
Submitted:
09 November 2023
Posted:
10 November 2023
You are already at the latest version
Abstract
Diffuse large B-cell lymphoma (DLBCL) is the most common subtype of non-Hodgkin lymphoma and a heterogeneous disease characterized by mature B-cell neoplasms. The standard immunochemotherapy for DLBCL is R-CHOP, which includes rituximab, cyclophosphamide, doxoru-bicin, vincristine, and prednisone. Up to 30-40% of patients with DLBCL either exhibit primary refractory disease to standard treatment or experience relapse after the initial response. A 72-year-old man diagnosed with DLBCL involving chromosomal translocations t(1;22)(q21;q11.2) and t(6;18)(p25;q21) showed primary refractory disease after the fourth cycle of R-CHOP. The patient ultimately experienced cardiac involvement by the lymphoma and received salvage chemotherapy. He passed away about 15 months away after the diagnosis of DLBCL. We conducted fluorescence in situ hybridization (FISH) for further analysis of the chromosomal translocations. The breakpoint of chromosome 1q21 was located at a distance of around 151 Mb from the telomeric end of chromosome 1p. The breakpoint in chromosome 22q11 contains the immunoglobulin lambda locus. Furthermore, the breakpoint of chromosome 6p was in the telomeric region of chromosome 6p21. The breakpoint of chromosome 18q21 contains BCL2. This case report presents the first documented co-occurrence of chromosomal translocations t(1;22)(q21;q11.2) and t(6;18)(p25;q21) in a patient with DLBCL. These chromosomal translocations may indicate a worse clinical outcome.
Keywords:
diffuse large B-cell lymphoma
; fluorescence in situ hybridization
; 1q21
; immunoglobulin lambda
; BCL2
1. Introduction
Non-Hodgkin lymphoma (NHL) is the most common hematological malignancy and diffuse large B-cell lymphoma (DLBCL) is the most frequent subtype of NHL accounting for 30-40%. DLBCL results from the clonal proliferation of a germinal or post-germinal malignant B cell. DLBCL is categorized into two subtypes based on the cell of origin: germinal center B-cell-like (GCB) and activated B-cell-like (ABC). In general, the ABC subtype has a poorer prognosis compared to the GCB subtype. The diagnosis is generally made from the biopsy of the suspicious lymph node. The standard frontline treatment for most patinets with DLBCL remains rituximab and cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP), with or without radiation [1]. However, further classification of treatment for patients with DLBCL based on variants or subgroups is generally not established. The 5-year overall survival (OS) in DLBCL ranges from 79.5% for stage I to 54.7% for stage IV disease, with a median 5-year OS of 64.6%. Despite receiving standard treatment, up to 30-40% of patients with DLBCL either show disease progression during or at the end of treatment (primary refractory) or relapse after the initial response [2]. This is suspected to be due to the classification of DLBCL comprising clinically, pathologically, and biologically heterogeneous tumors [2,3]. Therefore, characterizing primary refractory or relapse patients at the individual level may facilitate the development of effective treatment strategies aimed at improving the overall prognosis of DLBCL.
We are reporting a case of DLBCL coexisting with chromosomal translocations t(1;22)(q21;q11.2) and t(6;18)(p25;q21). This case demonstrated primary refractory disease during R-CHOP treatment and exhibited an aggressive clinical course. We conducted fluorescence in situ hybridization (FISH) analysis to examine the precise chromosomal breakpoints, and as far as our knowledge extends, no similar case has been previously reported.
2. Case Presentation
A 72-year-old man was referred to our hospital with a fever >38°C, fatigue, and elevated lactate dehydrogenase (LDH). His Eastern Cooperative Oncology Group performance status (ECOG PS) was 1. He had a medical history of bladder cancer at the age of 68 years, which was treated with transurethral resection plus intravesical bacillus Calmette-Guerin therapy. 18F-fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) for bladder cancer staging revealed increased 18F-FDG accumulation in the submandibular, subclavian, and intra-abdominal lymph nodes. Because there were no superficial lymph nodes available for biopsy, he was followed up with imaging due to suspicion of low-grade NHL, which had remained stable for about 4 years. In addition, his medical history included chronic atrial fibrillation, reflux esophagitis, and a previous surgery for ossification of the ligamentum flavum. He was prescribed apixaban for atrial fibrillation and rabeprazole sodium for reflux esophagitis. He had no history of familial genetic disorder, smoking, or known allergies to food or medication.
At the time of our hospital referral, physical examination revealed palpable enlarged lymph nodes extending from the left neck to the left submandibular region. Blood analysis showed the following findings: hemoglobin, 145 g/L; white blood cell count, 8.1 × 109/L (93% segmented neutrophils, 7% lymphocytes); platelet count, 331 × 109/L; LDH, 808 U/L (normal range, 124-222 U/L); C-reactive protein, 6.3 mg/L (normal range, 0.0-1.4 mg/L); and soluble interleukin-2 receptor alpha, 2,393 U/mL (normal range, 122-496 U/mL). Hepatitis B surface and core antibodies were positive, but hepatitis B virus DNA was not detected. CT imaging demonstrated a rapid increase in the size of the left cervical lymph nodes, which were compressing his trachea and thyroid (Figure 1A). The paraaortic and mesenteric lymph nodes were also enlarged, but their size remained similar to previous imaging during the follow-up. A needle biopsy of the left cervical lymph nodes was performed, which revealed diffuse infiltration by medium- to large-sized atypical lymphocytes, which disrupted the normal lymph node structure. (Figure 1B). These lymphocytes were found to be positive for CD10, CD20 (Figure 1C), CD79a, MUM1, BCL2, and BCL6, but negative for CD3, CD5, and Epstein-Barr virus-encoded small RNA (EBER). Bone marrow aspiration revealed increased number of abnormal lymphocytes (Figure 1D) which were CD20 positive and cytogenetic abnormalities 46,XY,t(1;22)(q21;q11.2) and t(6;18)(p25;q21) in 20/20 of the metaphases analyzed (Figure 1E). The ratio of kappa and lambda immunoglobulin light chains, determined by flow cytometry in CD45/side scatter gating using the bone marrow cells, was 0.2 (normal range, 0.3-3.0) [4]. The upper endoscopy showed no evidence of lymphoma invasion. The cardiac echocardiogram showed mild mitral regurgitation, moderate pulmonary hypertension, but normal left ventricular systolic function. The electrocardiogram showed atrial fibrillation.
A diagnosis of GCB DLBCL, stage IVB was made [5]. According to the National Comprehensive Cancer Network International Prognostic Index (NCCN-IPI), his NCCN-IPI score was 6, placing him in the high-risk group [6]. The patient received R-CHOP (rituximab 375 mg/m2 on day 1, cyclophosphamide 750 mg/m2 on day 2, doxorubicin 50 mg/m2 on day 2, vincristine 2 mg on day 2, and prednisone 100 mg on days 2-6). Oral fluconazole was administrated for fungal prophylaxis, and oral trimethoprim-sulfamethoxazole was administrated to prevent Pneumocystis jirovecii pneumonia. He experienced a grade 4 neutropenia according to the Common Terminology Criteria for Adverse Events (CTCAE). He received granulocyte-colony stimulating factor and his neutrophil count was recovered. After the third cycle of R-CHOP, CT imaging showed continued lymph node shrinkage. Additionally, the bone marrow aspiration did not detect any apparent abnormal lymphocytes and showed a normal karyotype. However, the left cervical lesion enlarged again after the fourth cycle of R-CHOP. We added radiation therapy (40 Gy/20 Fr) for the enlarged left cervical lesion. The patient received a total of six cycles of R-CHOP.
The patient visited the nearest hospital with the chief complaints of palpitations, dizziness, and loss of consciousness. He was diagnosed with sustained ventricular tachycardia there and subsequently referred to our hospital. Further analysis revealed that the right ventricle of the heart was ultimately invaded by DLBCL, as detected by cardiac echocardiography, CT, and cardiac magnetic resonance imaging. A relapse was confirmed approximately 4 months after completing R-CHOP treatment. The sustained ventricular tachycardia was relieved with landiolol hydrochloride. To address the relapse of DLBCL, he received R-GCD (rituximab 375 mg/m2 on day 8, gemcitabine 1000 mg/m2 on day 1 and 8, carboplatin AUC = 5 on day 1, and dexamethasone 16.5 mg on days 1-4). However, prior to the fourth cycle of R-GCD, blood examinations showed an increase in LDH and soluble interleukin-2 receptor alpha levels, and CT imaging revealed an increase in pericardial fluid. He was considered to have progressive disease after the third cycle of R-GCD and was switched to Pola-RB (rituximab 375 mg/m2 on day 1, polatuzumab vedotin 1.8 mg/m2 on day 2, and bendamustine 90 mg/m2 on day 2-3). Even after the second Pola-RB, his disease continued to progress, and the pericardial fluid remained increased by CT imaging. However, pericardiocentesis was not performed due to the absence of findings indicating cardiac tamponade, based on the consultation with the cardiologist. He subsequently received dose-adjusted EPOCH (etoposide 50 mg/m2 on day 1-4, vincristine 0.4 mg/m2 on day 1-4, doxorubicin 10 mg/m2 on day 1-4, cyclophosphamide 560 mg/m2 on day 5, and prednisone 60 mg on days 1-5). Unfortunately, he passed away on day 6 of the first EPOCH cycle, approximately 5 months after the relapse. The cause of his death was suspected to be a lethal arrhythmia due to the progression of lymphoma.
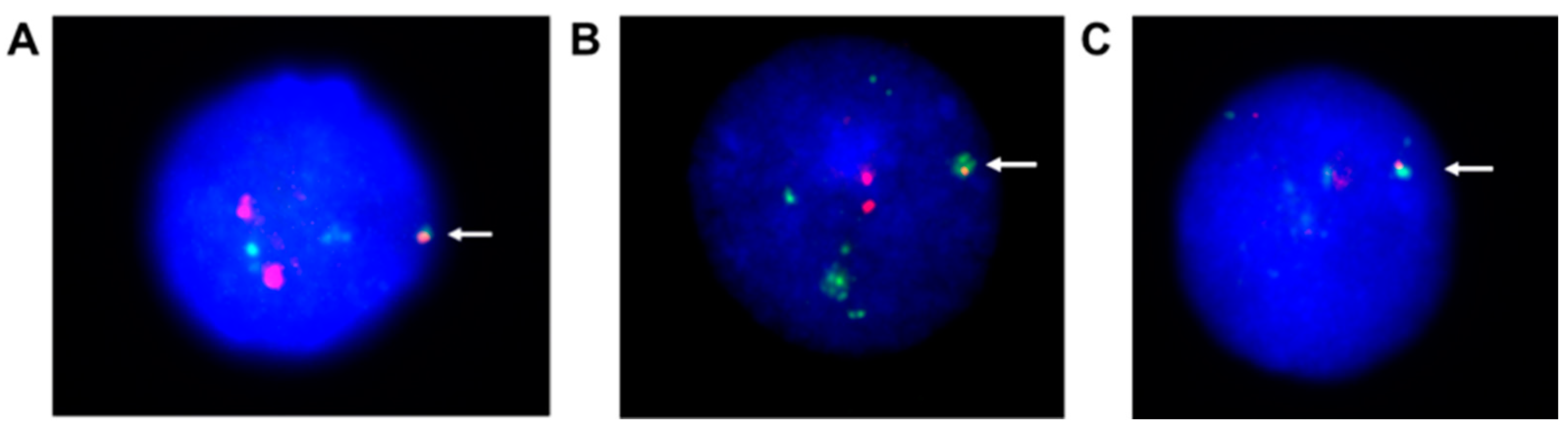
FISH analysis was conducted to examine the precise chromosomal breakpoints using bone marrow samples. The analysis of t(1;22)(q21;q11.2) indicated that the breakpoint of chromosome 1q21 was in a bacterial artificial chromosome (BAC) clone, RP11-316M1, located at a distance of around 151 Mb from the telomeric end of chromosome 1p, whereas the breakpoint in chromosome 22q11 was in BAC clone RP11-165G5, which contains the immunoglobulin lambda (IGL) locus (Figure 2A). Analysis of t(6;18)(p25;q21) indicated that the breakpoint of chromosome 6p was in the telomeric region of chromosome 6p21, whereas that of chromosome 18q21 was in BAC clone RP11-299P2, which contains BCL2 (Figure 2B-C).
3. Discussion
We present a case of chemo-refractory DLBCL who exhibited rare chromosomal translocations 46,XY,t(1;22)(q21;q11.2) and t(6;18)(p25;q21). Transformation of DLBCL from low-grade NHL, like follicular lymphoma (FL), is suspected based on the clinical course. The patient did not respond to standard chemotherapy with R-CHOP, indicating primary refractory disease. Additionally, he exhibited rare cardiac involvement due to lymphoma and experienced an aggressive clinical course, even after receiving salvage chemotherapy regimens. Regrettably, the patient passed away. FISH analysis using bone marrow sample was conducted.
The chromosomal abnormalities in DLBCL vary, and there is no single specific chromosomal abnormality that characterizes all cases of DLBCL. DLBCL is a heterogeneous disease with various subtypes, and there are genetic and chromosomal alterations among individual patients. Nevertheless, some characteristic genetic abnormalities have been reported in subtypes of DLBCL cases, which may impact the prognosis and treatment strategies. These genetic abnormalities include translocations of the BCL2, BCL6, and MYC genes, known as double-hit or triple-hit lymphomas [3].
FISH analysis was performed for further analysis in our case. 18q21 is frequently detected in FL, and its role in the transformation from FL was highly suspected based on the FISH analysis of t(6;18)(p25;q21) [7]. Moreover, the breakpoint of chromosome 1q21 was detected from the analsis of t(1;22)(q21;q11.2). Because numerous genes located on chromosome 1q21 are linked to B-cell lymphoma, including BCL9, MCL1, and IRTA1 [8,9,10,11], a gene on chromosome 1q21 in this patient might be dysregulated due to the IGL translocation. Consequently, the IGL translocation might be associated with the development and progression of lymphoma [12]. In addition, t(6;18) might cause overexpression of BCL2, which is associated with poor prognosis in DLBCL [13]. This might be attributed to a super-enhancer located within the 6p21-25 promoter region. Accordingly, BCL2 positivity might be confirmed through immunohistochemical staining in our case.
The NCCN-IPI is a valuable tool for stratifying prognostically relevant subgroups of DLBCL in the current era of rituximab-based treatment. It considers factors such as age, LDH, ECOG PS, Ann Arbor stage, and the presence of extranodal disease. Based on this assessment, the patient was classified into the high-risk group, with estimated 5-year overall survival (OS) at 33% and 5-year progression-free survival at 30% in the NCCN cohort, which implies a poor prognosis.
This patient with DLBCL, harboring chromosomal translocations 46,XY,t(1;22)(q21;q11.2) and t(6;18)(p25;q21), exhibited primary refractory disease to R-CHOP. Subsequently, salvage chemotherapy was administered at the timing of the relapse after completing 6 cycles of R-CHOP. Unfortunately, he passed away approximately 15 months after being diagnosed with DLBCL. Notably, the NCCN-IPI does not consider chromosomal abnormalities. By incorporating chromosomal abnormalities into the assessment, we may achieve a more precise prognosis and make more effective treatment strategy decisions to improve the prognosis in patients with DLBCL.
Cardiac lymphoma is categorized into primary cardiac lymphoma and secondary cardiac lymphoma. In our case, it was classified as secondary lymphoma due to cardiac involvement observed at the time of relapse. Secondary cardiac involvement due to lymphoma is more common compared to primary cardiac lymphoma and has been reported in up to 25% of patients with nodal disease. The most prevalent form of secondary cardiac involvement occurs in patients with DLBCL. In most cases of secondary cardiac lymphoma, symptoms are attributed to heart failure or rhythm alterations [14], which is similar to our case. While there are no established guidelines for the management of cardiac lymphoma, treatment approaches for cardiac lymphoma involve chemotherapy, often combined with radiotherapy, surgery, autologous hematopoietic stem cell transplantation, and chimeric antigen receptor (CAR) T-cell therapy [15,16]. Unfortunately, in our case of secondary cardiac lymphoma, autologous hematopoietic stem cell transplantation and CAR T-cell therapy were not considered due to the patient’s age and overall general condition.
We selected R-GCD, Pola-RB, and EPOCH as the salvage treatments for this patient. For the patients ineligible for transplantation or CAR T-cell therapy, polatuzumab vedotin in the Pola-RB regimen is an effective treatment in challenging-to-treat settings. It delivers monomethyl auristatin E, a microtubule inhibitor, to B-cells [17]. Regarding EPOCH, which includes doxorubicin, despite its potential for cardiac toxicity, we chose it because the anthracycline dosage did not reach the upper limit. Additionally, his ventricular tachycardia was caused by secondary cardiac lymphoma rather than cardiac toxicity.
There are also some limitations in our case report. First, a definite diagnosis was not made at the age of 68, and he was subsequently followed up as having a low-grade NHL with imaging. Second, due to the insufficient sample volume obtained from the lymph node needle biopsy, the FISH was performed using the bone marrow samples at age of 72 which were used to detect chromosomal translocations. Third, we were not able to identify genes on 1q21 and 6p25 using the available analytical methods.
4. Conclusions
To the best of our knowledge, this is the first case report of DLBCL coexistent with chromosomal translocations t(1;22)(q21;q11.2) and t(6;18)(p25;q21). Our data suggests that these translocations may play a role in the development of refractory DLBCL. To gain a better understanding of the biological and clinical significance of these translocations, it is crucial to accumulate more cases similar to ours to improve prognosis in the future.
5. Materials and Methods
5.1. Cytogenetic analysis by G-Banding
Cytogenetic analysis by G-banding using the bone marrow cells was outsourced to SRL (Tokyo, Japan). The bone marrow cells were cultured after adding phytohemagglutinin (PHA) free culture medium and subjected to G-banding after the specimen preparation. The detailed methodology follows that of Seabright, et al [18].
5.2. FISH
BACs located at 1q21.3 (RP11-316M1), 6p21.31 (RP3-329A5), 6p24.3 (RP11-328K6), 18q21.33 (RP11-299P2), and 22q11.2 (RP11-165G5) were purchased from BAC/PAC Resources (Oakland, CA) and used for FISH probes. DNA from BAC clones were directly labeled by nick translation with Spectrum-Green and/or Spectrum-Red according to the manufacturer’s instructions (Abbott, Abbott Park, IL, USA). Information of BAC clones were obtained via the website of the National Center for Biotechnology Information (NCBI), and the probes were confirmed to map to the precise chromosome bands using metaphase spreads from the peripheral-blood lymphocytes from healthy donors. Chromosome preparation for cytogenetics was performed according to the standard procedure. Briefly, cells were cultured in RPMI 1640 for 24 hours, treated with colcemid (final concentration, 0.05 mg/mL) for 30 minutes, harvested with hypotonic potassium chloride (0.075M KCl), and fixed with methanol/glacial acetic acid (3:1, cornoy solution).
Author Contributions
Conception and design: H.K., Y.K., I.H.; Acquisition of data: H.K., R.T., M.M.; Analysis of data: I.H., Sivasundaram K., M.A., S.T.; Interpretation of data: H.K., Y.K., I.H., A.T., Shinya K., M.M.; Writing-original draft: H.K., Y.K., I.H.; Writing-review and editing: H.K., Y.K., I.H., Sivasundaram K., R.T., M.A., S.T., A.T., Shinya K., M.M.
Funding
This research study was partially supported by the 2023 Japanese Society of Hematology Research Grant (Y.K.).
Institutional Review Board Statement
The study was approved by the institutional review board of Karatsu Red Cross Hospital and Aichi Medical University.
Informed Consent Statement
The patient provided informed consent.
Data Availability Statement
The data used to support the findings of the study are included within the article.
Acknowledgments
We would like to express our gratitude to all of the hospital staff for caring for the patient. We would like to thank Peter Chandler, Cancer Science Institute of Singapore, National University of Singapore, Singapore for the English language review.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Susanibar-Adaniya, S.; Barta, S. K. , 2021 Update on Diffuse large B cell lymphoma: A review of current data and potential applications on risk stratification and management. Am J Hematol 2021, 96, 617–629. [Google Scholar] [CrossRef] [PubMed]
- Duarte, C.; Kamdar, M. , Management Considerations for Patients With Primary Refractory and Early Relapsed Diffuse Large B-Cell Lymphoma. Am Soc Clin Oncol Educ Book 2023, 43, e390802. [Google Scholar] [CrossRef] [PubMed]
- Testoni, M.; Zucca, E.; Young, K. H.; Bertoni, F. , Genetic lesions in diffuse large B-cell lymphomas. Ann Oncol 2015, 26, 1069–1080. [Google Scholar] [CrossRef] [PubMed]
- Marti, G. E.; Rawstron, A. C.; Ghia, P.; Hillmen, P.; Houlston, R. S.; Kay, N.; Schleinitz, T. A.; Caporaso, N.; International Familial, C. L. L. C. , Diagnostic criteria for monoclonal B-cell lymphocytosis. Br J Haematol 2005, 130, 325–332. [Google Scholar] [CrossRef] [PubMed]
- Hans, C. P.; Weisenburger, D. D.; Greiner, T. C.; Gascoyne, R. D.; Delabie, J.; Ott, G.; Muller-Hermelink, H. K.; Campo, E.; Braziel, R. M.; Jaffe, E. S.; Pan, Z.; Farinha, P.; Smith, L. M.; Falini, B.; Banham, A. H.; Rosenwald, A.; Staudt, L. M.; Connors, J. M.; Armitage, J. O.; Chan, W. C. , Confirmation of the molecular classification of diffuse large B-cell lymphoma by immunohistochemistry using a tissue microarray. Blood 2004, 103, 275–282. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.; Sehn, L. H.; Rademaker, A. W.; Gordon, L. I.; Lacasce, A. S.; Crosby-Thompson, A.; Vanderplas, A.; Zelenetz, A. D.; Abel, G. A.; Rodriguez, M. A.; Nademanee, A.; Kaminski, M. S.; Czuczman, M. S.; Millenson, M.; Niland, J.; Gascoyne, R. D.; Connors, J. M.; Friedberg, J. W.; Winter, J. N. , An enhanced International Prognostic Index (NCCN-IPI) for patients with diffuse large B-cell lymphoma treated in the rituximab era. Blood 2014, 123, 837–842. [Google Scholar] [CrossRef] [PubMed]
- Lee, M. S.; Blick, M. B.; Pathak, S.; Trujillo, J. M.; Butler, J. J.; Katz, R. L.; McLaughlin, P.; Hagemeister, F. B.; Velasquez, W. S.; Goodacre, A.; et al. , The gene located at chromosome 18 band q21 is rearranged in uncultured diffuse lymphomas as well as follicular lymphomas. Blood 1987, 70, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Willis, T. G.; Zalcberg, I. R.; Coignet, L. J.; Wlodarska, I.; Stul, M.; Jadayel, D. M.; Bastard, C.; Treleaven, J. G.; Catovsky, D.; Silva, M. L.; Dyer, M. J. , Molecular cloning of translocation t(1;14)(q21;q32) defines a novel gene (BCL9) at chromosome 1q21. Blood 1998, 91, 1873–1881. [Google Scholar] [CrossRef] [PubMed]
- Wenzel, S. S.; Grau, M.; Mavis, C.; Hailfinger, S.; Wolf, A.; Madle, H.; Deeb, G.; Dorken, B.; Thome, M.; Lenz, P.; Dirnhofer, S.; Hernandez-Ilizaliturri, F. J.; Tzankov, A.; Lenz, G. , MCL1 is deregulated in subgroups of diffuse large B-cell lymphoma. Leukemia 2013, 27, 1381–1390. [Google Scholar] [CrossRef] [PubMed]
- Miller, I.; Hatzivassiliou, G.; Cattoretti, G.; Mendelsohn, C.; Dalla-Favera, R. , IRTAs: a new family of immunoglobulinlike receptors differentially expressed in B cells. Blood 2002, 99, 2662–2669. [Google Scholar] [CrossRef] [PubMed]
- Hanamura, I. , Gain/Amplification of Chromosome Arm 1q21 in Multiple Myeloma. Cancers (Basel) 2021, 13, (2). [Google Scholar] [CrossRef] [PubMed]
- Fujimoto, Y.; Nomura, K.; Fukada, S.; Shimizu, D.; Shimura, K.; Matsumoto, Y.; Horiike, S.; Nishida, K.; Shimazaki, C.; Abe, M.; Taniwaki, M. , Immunoglobulin light chain gene translocations in non-Hodgkin’s lymphoma as assessed by fluorescence in situ hybridisation. Eur J Haematol 2008, 80, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Tsuyama, N.; Sakata, S.; Baba, S.; Mishima, Y.; Nishimura, N.; Ueda, K.; Yokoyama, M.; Terui, Y.; Hatake, K.; Kitagawa, M.; Ishizuka, N.; Tomita, N.; Takeuchi, K. , BCL2 expression in DLBCL: reappraisal of immunohistochemistry with new criteria for therapeutic biomarker evaluation. Blood 2017, 130, 489–500. [Google Scholar] [CrossRef] [PubMed]
- Lucchini, E.; Merlo, M.; Ballerini, M.; Porcari, A.; Sinagra, G.; Pagnan, L.; Rensi, M.; Romano, A.; Bussani, R.; Ballotta, L.; Zaja, F. , Case Report: Cardiac Involvement by Lymphoma: Rare but Heterogeneous Condition With Challenging Behaviors. Front Oncol 2021, 11, 665736. [Google Scholar] [CrossRef] [PubMed]
- Yoshihara, M.; Itamura, H.; Fukushima, N.; Itoh, M.; Furukawa, K.; Nagatomo, D.; Kamachi, K.; Kitamura, H.; Shindo, T.; Kubota, Y.; Sueoka, E.; Morita, S.; Ichinohe, T.; Kimura, S. , Therapeutic management in cardiac lymphoma. Leuk Lymphoma 2014, 55, 1215–1217. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Li, Z.; Li, Y.; Zhao, Y.; Shi, M. , Relapsed/refractory diffuse large B cell lymphoma with cardiac involvement: A case report and literature review. Front Oncol 2023, 13, 1091074. [Google Scholar] [CrossRef] [PubMed]
- Arcari, A.; Cavallo, F.; Puccini, B.; Vallisa, D. , New treatment options in elderly patients with Diffuse Large B-cell Lymphoma. Front Oncol 2023, 13, 1214026. [Google Scholar] [CrossRef] [PubMed]
- Seabright, M. , A rapid banding technique for human chromosomes. Lancet 1971, 2, 971–972. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Cervical computed tomography (CT), histology of the lymph nodes and the bone marrow, and the chromosomal analysis at the time of our hospital referral. A) Contrast-enhanced CT showing enlarged lymph nodes in the left neck (arrow). B) Hematoxylin and Eosin staining of the lymph nodes (magnification 40×). C) Immunostaining of the lymph nodes with an anti-CD20 antibody (magnification 20×). D) May-Grünwald Giemsa staining of the bone marrow (magnification 100×). The arrow indicates an atypical lymphocyte. E) G-banded karyotyping revealed t(1;22)(q21;q11.2) and t(6;18)(p25;q21). The arrows indicate translocated chromosomes.
Figure 1.
Cervical computed tomography (CT), histology of the lymph nodes and the bone marrow, and the chromosomal analysis at the time of our hospital referral. A) Contrast-enhanced CT showing enlarged lymph nodes in the left neck (arrow). B) Hematoxylin and Eosin staining of the lymph nodes (magnification 40×). C) Immunostaining of the lymph nodes with an anti-CD20 antibody (magnification 20×). D) May-Grünwald Giemsa staining of the bone marrow (magnification 100×). The arrow indicates an atypical lymphocyte. E) G-banded karyotyping revealed t(1;22)(q21;q11.2) and t(6;18)(p25;q21). The arrows indicate translocated chromosomes.
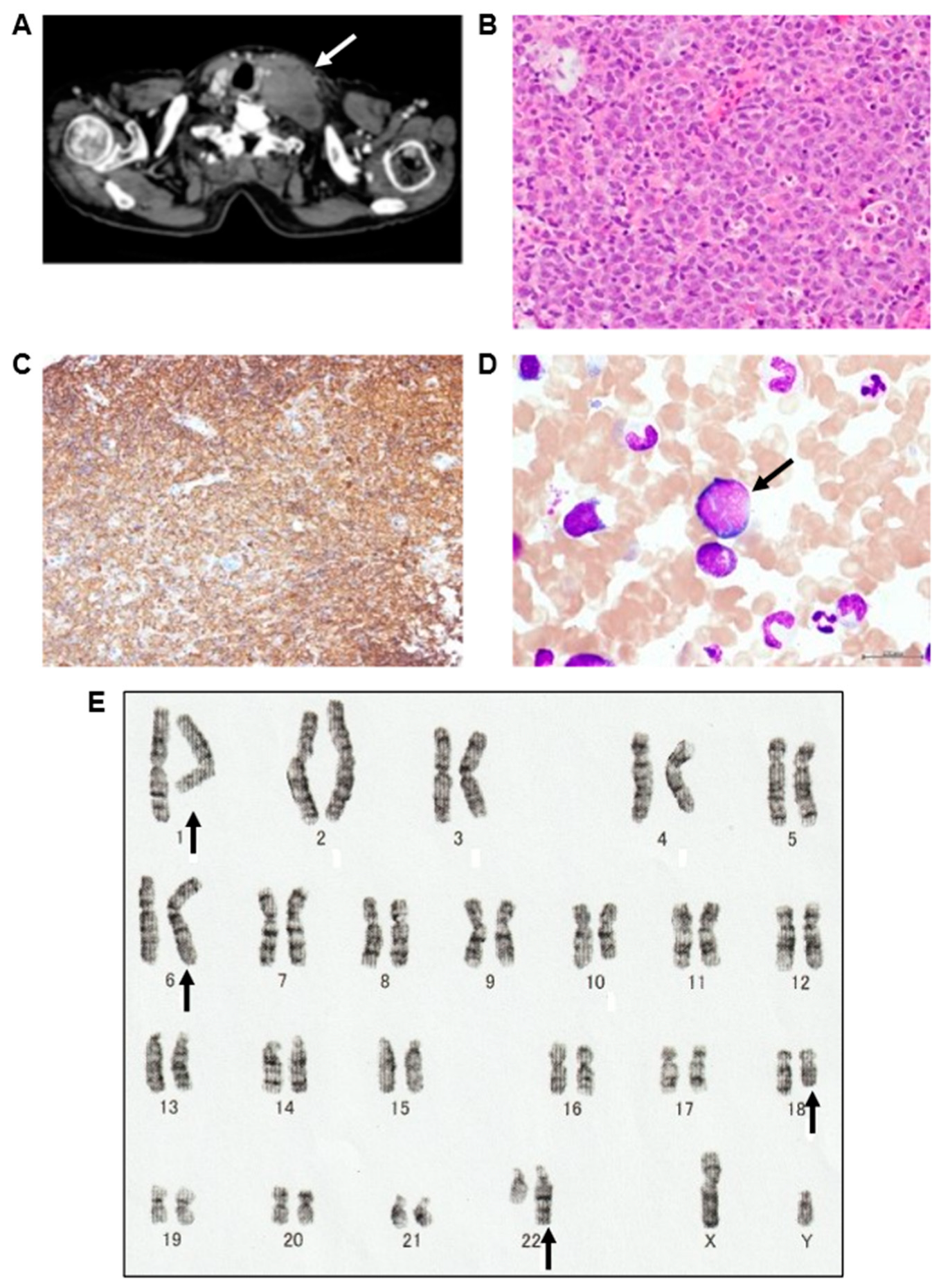
Figure 2.
Fluorescence in situ hybridization (FISH) analysis. A) FISH analysis of BAC clones RP11-316M1 containing chromosome 1q21.3 (red), and RP11-165G5 containing chromosome 22q11.22 (green). The arrow indicates a FISH signal at the position of the original chromosome. B) FISH analysis of BAC clone RP11-328K6 harboring chromosome 6p24.3 (green), and RP11-299P2 containing chromosome 18q21.33 (red). The arrow indicates a FISH signal at the position of the original chromosome. C) FISH analysis of BAC clone RP3-329A5 containing chromosome 6p21.31 (green), and RP11-299P2 containing chromosome 18q21.33 (red). The arrow indicates a FISH signal at the position of the original chromosome.
Figure 2.
Fluorescence in situ hybridization (FISH) analysis. A) FISH analysis of BAC clones RP11-316M1 containing chromosome 1q21.3 (red), and RP11-165G5 containing chromosome 22q11.22 (green). The arrow indicates a FISH signal at the position of the original chromosome. B) FISH analysis of BAC clone RP11-328K6 harboring chromosome 6p24.3 (green), and RP11-299P2 containing chromosome 18q21.33 (red). The arrow indicates a FISH signal at the position of the original chromosome. C) FISH analysis of BAC clone RP3-329A5 containing chromosome 6p21.31 (green), and RP11-299P2 containing chromosome 18q21.33 (red). The arrow indicates a FISH signal at the position of the original chromosome.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



