Submitted:
26 November 2023
Posted:
27 November 2023
You are already at the latest version
Abstract
Most abdominopelvic structures can find their way to a groin hernia. However, location, and relative fixation are important for migration. Gastric outlet obstruction (GOO) from a stom-ach-containing groin hernia (SCOGH) is exceedingly rare. In the current report, we present a 77-year-old man who presented with GOO from SCOGH to our facility. We performed a review of the literature following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) of patient presenting with SCOGH since it was first reported in 1802. Ninety-one cases of SCOGH were identified (85 inguinal and 6 femoral) over the last two centuries (1802-2023). GOO from SCOGH occurred in 48% of patients in one review and 18% in our world literature review, but initial presentation ranged from completely asymptomatic to peritonitis. Man-agement varied from entirely conservative treatment to elective hernia repair to emergent lap-arotomy. Only one case of laparoscopic management was documented. Twenty-one deaths from SCOGH were reported, with most occurring in early manuscripts (1802-1896 [n=9] and 1910-1997 [n=10]). In the recent medical era, outcomes for patients with this rare clinical presentation are satisfactory and treatment ranging from conservative, non-operative management to surgical repair should be tailored towards patients’ clinical presentation.
Keywords:
Femoral Hernia
; Amyand hernia
; Hernia of Littre
; Sliding Hernia
; Gastric volvulus
1. Introduction
With more than 20 million groin hernia repairs performed every year worldwide, this represents one of the most common operations performed by general surgeons globally [1]. It is not uncommon to find abdominopelvic organs within the groin hernia sac. Proximity, chronicity, and gravity make some organs more likely to be found within the femoral or inguinal hernia sac compared to others. A chronic indirect inguinal hernia might lead to adherence of the posterior wall of the hernia sac to an intraabdominal viscus, making that wall indistinguishable from the hernia sac. This type of hernia is called a sliding hernia [2]. Most commonly, omentum, small bowel, sigmoid colon on the left, ileocecal contents on the right, or bladder are found in sliding hernias [2,3].
Less commonly, a Meckel’s diverticulum (a hernia of Littre) [4], the inflamed appendix (an Amyand hernia) [5], or ovaries with fallopian tubes [6] can be found within the hernia sac. Other eponyms in groin hernias include a two loop incarceration of the small bowel creating a “W” configuration, termed a Maydl’s hernia [7], and an inflamed appendix within the femoral canal, called a de Garengeot hernia [8].
Exceedingly rare contents of the hernia sac include the ureter [9], transverse colon [10], the pancreas [11], and the gallbladder [12]. The spleen [13] and the uterus [14] have also been documented in inguinal hernias in newborns with congenital disorders. The stomach is also uncommonly found in groin hernias.
Given the relative fixation and lack of proximity of the stomach to the groin, it is extremely rare to find it within the groin hernial contents. Thus, stomach-containing groin hernias (SCOGH) have uncommonly been reported in the literature with less than one hundred cases since it was initially documented 1802 [15]. The clinical presentation of patients with SCOGH is highly variable but commonly includes gastric outlet obstruction (GOO).
In the present report, we reviewed the literature of patients with SCOGH and present a case recently encountered in our practice. Pathophysiology, a brief history, and outcomes related to this rare entity are discussed.
2. Materials and Methods
We review a case report of a patient who presented with a SCOGH at our institution. The medical records were reviewed for this patient in the computer patient record system. Informed consent was obtained from the patient for the publication of this report. This work has been reported in line with the SCARE criteria and following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines [16]. SH, JF, and MA reviewed all the papers and selected all manuscripts required for inclusion. The initial literature review was performed in March of 2023. Various combinations of keywords including “hernia”, “inguinal hernia”, “sliding hernia”, “femoral hernia”, “groin”, and “stomach” were used for our searches. No time restriction (beyond that of the existing databases) or language restriction was imposed. Databases including PubMed, MEDLINE (via PubMed), and Embase were initially queried. Subsequently, Cochrane Library, Google, Google Scholar, and ResearchGate were utilized to search and acquire reports that were new and/or unavailable from the previous databases. Further manuscripts were identified by close examination of the references of the index papers and main reviews on this subject [17,18,19]. These manuscripts were included in our review if they were appropriate references and did not duplicate our original findings of patients with SCOGH reviewed elsewhere.
The PRISMA flow chart depicts the screening process (Figure 1). All the abstracts were analyzed within an EndNote group to eliminate irrelevant and duplicated studies. Google translate was utilized to translate articles in other languages. Full text for a handful of articles was unavailable for a variety of reasons. These include lack of electronic copies, restrictions by foreign countries, incomplete scanning, and older manuscript dates.
3. Results
3.1. Case Report
A 77-year-old man with chronic obstructive pulmonary disease (COPD; on 4L of home oxygen), hypertension, and class III chronic kidney disease presented to the Emergency Department (ED) at our institution in February of 2023 with an incarcerated left inguinal hernia. He had a one-day history of abdominal pain, nausea, and vomiting. He reported presence of the hernia for over 10 years. His last bowel movement had been the night prior to presentation to the ED. On physical examination, he was tachycardic to 100 beats per minute and normotensive with a blood pressure of 110/70 mmHg. His abdomen was soft and mildly tender to deep palpation. He had a left inguinal bulge that was tender to palpation and irreducible. He had no leukocytosis, and his serum lactic acid level was within normal limits. Due to the patient’s presentation and symptomatology, a nasogastric tube (NGT) was placed in the emergency department for decompression. A subsequent Kidney-Ureter-Bladder X-ray demonstrated the tip of the NGT within the left groin. Computed tomography confirmed GOO from an incarcerated stomach within the left groin hernia. There was no radiographic evidence of bowel ischemia or compromise (Figure 2).
Intravenous fluid (IVF) administration and NGT decompression were immediately started. His tachycardia promptly resolved after initiating IVF. Serial abdominal examinations were performed and after a few hours of NGT decompression his left inguinal hernia was able to be reduced. Because he was not interested in surgical intervention, he was started on oral feeds a day later and once he was tolerating his diet well, he was discharged home from the hospital. He was doing well at a six-week follow up visit in clinic and still not interested in elective surgical repair of his hernia.
3.2. Review of the Literature
A systematic review of the literature revealed 90 cases of SCOGH, with the present report adding an additional case to the world literature. Other than English, the Spanish and French literature were the most reported languages identifying this clinical entity. Most reports include single cases with a literature review at the time of the publication. Several documents indicated the existence of only 60 cases prior to 1980 [19,20,21].
The first comprehensive review of SCOGH was published by Davey and Strange in 1954.[18] This manuscript accounted for 34 inguinal and 3 femoral hernias and was inclusive of the prior 150 years and up to the date of publication [18]. A second review in 1960 added only 6 further cases of inguinal hernias with stomach contents to the literature [19].
The most recent review includes 21 cases from 1942 to 2020 of patients who presented with SCOGH [17]. Within this review, there were 10 patients who presented with GOO. This manuscript focused on the management of this condition with emphasis on patients presenting acutely because of perforation. This review was of the English literature only and was limited to reports digitally available. All patients with gastric perforation required laparotomy with one exception, which was addressed laparoscopically [17] .
Our analysis identified 90 unique patients with SCOGH encompassing a period of over two centuries (1802 to 2022). In addition, we include a patient who presented to our institution in February of 2023 with GOO from SCOGH. Thus, a total of 92 patients (86 inguinal and 6 femoral) are included in the present review (Table 1). If available, patient characteristics and clinical presentation for each case are included in Table 2 and Table 3, inguinal and femoral cases, respectively. Online Resource 1 includes the respective references.
3.2.1. Patient Demographics
The mean age for the entire cohort was 69.6 ± 12.9 years-old (range 28 to 87 years-old) (Table 1). Most patients were men overall, but female gender was more common in femoral hernias with SCOGH (66.7%). For 73 cases, laterality was included in the reports and 97.5% occurred on the left. Two cases reported bilateral hernias. Six patients had femoral hernias.
3.2.2. Complications
The mean duration for history of a hernia was 23.1 ± 10.8 years (range 10 to 50 years). Gastrointestinal symptoms related to obstruction (nausea, emesis, abdominal pain) were the most commonly reported symptoms (47.8%). GOO was reported in 17, absent in 14, and not reported in 61 patients. Five cases explicitly reported no symptoms. Gastric rupture was emphasized for some reports and in manuscript review [17,22]. Other complications included aspiration pneumonia directly attributed to this entity [23]. Gastric volvulus in a patient with SCOGH was reported in one manuscript [24].
3.2.3. Mortality
Death directly attributed to SCOGH was reported in 21 cases (22.8%). However, most mortalities occurred in early publications (1802-1896 [n=9] and 1910-1997 [n=10]). Only two mortalities occurred in the recent era (2019 and 2021), but these patients were 75 and 84-years old, respectively. Only one death was identified from a femoral hernia containing stomach in a 47-year-old woman, which was reported in 1885 [25].
3.2.4. Management
Nine inguinal and one femoral hernia containing stomach were reported at autopsy, but these were all early reports (1802 to 1896). Elischer successfully operated emergently on two patients with SCOGH in 1923 [26]. The first hernia repaired in the elective setting was reported by de Vernejoul and de Luna in 1925 [27].
Heylen’s manuscript addressed the management of this condition with emphasis on patients presenting acutely because of gastric perforation. All patients with gastric perforation required laparotomy with one exception, which was addressed laparoscopically [17].
Conservative management was explicitly undertaken in 12 patients with SCOGH. The reasons for this approach were cited as high-risk operative candidates. Nasogastric decompression was initially undertaken in patients who presented with emesis or acute incarceration. This was also the management for the patient that presented to our institution.
4. Discussion
The stomach is a fixed structure in the upper abdomen. The gastrophrenic, gastrosplenic, hepatogastric, and hepatoduodenal ligaments provide fixation to the stomach superiorly [28]. This arrangement combined with distance, makes the stomach an unusual visitor to the groin. The groin finds a visiting stomach in the following fashion. First, the inferior fixation of the stomach to the greater omentum and the gastrocolic ligament is more tenuous compared to the superior fixation. Initial migration of the omentum to the groin hernia sac (which is common) with continuous traction and chronicity may eventually lead the stomach to travel within the groin hernia sac [29]. This downward movement of the stomach is termed gastroptosis [30]. Chronicity is thus the second element that makes this migration possible. This is further evidenced by our review, which found that the reported average of time for symptoms of a stomach containing groin hernia was 23.1 ± 10.8 years (range 10 to 50 years).
Multiple mechanisms for the descent of the stomach into the groin have been proposed as early as 1912 by Chambard,[29] 1927 by Sicot,[31] and 1930 by Novaro [32]. Three mechanisms remain constant in the literature: (1) downward pulling of the omentum into the inguinal hernia sac, (2) chronicity, and (3) short stature of patients. Downward deviation of the diaphragm as a result of chronic COPD might also be a contributing factor (as in our patient) [20]. Giant inguinoscrotal hernias, defined by the extension of the hernia down to midthigh while the patient is standing, has also been documented as a risk factor [33].
The likelihood of these three mechanisms occurring in groin hernias simultaneously is so infrequent that in over more than two centuries less than 100 stomach-containing groin hernias have been reported in the literature. The first case of a hernia sac containing stomach appeared in the literature in 1802, and it was diagnosed at autopsy. The patient had been suffering from symptoms of this hernia for 32 years until his demise at age 64 [15]. It took 152 years for the first comprehensive and intriguing review to appear in the literature by Davey and Strange in 1954 [18]. This review included 34 inguinal and 3 femoral hernias. Our review adds 51 inguinal (including one of our own) and 3 femoral hernias to the world literature.
The first eight reports of SCOGH were documented at autopsy (n=8 from 1802 to 1896) [15]. The first case of a femoral hernia containing stomach was documented by Keller in 1885 [25]. The first laparotomy performed identifying SCOGH occurred in 1897 [34]. The first radiographic evidence of SCOGH was first published in the literature in 1915 [34]. Successful outcomes for an emergent operation from SCOGH were initially described by Elischer in 1923 [26]. The first woman with SCOGH was reported in 1925 [18,27]. The first case of SCOGH repaired in the elective setting is credited to de Vernejoul and de Luna in 1925 [27].
Laterality and sex are important for migration of the stomach into the groin. Our analysis identified left laterality for 78% and 100% of the cases and male sex for 95% and 33% of the cases for inguinal and femoral hernias in patients with SCOGH, respectively.
Clinical presentation for SCOGH ranged from entirely asymptomatic to an acute abdomen. Overall, the most common complaint was related to obstructive symptoms, occurring in nearly half of the cases in our analysis. GOO from SCOGH occurred in 18.5% of cases. There was also a wide spectrum of management in patients with SCOGH from entirely conservative (n=11; 12%), to elective operative intervention, to emergent operative management. Management varied from a groin approach with or without laparotomy for elective cases to laparotomy with or without a groin incision in emergent cases. One report documented an exclusively laparoscopic hernia repair [17]. Haylen’s manuscript provides an excellent review of the surgical approach depending on clinical presentation [17].
While mortality has been reported in patients with SCOGH, these deaths occurred in earlier reports. For recent reports, mortality is uncommon and most patients did well regardless of management strategy (conservative, non-operative management [as in our case] to elective operations,[27] or urgent operations[17,26]).
5. Conclusions
Our review shows that almost any abdominopelvic organ, even the naturally superiorly located stomach, can migrate to the groin, enter the groin hernia sac, and present as an asymptomatic or symptomatic hernia. The stomach is rarely found in groin hernias owing to its fixation to the upper abdomen; however, omental downward displacement combined with chronicity are common mechanisms leading to SCOGH. Commonly, patients present with symptoms related to GOO, though some patients may remain asymptomatic entirely. Conservative management is permissible depending on clinical presentation, patient preferences, and operative risk. For SCOGH presenting with symptoms of GOO, immediate NGT decompression is encouraged and may allow for reduction of an initially incarcerated SCOGH and ultimately permit conservative management. Modern diagnostic tools and contemporary management strategies allow for early identification and improved outcomes for patients with SCOGH.
6. Patents
Informed consent was obtained by the patient for publication of this manuscript and is available upon request.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
“Conceptualization, S.H., J.F. and M.A.; methodology, M.A, and J.F.; software, M.A., and J.F.; validation, KW., J.F. and M.A.; formal analysis, M.A, J.F., S.H, C.W., J.M., and S.H,; investigation, J.F., M.A., S.H., J.M., and C.W.; resources, J.F., M.A., S.H., J.M.; data curation, J.F., M.A., S.H., J.M.; writing—original draft preparation, J.F., M.A., S.H., J.M.; writing—review and editing, J.F., M.A., S.H., J.M.; visualization, J.F., M.A., S.H., J.M.; supervision, S.H.; project administration, S.H.; funding acquisition, S.H. All authors have read and agreed to the published version of the manuscript.” Please turn to the CRediT taxonomy for the term explanation. Authorship must be limited to those who have contributed substantially to the work reported.
Funding
This research received no external funding.
Institutional Review Board Statement
All procedures performed in the studies involving human participates were in accordance with the ethical standards of the institution and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Appropriate Institutional Board Review approval was not required for this systematic review.
Informed Consent Statement
Informed consent was obtained by the patient for publication of this manuscript and is available upon request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Huerta, S.; Patel, P.M.; Mokdad, A.A.; Chang, J. Predictors of inguinodynia, recurrence, and metachronous hernias after inguinal herniorrhaphy in veteran patients. Am, J. Surg 2016, 212, 391–8. [Google Scholar] [CrossRef] [PubMed]
- Ponka, J.L.; Brush, B.E. Sliding inguinal hernia in patients over 70 years of age. Journal of the American, G.eriatrics Society 1978, 26, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Huerta, S.; Fairbanks, T.; Cinat, M. Incarcerated vesicoinguinal hernia presenting with gross hematuria. J Am Coll Surg 2005, 201, 992–3. [Google Scholar] [CrossRef] [PubMed]
- Dunn, T.M.; Markgraf, W.H. Littre hernia—incarcerated meckel's diverticulum. The American Journal of Surgery 1962, 103, 144–45. [Google Scholar] [CrossRef] [PubMed]
- Michalinos, A.; Moris, D.; Vernadakis, S. Amyand's hernia: A review. The American Journal of Surgery 2014, 207, 989–95. [Google Scholar] [CrossRef] [PubMed]
- Goyal, S.; Shrivastva, M.; Verma, R.; Goyal, S. “Uncommon contents of inguinal hernial sac”: A surgical dilemma. Indian Journal of Surgery 2015, 77, 305–09. [Google Scholar] [CrossRef] [PubMed]
- Ganesaratnam, M. Maydl's hernia: Report of a series of seven cases and review of the literature. British journal of surgery 1985, 72, 737–38. [Google Scholar] [CrossRef] [PubMed]
- Taveras, L.R.; Huerta, S. A case report of a de garengeot hernia in a nonagenarian veteran. Int J Surg Case Rep 2017, 41, 301–03. [Google Scholar] [CrossRef]
- Sidiqi, M.M.; Menezes, G. Asymptomatic herniation of ureter in the routine inguinal hernia: A dangerous trap for general surgeons. Int J Surg Case Rep 2018, 49, 244–46. [Google Scholar] [CrossRef]
- Aldhafar, A.; Mohammed, A.; Alwabari, M.; Aldhafar, R. A strangulated right inguinal hernia containing the transverse colon: An unusual case report. Asian Journal of Case Reports in Surgery 2020, 5, 10–13. [Google Scholar]
- Fitz, E.; Chihara, R.; Stanton-Maxey, KJ. Gastric perforation associated with bilateral inguinal hernias. J Am Coll Surg 2016, 222, e12–3. [Google Scholar] [CrossRef] [PubMed]
- Tajti J, Jr., Pieler J, Abraham S, Simonka Z, Paszt A, Lazar G. Incarcerated gallbladder in inguinal hernia: A case report and literature review. BMC Gastroenterol 2020, 20, 425. [CrossRef] [PubMed]
- Chen, G.; Wang, X.; Zhao, Y.; Zhu, L.; Tang, D. Splenogonadal fusion: A case report and review of the literature. BMC Urol 2021, 21, 16. [Google Scholar] [CrossRef] [PubMed]
- Arredondo Montero, J.; Guillen Redondo, P.; Antona, G.; Bronte Anaut, M. Newborn inguinal hernia containing uterus, ovary and fallopian tube. An Pediatr (Engl Ed) 2023, 98, 232–33. [Google Scholar] [CrossRef] [PubMed]
- Lallement, L. J Med Chir Pharm 1802, 1, 329.
- McInnes, M.D.; Moher, D.; Thombs, B.D.; McGrath, T.A.; Bossuyt, P.M.; Clifford, T.; Cohen, J.F.; Deeks, J.J.; Gatsonis, C.; Hooft, L. Preferred reporting items for a systematic review and meta-analysis of diagnostic test accuracy studies: The prisma-dta statement. Jama 2018, 319, 388–96. [Google Scholar] [CrossRef] [PubMed]
- Heylen, J.; Campioni-Norman, D.; Lowcock, D.; Varatharajan, L.; Kostalas, M.; Irukulla, M.; Ratnasingham, K. Inguinoscrotal hernias containing stomach: Risk of emergency presentation. Ann R Coll Surg Engl 2021, 103, 713–17. [Google Scholar] [CrossRef] [PubMed]
- Davey, W.; Strange, S. The stomach as a content of inguinal and femoral herniae. British Journal of Surgery 1954, 41, 651–58. [Google Scholar] [CrossRef] [PubMed]
- Ship, A.G.; Glick, A.H.; Goldenson, AB. Incarceration of the stomach in an inguinal hernia: Report of a case. New England Journal of Medicine 1960, 262, 78–80. [Google Scholar] [CrossRef]
- Diaz Oller, J.; Medina Dominguez, M.T.; Arcos Navarro, A.; Alia Diaz, J.J.; Asanza Llorente, J.A.; Numancia Andreu, M.B.; Nevado Infante, A.; Martos Torres, J.; Moya Vazquez, RJ. [stomach in inguinal-scrotal hernia]. Rev Esp Enferm Dig 1997, 89, 325–8. [Google Scholar]
- Ogul, H.; Yuce, I.; Eren, S.; Kantarci, M. Bilateral inguinal hernia with uncommon content. Can J Gastroenterol 2013, 27, 14. [Google Scholar] [CrossRef]
- Heylen, J.; Campioni-Norman, D. Bilateral inguinoscrotal hernia with gastric contents and subsequent perforation: Lessons in operative management. International Journal of Surgery Case Reports 2020, 77, 853–56. [Google Scholar] [CrossRef]
- Fazekas, B.; Frecker, P.; Francis, L.; Patel, K. Aspiration pneumonia as a complication of a rare type of hernia. Int J Surg Case Rep 2014, 5, 1061–3. [Google Scholar] [CrossRef]
- Ferdinand, E.; Amir, R.; Manjunath, S. Serendipity of giant proportions. Clin Gastroenterol Hepatol 2013, 11, A25–6. [Google Scholar] [CrossRef]
- Keller, O. Schenkelhernie mit magen als inhalt. Inag Diss, Bern 1885.
- Elisscher EV. Ibid 1923, 50, 1814.
- de Vernejoul, de Luna D. Sociétés de province: Société de chirurgie de marseille: Volumineuse hernie inguinale renfermant l'estomac et les annexes gauches. Pr Med 1925, 33, 208. [Google Scholar]
- Grantham, T.A.; Ramachandran, R.; Parvataneni, S.; Gaduputi, V. Stomach within a large inguinal hernia. Cureus 2022, 14, e24783. [Google Scholar] [CrossRef] [PubMed]
- Chambard, ME. La hernie inguinale de l'estomac. Rev, de gynec e d'obst 1912, 19, 61–79. [Google Scholar]
- Natsis, K.; Apostolidis, S.; Papadopoulou, A.; Vlasis, K.; Totlis, T.; Skandalakis, P. Gastric femoral hernia in a male cadaver with gastroptosis: Case report and review of the literature. Hernia 2008, 12, 205–08. [Google Scholar] [CrossRef]
- Sicot, R. Contribu a l'etude des hernies inguinales de l'etomc. These de Paris 1927.
- Novaro, N. Arch Ital Chir 1920, 27, 483.
- Lajevardi, S.S.; Gundara, J.S.; Collins, S.A.; Samra, JS. Acute gastric rupture in a giant inguinoscrotal hernia. J Gastrointest Surg 2015, 19, 2283–5. [Google Scholar] [CrossRef] [PubMed]
- Brunner, F. Kleinere mittheilungen: Ein fall von hernia ventriculi inguinalis incarcerata. Zentralbl f Chir 1897, 24, 919–21. [Google Scholar]
Figure 1.
PRISMA flow-chart describing the process of our literature search. *Total number of patients includes our present case.
Figure 1.
PRISMA flow-chart describing the process of our literature search. *Total number of patients includes our present case.
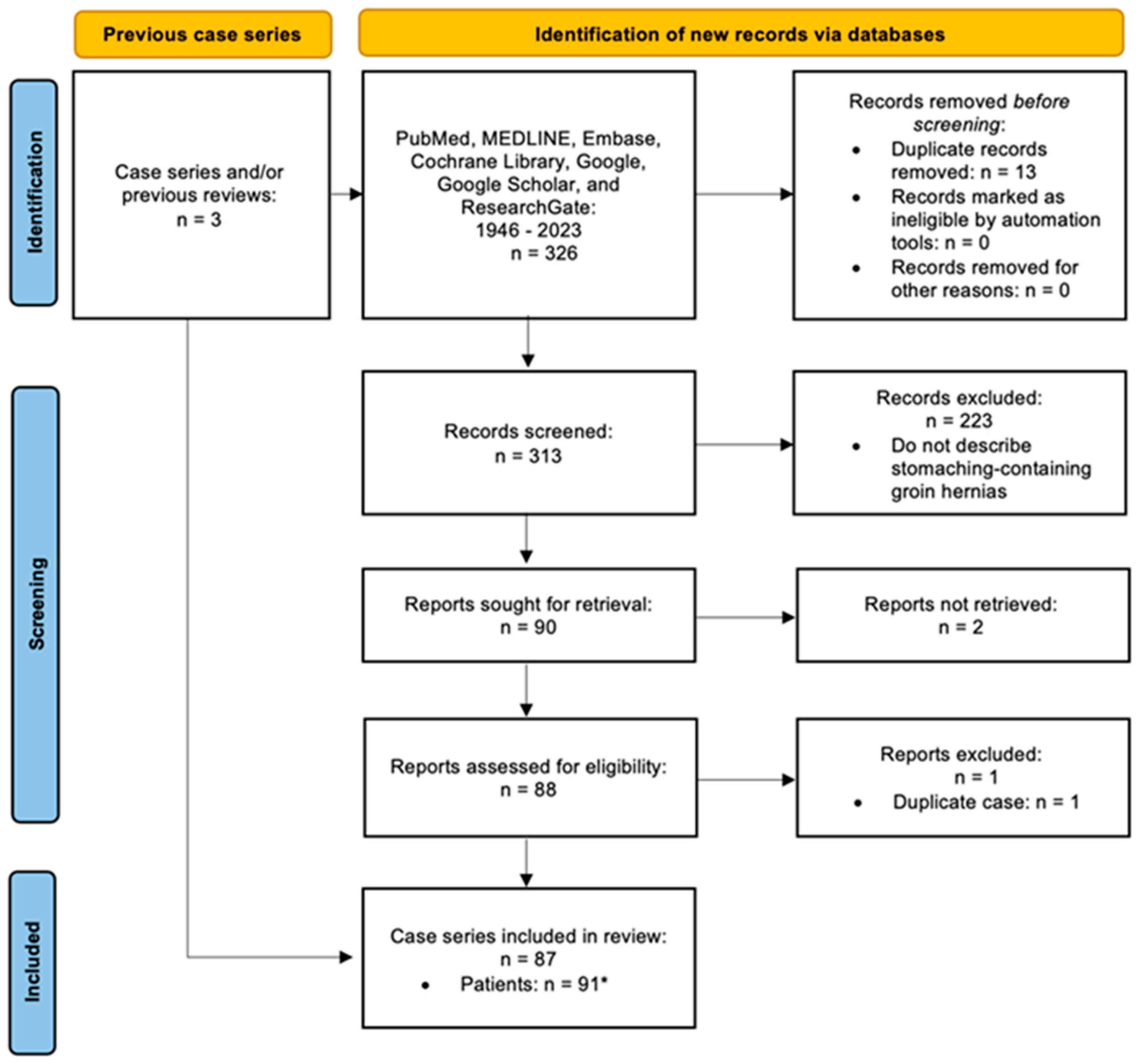
Figure 2.
A, Sagittal computed tomography image of the abdomen depicting the stomach extending into the left groin causing gastric outlet obstruction. B, Coronal radiograph of the abdomen depicting the tip of the nasogastric tube in the left groin (arrow).
Figure 2.
A, Sagittal computed tomography image of the abdomen depicting the stomach extending into the left groin causing gastric outlet obstruction. B, Coronal radiograph of the abdomen depicting the tip of the nasogastric tube in the left groin (arrow).
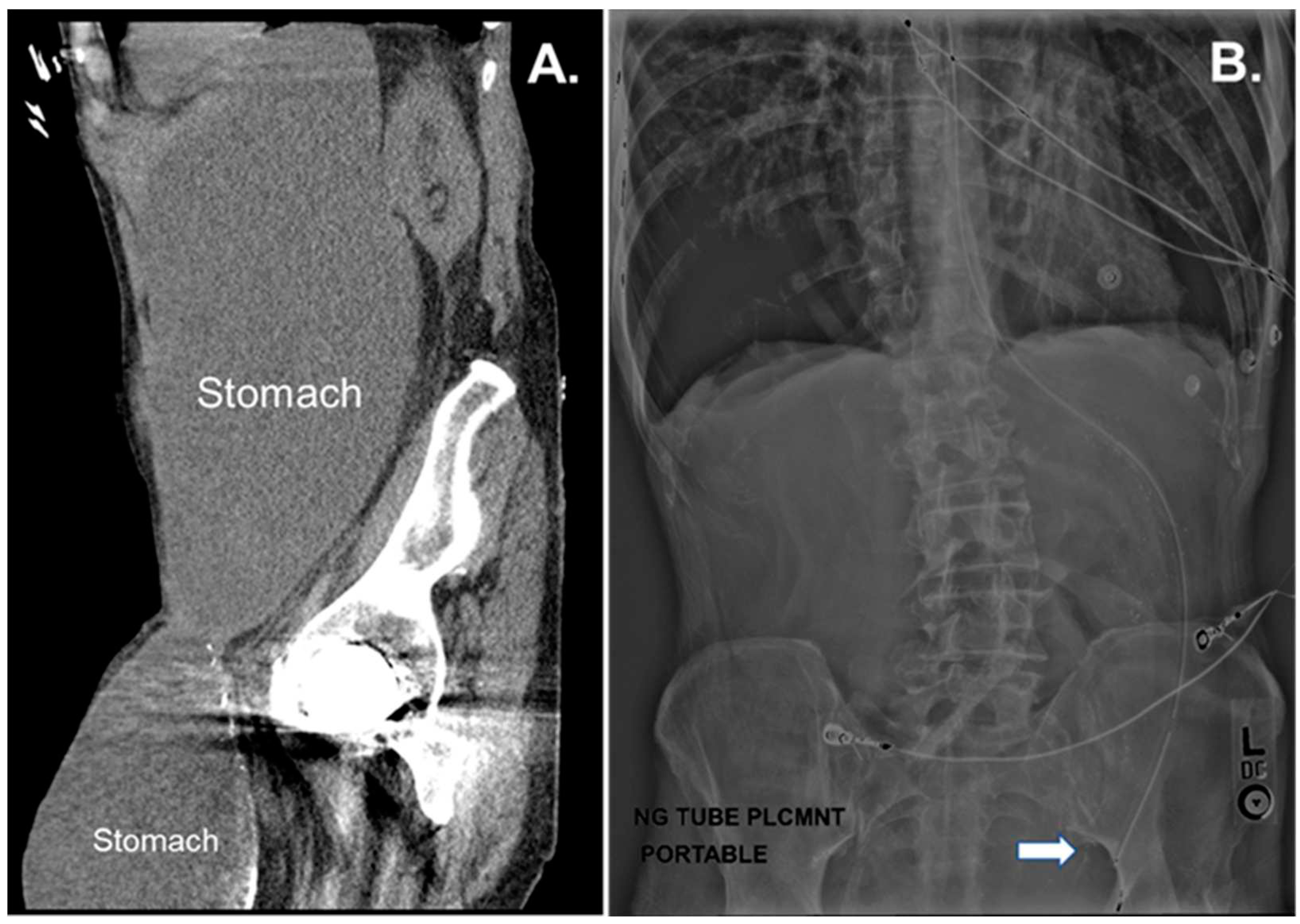

Table 1.
Characteristics of patients presenting with stomach-containing groin hernias (n=92).
| Characteristics | Inguinal (n=86) | Femoral (n=6) |
|---|---|---|
| Age [Years (SD)*] | ||
| 74.2 (13.0) | 62.0 (11.5) | |
| Sex [male (%)] | 95.2 | 33.3 |
| Laterality [Left (%)] | 78.0 | 100.0 |
* Standard Deviation.
Table 2.
Characteristics and clinical presentation for the 86 patients with stomach-containing inguinal hernias, ordered by chronological occurrence.
Table 2.
Characteristics and clinical presentation for the 86 patients with stomach-containing inguinal hernias, ordered by chronological occurrence.
| n | Reference, Year a | Age | Sex | Laterality | Clinical Presentation |
|---|---|---|---|---|---|
| 1 | Lallement, 1802 | 64 | Male | NR | Abdominal pain/discomfort and vomiting |
| 2 | Yvan, 1830 | NR | Male | NR | Vomiting |
| 3 | Febre, 1832 | 73 | Male | Right | No symptoms |
| 4 | Fogt, 1884 | 60 | Male | Left | Vomiting |
| 5 | Schmidt, 1885 | 65 | Male | Left | Hematemesis and inguinal pain |
| 6 | Chiari, 1888 | 74 | Male | Right | No symptoms |
| 7 | Lewin, 1893 | 53 | Male | Left | Emesis and pain |
| 8 | Chevereau, 1894 | 77 | Male | Left | Emesis and pain |
| 9 | Souligoux, 1896 | NR | Male | Left | NR |
| 10 | Brunner, 1897 | 28 | Male | NR | NR |
| 11 | Hilgeneriner, 1910 | 52 | Female | Left | Pain and vomiting |
| 12 | Chambard, 1912 | 62 | Male | Left | Vomiting, pain and an incarcerated hernia |
| 13 | Rieder, 1915 | 62 | Male | Left | Hematemesis and melena |
| 14 | Ahrens, 1920 | 40 | Male | Right | Pain |
| 15 | Maag, 1920 | 81 | Male | Left | No symptoms |
| 16 | Stokes, 1922 | 42 | Male | Right | Vomiting and an incarcerated hernia |
| 17 | Elischer, 1923 | 53 | Male | Left | Nausea and an incarcerated hernia |
| 18 | Elischer, 1923 | 70 | Male | Left | Incarcerated hernia |
| 19 | Dressen, 1925 | 62 | Male | Left | Vomiting, pain, and inguinal symptoms when eating |
| 20 | de Vernejoul, 1925 | 57 | Female | Left | NR |
| 21 | Sicot, 1927 | 59 | Male | Left | Pain, vomiting, and dyspepsia |
| 22 | Lipkin, 1928 | 60 | Male | Left | Incarcerated hernia |
| 23 | Siegmund, 1929 | NR | Male | Right | NR |
| 24 | Novaro, 1930 | 53 | Male | Right | Vomiting, pain, and an irreducible hernia |
| 25 | Rodzevich, 1935 | 54 | Male | Left | Vomiting and abdominal pain |
| 26 | Oakley, 1937 | 81 | Male | Right | Abdominal and groin pain |
| 27 | Herrmann, 1937 | 80 | Male | Left | Vomiting |
| 28 | Lemaitre, 1937 | 51 | Male | Left | Dyspepsia |
| 29 | Lust, 1937 | 62 | Male | Left | NR |
| 30 | Alexsandrovskiv, 1940 | 73 | Male | Left | Incarcerated hernia |
| 31 | Feldman, 1943 | 66 | Male | Right | No symptoms |
| 32 | Hartley, 1945 | 67 | Male | Left | Dyspepsia |
| 33 | Simmons, 1949 | 66 | Male | Left | Nausea, vomiting, and abdominal pain |
| 34 | Lewis, 1950 | 69 | Male | Right | Occasional vomiting |
| 35 | Anger, 1952 | 74 | Male | Left | Vague symptoms |
| 36 | Bernard, 1953 | NR | NR | NR | NR |
| 37 | Meinterz, 1953 | NR | NR | NR | NR |
| 38 | Davey, 1954 | 61 | Male | Left | Vomiting with markedly distended and tense abdomen |
| 39 | Legrand, 1955 | NR | NR | NR | NR |
| 40 | D'Eshougues, 1956 | NR | NR | NR | NR |
| 41 | Allende, 1956 | NR | NR | NR | NR |
| 42 | Kislenskii, 1959 | NR | NR | Left | NR |
| 43 | Hagarty, 1959 | NR | NR | NR | NR |
| 44 | Ship, 1960 | 83 | Male | Left | Persistent nausea and vomiting |
| 45 | Herrera, 1960 | NR | NR | NR | NR |
| 46 | Jackson, 1964 | NR | NR | NR | Strangulation and perforation of the stomach in the inguinal canal |
| 47 | Falugiani, 1968b | NR | NR | NR | NR |
| 48 | Gue, 1970 | NR | NR | NR | NR |
| 49 | Soudek, 1975 | NR | NR | NR | NR |
| 50 | Padmanabhan, 1976 | 65 | Male | Left | NR |
| 51 | Nagendran, 1977 | NR | NR | NR | NR |
| 52 | Rozencwajg, 1981 | NR | NR | NR | NR |
| 53 | Udwadia, 1984 | NR | NR | NR | Hematemesis |
| 54 | Quaranta, 1984 | NR | NR | NR | NR |
| 55 | Resente,1986 | NR | NR | NR | NR |
| 56 | Naraynsingh, 1987 | 62 | Male | Left | Recurrent bouts of vomiting, recurrent GOO |
| 57 | Levy, 1987 | 49 | Male | Left | Abdominal pain, nausea, and weight loss |
| 58 | Loizate, 1988 | NR | NR | NR | Upper gastrointestinal tract hemorrhage |
| 59 | Broquet, 1992 | 64 | Female | Bilateral | Perforation of gastric ulcer within the hernia sac |
| 60 | Diaz, 1997 | NR | NR | NR | NR |
| 61 | Diaz, 1997 | NR | NR | NR | NR |
| 62 | Walgenbach, 2001 | 72 | Male | Left | A 6-hour history of abdominal distension and pain |
| 63 | Birnbaum, 2011 | 86 | Male | Right | Nausea and vomiting |
| 64 | Dogar, 2011 | 65 | Male | Left | Irreducible groin bulge, abdominal pain, distention, darkish red vomitus, and obstipation |
| 65 | Kerschaever, 2012 | 79 | Male | Left | Anorexia, vomiting, and abdominal distension |
| 66 | Ogul, 2013 | 56 | Male | Left | Recurrent vomiting and bilateral incarcerated groin bulges |
| 67 | Ferdinand, 2013 | 73 | Male | Right | Iron deficiency anemia and gastric volvulus |
| 68 | Fazekas, 2014 | 85 | Male | Left | Three-day history of gastrointestinal obstructive symptoms |
| 69 | Creedon, 2014 | 87 | Male | Left | Colicky abdominal pain for 48 hours and vomiting |
| 70 | Patel, 2014 | 85 | Male | Left | 3-day history of profuse vomiting and abdominal pain |
| 71 | Lajevardi, 2015 | 83 | Male | Left | Four-day history of vomiting and constipation |
| 72 | Fitz, 2016 | 46 | Male | Bilateral | Severe abdominal pain after dinner brought in by ambulance to the emergency department |
| 73 | Mora-Guzman, 2016 | 79 | Male | Right | Abdominal pain and vomiting |
| 74 | Perez-Pueyo, 2016 | 61 | Male | Left | Gastric necrosis secondary to an incarcerated inguinal hernia |
| 75 | Nugud, 2017 | 67 | Male | Left | Bilious vomiting with abdominal pain |
| 76 | Sayad, 2019 | 50 | Male | NR | Severe abdominal pain |
| 77 | Junge, 2019 | 75 | Male | Left | Abdominal pain and nausea |
| 78 | Mehta, 2019 | 75 | Male | Left | 5-day history of hematemesis |
| 79 | Heylen, 2020 | 74 | Male | Left | Dark vomitus and generalized abdominal tenderness |
| 80 | Patel, 2021b | 84 | Male | NR | Nausea, vomiting, constipation, GOO, and eventual peritonitis |
| 81 | Vinod, 2021 | 49 | Male | Left | Acute abdominal pain with nausea and dysuria |
| 82 | Alexandre, 2022 | 71 | Male | Left | Nausea, vomiting, constipation, and GOO |
| 83 | Grantham, 2022 | 81 | Male | Lett | Coffee ground emesis |
| 84 | Abbakar, 2022 | 84 | Male | Right | Double GOO. One-day history of severe abdominal pain and dark brown vomiting |
| 85 | Huerta, 2023b | 77 | Male | Left | Abdominal pain, nausea, vomiting, and GOO |
GOO = gastric outlet obstruction; NR = not recorded; aFull reference details included in Online Resource 1; bFrom posters, abstracts, presentations, and/or present case.
Table 3.
Characteristics and clinical presentation for the 6 patients with stomach-containing femoral hernias, ordered by chronological occurrence.
Table 3.
Characteristics and clinical presentation for the 6 patients with stomach-containing femoral hernias, ordered by chronological occurrence.
| Reference, Yeara | Age | Sex | Laterality | Clinical Presentation |
|---|---|---|---|---|
| Keller, 1885 | 47 | Female | Left | 3-day history of abdominal pain and vomiting |
| Spiegel, 1920 | 55 | Female | Left | Gastric strangulation |
| Cave, 1948 | 56 | Female | Left | Dyspepsia |
| Davey, 1954 | 68 | Male | Left | No symptoms |
| Cade, 1984 | 79 | Female | Left | Abdominal pain, emesis, and hematemesis |
| Natsis, 2008 | 67 | Male | Left | Findings at autopsy |
aFull reference details included in Online Resource 1.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



