
Submitted:
23 November 2023
Posted:
23 November 2023
You are already at the latest version
Abstract
Osteoporosis is characterized by low bone mass and structural deterioration of bone tissue with increased risk of fracture. The population that is most at risk for primary osteoporosis in-cludes post-menopausal women.
Among different approaches, nutraceuticals are increasingly popular in developed countries since can contribute to bone health and can delay the onset of pathological bone loss.
Our review covers three main aspects. Firstly, we discuss the current state of the two con-ditions, osteopenia, and osteoporosis. Secondly, we focus on the latest developments in natural Nutraceuticals and their effectiveness in reducing bone loss. Finally, we conduct a Strengths, Weaknesses, Opportunities, and Threats (SWOT) analysis to examine the pros and cons of Nutraceuticals assumption.
Nutraceuticals hold great promise, but we must address challenges such as regulatory control and experimental evidence to fully realize their potential. Other challenges include identifying the source of raw materials, ensuring the purity of the compound, avoiding contamination or the presence of other active compounds, maintaining product quality, and preventing interactions with other elements or drugs.
By addressing these challenges, the scientific community can ensure more reliable indica-tions for the use of Nutraceuticals and help people lead healthier lives.
Keywords:
osteopenia
; osteoporosis
; nutraceuticals
; prevention
; lifestyle
; bone health
; minerals
; phytochemicals.
1. Introduction
Preventing osteopenia and osteoporosis is crucial for ensuring bone health during aging [1,2,3]. Osteopenic and osteoporotic patient management carries significant health, social, and economic burdens on countries with an increase in the population's average age. Financial costs are direct, especially concerning treating osteoporotic fractures, and indirect, such as disability and loss of productivity. Osteopenia and osteoporosis bone loss prevention can significantly reduce the costs incurred by the health system and improve the quality of life [4]. Although various available therapeutic options exist, they present side effects, which are primarily responsible for discontinuing therapy [5]. Moreover, a segment of the high-risk fracture population does not receive care due to cultural and socio-economic factors and the diffusion in the last decade of unjustified skepticism against official medicine [6].
Lifestyle contributes to maintaining bone density and preventing bone loss in terms of physical activity and nutrition habits. In recent times, research has increasingly focused on different approaches that can be complementary to or help delaying the pharmacological treatment in subject at risk of bone fragility [7,8].
In this context, using nutraceuticals may promote healthy aging and reduce the risk of osteoporosis in elderly individuals. A recent classification divides Nutraceuticals based on diverse sources: natural/traditional and unnatural/nontraditional [9]. Traditional nutraceuticals come directly from natural sources. They are further divided into nutrients, herbals, phytochemicals, probiotics, and enzymes based on their chemical constituents. In contrast, nontraditional nutraceuticals are artificially synthesized (agriculture breeding or biotechnology). They can be classified as fortified or recombinant, depending on the procession process.
“Our literature review describes the state of the art on osteopenia and osteoporosis. Then, we will discuss and highlight the latest developments in natural nutraceuticals that have been found to promote bone health and prevent osteoporosis. We will also analyze Nutraceutical's advantages and disadvantages through a SWOT (Strengths, Weaknesses, Opportunities, Threats) analysis.
2. Osteopenia and osteoporosis
2.1. Bone
Bone is a mineralized connective organ exerting essential body functions: muscle attachment and locomotion, soft tissue support, vital organs protection, bone marrow harboring, calcium (Ca) and phosphate (P) storage, and homeostasis [10].
Recent studies showed that bone may have additional endocrine roles in glucose metabolism [11,12,13,14]. During development, the skeletal system maintains its total size and shape via bone modeling. In this process, resorption and formation are uncoupled: in one anatomical site, the bone degrades, while new bone formation occurs in another [15,16].
Mature bone tissue consists of an abundant calcified extracellular matrix (ECM) that supports and interacts with the resident cell types that help in bone development and maintenance: osteoblasts and osteocytes, osteoclasts, hypertrophic chondrocytes, and bone lining cells. Osteoblasts, derived from mesenchymal cells, serve for bone formation. Osteocytes are terminally differentiated osteoblasts in the mineralized bone that help control the timing and site of the remodeling process [17]. Osteoclasts originate from hematopoietic precursor cells and are responsible for bone resorption. Hypertrophic chondrocytes serve as a template for bone formation; this process continues at the epiphyseal growth plate during growth. Bone lining cells are quiescent osteoblasts that cover the bone surfaces, where neither bone resorption nor bone formation occurs. Their role must be understood entirely (Florencio-Silva et al., 2015).
Besides cells, the ECM comprises a nanostructured organic phase rich in collagen (mainly type 1, mucopolysaccharides, and water, providing flexibility and tensile strength and an inorganic mineral phase presenting nanocrystalline hydroxyapatite (HA) (calcium phosphate), ensuring bone mechanical rigidity and compressive strength [18,19,20,21,22,23].
2.2. Bone remodeling
Bone remodeling is a continuous process that occurs throughout life. It involves replacing old or damaged tissue with new tissue, which helps maintain mineral balance and structural integrity [24,25]. This tightly regulated process involves mechanical and chemical signals and systemic and local factors. Bone resorption and formation occur spatially and temporally alternate to ensure that the overall bone volume and structure remain unchanged.
The bone remodeling cycle consists of five steps: activation, resorption, reversal, formation, and termination/quiescence. In the activation phase, bone cells fuse to form multinucleated preosteoclasts, which bind to the matrix and create sealing zones [26]. Osteocytes initiate all these signals, detecting bone matrix damage and communicating with other cells through their extensive network of dendritic processes [27,28,29]. Remodeling can also be initiated in response to systemic hormone changes, such as parathyroid hormone (PTH), to allow access to bone Ca stores. In the resorption phase, osteoclasts degrade the bone matrix and end with programmed cell death [30,31]. The reversal phase is not fully understood but switches to osteoblast-mediated bone formation, promoting new bone deposition [32]. Osteoclasts may either secrete cytokines or act via a regulatory surface receptor to release osteogenic signals to prompt bone formation [33,34]. Other signaling pathways may include matrix-derived factors such as BMP-2, transforming growth factor b, and insulin-like growth factor (IGF) [32,35]. In the formation phase, osteoblasts differentiate and secrete molecules to aid in bone formation, while in the termination/quiescence phase, remodeling concludes with an equal amount of resorbed and newly formed bone [27,36,37,38]. In the termination/quiescence phase, remodeling concludes when an equal quantity of newly formed bone replaces resorbed bone. After mineralization, osteoblasts may undergo different paths, for example, apoptosis, change in bone-lining cells, or become entombed within the bone matrix and terminally differentiate into osteocytes. Lastly, the bone surface undergoes a new remodeling cycle.
Systemic and local factors tightly control the remodeling cycle throughout signaling pathways, endocrine regulation, sex hormones, and growth factors. These control systems can act synergically or antagonistically, contributing to remodeling. Dis-regulations within this complicated functional network can be responsible for pathology conditions or diseases and thus be the starting point for new treatments. Table 1 summarizes and describes the significant players orchestrating the remodeling cycle [39].
2.3. Risk factors
Several risk factors are linked to low bone mass disorders and can be modifiable or unmodifiable. Unmodifiable factors are individuals, such as gender, ethnicity, aging, genetics, previous fractures or medications, comorbidities, and family history [40]. The risk and incidence of bone fractures are higher in women than men, with the chance increasing steeply with aging [40]. Indeed, this condition affects bone quantity and quality at cellular, molecular, and genetic levels and leads to alterations in the number, activity, and response of bone cells, resulting in bone loss and bone fragility [41]. These alterations favor the differentiation of mesenchymal stem cells into adipocytes instead of osteoblasts, leading to bone fat marrow accumulation [42].

Table 1.
Summary of the major players involved in bone remodeling.
| Bone remodeling regulation system |
Description |
|---|---|
| RANKL/RANK/OPG pathway |
|
| Wnt pathway |
|
| Endocrine regulation |
|
| Paracrine regulation |
|
Genetics is another risk factor for bone loss, and about 90 loci are associated with DXA-derived bone mineral density (BMD) and several other ones related to bone parameters such as bone geometry, shape, and microarchitecture. As reported by Rivadeneira et al., the involvement of genome-wide association studies (GWAS) has led researchers to discover several pathways that are potential targets for osteoporosis treatment [63]. It is also critical to consider the comorbidities that may affect the osteoporosis course and increase the risk of subsequent multiple fractures, especially in the presence of sarcopenia [64].
Osteoporosis severity indeed worsens in the presence of inflammatory bowel and joint diseases, breast and prostate cancer treated with chemotherapy or hormone therapy, diabetes, and celiac disease [65].
Modifiable risk factors are sex hormones, use of medications like glucocorticoids, body mass and body size, low Ca and vitamin D intake, hyperthyroidism, lifestyle habits (sedentary, cigarette smoking, excessive alcohol intake, and disuse/microgravity conditions) [66]. Estrogen binds the ERα receptor, an inhibitor of RANKL and an enhancer of OPG production in bone cells, thus acting on bone turnover [66]. Due to the estrogen deficiency, menopausal females have an overall increase in bone turnover, intensifying the responsiveness towards PTH and enhancing the resorption rate and amount. Another important modifiable factor is diet and nutrition. Insufficient Ca intake and hypovitaminosis D can lead to secondary hyperparathyroidism, which increases the production of IGF-binding protein, thus reducing the IGF action on bone cells [67]. It turns out that bone loss and skeletal turnover increase, while BMD decreases [68]. Moreover, with increasing age, there is a decline in energy intake by up to 20% in elders >65 years, and diet plays an essential role in muscle strength in elders [69].
In general, the Mediterranean diet, i.e., rich in vegetables, fruits, fish, and good fats, with reduced alcohol consumption, enhances muscle strength and functionality in older people. Due to the presence of thousands of chemical compounds, tobacco smoke affects (BMD) both directly and indirectly, impacting the RANK-RANKL-OPG pathway, intestinal microbiota composition, and Ca–P balance [70].
Lifestyle habits have essential consequences on GUT microbiota, crucial in maintaining the bone tissue’s overall health [71]. Within the modifiable factors, physical activity and exercise improve muscle mass, strength, and function, playing a protective role in mobility and bone health. In detail, weight-bearing and muscle-strengthening movements positively affect bone formation and, consequently, BMD [69]. Among environmental factors, air pollution could be partially adjustable. Higher levels of nitrogen oxide were associated with bone damage [72]. Heavy metals such as cadmium (Cd), lead (Pb), chromium (Cr), mercury (Hg), cobalt (Co), and other metal ions and trace elements have been the major contributors to bone damage. Endocrine disruptors like bisphenol A, phthalates, and per- and poly-fluoroalkyl compounds may cause a decrease in BMD [73].
The first therapeutic approach in clinical practice for treating osteoporosis is correcting or eliminating the "modifiable risk" factors like smoking, alcohol abuse, sedentary life, and all environmental conditions that increase the risk of falling. At the same time, the dietary intake or supplementation with vitamin D and Ca is of concern [74]. Vitamin D primarily aims to increase intestinal absorption of Ca, and the National osteoporosis Foundation recommends a daily intake of 800-1000 IU per day for over-50s. Indeed, physiological values of Ca and vitamin D are also a prerequisite for any drug treatment of osteoporosis.
2.4. Epidemiology and etiology of osteoporosis
Any process that causes an increase in the rate of bone remodeling will result in overall bone density loss. Peak bone mass comes about in the third decade of life, with exact age varying with sex and skeletal sites. After peaking, both sexes experience a decline in bone mass, but the loss can reach pathological levels during menopause in women. Bone loss negatively affects cortical and trabecular bone mass more rapidly in trabecular than cortical bone because the first one is more porous and has a higher turnover than the second one, thus increasing porosity and leading to skeletal fragility [75].
Osteopenia and osteoporosis occur when BMD values decrease due to an osteo-metabolic imbalance that disrupts the microarchitecture of bone tissue [76].
Osteopenia is a clinical term that describes a decrease in BMD below average reference values, yet not low enough to meet the diagnostic criteria of osteoporosis [77], thus describing it as a condition of “low bone density” or “decreased bone density.” However, the worsening of osteopenia leads to an increased risk of skeletal fractures, and consequently, preventing the development of osteoporosis and osteoporotic fractures is of great interest.
Osteoporosis is a common, debilitating, chronic, progressive, systemic, and metabolic skeletal disease affecting approximately 200 million women worldwide, resulting in painful fractures [78]. In European Union, it is assessed that among more than 23 million men and women are at high risk of osteoporotic fractures [79].
Primary Osteoporosis forms are related to female post-menopausal state (Type I) due to estrogen deficiency or advancing age (Type II) in men and women. Secondary OP derives from pre- or co-existing pathologies, medical conditions, or medications interfering with physiological bone formation [80].
The term “fragility fractures” indicates all the fractures resulting from low-level or low-energy trauma, such as a fall from standing height or less [81]. This type of fracture is generally considered the clinical outcome of osteoporosis. The most relevant consequence is that a patient who has sustained one fragility fracture is at high risk of experiencing secondary fractures, especially in the first two years following the initial fracture.
The most frequent fractures occur at the hip, spine, and forearm, even if other sites are included, such as the humerus, ribs, tibia, pelvis, and other femoral sites. The severe fracture complications are pain, loss of quality of life with substantial disability and loss of independence, and an increased risk of morbidity and mortality [82], with an approximately 20% mortality rate after hip and spine fractures [83]. As a further consequence, fragility fractures not only significantly impact the health and quality of life but also impose a significant economic burden on the health system [4].
For all these reasons, preventing fragility fractures is of significant concern. A multidisciplinary approach includes pharmacological intervention and changing lifestyle habits like nutrition and physical activity.
Fortunately, substantial advances in the diagnosis, prevention, and treatment of osteoporosis have emerged in the last decade to modify risk factors and tackle the ongoing osteoporosis crisis in the population [84].
2.5. Diagnosis
According to the World Health Organization's (WHO) indications, osteopenia and osteoporosis diagnosis relies mainly on BMD evaluation by densitometric investigation. The dual-energy x-ray absorptiometry (DXA) technique at the lumbar spine, proximal femur, or total hip is considered optimal for measuring BMD, recognized as a standard diagnostic criterion. The measurement unit is the number of standard deviations compared to peak bone mass (the average of healthy adults of the same gender), the “T score.” Conventionally, a T-score between − 1.0 and − 2.5 SD indicates osteopenia, while a value equal to or less than -2.5 defines osteoporosis. Severe osteoporosis presents a T-score below 2.5 SD with the simultaneous presence of one or more fragility fractures. Therefore, as the T-score decreases, the relative fracture risk increases. Thus, the T-score effectively identifies individuals at increased fracture risk and offers a cut-off point for diagnosing osteoporosis [85].
However, it is true that osteoporosis prevalence strictly depends on screening availability. Screening strategies with standard dual-energy X-ray absorptiometry (DXA) in women over 50 years are applied, but mostly in Western countries, and still need to be utilized in many other developing countries [86]. Moreover, osteoporosis in men is still largely underdiagnosed, and usually, the diagnosis occurs in the presence of a fragility fracture.
Other diagnostic imaging techniques for evaluating BMD are quantitative computerized tomography (QCT) or ultrasound (QUS) studies and conventional radiology to diagnose spinal fractures. QUS studies demonstrated that they were not inferior to lumbar or femoral DXA in terms of accuracy. However, this technique does not represent a direct measurement of BMD, so it cannot be used to diagnose osteoporosis, according to WHO criteria.
Traditional radiology allows the diagnosis of osteoporotic fractures in the most involved sites: spine, ribs, pelvis, proximal femur, proximal humerus, distal radius, and calcaneus. MRI applies when several vertebrae are involved in fractures, thanks to the possibility of distinguishing recent fractures from older ones [87].
An easier and BMD-independent way to identify individuals at high fracture risk is the available fracture risk algorithm “FRAX," a computer-based algorithm that provides models for assessing fracture probability in men and women. FRAX uses clinical risk factors to estimate 10-year fracture probability based on validation in independent cohorts with a similar geographic distribution. It has intrinsic limitations due mainly to the use of dichotomous variables only, and it should not be considered a gold standard but is reliable in assessing fracture risk [87,88].
In the context of diagnosis, there is an urgent need to identify measurable biomarkers in clinical trials that are useful in clinical practice.
2.6. Therapeutical approaches
Osteoporosis is a latent disease that can be prevented and treated, but it is often only detectable in its final stages [89].
Table 2 shows a summary of drugs used in clinical practice and involved in clinical trials, with attention to potential adverse effects. Currently, there are various classes of drugs available for osteoporosis treatment. Still, they possess adverse effects like atrial fibrillation, atypical subtrochanteric fracture, delayed fracture healing, hypersensitivity reactions, hot flashes, leg cramps, and gastrointestinal effects like nausea, vomiting, and constipation [90]. However, the current Literature highlights that approved drugs for treating osteoporosis reduce the risk of fragility fractures and their severe consequences in terms of disability and related mortality, thus exceeding the risk of adverse events.
The most used treatments for women and men are bisphosphonates and calcitonin, which act by inhibiting bone resorption. Other drugs act with an anabolic mechanism of action (teriparatide and abaloparatide) or with a dual anabolic/antiresorptive mechanism (romosozumab and strontium ranelate). In the case of post-menopausal osteoporosis, pharmacological treatment begins with estrogens as hormone replacement therapy to manage menopause symptoms and strengthen bones, thus acting as both prevention and treatment of bone fragility. Other classes of drugs are selective estrogen receptor modulators (SERMs) for women, RANKL inhibitors, PTH analogs, calcitonin, and anti-sclerostin inhibitors for both men and women [91].
Table 2.
Pharmacological drugs used for osteoporosis.
| Drug class | Mechanism of action | Adverse effects | Refs. |
| Anti-resorptive drugs | |||
| Non-nitrogen-containing bisphosphonates (NNBP) (Etidronate, Clodronate, Tiludronate) | Induction of osteoclast apoptosis by conversion into ATP analogues in the cytoplasm | Atypical femoral fractures, osteonecrosis of the jaw, acid regurgitation hypocalcemia, esophageal ulcers | [92] |
| Nitrogen-containing bisphosphonates (NBP) (Alendronate, Risedronate, Ibandronate, Neridronate, Pamidronate) |
Inhibition of mevalonate pathway (cholesterol biosynthesis) | Dysphagia, nausea, constipation/diarrhea, gastritis, flatulence | [93] |
| Selective estrogen receptor modulators (SERMs) (Tamoxifen, Raloxifene, Bazedoxifene, Ospemifene) | Bind to estrogen receptors with an agonistic effect at bone and hepatic level and a partially antagonistic effect at breast and the genitourinary system level | Hot flushes, leg cramps, risk of blood clots and stroke, increased likelihood of developing uterine cancer, blood clots, and menopausal symptoms | [94,95] |
| RANKL inhibitor (Denosumab) | Binding to RANKL leads to osteoclast inactivation and apoptosis | Jaw osteonecrosis, musculoskeletal pain, atypical femoral fracture, gastrointestinal symptoms | [96] |
| Enzyme replacement therapy (ERT) (Estrogen) | Bind to estrogen receptors, inducing osteoclast apoptosis | Breast cancer, heart disease, stroke, venous thrombo-embolic disorders | [97] |
| Calcitonin | Inhibit osteoclast function | Vomiting, nausea, inflammation at the injection site, diarrhea, gastrointestinal signs, stomach pain | [98] |
| Cathepsin K inhibitor (Odanacatib and Balicatib)* |
Inhibit osteoclast resorption | Skin adverse experiences | [99,100,101] |
| Bone-forming drugs | |||
| PTH analogs (Teriparatide) |
Bind PTH1R on osteoblasts, increasing bone formation | Dizziness, nausea, headache, leg cramps, osteosarcoma | [102] |
| Human PTH-related protein (PTHrP) (Abaloparatide) |
Bind PTH1R on osteoblasts, increasing bone formation | Gastrointestinal symptoms, site reaction, osteosarcoma, dizziness, myalgia | [103] |
| Dual-actions drugs | |||
| Anti-sclerostin antibody (Romosozumab) | Binds to sclerostin, preventing the inhibition of the Wnt pathway by sclerostin, and reduces bone resorption | Stroke, cardiovascular disorders, myocardial infarction | [104,105] |
| Strontium ranelate (Protelos, Osseor) | Bind to Ca sensing receptors inhibiting osteoclast activity | Cardiovascular risk and non-fatal myocardial infarctions | [106,107,108] |
Note: *not FDA-approved drug.
3. Nutraceuticals
Thanks to increased knowledge about the protective role of numerous bioactive compounds, adequate nutrition has been associated with health, which is now seen as a low risk of developing diseases instead of the absence of pathologies [109,110]. This awareness among people of the benefits of nutrition has caused a rise in the demand for nutraceuticals [111,112,113,114].
Nutraceutical is a term that combines "nutrient," referring to nourishing food, and "pharmaceutical," which denotes medical drugs. Nutraceuticals are nutrient formulations that are non-specific in action and help maintain and improve health, thus preventing various diseases and health issues. Nutraceuticals are a powerful resource that can be used "beyond the diet but before the drugs" to prevent and treat pathological conditions as "pharma-foods" [115]. In recent years, the focus of nutraceuticals has shifted to efficacy, safety, epidemiology, and toxicity [116,117].
A clear distinction between supplements and nutraceuticals is still lacking. Generally, nutraceuticals include single or combinations of pro- and pre-biotic edible substances and food for special medical uses. On the other hand, food supplements include single or combinations of minerals, vitamins, protein supplements, functional foods, and herbal products that act as agents to compensate for deficiencies in micro- or macronutrients [118].
3.1. Nutraceutical for bone health
Nutraceutical products are abundant and constantly increasing, constituting a non-homogeneous and diversified group. Nutraceuticals can be classified based on different parameters such as source, chemical constitution, and bioavailability. However, there is a need for a standardized nomenclature and classification. Concerning bone health, a wide range of nutraceuticals exist. Rajput et al. described four main categories: minerals, herbs and phytochemicals, dairy products, and miscellaneous [119]. Figure 1 visually depicts this categorization.
3.1.1. Minerals
Calcium
Calcium (Ca) makes up 1.9% of the body by weight, and 99% of Ca resides in bones and teeth in the form of P salt, which provides mechanical rigidity. Ca intake is critical throughout the whole life for physiological skeletal growth and development, as well as for bone mineralization. During teenage years, calcium intake helps attaining the peak BMD, which can later help delaying osteoporosis. PTH mobilize Ca from the bones if its loss from the extracellular fluid exceeds its intake via the gut to protect the neuromuscular system; excess PTH production such as in primary hyperparathyroidism, can lead to osteoporosis [120].
The recommended Ca intake is about 1200 mg/day for young adults, 1000 mg/day for women aged 25 to 50, and 1500 mg/day for post-menopausal women [121,122]. A sufficient Ca intake is necessary for the efficacy of various potent therapeutic agents, such as bisphosphonates.
Ca-rich foods include milk, cheese, yogurt, soybeans, and dry leafy vegetables like spinach, but also salmon, almonds, legumes, tofu, seafood, and Ca-fortified foods, especially orange juice [123]. Attention must be paid to the assumption of oxalic and phytic acid and Na consumption since they can interfere with Ca absorption [124].
Magnesium
Magnesium (Mg) is fundamental for energy metabolism (it binds ATP) and acts as a cofactor for many enzymes. Moreover, this mineral stabilizes the cell membrane with its positive charge [125]. In the human body, about 60% of the entire (Mg) resides in the bones, either on the hydroxyapatite surface or in the hydration shell of the crystals. Similarly to Ca, it can be mobilized by increased intestinal absorption to maintain serum levels proper for the numerous physiological functions in the body [126]. The excessive intake of Mg might harm osseous metabolism by interfering with the generation of hydroxyapatite crystals due to competition with Ca, thus reducing bone mass [127].
Magnesium deficiency profoundly impacts bone health both directly (enhancing osteoclast and reducing osteoblast activity, decreasing bone stiffness, altering the apatite crystal structure, and leading to larger crystals that cannot bear the physiological load) and indirectly (interfering with vitamin D and PTH, and consequently with the homeostasis of Ca) [127,128]. In addition, Mg contrasts the acidic environment of inflammation and protects the skeleton from deteriorating effects like releasing inflammatory cytokines that stimulate bone loss.
The primary sources of Mg are green vegetables (spinach), legumes, nuts, seeds, and unprocessed grains. Excessive intake of alcohol and coffee, inappropriate diet, stress, and various diseases can adversely influence the content of Mg in the body [41].
Phosphorous
Together with Ca, phosphorus is an essential bone-forming element for mineralization. There is little evidence that it affects the incidence of osteoporosis.
Potassium
Potassium helps maintain an alkaline environment, balancing the endogenous acids produced from acid-generating foods like meat. This mechanism contributes to preserving Ca in bones, which might otherwise be mobilized to maintain normal pH. From this perspective, potassium-rich foods help prevent osteoporosis [129,131]. Potassium can be found naturally in many foods such as bananas, avocados, spinach, squash, cantaloupe, artichokes, potatoes, sweet potatoes, oranges, dried apricots, and prunes [131].
Iron
Iron acts as a cofactor in enzymes involved in collagen bone matrix synthesis, prolyl, and lysyl hydroxylases, and in converting vitamin D to the active form. This, in turn, influences the absorption of calcium in the body [129].
On the other hand, conditions of iron overload are associated with weakened bones, altered bone microarchitecture, biomechanics, and an increased risk of bone fractures [132]. Iron is available in two forms in foods: heme iron, found in animal products such as meat, poultry, and fish, and non-heme iron, which is present in plant-based foods such as cereals, pulses, legumes, grains, nuts, and vegetables [133].
Zinc
Boron
Boron stabilizes and increases the half-life of vitamin D and estrogen, thus preventing loss of Ca and bone demineralization. Studies conducted on humans have revealed that boron taken from the diet is helpful in bone loss prevention [136]. Several foods contain boron, such as avocado, apricots (dried), currants, raisins, hazelnuts, and others [137].
Copper
Copper is involved in collagen fibril formation; thereby, it is essential for increasing the mechanical strength of bone matrix [129,138,139]. Conlan et al. reported significant deficiency in old patients with femoral neck fractures compared to control groups [140].
In addition, copper is a cofactor for all antioxidant enzymes and eliminates the body's free radicals caused by osteoclast activation. Fruits, legumes, potatoes, and cereals are some foods containing copper [141].
3.1.2. Herbs & phytochemicals
Curcumin
Curcuma longa is a main coloring component of turmeric originally used as a spice in the Indian subcontinent. Several studies described curcumin in vitro and in vivo potential in contrasting bone loss by downregulating NF-κB, Wnt/β-catenin, RANKL, and TNF-α [142,143,144] and enhancing the osteoblast differentiation of human adipose-derived MSCs by inhibiting Wnt/β-catenin signaling [145].
Alfalfa
Alfalfa (Medicago sativa L.) is a plant indigenous to the Eurasian continent, which contains ipriflavone, an isoflavone derivative able to directly inhibit bone resorption, enhance osteoblast proliferation and induce estrogen-mediated calcitonin secretion [146]. Indeed, ipriflavone enhances estrogenic activity, potentiating the protective action of estrogen on bones [147].
Red clover
Horsetail
Equisetum arvense L., commonly known as horsetail, is native to the northern hemisphere. It is a commonly used herb in the treatment of osteoporosis, as it contains numerous phytoconstituents favorable for bone health, such as silica, flavonoids (quercetin, kaempferol, luteolin, and apigenin), and triterpenoids (oleanolic acid, betulinic acid, and ursolic acid). Silica support collagen formation and bone calcification, and flavonoids preserve bone, avoiding bone resorption and stimulating osteoblast differentiation [150,151].
Citrus fruits
Oranges, grapefruit, and lemons are rich sources of micronutrients like potassium, magnesium, vitamin C, and folic acid, limonoids, and flavonoids. Beyond the already discussed mineral properties, limonoids and flavonoids possess antioxidant effects, thus contrasting oxidative stress produced during bone resorption that contributes to osteoporosis [152].
Alliaceae and Brassicaceae
Polysulfides contained in Alliaceae and isothiocyanates in Brassicaceae have anti-inflammatory, antioxidants, vasorelaxant, and hypolipemic potential. These compounds can stimulate osteoblast bone-forming activity AND reduce osteoclast bone resorption by releasing hydrogen sulfide (H2S), a gasotransmitter. To read in detail about the Alliaceae- and Brassicaceae-derived organosulfur compounds and their effects on bone loss in vitro and in vivo, please refer to the review by Gambari et al. [153].
Among the Alliaceae family, onion (Allium cepa L.) is a bulb-shaped vegetable that is rich in flavonoids such as quercetin, rutin, and organo-sulfur conjugates [154]. Pre-clinical studies have suggested that onion can inhibit resorption of bone and differentiation of osteoclast, which helps maintain normal bone mineral density [155,156].
Onion has also been found to have beneficial effects on bone density in peri- and post-menopausal women [157].
Garlic (Allium sativum) has been shown to reduce oxidative stress in menopausal women when administered in tablet form over a period of 30 days [158].
Oxidative stress is a key player in the development and progression of osteoporosis. The reduction of plasma levels of carbonyl groups and Advanced Oxidation Protein products and an increase in the total antioxidant capacity were observed. Garlic and leek have also been found to suppress bone resorption [159].
Green tea
The beverage derived from dried leaves of Camellia sinensis contains polyphenolic compounds known as catechins, which include epigallocatechin gallate, epicatechin gallate, epicatechin, and epigallocatechin [160]. Epigallocatechin-3-gallate can suppress osteoclast formation and bone resorption by causing osteoclast cell death, suppressing matrix metalloproteinase-9 in osteoblast, inhibiting IL-6, suppressing p44/p42 mitogen-activated protein, and down-regulating RANKL-induced expression. At the same time, epigallocatechin-3-gallate can reduce TNF-α and IL-6, promoting osteoblast survival and positively acting on bone formation [161].
Herba Epimedii
Herba Epimedii (HEP) is a traditional Chinese medicine that contains icariin, a flavonoid glycoside which has been found to prevent inflammatory bone loss by inhibiting lipopolysaccharide-induced osteoclastogenesis, TNF-α, and IL-6, as well as the production of cyclooxygenase type-2 and prostaglandin E2 [162].
Berries
Berries include strawberries, blueberries, raspberries, blackberries, and blackcurrants, rich in organic acids like fumaric and citric acid, vitamins like A, B9, C, E, and K, minerals, and carotenoids. Berries have antioxidant [163] and anti-inflammatory properties; they improve osteoblast differentiation by modulating some enzymes, cellular singling pathways, and gene expression. For example, raspberry trans-retinoid acid and ketones stimulate osteoblast differentiation by improving osteocalcin expression in the stem cell culture system. Berries also contain phenolics like flavonoids (anthocyanins, flavonols, and flavanols), phenolic acids, proanthocyanidins, ellagitannins, gallotannins, and stilbenoids. Anthocyanidine seems to inhibit RANKL and, consequently, osteoclastogenesis [164].
Plums
Dried plums or prunes contain carbohydrates, vitamins A, B, and K, potassium, Ca, magnesium, boron, selenium, dietary fibres and polyphenols like chlorogenic acid, rutin, and proanthocyanidin. Boron and selenium positively affect bone metabolism, helping the maintenance of BMD; polyphenols decrease bone resorption, acting on RANKL signaling [165]. Arjmandi et al. observed that administering dried plums on fifty-eight post-menopausal females induced higher levels of IGF-1 and bone-specific alkaline phosphatase (BSAP)[166].
Resveratrol
It is a phytoestrogen, a polyphenolic compound found in red wine and several nourishments like nuts, grapes, and cranberries. Resveratrol acts on Runx2 and Osterix in osteoprogenitor cells and on osteoclast gene expression via RANKL. In addition, it possesses antioxidant and anti-inflammatory properties [167,168].
3.1.3. Dairy products
Milk and milk-derived products are rich in Ca, proteins, lipids, potassium, sodium, zinc, P, and vitamins A and B2, thus valuable for bone loss prevention. Functional milk compounds like casein phosphopeptide, milk basic protein (MBP), and lactoferrin contribute to bone health by enhancing osteoblast proliferation and differentiation while preventing osteoclast formation. Indeed, the administration of MBP (40 mg/day) on healthy menopausal females showed positive effects on BMD [169,170,171].
3.1.4. Miscellaneous
Probiotics
Probiotics are bacterial components of the physiologic human intestinal flora (probiotic means “for life”). They generate final products of short-chain fatty acids and lactate metabolism. Thanks to the production of vitamins D, C, K, and folate, which are associated with Ca metabolism and are essential for bone formation, they act positively on bone health. Lactobacillus and Bifidobacteria are commonly investigated bacteria for bone [172].
Prebiotics
The food ingredients that are not digested but selectively fermented by the intestinal microflora potentially support bacteria growth, generating positive effects for the host. Among them, non-digestible oligosaccharides (NODs) can enhance mineral absorption to boost bone mineralization [173,174]. NODs include lactulose, galactooligosaccharides (GOS), fructooligosaccharides (FOS), oligofructose, and inulin [175].
Polyunsaturated fatty acid
PUFAs (Polyunsaturated fatty acids) primarily contain n-6 and n-3 fatty acids as two main classes; n-6 fatty acids derive from linoleic acid, present in vegetable oils; n-3 fatty acids, eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) are found in fish and fish oil. An elevated omega-3/omega-6 fatty acids ratio is associated with a positive stimulation of bone remodeling by three main pathways: Ca absorption, inflammatory cytokines, and peroxisomes proliferators-activated receptor gamma [176].
Melatonin
It is a hormone secreted and released by the pineal gland at night and is responsible for diurnal variation. Melatonin increases human growth hormone, corticosteroids, and osteoclast metabolism. At the same time, it stimulates matrix proteins (procollagen type I c-peptide) and osteoprotegerin, thus balancing osteoclast differentiation [177]. It also acts as a scavenger of hydroxyl and pyroxyl molecules with antioxidant activity [178]. The administration of melatonin to Wistar rats demonstrated beneficial effects on bone volume and stiffness compared to the control group [179].
3.2. Effects on GUT microbiota.
One of the health benefits of nutraceuticals may be their potential to affect and change gut microbiota by modifying its composition, thus interfering with patient's health status [180]. The gastrointestinal tract is the most developed microbiota in the body, but microorganisms also colonize other areas such as the respiratory tract, skin, and vagina [181].
In a healthy adult, the gut microbiota is dominated by six bacterial Phyla, with Firmicutes and Bacteroidetes making up 90% of total. The proportion of these two phyla remains constant throughout a person's life. The other Phyla are Proteobacteria, Actinobacteria, Fusobacteria, and Verrucomicrobia [182].
The gut microbiota (GM) regulates bone metabolism through both direct and indirect mechanisms. Directly, GM affects bone remodeling by releasing extracellular vesicles (EVs) or microbial metabolites like short-chain fatty acids (SCFAs), polyamines, and hydrogen sulfide (H2S). Indirectly, it regulates bone remodeling by interacting with immune cells, such as T helper cells 17 (Th17 cells) and T regulatory cells (Treg cells), or hormones like estrogen and PTH. For a detailed review on how the gut microbiota modulates bone remodeling, please refer to [71]
Gut-associated metabolites (GAMs) are small molecules produced by food metabolism by gut bacteria. They can affect the host's energy metabolism and immune local and systemic homeostasis [183,184,185,186,187,188]. GAMs can degrade amino-acids forming short-chain fatty acids (SCFAs) and other metabolites like acetate (C2), propionate (C3), butyrate (C4), pentanoate (C5), and hexanoate (C6) [76] . Moreover, they may interfere with the regulation of lipid metabolism, majorly affecting glycerol, phospholipids, fatty acids, bile acids, and sphingolipids [189]. In osteoporotic patients, lipid metabolism changes can lead to the accumulation of lipids, which result in lipid oxidation and the production of lipid metabolites. These metabolites can activate peroxisome proliferator-activated receptor γ (PPARγ), responsible for inhibiting osteoblast differentiation and stimulating adipogenesis [76].
4. Discussion
We utilized the "Strengths, Weaknesses, Opportunities, Threats (SWOT)" analysis to identify and discuss the advantages and disadvantages of Nutraceuticals for preventing bone loss and osteoporosis (Figure 2). The SWOT analysis is a helpful tool for strategic planning. It helps identifying the characteristics of a project, program, or organization and its relationship with the operating environment. This analysis framework enables us to define future directions to achieve an objective by considering internal and external variables. The SWOT analysis uses a matrix divided into four fields: Strengths, Weaknesses, Opportunities, and Threats. Strengths are internal factors that can be leveraged, whereas weaknesses are internal limitations that must be addressed. Opportunities are external possibilities that can be capitalized on, while threats are external issues that need to be evaluated and faced. Internal variables can be managed, whereas external variables are beyond its control but can be managed to limit risks and capitalize on positive factors. The SWOT analysis has several advantages, such as providing an effective cross-reading and in-depth analysis of the context, which results in an outline of possible strategies. However, the limitations of SWOT analysis mainly arise from the risk of subjectivity and oversimplification by the evaluation team.
4.1. Strengths
Natural nutraceuticals are a vast, heterogeneous group mainly derived from natural food.
They can be prepared for patients in various “friendly” forms, such as tablets, capsules, liquids, and powders, making them more convenient for consumption.
Nutraceuticals hold promises for osteopenia and osteoporosis, as they seem to have fewer side effects and a lower drug interaction risk than conventional pharmaceuticals [190]. Nutraceuticals can also be combined with other nutraceuticals, supplements, or drugs to enhance their therapeutic effects or improve absorption [119,191].
4.2. Weakness
Nutraceuticals’ availability is often subject to non-homogenous distribution across countries, seasonal variations, and crop yield fluctuations. This diversification can impact the quantity and quality of nutraceutical ingredients, leading to potential supply shortages or price fluctuations.
Moreover, the manufacturing process can be complex, time-consuming, expensive, and carry contaminants. Nutraceutical contamination can occur during any stage of production with pesticides, heavy metals and metalloids, mycotoxins, and radioactivity, or adulterated with drugs, with alterations in quality and safety. The population and healthcare professionals should be better informed regarding the concept and usefulness of nutraceuticals and regarding the potential adverse effects associated with their possible contamination [192].
Lastly, it is important to carefully evaluate the potential interference of nutraceuticals with other nutraceuticals or therapeutic drugs to avoid undesired changes in absorption, bioavailability, transport, metabolism, elimination, and side effects [193].
4.3. Opportunities
The global nutraceuticals market, constantly increasing within the healthcare sector, has recently shifted towards prevention strategies instead of costly therapeutical ones. Additionally, consumers prefer natural and organic ingredients and personalized nutrition over synthetic pharmaceutics, which may have potential side effects. The variety of nutraceuticals and their formulations allow for a wide distribution range, including hypermarkets, supermarkets, pharmacies, and online sales channels. The nutraceuticals field is an attractive market for Academia, pharmaceutical and food companies, and this will hopefully increase efforts to improve efficiency, quality, and variety.
Consumers are becoming more aware of natural-based alternatives and nutraceuticals, which may lead to better patient compliance. With an increasing aging population, preserving bone and joint health and avoiding drugs has become a top priority.
4.4. Threats
There is a non-homogeneous regulation of nutraceuticals worldwide since their definition varies from country to country, according to the different national regulatory agencies. Moreover, requirements for Nutraceuticals’ production are not stringent as much as for drugs causing lack of data on safety and outcomes.
In some countries, nutraceuticals are primarily regulated as a food category, focusing on safety and labeling [194]. However, they do not always have a specific definition distinct from other food-derived categories, such as supplements, herbal products, pre- and pro-biotics, functional foods, and fortified foods. Table 3 shows an overview of the Nutraceuticals' regulation in the main areas/countries. For a detailed update of the "regulatory framework and pertinent policies concerning nutraceuticals in some of the key global markets," see the review of Chopra et al. [195]. Overall, Nutraceuticals require a proper and unequivocal definition and a shared regulation to protect the category and safeguard consumers' health while avoiding counterfeits.
It has been reported that Nutraceuticals can have positive effects, but their quality and active compounds need to be systematically assessed. Unfortunately, most data on the uniformity and quality of these products are currently unavailable [196]. This highlights the need for a common regulation of Nutraceuticals. More studies need to be conducted to demonstrate the effectiveness of Nutraceuticals in preventing osteopenia and osteoporosis. It is essential to have proper knowledge about the dosage and intake regimen to avoid inappropriate use or overuse that can lead to toxic effects and health complications.
Self-medication is a potential risk and patients only sometimes disclose supplement use to their physicians. Therefore, a dedicated effort is necessary to establish a more solid basis for using these compounds [190,197].
It is necessary to reflect on the traditional drug's Clinical Trial model and consider whether it is practical for Nutraceuticals. Some authors criticize this model [198,199,200,201,202,203] because it can be costly and only sometimes feasible to assess nutraceuticals' safety, efficacy, and mechanisms of action [204,205].
The multifunctional nature of nutraceuticals can make it hard to estimate their effects and to choose the appropriate time points and biomarkers. Another issue concerns control groups. Is it possible to recruit "real" placebo groups and healthy participants? [206]. In addition, patients enrolled in a clinical trial for nutraceuticals must maintain specific healthy lifestyle habits not to influence data; this, in turn, can generate a high dropout rate.
The statistical analysis method used for Nutraceuticals may require some changes. The commonly used p-value only sometimes considers the effect size and only partially addresses the accuracy of the study hypothesis. Therefore, alternative frameworks such as statistical power, and false positives and negatives have been proposed as potential solutions [207]. It has been proposed that a change in focus is needed when evaluating nutrients. Instead of mainly looking at their effectiveness, we should also consider the potential harm they might cause. Some nutrition and nutraceutical studies utilized the N-of-1 study design which may address their heterogeneity, and crossover features, including carry-over effects [208,209,210,211,212]. There is a significant concern regarding how to create a patent strategy for Nutraceuticals that can attract investments and investors. Discovering new ingredients with scientifically proven health benefits is crucial for this purpose. However, it is challenging because natural ingredients that are beneficial to health cannot be patented.
Furthermore, synthetic food supplements pose a significant challenge and competition as they constitute a large market. This is especially true for single nutrients, such as vitamins, minerals, amino acids, and antioxidants, that are not included in the Nutraceuticals category.
Table 3.
Overview of Nutraceuticals’ regulations.
| Area/Country | Regulation | Ref/Link |
| European Union (EU) |
The European Food and Safety Authority (EFSA) is responsible for regulating food legislation and considers food supplements as foods. | EU regulation CE n. 178/2002 |
| The European Commission has established harmonized rules to safeguard consumers against possible health risks for ingredients other than vitamins and minerals. | https://www.efsa.europa.eu/en/topics/topic/food-supplements | |
| New products must meet strict development and quality requirements. Before the products reach the market, EFSA must authorize any health claim, and subsequently, each EU State can decide to set specific approval regulations and/or authorization. However, EFSA does not have any mandate to act against any unsafe products once they are on the market | Directive 2002/46/EC | |
| United States | The Food and Drug Administration (FDA) regulates nutraceuticals differently from “conventional foods” and drugs. In 1994, the Dietary Supplement Health and Education Act (DSHEA) stated that manufacturers must ensure nutraceutical safety and efficacy before market release. It is not mandatory for FDA to approve or register nutraceuticals before producing or selling them. However, nutraceuticals must meet high standards of trial design and patient safety and be reviewed by the Investigational New Drug (IND) application process. FDA is authorized to act against any unsafe product after it reaches the market. |
[213] |
| India | The Food Safety and Standards Act does not assign any specific legal status to nutraceuticals. | Food safety and Standard Act, 2006 No. 34 OF 2006. |
| Australia | Nutraceuticals come under the category of food, and therefore, the national regulations for food are applied. | Therapeutic Goods Administration (TGA) |
| Canada | There are explicit sets of rules for supplements and nutraceuticals that are regulated more closely as a drug than a food category. | [214,215] |
| Latin America | Colombia, Brazil, and Argentina require the registration of a new nutraceutical in the market. In Brazil, animal and/or human clinical studies before product registration are mandatory. Mexico and Chile follow a notification-based approach. |
[213] |
| China and Taiwan | Before product registration, regulators require animal and/or human clinical studies. | [213] |
| Japan | It was the first country to recognize and regulate functional foods through the establishment of Foods for Specified Health Use (FOSHU) in 1991. Later, this evolved into the 2003 Health Promotion Law, which allowed foods with beneficial health activities and meeting FOSHU requirements (including safety and nutritionally appropriate ingredient content) to obtain approval as nutraceutical. Japan has a well-established market in nutraceuticals dating back to the 1980s | [194] |
5. Conclusions
An aware consumption of specific Nutraceuticals may help preventing a worsening of the general bone status. However, Nutraceuticals still face many challenges and objectives to achieve. The path from now lies in creating an exhaustive and evidence-based pool of data on Nutraceuticals’ safety, effects, dosage, potential adverse effects, and interactions with other compounds. New studies are mainly required to understand the mechanism of action and investigate the effects on bone health. It is crucial targeting future clinical studies on post-menopausal women, susceptible to primary osteoporosis that is closely related to estrogen deficiency.
Author Contributions
Conceptualization, B.G., L.R., G.B.; methodology, L.R. and G.B.; data curation, G.B., G.D., L.G.; writing—original draft preparation, L.R. and G.B.; writing—review and editing, F.G. and L.G.; supervision, B.G.; project administration, B.G.; funding acquisition, B.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
No new data were created.
Acknowledgments
We would like to thank Patrizia Rappini for her assistance in preparing the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Albrecht, B.M.; Stalling, I.; Foettinger, L.; Recke, C.; Bammann, K. Adherence to Lifestyle Recommendations for Bone Health in Older Adults with and without Osteoporosis: Cross-Sectional Results of the OUTDOOR ACTIVE Study. Nutrients 2022, 14. [Google Scholar] [CrossRef]
- Zamudio-Rodríguez, A.; Letenneur, L.; Féart, C.; Avila-Funes, J.A.; Amieva, H.; Pérès, K. The Disability Process: Is There a Place for Frailty? Age Ageing 2020, 49, 764–770. [Google Scholar] [CrossRef] [PubMed]
- Cristea, M.; Noja, G.G.; Stefea, P.; Sala, A.L. The Impact of Population Aging and Public Health Support on EU Labor Markets. Int J Environ Res Public Health 2020, 17. [Google Scholar] [CrossRef] [PubMed]
- Kemmak, A.R.; Rezapour, A.; Jahangiri, R.; Nikjoo, S.; Farabi, H.; Soleimanpour, S. Economic Burden of Osteoporosis in the World: A Systematic Review. Med J Islam Repub Iran 2020, 34, 1–8. [Google Scholar]
- Lindsay, B.R.; Olufade, T.; Bauer, J.; Babrowicz, J.; Hahn, R. Patient-Reported Barriers to Osteoporosis Therapy. Arch Osteoporos 2016, 11. [Google Scholar] [CrossRef] [PubMed]
- Valentin, G.; Ravn, M.B.; Jensen, E.K.; Friis, K.; Bhimjiyani, A.; Ben-Shlomo, Y.; Hartley, A.; Nielsen, C.P.; Langdahl, B.; Gregson, C.L. Socio-Economic Inequalities in Fragility Fracture Incidence: A Systematic Review and Meta-Analysis of 61 Observational Studies. Osteoporosis International 2021, 32, 2433–2448. [Google Scholar] [CrossRef] [PubMed]
- Hejazi, J.; Davoodi, A.; Khosravi, M.; Sedaghat, M.; Abedi, V.; Hosseinverdi, S.; Ehrampoush, E.; Homayounfar, R.; Shojaie, L. Nutrition and Osteoporosis Prevention and Treatment. Biomedical Research and Therapy 2020, 7, 3709–3720. [Google Scholar] [CrossRef]
- Pandey, M.K.; Gupta, S.C.; Karelia, D.; Gilhooley, P.J.; Shakibaei, M.; Aggarwal, B.B. Dietary Nutraceuticals as Backbone for Bone Health. Biotechnol Adv 2018, 36, 1633–1648. [Google Scholar] [CrossRef] [PubMed]
- Nwosu, O.K.; Ubaoji, K.I. Nutraceuticals: History, Classification and Market Demand. In Functional Foods and Nutraceuticals; Springer International Publishing: Cham, 2020; pp. 13–22. [Google Scholar]
- Florencio-Silva, R.; Sasso, G.R.D.S.; Sasso-Cerri, E.; Simões, M.J.; Cerri, P.S. Biology of Bone Tissue: Structure, Function, and Factors That Influence Bone Cells. Biomed Res Int 2015, 2015. [Google Scholar] [CrossRef]
- DiGirolamo, D.J.; Clemens, T.L.; Kousteni, S. The Skeleton as an Endocrine Organ. Nature Publishing Group 2012, 8, 674–683. [Google Scholar] [CrossRef]
- Mera, P.; Laue, K.; Ferron, M.; Confavreux, C.; Wei, J.; Galán-Díez, M.; Lacampagne, A.; Mitchell, S.J.; Mattison, J.A.; Chen, Y.; et al. Osteocalcin Signaling in Myofibers Is Necessary and Sufficient for Optimum Adaptation to Exercise. Cell Metab 2016, 23, 1078–1092. [Google Scholar] [CrossRef]
- Mosialou, I.; Shikhel, S.; Liu, J.M.; Maurizi, A.; Luo, N.; He, Z.; Huang, Y.; Zong, H.; Friedman, R.A.; Barasch, J.; et al. MC4R-Dependent Suppression of Appetite by Bone-Derived Lipocalin 2. Nature 2017, 543, 385–390. [Google Scholar] [CrossRef]
- Oldknow, K.J.; MacRae, V.E.; Farquharson, C. Endocrine Role of Bone: Recent and Emerging Perspectives beyond Osteocalcin. Journal of Endocrinology 2015, 225, R1–R19. [Google Scholar] [CrossRef] [PubMed]
- Ubara, Y.; Fushimi, T.; Tagami, T.; Sawa, N.; Hoshino, J.; Yokota, M.; Katori, H.; Takemoto, F.; Hara, S. Histomorphometric Features of Bone in Patients with Primary and Secondary Hypoparathyroidism. Kidney Int 2003, 63, 1809–1816. [Google Scholar] [CrossRef] [PubMed]
- Ubara, Y.; Tagami, T.; Nakanishi, S.; Sawa, N.; Hoshino, J.; Suwabe, T.; Katori, H.; Takemoto, F.; Hara, S.; Takaichi, K. Significance of Minimodeling in Dialysis Patients with Adynamic Bone Disease. Kidney Int 2005, 68, 833–839. [Google Scholar] [CrossRef]
- Bellido, T. Osteocyte-Driven Bone Remodeling. Calcif Tissue Int 2014, 94, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Kronenberg, H.M. Developmental Regulation of the Growth Plate. Nature 2003, 423, 332–336. [Google Scholar] [CrossRef]
- Clarke, B. Normal Bone Anatomy and Physiology. Clin J Am Soc Nephrol 2008, 3 Suppl 3.
- Mackie, E.J.; Tatarczuch, L.; Mirams, M. The Skeleton: A Multi-Functional Complex Organ. The Growth Plate Chondrocyte and Endochondral Ossification. Journal of Endocrinology 2011, 211, 109–121. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.; Zhu, L.; Hou, N.; Lan, Y.; Wu, X.M.; Zhou, B.; Teng, Y.; Yang, X. Osteogenic Fate of Hypertrophic Chondrocytes. Cell Res 2014, 24, 1266–1269. [Google Scholar] [CrossRef]
- Duer, M.J. The Contribution of Solid-State NMR Spectroscopy to Understanding Biomineralization: Atomic and Molecular Structure of Bone. Journal of Magnetic Resonance 2015, 253, 98–110. [Google Scholar] [CrossRef]
- Zhang, W.; Zhu, Y.; Li, J.; Guo, Q.; Peng, J.; Liu, S.; Yang, J.; Wang, Y. Cell-Derived Extracellular Matrix: Basic Characteristics and Current Applications in Orthopedic Tissue Engineering. Tissue Eng Part B Rev 2016, 22, 193–207. [Google Scholar] [CrossRef]
- Bentolila, V.; Boyce, T.M.; Fyhrie, D.P.; Drumb, R.; Skerry, T.M.; Schaffler, M.B. Intracortical Remodeling in Adult Rat Long Bones after Fatigue Loading. Bone 1998, 23, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Manolagas, S.C. Birth and Death of Bone Cells: Basic Regulatory Mechanisms and Implications for the Pathogenesis and Treatment of Osteoporosis; 2000. B: and Death of Bone Cells.
- Hauge, E.M.; Qvesel, D.; Eriksen, E.F.; Mosekilde, L.; Melsen, F. Cancellous Bone Remodeling Occurs in Specialized Compartments Lined by Cells Expressing Osteoblastic Markers. Journal of Bone and Mineral Research 2001, 16, 1575–1582. [Google Scholar] [CrossRef] [PubMed]
- Atkins, G.J.; Findlay, D.M. Osteocyte Regulation of Bone Mineral: A Little Give and Take. Osteoporosis International 2012, 23, 2067–2079. [Google Scholar] [CrossRef] [PubMed]
- Dallas, S.L.; Prideaux, M.; Bonewald, L.F. The Osteocyte: An Endocrine Cell... and More. Endocr Rev 2013, 34, 658–690. [Google Scholar] [CrossRef]
- Tatsumi, S.; Ishii, K.; Amizuka, N.; Li, M.; Kobayashi, T.; Kohno, K.; Ito, M.; Takeshita, S.; Ikeda, K. Targeted Ablation of Osteocytes Induces Osteoporosis with Defective Mechanotransduction. Cell Metab 2007, 5, 464–475. [Google Scholar] [CrossRef]
- Delaissé, J.M.; Andersen, T.L.; Engsig, M.T.; Henriksen, K.; Troen, T.; Blavier, L. Matrix Metalloproteinases (MMP) and Cathepsin K Contribute Differently to Osteoclastic Activities. Microsc Res Tech 2003, 61, 504–513. [Google Scholar] [CrossRef]
- Xing, L.; Boyce, B.F. Regulation of Apoptosis in Osteoclasts and Osteoblastic Cells. Biochem Biophys Res Commun 2005, 328, 709–720. [Google Scholar] [CrossRef]
- Sims, N.A.; Martin, T.J. Coupling Signals between the Osteoclast and Osteoblast: How Are Messages Transmitted between These Temporary Visitors to the Bone Surface? Front Endocrinol (Lausanne) 2015, 6. [Google Scholar] [CrossRef]
- Delaisse, J.-M. The Reversal Phase of the Bone-Remodeling Cycle: Cellular Prerequisites for Coupling Resorption and Formation. Bonekey Rep 2014, 3. [Google Scholar] [CrossRef]
- Zhao, C.; Irie, N.; Takada, Y.; Shimoda, K.; Miyamoto, T.; Nishiwaki, T.; Suda, T.; Matsuo, K. Bidirectional EphrinB2-EphB4 Signaling Controls Bone Homeostasis. Cell Metab 2006, 4, 111–121. [Google Scholar] [CrossRef]
- Matsuo, K.; Otaki, N. Bone Cell Interactions through Eph/Ephrin: Bone Modeling, Remodeling and Associated Diseases. Cell Adh Migr 2012, 6, 148–156. [Google Scholar] [CrossRef]
- Clarke Anderson, H. Matrix Vesicles and Calcification. Curr Rheumatol Rep 2003, 5, 222–226. [Google Scholar] [CrossRef]
- Cui, L.; Houston, D.A.; Farquharson, C.; MacRae, V.E. Characterisation of Matrix Vesicles in Skeletal and Soft Tissue Mineralisation. Bone 2016, 87, 147–158. [Google Scholar] [CrossRef]
- Anderson, H.C.; Garimella, R.G.; Tague, S.E. THE ROLE OF MATRIX VESICLES IN GROWTH PLATE DEVELOPMENT AND BIOMINERALIZATION. Frontiers in Bioscience 2005, 822–837. [Google Scholar] [CrossRef]
- Kenkre, J.S.; Bassett, J.H.D. The Bone Remodelling Cycle. Ann Clin Biochem 2018, 55, 308–327. [Google Scholar] [CrossRef] [PubMed]
- Pouresmaeili, F.; Kamalidehghan, B.; Kamarehei, M.; Goh, Y.M. A Comprehensive Overview on Osteoporosis and Its Risk Factors. Ther Clin Risk Manag 2018, 14, 2029–2049. [Google Scholar] [CrossRef] [PubMed]
- Martiniakova, M.; Babikova, M.; Mondockova, V.; Blahova, J.; Kovacova, V.; Omelka, R. The Role of Macronutrients, Micronutrients and Flavonoid Polyphenols in the Prevention and Treatment of Osteoporosis. Nutrients 2022, 14. [Google Scholar] [CrossRef] [PubMed]
- Demontiero, O.; Vidal, C.; Duque, G. Aging and Bone Loss: New Insights for the Clinician. Ther Adv Musculoskelet Dis 2012, 4, 61–76. [Google Scholar] [CrossRef] [PubMed]
- Logan, C.Y.; Nusse, R. The Wnt Signaling Pathway in Development and Disease. Annu Rev Cell Dev Biol 2004, 20, 781–810. [Google Scholar] [CrossRef] [PubMed]
- Hill, T.P.; Später, D.; Taketo, M.M.; Birchmeier, W.; Hartmann, C. Canonical Wnt/β-Catenin Signaling Prevents Osteoblasts from Differentiating into Chondrocytes. Dev Cell 2005, 8, 727–738. [Google Scholar] [CrossRef]
- Li, J.; Sarosi, I.; Cattley, R.C.; Pretorius, J.; Asuncion, F.; Grisanti, M.; Morony, S.; Adamu, S.; Geng, Z.; Qiu, W.; et al. Dkk1-Mediated Inhibition of Wnt Signaling in Bone Results in Osteopenia. Bone 2006, 39, 754–766. [Google Scholar] [CrossRef]
- Goldring, S.R.; Goldring, M.B. Eating Bone or Adding It: The Wnt Pathway Decides; 2007. T: Bone or Adding It.
- Li, J.Y.; Walker, L.D.; Tyagi, A.M.; Adams, J.; Neale Weitzmann, M.; Pacifici, R. The Sclerostin-Independent Bone Anabolic Activity of Intermittent PTH Treatment Is Mediated by T-Cell-Produced Wnt10b. Journal of Bone and Mineral Research 2014, 29, 43–54. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, C.A.; Plotkin, L.I.; Galli, C.; Goellner, J.J.; Gortazar, A.R.; Allen, M.R.; Robling, A.G.; Bouxsein, M.; Schipani, E.; Turner, C.H.; et al. Control of Bone Mass and Remodeling by PTH Receptor Signaling in Osteocytes. PLoS One 2008, 3. [Google Scholar] [CrossRef] [PubMed]
- Silva, B.C.; Bilezikian, J.P. Parathyroid Hormone: Anabolic and Catabolic Actions on the Skeleton. Curr Opin Pharmacol 2015, 22, 41–50. [Google Scholar] [CrossRef]
- van Driel, M.; van Leeuwen, J.P.T.M. Vitamin D Endocrine System and Osteoblasts. Bonekey Rep 2014, 3. [Google Scholar] [CrossRef] [PubMed]
- Carter, P.H.; Schipani, E. The Roles of Parathyroid Hormone and Calcitonin in Bone Remodeling: Prospects for Novel Therapeutics; 2006; Vol. 6.
- Iglesias, L.; Yeh, J.K.; Castro-Magana, M.; Aloia, J.F. Effects of Growth Hormone on Bone Modeling and Remodeling in Hypophysectomized Young Female Rats: A Bone Histomorphometric Study. J Bone Miner Metab 2011, 29, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, R.S.; Jilka, R.L.; Parfitt, A.M.; Manolagas, S.C. Inhibition of Osteoblastogenesis and Promotion of Apoptosis of Osteoblasts and Osteocytes by Glucocorticoids Potential Mechanisms of Their Deleterious Effects on Bone; 1998; Vol. 102.
- Khosla, S.; Oursler, M.J.; Monroe, D.G. Estrogen and the Skeleton. Trends in Endocrinology and Metabolism 2012, 23, 576–581. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.H.; Chen, L.R.; Chen, K.H. Osteoporosis Due to Hormone Imbalance: An Overview of the Effects of Estrogen Deficiency and Glucocorticoid Overuse on Bone Turnover. Int J Mol Sci 2022, 23. [Google Scholar] [CrossRef]
- Lv, H.; Jiang, F.; Guan, D.; Lu, C.; Guo, B.; Chan, C.; Peng, S.; Liu, B.; Guo, W.; Zhu, H.; et al. Metabolomics and Its Application in the Development of Discovering Biomarkers for Osteoporosis Research. Int J Mol Sci 2016, 17. [Google Scholar] [CrossRef]
- Vanderschueren, D.; Vandenput, L.; Boonen, S.; Lindberg, M.K.; Bouillon, R.; Ohlsson, C. Androgens and Bone. Endocr Rev 2004, 25, 389–425. [Google Scholar] [CrossRef]
- Bruderer, M.; Richards, R.G.; Alini, M.; Stoddart, M.J. Role and Regulation of Runx2 in Osteogenesis. Eur Cell Mater 2014, 28, 269–286. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Wu, X.; Lei, W.; Pang, L.; Wan, C.; Shi, Z.; Zhao, L.; Nagy, T.R.; Peng, X.; Hu, J.; et al. TGF-Β1-Induced Migration of Bone Mesenchymal Stem Cells Couples Bone Resorption with Formation. Nat Med 2009, 15, 757–765. [Google Scholar] [CrossRef] [PubMed]
- Blackwell, K.A.; Raisz, L.G.; Pilbeam, C.C. Prostaglandins in Bone: Bad Cop, Good Cop? Trends in Endocrinology and Metabolism 2010, 21, 294–301. [Google Scholar] [CrossRef] [PubMed]
- Bertolini, D.R.; Nedwin, G.E.; Bringman, T.S.; Smith, D.D.; Mundy, G.R. Stimulation of Bone Resorption and Inhibition of Bone Formation in Vitro by Human Tumour Necrosis Factors. Nature 1986, 319, 516–518. [Google Scholar] [CrossRef] [PubMed]
- David Roodman, G. Calcified Tissue International Role of Cytokines in the Regulation of Bone Resorption; 1993.
- Trajanoska, K.; Rivadeneira, F. The Genetic Architecture of Osteoporosis and Fracture Risk. Bone 2019, 126, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Teng, Z.; Zhu, Y.; Yu, X.; Liu, J.; Long, Q.; Zeng, Y.; Lu, S. An Analysis and Systematic Review of Sarcopenia Increasing Osteopenia Risk. PLoS One 2021, 16. [Google Scholar] [CrossRef] [PubMed]
- David, C.; Confavreux, C.B.; Mehsen, N.; Paccou, J.; Leboime, A.; Legrand, E. Severity of Osteoporosis: What Is the Impact of Co-Morbidities? Joint Bone Spine 2010, 77. [Google Scholar] [CrossRef]
- Li, H.; Xiao, Z.; Quarles, L.D.; Li, W. Osteoporosis: Mechanism, Molecular Target and Current Status on Drug Development. Curr Med Chem 2020, 28, 1489–1507. [Google Scholar] [CrossRef]
- Deplas, A.; Debiais, F.; Alcalay, M.; Bontoux, D.; Thomas, P. Bone Density, Parathyroid Hormone, Calcium and Vitamin D Nutritional Status of Institutionalized Elderly Subjects. J Nutr Health Aging 2004, 8, 400–404. [Google Scholar]
- Ross, A.Catharine.; Taylor, L.C.; Yaktine, L.A.; Del Valle, B.H.; Institute of Medicine (U.S.). Committee to Review Dietary Reference Intakes for Vitamin D and Calcium. In Dietary Reference Intakes for Calcium and Vitamin D; National Academies Press: Washington, D.C., 2011; ISBN 978-0-309-16394-1. [Google Scholar]
- Papadopoulou, S.K.; Papadimitriou, K.; Voulgaridou, G.; Georgaki, E.; Tsotidou, E.; Zantidou, O.; Papandreou, D. Exercise and Nutrition Impact on Osteoporosis and Sarcopenia—the Incidence of Osteosarcopenia: A Narrative Review. Nutrients 2021, 13. [Google Scholar] [CrossRef]
- Ratajczak, A.E.; Szymczak-Tomczak, A.; Rychter, A.M.; Zawada, A.; Dobrowolska, A.; Krela-Kaźmierczak, I. Impact of Cigarette Smoking on the Risk of Osteoporosis in Inflammatory Bowel Diseases. J Clin Med 2021, 10. [Google Scholar] [CrossRef]
- Lyu, Z.; Hu, Y.; Guo, Y.; Liu, D. Modulation of Bone Remodeling by the Gut Microbiota: A New Therapy for Osteoporosis. Bone Res 2023, 11. [Google Scholar] [CrossRef]
- Prada, D.; Crandall, C.J.; Kupsco, A.; Kioumourtzoglou, M.A.; Stewart, J.D.; Liao, D.; Yanosky, J.D.; Ramirez, A.; Wactawski-Wende, J.; Shen, Y.; et al. Air Pollution and Decreased Bone Mineral Density among Women’s Health Initiative Participants. EClinicalMedicine 2023, 57. [Google Scholar] [CrossRef] [PubMed]
- Snega Priya, P.; Pratiksha Nandhini, P.; Arockiaraj, J. A Comprehensive Review on Environmental Pollutants and Osteoporosis: Insights into Molecular Pathways. Environ Res 2023, 237. [Google Scholar] [CrossRef] [PubMed]
- Sunyecz, J.A. The Use of Calcium and Vitamin D in the Management of Osteoporosis; 2008; Vol. 4.
- Lu, J.; Shin, Y.; Yen, M.S.; Sun, S.S. Peak Bone Mass and Patterns of Change in Total Bone Mineral Density and Bone Mineral Contents From Childhood Into Young Adulthood. Journal of Clinical Densitometry 2016, 19, 180–191. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, R.K.; Sapra, L.; Mishra, P.K. Osteometabolism: Metabolic Alterations in Bone Pathologies. Cells 2022, 11. [Google Scholar] [CrossRef] [PubMed]
- Varacallo, M.A.; Fox, E.J. Osteoporosis and Its Complications. Medical Clinics of North America 2014, 98, 817–831. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.; Huang, X.; Wu, J.; Lin, X.; Zhou, X.; Zhu, Z.; Pan, X.; Xu, J.; Qiao, J.; Zhang, T.; et al. The Global Burden of Osteoporosis, Low Bone Mass, and Its Related Fracture in 204 Countries and Territories, 1990-2019. Front Endocrinol (Lausanne) 2022, 13. [Google Scholar] [CrossRef]
- Kanis, J.A.; Norton, N.; Harvey, N.C.; Jacobson, T.; Johansson, H.; Lorentzon, M.; Mccloskey, E. V; Willers, C.; Borgström, F. SCOPE 2021: A New Scorecard for Osteoporosis in Europe. [CrossRef]
- Feng, X.; McDonald, J.M. Disorders of Bone Remodeling. Annual Review of Pathology: Mechanisms of Disease 2011, 6, 121–145. [Google Scholar] [CrossRef]
- Sanders, K.M.; Pasco, J.A.; Ugoni, A.M.; Nicholson, G.C.; Seeman, E.; Martin, T.J.; Skoric, B.; Panahi, S.; Kotowicz, M.A. The Exclusion of High Trauma Fractures May Underestimate the Prevalence of Bone Fragility Fractures in the Community: The Geelong Osteoporosis Study. Journal of Bone and Mineral Research 1998, 13, 1337–1342. [Google Scholar] [CrossRef]
- Hall, S.E.; Criddle, R.A.; Comito, T.L.; Prince, R.L. A Case-Control Study of Quality of Life and Functional Impairment in Women with Long-Standing Vertebral Osteoporotic Fracture; 1999.
- Maghbooli, Z.; Hossein-Nezhad, A.; Jafarpour, M.; Noursaadat, S.; Ramezani, M.; Hashemian, R.; Moattari, S. Direct Costs of Osteoporosis-Related Hip Fractures: Protocol for a Cross-Sectional Analysis of a National Database. BMJ Open 2017, 7. [Google Scholar] [CrossRef]
- Adami, G.; Fassio, A.; Gatti, D.; Viapiana, O.; Benini, C.; Danila, M.I.; Saag, K.G.; Rossini, M. Osteoporosis in 10 Years Time: A Glimpse into the Future of Osteoporosis. Ther Adv Musculoskelet Dis 2022, 14. [Google Scholar] [CrossRef]
- Kanis, J.A.; Study Group, H.O. Osteoporosis International WHO Study Document Assessment of Fracture Risk and Its Application to Screening for Postmenopausal Osteoporosis: Synopsis of a WHO Report; 1994; Vol. 4.
- Khashayar, P.; Taheri, E.; Adib, G.; Zakraoui, L.; Larijani, B. Osteoporosis Strategic Plan for the Middle East and North Africa Region. Arch Osteoporos 2019, 14. [Google Scholar] [CrossRef]
- Nuti, R.; Brandi, M.L.; Checchia, G.; Di Munno, O.; Dominguez, L.; Falaschi, P.; Fiore, C.E.; Iolascon, G.; Maggi, S.; Michieli, R.; et al. Guidelines for the Management of Osteoporosis and Fragility Fractures. Intern Emerg Med 2019, 14, 85–102. [Google Scholar] [CrossRef] [PubMed]
- McCloskey, E. V.; Johansson, H.; Oden, A.; Kanis, J.A. From Relative Risk to Absolute Fracture Risk Calculation: The FRAX Algorithm. Curr Osteoporos Rep 2009, 7, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Doosti-Irani, A.; Poorolajal, J.; Cheraghi, Z.; Irani, A.D.; Khalilian, A.; Esmailnasab, N. Prevalence of Osteoporosis in Iran: A Meta-Analysis Association of Body Mass Index with Dyslipidemia among the Government Staff of Kermanshah, Iran: A Cross-Sectional Study View Project GLIMMIX Model Applied to a Study of Food Items and Related Nutrients; Tehran Lipid and Glucose Study (TLGS). View Project Prevalence of Osteoporosis in Iran: A Meta-Analysis; 2013.
- Rizzoli, R.; Reginster, J.Y.; Boonen, S.; Bréart, G.; Diez-Perez, A.; Felsenberg, D.; Kaufman, J.M.; Kanis, J.A.; Cooper, C. Adverse Reactions and Drug-Drug Interactions in the Management of Women with Postmenopausal Osteoporosis. Calcif Tissue Int 2011, 89, 91–104. [Google Scholar] [CrossRef]
- Komm, B.S.; Chines, A.A. An Update on Selective Estrogen Receptor Modulators for the Prevention and Treatment of Osteoporosis. Maturitas 2012, 71, 221–226. [Google Scholar] [CrossRef]
- Ukon, Y.; Makino, T.; Kodama, J.; Tsukazaki, H.; Tateiwa, D.; Yoshikawa, H.; Kaito, T. Molecular-Based Treatment Strategies for Osteoporosis: A Literature Review. Int J Mol Sci 2019, 20. [Google Scholar] [CrossRef] [PubMed]
- Rogers, M.J.; Mönkkönen, J.; Munoz, M.A. Molecular Mechanisms of Action of Bisphosphonates and New Insights into Their Effects Outside the Skeleton. Bone 2020, 139. [Google Scholar] [CrossRef]
- Goldstein, S.R. Selective Estrogen Receptor Modulators and Bone Health. Climacteric 2022, 25, 56–59. [Google Scholar] [CrossRef] [PubMed]
- McIntosh, J.G.; Saya, S.; Minshall, J.; Bickerstaffe, A.; Hewabandu, N.; Qama, A.; Emery, J.D. Benefits and Harms of Selective Oestrogen Receptor Modulators (SERMs) to Reduce Breast Cancer Risk: A Cross-Sectional Study of Methods to Communicate Risk in Primary Care. British Journal of General Practice 2019, 69, E836–E842. [Google Scholar] [CrossRef]
- Cummings, S.R.; Ferrari, S.; Eastell, R.; Gilchrist, N.; Jensen, J.B.; McClung, M.; Roux, C.; Törring, O.; Valter, I.; Wang, A.T.; et al. Vertebral Fractures After Discontinuation of Denosumab: A Post Hoc Analysis of the Randomized Placebo-Controlled FREEDOM Trial and Its Extension. Journal of Bone and Mineral Research 2018, 33, 190–198. [Google Scholar] [CrossRef]
- Kim, B.; Cho, Y.; Lim, W. Osteoporosis Therapies and Their Mechanisms of Action (Review). Exp Ther Med 2021, 22. [Google Scholar] [CrossRef] [PubMed]
- Bandeira, L.; Lewiecki, E.M.; Bilezikian, J.P. Pharmacodynamics and Pharmacokinetics of Oral Salmon Calcitonin in the Treatment of Osteoporosis. Expert Opin Drug Metab Toxicol 2016, 12, 681–689. [Google Scholar] [CrossRef] [PubMed]
- Stoch, S.A.; Wagner, J.A. Cathepsin K Inhibitors: A Novel Target for Osteoporosis Therapy. Clin Pharmacol Ther 2008, 83, 172–176. [Google Scholar] [CrossRef]
- Dai, R.; Wu, Z.; Chu, H.Y.; Lu, J.; Lyu, A.; Liu, J.; Zhang, G. Cathepsin K: The Action in and Beyond Bone. Front Cell Dev Biol 2020, 8. [Google Scholar] [CrossRef]
- Drake, M.T.; Clarke, B.L.; Oursler, M.J.; Khosla, S. Cathepsin K Inhibitors for Osteoporosis: Biology, Potential Clinical Utility, and Lessons Learned. Endocr Rev 2017, 38, 325–350. [Google Scholar] [CrossRef]
- Girotra, M.; Rubin, M.R.; Bilezikian, J.P. The Use of Parathyroid Hormone in the Treatment of Osteoporosis. Rev Endocr Metab Disord 2006, 7, 113–121. [Google Scholar] [CrossRef]
- Boyce, E.G.; Mai, Y.; Pham, C. Abaloparatide: Review of a Next-Generation Parathyroid Hormone Agonist. Annals of Pharmacotherapy 2018, 52, 462–472. [Google Scholar] [CrossRef]
- Clarke, B.L. Anti-Sclerostin Antibodies: Utility in Treatment of Osteoporosis. Maturitas 2014, 78, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.Y.; Bolster, M.B. Profile of Romosozumab and Its Potential in the Management of Osteoporosis. Drug Des Devel Ther 2017, 11, 1221–1231. [Google Scholar] [CrossRef] [PubMed]
- Pilmane, M.; Salma-Ancane, K.; Loca, D.; Locs, J.; Berzina-Cimdina, L. Strontium and Strontium Ranelate: Historical Review of Some of Their Functions. Materials Science and Engineering C 2017, 78, 1222–1230. [Google Scholar] [CrossRef]
- Reginster, J.Y.; Seeman, E.; De Vernejoul, M.C.; Adami, S.; Compston, J.; Phenekos, C.; Devogelaer, J.P.; Curiel, M.D.; Sawicki, A.; Goemaere, S.; et al. Strontium Ranelate Reduces the Risk of Nonvertebral Fractures in Postmenopausal Women with Osteoporosis: Treatment of Peripheral Osteoporosis (TROPOS) Study. Journal of Clinical Endocrinology and Metabolism 2005, 90, 2816–2822. [Google Scholar] [CrossRef]
- Donneau, A.F.; Reginster, J.Y. Cardiovascular Safety of Strontium Ranelate: Real-Life Assessment in Clinical Practice. Osteoporosis International 2014, 25, 397–398. [Google Scholar] [CrossRef]
- Riso, P.; Soldati, L. Food Ingredients and Supplements: Is This the Future? J Transl Med 2012, 10. [Google Scholar] [CrossRef]
- Fenech, M.; El-Sohemy, A.; Cahill, L.; Ferguson, L.R.; French, T.A.C.; Tai, E.S.; Milner, J.; Koh, W.P.; Xie, L.; Zucker, M.; et al. Nutrigenetics and Nutrigenomics: Viewpoints on the Current Status and Applications in Nutrition Research and Practice. J Nutrigenet Nutrigenomics 2011, 4, 69–89. [Google Scholar] [CrossRef] [PubMed]
- da Costa, J.P. A Current Look at Nutraceuticals – Key Concepts and Future Prospects. Trends Food Sci Technol 2017, 62, 68–78. [Google Scholar] [CrossRef]
- Elkhalifa, A.E.O.; Alshammari, E.; Adnan, M.; Alcantara, J.C.; Awadelkareem, A.M.; Eltoum, N.E.; Mehmood, K.; Panda, B.P.; Ashraf, S.A. Okra (Abelmoschus Esculentus) as a Potential Dietary Medicine with Nutraceutical Importance for Sustainable Health Applications. Molecules 2021, 26. [Google Scholar] [CrossRef]
- Chanda, S.; Tiwari, R.K.; Kumar, A.; Singh, K. Nutraceuticals Inspiring the Current Therapy for Lifestyle Diseases. Adv Pharmacol Sci 2019, 2019. [Google Scholar] [CrossRef]
- Scicchitano, P.; Cameli, M.; Maiello, M.; Modesti, P.A.; Muiesan, M.L.; Novo, S.; Palmiero, P.; Saba, P.S.; Pedrinelli, R.; Ciccone, M.M. Nutraceuticals and Dyslipidaemia: Beyond the Common Therapeutics. J Funct Foods 2014, 6, 11–32. [Google Scholar] [CrossRef]
- Santini, A.; Novellino, E. Nutraceuticals - Shedding Light on the Grey Area between Pharmaceuticals and Food. Expert Rev Clin Pharmacol 2018, 11, 545–547. [Google Scholar] [CrossRef]
- Fernandes, S.D.; Narayana, R.C.; Narayanan, A. V. The Emergence of India as a Blossoming Market for Nutraceutical Supplements: An Overview. Trends Food Sci Technol 2019, 86, 579–585. [Google Scholar] [CrossRef]
- Rajasekaran, A.; Kalaivani, M. Designer Foods and Their Benefits: A Review. J Food Sci Technol 2013, 50, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Puri, V.; Nagpal, M.; Singh, I.; Singh, M.; Dhingra, G.A.; Huanbutta, K.; Dheer, D.; Sharma, A.; Sangnim, T. A Comprehensive Review on Nutraceuticals: Therapy Support and Formulation Challenges. Nutrients 2022, 14. [Google Scholar] [CrossRef] [PubMed]
- Rajput, R.; Wairkar, S.; Gaud, R. Nutraceuticals for Better Management of Osteoporosis: An Overview. J Funct Foods 2018, 47, 480–490. [Google Scholar] [CrossRef]
- Krall, E.A.; Wehler, C.; Garcia, R.I.; Harris, S.S.; Dawson-Hughes, B. Calcium and Vitamin D Supplements Reduce Tooth Loss in the Elderly; 2001; Vol. 111.
- Price, C.T.; Langford, J.R.; Liporace, F.A. Open Access Essential Nutrients for Bone Health and a Review of Their Availability in the Average North American Diet; 2012; Vol. 6.
- Manske, S.L.; Lorincz, C.R.; Zernicke, R.F. Bone Health: Part 2, Physical Activity. Sports Health 2009, 1, 341–346. [Google Scholar] [CrossRef] [PubMed]
- Price, C.T.; Langford, J.R.; Liporace, F.A. Essential Nutrients for Bone Health and a Review of Their Availability in the Average North American Diet; 2012; Vol. 6.
- Karpouzos, A.; Diamantis, E.; Farmaki, P.; Savvanis, S.; Troupis, T. Nutritional Aspects of Bone Health and Fracture Healing. J Osteoporos 2017, 2017. [Google Scholar] [CrossRef] [PubMed]
- Sojka, J.E. Magnesium Supplementation and Osteoporosis. Nutr Rev 2009, 53, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Rondanelli, M.; Faliva, M.A.; Tartara, A.; Gasparri, C.; Perna, S.; Infantino, V.; Riva, A.; Petrangolini, G.; Peroni, G. An Update on Magnesium and Bone Health. BioMetals 2021, 34, 715–736. [Google Scholar] [CrossRef]
- Castiglioni, S.; Cazzaniga, A.; Albisetti, W.; Maier, J.A.M. Magnesium and Osteoporosis: Current State of Knowledge and Future Research Directions. Nutrients 2013, 5, 3022–3033. [Google Scholar] [CrossRef]
- Capozzi, A.; Scambia, G.; Lello, S. Calcium, Vitamin D, Vitamin K2, and Magnesium Supplementation and Skeletal Health. Maturitas 2020, 140, 55–63. [Google Scholar] [CrossRef]
- Palacios, C. The Role of Nutrients in Bone Health, from A to Z. Crit Rev Food Sci Nutr 2006, 46, 621–628. [Google Scholar] [CrossRef] [PubMed]
- Takeda, E.; Yamamoto, H.; Yamanaka-Okumura, H.; Taketani, Y. Dietary Phosphorus in Bone Health and Quality of Life. Nutr Rev 2012, 70, 311–321. [Google Scholar] [CrossRef] [PubMed]
- He, F.J.; MacGregor, G.A. Beneficial Effects of Potassium on Human Health. In Proceedings of the Physiologia Plantarum; August 2008; Vol. 133; pp. 725–735. [Google Scholar]
- Balogh, E.; Paragh, G.; Jeney, V. Influence of Iron on Bone Homeostasis. Pharmaceuticals 2018, 11. [Google Scholar] [CrossRef]
- Kraemer, K.; Zimmermann, M.B. Nutritional Anemia. In; Kraemer, K., Zimmermann, M.B., Eds.; SIGHT AND LIFE, : Basel, Switzerland, 2007 ISBN 3-906412-33-4.
- Wuehler, S.E.; Peerson, J.M.; Brown, K.H. Use of National Food Balance Data to Estimate the Adequacy of Zinc in National Food Supplies: Methodology and Regional Estimates. Public Health Nutr 2005, 8, 812–819. [Google Scholar] [CrossRef]
- Sandstead, H.H.; Freeland-Graves, J.H. Dietary Phytate, Zinc and Hidden Zinc Deficiency. Journal of Trace Elements in Medicine and Biology 2014, 28, 414–417. [Google Scholar] [CrossRef]
- Devirian, T.A.; Volpe, S.L. The Physiological Effects of Dietary Boron. Crit Rev Food Sci Nutr 2003, 43, 219–231. [Google Scholar] [CrossRef]
- Pizzorno, L. Nothing Boring About Boron; 2015; Vol. 14.
- Mutlu, M.; Argun, M.; Kilic, E.; Saraymen, R.; Yazar, A.S. Magnesium, Zinc and Copper Status in Osteoporotic, Oshteopenic and Normal Post-Menopausal Women; 2007; Vol. 35.
- Zofkova, I.; Davis, M.; Blahos, J. Trace Elements Have Beneficial, as Well as Detrimental Effects on Bone Homeostasis. Physiol Res 2017, 66, 391–402. [Google Scholar] [CrossRef] [PubMed]
- CONLAN, D.; KORULA, R.; TALLENTIRE, D. Serum Copper Levels in Elderly Patients with Femoral-Neck Fractures. Age Ageing 1990, 19, 212–214. [Google Scholar] [CrossRef]
- Rubio, C.; Gutiérrez, Á.J.; Revert, C.; Reguera, J.I.; Burgos, A.; Hardisson, A. Daily Dietary Intake of Iron, Copper, Zinc and Manganese in a Spanish Population. Int J Food Sci Nutr 2009, 60, 590–600. [Google Scholar] [CrossRef]
- Kim, J.H.; Gupta, S.C.; Park, B.; Yadav, V.R.; Aggarwal, B.B. Turmeric (Curcuma Longa) Inhibits Inflammatory Nuclear Factor (NF)-ΚB and NF-ΚB-Regulated Gene Products and Induces Death Receptors Leading to Suppressed Proliferation, Induced Chemosensitization, and Suppressed Osteoclastogenesis. Mol Nutr Food Res 2012, 56, 454–465. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Aggarwal, B.B. Activation of Transcription Factor NF-B Is Suppressed by Curcumin (Diferulolylmethane)*; 1995.
- Von Metzler, I.; Krebbel, H.; Kuckelkorn, U.; Heider, U.; Jakob, C.; Kaiser, M.; Fleissner, C.; Terpos, E.; Sezer, O. Curcumin Diminishes Human Osteoclastogenesis by Inhibition of the Signalosome-Associated IκB Kinase. J Cancer Res Clin Oncol 2009, 135, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Wang, N.; Wang, F.; Gao, Y.; Yin, P.; Pan, C.; Liu, W.; Zhou, Z.; Wang, J. Curcumin Protects Human Adipose-Derived Mesenchymal Stem Cells against Oxidative Stress-Induced Inhibition of Osteogenesis. J Pharmacol Sci 2016, 132, 192–200. [Google Scholar] [CrossRef] [PubMed]
- Alexandersen, P. Ipriflavone in the Treatment of Postmenopausal Osteoporosis<SUBTITLE>A Randomized Controlled Trial</SUBTITLE>. JAMA 2001, 285, 1482. [Google Scholar] [CrossRef]
- Compston, J.E. Sex Steroids and Bone. Physiol Rev 2001, 81, 419–447. [Google Scholar] [CrossRef]
- Occhiuto, F.; De Pasquale, R.; Guglielmo, G.; Palumbo, D.R.; Zangla, G.; Samperi, S.; Renzo, A.; Circosta, C. Effects of Phytoestrogenic Isoflavones from Red Clover (Trifolium Pratense L.) on Experimental Osteoporosis. Phytother. Res 2007, 21, 130–134. [Google Scholar] [CrossRef]
- Clifton-Bligh, P.B.; Baber, R.J.; Fulcher, G.R.; Nery, M.-L.; Moreton, T. The Effect of Isoflavones Extracted from Red Clover (Rimostil) on Lipid and Bone Metabolism. Menopause 2001, 8, 259–265. [Google Scholar] [CrossRef]
- Costa-Rodrigues, J.; Carmo, S.C.; Silva, J.C.; Fernandes, M.H.R. Inhibition of Human in Vitro Osteoclastogenesis by Equisetum Arvense. Cell Prolif 2012, 45, 566–576. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.H.; Jung, J.W.; Ha, B.G.; Hong, J.M.; Park, E.K.; Kim, H.J.; Kim, S.Y. The Effects of Luteolin on Osteoclast Differentiation, Function in Vitro and Ovariectomy-Induced Bone Loss. Journal of Nutritional Biochemistry 2011, 22, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Perut, F.; Roncuzzi, L.; Avnet, S.; Massa, A.; Zini, N.; Sabbadini, S.; Giampieri, F.; Mezzetti, B.; Baldini, N. Strawberry-Derived Exosome-like Nanoparticles Prevent Oxidative Stress in Human Mesenchymal Stromal Cells. Biomolecules 2021, 11, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Gambari, L.; Grigolo, B.; Grassi, F. Dietary Organosulfur Compounds: Emerging Players in the Regulation of Bone Homeostasis by Plant-Derived Molecules. Front Endocrinol (Lausanne) 2022, 13. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.X.; Lin, F.J.; Li, H.; Li, H. Bin; Wu, D.T.; Geng, F.; Ma, W.; Wang, Y.; Miao, B.H.; Gan, R.Y. Recent Advances in Bioactive Compounds, Health Functions, and Safety Concerns of Onion (Allium Cepa L.). Front Nutr 2021, 8. [Google Scholar] [CrossRef] [PubMed]
- Wong, R.W.K.; Rabie, A.B.M. Effect of Quercetin on Preosteoblasts and Bone Defects; 2008; Vol. 2.
- Tsuji, M.; Yamamoto, H.; Sato, T.; Mizuha, Y.; Kawai, Y.; Taketani, Y.; Kato, S.; Terao, J.; Inakuma, T.; Takeda, E. Dietary Quercetin Inhibits Bone Loss without Effect on the Uterus in Ovariectomized Mice. J Bone Miner Metab 2009, 27, 673–681. [Google Scholar] [CrossRef] [PubMed]
- Suleria, H.A.R.; Butt, M.S.; Anjum, F.M.; Saeed, F.; Khalid, N. Onion: Nature Protection Against Physiological Threats. Crit Rev Food Sci Nutr 2015, 55, 50–66. [Google Scholar] [CrossRef] [PubMed]
- Ahmadian, F.; Mozaffari-Khosravi, H.; Azaraein, M.H.; Faraji, R.; Zavar-Reza, J. The Effect of Consumption of Garlic Tablet on Proteins Oxidation Biomarkers in Postmenopausal Osteoporotic Women: A Randomized Clinical Trial. Electron Physician 2017, 9, 5670–5675. [Google Scholar] [CrossRef] [PubMed]
- Weaver, C.M.; Alekel, D.L.; Ward, W.E.; Ronis, M.J. Flavonoid Intake and Bone Health. J Nutr Gerontol Geriatr 2012, 31, 239–253. [Google Scholar] [CrossRef] [PubMed]
- Ko, C.H.; Lau, K.M.; Choy, W.Y.; Leung, P.C. Effects of Tea Catechins, Epigallocatechin, Gallocatechin, and Gallocatechin Gallate, on Bone Metabolism. J Agric Food Chem 2009, 57, 7293–7297. [Google Scholar] [CrossRef]
- Shen, C.L.; Chyu, M.C.; Wang, J.S. Tea and Bone Health: Steps Forward in Translational Nutrition1-5. American Journal of Clinical Nutrition 2013, 98. [Google Scholar] [CrossRef]
- Hsieh, T.P.; Sheu, S.Y.; Sun, J.S.; Chen, M.H. Icariin Inhibits Osteoclast Differentiation and Bone Resorption by Suppression of MAPKs/NF-ΚB Regulated HIF-1α and PGE2 Synthesis. Phytomedicine 2011, 18, 176–185. [Google Scholar] [CrossRef]
- Perut, F.; Roncuzzi, L.; Avnet, S.; Massa, A.; Zini, N.; Sabbadini, S.; Giampieri, F.; Mezzetti, B.; Baldini, N. Strawberry-Derived Exosome-like Nanoparticles Prevent Oxidative Stress in Human Mesenchymal Stromal Cells. Biomolecules 2021, 11, 1–14. [Google Scholar] [CrossRef]
- Davicco, M.-J.; Wittrant, Y.; Coxam, V. Berries, Their Micronutrients and Bone Health. Curr Opin Clin Nutr Metab Care 2016, 19, 453–457. [Google Scholar] [CrossRef]
- Jabeen, Q.; Aslam, N. The Pharmacological Activities of Prunes: The Dried Plums. Article in Journal of Medicinal Plants Research 2011, 5, 1508–1511. [Google Scholar]
- Arjmandi, B.H.; Khalil, D.A.; Lucas, E.A.; Georgis, A.; Stoecker, B.J.; Hardin, C.; Payton, M.E.; Wild, R.A. Dried Plums Improve Indices of Bone Formation in Postmenopausal Women; 2002; Vol. 11.
- Tou, J.C. Resveratrol Supplementation Affects Bone Acquisition and Osteoporosis: Pre-Clinical Evidence toward Translational Diet Therapy. Biochim Biophys Acta Mol Basis Dis 2014, 1852, 1186–1194. [Google Scholar] [CrossRef]
- Lin, Q.; Huang, Y.-M.; Xiao, B.-X.; Ren, G.-F. Effects of Resveratrol on Bone Mineral Density in Ovarectomized Rats; 2005.
- Toba, Y.; Takada, Y.; Matsuoka, Y.; Morita, Y.; Motouri, M.; Hirai, T.; Suguri, T.; Aoe, S.; Kawakami, H.; Kumegawa, M.; et al. Milk Basic Protein Promotes Bone Formation and Suppresses Bone Resorption in Healthy Adult Men. Biosci Biotechnol Biochem 2001, 65, 1353–1357. [Google Scholar] [CrossRef]
- Toba, Y.; Takada, Y.; Yamamura, J.; Tanaka, M.; Matsuoka, Y.; Kawakami, H.; Itabashi, A.; Aoe, S.; Kumegawa, M. Milk Basic Protein: A Novel Protective Function of Milk against Osteoporosis. Bone 2000, 27, 403–408. [Google Scholar] [CrossRef]
- AOE, S.; TOBA, Y.; YAMAMURA, J.; KAWAKAMI, H.; YAHIRO, M.; KUMEGAWA, M.; ITABASHI, A.; TAKADA, Y. Controlled Trial of the Effects of Milk Basic Protein (MBP) Supplementation on Bone Metabolism in Healthy Adult Women. Biosci Biotechnol Biochem 2001, 65, 913–918. [Google Scholar] [CrossRef] [PubMed]
- Parvaneh, K.; Jamaluddin, R.; Karimi, G.; Erfani, R. Effect of Probiotics Supplementation on Bone Mineral Content and Bone Mass Density. The Scientific World Journal 2014, 2014. [Google Scholar] [CrossRef]
- Scholz-Ahrens, K.E.; Schaafsma, G.; van den Heuvel, E.G.; Schrezenmeir, J. Effects of Prebiotics on Mineral Metabolism. Am J Clin Nutr 2001, 73, 459s–464s. [Google Scholar] [CrossRef]
- Weaver, C.M.; Martin, B.R.; Nakatsu, C.H.; Armstrong, A.P.; Clavijo, A.; McCabe, L.D.; McCabe, G.P.; Duignan, S.; Schoterman, M.H.C.; Van Den Heuvel, E.G.H.M. Galactooligosaccharides Improve Mineral Absorption and Bone Properties in Growing Rats through Gut Fermentation. J Agric Food Chem 2011, 59, 6501–6510. [Google Scholar] [CrossRef] [PubMed]
- Whisner, C.M.; Castillo, L.F. Prebiotics, Bone and Mineral Metabolism. Calcif Tissue Int 2018, 102, 443–479. [Google Scholar] [CrossRef]
- Maggio, M.; Artoni, A.; Lauretani, F.; Borghi, L.; Nouvenne, A.; Valenti, G.; Ceda, G. The Impact of Omega-3 Fatty Acids on Osteoporosis. Curr Pharm Des 2009, 15, 4157–4164. [Google Scholar] [CrossRef]
- Satomura, K.; Tobiume, S.; Tokuyama, R.; Yamasaki, Y.; Kudoh, K.; Maeda, E.; Nagayama, M. Melatonin at Pharmacological Doses Enhances Human Osteoblastic Differentiation in Vitro and Promotes Mouse Cortical Bone Formation in Vivo. J Pineal Res 2007, 42, 231–239. [Google Scholar] [CrossRef]
- Purushothaman, A.; Sheeja, A.A.; Janardanan, D. Hydroxyl Radical Scavenging Activity of Melatonin and Its Related Indolamines. Free Radic Res 2020, 54, 373–383. [Google Scholar] [CrossRef]
- Tresguerres, I.F.; Tamimi, F.; Eimar, H.; Barralet, J.E.; Prieto, S.; Torres, J.; Calvo-Guirado, J.L.; Tresguerres, J.A.F. Melatonin Dietary Supplement as an Anti-Aging Therapy for Age-Related Bone Loss. Rejuvenation Res 2014, 17, 341–346. [Google Scholar] [CrossRef]
- Catinean, A.; Neag, M.A.; Muntean, D.M.; Bocsan, I.C.; Buzoianu, A.D. An Overview on the Interplay between Nutraceuticals and Gut Microbiota. PeerJ 2018, 2018. [Google Scholar] [CrossRef] [PubMed]
- Montalto, M.; D’Onofrio, F.; Gallo, A.; Cazzato, A.; Gasbarrini, G. Intestinal Microbiota and Its Functions. Digestive and Liver Disease Supplements 2009, 3, 30–34. [Google Scholar] [CrossRef]
- Tang, W.H.W.; Hazen, S.L. The Contributory Role of Gut Microbiota in Cardiovascular Disease. Journal of Clinical Investigation 2014, 124, 4204–4211. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.W.; An, J.H.; Park, H.; Yang, J.Y.; Choi, H.J.; Kim, S.W.; Park, Y.J.; Kim, S.Y.; Yim, M.; Baek, W.Y.; et al. Positive Regulation of Osteogenesis by Bile Acid through FXR. Journal of Bone and Mineral Research 2013, 28, 2109–2121. [Google Scholar] [CrossRef] [PubMed]
- Lucas, S.; Omata, Y.; Hofmann, J.; Böttcher, M.; Iljazovic, A.; Sarter, K.; Albrecht, O.; Schulz, O.; Krishnacoumar, B.; Krönke, G.; et al. Short-Chain Fatty Acids Regulate Systemic Bone Mass and Protect from Pathological Bone Loss. Nat Commun 2018, 9. [Google Scholar] [CrossRef] [PubMed]
- Montalvany-Antonucci, C.C.; Duffles, L.F.; de Arruda, J.A.A.; Zicker, M.C.; de Oliveira, S.; Macari, S.; Garlet, G.P.; Madeira, M.F.M.; Fukada, S.Y.; Andrade, I.; et al. Short-Chain Fatty Acids and FFAR2 as Suppressors of Bone Resorption. Bone 2019, 125, 112–121. [Google Scholar] [CrossRef]
- Park, E.J.; Kim, S.A.; Choi, Y.M.; Kwon, H.K.; Shim, W.; Lee, G.; Choi, S. Capric Acid Inhibits NO Production and STAT3 Activation during LPS-Induced Osteoclastogenesis. PLoS One 2011, 6. [Google Scholar] [CrossRef]
- Wang, F.; Ma, L.; Ding, Y.; He, L.; Chang, M.; Shan, Y.; Siwko, S.; Chen, G.; Liu, Y.; Jin, Y.; et al. Fatty Acid Sensing GPCR (GPR84) Signaling Safeguards Cartilage Homeostasis and Protects against Osteoarthritis. Pharmacol Res 2021, 164. [Google Scholar] [CrossRef]
- Zhao, Y.X.; Song, Y.W.; Zhang, L.; Zheng, F.J.; Wang, X.M.; Zhuang, X.H.; Wu, F.; Liu, J. Association between Bile Acid Metabolism and Bone Mineral Density in Postmenopausal Women. Clinics 2020, 75. [Google Scholar] [CrossRef]
- Liu, L.; Fu, C.; Li, F. Acetate Affects the Process of Lipid Metabolism in Rabbit Liver, Skeletal Muscle and Adipose Tissue. Animals 2019, 9. [Google Scholar] [CrossRef]
- Alali, M.; Alqubaisy, M.; Aljaafari, M.N.; Alali, A.O.; Baqais, L.; Molouki, A.; Abushelaibi, A.; Lai, K.S.; Lim, S.H.E. Nutraceuticals: Transformation of Conventional Foods into Health Promoters/Disease Preventers and Safety Considerations. Molecules 2021, 26. [Google Scholar] [CrossRef] [PubMed]
- Godad, A.; Ansari, A.; Bhatia, N.; Ali, A.; Zine, S.; Doshi, G. Drug Nutraceutical Interactions. In Industrial Application of Functional Foods, Ingredients and Nutraceuticals; Elsevier, 2023; pp. 663–723.
- Gil, F.; Hernández, A.F.; Martín-Domingo, M.C. Toxic Contamination of Nutraceuticals and Food Ingredients. In Nutraceuticals; Elsevier, 2016; pp. 825–837.
- Anadón, A.; Martínez-Larrañaga, M.R.; Ares, I.; Martínez, M.A. Interactions between Nutraceuticals/Nutrients and Therapeutic Drugs. In Nutraceuticals; Elsevier, 2016; pp. 855–874.
- Santini, A.; Cammarata, S.M.; Capone, G.; Ianaro, A.; Tenore, G.C.; Pani, L.; Novellino, E. Nutraceuticals: Opening the Debate for a Regulatory Framework. Br J Clin Pharmacol 2018, 84, 659–672. [Google Scholar] [CrossRef] [PubMed]
- Chopra, A.S.; Lordan, R.; Horbańczuk, O.K.; Atanasov, A.G.; Chopra, I.; Horbańczuk, J.O.; Jóźwik, A.; Huang, L.; Pirgozliev, V.; Banach, M.; et al. The Current Use and Evolving Landscape of Nutraceuticals. Pharmacol Res 2022, 175. [Google Scholar] [CrossRef] [PubMed]
- Lockwood, G.B. The Quality of Commercially Available Nutraceutical Supplements and Food Sources. Journal of Pharmacy and Pharmacology 2011, 63, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Ronis, M.J.J.; Pedersen, K.B.; Watt, J. Adverse Effects of Nutraceuticals and Dietary Supplements. Annu Rev Pharmacol Toxicol 2018, 58, 583–601. [Google Scholar] [CrossRef] [PubMed]
- Bonds, D.E.; Harrington, M.; Worrall, B.B.; Bertoni, A.G.; Eaton, C.B.; Hsia, J.; Robinson, J.; Clemons, T.E.; Fine, L.J.; Chew, E.Y. Effect of Long-Chain ω-3 Fatty Acids and Lutein+zeaxanthin Supplements on Cardiovascular Outcomes: Results of the Age-Related Eye Disease Study 2 (AREDS2) Randomized Clinical Trial. JAMA Intern Med 2014, 174, 763–771. [Google Scholar] [CrossRef]
- Goodman, G.E.; Thornquist, M.D.; Balmes, J.; Cullen, M.R.; Meykens, F.L.; Omenn, G.S.; Valanis, B.; Williams, J.H. The Beta-Carotene and Retinol Efficacy Trial: Incidence of Lung Cancer and Cardiovascular Disease Mortality during 6-Year Follow-up after Stopping β-Carotene and Retinol Supplements. J Natl Cancer Inst 2004, 96, 1743–1750. [Google Scholar] [CrossRef]
- Manson, J.E.; Cook, N.R.; Lee, I.-M.; Christen, W.; Bassuk, S.S.; Mora, S.; Gibson, H.; Gordon, D.; Copeland, T.; D’Agostino, D.; et al. Vitamin D Supplements and Prevention of Cancer and Cardiovascular Disease. New England Journal of Medicine 2019, 380, 33–44. [Google Scholar] [CrossRef] [PubMed]
- Hercberg, S.; Galan, P.; Preziosi, P.; Bertrais, S.; Mennen, L.; Malvy, D.; Roussel, A.-M.; Favier, A.; Briançon, S. The SU.VI.MAX Study A Randomized, Placebo-Controlled Trial of the Health Effects of Antioxidant Vitamins and Minerals.
- Lippman, S.M.; Klein, E.A.; Goodman, P.J.; Lucia, M.S.; Thompson, I.M.; Ford, L.G.; Parnes, H.L.; Minasian, L.M.; Gaziano, J.M.; Hartline, J.A.; et al. Effect of Selenium and Vitamin E on Risk of Prostate Cancer and Other Cancers: The Selenium and Vitamin E Cancer Prevention Trial (SELECT). JAMA 2009, 301, 39–51. [Google Scholar] [CrossRef] [PubMed]
- Sesso, H.D.; Rist, P.M.; Aragaki, A.K.; Rautiainen, S.; Johnson, L.G.; Friedenberg, G.; Copeland, T.; Clar, A.; Mora, S.; Moorthy, M.V.; et al. Multivitamins in the Prevention of Cancer and Cardiovascular Disease: The COcoa Supplement and Multivitamin Outcomes Study (COSMOS) Randomized Clinical Trial. American Journal of Clinical Nutrition 2022, 115, 1501–1510. [Google Scholar] [CrossRef]
- Durazzo, A.; Lucarini, M.; Santini, A. Nutraceuticals in Human Health. Foods 2020, 9. [Google Scholar] [CrossRef] [PubMed]
- Evans, M.; Lewis, E.D.; Antony, J.M.; Crowley, D.C.; Guthrie, N.; Blumberg, J.B. Breaking New Frontiers: Assessment and Re-Evaluation of Clinical Trial Design for Nutraceuticals. Front Nutr 2022, 9. [Google Scholar] [CrossRef] [PubMed]
- Saldanha, L.G. US Food and Drug Administration Regulations Governing Label Claims for Food Products, Including Probiotics. In Proceedings of the Clinical Infectious Diseases; February 1 2008; Vol. 46.
- Nuzzo, R. Scientific Method: Statistical Errors. Nature 2014, 506, 150–152. [Google Scholar] [CrossRef] [PubMed]
- Kaput, J. Developing the Pathway to Personalized Health: The Potential of N-of-1 Studies for Personalizing Nutrition. Journal of Nutrition 2021, 151, 2863–2864. [Google Scholar] [CrossRef]
- Ma, Y.; Fu, Y.; Tian, Y.; Gou, W.; Miao, Z.; Yang, M.; Ordovás, J.M.; Zheng, J.S. Individual Postprandial Glycemic Responses to Diet in N-of-1 Trials: Westlake N-of-1 Trials for Macronutrient Intake (WE-MACNUTR). Journal of Nutrition 2021, 151, 3158–3167. [Google Scholar] [CrossRef]
- Potter, T.; Vieira, R.; De Roos, B. Perspective: Application of N-of-1 Methods in Personalized Nutrition Research. Advances in Nutrition 2021, 12, 579–589. [Google Scholar] [CrossRef] [PubMed]
- Soldevila-Domenech, N.; Boronat, A.; Langohr, K.; de la Torre, R. N-of-1 Clinical Trials in Nutritional Interventions Directed at Improving Cognitive Function. Front Nutr 2019, 6. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.; Ma, Y.; Fu, Y.; Zheng, J.-S. Application of N-of-1 Clinical Trials in Personalized Nutrition Research: A Trial Protocol for Westlake N-of-1 Trials for Macronutrient Intake (WE-MACNUTR); 8190. A: of N-of-1 Clinical Trials in Personalized Nutrition Research.
- Paller, C.J.; Denmeade, S.R.; Carducci, M.A. Challenges of Conducting Clinical Trials of Natural Products to Combat Cancer. Clin Adv Hematol Oncol 2016, 14, 447–455. [Google Scholar] [PubMed]
- Tapsell, L.C. The Journal of Nutrition Evidence for Health Claims on Food: How Much Is Enough? Evidence for Health Claims: A Perspective from the Australia-New Zealand Region 1,2; 2008; Vol. 138.
- L’abbé, M.R.; Dumais, L.; Chao, E.; Junkins, B. The Journal of Nutrition Evidence for Health Claims on Food: How Much Is Enough? Health Claims on Foods in Canada 1-3; 2008; Vol. 138.
Figure 1.
Nutraceuticals for bone health.

Figure 2.
SWOT analysis identifies the advantages and disadvantages of Nutraceuticals for preventing bone loss and osteoporosis. INT: internal context. EXT: external context.
Figure 2.
SWOT analysis identifies the advantages and disadvantages of Nutraceuticals for preventing bone loss and osteoporosis. INT: internal context. EXT: external context.
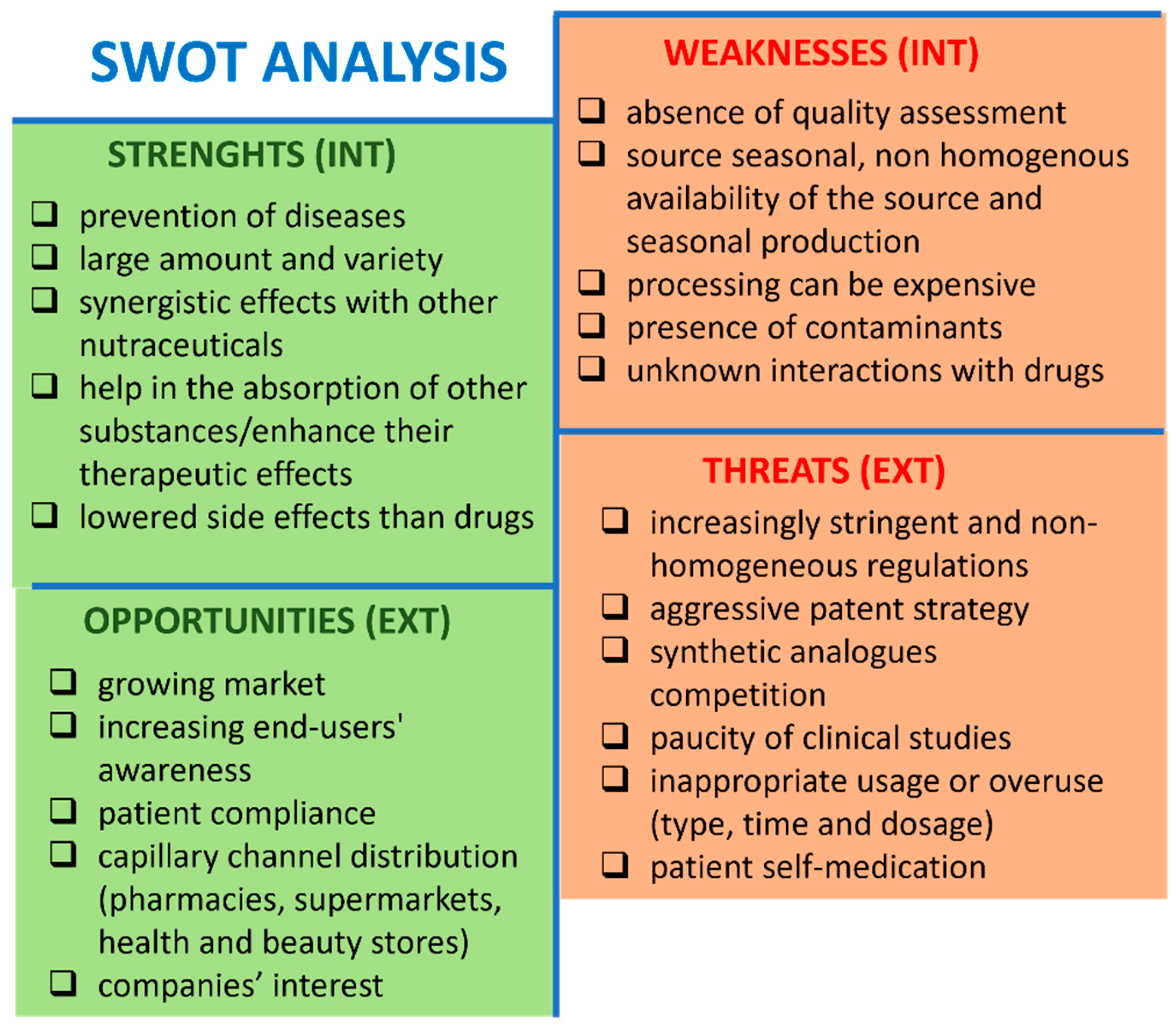
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



