Submitted:
15 November 2023
Posted:
16 November 2023
You are already at the latest version
Abstract
Abstract Introduction: An important indicator of a hospital's quality of care is the frequency of visits to the emergency department (ED). If a patient returns to the emergency room (ED) shortly after being evaluated or treated, it is generally assumed that their initial evaluation or treatment was inadequate. Objectives: The purpose of this study is to identify the main reasons for patient revisits to the emergency department in Hail. Studies suggest that researchers usually report the reasons for revisiting patients after 72 hours to patients themself. Therefore, alternative hypotheses will attribute the reasons to the system or physician's skill. To test these hypotheses, a methodology was developed. Method: The study analyzed patients discharged from King Khalid Hospital within 72 hours of discharge, involving all adults, regardless of health status or location Results: In February 2019, 17461 ED visits occurred, with 11% returning within 72 hours. In February 2022, 880 of 8749 visits resulted in a 10% return visit, with 30 randomly selected return visits.Conclusion: Increased community awareness post-COVID-19 may explain differences in ED revisit rates between 2022 and 2019, with system errors and patient information re-entry being associated
Keywords:
72-hours revisits
; Emergency department
; Electronic record
; Saudi Arabia
; sick leave
1. Introduction
Recurring visits to a hospital’s emergency department (ED) are an important indicator of the quality of the care they provide [1]. It is typically assumed that a patient’s initial evaluation or treatment was inadequate when they return to the emergency department (ED) shortly after being seen [2]. A patient’s presentation for the same primary complaint within 72 hours of discharge from the emergency department is considered an unplanned return [3,4]. However, little is known about the circumstances of these subsequent visits. In various time frames, previous researchers have demonstrated various indications [6].
It is known that a significant number of patients utilize emergency departments for non-emergency issues, therefore, many short-term return visits may be medically unnecessary. However, considering the visit as medically unnecessary does not imply that patients are abuse or misuse emergency services. Patients who return to the emergency department or re-meet with emergency physicians have not previously sought treatment elsewhere. Indeed, they are giving the health providers a second chance to resolve their issue [5].
In Saudi Arabia, the emergency department (ED) is frequently overcrowded. This put a lot of pressure on the Saudi health care system and makes it hard to get urgent care quickly and increases the risk of viral infections like the Middle East Respiratory Syndrome Coronavirus. Therefore, to boost service quality, efficiency, and patient safety in health care, a 72-hour ED visit has been established as a standard for quality and patient safety [1].
A study conducted in Taiwan by Chiu et al. examined the reasons for ED revisit. During the period January 1,2006 to December 31, 2006, there were more than 1899 revisits during 72 hours out of 34,714 visits. The most common complaint was misdiagnosed abdominal pain [6].
Ahmed et al. (2020) explored patients’ revisits between May and October 2016 single university hospital in Oman; 401 patients a have returned to the ED and the majority of returning patients were female; most of those patients’ revisit were related to obstetric [1].
In Saudi Arabia, Majed et al. (2021) carried out a study in a Medical city in Riyadh from January to December 2017. Out of 182,602 visits to the emergency department, 11,177 were unscheduled return visits, the data were extracted from the electronic medical record-integrated database (BEST Care 2.0 system). They applied a computerized simple random sampling method and enrolled 375 revisits. Abdominal pain was the most common major complaint that patients brought up during their first and second visit [7]. Another study by Anwar et al. (2018) was carried out in Riyadh, Saudi Arabia between April 2015, and July 2017, A 11,057 children with at least one chronic disease were included in the study. A revisit was 1211 with 83 having had a second ED revisit within 72 hours of being discharged. Respiratory conditions accounted for most ED revisits, according to ICD-10 codes. [8]. The study was conducted on the same organization with chronic diseases. With at least one chronic disease: 3,144 of 24,206 patients had their first ED visit, and 319 of them had a second visit within 72 hours. Diseases of the circulatory system were the most common reason for the first ED visit within 72 hours of the initial one, and various symptoms were the most common reason for the second ED visit within 72 hours of the initial diagnosis [9].
It was found from the above that most of the studies were conducted in central cities and it is difficult to take and apply their results to other Saudi cities such as Hail, and this reveals the extent of our need to know the reasons that lead to the return of emergency visitors.
As it was shown from previous studies, the effect of the return of the visitors appears on the statistical data. In some studies, we have noticed that the revisit constitutes a large percentage of the number of visitors. Therefore, it is important to know the correct ratio.
The aim of this study is to know the cause of patients returning to ED in King Khalid hospital in hail to improve the quality of emergency services provided to the residents of the Hail region. To provide accurate statistical data about the return of emergency visitors. As well as improving admission and discharge policies for patient revisit to the emergency department.
This study aimed to examine the frequency and factors contributing to emergency department patients’ revisits to a general hospital in Saudi Arabia within 72 hours. This can be enhancing the services provided in emergency departments within the hospitals of the northern region.
The objective of this research is to identify the main causes of patient revisits to emergency department in Hail. Based on the literatures, the researcher hypotheses tend to relate the reasons of revisit during 72 hours to the patients. Thus, the alternative hypotheses will associate the reasons to the system or physician skills. As result, the methodology was built to test these hypotheses.
2. Methods
2.1. Study design and setting
This study utilized a retrospective observation design. This study was conducted in a public hospital in Hail city with a capacity of 285 beds. Annually it receives about 61,000 visitors in the emergency department [10].
The study was conducted on the data of patients who returned to the emergency department within 72 hours from the time of discharge. Specifically, on the months of February 2019 and February 2022. The study includes all adults ‘data of both genders, without any health restrictions or certain conditions, such as being free of chronic diseases or living in a certain neighborhood.
2.2. Study Tools
The tools used in this research are mainly software programs. The data was extracted from Oasis system. (OASIS company, Al Murjan Holding Group, United States). OASIS Company owns a local health information system built in the mid-1990s that specializes in the operation and management of hospitals. OASIS system is one of the largest and most comprehensive systems for healthcare management in the Middle East, offering a wide range of clinical and non-clinical subsystems, that can also run on a modular basis to suit the requirement of varying sizes of hospitals. In 24 years, it has become one of the best and most powerful operating systems in the local and Gulf markets, and we used information extract from oasis system, that automated retrieval of specific information related to a selected topic from a text body or bodies is known as information extraction (IE). Information can be extracted from text documents, databases, websites, or multiple sources using information extraction tools. IE can extract information from machine-readable text that is unstructured, semi-structured, or structured. After collection of data, the data will be analyzed using Excel Microsoft Office.
2.3. Data collection and analysis
Ethical approval was obtained from the Scientific Research for the Research Ethics committee (REC) at the University of Ha’il, Hail, Saudi Arabia(H-2023-021). This research follows all ethical standards of research when collecting the data. The data was collected and analyzed with high integrity.
Data has been extracted from Oasis for February 2019 and February 2022 as an Excel sheet. The month of February was chosen for the presence of all classes of society, and the years 2019 and 2022 were chosen to make a comparison between the causes before the COVID-19 pandemic and after the COVID-19 pandemic. The factors selected in agreement by the investigation team were predetermined prior to the start of the study, where the reasons for reconsideration were categorized by medical, patient-, and system-related factors. The statistical tests used are percentage and frequency. The extracted data include the number of total patient visits, total patient revisits, male visits, male revisits, female visits, female revisits. Saudi visits, Saudi revisit. The stratified random sample was used to collect and divide the data based on Saudi revisit and non-Saudi revisits. A total number sample of 60 visitors to the emergency department was obtained. In the year of 2019, 30 visitors were taken, 25 Saudis and 5 non-Saudis, because the percentage of Saudis for the year 2019 is higher than non-Saudis, while in the year of 2022, 30 visitors were taken, 22 Saudis and 8 non-Saudis. Medical records were reviewed when needed to find out the reasons for patients returning to the emergency department.
3. Result
There were 17461 ED visits in February 2019. Of these total visits, 1953 (11%) had a return visit to the ED within 72 hours after the ED discharge from Hospital. A sample of 30 return visits was included in the study to find out the factors contributing to the revisits. The most attributed factors for revisits were as follows: medical-related factor 1 patients (3%); patient-related factor 3 patients (10%); sick leave-related factors 10 patients (33%); and system-related factors 16 patients (54%). Figure 1.
Table 1 illustrates the demographic data of patients in February 2019. The mean age of the male revisits was 31 years, while the females were 31 years, with an age range between 1 and 97 years. There were more males (57%, n = 1072) than females (43%, n = 821). The Saudi revisit was 1708 (86%), while the non-Saudis were 278 (14%).
The number of male visits in February 2019 was 10675 patients, the number of male revisits in February 2019 was 1072 patients, and the number of female visits in February,2019 was 6812 patients. The number of female revisits in February 2019 was 1821 patients. Number of Saudi visits in February 2019 was 14706 patients, number of Saudi revisits in February 2019 was 1708 patients. While the number of non-Saudi visits in February 2019 was 2501, the number of non-Saudi revisits in February 2019 was 278.
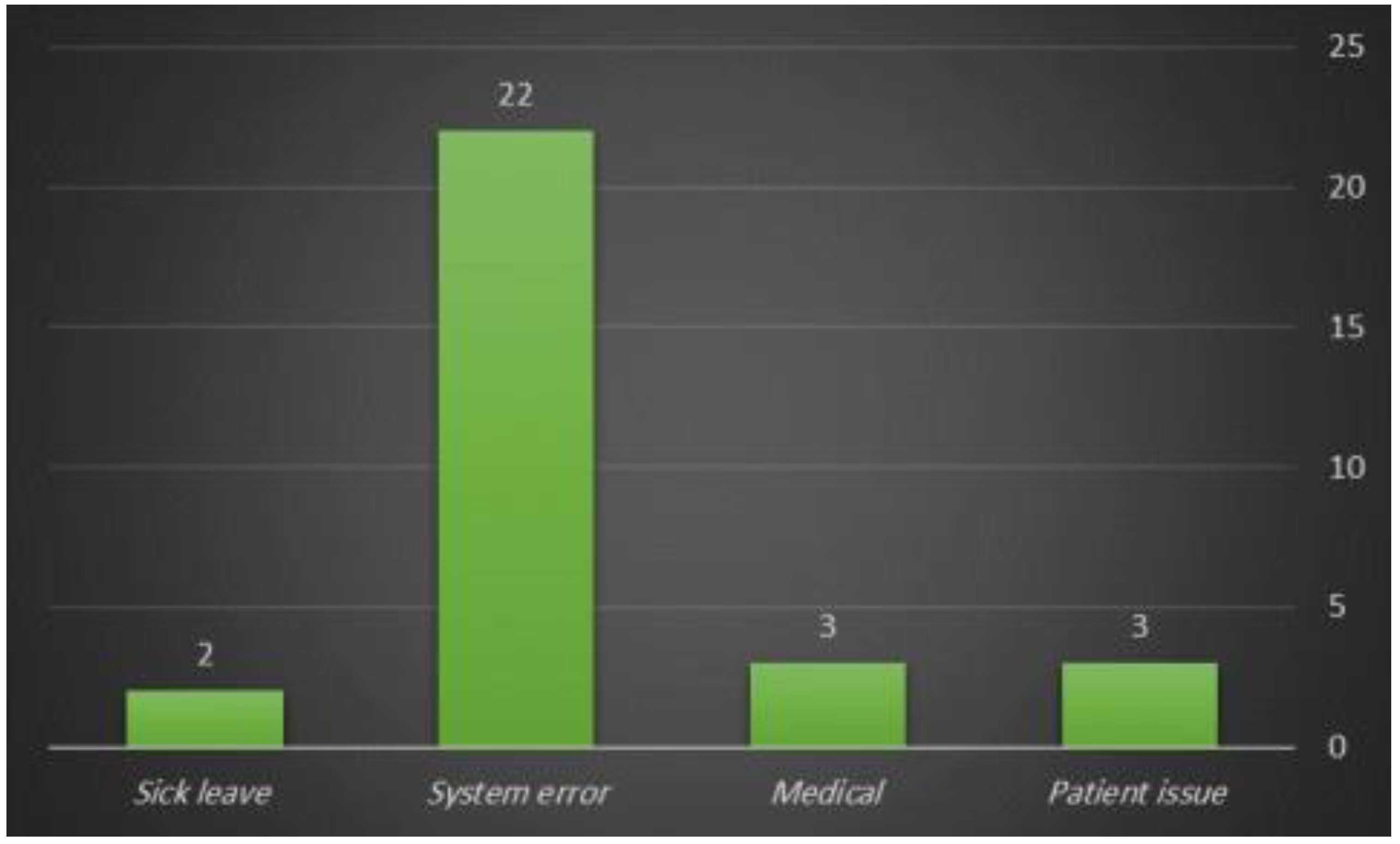
There were 8749 ED visits in February 2022. Of these total visits, 880 (10%) had a return visit to the ED within 72 hours after the ED discharge from King Khalid Hospital. A sample of 30 return visits was included in the study to find out the causes of revisits. The most attributed factors for revisit were as follows: medical-related factor 3 patients (10%); patient-related factor 3 patients (10%); sick leave related factors 2 patients (7%); and system-related factors 22 patients (73%). Figure 2.
Table 1 illustrates the demographic data for the revisits in February 2022. The mean age of the male revisits was 35 years, while the females were 36 years, with an age range between 18 and 97 years. There were more males (65%, n = 555) than females (35%, n = 305). The Saudi revisit was 554 (80%), while non-Saudis were 141 (20%).
The number of male visits in February 2022 was 5110 (90%) patients, the number of male revisits in February 2022 was 555 (10%) patients, and the number of female visits in February 2022 was 3345 (92%) patients. The number of female revisits in February 2022 was 305 (8%) patients. Number of Saudi visits in February,2022 was 6055 (92%) patients, number of Saudi revisits in February 2022 was 554 (8%) patients, while number of non-Saudi visits in February,2022 was 1597 (92%) patients, number of non-Saudi revisits in February,2022 was 141 (8%) patients.
The generally revisit rate in 2022 was (10%) less than the revisit rate in 2019 (11%).

Table 1.
The demographic data of patients in February 2019 and February 2022.
| February 2019 | February 2022 | |||
|---|---|---|---|---|
| Variable | Visits | Revisits (%) | Visit | Revisit (%) |
| Patient | 17461 | 1953 (11) | 8749 | 880 (10) |
| Gender | ||||
| Male | 10675 | 1072 (57) | 5110 | 555 (65) |
| Female | 6812 | 821 (43) | 3345 | 305 (35) |
| Nationality | ||||
| Saudi | 14797 | 1708 (86) | 6055 | 554 (80) |
| Non-Saudi | 278 (14) | 1597 | 141 (20) | |
| Average Age (years) | ||||
| Male | 31 | 35 | ||
| Female | 31 | 36 | ||
Figure 1.
The Causes of patient Revisits in February,2019 (n = 30). Note: Medical here mean misdiagnosis, patient issue; Discharge Against Medical Advice (DAMA), System error: double entry.
Figure 1.
The Causes of patient Revisits in February,2019 (n = 30). Note: Medical here mean misdiagnosis, patient issue; Discharge Against Medical Advice (DAMA), System error: double entry.
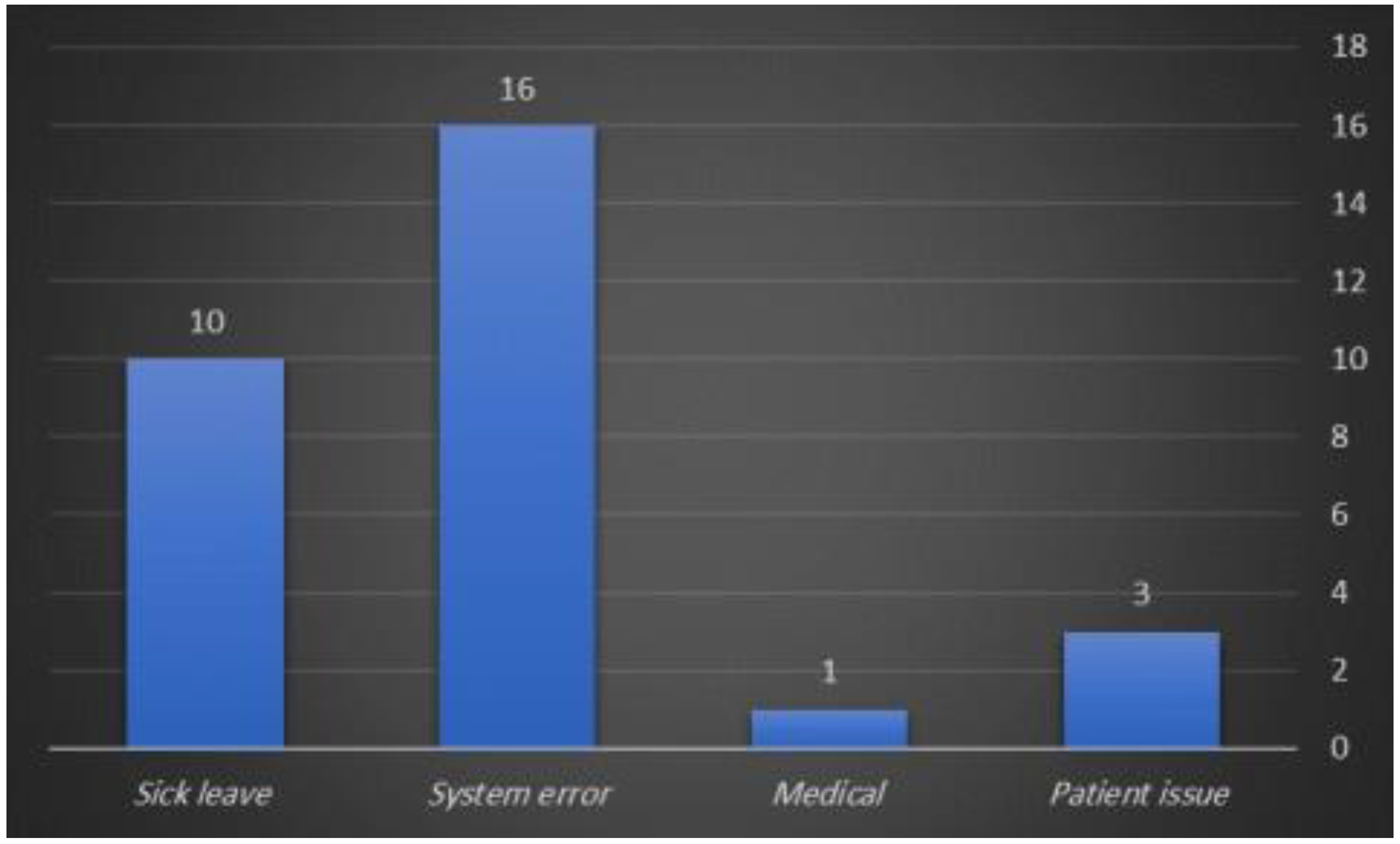
Figure 2.
The Causes of patient Revisits in February, 2022 (n = 30). Note: Medical: Geriatric medicine, misdiagnosis, foreign body, Patient issue: Discharge Against Medical Advice (DAMA), not emergency case, System error: double entry.
Figure 2.
The Causes of patient Revisits in February, 2022 (n = 30). Note: Medical: Geriatric medicine, misdiagnosis, foreign body, Patient issue: Discharge Against Medical Advice (DAMA), not emergency case, System error: double entry.
4. Discussion
The main goal of our study was to investigate the rate and cause of patients who returned to the emergency department in a public hospital in Hail, Saudi Arabia, within 72 hours from the time of discharge, especially in the months of February 2019 and February 2022.
In February 2019, there were 17461 visits to the ED, while in February 2022, there were 8749 ED visits, and in February 2019, there were 1953 (11% of these total visits) who returned to the ED within 72 hours of being discharged from the Hospital. In 2022, 880 (or 10%) of these total visitors returned to the ED within 72 hours of ED discharge from the Hospital. In comparison to most studies, the incidence of ED revisits during both years was high. This is possibly a result of healthcare convenience and culture, which is made possible by the national healthcare system. Also, may be due to many residents of this area choose to visit the ED rather than primary care facilities in Hail [23]. Additionally, because the ED is accessible and open around-the-clock, patients may decide to forego the outpatient clinics because their medical requirements are immediately treated there.
With an incidence rate of 11% in 2019 and 10% in 2022, the study analyzed the rates of ED revisits within 72 hours, and this rate is regarded as high compared to comparable worldwide studies.
For example, in Singapore, 3.25 percent of all patients who visited the ED again within 72 hours following their initial visit were tracked down [11]. and 5.4 percent of Taiwan emergency patients who returned to the ED within 72 hours [6]. In contrast, a previous study in Riyadh between September 13, 2015, and July 29, 2017, evaluated the rates of adults with chronic diseases returning to the emergency department (ED) within 72 hours. The findings showed an incidence rate of 13%, which is higher than previous reports and likely stems from their focus on patients who only returned with chronic diseases [9].
Differences in incidence rates between studies may be due to varying definitions of a return visit and inclusion and exclusion criteria for various groups.
We noted in our study that the re-visit rate in 2022 was (10%) lower than the re-visit rate in 2019 (11%), and this may be related to the increase in community awareness after the COVID 19 pandemic. Also, it may be that another urgent care hospital was established in the same city over this period, which might be contributed by taking a share of ED visits [12].
The hospital where the study took a place follows the Canadian Triage and Acuity Scale (CTAS), where cases are classified into five levels: level 1-Resuscitation level 2-Emergent level 3-Urgent level 4-Less urgent level 5-non-Urgent [13]. In 2019, all triage levels were accepted, while in 2022 1, 2 and 3 are accepted as directed by the hospital management and may be related due to re-visit decreases in 2022.
The rate of men re-visits more than women re-visits in our study, which is comparable to international studies [1], However, women may have been more concerned with their health or had lower employment rates, giving them more free time to visit doctors during office hours. It has been observed that men often seek medical assistance later in the course of their illness, and that this later timing may lead to an increase in the frequency of male hospitalizations or ER visits [6,14].
We note a decrease in the rate of women re-visits to men re-visits in 2022 compared to 2019, and, I think we can say a decrease in the number visit and revisit can be attributed to an establishment of other health care settings related to obstetric.
For both male and female, the decreased number of visit/revisits can be as a result of an establishment of other healthcare settings, enhanced awareness about COVID-19 infection and avoiding going to ED unless it is necessary.
Traffic accidents injury dropped for both genders. However, we cannot draw a conclusion about the car accidents based on gender, because we do not have the ratios of driving men/women, for women as it was in 2019, 27281 male accidents, 5629 female accidents, while in 2020 was 21492 male accidents and 2069 female accidents [15].
Our study found that the mean age was 31 for patients who had return visits in 2019, which is comparable to a study conducted at King Fahd University Hospital (KFHU) in the Eastern Province of Saudi Arabia [16]. While in 2022 the mean age was 35 for male re-visits to the ED and 36 for female re-visits, the reason for this difference in mean age between years may be due to in 2022, children were not accepted to the hospital.
We note through our study that non-Saudis revisits decreased in 2022; it was 8% compared to 2019, and it was 10% while the Saudis revisits decreased in 2022; it was 8% compared to 2019, and it was 10%. Perhaps the reason for the difference in the non-Saudis revisits during the two years that it was may be due to the decrease in the percentage of the non-Saudi population of Saudi Arabia in 2021 to 8.6%. [17], Also difference in the Saudis revisits during the two years possible due to a decrease in visits in general.
In this study, included medical-related factors are defined as misdiagnosis, geriatric medicine, and foreign body; patient-related factors include Discharge Against Medical Advice (DAMA); sick leave related factors include re-enter of sick leave, while system-related factors include double-enter patient into ED.
Patient-related factors accounted for 10% of the revisits for both years, comparable to a study conducted in Taiwan, which was 10.9% [6]. The results of Hung et al. were 14,2% [18] and those of Liaw et al. were 9.1% [19]. Common problems included non-compliant patients, anxiety, needs for certificates or other needs for legal purposes, needs to care for the patients wanted from families, or subjective needs of the patients and to bypass the OPD arrangement. Pierce et al. were different [20]. they found that patient-related factors were responsible for most repeat visits (53%), primary factors accounting for patient-related return visits were left the ED against medical advice or left before being instructed to do so, left without being seen by a physician. Patients may want to bypass the outpatient clinics because the ED is convenient, running 24 hours a day, and their medical needs are met instantaneously. Also, it may be due to patient discharge against medical advice (DAMA). Lerman and Kobernick concluded that 15% of their revisits could have been avoided by better patient education [21], so maybe we can be avoided by patient education or improve our polices.
In our study, we noted that the medical factors of the revisits for both years were lower compared to previous studies. The study by Pierce et al. found that 18% patient returns were the result of physician related factors [20] and Chiu et al. found that 8.6% patient revisits were related physician factors [6], while the study in the Eastern province of Saudi Arabia found 16.7% patient revisits due to physician factors [16]. In fact, the differentiation of the normal course illness, suboptimal treatment, hyper anxiety reaction, and medical errors is difficult. Perhaps the difference in percentages between studies was due to the different definitions of factors related to the physician, as their definition was related to disease or medical errors, while in our study it was related to misdiagnosis, a foreign body, or geriatric medicine. Nevertheless, we noticed a difference between the two years in our study, as 2019 it was 3% while in 2022 it was 10%, However may be due to part from the early discharge of patients when admission to ward was may be required, Also Some patients may need long-term care. In addition, this may be due to the paper medical files’ partial transformation to an electronic file including the clinical notes, which allows knowing the reasons related to the medical more clearly.
In our study we noted system related factors of the revisits in 2019 it was 54% while in 2022 it was73% were higher than study conducted in Eastern province of Saudi Arabia it was 4.2% [16]. Perhaps the reason for the difference between the two studies was due to the different system-related factors definition, so the study was in the eastern region of the Kingdom of Saudi Arabia, whereas system-related factors included follow-up, called back for abnormal investigations, unscheduled refill of medication, and admission. However, in our study, system-related factors included double-entry of patients in the system to the ED. This may be patients did not wait in the emergency department until they received treatment, but they returned to the ED the next day or re-enter the patients after they had left the system by mistake. Furthermore, in 2022, our hospital will undergo a transformation to an electronic record. We noticed a decrease in the number of sick leaves for the year 2022; it was 7% compared to 2019; it was 33%. However, this may be due to the fact that in 2019, when the patient needs a sick leave and did not request it at the time of the visit, the doctor needs to re-enter the patient into the ED system again in order to be written, while in 2022 the patient can request the sick leave without the need to re-enter the patient into the ED system again, thanks to the transformation to electronic medical record in 2022.
5. Limitation
We were unable to get certain specific information about some of the patients during the extraction of patient information from paper files and computerized records, we lacked information on several patient characteristics, such as compliance with treatments. The patient data was also on paper files in 2019, this made it difficult to find the exact reason for the patient’s re-visit. The fact that this study only included data from a single location and could not be compared to data from other centers was another limitation. Additionally, there was no proof that the non-reattenders did not seek medical attention at other EDs in the area. The interpretation of this retrospective study may have been constrained by incomplete data or selection bias due to the reliance on precise data collection and recording. Differentiation between the natural course of a disease, suboptimal therapy, overanxious reactions, and medical errors is difficult.
6. Conclusions
In this study, an ED revisit is associated with system error and the re-admission of the patient back into the ED. We may be able to limit system error by the electronic medical system. The rate of revisits as an index to gauge the performance of the ED is far from ideal, Revisits should be named as follow-up because only the ED service is available outside of office hours. Revisits, either to the ED or to outpatient clinics, should be used as a tool to address many of the risk problems of emergency medicine, and giving patients clear instructions and education on the disease process upon discharge and identifying when patients should come to the ED might help in decreasing the revisit rate. Establishing a policy of chart audits to review return-visit patients’ emergency situations.
Conflicts of Interest
The researchers have no conflict of interest or partiality in this research.
References
- Al-Alawi, A., & Fayyaz, J. (2020). Patterns of return visits to the Emergency Department among adult patients: an experience from tertiary hospital. audi Journal of Emergency Medicine. [CrossRef]
- Rogers JT. (1985). Risk management in emergency medicine. Dallas, TX: American College of Emergency Physicians.
- Nunez S, Hexdall A, Aguirre-Jaime A. (2006). Unscheduled returns to the emergency department: an outcome of medical errors? Qual Saf Health Care.
- Lindsay P, Schull M, Branskill S, et al. (2002). The development of indicators to measure the quality of clinical care in emergency departments following a modified-delphi approach. Acad Emerg Med.
- Gregory LH. Specific high-risk medicolegal issues. (1991) In: Emergency medicine risk management: a comprehensive review. Dallas, TX: American College of Emergency Physicians.
- Wu, C., Wang, F., Chiang, Y., Chiu, Y., Lin, T., Fong Fu, L., et al. (2010). Unplanned Emergency Department Revisits within 72 Hours to a Secondary Teaching Referral Hospital in Taiwan. Journal of Emergency Medicine. [CrossRef]
- Nasradeen, M., Althunayan, M., Aljamaan, A., Aljehani, A., Alqahtani, F., Aljerian, N., et al. (2021). Reasons for unscheduled return visits within 72 hours to the adult emergency department in Riyadh. Saudi Journal of Emergency Medicine. [CrossRef]
- Ahmed, A. E., ALMuqbil, B. I., Alrajhi, M. N., Almazroa, H. R., AlBuraikan, D. A., Albaijan, M. A., et al. (2018). Emergency department 72-hour revisits among children with chronic diseases: A Saudi Arabian study. BMC Pediatrics. [CrossRef]
- Ahmed, A. E., Alburaikan, D. A., Almazroa, H. R., Alrajhi, M. N., Almuqbil, B. I., Albaijan, M. A., et al. (2018). Seventy-two-hour emergency department revisits among adults with chronic diseases: A Saudi Arabian study. herapeutics and Clinical Risk Management. [CrossRef]
- Sabq online newspaper. (2018). Learn about the history of the Seven Kings’ visit to Hail.
- Kuan WS, Mahadevan M. (2009) Emergency unscheduled returns: can we do better? Singapore Med J.
- Opening of Sharaf Hospital in Hail. (2020)- Albilad.
- THA CANADIN TRIAGE AND ACUITY SCALE combined Adult/Paediatric Educational Program. (2007). Canadian Association of Emergency Phsicans (CAEP)with the consent of the CTAS National Working Group (NWG).
- Directorate-General of Budget. Accounting and statistics, executive Yuan, ROC (Taiwan); 2012. Available from: http://www.stat.gov.tw/public/Attachment/081918204771.doc. Accessed December 7, 2020.
- Ministry of Health in KSA (2021). Number of injuries and deaths by traffic accidents.
- Alshahrani, M., Katbi, F., Bahamdan, Y., Alsaihati, A., Alsubaie, A., Althawadi, D., et al. (2020). Frequency, causes, and outcomes of return visits to the emergency department within 72 hours: A retrospective observational study. Journal of Multidisciplinary Healthcare. [CrossRef]
- Population Estimates in the by Midyear of 2021. (2021). General Authority for Statistic.
- Hung SC, Chew G, Kong CT, et al. (2004) Unplanned emergency department revisits within 72 hours. J Taiwan Emerg Med.
- Liaw SJ, Bullard MJ, Hu PM, et al. (1999). Rates and causes of emergency department revisits within 72 hours. J Formos Med Assoc.
- Pierce JM, Kellerman AL, Oster C. (1990) “Bounces”: an analysis of short-term return visits to a public hospital emergency department. Ann Emerg Med.
- Lerman B, Kobernick MS. (1987). Return visits to the emergency department. J Emerg Med.
- Rising, K. L., Padrez, K. A., O’Brien, M., Hollander, J. E., Carr, B. G., & Shea, J. A. (2015). Return visits to the emergency department: The patient perspective. Annals of Emergency Medicine. [CrossRef]
- Almansour, H. (2021). Factors influencing job satisfaction among recently qualified resident doctors A qualitative study. Asia Pacific Journal of Health Management. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



