
Submitted:
08 November 2023
Posted:
08 November 2023
You are already at the latest version
Abstract
Introduction: Outcome measures using telerehabilitation (TR) in the context of post-stroke rehabilitation is an area of emerging research. The current review assesses the literature related to TR for patients requiring post-stroke rehabilitation. The purpose of this study additionally is to survey the outcome measures used in TR studies and to define which parts of the International Organization of Functioning are measured in trials.
Methods: TR studies were searched in Cochrane Central Register of Controlled Trials, PubMed, Embase, Scopus, Google Scholar, and Web of Science from 2016 to June 2023. Two reviewers individually assessed the full text. Disagreements about inclusion or exclusion were determined by consensus or by checking with a third reviewer.
Results: A total of 24 studies were included in the current review. The results were synthesized and reported considering the implications of the results within clinical practice, areas of investigation, and strategic implementation.
Conclusions: The current scoping review recognized a wide range of outcome measures used in TR studies and helped elucidate gaps in the current use of outcome measures in the literature. The scoping review also informs researchers and end users (i.e. clinicians and policymakers) regarding the most suitable outcome measures for TR.
Keywords:
post‐stroke
; dependence variable
; telerehabilitation
; review
; telecare
1. Introduction
The use of innovative technology for the treatment of cognitive and motor impairments in stroke during the critical golden hour is of paramount importance [1]. Recently, the use of telerehabilitation (TR), which we define as the ability to provide assessment and intervention to people who require rehabilitative services via telecommunication, has emerged as a substitute for in-person therapy [2]. Recent studies have shown that TR can positively affect motor functions such as balance, mobility, and postural control [1,3].
TR offers a solution to address some of the accessibility challenges faced by individuals living with stroke [2,4]. A study found that TR interventions for stroke found no change between telehealth and face-to-face interventions for activities of daily living, balance, and upper extremity involvement [5]. Within TR, communication between patients and qualified rehabilitation professionals is facilitated via technologies like telephones and internet-based videoconferencing. Assessing the efficacy of these interventions is crucial to advancing the field of TR [1]. Many tools have been developed to assess both the outcomes of stroke and the efficacy of post-stroke interventions [6].
A study showed that there is a growing need for improvements in stroke care [7]. This study provided strong evidence supporting the effectiveness of both virtual reality (VR) and TR in enhancing stroke care, offering valuable guidance on selecting appropriate outcome measures for assessing the impact of these interventions on stroke survivors and their families [7]. A recent literature review recognized numerous assessment tools utilized in stroke therapy [8]. Another review of outcome measures utilized in randomized controlled trials (RCTs) identified 30 distinct measures documented in RCTs, which gauged the efficacy of interventions in stroke therapy [9]. The adequacy of TR relative to the status quo is confirmed when outcome measures demonstrate no significant decline in performance compared to traditional treatment [5]. Thus, choice of appropriate outcome metric to utilize in research and in clinical practice is imperative.
It is important to note that when selecting outcome measures for clinical observation for patient improvement, the consideration should assess not just impairments in motor function, but also encompass various factors such as the patient’s lifestyle and daily preferences [9]. There are numerous advantages to employing standardized outcome measures, which include the ability to identify patients at risk of experiencing adverse or unfavorable outcomes, determining the most effective interventions tailored to specific contexts, and assessing organizational performance [2]. Clinicians have supported the utilization of standardized tools in therapy for several years. Diana’s work in 2017 emphasized the importance of clear outcome measurements with a focus on TR and VR [10]. However, there remains a lack of consensus regarding the use of outcome measures to enable meaningful comparisons across interventions and studies [4]. This gap in consensus persists from January 2015 until the present day, especially in the context of TR. Considering the COVID-19 pandemic, during which the healthcare industry relied heavily on telerehabilitation interventions, there is a pressing need for establishing a consistent approach in this regard [11].
The current review is the first to our knowledge that seeks to elucidate the outcome measures applied in TR, a field that is rapidly evolving. With the aim of establishing comprehensive guidelines for the utilization of outcome measures in TR, particularly within the realm of stroke rehabilitation, we have conducted a scoping review that systematically synthesizes the prevalent outcome measurement practices. The present study aims to delineate the findings from this scoping review.
2. Methods
The Arksey and O’Malley framework from the University of York was used as guidance for a methodologically rigorous approach to systematically review the outcome metrics utilized to evaluate the efficacy of TR [12]. The York framework has been used broadly in knowledge synthesis trials, and consists of five stages as follows: Stage 1) Classifying the research question; Stage 2) Recognizing relevant studies based on the research question; Stage 3) trial selection; Stage 4) Charting the information within the selected trials; and Stage 5) Organizing, summarizing and reporting the findings of the scoping review. The research questions for the current review were as follows: which outcome measures are used in TR stroke therapy trials and at what time points are they controlled (admission, discharge, and follow-up of the patient) subsequent to a stroke? Which functions from the International Classification of Functioning (ICF) are assessed in the outcome measures?
2.1. Eligibility Criteria
The inclusion criteria for this scoping review consisted of trials: 1) involving stroke patients, 2) recounting a rehabilitation intervention using TR, 3) written in English, and 4) published after January 2015. The exclusion criteria were: 1) papers published in non-English languages, 2) papers not reporting outcome measures, 3) papers only reporting laboratory measures, 4) discussion and protocol papers or commentary and qualitative studies, 5) poster presentations, abstracts, or papers without enough information about the treatment, and 6) papers only reporting the change and development of the technology. The search was completed using study design or date of publication.
2.2. Search Strategy
The literature search was done by a librarian professional in the field of therapy, which included: PubMed Embase, The Cochrane Central Register of Controlled Trials (Cochrane Library), the Cumulative Index to Nursing and Allied Health Literature (CINAHL), and the Physiotherapy Evidence Database (PEDro) (until July 2023) to classify potentially related studies.
2.3. Data Collection Process
Two of the reviewers (MGN and MF) independently investigated the titles and abstracts extracted from the database searches to determine whether they fit the inclusion criteria. Disagreements about the inclusion or exclusion criteria of a specific paper based on the review of its abstract were determined by reaching a consensus or consulting a third reviewer (AS). Data extraction arrangements were established based on the current literature in the field and on the questions of the research. Extraction of the data was based on essential information according to questions of the current review such as a) the study’s authors, b) the year of publication, c) the objective(s) of the trial, d) the design of the trial, e) country, f) outcome measures reported, g) patient characteristics (e.g. age, sex, socio-economic status, level of education, motor functional level, the phase of the stroke, type of the stroke), h) related ICF domains, i) period of time at which the assessment is taken (e.g. admission, discharge, follow-up), j) technology used for TR, and k) details on the TR intervention. The outcome measures were categorized according to the ICF domains [12].
2.4. Critical Appraisal of the Included Articles
The modified Critical Appraisal Skills Programme (CASP) tool [13] was used for assessing the quality of each of the included studies by the three reviewers (MGN, MF, and AS). The CASP tool is an instrument used for evaluating the strengths and limitations of any qualitative research approach [14]. The tool has ten questions that each emphasizes different methodological domains of a qualitative study. The identification of the research questions, the relevance of the methodology (including study design), description of the population and sample size, outcomes, suitability of analysis methodologies, relevance, and clarification of results. Information was obtained from studies achieving scores greater than 50% according to the CASP scoring system.
2.5. Quality Assessment
We used the CASP tools for assessing the quality of studies, primarily case-control studies and clinical trials. The CASP RCT checklist evaluates 11 critical criteria:
- 1)
- Did the study address a clearly focused research question?
- 2)
- Was the assignment of participants to interventions randomized?
- 3)
- Were all participants who entered the study accounted for at its conclusion?
- 4)
- Was blinding appropriately addressed for participants, assessors, and therapists?
- 5)
- Were the study groups similar at the start of the randomized controlled trial?
- 6)
- Apart from the experimental intervention, did each study group receive the same level of care (i.e., were they treated equally)?
- 7)
- Were the effects of intervention reported comprehensively?
- 8)
- Was the precision of the estimate of the intervention or treatment effect reported?
- 9)
- Did the benefits of the experimental intervention outweigh the harms and costs?
- 10)
- Could the results be applied to your local population/in your context?
- 11)
- Would the experimental intervention provide greater value to the people in your care than any of the existing interventions?
The CASP case-control study checklist also includes 11 questions:
- 1)
- Did the study address a clearly focused issue?
- 2)
- Did the authors use an appropriate method to answer their question?
- 3)
- Were the cases recruited appropriately?
- 4)
- Were the controls selected appropriately?
- 5)
- Was the exposure accurately measured to minimize bias?
- 6)
- Aside from the experimental intervention, were the groups treated equally, and did the authors account for the potential confounding factors in the design and/or in their analysis?
- 7)
- How large was the treatment effect?
- 8)
- How precise was the estimate of the treatment effect?
- 9)
- Are the results credible?
- 10)
- Can the results be applied to the local population?
- 11)
- Do the results of this study fit with other available evidence?
Responses to these questions were recorded as ‘‘Yes", “No”, or “Can’t”. In the current review, seven studies were evaluated using the CASP RCT checklist (Table 1).
In addition, when appraising other studies using the CASP case-control study checklist, questions 4 (Were the controls selected appropriately?) and 6 (Aside from the experimental intervention, were the groups treated equally, and did the authors account for the potential confounding factors in the design and/or in their analysis?) were deemed not applicable since the reported trials were uncontrolled trials. Thus, the total number of questions for the latter studies was nine rather than 11. Sixteen out of the 23 trials had scores between 7 and 9 out of 9, with only two studies scoring 7. Six of the included trials had a score between 8 and 9 out of 11, whereas only four studies scored 7.
3. Results
The exploration of the electronic databases recognized 550 manuscripts after duplicate studies were removed. After screening of the titles and abstracts, 136 studies remained. After a full-text review process, 110 articles were excluded, leaving a total of 24 included studies. Reasons for exclusion of studies are depicted in Figure 1. This study was done in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [15].
3.1. Included Studies
The current scoping review encompasses a comprehensive analysis of 24 trials. This review is organized into three key sections: a) essential characteristics of the trials, which includes details about the authors, location, publication year, study design, subject characteristics, type of stroke, TR explanation, and the numerical score of the quality of the studies, b) TR outcome measures used in assessing post-stroke patients, and c) areas of the ICF covered by these outcome measures. The included trials were published between 2015 and 2023, and most of the trials were conducted in the USA and Canada. The most common study designs were quantitative approaches such as RCTs, CTs, case studies with one group and two groups with pre and post-test intervention (Table 1).
3.2. Participant Characteristics
The study participants primarily consisted of males (335) who had experienced various stroke conditions, including ischemic, subacute, and chronic stroke with symptoms such as hemiparesis, aphasia, and other neurological disorders. These individuals were willing and consenting to begin a rehabilitation protocol. All studies provided detailed information on age, gender distribution, and the total number of participants. Two of the studies included a single case study involving post-stroke patients (Table 1). All of the studies used TR intervention and two studies used TR with VR. The TR interventions were provided via various modalities, including video games, an internet-connected computer and laptop, TR application, serious games, and robot-based TR (Table 1)
3.3. Frequently Used Outcome Measures
A total of 20 outcomes were used in the scoping review (15 outcomes in TR studies and five outcomes in TR studies with VR). The most used outcomes were the Fugl–Meyer Assessment of the Recovery of patients with stroke (FMA), balance, and motor function in the upper limb function is mostly outcome in studies. All outcome measures were used pre- and post-protocol based on TR (Table 2).
3.4. ICF, Disability, and Health Domain
The ICF serves as a framework comprising domains or categories, offering valuable guidelines for reporting functioning, performance, and health in clinical assessments. In the current study, none of the trials employed the ICF guidelines for outcome measurement, but encompassing aspects of both upper and lower limb function, structural aspects, and physical activity. The majority of the pooled studies focus on upper limb function (trunk mobility and functional recovery) [16,17,18,19,20,21] and some studies focus on lower limb function (balance and gait) [16,22,23,24,25,26]
4. Discussion
In recent years, TR has emerged as a new technology for treating and rehabilitating stroke patients [26]. In the current review, we have identified more than 20 outcome measures that illustrate a broad range of assessments utilized in trials focused on stroke rehabilitation with interventions provided through TR. Among these measures, the most commonly used was the FMA. FMA is a performance-based deficiency index and is designed to measure motor function, balance, awareness, and joint functioning in stroke patients. It serves multiple purposes, including measuring motor recovery, assessing disease severity, and aiding in treatment planning and evaluation.
In contrast, other studies have employed various other tools to assess a common outcome such as balance [7]. These tools encompass diverse measurements, including gait speed, Barthel Index (BI), Berg Balance Scale (BBS), Stroke Impact Scale (SIS), and quality of life (QOL) metric. Importantly, the FMA has demonstrated outstanding reliability in both inter-rater and intra-rater assessments, exhibits strong construct validity, and is highly responsive to detecting changes in patient’s conditions. The BBS is a reliable tool, but it may not be sensitive enough to detect subtle yet clinically significant changes in balance in individual subjects, particularly those recovering from stroke [15]. It is a relatively inexpensive test and can be used with a wide range of populations, including healthy individuals and patients. It evaluates balance through a comprehensive assessment that encompasses two distinct dimensions, static and dynamic, via a structured questionnaire [28].
Gait analysis is another valuable measurement that was utilized in five of the included studies to meticulously assess details of step and gait speed in stroke patients [29]. In addition, the Stroke Impact Scale (SIS) is a widely used measure due to its reliability, validity, and sensitivity to change [30]. The SIS contains a question to evaluate the patient’s global perception of their percentage of recovery [30]. Another frequently utilized measure that was used in studies is the Barthel Index (BI). However, there is a strong need for greater consistency in methods, content, and scoring across studies, given that the “BI” acronym is associated with various assessment methodologies. For example, some studies have adopted a 10-item scale, scoring on a range of 0 to 100 with 5-point increments [31]. This approach has been used in several multicenter stroke trials, and we call for more uniform application of this tool for stroke trials. Consistency in result reporting will allow for more appropriate pooling of data for literature review and meta-analysis.
In general, all the aforementioned outcome measures aim to capture important changes in patients who are undergoing stroke rehabilitation, whether by TR or more traditional means. Importantly, most studies have highlighted that patient satisfaction plays a pivotal role in their recovery and motivation to continue with rehabilitation to regain function. Surprisingly, only two studies incorporated a thorough assessment of patient satisfaction and motivation, using tools like the Client Satisfaction Scale (CSS) and the Canadian Occupational Performance Measure (COPM). Upon examining the satisfaction levels of patients who underwent TR following a stroke, the results unequivocally indicate that TR can be a highly effective intervention in the realm of rehabilitation.
Our scoping review identified various evaluation questions that pertained to changes in health service utilization, intervention costs, and the utilization of comprehensive assessment tools to gauge aspects of patient safety, comfort, ease of use, and the efficiency-related consequences resulting from interactions with the technology [31]. This scoping review focused on motor functions such as upper-extremity function, balance, and postural control, yielding outcomes similar to those observed in previous research, such as the study conducted in 2017 [7]. Notably, the trial of Tate et al. found a limited number of studies (8.8%) that assessed specific motor, sensory, and other bodily functions [32]. It is worth mentioning that the majority of the studies in the Tate et al. publication predominantly evaluated domains related to mental function [32]. In contrast, our scoping review identified only two studies that used the Mini-Mental State Examination (MMSE). Future studies should prioritize outcome measures that support ICF domains using TR. Adhering to the Canadian Best Practice Recommendations for Stroke Care can comprehensively cover the various aspects of the ICF framework during both the short- and long-term recovery in stroke patients.
5. Conclusions
Our review included RCTs that provided essential information regarding participant demographics, including age and sex, as well as details about the interventions and the specific type of TR employed for rehabilitation. A majority of these studies assessed outcomes related to motor function, consistently reporting improvements in this domain. However, it is important to note that most studies did not include information about the cost implications of the interventions, which could provide valuable insights for healthcare providers, clinicians, patients, and their families when making decisions based on using new technology with TR. Future studies should emphasize measuring the utilization and feasibility of these outcomes within the context of TR while also providing detailed cost-related information. Furthermore, future studies should investigate the standards that guide the selection of outcomes by clinicians and investigators. It is crucial to explore the reasons behind the exclusion of certain outcomes, such as the need to establish new protocols for professionals, ensuring the availability of assessment tools in the same language as the patients, managing the time required for assessments, and addressing equipment-related prerequisites for the utilization of specific tools. Understanding and addressing these factors will contribute to the improvement of outcome selection processes in TR and related research.
References
- Vellata, C.; Belli, S.; Balsamo, F.; Giordano, A.; Colombo, R.; Maggioni, G. Effectiveness of telerehabilitation on motor impairments, non-motor symptoms and compliance in patients with Parkinson's disease: A systematic review. Front Neurol. 2021, 12, 627999. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Zhang, D.; Chen, J.; Tang, K.; Li, X.; Hou, Z. Research hotspots and trends of brain-computer interface technology in stroke: A bibliometric study and visualization analysis. Front Neurol. 2023, 17. [Google Scholar] [CrossRef]
- Shen, J.; Zhang, X.; Lian, Z. Impact of wooden versus nonwooden interior designs on office workers’ cognitive performance. Percept Mot Skills. 2020, 127, 36–51. [Google Scholar] [CrossRef] [PubMed]
- Nakhostin Ansari, N. Bahramnezhad, F.; Anastasio, AT.; Hassanzadeh, G.; Shariat. A.; Telestroke: A Novel Approach for Post-Stroke Rehabilitation. MDPI. 2023. p. 1186.
- Laver, KE.; Adey-Wakeling, Z.; Crotty, M.; Lannin, NA.; George, S.; Sherrington, C. Telerehabilitation services for stroke. Cochrane Database Syst Rev. 2020. [Google Scholar] [CrossRef] [PubMed]
- Scuteri, D.; Mantovani, E.; Tamburin, S.; Sandrini, G.; Corasaniti, MT.; Bagetta., G. Opioids in post-stroke pain: A systematic review and meta-analysis. Front Pharmacol. 2020, 11, 587050. [Google Scholar] [CrossRef] [PubMed]
- Veras, M.; Kairy, D.; Rogante, M.; Giacomozzi., C.; Saraiva., S. Scoping review of outcome measures used in telerehabilitation and virtual reality for post-stroke rehabilitation. J Telemed Telecare. 2017, 23, 567–587. [Google Scholar] [CrossRef]
- Zeng, X.; Zhang, Y.; Kwong, JS.; Zhang, C.; Li., S.; Sun., F. The methodological quality assessment tools for preclinical and clinical studies, systematic review and meta-analysis, and clinical practice guideline: A systematic review. J Evid Based Med. 2015, 8, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Gold, DA. An examination of instrumental activities of daily living assessment in older adults and mild cognitive impairment. J Clin Exp Neuropsychol. 2012, 34, 11–34. [Google Scholar] [CrossRef]
- Diana, C.; Mirela, I.; Sorin, M. Approaches on the relationship between competitive strategies and organizational performance through the Total Quality Management (TQM). Quality-Access to Success. 2017, 8. [Google Scholar]
- Edwards, D.; Kumar, S.; Brinkman, L.; Ferreira, IC.; Esquenazi, A.; Nguyen, T. Telerehabilitation Initiated Early in Post-Stroke Recovery: A Feasibility Study. Neurorehabil Neural Repair. 2023, 37, 131–141. [Google Scholar] [CrossRef]
- Arksey, H.; O'Malley, L. Scoping studies: Towards a methodological framework. Int J Soc Res Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Stucki, G.; Cieza, A.; Ewert, T.; Kostanjsek, N.; Chatterji, TB. Application of the International Classification of Functioning, Disability and Health (ICF) in clinical practice. Disabil Rehabil. 2002, 24, 281–282. [Google Scholar] [CrossRef] [PubMed]
- Long, HA.; French, DP.; Brooks, JM. Optimising the value of the critical appraisal skills programme (CASP) tool for quality appraisal in qualitative evidence synthesis. Res Methods Med Health Sci. 2020, 1, 31–42. [Google Scholar] [CrossRef]
- Tam, WW.; Tang, A.; Woo, B.; Goh, SY. Perception of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement of authors publishing reviews in nursing journals: A cross-sectional online survey. BMJ open. 2019, 9, e026271. [Google Scholar] [CrossRef]
- Anderson, M.; Dexter, B.; Hancock, A.; Hoffman, N.; Kerschke, S.; Hux, K. Implementing Team-Based Post-Stroke Telerehabilitation: A Case Example. Int J Telerehabili. 2022, 14. [Google Scholar] [CrossRef] [PubMed]
- Cramer, SC.; Dodakian, L.; Le, V.; McKenzie, A.; See, J.; Augsburger, R. A feasibility study of expanded home-based telerehabilitation after stroke. Front Neurol. 2021, 11, 611453. [Google Scholar] [CrossRef] [PubMed]
- Marianna, C.; Francesco, A.; Paolo, T.; Loris, P.; Tiziana, M.; Giuseppe, N. Stroke Telerehabilitation in Calabria: A Health Technology Assessment. Front Neurol. 2022.
- Uswatte, G.; Taub, E.; Lum, P.; Brennan, D.; Barman, J.; Bowman, MH. Tele-rehabilitation of upper-extremity hemiparesis after stroke: Proof-of-concept randomized controlled trial of in-home constraint-induced movement therapy. Restor Neurol Neurosci. 2021, 39, 303–318. [Google Scholar] [CrossRef]
- Rozevink, SG.; van der Sluis, CK.; Hijmans, JM. HoMEcare aRm rehabiLItatioN (MERLIN): Preliminary evidence of long term effects of telerehabilitation using an unactuated training device on upper limb function after stroke. J NeuroEng Rehabi. 2021, 18, 1–9. [Google Scholar] [CrossRef]
- Nam, C.; Zhang, B.; Chow, T.; Ye, F.; Huang, Y.; Guo, Z. Home-based self-help telerehabilitation of the upper limb assisted by an electromyography-driven wrist/hand exoneuromusculoskeleton after stroke. J NeuroEng Rehabi. 2021, 18, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Chen, S-C.; Lin, C-H.; Su, S-W.; Chang, Y-T.; Lai, C-H. Feasibility and effect of interactive telerehabilitation on balance in individuals with chronic stroke: A pilot study. J NeuroEng Rehabi. 2021, 18, 1–11. [Google Scholar] [CrossRef]
- Burgos, PI.; Lara, O.; Lavado, A.; Rojas-Sepúlveda, I.; Delgado, C.; Bravo, E. Exergames and telerehabilitation on smartphones to improve balance in stroke patients. Brain Sci. 2020, 10, 773. [Google Scholar] [CrossRef]
- Saywell, NL.; Mudge, S.; Kayes, NM.; Stavric, V. Taylor D. A six-month telerehabilitation programme delivered via readily accessible technology is acceptable to people following stroke: A qualitative study. Physiother. 2023.
- Lee, SJ.; Lee, EC.; Kim, M.; Ko, S-H.; Huh, S.; Choi, W. Feasibility of dance therapy using telerehabilitation on trunk control and balance training in patients with stroke: A pilot study. Med. 2022, 101. [Google Scholar] [CrossRef]
- Salgueiro, C.; Urrútia, G.; Cabanas-Valdés, R. Telerehabilitation for balance rehabilitation in the subacute stage of stroke: A pilot controlled trial. Neurorehabil. 2022, 51, 91–99. [Google Scholar] [CrossRef]
- Anwer, S.; Waris, A.; Gilani, SO.; Iqbal, J.; Shaikh, N.; Pujari, AN. Rehabilitation of upper limb motor impairment in stroke: A narrative review on the prevalence, risk factors, and economic statistics of stroke and state of the art therapies. Health. 2022: MDPI.
- Rossetti, G.; Cazabet, R. Community discovery in dynamic networks: A survey. ACM computing surveys (CSUR). 2018, 51, 1–37. [Google Scholar] [CrossRef]
- Chen, S.; Lach, J.; Lo, B.; Yang, G-Z. Toward pervasive gait analysis with wearable sensors: A systematic review. J Biomed Inform X 2016, 20, 1521–1537. [Google Scholar] [CrossRef]
- Hauer, KA.; Kempen, GI.; Schwenk, M.; Yardley, L.; Beyer, N.; Todd, C. Validity and sensitivity to change of the falls efficacy scales international to assess fear of falling in older adults with and without cognitive impairment. Gerontol. 2011, 57, 462–472. [Google Scholar] [CrossRef] [PubMed]
- Quinn, TJ.; Langhorne, P.; Stott, DJ. Barthel index for stroke trials: Development, properties, and application. Stroke. 2011, 42, 1146–1151. [Google Scholar] [CrossRef] [PubMed]
- Tate, RL.; Godbee, K.; Sigmundsdottir, L. A systematic review of assessment tools for adults used in traumatic brain injury research and their relationship to the ICF. Neurorehabilit. 2013, 32, 729–750. [Google Scholar] [CrossRef]
Figure 1.
PRISMA 2023 flow diagram for the scoping review about TR and stroke as rehabilitation.
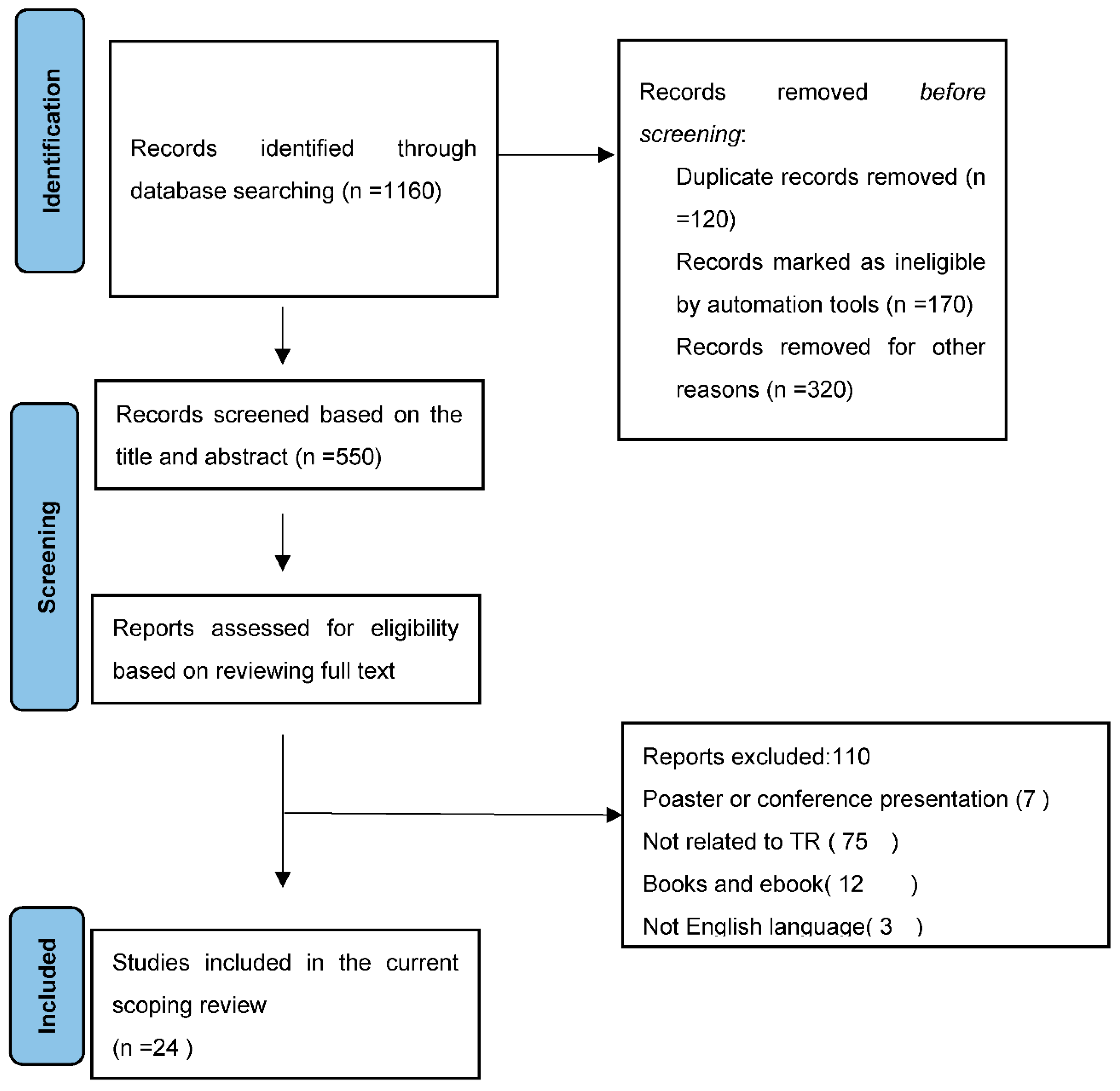

Table 1.
The characteristic of the studies.
| First Author, Year – Country |
Design; Participant’s Age Group; Sex |
Type of Stroke; Phase Of Stroke Rehabilitation |
Type of VR Or TR Brief Description Of The System | CASP |
| Cramer; 2023 – USA | Randomized Clinical Trial; 124 Adult; M=90, F=34, age of 61 |
Stroke with arm motor deficits | TR: intensive arm motor therapy in the clinic (IC), or in the patient’s home using TR to deliver services via an internet-connected computer |
8/11 |
| Toh; 2023 – Hong Kong | Mixed-Methods Study; 11 Adult; M=4, F=7, age≥18 years | Limb telerehabilitation in persons with stroke |
TR: The wearable device, telerehabilitation application | 9/9 |
| Marianna, 2022 – Italy | Clinical Trail study 19 patients M=13F=6 Age: 61.1 ±8.3 years |
Post-stroke patients with a diagnosis of first-ever ischemic (n = 14) or hemorrhagic stroke (n = 5), |
TR: The entire TR intervention was performed (online and offline) using the Virtual Reality Rehabilitation System (VRRS) (Khymeia, Italy). |
9/9 |
| Allegue; 2022 – Canada | Mixed method Case Study; 5 Adult; M=3, F=2 Age: 41-89 |
Stroke Survivors | TR+VR:( VirTele): Virtual Reality Combined With Telerehabilitation |
9/9 |
| Salgueiro; 2022 - Spain | Prospective Controlled Trial; 49 Adult; M=31, F=18, Age: 55-82 | Subjects with a worsening of their stroke symptoms or any of the comorbidities (eg: another neurological disease or orthopaedic problem of the lower limbs) | TR: using AppG | 9/9 |
| Salgueiro; 2022 – Spain | Prospective, Single-Blinded, Randomized Controlled Trial (RCT); 30 Adult; M=20, F=10, being over 18 years of age |
Chronic Stroke Survivors | TR: The practice of specific lumbopelvic stability exercises, known as core-stability exercises (CSE). |
9/11 |
| Anderson; 2022 – USA | Case study design and experimental study , One participants F=1, 37 years old |
Stroke with the etiology was a subarachnoid hemorrhage caused by a ruptured aneurysm at the left middle cerebral artery bifurcation | TR: framework for telerehabilitation and the effects of team-based remote service delivery | 9/9 |
| So Jung Lee; 2022 – Republic Of Korea | Randomized Control Trial (RCT); 17 Adult eligible; 14 participants were finished M=10, F=4, Age: Exprimental group=9 Control group =8 |
patients with subacute or chronic stroke | TR: videoconferencing using Zoom | 8/11 |
| Dawson; 2022 – Canada | Pilot, Single-Blind (Assessor), Randomized Control Trial (RCT); 17 Adult; M=9, F=8, Age:42-75 |
Stroke survival with fluent in written and spoken English and have no severe aphasia | TR: A strategy training rehabilitation approach (tele-CO-OP) | 8/11 |
| Uswatte; 2021 - Birmingham | Randomized clinical trials design 24 Adults ≥1-year post- Age: 48-72 M=13, F=11 |
Upper-extremity hemiparesis after stroke |
TR: using a computer-generated random numbers table, to in-lab or tele-health delivery of CIMT | 8/11 |
| Samantha, 2021 | A randomized controlled. M=8 F=3 Age = 66.0 ± 8.4 |
Upper limb function after stroke. |
TR: Home care arm rehabilitation (MERLIN) is a combination of an unactuated training device using serious games and a telerehabilitation platform in the patient’s home situation. | 9/9 |
| Samantha, 2021 | A randomized controlled. M=8 F=4 Age = 64.8 ± 8.5 |
Upper limb function in chronic stroke. | TR: Home care arm rehabilitation (MERLIN): telerehabilitation using an unactuated device based on serious games improves the upper limb function in chronic stroke. | 8/9 |
| Shih-Ching, 2021 | prospective case-controlled pilot study 30 patients F=6 M=9 Age: 51-68 |
chronic stroke | TR: Three commercially available video games | 9/9 |
| Chingyi, 2021 | A single-group trial 11participants F=6 M=5 Age: 44-66 |
chronic stroke(hemorrhagic/ Ischemic) | TR: A home-based self-help telerehabilitation program assisted by the aforementioned EMG-driven WH-ENMS | 7/9 |
| Marin-Pard, 2021 | Case study and Clinical trail studyOne participantsages =67 years oldM=1 | Chronic stroke With upper extremity hemiparesis | TR: Tele-REINVENT system consists of a laptop computer with all necessary programs preloaded, configured, and displayed in an easy-to-use manner, a pair of EMG sensors with the enclosed acquisition board, and a package of disposable electrodes | 7/9 |
| Cramer; 2021 – USA | Prospective, Single-Group, Therapeutic Feasibility Trial ; 13 Adult; M=9, F=4, median age 61 | Home-Based Telerehabilitation After Stroke |
TR: Patients received 12 weeks of TR therapy, 6 days/week, with a live clinic assessment at the end of week 6 and week 12. Patients were free to call the lab with questions. |
9/9 |
| Kessler; 2021 – Canada | Multiple Baseline Single-Case Experimental Design (SCED); 8 Adult; M=6, F=2 Age: 50-83 |
Stroke survivors |
TR: telerehabilitation occupational performance coaching. |
9/9 |
| Saywell, 2020 | Randomized controlled trial ACTIV: n = 47; control: n = 48 N= 95 participants M=49 F=46 |
Participants had experienced a first-ever hemispheric stroke of hemorrhagic or ischemic origin and were discharged from inpatient, outpatient, or community physiotherapy services to live in their own home | TR: Augmented Community Telerehabilitation Intervention | 9/11 |
| Burgos; 2020 , Chile | Clinincal study 6 participants M=3 F=3 |
Chronic stage: in early subacute stroke (seven weeks of progress). | TR: low-cost telemedicine(Therapist monitoring was done by connecting to the web platform and watching games scores daily at the scheduled session time or afterwards based on therapist availability) | 9/9 |
| Ora; 2020 – Norway | Pilot Randomized Controlled Trial; 30 Adult; M=19, F=11 Age> 18 |
Post-stroke with aphasia | TR: using a portable Fujitsu PC (laptop) with necessary software and material. |
9/11 |
| Huzmeli; 2017 - Turkey | Clinical trials study, 10 Adult; M=6, F=4, Age:45-60 |
Patients with Stroke who were hemiplegic and had sufficient equipment | TR: video communication(, TR was applied by contacting the patients via laptops with a camera and microphone and an internet connection) | 9/9 |
| Ivanova; 2017 – Germany | Clinical Trail study6 participants Age: 51-89 years M=4 F=1 |
Motor Relearning after Stroke (Five patients were in the subacute phase; one patient was considered chronic. All participants showed deficits in the motor activity of the shoulder, arm and hand function) | TR: Haptic Devices for Stroke Rehabilitation and Robot-based telerehabilitation system. | 9/9 |
| Dodakian; 2017 – USA | Clinical tails study 12Adult; M=6, F=6 Age:26-75 |
Patients with chronic hemiparetic stroke | TR: Individualized exercises and games, stroke education. |
9/9 |
| Özgün; 2017– Turkey | A Pilot Study, Study 10Adult; M=6, F=4 Age=44-61 |
Patients with Stroke | TR: giving rehabilitation services with computer-based technologies and communication tool. | 8/9 |
Table 2.
Frequency of used outcome measures in TR intervention studies.
| Study (First Author, Year) | Standardized Outcome | Instrument | Reported Findings | ICF Domain | Focus of the Outcome |
|---|---|---|---|---|---|
| Cramer; 2023 – USA | Upper and lower limb function | Fugel-meyer motor assessment | The findings of this study suggest that telerehabilitation has the potential to substantially increase access to rehabilitation therapy on a large scale. |
b730 | Suboptimal rehabilitation therapy doses |
| Toh; 2023 – Hong Kong | Usability of the wristwatch | the System Usability Scale (SUS) questionnaire | The results demonstrated that the usability of the proposed wristwatch and telerehabilitation system was rated highly by the participants |
S730 | Upper limb |
| Marianna, 2022 – Italy | Motor recovery | Barthel Index (BI);Fugl-Meyer motor score (FM) and Motricity Index (MI) |
The results demonstrate the TR tool promotes motor and functional recovery in post-stroke patients. |
b730 | Upper limb |
| Allegue; 2022 – Canada | Improvement of UE motor function |
Berg Balance Assessment: Functional Gait Assessment: Activity-specific Balance Confidence Scale ndependently performs |
The results show most survivors of stroke found the technology easy to use and useful. | b730 | Arm feasibility |
| Salgueiro; 2022 – Spain | Balance in sitting position | The Spanish-version of the Trunk Impairment Scale 2.0 (S-TIS 2.0),Function in Sitting Test (S-FIST), Berg Balance Scale (BBS), Spanish-version of Postural Assessment for Stroke Patients (S-PASS), Brunel Balance Assessment (BBA)Gait assessment |
The results show greater improvement in balance in both sitting and standing position. |
b730 | Feasibility of core stability exercises |
| Salgueiro; 2022 – Spain | Balance and gait | Spanish-Trunk Impairment Scale (S-TIS 2.0) Sitting Test Spanish-Postural Assessment Scale |
The results show improvement trunk function and sitting balance. |
b730 | Trunk control, balance, and gait |
| So Jung Lee; 2022 – Republic Of Korea | Trunk control and balance function the functional movement and locomotion necessary for sitting, standing, and walking dependent walker ADLs Health-related QoL |
the Trunk Impairment Scale (TIS) scores the Berg Balance Scale (BBS), Timed Up and Go (TUG) test, Functional Ambulation Categories (FAC), Korean Modified Barthel Index (K-MBI) scores EuroQoL 5 Dimension (EQ-5D) tool. |
The results show significant improvement in the TIS scores. | b730 | Subacute or chronic stroke |
| Dawson; 2022 – Canada | Self-identified in everyday life activities and mood | the Canadian Occupational Performance Measure (COPM) The PHQ-9 |
The results show high satisfaction and engagement. | b730 | Improvements in social participation |
| Uswatte; 2021 - Birmingham | The outcome is the motor capacity | built-in sensors and video cameras Participant Opinion Survey (POS)1 the Motor Activity Log (MAL) The Wolf Motor Function Test (WMFT) |
The results show large improvements in everyday use of the more-affected arm. |
S730 | The focus is on Upper-extremity hemiparesis |
| Samantha, 2021 | Improvement of the upper limb motor ability quality of life, user satisfaction and motivation. |
Wolf Motor Function Test (WMFT), arm function tests, The EuroQoL-5D-5L (EQ-5D) The Intrinsic Motiva- tion Inventory (IMI), System Usability Scale (SUS) and Dutch-Quebec User |
The WMFT, ARAT, and EQ-5D did not show significant differences 6 months after the training period when compared to directly after training. However, the FMA-UE results were significantly better at 6 months than at baseline. | S730 | Upper limb |
| Samantha, 2021 | Limb motor ability Quality of life |
Wolf Motor Function Test (WMFT), Action Research Arm Test (ARAT), Assessment-Upper Extremity (FMA-UE), EuroQoL-5D (EQ-5D). |
The results show progress in monitored game settings, user satisfaction and motivation. | S730 | Upper limb |
| Shih-Ching, 2021 | functional mobility, balance, and fall risk, the degree of perceived efficacy, classifying the strength in each of three lower extremity muscle actions (hip f , Gait |
Berg Balance Scale (BBS) scores. the Timed Up and Go (TUG) test, Modifed Falls Efcacy Scale, Motricity Index, Functional Ambulation Category |
The results show improvement in balance. | b730 | Balance |
| Chingyi, 2021 | the upper limb assessment, the upper limb voluntary function, the functional ability and motion speed of the upper limb, the basic quality of participant’s ADLs, spasticity |
The Fugl–Meyer Assessment (FMA),Action Research Arm Test (ARAT), Wolf Motor Function Test (WMFT), Motor Functional Independence Measure (FIM), Modifed Ashworth Scale (MAS |
The results show improvements in the entire upper limb. | S730 | Upper limb |
| Marin-Pard, 2021 | EMG Signal Processing | Biofeedback, modular electromyography (EMG) |
The results show development of a muscle-computer interface. | S730 | Upper limb Function |
| Cramer; 2021 – USA | Upper and lower lime function | Fugel-meyer motor assessment | The results show assessments spanning numerous dimensions of stroke outcomes were successfully implemented. |
b730 | Limb weakness |
| Kessler; 2021 – Canada | Satisfaction of using telerehabilitation the Client Satisfaction Scale (CSS) |
the Client Satisfaction Scale (CSS) the Canadian Occupational Performance Measure (COPM) |
The results show high satisfaction and a strong therapeutic relationship. | b730 | Occupational performance coaching |
| Saywell, 2020 | physical function , Hand grip strength and Balance , Self-efficacy. , Health outcomes |
The physical subcomponent of the Stroke Impact Scale), A JAMAR hand-held dyna-mometer, The Stroke Self-Efficacy Questionnaire (SSEQ) , The overall stroke recovery rating of the SIS3.0 |
The findings of this trial showed that rehabilitation augmented using readily accessible technology. |
b730 | Physical function |
| Burgos; 2020 , Chile | Balance and functional independence user experience | BBS and Mini-BESTest (MBT) , The Barthel Index (BI), The System Usability Scale (SUS) |
The results demonstrate that a complementary low-cost telemedicine approach is feasible, and that it can significantly improve the balance of stroke patients. |
b730 | Dosage and overall treatment |
| Ora; 2020 – Norway | Feasibility and acceptability of speech and language therapy | The videoconference software called Cisco Jabber/Acano | The results show tolerable technical fault rates with high satisfaction among patients. | b730 | Post-stroke aphasia |
| Ivanova; 2017 – Germany | Motor relearning collection of instant feedback visualizations, incorporating Telerehabilitation, Arm motor gains , Depression , Pain, Speed |
collection of instant feedback visualizations , | The results show tele system for stroke rehabilitation using haptic therapeutic devices is currently being implemented into full functionality. | b730 | Stroke patients in recovering voluntary motor movement capability |
| Dodakian; 2017 – USA | incorporating telerehabilitation , arm motor gains , Depression Pain , Speed |
vital signs, magnetic resonance imaging, FM Scale, Box and Blocks (B&B), NIHSS, Barthel Index, Geriatric Depression Scale (GDS) question form, Mini- Status Exam (MMSE), Optimization in Primary and Secondary Control Scale (adapted from Mackay et al20), The Medical Outcomes Study Social Support Survey, Mental Adjustment to Stroke Scale (Fighting Spirit subscore), Stroke-Specific Quality of Life Scale, Modified functional reach forward displacement (cm) Shoulder pain Gait velocity stroke self-efficacy questionnaire |
The results support the feasibility and utility of a home-based system to effectively deliver telerehabilitation. | b730 | Hemiparetic stroke |
| Özgün; 2017– Turkey | cognitive levels balance quality of life |
the Mini Mental State Examination, the Berg Balance Scale, the Short Form- 36 (SF-36) Quality of Life Scale |
The results show the improvement of using TR programs. | b730 | TR in patients with hemiplegia |
1Participant Opinion Survey.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



