Submitted:
01 November 2023
Posted:
03 November 2023
You are already at the latest version
Abstract
A partial or complete pulpotomy is a type of vital pulp therapy (VPT) that aims to remove the in-flamed, infected pulp, leaving behind healthy, vital pulp that is capable of healing. VPT has gained renewed popularity as a treatment option in permanent mature posterior teeth with irre-versible/moderate-severe pulpitis, its high success rates matching that of root canal treatment (RCT). There is currently no consensus regarding diagnostic and prognostic predictors of success of pulpotomies for managing such cases. Therefore, we conducted a scoping review to identify and analyze how these factors affect the outcome of treatment. A literature search using the PRISMA guidelines was undertaken using PubMed and Scopus on July 7, 2023. A total of 22 studies met the inclusion criteria and were qualitatively analyzed by two reviewers. The follow-ing diagnostic and prognostic factors were recognized and discussed; presenting signs and symptoms, periapical diagnosis, bleeding time, indicators of inflammation (bleeding time, con-centration of inflammatory biomarkers), patient age and medical status, the depth, activity and location of caries, and restorative factors. Based on the studies assessed, there is limited evidence to support their prognostic value. Further research is necessary to identify solid predictors of outcome.
Keywords:
vital pulp therapy
; irreversible pulpitis
; pulpotomy
; deep caries
; carious pulp exposure
; pulpal diagnostics
1. Introduction
Irreversible pulpitis, associated with lingering and moderate to severe dental pain, is one of the most prevalent presenting conditions for an emergency visit to a dental facility [1,2,3]. Often, the appointment time scheduled for emergency patients is shorter than that for a planned visit. Yet, the treatment still needs to be performed efficiently and effectively to manage pain and, in some cases, prevent infection and possible subsequent spread of infection [4]. Such emergency treatment may be temporary, particularly when root canal treatment (RCT) is planned. It is associated with inherent difficulty to accurately diagnose the pulpal status [5]. Where the pulp is still partially viable, a pulpotomy can provide a time saving, feasible and conservative treatment [5].
Traditionally, pulpitis has been referred to as reversible or irreversible [6], an entity which is diagnosed based on presenting signs, symptoms and responses to various diagnostic tests. The American Association of Endodontists (AAE) Glossary of Endodontic Terms lists symptomatic irreversible pulpitis as “lingering thermal pain, spontaneous pain, referred pain” [7]. Typically, symptomatic irreversible pulpitis is characterized by a painful lingering and exaggerated response to hot and/or cold stimuli that can be reproduced with pulp sensibility tests and/or spontaneous, radiating pain that may sometimes disturb the patient’s sleep or worsen in a supine position [8,9,10]. Currently, in the literature, there is high heterogeneity as to what signs and symptoms lead to a diagnosis of irreversible pulpitis. Furthermore, the value of current diagnostic tests is debatable as they do not always reflect the true histological condition of the pulp [11,12,13]. Histologically, irreversible pulpitis is characterized by micro-abscess formation, localized pulpal necrosis and often the presence of bacteria within the pulp [14,15].
In the past decade, dentistry has seen a paradigm shift towards minimally invasive procedures and objectives, including the preservation of the vitality of the pulp [16,17]. To this end, vital pulp therapy (VPT) comprises a range of procedures that aims to preserve the vitality and function of the pulp after injury [18]. VPT includes indirect and direct pulp capping (IPC and DPC, respectively), as well as partial and complete pulpotomy [18]. A partial pulpotomy generally involves the removal of 2-3 mm of the exposed pulp, whereas a coronal or complete pulpotomy involves the removal of the entire coronal pulp to the level of the orifice(s) or cementoenamel junction (CEJ). The terminology ‘irreversible pulpitis’ has historically dictated RCT as the preferred treatment option, with the other alternative being tooth extraction. These options are substantiated by a dated understanding of the pathophysiology of pulpitis referred to as the ‘pulp strangulation theory’, whereby the entire pulp is considered incapable of healing [19]. There is clear scientific evidence against the pulp strangulation theory [20]. Furthermore, a histological study revealed that inflammation is limited to the coronal pulp in teeth with symptoms of irreversible pulpitis, with the radicular pulp free from bacterial invasion and inflammation [13].
Historically, partial pulpotomies were performed for immature teeth with caries or traumatic pulp exposure [21,22]. In contemporary literature, pulpotomy is recognized as an effective and highly successful treatment option for permanent mature teeth with symptoms of irreversible pulpitis [5,23,24]. Additionally, it has been shown to have better and more predictable outcome than IPC and DPC [25]. This has highlighted the need for updated definitions to categorize the various “stages” of pulpitis.
It appears that the AAE classification is the most widely used system for classifying pulpitis on a global scale. Pulpitis is therein defined as reversible or irreversible, and further into symptomatic or asymptomatic irreversible pulpitis [6]. Similarly, the European Society of Endodontology (ESE) considers spontaneous, radiating pain that lingers after the removal of the stimulus, to be indicative of partial or total irreversible pulpitis [26]. However, these current classifications over-simplify the complex and dynamic nature of pulpitis. For example, it has been shown that the clinical diagnosis of irreversible pulpitis only matched the histological diagnosis in 84% of cases [13]. As early as 2013, Asgary and Eghbal introduced the term “partial irreversible pulpitis” which better recognizes that pulp necrosis is frequently contained to the coronal pulp [27]. In 2017, Wolters and colleagues [28] introduced a new classification system into initial, mild, moderate or severe pulpitis, which recommended a corresponding VPT treatment for each diagnosis (Table 1).
A prospective clinical study conducted by Careddu and Duncan [24] explored the connection between the diagnosis of pulpitis according to the AAE and the proposed Wolters diagnosis. The results showed that there was a strong correlation between mild and reversible pulpitis, while moderate and severe pulpitis were highly associated with irreversible pulpitis. This review paper will use the Wolters “moderate-severe pulpitis” and “irreversible pulpitis” synonymously for painful conditions with vital pulps. The S3 Guidelines recommend defining pulpitis as spontaneous or nonspontaneous, while acknowledging no new classification consensus has been reached [29]. The moderate-severe pulpitis terminology better conveys that this condition can be successfully treated by pulpotomy, something supported by the findings of this paper.
RCT enjoys high success rates, particularly in vital pulps without periapical radiolucency (PARL) [30,31,32]. However, molar RCT is expensive, technique-sensitive and time-consuming, as it often requires multiple appointments. One advantage of a partial or complete pulpotomy is that it can be completed in a single appointment, which includes the placement of a definitive restoration [33,34]. The procedure is also less technically difficult, with fewer iatrogenic complications possible, less costly, and less time-consuming to perform than RCT [5,35]. Thus, it may be particularly suited to public health dentistry and for general dentists who have limited appointment times for emergency patients, as it is an extremely appealing option. Furthermore, some randomized controlled trials that have compared postoperative pain after RCT or pulpotomy have shown that pulpotomy results in lower postoperative pain in the short-term [10,36]. This may occur because of the rapid decrease in tissue pressure and the reduction of inflammatory mediators after VPT, along with the ablation of the sensitized nociceptive nerve endings [37]. In addition, pulpotomy preserves other neural functions of the dental pulp dentin complex, including maintenance of the immune defense mechanisms [38,39]. Finally, it is well documented that pulp chamber pulpotomy is an effective treatment for moderate - severe pulpitis, which may have success rates that are similar or even superior compared to those that are reported for RCT; Asgary reported an overall success of 98% for RCT versus 99% for CEM or MTA pulpotomy at 2 years, and Beaquis found pulpotomy had higher success than RCT (77% and 67%, respectively) [9,40]. It is important to note that both studies found no significant difference in overall success between the two treatment arms. This has been further highlighted in a systematic review and meta-analysis highlighting that there is no difference in postoperative pain or success between treatment modalities [41].
Despite the benefits of pulpotomy over RCT, and the high success rates reported in the literature, this treatment option has not yet been widely adopted by general and specialist dental practitioners for the management of moderate - severe pulpitis in permanent mature posterior teeth [9,42]. This may be in part due to conflicting information in the literature concerning the clinical protocol that should be adhered to for VPT. In addition, there is confusion regarding diagnostic factors and prognostic predictors for the success of a partial or complete pulpotomy in cases with moderate-severe pulpitis. In this study, diagnostic factors were those that helped inform about pulpitis, and prognostic factors were those that influenced pulpotomy outcome. A database literature search was conducted based on a defined search criterion to explore the diagnostic and prognostic factors that impact the outcome of partial or complete pulpotomy in permanent mature premolars and molars (posterior teeth) with moderate-severe pulpitis. This review also highlights the differences and shortcomings in current clinical studies to identify the knowledge gaps.
2. Materials and Methods
This scoping review was conducted according to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines for Scoping Reviews Checklist [43]. It was registered with the OSF Registries (registration DOI https://doi.org/10.17605/OSF.IO/4FNBU). A literature search was conducted on PubMed and Scopus on 7th July 2023 using the following search strategy:
“Irreversible pulpitis” OR “moderate pulpitis” OR “moderate inflammat*” OR “severe pulpitis” OR “severe inflammat*” OR “acute pulpitis” OR “pulpal inflammat*”
AND
“Vital pulp therapy” OR VPT OR Pulpotomy OR “Vital pulp treatment”
AND
(((Permanent OR adult) AND (teeth OR tooth OR molar* OR dentition OR premolar*)) OR "Dentition, Permanent"[Mesh])
AND
Success OR Retention OR Vitality OR Outcome OR Pain OR Survival
The Scopus search differed in that the MeSH (Medical Subject Headings) term was omitted. Additionally, relevant literature was hand-searched and PubMed and Scopus were screened monthly. Appropriate papers were then subjectively added.
All study types were included: reviews, meta-analyses, systematic reviews, and clinical studies. Papers were excluded if they were not written in English or were not on human teeth in vivo. Only papers that reported on partial and/or complete pulpotomies on permanent mature (complete root development) posterior teeth with symptoms of irreversible pulpitis (moderate-severe pulpitis) were included in the qualitative analysis. For papers that included immature and mature teeth, reversible and irreversible pulpitis, and anterior and posterior teeth, authors were contacted for the raw data to differentiate the variables. However, only one author [8] provided such information.
Using the online software Covidence, 211 studies were imported for screening (102 from PubMed and 109 from Scopus). After the removal of duplicates (91 studies), 120 studies were screened from their title and abstract by two reviewers (H.M. and P.W.), of which 60 studies were excluded. A total of 60 studies had their full texts read by the two reviewers, and the papers were assessed using a Microsoft Word table documenting the variables. Twenty-two papers met the inclusion criteria, and 38 studies were excluded for various reasons as agreed by the two reviewers (Figure 1). If there was a conflict in the inclusion/exclusion of a paper, the reviewers met in person to discuss the reasoning and a mutual decision was made.
3. Results
A qualitative analysis of the included papers was undertaken. The included clinical studies are presented in Table 2. Particular emphasis was placed on the diagnostic and prognostic factors of age, medical status exclusions, the periapical and pulpal diagnoses, the time to the definitive restoration placement, pulp capping material and markers of inflammation; bleeding time, hemostasis protocol and other markers mentioned.
The criteria used to determine success in each study were evaluated. Outcomes reported included post-operative pain, presentation of apical tissues, presence of sinus tracts or swellings. Details for respective outcomes are reported in Table 2.
Sample sizes, number of participants that were followed-up and the drop-out rate were also listed. The analysis defined follow-up numbers and drop-out rates as inclusive of any teeth that failed up to the review period because these patients were reviewed ahead of time, out of necessity. The drop-out rate was the number of patients who did not attend for review, as a percentage of sample size. Furthermore, when pulpotomy was compared with RCT, these parameters were documented specifically for the pulpotomy group only in Table 2, excluding the 2015 paper by Asgary et al. [5]. For this article, the overall numbers for RCT and VPT were recorded due to limited information provided in the paper.
Exclusion criteria for not performing a pulpotomy in each study were also reported in Table 2. However, standard exclusion criteria across the studies included a tooth that had no response to pulp sensibility testing, pathologic/abnormal probing depths and mobility indicative of periodontal disease, was unrestorable, or with evidence of internal or external root resorption, or root canal calcification.
3.1. Diagnostic Factors Examined
3.1.1. Presenting Signs and Symptoms
As mentioned, this review paper adopted Wolters' proposed classification for pulpitis severity, which is highly correlated with irreversible pulpitis as defined by the AAE [24]. Seven papers specifically defined irreversible pulpitis according to the AAE definition [7], yet in the inclusion criteria none of these studies used this definition as verbatim [24,25,44,45,46,47,48]. One study used the 2019 ESE definition [49]. Another paper compared the Wolters’ classification with the AAE classification of pulpitis [24]. In this paper, one minor deviation from Wolters’ classification was in the patient assessment section for mild pulpitis. Wolters’ definition specifies a stimulated pain duration of up to 20 seconds, but pain duration was not mentioned in the categorization of study participants. Rather, it was stated that pain was triggered by cold or percussion. The remainder of the studies used a modified or individualized definition of irreversible pulpitis. However, based on the descriptions provided, it appears that there are no major differences in the definitions.
Few studies analyzed the impact of pre-operative pain severity on pulpotomy prognosis. Anta et al. [50] found that treatment outcomes were not affected by pre-operative pain severity (moderate and severe), but no scale or descriptors were used to define these. In contrast, Careddu and Duncan [24] revealed that mild pulpitis had a significantly better outcome than severe pulpitis when a partial pulpotomy was performed. Yet, there was no significant difference in outcome between mild and moderate pulpitis. A systematic review found that there was no difference in the success of pulpotomy between symptomatic and asymptomatic irreversible pulpitis, suggesting that lack of pain is not a prognostic factor [25].
3.1.2. Periapical Diagnosis
Ørstavik developed the periapical index (PAI) to grade the appearance of the periapical region on a conventional periapical radiograph [51]. Clinicians and researchers use this classification to categorize periapical health or disease, as well as to recognize healing. Eight studies utilized the PAI scoring system to identify the pre-operative periapical diagnosis and/or the outcome of pulpotomy [40,45,46,47,48,50,52,53,54]. One study included teeth with and without PARL as defined by the PAI score but did not provide the number of cases in each classification [53]. Many studies excluded teeth with radiographic evidence of apical periodontitis but failed to mention the presence or absence of tenderness to percussion or palpation, therefore failing to accurately diagnose the periapical condition [35,49,55].
Multiple studies showed that the presence of apical periodontitis, whether radiographic or clinical, does not have a statistically significant impact on the outcome [5,24,45,53]. Two studies included cases with a pre-operative PAI scores of 3 [40,45]. Anta et al. [50] was the only study included in the review that found that the pre-operative periapical condition affected the outcome. They concluded that the success of complete pulpotomy with Biodentine was significantly higher for cases with a pre-operative PAI score of 1 compared to those with a score of 2, yet this study was underpowered to reliably assess this statistically, and there was a significantly skewed distribution of cases towards a PAI score of 1. Yet, most authors consider a PAI score of 1 and 2 to be healthy [51,56,57]. Furthermore, the study by Kumar et al. [58] considered widening of the periodontal ligament (PDL) to be a treatment failure. Whilst restorative factors certainly may have played a role in the low success rate (see Section 4.1.8), the strict criteria for success also likely contributed.
3.1.3. Inflammation; Bleeding Time and Biomarkers
The bleeding time has been suggested to be an indicator of the extent of inflammation in the pulp, and therefore a diagnostic factor of pulpitis. Some of the studies did not mention the time to achieve hemostasis [5,27,40]. Kumar et al. [58] excluded cases where bleeding couldn’t be controlled after “several” minutes but the specific time period was also not quantified. The majority of the studies restricted hemostasis time to 10 minutes and performed pulpectomy if bleeding exceeded this [8,10,35,44,47,49,52,53]. One study did not include a limit for the time to achieve hemostasis and showed a range for bleeding stoppage of 3-25 minutes for children’s teeth with complete root maturation (mean 7 minutes). The one tooth that failed had a bleeding time of 7 minutes, while teeth, which bled for 25, 15, 14 and 12 minutes succeeded. They found that the bleeding time did not affect success [45].
Regarding pulpotomy outcome, few studies statistically analyzed whether bleeding time was a prognostic factor. Anta et al. [50] limited the time to hemostasis to 5 minutes but found that the bleeding stoppage time did not influence the outcome of treatment. Aldeen et al. [34] limited bleeding time to 6 minutes and observed that all failures occurred in the 4–6-minute bleeding time category, but this was not statistically significant. According to Baranwal's findings, achieving hemostasis typically required 8-10 minutes in the majority of cases. However, statistical analysis was not conducted on this particular factor [53]. Careddu and Duncan [24] similarly found that bleeding time was not a prognostic factor for the success of partial pulpotomy, regardless of the severity of pulpitis. Only one of the included studies mentioned the appearance of the pulp or bleeding severity that was observed intra-operatively [8]. A vital pulp was judged by the appearance of bright red blood that was overflowing from the exposure site.
One study examined the concentration of an inflammatory biomarker: matrix metalloproteinase-9 (MMP-9) [47]. Its concentration is known to be elevated during pulpal inflammation. No correlation was found between the bleeding time and MMP-9 concentration. This study did, however, find that the concentration of MMP-9 was highly correlated with the outcome of complete MTA pulpotomy.
3.2. Prognostic Factors Examined
3.2.1. Patient Age
The age range of the patients in the 22 included studies was 9 to 78 years old. Most of the studies did not include any patients over the age of 60, with the distribution skewed towards a younger age group in the 20–30 year range. Most papers did not conduct statistical analysis on age and treatment outcome correlation, with the majority only providing the distribution within the study groups, age range and/or mean. One study, Asgary et al. [5], grouped the patient’s age at the time of treatment into < 20 years old, 21-29 years old, and ≥ 30 years old and found that the age did not significantly affect the outcome of complete pulpotomy. It is important to note that this study had a bias towards a younger demographic. One included study found that age significantly affected the outcome of treatment [50]. Their results showed that patients in the younger age group (20-25 years) had significantly better outcomes for complete pulpotomy than for the other age groups included (26-30, 31-35, 36-40 and >40 years old). However, the study was underpowered with only 52 patients followed up at 12 months, which is lower than what the power analysis determined (68 patients) due to a 21% drop-out rate. The power calculation in this study also used an uncommon margin of error of 10%, leading to a greater spread of acceptable sample size values. Furthermore, there is a severely skewed distribution of pulpotomies that were performed in the 20–25 year age group.
3.2.2. Medical Status
The medical status of the patients included in the studies was highly heterogeneous. Asgary’s papers excluded any patients with active systemic disease, physical or mental disability, though these parameters were not defined [5,27,59]. Some papers only included patients who had a non-contributory medical history, though this was also not defined [45,48]. While other papers failed to mention the medical status altogether [24,34,49,53]. Most papers mentioned only including healthy patients [35,40,46,47,50,52]. Kumar et al. [58] more specifically excluded patients with systemic disease, opioid or steroid therapy or who were taking antibiotics. Uesrichai et al. [8] included patients categorized as an American Society of Anesthesiologists (ASA) Class I or II. No papers statistically analyzed or discussed how a medical condition or medication affected the outcome of treatment.
3.2.3. Caries Depth, Activity and Location
The ESE defines deep caries as caries that reaches the inner quarter of dentine, with a zone of hard/firm dentine that can be seen radiographically between the radiolucent lesion and the pulp. Extremely deep caries penetrates the entire thickness of the dentine, being continuous with the pulp space radiographically [26]. Aldeen et al. [34] designed their study to determine how the activity level/speed of progression (determined by the color and surface texture after removal of peripheral caries) and depth (deep or extremely deep) of caries affected the outcome of partial pulpotomy with MTA. They found that the degree of caries activity did not significantly affect the outcome. However, 4/24 rapidly progressing lesions failed, while no failures were seen in the 12 lesions with slow progression. Similarly, no significant differences were observed for caries depth, with 3/16 extremely deep lesions failures and only 1/20 failures in the deep caries group. Two studies assessed the location of caries (occlusal versus proximal) and found that it was not a prognostic factor [49,50].
Multiple studies excluded teeth that were necrotic or "partially necrotic"" on exposure, defined as non-bleeding or insufficient bleeding, respectively [8,34,45,46,48,50,52,53,55,60]. Other studies excluded teeth that had no pulp exposure after caries removal, yet the teeth had signs and symptoms of moderate-severe pulpitis [8,24,45,46,48,49,52,53,59,60]. One study also found that there was no difference in outcome if the pulp exposure was carious or mechanically created in order to perform the pulpotomy [50].
3.2.4. Restorative Factors
Opinions differ in the literature regarding whether a definitive restoration should be placed during the same appointment as the pulpotomy, or if the tooth should be temporarily filled and restored at a subsequent appointment. In one study, the entire cavity was restored with Biodentine, then 2-3 mm were removed 1-week post-pulpotomy and a composite resin (CR) was placed [24]. All 4 patients who failed to return for the CR filling later attended an emergency appointment. Each patient presented with dislodged Biodentine, causing symptoms that required root canal treatment. Asgary and Ehsani [59] placed permanent restorations during the same visit, but in subsequent papers, Asgary recommends postponing the placement of a final restoration (7 days post-pulpotomy) [5,27]. None of the included studies evaluated how specifically the quality of restoration affected the outcome of treatment.
The time elapsed between the pulpotomy, and placement of a definitive restoration was also considered to be a prognostic factor. The majority of studies placed the definitive restoration in the same appointment (immediately) as the pulpotomy [8,10,34,35,47,48,49,54,55,59]. The rest of the studies placed the definitive restoration within 1 week [5,24,27,45,46,50,53,58,60], except for two studies which placed it at 2 weeks post-pulpotomy [44,52].

Table 2.
Characteristics of the included studies.
| Author, Year | Sample Size (SS), Follow-up (F/U), Drop-out (D/O) |
Partial or Complete Pulpotomy Type (PP, CP, respectively), Material(s) Used |
Age (Yrs), Time to Rest’n | Other Exclusions |
Pulpitis Diagnosis, Periapical Diagnosis |
Inflammation: Bleeding Time (mins), Agent, Other Indicators | Definition of Success Including Radiographic Appearance. P/O Pain. Success Rate & Recall Period |
Diagnostic/Prognostic Factors Examined for Success (Statistical Significance Indicated by P < 0.05) |
|---|---|---|---|---|---|---|---|---|
| Airsang [44] 2022 | SS: 60 F/U: 53 D/O: 12% |
CP NeoMTA or Biodentine |
=26) 2 weeks |
No pulp exposure, no significant medical history | AAE Glossary definition; exaggerated and prolonged response to EPT and cold. No AP including PDL widening. |
Limit < 10 mins 2.5% NaOCl |
Not well-defined. Asymptomatic, no TTP, swelling, fistulae, sinus tract, integrity of rest’n, ERR, IRR, furcal or periapical pathosis. P/O pain not reported. Success: 86% 12 months (materials combined). |
Pulp capping material (P > 0.05) |
| Aldeen [34] 2023 | SS: 40 F/U: 36 D/O: 10% |
PPMTA | 18-25 Immediate |
Partially necrotic | Spontaneous pain or pain exacerbated by cold stimuli lasting for a few seconds to several hours (lingering) compared to controls. No prominent PARL. |
Limit ≤ 6 mins 2.5% NaOCl |
Response to cold WNL, no abnormal mobility, fistulae, PARL, IRR or ERR. P/O pain not reported. Success: 88.9% 12 months. |
Caries depth and activity, bleeding time (P > 0.05) |
| Anta [50] 2022 | SS: 66 F/U: 52 D/O: 21% |
CP Biodentine |
=26 ± 8) 1 week |
Not in “good general health” | Spontaneous, nocturnal and provoked and exacerbated by hot and cold foods and/or radiating pain. Responded positively to cold and EPT. PAI 1 or 2 included. |
Limit ≤ 5 mins Saline |
Asymptomatic, non-mobile, no TTP, defective rest’n, sinus tract, IRR or ERR. PAI 1 or 2 with no increase in PAI score. P/O pain not reported. Success: 87% 12 months. |
Age and PAI score (P < 0.05). Location of caries, mechanical or carious pulp exposure, pre-operative pain (moderate or severe), bleeding time, pre-operative tenderness to percussion and treatment time (P > 0.05) |
| Asgary [27] 2013 | SS: 413 F/U: 346 D/O: 16% |
CP CEM or MTA |
=27 ± 8.5) 1 week |
Active systemic disease, physical or mental disability, or pregnant or nursing | Spontaneous pain for a few seconds to several hours with extensive caries, pain exacerbated by hot or cold fluids and/or radiating pain. With/without periapical involvement. |
No limit Saline |
Asymptomatic, no abscess, swelling, sinus tract, redness or tenderness. Modified Strindberg criteria for radiographic success P/O pain: no significant difference in pain intensity after MTA or CEM CP (recorded every 24 hours for 7 days) Success: 93.9% 12 months |
Pulp capping material (P > 0.05) |
| Asgary [5] 2015 | SS: 407 F/U: 271 D/O: 33% |
CP (compared with RCT) CEM or MTA |
9-65 1 week |
Active systemic disease, physical or mental disability | Spontaneous pain or pain exacerbated with hot and cold stimuli that lasts for a few seconds to several hours (lingering) compared to control teeth. With/without periapical involvement. |
No limit Saline |
Asymptomatic, no abscess, swelling, sinus tract, redness or tenderness. Modified Strindberg criteria for radiographic success. P/O pain: reported in an earlier report [61]. Success: 71.3% 5 years. |
Pulp capping material, age, pre-operative PARL, outcome compared with RCT (P > 0.05) |
| Asgary [59] 2009 | SS: 12 F/U: 12 D/O: 0% |
CP NEC |
14-62 Immediate |
Medical contraindication | Moderate to severe pain, history of lingering pain. Periapical status not mentioned. |
5 mins Saline |
No mobility, no TTP, asymptomatic, normal periodontium radiographically. P/O pain not reported. Success: 92% (μ 15.8 months). |
Not mentioned |
| Baranwal [53] 2022 | SS: 61 F/U: 54 D/O: 11% |
PP or CP Biodentine |
18-40 1 week |
No pulp exposure, partial necrosis on exposure | With/without spontaneous sharp or dull pain, lingering pain with hot or cold. With/without periapical involvement defined by PAI. |
Limit ≤ 10 mins 3% NaOCl |
Absence of S&S, no ERR, IRR, furcal or new periapical pathosis. Resolved or reduced size of PARL. P/O pain not reported. Success: 80.7% (PP), 92.8% (CP) 12 months. |
Pre-operative PARL, CP or PP outcome (P > 0.05) |
| Beauquis [40] 2022 | SS: 44 F/U: 35 D/O: 20% |
CP (compared with RCT)Biodentine |
=34.8) Immediate (or within 4 weeks) |
Systemic conditions | Spontaneous, radiating pain that lingers after removal of cold stimulus. PAI 1, 2 or 3 included. |
Limit not quantified Saline |
Absence of S&S, no ERR, IRR or furcal bone loss. PAI 1 or 2, maintenance of PAI 3 or drop in score if pre-operative PAI > 3. P/O pain: no difference in reduction of pain at any time period (24 hrs & 7 days) between RCT & CP. Success: 76% 12 months. |
Outcome compared with RCT (P > 0.05) |
| Careddu [24] 2021 | SS: 51 F/U: 41 D/O: 20% |
PP Biodentine |
14-60 1 week |
No pulp exposure | Wolter’s classification and AAE classification. Absence/presence of TTP; radiographic appearance not mentioned. |
Limit ≤ 6 mins 2.5% NaOCl |
Responsive, non-lingering to cold testing, asymptomatic, no TTP, no PARL. Also considered unresponsive but successful as a sub-category. P/O pain: whilst P/O was generally absent at 24 hours, at 7 days >50% of pts reported increased sensitivity to cold that gradually subsided within 3 months. Success: 90% overall for PP; 88% for moderate & 60% for severe pulpitis 12 months. |
Mild pulpitis had a better outcome than severe (p<0.05). TTP, bleeding time, RP or IP, moderate or mild pulpitis (P > 0.05) |
| Elmas [45] 2023 | SS: 25 F/U: 25 D/O: 0% |
CP MTA |
=10.8) 3 days |
Contributory medical history, no pulp exposure, necrotic or partially necrotic on exposure | AAE Glossary definition; spontaneous pain or pain exacerbated by cold stimuli lasting for much longer than control teeth. PAI 1, 2, 3 or 4 included. |
No limit (range 3-25 mins) Saline |
No pain, TTP, sinus tract, swelling, IRR or ERR. No new furcal pathosis or PARL, reduction in PAI score. P/O pain: at 2 days, 64.6% of cases had complete pain relief, 31.2% scored 2/8 & 4.2% scored 4/8. No pts took analgesics in this period. Success: 96% 12 months. |
PAI score, bleeding time (P > 0.05) |
| Hussain [55] 2022 | SS: 20 F/U: 17 D/O: 15% |
CP MTA |
25-55 Immediate |
Contributory medical history, necrotic or partially necrotic on exposure | Exaggerated response with cold & heat lingering for >15 seconds. No PARL. |
Limit ≤5 mins Saline |
No history of spontaneous pain (except 1 week P/O), TTP, tenderness to palpation, swelling, ERR, IRR or PARL. Functional and responsive to EPT. P/O pain: at 2 days, all cases reported complete relief of pain and no pts had required analgesics. Success: 94% 12 months. |
Not mentioned |
| Jassal [52] 2022 | SS: 50 F/U: 49 D/O: 2% |
PP or CP Biodentine |
=24.8 ± 5) 2 weeks |
Not medically healthy, no pulp exposure, necrotic or partially necrotic on exposure | Spontaneous pain, heightened or lingering response to thermal or EPT, nocturnal pain. Normal apical tissues (PAI 1, nil TTP). |
Limit ≤ 10 mins 2.5% NaOCl |
No spontaneous pain or discomfort, heightened response to hot/cold, TTP or tenderness to palpation. P/O pain: no difference in pain reduction at any time periods between CP & CP (24 hrs, 48 hrs & 1 week), analgesic use was low. Success: 88% (PP), 91.6% (CP) 12 months. |
PP or CP outcome (P > 0.05) |
| Kumar [58] 2016 | SS: 54 F/U: 48 D/O: 11% |
CPPRF, MTA or CaOH | 14-32 24 hours |
Systemic disease, opioids or steroid therapy, taking antibiotics | Spontaneous, lingering pain exacerbated by hot and cold fluids and/or radiating pain. No periapical involvement. |
“Several minutes” (not quantified) Saline |
No abscess, swelling, sinus tract or tenderness. Modified Strindberg criteria for radiographic success (success had normal lamina dura. Widened PDL was considered a failure). P/O pain: no difference between the materials at 24 hrs or 7 days. Success: 37.5% for CaOH, 44.4% for MTA & 35.7% for PRF 12 months. |
Pulp capping material (P > 0.05) |
| R [49] 2021 | SS: 80 F/U: 80 D/O: 0% |
CP MTA |
16-35 Immediate |
Extremely deep caries | ESE definition; episodes of spontaneous, radiating pain that lingered after removal of stimulus. No PARL. |
Limit ≤ 10 mins 2.5% NaOCl |
No history of spontaneous pain, swelling or discomfort on chewing. Functional, PAI ≤ 2 , no IRR. P/O pain not reported. Success: 94% 12 months. |
Location of caries (occlusal versus proximal) (P > 0.05) |
| Ramani [46] 2022 | SS: 93 F/U: 88 D/O: 5% |
PP or CP MTA |
=23.3 ± 4.9) 1 week |
Systemically healthy, analgesic intake in the past week, antibiotics in the past month, partial necrosis on exposure | AAE Glossary definition; history of spontaneous pain or lingering pain that could be reproduced by cold testing. Normal apical tissues (PAI ≤2, nil TTP). |
Limit ≤ 6 mins 3% NaOCl |
Absence of S&S, no TTP, PAI <3, no furcal involvement, IRR or ERR P/O pain: 97.7% of pts reported pain at 24 hrs, none reported moderate-severe pain at day 7. In the CP group, analgesics were needed by fewer pts & mean consumption was also less than for PP (P < 0.05). Success: 97.7% PP, 98.8% CP 12 months. |
PP or CP outcome (P > 0.05) |
| Sánchez-Lara y Tajonar [35] 2022 | SS: 41 F/U: 41 D/O: 0% |
CP MTA |
=24.6 ± 15.8) Immediate |
Mild or moderate pain (<7 out of 10) except when there was deep caries, pathologic medically compromised | Spontaneous pain or pain exacerbated by thermal stimuli lasting for a few secs to several hours (lingering compared to control). No PARL. |
Limit ≤ 10 mins 2.5% NaOCl |
No persistent or spontaneous pain, no TTP, tenderness to palpation, sinus tract, discoloration, swelling, abnormal mobility or PDs. No PARL, furcal pathosis, IRR or ERR. P/O pain: 78.8% of pts had no pain at 24 hrs, at 7 days 97.5% had no pain. Pt satisfaction recorded (97.5% satisfied at 24 hrs). Success: 97.6% 12 months. |
Not mentioned |
| Sharma [47] 2021 | SS: 40 F/U: 40 D/O: 0% |
CP MTA |
=25.3 ± 6.2) Immediate |
Systemically unhealthy, history of taking long-acting NSAIDs in the past week | AAE Glossary definition of symptomatic irreversible pulpitis. Normal apical tissues (PAI ≤2). |
Limit ≤ 10 mins 2.5% NaOCl |
No S&S, IRR, ERR or furcal pathosis. PAI <3. P/O pain not reported. Success: 88% 12 months. |
Concentration of MMP-9 levels on treatment outcome and pre-treatment diagnosis (P < 0.05), bleeding time and MMP-9 concentration (P>0.05) |
| Taha [48] 2018 | SS: 64 F/U: 60 D/O: 6% |
CP Biodentine |
=33.2) Immediate or 2 weeks later |
Contributory medical history, no pulp exposure, partially necrotic on exposure | AAE Glossary definition; spontaneous pain or pain exacerbated by cold stimuli lasting for a few seconds to several hours (lingering) compared to control teeth. PAI 1, 2, 3 or 4 included. |
Limit ≤ 6 mins 2.5% NaOCl |
No history of spontaneous pain or discomfort (except 2 days P/O), no TTP or tenderness to palpation, swelling, sinus tract or new pathosis (furcal, periapical or resorption). Normal mobility and PDs. PAI 1 or 2 or reduction in pre-operative PAI score. P/O pain: at 2 days, 93% of pts reported complete pain relief (the rest reported mild pain 1-2/10). Success: 97% 12 months. |
Not mentioned |
| Taha [54] 2018 | SS: 17 F/U: 17 D/O: 0% |
CP Biodentine |
9-17 Immediate |
Not mentioned | AAE Glossary definition; spontaneous pain or pain exacerbated by cold stimuli lasting for a few seconds to several hours (lingering) compared to control teeth. PAI scores recorded. |
Limit ≤ 6 mins 2.5% NaOCl |
No history of spontaneous pain or discomfort (except first few days P/O), functional and asymptomatic, grade I mobility, no swelling or sinus tract. No IRR, ERR, PAI <3 or reduction in PAI score. P/O pain: at 2 days, all pts had complete pain relief & none required analgesics. Success: 94% 12 months. |
Not mentioned |
| Taha [10] 2023 | SS: 30 F/U: 29 D/O: 3% |
CPBiodentine |
=29.9) Immediate |
Tooth not in occlusion | History of spontaneous pain lasting for a few seconds to several hours, exacerbation of pain by hot & cold fluids, radiating pain. Normal apical tissues, symptomatic or asymptomatic AP included. |
Limit ≤ 10 mins 2.5% NaOCl |
No spontaneous pain (except first few days P/O), functional and asymptomatic, no TTP or tenderness to palpation. Soft tissue appears normal, no mobility, no pathosis (IRR, ERR, furcal pathosis or new PARL). P/O pain: CP had a lower mean pain score than RCT at 24 hrs (P < 0.05) but no difference at 2, 3, 5 & 7 days (P > 0.05). CP had lower analgesic use than RCT (P < 0.05). Pt satisfaction recorded: higher for CP in terms of duration of treatment, intraoperative pain, pleasantness & cost (P < 0.05). QOL assessment: improvements for RCT & CP. Success: 93% 12 months. |
Outcome compared with RCT (P > 0.05) |
| Taha [60] 2017 | SS: 50 F/U: 49 D/O: 2% |
PP MTA or CaOH |
=30.3 ± 9.6) 1 week |
Contributory medical history | Severe spontaneous lingering pain that could be reproduced by cold testing. Periapical status not mentioned. |
Limit ≤ 6 mins 2.5% NaOCl |
No history of spontaneous pain or discomfort (except first few days P/O), functional and asymptomatic, positive response to cold, no TTP or tenderness to palpation, grade I mobility with normal soft tissues. No IRR or ERR, PAI < 3. P/O pain not reported. Success: 85% MTA, 43% CaOH 2 years. |
Pulp capping material (P < 0.05) |
| Uesrichai [8] 2019 | SS: 27 F/U: 27 D/O: 0% |
PP MTA or Biodentine |
=11.4) Immediate |
ASA class ≥3, necrotic or partially necrotic on exposure, exposure size >1mm but <5mm, no pulp exposure | Spontaneous pain with sharp and lingering pain to cold testing. No prominent PARL included but PDL widening or condensing osteitis included. |
Limit ≤ 10 mins 2.5% NaOCl |
No S&S of pulpitis, abnormal mobility or fistula. Positive response to cold. Improvement of early periapical changes, absence of PARL, IRR and ERR. P/O pain not reported. Success: ~85% (range 8 months to 5.75 yrs). |
Not mentioned |
Abbreviations: sample mean, AAE: American Association of Endodontists, ASA: American Society of Anesthesiologists, CaOH: calcium hydroxide, CEM: calcium-enriched cement, CP: complete pulpotomy, D/O: drop-out, EPT: electric pulp testing, ERR: external root resorption, ESE: European Society of Endodontology, F/U: follow-up, Hrs: hours, IP: irreversible pulpitis, IRR: internal root resorption, mins: minutes, MMP-9: matrix metalloproteinase-9, MTA: mineral trioxide aggregate, NaOCl: sodium hypochlorite, NEC: new endodontic cement, NS-RCT: non-surgical root canal treatment, NSAIDs: non-steroidal anti-inflammatory drugs, P/O: post-operative, PAI: periapical index, PARL: periapical radiolucency, PDL: periodontal ligament, PDs: probing depths, PP: partial pulpotomy, PRF: platelet-rich fibrin, Pts: patients, QOL: quality of life, RCT: root canal treatment, Rest’n: restoration, RP: reversible pulpitis, S&S: signs and symptoms, SS: sample size, TTP: tenderness to percussion, WNL: within normal limits, Yrs: years
4. Discussion
4.1.1. Outcomes and Success Criteria
Partial and complete pulpotomies enjoy high success rates when treating moderate - severe pulpitis [25]. In the studies that met the inclusion criteria for the present review, the overall success rates ranged from 76-100% over 12 months. Few studies describe recall times that exceed 12 months; a longer observation period may result in lower clinical and radiographic outcomes [5].
Strindberg [62] first classified RCT success based on strict or loose criteria. Strict criteria only included healed cases, while loose criteria included those with signs of healing. There is considerable variation in the literature concerning the definition of VPT success. The recent ESE S3 guidelines identify the outcome measures for the treatment of pulpitis and apical periodontitis [63]. Accordingly, patient-centered outcomes are the most critical measures of outcome, with tooth survival being the central outcome measure as it directly affects the patient's Oral Health Related Quality of Life (OHRQoL) [10,64]. Two studies included in the review reported high patient satisfaction [35] , with one also assessing how Quality of Life was significantly improved after both RCT and pulpotomy [10]. Encouragingly, Taha et al. [10] reported that the pulpotomy group reported significantly higher patient satisfaction than RCT for duration of treatment, intra-operative pain, pleasantness and financial cost. The presence or absence of pain, tenderness, swelling and sinus tract, need for analgesics, tooth function, need for further intervention, and radiographic evidence of a reduction in size or absence of an apical lesion are other important outcome measures.
Post-operative pain relief and the need for analgesics are also important patient-centered outcomes. Post-operative pain scores were recorded in most studies, but the time periods and methodology of pain reporting varied [10,24,27,35,40,44,45,46,48,52,54,55,58] Pulpotomy results in pain relief comparable to that of RCT [27,40], with evidence suggesting lower pain scores may be achieved more efficiently with VPT [10]. The reason for post-operative pain should be considered as one study stated that the only case that reported pain at 7 days experienced complete resolution of pain after occlusal adjustment [35].
In some studies, a negative response to cold [8,60] or electric pulp testing (EPT) [55] constituted treatment failure, while most studies do not consider pulp sensibility testing at the review appointment(s). The absence of a response to cold and/or (EPT) does not necessarily mean the pulp is in fact necrotic [65]. Careddu and Duncan [24] found that 10 teeth in their partial pulpotomy study were unresponsive to cold testing but were asymptomatic and had no PARL at 12 months. The authors did not perform histological examination of these teeth so their pulp may be necrotic; however, it is important to recognize that these teeth may also be vital.
Table 2 provides detailed information concerning measures of successful treatment. Other than pulp sensibility testing, standards for success across the studies were relatively homogenous. A systematic review by Cushley et al. [66] emphasized the need for guidelines on reporting success, as high heterogeneity among the included studies prevented meta-analysis comparisons of success between RCT and coronal pulpotomy.
In the authors' opinion, it is essential to include the reason for treatment failure when reporting treatment outcomes. Some studies provided details on the reason for treatment failure, while others provided minimal or no information. In Table 2, success rates encompassed both endodontic and restorative failures. It is important to consider that a restorative failure is not often associated with an endodontic failure. Jassal et al. reported that 3 of the 5 failures that occurred were actually restorative failures. In three studies [48,59,60], the only failure that occurred was due to restoration fracture. Interestingly, Careddu & Duncan [24]did not consider 4 patients that experienced a restorative failure due to Biodentine dislodgement in their outcome reporting. Considering this, the success of pulpotomy itself may be higher than reported.
4.1.2. Partial Versus Complete Pulpotomy
It is currently unclear whether a partial or complete pulpotomy is the appropriate treatment for moderate - severe pulpitis in permanent posterior teeth. Inflammation of the pulp is usually confined to the carious exposure and does not extend more than a few mm beyond this point [11], yet it is not clinically possible to determine the precise extent of bacterial penetration and pulpal necrosis. This is why some advocate for a coronal pulpotomy as there is a greater chance of removal of all infected tissue [67]. One study performed 3-4 mm partial pulpotomies in teeth with mild, moderate and severe pulpitis according to Wolters’ 2017 classification and found that severe pulpitis cases had a statistically significantly poorer outcome than mild pulpitis; further there was no difference in outcomes between moderate and mild pulpitis [24]. Additionally, all teeth with severe pulpitis included in that study would be diagnosed with irreversible pulpitis according to the AAE classification, supporting complete pulpotomy for adequate removal of severely inflamed pulp tissue. The study by Ramani et al. [46] considered teeth that were abandoned mid-pulpotomy in the primary outcome. These teeth did not receive the intervention due to a bleeding time >6 minutes. Although no statistical significance was found between the groups, the partial pulpotomy had a lower primary outcome than complete pulpotomy (80.8% and 89.8%, respectively), which may have been due to the conservative nature of a partial pulpotomy. However, it is also important to note that the allocation system utilized in this study was likely the reason for the difference in the outcome, not due to the procedure itself.
Yet, randomized controlled trials that have compared partial and complete pulpotomies in teeth with irreversible pulpitis have not shown a significant difference in outcome between the two treatment modalities [46,52,53]. Nevertheless, a partial pulpotomy is more conservative as it preserves the cell-rich coronal pulp and limits the destruction of primary odontoblasts, thus allowing tertiary dentinogenesis to continue. This may at least theoretically improve the healing potential of the pulp in case of future insults [68,69]. A study by Baranwal et al. [53] also showed that partial pulpotomy cases resulted in a higher percentage of dentine bridge formation and a lower incidence of root canal calcification compared with complete pulpotomy.
4.1.3. Age and Medical Status as Prognostic Factors
This review recognized some major limitations in existing clinical studies. The assumption that age is a prognostic factor of treatment has resulted in many studies only performing pulpotomies in younger age groups. Some believe that VPT success rates are expected to be lower for mature pulps compared to immature ones. Histologically, mature pulps show a lower number of odontoblasts and progenitor cells that are important for pulpal healing and the formation of a hard tissue barrier [70]. Younger pulps have been shown to have greater blood supply and increased cellularity [71]. However, the apparently beneficial histological characteristics of younger pulps may not translate to pulpotomy higher success rates. A recent systematic review included an age range between 6-52 years old and found that age did not affect the outcome of partial pulpotomy in permanent teeth [72]. Furthermore, a retrospective study by Linuswanont et al. [73] that included mature and immature teeth found that the age of the patient was not a predictor of the outcome of MTA pulpotomy. Critically, studies examining the influence of age underrepresent older patients [50,73]. Additionally, the age groups chosen in the studies mostly have a low cut-off age for the oldest group that does not allow older patients to be separated out [5,50]. Future studies should include more equally weighted and older age groups as well as larger sample sizes, as the high success rate of treatment often precludes statistical analysis of age in many studies.
Current clinical studies often fail to mention the medical status of patients or only treat those who are medically healthy. Because treatment time is significantly less than that required for RCT on posterior teeth [74], VPT may be more beneficial for medically compromised patients. Sánchez-Lara y Tajonar et al. [35] reported that complete pulpotomies restored with a definitive amalgam restoration in the same appointment were all completed within 45 to 60 minutes. Furthermore, one study showed that patients who have received a pulpotomy required fewer analgesics and experienced less post-operative pain compared to those who received RCT [10]. This may reduce the risk of adverse drug reactions in medically compromised patients. There is little evidence in the literature as to which medical conditions or medications may negatively affect the outcome of a pulpotomy. A case report on a HIV (Human Immunodeficiency Virus) positive patient [75] demonstrated 12 month clinical and radiographic success of a complete pulpotomy to manage pulpitis characterized by spontaneous and lingering pain with hot and cold. Future studies should perform pulpotomies on patients with a variety of medical conditions or classify patients according to the ASA classification as Uesrichai et al. [8] did, to determine if there are any contraindications for VPTs.
4.1.4. Presenting Signs and Symptoms as Diagnostic Factors
The presenting signs and symptoms are important for obtaining a pulpal and periapical diagnosis. This review focused on teeth with moderate - severe pulpitis, as categorized by Wolters. It appears that there is a scarcity of research that explores how the signs and symptoms at presentation may affect the prognosis of pulpotomy. Anta et al. [50] showed that treatment outcomes were not affected by pre-operative pain severity (moderate or severe), but a pain scale and specified descriptors were not used to define the pain severity. Taha and Abdulkhader [54] discovered that, despite 25% of teeth in their study experiencing severe spontaneous pain rated 9-10/10, they still had a high success rate. In contrast, Careddu and Duncan [24] found that mild pulpitis had a significantly better outcome for partial pulpotomy than for teeth with severe pulpitis. Yet, there was no significant difference in the outcome between mild and moderate pulpitis. This suggests that a coronal pulpotomy may be more appropriate for severe pulpitis cases but also highlights the diagnostic dilemma of existing pulpitis treatment recommendations.
One of the characteristic features of moderate - severe pulpitis is the presence of lingering pain after performing a cold test. The term ‘lingering’ is highly subjective. Some papers specify, in seconds, what is considered to be a lingering response [5,10,24,27,35,48,54]; for example, one paper defined this as pain lasting over 15 seconds after a cold and heat test [55]. Moreover, many studies failed to mention comparing the duration of cold stimulation with that of a control tooth/teeth to define ‘lingering pain’ [8,10,24,27,40,44,46,47,49,50,52,53,58,59,60]. In order to identify which pre-operative signs and symptoms may predict successful treatment, standardized sensibility tests and pain duration following testing are necessary.
4.1.5. Does the Apical Status Affect Prognosis?
It is well established that apical periodontitis precedes total pulp necrosis [14,76]. As bacteria enter the pulp, superficial necrosis and micro-abscesses will form, while the pulp below this remains vital [77,78]. Therefore, the presence of apical periodontitis should not be a definite contraindication to pulpotomy and does not appear to be a prognostic factor in the literature [5,40,50,53]. Taha and Abdelkhader [48] performed complete pulpotomies on 4 teeth that had a PAI score of 3, and 5 teeth with a PAI score of 4. Additionally, 44% of the teeth included were tender to percussion at the time of treatment. The authors were not able to perform statistical analysis as only 8 teeth in total had a pre-operative PARL but found that 7 of the 8 teeth healed (based on loose criteria). Cone-beam computed tomography (CBCT) has been shown to have a higher sensitivity for apical periodontitis [79]. Only one study included in the qualitative analysis used CBCT to determine the radiographic outcome [53]. A study by Hashem et al. [80] showed that CBCT was more sensitive for the detection of apical radiolucency than PA radiographs after IPC with Biodentine or glass ionomer cement (GIC). Patients with symptomatic apical periodontitis underwent pre-operative and 12-month post-operative CBCT scans, which showed that the presence of a periapical radiolucency did not impact treatment success. CBCT scans were not done for all included patients, so the impact on outcome cannot be fully evaluated due to the possibility that some teeth may have had pre-operative asymptomatic apical periodontitis.
4.1.6. Depth of Caries as a Prognostic Factor
The depth of the carious lesion may be a diagnostic predictor for the success of pulpotomy. Radiographically, caries can be classified as deep or extremely deep depending on whether or not dentine is present between the pulp chamber space and the carious lesion, respectively [26]. It has been observed that bacteria were located in the primary dentine for deep caries, while extremely deep lesions contained bacteria in the tertiary dentine and the pulp [81]. Although the depth of the carious lesion was not found to be statistically significant for the outcome of partial pulpotomy, all failures did occur in the teeth with extremely deep caries, suggesting that a partial pulpotomy may not be sufficient for the removal of the severely inflamed, necrotic tissue [24,34]. Furthermore, Careddu and Duncan [24] found that all of the teeth with extremely deep caries resulted in pulp exposure after non-selective caries removal and received a pulpotomy. However, a pulp exposure only occurred in 42% of the deep lesions, and therefore the majority of these teeth did not receive the treatment.
4.1.7. Inflammation; Degree of Bleeding, Bleeding Time and Concentration of Biomarkers
A necrotic or partially necrotic pulp upon exposure was commonly excluded from receiving a pulpotomy in the studies assessed. Partially necrotic pulps were characterized by insufficient bleeding, whereas necrotic was non-bleeding on exposure with/without exudate [8,60]. Paradoxically, VPT works on the philosophy that the superficial pulp is necrotic/severely inflamed while the remainder of the pulp is healthy and vital. From a technical standpoint, it can be observed that all of these teeth with moderate-severe pulpitis exhibit partial pulp necrosis. Partial or complete pulp necrosis upon exposure may be excluded from receiving a partial pulpotomy, as only 2-3 mm of the pulp is removed which may not be sufficient. Yet, this does not rule out a coronal pulpotomy as a treatment option. Irrespective of the appearance of the pulp upon exposure, if there is bleeding evident at the orifice(s), a coronal pulpotomy can still be performed.
Several studies opted to exclude teeth that did not exhibit pulp exposure following non-selective caries removal, essentially ignoring the clinical signs and symptoms. One study excluded 7 teeth (2 with moderate & 1 with severe pulpitis) as there was no carious pulp exposure [24]. These teeth received an indirect pulp cap with calcium hydroxide (CaOH). Within 5 months, 1 tooth with moderate pulpitis developed pulp necrosis and a PARL, requiring RCT. In this current review, only teeth with moderate to severe pulpitis symptoms were included as part of the criteria. There is debate over whether teeth with moderate-severe pulpitis but without carious pulp exposure should still undergo a pulpotomy. While some aim for conservatism, the chance of severe inflammation and microabscess formation in the pulp is high. Furthermore, Ricucci et al. [13] found that the clinical diagnosis corresponded with the histological diagnosis of irreversible pulpitis in 84% of cases and that irreversible pulpitis was always characterized by the presence of bacteria within the pulp [82]. The goal of VPT is to prevent apical periodontitis and conserve healthy hard and soft tissue. If deep caries is left, or if bacteria have entered the pulp already, pulp necrosis and apical periodontitis may ensue as the microbes are sealed from the external environment but can still receive nutrients for their sustained survival and pathogenicity from the pulpal tissues and dentine matrix [83].
Clinicians frequently hold the belief that the extent of bleeding and time to hemostasis may serve as an indicator of whether the tooth's pulp is reparable or not, and therefore its suitability for VPT. However, the relationship between bleeding times and degree of pulpal inflammation is not fully understood [73]. Matsuo et al. [84] performed DPC using CaOH on carious teeth with varying degrees of pulpitis. This study served as the basis for the belief that excessive pulpal bleeding may indicate a pulp that is excessively inflamed, and less likely to respond favorably to VPT. However, this study only described DPC, which many consider to be too conservative for teeth with moderate to severe pulpitis [18,82].
Sharma et al. [47] was the only study to investigate the relationship between inflammation (measured by the concentration of MMP-9) and bleeding time and found no such correlation. This suggests that the time to achieve hemostasis is not an effective indicator of pulp inflammation severity. A study by Waterhouse and colleagues [85] found no difference in the bleeding stoppage time between normal pulps and those that were inflamed, again suggesting that the extent of bleeding may not be a diagnostic indicator. Another study found that the average bleeding time increased with pulpitis severity, but this was not statistically significant [24].
The threshold time to hemostasis for pulpotomy to be performed greatly varies in the literature. One review considers a healthy bleeding time to be within 8-15 minutes [86], with another suggesting that hemostasis should be achieved within 10 minutes [87]. In most of the papers reviewed, statistical analysis was not performed to determine if bleeding time affected the outcome of partial or complete pulpotomy. Anta et al. [50] found that the bleeding time did not affect the outcome, but only included cases that took up to 5 minutes for bleeding stoppage. One study included bleeding times that ranged from 3 to 25 minutes and found that the only failure occurred in the tooth that had a bleeding time of 7 minutes [45]. Further studies with adequate power analysis should be conducted to determine whether the extent of bleeding or the bleeding time are both diagnostic and prognostic. Moreover, little is known about any impact anti-coagulant and anti-platelet medications may have on the bleeding time.
Some studies did not utilize NaOCl for the hemostasis protocol [5,27,40,45,50,55,58,59]. NaOCl has been shown to be effective at reducing hemorrhage and promoting hemostasis [88]. It is also a strong antibacterial that is used to disinfect the wound and remove necrotic infected pulp tissue [89]. A randomized controlled trial also showed that rinsing with 2.5% NaOCl resulted in better outcomes and less post-operative pain for DPC than rinsing with sterile saline [90]. However, no pulp tissue was removed. Thus, this procedure relied on chemical disinfection entirely. Other studies have shown no difference in outcome for pulpotomy when using NaOCl or saline [91,92].
Further studies with adequate power analysis need to be conducted to determine whether the extent of bleeding or the bleeding time are both diagnostic and prognostic, though to date there is no evidence that supports this.
Changes in biomarker profile and concentration are leading indicators of pulpal inflammatory progression, preceding microscopic and macroscopic changes [93]. The development of a chairside diagnostic biomarker test with high specificity and sensitivity may assist in future clinical decision-making between VPT or RCT. Matrix Metalloproteinase-9 (MMP-9) has been of particular interest in recent studies as it is expressed in high concentrations in inflamed pulps as an indicator of tissue breakdown [94,95]. Mente et al. [96] sampled pulpal blood after a partial pulpotomy in 44 teeth with deep caries and found that the MMP-9 levels were significantly higher in patients with moderate - severe pulpitis. However, there were no significant differences in levels between the reversible pulpitis group and the irreversible pulpitis group that had taken non-steroidal anti-inflammatories (NSAIDs) prior to treatment. This may mask the true histological status of the tooth and affect diagnostic decision-making. Unfortunately, a further limitation of that study is that the authors did not correlate the success of partial pulpotomy with the MMP-9 concentrations. Sharma et al. [47] obtained pulpal blood samples after pulp exposures to quantify MMP-9 concentrations in teeth with extremely deep caries and symptoms of irreversible pulpitis. The authors correlated these values with the outcome of a complete pulpotomy and found that an MMP-9 concentration of ≥ 334.8 ng/mL was a critical value for pulpotomy failure. The paper [47] reported the test to have 83% sensitivity, suggesting that only 17% of cases with MMP-9 ≥334.8 ng/mL would have a successful pulpotomy outcome. However, based on the information provided in the paper and definitions of test accuracy (Table S1), a contingency table (Table S2) was created. This table shows that 6 out of 11 (54.5%) teeth with a reading ≥ 334.8 ng/mL were actually successful after pulpotomy. Essentially, of the teeth where a test would indicate that no pulpotomy should be performed, more than half could have had a successful pulpotomy. However, the test did correctly identify all the pulpotomy failures, which is reassuring to a clinician. Further studies with large sample sizes on various profiles of biomarkers should be undertaken to assist with a more accurate chairside diagnostic test to determine the true inflammatory status of the pulp for appropriate management.
4.1.8. The Importance of a Definitive Restoration
Currently, no randomized controlled trials have compared the outcomes of pulpotomy with immediate versus delayed permanent restoration placement. However, as seen in the results (Table 2), definitive restorations were mostly placed within 1-2 weeks, and high success was observed. Potentially, one of the main prognostic factors for VPT success is the quality of the coronal seal of the restoration [97]. Many authors advocate for the placement of the definitive restoration in the same appointment for better outcomes [4,98,99]. All studies included in the systematic review by Ather et al. [25] had a permanent restoration either placed immediately, or within 1-month post-pulpotomy, which may have contributed to the high pooled success rate of 86%. Tan et al. [100] showed the placement of a GIC restoration resulted in a greater risk of late failure and need for further intervention than when amalgam or CR was placed. It has also been shown that a delay in placement of the permanent restoration negatively affected the prognosis of DPC [101]. However, a retrospective study showed that the quality of the restoration has no significant impact on the outcome of coronal pulpotomy [73]. Even teeth with marginal leakage and secondary caries can still show clinical and radiographic success after follow-up. Three studies in the review's qualitative analysis found that restorative reasons were the primary cause of treatment failure [24,52,59]. The success rate for complete pulpotomy in one study was particularly low [58]. While strict success criteria may have contributed, they found that the 1-year overall success rate for MTA was 44%. All teeth in the study were restored with Kalzinol for 24 hours. Kalzinol, a resin-reinforced zinc-oxide eugenol (ZOE) cement, is used as an intermediate restorative material [102], and has been shown to be strongly associated with microleakage [103]. In addition, ZOE cements can delay the setting reaction of MTA [104], which may have contributed to further microleakage resulting in long-term radiographic failure. Furthermore, teeth in this study were only permanently restored with resin-modified GIC (RMGIC) and CR if they were asymptomatic at 24 hours, those that were symptomatic were considered a failure. It's possible that these teeth may have succeeded given more time. Others found that over 50% of patients reported increased sensitivity to cold at 7 days post-pulpotomy, which gradually subsided in the following 3 months [25].
When using MTA or calcium silicate cement (CSC) as a pulp capping material, it is common to place a moist cotton pellet for 24 hours before restoring the tooth [44,60]. However, placing a moist cotton pellet over MTA offers little additional benefit for the setting reaction [105], and there is clear evidence that etching and placement of a CR restoration can be done after initial setting of the material (approximately 10 minutes) [106,107].
4.1.9. Pulp Capping Material
The success of VPT has significantly increased with the introduction of biocompatible and bioregenerative materials such as MTA and other CSCs [60,108,109]. Pulp capping materials induce superficial pulpal necrosis and inflammation to stimulate healing and the formation of a hard tissue barrier [110,111].
CaOH is no longer recommended as a pulp capping material due to the presence of tunnel defects in the hard tissue barrier. This is a potential source of microleakage, and the deeper coagulation necrosis and inflammation that is observed, leads to poorer outcomes [25,112,113,114].
Frequently, there are no significant outcome differences found among different MTA and CSC varieties across various VPT treatments [115]; however, a systematic review did find Biodentine to be superior [25]. As long as the remaining pulp is non-inflamed and is capable of healing, hemorrhage has been controlled, and the pulp capping material has provided a bacterial tight seal, the VPT should be successful [5]. Histological examination of successful cases has shown continued pulp vitality with the absence of inflammatory infiltrate. Figure 2 illustrates the healing response of an inflamed pulp when treated with a pulpotomy. The case report [116] refers to a young patient and a full MTA pulpotomy of tooth #29 (45 in FDI numbering) with a diagnosis of irreversible pulpitis and symptomatic apical periodontitis. The tooth was extracted 10 months post-operatively for orthodontic reasons, despite enjoying clinical and radiographic success, and the tooth was submitted to histological examination. Figure 2 discloses the MTA material just superior to a hard dentine bridge. The deeper odontoblastic layer is intact despite a segment of superficial odontoblasts just below the dentine bridge being destroyed. Figure 2 also shows that the remaining pulp tissue below the dentine bridge is completely free of inflammatory infiltrate. These images are a compelling example of the pulp showing repair and maintenance of its vitality, with the absence of any chronic inflammation or dystrophic mineralization, after VPT has been performed.
4.1.10. Potential Risks and Complications Associated with Pulpotomies
There are concerns about the potential risks of VPTs. Pulp canal obliteration (PCO) may occur whereby the radiographic pulp space cannot be visualized, making future RCT more difficult [117]. The risk of developing PCO after pulpotomies is extremely low [52,54], with some reports showing no incidence of calcification [48]. One study found that the incidence of root canal calcification was significantly higher in the complete pulpotomy group, compared to the partial pulpotomy group [53]. It is important to note that PCO signifies a healthy pulp, and the chances of future pulp necrosis are low [118,119]. Internal root resorption (IRR) has been reported after VPT [115]. It is associated with long-standing chronic inflammation in a vital pulp that has some extent of coronal necrotic tissue present [120]. One study on 20 teeth showed 1 tooth that had radiographic evidence of internal resorption despite complete healing of the pre-operative PARL [54]. Thus, overall, the risk of the development of IRR in the literature appears low. Asgary and Ehsani [59] histologically examined the one case that failed due to prosthodontic reasons and found that there was evidence of arrested internal resorption with no evidence of inflammation within the pulp tissue in addition to the presence of a complete hard tissue barrier. Additionally, Taha and Abdulkhader [54] also reported a case of internal root resorption in a lower molar with evidence of preoperative radiolucency that was resolved at 12 months.
Tooth discoloration is another risk after VPT, particularly after complete pulpotomy [121]. It is an important patient-centered outcome measure related to esthetics, however; in posterior teeth discoloration is less of an esthetic concern. The papers included in the analysis reported a very low incidence of tooth discoloration, with many reporting no discoloration at all [45,48,49,52,54,60]. MTA appears to have the highest risk of discoloration due to the presence of bismuth oxide [8]. Residual NaOCl in contact with bismuth oxide may also lead to further discoloration of the tooth, which is why rinsing with sterile saline prior to MTA placement is advocated by some [122]. Biodentine application appears to result in significantly less discoloration than MTA [8,24,123].
Finally, it is difficult to determine the vitality of the pulp after treatment. Pulp sensibility tests are less reliable in teeth that have received a pulpotomy, particularly a coronal pulpotomy. A randomized controlled trial found that 94% of teeth responded to EPT after a partial pulpotomy, whereas this was only 63% after complete pulpotomy [52]. Following a pulpotomy, teeth are more likely to respond to EPT than cold testing, making EPT a more useful diagnostic tool for teeth with a history of VPT [124]. The absence of a response to cold and/or EPT does not reflect the true histological status of the pulp, and a clinician should consider clinical and radiographic signs and symptoms before deciding on the outcome of the previous pulpotomy.
5. Conclusions
A partial or complete pulpotomy should be offered to patients for the treatment of moderate to severe pulpitis, as an alternative to root canal treatment and extraction. High long-term success rates are reported in the literature [5,66]. It is essential to update existing diagnostic classifications to recognize that the current term "irreversible pulpitis" is no longer validated [25]. Guidelines to assist a clinician in the decision-making process can be generated once the diagnostic and prognostic predictors of successful pulpotomy have been recognized and corroborated. Future studies should focus on assessing how different medical conditions or medications may affect the outcome of VPT. The age range and number of participants in older age groups should also be addressed in studies as age has not shown to be a prognostic factor of treatment [5,72]. Such a treatment option would be particularly beneficial for older patients. The bleeding time has historically been perceived to be a predictor of the extent of inflammation, with longer bleeding times indicating an irreversibly inflamed pulp that would not remain vital [34]. From the studies analyzed in this scoping review, it is evident that bleeding time is likely not a predictor of success or failure of pulpotomy [8,24,34,45,50]. Nevertheless, a practical limit may be adopted according to time constraints of a practitioner.
Biomarkers are a potentially promising quantitative method for identifying the extent of pulp inflammation, and therefore guiding treatment decisions [47,96]. Future studies should consider enrolling high numbers of participants to identify a biomarker with high specificity and sensitivity for pulpotomy outcomes.
This study was not a systematic review or meta-analysis. Thus, studies were not formally evaluated for risk of bias or heterogeneity. The conclusions of this scoping review do, however, validate pulpotomy as a predictable treatment for permanent mature posterior teeth with symptoms of moderate to severe pulpitis, and encourage further research into the potential diagnostic and prognostic predictors of outcome.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Tables S1 and S2.
Author Contributions
Conceptualization, C.P., O.P. and P.W.; methodology, H.M. and P.W.; resources, O.P. and P.W.; data curation, H.M. and P.W.; writing – original draft, H.M.; writing – review & editing, C.P., H.M., O.P. and P.W.; supervision, O.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Acknowledgments
Thanks to Dr Chompu-Inwai for providing the reviewers with the raw data from their clinical study [8], allowing its inclusion into the qualitative analysis section.
Conflicts of Interest
The authors have no conflicts of interest to declare.
References
- Yu, J.; Zhang, T.; Zhao, D.; Haapasalo, M.; Shen, Y. Characteristics of endodontic emergencies during coronavirus disease 2019 outbreak in Wuhan. J Endod 2020, 46, 730-735. [CrossRef]
- Currie, C.C.; Stone, S.J.; Durham, J. Pain and problems: a prospective cross-sectional study of the impact of dental emergencies. J Oral Rehabil 2015, 42, 883-889. [CrossRef]
- Edwards, D.; Rasaiah, S.; Hamzah Ahmed, S.; Breckons, M.; Stone, S.J.; Currie, C.C.; Durham, J.; Whitworth, J. The financial and quality of life impact of urgent dental presentations: a cross-sectional study. Int Endod J 2023, 56, 697-709. [CrossRef]
- McDougal, R.A.; Delano, E.O.; Caplan, D.; Sigurdsson, A.; Trope, M. Success of an alternative for interim management of irreversible pulpitis. J Am Dent Assoc 2004, 135, 1707-1712. [CrossRef]
- Asgary, S.; Eghbal, M.J.; Fazlyab, M.; Baghban, A.A.; Ghoddusi, J. Five-year results of vital pulp therapy in permanent molars with irreversible pulpitis: a non-inferiority multicenter randomized clinical trial. Clin Oral Investig 2015, 19, 335-341. [CrossRef]
- American Association of Endodontists. Endodontic diagnosis. Available online: https://www.aae.org/specialty/wp-content/uploads/sites/2/2017/07/endodonticdiagnosisfall2013.pdf (accessed on 5/5/2022).
- American Association of Endodontists. Glossary of endodontic terms. Available online: https://www.aae.org/specialty/clinical-resources/glossary-endodontic-terms/ (accessed on 5/5/2022).
- Uesrichai, N.; Nirunsittirat, A.; Chuveera, P.; Srisuwan, T.; Sastraruji, T.; Chompu-Inwai, P. Partial pulpotomy with two bioactive cements in permanent teeth of 6- to 18-year-old patients with signs and symptoms indicative of irreversible pulpitis: a noninferiority randomized controlled trial. Int Endod J 2019, 52, 749-759. [CrossRef]
- Asgary, S.; Eghbal, M.J.; Shahravan, A.; Saberi, E.; Baghban, A.A.; Parhizkar, A. Outcomes of root canal therapy or full pulpotomy using two endodontic biomaterials in mature permanent teeth: a randomized controlled trial. Clin Oral Investig 2022, 26, 3287-3297. [CrossRef]
- Taha, N.A.; Abuzaid, A.M.; Khader, Y.S. A randomized controlled clinical trial of pulpotomy versus root canal therapy in mature teeth with irreversible pulpitis: outcome, quality of life, and patients' satisfaction. J Endod 2023, 49, 624-631.e622. [CrossRef]
- Seltzer, S.; Bender, I.B.; Ziontz, M. The dynamics of pulp inflammation: correlations between diagnostic data and actual histologic findsings in the pulp. Oral Surg Oral Med Oral Pathol 1963, 16, 846-977.
- Mejàre, I.A.; Axelsson, S.; Davidson, T.; Frisk, F.; Hakeberg, M.; Kvist, T.; Norlund, A.; Petersson, A.; Portenier, I.; Sandberg, H.; et al. Diagnosis of the condition of the dental pulp: a systematic review. Int Endod J 2012, 45, 597-613. [CrossRef]
- Ricucci, D.; Loghin, S.; Siqueira, J.F. Correlation between clinical and histologic pulp diagnoses. J Endod 2014, 40, 1932-1939. [CrossRef]
- Yamasaki, M.; Kumazawa, M.; Kohsaka, T.; Nakamura, H.; Kameyama, Y. Pulpal and periapical tissue reactions after experimental pulpal exposure in rats. J Endod 1994, 20, 13-17. [CrossRef]
- Bjørndal, L.; Ricucci, D. Pulp inflammation: from the reversible pulpitis to pulp necrosis during caries progression. In The Dental Pulp: Biology, Pathology, and Regenerative Therapies, Goldberg, M., Ed.; Springer Berlin Heidelberg: Berlin, Heidelberg, 2014; pp. 125-139. ISBN 978-3-642-55160-4.
- Murdoch-Kinch, C.A.; McLean, M.E. Minimally invasive dentistry. J Am Dent Assoc 2003, 134, 87-95. [CrossRef]
- Santos, J.M.; Pereira, J.F.; Marques, A.; Sequeira, D.B.; Friedman, S. Vital pulp therapy in permanent mature posterior teeth with symptomatic irreversible pulpitis: a systematic review of treatment outcomes. Medicina (Kaunas) 2021, 57, 573. [CrossRef]
- American Association of Endodontists. AAE position statement on vital pulp therapy. Available online: https://f3f142zs0k2w1kg84k5p9i1o-wpengine.netdna-ssl.com/wp-content/uploads/2021/05/VitalPulpTherapyPositionStatement_v2.pdf (accessed on 04/05/2023).
- Van Hassel, H.J. Physiology of the human dental pulp. Oral Surg Oral Med Oral Pathol 1971, 32, 126-134. [CrossRef]
- Heyeraas, K.J.; Berggreen, E. Interstitial fluid pressure in normal and inflamed pulp. Crit Rev Oral Biol Med 1999, 10, 328-336. [CrossRef]
- Mejàre, I.; Cvek, M. Partial pulpotomy in young permanent teeth with deep carious lesions. Endod Dent Traumatol 1993, 9, 238-242. [CrossRef]
- Cvek, M. A clinical report on partial pulpotomy and capping with calcium hydroxide in permanent incisors with complicated crown fracture. J Endod 1978, 4, 232-237. [CrossRef]
- Asgary, S.; Eghbal, M.J.; Fazlyab, M.; Baghban, A.A.; Ghoddusi, J. Five-year results of vital pulp therapy in permanent molars with irreversible pulpitis: a non-inferiority multicenter randomized clinical trial. Clin Oral Investig 2014, 19, 335-341. [CrossRef]
- Careddu, R.; Duncan, H.F. A prospective clinical study investigating the effectiveness of partial pulpotomy after relating preoperative symptoms to a new and established classification of pulpitis. Int Endod J 2021, 54, 2156-2172. [CrossRef]
- Ather, A.; Patel, B.; Gelfond, J.A.L.; Ruparel, N.B. Outcome of pulpotomy in permanent teeth with irreversible pulpitis: a systematic review and meta-analysis. Sci Rep 2022, 12. [CrossRef]
- Duncan, H.F.; Galler, K.M.; Tomson, P.L.; Simon, S.; El-Karim, I.; Kundzina, R.; Krastl, G.; Dammaschke, T.; Fransson, H.; Markvart, M.; et al. European society of endodontology position statement: management of deep caries and the exposed pulp. Int Endod J 2019, 52, 923-934. [CrossRef]
- Asgary, S.; Eghbal, M.J. Treatment outcomes of pulpotomy in permanent molars with irreversible pulpitis using biomaterials: a multi-center randomized controlled trial. Acta Odontol Scand 2013, 71, 130-136. [CrossRef]
- Wolters, W.J.; Duncan, H.F.; Tomson, P.L.; Karim, I.E.; McKenna, G.; Dorri, M.; Stangvaltaite, L.; van der Sluis, L.W.M. Minimally invasive endodontics: a new diagnostic system for assessing pulpitis and subsequent treatment needs. Int Endod J 2017, 50, 825-829. [CrossRef]
- Duncan, H.F.; Kirkevang, L.L.; Peters, O.A.; El-Karim, I.; Krastl, G.; Del Fabbro, M.; Chong, B.S.; Galler, K.M.; Segura-Egea, J.J.; Kebschull, M.; et al. Treatment of pulpal and apical disease: the european society of endodontology (ESE) S3-level clinical practice guideline. Int Endod J 2023. [CrossRef]
- Ng, Y.L.; Mann, V.; Rahbaran, S.; Lewsey, J.; Gulabivala, K. Outcome of primary root canal treatment: systematic review of the literature - part 2. influence of clinical factors. Int Endod J 2008, 41, 6-31. [CrossRef]
- Sjögren, U.; Hägglund, B.; Sundqvist, G.; Wing, K. Factors affecting the long-term results of endodontic treatment. J Endod 1990, 16, 498-504. [CrossRef]
- Ricucci, D.; Russo, J.; Rutberg, M.; Burleson, J.A.; Spångberg, L.S. A prospective cohort study of endodontic treatments of 1,369 root canals: results after 5 years. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2011, 112, 825-842. [CrossRef]
- Zhang, M.; Xiong, Y.; Wang, X.; Wang, Y.; Cai, Y.; Xu, J.; Zhang, C.; Li, J. Factors affecting the outcome of full pulpotomy in permanent posterior teeth diagnosed with reversible or irreversible pulpitis. Sci Rep 2022, 12. [CrossRef]
- Aldeen, R.Z.; Aljabban, O.; Almanadili, A.; Alkurdi, S.; Eid, A.; Mancino, D.; Haikel, Y.; Kharouf, N. The influence of carious lesion and bleeding time on the success of partial pulpotomy in permanent molars with irreversible pulpitis: a prospective study. Bioengineering (Basel) 2023, 10, 700. [CrossRef]
- Sánchez-Lara y Tajonar, R.G.; Vergara-Tinoco, J.V.; Dammaschke, T.; Domínguez-Pérez, R.A. A pilot feasibility study to establish full pulpotomy in mature permanent teeth with symptomatic irreversible pulpitis as a routine treatment in mexican public healthcare services. Healthcare (Basel) 2022, 10, 2350. [CrossRef]
- Galani, M.; Tewari, S.; Sangwan, P.; Mittal, S.; Kumar, V.; Duhan, J. Comparative evaluation of postoperative pain and success rate after pulpotomy and root canal treatment in cariously exposed mature permanent molars: a randomized controlled trial. J Endod 2017, 43, 1953-1962. [CrossRef]
- Rosenberg, P.A. Clinical strategies for managing endodontic pain. Endod Topics 2002, 3, 78-92. [CrossRef]
- Philip, N.; Suneja, B. Minimally invasive endodontics: a new era for pulpotomy in mature permanent teeth. Br Dent J 2022, 233, 1035-1041. [CrossRef]
- Lin, L.M.; Ricucci, D.; Saoud, T.M.; Sigurdsson, A.; Kahler, B. Vital pulp therapy of mature permanent teeth with irreversible pulpitis from the perspective of pulp biology. Aust Endod J 2020, 46, 154-166. [CrossRef]
- Beauquis, J.; Setbon, H.M.; Dassargues, C.; Carsin, P.; Aryanpour, S.; Van Nieuwenhuysen, J.-P.; Leprince, J.G. Short-term pain evolution and treatment succes of pulpotomy as irreversible pulpitis permanent treatment: a non-randomized clinical study. J Clin Med 2022, 11, 787. [CrossRef]
- Tomson, P.L.; Vilela Bastos, J.; Jacimovic, J.; Jakovljevic, A.; Pulikkotil, S.J.; Nagendrababu, V. Effectiveness of pulpotomy compared with root canal treatment in managing non-traumatic pulpitis associated with spontaneous pain: A systematic review and meta-analysis. Int Endod J 2022. [CrossRef]
- Wisniewski, J.F.; Norooz, S.; Callahan, D.; Mohajeri, A. Survey of vital pulp therapy treatment in permanent dentition being taught at U.S. dental schools. J Endod 2022, 48, 1107-1112. [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O'Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med 2018, 169, 467-473. [CrossRef]
- Airsang, A.J.; Shankaregowda, A.M.; Meena, N.; Lingaiah, U.; Lakshminarasimhaiah, V.; Harti, S. Comparative assessment of complete pulpotomy in mature permanent teeth with carious exposure using calcium silicate cement: a randomized clinical trial. World J. Dent. 2022, 13, S135-S143. [CrossRef]
- Elmas, S.; Kotan, D.A.; Odabaş, M.E. Two-year outcomes of coronal pulpotomy in young permanent molars with clinical signs indicative of irreversible pulpitis. Pediatr Dent 2023, 45, 46-52.
- Ramani, A.; Sangwan, P.; Tewari, S.; Duhan, J.; Mittal, S.; Kumar, V. Comparative evaluation of complete and partial pulpotomy in mature permanent teeth with symptomatic irreversible pulpitis: A randomized clinical trial. Int Endod J 2022. [CrossRef]
- Sharma, R.; Kumar, V.; Logani, A.; Chawla, A.; Mir, R.A.; Sharma, S.; Kalaivani, M. Association between concentration of active MMP-9 in pulpal blood and pulpotomy outcome in permanent mature teeth with irreversible pulpitis – a preliminary study. Int Endod J 2021, 54, 479-489. [CrossRef]
- Taha, N.A.; Abdelkhader, S.Z. Outcome of full pulpotomy using biodentine in adult patients with symptoms indicative of irreversible pulpitis. Int Endod J 2018, 51, 819-828. [CrossRef]
- R, R.; Aravind, A.; Kumar, V.; Sharma, S.; Chawla, A.; Logani, A. Influence of occlusal and proximal caries on the outcome of full pulpotomy in permanent mandibular molar teeth with partial irreversible pulpitis: a prospective study. Int Endod J 2021, 54, 1699-1707. [CrossRef]
- Anta, S.; Diouma, N.; Ousmane, N.S.; Fatou, L.B.; Florence, F.; Babacar, T. Evaluation of complete pulpotomy with biodentine on mature permanent molars with signs and symptoms of symptomatic irreversible pulpitis: 12-months follow-up. J Endod 2022, 48, 312-319. [CrossRef]
- Ørstavik, D.; Kerekes, K.; Eriksen, H.M. The periapical index: a scoring system for radiographic assessment of apical periodontitis. Dent Traumato 1986, 2, 20-34. [CrossRef]
- Jassal, A.; Nawal, R.R.; Yadav, S.; Talwar, S.; Yadav, S.; Duncan, H.F. Outcome of partial and full pulpotomy in cariously exposed mature molars with symptoms indicative of irreversible pulpitis: a randomized controlled trial. Int Endod J 2022. [CrossRef]
- Baranwal, H.; Mittal, N.; Yadav, J.; Rani, P.; Kumar, N. Outcome of partial pulpotomy verses full pulpotomy using biodentine in vital mature permanent molar with clinical symptoms indicative of irreversible pulpitis: a randomized clinical trial. J Conserv Dent 2022, 25, 317-323. [CrossRef]
- Taha, N.A.; Abdulkhader, S.Z. Full pulpotomy with biodentine in symptomatic young permanent teeth with carious exposure. J Endod 2018, 44, 932-937. [CrossRef]
- Hussain, M.I.; Bashar, A.M. Outcome of mineral trioxide aggregate pulpotomy for mature permanent molars with symptoms indicative of irreversible pulpitis. Mymensingh Med J 2022, 31, 223-229. [CrossRef]
- Kirkevang, L.L.; Vaeth, M.; Wenzel, A. Ten-year follow-up of root filled teeth: a radiographic study of a Danish population. Int Endod J 2014, 47, 980-988. [CrossRef]
- Frisk, F.; Hugosson, A.; Kvist, T. Is apical periodontitis in root filled teeth associated with the type of restoration? Acta Odontol Scand 2015, 73, 169-175. [CrossRef]
- Kumar, V.; Juneja, R.; Duhan, J.; Sangwan, P.; Tewari, S. Comparative evaluation of platelet-rich fibrin, mineral trioxide aggregate, and calcium hydroxide as pulpotomy agents in permanent molars with irreversible pulpitis: a randomized controlled trial. Contemp Clin Dent 2016, 7, 512-518. [CrossRef]
- Asgary, S.; Ehsani, S. Permanent molar pulpotomy with a new endodontic cement: a case series. J Conserv Dent 2009, 12, 31-36. [CrossRef]
- Taha, N.A.; Khazali, M.A. Partial pulpotomy in mature permanent teeth with clinical signs indicative of irreversible pulpitis: a randomized clinical trial. J Endod 2017, 43, 1417-1421. [CrossRef]
- Asgary, S.; Eghbal, M.J. The effect of pulpotomy using a calcium-enriched mixture cement versus one-visit root canal therapy on postoperative pain relief in irreversible pulpitis: a randomized clinical trial. Odontology 2010, 98, 126-133. [CrossRef]
- Strindberg, L.Z. The dependence of the results of pulp therapy on certain factors; an analytic study based on radiographic and clinical follow-up examinations. Acta Odontol Scand 1956.
- Duncan, H.F.; Nagendrababu, V.; El-Karim, I.; Dummer, P.M.H. Outcome measures to assess the effectiveness of endodontic treatment for pulpitis and apical periodontitis for use in the development of european society of endodontology S3-level clinical practice guidelines: a consensus-based development. Int Endod J 2021, 54, 2184-2194. [CrossRef]
- Tan, H.; Peres, K.; Peres, M. Retention of teeth and oral health–related quality of life. J Dent Res 2016, 95, 1350-1357. [CrossRef]
- Donnermeyer, D.; Dammaschke, T.; Lipski, M.; Schäfer, E. Effectiveness of diagnosing pulpitis: a systematic review. Int Endod J 2022. [CrossRef]
- Cushley, S.; Duncan, H.F.; Lappin, M.J.; Tomson, P.L.; Lundy, F.T.; Cooper, P.; Clarke, M.; El Karim, I.A. Pulpotomy for mature carious teeth with symptoms of irreversible pulpitis: a systematic review. J Dent 2019, 88, 103158-103158. [CrossRef]
- Taha, N.A.; Al-khatib, H. 4-year follow-up of full pulpotomy in symptomatic mature permanent teeth with carious pulp exposure using a stainproof calcium silicate–based material. J Endod 2022, 48, 87-95. [CrossRef]
- George, R. Is partial pulpotomy in cariously exposed posterior permanent teeth a viable treatment option? Evid Based Dent 2020, 21, 112-113. [CrossRef]
- Duncan, H.F. Present status and future directions - vital pulp treatment and pulp preservation strategies. Int Endod J 2022. [CrossRef]
- Hossain, M.Z.; Daud, S.; Nambiar, P.; Razak, F.A.; Ab-Murat, N.; Saub, R.; Bakri, M.M. Correlation between numbers of cells in human dental pulp and age: implications for age estimation. Arch Oral Biol 2017, 80, 51-55. [CrossRef]
- Morse, D.R. Age-related changes of the dental pulp complex and their relationship to systemic aging. Oral Surg Oral Med Oral Pathol 1991, 72, 721-745. [CrossRef]
- Elmsmari, F.; Ruiz, X.-F.; Miró, Q.; Feijoo-Pato, N.; Durán-Sindreu, F.; Olivieri, J.G. Outcome of partial pulpotomy in cariously exposed posterior permanent teeth: a systematic review and meta-analysis. J Endod 2019, 45, 1296-1306.e1293. [CrossRef]
- Linsuwanont, P.P.; Wimonsutthikul, K.D.D.S.; Pothimoke, U.D.D.S.; Santiwong, B.P. Treatment outcomes of mineral trioxide aggregate pulpotomy in vital permanent teeth with carious pulp exposure: the retrospective study. J Endod 2016, 43, 225-230. [CrossRef]
- Asgary, S.; Eghbal, M.J.; Ghoddusi, J. Two-year results of vital pulp therapy in permanent molars with irreversible pulpitis: an ongoing multicenter randomized clinical trial. Clin Oral Investig 2014, 18, 635-641. [CrossRef]
- Hussain, M.I.; Bashar, A.K.M.; Zakir Hossain Shikder, A.H.M. Alternative management of acute irreversible pulpitis of an adult HIV-positive patient: a case report. Bangladesh Med Res Counc Bull 2021, 47, 230-234. [CrossRef]
- Stashenko, P.; Wang, C.Y.; Riley, E.; Wu, Y.; Ostroff, G.; Niederman, R. Reduction of infection-stimulated periapical bone resorption by the biological response modifier PGG glucan. J Dent Res 1995, 74, 323-330. [CrossRef]
- Langeland, K. Pulp histology and physiology. In Pathways of the Pulp, Cohen, S., Burns, R., Eds.; CV Mosby: St Louis, USA, 1976; pp. 203-290.
- Langeland, K. Tissue response to dental caries. Dent Traumato 1987, 3, 149-171. [CrossRef]
- Kanagasingam, S.; Lim, C.X.; Yong, C.P.; Mannocci, F.; Patel, S. Diagnostic accuracy of periapical radiography and cone beam computed tomography in detecting apical periodontitis using histopathological findings as a reference standard. Int Endod J 2017, 50, 417-426. [CrossRef]
- Hashem, D.; Mannocci, F.; Patel, S.; Manoharan, A.; Brown, J.E.; Watson, T.F.; Banerjee, A. Clinical and radiographic assessment of the efficacy of calcium silicate indirect pulp capping: a randomized controlled clinical trial. J Dent Res 2015, 94, 562-568. [CrossRef]
- Demant, S.; Dabelsteen, S.; Bjørndal, L. A macroscopic and histological analysis of radiographically well-defined deep and extremely deep carious lesions: carious lesion characteristics as indicators of the level of bacterial penetration and pulp response. Int Endod J 2021, 54, 319-330. [CrossRef]
- Ricucci, D.; Siqueira, J.F.; Li, Y.; Tay, F.R. Vital pulp therapy: histopathology and histobacteriology-based guidelines to treat teeth with deep caries and pulp exposure. J Dent 2019, 86, 41-52. [CrossRef]
- Sundqvist, G.; Figdor, D. Life as an endodontic pathogen. Endod Topics 2003, 6, 3-28. [CrossRef]
- Matsuo, T.; Nakanishi, T.; Shimizu, H.; Ebisu, S. A clinical study of direct pulp capping applied to carious-exposed pulps. J Endod 1996, 22, 551-556. [CrossRef]
- Waterhouse, P.J.; Nunn, J.H.; Whitworth, J.M. Prostaglandin E2 and treatment outcome in pulp therapy of primary molars with carious exposures. Int J Paediatr Dent 2002, 12, 116-123. [CrossRef]
- Leong, D.J.X.; Yap, A.U. Vital pulp therapy in carious pulp–exposed permanent teeth: an umbrella review. Clin Oral Investig 2021, 25, 6743-6756. [CrossRef]
- Aguilar, P.M.D.D.S.; Linsuwanont, P.D.D.S.M.P. Vital pulp therapy in vital permanent teeth with cariously exposed pulp: a systematic review. J Endod 2011, 37, 581-587. [CrossRef]
- Hafez, A.A.; Cox, C.F.; Tarim, B.; Otsuki, M.; Akimoto, N. An in vivo evaluation of hemorrhage control using sodium hypochlorite and direct capping with a one- or two-component adhesive system in exposed nonhuman primate pulps. Quintessence Int 2002, 33, 261-272.
- Vostatek, S.F.; Kanellis, M.J.; Weber-Gasparoni, K.; Gregorsok, R.L. Sodium hypochlorite pulpotomies in primary teeth: a retrospective assessment. Pediatr Dent 2011, 33, 327-332.
- Ballal, N.; Duncan, H.F.; Wiedemeier, D.B.; Rai, N.; Jalan, P.; Bhat; Belle, V.S.; Zehnder, M. MMP-9 levels and NaOCl lavage in randomized trial on direct pulp capping. J Dent Res 2021, 2203452110468-220345211046874. [CrossRef]
- Özgür, B.; Uysal, S.; Güngör, H.C. Partial pulpotomy in immature permanent molars after carious exposures using different hemorrhage control and capping materials. Pediatr Dent 2017, 39, 364-370.
- Tunç, E.Ş.; Şaroğlu, I.; Sarı, Ş.; Günhan, Ö. The effect of sodium hypochlorite application on the success of calcium hydroxide pulpotomy in primary teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006, 102, e22-e26. [CrossRef]
- Zanini, M.; Meyer, E.; Simon, S. Pulp inflammation diagnosis from clinical to inflammatory mediators: a systematic review. J Endod 2017, 43, 1033-1051. [CrossRef]
- Al-Ali, M.; Camilleri, J. The scientific management of deep carious lesions in vital teeth using contemporary materials—a narrative review. Front Dent Med 2022, 3. [CrossRef]
- Ballal, V.; Rao, S.; Bagheri, A.; Bhat, V.; Attin, T.; Zehnder, M. MMP-9 in dentinal fluid correlates with caries lesion depth. Caries Res 2017, 51, 460-465. [CrossRef]
- Mente, J.; Petrovic, J.; Gehrig, H.; Rampf, S.; Michel, A.; Schürz, A.; Pfefferle, T.; Saure, D.; Erber, R. A prospective clinical pilot study on the level of matrix metalloproteinase-9 in dental pulpal blood as a marker for the state of inflammation in the pulp tissue. J Endod 2016, 42, 190-197. [CrossRef]
- Trope, M.D.M.D. Regenerative Potential of Dental Pulp. J Endod 2008, 34, S13-S17. [CrossRef]
- Munoz-Sanchez, M.-L.; Linas, N.; Decerle, N.; Nicolas, E.; Hennequin, M.; Cousson, P.-Y. A combination of full pulpotomy and chairside CAD/CAM endocrown to treat teeth with deep carious lesions and pulpitis in a single session: a preliminary study. International Journal of Environmental Research and Public Health 2020, 17, 6340.
- Mente, J.; Hufnagel, S.; Leo, M.; Michel, A.; Gehrig, H.; Panagidis, D.; Saure, D.; Pfefferle, T. Treatment outcome of mineral trioxide aggregate or calcium hydroxide direct pulp capping: long-term results. J Endod 2014, 40, 1746-1751. [CrossRef]
- Tan, S.Y.; Yu, V.S.H.; Lim, K.C.; Tan, B.C.K.; Neo, C.L.J.; Shen, L.; Messer, H.H. Long-term pulpal and restorative outcomes of pulpotomy in mature permanent teeth. J Endod 2020, 46, 383-390. [CrossRef]
- Barthel, C.R.; Rosenkranz, B.; Leuenberg, A.; Roulet, J.-F. Pulp capping of carious exposures: treatment outcome after 5 and 10 years: a retrospective study. J Endod 2000, 26, 525-528. [CrossRef]
- Lim, K.C. Microleakage of intermediate restorative materials. J Endod 1990, 16, 116-118. [CrossRef]
- Tewari, S.; Tewari, S. Assessment of coronal microleakage in intermediately restored endodontic access cavities. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2002, 93, 716-719. [CrossRef]
- Camilleri, J. Scanning electron microscopic evaluation of the material interface of adjacent layers of dental materials. Dent Mater 2011, 27, 870-878. [CrossRef]
- Sluyk, S.; Moon, P.; Hartwell, G. Evaluation of setting properties and retention characteristics of mineral trioxide aggregate when used as a furcation perforation repair material. J Endod 1998, 24, 768-771. [CrossRef]
- Ha, W.N.; Nicholson, T.; Kahler, B.; Walsh, L.J. Methodologies for measuring the setting times of mineral trioxide aggregate and Portland cement products used in dentistry. Acta Biomater Odontol Scand 2016, 2, 25-30. [CrossRef]
- Tsujimoto, M.; Tsujimoto, Y.; Ookubo, A.; Shiraishi, T.; Watanabe, I.; Hayashi, Y. Timing for composite resin placement on mineral trioxide aggregate. J Endod 2013, 39, 1167-1170. [CrossRef]
- Zanini, M.; Hennequin, M.; Cousson, P.Y. Which procedures and materials could be applied for full pulpotomy in permanent mature teeth? a systematic review. Acta Odontol Scand 2019, 77, 541-551. [CrossRef]
- Bjørndal, L.; Simon, S.; Tomson, P.L.; Duncan, H.F. Management of deep caries and the exposed pulp. Int Endod J 2019, 52, 949-973. [CrossRef]
- Delfino, M.M.; Jampani, J.L.d.A.; Lopes, C.S.; Guerreiro-Tanomaru, J.M.; Tanomaru-Filho, M.; Sasso-Cerri, E.; Cerri, P.S. Participation of fibroblast growth factor-1 and interleukin-10 in connective tissue repair following subcutaneous implantation of bioceramic materials in rats. Int Endod J 2023, 56, 385-401. [CrossRef]
- Asgary, S.; Hassanizadeh, R.; Torabzadeh, H.; Eghbal, M.J. Treatment outcomes of 4 vital pulp therapies in mature molars. J Endod 2018, 44, 529-535. [CrossRef]
- Hosseinpour, S.; Gaudin, A.; Peters, O.A. A critical analysis of research methods and experimental models to study biocompatibility of endodontic materials. Int Endod J 2022. [CrossRef]
- Mejare, I.; Hasselgren, G.; Hammarstrom, L.E. Effect of formaldehyde containing drugs on human dental pulp evaluated by enzyme histochemical technique. Scand J Dent Res 1976, 84, 29-36.
- Torabinejad, M.; Parirokh, M. Mineral trioxide aggregate: a comprehensive literature review—part II: leakage and biocompatibility investigations. J Endod 2010, 36, 190-202. [CrossRef]
- Asgary, S.; Eghbal, M.J.; Bagheban, A.A. Long-term outcomes of pulpotomy in permanent teeth with irreversible pulpitis: a multi-center randomized controlled trial. Am J Dent 2017, 30, 151-155.
- Chueh, L.H.; Chiang, C.P. Histology of Irreversible pulpitis premolars treated with mineral trioxide aggregate pulpotomy. Oper Dent 2010, 35, 370-374. [CrossRef]
- McCabe, P.S.; Dummer, P.M.H. Pulp canal obliteration: an endodontic diagnosis and treatment challenge. Int Endod J 2012, 45, 177-197. [CrossRef]
- Jacobsen, I.; Kerekes, K. Long-term prognosis of traumatized permanent anterior teeth showing calcifying processes in the pulp cavity. Scand J Dent Res 1977, 85, 588-598. [CrossRef]
- Robertson, A.; Andreasen, F.M.; Bergenholtz, G.; Andreasen, J.O.; Norén, J.G. Incidence of pulp necrosis subsequent to pulp canal obliteration from trauma of permanent incisors. J Endod 1996, 22, 557-560. [CrossRef]
- Tronstad, L. Root resorption - etiology, terminology and clinical manifestations. Dent Traumato 1988, 4, 241-252. [CrossRef]
- Felman, D.; Parashos, P. Coronal tooth discoloration and white mineral trioxide aggregate. J Endod 2013, 39, 484-487. [CrossRef]
- Camilleri, J. Color stability of white mineral trioxide aggregate in contact with hypochlorite solution. J Endod 2014, 40, 436-440. [CrossRef]
- Taha, N.A.; Al-Rawash, M.H.; Imran, Z.A. Outcome of full pulpotomy in mature permanent molars using 3 calcium silicate-based materials: A parallel, double blind, randomized controlled trial. Int Endod J 2022, 55, 416-429. [CrossRef]
- Aravind, A.; R, R.; Sharma, R.; Rana, A.; Sharma, S.; Kumar, V.; Chawla, A.; Logani, A. Response to pulp sensibility tests after full pulpotomy in permanent mandibular teeth with symptomatic irreversible pulpitis: a retrospective data analysis. J Endod 2022, 48, 80-86. [CrossRef]
Figure 1.
PRISMA flowchart
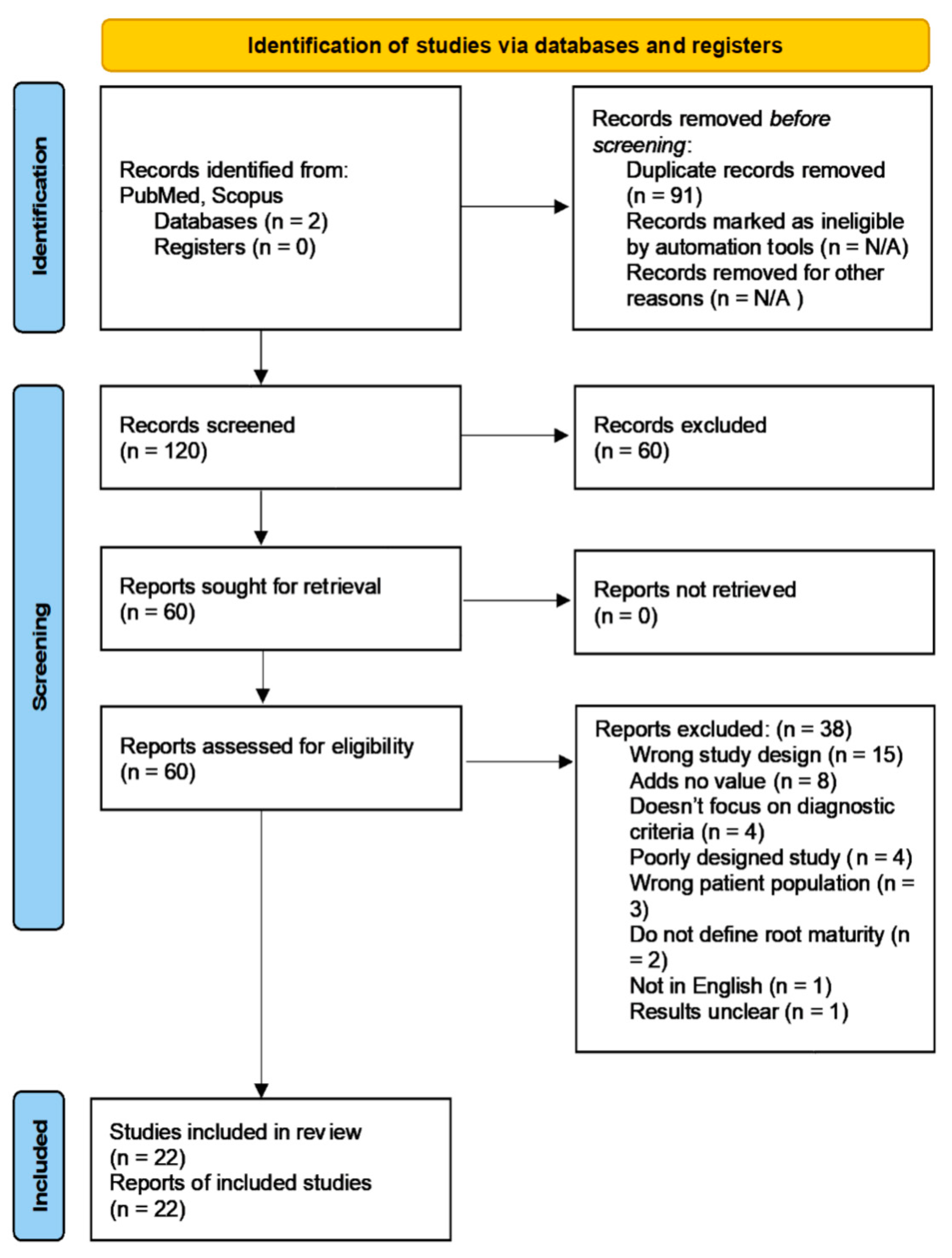
Figure 2.
Reprinted with permission from Operative Dentistry. Microphotographs of hematoxylin and eosin-stained tissue sections of tooth #29 (45 in FDI numbering). 2A: Low-power (original magnification 10x) microphotograph showing a thin reparative dentin bridge below MTA and no inflammation in the underlying residual pulp tissue. A short segment of superficial odontoblastic layer just below the dentin bridge was destroyed. However, the deeper odontoblastic layer was intact. 2B: High-power (original magnification 50x) microphotograph revealing no inflammation and a small focus of dystrophic calcification (arrow) in the underlying residual pulp tissue. 2C: Low-power (original magnification 10x) microphotograph of a deeper tissue section showing a thicker reparative dentin bridge below MTA and the nearly normal underlying residual pulp tissue. 2D: High-power (original magnification 50x) microphotograph exhibiting the reparative dentin bridge that made up of osteodentin and no inflammation in the underlying residual pulp tissue. From Chueh and Chiang [116], reprinted with permission.
Figure 2.
Reprinted with permission from Operative Dentistry. Microphotographs of hematoxylin and eosin-stained tissue sections of tooth #29 (45 in FDI numbering). 2A: Low-power (original magnification 10x) microphotograph showing a thin reparative dentin bridge below MTA and no inflammation in the underlying residual pulp tissue. A short segment of superficial odontoblastic layer just below the dentin bridge was destroyed. However, the deeper odontoblastic layer was intact. 2B: High-power (original magnification 50x) microphotograph revealing no inflammation and a small focus of dystrophic calcification (arrow) in the underlying residual pulp tissue. 2C: Low-power (original magnification 10x) microphotograph of a deeper tissue section showing a thicker reparative dentin bridge below MTA and the nearly normal underlying residual pulp tissue. 2D: High-power (original magnification 50x) microphotograph exhibiting the reparative dentin bridge that made up of osteodentin and no inflammation in the underlying residual pulp tissue. From Chueh and Chiang [116], reprinted with permission.
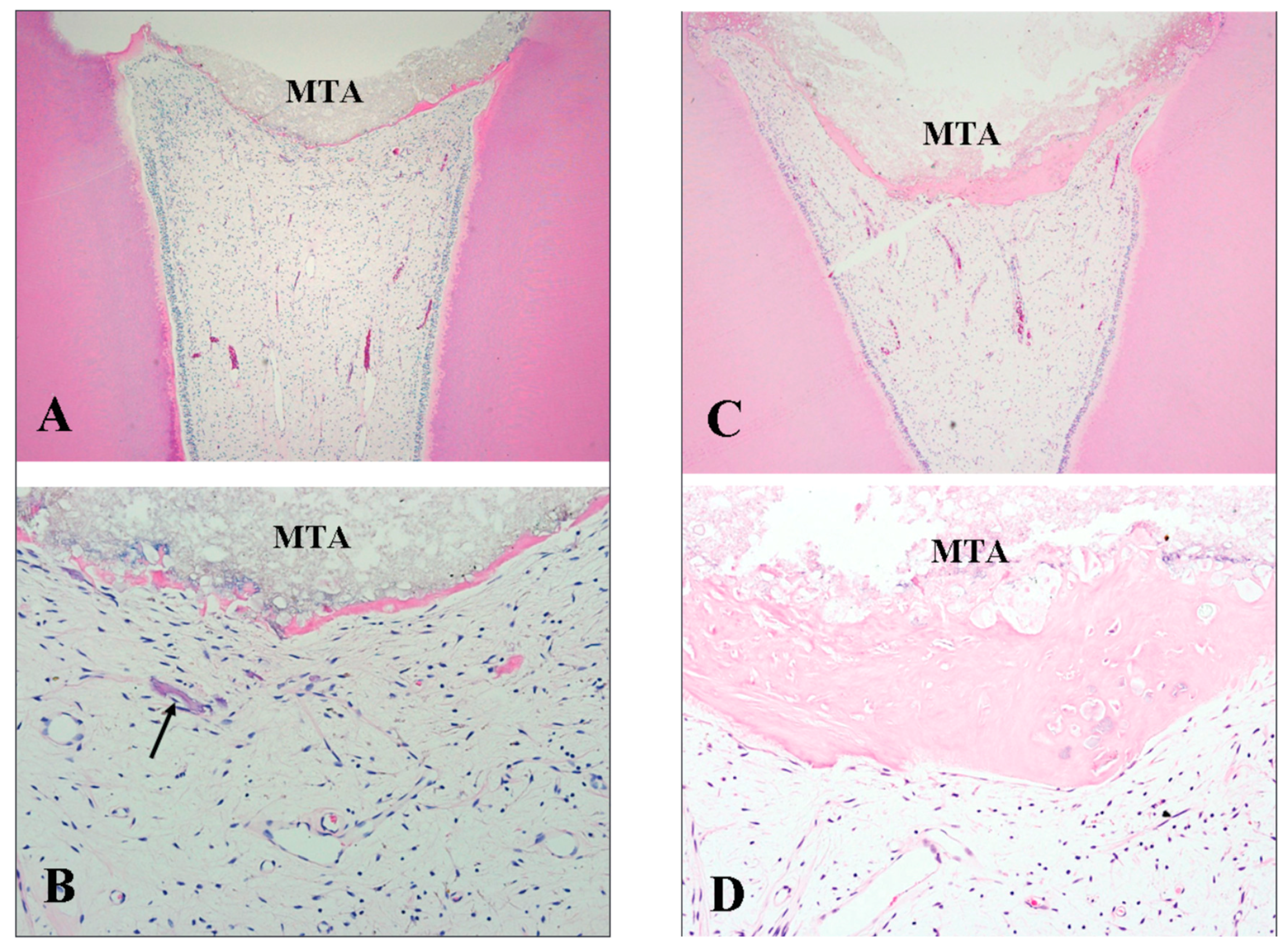
Table 1.
Wolters’ proposed classification of pulpitis adapted from [28].
Table 1.
Wolters’ proposed classification of pulpitis adapted from [28].
| Diagnosis | Signs and Symptoms | Recommended Management |
|---|---|---|
| Initial pulpitis | Heightened but not lengthened response to cold, no tenderness to percussion and no spontaneous pain. | Indirect pulp capping |
| Mild pulpitis | Heightened and lengthened reaction to cold, warm or sweet that lasts no longer than 20 seconds. The tooth may or may not be tender to percussion. | Indirect pulp capping |
| Moderate pulpitis | Heightened and prolonged reaction to cold that lasts for longer than 20 seconds. The tooth may or may not have tenderness to percussion. Spontaneous dull pain can be suppressed by simple analgesics. | Coronal or partial pulpotomy |
| Severe pulpitis | Severe spontaneous pain with hot and cold, sharp or dull throbbing pain that is usually worse when lying down. The tooth is tender to percussion and palpation. | Coronal pulpotomy (note that pulpectomy is indicated if hemostasis cannot be achieved, or no bleeding is noted from one or more of the canals) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



