Submitted:
13 November 2023
Posted:
13 November 2023
Read the latest preprint version here
Abstract
Data show that ischemic stroke is one of the leading causes of death and disability worldwide. Knowledge of ischemic stroke-related guidelines is vital for health care professionals working in the Emergency Departments (EDs) because it affects the early diagnosis and timely treatment to combating stroke. We aimed to explore knowledge regarding the recognition and management of the ischemic stroke among Greek-Cypriot emergency health care personnel (nurses and physicians). A descriptive cross-sectional correlation study was implemented from November 2019 to April 2020 across 4 private and 7 public EDs in Cyprus. Data were collected with the use of a self-reported questionnaire, developed by the research team. 255 nurses [Response Rate (RR): 74.1%] and 26 physicians (RR; 47.3%) completed the questionnaire. The participants gave a correct answer to an average of 12.9 statements from a total of 28 (SD: 4.2) with nurses and physicians scoring a mean of 12.9 (SD:4.1) and 15,7 (SD: 4) respectively. Participating hospitals scored an average of 10.3 to 14.1. Participants with previous training scored an average of 1.45 addi-tional correct answers. Greek-Cypriot health care professionals in EDs reported poor to moderate knowledge about ischemic stroke highlighting the need for targeted and continuous education, and further study of factors related with this may be of interest. Also, development and implementation of evidence-based protocols and enhanced education regarding ischemic stroke should be considered essential interventions for emergency health care professionals.
Keywords:
early arrival
; emergency department
; healthcare professionals
; hospital care
; knowledge
; man-agement
; prehospital care
; recognition
; stroke
1. Introduction
Stroke represents a major healthcare burden as it is associated with significant morbidity, including disability, and mortality [1,2,3]. Modern intra-arterial therapies of ischemic stroke (thrombolysis/ thrombectomy) have a narrow optimal therapeutic window, beyond which clinical outcomes deteriorate [4,5]. Therefore, timely recognition and management of patients suffering an ischemic stroke is vital, since it renders more patients as suitable candidates for such therapies.
Guidelines on stroke diagnosis and management are renewed regularly [5,6,7]. It is, however, a matter of ongoing research whether healthcare professionals involved in stroke care have up-to-date knowledge on this subject. A significant amount of research has been dedicated on pre-hospital acute stroke care; from the assessment of knowledge [8,9] to the development of triage techniques [10] and targeted educational interventions for improving knowledge and optimizing stroke recognition and fast transfer to dedicated stroke centers [11,12,13]. What is also pivotal, however, is the timely admission of the stroke patients to the Emergency Department (ED). Delays in first-contact diagnosis and interfacility transfer are to be attributed to the hospital-to-hospital transfer [14], whereas hospital door-to-revascularization delays are dependent mainly on the ED staff, nurses and physicians, who represent the next set of healthcare professionals (HCPs) that the stroke patient encounters, following paramedics [15,16]. Stroke patients might also present themselves straight to the ED, thus making ED personnel their first medical contact. Among various barriers highlighted by review articles as hindering guideline-based management of stroke patients [17,18], insufficient knowledge and stroke unawareness are encountered among personnel involved in acute stroke care, mainly EDs, whether physicians [19,20,21,22,23,24,25,26] or nurses [20,21,22,23,27,28,29,30,31,32,33]. The phenomenon is universal; studies have explored ED personnel from the USA [21,28,29,30,31], Great Britain [27], Scandinavia [19,23], India [33], Kenya [34], Saudi Arabia [25,26] and Australia [22,24], countries, that is, with diverse management and various levels of acute stroke care. Level of knowledge regarding signs and symptoms of stroke and eligibility criteria for intra-arterial therapies have been quantified in most studies through physically administered [20,21,27,28,29,31,33,34], mailed [19,22] or web-based [24,25,30] questionnaires, usually author-developed [27,28,31] and based on available guidelines or fast stroke-recognition codes or scales.
In recognition of the critical role played by ED in minimizing door-to-revascularization times and enhancing stroke outcomes, we embarked on a study in the Republic of Cyprus. Our research aimed to assess the knowledge of stroke recognition and management among healthcare professionals working in the ED for the first time in Cyprus. Given that both nurses and physicians play key roles in the initial in-hospital stroke care within Greek-Cypriot EDs, our study targeted both of these healthcare provider populations.
2. Materials and Methods
2.1. Design and Setting
This was a descriptive comparative study, which invited all 12 Emergency Departments (EDs) of public and private hospitals (seven and five hospitals, respectively) across the Republic of Cyprus to participate. All seven public [Hospital A (HA), Hospital B (HB), Hospital C (HC), Hospital D (HD), Hospital E (HE), Hospital F (HF), Hospital G (HG)] and four of the five private hospitals [Private Hospital A (PHA), Private Hospital B (PHB), Private Hospital C (PHC), Private Hospital D (PHD)] provided consent. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) was followed [35].
2.2. Participants and Sample Size
Target population consisted of nurses and physicians (termed HCPs hereafter) who had worked for at least one shift at an ED of a consent-granting medical institution, had the ability to read and write in Greek, and had provided a written informed consent. No criteria for exclusion were applied. A power analysis was conducted using the G-Power statistical software [36] to detect a small effect size (R2=0.06) related to the demographic characteristics of ED HCPs on their stroke knowledge. In this analysis, a linear regression model was utilized, which included 7 variables, and it determined that, in order to achieve a statistical power of 80% and maintain a 5% level of statistical significance, a minimum sample size of 247 individuals would be necessary. Convenient sampling was implemented for enrollees and a total of 399 questionnaires were distributed.
2.3. Data Collection and Instrument
Data collection took place from November 2019 to April 2020 during which an anonymous self-administered paper questionnaire was distributed to participants in the participated EDs by the research team. All EDs were accessed at least 3 times each, during the 3 different shifts of the same day, and ED HCPs were invited to participate anonymously, after a brief presentation of the study aim. The questionnaire commenced with an introductory cover letter that provided a comprehensive explanation of the study and its objectives. The survey sheet, comprising 37 questions, covered the following areas:
- -
- Personal data (8 closed-ended questions): This section assessed social demographics (age, gender, profession, education level), employment status (type of hospital, years of work experience) and previous education or training in stroke along with the sources of such education.
- -
-
Knowledge on stroke recognition and management (28 questions). This section assessed:
- (a)
- General knowledge on stroke [Question regarding general knowledge on stroke (QGK)]: 4 questions with possible responses include ‘right’, ‘wrong’ or 'I don't know’
- (b)
- Knowledge on stroke recognition [Question regarding knowledge on stroke recognition (QKSR)]: 2 multiple choice questions and 6 questions with possible responses include ‘right’, ‘wrong’ or 'I don't know’
- (c)
- Knowledge on stroke management [Question regarding knowledge on stroke management (QKSM)]: 2 multiple choice questions and 14 questions with possible responses include ‘right’, ‘wrong’ or 'I don't know’]
- (d)
- Self assessment on knowledge on stroke recognition and management: 1 question with possible responses include 'poorly’, 'well’, 'very well’ and ‘expert’.
Participants were not afforded any preparation time; they were required to complete the questionnaires under the supervision of a member of the research team within a maximum of 15 minutes. Subsequently, the completed questionnaires were placed in anonymous envelopes, while the signed consent documents were stored separately.
2.4. Questionnaire Development
A pertinent questionnaire in the Greek language had not been previously created. Additionally, existing literature did not adequately incorporate the latest stroke guidelines, specifically those from 2018, which were in effect during the study. In light of these factors, we chose to undertake a systematic process to develop a new tool for assessing knowledge of stroke recognition and management. This new instrument was designed to align with the 2018 American Heart Association (AHA) and American Stroke Association (ASA) stroke guidelines [37], as well as their 2019 update [5], all adapted to the Greek language.
The questionnaire package was developed by study researchers through a staged procedure, according to the Delphi method [38], in which the following individuals were involved: the main researcher; a nurse with 4 years’ experience in an acute stroke care unit abroad; a stroke-specialist/Neurologist with a 10-year experience in a dedicated stroke care center abroad; a Professor of Neurology of the Medical School of the University of Cyprus; an Internal Medicine specialist, with further specialization in acute stroke care in the Stroke Unit of the Royal Infirmary of Edinburgh; and a nurse with a 10-year experience in ED. During the first stage, the main researcher proposed to the committee 35 knowledge questions, based on the 2018 ASA/AHA stroke guidelines, and 10 personal data ones. Three stages followed, during which the members of the committee graded the questions on a 5-point Likert scale, and, under the agreement that questions accumulatively scoring below 80% would be excluded, ended up with 28 knowledge and 8 personal data questions. The aforementioned questions were categorized into the following sections: general inquiries (consisting of 4 questions), questions related to stroke recognition (comprising 8 questions), and questions concerning stroke management and in-hospital follow-up (totaling 16 questions). The survey was completed by a convenience sample of 15 nurses in the HD, not included in the study’s final sample, and redistributed 15 days later, for internal consistency assessment.
2.4. Ethics Approval
The study was initially approved by the National Committee of Bioethics of Cyprus (EEBK/EP/2019.01.74) followed by approval from the Ministry of Health of the Republic of Cyprus (0514/2019). Each hospital administration was then approached and consent for enrollment of personnel from the respective ED was requested. All participants gave their informed written consent. Furthermore, the study's cover letter explicitly stated that all data would be kept deidentified, accessible solely to the research team, and securely stored in pass-word-protected files. We also emphasized the voluntary nature of participation in the study. Each questionnaire package was delivered in unmarked, sealed envelopes without any identifiable features. The study was conducted in accordance with the principles outlined in the Declaration of Helsinki. It's important to note that no interventions were conducted on patients during the course of this study.
2.5. Data Analysis
The internal consistency of the tool was calculated with the Cronbach’s alpha and the inter-rater reliability with the kappa statistic [39]. Kappa values, representing the agreement between the answers provided by the 15 participants during the first and the second time the questionnaire package was distributed, were interpreted as follows: 0.00–0.20 no agreement; 0.21–0.40 satisfactory; 0.41–0.60 moderate; 0.61–0.80 strong; and 0.81–1.00 almost perfect [40]. The knowledge level of study participants, that is the sum of correct answers across the 28 questionnaire items, was presented as mean +/- standard deviation. The correlations between stroke knowledge levels and the characteristics of participants were investigated through independent samples t-tests and ANOVA, comparing different groups of participants, according to e.g., previous training on stroke care or years of work experience. Variables that were found to be statistically significantly associated with stroke knowledge in univariate analysis were then entered into a multivariate, linear regression model to identify independent predictors of stroke knowledge. Statistical analysis was performed with the Statistical Package for Social Sciences (SPSS), version 25.
3. Results
3.1. Questionnaire Testing
Cronbach’s alpha was found to be 0.71 for the complete 28-item stroke knowledge questionnaire, 0.66 for the 4 general knowledge items, 0.45 for the 8 items regarding stroke recognition, and 0.62 for the remaining items on stroke treatment and follow-up. Table 1 presents the 28-item stroke knowledge questionnaire, translated in English, and the respective kappa values, all of which demonstrated an agreement percentage of over 70%, denoting acceptable inter-rater variability.
3.2. Characteristics of the Srudy Participants
281 questionnaires were returned completed [response rate (RR) 70.4%]. In particular, response rate among nurses was 74.1% (255 questionnaires returned out of 344 distributed), while among physicians 47.3% (26 out of 55). Participants were predominantly female (53%); more than half (55.2%) belonged to the age group of 30-39 years. Regarding educational attainment, almost two out of three (61.9%) were university graduates, while a Master’s degree had been obtained by 35.3% of respondents. 70% of respondents had a work experience of over 4 years in an ED and the largest contribution to the study sample came from the four state hospitals HB, HC, HD and HE: 10.7%, 18.5%, 26.3% and 10% of total returned questionnaires, respectively. Private hospitals contributed to 15.7% of study participants.
As for prior education or training relevant to stroke care, more than half of ED HCPs (55.9%) stated that they had received such training in the past. Table 2 presents the sources of such education or training.
3.2 Stroke Knowledge Levels
As demonstrated on Table 3, study participants, either nurses or physicians, fared rather poorly at the 28-item stroke knowledge questionnaire. Participants produced equally low scores in the stroke recognition and stroke management parts of the questionnaire, which were significantly lower than the respective general knowledge section scores. The distribution of achieved scores followed the normal distribution, with the majority of nurses’ total scores hovering between 10-20 and the physicians’ ones between 15-20. Figure 1 demonstrates the ranking of the stroke knowledge questionnaire items according to the percentage of participants who answered correctly. As expected, the general knowledge questions (1-4) were answered correctly by the majority of respondents. When isolating physicians though, the most frequent correct answer was corresponding to question 7 (acute ischemic stroke mimics – hypoglycemia), reaching 96.2%. As for the four items with the lowest scores (questions 26, 16, 25, and 14, with correct answers provided by only 7.1%, 13.2%, 16%, and 17.8% of participants respectively), all were related to thrombolysis. They covered topics such as the transfer of thrombolysed patients to the ICU, the acceptable body temperature to commence thrombolysis, the completion of blood workup and other necessary tests before the administration of thrombolysis, and the recommended thrombolysis time window. Participant self-assessment indicated that 58.4% felt they performed 'well,' 21% 'very well,' and 20.6% 'poorly.'
3.3 Univariate and Multivariate Predictors of Stroke Knowledge
The observed difference in stroke knowledge in favor of ED physicians versus nurses was found to be statistically significant in total knowledge score (p < 0.001) and in stroke recognition knowledge (p=0.001). Prior participation in stroke education/training, reported by 137 nurses and 20 physicians, was associated with a statistically significantly higher stroke knowledge score by 1.45 units on average. Other sociodemographic factors, such as gender, age, or type of hospital (public vs. private) had no impact univariately on the performance on the knowledge questionnaire.
With regard to work experience, participants were divided into 6 groups, with <1, 1–5, 6–10, 11–20, 21–30, and >30 years of work experience in EDs. This variable, together with the aforementioned ones in univariate analysis, were entered into a multivariate linear regression model, the results of which are demonstrated in Supplemental Table S1. In particular, a statistically significant effect of the participants’ work experience on stroke knowledge was found, with all groups of work experience being superior to the <1 year of work experience, and with increasing beta values as age increases (see Table S1). Moreover, significant differences among participating hospitals were evident, with the HC exhibiting the highest scores, although no difference was, again, found collectively among public versus private hospitals. Educational attainment was, surprisingly, found to not influence stroke knowledge, with the exception of a small tendency towards statistical significance of mastering a university’s degree. The superiority of physicians’ knowledge versus nurses displayed in univariate analysis retained its statistical significance within the multivariate model, driven here mainly by a difference in stroke recognition/diagnosis. Finally, having prior education or training on stroke was once again found to be a statistically significant and independent predictor of higher levels of knowledge in general stroke knowledge, stroke recognition, and stroke management.
4. Discussion
In this study, we demonstrated rather low levels of stroke knowledge among HCPs working in EDs throughout the Republic of Cyprus, using a newly developed and validated questionnaire. Higher levels of good stroke knowledge, were found in multivariate analysis to be significantly associated with: extensive experience, being a physician rather than a nurse; and prior education or training in stroke management.
The level of stroke knowledge among HCPs in the present study was found to be 46%, proportionally rated among the lowest in available literature, since overall rates range roughly from 50 to 70%. Harper et al., demonstrated in one of the first studies in the field, a mean score of 53% of stroke knowledge among 20 US nurses who had completed a short, 10-item questionnaire [28]. In another study from the US, 63 nurses and paramedics scored 58% on average on a 10-item, evidence-based, multiple choice, knowledge quiz [29]. In a study from Brazil, 20 nurses were tested on the recognition of stroke signs and symptoms and scored an average of 68.5% [32], while other populations of emergency health care professionals from Saudi Arabia [11] and India [33] achieved even higher scores, namely 64% and 68.8% respectively. In a recent nationwide study from Malaysia, conducted with an online questionnaire among HCPs was found that 76% of the respondents had good knowledge of stroke [41].
Comparing, however, stroke knowledge levels from various studies can be challenging, since i) the types of healthcare professionals studied are not uniform: nurses, paramedics, physicians, even medical students [34], with various training backgrounds, are included in various combinations; ii) the stroke care settings are diverse: dedicated stroke care units, emergency departments, or pre-hospital emergency services; iii) the tools used to quantify stroke knowledge are, again, not universal, and most often author-developed for the purposes of every single study; and iv) study populations stem from different countries, with vast differences in stroke care organization and large deviations in the implementation of guideline-based therapies. Despite these shortcomings, a universal conclusion can indeed be reached, and that would be of an overall sub-optimal stroke knowledge level among healthcare professionals engaged in stroke care.
Should one look into specific fields of stroke knowledge, would realize that the guideline-proposed time-window for thrombolysis in patients with acute ischemic stroke was known to only 17.8% of the participants in our study, a percentage significantly lower than the ones reported in relevant literature. In a study in an academic, US, tertiary hospital that involved 58 emergency department healthcare providers, 56% of respondents were familiar with the 3-hour thrombolysis time-window [21], whereas in a stroke referral center in Kenya 53.8% of respondents were aware of it, although 2/3 of participants were medical students [34]. Similar results were found in a Chinese study with 54% of community physicians be aware of the time – window for thrombolysis [42]. The extremely low performance of Greek-Cypriot ED HCPs in the corresponding question regarding the current guideline of the 3-hour thrombolysis time-window was accompanied by a knowledge gap regarding other, thrombolysis-related, questionnaire items, namely questions 21, 25, 26, 16 (see Figure 1 and Table 1). Albart et al., also found lower knowledge results regarding thrombolysis, albeit the high overall knowledge scores [41], underlining the need for urgent, targeted training/education on thrombolysis for HCPs involved in the care of stroke patients.
Regarding the stroke recognition codes, only 24.9% of the respondents in our study stated that the NIHSS was the proposed tool for AIS severity assessment, which probably denotes unfamiliarity with the scale. This finding is in line with the 62% of US ED workers in the study by Lamba et al that reported being unfamiliar with the NIHSS [21] and the 31.25% of prior knowledge of the NIHSS among ED nurses in a rural hospital in Brazil [32]. In stark contrast to that, Reynolds et al. reported high levels of knowledge of NIHSS, amounting to 88.6%, in a sample of 88 nurses which, however, were highly specialized as they were employed in neurocritical care in a US university hospital [31]. Dissemination of material concerning the NIHSS, along with dedicated, focused, and repeated training in NIHSS completion in diverse clinical scenarios (from the comatose to the aphasic stroke patient) is deemed necessary within the Greek-Cypriot EDs.
We herein demonstrated a significant and rather linear association between years of work experience and performance in the stroke knowledge test, which proved to be an independent predictor in multivariate analysis across all groups of work experience, when compared to the <1-year experience. This finding lies in accordance with other studies. Specifically, Harper et al., showed that more years of experience in emergency nursing were correlated with higher knowledge scores [28]. The level of clinical experience among sub-Saharan nurses was the most significant predictor of certain knowledge or skills, such as the choice of the appropriate IV fluid to be administered in stroke patients or the time-window for thrombolysis, as described by Lin et al. [34]. However, this observation has not been consistent across relevant literature. A polish study showed that paramedics with less than 11 years of experience were more well-grounded compared to their experienced colleagues. The finding was attributed to the recent training and the up to date guidelines [43]. Adelman et al. showed, in a large sample of 875 nurses in a single US academic center, no association of clinical experience, expressed in years of employment (<1, 1-3, 4-10, and ≥11), with adequate knowledge on stroke warning signs [30]; one could argue, though, that stroke knowledge was, in this study, rather restrained to only one aspect of stroke, that of early recognition through warning signs, and did not include other measures of stroke awareness, such as thrombolysis issues or patient management following that. A wider stroke knowledge base could possibly have discriminated an experienced from an inexperienced health professional involved in stroke care.
As regards to the contribution of previous stroke education or training on higher stroke knowledge levels, a 2009 study demonstrated that reading relevant literature on stroke and participating in Continued Medical Education (CME) activities, was associated with higher stroke knowledge up to 45% and 15% respectively in US nurses [28]. Having studied, however, relevant material in the preceding year did not provide a benefit to the nurses enrolled in another US study as opposed to participation in CME and being a certified ED nurse [29]. In our study, educational attainment did not affect stroke knowledge levels, but prior education or training did; nevertheless, we did not look more closely into the way different sources of prior exposure to stroke knowledge (self-study; CME; congress workshop etc.) influenced achieved scores. From an organizational point of view, it would be useful to know which interventions aid the most in building confidence in stroke care, so that hospitals provide their ED staff with more targeted educational interventions.
With respect to the difference observed in our study among nurses and physicians, no study, to the best of our knowledge, has investigated this matter to date. The study by Albart et al., compared knowledge of different physician categories and other HCPs, including nurses, without giving though a clear notion on the nurses score [41]. The higher stroke knowledge of physicians versus nurses observed herein should be interpreted with caution and should by no means be generalized, because a significantly lower response rate was noted among Greek-Cypriot ED physicians that were called to participate than among nurses (47.3 vs. 74.1%, respectively); this could be related to a luck of willingness by a significant number of physicians with lower levels of stroke knowledge, to take the test, thus not included in our study, which could have ameliorated the herein reported knowledge differential.
5. Limitations
The present survey aimed to evaluate the knowledge of stroke recognition and management among healthcare professionals in the ED for the first time in Cyprus. However, it's essential to acknowledge certain limitations, primarily related to the sampling methodology and sample size. The issue of the response rate is the first of the limitations of our study. Low response rates obviously reduce the generalizability of our study. Moreover, they most probably cause an overestimation of the reported knowledge levels, since HCPs who refused to participate are most likely insecure about the status of their stroke knowledge. As a result, one could safely assume that the actual knowledge levels are even lower and a greater effort must be employed to improve them. The comparison of the current study’s’ response rates to those from existing literature is challenging for many reasons, including the diversity of types of healthcare professionals included in studied populations and the variety of enrollment methods (online surveys, face-to-face recruitment, questionnaires sent by regular or electronic mail, etc.). A study that included 875 inpatient and ED nurses from a large academic hospital in the US, recruited via an online survey, displayed an overall response rate of 84% [30]. Two studies that enrolled only emergency physicians, one in Saudi Arabia [25] and the other in Australasia [24] both web-based, yielded response rates of only 27% and 13%, respectively. Nevertheless, comparison to the response rate of physicians in our study (47.3%) would likely be unfair, since face-to-face recruitment was applied in our study, an approach expected to be more effective in recruiting study participants. Lastly, in the study by Thomas et al in 1999, invitation to participate was sent by regular mail to nurses in Northeastern England with a response rate 80% [27].
A second limitation would be that private hospitals were rather under-represented in the final sample (15.7% of respondents). The majority, however, of acute ischemic stroke cases in the Republic of Cyprus, are directed by the EMS to the AEDs of public hospitals and are treated there, rendering the rather low representation of private hospitals fair. The refusal of a whole private hospital to participate in the study has, again, probably resulted in a slight overestimation of overall stroke knowledge levels but is expected to have affected the generalizability of the study only minimally.
Lastly, the questionnaire used to assess stroke knowledge was author-developed for the specific study and has not been tested before. However, it demonstrated acceptable internal consistency, with a Cronbach’s alpha coefficient (0.71) almost identical to the one of the questionnaires developed by Thomas et al. (0.7); both questionnaires were developed by a multidisciplinary team of experts and based on current guidelines [27].
6. Conclusions
With the use of a newly developed questionnaire based on current knowledge on the management of patients with acute ischemic stroke, we found that the stroke knowledge levels of AED nurses and physicians in the Republic of Cyprus has significant room for improvement. Prior efforts to augment stroke knowledge in various populations of health professionals involved in stroke care through educational or training interventions have been effective, with post- versus pre- intervention knowledge levels showing clear improvement. Years of work experience do give an advantage, but are timely to gain, and certain aspects of stroke knowledge highlighted herein, such as knowledge on thrombolysis, need to be urgently improved. Dedicated stroke guideline courses should be offered, probably by the Ministry of Health, along with workshops with hands-on training on practical aspects, such as the implementation of scales like the NIHSS in various clinical scenarios. Additionally, hospital and pre-hospital staff involved in stroke care could be subject to yearly examinations with formal stroke knowledge tests. Such interventions should not be on a one-off basis, but repeated at regular intervals, since knowledge and practice guidelines evolve and ED staff is renewed. Finally, it is the entire ED staff that needs to be the target of these interventions, with no discriminations made, since nurses and physicians share on one hand a rather uniformly low stroke knowledge base within the Greek-Cypriot AEDs, and on the other the common responsibility of managing acute stroke patients optimally.
Supplementary Materials
The following supporting information can be downloaded at: www.mdpi.com/xxx/s1, Table S1: Multiple linear regression model predicting stroke knowledge as measured with the 28-item stroke knowledge questionnaire.
Author Contributions
Conceptualization, C.R, N.M., M.K. and M.M.; methodology, C.R., K.M., N.M. M.M.; software, M.K.; validation, C.R., N.M. and M.K.; formal analysis, C.R. and K.M.; investigation, C.R. and N.M.; resources, M.K., E.P. and N.M.; data curation, C.R. and M.K.; writing—original draft preparation, C.R. and M.M.; writing—review and editing, C.R., N.M., M.K., E.P. and M.M.; visualization, C.R. and K.M.; supervision, M.M., N.M., M.K.; project administration, M.M.; funding acquisition, M.M. All authors have read and agreed to the published version of the manuscript.”
Funding
This research was funded by the Cyprus University of Technology (internal funding/research activity 3/319).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Cyprus Bioethics Committee (EEBK/EP/2019.01.74) followed by approval from the Ministry of Health of the Republic of Cyprus (0514/2019).
Informed Consent Statement
The participants provided their written informed consent to participate in this study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
The research team would like to thank all nurses and physicians who participated in this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Patel, A.; Berdunov, V.; King, D.; Quayyum, Z.; Wittenberg, R.; Knapp, M. Current, Future and Avoidable Costs of Stroke in the UK, Executive Summary Part 2. Stroke Assoc. 2017, 12. [Google Scholar]
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics—2020 Update: A Report from the American Heart Association. Circulation 2020, E139–E596. [Google Scholar] [CrossRef] [PubMed]
- Wafa, H.A.; Wolfe, C.D.A.; Emmett, E.; Roth, G.A.; Johnson, C.O.; Wang, Y. Burden of Stroke in Europe: Thirty-Year Projections of Incidence, Prevalence, Deaths, and Disability-Adjusted Life Years. Stroke 2020, 51, 2418–2427. [Google Scholar] [CrossRef] [PubMed]
- He, A.H.; Churilov, L.; Mitchell, P.J.; Dowling, R.J.; Yan, B. Every 15-Min Delay in Recanalization by Intra-Arterial Therapy in Acute Ischemic Stroke Increases Risk of Poor Outcome. Int. J. Stroke 2015, 10, 1062–1067. [Google Scholar] [CrossRef] [PubMed]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke; 2019; Vol. 50; ISBN 0000000000000.
- Jauch, E.C.; Saver, J.L.; Adams, H.P.; Bruno, A.; Connors, J.J.B.; Demaerschalk, B.M.; Khatri, P.; McMullan, P.W.; Qureshi, A.I.; Rosenfield, K.; et al. Guidelines for the Early Management of Patients with Acute Ischemic Stroke: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 2013, 44, 870–947. [Google Scholar] [CrossRef] [PubMed]
- Kleindorfer, D.O.; Towfighi, A.; Chaturvedi, S.; Cockroft, K.M.; Gutierrez, J.; Lombardi-Hill, D.; Kamel, H.; Kernan, W.N.; Kittner, S.J.; Leira, E.C.; et al. 2021 Guideline for the Prevention of Stroke in Patients With Stroke and Transient Ischemic Attack: A Guideline From the American Heart Association/American Stroke Association. Stroke 2021, 52, E364–E467. [Google Scholar] [CrossRef]
- Althubaity, E.; Yunus, F.; Khathaami, A. Al Assessment of the Experience of Saudi Emergency Medical Services Personnel with Acute Stroke. Neurosciences 2013, 18, 40–45. [Google Scholar]
- Li, T.; Munder, S.P.; Chaudhry, A.; Madan, R.; Gribko, M.; Arora, R. Emergency Medical Services Providers’ Knowledge, Practices, and Barriers to Stroke Management. Open Access Emerg. Med. 2019, 11, 297–303. [Google Scholar] [CrossRef]
- Dibiasio, E.L.; Jayaraman, M. V.; Oliver, L.; Paolucci, G.; Clark, M.; Watkins, C.; Delisi, K.; Wilks, A.; Yaghi, S.; Hemendinger, M.; et al. Emergency Medical Systems Education May Improve Knowledge of Pre-Hospital Stroke Triage Protocols. J. Neurointerv. Surg. 2020, 12, 370–373. [Google Scholar] [CrossRef]
- Shire, F.; Kasim, Z.; Alrukn, S.; Khan, M. Stroke Awareness among Dubai Emergency Medical Service Staff and Impact of an Educational Intervention. BMC Res. Notes 2017, 10, 255. [Google Scholar] [CrossRef]
- Gorchs-Molist, M.; Solà-Muñoz, S.; Enjo-Perez, I.; Querol-Gil, M.; Carrera-Giraldo, D.; Nicolàs-Arfelis, J.M.; Jiménez-Fàbrega, F.X.; de la Ossa, N.P. An Online Training Intervention on Prehospital Stroke Codes in Catalonia to Improve the Knowledge, Pre-Notification Compliance and Time Performance of Emergency Medical Services Professionals. Int. J. Environ. Res. Public Health 2020, 17, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Sveikata, L.; Melaika, K.; Wiśniewski, A.; Vilionskis, A.; Petrikonis, K.; Stankevičius, E.; Jurjans, K.; Ekkert, A.; Jatužis, D.; Masiliūnas, R. Interactive Training of the Emergency Medical Services Improved Prehospital Stroke Recognition and Transport Time. Front. Neurol. 2022, 13. [Google Scholar] [CrossRef] [PubMed]
- Prabhakaran, S.; Ward, E.; John, S.; Lopes, D.K.; Chen, M.; Temes, R.E.; Mohammad, Y.; Lee, V.H.; Bleck, T.P. Transfer Delay Is a Major Factor Limiting the Use of Intra-Arterial Treatment in Acute Ischemic Stroke. Stroke 2011, 42, 1626–1630. [Google Scholar] [CrossRef] [PubMed]
- McTaggart, R.A.; Ansari, S.A.; Goyal, M.; Abruzzo, T.A.; Albani, B.; Arthur, A.J.; Alexander, M.J.; Albuquerque, F.C.; Baxter, B.; Bulsara, K.R.; et al. Initial Hospital Management of Patients with Emergent Large Vessel Occlusion (ELVO): Report of the Standards and Guidelines Committee of the Society of NeuroInterventional Surgery. J. Neurointerv. Surg. 2017, 9, 316–323. [Google Scholar] [CrossRef] [PubMed]
- Leong, B.Y.G.; Ni, H.M.J.; Tiah, L.; Tan, C. The Challenge of Tightening Door-to-Needle Timings in a Telestroke Setting: An Emergency Medicine Driven Initiative. Cureus 2020, 12. [Google Scholar] [CrossRef]
- Craig, L.E.; McInnes, E.; Taylor, N.; Grimley, R.; Cadilhac, D.A.; Considine, J.; Middleton, S. Identifying the Barriers and Enablers for a Triage, Treatment, and Transfer Clinical Intervention to Manage Acute Stroke Patients in the Emergency Department: A Systematic Review Using the Theoretical Domains Framework (TDF). Implement. Sci. 2016, 11, 157. [Google Scholar] [CrossRef]
- Baatiema, L.; Otim, M.; Mnatzaganian, G.; Aikins, A.D.G.; Coombes, J.; Somerset, S. Towards Best Practice in Acute Stroke Care in Ghana: A Survey of Hospital Services. BMC Health Serv. Res. 2017, 17, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Bruins Slot, K.; Murray, V.; Boysen, G.; Berge, E. Thrombolytic Treatment for Stroke in the Scandinavian Countries. Acta Neurol. Scand. 2009, 120, 270–276. [Google Scholar] [CrossRef] [PubMed]
- Meurer, W.J.; Majersik, J.J.; Frederiksen, S.M.; Kade, A.M.; Sandretto, A.M.; Scott, P.A. Provider Perceptions of Barriers to the Emergency Use of TPA for Acute Ischemic Stroke: A Qualitative Study. BMC Emerg. Med. 2011, 11, 5. [Google Scholar] [CrossRef]
- Lamba, S.; Murano, T.; Nagurka, R. Emergency Department Healthcare Providers’ Knowledge of Ischemic Stroke. Res. Dev. Med. Educ. 2013, 2, 50–53. [Google Scholar] [CrossRef]
- Williams, J.M.; Jude, M.R.; Levi, C.R. Recombinant Tissue Plasminogen Activator (Rt-PA) Utilisation by Rural Clinicians in Acute Ischaemic Stroke: A Survey of Barriers and Enablers. Aust. J. Rural Health 2013, 21, 262–267. [Google Scholar] [CrossRef]
- Stecksén, A.; Lundman, B.; Eriksson, M.; Glader, E.L.; Asplund, K. Implementing Thrombolytic Guidelines in Stroke Care: Perceived Facilitators and Barriers. Qual. Health Res. 2014, 24, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Grady, A.M.; Bryant, J.; Carey, M.L.; Paul, C.L.; Sanson-Fisher, R.W.; Levi, C.R. Agreement with Evidence for Tissue Plasminogen Activator Use among Emergency Physicians: A Cross-Sectional Survey. BMC Res. Notes 2015, 8, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Al Khathaami, A.M.; Aloraini, H.; Almudlej, S.; Al Issa, H.; Elshammaa, N.; Alsolamy, S. Knowledge and Attitudes of Saudi Emergency Physicians toward T-PA Use in Stroke. Neurol. Res. Int. 2018, 2018. [Google Scholar] [CrossRef]
- Alanazi, A.; Alosaimi, M.; Aldawsari, R.M.; Alatwai, A.M.; Idris, M.A. Saudi Emergency Physicians ’ Knowledge about Recombinant Tissue Plasminogen Activator for Acute Ischemic Stroke. 2019, 10, 49–53. [Google Scholar]
- Thomas, L.H.; Harrington, K.; Rogers, H.; Langhorne, P.; Smith, M.; Bond, S. Development of a Scale to Assess Nurses’ Knowledge of Stroke: A Pilot Study. Clin. Rehabil. 1999, 13, 518–526. [Google Scholar] [CrossRef] [PubMed]
- Harper, J.P. Emergency Nurses’ Knowledge of Evidence-Based Ischemic Stroke Care: A Pilot Study. J. Emerg. Nurs. 2007, 33, 202–207. [Google Scholar] [CrossRef]
- Traynelis, L. Emergency Department Nurses’ Knowledge of Evidence-Based Ischemic Stroke Care. Kaleidoscope 2012, 10. [Google Scholar]
- Adelman, E.E.; Meurer, W.J.; Nance, D.K.; Kocan, M.J.; Maddox, K.E.; Morgenstern, L.B.; Skolarus, L.E. Stroke Awareness among Inpatient Nursing Staff at an Academic Medical Center. Stroke 2014, 45, 271–273. [Google Scholar] [CrossRef]
- Reynolds, S.S.; Murray, L.L.; Mclennon, S.M.; Bakas, T. Implementation of a Stroke Competency Program to Improve Nurses’ Knowledge of and Adherence to Stroke Guidelines. J. Neurosci. Nurs. 2016, 48, 328–335. [Google Scholar] [CrossRef]
- Sbampato dos Santos, J.V.; Aparecida de Melo, E.; Lopes da Silveira Junior, J.; Nascimento Vasconcelos, N.; de Castro Lima, M.; Moreira Damázio, L.C. The Effects of Nursing Training on the Evaluation of Patients With Cerebrovascular Accident. J. Nurs. UFPE / Rev. Enferm. UFPE 2017, 11, 1763–1768. [Google Scholar] [CrossRef]
- Baby, P.; Srijithesh, P.; Ashraf, J.; Kannan, D. Emergency Nurses’ Knowledge about Tissue Plasminogen Activator Therapy and Their Perception about Barriers for Thrombolysis in Acute Stroke Care. Int. J. Noncommunicable Dis. 2019, 4, 121. [Google Scholar] [CrossRef]
- Lin, C.; Vakani, R.; Kussin, P.; Guhwe, M.; Farjat, A.E.; Choudhury, K.; Renner, D.; Oduor, C.; Graffagnino, C. Assessment of Healthcare Personnel Knowledge of Stroke Care at a Large Referral Hospital in Sub-Saharan Africa – A Survey Based Approach. J. Clin. Neurosci. 2017, 42, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Vandenbroucke, J.P.; Von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and Elaboration. PLoS Med. 2007, 4. [Google Scholar] [CrossRef]
- Erdfelder, E.; FAul, F.; Buchner, A.; Lang, A.G. Statistical Power Analyses Using G*Power 3.1: Tests for Correlation and Regression Analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef]
- Jauch, E.C.; Saver, J.L.; Adams, H.P.; Bruno, A.; Connors, J.J.B.; Demaerschalk, B.M.; Khatri, P.; McMullan, P.W.; Qureshi, A.I.; Rosenfield, K.; et al. Guidelines for the Early Management of Patients with Acute Ischemic Stroke: A Guideline for Healthcare Professionals from the American Heart Association / American Stroke Association; 2018; Vol. 44; ISBN 9780309140942.
- Gnatzy, T.; Warth, J.; von der Gracht, H.; Darkow, I.L. Validating an Innovative Real-Time Delphi Approach - A Methodological Comparison between Real-Time and Conventional Delphi Studies. Technol. Forecast. Soc. Change 2011, 78, 1681–1694. [Google Scholar] [CrossRef]
- Sim, J.; Wright, C.C. The Kappa Statistic in Reliability Studies: Use, Interpretation, and Sample Size Requirements. Phys. Ther. 2005, 85, 257–268. [Google Scholar] [CrossRef]
- De Vet, H.C.W.; Terwee, C.B.; Mokkink, L.B.; Knol, D.L. Measurement in Medicine: A Practical Guide. Meas. Med. A Pract. Guid. 2011, 1–338. [Google Scholar] [CrossRef]
- Albart, S.A.; Khan, A.H.K.Y.; Rashid, A.A.; Zaidi, W.A.W.; Bidin, M.Z.; Looi, I.; Hoo, F.K. Knowledge of Acute Stroke Management and the Predictors among Malaysian Healthcare Professionals. PeerJ 2022, 10, e13310. [Google Scholar] [CrossRef]
- Liu, X.; Weng, Y.; Liu, R.; Zhao, J. Significant Stroke Knowledge Deficiencies in Community Physician Improved with Stroke 120. J. Stroke Cerebrovasc. Dis. 2019, 28, 1–6. [Google Scholar] [CrossRef]
- Blek, N.; Szarpak, L. Profile of Practices and Knowledge on Stroke among Polish Emergency Medical Service Staff. Disaster Emerg. Med. J. 2021, 6, 55–62. [Google Scholar] [CrossRef]
Figure 1.
Ranking of questions of stroke knowledge questionnaire according to percentage of participant that answered correctly (N=281).
Figure 1.
Ranking of questions of stroke knowledge questionnaire according to percentage of participant that answered correctly (N=281).
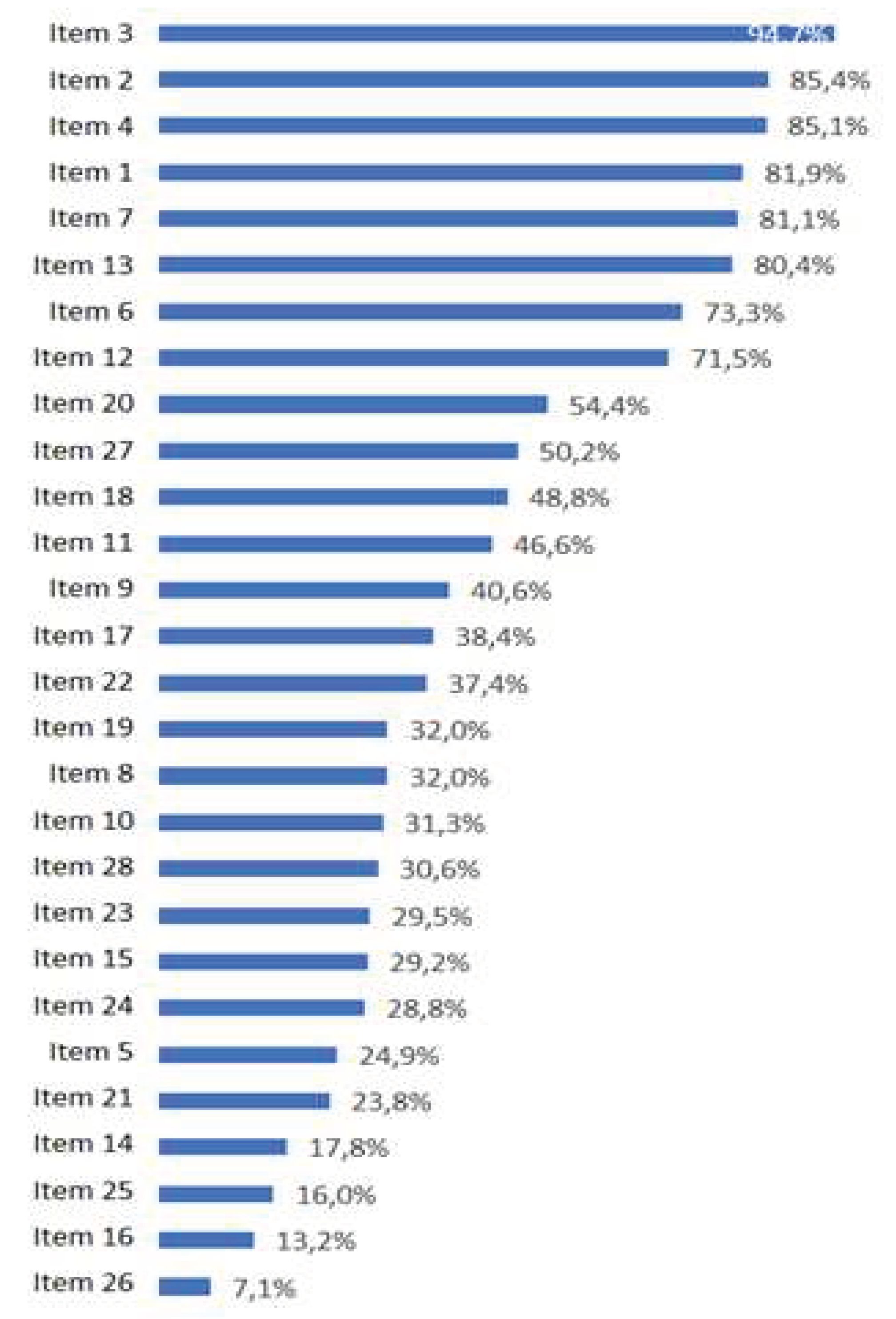

Table 1.
28-item, author-developed questionnaire on stroke knowledge and respective kappa values and agreement percentages (run-in sample, N=15).
Table 1.
28-item, author-developed questionnaire on stroke knowledge and respective kappa values and agreement percentages (run-in sample, N=15).
| Question | Kappa | Agreement percentage |
|---|---|---|
| 1. Every patient presenting with an AIS should be treated as a medical emergency, whether eligible for thrombolysis or not (QGN) | 0.73 | 87% |
| 2. AIS represents a life-threatening situation (QGN) | 0.86 | 93% |
| 3. EDs play a vital role in the early recognition of AIS and the timely commencement of treatment (QGN) | 1.00 | 100% |
| 4. EMS personnel should inform ED about the transfer of a patient with probable AIS (QGN) | 0.33 | 73% |
| 5. NIHSS is the proposed scale for AIS severity assessment (QKSR) | 0.55 | 80% |
| 6. A patient presenting to the ED with AIS is most likely to experience which of the following symptoms? i) tremor, dizziness, vomiting; ii) altered level of consciousness, tachypnea, cyanosis; iii) unilateral arm or leg weakness or face drooping or difficulty speaking; (QKSR) | 0.47 | 80% |
| 7. Which of the following can mimic an AIS? i) Hypoglycemia, ii) hyperkalemia, iii) heat stroke, iv) pulmonary embolism (QKSR) | 0.59 | 87% |
| 8. Brain MRI is the recommended diagnostic modality to differentiate between ischemic and hemorrhagic stroke (QKSR) | 0.48 | 73% |
| 9. In a patient with suspected stroke, clinical examination and history taking can securely differentiate between ischemic and hemorrhagic stroke (QKSR) | 0.21 | 67% |
| 10. 60 minutes is the maximum time allowed from the arrival of the patient at the AED and the commencement of diagnostic examinations (QKSR) | 0.71 | 87% |
| 11. A patient with suspected stroke, regardless of severity and neurological deficit, must be placed in bed, supine (QKSR) | 1.00 | 100% |
| 12. In patients with suspected AIS, blood pressure should be measured on both arms and a finger stick glucose test performed (QKSR) | 0.59 | 80% |
| 13. Hypotension and hypovolemia should be treated before starting thrombolysis (QKSM) | 1.00 | 100% |
| 14. Thrombolysis must be administered to eligible AIS patients within a time-window of 3 hours (QKSM) | 0.57 | 80% |
| 15. Patients aged over 80 years should be excluded from thrombolysis (QKSM) | 0.47 | 80% |
| 16. In an AIS patient about to receive thrombolysis, the maximum acceptable body temperature is: i) 37 °C, ii) 37,5 °C, iii) 38 °C, iv) 38,5 °C (QKSM) | 0.25 | 73% |
| 17. The lowest acceptable blood glucose level for a patient about to receive thrombolysis is 60 mg/dl (QKSM) | 0.86 | 93% |
| 18. If the patient that is about to receive thrombolysis demonstrates an oxygen saturation of <94%, we administer oxygen via nasal cannula and proceed with thrombolysis as planned (QKSM) | 0.66 | 87% |
| 19. What is the recommended dose of rt-PA in an AIS patient? i) 0.9mg/kg, ii) 90mg/kg, iii) 0.6mg/kg; iv) 1.3mg/kg (QKSM) | 0.86 | 93% |
| 20. What is the maximum acceptable blood pressure before administering thrombolysis? i) 200/115mmHg; 230/115mmHg; iii) 215/120mmHg; iv) 185/110mmHg (QKSM) | 0.42 | 87% |
| 21. During the administration of thrombolysis, blood pressure must be measured every 30 minutes (QKSM) | 0.66 | 87% |
| 22. Administration of aspirin is recommended within 24 to 48 hours after thrombolysis (QKSM) | 0.81 | 93% |
| 23. Thrombolysis can be administered to an AIS patient who is receiving a therapeutic dose of heparin (QKSM) | 0.42 | 87% |
| 24. Maximum allowed dose of r-tPA is 40 mg (QKSM) | 0.84 | 93% |
| 25. For thrombolysis to be administered, blood tests, chest x-ray and electrocardiogram must all be completed (QKSM) | 0.81 | 93% |
| 26. After thrombolysis treatment, the patient must be transferred to an ICU for 12 hours (QKSM) | 1.00 | 100% |
| 27. In a patient who has received thrombolysis, vital signs should be taken regularly only during the first 12 hours receiving r-tPA (QKSM) | 1.00 | 100% |
| 28. In a patient with a severe stroke and large-vessel occlusion, thus with an indication for thrombectomy, we immediately administer thrombolysis (if the patient is eligible for that) and thrombectomy follows (QKSM) | 0.86 | 93% |
AIS: Acute Ischemic Stroke; ED: Emergency Department; EMS: Emergency Medical Services; ICU: Intensive Care Unit; NIHSS: National Institutes of Health Stroke Scale; MRI: Magnetic Resonance Imaging; QGN: Question regarding general knowledge on stroke; QKSM: Question regarding knowledge on stroke management; QKSR: Question regarding knowledge on stroke recognition; r-tPA: recombinant-tissue Plasminogen Activator.
Table 2.
Sources of prior education/ training in stroke care among Emergency Departments healthcare professionals (Ν=157*).
Table 2.
Sources of prior education/ training in stroke care among Emergency Departments healthcare professionals (Ν=157*).
| Nurses | Physicians | Total | |
|---|---|---|---|
| Where did you last receive stroke education or training? | Ν (%) | Ν (%) | Ν (%) |
| Self-guided study | 3 (2.2) | 2 (10) | 5 (3.2) |
| Congress/ educational workshop | 49 (35.8) | 8 (40) | 57 (36.3) |
| Class (post-graduate level) | 6 (4.4) | 1 (5) | 7 (4.5) |
| Class (undergraduate level) | 38 (27.7) | 8 (40) | 46 (29.3) |
| Brief presentation on stroke care | 37 (27) | 0 (0) | 37 (23.5) |
| Leaflet/ other printed material | 4 (2.9) | 1 (5) | 5 (3.2) |
| Total | 137 (100) | 20 (100) | 157 (100) |
* Only respondents who stated they had had relevant stroke education/ training in the past were included in this table.
Table 3.
Performance of study participants in the 28-item stroke knowledge questionnaire (N=281)
| Nurses | Physicians | Total | |
|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | |
| Total score | 12.6 (4.1) | 15.7 (4) | 12.9 (4.2) |
| General knowledge on stroke (4 items) | 3.5 (0.9) | 3.7 (0.9) | 3.5 (0.9) |
| Stroke recognition (8 items) | 3.9 (1.6) | 5 (1.5) | 4 (1.6) |
| Stroke treatment (16 items) | 5.2 (2.7) | 7 (2.4) | 5.4 (2.7) |
SD: Standard Deviation.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



