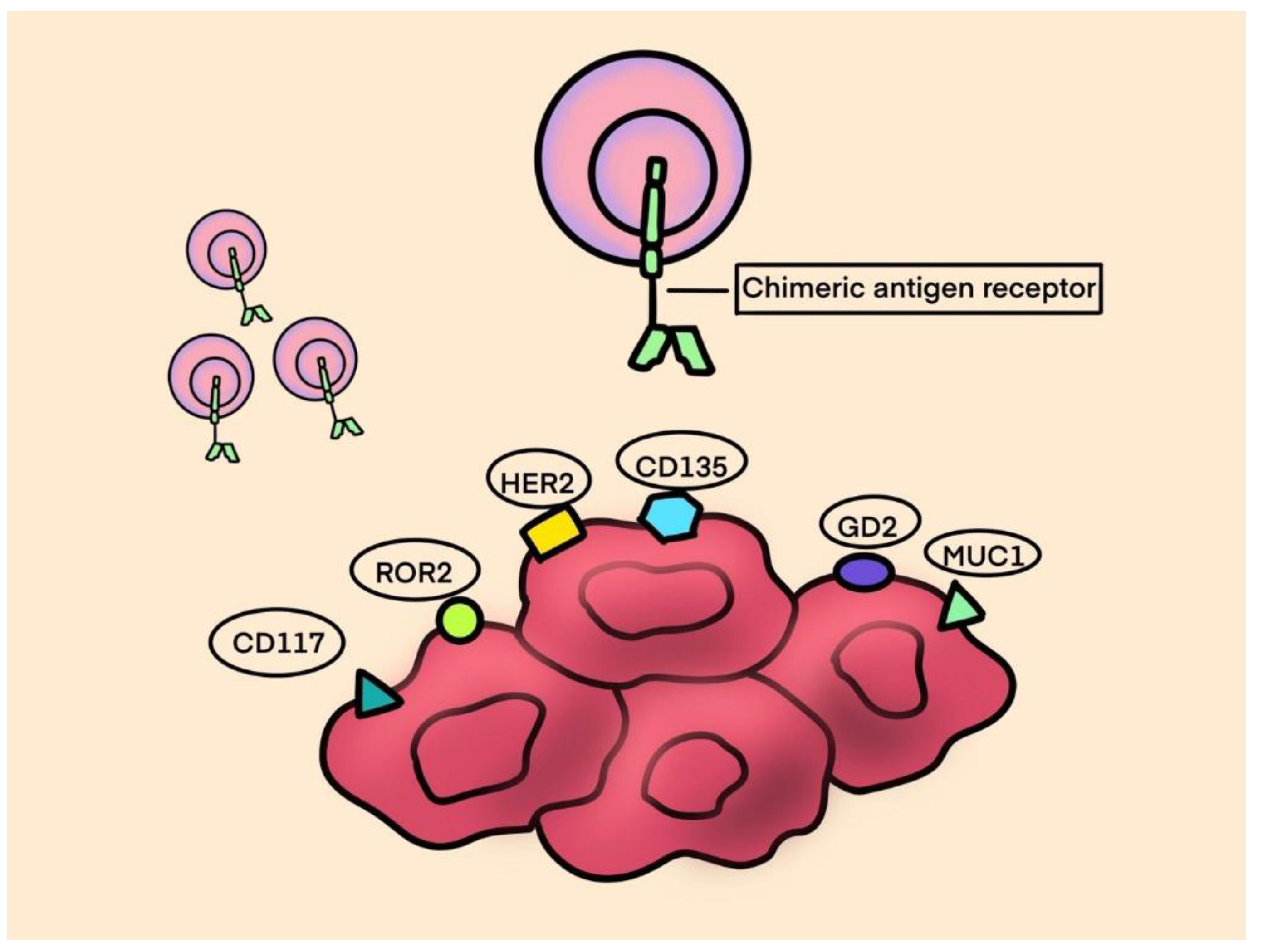
Figure 3.
TCR.
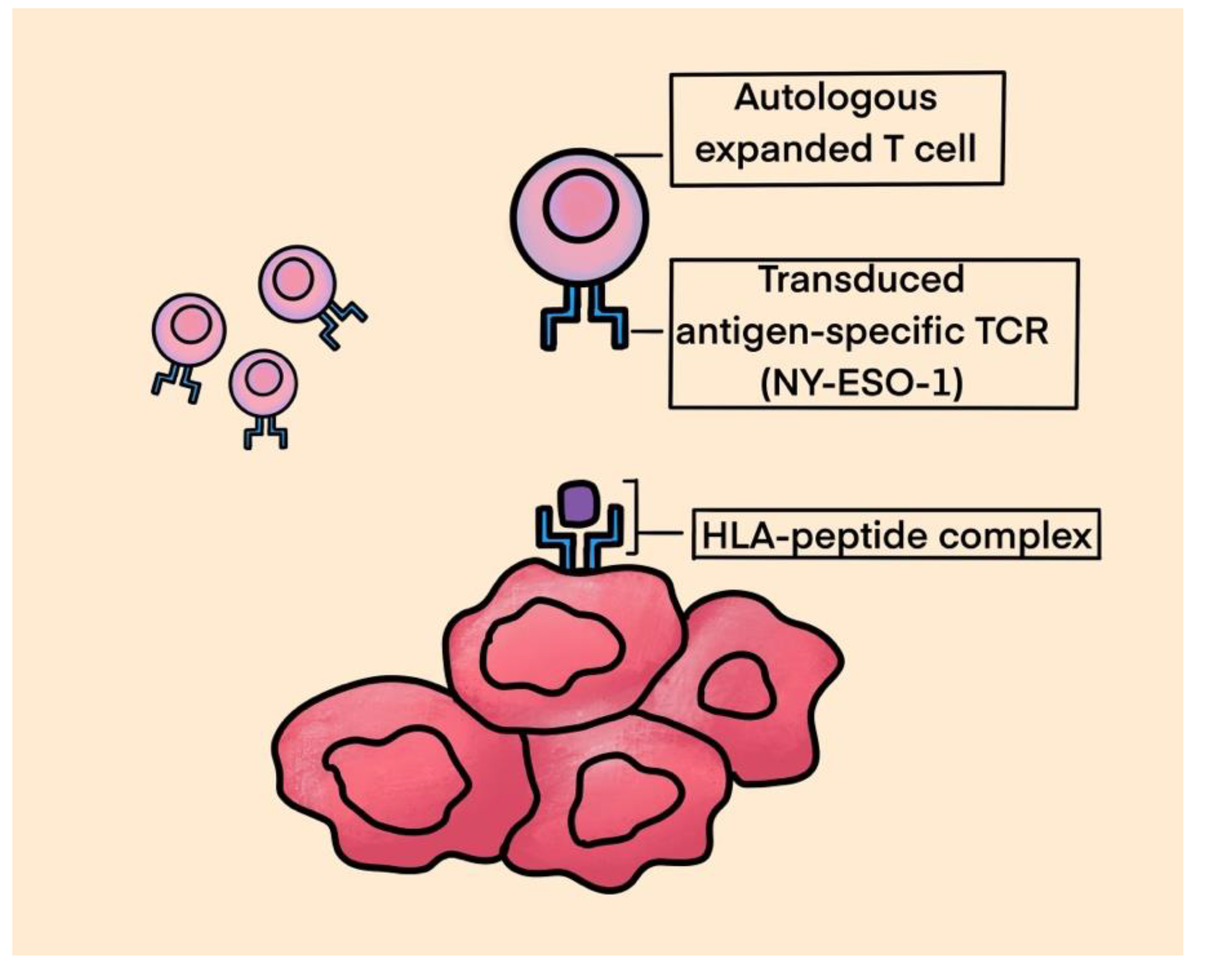
Table 1.
WHO Classification of Soft Tissue Sarcomas [61].
Table 1.
WHO Classification of Soft Tissue Sarcomas [61].
| Adipocytic tumors | Atypical lipomatous tumor Well-differentiated liposarcoma Liposarcoma, NOS Dedifferentiated liposarcoma Myxoid/round cell liposarcoma Pleomorphic liposarcoma |
|---|---|
| Fibroblastic/myofibroblastic tumors | Dermatofibrosarcoma protuberans Fibrosarcomatous dermatofibrosarcoma protuberans Pigmented dermatofibrosarcoma protuberans Solitary fibrous tumor, malignant Inflammatory myofibroblastic tumor Low-grade myofibroblastic tumor Fibrosarcoma Myxofibrosarcoma Low-grade fibromyxoid sarcoma Sclerosing epithelioid fibrosarcoma |
| So-called Fibrohistiocytic tumors | Giant cell tumor of soft parts NOS Malignant tenosynovial giant cell tumour |
| Smooth muscle tumors | Leiomyosarcoma |
| Pericytic (perivascular) tumors | Malignant glomus tumor |
| Skeletal muscle tumors |
Embryonal rhabdomyosarcoma Alveolar rhabdomyosarcoma Pleomorphic rhabdomyosarcoma Spindle cell/sclerosing rhabdomyosarcoma |
| Vascular tumors |
Retiform hemangioendothelioma Papillary intralymphatic angioendothelioma Composite hemangioendothelioma Pseudomyogenic hemangioendothelioma Kaposi sarcoma Epithelioid hemangioendothelioma Angiosarcoma of soft tissue |
| Chondro-osseous tumors |
Soft tissue chondroma Extraskeletal osteosarcoma |
| Gastrointestinal stromal tumors | Gastrointestinal stromal tumor, malignant |
| Nerve sheath tumors |
Malignant peripheral nerve sheath tumors Melanotic malignant nerve sheath tumor Granular cell tumor, malignant Perineurioma, malignant |
| Tumors of uncertain differentiation | Ossifying fibromyxoid tumor, malignant Stromal sarcoma, NOS Myoepithelial carcinoma Phosphaturic mesenchymal tumor, malignant Synovial sarcoma NOS Synovial sarcoma, spindle cell Synovial sarcoma, biphasic Epithelioid sarcoma Alveolar soft part sarcoma Clear cell sarcoma Extraskeletal myxoid chondosarcoma Extraskeletal Ewing sarcoma Desmoplastic small round cell tumor Perivascular epithelioid tumour, malignant (PEComa) Intimal sarcoma |
| Undifferentiated/unclassified sarcoma | Undifferentiated spindle cell sarcoma Undifferentiated pleomorphic sarcoma Undifferentiated round cell sarcoma Undifferentiated epithelioid sarcoma Undifferentiated sarcoma, NOS |
Table 2.
WHO Classification of Bone Sarcoma [61].
Table 2.
WHO Classification of Bone Sarcoma [61].
| Chondrogenic tumors | Chondrosarcoma Dedifferentiated chondrosarcoma Mesenchymal chondrosarcoma Clear cell chondrosarcoma |
|---|---|
| Osteogenic tumors | Osteoblastoma Osteosarcoma Conventional osteosarcoma: chondroblastic, fibroblastic, osteoblastic Periosteal osteosarcoma |
| Osteoclastic giant cell rich tumors | Giant cell tumor of bone, malignant |
| Fibrohistiocytic tumors | Undifferentiated high grade pleomorphic sarcoma of bone (previously Malignant fibrous histiocytoma) |
| Notochordal tumors | Chordoma Dedifferentiated chordoma |
| Vascular tumors |
Epithelioid hemangioendothelioma Angiosarcoma |
| Undifferentiated small round cell sarcoma of bone and soft tissue |
Ewing sarcoma Round cell sarcoma with EWSR1 non-ETS fusion Sarcoma with BCOR genetic alterations |
| Fibrogenic tumors | Fibrosarcoma |
Table 3.
Results of Selected Trials of Immunotherapy in Sarcoma.
| Clinical Trial/Design |
Phase | Agent/Intervention | Indication/Prior lines of treatment | Evaluated patients (n) and Tumor Subtypes | ORR (%) | PFS (weeks (w) or months (m)) | OS (w or m) | Outcomes in subtypes/Notes |
|---|---|---|---|---|---|---|---|---|
| ICI monotherapy or combination | ||||||||
|
Maki et al. 2013 [33] |
Phase II | ipilimumab | Locally recurrent or metastatic SS, at least 1 prior line treatment | 6 SS |
0% |
1.85 m |
8.75 m | |
|
Tawbi et al. (SARC028) 2017 [32] |
Phase II | pembrolizumab | Advanced/metastatic STS or bone sarcoma, at least 1 prior line treatment | 40 BS cohort (22 OS, 13 ES, 5 CS) | - | 8 w |
52 w | 1 PR in CS and 1 PR in OST |
| 40 STS cohort (10 LMS, 10 LPS, 10 SS, 10 UPS) |
- | 18 w |
49 w | 1 CR and 3 PR In UPS< 2 PR In LPS, 1 PR in SS | ||||
|
Ben-Ami et al. 2017 [34] |
Phase II | nivolumab | Advanced or metastatic uterine LMS, at least 1 prior line of treatment | 12 LMS | 0% |
1.8 m |
- | |
|
D’ Angelo et al. Alliance A091401 2018 [40] |
Phase II | nivolumab/ipilimumab vs nivolumab |
Advanced or metastatic BS and STS, at least 1 prior line of treatment | Nivolumab/ipilimumab– 42 (3 AS, 4 BS, 14 LMS, 2 LPS, 6 SCS, 2 SS, 6 UPS/MFH, 1 unspecified sarcoma, 4 others) |
16% |
4.1 m |
10.7 m | Response in uterine LMS, non-uterine LMS, MFS, UPS/MFH, AS |
| Nivolumab– 43 (5 BS, 15 LMS, 3 LPS, 2 unspecified sarcoma, 5 SCS, 2 SS, 5 UPS, 6 others |
5% |
1.7 m | 10.7 m | 1 PR in ASPS and 1 PR in non-uterine LMS | ||||
|
Uboha et al. 2019 [41] |
Phase II | spartalizumab + LAG525 (anti-LAG3) | Advanced solid tumors and hematologic malignancies | 10 | CBR 40% | - | - | Sarcoma cohort did not meet the expansion criterion |
|
Zhou et al. 2020 [62] |
Retrospective | nivolumab + ipilimumab | Advanced or metastatic STS, 87% received at least 1 prior line | 38 (9 LMS, 8 Sarcoma NOS, 6 LPS, 5 MFS, 3 MPNST, 2 SFT, 1 Breast AS, 1 FDFP, 1 RMS, 1 SS) |
15% |
2.7m |
12 m |
CR in 1 MFS 1 PR in each MPNST, SFT, MFS, DDLS, and sarcoma NOS |
|
Naqash et al. 2021 [42] |
Phase II | pembrolizumab | Advanced or metastatic ASPS | 43 | 37.2% |
- | - | |
|
Blay et al. French AcSé 2021 [36] |
Phase II | pembrolizumab | Advanced rare sarcoma | 98 (34 chordoma, 14 ASPS, 11 SMRT, 8 DSCRT, 31 other histotypes) |
15.3 | 2.75 m |
19.7 m |
Highest ORR In chordoma, ASPS, SMRT, DSCRT |
|
Delyon et al. 2022 [63] |
Phase II | pembrolizumab | Classic/endemic Kaposi sarcoma with extensive cutaneous extension, 71% had at least 1 prior line | 17 (8 classic KS and 9 endemic KS) |
71% |
- | - | |
|
Zer et al. 2022 [64] |
Phase II | ipilimumab and nivolumab | Classic Kaposi sarcoma, at least 1 prior line of treatment | 11 | 45% |
not reached |
- | |
|
Somaiah et al. 2022 [65] |
Phase II | durvalumab + tremelimumab. | Advanced or metastatic sarcoma (BS and STS), 91% had at least 1 prior line | 57 (3 DDLPS, 2WDLPS, 1 PLS, 5 AS, 5 LMS, 5 UPS, 5 SS, 1 CDOS, 4 COS, 10 ASPS, 5 chordomas, 11 other sarcomas) | 12% |
2.8 m | 21.6 m | ASPS ORR 40% |
| ICI combination with TKI | ||||||||
|
Schoffski et al. 2016 [66] |
Ia/Ib | pembrolizumab + olaratumab (monoclonal antibody against platelet derived growth factor receptor alpha) | Advanced or metastatic STS, 92% had at least 1 prior line | 28 | 21.4% | 2.7 m | 14.8 m | |
|
Paoluzzie et al. 2016 [67] |
Retrospective study | durvalumab + pazopanib | Metastatic STS and BS, median 2 prior lines of treatment | 28 (24 STS, 4 BS with 24 evaluable patients) | 10% | - | - | 3 PR (1 DDCS with nivolimab alone), 1 EpS, 1 MOS) |
|
Wilky et al. 2019 [48] |
Phase II | pembrolizumab + axitinib | Advanced or metastatic STS, 81% with at least 1 prior line of treatment | 33 (12 ASPS, 6 LMS (4 uterine), 5 High grade PS, 2 DDLPS, 8 other histotypes) | 25% |
4.7 m | 18.7 m | ASPS ORR 50%, |
|
Xie et al. APFAO trial 2020 [49] |
Phase II | camrelizumab + apatinib | Advanced or metastatic OS, at least 1 prior line of treatment | 43 (OS including osteoblastic, chondroblastic, fibroblastic and small cell) | 20.1% | 6.2 m |
11.3 m | |
|
Palmerini et al. IMMUNOSARC 2020 [46] |
Phase II | nivolumab + sunitinib | Advanced BS cohort, at least 1 prior line of treatment | 40 (17 OS, 14 CS, 8 ES, 1 bone UPS, 4 DDCS) | 5% | 3.7 m | 14.2 m | 1 CR in DDCS and 1 PR in OS |
|
Martin-Broto et al. IMMUNOSARC 2020 [68] |
Phase I/II | nivolumab + sunitinib | Metastatic STS, at least 1 prior line of treatment | 52 (9 SS, 8 UPS, 7 clear cell sarcoma, 7 SFT, 7 EpS, 5 AS, 4 ESMCS, 4 ASPS, 1 EHET) | 21% | 5.6 m |
- | 1 CR in AS, 2 PR in ASPS, 1 PR in ESMCS and 1PR in SS |
|
Kim et al. 2021 [50] |
Phase II | durvalumab + pazopanib | Advanced or metastatic STS, at least 1 prior line of treatment | 46 |
28.3% | 7.7 m | - | Objective responses in ASPS, AS, UPS, DSRCT |
|
Cousin et al. REGOMUNE 2022 [69] |
Phase II | avelumab + regorafenib | Advanced or metastatic STS, at least 1 prior line of treatment | 43 (22 LMS, 9 SS, 4 LPS, 4 UPS, 10 other subtypes) | 9.3% | 1.8 m | 15.1 m | |
|
Allred et al. Alliance A091902 trial 2023 [70] |
Phase II | nivolumab with carbozantinib | Advanced AS, previously treated | 18 (AS including 12 cutaneous, 1 liver, 2 breast, 6 others) | 72% | 9.6 m |
20.5 m | |
|
Eulo et al. 2023 [71] |
Phase II | nivolumab/ipilimumab + cabozantinib N/I + C |
Metastatic STS that lacks translocation, at least 1 prior line of treatment | 69 (N/I + C arm) |
11% | 5.4 m | - | |
| 36 (C only arm) |
6% | 3.8 m | - | |||||
| ICI combination with chemotherapy | ||||||||
|
Toulmonde et al. 2018 [53] |
Phase II | pembrolizumab + metronomic cyclophosphamide | Advanced or metastatic STS, 97% with at least 1 prior line of treatment | 50 (15 LMS, 16 UPS, 16 other sarcomas, 10 GIST) |
2% | 1.4 m | - | |
|
Italiano et al. Amended PEMBROSARC 2022 [25] |
Phase II | pembrolizumab with metronomic cyclophosphamide | TLS-positive advanced STS, 63% had at least 1 prior line of treatment | 35 (12 WDLPS/DDLPS, 4 LMS, 6 UPS, 3 EpS, 10 other histotypes) | 30% |
6m PFS 40% |
- | PR: 5 in DDLPS, 3 EpS, 1 LMS SD: 6 DDLPS, 1 FMS, 1 MFS, 1 uterine LMS, 1 UPS |
|
Nathenson et al. 2020 [72] |
Phase II | pembrolizumab + eribulin | Metastatic STS, at least 1 prior line of treatment | 19 LMS (11 uterine LMS) | 5.3% |
11.1 w |
- | |
|
Smrke et al. 2021 [73] |
Phase I | pembrolizumab + gemcitabine | Advanced or metastatic LMS, UPS | 13 (2 UPS, 11 LMS) | - | 5.1 m | - | LMS - DCR 73% (8 SD, 3 PD) UPS - DCR 100% (2 PR) |
|
Wagner et al. 2022 [74] |
Phase I/II | avelumab + trabectedin | Advanced or metastatic LPS and LMS, 86% had at least 1 prior line of treatment | 35, only 23 evaluable (24 with LMS, 11 with LPS |
13% | 8.3 m |
27 m | LMS 4 PR, 9 SD LPS 7 SD |
|
Toulmonde et al. 2022 [75] |
Phase Ib | durvalumab + trabectedin | Advanced or metastatic STS cohort, at least 1 prior line of treatment | 16 (6 LMS, 2 DDLPS, 8 others) |
7% |
12m PFS 14.3% |
- | |
|
Adnan et al. Gallant trial 2022 [76] |
Phase II | nivolumab + metronomic gemcitabine, doxorubicin, and docetaxel | Advanced or metastatic STS, at least 1 prior line of treatment |
39 (15 LMS, 4 PS, 4 SS, 3 LPS, 3 OS, 10 others) | 20.5% |
4.6 m | 6.2 m | mPFS 2 m historically in previously treated patients |
|
Andreou et al. NITRA-SARC 2023 [57] |
Phase II | nivolumab + trabectedin | Advanced or metastatic STS, at least 1 prior line of treatment | Group A – 43 (28 LMS and 15 LPS) | - | 5.5 m | 18.7 m | |
| Group B – 49 (12 UPS, 11 SCS, 6 FMS, 5 SS, 4 EpS) | - | 2.3 m | 5.6 m | |||||
|
Beveridge et al. ImmunoSarc2 Cohort 7b 2023 [77] |
Phase Ib | doxorubicin and dacarbazine plus nivolumab and nivolumab maintenance 1 year | Advanced or metastatic LMS, anthracycline naïve patients | 16 LMS | 56% | 8.67 m | - | |
| ICI as front line | ||||||||
|
Pollack et al. 2020 [54] |
Phase I/II | pembrolizumab + doxorubicin | Anthracycline naïve sarcoma Excluding ES, ARMS, ERMS, 76% with no prior line of treatment |
37 (11 LMS, 4 DDLPS, 3 CCCS, 3 UPS, 2 SFT, 2 ESS, 2 EHET, 8 other histotypes | 19% | 8.1 m |
27.6 m |
|
|
Livingston et al. 2021 [55] |
Phase II | pembrolizumab + doxorubicin | Anthracycline Naïve advanced STS, 86.7% had no prior treatment | 28 (7 LPS, 10 LMS, 1 SS, 4 UPS, 2 AS, 6 other histotypes) |
36.7% | 5.7 m | 17 m | The most clinical benefit in UPS, EpAS, LMS, LPS |
|
Maleddu et al. 2023 [58] |
Phase II | doxorubicin + anti-CTLA-4 zalifrelimab and anti-PD1 balstilimab | Advanced or metastatic STS, no prior doxorubicin or ICI | 28 | 36% |
25.6 m | - | Responses seen in IS, AS, MPNST, LPS, LMS, ESS, UPS, and SEpF. |
|
Gordon et al. SAINT Trial 2023 [78] |
Phase I/II | ipilimumab + nivolumab and trabectedin | Advanced or metastatic STS, treatment naive | 101 (14 LPS, 26 LMS, 9 UPS, 7 RMS, 5 SS, 4 clear CS, 4 PS, 4 MFS, 3 PNST, 3 MLS, 2 carcinosarcoma, 2 DSRCT, 2 sarcoma NOS) | 25.3% | 6.7 m | 24.6 m |
|
|
Chen et al. 2021 [38] |
Retrospective | nivolumab + ipilimumab vs nivolumab | Metastatic STS (100% PD-L1 positive tumors – PD-L1 expression >1%), treatment naive |
74 - Nivolumab and ipilimumab arm -(43 non-uterine LMS, 20 LPS, 11 SS) | - | 4.1 m | 12.2 m |
|
| 76 - Nivolumab arm (40 non-uterine LMS, 22 LPS, 14 SS) | - | 2.2 m | 9.2 m |
|||||
Alveolar rhabdomyosarcoma – ARMS; Alveolar soft part sarcoma – ASPS; Angiosarcoma – AS; Desmoplastic small round cell tumor - DSRCT; Dedifferentiated chondrosarcoma – DDCS; Epithelioid sarcoma – EpS; Extraskeletal myxoid chondrosarcoma – ESMCS; Breast angiosarcoma – breast AS; Chondrosarcoma – CS; Chondroblastic osteosarcoma – CDOS; Clear cell chondrosarcoma – CCCS; Clear cell sarcoma – Clear CS; Conventional osteosarcoma – COS; Dedifferentiated liposarcoma – DDLPS; Embryonal rhabdomyosarcoma – ERMS; Epithelioid Angiosarcoma – EpAS; Endothelial stromal sarcoma – ESS; Epithelioid hemangioendothelioma – EHET; Epithelioid sarcoma – EpS; Fibromyxoid sarcoma – FMS; Fibrosarcomatous dermatofibrosarcoma protuberans – FDFP; Gastrointestinal stromal tumor – GIST; High grade pleomorphic sarcoma – High grade PS; Intimal sarcoma – IS; Pleomorphic liposarcoma – PLS; Pleomorphic sarcoma – PS; Malignant fibrous histiocytoma – MFH; Malignant peripheral nerve sheath tumor – MPNST; Maxillary osteosarcoma – MOS; Myxofibrosarcoma – MFS; Leiomyosarcoma – LMS; Liposarcoma – LPS; Osteosarcoma – OS; Rhabdomyosarcoma – RMS; Sclerosing epithelioid fibrosarcoma – SEpF; Spindle cell sarcoma – SCS; Smarca4 deficient malignant rhabdoid tumor – SMRT; Solitary fibrous tumor – SFT; Synovial sarcoma – SS; Undifferentiated pleomorphic sarcoma – UPS; Well-differentiated liposarcoma – WDLPS. ORR – objective response rate; OS – overall survival; PFS –progression free survival.
Table 5.
Ongoing Trials for TCR therapy in Sarcoma.
| Clinical trial | Phase | Intervention | Disease |
|---|---|---|---|
| NCT03462316 | Phase I | Anti-NY-ESO-1 (TCR Affinity Enhancing Specific T cell Therapy) | Advanced bone and soft tissue sarcoma that failed first line |
| NCT05296564 | Phase I | Anti-HBI 0201-ESO TCRT (anti-NY-ESO-1 TCR-Gene Engineered Lymphocytes) | NY-ESO-1 -Expressing Metastatic cancers (synovial sarcoma, STS, etc) that failed first line or second line, recurrence of disease, progression of disease |
| NCT03132922 | Phase I | Genetically Engineered Anti-MAGE-A4 | MAGE-A4 Positive Tumors (synovial sarcoma, myxoid round cell liposarcoma) failed first line of therapy |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



