Submitted:
14 November 2023
Posted:
14 November 2023
You are already at the latest version
Abstract
Objectives. Invasive fungal spondylodiscitis (IFSD) is rare and could be lethal in certain circumstances. Previous literature revealed limited data concerning the outcomes. This study aimed to establish a risk-scoring system. Methods. A total of 53 patients were included in the study from a multi-centered database in Taiwan. All the clinicopathological and laboratory data were retrospectively analyzed. Variables strongly related to 1-year mortality were identified using a multivariate Cox proportional hazards model. A receiver operating characteristic curve was used to express the performance of our IFSD scoring model. Results. Five strong predictors were included in the IFSD score: predisposing immunocompromised state, the initial presentation of either radiculopathy or myelopathy, initial laboratory findings of WBC > 12.0 or < 0.4 103/uL, hemoglobin < 8 g/dL, and evidence of candidemia. 1-year mortality rates for patients with IFSD Scores of 0, 1, 2, 3, and 4 were 0%, 16.7%, 56.3%, 72.7%, and 100%, respectively. The area under the curve of the receiver operating characteristic curve was 0.823. Conclusions. We developed a practical scoring model with easily obtained demographic, clinical, and laboratory parameters to predict the probability of 1-year mortality in patients with IFSD. However, more large-scale and international validations would be necessary before this scoring model is commonly used.
Keywords:
invasive fungal infection
; fungus
; candida
; aspergillus
; spondylodiscitis
; osteomyelitis
; mortality
; chang gung research database
1. Introduction
Spinal infections are approximately 2.2/100,000 per year [1,2,3]. Out of those, infections involving the intervertebral disc and adjacent vertebral bony structures are classified as spondylodiscitis, which accounts for 2–7% of all cases of spinal infection [4,5]. The pathogen of spondylodiscitis can be pyogenic, granulomatous (tuberculosis, brucellosis, fungal infection), or parasitic [6,7]. The incidence of opportunistic fungal spondylodiscitis has surged during the past four decades because the number of patients with immunocompromised status has grown statistically (approximately 1% of all infectious spondylodiscitis) [4,8]. The most common species are Candida, followed by Aspergillus, Cryptococcus, and Coccidioides [1,9,10,11]. The on-time diagnosis of fungal spinal infections is often hindered by its discrete nature and non-specific symptoms. If the treatment is delayed, it could lead to irreversible neurologic deficits, deformities, systemic infection, and even mortality [12,13]. The overall mortality rate was around 20% [14,15]. Several risk factors for developing fungal spondylodiscitis have been investigated, mainly related to immunocompromised states [13]. In 2002, clinical experts formed a consensus committee named the European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group. They had issued a standard definition for invasive fungal infections [16]. The probability of the diagnosis of invasive fungal infection was classified into three tiers: “proven,” “probable,” and “possible.” “Proven” invasive fungal spondylodiscitis (IFSD) requires evidence of fungus species by culture of tissue or pus taken from a disease site without concurrent infection of other organisms. By contrast, “probable” IFSD indicates an immunocompromised host with ongoing fungal sepsis originating from the respiratory tract, the urinary tract, the gastrointestinal tract, and the central nervous system, whereas “possible” IFSD is preferred based on appropriate host factors and clinical evidence but without mycological support. Despite several revisions that have been made over the last 20 years, these updated definitions have not been proven applicable in clinical, diagnostic, and epidemiologic research of a broader range of patients at high risk of immunocompromised status [17,18,19,20]. Other predictors had also been evaluated for the association with mortality, including age, sex, clinical findings of neurological deficits, laboratory data, and different treatment strategies. However, their results were also unsatisfied with statistical significance [21]. As a result, we focused only on the “proven” invasive fungal spondylodiscitis (IFSD). We performed a multicentered retrospective study to construct a risk-scoring system based on easily obtained demographic, clinical, and laboratory parameters to predict the probability of 1-year mortality in patients with IFSD.
2. Materials and Methods
2.1. Chang Gung Research Database (CGRD)
We collected the patient data from the Chang Gung Memorial Hospital (CGMH), which has more than 10,000 beds and admitted more than 280,000 patients each year from 2 medical centers, 2 regional hospitals, and 3 district hospitals from the northeast to the south of Taiwan: Keelung, Taipei, Linkou, Taoyuan, Yunlin, Chiayi, and Kaohsiung. The Chang Gung Research Database (CGRD) harbors medical records from the above seven medical institutions. The basic architecture for the CGRD includes de-identified information from electronic medical records for routine epidemiologic health care studies, with several profiles for laboratory data, in-patient data, out-patient data, emergency room data, pathological data, radiological data, nursing data, charging data, disease category data, surgery data, and mortality outcomes. All the healthcare providers from CGMH can access the data for their clinical practice. Further details about the CGRD have been reported [22,23].
2.2. Patient Selection
From January 2000 to December 2019, we obtained the data from CGRD of patients with infective spondylodiscitis based on the International Classification of Diseases, ICD-9 codes (722.9, 720.89, 720.9), and ICD-10 codes (M4630-M4659, M4680-M4699). Patients under 18 without antifungal agent use or with antifungal agent treatment less than one week and without evidence of blood culture, CT-guide biopsy/surgically acquired pus, or tissue culture positive for fungal infection were excluded.
2.3. Variables and Outcomes
We divided the patients into two groups based on the primary outcome, 1-year mortality. Data including age, sex, predisposing immunocompromised state, initial clinical manifestations and radiological findings, pre-treatment laboratory findings, microbiologic results (blood culture, tissue/ pus culture obtained from CT-guide biopsy or open surgical biopsy), different treatment strategies (non-surgical or surgical management), surgically related complications and in-hospital general complications (respiratory failure, hospital-acquired pneumonia, acute kidney injury, urinary tract infection, electrolyte imbalance, acute coronary syndrome, metabolic encephalopathy, upper gastrointestinal tract bleeding, and pressure sore) were compared between the two groups. The tested variables used for predicting the model of 1-year mortality were all recorded at the time of the first diagnosis of invasive fungal spondylodiscitis. All table values were displayed as numbers (percentages) or median (interquartile range).
We defined those with predisposing immunocompromised state according to previous research [19,24]: patients who have at least one of the following factors: (1) Disturbance of the epithelial barrier caused by broad-spectrum or multiple antibiotic therapies, hemodialysis/peritoneal dialysis, major trauma, and surgery, and (2) Disease or dysfunction of mononuclear phagocytes or neutrophils, resulting from chemotherapy or radiotherapy, aplastic anemia, chronic granulomatous disease, advanced liver cirrhosis/ failure, (3) Defect or dysfunction of T-lymphocyte cell-mediated immunity caused by Acquired Immunodeficiency Syndrome, Hodgkin’s disease, solid organ transplantation, systemic chemotherapy, radiotherapy, hematologic malignancy and prolonged use of corticosteroids (> 0.3mg/kg for over 3 weeks).
The clinical neurologic deficits (fever, radicular pain, muscular weakness, myelopathy) were recorded as soon as the symptoms started, whether at the outpatient department, emergency room or after hospital admission. The onset time for a radiological diagnosis was calculated by weeks. There are five different modalities for diagnosing spondylodiscitis: X-rays, Computed Tomography (CT), Magnetic Resonance Imaging (MRI), Tc-99m methylene diphosphonate bone scan, and Gallium Inflammation Scan. The detailed information includes disc space narrowing, endplate erosion, vertebral body collapse, translation or distraction for X-rays; endplate erosion, vertebral body collapse, paraspinal tissue abscess, epidural abscess for CTs; loss of intradiscal key sign, T2 edema signal change, cord/sac compression, root compression, paraspinal tissue abscess for MRIs. Surgical interventions for IFSD include laminectomy/discectomy (decompression), transpedicular screw insertion (fixation), and posterolateral/ transforaminal interbody fusion (fusion), depending on the severity and stage of this disease. Sometimes, the patients receive two or more surgeries during a single hospitalization.
2.4. Statistical Analysis
We used Pearson's chi-squared test to analyze categorical variables and the Wilcoxon rank-sum test to analyze continuous variables. To avoid bias among this mixture of straight and binary variables, the multivariate Cox proportional hazards model was used to analyze the effect of those selected time-to-event predictors on 1-year mortality. The outcome was also graphically displayed according to the Kaplan–Meier method, comparing cumulative events by the log-rank test. Lastly, a receiver operating characteristic (ROC) curve was used to show the performance of our IFSD grading model in the graphic. The statistical calculations were done with the IBM SPSS Statistics for Windows, Version 28.0. Armonk, NY: IBM Corp. When p < 0.05, the differences were considered statistically significant.
3. Results
3.1. Patient Characteristics and Clinical Manifestations
In total, 53 patients with a definite diagnosis of proven IFSD were retrospectively studied over 20 years. Except for the much higher overall 1-year mortality rate (45.3%), the mean age (around 65) and male predominance were compatible with studies previously reported [13,21,25]. Predisposing immunocompromised state is seen in about one-third of all the IFSD patients involved and possesses one of the striking predictors for 1-year mortality (50.0% vs. 17.2%, p = 0.011). Fever is the typical initial symptom, whereas neurologic deficits are distinct among patients. About 62.3% of patients experience radicular pain, followed by muscular weakness (43.4%) and myelopathy (13.2%). The onset time to diagnosis is lengthy, with a median of three weeks. Kimona et al. have mentioned that a delayed diagnosis may hinder biological evidence from cultures and biopsies, reduce IFSD pathogen clearance rate, and negatively affect treatment outcomes [26]. Detailed comparisons of baseline characteristics between two groups stratified by 1-year mortality were listed in Table 1.
3.2. Radiologic and Laboratory Diagnosis
Five different diagnostic imaging: X-rays (in 44 cases), CTs (in 26 cases), MRIs (in 47 cases), Bone scans (in 17 cases), and Inflammatory scans (in 22 cases) were used with flexibility. In traditional radiology, X-rays of the relevant spinal segment are the first-line tool for patients with the above-mentioned clinical symptoms. The sensitivity and specificity are relatively low at 82% and 57% [27]. However, the disc space narrowing, endplate erosions, and vertebral body collapse may appear days or weeks after the infection starts, depending on the pathogen's virulence and the disease's natural course [28,29]. A negative native X-ray does not exclude spondylodiscitis. For patients with contraindications to MRI (devices like pacemaker and ventriculoperitoneal shunt) or with claustrophobia, Computed Tomography (CT) is the best alternative. The enhanced CT studies provide information on endplate erosion, vertebral body collapse, and paraspinal/epidural abscess. CT is also practical for invasive procedures for IFSD, such as fine-needle biopsy and abscess drain placement [30,31]. MRI with contrast is the gold standard in imaging studies to detect spondylodiscitis. Specificity and sensitivity are marked high at 96% and 92% [32,33]. MRI uses different phases to reveal signal changes over the intervertebral disc, vertebral body, paraspinal tissue, and compression to the neural structures (cord, dural sac, nerve roots) [34]. According to previous studies, IFSD usually resulted in disk narrowing, destruction of the endplates, and inflammation of the paraspinal tissue [35]. These imaging findings are consistent with what we found in our case. Bone scintigraphy with 99 technetium-labeled leukocytes and inflammatory scan with 67gallium citrate have low specificity but relatively high sensitivity to 86% for diagnosing spondylodiscitis [36]. The advantage of those two radioactively labeled techniques is the potential to detect other sources of infection. Most infections in this study were in the lumbar spine (37 cases, 69.8%) followed by thoracic (11 cases, 20.8%), cervical (7 cases, 13.2%) and sacral spine (5 cases, 9.4%). Furthermore, seven of them involved two regions. Miller et al. described a case series of spinal infection by Candida [25], 33 cases (55.9%) affecting the lumbar spine, followed by thoracic (17 cases, 28.8%), combined thoracic to lumbar (6 cases, 10.2%), and cervical (3 cases, 5.1%), which is similar to our findings.
Several initially recorded laboratory indicators, including higher white blood cell count (12.4 vs. 11.0 103/µL, p = 0.040), higher C-reactive protein concentration (150 vs. 50 mg/µL, p = 0.002), lower hemoglobin (9.0 vs. 10.2 g/µL, p = 0.034), lower platelet count (169 vs. 291 103/µL, p = 0.021), as well as a positive finding of candidemia (66.7% vs. 31.0%, p = 0.010), led to 1-year mortality with statistical significance. As expected, the majority of infections were due to Candida albicans, representing 32 cases (60.4%), followed by C. tropicalis (7 cases, 13.2%), C. parapsilosis (4 cases, 7.5%), C. glabrata (3 cases, 5.7%). Only 1 case (1.9%) for each isolated pathogen: Aspergillus, C. krusei, C. lusitaniae, Cryptococcus neoformans, Debaryomyces hansenii, and Fonsecaea pedrosoi. Candida albicans were identified more often in the survivors’ group (72.4% vs. 45.8%, p = 0.049).
3.3. Treatment Strategies and Complications
For the use of antifungal agents in our study, 43 patients (81.1%) were treated with intravenous Fluconazole, followed by 13 patients (24.5%) with Micafungin, 11 patients (20.7%) with Anidulafungin, 10 patients (18.9%) with Amphotericin B and 2 patients (3.8%) each for the rest: Itraconazole, Voriconazole, Posaconazole and Caspofungin. The median treatment course for antifungal agents is 27 days (11.0-61.0). The results were similar to the 28-patient case series mentioned before [21]. 35 patients (66.0%) were treated with one or more surgeries for IFSD. The indications for surgical intervention were the need to (1) collect pus or infected tissue for definite diagnosis of IFSD, (2) debride and decompress the involved spinal and neural structures, (3) treat cases refractory to medical treatment with disease progression, and (4) stabilize the unstable spine resulted from the vertebral body, disc disruption, and longitudinal ligaments disruption. Regarding the treatment strategies, the chances of receiving necessary surgical interventions were higher in the survivors’ group (82.8% vs. 45.8%, p = 0.005). 11 patients (31.4%) had a laminectomy alone for decompression. The remaining 24 (68.6%) patients had a combined decompression, fixation, and fusion with instrumentation at the first surgery. The selection of surgical strategies was similar between the non-survivors and survivors’ groups (36.4% vs. 37.3% compared to debridement only, p = 0.011). 10 patients (28.6%) received only one neurosurgical operation, whereas 25 patients (71.4%) received at least two operations, with the chances significantly higher in the non-survivors group (80.0% vs. 64.0%, p = 0.002).
Two surgical-related complications were recorded. 5 cases (9.4%) had superficial wound infection, and 7 cases (13.2%) had uncontrolled infection that needed further debridement. Both events did not reach statistical differences between the non-survivors and survivors’ groups. As for general complications, there were 19 cases (35.8%) with respiratory failure, 17 cases (32.1%) with hospital-acquired pneumonia, 13 cases (24.5%) with acute kidney injury, 13 cases (24.5%) with urinary tract infection, 18 cases (34.0%) with electrolyte imbalance, 3 cases (5.7%) with acute coronary syndrome, 10 cases (18.9%) with metabolic encephalopathy, 10 cases (18.9%) with UGI bleeding and 4 cases (7.5%) with pressure sores. All the significant complications were higher in the non-survivors group. Five of the above reached statistical difference, including respiratory failure (62.5% vs. 13.8%, p < 0.001), hospital-acquired pneumonia (58.3% vs. 10.3%, p < 0.001), acute kidney injury (45.8% vs. 6.9%, p = 0.001), electrolyte imbalance (50.0% vs. 20.7%, p = 0.025) and metabolic encephalopathy (37.5% vs. 3.4%, p = 0.002).
4. Discussion
Our retrospective study used a strict and robust diagnostic definition combining clinical, radiological, and compulsory mycological identification to prevent selection bias. The following are some significant findings that need to be addressed.
4.1. The Previous Studies
Literature searches of the online databases, including PubMed, Web of Science, Cochrane Central Register of Controlled Trials, and EMBASE, were performed. To date, 32 case reports, 5 case series, 1 retrospective cohort, and 2 reviews related to IFSD have been reported. Fungi are typically considered harmless organisms and are part of the normal human flora. However, in the presence of impaired host immunity or repeated intravascular access, they can become invasive. Invasive fungal spondylodiscitis was associated with high morbidity and mortality [37]. IFSD can occur either through hematogenous seeding from a distant infection focus or via direct extension of a contiguous infection from adjacent organs [38]. Hematogenous dissemination is considered the primary disease mechanism that brings pathogens to the surrounding vascular network around vertebral bodies and intervertebral discs in adults [39]. Plain radiographs/ X-rays typically show erosive and destructive vertebral changes with intervertebral disc space narrowing, but these findings may not be radiographically visible for weeks to months [40]. Although CT scanning indicates instant bony changes and reveals the presence of paravertebral involvement or spinal canal compression [41], the provided information is still insufficient for the following treatment modalities. As a result, MRI should always be considered the imaging of choice for vertebral spondylodiscitis if feasible [42]. A definitive microbiological diagnosis of IFSD requires the culture of a biopsy specimen to distinguish pathogens of fungi from bacteria, mycobacteria, and also malignancies such as multiple myeloma and metastatic disease. Needle biopsy under fluoroscopy or CT guidance for specimens should target the involved vertebral bodies, intervening discs, or paraspinal soft tissues [43]. If the results are negative, repeated needle or open biopsies are still necessary because empirical therapies for IFSD are vastly different based on the pathogens. Treatment was commonly delayed because of the difficulty in definite diagnosis, which has been mentioned in other series with an average of 6 weeks (median, 1–11 weeks) [13,44]. Other than Candida albicans, the other fungal organisms are discrete with their slow-growing nature, sometimes complex to cultivate in cultures. Back pain is the most common clinical manifestation, followed by fever and neurological deficits [45]. Longer delays were correlated with a less favorable neurological outcome [46]. Besides, several reported factors also affect the outcomes, including the preexisting immunodeficiency secondary to human immunodeficiency virus infection, the use of immunosuppressive drugs such as glucocorticoids or chemotherapy, the prolonged use of intravenous nutrition support, hemodialysis, recent surgery, burns with disrupted skin barrier, and the presence of neutropenia [35,47,48]. The pathogen isolated through cultures has been mostly Candida, Aspergillus, and Cryptococcus [1,4]. Both results matched our findings. Surgical treatment is not mandatory in every IFSD case. No consensus has been made on the best surgical timing [49,50]. It should be performed in cases with progressive neurological deficits or with evidence of spinal instability. Even if the infection is uncontrolled, the subsequent surgical treatment should be considered carefully because a complete and radical debridement of all the involved tissue is complex and could exhaust patients and surgeons and generate unnecessary surgical-related complications. The reoperation may also spread the infection toward the adjacent neural structures. In one study, segment instrumentation and bone grafting are not suggested because they lead to overpressure on adjacent vertebral structures, resulting in further instability and higher chances of biofilm formation [51]. As a result, a sufficient and comprehensive antifungal treatment should be the top priority for IFSD patients. The optimized management of invasive fungal spondylodiscitis remains unclear. The suggested first-line antifungal drugs are amphotericin B or fluconazole, with an extended treatment course of at least 6 to 10 weeks [52]. Both agents are equally effective. The total length of antifungal therapy has to be determined. Miller et al. recommend considering treatment completed until the patient matches all three indicators: normalized ESR and CRP, clinically resolved symptoms, and improved inflammatory changes over imaging studies [25]. These recommendations are consistent with the Infectious Diseases Society of America practice guidelines for treating candidiasis [52]. Concerning the survival analysis, only 1 cohort study investigates the relationship between the risk factors and the 1-year mortality of 28 Candida vertebral osteomyelitis patients [21]. This survival analysis revealed the elderly (median age, 78 vs. 50 years, p = 0.02) and the patients with a higher Charlson comorbidity index score (median, 6 vs. 2.5, p = 0.001). There was no difference between the survivors and the non-survivors regarding clinical, radiological, biological, or microbiological findings. There was no scoring system for the overall survival of patients with IFSD proposed before. A clear understanding of the various prognostic factors could give the patients and their families realistic impressions of survival. It could also elevate physicians' awareness to treat individuals with a higher sum of the score cautiously and aggressively.
4.2. Our IFSD Score
We selected the contributive indicators and dichotomized the continuous variables into binary variables for the multivariate Cox proportional hazards analysis (Table 2). About the cut points, simply selecting the medians without investigating each relationship with the outcome might lead to significant bias. As a result, decisions had been made as the following: defining age > 65 years old as the elderly, body temperature > 38.3℃ and < 36.0℃ as hyperthermia and hypothermia, WBC > 12.0 or < 0.4 103/µL and platelet < 100 103/µL as sepsis based on the International Guidelines for Management of Severe Sepsis and Septic Shock [53], CRP >100 mg/dL as severe systemic infection based on previous research [54], and hemoglobin < 8 mg/dL as severe anemia based on the World Health Organization guidelines [55] for all the continuous variables. The 1-year mortality of IFSD patients was statistically significant with the preexisting immunocompromised state (HR 3.01, p = 0.024), the initial presentation of either radiculopathy or myelopathy (HR 4.04, p = 0.012), initial laboratory positive findings of leukocytosis or extreme leukopenia (HR 2.83, p = 0.049), severe anemia (HR 4.93, p = 0.014), and strongly correlated with evidence of candidemia (HR 2.78, p = 0.052).
Every clinical grading scale balances the simplicity and accuracy of outcome prediction. To make this score clinically applicable, the prognosis-predicting model must be simple enough for every healthcare provider across different specialties, including physicians and nurses from local clinics, district hospitals, and medical centers. As a result, we developed a 1-year mortality risk stratification scale (the IFSD Score, in Table 3) using the data of 53 IFSD cases with the five top-ranked predictors mentioned above. All five predictors were assigned with 1 point each. The range of IFSD Scores was 0 to 5. 1-year mortality rates for patients with IFSD Scores of 0, 1, 2, 3, and 4 were 0%, 16.7%, 56.3%, 72.7%, and 100%, respectively (in Figure 1). 4 cases (7.5%) scored 0; 18 cases (34.0) scored 1; 16 cases (30.2%) scored 2; 11 cases (20.8%) scored 3; and 4 cases (7.5%) scored 4. No patient in the CGRD cohort had an IFSD Score of 5. However, given that no patient with an ICH Score of 4 survived, an ICH Score of 5 would be expected with extremely high mortality risk. Each increase in the IFSD Score was associated with a marked increase in 1-year mortality (p <0.001). The mortality rates rose more than three times from an IFSD Score of 1 to 2, indicating a decisive difference in clinical outcomes at this turning point. The time-dependent 1-year survival curve was depicted in Figure 2 according to the Kaplan–Meier method. The area under the curve (AUC) of the receiver operating characteristic curve was 0.823 (p < 0.001). For a diagnostic model to be meaningful, the AUC ≥ 0.8 is considered good and representative [56]. As a result, our model generates an excellent performance.
4.3. Limitations
The main limitation of our work was its retrospective nature, including enrolment biases, patients lost to follow-up, and missing data. Still, some questions were left unanswered. For instance, the study endpoint, long-term follow-up of functional outcome, and the recurrence rate were not available in the database. The different clinical experiences of spine surgeons from all seven hospitals led to various treatment options and surgical strategies. The selection and priority of the antifungal agents, the indications for surgical intervention, and the perioperative care cannot be standardized. Also, the rareness of the disease might produce low statistical power because of the small sample size. More large-scale and international validations would be necessary before this scoring model is commonly used.
5. Conclusions
Invasive spondylodiscitis due to fungi was once rare but now is increasing. Most of our patients were treated according to clinical experience and current guidelines. It is unclear if they would have had better outcomes with different treatment and surgical strategies. With 53 patients included over 19 years, this work represents the most extensive report of IFSD in the literature to date. We developed the IFSD score with easily obtained demographic, clinical, and laboratory parameters to predict the 1-year mortality rate. This model could help physicians with quicker awareness to identify IFSD patients with a greater 1-year mortality risk of over 50% at a score over two. We plan to use the scoring system in our daily clinical practice to validate whether this model can predict survival accurately. Further prospective trials will investigate long-term functional outcomes and the disease recurrence rate as endpoints.
Author Contributions
Conception and design: Ming-Hsue Lee, Kuo-Tai Chen, Chao-Chun Yang. Acquisition of data: Chia-Yen Liu, Meng-Hung Lin, Yao-Hsu Yang, Chao-Chun Yang. Analysis and interpretation of data: Chia-Yen Liu, Meng-Hung Lin, Chao-Chun Yang. Drafting the article: Chao-Chun Yang, Chia-Yen Liu. Critically revising the article: Ming-Hsue Lee, Chung-Yu Huang. Reviewed submitted version of manuscript: All authors. Study supervision: Ming-Hsue Lee, Chung-Yu Huang, Yao-Hsu Yang.
Funding
This work was supported by the Chang Gung Medical Research Program Foundation (grant number CORPG6G0203, CGRPG6L0031). The funding source played no role in study design and conduct, data collection, analysis or interpretation, manuscript writing, or submitting it for publication.
Institutional Review Board Statement
This retrospective cohort study was approved by the Institutional Review Board of Chang Gung Medical Foundation (IRB number: 201901636B0). The Ethics Committee waived the requirement for informed consent for this study, and the data were analyzed anonymously. This study was performed under relevant guidelines and regulations.
Acknowledgments
We thank the Health Information and Epidemiology Laboratory of Chiayi Chang Gung Memorial Hospital for their comments and assistance in the data analysis.
Conflicts of Interest
All authors declare that they have no conflicts of interest.
Abbreviations
Invasive Fungal Spondylodiscitis (IFSD), Chang Gung Research Database (CGRD), Chang Gung Memorial Hospital (CGMH), International Classification of Diseases (ICD), Computed Tomography (CT), Magnetic Resonance Imaging (MRI), End Stage Renal Disease (ESRD), Hemodialysis (H/D), Peritoneal Dialysis (P/D), Acquired Immunodeficiency Syndrome (AIDS), Conus Medullaris Syndrome (CMS), Cauda Equina Syndrome (CES)
References
- Grammatico, L., et al., Epidemiology of vertebral osteomyelitis (VO) in France: analysis of hospital-discharge data 2002-2003. Epidemiol Infect, 2008. 136(5): p. 653-60. [CrossRef]
- Beronius, M., B. Bergman, and R. Andersson, Vertebral osteomyelitis in Göteborg, Sweden: a retrospective study of patients during 1990-95. Scand J Infect Dis, 2001. 33(7): p. 527-32. [CrossRef]
- Babic, M. and C.S. Simpfendorfer, Infections of the Spine. Infect Dis Clin North Am, 2017. 31(2): p. 279-297. [CrossRef]
- Kim, C.W., et al., Fungal infections of the spine. Clin Orthop Relat Res, 2006. 444: p. 92-9. [CrossRef]
- Geisler Crone, C., et al., Clinical characteristics of pyogenic vertebral osteomyelitis, and factors associated with inadequate treatment response. Int J Infect Dis, 2021. 108: p. 487-493. [CrossRef]
- Gouliouris, T., S.H. Aliyu, and N.M. Brown, Spondylodiscitis: update on diagnosis and management. J Antimicrob Chemother, 2010. 65 Suppl 3: p. iii11-24. [CrossRef]
- Hadjipavlou, A.G., et al., Hematogenous pyogenic spinal infections and their surgical management. Spine (Phila Pa 1976), 2000. 25(13): p. 1668-79. [CrossRef]
- Parry, M.F., et al., Candida osteomyelitis and diskitis after spinal surgery: an outbreak that implicates artificial nail use. Clin Infect Dis, 2001. 32(3): p. 352-7. [CrossRef]
- Tay, B.K., J. Deckey, and S.S. Hu, Spinal infections. J Am Acad Orthop Surg, 2002. 10(3): p. 188-97. [CrossRef]
- Wu, M.-H., et al., Treatment outcomes of fungal vertebral osteomyelitis: A case series study and literature review. Formosan Journal of Musculoskeletal Disorders, 2015. 6: p. 89-97. [CrossRef]
- Talha, K.M., et al., Native Vertebral Osteomyelitis in Patients with Staphylococcus Aureus Bacteremia. Am J Med Sci, 2022. 363(2): p. 140-146. [CrossRef]
- Cobar, A., et al., Journal of Spine Fungal Spondylodiscitis: Review. Journal of Spine, 2016. 5. [CrossRef]
- Frazier, D.D., et al., Fungal infections of the spine. Report of eleven patients with long-term follow-up. J Bone Joint Surg Am, 2001. 83(4): p. 560-5.
- Caldera, G., et al., Fungal Spondylodiscitis: Review. Journal of Spine, 2016. 2016: p. 1-6. [CrossRef]
- Ganesh, D., et al., Fungal Infections of the Spine. Spine, 2015. 40(12): p. E719-E728. [CrossRef]
- Ascioglu, S., et al., Defining opportunistic invasive fungal infections in immunocompromised patients with cancer and hematopoietic stem cell transplants: an international consensus. Clin Infect Dis, 2002. 34(1): p. 7-14. [CrossRef]
- Peter Donnelly, J., Consensus definitions for invasive fungal disease: Strengths, limitations, and revisions. Med Mycol, 2006. 44(Supplement_1): p. S285-s288. [CrossRef]
- De Pauw, B., et al., Revised definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) Consensus Group. Clin Infect Dis, 2008. 46(12): p. 1813-21. [CrossRef]
- Donnelly, J.P., et al., Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin Infect Dis, 2020. 71(6): p. 1367-1376. [CrossRef]
- Tsitsikas, D.A., et al., Impact of the revised (2008) EORTC/MSG definitions for invasive fungal disease on the rates of diagnosis of invasive aspergillosis. Med Mycol, 2012. 50(5): p. 538-42. [CrossRef]
- Richaud, C., et al., Candida vertebral osteomyelitis (CVO) 28 cases from a 10-year retrospective study in France. Medicine (Baltimore), 2017. 96(31): p. e7525. [CrossRef]
- Tsai, M.S., et al., Chang Gung Research Database: A multi-institutional database consisting of original medical records. Biomed J, 2017. 40(5): p. 263-269. [CrossRef]
- Shao, S.C., et al., The Chang Gung Research Database-A multi-institutional electronic medical records database for real-world epidemiological studies in Taiwan. Pharmacoepidemiol Drug Saf, 2019. 28(5): p. 593-600. [CrossRef]
- Nesković, V., Preoperative assesment of the immunocompromised patient. Acta Chir Iugosl, 2011. 58(2): p. 185-92. [CrossRef]
- Miller, D.J. and G.C. Mejicano, Vertebral osteomyelitis due to Candida species: case report and literature review. Clin Infect Dis, 2001. 33(4): p. 523-30. [CrossRef]
- Issa, K., et al., Delay in Diagnosis of Vertebral Osteomyelitis Affects the Utility of Cultures. Surg Technol Int, 2016. 29: p. 379-383.
- Grados, F., et al., Suggestions for managing pyogenic (non-tuberculous) discitis in adults. Joint Bone Spine, 2007. 74(2): p. 133-9. [CrossRef]
- Boody, B.S., et al., Vertebral Osteomyelitis and Spinal Epidural Abscess: An Evidence-based Review. J Spinal Disord Tech, 2015. 28(6): p. E316-27. [CrossRef]
- Cornett, C.A., et al., Bacterial Spine Infections in Adults: Evaluation and Management. J Am Acad Orthop Surg, 2016. 24(1): p. 11-8. [CrossRef]
- Enoch, D.A., et al., Value of CT-guided biopsy in the diagnosis of septic discitis. J Clin Pathol, 2008. 61(6): p. 750-3. [CrossRef]
- Chew, F.S. and M.J. Kline, Diagnostic yield of CT-guided percutaneous aspiration procedures in suspected spontaneous infectious diskitis. Radiology, 2001. 218(1): p. 211-4. [CrossRef]
- Diehn, F.E., Imaging of spine infection. Radiol Clin North Am, 2012. 50(4): p. 777-98. [CrossRef]
- Zimmerli, W., Clinical practice. Vertebral osteomyelitis. N Engl J Med, 2010. 362(11): p. 1022-9. [CrossRef]
- Foreman, S.C., et al., MR and CT Imaging to Optimize CT-Guided Biopsies in Suspected Spondylodiscitis. World Neurosurg, 2017. 99: p. 726-734.e7. [CrossRef]
- Gathe, J.C., Jr., et al., Candida osteomyelitis. Report of five cases and review of the literature. Am J Med, 1987. 82(5): p. 927-37. [CrossRef]
- Treglia, G., et al., The role of nuclear medicine in the diagnosis of spondylodiscitis. Eur Rev Med Pharmacol Sci, 2012. 16 Suppl 2: p. 20-5.
- Sethi, S., et al., Aspergillus vertebral osteomyelitis in immunocompetent patients. Indian J Orthop, 2012. 46(2): p. 246-50. [CrossRef]
- Sapico, F.L. and J.Z. Montgomerie, Vertebral osteomyelitis. Infect Dis Clin North Am, 1990. 4(3): p. 539-50. [CrossRef]
- Waldvogel, F.A., G. Medoff, and M.N. Swartz, Osteomyelitis: a review of clinical features, therapeutic considerations, and unusual aspects. N Engl J Med, 1970. 282(4): p. 198-206. [CrossRef]
- Bonakdar-pour, A. and V.D. Gaines, The radiology of osteomyelitis. Orthop Clin North Am, 1983. 14(1): p. 21-37. [CrossRef]
- Golimbu, C., H. Firooznia, and M. Rafii, CT of osteomyelitis of the spine. AJR Am J Roentgenol, 1984. 142(1): p. 159-63. [CrossRef]
- Lew, D.P. and F.A. Waldvogel, Osteomyelitis. N Engl J Med, 1997. 336(14): p. 999-1007. [CrossRef]
- Kang, M., et al., CT-guided fine-needle aspiration biopsy of spinal lesions. Acta Radiol, 1999. 40(5): p. 474-8. [CrossRef]
- Broner, F.A., D.E. Garland, and J.E. Zigler, Spinal infections in the immunocompromised host. Orthop Clin North Am, 1996. 27(1): p. 37-46. [CrossRef]
- Gerometta, A., F. Bittan, and J.C. Rodriguez Olaverri, Postoperative spondilodiscitis. Int Orthop, 2012. 36(2): p. 433-8. [CrossRef]
- Kushwaha, V.P., et al., Musculoskeletal coccidioidomycosis. A review of 25 cases. Clin Orthop Relat Res, 1996(332): p. 190-9.
- Almekinders, L.C. and W.B. Greene, Vertebral Candida infections. A case report and review of the literature. Clin Orthop Relat Res, 1991(267): p. 174-8.
- Bross, J., et al., Risk factors for nosocomial candidemia: a case-control study in adults without leukemia. Am J Med, 1989. 87(6): p. 614-20. [CrossRef]
- Williams, R.L., et al., Fungal spinal osteomyelitis in the immunocompromised patient: MR findings in three cases. AJNR Am J Neuroradiol, 1999. 20(3): p. 381-5.
- Tang, T.J., et al., Aspergillus osteomyelitis after liver transplantation: conservative or surgical treatment? Eur J Gastroenterol Hepatol, 2000. 12(1): p. 123-6.
- Hummel, M., et al., Aspergillosis with Aspergillus osteomyelitis and diskitis after heart transplantation: surgical and medical management. J Heart Lung Transplant, 1993. 12(4): p. 599-603.
- Rex, J.H., et al., Practice guidelines for the treatment of candidiasis. Infectious Diseases Society of America. Clin Infect Dis, 2000. 30(4): p. 662-78. [CrossRef]
- Dellinger, R.P., et al., Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med, 2013. 41(2): p. 580-637. [CrossRef]
- Devran, O., et al., C-reactive protein as a predictor of mortality in patients affected with severe sepsis in intensive care unit. Multidiscip Respir Med, 2012. 7(1): p. 47. [CrossRef]
- WHO, Hemoglobin Concentrations for the Diagnosis of Anemia and Assessment of Severity. World Health Organization, Geneva, 2011.
- Nahm, F.S., Receiver operating characteristic curve: overview and practical use for clinicians. Korean J Anesthesiol, 2022. 75(1): p. 25-36. [CrossRef]
Figure 1.
The IFSD Score and 1-year mortality. Each increase in the IFSD Score was associated with a marked increase in 1-year mortality (p <0.001*). No patient in our cohort study had an IFSD score of 5. IFSD, invasive fungal spondylodiscitis. * p <0.05, clinical significance.
Figure 1.
The IFSD Score and 1-year mortality. Each increase in the IFSD Score was associated with a marked increase in 1-year mortality (p <0.001*). No patient in our cohort study had an IFSD score of 5. IFSD, invasive fungal spondylodiscitis. * p <0.05, clinical significance.
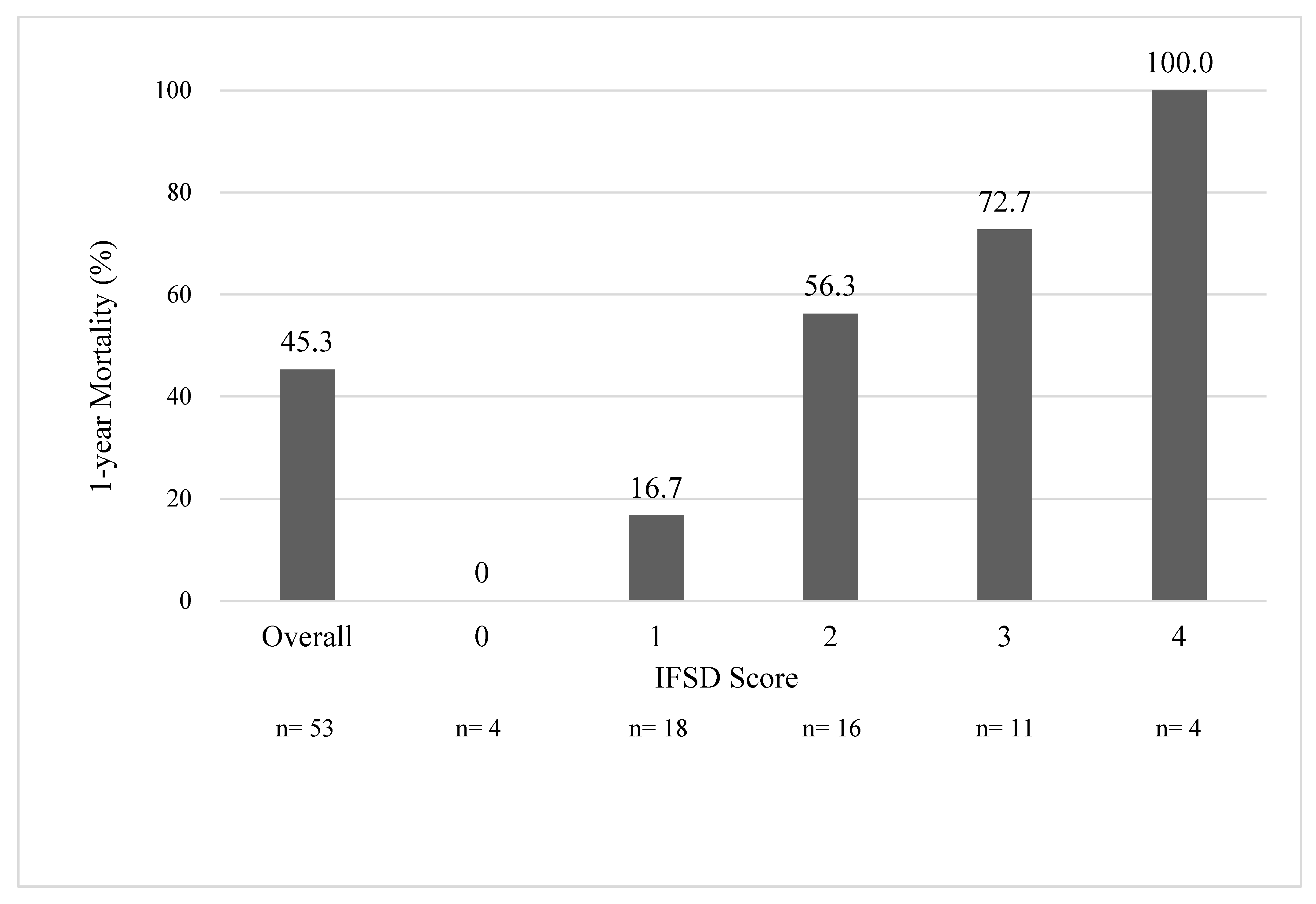
Figure 2.
Time-dependent, 1-year-survival Kaplan-Meier curves by different IFSD scores. IFSD, invasive fungal spondylodiscitis.
Figure 2.
Time-dependent, 1-year-survival Kaplan-Meier curves by different IFSD scores. IFSD, invasive fungal spondylodiscitis.
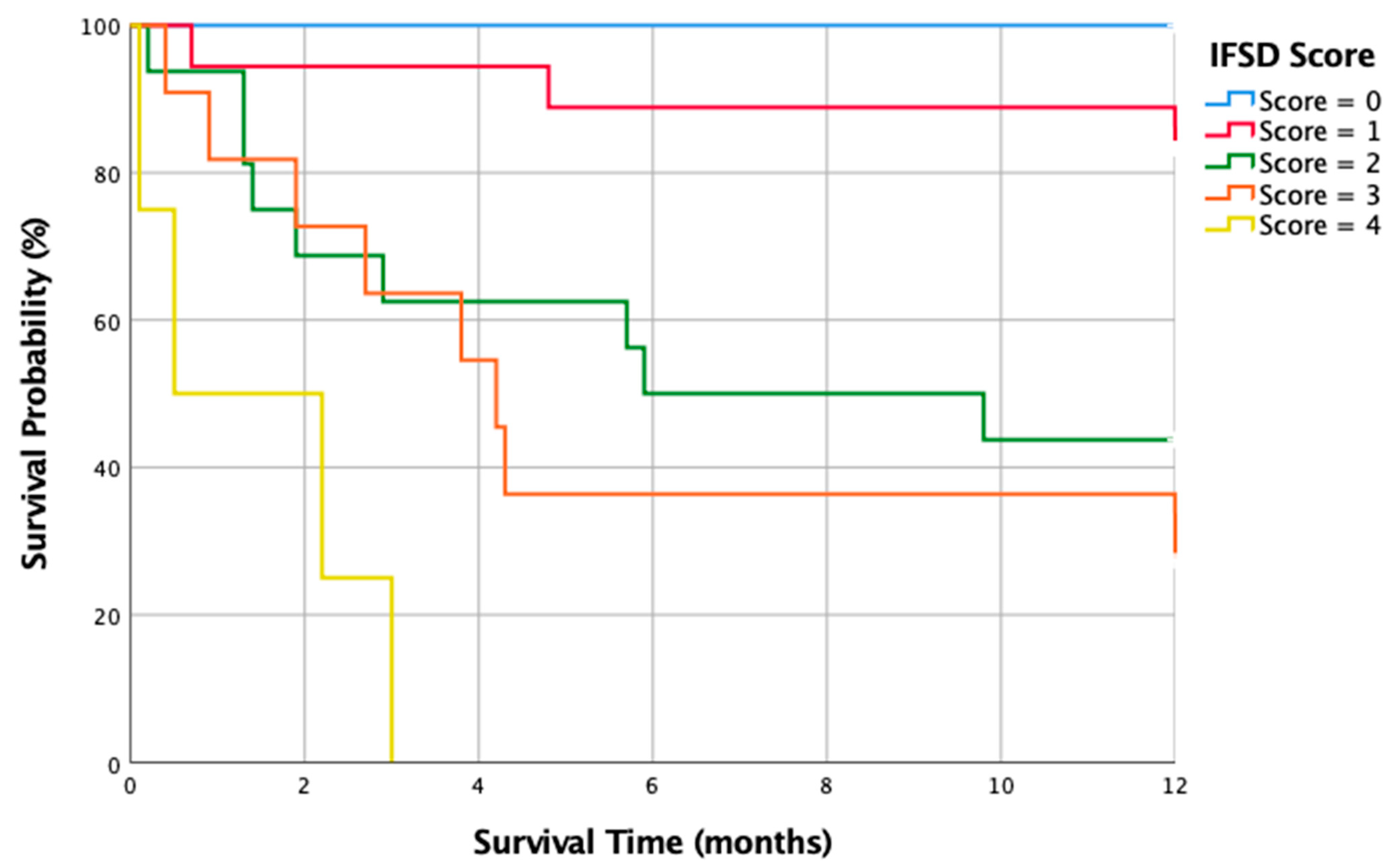
Figure 3.
The ROC curve and the AUC. This IFSD scoring model provides excellent performance in predicting a 1-year mortality rate (AUC = 0.823, p < 0.001*). ROC, receiver operating characteristic; AUC, the area under the curve; IFSD, invasive fungal spondylodiscitis. * p <0.05, clinical significance.
Figure 3.
The ROC curve and the AUC. This IFSD scoring model provides excellent performance in predicting a 1-year mortality rate (AUC = 0.823, p < 0.001*). ROC, receiver operating characteristic; AUC, the area under the curve; IFSD, invasive fungal spondylodiscitis. * p <0.05, clinical significance.
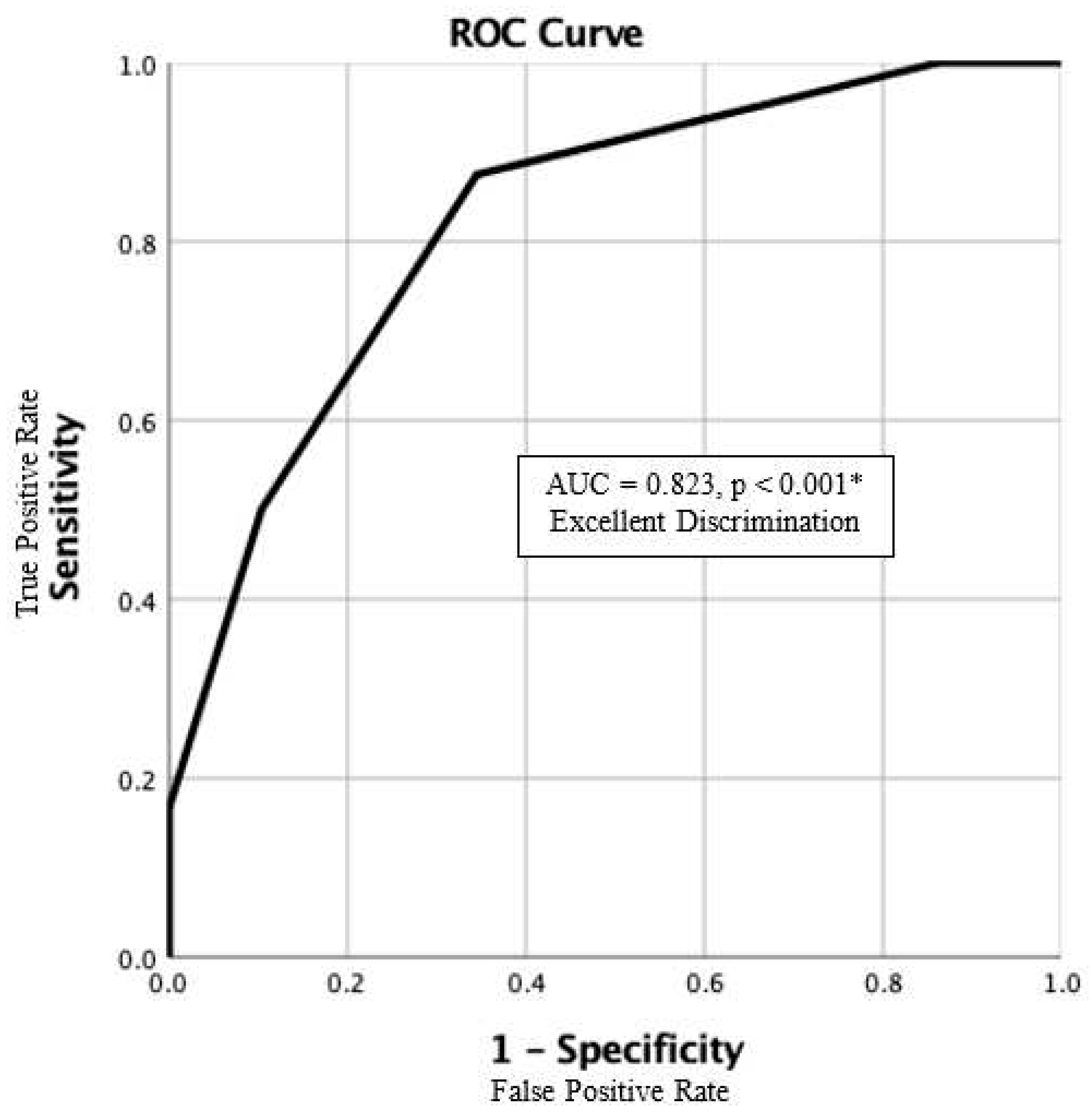

Table 1.
Clinical and biological characteristics of 53 patients with invasive fungal spondylodiscitis and the survival subgroup analysis. IQ, interquartile; VB, vertebral body; WBC, white blood count; Hb, hemoglobin; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; UGI, upper gastrointestinal tract. * p <0.05, clinical significance.
Table 1.
Clinical and biological characteristics of 53 patients with invasive fungal spondylodiscitis and the survival subgroup analysis. IQ, interquartile; VB, vertebral body; WBC, white blood count; Hb, hemoglobin; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; UGI, upper gastrointestinal tract. * p <0.05, clinical significance.
| All | 1-year Mortality | |||
| Dead (n=24) | Survivors (n=29) | p value | ||
|
Age, years, median, interquartile range |
65.6 (56.1-74.0) | 67.5 (59.1-74.8) | 64.0 (49.4-73.8) | 0.090 |
| Male, n, % | 35 (66.0) | 16 (66.7) | 19 (65.5) | 0.930 |
| Predisposing Immunocompromised State, n, % | 17 (32.1) | 12 (50.0) | 5 (17.2) | 0.011 |
| Initial Clinical Manifestations | ||||
| Fever, n, % | 30 (56.6) | 15 (62.5) | 15 (51.7) | 0.431 |
| Radicular pain, n, % | 33 (62.3) | 15 (62.5) | 18 (62.1) | 0.974 |
| Muscular weakness, n, % | 23 (43.4) | 11 (45.8) | 12 (41.4) | 0.745 |
| Myelopathy, n, % | 7 (13.2) | 4 (16.7) | 3 (10.3) | 0.499 |
| Onset time to diagnosis, weeks, median, interquartile range |
3.0 (2.0-5.0) | 3.0 (1.8-4.0) | 3.0 (2.0-8.0) | 0.578 |
| Initial Radiological Findings | ||||
| X-rays | ||||
| Disc space narrowing, n, % | 35 (79.5) | 12 (75.0) | 23 (82.1) | 0.572 |
| Endplate erosion, n, % | 30 (68.2) | 9 (56.3) | 20 (71.4) | 0.307 |
| VB collapse, n, % | 10 (22.7) | 2 (12.5) | 8 (28.6) | 0.221 |
| CTs | ||||
| Endplate erosion, n, % | 23 (88.5) | 12 (85.7) | 10 (91.7) | 0.867 |
| VB collapse, n, % | 15 (57.7) | 9 (64.3) | 6 (50.0) | 0.462 |
| Paraspinal tissue abscess, n, % | 23 (88.5) | 11 (78.6) | 11 (100.0) | 0.356 |
| Epidural abscess, n, % | 17 (65.4) | 7 (50.0) | 16 (83.3) | 0.006* |
| MRIs | ||||
| Loss of intradiscal key sign, n, % | 44 (93.6) | 18 (94.7) | 26 (92.9) | 0.796 |
| VB signal change T2 edema, n, % | 38 (80.9) | 15 (78.9) | 23 (82.1) | 0.785 |
| Cord/Sac compression, n, % | 35 (79.5) | 12 (75.0) | 23 (82.1) | 0.572 |
| Root compression, n, % | 30 (68.2) | 9 (56.3) | 20 (71.4) | 0.307 |
| Paraspinal tissue abscess, n, % | 10 (22.7) | 10 (22.7) | 8 (28.6) | 0.221 |
| Bone scans | ||||
| Positive for spondylodiscitis, n, % | 13 (76.5) | 5 (55.6) | 8 (100.0) | 0.001* |
| Inflammatory scans | ||||
| Positive for spondylodiscitis, n, % | 19 (86.4) | 6 (66.7) | 13 (100.0) | 0.069 |
| Pre-treatment Lab Findings | ||||
| WBC, 103/uL, median, IQ range | 10.5 (7.1-13.7) | 12.4 (8.9-14.2) | 11.0 (7.6-12.5) | 0.040* |
| Hb, g/dL, median, IQ range | 9.7 (8.6-10.9) | 9.0 (8.2-10.1) | 10.2 (9.4-11.2) | 0.034* |
| Platelet, 103/uL, median, IQ range | 257 (134.0-350.0) | 169 (101.5-293.5) | 291 (179.0-407.0) | 0.021* |
| ESR, mm/h, median, IQ range | 86 (56.5-103) | 95 (58.0-112.3) | 82 (57.0-101.0) | 0.585 |
| CRP, mg/dL, median, IQ range | 94 (41.0-162.8) | 150 (91.3-195.5) | 50 (25.0-112.0) | 0.002* |
| Candidemia, n, % | 25 (47.2) | 16 (66.7) | 9 (31.0) | 0.010* |
| Fungal Species | ||||
| Aspergillus unspecified, n, % | 1 (1.9) | 1 (4.2) | 0 (0.0) | - |
| Candida albicans, n, % | 32 (60.4) | 11 (45.8) | 21 (72.4) | 0.049* |
| Candida glabrata, n, % | 3 (5.7) | 2 (8.3) | 1 (3.4) | 0.444 |
| Candida krusei, n, % | 1 (1.9) | 0 (0.0) | 1 (3.4) | - |
| Candida parapsilosis, n, % | 4 (7.5) | 2 (8.3) | 2 (6.9) | 0.844 |
| Candida tropicalis, n, % | 7 (13.2) | 4 (16.7) | 3 (10.3) | 0.499 |
| Canda lusitaniae, n, % | 1 (1.9) | 1 (4.2) | 0 (0.0) | - |
| Candida unspecified, n, % | 1 (1.9) | 1 (4.2) | 0 (0.0) | - |
| Cryptococcus neoformans, n, % | 1 (1.9) | 1 (4.2) | 0 (0.0) | - |
| Debaryomyces hansenii | 1 (1.9) | 1 (4.2) | 0 (0.0) | - |
| Fonsecaea pedrosoi | 1 (1.9) | 0 (0.0) | 1 (3.4) | - |
| Treatment Strategies | ||||
| Non-surgical treatment, n, % | 18 (34.0) | 13 (54.2) | 5 (17.2) | 0.005* |
| Surgical intervention, n, % | 35 (66.0) | 11 (45.8) | 24 (82.8) | - |
| Debridement Only, n, % | 11 (31.4) | 4 (36.4) | 7 (37.5) | 0.011* |
| Debridement + Instrumentation n, % | 24 (68.6) | 9 (63.6) | 16 (62.5) | - |
| Multiple-stage OP, n, % | 25 (71.4) | 8 (80.0) | 16 (64.0) | 0.002* |
| 1-stage OP, n, % | 10 (28.6) | 2 (20.0) | 9 (36.0) | - |
| Surgical Related Complications | ||||
| Superficial wounds infection, n, % | 5 (9.4) | 1 (4.2) | 4 (13.8) | 0.233 |
| Reoperation for debridement, n, % | 7 (13.2) | 3 (12.5) | 4 (13.8) | 0.890 |
| General Complications | ||||
| Respiratory failure, n, % | 19 (35.8) | 15 (62.5) | 3 (13.8) | <0.001* |
| Hospital acquired pneumonia, n, % | 17 (32.1) | 14 (58.3) | 3 (10.3) | <0.001* |
| Acute kidney injury, n, % | 13 (24.5) | 11 (45.8) | 2 (6.9) | 0.001* |
| Urinary tract infection, n, % | 13 (24.5) | 7 (29.2) | 6 (20.7) | 0.475 |
| Electrolyte imbalance, n, % | 18 (34.0) | 12 (50.0) | 6 (20.7) | 0.025* |
| Acute coronary syndrome, n, % | 3 (5.7) | 2 (8.3) | 1 (3.4) | 0.444 |
| Metabolic encephalopathy, n, % | 10 (18.9) | 9 (37.5) | 1 (3.4) | 0.002* |
| UGI bleeding, n, % | 10 (18.9) | 7 (29.2) | 3 (10.3) | 0.081 |
| Pressure sore, n, % | 4 (7.5) | 1 (4.2) | 3 (10.3) | 0.397 |
Table 2.
Investigating predictors for 1-year mortality using a multivariable Cox proportional hazards model. Four of them were statistically significant, and one of them was strongly related. BT, body temperature; WBC, white blood count; Hb, hemoglobin; CRP, C-reactive protein. * p <0.05, clinical significance.
Table 2.
Investigating predictors for 1-year mortality using a multivariable Cox proportional hazards model. Four of them were statistically significant, and one of them was strongly related. BT, body temperature; WBC, white blood count; Hb, hemoglobin; CRP, C-reactive protein. * p <0.05, clinical significance.
| Hazard ratio | 95.0% Confidence interval | p value | ||
| Lower | Upper | |||
| Age > 65 | 1.53 | 0.63 | 3.69 | 0.346 |
| Immunocompromised | 3.01 | 1.15 | 7.84 | 0.024* |
| BT > 38.3 or < 36 | 2.44 | 0.84 | 7.11 | 0.103 |
| Radiculopathy or Myelopathy | 4.04 | 1.37 | 11.93 | 0.012* |
| WBC > 1.2 or < 0.4 | 2.83 | 1.00 | 7.95 | 0.049* |
| Hemoglobin < 8 | 4.93 | 1.39 | 17.50 | 0.014* |
| Platelet < 100 | 0.86 | 0.24 | 3.17 | 0.826 |
| CRP > 100 | 1.90 | 0.68 | 5.29 | 0.218 |
| Candidemia | 2.78 | 0.99 | 7.77 | 0.052 |
Table 3.
The proposed IFSD score. Each predictor is assigned 1 point. The range of IFSD Scores is 0 to 5. IFSD, invasive fungal spondylodiscitis; WBC, white blood count; Hb, hemoglobin.
Table 3.
The proposed IFSD score. Each predictor is assigned 1 point. The range of IFSD Scores is 0 to 5. IFSD, invasive fungal spondylodiscitis; WBC, white blood count; Hb, hemoglobin.
| The IFSD Score | ||
| Component | IFSD Score Points | |
| Immune State | ||
| Immunocompromised | 1 | |
| Immunocompetent | 0 | |
| Neurological Deficits | ||
| Radiculopathy or Myelopathy | 1 | |
| None | 0 | |
| WBC Count (103/uL) | ||
| > 12.0 or < 0.4 | 1 | |
| 0.4 to 12.0 | 0 | |
| Hemoglobin (g/dL) | ||
| <8 | 1 | |
| ≧8 | 0 | |
| Evidence of Candidemia | ||
| Yes | 1 | |
| None | 0 | |
| Overall IFSD score | Sum of the points above (0-5) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



