
Submitted:
27 November 2023
Posted:
29 November 2023
You are already at the latest version
Abstract
Prediabetes, a pivotal phase in glucose metabolism between normalcy and diabetes, exerts a profound influence on the aging process and the risk of age-related diseases. This comprehensive review delves into the intricate web of blood-based biomarkers that collectively expedite senescence, marking the transition from a state of health to age-related complications. Key findings underscore the significance of diverse biomarkers, such as telomere length, p16INK4a, senescence-associated secretory phenotype (SASP) factors, DNA methylation clocks, advanced glycation end products (AGEs), inflammatory and oxidative stress markers, circulating hormones, and additional factors like folate, B12, osteocalcin, and more. Not only do these biomarkers serve as indicators of senescence, but they actively fuel chronic inflammation, oxidative stress, and metabolic dysregulation, all of which contribute to accelerated aging. The implications of this understanding are profound, as prediabetes emerges as a critical period in an individual's life, influencing various physiological systems, including the vascular and neural systems, metabolic functions, hormonal regulation, and bone health. Recognizing the profound influence of prediabetes on senescence provides a foundation for personalized intervention strategies to mitigate age-related complications and promote healthy aging. Future research directions call for a more diverse array of biomarkers, in-depth exploration of their roles, and the development of tailored precision medicine strategies to ensure a holistic understanding and effective management of prediabetes-induced senescence and its implications for aging. This knowledge has far-reaching implications for public health and clinical practice, emphasizing the need for early detection and intervention in prediabetic individuals to enhance the quality of life in an aging population with diverse needs.
Keywords:
prediabetes
; senescence
; blood-based biomarkers
; aging
; age-related diseases
; inflammation
; oxidative stress
; vascular dynamics
; metabolic disorders
; chronic inflammation
1. Introduction
The global prevalence of prediabetes, a metabolic state characterized by insulin resistance, elevated blood glucose levels that are below the threshold for diabetes diagnosis, has emerged as a significant public health concern [1]. Prediabetes is a critical precursor to type 2 diabetes (T2D), however often remains undiagnosed while individuals with prediabetes are at a heightened risk of transitioning to T2D [2]. It is also associated with a range of adverse health outcomes and age-related complications, including cardiovascular diseases, neurodegenerative disorders, and frailty [3]. Given the growing aging population worldwide, a comprehensive understanding of how prediabetes impacts senescence is of great significance.
The relationship between aging and chronic illnesses like diabetes has drawn significant attention in the field of public health as the world's population ages [4]. Between normoglycemia and overt diabetes, prediabetes which is defined by increased blood glucose levels is a critical stage in the continuum of glucose dysregulation[5]. It is critical to comprehend the many mechanisms by which prediabetes affects the aging process. The realization that prediabetes contributes to an accelerated aging phenotype in addition to predisposing people to diabetes is the driving force behind this extensive research [6]. The evaluation of blood-based biomarkers, which act as markers of underlying physiological and molecular processes connecting prediabetes and senescence, is a crucial component of this study [7].
Assessing blood-based biomarkers within the framework of prediabetes-induced senescence provides a comprehensive viewpoint on the complex interplay between metabolic dysregulation and aging [8]. This is especially important because aging-related diseases and prediabetes share many pathophysiological pathways [9]. This review is important because it could give researchers and physicians the resources they need to identify people who are at risk of developing prediabetes as well as premature aging. By facilitating early intervention and preventive steps to lessen age-related issues, it provides a proactive approach to healthcare [10]. Furthermore, figuring out the biomarkers linked to senescence brought on by prediabetes is crucial for deciphering the molecular causes of aging and presents chances for focused interventions that can lessen the negative effects of prediabetes on older persons' health [11].
In addition to adding to our understanding of the aging process, the scientific investigation of blood-based biomarkers in prediabetes-induced senescence holds enormous promise for enhancing the health and well-being of prediabetic persons [12]. We can find new treatment targets and preventive measures by dissecting the relationships between particular biomarkers and accelerated aging [13]. With a deeper understanding of the relationship between metabolic health and senescence and, ultimately, guidance for the development of interventions to promote healthy aging and lessen the burden of age-related diseases among prediabetic individuals, these insights could have far-reaching implications for the fields of gerontology and diabetes care [14].
This comprehensive review aims to investigate the relationship between prediabetes and age-related changes, with a specific focus on blood-based biomarkers. It will delve into the impact of prediabetes on telomere length, p16INK4a expression, senescence-associated secretory phenotype (SASP) factors, DNA methylation clocks, advanced glycation end products (AGEs), inflammatory markers, and oxidative stress markers. It will further explore the influence of prediabetes on circulating hormones, growth factors, and metabolic markers. It aims to provide a thorough exploration of these various blood-based biomarkers that are associated with both prediabetes and senescence by synthesizing existing knowledge on these biomarkers. Understanding this connection is of paramount importance in the context of contemporary healthcare, as it holds the potential to shed light on the mechanisms underlying accelerated biological aging in prediabetic individuals and provide valuable insights into the pathogenesis of age-related chronic diseases. This analysis will contribute to our understanding of the complex relationship between prediabetes and the aging process, ultimately facilitating the development of targeted interventions and strategies for mitigating the adverse effects of prediabetes-induced senescence.
2. Age-Related Changes in Plasma Biochemistry and Vascular Dynamics in Prediabetes
2.1. Prediabetes as a Precursor to Age-Related Vascular Changes
A key prelude to age-related vascular alterations is prediabetes, which is defined by high blood glucose levels that do not fulfil the criteria for diabetes [15]. The circulatory system, which includes the arteries and veins, undergoes structural and functional changes as a result of the complex and diverse process of vascular aging [16]. It is essential for the emergence of hypertension and associated problems, as well as age-related cardiovascular illnesses [17]. Prediabetes can dramatically accelerate vascular aging, increasing the risk of cardiovascular morbidity and mortality in those who have it. Prediabetes affects about one in three persons in many countries [18].
Oxidative stress is one of the main ways that prediabetes affects the aging of the blood vessels [19]. Increased oxidative stress, which is defined as an imbalance between reactive oxygen species (ROS) and antioxidant defences, is common in people with prediabetes [19]. This oxidative load may eventually contribute to vascular aging by causing oxidative damage to the walls of blood vessels (See Figure 1) [20]. Chronic rise of blood glucose and variations in insulin resistance in prediabetes intensify oxidative stress and foster an environment that is favourable for oxidative alteration of lipids and proteins in the vascular system [21]. This accelerates these vascular alterations and raises the risk of age-related cardiovascular problems such endothelial dysfunction and atherosclerosis[21].
Furthermore, prediabetes is closely associated with chronic low-grade inflammation, often referred to as “meta-inflammation” [22]. Vascular aging is primarily caused by inflammatory processes, which prediabetes exacerbates [19]. Prediabetes' pro-inflammatory condition can encourage immune cells within the vascular wall to become activated, triggering an inflammatory response that hastens the aging process of the vessels [23]. As a result, blood vessel stiffening, atherosclerotic plaque development, and decreased vascular reactivity occur[23]. The significance of prediabetes as a prelude to vascular alterations associated with aging is noteworthy, emphasizing the need to comprehend these mechanisms and ascertain pertinent blood-based indicators to oversee and address this metabolic disorder [24]. This review explores the role of such biomarkers in tracking the progression of vascular aging in prediabetes and their potential for mitigating the adverse outcomes associated with this accelerated aging process.
2.2. Altered Plasma Biochemistry and Its Implications for Senescence
The biochemical makeup of blood is significantly impacted by prediabetes, which creates the conditions for accelerated senescence [25]. A vital factor in determining general health, plasma biochemistry affects a number of physiological functions [26]. Blood plasma composition is altered in prediabetic individuals due to dysregulated glucose and lipid metabolism in the systemic environment [27]. Elevated levels of circulating inflammatory markers, such as C-reactive protein (CRP) and interleukin-6 (IL-6), are one of the major biochemical alterations linked to prediabetes [28]. Pro-inflammatory signals play a role in the persistent low-grade inflammation that is frequently observed in prediabetes, a condition that is sometimes called "inflammaging" [29]. Since inflammation is a major factor in senescence, a persistently inflammatory environment speeds up the aging of many organ systems [30].
Figure 1.
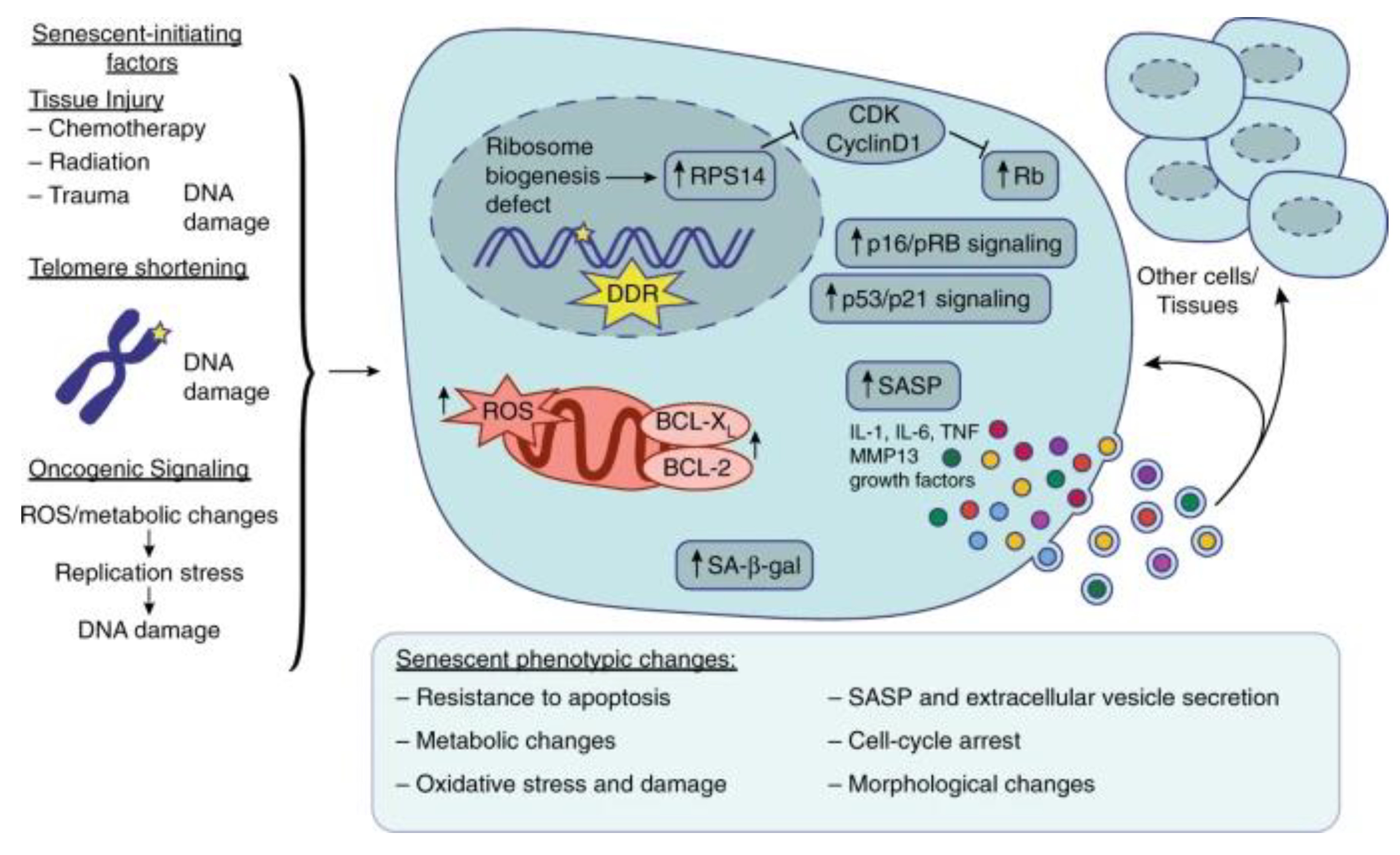
Overview of Prediabetes induced vascular senescence as adapted from source and redrawn from Bio Render: Several factors can induce senescence in different tissues, such as tissue injury, telomere shortening, and oncogenic signalling that all lead to DNA damage, the DNA damage response (DDR), and consequent cell cycle arrest by activation of p16/pRB signalling and/or p53/p21 signalling. Nucleolar stress and ribosome biogenesis defects can also induce RPS14 accumulation in the nucleus and activates Rb by inhibiting the CDK4/cyclin D1 complex, leading to cell cycle arrest. Senescent cells also exhibit increased senescence-associated β-galactosidase (SA-β-gal) production, reactive oxygen species (ROS) accumulation, and anti-apoptotic factors such as BCL-XL and BCL-2. Senescent cells exhibit several phenotypic changes such as a resistance to apoptosis, oxidative stress and damage, metabolic changes, morphological changes, cell cycle arrest, and extracellular vesicle secretion containing SASP factors such as IL-1, IL-6, TNF, MMP13, and various growth factors. This SASP can either feedback in an autocrine manner to the senescent cell or in a paracrine manner influence and promote senescence and inflammation in the surrounding cells and tissues [31].
Figure 1.
Overview of Prediabetes induced vascular senescence as adapted from source and redrawn from Bio Render: Several factors can induce senescence in different tissues, such as tissue injury, telomere shortening, and oncogenic signalling that all lead to DNA damage, the DNA damage response (DDR), and consequent cell cycle arrest by activation of p16/pRB signalling and/or p53/p21 signalling. Nucleolar stress and ribosome biogenesis defects can also induce RPS14 accumulation in the nucleus and activates Rb by inhibiting the CDK4/cyclin D1 complex, leading to cell cycle arrest. Senescent cells also exhibit increased senescence-associated β-galactosidase (SA-β-gal) production, reactive oxygen species (ROS) accumulation, and anti-apoptotic factors such as BCL-XL and BCL-2. Senescent cells exhibit several phenotypic changes such as a resistance to apoptosis, oxidative stress and damage, metabolic changes, morphological changes, cell cycle arrest, and extracellular vesicle secretion containing SASP factors such as IL-1, IL-6, TNF, MMP13, and various growth factors. This SASP can either feedback in an autocrine manner to the senescent cell or in a paracrine manner influence and promote senescence and inflammation in the surrounding cells and tissues [31].
Moreover, abnormal lipid profiles, such as elevated triglyceride and decreased high-density lipoprotein (HDL) cholesterol levels, are linked to prediabetes [32]. Due to its pro-atherogenic nature, dyslipidaemia encourages the build-up of cholesterol in blood vessel walls and the onset of atherosclerosis, a disease generally associated with advanced age [33]. Atherosclerosis raises the risk of cardiovascular events like heart attacks and strokes by limiting blood flow and encouraging the formation of blood clots [34]. The combined effect of these changed parameters related to plasma biochemistry speeds up the aging process of organ and vascular systems [7].
Prediabetes causes hyperglycaemia by upsetting glucose homeostasis and going beyond inflammation and dyslipidaemia [35]. The glycation of proteins, including those essential for vascular health, is promoted by elevated blood glucose levels [36]. This process results in the formation of advanced glycation end products (AGEs), which promote oxidative stress and the stiffening of arterial walls [37]. AGEs have broad implications for age-related complications like renal dysfunction and neurodegenerative diseases, in addition to their association with vascular senescence [38]. Examining the interaction between these biochemical alterations and the aging process in prediabetes is essential because the altered plasma biochemistry in prediabetes is a critical link in the chain of events that accelerates senescence [9].
2.3. Role of Biomarkers in Plasma Biochemistry Changes
As a metabolic state that lies between normoglycemia and diabetes, prediabetes is characterized by a complex interplay of biochemical factors, many of which are important biomarkers for changes in plasma biochemistry [39]. These biomarkers are essential for comprehending the pathophysiological changes linked to prediabetes and how they affect senescence [40]. A number of important biomarkers emerge in the context of changes in plasma biochemistry, providing insight into the biochemical dysregulations that underlie accelerated aging and age-related vascular dynamics [41].
2.3.1. Telomere Length: Genomic stability depends on telomeres, the protective caps that sit at the ends of chromosomes [42]. Since telomere shortening is a sign of cellular aging and senescence, their length is a crucial factor in determining cellular lifespan [43]. Telomere shortening occurs at a significantly faster rate in the setting of prediabetes, a disorder characterized by oxidative stress, low-grade inflammation, and chronic metabolic disruptions [44]. Telomeres are significantly impacted by these environmental factors, which are frequently linked to prediabetes, hastening their attrition [45]. Telomere length thus functions as a biomarker reflecting the accelerated aging of cells in prediabetic subjects [44]. This phenomenon has broader implications because, in addition to indicating cellular aging, short telomeres also contribute to the general senescence seen in prediabetic people [44]. Deciphering the complex interplay between prediabetes and accelerated senescence which will illuminate the molecular mechanisms underlying this condition's effects on aging and age-related illnesses requires an understanding of the dynamics of telomere length [44].
2.3.2. p16INK4a: In the context of cellular senescence, p16INK4a functions as a critical regulator. Senescence-related irreversible growth arrest of cells is regulated by this biomarker, which functions as a sentinel [46]. The expression of p16INK4a is generally higher and more prominent in prediabetes than in non-prediabetic people [47]. This upregulation, which is a result of the inflammatory and metabolic environment linked to prediabetes, indicates a higher frequency of senescent cells [48]. The high frequency of p16INK4a in prediabetics highlights the harmful effects of this metabolic disorder on the integrity of cells [49]. A state of cellular stress and dysfunction, indicated by elevated p16INK4a levels, is linked to prediabetic individuals' age-related health conditions as well as the general aging process [50]. Comprehending the function of p16INK4a is crucial for unravelling the connection between prediabetes and cellular senescence, providing insight into the molecular processes that underpin the condition's impact on the aging process [51].
2.3.3. Senescence-Associated Secretory Phenotype (SASP) Factors: The SASP is a broad category of substances secreted by senescent cells, which includes growth factors, chemokines, and pro-inflammatory cytokines [52]. These elements have a significant impact on nearby cells and tissues as well as the microenvironment that senescent cells are in [52]. The production of SASP factor is primarily driven by the chronic low-grade inflammation that is a feature of prediabetes [53]. Consequently, increased blood levels of SASP factors are linked to prediabetes [54]. These biomarkers demonstrate how senescent cells actively promote inflammation and modify plasma biochemistry [55]. The elevated SASP factor levels in prediabetes serve as indicators of the role of senescence in the systemic changes in plasma biochemistry and the overall inflammatory milieu [56]. The senescence process in prediabetes and its consequences for age-related health conditions are further complicated by the interaction between senescence and inflammation, which is reflected by SASP factors [57]. Comprehending the functions of SASP factors in modifications to plasma biochemistry is essential for clarifying the ways in which prediabetes hastens senescence and influences aging [58].
2.3.4. DNA Methylation Clocks: Epigenetic modifications, specifically DNA methylation, are essential for controlling gene expression and are crucial in the aging process [59]. DNA methylation clocks have become useful biomarkers for determining the rate of aging because they quantify the epigenetic age of cells or tissues [60]. These epigenetic clocks frequently show an accelerated aging pattern in the context of prediabetes [60]. This acceleration is explained by the disruption of DNA methylation patterns caused by the metabolic and oxidative stress linked to prediabetes [61]. As a result, prediabetic people have changes in their epigenetic landscape that correspond to an older biological age [60]. These biomarkers provide important clues about the epigenetic modifications that accelerate senescence in prediabetes and shed light on the underlying mechanisms and consequences for age-related disorders [62]. Comprehending the functions of DNA methylation clocks is crucial in clarifying the ways in which prediabetes affects the epigenetic control of aging and its wider consequences on health conditions associated with aging.
2.3.5. Advanced Glycation End Products (AGEs): Advanced Glycation End Products, commonly known as AGEs, serve as critical biomarkers in the context of prediabetes-induced senescence [63]. Prediabetes is often associated with elevated levels of AGEs, which stem from the persistent hyperglycaemia and oxidative stress characteristic of the condition [19]. AGEs are formed through a non-enzymatic reaction between sugars and proteins, and their accumulation is indicative of glycation and oxidative damage [64]. In prediabetes, the heightened levels of AGEs underscore the accelerated aging of tissues and systems, with profound implications for age-related complications [65]. These biomarkers reflect the complex biochemical changes that drive senescence and contribute to age-related alterations in vascular dynamics and other physiological processes [66]. Comprehending the functions of DNA methylation clocks is crucial in clarifying the ways in which prediabetes affects the epigenetic control of aging and its wider consequences on health conditions associated with aging [67].
3. Circulating Hormones and Growth Factors Associated with Aging in Prediabetes
3.1. Hormonal Shifts in Prediabetes and Their Influence on Senescence
A complex interplay of hormonal changes, with significant implications for the senescence process, characterizes prediabetes [25]. An interruption in the insulin-like growth factor (IGF) axis is one of the primary hormonal changes linked to prediabetes [68]. Changes in the levels and bioavailability of insulin-like growth factor 1 (IGF-1), a hormone essential for tissue repair, cell growth, and differentiation, are frequently observed in prediabetic individuals [69]. Insulin resistance, a defining feature of prediabetes, can hinder IGF-1 signalling, exacerbating systemic metabolic abnormalities [70]. This disturbance of the IGF axis causes accelerated aging of cells and is associated with the senescence of different tissues, which affects the tissues' ability to regenerate and their overall physiological function [71]. Furthermore, prediabetics have different hormonal profiles for other growth factors, like brain-derived neurotrophic factor (BDNF), which is important for neuronal health and cognitive function [72]. Particularly in older adults, altered BDNF levels in prediabetes can have an impact on cognitive health [73]. The complex relationships between hormonal changes in prediabetes and their effects on aging are highlighted by the disruptions in BDNF signalling, which can cause cognitive decline and exacerbate the senescence process [74].
Moreover, changes in the hormone’s leptin and adiponectin, which are secreted by adipose tissue, are part of the hormonal landscape of prediabetes [75]. Lower levels of adiponectin, a hormone that has anti-inflammatory and insulin-sensitizing qualities, are frequently seen in prediabetic people [76]. Aging-related metabolic alterations and insulin resistance can be made worse by decreased adiponectin levels [77]. On the other hand, because of modifications in adipose tissue, prediabetes is also associated with changes in leptin, a hormone involved in appetite regulation and energy expenditure [21]. These changes in hormones can affect body weight, metabolism, and general health, which can further accelerate the aging process [78]. In conclusion, deciphering the complex hormonal changes associated with prediabetes and how they affect senescence is essential to understanding the metabolic condition's wider effects on aging and age-related health issues [79].
3.2. Growth Factors and Their Role in Age-Associated Processes
Growth factors play a particularly important role in prediabetes-induced senescence [63]. Growth factors are essential for coordinating a number of physiological processes. Examples of these include vascular endothelial growth factor (VEGF), insulin-like growth factor 1 (IGF-1), and insulin-like growth factor-binding proteins (IGFBPs) [80]. The hormonal milieu in prediabetic individuals frequently involves changes to the IGF-1 and IGFBPs system [81]. These alterations have an effect on tissue healing, cell division, and growth and are intimately related to insulin resistance and metabolic dysregulation [82]. The IGF-1 signalling axis is disrupted, which speeds up senescence and reduces cells' and tissues' ability to regenerate [83]. Moreover, prediabetes is associated with alterations in VEGF levels, a crucial regulator of angiogenesis and vascular homeostasis [84]. Changes in VEGF levels can affect tissue perfusion and vascular dynamics, which can lead to the age-related vascular alterations that are frequently observed in people with prediabetes [85].
Clarifying the intricate interactions between hormonal changes and senescence requires an understanding of the roles played by these growth factors in age-related processes [86]. Changes in growth factors such as bone morphogenetic proteins (BMPs) and brain-derived neurotrophic factor (BDNF) are accompanied by modifications in IGF-1, IGFBPs, and VEGF, which in turn affect different physiological systems [87]. The regulation of cellular growth, tissue repair, angiogenesis, and neuroprotection depend on these growth factors, and their disruption in prediabetes highlights the complex effects of this metabolic disorder on the aging process [88]. Gaining insight into how growth factor dysregulation in prediabetes affects age-related physiological changes and the emergence of age-related health conditions requires an understanding of the complexities of this condition (see Table 1) [89].
3.3. Role of Biomarkers in Hormonal Changes
3.3.1. Circulating Growth Hormone (GH) and Insulin-like Growth Factor 1 (IGF-1): Variations in GH and IGF-1 levels are common in prediabetic individuals due to insulin resistance and metabolic changes, which are characteristics of prediabetes[70]. The insulin resistance seen in prediabetes is closely associated with these hormonal alterations, which are indicative of the endocrine system's influence on the disease and its function in mediating senescence [109].
3.3.2. Dehydroepiandrosterone Sulphate (DHEA-S): A significant decrease in the levels of the steroid hormone DHEA-S, which is generated by the adrenal glands, is frequently observed in people who are prediabetic [110]. This hormonal change plays a crucial role in the context of senescence brought on by prediabetes because it adds to the range of hormonal aging changes [57]. The synthesis of sex hormones, such as oestrogen and testosterone, which are essential for many physiological functions, begins with the production of DHEA-S [111]. The complex relationship between prediabetes and senescence is further highlighted by the drop in DHEA-S levels in prediabetes, which is indicative of a significant hormonal shift that affects the aging process [112].
3.3.3. Testosterone (in men): Changes in testosterone levels are frequently noted in male prediabetic individuals, impacting various aspects of the aging process [98]. These alterations may significantly affect bone density, muscle mass, and other aging-related factors[98]. The essential male sex hormone testosterone is essential for preserving bone health, muscle mass, and general vigour [113]. The hormonal changes associated with prediabetes underscore the impact of the illness on the endocrine system and its part in determining the course of aging in men [112]
3.3.4. Oestrogen (in women): Changes in oestrogen levels in women who are prediabetic can have a substantial effect on different aspects of aging [114]. These hormonal shifts may have an impact on cardiovascular health, bone density, and a number of other aging-related factors [114]. The main female sex hormone, oestrogen, has a significant impact on preserving cardiovascular health, bone health, and general well-being [115]. Changes in oestrogen levels in people with prediabetes highlight the impact of the disease on the endocrine system and how it affects how people age in women [116].
4. Age-Associated Inflammatory Factors in Prediabetes
4.1. Inflammatory Mediators in Prediabetes-Induced Senescence
Age-associated senescence is significantly influenced by chronic low-grade inflammation, which is a metabolic milieu characteristic of prediabetes [117]. A range of inflammatory mediators become prominent in this context. Notably, prediabetic individuals frequently have elevated levels of pro-inflammatory cytokines such as interleukin-6 (IL-6), C-reactive protein (CRP), and others [19]. These mediators of inflammation play a pivotal role as biomarkers reflecting the chronic inflammatory state associated with prediabetes [19]. For example, CRP is a sensitive indicator of systemic inflammation, and IL-6 is essential for controlling inflammation and immune responses [118]. Their increased risk of prediabetes is an essential component of the disease's pathophysiology rather than just a side effect [118]. The existence of these inflammatory mediators indicates how chronic inflammation contributes to senescence and how it speeds up aging in people who are prediabetic [119].
Furthermore, there is a strong correlation between prediabetes and elevated oxidative stress, which amplifies the influence of inflammatory mediators on senescence (see Table 2) [19]. Reactive oxygen species (ROS) and oxidative damage are caused by the pro-inflammatory state associated with prediabetes, which is characterized by the release of factors like tumour necrosis factor-alpha (TNF-α) [120]. The complex interplay between oxidative stress and inflammation in prediabetes-induced senescence is highlighted by these molecular events [121]. Knowing how inflammatory mediators contribute to prediabetes-induced senescence offers important new understandings of the processes that underlie the condition's acceleration of aging and its consequences for age-related medical disorders.
4.2. Chronic Inflammation and Its Implications for Senescence
In prediabetes, chronic inflammation is at the forefront of age-associated senescence and has a significant impact on multiple physiological systems [19]. Senescence is largely promoted by the chronic low-grade inflammation that is a feature of prediabetes [117]. In this context, prediabetic people frequently have elevated levels of various inflammatory mediators, including interleukin-1 beta (IL-1β), interleukin-18 (IL-18), and high-sensitivity C-reactive protein (hs-CRP) [131]. The systemic inflammation that accelerates aging is largely caused by these inflammatory factors [132]. Pro-inflammatory cytokines that can worsen immune responses and inflammatory pathways include IL-1β and IL-18 [133]. The persistent inflammatory state in prediabetes is reflected in hs-CRP, a sensitive marker of systemic inflammation [134]. The increased levels of these mediators indicate the critical role that chronic inflammation plays in the senescence brought on by prediabetes, impacting multiple physiological systems and hastening age-related health issues [135].
Moreover, oxidative stress and the inflammatory milieu in prediabetes are tightly linked, which further complicates the senescence process [136]. Tumour necrosis factor-alpha (TNF-α) and other inflammatory mediators in prediabetes frequently contribute to the production of reactive oxygen species (ROS) and oxidative damage [120]. These molecular interactions increase the level of oxidative stress in prediabetic people, which strengthens the influence of chronic inflammation on aging [19]. The complex processes that underlie the senescence seen in prediabetes are highlighted by the interaction between oxidative stress and inflammation [137]. It also emphasizes the necessity of investigating therapeutic approaches that address oxidative stress and inflammation in order to lessen the effects of prediabetes on age-related health issues and premature aging [138].
4.3. Role of Biomarkers in Inflammatory Factors
4.3.1. Senescence-Associated Secretory Phenotype (SASP) Factors: Higher than normal levels of SASP factors, a set of secreted factors linked to senescent cells, are frequently seen in prediabetic individuals [139]. The chronic inflammation frequently seen in prediabetes is the cause of this rise in SASP factors [140]. SASP factors are important indicators that highlight the proactive function of senescent cells in promoting inflammation and modifying the inflammatory environment in people with prediabetes [141].
4.3.2. Inflammatory Markers: Elevated levels of well-known inflammatory markers, such as interleukin-6 (IL-6) and C-reactive protein (CRP), are frequently used to diagnose prediabetes [142]. These markers are suggestive of the low-grade chronic inflammation that is commonly seen in people who are prediabetic [19]. A sensitive indicator of systemic inflammation, CRP captures the persistent pro-inflammatory milieu linked to prediabetes [143]. In a similar vein, IL-6, an important modulator of inflammation and immune responses, is crucial in mediating the inflammatory processes associated with prediabetes [144]. These inflammatory markers demonstrate the active role that chronic inflammation plays in determining the course of senescence and its role in the accelerated aging seen in prediabetic individuals [25]. The mechanisms underlying senescence in prediabetes and its implications for age-related health conditions are clarified by these markers, which also serve as important indicators of inflammation. (Chronic Inflammation, Prediabetes) [117].
5. Vascular and Neural System Aging in Prediabetes
5.1. Prediabetes-Induced Vascular Changes and Senescence
Prediabetes has a major impact on the vascular system's aging process, starting a series of alterations that greatly accelerate senescence [145]. The accelerated progression of atherosclerosis and endothelial dysfunction are two of the main characteristics of vascular aging in prediabetes [146]. Specifically, endothelial dysfunction is a major factor in aging because it indicates a decline in the endothelium's ability to control vascular tone, preserve homeostasis, and avoid blood clot formation [147]. Chronic hyperglycaemia and inflammation cause endothelial dysfunction in prediabetic people, which speeds up vascular senescence [19]. The existence of these vascular alterations highlights the complex interplay among prediabetes, endothelial dysfunction, and senescence, underscoring the diverse effects of prediabetes on the vascular system's aging process [148].
Moreover, age-related changes in prediabetes can also affect the neural system, which is intricately linked to the vascular system [85]. The illness affects overall neurological health and cognitive function by accelerating neural senescence[85]. A common feature of aging is cognitive decline, which is more likely to occur in people with prediabetes [149]. The vascular alterations associated with prediabetes, such as decreased cerebral blood flow and microvascular dysfunction, contribute to the neurodegenerative processes. Together, these elements cause the aging of neural tissue to occur more quickly [150]. Deciphering the connection between vascular alterations brought on by prediabetes and their consequences for the aging of the neural system is essential to understanding the larger influence of this metabolic disorder on aging and its consequences on neurological and cognitive health [151].

Table 3.
Biomarkers in Prediabetes-Induced Vascular and Neural System Aging.
| Biomarker | Role in Aging | Implications for Senescence | Ref. |
|---|---|---|---|
| Telomere Length | Reflects cellular aging and senescence | Accelerated aging and cellular senescence | [152] |
| p16INK4a | Regulates cellular senescence | Increased cellular senescence | [153] |
| Senescence-Associated Secretory Phenotype (SASP) Factors | Reflect senescent cell secretions | Promote inflammation and senescence | [154] |
| DNA Methylation Clocks | Epigenetic aging indicators | Accelerated epigenetic aging | [155] |
| Advanced Glycation End Products (AGEs) | Reflect glycation and oxidative stress | Contribute to accelerated aging and age-related complications | [156] |
| Inflammatory Markers | Indicators of inflammation | Contribute to inflammation associated with aging | [157] |
| Oxidative Stress Markers | Indicators of oxidative damage and stress | Exacerbate age-related oxidative damage | [156] |
| Endothelial Dysfunction | Indicators of vascular dysfunction | Exacerbate endothelial dysfunction and impact vascular health | [158] |
| Mitochondrial Dysfunction | Reflect mitochondrial function and health | Impair mitochondrial function associated with aging | [159] |
| Red Blood Cell Distribution Width (RDW) | Reflect changes in red blood cells | Indicate inflammation and metabolic changes affecting aging | [160] |
| Haemoglobin A1c (HbA1c) | Reflects long-term blood glucose levels | Accelerate aging due to chronic hyperglycaemia | [161] |
| Serum Albumin | Reflects nutritional status and frailty | Affect nutritional status and frailty | [159] |
| Circulating Growth Hormone (GH) and Insulin-like Growth Factor 1 (IGF-1) | Reflect hormonal changes | Influence insulin resistance and metabolic changes | [162] |
| DHEA-S | Reflects hormonal changes | Contribute to hormonal changes associated with aging | [163] |
| Testosterone (in men) | Reflects hormonal changes in men | Impact muscle mass, bone density, and aging | [63,164] |
| Oestrogen (in women) | Reflects hormonal changes in women | Affect bone density, cardiovascular health, and aging | [165] |
| Brain-Derived Neurotrophic Factor (BDNF) | Reflects changes in neurotrophic factors | Influence cognitive health, particularly in aging | [156] |
| IGF-Binding Proteins | Reflect changes in IGF-1 bioavailability | Contribute to metabolic and aging-related effects | [166] |
| Folate and B12 | Reflect nutritional deficiencies | Impact DNA methylation and repair essential for aging | [167] |
| Osteocalcin | Reflect changes in bone health | Affect bone health, a key consideration in aging | [168] |
| Adiponectin | Reflects changes in metabolic health | Impact insulin resistance and metabolic changes | [167] |
| Leptin | Reflects changes in adipose tissue | Impact metabolism and aging | [155] |
| Homocysteine | Reflects cardiovascular risk | May be more prevalent in prediabetic individuals | [156,169] |
| Insulin Resistance Markers | Reflect insulin resistance | May worsen with age in prediabetic individuals | [170,171] |
5.2. Neural System Aging and Cognitive Implications in Prediabetes
Prediabetes affects not only the aging of the vascular system but also the aging of the neural system, which has important implications for cognition [172]. An inevitable aspect of aging is cognitive decline, which is more likely to occur early in prediabetic people [173]. The vascular changes linked to prediabetes are intimately linked to the neurodegenerative changes that are observed in the condition [174]. Through processes like decreased cerebral blood flow and microvascular dysfunction, chronic hyperglycaemia and inflammation in prediabetes directly affect neural tissue. Together, these elements cause the aging of neural tissue to occur more quickly [175]. Prediabetic people exhibit more severe cognitive deficits, especially in areas linked to memory, executive function, and information processing speed [172]. Gaining an appreciation of the full impact of this metabolic condition on aging and cognitive health requires an understanding of the relationship between prediabetes-induced neural system aging and its cognitive implications [176].
Furthermore, through pathways involving oxidative stress, inflammation, and metabolic alterations, prediabetes can impact neural senescence [137]. Neuroinflammation, a defining feature of neurodegenerative diseases such as Alzheimer's disease, can result from these processes [137]. Neural senescence is exacerbated by pro-inflammatory mediators in the central nervous system that are activated by chronic inflammation and oxidative stress in prediabetes [177]. The complex interactions among these variables highlight the significance of treating cognitive health in people with prediabetes and creating plans to lessen the effects of neural system aging on cognition [178].
5.3. Role of Biomarkers in Vascular and Neural System Aging
5.3.1. Advanced Glycation End Products (AGEs): Advanced glycation end products (AGEs) become an important biomarker in the context of vascular and neural system aging in prediabetes [179]. Elevated levels of AGEs are a common feature of prediabetes, and they have significant implications for the development of age-related complications and the acceleration of aging [85]. A class of molecules known as AGEs is produced when proteins and lipids undergo non-enzymatic glycation and oxidation. An increased production and accumulation of AGEs is a result of prediabetes' chronic hyperglycaemia and oxidative stress [179]. These molecules actively contribute to the vascular and neural system aging seen in prediabetic individuals, in addition to reflecting the biochemical changes that drive senescence [7]. The increased levels of AGEs in prediabetes indicate that this biomarker plays a crucial role in determining the course of aging, emphasizing the significance of addressing AGE-related mechanisms to lessen the effects of prediabetes on the brain and vascular systems [12].
5.3.2 Endothelial Dysfunction: The vascular system ages significantly as a result of prediabetes, and endothelial dysfunction is emerging as a critical biomarker [180]. A common feature of vascular aging is endothelial dysfunction, which is made worse by this condition[180]. Endothelial cells are essential for controlling blood flow and preserving vascular homeostasis [181]. Chronic inflammation and hyperglycaemia aggravate endothelial dysfunction in prediabetic individuals, indicating a crucial phase of vascular senescence [19]. A more noticeable effect on endothelial markers like von Willebrand factor (vWF), a vital mediator of blood clotting and vascular health, is linked to endothelial dysfunction [182]. In order to lessen the effects of aging on prediabetic people, it is important to address endothelial markers, as the existence of endothelial dysfunction in the condition highlights the complex relationship between vascular aging and prediabetes [183].
6. Systemic Inflammaging in Prediabetes
6.1. The Link Between Prediabetes and Systemic Inflammaging
Systemic inflammaging, the long-term low-grade inflammation associated with aging, is markedly worsened in people with prediabetes, resulting in a complex interaction between the metabolic disorder and aging [56]. Prediabetes, via a variety of interrelated mechanisms, plays a major role in the promotion of inflammation [19]. The enduring pro-inflammatory condition associated with prediabetes, which is fuelled by oxidative stress and chronic hyperglycaemia, is crucial to this connection [184]. Systemic inflammation is facilitated by these factors, which also activate pro-inflammatory pathways and release pro-inflammatory cytokines. Interestingly, elevated levels of C-reactive protein (CRP), interleukin-6 (IL-6), and other inflammatory markers are frequently observed in prediabetic individuals, supporting the link between prediabetes and systemic inflammation [185]. These inflammation biomarkers show the complex relationship between prediabetes and the accelerated aging process, which ultimately results in the systemic inflammaging seen in this population. They also serve as indicators of the elevated inflammatory state in prediabetic individuals [186].
Figure 2.
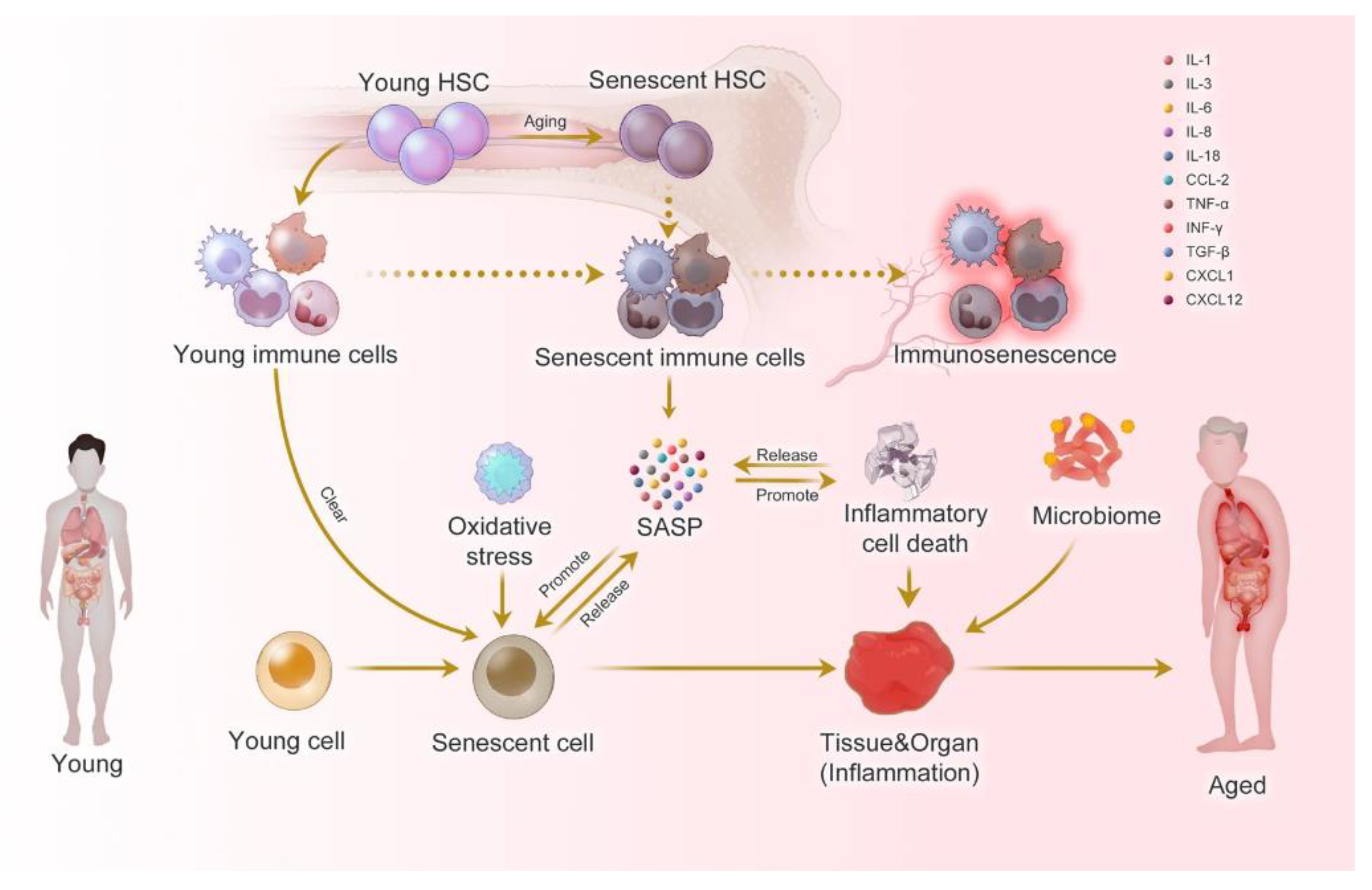
Prediabetes-induced systemic inflammaging (focusing on immunosenescence which is immune system aging) as adapted from source and Biorender: Inflammaging at the molecular, cellular, and organ levels. During the aging process, almost all cells in the body undergo senescence, a state characterized by a dysfunctional state and senescence-associated secretory phenotype (SASP). While immune cells play a crucial role in recognizing and eliminating these senescent cells, they are also affected by SASP, leading to a phenomenon called immunosenescence. Immunosenescence can impair the immunity to respond to infections and diseases, making the organism more vulnerable to illnesses. Moreover, the accumulation of senescent cells can trigger inflammation in organs, leading to organ damage and an increased risk of age-related diseases. This process is exacerbated by positive feedback loops that drive the accumulation of inflammation and organ damage, leading to further inflammation and an even higher risk of aging-related diseases [30].
Figure 2.
Prediabetes-induced systemic inflammaging (focusing on immunosenescence which is immune system aging) as adapted from source and Biorender: Inflammaging at the molecular, cellular, and organ levels. During the aging process, almost all cells in the body undergo senescence, a state characterized by a dysfunctional state and senescence-associated secretory phenotype (SASP). While immune cells play a crucial role in recognizing and eliminating these senescent cells, they are also affected by SASP, leading to a phenomenon called immunosenescence. Immunosenescence can impair the immunity to respond to infections and diseases, making the organism more vulnerable to illnesses. Moreover, the accumulation of senescent cells can trigger inflammation in organs, leading to organ damage and an increased risk of age-related diseases. This process is exacerbated by positive feedback loops that drive the accumulation of inflammation and organ damage, leading to further inflammation and an even higher risk of aging-related diseases [30].
Prediabetes also affects the endocrine system, causing hormonal changes that feed inflammation, which further contributes to systemic inflammaging [78]. For example, prediabetes is frequently associated with altered levels of adipokines, such as adiponectin and leptin, which promote a pro-inflammatory milieu [187]. The body's delicate balance between pro- and anti-inflammatory components is also impacted by this hormonal imbalance, which exacerbates inflammation [188]. The complex interaction of inflammatory markers, hormonal changes, and prediabetes highlights the complexity of systemic inflammation in this metabolic condition [189]. Comprehending the connection between prediabetes and systemic inflammation is crucial in order to appreciate the wider influence of this illness on the aging process and its consequences for health issues associated with aging [120].
6.2. Inflammatory Factors and Their Contribution to Senescence
The aging of different physiological systems is largely caused by the chronic inflammation that is a feature of systemic inflammaging in prediabetes [190]. A number of important inflammatory markers, including interleukin-6 (IL-6) and C-reactive protein (CRP), are frequently elevated in prediabetics [19]. These markers indicate a chronic pro-inflammatory condition that accelerates aging by substantially contributing to senescence[19]. A sensitive measure of systemic inflammation, CRP is a good way to see if prediabetes is still linked to a pro-inflammatory state [28]. Similarly, IL-6 plays a major role in coordinating the inflammatory processes associated with prediabetes. It is a central regulator of immune responses and inflammation [191]. The existence of these inflammatory markers emphasizes how crucial a role they play in encouraging senescence and the faster aging seen in prediabetic people [119].
Moreover, oxidative stress, which increases the effect of inflammatory factors on senescence, is intimately linked to chronic inflammation in prediabetes [119]. Reactive oxygen species (ROS) and oxidative damage are fostered by the pro-inflammatory state associated with prediabetes, which is marked by the release of factors like tumor necrosis factor-alpha (TNF-α) [192]. The complex interplay between oxidative stress and inflammation in prediabetes-induced senescence is highlighted by these molecular events [192]. The coexistence of oxidative stress and chronic inflammation in prediabetes, as well as their combined effect on senescence, provide a thorough understanding of the mechanisms through which the condition speeds up aging and emphasize the significance of treating inflammation in prediabetic individuals to manage age-related health conditions [19].
6.3. Role of Biomarkers in Systemic Inflammaging
6.3.1. Inflammatory Markers (continued): Interleukin-6 (IL-6) and C-reactive protein (CRP) are two inflammatory markers that play a significant role in the context of systemic inflammation in prediabetes [193]. Elevated levels of these inflammatory markers are often associated with prediabetes, indicating a persistent pro-inflammatory state that is commonly seen in the condition [19]. As a sensitive measure of systemic inflammation, CRP is an important window into the persistent pro-inflammatory environment linked to prediabetes [194]. In a similar vein, IL-6, an important modulator of inflammation and immune responses, is crucial in mediating the inflammatory processes associated with prediabetes [19]. These inflammatory markers are important markers of inflammation and play a major role in the chronic inflammation that comes with aging in people with prediabetes [137]. Understanding the mechanisms by which prediabetes accelerates systemic inflammaging and its implications for age-related health conditions depends on the identification of these biomarkers [29]. 6.3.2. Oxidative Stress Markers: The role of elevated oxidative stress in the context of systemic inflammation in prediabetes cannot be understated [195]. Elevated oxidative stress is frequently linked to prediabetes, which can worsen the age-related rise in reactive oxygen species (ROS) and oxidative damage [137]. Oxidative stress is closely associated with the chronic pro-inflammatory state that characterizes prediabetes, which fosters the production of reactive oxygen species (ROS) and subsequent oxidative damage [196]. The intricate relationship between prediabetes, inflammation, and oxidative stress is highlighted by the presence of oxidative stress markers, which further highlights the complex web of factors that contribute to systemic inflammation [197]. Understanding the wider effects of prediabetes on aging and its consequences for age-related health issues, especially in light of systemic inflammation, requires an understanding of the role of oxidative stress markers in this metabolic condition [198].
7. Regeneration and Metabolic Disorders in Prediabetes
7.1. Impaired Regeneration Mechanisms in Prediabetes
The body's ability to regenerate itself is greatly impacted by prediabetes, and this ability is crucial for preserving tissue integrity and fending off the consequences of aging [199]. A number of variables, such as oxidative stress, metabolic dysregulation, and chronic inflammation, are associated with impaired regeneration mechanisms in prediabetes [136]. The body's capacity to initiate and maintain regenerative processes is hampered by chronic inflammation, a defining feature of prediabetes [200]. The inflammatory mediators that are activated during a persistent pro-inflammatory state obstruct the body's regenerative processes, especially when it comes to tissue repair and cellular turnover [201]. Prediabetic individuals may encounter delayed wound healing and compromised tissue regeneration, particularly in tissues with a high cellular turnover rate like the skin and the lining of the gastrointestinal tract. These tissues are most affected by this hindrance to regeneration [202]. Understanding prediabetes' effects on aging and its consequences for age-related health conditions requires an understanding of the interaction between inflammation and regeneration brought on by the condition [200].
The impairment of regeneration mechanisms is further compounded by metabolic dysregulation in prediabetes. A defining feature of prediabetes is insulin resistance, which impairs the body's capacity to use glucose effectively for cellular upkeep and energy production. Since glucose is a necessary fuel for many regenerative mechanisms, such as tissue repair and cell proliferation, this metabolic disruption has a negative impact on the regenerative processes. Cellular energy deficiencies impair the body's capacity to mount a strong regenerative response in prediabetes, which is one of the factors contributing to the impaired regeneration seen in prediabetic patients. Gaining an appreciation of the complete influence of prediabetes on the aging process and its consequences for age-related health complications requires an understanding of the connection between impaired regeneration, prediabetes, and the related metabolic disorders.
7.2. Metabolic Disorders and Their Impact on Senescence
Senescence and the body's ability to regenerate itself are significantly impacted by prediabetes, a metabolic condition characterized by insulin resistance and dysregulated glucose metabolism [119]. One characteristic that sets prediabetes apart is insulin resistance, which impairs cells' ability to absorb glucose [136]. The main energy source for cellular processes, including regeneration, is glucose [203]. The metabolic abnormalities in prediabetic people make it difficult for glucose to be used efficiently, upsetting the energy balance required for regenerative processes [204]. This metabolic dysregulation impairs the body's capacity for effective tissue regeneration and repair, which in turn adds to the general senescence seen in prediabetic patients [89]. The complex relationship that exists between senescence and metabolic disorders highlights how critical it is to address metabolic factors in order to lessen the effects of prediabetes on aging [57].
Moreover, mitochondrial dysfunction, a major contributor to aging, is closely linked to metabolic disorders in prediabetes [205]. Impaired insulin signalling and elevated oxidative stress have a deleterious effect on prediabetes' mitochondria, the cellular powerhouses in charge of producing energy [196]. Because these mitochondrial disruptions reduce the cell's ability to produce energy for regenerative processes, they worsen cellular aging and senescence [196]. The complex mechanisms by which prediabetes accelerates the aging process are highlighted by the interplay between metabolic disorders, mitochondrial dysfunction, and senescence [206]. This underscores the importance of addressing metabolic factors to manage age-related health conditions in prediabetic individuals [206]. Comprehending how metabolic disorders contribute to prediabetes-induced senescence is essential to understanding how this metabolic condition affects aging in general and what that means for age-related health complications [47].
Figure 3.
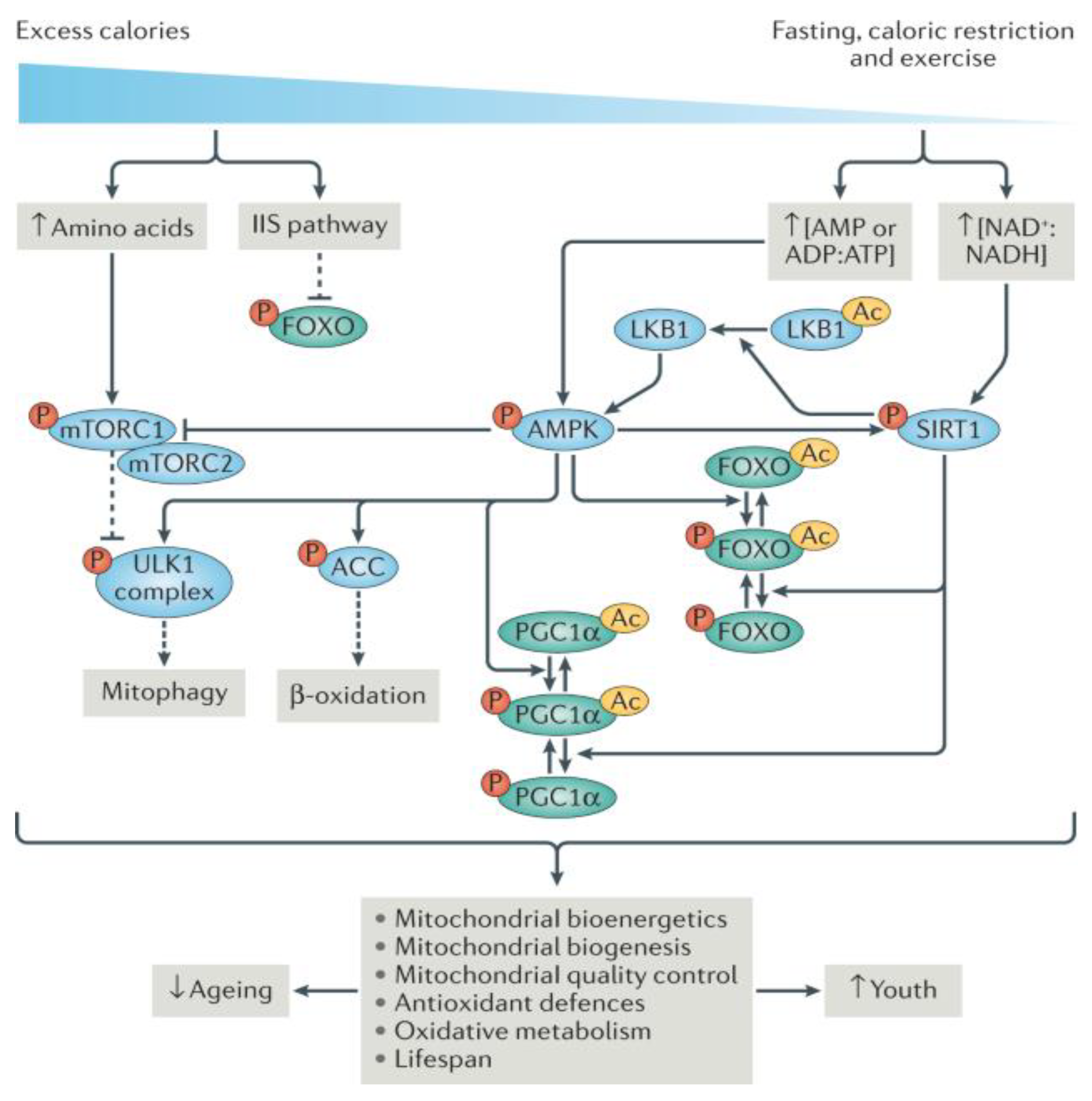
Prediabetes-induced metabolic aging as adapted from source and redrawn from BioRender: The concentrations of important metabolites like NAD+ and AMP rise whereas those of glucose, amino acids, and fats decrease during calorie restriction. A number of metabolic sensors, including insulin-IGF1 signaling (IIS), AMP kinase (AMPK), sirtuins (SIRTs), and the target of rapamycin (TOR), are modulated by these metabolites. Transcription factors like PGC1α and FOXO (peroxisome proliferator-activated receptor-γ coactivator) regulate mitochondrial physiology and homeostasis by acting as a bridge to metabolic sensors. Deficits in mitochondrial homeostasis lead to frailty and illness when this multilayer regulatory mechanism is dysregulated. The abbreviations Ac, ACC, and LKB1 stand for acetyl group, acetyl-CoA carboxylase, and UNC51-like kinase 1, respectively. [130].
Figure 3.
Prediabetes-induced metabolic aging as adapted from source and redrawn from BioRender: The concentrations of important metabolites like NAD+ and AMP rise whereas those of glucose, amino acids, and fats decrease during calorie restriction. A number of metabolic sensors, including insulin-IGF1 signaling (IIS), AMP kinase (AMPK), sirtuins (SIRTs), and the target of rapamycin (TOR), are modulated by these metabolites. Transcription factors like PGC1α and FOXO (peroxisome proliferator-activated receptor-γ coactivator) regulate mitochondrial physiology and homeostasis by acting as a bridge to metabolic sensors. Deficits in mitochondrial homeostasis lead to frailty and illness when this multilayer regulatory mechanism is dysregulated. The abbreviations Ac, ACC, and LKB1 stand for acetyl group, acetyl-CoA carboxylase, and UNC51-like kinase 1, respectively. [130].
7.3. Role of Biomarkers in Metabolic Changes
7.3.1. Mitochondrial Dysfunction: Mitochondria are the cellular powerhouses responsible for energy production, and their proper functioning is essential for various cellular processes, including regeneration [207]. However, in prediabetes, insulin resistance and metabolic alterations lead to disturbances in mitochondrial function, which manifest as decreased mitochondrial efficiency and increased oxidative stress [208]. The compromised mitochondrial function associated with prediabetes not only affects cellular energy production but also exacerbates aging and senescence in prediabetic individuals [209]. Mitochondrial dysfunction is a critical biomarker associated with metabolic changes in prediabetes [205].
7.3.2. Red Blood Cell Distribution Width (RDW): Increased Red Blood Cell Distribution Width (RDW) is a common biomarker of prediabetes, reflecting the condition's associated inflammation and metabolic abnormalities [210]. Red blood cell width variation, or RDW, is a measure of underlying inflammation and metabolic disturbances [211]. An increase in RDW is suggestive of these conditions [211]. When elevated RDW is seen in prediabetic patients, it indicates systemic inflammation and metabolic changes that impact aging [212]. The connection between RDW, inflammation, and metabolic alterations highlights the necessity of addressing these factors in order to reduce the risk of age-related health complications in people who are prediabetic [213].
7.3.3. Haemoglobin A1c (HbA1c): Elevated HbA1c levels in prediabetes can significantly affect how people age [214]. Higher HbA1c values indicate chronic hyperglycemia, while lower levels show the average blood glucose levels over an extended period of time [215]. In prediabetic people, long-term exposure to high blood sugar levels can hasten the aging process by impacting multiple organs and systems [88]. Advanced glycation end products (AGEs), which can harm proteins and lipids and result in tissue dysfunction, are formed in part by chronic hyperglycaemia. Because of the critical role that glycation-induced damage plays in the aging of organs and tissues, HbA1c is an important biomarker for understanding how prediabetes affects age-related health conditions, especially when it comes to diabetes-related aging [64].
7.3.4. Serum Albumin: Serum albumin levels, a biomarker of nutritional status, may be lower in prediabetic individuals [216]. Serum albumin levels dropping may have an impact on frailty and nutritional deficits [217]. The protein albumin is necessary to keep the colloid osmotic pressure constant and to carry vital nutrients throughout the bloodstream [218]. Reduced serum albumin levels in prediabetes may indicate insufficient dietary intake or poor nutrient absorption, which can lead to nutritional deficiencies [219]. These dietary deficits, especially in important vitamins and minerals, can make age-related health problems worse [220]. Additionally, decreased serum albumin levels have been linked to frailty in the elderly, which makes this biomarker an important one for assessing the possibility of frailty in people with prediabetes [217]. In order to effectively manage age-related health complications in this population, it is essential to comprehend the relationship between prediabetes, lower serum albumin levels, and their implications for nutritional status and frailty [221]. Nutritional deficiencies and pre-diabetes.
7.3.5. Folate and B12: Deficits in certain nutrients, especially folate and vitamin B12, can have a major impact on the metabolic alterations linked to prediabetes [222]. The processes of DNA methylation and repair, which are crucial for preserving genomic stability and controlling aging, are directly impacted by these deficiencies [223]. Prevalence of these nutritional deficiencies can be higher in prediabetic individuals, which can accelerate aging [224]. The correct operation of enzymes involved in DNA methylation, a process that regulates gene expression and controls cellular functions, depends on folate and vitamin B12 [225]. Dysregulated DNA methylation can impact aging-related gene expression patterns when it is insufficient [226]. Understanding the complete effects of this metabolic condition on aging and its implications for age-related health complications requires an understanding of the role that folate and vitamin B12 deficiencies play in prediabetes-induced metabolic changes and their impact on senescence [167].
7.3.6. Osteocalcin: Changes in osteocalcin levels are a sign of prediabetes and a biomarker of bone health [227]. Osteoblasts, the cells that form bones, produce a protein called osteocalcin [228]. These changed osteocalcin levels in prediabetic people have consequences for bone health, which is important for aging people [229]. Osteocalcin is essential for preserving the strength and density of bones [230]. Variations in its concentrations can affect bone turnover and, in turn, bone quality. This change in osteocalcin levels may result in decreased bone mineralization and density, which could put older people at higher risk for fractures and other bone-related problems [231]. It's critical to comprehend the relationship between osteocalcin levels and prediabetes in order to develop risk-reduction strategies and to comprehend the possible effects on bone health as we age [232].
7.3.7. Adiponectin: Reduced levels of adiponectin, an adipokine with important metabolic and anti-inflammatory properties, can aggravate insulin resistance and age-related metabolic changes in prediabetes [233]. The main job of the protein hormone adiponectin, which is secreted by adipose tissue, is to control the metabolism of fats and carbohydrates [234]. These metabolic processes can be disrupted by decreased adiponectin levels in prediabetes, especially when it comes to the body's inability to properly use insulin, which eventually results in insulin resistance [70]. One of the main causes of the aging-related metabolic alterations is the deteriorating insulin resistance [235]. Therefore, comprehending the mechanisms behind metabolic alterations and their implications for age-related health conditions requires an understanding of the relationship between prediabetes and adiponectin levels [236].
7.3.8. Leptin: Because of changes in adipose tissue, prediabetics may have changed leptin levels, which can ultimately impact metabolism and ageing [237]. The hormone leptin, which is mostly produced by adipocytes, is essential for controlling metabolism and hunger [238]. These changed leptin levels in prediabetes can have far-reaching effects [239]. Leptin resistance, or decreased sensitivity to leptin, may arise from abnormalities in leptin signalling caused by the alterations in adipose tissue [240]. Overeating, weight gain, and an unbalanced energy intake are all associated with leptin resistance and can aggravate metabolic changes and hasten the aging process [78]. Addressing the underlying mechanisms of age-related health issues in prediabetic individuals requires an understanding of the complex relationship between prediabetes, altered leptin levels, and their impact on metabolism and aging [241].
7.3.9. Brain-Derived Neurotrophic Factor (BDNF): Particularly in older adults, altered BDNF levels in prediabetes can have a major impact on cognitive health [242]. A protein called BDNF is essential for the development, upkeep, and plasticity of brain neurons [243]. Changes in BDNF levels in prediabetes may have an impact on cognitive function [244]. A higher risk of neurodegenerative diseases and cognitive decline have been linked to decreased BDNF levels [245]. A key component of aging is cognitive health, and abnormalities in BDNF levels can affect memory, learning, and other cognitive processes [246]. Understanding the possible effects on cognitive health in the context of aging and creating strategies to support cognitive well-being in prediabetic individuals require an understanding of the relationship between prediabetes and altered BDNF levels [247].
7.3.10. IGF-Binding Proteins: Metabolic and aging-related effects can be attributed to changes in IGF-binding proteins (IGFBPs) in prediabetes, which can have a major effect on the bioavailability of insulin-like growth factor 1 (IGF-1) [248]. IGFBPs play a crucial role in controlling the availability of IGF-1, a growth factor that is important for metabolism, cell division, and growth. Changes in IGFBPs in prediabetes can impact IGF-1 binding and release, which may impact its signaling pathways [249]. Variations in IGF-1 bioavailability can affect metabolic regulation and tissue maintenance, among other physiological processes [250]. Comprehending the relationship between prediabetes and IGFBPs is crucial to understanding the mechanisms behind effects related to metabolism and aging in this population [88]. Understanding IGFBPs' function in the context of prediabetes offers valuable information about possible treatment targets for reducing the age-related effects of this illness [80].
7.3.11. Homocysteine: An amino acid called homocysteine, which is involved in a number of metabolic processes, has been linked to an increased risk of cardiovascular disease and may be more common in people who are prediabetic [251]. It is well recognized that homocysteine contributes to the development of atherosclerosis and other cardiovascular diseases [252]. Elevated homocysteine levels in prediabetes can be caused by metabolic abnormalities as well as changes in folate and vitamin B12 levels [251]. This homocysteine increase can exacerbate oxidative stress and endothelial dysfunction, two conditions that hasten the vascular system's aging process[251]. Recognizing the age-related implications of prediabetes, especially with regard to the vascular system, requires an understanding of the relationship between elevated homocysteine levels, cardiovascular risk, and the condition [253].
7.3.12. Insulin Resistance Markers: One of the hallmarks of prediabetes is elevated insulin resistance markers, which can get worse with age [254]. One such marker is the Homeostatic Model Assessment of Insulin Resistance (HOMA-IR) [254]. One of the main features of prediabetes is insulin resistance, which is typified by the body's decreased sensitivity to the insulin hormone. Insulin resistance markers are frequently elevated in prediabetic individuals, indicating a compromised cell's ability to effectively absorb glucose [255]. Insulin resistance can progress more quickly in older people [256]. The deterioration of insulin resistance is a major factor in the age- and metabolic-related consequences of prediabetes [257]. Understanding the complete impact of prediabetes on the aging process requires an understanding of the role of insulin resistance markers in this condition and their potential to exacerbate age-related metabolic changes [2].
8. Perspectives for Future Research
8.1. Gaps in Current Understanding and the Need for Further Research
Although this thorough review clarifies the complex interactions among prediabetes, senescence, and blood-based biomarkers, there are still a number of unanswered questions that underscore the need for more in-depth study in the future [258]. First and foremost, investigating the temporal correlations between these biomarkers and prediabetes-induced senescence is imperative [12]. Examining whether particular biomarkers are early markers of prediabetes or if the condition only manifests them as it advances could yield important information for prompt diagnosis and treatment [259]. Furthermore, additional investigation is required to clarify the interplay and possible synergies between these biomarkers [259]. It is crucial to understand how various biomarkers may work together to accelerate age-related diseases and senescence in prediabetic people. This is an area that needs more research [260].
Furthermore, more research is needed to determine how pharmacological and lifestyle interventions affect blood-based biomarkers of prediabetes-induced senescence [261]. It is crucial to find interventions that can adjust these biomarker levels, delay aging, and lower the chance of age-related problems in people who are prediabetic [60]. Furthermore, it is an exciting direction for future research to investigate these biomarkers' potential as therapeutic targets [262]. Creating therapies that target the identified biomarkers directly could provide fresh approaches to improving health outcomes and delaying prediabetes-related senescence [263]. All things considered, filling in these knowledge gaps and carrying out additional research are essential to improving our comprehension of prediabetes-induced senescence and creating practical plans to lessen its effects on aging and age-related illnesses [264].
8.2. Potential Blood-Based Biomarkers and Intervention Strategies
Future studies should concentrate on finding more blood-based biomarkers that can function as early warning systems for age-related complications linked to prediabetes-induced senescence [6]. The identification of new biomarkers would improve our capacity to identify prediabetes early on and to take preventative action [265]. Furthermore, studies ought to focus on creating customized intervention plans according to the unique biomarker profiles of people who are prediabetic [266]. Customized therapies that focus on each patient's distinct biomarker patterns could offer more accurate and successful methods for slowing down aging and averting age-related illnesses [267]. It is crucial to look into how pharmacological treatments, dietary changes, and exercise routines might affect these biomarkers [267]. These intervention strategies may improve the general health and longevity of prediabetic individuals while also delaying the onset of senescence. The Role of Additional Biomarkers (e.g., Folate and B12, Osteocalcin) in Future Research on Prediabetes-Induced Senescence [264]
Subsequent investigations ought to delve into the complex functions of supplementary blood-based indicators, like folate and B12, concerning prediabetes-induced senescence [268]. It is crucial to look into how dietary deficiencies, particularly in regard to important nutrients like folate and B12, affect senescence and the effects of aging on people who are prediabetic [269]. Gaining knowledge about how these biomarkers affect DNA methylation and repair—both essential for good aging—can help identify the underlying processes [59].
Furthermore, future studies should concentrate on the function of biomarkers like osteocalcin in bone health and aging [270]. The importance of osteocalcin in preserving bone density and general skeletal health is widely established, and in the context of prediabetes-induced senescence, it can provide information about tactics for protecting musculoskeletal integrity in older prediabetic patients [229].
For a more comprehensive understanding of the condition's impact on aging, a thorough assessment of these additional biomarkers in prediabetes-induced senescence is imperative. It has the potential to reveal novel approaches to addressing nutritional inadequacies and bone health, two critical facets of ageing well. Future studies examining these biomarkers may lead to better therapeutic and preventive strategies for prediabetic patients in an effort to support healthy aging [47].
9. Conclusion
9.1. Summarizing Key Findings on Blood-Based Biomarkers in Prediabetes-Induced Senescence
Several important findings are highlighted in this thorough review of blood-based biomarkers in prediabetes-induced senescence [47]. Prediabetes is linked to a complex web of biomarkers that interact to speed up aging, raise the chance of developing age-related illnesses, and impact different physiological systems [271]. Telomere length, p16INK4a, advanced glycation end products (AGEs), senescence-associated secretory phenotype (SASP) factors, DNA methylation clocks, inflammatory markers, oxidative stress markers, circulating hormones, growth factors, and other biomarkers like folate and B12, osteocalcin, and others are some of these biomarkers [272]. The review highlights the fact that these biomarkers are active contributors to chronic inflammation, oxidative stress, and metabolic dysregulation all of which accelerate aging in addition to acting as markers of senescence [62]. With the potential to improve quality of life and encourage healthy aging, the thorough understanding of these biomarkers and their complex relationships with prediabetes-induced senescence serves as a basis for the development of customized intervention strategies aimed at mitigating age-related complications in prediabetic individuals [260].
9.2. Implications for Understanding Senescence and Aging-Related Disorders in Prediabetes
It is critical to comprehend the effects of aging and disorders related to senescence in the context of prediabetes [57]. This thorough analysis emphasizes that prediabetes is a crucial stage that profoundly affects age-related disorders and the aging process; it is not just a stage between normal glucose metabolism and diabetes. In this case, senescence—which is accelerated by the complex interactions among blood-based biomarkers—is essential [47]. The ramifications are extensive and touch on many physiological systems, such as the nervous and circulatory systems, metabolism, inflammation, and hormone control [273]. In addition, the review indicates that the influence of prediabetes on senescence can vary greatly among individuals, emphasizing the necessity of tailored intervention approaches to successfully lessen the effects of aging-related illnesses [274]. These findings highlight the significance of early detection and intervention in prediabetic individuals to promote healthy aging and lower the burden of age-related diseases, with significant implications for public health and clinical practice. In the end, gaining an understanding of the consequences of senescence in prediabetes is essential to improving our capacity to improve the well-being and quality of life for an aging population with a variety of needs.
9.3. Future Directions for Research Incorporating Diverse Biomarkers in Prediabetes-Induced Senescence
Future studies on prediabetes-induced senescence ought to focus on incorporating an even wider range of biomarkers in order to obtain a thorough grasp of the complex mechanisms underlying this condition. This strategy may entail both the discovery of novel blood-based biomarkers and a closer examination of the functions of those that have already been identified. Studies ought to investigate the interactions among these biomarkers and evaluate how they all contribute to physiological systems' aging process, which in turn affects age-related illnesses. Future research should also put a high priority on creating novel diagnostic instruments and intervention plans that make use of these various biomarkers for precision medicine. This will enable prediabetic patients to receive individualized care that will delay senescence and encourage healthy aging. A more nuanced understanding of the variability of prediabetes and the complex nature of senescence will be possible through the integration of a wide range of biomarkers, opening the door to more efficient and individualized treatment of this illness and its effects on aging.
Author Contributions
Conceptualization, N.A.M and A.G-A.M. and A.K.; writing—original draft preparation, N.A.M. and A.G-A.M.; writing—review and editing, N.A.M. and A.G-A.M.; supervision, A.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research has received no funding
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
The authors thank the College of Health Sciences.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Echouffo-Tcheugui, J.B.; Selvin, E. Prediabetes and What It Means: The Epidemiological Evidence. Annu Rev Public Health 2021, 42, 59–77. [Google Scholar] [CrossRef] [PubMed]
- Nolan, C.J.; Prentki, M. Insulin resistance and insulin hypersecretion in the metabolic syndrome and type 2 diabetes: Time for a conceptual framework shift. Diabetes and Vascular Disease Research 2019, 16, 118–127. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Gómez, M.E.; Zapico, S.C. Frailty, cognitive decline, neurodegenerative diseases and nutrition interventions. International Journal of Molecular Sciences 2019, 20, 2842. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Han, X.; Zhang, X.; Wang, S. Spatiotemporal evolution of global population ageing from 1960 to 2017. BMC public health 2019, 19, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Echouffo-Tcheugui, J.B.; Selvin, E. Prediabetes and what it means: the epidemiological evidence. Annual review of public health 2021, 42, 59–77. [Google Scholar] [CrossRef] [PubMed]
- Khan, R.M.M.; Chua, Z.J.Y.; Tan, J.C.; Yang, Y.; Liao, Z.; Zhao, Y. From pre-diabetes to diabetes: diagnosis, treatments and translational research. Medicina 2019, 55, 546. [Google Scholar] [CrossRef] [PubMed]
- Rybtsova, N.; Berezina, T.; Kagansky, A.; Rybtsov, S. Can blood-circulating factors unveil and delay your biological aging? Biomedicines 2020, 8, 615. [Google Scholar] [CrossRef] [PubMed]
- Dorcely, B.; Katz, K.; Jagannathan, R.; Chiang, S.S.; Oluwadare, B.; Goldberg, I.J.; Bergman, M. Novel biomarkers for prediabetes, diabetes, and associated complications. Diabetes Metab Syndr Obes 2017, 10, 345–361. [Google Scholar] [CrossRef] [PubMed]
- Pyo, I.S.; Yun, S.; Yoon, Y.E.; Choi, J.-W.; Lee, S.-J. Mechanisms of aging and the preventive effects of resveratrol on age-related diseases. Molecules 2020, 25, 4649. [Google Scholar] [CrossRef] [PubMed]
- De Biasi, A.; Wolfe, M.; Carmody, J.; Fulmer, T.; Auerbach, J. Creating an age-friendly public health system. Innovation in Aging 2020, 4, igz044. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.; Ma, Y.; Luo, Y.; Song, Y.; Xiong, G.; Ma, Y.; Sun, X.; Kan, C. Metabolic diseases and healthy aging: identifying environmental and behavioral risk factors and promoting public health. Front Public Health 2023, 11, 1253506. [Google Scholar] [CrossRef] [PubMed]
- Bahour, N.; Cortez, B.; Pan, H.; Shah, H.; Doria, A.; Aguayo-Mazzucato, C. Diabetes mellitus correlates with increased biological age as indicated by clinical biomarkers. Geroscience 2022, 44, 415–427. [Google Scholar] [CrossRef] [PubMed]
- Gu, Y.; Han, J.; Jiang, C.; Zhang, Y. Biomarkers, oxidative stress and autophagy in skin aging. Ageing research reviews 2020, 59, 101036. [Google Scholar] [CrossRef] [PubMed]
- Chia, C.W.; Egan, J.M.; Ferrucci, L. Age-Related Changes in Glucose Metabolism, Hyperglycemia, and Cardiovascular Risk. Circ Res 2018, 123, 886–904. [Google Scholar] [CrossRef] [PubMed]
- Mota, R.I.; Morgan, S.E.; Bahnson, E.M. Diabetic vasculopathy: macro and microvascular injury. Current pathobiology reports 2020, 8, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Fhayli, W.; Boëté, Q.; Harki, O.; Briançon-Marjollet, A.; Jacob, M.-P.; Faury, G. Rise and fall of elastic fibers from development to aging. Consequences on arterial structure-function and therapeutical perspectives. Matrix Biology 2019, 84, 41–56. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Yuan, Y.; Zheng, M.; Pan, A.; Wang, M.; Zhao, M.; Li, Y.; Yao, S.; Chen, S.; Wu, S. Association of age of onset of hypertension with cardiovascular diseases and mortality. Journal of the American College of Cardiology 2020, 75, 2921–2930. [Google Scholar] [CrossRef] [PubMed]
- Brannick, B.; Dagogo-Jack, S. Prediabetes and Cardiovascular Disease: Pathophysiology and Interventions for Prevention and Risk Reduction. Endocrinol Metab Clin North Am 2018, 47, 33–50. [Google Scholar] [CrossRef] [PubMed]
- Luc, K.; Schramm-Luc, A.; Guzik, T.; Mikolajczyk, T. Oxidative stress and inflammatory markers in prediabetes and diabetes. Journal of Physiology & Pharmacology 2019, 70. [Google Scholar]
- Izzo, C.; Vitillo, P.; Di Pietro, P.; Visco, V.; Strianese, A.; Virtuoso, N.; Ciccarelli, M.; Galasso, G.; Carrizzo, A.; Vecchione, C. The role of oxidative stress in cardiovascular aging and cardiovascular diseases. Life 2021, 11, 60. [Google Scholar] [CrossRef] [PubMed]
- Dilworth, L.; Facey, A.; Omoruyi, F. Diabetes Mellitus and Its Metabolic Complications: The Role of Adipose Tissues. International Journal of Molecular Sciences 2021, 22, 7644. [Google Scholar] [CrossRef] [PubMed]
- Foretz, M.; Guigas, B.; Viollet, B. Understanding the glucoregulatory mechanisms of metformin in type 2 diabetes mellitus. Nature Reviews Endocrinology 2019, 15, 569–589. [Google Scholar] [CrossRef] [PubMed]
- Chaudhary, M.R.; Chaudhary, S.; Sharma, Y.; Singh, T.A.; Mishra, A.K.; Sharma, S.; Mehdi, M.M. Aging, oxidative stress and degenerative diseases: mechanisms, complications and emerging therapeutic strategies. Biogerontology 2023, 24, 609–662. [Google Scholar] [CrossRef] [PubMed]
- Gianazza, E.; Brioschi, M.; Baetta, R.; Mallia, A.; Banfi, C.; Tremoli, E. Platelets in healthy and disease states: from biomarkers discovery to drug targets identification by proteomics. International journal of molecular sciences 2020, 21, 4541. [Google Scholar] [CrossRef] [PubMed]
- Aguayo-Mazzucato, C.; Andle, J.; Lee, T.B.; Midha, A.; Talemal, L.; Chipashvili, V.; Hollister-Lock, J.; van Deursen, J.; Weir, G.; Bonner-Weir, S. Acceleration of β cell aging determines diabetes and senolysis improves disease outcomes. Cell metabolism 2019, 30, 129–142. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.S.; Hossain, K.S.; Das, S.; Kundu, S.; Adegoke, E.O.; Rahman, M.A.; Hannan, M.A.; Uddin, M.J.; Pang, M.-G. Role of insulin in health and disease: an update. International journal of molecular sciences 2021, 22, 6403. [Google Scholar] [CrossRef] [PubMed]
- Derrick, S.A.; Kristo, A.S.; Reaves, S.K.; Sikalidis, A.K. Effects of dietary red raspberry consumption on pre-diabetes and type 2 diabetes mellitus parameters. International Journal of Environmental Research and Public Health 2021, 18, 9364. [Google Scholar] [CrossRef] [PubMed]
- Ellulu, M.S.; Samouda, H. Clinical and biological risk factors associated with inflammation in patients with type 2 diabetes mellitus. BMC Endocrine Disorders 2022, 22, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Barbu, E.; Popescu, M.-R.; Popescu, A.-C.; Balanescu, S.-M. Inflammation as a precursor of atherothrombosis, diabetes and early vascular aging. International Journal of Molecular Sciences 2022, 23, 963. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Li, C.; Zhang, W.; Wang, Y.; Qian, P.; Huang, H. Inflammation and aging: signaling pathways and intervention therapies. Signal Transduction and Targeted Therapy 2023, 8, 239. [Google Scholar] [CrossRef] [PubMed]
- Wan, M.; Gray-Gaillard, E.F.; Elisseeff, J.H. Cellular senescence in musculoskeletal homeostasis, diseases, and regeneration. Bone Res 2021, 9, 41. [Google Scholar] [CrossRef] [PubMed]
- Shahwan, M.J.; Jairoun, A.A.; Farajallah, A.; Shanabli, S. Prevalence of dyslipidemia and factors affecting lipid profile in patients with type 2 diabetes. Diabetes & Metabolic Syndrome: Clinical Research & Reviews 2019, 13, 2387–2392. [Google Scholar]
- Nguyen, M.T.; Fernando, S.; Schwarz, N.; Tan, J.T.; Bursill, C.A.; Psaltis, P.J. Inflammation as a therapeutic target in atherosclerosis. Journal of clinical medicine 2019, 8, 1109. [Google Scholar] [CrossRef] [PubMed]
- Honda, M. Reverse Heart Disease Naturally: Cures for high cholesterol, hypertension, arteriosclerosis, blood clots, aneurysms, myocardial infarcts and more; Hatherleigh Press: 2019.
- Gilon, P. The role of α-cells in islet function and glucose homeostasis in health and type 2 diabetes. Journal of molecular biology 2020, 432, 1367–1394. [Google Scholar] [CrossRef] [PubMed]
- Dozio, E.; Massaccesi, L.; Corsi Romanelli, M.M. Glycation and Glycosylation in Cardiovascular Remodeling: Focus on Advanced Glycation End Products and O-Linked Glycosylations as Glucose-Related Pathogenetic Factors and Disease Markers. Journal of Clinical Medicine 2021, 10, 4792. [Google Scholar] [CrossRef] [PubMed]
- Kosmopoulos, M.; Drekolias, D.; Zavras, P.D.; Piperi, C.; Papavassiliou, A.G. Impact of advanced glycation end products (AGEs) signaling in coronary artery disease. Biochimica et Biophysica Acta (BBA)-Molecular Basis of Disease 2019, 1865, 611–619. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Zhang, Z.; Ren, Y.; Wang, Y.; Fang, J.; Yue, H.; Ma, S.; Guan, F. Aging and age-related diseases: from mechanisms to therapeutic strategies. Biogerontology 2021, 22, 165–187. [Google Scholar] [CrossRef] [PubMed]
- Banday, M.Z.; Sameer, A.S.; Nissar, S. Pathophysiology of diabetes: An overview. Avicenna journal of medicine 2020, 10, 174–188. [Google Scholar] [CrossRef] [PubMed]
- Biessels, G.J.; Nobili, F.; Teunissen, C.E.; Simó, R.; Scheltens, P. Understanding multifactorial brain changes in type 2 diabetes: a biomarker perspective. The Lancet Neurology 2020, 19, 699–710. [Google Scholar] [CrossRef] [PubMed]
- Kudryashova, K.S.; Burka, K.; Kulaga, A.Y.; Vorobyeva, N.S.; Kennedy, B.K. Aging biomarkers: from functional tests to multi-omics approaches. Proteomics 2020, 20, 1900408. [Google Scholar] [CrossRef] [PubMed]
- Zheng, L.; Meng, Y.; Campbell, J.L.; Shen, B. Multiple roles of DNA2 nuclease/helicase in DNA metabolism, genome stability and human diseases. Nucleic acids research 2020, 48, 16–35. [Google Scholar] [CrossRef] [PubMed]
- Kamal, N.S.M.; Safuan, S.; Shamsuddin, S.; Foroozandeh, P. Aging of the cells: Insight into cellular senescence and detection Methods. European journal of cell biology 2020, 99, 151108. [Google Scholar]
- Gavia-García, G.; Rosado-Pérez, J.; Arista-Ugalde, T.L.; Aguiñiga-Sánchez, I.; Santiago-Osorio, E.; Mendoza-Núñez, V.M. Telomere length and oxidative stress and its relation with metabolic syndrome components in the aging. Biology 2021, 10, 253. [Google Scholar] [CrossRef] [PubMed]
- Tam, B.T.; Morais, J.A.; Santosa, S. Obesity and ageing: Two sides of the same coin. Obesity Reviews 2020, 21, e12991. [Google Scholar] [CrossRef] [PubMed]
- Safwan-Zaiter, H.; Wagner, N.; Wagner, K.-D. P16INK4A—More Than a Senescence Marker. Life 2022, 12, 1332. [Google Scholar] [CrossRef] [PubMed]
- Mbatha, N.A.; Mzimela, N.C.; Mushebenge, A.G.-A.; Khathi, A. Investigating the Impact of Prediabetes on the Aging Process through Longitudinal Analysis of Blood-Based Biomarkers: A Systematic Review and Meta-Analysis Protocol. medRxiv 2023, 2023.2007. 2031.23293409. [Google Scholar]
- Yi, H.-S.; Kim, S.Y.; Kim, J.T.; Lee, Y.-S.; Moon, J.S.; Kim, M.; Kang, Y.E.; Joung, K.H.; Lee, J.H.; Kim, H.J. T-cell senescence contributes to abnormal glucose homeostasis in humans and mice. Cell death & disease 2019, 10, 249. [Google Scholar]
- Xiong, Y.; Zhou, L. The signaling of cellular senescence in diabetic nephropathy. Oxidative medicine and cellular longevity 2019, 2019. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Liu, F.; Yang, P.; Xiong, F.; Yu, Q.; Li, J.; Zhou, Z.; Zhang, S.; Wang, C.-Y. Aging and stress induced β cell senescence and its implication in diabetes development. Aging (Albany NY) 2019, 11, 9947. [Google Scholar] [CrossRef] [PubMed]
- Cianflone, E.; Torella, M.; Biamonte, F.; De Angelis, A.; Urbanek, K.; Costanzo, F.S.; Rota, M.; Ellison-Hughes, G.M.; Torella, D. Targeting cardiac stem cell senescence to treat cardiac aging and disease. Cells 2020, 9, 1558. [Google Scholar] [CrossRef] [PubMed]
- Lopes-Paciencia, S.; Saint-Germain, E.; Rowell, M.-C.; Ruiz, A.F.; Kalegari, P.; Ferbeyre, G. The senescence-associated secretory phenotype and its regulation. Cytokine 2019, 117, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Lagoumtzi, S.M.; Chondrogianni, N. Senolytics and senomorphics: Natural and synthetic therapeutics in the treatment of aging and chronic diseases. Free Radical Biology and Medicine 2021, 171, 169–190. [Google Scholar] [CrossRef] [PubMed]
- Khosla, S.; Samakkarnthai, P.; Monroe, D.G.; Farr, J.N. Update on the pathogenesis and treatment of skeletal fragility in type 2 diabetes mellitus. Nature Reviews Endocrinology 2021, 17, 685–697. [Google Scholar] [CrossRef] [PubMed]
- Raucci, A.; Macrì, F.; Castiglione, S.; Badi, I.; Vinci, M.C.; Zuccolo, E. MicroRNA-34a: the bad guy in age-related vascular diseases. Cellular and Molecular Life Sciences 2021, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Teissier, T.; Boulanger, E.; Cox, L.S. Interconnections between inflammageing and immunosenescence during ageing. Cells 2022, 11, 359. [Google Scholar] [CrossRef] [PubMed]
- Khosla, S.; Farr, J.N.; Tchkonia, T.; Kirkland, J.L. The role of cellular senescence in ageing and endocrine disease. Nature Reviews Endocrinology 2020, 16, 263–275. [Google Scholar] [CrossRef] [PubMed]
- Tracy, E.P.; Hughes, W.; Beare, J.E.; Rowe, G.; Beyer, A.; LeBlanc, A.J. Aging-induced impairment of vascular function: Mitochondrial redox contributions and physiological/clinical implications. Antioxidants & Redox Signaling 2021, 35, 974–1015. [Google Scholar]
- Unnikrishnan, A.; Freeman, W.M.; Jackson, J.; Wren, J.D.; Porter, H.; Richardson, A. The role of DNA methylation in epigenetics of aging. Pharmacology & therapeutics 2019, 195, 172–185. [Google Scholar]
- Salameh, Y.; Bejaoui, Y.; El Hajj, N. DNA methylation biomarkers in aging and age-related diseases. Frontiers in Genetics 2020, 11, 171. [Google Scholar] [CrossRef] [PubMed]
- Samblas, M.; Milagro, F.I.; Martínez, A. DNA methylation markers in obesity, metabolic syndrome, and weight loss. Epigenetics 2019, 14, 421–444. [Google Scholar] [CrossRef] [PubMed]
- Maldonado, E.; Morales-Pison, S.; Urbina, F.; Solari, A. Aging Hallmarks and the Role of Oxidative Stress. Antioxidants 2023, 12, 651. [Google Scholar] [CrossRef] [PubMed]
- Barkabi-Zanjani, S.; Ghorbanzadeh, V.; Aslani, M.; Ghalibafsabbaghi, A.; Chodari, L. Diabetes mellitus and the impairment of male reproductive function: Possible signaling pathways. Diabetes & Metabolic Syndrome: Clinical Research & Reviews 2020, 14, 1307–1314. [Google Scholar]
- Twarda-Clapa, A.; Olczak, A.; Białkowska, A.M.; Koziołkiewicz, M. Advanced glycation end-products (AGEs): Formation, chemistry, classification, receptors, and diseases related to AGEs. Cells 2022, 11, 1312. [Google Scholar] [CrossRef] [PubMed]
- López-Otín, C.; Blasco, M.A.; Partridge, L.; Serrano, M.; Kroemer, G. Hallmarks of aging: An expanding universe. Cell 2023. [Google Scholar] [CrossRef] [PubMed]
- Basisty, N.; Kale, A.; Jeon, O.H.; Kuehnemann, C.; Payne, T.; Rao, C.; Holtz, A.; Shah, S.; Sharma, V.; Ferrucci, L. A proteomic atlas of senescence-associated secretomes for aging biomarker development. PLoS biology 2020, 18, e3000599. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Liu, H.; Hu, Q.; Wang, L.; Liu, J.; Zheng, Z.; Zhang, W.; Ren, J.; Zhu, F.; Liu, G.-H. Epigenetic regulation of aging: implications for interventions of aging and diseases. Signal Transduction and Targeted Therapy 2022, 7, 374. [Google Scholar] [CrossRef] [PubMed]
- Haywood, N.J.; Slater, T.A.; Matthews, C.J.; Wheatcroft, S.B. The insulin like growth factor and binding protein family: Novel therapeutic targets in obesity & diabetes. Molecular Metabolism 2019, 19, 86–96. [Google Scholar] [PubMed]
- Barclay, R.D.; Burd, N.A.; Tyler, C.; Tillin, N.A.; Mackenzie, R.W. The role of the IGF-1 signaling cascade in muscle protein synthesis and anabolic resistance in aging skeletal muscle. Frontiers in nutrition 2019, 6, 146. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Chi, X.; Wang, Y.; Setrerrahmane, S.; Xie, W.; Xu, H. Trends in insulin resistance: Insights into mechanisms and therapeutic strategy. Signal Transduction and Targeted Therapy 2022, 7, 216. [Google Scholar] [CrossRef] [PubMed]
- Koffi, K.A.; Doublier, S.; Ricort, J.-M.; Babajko, S.; Nassif, A.; Isaac, J. The role of GH/IGF axis in dento-alveolar complex from development to aging and therapeutics: A narrative review. Cells 2021, 10, 1181. [Google Scholar] [CrossRef] [PubMed]
- Ehtewish, H.; Arredouani, A.; El-Agnaf, O. Diagnostic, prognostic, and mechanistic biomarkers of diabetes mellitus-associated cognitive decline. International Journal of Molecular Sciences 2022, 23, 6144. [Google Scholar] [CrossRef] [PubMed]
- Sharma, G.; Parihar, A.; Talaiya, T.; Dubey, K.; Porwal, B.; Parihar, M.S. Cognitive impairments in type 2 diabetes, risk factors and preventive strategies. Journal of basic and clinical physiology and pharmacology 2020, 31, 20190105. [Google Scholar] [CrossRef] [PubMed]
- Balasubramanian, P.; Kiss, T.; Tarantini, S.; Nyúl-Tóth, Á.; Ahire, C.; Yabluchanskiy, A.; Csipo, T.; Lipecz, A.; Tabak, A.; Institoris, A. Obesity-induced cognitive impairment in older adults: a microvascular perspective. American Journal of Physiology-Heart and Circulatory Physiology 2021, 320, H740–H761. [Google Scholar] [CrossRef] [PubMed]
- Wondmkun, Y.T. Obesity, insulin resistance, and type 2 diabetes: associations and therapeutic implications. Diabetes, Metabolic Syndrome and Obesity, 3616. [Google Scholar]
- Kuryłowicz, A.; Koźniewski, K. Anti-inflammatory strategies targeting metaflammation in type 2 diabetes. Molecules 2020, 25, 2224. [Google Scholar] [CrossRef] [PubMed]
- Ou, M.-Y.; Zhang, H.; Tan, P.-C.; Zhou, S.-B.; Li, Q.-F. Adipose tissue aging: Mechanisms and therapeutic implications. Cell death & disease 2022, 13, 300. [Google Scholar]
- Salvestrini, V.; Sell, C.; Lorenzini, A. Obesity may accelerate the aging process. Frontiers in endocrinology 2019, 10, 266. [Google Scholar] [CrossRef] [PubMed]
- Le Couteur, D.G.; Solon-Biet, S.M.; Cogger, V.C.; Ribeiro, R.; de Cabo, R.; Raubenheimer, D.; Cooney, G.J.; Simpson, S.J. Branched chain amino acids, aging and age-related health. Ageing Research Reviews 2020, 64, 101198. [Google Scholar] [CrossRef] [PubMed]
- Slater, T.; Haywood, N.J.; Matthews, C.; Cheema, H.; Wheatcroft, S.B. Insulin-like growth factor binding proteins and angiogenesis: from cancer to cardiovascular disease. Cytokine & growth factor reviews 2019, 46, 28–35. [Google Scholar]
- Kasprzak, A. Insulin-like growth factor 1 (IGF-1) signaling in glucose metabolism in colorectal cancer. International Journal of Molecular Sciences 2021, 22, 6434. [Google Scholar] [CrossRef] [PubMed]
- Barone, E.; Di Domenico, F.; Perluigi, M.; Butterfield, D.A. The interplay among oxidative stress, brain insulin resistance and AMPK dysfunction contribute to neurodegeneration in type 2 diabetes and Alzheimer disease. Free Radical Biology and Medicine 2021, 176, 16–33. [Google Scholar] [CrossRef] [PubMed]
- Wan, M.; Gray-Gaillard, E.F.; Elisseeff, J.H. Cellular senescence in musculoskeletal homeostasis, diseases, and regeneration. Bone Research 2021, 9, 41. [Google Scholar] [CrossRef] [PubMed]
- Fadini, G.P.; Albiero, M.; Bonora, B.M.; Avogaro, A. Angiogenic abnormalities in diabetes mellitus: mechanistic and clinical aspects. The Journal of Clinical Endocrinology & Metabolism 2019, 104, 5431–5444. [Google Scholar]
- Schalkwijk, C.; Stehouwer, C. Methylglyoxal, a highly reactive dicarbonyl compound, in diabetes, its vascular complications, and other age-related diseases. Physiological reviews 2020, 100, 407–461. [Google Scholar] [CrossRef] [PubMed]
- Di Micco, R.; Krizhanovsky, V.; Baker, D.; d’Adda di Fagagna, F. Cellular senescence in ageing: from mechanisms to therapeutic opportunities. Nature reviews Molecular cell biology 2021, 22, 75–95. [Google Scholar] [CrossRef] [PubMed]
- Mancinelli, R.; Checcaglini, F.; Coscia, F.; Gigliotti, P.; Fulle, S.; Fanò-Illic, G. Biological aspects of selected myokines in skeletal muscle: focus on aging. International Journal of Molecular Sciences 2021, 22, 8520. [Google Scholar] [CrossRef] [PubMed]
- LeRoith, D.; Holly, J.M.; Forbes, B.E. Insulin-like growth factors: Ligands, binding proteins, and receptors. Molecular metabolism 2021, 52, 101245. [Google Scholar] [CrossRef] [PubMed]
- Bellary, S.; Kyrou, I.; Brown, J.E.; Bailey, C.J. Type 2 diabetes mellitus in older adults: clinical considerations and management. Nature Reviews Endocrinology 2021, 17, 534–548. [Google Scholar] [CrossRef]
- Dichtel, L.E.; Cordoba-Chacon, J.; Kineman, R.D. Growth Hormone and Insulin-Like Growth Factor 1 Regulation of Nonalcoholic Fatty Liver Disease. The Journal of Clinical Endocrinology & Metabolism 2022, 107, 1812–1824. [Google Scholar] [CrossRef]
- Biadgo, B.; Tamir, W.; Ambachew, S. Insulin-like Growth Factor and its Therapeutic Potential for Diabetes Complications - Mechanisms and Metabolic Links: A Review. Rev Diabet Stud 2020, 16, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Elpers, A.-L.; Steptoe, A. Associations between dehydroepiandrosterone sulphate (DHEAS) and cognitive function in 5,061 older men and women in the English Longitudinal Study of Ageing. Psychoneuroendocrinology 2020, 117, 104702. [Google Scholar] [CrossRef] [PubMed]
- Sinha, N.; Maiti, A.; Sinha, A.; Basu, A.; Das, T.C. Study of serum testosterone level in males with Prediabetes, before and after 3 months of metformin therapy, in patients attending a tertiary care hospital in West Bengal, Eastern India.
- De Paoli, M.; Zakharia, A.; Werstuck, G.H. The Role of Estrogen in Insulin Resistance: A Review of Clinical and Preclinical Data. The American Journal of Pathology 2021, 191, 1490–1498. [Google Scholar] [CrossRef] [PubMed]
- van den Beld, A.W.; Kaufman, J.M.; Zillikens, M.C.; Lamberts, S.W.J.; Egan, J.M.; van der Lely, A.J. The physiology of endocrine systems with ageing. Lancet Diabetes Endocrinol 2018, 6, 647–658. [Google Scholar] [CrossRef] [PubMed]
- Yen, H.H.; Hsieh, S.T.; Chen, C.L.; Yang, W.S.; Lee, P.C.; Lin, M.T.; Chen, C.N.; Yang, P.J. Circulating Diabetic Candidate Neurotrophic Factors, Brain-Derived Neurotrophic Factor and Fibroblast Growth Factor 21, in Sleeve Gastrectomy. Sci Rep 2020, 10, 5341. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.B.; Aleksic, S.; Gao, T.; Weiss, E.F.; Demetriou, E.; Verghese, J.; Holtzer, R.; Barzilai, N.; Milman, S. Insulin-like Growth Factor-1 and IGF Binding Proteins Predict All-Cause Mortality and Morbidity in Older Adults. Cells 2020, 9, 1368. [Google Scholar] [CrossRef] [PubMed]
- Sánchez, E.; Betriu, À.; López-Cano, C.; Hernández, M.; Fernández, E.; Purroy, F.; Bermúdez-López, M.; Farràs-Sallés, C.; Barril, S.; Pamplona, R. Characteristics of atheromatosis in the prediabetes stage: A cross-sectional investigation of the ILERVAS project. Cardiovascular diabetology 2019, 18, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Mangge, H.; Herrmann, M.; Almer, G.; Zelzer, S.; Moeller, R.; Horejsi, R.; Renner, W. Telomere shortening associates with elevated insulin and nuchal fat accumulation. Sci Rep 2020, 10, 6863. [Google Scholar] [CrossRef] [PubMed]
- Ungvari, Z.; Tarantini, S.; Sorond, F.; Merkely, B.; Csiszar, A. Mechanisms of Vascular Aging, A Geroscience Perspective: JACC Focus Seminar. Journal of the American College of Cardiology 2020, 75, 931–941. [Google Scholar] [CrossRef] [PubMed]
- Schafer, M.J.; Zhang, X.; Kumar, A.; Atkinson, E.J.; Zhu, Y.; Jachim, S.; Mazula, D.L.; Brown, A.K.; Berning, M.; Aversa, Z.; et al. The senescence-associated secretome as an indicator of age and medical risk. JCI Insight 2020, 5. [Google Scholar] [CrossRef] [PubMed]
- Reale, A.; Tagliatesta, S.; Zardo, G.; Zampieri, M. Counteracting aged DNA methylation states to combat ageing and age-related diseases. Mechanisms of Ageing and Development 2022, 206, 111695. [Google Scholar] [CrossRef] [PubMed]
- Dhindsa, S.; Zhang, N.; McPhaul, M.J.; Wu, Z.; Ghoshal, A.K.; Erlich, E.C.; Mani, K.; Randolph, G.J.; Edwards, J.R.; Mudd, P.A.; et al. Association of Circulating Sex Hormones With Inflammation and Disease Severity in Patients With COVID-19. JAMA Network Open 2021, 4, e2111398. [Google Scholar] [CrossRef] [PubMed]
- Berezin, A.E.; Berezin, A.A. Circulating Cardiac Biomarkers in Diabetes Mellitus: A New Dawn for Risk Stratification—A Narrative Review. Diabetes Therapy 2020, 11, 1271–1291. [Google Scholar] [CrossRef] [PubMed]
- Olcha, P.; Winiarska-Mieczan, A.; Kwiecień, M.; Nowakowski, Ł.; Miturski, A.; Semczuk, A.; Kiczorowska, B.; Gałczyński, K. Antioxidative, anti-inflammatory, anti-obesogenic, and antidiabetic properties of tea polyphenols—The positive impact of regular tea consumption as an element of prophylaxis and pharmacotherapy support in endometrial cancer. International Journal of Molecular Sciences 2022, 23, 6703. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Zhang, S.; Wang, L.; Pan, T.; Zhong, X. The relationship between red blood cell distribution and islet β-cell function indexes in patients with type 2 diabetes. BMC Endocrine Disorders 2021, 21, 7. [Google Scholar] [CrossRef] [PubMed]
- Torres-Zegarra, C.; Sundararajan, D.; Benson, J.; Seagle, H.; Witten, M.; Walders-Abramson, N.; Simon, S.; Huguelet, P.; Nokoff, N.; Cree-Green, M. Care for adolescents with polycystic ovary syndrome: development and prescribing patterns of a multidisciplinary clinic. Journal of pediatric and adolescent gynecology 2021, 34, 617–625. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Deng, X.; Zhou, J.; Qiu, K.; Deng, M.; Lin, Z.; Mosha, S.S.; Li, W. The association of serum cortisol level with microalbuminuria in patients with type 2 diabetes and prediabetes. International journal of medical sciences 2020, 17, 2998. [Google Scholar] [CrossRef] [PubMed]
- Janssen, J.A. Hyperinsulinemia and its pivotal role in aging, obesity, type 2 diabetes, cardiovascular disease and cancer. International Journal of Molecular Sciences 2021, 22, 7797. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, C.J.; Veras, K.; de Oliveira Carvalho, C.R. Dehydroepiandrosterone on metabolism and the cardiovascular system in the postmenopausal period. Journal of Molecular Medicine 2020, 98, 39–57. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.; Chen, L.-R.; Chen, K.-H. The Utilization of dehydroepiandrosterone as a sexual hormone precursor in premenopausal and postmenopausal women: An overview. Pharmaceuticals 2021, 15, 46. [Google Scholar] [CrossRef] [PubMed]
- Cappola, A.R.; Auchus, R.J.; El-Hajj Fuleihan, G.; Handelsman, D.J.; Kalyani, R.R.; McClung, M.; Stuenkel, C.A.; Thorner, M.O.; Verbalis, J.G. Hormones and Aging: An Endocrine Society Scientific Statement. The Journal of Clinical Endocrinology & Metabolism 2023, dgad225. [Google Scholar]
- Salonia, A.; Rastrelli, G.; Hackett, G.; Seminara, S.B.; Huhtaniemi, I.T.; Rey, R.A.; Hellstrom, W.J.; Palmert, M.R.; Corona, G.; Dohle, G.R. Paediatric and adult-onset male hypogonadism. Nature reviews Disease primers 2019, 5, 38. [Google Scholar] [CrossRef] [PubMed]
- Hur, M.-H.; Hong, J.H.; Yeo, S. Effects of aromatherapy on stress, fructosamine, fatigue, and sleep quality in prediabetic middle-aged women: a randomised controlled trial. European Journal of Integrative Medicine 2019, 31, 100978. [Google Scholar] [CrossRef]
- Bartz, D.; Chitnis, T.; Kaiser, U.B.; Rich-Edwards, J.W.; Rexrode, K.M.; Pennell, P.B.; Goldstein, J.M.; O’Neal, M.A.; LeBoff, M.; Behn, M. Clinical advances in sex-and gender-informed medicine to improve the health of all: a review. JAMA internal medicine 2020, 180, 574–583. [Google Scholar] [CrossRef] [PubMed]
- Qi, X.; Yun, C.; Pang, Y.; Qiao, J. The impact of the gut microbiota on the reproductive and metabolic endocrine system. Gut Microbes 2021, 13, 1894070. [Google Scholar] [CrossRef] [PubMed]
- Spinelli, R.; Parrillo, L.; Longo, M.; Florese, P.; Desiderio, A.; Zatterale, F.; Miele, C.; Raciti, G.A.; Beguinot, F. Molecular basis of ageing in chronic metabolic diseases. Journal of Endocrinological Investigation 2020, 43, 1373–1389. [Google Scholar] [CrossRef] [PubMed]
- Lavillegrand, J.-R.; Garnier, M.; Spaeth, A.; Mario, N.; Hariri, G.; Pilon, A.; Berti, E.; Fieux, F.; Thietart, S.; Urbina, T. Elevated plasma IL-6 and CRP levels are associated with adverse clinical outcomes and death in critically ill SARS-CoV-2 patients: inflammatory response of SARS-CoV-2 patients. Annals of Intensive Care 2021, 11, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Berlanga-Acosta, J.A.; Guillén-Nieto, G.E.; Rodríguez-Rodríguez, N.; Mendoza-Mari, Y.; Bringas-Vega, M.L.; Berlanga-Saez, J.O.; García del Barco Herrera, D.; Martinez-Jimenez, I.; Hernandez-Gutierrez, S.; Valdés-Sosa, P.A. Cellular senescence as the pathogenic hub of diabetes-related wound chronicity. Frontiers in Endocrinology 2020, 11, 573032. [Google Scholar] [CrossRef] [PubMed]
- Oguntibeju, O.O. Type 2 diabetes mellitus, oxidative stress and inflammation: examining the links. International journal of physiology, pathophysiology and pharmacology 2019, 11, 45. [Google Scholar] [PubMed]
- Szűcs, G.; Sója, A.; Péter, M.; Sárközy, M.; Bruszel, B.; Siska, A.; Földesi, I.; Szabó, Z.; Janáky, T.; Vígh, L. Prediabetes induced by fructose-enriched diet influences cardiac lipidome and proteome and leads to deterioration of cardiac function prior to the development of excessive oxidative stress and cell damage. Oxidative Medicine and Cellular Longevity 2019, 2019. [Google Scholar] [CrossRef] [PubMed]
- Peña, A.; Olson, M.L.; Ayers, S.L.; Sears, D.D.; Vega-López, S.; Colburn, A.T.; Shaibi, G.Q. Inflammatory Mediators and Type 2 Diabetes Risk Factors before and in Response to Lifestyle Intervention among Latino Adolescents with Obesity. Nutrients 2023, 15, 2442. [Google Scholar] [CrossRef] [PubMed]
- Teissier, T.; Boulanger, E.; Cox, L.S. Interconnections between Inflammageing and Immunosenescence during Ageing. Cells 2022, 11. [Google Scholar] [CrossRef] [PubMed]
- Pan, X.; Kaminga, A.C.; Wen, S.W.; Liu, A. Chemokines in Prediabetes and Type 2 Diabetes: A Meta-Analysis. Front Immunol 2021, 12, 622438. [Google Scholar] [CrossRef] [PubMed]
- Avramovic, D.; Archaimbault, S.A.; Kemble, A.M.; Gruener, S.; Lazendic, M.; Westenskow, P.D. TGFβ1 Induces Senescence and Attenuated VEGF Production in Retinal Pericytes. Biomedicines 2022, 10, 1404. [Google Scholar] [CrossRef] [PubMed]
- Tan, Q.; Liang, N.; Zhang, X.; Li, J. Dynamic Aging: Channeled Through Microenvironment. Front Physiol 2021, 12, 702276. [Google Scholar] [CrossRef] [PubMed]
- Yuan, T.; Yang, T.; Chen, H.; Fu, D.; Hu, Y.; Wang, J.; Yuan, Q.; Yu, H.; Xu, W.; Xie, X. New insights into oxidative stress and inflammation during diabetes mellitus-accelerated atherosclerosis. Redox Biology 2019, 20, 247–260. [Google Scholar] [CrossRef] [PubMed]
- An, Y.; Xu, B.-t.; Wan, S.-r.; Ma, X.-m.; Long, Y.; Xu, Y.; Jiang, Z.-z. The role of oxidative stress in diabetes mellitus-induced vascular endothelial dysfunction. Cardiovascular Diabetology 2023, 22, 237. [Google Scholar] [CrossRef] [PubMed]
- Khalil, R.; Diab-Assaf, M.; Lemaitre, J.-M. Emerging Therapeutic Approaches to Target the Dark Side of Senescent Cells: New Hopes to Treat Aging as a Disease and to Delay Age-Related Pathologies. Cells 2023, 12, 915. [Google Scholar] [CrossRef] [PubMed]
- Amorim, J.A.; Coppotelli, G.; Rolo, A.P.; Palmeira, C.M.; Ross, J.M.; Sinclair, D.A. Mitochondrial and metabolic dysfunction in ageing and age-related diseases. Nat Rev Endocrinol 2022, 18, 243–258. [Google Scholar] [CrossRef] [PubMed]
- Drake, A.M.; Coughlan, M.T.; Christophersen, C.T.; Snelson, M. Resistant starch as a dietary intervention to limit the progression of diabetic kidney disease. Nutrients 2022, 14, 4547. [Google Scholar] [CrossRef] [PubMed]
- Liberale, L.; Montecucco, F.; Tardif, J.-C.; Libby, P.; Camici, G.G. Inflamm-ageing: the role of inflammation in age-dependent cardiovascular disease. European heart journal 2020, 41, 2974–2982. [Google Scholar] [CrossRef] [PubMed]
- Dinarello, C.A. The IL-1 family of cytokines and receptors in rheumatic diseases. Nature Reviews Rheumatology 2019, 15, 612–632. [Google Scholar] [CrossRef] [PubMed]
- Elimam, H.; Abdulla, A.M.; Taha, I.M. Inflammatory markers and control of type 2 diabetes mellitus. Diabetes & Metabolic Syndrome: Clinical Research & Reviews 2019, 13, 800–804. [Google Scholar]
- Angulo, J.; El Assar, M.; Álvarez-Bustos, A.; Rodríguez-Mañas, L. Physical activity and exercise: Strategies to manage frailty. Redox biology 2020, 35, 101513. [Google Scholar] [CrossRef] [PubMed]
- Bhatti, J.S.; Sehrawat, A.; Mishra, J.; Sidhu, I.S.; Navik, U.; Khullar, N.; Kumar, S.; Bhatti, G.K.; Reddy, P.H. Oxidative stress in the pathophysiology of type 2 diabetes and related complications: Current therapeutics strategies and future perspectives. Free Radical Biology and Medicine 2022, 184, 114–134. [Google Scholar] [CrossRef] [PubMed]
- Halim, M.; Halim, A. The effects of inflammation, aging and oxidative stress on the pathogenesis of diabetes mellitus (type 2 diabetes). Diabetes & metabolic syndrome: clinical research & reviews 2019, 13, 1165–1172. [Google Scholar]
- Sivandzade, F.; Prasad, S.; Bhalerao, A.; Cucullo, L. NRF2 and NF-қB interplay in cerebrovascular and neurodegenerative disorders: molecular mechanisms and possible therapeutic approaches. Redox biology 2019, 21, 101059. [Google Scholar] [CrossRef] [PubMed]
- Narasimhan, A.; Flores, R.R.; Robbins, P.D.; Niedernhofer, L.J. Role of cellular senescence in type II diabetes. Endocrinology 2021, 162, bqab136. [Google Scholar] [CrossRef] [PubMed]
- Furman, D.; Campisi, J.; Verdin, E.; Carrera-Bastos, P.; Targ, S.; Franceschi, C.; Ferrucci, L.; Gilroy, D.W.; Fasano, A.; Miller, G.W. Chronic inflammation in the etiology of disease across the life span. Nature medicine 2019, 25, 1822–1832. [Google Scholar] [CrossRef] [PubMed]
- Zabetakis, I.; Lordan, R.; Tsoupras, A. The impact of nutrition and statins on cardiovascular diseases; Academic Press: 2019.
- Lainampetch, J.; Panprathip, P.; Phosat, C.; Chumpathat, N.; Prangthip, P.; Soonthornworasiri, N.; Puduang, S.; Wechjakwen, N.; Kwanbunjan, K. Association of tumor necrosis factor alpha, interleukin 6, and C-reactive protein with the risk of developing type 2 diabetes: a retrospective cohort study of rural Thais. Journal of diabetes research 2019, 2019. [Google Scholar] [CrossRef] [PubMed]
- Randeria, S.N.; Thomson, G.J.; Nell, T.A.; Roberts, T.; Pretorius, E. Inflammatory cytokines in type 2 diabetes mellitus as facilitators of hypercoagulation and abnormal clot formation. Cardiovascular diabetology 2019, 18, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Moshapa, F.T.; Riches-Suman, K.; Palmer, T.M. Therapeutic targeting of the proinflammatory IL-6-JAK/STAT signalling pathways responsible for vascular restenosis in type 2 diabetes mellitus. Cardiology research and practice 2019, 2019. [Google Scholar] [CrossRef] [PubMed]
- Chi, C.; Li, D.-J.; Jiang, Y.-J.; Tong, J.; Fu, H.; Wu, Y.-H.; Shen, F.-M. Vascular smooth muscle cell senescence and age-related diseases: State of the art. Biochimica et Biophysica Acta (BBA)-Molecular Basis of Disease 2019, 1865, 1810–1821. [Google Scholar] [CrossRef] [PubMed]
- de la Cruz-Ares, S.; Cardelo, M.P.; Gutiérrez-Mariscal, M.F.; Torres-Peña, J.D.; García-Rios, A.; Katsiki, N.; Malagón, M.M.; López-Miranda, J.; Pérez-Martínez, P.; Yubero-Serrano, M.E. Endothelial dysfunction and advanced glycation end products in patients with newly diagnosed versus established diabetes: from the CORDIOPREV study. Nutrients 2020, 12, 238. [Google Scholar] [CrossRef] [PubMed]
- Biswas, I.; Khan, G.A. Endothelial dysfunction in cardiovascular diseases. Basic Clin Underst Microcirc 2020, 10. [Google Scholar]
- Meza, C.A.; La Favor, J.D.; Kim, D.-H.; Hickner, R.C. Endothelial dysfunction: is there a hyperglycemia-induced imbalance of NOX and NOS? International journal of molecular sciences 2019, 20, 3775. [Google Scholar] [CrossRef] [PubMed]
- Marseglia, A.; Fratiglioni, L.; Kalpouzos, G.; Wang, R.; Bäckman, L.; Xu, W. Prediabetes and diabetes accelerate cognitive decline and predict microvascular lesions: a population-based cohort study. Alzheimer's & Dementia 2019, 15, 25–33. [Google Scholar]
- Yan, C.; Zhou, Y.; Chen, Q.; Luo, Y.; Zhang, J.H.; Huang, H.; Shao, A. Dysfunction of the neurovascular unit in diabetes-related neurodegeneration. Biomedicine & Pharmacotherapy 2020, 131, 110656. [Google Scholar]
- Moheet, A.; Mangia, S.; Seaquist, E.R. Impact of diabetes on cognitive function and brain structure. Ann N Y Acad Sci 2015, 1353, 60–71. [Google Scholar] [CrossRef] [PubMed]
- Vecoli, C.; Borghini, A.; Andreassi, M.G. The molecular biomarkers of vascular aging and atherosclerosis: telomere length and mitochondrial DNA4977 common deletion. Mutation Research/Reviews in Mutation Research 2020, 784, 108309. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, A.L.; Fernandes, A.; Aguilar-Pimentel, J.A.; de Angelis, M.H.; Guedes, J.R.; Brito, M.A.; Ortolano, S.; Pani, G.; Athanasopoulou, S.; Gonos, E.S.; et al. Towards frailty biomarkers: Candidates from genes and pathways regulated in aging and age-related diseases. Ageing Research Reviews 2018, 47, 214–277. [Google Scholar] [CrossRef] [PubMed]
- Prašnikar, E.; Borišek, J.; Perdih, A. Senescent cells as promising targets to tackle age-related diseases. Ageing Research Reviews 2021, 66, 101251. [Google Scholar] [CrossRef] [PubMed]
- Yeh, S.H.-H.; Shie, F.-S.; Liu, H.-K.; Yao, H.-H.; Kao, P.-C.; Lee, Y.-H.; Chen, L.-M.; Hsu, S.-M.; Chao, L.-J.; Wu, K.-W. A high-sucrose diet aggravates Alzheimer's disease pathology, attenuates hypothalamic leptin signaling, and impairs food-anticipatory activity in APPswe/PS1dE9 mice. Neurobiology of Aging 2020, 90, 60–74. [Google Scholar] [CrossRef] [PubMed]
- Kim, O.Y.; Song, J. The importance of BDNF and RAGE in diabetes-induced dementia. Pharmacological research 2020, 160, 105083. [Google Scholar] [CrossRef] [PubMed]
- Sankar, S.B.; Infante-Garcia, C.; Weinstock, L.D.; Ramos-Rodriguez, J.J.; Hierro-Bujalance, C.; Fernandez-Ponce, C.; Wood, L.B.; Garcia-Alloza, M. Amyloid beta and diabetic pathology cooperatively stimulate cytokine expression in an Alzheimer’s mouse model. Journal of neuroinflammation 2020, 17, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Infante-Garcia, C.; Garcia-Alloza, M. Review of the effect of natural compounds and extracts on neurodegeneration in animal models of diabetes mellitus. International journal of molecular sciences 2019, 20, 2533. [Google Scholar] [CrossRef] [PubMed]
- Maneechote, C.; Kerdphoo, S.; Jaiwongkam, T.; Chattipakorn, S.C.; Chattipakorn, N. Chronic Pharmacological Modulation of Mitochondrial Dynamics Alleviates Prediabetes-Induced Myocardial Ischemia–Reperfusion Injury by Preventing Mitochondrial Dysfunction and Programmed Apoptosis. Cardiovascular Drugs and Therapy 2021, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Balistreri, C.R.; Pisano, C.; Bertoldo, F.; Massoud, R.; Dolci, S.; Ruvolo, G. Red Blood Cell Distribution Width, Vascular Aging Biomarkers, and Endothelial Progenitor Cells for Predicting Vascular Aging and Diagnosing/Prognosing Age-Related Degenerative Arterial Diseases. Rejuvenation Res 2019, 22, 399–408. [Google Scholar] [CrossRef] [PubMed]
- Pinna, A.; Carlino, P.; Serra, R.; Boscia, F.; Dore, S.; Carru, C.; Zinellu, A. Red Cell Distribution Width (RDW) and Complete Blood Cell Count-Derived Measures in Non-Arteritic Anterior Ischemic Optic Neuropathy. Int J Med Sci 2021, 18, 2239–2244. [Google Scholar] [CrossRef] [PubMed]
- Gratuze, M.; Joly-Amado, A.; Buee, L.; Vieau, D.; Blum, D. Overview on Tau and Tauopathies. Tau Biology 2020, 1184, 259. [Google Scholar]
- Powrie, Y.S.L.; Smith, C. Central intracrine DHEA synthesis in ageing-related neuroinflammation and neurodegeneration: therapeutic potential? Journal of Neuroinflammation 2018, 15, 289. [Google Scholar] [CrossRef] [PubMed]
- Thonusin, C.; Pantiya, P.; Sumneang, N.; Chunchai, T.; Nawara, W.; Arunsak, B.; Siri-Angkul, N.; Sriwichaiin, S.; Chattipakorn, S.C.; Chattipakorn, N. Effectiveness of high cardiorespiratory fitness in cardiometabolic protection in prediabetic rats. Molecular Medicine 2022, 28, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Rettberg, J.R.; Yao, J.; Brinton, R.D. Estrogen: a master regulator of bioenergetic systems in the brain and body. Front Neuroendocrinol 2014, 35, 8–30. [Google Scholar] [CrossRef] [PubMed]
- Deng, J.; Yan, F.; Tian, J.; Qiao, A.; Yan, D. Potential clinical biomarkers and perspectives in diabetic cardiomyopathy. Diabetology & Metabolic Syndrome 2023, 15, 35. [Google Scholar] [CrossRef]
- Carranza-Naval, M.J.; Vargas-Soria, M.; Hierro-Bujalance, C.; Baena-Nieto, G.; Garcia-Alloza, M.; Infante-Garcia, C.; Del Marco, A. Alzheimer’s disease and diabetes: Role of diet, microbiota and inflammation in preclinical models. Biomolecules 2021, 11, 262. [Google Scholar] [CrossRef] [PubMed]
- Meng, J.-M.; Cao, S.-Y.; Wei, X.-L.; Gan, R.-Y.; Wang, Y.-F.; Cai, S.-X.; Xu, X.-Y.; Zhang, P.-Z.; Li, H.-B. Effects and mechanisms of tea for the prevention and management of diabetes mellitus and diabetic complications: An updated review. Antioxidants 2019, 8, 170. [Google Scholar] [CrossRef] [PubMed]
- Carrageta, D.F.; Dias, T.R.; Alves, M.G.; Oliveira, P.F.; Monteiro, M.P.; Silva, B.M. Anti-obesity potential of natural methylxanthines. Journal of Functional Foods 2018, 43, 84–94. [Google Scholar] [CrossRef]
- Biessels, G.J.; Despa, F. Cognitive decline and dementia in diabetes mellitus: mechanisms and clinical implications. Nature Reviews Endocrinology 2018, 14, 591–604. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Jahrling, J.B.; Denner, L.; Dineley, K.T. Targeting insulin for Alzheimer’s disease: mechanisms, status and potential directions. Journal of Alzheimer's Disease 2018, 64, S427–S453. [Google Scholar] [CrossRef] [PubMed]
- van Duinkerken, E.; Ryan, C.M. Diabetes mellitus in the young and the old: Effects on cognitive functioning across the life span. Neurobiology of disease 2020, 134, 104608. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Wang, J.; Chao, C.T.; Chien, K.L.; Huang, J.W. Frailty is associated with a higher risk of developing delirium and cognitive impairment among patients with diabetic kidney disease: A longitudinal population-based cohort study. Diabetic Medicine 2021, 38, e14566. [Google Scholar] [CrossRef] [PubMed]
- Hayden, M.R. Type 2 diabetes mellitus increases the risk of late-onset Alzheimer’s disease: ultrastructural remodeling of the neurovascular unit and diabetic gliopathy. Brain sciences 2019, 9, 262. [Google Scholar] [CrossRef] [PubMed]
- Horton, W.B.; Barrett, E.J. Microvascular Dysfunction in Diabetes Mellitus and Cardiometabolic Disease. Endocr Rev 2021, 42, 29–55. [Google Scholar] [CrossRef] [PubMed]
- Silveira, A.C.; Dias, J.P.; Santos, V.M.; Oliveira, P.F.; Alves, M.G.; Rato, L.; Silva, B.M. The action of polyphenols in diabetes mellitus and Alzheimer's disease: a common agent for overlapping pathologies. Current Neuropharmacology 2019, 17, 590–613. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.S.H.; Hegde, V. Obesity and diabetes mediated chronic inflammation: a potential biomarker in Alzheimer’s disease. Journal of personalized medicine 2020, 10, 42. [Google Scholar] [CrossRef] [PubMed]
- Krivanek, T.J.; Gale, S.A.; McFeeley, B.M.; Nicastri, C.M.; Daffner, K.R. Promoting successful cognitive aging: a ten-year update. Journal of Alzheimer's Disease 2021, 81, 871–920. [Google Scholar] [CrossRef] [PubMed]
- Khalid, M.; Petroianu, G.; Adem, A. Advanced glycation end products and diabetes mellitus: Mechanisms and perspectives. Biomolecules 2022, 12, 542. [Google Scholar] [CrossRef] [PubMed]
- Medina-Leyte, D.J.; Zepeda-García, O.; Domínguez-Pérez, M.; González-Garrido, A.; Villarreal-Molina, T.; Jacobo-Albavera, L. Endothelial dysfunction, inflammation and coronary artery disease: potential biomarkers and promising therapeutical approaches. International journal of molecular sciences 2021, 22, 3850. [Google Scholar] [CrossRef] [PubMed]
- Ashby, J.W.; Mack, J.J. Endothelial control of cerebral blood flow. The American Journal of Pathology 2021, 191, 1906–1916. [Google Scholar] [CrossRef] [PubMed]
- Theofilis, P.; Sagris, M.; Oikonomou, E.; Antonopoulos, A.S.; Siasos, G.; Tsioufis, C.; Tousoulis, D. Inflammatory mechanisms contributing to endothelial dysfunction. Biomedicines 2021, 9, 781. [Google Scholar] [CrossRef] [PubMed]
- Coco, C.; Sgarra, L.; Potenza, M.A.; Nacci, C.; Pasculli, B.; Barbano, R.; Parrella, P.; Montagnani, M. Can epigenetics of endothelial dysfunction represent the key to precision medicine in type 2 diabetes mellitus? International Journal of Molecular Sciences 2019, 20, 2949. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.; Jaggers, R.M.; Gopalkrishna, S.; Dahdah, A.; Murphy, A.J.; Hanssen, N.M.; Nagareddy, P.R. Oxidative stress in neutrophils: implications for diabetic cardiovascular complications. Antioxidants & redox signaling 2022, 36, 652–666. [Google Scholar]
- Stanimirovic, J.; Radovanovic, J.; Banjac, K.; Obradovic, M.; Essack, M.; Zafirovic, S.; Gluvic, Z.; Gojobori, T.; Isenovic, E.R. Role of C-reactive protein in diabetic inflammation. Mediators of Inflammation 2022, 2022. [Google Scholar] [CrossRef] [PubMed]
- Forrester, J.V.; Kuffova, L.; Delibegovic, M. The role of inflammation in diabetic retinopathy. Frontiers in immunology 2020, 11, 583687. [Google Scholar] [CrossRef] [PubMed]
- Landecho, M.F.; Tuero, C.; Valentí, V.; Bilbao, I.; de la Higuera, M.; Frühbeck, G. Relevance of leptin and other adipokines in obesity-associated cardiovascular risk. Nutrients 2019, 11, 2664. [Google Scholar] [CrossRef] [PubMed]
- Placha, D.; Jampilek, J. Chronic inflammatory diseases, anti-inflammatory agents and their delivery nanosystems. Pharmaceutics 2021, 13, 64. [Google Scholar] [CrossRef] [PubMed]
- Zatterale, F.; Longo, M.; Naderi, J.; Raciti, G.A.; Desiderio, A.; Miele, C.; Beguinot, F. Chronic adipose tissue inflammation linking obesity to insulin resistance and type 2 diabetes. Frontiers in physiology 2020, 10, 1607. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, R.; Viana, S.D.; Nunes, S.; Reis, F. Diabetic gut microbiota dysbiosis as an inflammaging and immunosenescence condition that fosters progression of retinopathy and nephropathy. Biochimica Et Biophysica Acta (BBA)-Molecular Basis of Disease 2019, 1865, 1876–1897. [Google Scholar] [CrossRef] [PubMed]
- Kistner, T.M.; Pedersen, B.K.; Lieberman, D.E. Interleukin 6 as an energy allocator in muscle tissue. Nature metabolism 2022, 4, 170–179. [Google Scholar] [CrossRef] [PubMed]
- Battineni, G.; Sagaro, G.G.; Chintalapudi, N.; Amenta, F.; Tomassoni, D.; Tayebati, S.K. Impact of obesity-induced inflammation on cardiovascular diseases (CVD). International Journal of Molecular Sciences 2021, 22, 4798. [Google Scholar] [CrossRef] [PubMed]
- Bashir, H.; Bhat, S.A.; Majid, S.; Hamid, R.; Koul, R.K.; Rehman, M.U.; Din, I.; Bhat, J.A.; Qadir, J.; Masood, A. Role of inflammatory mediators (TNF-α, IL-6, CRP), biochemical and hematological parameters in type 2 diabetes mellitus patients of Kashmir, India. Medical journal of the Islamic Republic of Iran 2020, 34, 5. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, L.J.H.; Petersen, J.E.V.; Eugen-Olsen, J. Soluble urokinase plasminogen activator receptor (suPAR) as a biomarker of systemic chronic inflammation. Frontiers in immunology 2021, 12, 780641. [Google Scholar] [CrossRef] [PubMed]
- Podkowińska, A.; Formanowicz, D. Chronic kidney disease as oxidative stress-and inflammatory-mediated cardiovascular disease. Antioxidants 2020, 9, 752. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Kukreti, R.; Saso, L.; Kukreti, S. Mechanistic insight into oxidative stress-triggered signaling pathways and type 2 diabetes. Molecules 2022, 27, 950. [Google Scholar] [CrossRef] [PubMed]
- Aleksandrova, K.; Koelman, L.; Rodrigues, C.E. Dietary patterns and biomarkers of oxidative stress and inflammation: A systematic review of observational and intervention studies. Redox biology 2021, 42, 101869. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.Y.; Kim, D.H.; Lee, E.K.; Chung, K.W.; Chung, S.; Lee, B.; Seo, A.Y.; Chung, J.H.; Jung, Y.S.; Im, E. Redefining chronic inflammation in aging and age-related diseases: proposal of the senoinflammation concept. Aging and disease 2019, 10, 367. [Google Scholar] [CrossRef] [PubMed]
- Boyajian, J.L.; Ghebretatios, M.; Schaly, S.; Islam, P.; Prakash, S. Microbiome and human aging: probiotic and prebiotic potentials in longevity, skin health and cellular senescence. Nutrients 2021, 13, 4550. [Google Scholar] [CrossRef] [PubMed]
- Moura, J.; Madureira, P.; Leal, E.; Fonseca, A.; Carvalho, E. Immune aging in diabetes and its implications in wound healing. Clinical Immunology 2019, 200, 43–54. [Google Scholar] [CrossRef] [PubMed]
- Patankar, J.V.; Becker, C. Cell death in the gut epithelium and implications for chronic inflammation. Nature Reviews Gastroenterology & Hepatology 2020, 17, 543–556. [Google Scholar]
- Burgess, J.L.; Wyant, W.A.; Abdo Abujamra, B.; Kirsner, R.S.; Jozic, I. Diabetic Wound-Healing Science. Medicina (Kaunas) 2021, 57. [Google Scholar] [CrossRef] [PubMed]
- Luo, G.; Wosinski, P.; Salazar-Noratto, G.E.; Bensidhoum, M.; Bizios, R.; Marashi, S.-A.; Potier, E.; Sheng, P.; Petite, H. Glucose Metabolism: Optimizing Regenerative Functionalities of Mesenchymal Stromal Cells Postimplantation. Tissue Engineering Part B: Reviews 2023, 29, 47–61. [Google Scholar] [CrossRef] [PubMed]
- Dubey, P.; Thakur, V.; Chattopadhyay, M. Role of minerals and trace elements in diabetes and insulin resistance. Nutrients 2020, 12, 1864. [Google Scholar] [CrossRef] [PubMed]
- Prasun, P. Mitochondrial dysfunction in metabolic syndrome. Biochimica et Biophysica Acta (BBA)-Molecular Basis of Disease 2020, 1866, 165838. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Wu, K.K.; Jiang, X.; Xu, A.; Cheng, K.K. The role of adipose tissue senescence in obesity-and ageing-related metabolic disorders. Clinical science 2020, 134, 315–330. [Google Scholar] [CrossRef] [PubMed]
- Madan, S.; Uttekar, B.; Chowdhary, S.; Rikhy, R. Mitochondria lead the way: Mitochondrial dynamics and function in cellular movements in development and disease. Frontiers in Cell and Developmental Biology 2022, 9, 781933. [Google Scholar] [CrossRef] [PubMed]
- Teodoro, J.S.; Nunes, S.; Rolo, A.P.; Reis, F.; Palmeira, C.M. Therapeutic options targeting oxidative stress, mitochondrial dysfunction and inflammation to hinder the progression of vascular complications of diabetes. Frontiers in physiology 2019, 9, 1857. [Google Scholar] [CrossRef] [PubMed]
- Pinti, M.V.; Fink, G.K.; Hathaway, Q.A.; Durr, A.J.; Kunovac, A.; Hollander, J.M. Mitochondrial dysfunction in type 2 diabetes mellitus: an organ-based analysis. American Journal of Physiology-Endocrinology and Metabolism 2019. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, J.P.; Lamiral, Z.; Bakris, G.; Mehta, C.; White, W.B.; Zannad, F. Red cell distribution width in patients with diabetes and myocardial infarction: an analysis from the EXAMINE trial. Diabetes, Obesity and Metabolism 2021, 23, 1580–1587. [Google Scholar] [CrossRef] [PubMed]
- Arkew, M.; Gemechu, K.; Haile, K.; Asmerom, H. Red blood cell distribution width as novel biomarker in cardiovascular diseases: a literature review. Journal of Blood Medicine 2022, 413–424. [Google Scholar] [CrossRef] [PubMed]
- Kavvasoglu, B.; Akdemir, S.; Kurt, M. A routine but overlooked parameter for impaired glucose control: red cell distribution width. Eur Rev Med Pharmacol Sci 2022, 26, 2431–2436. [Google Scholar] [PubMed]
- Zhou, W.; Sailani, M.R.; Contrepois, K.; Zhou, Y.; Ahadi, S.; Leopold, S.R.; Zhang, M.J.; Rao, V.; Avina, M.; Mishra, T. Longitudinal multi-omics of host–microbe dynamics in prediabetes. Nature 2019, 569, 663–671. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, A.; Deng, Y.; Lane, A.; Benkeser, D.; Cui, X.; Staimez, L.; Ford, C.; Khan, F.; Markley Webster, S.; Leong, A. Impact of mismatches in HbA1c vs glucose values on the diagnostic classification of diabetes and prediabetes. Diabetic Medicine 2020, 37, 689–696. [Google Scholar] [CrossRef] [PubMed]
- Beck, R.W.; Bergenstal, R.M.; Cheng, P.; Kollman, C.; Carlson, A.L.; Johnson, M.L.; Rodbard, D. The relationships between time in range, hyperglycemia metrics, and HbA1c. Journal of diabetes science and technology 2019, 13, 614–626. [Google Scholar] [CrossRef] [PubMed]
- Kesika, P.; Sivamaruthi, B.S.; Chaiyasut, C. Do probiotics improve the health status of individuals with diabetes mellitus? A review on outcomes of clinical trials. BioMed research international 2019, 2019. [Google Scholar] [CrossRef] [PubMed]
- Yanagita, I.; Fujihara, Y.; Iwaya, C.; Kitajima, Y.; Tajima, M.; Honda, M.; Teruya, Y.; Asakawa, H.; Ito, T.; Eda, T. Low serum albumin, aspartate aminotransferase, and body mass are risk factors for frailty in elderly people with diabetes–a cross-sectional study. BMC geriatrics 2020, 20, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Ismail, M.T.; Elbaih, A.H. Principles of intravenous fluids therapy. EC Emerg Med Critical Care 2020, 4, 24–46. [Google Scholar]
- Petroni, M.L.; Brodosi, L.; Marchignoli, F.; Sasdelli, A.S.; Caraceni, P.; Marchesini, G.; Ravaioli, F. Nutrition in patients with type 2 diabetes: Present knowledge and remaining challenges. Nutrients 2021, 13, 2748. [Google Scholar] [CrossRef] [PubMed]
- Barbagallo, M.; Veronese, N.; Dominguez, L.J. Magnesium in aging, health and diseases. Nutrients 2021, 13, 463. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Maxwell, C.A.; Yu, F. Biological processes and biomarkers related to frailty in older adults: a state-of-the-science literature review. Biological research for nursing 2019, 21, 80–106. [Google Scholar] [CrossRef] [PubMed]
- Boachie, J.; Adaikalakoteswari, A.; Samavat, J.; Saravanan, P. Low vitamin B12 and lipid metabolism: evidence from pre-clinical and clinical studies. Nutrients 2020, 12, 1925. [Google Scholar] [CrossRef] [PubMed]
- Tiwari, V.; Wilson, D.M. DNA damage and associated DNA repair defects in disease and premature aging. The American Journal of Human Genetics 2019, 105, 237–257. [Google Scholar] [CrossRef] [PubMed]
- Andes, L.J.; Cheng, Y.J.; Rolka, D.B.; Gregg, E.W.; Imperatore, G. Prevalence of prediabetes among adolescents and young adults in the United States, 2005-2016. JAMA pediatrics 2020, 174, e194498. [Google Scholar] [CrossRef] [PubMed]
- Dhar, G.A.; Saha, S.; Mitra, P.; Nag Chaudhuri, R. DNA methylation and regulation of gene expression: Guardian of our health. The Nucleus 2021, 64, 259–270. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Wang, J.; Wang, L.; Gao, Y.; Feng, G.; Li, G.; Zou, J.; Yu, M.; Li, Y.F.; Liu, C. Lipid metabolism dysfunction induced by age-dependent DNA methylation accelerates aging. Signal Transduction and Targeted Therapy 2022, 7, 162. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Qi, C.; Zheng, C.; Gan, K.; Ren, L.; Song, G. Effects of glycated hemoglobin level on bone metabolism biomarkers in patients with type 2 diabetes mellitus. Diabetes, Metabolic Syndrome and Obesity 2020, 1785–1791. [Google Scholar] [CrossRef] [PubMed]
- Bellido, T.; Plotkin, L.I.; Bruzzaniti, A. Bone cells. In Basic and applied bone biology; Elsevier, 2019; pp. 37–55. [Google Scholar]
- Costantini, S.; Conte, C. Bone health in diabetes and prediabetes. World journal of diabetes 2019, 10, 421. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-M.; Lin, C.; Stavre, Z.; Greenblatt, M.B.; Shim, J.-H. Osteoblast-osteoclast communication and bone homeostasis. Cells 2020, 9, 2073. [Google Scholar] [CrossRef] [PubMed]
- Anabtawi, A.; Le, T.; Putman, M.; Tangpricha, V.; Bianchi, M.L. Cystic fibrosis bone disease: Pathophysiology, assessment and prognostic implications. Journal of Cystic Fibrosis 2019, 18, S48–S55. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, A.J.; Scott, D.; Ebeling, P.R. Exploring the links between common diseases of ageing—osteoporosis, sarcopenia and vascular calcification. Clinical Reviews in Bone and Mineral Metabolism 2019, 17, 1–23. [Google Scholar] [CrossRef]
- Khoramipour, K.; Chamari, K.; Hekmatikar, A.A.; Ziyaiyan, A.; Taherkhani, S.; Elguindy, N.M.; Bragazzi, N.L. Adiponectin: Structure, physiological functions, role in diseases, and effects of nutrition. Nutrients 2021, 13, 1180. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.M.D. Adiponectin: role in physiology and pathophysiology. International journal of preventive medicine 2020, 11. [Google Scholar]
- Shou, J.; Chen, P.-J.; Xiao, W.-H. Mechanism of increased risk of insulin resistance in aging skeletal muscle. Diabetology & metabolic syndrome 2020, 12, 1–10. [Google Scholar]
- Bleve, A.; Motta, F.; Durante, B.; Pandolfo, C.; Selmi, C.; Sica, A. Immunosenescence, inflammaging, and frailty: role of myeloid cells in age-related diseases. Clinical reviews in allergy & immunology 2022, 1–22. [Google Scholar]
- Sardu, C.; D’Onofrio, N.; Torella, M.; Portoghese, M.; Loreni, F.; Mureddu, S.; Signoriello, G.; Scisciola, L.; Barbieri, M.; Rizzo, M.R. Pericoronary fat inflammation and Major Adverse Cardiac Events (MACE) in prediabetic patients with acute myocardial infarction: effects of metformin. Cardiovascular Diabetology 2019, 18, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Friedman, J.M. Leptin and the endocrine control of energy balance. Nature Metabolism 2019, 1, 754–764. [Google Scholar] [CrossRef] [PubMed]
- Pereira, S.; Cline, D.L.; Glavas, M.M.; Covey, S.D.; Kieffer, T.J. Tissue-specific effects of leptin on glucose and lipid metabolism. Endocrine reviews 2021, 42, 1–28. [Google Scholar] [CrossRef] [PubMed]
- Gruzdeva, O.; Borodkina, D.; Uchasova, E.; Dyleva, Y.; Barbarash, O. Leptin resistance: underlying mechanisms and diagnosis. Diabetes, metabolic syndrome and obesity: targets and therapy 2019, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Rubio-Ruiz, M.E.; Guarner-Lans, V.; Pérez-Torres, I.; Soto, M.E. Mechanisms underlying metabolic syndrome-related sarcopenia and possible therapeutic measures. International journal of molecular sciences 2019, 20, 647. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Chen, D.; Xiu, M.; Li, J.; Zhang, X.Y. Diabetes mellitus, cognitive deficits and serum BDNF levels in chronic patients with schizophrenia: A case-control study. Journal of Psychiatric Research 2021, 134, 39–47. [Google Scholar] [CrossRef] [PubMed]
- De Vincenti, A.P.; Ríos, A.S.; Paratcha, G.; Ledda, F. Mechanisms that modulate and diversify BDNF functions: implications for hippocampal synaptic plasticity. Frontiers in cellular neuroscience 2019, 13, 135. [Google Scholar] [CrossRef] [PubMed]
- Sumbul-Sekerci, B.; Sekerci, A.; Pasin, O.; Durmus, E.; Yuksel-Salduz, Z.I. Cognition and BDNF levels in prediabetes and diabetes: A mediation analysis of a cross-sectional study. Frontiers in Endocrinology 2023, 14, 1120127. [Google Scholar] [CrossRef] [PubMed]
- Azman, K.F.; Zakaria, R. Recent advances on the role of brain-derived neurotrophic factor (BDNF) in neurodegenerative diseases. International Journal of Molecular Sciences 2022, 23, 6827. [Google Scholar] [CrossRef] [PubMed]
- Miranda, M.; Morici, J.F.; Zanoni, M.B.; Bekinschtein, P. Brain-derived neurotrophic factor: a key molecule for memory in the healthy and the pathological brain. Frontiers in cellular neuroscience 2019, 363. [Google Scholar] [CrossRef] [PubMed]
- Sebastian, M.J.; Khan, S.K.; Pappachan, J.M.; Jeeyavudeen, M.S. Diabetes and cognitive function: An evidence-based current perspective. World J Diabetes 2023, 14, 92–109. [Google Scholar] [CrossRef] [PubMed]
- Amiri, N.; Fathei, M.; Mosaferi Ziaaldini, M. Effects of resistance training on muscle strength, insulin-like growth factor-1, and insulin-like growth factor–binding protein-3 in healthy elderly subjects: a systematic review and meta-analysis of randomized controlled trials. Hormones 2021, 20, 247–257. [Google Scholar] [CrossRef] [PubMed]
- Bailes, J.; Soloviev, M. Insulin-like growth factor-1 (IGF-1) and its monitoring in medical diagnostic and in sports. Biomolecules 2021, 11, 217. [Google Scholar] [CrossRef] [PubMed]
- Vitale, G.; Pellegrino, G.; Vollery, M.; Hofland, L.J. Role of IGF-1 system in the modulation of longevity: controversies and new insights from a centenarians' perspective. Frontiers in endocrinology 2019, 10, 27. [Google Scholar] [CrossRef] [PubMed]
- Mutavdzin, S.S.; Djuric, D.M. Homocysteine and Related B Vitamins in Pre-diabetes and Diabetes Mellitus. In Biochemistry of Cardiovascular Dysfunction in Obesity; Springer, 2020; pp. 329–351. [Google Scholar]
- Moretti, R.; Giuffre, M.; Caruso, P.; Gazzin, S.; Tiribelli, C. Homocysteine in neurology: a possible contributing factor to small vessel disease. International Journal of Molecular Sciences 2021, 22, 2051. [Google Scholar] [CrossRef] [PubMed]
- Tinelli, C.; Di Pino, A.; Ficulle, E.; Marcelli, S.; Feligioni, M. Hyperhomocysteinemia as a risk factor and potential nutraceutical target for certain pathologies. Frontiers in nutrition 2019, 6, 49. [Google Scholar] [CrossRef] [PubMed]
- Sondrup, N.; Termannsen, A.-D.; Eriksen, J.N.; Hjorth, M.F.; Færch, K.; Klingenberg, L.; Quist, J.S. Effects of sleep manipulation on markers of insulin sensitivity: A systematic review and meta-analysis of randomized controlled trials. Sleep Medicine Reviews 2022, 62, 101594. [Google Scholar] [CrossRef] [PubMed]
- Alam, S.; Sarker, M.M.R.; Sultana, T.N.; Chowdhury, M.N.R.; Rashid, M.A.; Chaity, N.I.; Zhao, C.; Xiao, J.; Hafez, E.E.; Khan, S.A. Antidiabetic phytochemicals from medicinal plants: prospective candidates for new drug discovery and development. Frontiers in endocrinology 2022, 13, 800714. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, B.; Sultana, R.; Greene, M.W. Adipose tissue and insulin resistance in obese. Biomedicine & Pharmacotherapy 2021, 137, 111315. [Google Scholar]
- Kitada, M.; Ogura, Y.; Monno, I.; Koya, D. Sirtuins and type 2 diabetes: role in inflammation, oxidative stress, and mitochondrial function. Frontiers in endocrinology 2019, 10, 187. [Google Scholar] [CrossRef] [PubMed]
- Loomba, R.; Friedman, S.L.; Shulman, G.I. Mechanisms and disease consequences of nonalcoholic fatty liver disease. Cell 2021, 184, 2537–2564. [Google Scholar] [CrossRef] [PubMed]
- Kenner, B.; Chari, S.T.; Kelsen, D.; Klimstra, D.S.; Pandol, S.J.; Rosenthal, M.; Rustgi, A.K.; Taylor, J.A.; Yala, A.; Abul-Husn, N. Artificial intelligence and early detection of pancreatic cancer: 2020 summative review. Pancreas 2021, 50, 251. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Gan, D.; Lin, S.; Zhong, Y.; Chen, M.; Zou, X.; Shao, Z.; Xiao, G. Metformin in aging and aging-related diseases: Clinical applications and relevant mechanisms. Theranostics 2022, 12, 2722. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Q.; Li, J.T.; Sun, P.; Wang, L.L.; Sun, L.Z.; Pang, S.G. Effects of lifestyle interventions on glucose regulation and diabetes risk in adults with impaired glucose tolerance or prediabetes: a meta-analysis. Arch Endocrinol Metab 2022, 66, 157–167. [Google Scholar] [CrossRef] [PubMed]
- Jung, G.; Hernández-Illán, E.; Moreira, L.; Balaguer, F.; Goel, A. Epigenetics of colorectal cancer: biomarker and therapeutic potential. Nature reviews Gastroenterology & hepatology 2020, 17, 111–130. [Google Scholar]
- HAN, H. CLINICAL-COMMUNITY LINKAGE STRATEGIES. Applied Population Health Approaches for Asian American Communities 2022, 151. [Google Scholar]
- Justice, J.N.; Leng, I.; LeBrasseur, N.K.; Tchkonia, T.; Kirkland, J.L.; Mitin, N.; Liu, Y.; Kritchevsky, S.B.; Nicklas, B.J.; Ding, J. Caloric restriction intervention alters specific circulating biomarkers of the senescence-associated secretome in middle-aged and older adults with obesity and prediabetes in an 18-week randomized controlled trial. J Gerontol A Biol Sci Med Sci 2023. [Google Scholar] [CrossRef] [PubMed]
- Bönhof, G.J.; Herder, C.; Strom, A.; Papanas, N.; Roden, M.; Ziegler, D. Emerging biomarkers, tools, and treatments for diabetic polyneuropathy. Endocrine reviews 2019, 40, 153–192. [Google Scholar] [CrossRef] [PubMed]
- Ortiz-Martínez, M.; González-González, M.; Martagón, A.J.; Hlavinka, V.; Willson, R.C.; Rito-Palomares, M. Recent developments in biomarkers for diagnosis and screening of type 2 diabetes mellitus. Current Diabetes Reports 2022, 22, 95–115. [Google Scholar] [CrossRef] [PubMed]
- Green, S.; Hillersdal, L. Aging biomarkers and the measurement of health and risk. History and Philosophy of the Life Sciences 2021, 43, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Akbulut, S. An assessment of serum vitamin B12 and folate in patients with Crohn's disease. Medicine (Baltimore) 2022, 101, e31892. [Google Scholar] [CrossRef] [PubMed]
- Wu, Q.; Gao, Z.-J.; Yu, X.; Wang, P. Dietary regulation in health and disease. Signal Transduction and Targeted Therapy 2022, 7, 252. [Google Scholar] [CrossRef] [PubMed]
- Bottani, M.; Banfi, G.; Lombardi, G. The clinical potential of circulating miRNAs as biomarkers: present and future applications for diagnosis and prognosis of age-associated bone diseases. Biomolecules 2020, 10, 589. [Google Scholar] [CrossRef] [PubMed]
- Paton, B.; Suarez, M.; Herrero, P.; Canela, N. Glycosylation biomarkers associated with age-related diseases and current methods for glycan analysis. International Journal of Molecular Sciences 2021, 22, 5788. [Google Scholar] [CrossRef] [PubMed]
- Sławińska, N.; Krupa, R. Molecular Aspects of Senescence and Organismal Ageing-DNA Damage Response, Telomeres, Inflammation and Chromatin. Int J Mol Sci 2021, 22. [Google Scholar] [CrossRef] [PubMed]
- Jänig, W. The integrative action of the autonomic nervous system: neurobiology of homeostasis; Cambridge University Press, 2022. [Google Scholar]
- Strasser, B.; Wolters, M.; Weyh, C.; Krüger, K.; Ticinesi, A. The effects of lifestyle and diet on gut microbiota composition, inflammation and muscle performance in our aging society. Nutrients 2021, 13, 2045. [Google Scholar] [CrossRef] [PubMed]
Table 1.
Circulating Hormones and Growth Factors Associated with Aging in Prediabetes.
| Circulating Indicators of Aging | Dynamics during Aging | Function/Risk Factor | Reasons for the Condition | Lifespan Influence | Ref. |
|---|---|---|---|---|---|
| Growth Hormone (GH) | Altered levels | Impact on muscle mass, bone density | Insulin resistance | Influence on aging | [90] |
| Insulin-like Growth Factor 1 (IGF-1) | Variations during aging | Regulation of cell growth, repair | Metabolic changes | Potential lifespan influence | [91] |
| Dehydroepiandrosterone Sulfate (DHEA-S) | Decreased levels | Hormonal changes | Prediabetes | Aging effect | [92] |
| Testosterone (in men) | Changes in aging | Impact on muscle and bone health | Hormonal alterations | Potential influence on lifespan | [93] |
| Estrogen (in women) | Hormonal shifts during aging | Effects on bone density, cardiovascular health | Menopause and prediabetes | Aging impact | [94] |
| Circulating Growth Factors | Alterations with age | Role in cell growth, repair, and regeneration | Aging process | Lifespan variations | [95] |
| Brain-Derived Neurotrophic Factor (BDNF) | Age-related changes | Cognitive health in aging | Prediabetes and aging | Potential influence on lifespan | [96] |
| Insulin-Like Growth Factor-Binding Proteins (IGFBPs) | Age-related alterations | Modulation of IGF-1 effects | Metabolic changes | Aging and lifespan | [97] |
| Additional Factors in Aging | Dynamics during aging | Various influences on aging | Prediabetes and aging | Lifespan variations | [98] |
| Telomere Length | Shortening with age | Cellular aging indicator | Oxidative stress, inflammation | Influence on aging | [99] |
| p16INK4a | Increased levels with age | Cellular senescence regulator | Prediabetes and aging | Accelerated aging | [100] |
| Senescence-Associated Secretory Phenotype (SASP) Factors | Elevated levels with age | Impact on inflammation and biochemistry | Chronic inflammation | Aging implications | [101] |
| DNA Methylation Clocks | Accelerated aging with age | Epigenetic changes indicator | Metabolic and oxidative stress | Influence on aging | [102] |
| Advanced Glycation End Products (AGEs) | Increased levels with age | Age-related complications indicator | Glycation and oxidative stress | Accelerated aging | [64] |
| Inflammatory Markers | Elevated with age | Indicators of chronic inflammation | Prediabetes and aging | Aging and inflammation | [103,104] |
| Oxidative Stress Markers | Increased with age | Oxidative damage indicators | Prediabetes and aging | Influence on aging | [105] |
| Red Blood Cell Distribution Width (RDW) | Increased with age | Inflammation and metabolic changes indicator | Prediabetes and aging | Influence on aging | [106] |
| Hemoglobin A1c (HbA1c) | Elevated with age | Impact of hyperglycaemia on tissues and systems | Chronic hyperglycaemia | Aging and diabetes | [107] |
| Serum Albumin | Decreased with age | Nutritional status indicator | Prediabetes and aging | Influence on aging | [108] |
Table 2.
Age-associated Inflammatory Mediators in Prediabetes-Induced Senescence.
| Circulating Biomarker | Dynamics during Aging | Function/Risk Factor in Aging | Molecule Longevity Influence | Ref. |
|---|---|---|---|---|
| Inflammatory Mediators | Changes during aging | Role in chronic inflammation and aging | May influence lifespan | [122] |
| Pro-inflammatory Cytokines (e.g., IL-6) | Increased levels | Chronic inflammation and aging | May shorten lifespan | [30,123] |
| Chemokines (e.g., MCP-1) | Altered dynamics | Recruitment of immune cells, aging | May impact lifespan | [124] |
| Growth Factors (e.g., TGF-β1) | Varied with age | Modulation of cell growth, aging | Influence on lifespan | [125] |
| Senescence-Associated Secretory Phenotype (SASP) Factors | Increased with age | Promotion of inflammation and aging | May influence lifespan | [126] |
| Inflammatory Markers (e.g., CRP) | Elevated with age | Indicators of chronic inflammation | May impact lifespan | [56] |
| Oxidative Stress Markers (e.g., ROS) | Increased with age | Indicators of oxidative damage | May influence lifespan | [127] |
| Endothelial Markers (e.g., vWF) | Altered dynamics | Indicators of endothelial dysfunction | May impact lifespan | [128] |
| DNA Damage Markers (e.g., 8-OHdG) | Increased levels | Indicators of DNA damage and aging | May influence lifespan | [129] |
| Mitochondrial Dysfunction Markers (e.g., mtDNA) | Changes during aging | Indicators of impaired mitochondrial function | May impact lifespan | [130] |
| Immune System Biomarkers (e.g., CD4+ T cells) | Altered dynamics | Immune system indicators in aging | May influence lifespan | [123] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



