Submitted:
30 October 2023
Posted:
31 October 2023
You are already at the latest version
Abstract
Metabolic syndrome is a growing global health problem. Evidence suggests that diets rich in phytochemical-containing herbs and spices can contribute to reduced risk of chronic disease. This review assesses the scope of evidence supporting the use of herbs and spices in the diet for prevention or treatment of metabolic syndrome and associated health conditions.
A search of PubMed and Scopus databases was carried out to assess the available clinical or cohort evidence for culinary doses of commonly used herbs and spices. Trials that were measuring health factors related to metabolic disorders or the health of individuals with metabolic syndrome or associated diseases were included.
Out of a total of 1742 papers identified, there were 146 relevant studies on black pepper, chilli, cardamom, cinnamon, coriander, cumin, fennel, fenugreek, garlic, ginger, Nigella seed, rosemary, sage and turmeric. No relevant research was found for cloves, mint, oregano, parsley or thyme. Cinnamon, fenugreek and ginger were the herbs/spices with the most published trials on them and showed promise for glycaemic control. Cardamom appears to have potential to reduce inflammatory markers, and cinnamon, ginger and turmeric for blood lipids. Patients with type 2 diabetes were the population most likely to be included in studies, but the preventative benefits of herbs/spices in healthy populations were also investigated, particularly for chilli, ginger and cinnamon. There is evidence for the beneficial effect of culinary doses of many common herbs/spices in the prevention and treatment of metabolic syndrome and associated disorders.
Keywords:
diabetes
; herbs and spices
; metabolic syndrome
; nutrition
; phytochemicals
; preventative health
1. Introduction
Metabolic syndrome and associated conditions such as obesity, diabetes and cardiovascular disease are a growing global health problem. Between 2000 and 2019, global diabetes rates grew by more than 1.5% annually and prevalence rates for all other metabolic diseases also increased [1]. Poor diet and physical inactivity are risk factors for the development of metabolic syndrome and lifestyle changes are key for treatment [2].
Research indicates that the inclusion of herbs and spices in the diet, as is often the case in Mediterranean and Asian diets, may contribute to positive long-term health outcomes [3, 4]. Herbs and spices are a particularly rich source of phytochemicals and consumption of diets rich in phytochemicals have been linked with reduced risk of cardiometabolic disease and obesity [5, 6].
Many studies looking at the health benefits of herbs and spices use high-dose extracts; however, these do not reflect the main way that the general public might be able to take advantage of relatively cheap additions to the diet. Are these more expensive high-dose formulations necessary for everyone to benefit from herbs and spices, or do culinary doses provide benefit too?
Some research has begun to investigate this question. Clinical studies using herb and spice mixes to improve physiological responses to food have indicated that inclusion of herbs/spices in the diet may have preventative or therapeutic benefits [7-15]. The spice mixes used in these studies ranged in dose from 6g to 23.5g and positively impacted vascular function, blood glucose and insulin and blood lipids following meals. However, the reasons for the specific herb/spice mixes chosen and doses used were often not explained. There is no consensus on whether dose matters for effect. Doses of 6g of Italian herb mixes [8], 23.5g of Asian spices [11] or a combination of Mediterranean herbs and Asian spices at doses of 14.5g [10] and between 0.5 and 6.6g [13, 14] have been found to have benefit. The lack of consistency in herb/spice mix formulation makes it challenging to attribute benefits to a particular herb/spice, combination of herb/spices or dose.
Zanzer et al assessed the effect of concentrated liquid extracts of individual spices but standardized to equal polyphenol content, enabling the different effects from each spice to be elucidated [15]. The dose of polyphenols provided from each extract corresponded to the amount found in 6g of cinnamon. Cinnamon and turmeric positively impacted on blood sugar levels, and turmeric reduced appetite, however, ginger and star anise did not have any effect. Therefore, individual effects from different herbs needs to be clarified.
The purpose of a scoping review is to highlight a body of evidence, explore how it has been reported on and identify evidence gaps [16]. It can also be used to inform development of future systematic reviews [17]. The many different types of evidence available for the health benefits of herbs/spices mean that identifying clear patterns in the research is challenging.
Therefore, the aim of this review was to assess the clinical evidence available for the metabolic health benefits of culinary doses of a range of common herbs and spices and to investigate whether there was consistency in the doses used and outcomes found. The most promising herbs and spices in the diet for specific health outcomes or populations can be identified, as well as what future clinical research is needed to confirm this effect.
2. Materials and Methods
A number of previous reviews have identified herbs/spices with evidence of benefit in health generally and metabolic syndrome and associated disorders more specifically [2, 3, 18-24]. These were assessed to determine a list of herbs/spices that were most likely to have adequate evidence for this scoping review: black pepper (Piper nigrum L.), cardamom (Elletaria cardamomum (L.) Maton), chilli (Capsicum frutescens L.), cinnamon (Cinnamomum sp), cloves (Syzygium aromaticum (L.) Merr. & L.M.Perry), cumin (Cuminum cyminum L.), fennel (Foeniculum vulgare Mill.), fenugreek (Trigonella foenum-graecum L.), garlic (Allium sativum L.), ginger (Zingiber officinale Roscoe), mint (Mentha sp), Nigella seed (Nigella sativa L.), oregano (Origanum vulgare L.), parsley (Petroselinum crispum (Mill.) Fuss), rosemary (Salvia rosmarinus Spenn.), sage (Salvia officinalis L.), thyme (Thymus vulgaris L.) and turmeric (Curcuma longa L.). A scoping review methodology was then used, referring to the preferred reporting items for systematic reviews and meta-analyses extension for scoping reviews [25].
2.1. Search strategy
The PICO (population, intervention, comparison, outcome) strategy was used to formulate search terms. The research question was: do herbs and spices affect symptoms of metabolic syndrome in healthy or relevant diseased populations. Population was healthy individuals or those with metabolic syndrome and related disorders. Intervention was single herbs or spices at culinary doses. Comparison was a control or no treatment. Outcome was a change in metabolic syndrome symptoms or a change in metabolic biomarkers: blood glucose, lipids, insulin or inflammatory markers. PubMed and Scopus were searched in January 2023 with no date restrictions applied. A search of PubMed database was carried out using the search terms: (“black pepper" or "Piper nigrum" or "black seed" or "black cumin" or "Nigella sativa" or cardamom or "Elettaria cardamomum" or chilli or "Capsicum frutescens" or cinnamon or "Cinnamomum zeylanicum" or cloves or "Syzygium aromaticum" or coriander or "Coriandrum sativum" or cumin or "Cuminum cyminum" or fennel or "Foeniculum vulgare" or fenugreek or "Trigonella foenum-graecum" or garlic or "Allium sativum" or ginger or "Zingiber officinale" or mint or "Mentha" or oregano or "Origanum vulgare" or parsley or "Petroselinum crispum" or rosemary or "Rosmarinus officinalis" or sage or "Salvia officinalis" or thyme or "Thymus vulgaris" or turmeric or "Curcuma longa") AND (metabol* or diabetes or obesity or cardiovascular or "blood glucose" or "blood sugar" or "blood lipids" or "blood fats" or "blood insulin"). The results were filtered by Clinical Trial as article type. Each herb/spice was searched for separately in Scopus, with the following search term: TITLE-ABS-KEY ({herb/spice name}) AND TITLE-ABS-KEY (metabolic OR metabolism OR diabetes OR obesity OR cardiovascular) AND TITLE (clinical OR human). Additional studies were found using Google scholar and hand searching reference lists from relevant reviews.
2.2. Inclusion and exclusion criteria
The inclusion criteria were use of whole herb/spice or powdered/ground herb/spice in food, drinks or encapsulated and at doses that could reasonably be achieved in the diet without negatively impacting palatability. Concentrated extracts or oils and combinations of herbs or spices were excluded. Studies of water infusions or herbal teas were included when the formulation and quantity was what might be reasonably consumed at home. Any studies that administered herbal formulations or more than one herb/spice at a time were excluded, however, those with multiple individual herbs/spices being investigated in separate arms of the study were included. To ensure a broad range of different studies, clinical or cohort trials that were measuring health factors related to metabolic disorder or the health of individuals with metabolic disease or related conditions were included. Studies were included regardless of the age or health status of participants, as the intention was to determine the potential for herbs and spices to both prevent and treat metabolic disease. However, if the participants had a co-morbidity not related to metabolic syndrome the study was excluded. Studies were included regardless of language. Any retrieved studies not in English were translated using Google Translate. Animal and in vitro studies were excluded. Reviews were excluded.
2.3. Study selection and data collection
The articles identified from title and abstract screening were added into a Microsoft Excel spreadsheet, the papers retrieved, and final inclusion decisions made by reading the full text. Two reviewers (MM and VR) screened this list to decide on the final included studies. For each article, the following data were entered into the spreadsheet: study type, herb/spice investigated, population, dose of herb/spice, length of study and outcome measures. The evidence for each herb/spice was clustered into type of metabolic health measurement investigated, and whether there were positive findings or not. The Jadad Scale was used to score the methodological quality of the clinical trials. The Jadad scale was originally developed for assessing clinical trials in pain research, but has been widely adapted and is considered to offer the best validity and reliability evidence [26]. One point is scored for each of the following: a mention of randomization; description of an appropriate randomization method; mention of blinding; description of appropriate blinding method; and, all participants in the trial being accounted for in the results. Trials that scored 0 – 2 were considered low quality and those scoring 3 – 5 were considered high quality.
3. Results
The PubMed search identified 792 results while the Scopus search produced 925 results. An additional 25 papers were found from Google Scholar and reference list scanning. Title and abstract screening led to 258 papers for full text screening. This led to a total of 146 relevant papers for data extraction (Figure 1).
Evidence was found for black pepper, chilli, cardamom, cinnamon, cloves, coriander, cumin, fennel, fenugreek, garlic, ginger, Nigella seed, rosemary, sage and turmeric. No relevant research was found for mint, oregano, parsley or thyme. Table 1 summarises the included studies. The rationale behind studies excluded at full text screen is shown in Supplementary Table 1.
3.1. Black pepper
There was one single-blind cross-over trial on black pepper in healthy adults. A dose of 1.3g added to a meal had no impact on appetite or thermogenesis [27].
3.2. Cardamom
Ten studies (9 double-blind RCTs and one clinical study) looked at the impact of cardamom on inflammation and a range of metabolic markers in individuals with hypertension [28], diabetes [29-31], prediabetes [32], poly-cystic ovarian syndrome (PCOS) [33, 34] and non-alcoholic fatty liver disease (NAFLD) [35, 36]. All the studies on cardamom used 3g/day for between 8 and 20 weeks. Five out of six studies that investigated inflammatory markers found positive effects [31-34, 36, 37], two studies found benefits on blood glucose and insulin, two studies found no benefit from cardamom on blood lipids, while effects on blood pressure were variable.
There were more trials with positive findings than an absence of effect in the three main metabolic health markers. The strongest research area was inflammatory markers, with five studies finding a beneficial effect and no studies indicating a lack of effect.
3.3. Chilli
Eleven clinical studies [9, 38-47] and two prospective cohort studies [48, 49] investigated the effects of chilli on appetite, vascular function, and blood glucose, insulin and lipids. Apart from one study looking at the effect of chilli on glucose and insulin in pregnant women with gestational diabetes [47], all the included studies were in healthy individuals.
Four of the intervention studies used doses of 30g of fresh chilli [38-40, 42], the other seven intervention studies used doses of 0.6g [46], 1.25g [47], 3.09g [43, 44], 5g [41] a meal with chilli containing 5.82mg of capsaicinoids [9] or chilli capsules containing 10mg of capsaicinoids [45].
Appetite and/or thermogenesis or metabolic rate were measured in eight out of thirteen of the studies and five of these found a beneficial effect. There were as many studies finding positive results as those showing no effect for the key metabolic biomarkers of blood glucose, insulin and lipids (see Figure 2).
One cross-over study found an improvement in diet-induced thermogenesis [42] one single-blind cross-over study found increased metabolic rate [43] and one single-blind cross-over study found decreased appetite from chilli [44], however, four studies found no effect on metabolic rate or energy intake [9, 40, 45, 46]. Chilli was associated with increased energy intake, but lower incidence of being overweight/obese in one prospective cohort study [48]. A second cohort study found an inverse relationship between chilli consumption and hypertension [49]. Reduction in insulin was found in three studies [9, 39, 47], while an increase was found in one [41]. There was no change in blood glucose levels from two randomized cross-over studies [38, 40], while one double-blind RCT [47] and one clinical study [41] found significant reduction in glucose from chilli consumption. The quality of the clinical studies was generally low [8 low and 3 high according to Jadad scores], mainly due to the difficulty in blinding consumption of chilli in food.
3.4. Cinnamon
There were 41 studies looking at the benefits of culinary doses of cinnamon. Ten in healthy individuals [50-59], nineteen in those with diabetes [60-78], six in women with PCOS [79-84], one in Asian Indians with metabolic syndrome [85], one in patients with NAFLD [86], one in individuals with impaired glucose tolerance [87], one in sedentary women with obesity [88], one in women with dyslipidaemia [89], and one in prediabetic individuals [90]. Doses ranged from 1 to 6g; either as a single dose or daily for between 2 weeks and 6 months. Whether a positive effect was seen or not did not appear to correlate with dosage.
Beneficial effects on glucose were found in 6 randomized cross-over studies, 1 randomized trial and 10 double-blind RCTs from doses of 0.5-6g/day, 100ml of cinnamon tea or single doses of 5-6g of cinnamon [50-52, 54, 56, 58, 59, 66-68, 70, 71, 78, 80, 85, 86, 88], while 7 double-blind RCTs, 3 single-blind RCTs and one randomized cross-over study found no effect from a single dose of 1-6g or 1-1.5g/day [53, 63, 72-74, 76, 77, 82, 84, 87, 90].
Beneficial effects on insulin were found in 4 randomized cross-over studies, 10 double-blind RCTs and 1 single-blind RCT from doses of 1-3g/day or single doses of 3-6g of cinnamon [50, 53, 58-60, 64, 67, 70, 76, 78, 80-82, 85, 86], while 6 double-blind RCTs, 1 single-blind RCT and 1 randomized cross-over study found no effect from doses of 1-1.5g/day or a single dose of 6g [53, 61, 71, 72, 74, 77, 87, 90].
3.5. Coriander seed
One single-blind RCT found that 2g/day of coriander seeds for 40 days improved average body mass index (BMI) from 27.3 to 26.7 and blood lipids (total cholesterol, low-density lipoprotein (LDL) and high-density lipoprotein (HDL)), as well as systolic blood pressure in patients with hyperlipidaemia [91].
3.6. Cumin
Two clinical studies looked at the benefit of cumin on anthropometric measures, blood insulin and blood lipid levels in overweight adults [92] and women with dyslipidaemia [89]. The randomized clinical trial by Zare et al used a dose of 6g/day for 3 months and this reduced all blood lipid measurements, as well as anthropometric measurements of weight, body mass index (BMI), waist circumference and fat [92], while Pishdad et al used 3g/day for 8 weeks in a double-blind RCT and found a benefit on total cholesterol, but not LDL or HDL cholesterol [89].
3.7. Fennel
One single-blind crossover study found that a single dose of 2g of fennel as a tea decreased appetite in healthy women, but did not impact food consumption [93].
3.8. Fenugreek
There were twenty studies looking at fenugreek, mainly for its impact on blood glucose, insulin and lipids, in healthy individuals [93- 96], diabetics [97-110], individuals with coronary artery disease [111] and adults with hyperlipidaemia/hypercholesterolaemia [112, 113]. Quantities ranged from 2g up to 100g, with the majority of studies using 10-15g/day. Effects on blood insulin, glucose and lipids were promising, with 11 out of 14 studies showing significant positive effects on blood glucose, 7 out of 8 studies finding significant changes in insulin and 6 out of 8 studies significantly improving blood lipids, regardless of dose used. However, excluding low-quality studies reduced the number of studies indicating a benefit on blood glucose (to 4 out of 5 studies) and blood lipid levels (to 1 out of 2 studies).
3.9. Garlic
There were ten clinical studies (4 double-blind RCTs and 6 single-blind or randomized clinical studies) and two cohort studies looking at the benefits of garlic. The two cohort studies investigated the long-term correlation between garlic intake and hypertension, and both found inverse associations [114, 115]. Both clinical trials that looked at the effect of garlic on blood pressure (BP) found benefit when participants consumed 20g or 100mg/kg bodyweight of fresh garlic daily [116, 117]. Most of the studies investigated the impact of garlic on blood lipids. One clinical study was carried out in overweight smokers [118]. Four clinical studies looked at platelet function [119], cholesterol [120, 121], immunity and cancer markers [122] in healthy individuals. Two studies looked at multiple outcomes in patients with metabolic syndrome [117, 123], one study investigated NAFLD [124] and two studies looked at individuals with hyperlipidaemia [91, 116]. For the interventional studies, doses ranged from 1.6g to 40g, with higher doses of fresh garlic compared with dried garlic powder. All but two of the clinical studies looked at blood lipids and seven out of eight found a benefit. Fresh garlic in doses of 100mg/kg body weight, 20g or 40g/day significantly reduced triglycerides in three studies [116, 117, 120], while two studies found that 1.6g/day of dried garlic reduced triglycerides [123, 125]. Total cholesterol was significantly reduced by 1.6, 2 or 3g/day dried garlic and 20g or 40g of fresh garlic [91, 116, 120, 121, 125]. Only one study of overweight participants at risk of cardiovascular disease found no impact of 2.1g of garlic on blood lipids [118].
3.10. Ginger
Out of a total of 24 studies on ginger, six were carried out on healthy individuals to look at blood clotting [126], energy intake and appetite [27], thermoregulatory function or thermogenesis and appetite [127, 128], anthropometric measurements [129, 130], anthropometric measurements and blood glucose and fats [131], and cardiovascular risk factors [111]. There were 11 studies on patients with type 2 diabetes looking at the impact of ginger on blood sugar, insulin and blood lipids [132-134], metabolic health and inflammation [135, 136], fasting blood glucose and insulin sensitivity [137, 138], blood glucose, insulin and inflammation [139], vascular function [140], anthropometric measurements and blood pressure [62], and anthropometric measurements and inflammation [141]. One study looked at the effects of 1.5g of ginger on anthropometric measurements and insulin resistance in women with PCOS [81]. One study looked at the effect of 3g/day on blood lipids in individuals with hyperlipidaemia [142]. Two studies looked at the impact of ginger on liver function, anthropometric measurements, blood sugar and inflammatory markers in individuals with NAFLD [143, 144]. One looked at the impact of 1g of ginger daily in obese children with NAFLD [143], while in the other study, adults were given 1.5g/day [144]. A pilot study investigated the impact of 1g/day of ginger on thyroid symptom score, anthropometric measurements, blood glucose and blood lipids in hypothyroid patients [145].
Ginger was used in doses that ranged from 1g to 10g of dried powdered ginger for a single dose or up to 12 weeks daily; apart from one study that used 15g of fresh ginger or 40g of cooked ginger [126] and another study using 20g of fresh ginger [27]. There did not appear to be a correlation between dose and efficacy. All seven studies that investigated the impact of ginger (doses of 1.5 - 3g/day) on insulin found a benefit, ten out of 12 found positive effects on blood glucose (doses of 1.2 - 3g/day), six out of seven found a positive effect on blood lipids, such as total cholesterol, LDL and triglycerides (doses of 1 - 3g) and four out of five studies looking at inflammatory markers (doses of 1.5 - 3g) found a benefit. The studies were mainly of high quality (22 out of 24) according to Jadad scoring, with 18 double-blind RCTs, three randomized cross-over studies and three placebo-controlled study.
3.11. Nigella seeds
There were 17 studies on Nigella seeds, mainly investigating their effect on anthropometric measurements, blood glucose, insulin and lipids. One double-blind RCT was carried out on healthy male volunteers [146]. A large double-blind RCT looked at the impact of 1.5g/day of Nigella seeds in 250 healthy men with metabolic syndrome [147]. One double-blind RCT was carried out on men with obesity [148]. Two studies were carried out with thyroiditis patients [149, 150], four in individuals with metabolic syndrome [151-154], three in patients with hyperlipidemia/hypercholesterolaemia [155-157], three in patients with type 2 diabetes [158-160], and two in patients with NAFLD [161, 162]. The studies on Nigella seeds used between 500mg and 3g/day for durations ranging from 4 weeks to one year.
Nigella seeds improved anthropometric measurements such as BMI and weight in three out of seven studies that included them (at doses of 2 -3g/day), improved blood glucose in five out of ten studies (at doses of 500mg – 2g/day), insulin (at 2g/day) in three out of four studies, blood lipids in seven out of 11 studies (at 500mg - 2g/day) and inflammatory markers in one out of four studies (at a dose of 2g/day). Of the 17 studies, 13 were high-quality according to Jadad.
3.12. Rosemary
The one high-quality, double-blind RCT on rosemary found no impact on liver enzymes, anthropometric measurements, fasting blood glucose, insulin and blood lipids from 4g/day for 8 weeks in patients with NAFLD [163].
3.13. Sage
One low-quality, non-randomized cross-over study found that drinking 600ml of sage tea daily for 4 weeks improved lipid profile but had no effect on blood glucose in healthy female volunteers aged 40-50 years [164].
3.14. Turmeric
Four out of the eleven studies on turmeric looked at patients with type 2 diabetes [165-168]. One turmeric study was carried out on healthy volunteers to investigate glycaemic effect [169]. Three other studies were carried out on individuals who were stated to be overweight, obese or prediabetic, with no other health issues [90, 170, 171]. Two studies looked at the effect of turmeric on NAFLD [172, 173]. The studies used between 1 and 3g/day for between 4 and 12 weeks, or single doses of 1g [90] and 6g [170].
All studies were high quality according to Jadad. Three out of five studies investigating anthropometric measurements such as weight and BMI found some positive effect from turmeric (at a dose of 2.1g/day). Four out of seven studies found improvements in blood glucose levels (at doses of 2.1 - 2g/day), one out of two studies found improvements in insulin (from a dose of 2g/day) and five out of six studies found improvements in blood lipids such as triglycerides, total cholesterol and LDL (at doses of 2.1 – 2.4g/day). Out of three studies looking at inflammatory markers, two found beneficial effects from 2.1-2.4g/day of turmeric powder in capsules.
3.15. Herb/spice efficacy
Figure 2 identifies the main health markers measured and whether effects were seen for each of the herbs and spices in all studies and only in high-quality studies. Blood glucose and insulin were the most commonly measured markers, followed by blood lipids, then inflammatory markers. Only including high-quality studies did not make a big difference to the pattern of responses seen for glucose, insulin or inflammatory markers. However, the benefits of fenugreek and garlic on blood lipids were not apparent when only high-quality studies were considered.
Figure 2 identifies the main health markers measured and whether effects were seen for each of the herbs and spices in all studies and only in high-quality studies: (a) Number of studies showing an effect or lack of effect for each of the herbs and spices on blood glucose; (b) Number of high-quality studies showing an effect or lack of effect for each of the herbs and spices on blood glucose; (c) Number of studies showing an effect or lack of effect for each of the herbs and spices on insulin; (d) Number of high-quality studies showing an effect or lack of effect for each of the herbs and spices on insulin; (e) Number of studies showing an effect or lack of effect for each of the herbs and spices on blood lipids; (f) Number of high-quality studies showing an effect or lack of effect for each of the herbs and spices on blood lipids; (g) Number of studies showing an effect or lack of effect for each of the herbs and spices on inflammatory markers; (h) Number of high-quality studies showing an effect or lack of effect for each of the herbs and spices on inflammatory markers.
3.16. Adverse effects
No adverse effects were reported for any of the studies at the doses used.
3.17. Study quality
Studies were scored for quality using Jadad (details on the scores given are provided in Supplementary Table 2). There were 40 low-quality studies (28% of the scored studies), 97 high quality studies (66% of the scored studies), four studies for which there was not enough information to score them and five cohort or observational studies for which quality could not be assessed using the Jadad criteria. Of the 146 studies, 81 were double-blind RCTs, 30 were cross-over clinical studies, 30 were single-blind or parallel clinical studies, two were prospective cohort studies, one was a retrospective cohort study and two were cross-sectional observational studies.
4. Discussion
The aim of this scoping review was to assess the clinical evidence available for culinary doses of herbs and spices, what doses are used and in which health conditions, with a view to identifying areas that need further research. In this review, there were a total of 146 studies looking at the effects of black pepper, chilli, cardamom, cinnamon, cloves, coriander, cumin, fennel, fenugreek, garlic, ginger, Nigella seed, rosemary, sage and turmeric on metabolic health. Cinnamon, fenugreek and ginger showed the most promise on control of blood glucose and insulin. Cinnamon, ginger, Nigella seed and turmeric were most promising for beneficial effects on blood lipid levels. Cardamom, ginger and turmeric showed promise for reducing systemic inflammation due to a decrease in inflammatory markers.
Some herbs/spices were more likely to be researched in a specific population or in an investigation of a specific metabolic biomarker. This either indicates increased efficacy or traditional associations and observations stimulating more research in these areas. Findings from in vitro studies or in vivo animal research may also have prompted researchers to focus on a particular herb and effect. For example, despite not having a traditional association with inflammation, anti-inflammatory effects of cardamom have been found in an animal model [175].
Cardamom was only investigated in individuals with disease associated with metabolic syndrome and no studies were carried out in healthy individuals. Most studies investigated the impact of cardamom on inflammatory markers. Metabolic syndrome involves increased inflammation, therefore, changes in inflammatory markers are more likely to be observed in those with metabolic syndrome than healthy individuals. Preclinical research has identified the potential of cardamom to be of use in inflammation and hyperlipidaemia. Cardamom reduced swelling and downregulated inflammatory cytokines such as cyclo-oxygenase-2 (COX-2) in an animal model [175]. This confirms the finding in this scoping review that cardamom has anti-inflammatory activity. A terpenoid compound from cardamom, 1,8-cineole, prevented lipid oxidation in vitro and lowered serum lipid levels in zebrafish, while cardamom oil at a dose of 3g/kg reduced total cholesterol, LDL-cholesterol and triglycerides in Wistar rats [176]. This scoping review did not identify any clinical studies showing a beneficial effect of cardamom on blood lipids, which may reflect a failure of animal studies to relate to effects in humans, or be due to the difference in dose or formulation.
Almost all the studies of chilli were carried out in healthy individuals. Chilli did not have marked effects on the main insulin, glucose, lipids and inflammatory biomarkers, which may reflect the use of healthy populations for most studies, the doses used or difficulty in blinding chilli consumption in food. It showed more promise for impacting thermogenesis, metabolic rate and appetite. The key active compound in chilli is capsaicin and this binds to transient receptor potential vanilloid receptor 1 (TRPV1) to activate metabolic modulators such as peroxisome proliferator activated receptor (PPAR)α and glucagon-like peptide (GLP)1 (177). Capsaicin has also been found to decrease ghrelin secretion [177], which would explain its appetite-suppressing effects.
The majority of studies of cinnamon were carried out in patients with diabetes, indicating the strong association of this spice with blood sugar control [eg, 178, 179, 180]. This impact on blood sugar is thought to be due to an insulin-mimetic effect and via inhibition of digestive enzymes such as α-amylase in the gastrointestinal tract [178, 180]. Cinnamon activates both PPARα and PPARγ, which would explain an effect on glycaemia [181]. However, there was considerable heterogeneity in the effect of cinnamon on blood sugar and blood insulin across the different studies in this review. Cinnamon was more likely to positively impact blood sugar and insulin in healthy individuals than those with type 2 diabetes. Seven out of nine studies (77%) looking at the impact of cinnamon on blood sugar in healthy individuals found a benefit, while only seven out of fifteen studies (47%) looking at the impact of cinnamon on blood sugar in diabetic patients found a benefit. This suggests that it could be of preventative and therapeutic benefit, however, due to the heterogeneity of the results, systematic reviews isolating the impact of dose and health of the participants on outcomes would be interesting. There are a number of meta-analyses of cinnamon in diabetes [178, 181-188]; however, there did not appear to be any assessing blood glucose control in healthy individuals.
The effects on blood sugar, insulin and lipids from cinnamon appeared to be quite mixed from both this scoping review and published meta-analyses. Well-researched areas, such as is found with cinnamon, often highlight heterogenous results. This indicates that further research is needed to separate out the factors that impact on efficacy, such as dose, presence in a food matrix, population or duration of study. Yu et al found that dosage did impact on efficacy, with a dose of less than 1.2g significantly reducing fasting blood glucose, when pooled results found no benefit [181]. There have been at least eight meta-analyses of clinical trials of cinnamon looking at LDL-cholesterol. Six found decreases in LDL-cholesterol [181, 182, 186, 189-191], but two found no impact on LDL-cholesterol [192, 193]. Yu et al found that the effect of cinnamon on LDL-C was influenced by dose [181], which may explain some of the heterogeneity.
Fennel has been used traditionally for its digestive properties [194], but it has also been found to have anti-inflammatory and antihyperlipidaemic activity [20]. Bae et al found that fennel did not impact food consumption, however, it did reduce appetite, indicating that further research might be beneficial [93].
The impact of fenugreek was investigated in patients with diabetes in 14 studies and healthy individuals in six studies. The effects on blood glucose and insulin were mainly positive whether in a healthy or diseased population, however, high-quality studies were less likely to find benefit. Larger doses of fenugreek tended to be used, as the beneficial effect was usually considered to be from the soluble fibre in the seeds [195], although some studies suggest an effect of other compounds such as flavonoids, saponins and the alkaloid trigonelline [196, 197]. As a relatively mild-flavoured spice, larger amounts are palatable in the diet. The studies using larger quantities incorporated the seed powder into a food matrix, such as being baked into bread, therefore they were considered culinary doses and included.
Nine meta-analyses on fenugreek in metabolic syndrome or associated conditions have been published in the last ten years [195-203]. All of those that assessed effects on blood glucose found a benefit, but concerns were raised about the quality of the clinical trials. A review of fenugreek in blood pressure found a dose-dependent effect; with doses greater than 15g/day for longer than 12 weeks being effective [198]. Neelakantan et al also found that dose impacted on the effect of fenugreek on glycaemia, with those higher than 5g being effective [195].
Studies on garlic looked almost exclusively at blood lipid levels whether in healthy populations or those with metabolic disorders. Garlic has a strong association with cardiovascular health and cholesterol levels [204-206], however, much of the published research has looked at the effect of standardised garlic extracts, rather than its consumption in food. Systematic reviews and umbrella reviews have identified strong potential for garlic in hyperlipidaemia, hypertension and inflammation [204-206].
This review has confirmed the benefits of garlic for hyperlipidaemia and indicates that concentrated extracts may not be necessary to benefit from some of the positive health effects from garlic, as both lower and higher doses showed efficacy. There was no relationship between dose and size of effect; for example, the reductions in total cholesterol from 2, 20 and 40g of garlic compared with control were 82, 19 and 51mg/dl, respectively [91, 116, 120]. Both low- and high-quality studies according to Jadad score showed effectiveness. Garlic and its phytochemicals have been found to have anti-hyperlipidaemic activity via 3-hydroxy-3-methylglutaryl CoA (HMG CoA) inhibition and reduction of cholesterol synthesis; hypotensive activity via angiotensin-converting enzyme (ACE) inhibition, downregulation of angiotensin II and stimulation of nitric oxide; and, anti-inflammatory/anti-atherosclerotic effects via COX inhibition, decreased synthesis of thromboxane B2, decreased production of leukotriene C4 and reduction of LDL oxidation [207]. There are feasible mechanisms of action for the findings and evidence for the benefits of garlic is building.
Most of the ginger studies in healthy populations looked at thermoregulatory function and appetite rather than metabolic biomarkers of glucose, insulin or lipids. The obvious sensorial heating effects on the body from ginger can explain this choice of research. Activation of TRPV1 by pungent principles in spices such as ginger leads to a sensation of heat in the mouth on consumption and has been suggested to have a thermogenic effect [208]. Studies in diabetic patients appeared largely positive for blood glucose, insulin and lipid levels. Whether this is via activation of TRPV1 receptors, anti-inflammatory effects through inhibition of COX and lipoxygenase or another mechanism remains to be investigated.
Both Nigella seeds and turmeric were investigated in a range of health conditions, with no predominance of either healthy individuals or those with type 2 diabetes. This reflects the broad range of uses of these herbs/spices in traditional medicine.
The studies on Nigella seeds were heterogenous in terms of the populations investigated and effects seen. The health effects are broad and many traditional medicine systems consider it to be a panacea [209-211], which has led to a lack of focus for research into its benefits. However, the phytochemical thymoquinone, found in the essential oil of the seed, has been identified as being responsible for some of the health benefits [209]. This may indicate there is likely to be more benefit from the use of Nigella seed oil than the seeds. A meta-analysis by Daryabeygi-Khotbehsara et al found that there was a reduction of triglycerides by Nigella seed oil, but not the seeds [212]. Sahebkar et al found that Nigella seed powder was more effective than the oil for reducing blood pressure [213], while Askari et al found that the oil was more effective than the powder for blood glucose control [214]. It is likely that thymoquinone and other terpenoids are responsible for supporting with healthy blood lipid and glucose levels, but other phytochemicals not found in the oil are responsible for the hypotensive effect. This indicates the importance of assessing the effect of culinary uses separately from that of concentrated food supplements or extracts. Future research focusing on whether dose and formulation impact on effect and efficacy would be of interest.
There are at least 10 meta-analyses on the use of Nigella seeds for metabolic syndrome and associated conditions [212-221]. These all find benefits of Nigella seeds on anthropometric measurements such as body weight, blood lipids, glucose control and inflammation, apart from a review of studies on patients with NAFLD, which found mixed results on blood lipids, inflammatory markers and glucose control [220].
Most studies on turmeric found a beneficial effect, with the most promising areas being inflammation and blood lipids. A meta-review on the health benefits of turmeric by Rolfe et al identified osteoarthritis and metabolic syndrome to be the most promising areas of research [222]. Turmeric is well researched for its use in inflammatory conditions such as osteoarthritis, however, most research focuses on high-dose curcumin extracts due to the poor bioavailability of curcumin [223]. Therefore, it is interesting that the relatively low doses of 2g were found to have some effect in this review. Sahebkar found in a meta-analysis that overall turmeric reduced CRP, but that bioavailability-improved preparations of curcuminoids were superior [224], so it may be that higher doses are preferable but not essential.
Nearly all of the spices, but none of the herbs, investigated had some evidence to support their use in culinary doses for the prevention or treatment of metabolic syndrome and associated disorders. Four mixed herb/spice intervention studies found metabolic benefits from Italian herb seasoning mixes or mixes containing Mediterranean herbs rosemary, basil, thyme, oregano and parsley [8, 10, 13, 14], however, this scoping review has found a lack of studies to confirm the effects of individual herbs mint, parsley, thyme, rosemary, sage and oregano. These plants are particularly rich sources of volatile oils, therefore, research investigating the antimicrobial properties of the essential oil is abundant [eg, 225, 226]. In vitro antimicrobial research is relatively easy to carry out, which may explain why other properties of these herbs have not been investigated to date. In addition to volatile oils, as is the case with the spices cinnamon, turmeric and ginger, these herbs are also good sources of polyphenols [24]. Further research into the general health benefits of adding these herbs to the diet would be beneficial.
Considering the widespread use of black pepper in food, it was surprising that there was only one study investigating the impact of this popular condiment for health. It may be that flavour prevents the use of large enough quantities in food for this spice to be of benefit. One study of black pepper was excluded as it investigated the use of a water extract made from 20g of black pepper, which was not representative of culinary use [15]. It was not clear from the methodology what final dose was consumed. However, if it was a comparable dose to that used by Gregersen et al [27], then the two studies found opposite effects on appetite, with Zanzer et al finding an effect of black pepper on appetite, but Gregersen et al finding none. Black pepper contains piperine, which is recognised as a phytochemical that enhances absorption of other food components [227], as well as some prescription drugs [228]. The benefits of black pepper could be largely due to its ability to improve bioavailability of polyphenols and other phytochemicals in herb/spice mixtures.
Changes in insulin, blood sugar and blood lipids were the most common biomarkers to be investigated. Effective glycaemic control, whether via eating foods with a low glycaemic index or adding in herbs/spices and other phytochemical-containing plant foods that help to reduce the glycaemic index of foods, is crucial for management and prevention of diabetes, as well as the reduction of cardiometabolic risk factors in diabetics [229]. In terms of coronary heart disease risk, only LDL cholesterol has been proven in formal clinical trials to be a biomarker that can be considered a causative factor. Other factors such as HDL cholesterol, triacylglycerol, vascular function and oxidative damage require further evidence before their measurement can be considered predictive [230]. This scoping review found promise for cardamom, cinnamon, fenugreek, garlic, ginger, Nigella seeds and turmeric, as there were positive findings from at least five different studies for one or more of these biomarkers. However, whether this translates to clinically significant effects for those with metabolic syndrome remains to be seen.
4.1. Limitations and future directions
Heterogeneity in the methodology is a major limiting factor in both interpreting the results of this scoping review and the many systematic reviews that have been carried out in this area. As herbs/spices are complex in terms of phytochemistry, as well as effect, and there are not accepted doses used, comparisons across different studies are challenging.
The doses used in different studies varied more greatly for herbs/spices where both fresh and dried can be used, such as ginger, garlic and chilli. The difficulty in comparing fresh with dried herbs/spices could be overcome in the future by ensuring that phytochemical analysis of fresh versus dried samples is carried out. Methodologies that account for differences such as these will add value and enable clearer comparison of one study with another. Most dried herbs/spices were used in doses of between 1 and 6g, which is representative of the amounts usually used in cooking [however, the doses were usually chosen based on what amounts had been found to be beneficial in previous studies]. A notable exception was fenugreek, which was used in higher doses for the additional fibre benefits. It is possible that investigating higher doses of other herbs/spices may also indicate greater benefit, but this would have to be weighed against palatability.
The combination of multiple herbs and spices is likely to have greater beneficial effect than any individual herb or spice, due to greater quantity and variety of phytochemicals. A limitation of this scoping review is that focusing on individual herbs prevents comparisons being made with the efficacy of herb/spice mixes. Future research could compare the impact of adding a single herb/spice with that from the synergy of a mix of herbs and spices in the diet providing a rich variety of phytochemicals.
The duration of the clinical trials is also likely to be a major limiting factor in determining whether consuming herbs and spices in the diet is likely to have a noticeable effect on metabolic syndrome and cardiovascular health. Although duration of study did not appear to impact on whether the effect was positive or not in the studies included in this review, any dietary intervention for preventative health needs to be assessed over a longer period, which adds considerable cost and complexity to trials. Many of these diseases develop over a long period of time, so the next step should be to measure changes in biomarkers associated with them over longer periods. Identifying metabolite markers that indicate increased consumption of specific herbs may be of use here, as has been suggested for measuring intake of polyphenol-rich foods [231].
The health benefits of herbs/spices are likely due to their phytochemical content and complex interactions between these molecules, other dietary components, the microbiome and the gut wall. Phytochemicals, and polyphenols specifically, have been found to impact carbohydrate absorption and metabolism, gut bacteria populations and uptake of glucose into muscle and adipose tissue [232]. None of the studies incorporated analysis of the phytochemical content of the herbs/spices used, which would have been a useful addition to tease out mechanisms or which bioactive phytochemicals are driving the effects. The impact of any dietary intervention is dependent on multiple other factors, such as the remaining diet, participants’ stress levels and physical activity; therefore teasing out the true impact of individual herbs/spices remains a challenge.
5. Conclusions
Overall, this scoping review has highlighted that there is evidence for the beneficial effect of culinary doses of cardamom, cinnamon, chilli, fenugreek, garlic, ginger, Nigella seeds and turmeric in the prevention and treatment of metabolic syndrome and associated disorders. Cardamom, ginger and turmeric appear to have most potential for inflammation linked to metabolic syndrome, garlic, ginger and turmeric for blood lipids, and cinnamon, ginger and fenugreek for blood glucose control. Future research needs to address which factors are most important to unlocking these benefits: the food matrix; combinations of different herbs/spices; duration of consumption; and, how herb/spice intake interacts with other important lifestyle changes.
Supplementary Materials
Supporting information can be downloaded at:www.mdpi.com/xxx/s1, Table S1: Excluded papers; Table S2: JADAD scoring.
Author Contributions
Conceptualization, M.M., S.M. and V.R.; methodology, M.M. and V.R.; validation, M.M., and V.R.; formal analysis, M.M. and V.R.; investigation, M.M. and V.R.; data curation, M.M.; writing—original draft preparation, M.M.; writing—review and editing, , M.M., A.R.M., S.M. and V.R.; visualization, M.M. and A.R.M.; supervision, V.R. All authors have read and agreed to the published version of the manuscript.”.
Funding
This research received no external funding.
Data Availability Statement
The data presented in this study are openly available in FigShare at doi: 10.6084/m9.figshare.24411967.
Acknowledgments
Professor Elizabeth Opara provided advice on interpretation of the data.
Conflicts of Interest
Authors M.M., V.R., and S.M. are employed by Pukka Herbs Ltd, a herbal tea manufacturer.
References
- Chew NWS, Ng CH, Tan DJH, Kong G, Lin C, Chin YH, et al. The global burden of metabolic disease: Data from 2000 to 2019. Cell Metab. 2023, 35(3), 414-428.e3.
- Alkhatib DH, Jaleel A, Tariq MNM, Feehan J, Apostolopoulos V, Cheikh Ismail L, et al. The role of bioactive compounds from dietary spices in the management of metabolic syndrome: an overview. Nutrients. 2021, 14(1), 175.
- Jiang TA. Health benefits of culinary herbs and spices. J AOAC International. 2019, 102(2), 395-411.
- Pallauf K, Giller K, Huebbe P, Rimbach G. Nutrition and healthy ageing: calorie restriction or polyphenol-rich "MediterrAsian" diet? Oxid Med Cell Longev. 2013, 2013:707421.
- Bahadoran Z, Golzarand M, Mirmiran P, Saadati N, Azizi F. The association of dietary phytochemical index and cardiometabolic risk factors in adults: Tehran Lipid and Glucose Study. J Hum Nutr Diet. 2013, 26 Suppl 1, 145-53.
- Dzah CS, Asante-Donyinah D, Letsyo E, Dzikunoo J, Adams ZS. Dietary polyphenols and obesity: a review of polyphenol effects on lipid and glucose metabolism, mitochondrial homeostasis, and starch digestibility and absorption. Plant Foods Hum Nutr. 2022, 78, 1–12.
- Haldar S, Chia SC, Henry CJ. Polyphenol-rich curry made with mixed spices and vegetables increases postprandial plasma GLP-1 concentration in a dose-dependent manner. Eur J Clin Nutr. 2018, 72(2), 297-300.
- Huang Y, Tsai MF, Thorat RS, Xiao D, Zhang X, Sandhu AK, et al. Endothelial function and postprandial glucose control in response to test-meals containing herbs and spices in adults with overweight/obesity. Front Nutr. 2022, 9, 811433.
- Kroff J, Hume DJ, Pienaar P, Tucker R, Lambert EV, Rae DE. The metabolic effects of a commercially available chicken peri-peri (African bird's eye chilli) meal in overweight individuals. Br J Nutr. 2017, 117(5), 635-644.
- McCrea CE, West SG, Kris-Etherton PM, Lambert JD, Gaugler TL, Teeter DL, et al. Effects of culinary spices and psychological stress on postprandial lipemia and lipase activity: results of a randomized crossover study and in vitro experiments. J Transl Med. 2015, 13, 7.
- Nakayama H, Tsuge N, Sawada H, Masamura N, Yamada S, Satomi S, et al. A single consumption of curry improved postprandial endothelial function in healthy male subjects: a randomized, controlled crossover trial. Nutr J. 2014, 13, 67.
- Oh ES, Petersen KS, Kris-Etherton PM, Rogers CJ. Spices in a high-saturated-fat, high-carbohydrate meal reduce postprandial proinflammatory cytokine secretion in men with overweight or obesity: a 3-period, crossover, randomized controlled trial. J Nutr. 2020, 150(6), 1600-1609.
- Petersen KS, Rogers CJ, West SG, Proctor DN, Kris-Etherton PM. The effect of culinary doses of spices in a high-saturated fat, high-carbohydrate meal on postprandial lipemia and endothelial function: a randomized, controlled, crossover pilot trial. Food Funct. 2020, 11(4), 3191-3200.
- Petersen KS, Davis KM, Rogers CJ, Proctor DN, West SG, Kris-Etherton PM. Herbs and spices at a relatively high culinary dosage improves 24-hour ambulatory blood pressure in adults at risk of cardiometabolic diseases: a randomized, crossover, controlled-feeding study. Am J Clin Nutr. 2021, 114(6), 1936-1948.
- Zanzer YC, Plaza M, Dougkas A, Turner C, Östman E. Black pepper-based beverage induced appetite-suppressing effects without altering postprandial glycaemia, gut and thyroid hormones or gastrointestinal well-being: a randomized crossover study in healthy subjects. Food Funct. 2018, 9(5), 2774-2786.
- Peters MDJ, Marnie C, Colquhoun H, Garritty CM, Hempel S, Horsley T, et al. Scoping reviews: reinforcing and advancing the methodology and application. Syst Rev. 2021, 10, 263.
- Cacchione PZ. The evolving methodology of scoping reviews. Clinical Nursing Research. 2016, 25(2), 115-119.
- Agarwal AK. Spice up your life: adipose tissue and inflammation. J Lipids. 2014, 2014, 182575.
- Akhter S. Low to no cost remedies for the management of diabetes mellitus; global health concern. J Diabetes Metab Disord. 2021, 20(1), 951-962.
- Bower A, Marquez S, de Mejia EG. The health benefits of selected culinary herbs and spices found in the traditional mediterranean diet. Crit Rev Food Sci Nutr. 2016, 56(16), 2728-46.
- Deekshith C, Jois M, Radcliffe J, Thomas J. Effects of culinary herbs and spices on obesity: a systematic literature review of clinical trials. J Functional Foods. 2021, 81, 104449.
- Gupta K, Testa H, Greenwood T, Kostek M, Haushalter K, Kris-Etherton PM, et al. The effect of herbs and spices on risk factors for cardiometabolic diseases: a review of human clinical trials. Nutr Rev. 2022, 80(3), 400-427.
- Opara EI. Culinary herbs and spices: what can human studies tell us about their role in the prevention of chronic non-communicable diseases? J Sci Food Agric. 2019, 99(10), 4511-4517. [CrossRef]
- Opara EI, Chohan M. Culinary herbs and spices: Their bioactive properties, the contribution of polyphenols and the challenges in deducing their true health benefits. Int J Mol Sci. 2014, 15(10), 19183-202. [CrossRef]
- Tricco AC, Lillie E, Zarin W, O'Brien KK, Colquhoun H, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018, 169(7), 467-473.
- Olivo SA, Macedo LG, Gadotti IC, Fuentes J, Stanton T, Magee DJ. Scales to assess the quality of randomized controlled trials: a systematic review. Phys Ther. 2008, 88(2), 156-75.
- Gregersen NT, Belza A, Jensen MG, Ritz C, Bitz C, Hels O, et al. Acute effects of mustard, horseradish, black pepper and ginger on energy expenditure, appetite, ad libitum energy intake and energy balance in human subjects. Br J Nutr. 2013, 109(3), 556-63.
- Verma SK, Jain V, Katewa SS. Blood pressure lowering, fibrinolysis enhancing and antioxidant activities of cardamom (Elettaria cardamomum). Indian J Biochem Biophys. 2009, 46(6), 503-6.
- Aghasi M, Koohdani F, Qorbani M, Nasli-Esfahani E, Ghazi-Zahedi S, Khoshamal H, et al. Beneficial effects of green cardamom on serum SIRT1, glycemic indices and triglyceride levels in patients with type 2 diabetes mellitus: a randomized double-blind placebo controlled clinical trial. J Sci Food Agric. 2019, 99(8), 3933-3940.
- Aghasi M, Koohdani F, Qorbani M, Nasli-Esfahani E, Ghazi-Zahedi S, Khoshamal H, et al. Beneficial effects of green cardamom on serum SIRT1, glycemic indices and triglyceride levels in patients with type 2 diabetes mellitus: a randomized double-blind placebo controlled clinical trial. J Sci Food Agric. 2019, 99(8), 3933-3940. [CrossRef]
- Ghazi Zahedi S, Koohdani F, Qorbani M, Nasli-Esfahani E, Aghasi M, Khoshamal H, et al. The effects of Elettaria cardamom supplementation on inflammatory markers and vascular function in patients with type 2 diabetes mellitus: A mechanism -based randomized clinical trial. J Her Med. 2021, 25, 100403.
- Kazemi S, Yaghooblou F, Siassi F, Rahimi Foroushani A, Ghavipour M, et al. Cardamom supplementation improves inflammatory and oxidative stress biomarkers in hyperlipidemic, overweight, and obese pre-diabetic women: a randomized double-blind clinical trial. J Sci Food Agric. 2017, 97(15), 5296-5301.
- Cheshmeh S, Ghayyem M, Khamooshi F, Heidarzadeh-Esfahani N, Rahmani N, Hojati N, et al. Green cardamom plus low-calorie diet can decrease the expression of inflammatory genes among obese women with polycystic ovary syndrome: a double-blind randomized clinical trial. Eat Weight Disord. 2022, 27(2), 821-830.
- Cheshmeh S, Elahi N, Ghayyem M, Mosaieby E, Moradi S, Pasdar Y, et al. Effect of green cardamom on the expression of genes implicated in obesity and diabetes among obese women with polycystic ovary syndrome: a double blind randomized controlled trial. Genes Nutr. 2022, 17(1), 17.
- Daneshi-Maskooni M, Keshavarz SA, Qorbani M, Mansouri S, Alavian SM, Badri-Fariman M, et al. Green cardamom increases Sirtuin-1 and reduces inflammation in overweight or obese patients with non-alcoholic fatty liver disease: a double-blind randomized placebo-controlled clinical trial. Nutr Metab (Lond). 2018, 15, 63.
- Daneshi-Maskooni M, Keshavarz SA, Qorbani M, Mansouri S, Alavian SM, Badri-Fariman M, et al. Green cardamom supplementation improves serum irisin, glucose indices, and lipid profiles in overweight or obese non-alcoholic fatty liver disease patients: a double-blind randomized placebo-controlled clinical trial. BMC Complement Altern Med. 2019, 19(1), 59.
- Ghazi Zahedi S, Koohdani F, Qorbani M, Nasli-Esfahani E, Aghasi M, Khoshamal H, et al. Effects of green cardamom supplementation on serum levels of Hs-CRP, dimethylarginine, nitric oxide and blood pressure in patients with type 2 diabetes: a randomized, double-blind, placebo controlled, clinical trial. J Her Med. 2022, 32, 100555.
- Ahuja KD, Robertson IK, Geraghty DP, Ball MJ. Effects of chili consumption on postprandial glucose, insulin, and energy metabolism. Am J Clin Nutr. 2006, 84(1), 63-9.
- Ahuja KD, Ball MJ. Effects of daily ingestion of chilli on serum lipoprotein oxidation in adult men and women. Br J Nutr. 2006, 96(2), 239-42.
- Ahuja KD, Robertson IK, Geraghty DP, Ball MJ. The effect of 4-week chilli supplementation on metabolic and arterial function in humans. Eur J Clin Nutr. 2007, 61(3), 326-33.
- Chaiyasit K, Khovidhunkit W, Wittayalertpanya S. Pharmacokinetic and the effect of capsaicin in Capsicum frutescens on decreasing plasma glucose level. J Med Assoc Thai. 2009, 92(1), 108-13.
- Clegg ME, Golsorkhi M, Henry CJ. Combined medium-chain triglyceride and chilli feeding increases diet-induced thermogenesis in normal-weight humans. Eur J Nutr. 2013, 52(6), 1579-85.
- Janssens PL, Hursel R, Martens EA, Westerterp-Plantenga MS. Acute effects of capsaicin on energy expenditure and fat oxidation in negative energy balance. PLoS One. 2013, 8(7), e67786.
- Janssens PL, Hursel R, Westerterp-Plantenga MS. Capsaicin increases sensation of fullness in energy balance, and decreases desire to eat after dinner in negative energy balance. Appetite. 2014, 77, 44-9.
- Kang C, Zhang Y, Zhu X, Liu K, Wang X, Chen M, et al. Healthy subjects differentially respond to dietary capsaicin correlating with specific gut enterotypes. J Clin Endocrinol Metab. 2016, 101(12), 4681-4689.
- Reinbach HC, Martinussen T, Møller P. Effects of hot spices on energy intake, appetite and sensory specific desires in humans. Food Quality and Preference. 2010, 21(6), 655–661.
- Yuan LJ, Qin Y, Wang L, Zeng Y, Chang H, Wang J, et al. Capsaicin-containing chili improved postprandial hyperglycemia, hyperinsulinemia, and fasting lipid disorders in women with gestational diabetes mellitus and lowered the incidence of large-for-gestational-age newborns. Clin Nutr. 2016, 35(2), 388-393.
- Shi Z, Riley M, Taylor AW, Page A. Chilli consumption and the incidence of overweight and obesity in a Chinese adult population. Int J Obes (Lond). 2017, 41(7), 1074-1079.
- Shi Z, Riley M, Brown A, Page A. Chilli intake is inversely associated with hypertension among adults. Clin Nutr ESPEN. 2018, 23, 67-72.
- Atkinson FS, Stockmann KS, Ek KL, Brand-Miller JC. Cassia but not cinnamon reduces postprandial glucose and insulin responses to oatmeal in lean, young adults. Asia Pacific J Clin Nutr. 2008, 17, S137–S137.
- Bernardo MA, Silva ML, Santos E, Moncada MM, Brito J, Proença L, et al. Effect of cinnamon tea on postprandial glucose concentration. J Diabetes Res. 2015 2015, 913651.
- Hlebowicz J, Darwiche G, Björgell O, Almér LO. Effect of cinnamon on postprandial blood glucose, gastric emptying, and satiety in healthy subjects. Am J Clin Nutr. 2007, 85(6), 1552-6.
- Hlebowicz J, Hlebowicz A, Lindstedt S, Björgell O, Höglund P, Holst JJ, et al. Effects of 1 and 3 g cinnamon on gastric emptying, satiety, and postprandial blood glucose, insulin, glucose-dependent insulinotropic polypeptide, glucagon-like peptide 1, and ghrelin concentrations in healthy subjects. Am J Clin Nutr. 2009, 89(3), 815-21.
- Magistrelli A, Chezem JC. Effect of ground cinnamon on postprandial blood glucose concentration in normal-weight and obese adults. J Acad Nutr Diet. 2012, 112(11), 1806-9.
- Markey O, McClean CM, Medlow P, Davison GW, Trinick TR, Duly E, et al. Effect of cinnamon on gastric emptying, arterial stiffness, postprandial lipemia, glycemia, and appetite responses to high-fat breakfast. Cardiovasc Diabetol. 2011, 10, 78.
- Mettler S, Schwarz I, Colombani PC. Additive postprandial blood glucose-attenuating and satiety-enhancing effect of cinnamon and acetic acid. Nutr Res. 2009, 29(10), 723-7.
- Soares APDC, de Faria NC, Graciano GF, Dos Santos ALS, Valenzuela VDC, Toulson Davisson Correia MI, et al. Cinnamon infusion reduces satiety and increases energy intake: a randomized crossover trial. Ann Nutr Metab. 2022, 78(5), 265-272.
- Solomon TP, Blannin AK. Effects of short-term cinnamon ingestion on in vivo glucose tolerance. Diabetes Obes Metab. 2007, 9(6), 895-901.
- Solomon TP, Blannin AK. Changes in glucose tolerance and insulin sensitivity following 2 weeks of daily cinnamon ingestion in healthy humans. Eur J Appl Physiol. 2009, 105(6), 969-76.
- Akilen R, Tsiami A, Devendra D, Robinson N. Glycated haemoglobin and blood pressure-lowering effect of cinnamon in multi-ethnic Type 2 diabetic patients in the UK: a randomized, placebo-controlled, double-blind clinical trial. Diabet Med. 2010, 27(10), 1159-67.
- Altschuler JA, Casella SJ, MacKenzie TA, Curtis KM. The effect of cinnamon on A1C among adolescents with type 1 diabetes. Diabetes Care. 2007, 30(4), 813-6.
- Azimi P, Ghiasvand R, Feizi A, Hosseinzadeh J, Bahreynian M, Hariri M, et al. Effect of cinnamon, cardamom, saffron and ginger consumption on blood pressure and a marker of endothelial function in patients with type 2 diabetes mellitus: A randomized controlled clinical trial. Blood Press. 2016, 25(3), 133-40.
- Blevins SM, Leyva MJ, Brown J, Wright J, Scofield RH, Aston CE. Effect of cinnamon on glucose and lipid levels in non insulin-dependent type 2 diabetes. Diabetes Care. 2007, 30(9), 2236-7.
- Crawford P. Effectiveness of cinnamon for lowering hemoglobin A1C in patients with type 2 diabetes: a randomized, controlled trial. J Am Board Fam Med. 2009, 22(5), 507-12. [CrossRef]
- Davari M, Hashemi R, Mirmiran P, Hedayati M, Sahranavard S, Bahreini S, et al. Effects of cinnamon supplementation on expression of systemic inflammation factors, NF-kB and sirtuin-1 (SIRT1) in type 2 diabetes: a randomized, double blind, and controlled clinical trial. Nutr J. 2020, 19(1), 1.
- Khan A, Safdar M, Ali Khan MM, Khattak KN, Anderson RA. Cinnamon improves glucose and lipids of people with type 2 diabetes. Diabetes Care. 2003, 26(12), 3215-8. [CrossRef]
- Lira Neto JCG, Damasceno MMC, Ciol MA, de Freitas RWJF, de Araújo MFM, Teixeira CRS, et al. Efficacy of cinnamon as an adjuvant in reducing the glycemic biomarkers of type 2 diabetes mellitus: a three-month, randomized, triple-blind, placebo-controlled clinical trial. J Am Nutr Assoc. 2022, 41(3), 266-274.
- Mirfeizi M, Mehdizadeh Tourzani Z, Mirfeizi SZ, Asghari Jafarabadi M, Rezvani HR, Afzali M. Controlling type 2 diabetes mellitus with herbal medicines: a triple-blind randomized clinical trial of efficacy and safety. J Diabetes. 2016, 8(5), 647-56.
- Mirmiran P, Davari M, Hashemi R, Hedayati M, Sahranavard S, Bahreini S, et al. A randomized controlled trial to determining the effect of cinnamon on the plasma levels of soluble forms of vascular adhesion molecules in type 2 diabetes mellitus. Eur J Clin Nutr. 2019, 73(12), 1605-1612.
- Mirmiranpour H, Huseini HF, Derakhshanian H, Khodaii Z, Tavakoli-Far B. Effects of probiotic, cinnamon, and synbiotic supplementation on glycemic control and antioxidant status in people with type 2 diabetes; a randomized, double-blind, placebo-controlled study. J Diabetes Metab Disord. 2019, 19(1), 53-60.
- Sahib AS. Anti-diabetic and antioxidant effect of cinnamon in poorly controlled type-2 diabetic Iraqi patients: a randomized, placebo-controlled clinical trial. J Intercult Ethnopharmacol. 2016, 5(2), 108-13.
- Suppapitiporn S, Kanpaksi N, Suppapitiporn S. The effect of cinnamon cassia powder in type 2 diabetes mellitus. J Med Assoc Thai. 2006, 89 Suppl 3, S200-5.
- Talaei B, Amouzegar A, Sahranavard S, Hedayati M, Mirmiran P, Azizi F. Effects of cinnamon consumption on glycemic indicators, advanced glycation end products, and antioxidant status in type 2 diabetic patients. Nutrients. 2017, 9(9), 991.
- Vanschoonbeek K, Thomassen BJ, Senden JM, Wodzig WK, van Loon LJ. Cinnamon supplementation does not improve glycemic control in postmenopausal type 2 diabetes patients. J Nutr. 2006, 136(4), 977-80.
- Wainstein J, Stern N, Heller S, Boaz M. Dietary cinnamon supplementation and changes in systolic blood pressure in subjects with type 2 diabetes. J Med Food. 2011, 14(12), 1505-10.
- Zahedifar A, Khodashenas M, Bijari B, Zahedifar F. Effects of cinnamon on fasting blood sugar and hemoglobin A1C in patients with type II diabetes mellitus: a randomized clinical trial. [In Persian]. J Mazandaran Univ Med Sci. 2018, 27(156), 80-88.
- Zahmatkesh M, Fallah Huseini H, Hajiaghaee R, Heidari M, Mehrafarin A, Tavakoli-far B. The effects of Cinnamomum zeylanicum J. Presl on blood glucose level in patients with type 2 diabetes, a double-blind clinical trial. J Med Plants. 2012, 11 (SUPPL. 8), 258-263.
- Zare R, Nadjarzadeh A, Zarshenas MM, Shams M, Heydari M. Efficacy of cinnamon in patients with type II diabetes mellitus: a randomized controlled clinical trial. Clin Nutr. 2019, 38(2), 549-556.
- Borzoei A, Rafraf M, Niromanesh S, Farzadi L, Narimani F, Doostan F. Effects of cinnamon supplementation on antioxidant status and serum lipids in women with polycystic ovary syndrome. J Tradit Complement Med. 2017, 8(1), 128-133.
- Borzoei A, Rafraf M, Asghari-Jafarabadi M. Cinnamon improves metabolic factors without detectable effects on adiponectin in women with polycystic ovary syndrome. Asia Pac J Clin Nutr. 2018, 27(3), 556-563.
- Dastgheib M, Barati-Boldaji R, Bahrampour N, Taheri R, Borghei M, Amooee S, et al. A comparison of the effects of cinnamon, ginger, and metformin consumption on metabolic health, anthropometric indices, and sexual hormone levels in women with poly cystic ovary syndrome: A randomized double-blinded placebo-controlled clinical trial. Front Nutr. 2022, 9, 1071515.
- Hajimonfarednejad M, Nimrouzi M, Heydari M, Zarshenas MM, Raee MJ, Jahromi BN. Insulin resistance improvement by cinnamon powder in polycystic ovary syndrome: A randomized double-blind placebo controlled clinical trial. Phytother Res. 2018, 32(2), 276-283.
- Kort DH, Lobo RA. Preliminary evidence that cinnamon improves menstrual cyclicity in women with polycystic ovary syndrome: a randomized controlled trial. Am J Obstet Gynecol. 2014 211(5), 487.e1-6.
- Khan AA, Begum W. Efficacy of Darchini in the management of polycystic ovarian syndrome: A randomized clinical study. J Her Med. 2019, 15, 100249.
- Gupta Jain S, Puri S, Misra A, Gulati S, Mani K. Effect of oral cinnamon intervention on metabolic profile and body composition of Asian Indians with metabolic syndrome: a randomized double -blind control trial. Lipids Health Dis. 2017, 16(1), 113.
- Askari F, Rashidkhani B, Hekmatdoost A. Cinnamon may have therapeutic benefits on lipid profile, liver enzymes, insulin resistance, and high-sensitivity C-reactive protein in nonalcoholic fatty liver disease patients. Nutr Res. 2014, 34(2), 143-8.
- Wickenberg J, Lindstedt S, Berntorp K, Nilsson J, Hlebowicz J. Ceylon cinnamon does not affect postprandial plasma glucose or insulin in subjects with impaired glucose tolerance. Br J Nutr. 2012, 107(12), 1845-9.
- Gutierrez JL, Bowden RG, Willoughby DS. Cassia cinnamon supplementation reduces peak blood glucose responses but does not improve insulin resistance and sensitivity in young, sedentary, obese women. J Diet Suppl. 2016, 13(4), 461-71.
- Pishdad S, Nadjarzadeh A, Salehi Abargouei A, Karimi Nazari E, Papoli M. Effect of cumin and cinnamon on lipid profile in middle-aged women with dyslipidemia: a double blind, randomized controlled clinical trial. Progr Nutr [Internet]. 2018, 20(2-S), 232-7.
- Lee MS, Wahlqvist ML, Chou YC, Fang WH, Lee JT, Kuan JC, et al. Turmeric improves post-prandial working memory in pre-diabetes independent of insulin. Asia Pac J Clin Nutr. 2014, 23(4), 581-91.
- Zeb F, Safdar M, Fatima S, Khan S, Alam S, Muhammad M, et al. Supplementation of garlic and coriander seed powder: Impact on body mass index, lipid profile and blood pressure of hyperlipidemic patients. Pak J Pharm Sci. 2018, 31(5), 1935-1941.
- Zare R, Heshmati F, Fallahzadeh H, Nadjarzadeh A. Effect of cumin powder on body composition and lipid profile in overweight and obese women. Complement Ther Clin Pract. 2014, 20(4), 297-301.
- Bae J, Kim J, Choue R, Lim H. Fennel (Foeniculum vulgare) and fenugreek (Trigonella foenum-graecum) tea drinking suppresses subjective short-term appetite in overweight women. Clin Nutr Res. 2015, 4(3), 168-74.
- Gopalpura PB, Jayanthi C, Dubey S. Effect of Trigonella foenum-graecum seeds on the glycemic index of food: A clinical evaluation. Int J Diab Dev Ctries. 2007, 27(2), 41-45.
- Kiss R, Szabó K, Gesztelyi R, Somodi S, Kovács P, Szabó Z, et al. Insulin-sensitizer effects of fenugreek seeds in parallel with changes in plasma MCH levels in healthy volunteers. Int J Mol Sci. 2018, 19(3), 771.
- Robert SD, Ismail AA, Rosli WI. Reduction of postprandial blood glucose in healthy subjects by buns and flatbreads incorporated with fenugreek seed powder. Eur J Nutr. 2016, 55(7), 2275-80.
- Bhadauria SS, Kushwah A. Fenugreek seeds as a therapeutic supplement for patients with noninsulin dependent diabetes mellitus: a cross-sectional study. J Clin Diagnostic Res. 2021, 15(4), BC21–BC23. [CrossRef]
- Geberemeskel GA, Debebe YG, Nguse NA. Antidiabetic effect of fenugreek seed powder solution (Trigonella foenum-graecum L.) on hyperlipidemia in diabetic patients. J Diabetes Res. 2019, 2019, 8507453.
- Hadi A, Arab A, Hajianfar H, Talaei B, Miraghajani M, Babajafari S, Marx W, Tavakoly R. The effect of fenugreek seed supplementation on serum irisin levels, blood pressure, and liver and kidney function in patients with type 2 diabetes mellitus: a parallel randomized clinical trial. Complement Ther Med. 2020, 49, 102315.
- Hassani SS, Arezodar FF, Esmaeili SS, Gholami-Fesharaki M. The effect of combined therapy with fenugreek and nutrition training based on iranian traditional medicine on FBS, HGA1C, BMI, and waist circumference in type 2 diabetic patients: a randomized double-blinded clinical trial. J Advances Med Biomed Res. 2019a, 27(120), 37-42.
- Hassani SS, Fallahi Arezodar F, Esmaeili SS, Gholami-Fesharaki M. Effect of fenugreek use on fasting blood glucose, glycosylated hemoglobin, body mass index, waist circumference, blood pressure and quality of life in patients with type 2 diabetes mellitus: a randomized, double-blinded, placebo-controlled clinical trials. Galen Med J. 2019, 8, e1432.
- Kassaian N, Azadbakht L, Forghani B, Amini M. Effect of fenugreek seeds on blood glucose and lipid profiles in type 2 diabetic patients. Int J Vitam Nutr Res. 2009, 79(1), 34-9.
- Losso JN, Holliday DL, Finley JW, Martin RJ, Rood JC, Yu Y, et al. Fenugreek bread: a treatment for diabetes mellitus. J Med Food. 2009, 12(5), 1046-9.
- Madar Z, Abel R, Samish S, Arad J. Glucose-lowering effect of fenugreek in non-insulin dependent diabetics. Eur J Clin Nutr. 1988, 42(1), 51-4.
- Najdi RA, Hagras MM, Kamel FO, Magadmi RM. A randomized controlled clinical trial evaluating the effect of Trigonella foenum-graecum (fenugreek) versus glibenclamide in patients with diabetes. Afr Health Sci. 2019, 19(1), 1594-1601.
- Rafraf M, Malekiyan M, Asghari-Jafarabadi M, Aliasgarzadeh A. Effect of fenugreek seeds on serum metabolic factors and adiponectin levels in type 2 diabetic patients. Int J Vitam Nutr Res. 2014, 84(3-4), 196-205.
- Sharma RD. Effect of fenugreek seeds and leaves on blood glucose and serum insulin responses in human subjects. Nutrition Research. 1986, 6(12), 1353-1364.
- Sharma RD, Raghuram TC, Rao NS. Effect of fenugreek seeds on blood glucose and serum lipids in type I diabetes. Eur J Clin Nutr. 1990, 44(4), 301-6.
- Sharma RD, Sarkar A, Hazra DK, Misra B, Singh JB, Maheshwari BB, et al. Hypolipidaemic effect of fenugreek seeds: a chronic study in non-insulin dependent diabetic patients. Phytotherapy Research. 1996, 10, 332-334.
- Tavakoly R, Maracy MR, Karimifar M, Entezari MH. Does fenugreek (Trigonella foenum-graecum) seed improve inflammation, and oxidative stress in patients with type 2 diabetes mellitus? A parallel group randomized clinical trial. Eur J Integrative Med. 2018, 18, 13–17.
- Bordia A, Verma SK, Srivastava KC. Effect of ginger (Zingiber officinale Rosc.) and fenugreek (Trigonella foenumgraecum L.) on blood lipids, blood sugar and platelet aggregation in patients with coronary artery disease. Prostaglandins Leukot Essent Fatty Acids. 1997, 56(5), 379-84.
- Sowmya P, Rajyalakshmi P. Hypocholesterolemic effect of germinated fenugreek seeds in human subjects. Plant Foods Hum Nutr. 1999, 53(4), 359-65.
- Yousefi E, Zareiy S, Zavoshy R, Noroozi M, Jahanihashemi H, Ardalani H. Fenugreek: a therapeutic complement for patients with borderline hyperlipidemia: a randomised, double-blind, placebo-controlled, clinical trial. Adv Integ Med. 2017, 4(1), 31–35.
- Qidwai W, Qureshi R, Hasan SN, Azam SI. Effect of dietary garlic (Allium Sativum) on the blood pressure in humans--a pilot study. J Pak Med Assoc. 2000, 50(6), 204-7.
- Zhang S, Liu M, Wang Y, Zhang Q, Liu L, Meng G, et al. Raw garlic consumption is inversely associated with prehypertension in a large-scale adult population. J Hum Hypertens. 2020, 34(1), 59-67.
- Aslani N, Entezari MH, Askari G, Maghsoudi Z, Maracy MR. Effect of garlic and lemon juice mixture on lipid profile and some cardiovascular risk factors in people 30-60 years old with moderate hyperlipidaemia: a randomized clinical trial. Int J Prev Med. 2016, 7, 95.
- Choudhary PR, Jani RD, Sharma MS. Effect of raw crushed garlic (Allium sativum L.) on components of metabolic syndrome. J Diet Suppl. 2018, 15(4), 499-506.
- van Doorn MB, Espirito Santo SM, Meijer P, Kamerling IM, Schoemaker RC, Dirsch V, et al. Effect of garlic powder on C-reactive protein and plasma lipids in overweight and smoking subjects. Am J Clin Nutr. 2006, 84(6), 1324-9.
- Scharbert G, Kalb ML, Duris M, Marschalek C, Kozek-Langenecker SA. Garlic at dietary doses does not impair platelet function. Anesth Analg. 2007, 105(5), 1214-8.
- Bakhsh R, Chughtai MI. Influence of garlic on serum cholesterol, serum triglycerides, serum total lipids and serum glucose in human subjects. Nahrung. 1984, 28(2), 159-63.
- Roberts K, Jahner DKW, Buddington RK. Influence of garlic supplementation on human fecal flora and serum lipid levels. FASEB Journal 1998, 12(5), A876.
- Charron CS, Dawson HD, Albaugh GP, Solverson PM, Vinyard BT, Solano-Aguilar GI, et al. A single meal containing raw, crushed garlic influences expression of immunity- and cancer-related genes in whole blood of humans. J Nutr. 2015, 145(11), 2448-55.
- Sangouni AA, Alizadeh M, Jamalzehi A, Parastouei K. Effects of garlic powder supplementation on metabolic syndrome components, insulin resistance, fatty liver index, and appetite in subjects with metabolic syndrome: a randomized clinical trial. Phytother Res. 2021, 35(8), 4433-4441.
- Sangouni AA, Mohammad Hosseini Azar MR, Alizadeh M. Effects of garlic powder supplementation on insulin resistance, oxidative stress, and body composition in patients with non-alcoholic fatty liver disease: A randomized controlled clinical trial. Complement Ther Med. 2020, 51, 102428.
- Sangouni AA, Mohammad Hosseini Azar MR, Alizadeh M. Effect of garlic powder supplementation on hepatic steatosis, liver enzymes and lipid profile in patients with non-alcoholic fatty liver disease: a double-blind randomised controlled clinical trial. Br J Nutr. 2020, 124(4), 450-456.
- Janssen PL, Meyboom S, van Staveren WA, de Vegt F, Katan MB. Consumption of ginger (Zingiber officinale roscoe) does not affect ex vivo platelet thromboxane production in humans. Eur J Clin Nutr. 1996, 50(11), 772-4.
- Miyamoto M, Matsuzaki K, Katakura M, Hara T, Tanabe Y, Shido O. Oral intake of encapsulated dried ginger root powder hardly affects human thermoregulatory function, but appears to facilitate fat utilization. Int J Biometeorol. 2015, 59(10), 1461-74.
- Mansour MS, Ni YM, Roberts AL, Kelleman M, Roychoudhury A, St-Onge MP. Ginger consumption enhances the thermic effect of food and promotes feelings of satiety without affecting metabolic and hormonal parameters in overweight men: a pilot study. Metabolism. 2012, 61(10), 1347-52.
- Ebrahimzadeh Attari V, Asghari Jafarabadi M, Zemestani M, Ostadrahimi A. Effect of Zingiber officinale supplementation on obesity management with respect to the uncoupling protein 1 -3826A>G and ß3-adrenergic receptor Trp64Arg polymorphism. Phytother Res. 2015, 29(7), 1032-9.
- Ebrahimzadeh Attari V, Ostadrahimi A, Asghari Jafarabadi M, Mehralizadeh S, Mahluji S. Changes of serum adipocytokines and body weight following Zingiber officinale supplementation in obese women: a RCT. Eur J Nutr. 2016, 55(6), 2129-36.
- Ebrahimzadeh Attari V, Mahluji S, Asghari Jafarabadi M, Ostadrahimi A. Effects of supplementation with ginger (Zingiber officinale Roscoe) on serum glucose, lipid profile and oxidative stress in obese women: a randomized, placebo-controlled clinical trial. Pharm Sci. 2015, 21(4), 184-191.
- Carvalho GCN, Lira-Neto JCG, Araújo MFM, Freitas RWJF, Zanetti ML, Damasceno MMC. Effectiveness of ginger in reducing metabolic levels in people with diabetes: a randomized clinical trial. Rev Lat Am Enfermagem. 2020, 28, e3369.
- Khandouzi N, Shidfar F, Rajab A, Rahideh T, Hosseini P, Mir Taheri M. The effects of ginger on fasting blood sugar, hemoglobin a1c, apolipoprotein B, apolipoprotein a-I and malondialdehyde in type 2 diabetic patients. Iran J Pharm Res. 2015, 14(1), 131-40.
- Mahluji S, Attari VE, Mobasseri M, Payahoo L, Ostadrahimi A, Golzari SE. Effects of ginger (Zingiber officinale) on plasma glucose level, HbA1c and insulin sensitivity in type 2 diabetic patients. Int J Food Sci Nutr. 2013, 64(6), 682-6.
- Mahluji S, Ostadrahimi A, Mobasseri M, Ebrahimzade Attari V, Payahoo L. Anti-inflammatory effects of Zingiber officinale in type 2 diabetic patients. Adv Pharm Bull. 2013, 3(2), 273-6.
- Arablou T, Aryaeian N, Valizadeh M, Sharifi F, Hosseini A, Djalali M. The effect of ginger consumption on glycemic status, lipid profile and some inflammatory markers in patients with type 2 diabetes mellitus. Int J Food Sci Nutr. 2014, 65(4), 515-20.
- Hajimoosayi F, Jahanian Sadatmahalleh S, Kazemnejad A, Pirjani R. Effect of ginger on the blood glucose level of women with gestational diabetes mellitus (GDM) with impaired glucose tolerance test (GTT): a randomized double-blind placebo-controlled trial. BMC Complement Med Ther. 2020, 20(1), 116.
- Mozaffari-Khosravi H, Talaei B, Jalali BA, Najarzadeh A, Mozayan MR. The effect of ginger powder supplementation on insulin resistance and glycemic indices in patients with type 2 diabetes: a randomized, double-blind, placebo-controlled trial. Complement Ther Med. 2014, 22(1), 9-16.
- Shidfar F, Rajab A, Rahideh T, Khandouzi N, Hosseini S, Shidfar S. The effect of ginger (Zingiber officinale) on glycemic markers in patients with type 2 diabetes. J Complement Integr Med. 2015, 12(2), 165-70.
- Zarezadeh M, Saedisomeolia A, Khorshidi M, Kord Varkane H, Makhdoomi Arzati M, Abdollahi M, et al. Asymmetric dimethylarginine and soluble inter-cellular adhesion molecule-1 serum levels alteration following ginger supplementation in patients with type 2 diabetes: a randomized double-blind, placebo-controlled clinical trial. J Complement Integr Med. 2018, 16(2), /j/jcim.2019.16.issue-2/jcim-2018-0019/jcim-2018-0019.xml.
- Mohammadzadeh Honarvar N, Zarezadeh M, Khorshidi M, Makhdoomi Arzati M, Yekaninejad MS, Abdollahi M, et al. The effect of an oral ginger supplementation on NF-κB concentration in peripheral blood mononuclear cells and anthropomorphic data of patients with type 2 diabetes: a randomized double-blind, placebo-controlled clinical trial. Complement Ther Med. 2019, 42, 7-11.
- Alizadeh-Navaei R, Roozbeh F, Saravi M, Pouramir M, Jalali F, Moghadamnia AA. Investigation of the effect of ginger on the lipid levels. A double blind controlled clinical trial. Saudi Med J. 2008, 29(9), 1280-4.
- Kamari N, Moradinazar M, Qasemi M, Khosravy T, Samadi M, Abdolahzad H. Combination of the effect of ginger and anti-inflammatory diet on children with obesity with nonalcoholic fatty liver disease: a randomized clinical trial. Food Sci Nutr. 2023, 11(4), 1846-1859.
- Rafie Hosseini SA, Hajiani E, Saki Malehi A, Mard SA. Effect of ginger powder supplementation in patients with non-alcoholic fatty liver disease: a randomized clinical trial. Clin Exper Gastroenterol. 2020, 13, 35–45.
- Ashraf H, Heydari M, Shams M, Zarshenas MM, Tavakoli A, Sayadi M. Efficacy of ginger supplementation in relieving persistent hypothyroid symptoms in patients with controlled primary hypothyroidism: a pilot randomized, double-blind, placebo-controlled clinical trial. Evid Based Complement Alt Med. 2022, 5456855–10.
- Pelegrin S, Galtier F, Chalançon A, Gagnol JP, Barbanel AM, Pélissier Y, et al. Effects of Nigella sativa seeds (black cumin) on insulin secretion and lipid profile: A pilot study in healthy volunteers. Br J Clin Pharmacol. 2019, 85(7), 1607-1611.
- Amin F, Islam N, Anila N, Gilani AH. Clinical efficacy of the co-administration of Turmeric and Black seeds (Kalongi) in metabolic syndrome - a double blind randomized controlled trial - TAK-MetS trial. Complement Ther Med. 2015, 23(2), 165-74.
- Datau EA, Wardhana, Surachmanto EE, Pandelaki K, Langi JA, Fias. Efficacy of Nigella sativa on serum free testosterone and metabolic disturbances in central obese male. Acta Med Indones. 2010 42(3), 130-4.
- Farhangi MA, Dehghan P, Tajmiri S, Abbasi MM. The effects of Nigella sativa on thyroid function, serum vascular endothelial growth factor (VEGF) - 1, Nesfatin-1 and anthropometric features in patients with Hashimoto's thyroiditis: a randomized controlled trial. BMC Complement Altern Med. 2016, 16(1), 471.
- Farhangi MA, Tajmiri S. The effects of powdered black cumin seeds on markers of oxidative stress, intracellular adhesion molecule (ICAM)-1 and vascular cell adhesion molecule (VCAM)-1 in patients with Hashimoto's thyroiditis. Clin Nutr ESPEN. 2020, 37, 207-212.
- Ibrahim RM, Hamdan NS, Ismail M, Saini SM, Abd Rashid SN, Abd Latiff L, et al. Protective effects of Nigella sativa on metabolic syndrome in menopausal women. Adv Pharm Bull. 2014, 4(1), 29-33.
- Mohtashami A, Mahaki B, Azadbakht L, Entezari MH. Effects of bread with Nigella sativa on lipid profiles, apolipoproteins and inflammatory factor in metabolic syndrome patients. Clin Nutr Res. 2016, 5(2), 89-95.
- Mohtashami A. Effects of bread with Nigella Sativa on blood glucose, blood pressure and anthropometric indices in patients with metabolic syndrome. Clin Nutr Res. 2019, 8(2), 138-147.
- Shirazi M, Khodakarami F, Feizabad E, Ghaemi M. The effects of Nigella sativa on anthropometric and biochemical indices in postmenopausal women with metabolic syndrome. Endocrine. 2020, 69(1), 49-52.
- Ibrahim RM, Hamdan NS, Mahmud R, Imam MU, Saini SM, Rashid SN, et al. A randomised controlled trial on hypolipidemic effects of Nigella sativa seeds powder in menopausal women. J Transl Med. 2014, 12, 82.
- Qidwai W, Hamza HB, Qureshi R, Gilani A. Effectiveness, safety, and tolerability of powdered Nigella sativa (kalonji) seed in capsules on serum lipid levels, blood sugar, blood pressure, and body weight in adults: results of a randomized, double-blind controlled trial. J Altern Complement Med. 2009, 15(6), 639-44.
- Sabzghabaee AM, Dianatkhah M, Sarrafzadegan N, Asgary S, Ghannadi A. Clinical evaluation of Nigella sativa seeds for the treatment of hyperlipidemia: a randomized, placebo controlled clinical trial. Med Arch. 2012, 66(3), 198-200.
- Badar A, Kaatabi H, Bamosa A, Al-Elq A, Abou-Hozaifa B, Lebda F, et al. Effect of Nigella sativa supplementation over a one-year period on lipid levels, blood pressure and heart rate in type-2 diabetic patients receiving oral hypoglycemic agents: nonrandomized clinical trial. Ann Saudi Med. 2017, 37(1), 56-63.
- Kaatabi H, Bamosa AO, Badar A, Al-Elq A, Abou-Hozaifa B, Lebda F, et al. Nigella sativa improves glycemic control and ameliorates oxidative stress in patients with type 2 diabetes mellitus: placebo controlled participant blinded clinical trial. PLoS One. 2015, 10(2), e0113486.
- Bamosa AO, Kaatabi H, Lebdaa FM, Elq AM, Al-Sultanb A. Effect of Nigella sativa seeds on the glycemic control of patients with type 2 diabetes mellitus. Indian J Physiol Pharmacol. 2010, 54(4), 344-54.
- Darand M, Darabi Z, Yari Z, Saadati S, Hedayati M, Khoncheh A, et al. Nigella sativa and inflammatory biomarkers in patients with non-alcoholic fatty liver disease: results from a randomized, double-blind, placebo-controlled, clinical trial. Complement Ther Med. 2019, 44, 204-209.
- Darand M, Darabi Z, Yari Z, Hedayati M, Shahrbaf MA, Khoncheh A, et al. The effects of black seed supplementation on cardiovascular risk factors in patients with nonalcoholic fatty liver disease: a randomized, double-blind, placebo-controlled clinical trial. Phytother Res. 2019, 33(9), 2369-2377.
- Akbari S, Sohouli MH, Ebrahimzadeh S, Ghanaei FM, Hosseini AF, Aryaeian N. Effect of rosemary leaf powder with weight loss diet on lipid profile, glycemic status, and liver enzymes in patients with nonalcoholic fatty liver disease: a randomized, double-blind clinical trial. Phytother Res. 2022, 36(5), 2186-2196.
- Sá CM, Ramos AA, Azevedo MF, Lima CF, Fernandes-Ferreira M, Pereira-Wilson C. Sage tea drinking improves lipid profile and antioxidant defences in humans. Int J Mol Sci. 2009, 10(9), 3937-3950.
- Maithili Karpaga Selvi N, Sridhar MG, Swaminathan RP, Sripradha R. Efficacy of turmeric as adjuvant therapy in type 2 diabetic patients. Indian J Clin Biochem. 2015, 30(2), 180-6.
- Darmian MA, Hoseini R, Amiri E, Golshani S. How combined and separate aerobic training and turmeric supplementation alter lipid profile and glycemic status? A clinical trial in middle-aged females with type 2 diabetes and hyperlipidemia. Int. Cardiovasc. Res. J. 2021, 15(3), e118791, 111-118.
- Darmian MA, Hoseini R, Amiri E, Golshani S. Downregulated hs-CRP and MAD, upregulated GSH and TAC, and improved metabolic status following combined exercise and turmeric supplementation: a clinical trial in middle-aged women with hyperlipidemic type 2 diabetes. J. Diabetes Metab. Disord. 2022, 21(1), 275-283.
- Adab Z, Eghtesadi S, Vafa MR, Heydari I, Shojaii A, Haqqani H, et al. Effect of turmeric on glycemic status, lipid profile, hs-CRP, and total antioxidant capacity in hyperlipidemic type 2 diabetes mellitus patients. Phytother Res. 2019, 33(4), 1173-1181.
- Srinivasan A, Selvarajan S, Kamalanathan S, Kadhiravan T, Prasanna Lakshmi NC, Adithan S. Effect of Curcuma longa on vascular function in native Tamilians with type 2 diabetes mellitus: A randomized, double-blind, parallel arm, placebo-controlled trial. Phytother Res. 2019, 33(7), 1898-1911.
- Wickenberg J, Ingemansson SL, Hlebowicz J. Effects of Curcuma longa (turmeric) on postprandial plasma glucose and insulin in healthy subjects. Nutr J. 2010, 9, 43.
- Nieman DC, Cialdella-Kam L, Knab AM, Shanely RA. Influence of red pepper spice and turmeric on inflammation and oxidative stress biomarkers in overweight females: a metabolomics approach. Plant Foods Hum Nutr. 2012, 67(4), 415-21.
- Uchio R, Okuda-Hanafusa C, Saji R, Kawasaki K, Muroyama K, Murosaki S, et al. A hot water extract of Curcuma longa L. improves fasting serum glucose levels in participants with low-grade inflammation: reanalysis of data from two randomized, double-blind, placebo-controlled trials. Nutrients. 2022, 14(18), 3763.
- Jarhahzadeh M, Alavinejad P, Farsi F, Husain D, Rezazadeh A. The effect of turmeric on lipid profile, malondialdehyde, liver echogenicity and enzymes among patients with nonalcoholic fatty liver disease: a randomized double blind clinical trial. Diabetol Metab Syndr. 2021, 13(1), 112.
- Navekar R, Rafraf M, Ghaffari A, Asghari-Jafarabadi M, Khoshbaten M. Turmeric supplementation improves serum glucose indices and leptin levels in patients with nonalcoholic fatty liver diseases. J. Am. Coll. Nutr. 2017, 36(4), 261-267.
- Kandikattu HK, Rachitha P, Jayashree GV, Krupashree K, Sukhith M, Majid A, et al. Anti-inflammatory and anti-oxidant effects of cardamom (Elettaria repens (Sonn.) Baill) and its phytochemical analysis by 4D GCXGC TOF-MS. Biomed Pharmacother. 2017, 91, 191-201.
- Yahyazadeh R, Ghasemzadeh Rahbardar M, Razavi BM, Karimi G, Hosseinzadeh H. The effect of Elettaria cardamomum (cardamom) on the metabolic syndrome: narrative review. Iran J Basic Med Sci. 2021, 24(11), 1462-1469.
- Panchal SK, Bliss E, Brown L. Capsaicin in metabolic syndrome. Nutrients. 2018, 10(5), 630.
- Akilen R, Tsiami A, Devendra D, Robinson N. Cinnamon in glycaemic control: systematic review and meta analysis. Clin Nutr. 2012, 31(5), 609-15.
- Sharma S, Mandal A, Kant R, Jachak S, Jagzape M. Is cinnamon efficacious for glycaemic control in type-2 diabetes mellitus? J. Pak. Med. Assoc. 2020, 70(11), 2065-2069.
- Silva ML, Bernardo MA, Singh J, de Mesquita MF. Cinnamon as a complementary therapeutic approach for dysglycemia and dyslipidemia control in type 2 diabetes mellitus and its molecular mechanism of action: a review. Nutrients. 2022, 14(13), 2773.
- Yu T, Lu K, Cao X, Xia H, Wang S, Sun G, et al. The effect of cinnamon on glycolipid metabolism: a dose-response meta-analysis of randomized controlled trials. Nutrients. 2023, 15(13), 2983.
- Allen RW, Schwartzman E, Baker WL, Coleman CI, Phung OJ. Cinnamon use in type 2 diabetes: an updated systematic review and meta-analysis. Ann Fam Med. 2013, 11(5), 452-9.
- Baker WL, Gutierrez-Williams G, White CM, Kluger J, Coleman CI. Effect of cinnamon on glucose control and lipid parameters. Diabetes Care. 2008, 31(1), 41-3.
- Davis PA, Yokoyama W. Cinnamon intake lowers fasting blood glucose: meta-analysis. J. Med. Food. 2011, 14(9), 884-9.
- Deyno S, Eneyew K, Seyfe S, Tuyiringire N, Peter EL, Muluye RA, et al. Efficacy and safety of cinnamon in type 2 diabetes mellitus and pre-diabetes patients: a meta-analysis and meta-regression. Diabetes Res. Clin. Pract. 2019, 156, 107815.
- Jamali N, Kazemi A, Saffari-Chaleshtori J, Samare-Najaf M, Mohammadi V, Clark CCT. The effect of cinnamon supplementation on lipid profiles in patients with type 2 diabetes: a systematic review and meta-analysis of clinical trials. Complement. Ther. Med. 2020, 55, 102571.
- Leach MJ, Kumar S. Cinnamon for diabetes mellitus. Cochrane Database Syst. Rev. 2012, 2012(9), CD007170.
- Ranasinghe P, Jayawardana R, Galappaththy P, Constantine GR, de Vas Gunawardana N, Katulanda P. Efficacy and safety of 'true' cinnamon (Cinnamomum zeylanicum) as a pharmaceutical agent in diabetes: a systematic review and meta-analysis. Diabet. Med. 2012, 29(12), 1480-92.
- Heydarpour F, Hemati N, Hadi A, Moradi S, Mohammadi E, Farzaei MH. Effects of cinnamon on controlling metabolic parameters of polycystic ovary syndrome: a systematic review and meta-analysis. J. Ethnopharmacol. 2020, 254, 112741.
- Kutbi EH, Sohouli MH, Fatahi S, Lari A, Shidfar F, Aljhdali MM, et al. The beneficial effects of cinnamon among patients with metabolic diseases: a systematic review and dose-response meta-analysis of randomized-controlled trials. Crit. Rev. Food Sci. Nutr. 2022, 62(22), 6113-6131.
- Wu T, Huang W, He M, Yue R. Effects of cinnamon supplementation on lipid profiles among patients with metabolic syndrome and related disorders: a systematic review and meta-analysis. Complement Ther Clin Pract. 2022, 49, 101625.
- Krittanawong C, Isath A, Scott CZ, Wang Z, Kaplin S, Jneid H, et al. Association between cinnamon consumption and risk of cardiovascular health: a systematic review and meta-analysis. Am J Med. 2022, 135(1), 110-117.
- Maierean SM, Serban MC, Sahebkar A, Ursoniu S, Serban A, Penson P, et al. The effects of cinnamon supplementation on blood lipid concentrations: a systematic review and meta-analysis. J. Clin. Lipidol. 2017, 11(6), 1393-1406.
- Valussi M. Functional foods with digestion-enhancing properties. Int J Food Sci Nutr. 2012, 63 Suppl 1, 82-9.
- Neelakantan N, Narayanan M, de Souza RJ, van Dam RM. Effect of fenugreek (Trigonella foenum-graecum L.) intake on glycemia: a meta-analysis of clinical trials. Nutr. J. 2014, 13, 7.
- Askarpour M, Alami F, Campbell MS, Venkatakrishnan K, Hadi A, Ghaedi E. Effect of fenugreek supplementation on blood lipids and body weight: A systematic review and meta-analysis of randomized controlled trials. J. Ethnopharmacol. 2020, 253, 112538.
- Shabil M, Bushi G, Bodige PK, Maradi PS, Patra BP, Padhi BK, et al. Effect of fenugreek on hyperglycemia: a systematic review and meta-analysis. Medicina (Kaunas). 2023, 59(2), 248.
- Amini MR, Payandeh N, Sheikhhossein F, Pourreza S, Ghalandari H, Askarpour M, et al. The effects of fenugreek seed consumption on blood pressure: a systematic review and meta-analysis of randomized controlled trials. High Blood Press. Cardiovasc. Prev. 2023, 30(2), 123-133.
- Correia AGDS, Alencar MB, Dos Santos AN, da Paixão DCB, Sandes FLF, Andrade B, et al. Effect of saffron and fenugreek on lowering blood glucose: a systematic review with meta-analysis. Phytother Res. 2023, 37(5), 2092-2101.
- Fakhr L, Chehregosha F, Zarezadeh M, Chaboksafar M, Tarighat-Esfanjani A. Effects of fenugreek supplementation on the components of metabolic syndrome: a systematic review and dose-response meta-analysis of randomized clinical trials. Pharmacol Res. 2023, 187, 106594.
- Gong J, Fang K, Dong H, Wang D, Hu M, Lu F. Effect of fenugreek on hyperglycaemia and hyperlipidemia in diabetes and prediabetes: a meta-analysis. J. Ethnopharmacol. 2016, 194, 260-268.
- Heshmat-Ghahdarijani K, Mashayekhiasl N, Amerizadeh A, Teimouri Jervekani Z, Sadeghi M. Effect of fenugreek consumption on serum lipid profile: a systematic review and meta-analysis. Phytother Res. 2020, 34(9), 2230-2245.
- Khodamoradi K, Khosropanah MH, Ayati Z, Chang D, Nasli-Esfahani E, Ayati MH, et al. The effects of fenugreek on cardiometabolic risk factors in adults: a systematic review and meta-analysis. Complement. Ther. Med. 2020, 52, 102416.
- Gadidala SK, Johny E, Thomas C, Nadella M, Undela K, Adela R. Effect of garlic extract on markers of lipid metabolism and inflammation in coronary artery disease (CAD) patients: A systematic review and meta-analysis. Phytother Res. 2023, 37(6), 2242-2254.
- Schwingshackl L, Missbach B, Hoffmann G. An umbrella review of garlic intake and risk of cardiovascular disease. Phytomedicine. 2016, 23(11), 1127-33.
- Varshney R, Budoff MJ. Garlic and Heart Disease. J. Nutr. 2016, 146(2), 416S-421S.
- Sobenin IA, Myasoedova VA, Iltchuk MI, Zhang DW, Orekhov AN. Therapeutic effects of garlic in cardiovascular atherosclerotic disease. Chin. J. Nat. Med. 2019, 17(10), 721-728.
- Westerterp-Plantenga M, Diepvens K, Joosen AM, Bérubé-Parent S, Tremblay A. Metabolic effects of spices, teas, and caffeine. Physiol. Behav. 2006, 89(1), 85-91.
- Ahmad A, Husain A, Mujeeb M, Khan SA, Najmi AK, Siddique NA, et al. A review on therapeutic potential of Nigella sativa: A miracle herb. Asian Pac. J. Trop. Biomed. 2013, 3(5), 337-52.
- Dalli M, Bekkouch O, Azizi SE, Azghar A, Gseyra N, Kim B. Nigella sativa L. phytochemistry and pharmacological activities: a review (2019-2021). Biomolecules. 2021, 12(1), 20.
- Salehi B, Quispe C, Imran M, Ul-Haq I, Živković J, Abu-Reidah IM, et al. Nigella plants - traditional uses, bioactive phytoconstituents, preclinical and clinical studies. Front. Pharmacol. 2021, 12, 625386.
- Daryabeygi-Khotbehsara R, Golzarand M, Ghaffari MP, Djafarian K. Nigella sativa improves glucose homeostasis and serum lipids in type 2 diabetes: A systematic review and meta-analysis. Complement. Ther. Med. 2017, 35, 6-13.
- Sahebkar A, Soranna D, Liu X, Thomopoulos C, Simental-Mendia LE, Derosa G, et al. A systematic review and meta-analysis of randomized controlled trials investigating the effects of supplementation with Nigella sativa (black seed) on blood pressure. J. Hypertens. 2016, 34(11), 2127-35.
- Askari G, Rouhani MH, Ghaedi E, Ghavami A, Nouri M, Mohammadi H. Effect of Nigella sativa (black seed) supplementation on glycemic control: A systematic review and meta-analysis of clinical trials. Phytother. Res. 2019, 33(5), 1341-1352.
- Hallajzadeh J, Milajerdi A, Mobini M, Amirani E, Azizi S, Nikkhah E, et al. Effects of Nigella sativa on glycemic control, lipid profiles, and biomarkers of inflammatory and oxidative stress: a systematic review and meta-analysis of randomized controlled clinical trials. Phytother. Res. 2020, 34(10), 2586-2608.
- Kavyani Z, Musazadeh V, Golpour-Hamedani S, Moridpour AH, Vajdi M, Askari G. The effect of Nigella sativa (black seed) on biomarkers of inflammation and oxidative stress: an updated systematic review and meta-analysis of randomized controlled trials. Inflammopharmacology. 2023, 31(3), 1149-1165.
- Montazeri RS, Fatahi S, Sohouli MH, Abu-Zaid A, Santos HO, Găman MA, et al. The effect of Nigella sativa on biomarkers of inflammation and oxidative stress: a systematic review and meta-analysis of randomized controlled trials. J. Food Biochem. 2021, 45(4), e13625.
- Mousavi SM, Sheikhi A, Varkaneh HK, Zarezadeh M, Rahmani J, Milajerdi A. Effect of Nigella sativa supplementation on obesity indices: a systematic review and meta-analysis of randomized controlled trials. Complement. Ther. Med. 2018, 38, 48-57.
- Namazi N, Larijani B, Ayati MH, Abdollahi M. The effects of Nigella sativa L. on obesity: a systematic review and meta-analysis. J. Ethnopharmacol. 2018, 219, 173-181.
- Tang G, Zhang L, Tao J, Wei Z. Effect of Nigella sativa in the treatment of nonalcoholic fatty liver disease: a systematic review and meta-analysis of randomized controlled trials. Phytother. Res. 2021, 35(8), 4183-4193.
- Tavakoly R, Arab A, Vallianou N, Clark CCT, Hadi A, Ghaedi E, Ghavami A. The effect of Nigella sativa L. supplementation on serum C-reactive protein: a systematic review and meta-analysis of randomized controlled trials. Complement. Ther. Med. 2019, 45, 149-155.
- Rolfe V. Mackonochie M, Mills S, MacLennan E. Turmeric/curcumin health outcomes: A meta-review of systematic reviews. Eur. J. Integ. Med. 2020, 40, 101252.
- Dei Cas M, Ghidoni R. Dietary curcumin: correlation between bioavailability and health potential. Nutrients. 2019, 11(9), 2147.
- Sahebkar A. Are curcuminoids effective C-reactive protein-lowering agents in clinical practice? Evidence from a meta-analysis. Phytother. Res. 2014, 28(5), 633-42.
- Sakkas H, Papadopoulou C. Antimicrobial activity of basil, oregano, and thyme essential oils. J. Microbiol. Biotechnol. 2017, 27(3), 429-438.
- El-Kased RF, El-Kersh DM. GC-MS profiling of naturally extracted essential oils: antimicrobial and beverage preservative actions. Life (Basel). 2022, 12(10), 1587.
- Wightman EL, Reay JL, Haskell CF, Williamson G, Dew TP, Kennedy DO. Effects of resveratrol alone or in combination with piperine on cerebral blood flow parameters and cognitive performance in human subjects: a randomised, double-blind, placebo-controlled, cross-over investigation. Br. J. Nutr. 2014, 112(2), 203-13.
- Ajazuddin, Alexander A, Qureshi A, Kumari L, Vaishnav P, Sharma M, et al. Role of herbal bioactives as a potential bioavailability enhancer for active pharmaceutical ingredients. Fitoterapia. 2014, 97, 1-14.
- Chiavaroli L, Lee D, Ahmed A, Cheung A, Khan TA, Blanco S, et al. Effect of low glycaemic index or load dietary patterns on glycaemic control and cardiometabolic risk factors in diabetes: systematic review and meta-analysis of randomised controlled trials. BMJ. 2021, 374, n1651.
- Mensink RP, Aro A, Den Hond E, German JB, Griffin BA, ter Meer H-U, et al. PASSCLAIM – Diet-related cardiovascular disease. Eur. J. Nutr. 2003, 42(Suppl 1), 1/6-1/27.
- Edmands WM, Ferrari P, Rothwell JA, Rinaldi S, Slimani N, Barupal DK, et al. Polyphenol metabolome in human urine and its association with intake of polyphenol-rich foods across European countries. Am. J. Clin. Nutr. 2015, 102(4), 905-13.
- Shahwan M, Alhumaydhi F, Ashraf GM, Hasan PMZ, Shamsi A. Role of polyphenols in combating type 2 diabetes and insulin resistance. Int. J. Biol. Macromol. 2022, 206, 567-579.
Figure 1.
PRISMA flow diagram of the screening process. *The number of studies for all the individual herbs has a total sum of more than 145, as some studies included more than one herb in each arm of the study.
Figure 1.
PRISMA flow diagram of the screening process. *The number of studies for all the individual herbs has a total sum of more than 145, as some studies included more than one herb in each arm of the study.
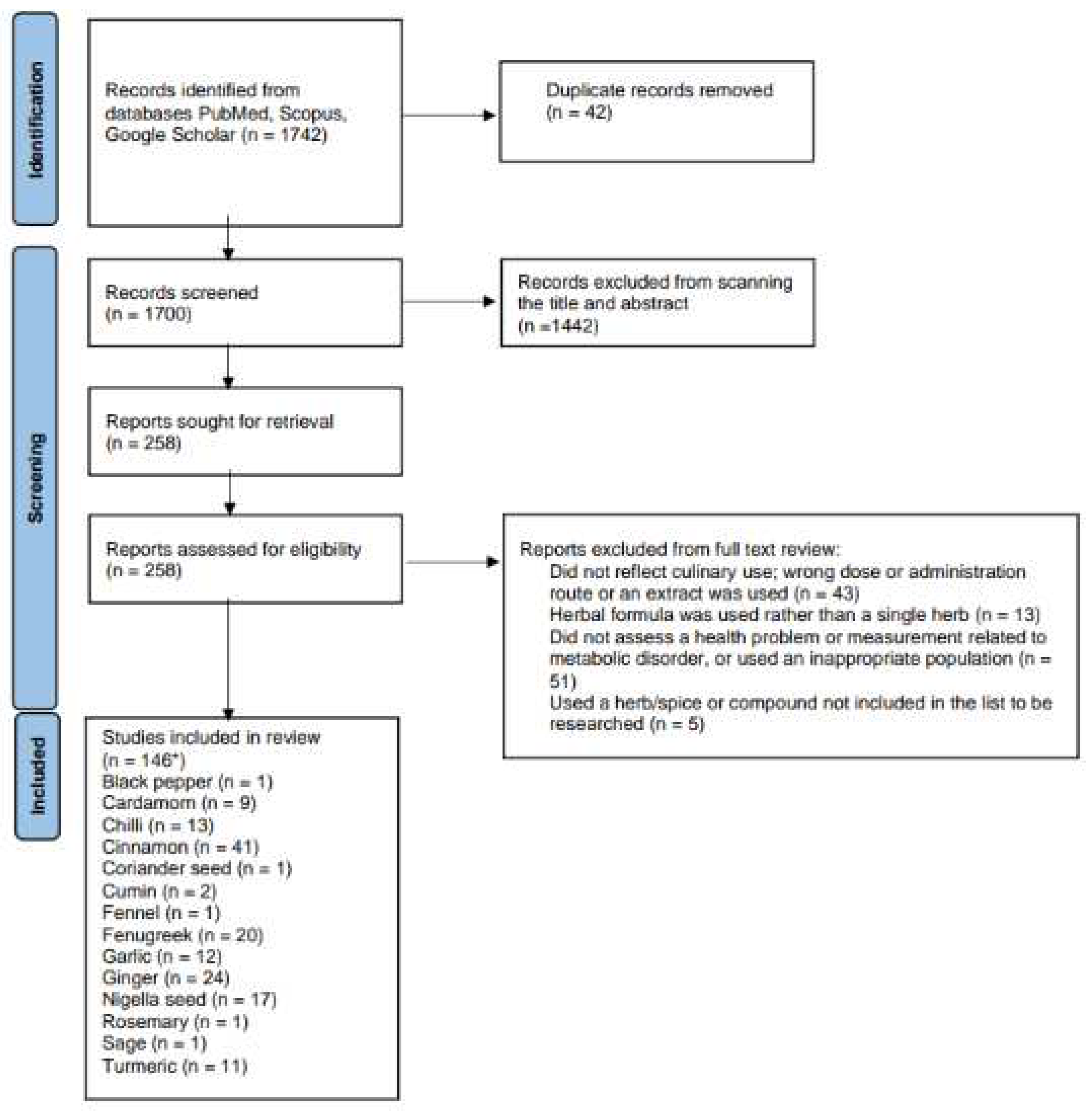
Figure 2.
Number of studies and high-quality studies demonstrating an effect of herbs/spices in specific cardiometabolic biomarkers.
Figure 2.
Number of studies and high-quality studies demonstrating an effect of herbs/spices in specific cardiometabolic biomarkers.
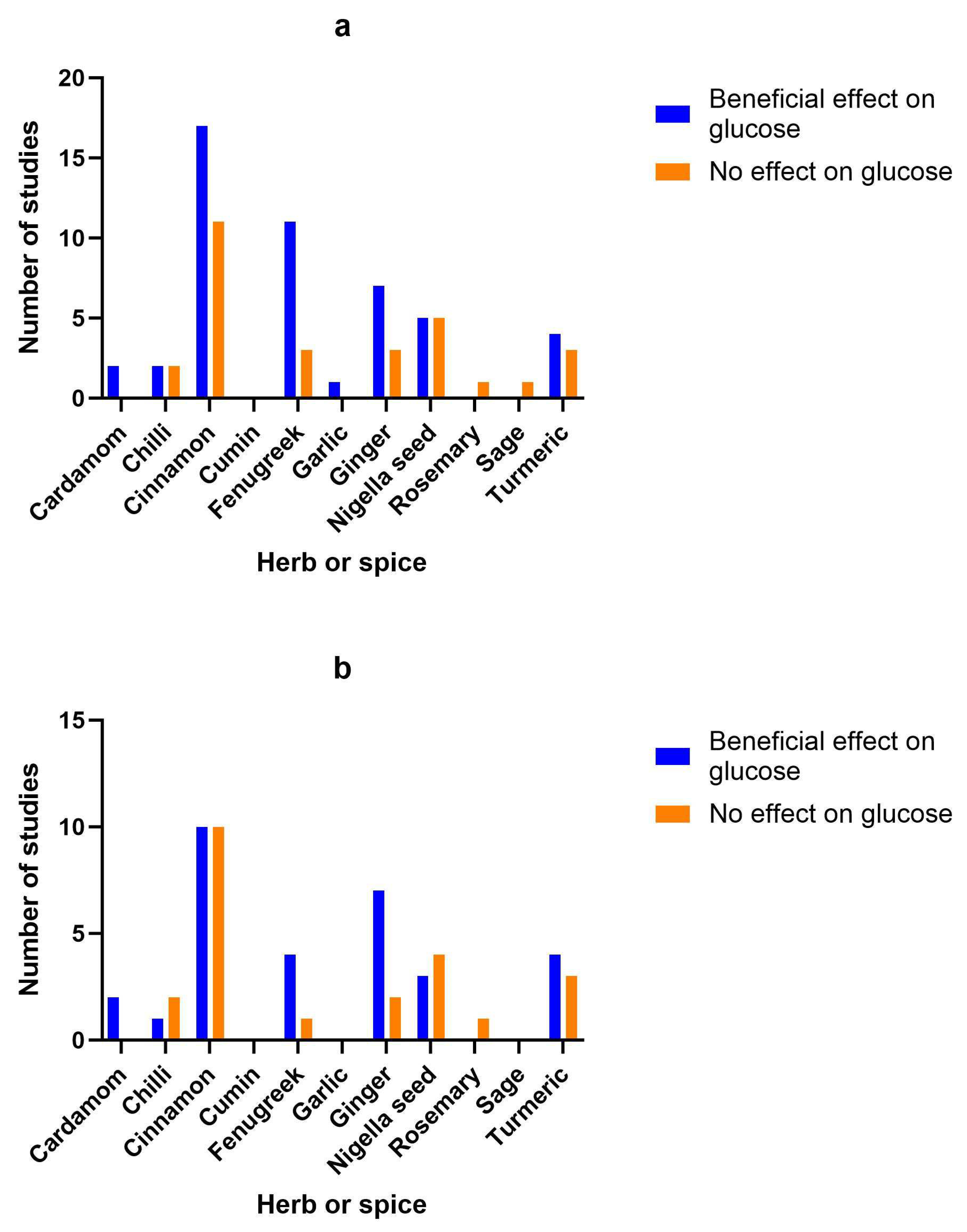
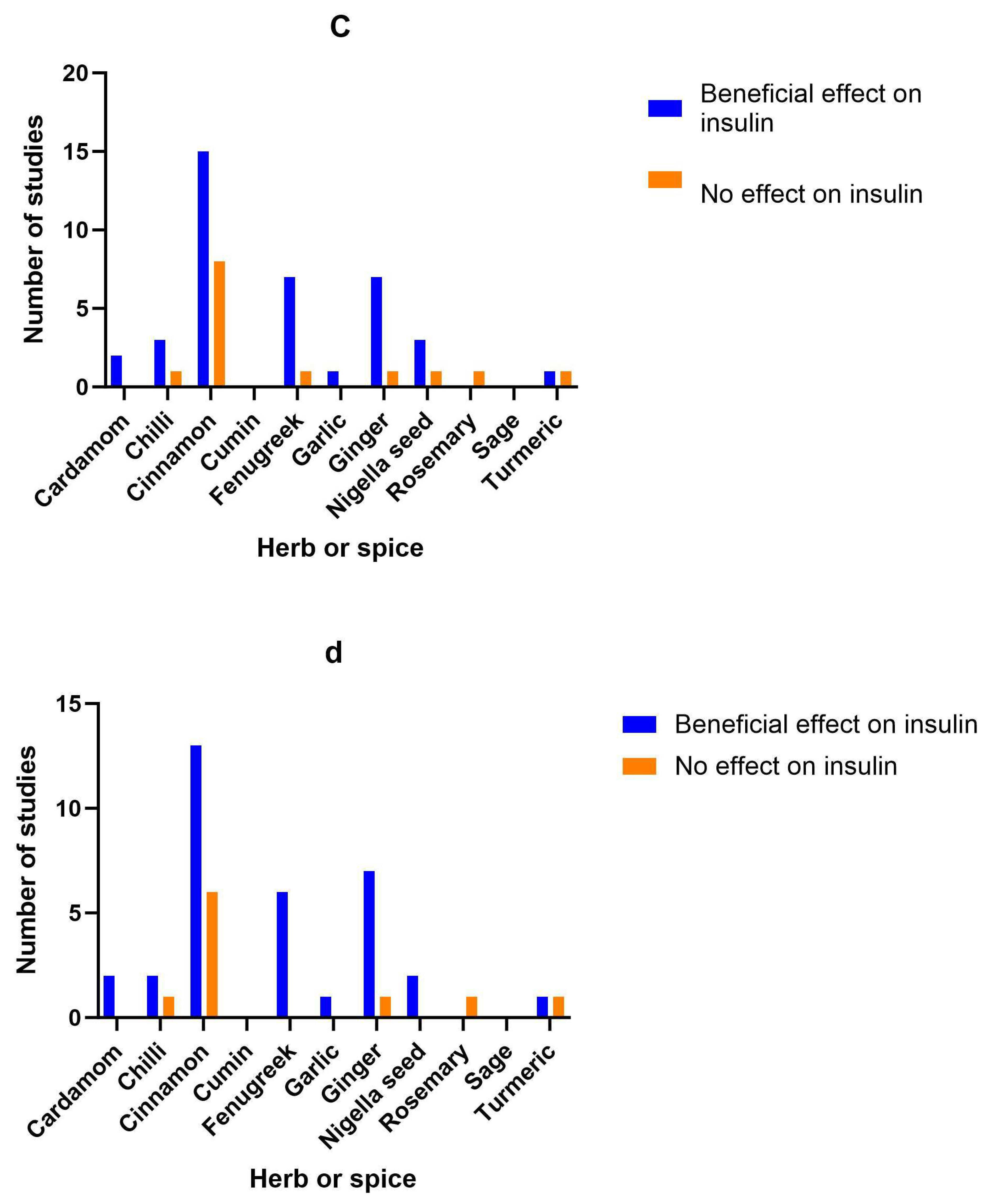
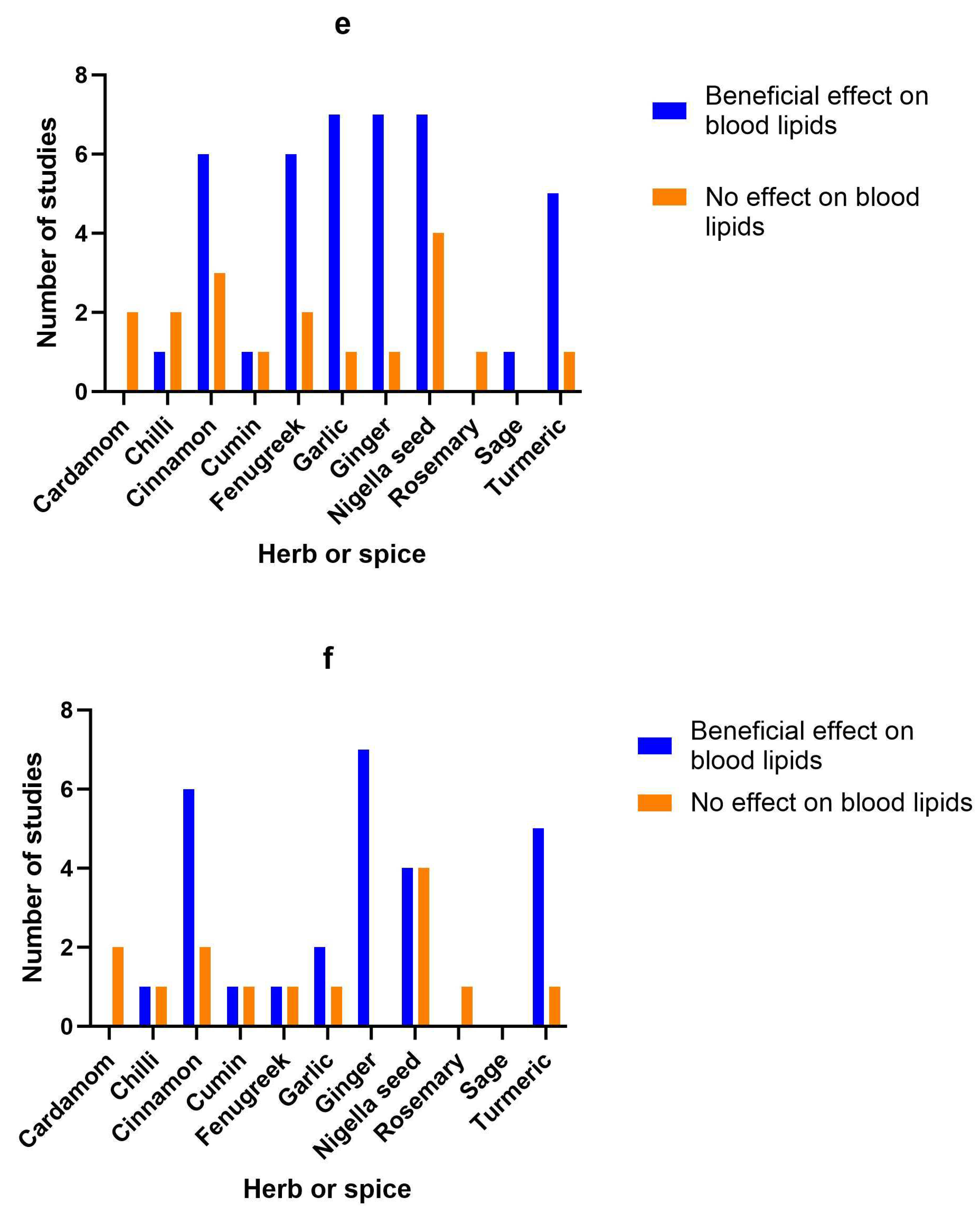
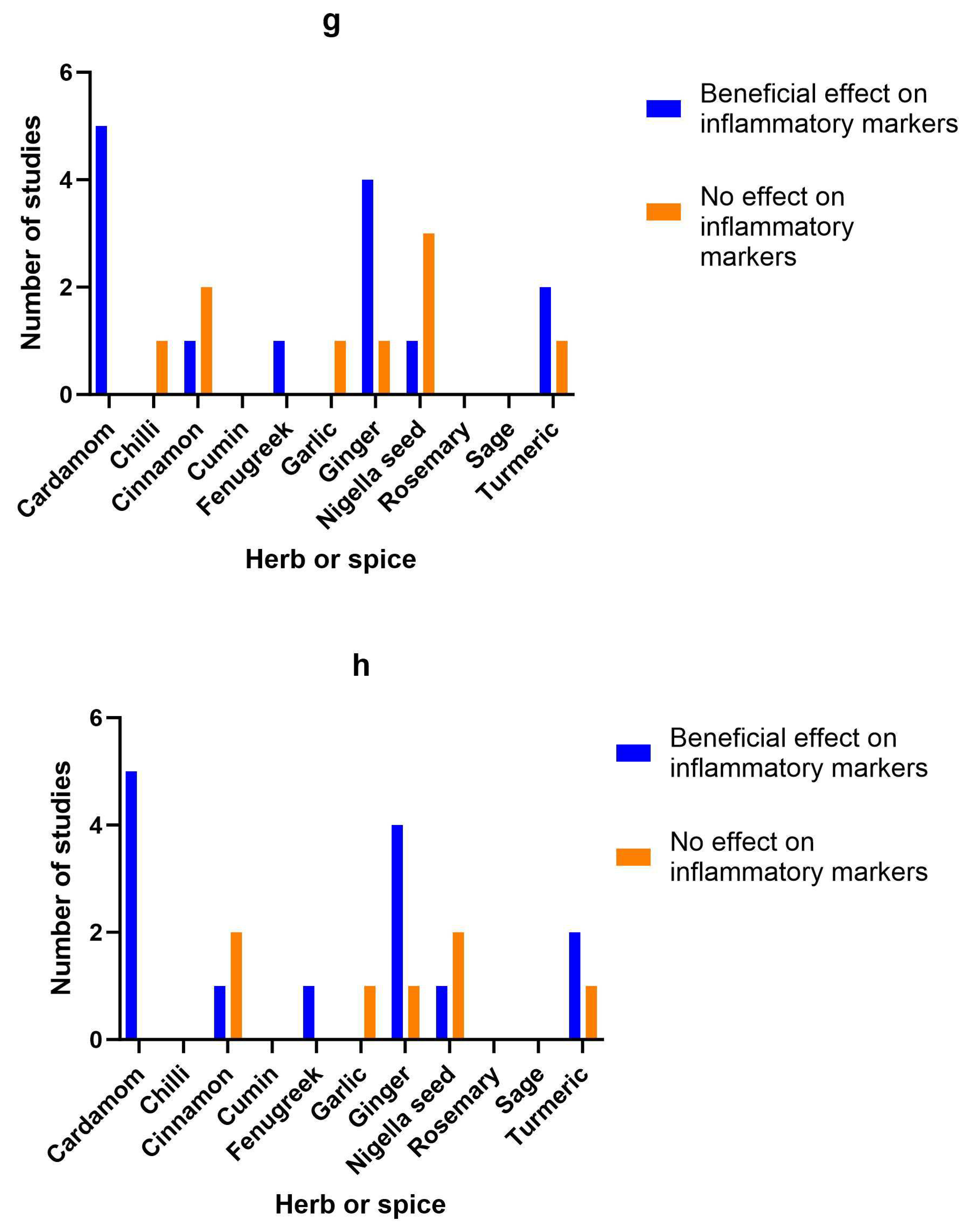

Table 1.
Summary of results from included studies.
| Herb or spice | Reference | Study type | Population | Dose and formulation | Length of intervention | Findings | Study Quality |
|---|---|---|---|---|---|---|---|
| Cardamom | 28 | Single-blind clinical trial | 20 individuals with hypertension | 3g/day in capsules | 12 weeks | BP significantly decreased and fibrinolytic activity increased. Fibrinogen and lipid levels did not change. | Low |
| 32 | Double-blind RCT | 80 prediabetic subjects | 3g/day in capsules | 8 weeks | Inflammatory markers CRP, CRP:IL-6 ratio and oxidative stress marker MDA were all decreased significantly | High | |
| 29 | Double-blind RCT | 83 overweight or obese diabetic patients | 3g/day in capsules | 10 weeks | There was an improvement in HbA1c, insulin control and TG and an increase in Sirt1. Cholesterol levels did not change. | High | |
| 36 | Double-blind RCT | 87 overweight or obese patients with NAFLD | 3g/day in capsules | 12 weeks | Cardamom improved fatty liver grade, blood glucose, lipids and irisin, but BMI, total cholesterol and FBG were not changed. | High | |
| 37 | Double-blind RCT | 83 pts with type 2 diabetes | 3g/day in capsules | 10 weeks | Cardamom led to a sig decrease in CRP and systolic BP, and an increase in serum NO. Serum ADMA and diastolic BP did not change. | High | |
| 31 | Double-blind RCT | 83 overweight pts with type 2 diabetes | 3g/day in capsules | 10 weeks | VCAM, ICAM, E-selectin and IL-6 were sig decreased in the cardamom group. MMP-9 and CD163 levels were unchanged. | High | |
| 35 | Double-blind RCT | 87 pts with NAFLD | 3g/day in capsules | 12 weeks | Cardamom sig increased Sirt1 and decreased inflammatory markers hs-CRP, IL-6, TNFα and liver marker ALT, as well as improving the degree of fatty liver. Weight, BMI and AST did not change. | High | |
| 34 | Double-blind RCT | 194 obese women with PCOS | 3g/day in capsules | 16 weeks | Anthropometric indices decreased. Glycemic indices and androgen hormones improved. | High | |
| 33 | Double-blind RCT | 194 obese women with PCOS | 3g/day in capsules | 16 weeks | LH, androstenedione and dehydroepiandrosterone were decreased. FSH increased. Inflammatory markers TNFα, IL-6 and CRP were decreased | High | |
| Chilli | 42 | Cross-over clinical trial | 7 healthy volunteers | 30g fresh chilli | Single dose | A combination of chilli and medium-chain TG sig increased diet-induced thermogenesis | Low |
| 38 | Randomized cross-over study | 36 healthy participants | 30g/day chilli in food | 8 weeks | When participants with a BMI >26 consumed a chilli-containing meal after 4 weeks of daily chilli, there was reduced C-peptide and insulin and higher hepatic clearance of insulin. But blood glucose and energy expended were not sig changed. | High | |
| 39 | Randomized cross-over study | 27 healthy adults | 30g/day chilli in food | 8 weeks | Consumption of chilli increased the resistance of lipoproteins to oxidation, but had no effect on serum lipids, lipoproteins and total antioxidant score. | Low | |
| 40 | Randomized cross-over study | 36 healthy participants | 30g/day chilli in food | 8 weeks | There were no effects on metabolic or vascular parameters (glucose, lipids, BP, insulin). However, in men, chilli decreased resting heart rate and increased myocardial perfusion time. | High | |
| 9 | Randomized cross-over study | 34 healthy overweight volunteers | Meal containing chilli with 5.82mg total capsaicinoids | Single dose | Chilli decreased post-prandial insulin when added to a meal. Metabolic rate, core temperature, CRP and microvascular reactivity were unchanged. | Low | |
| 46 | Cross-over clinical trial | 40 healthy adults | 0.6g in food | Single dose | Eating a meal with chilli in increased the desire to eat sweet food, but had no impact on energy intake | Low | |
| 45 | Randomized cross-over study | 12 healthy adults | 10mg capsaicinoids/day in capsules | 5 weeks | There was no change in anthropometric and metabolic measurements from chilli consumption. Chilli increased the firmicutes/bacteroidetes ratio and faecalibacterium abundance that coincided with the increase of plasma levels of GLP-1 and GIP and the decrease of plasma ghrelin level. Benefits were linked to gut enterotypes. | Low | |
| 47 | Double-blind RCT | 42 pregnant women with gestational diabetes | 1.25g/day added to food | 4 weeks | Postprandial glucose, insulin and insulin resistance were sig reduced by chilli. Serum cholesterol and triglyceride were also reduced by chilli. Serum calcitonin gene-related peptide was sig increased by chilli. When the babies were born, chilli had sig reduced the incidence of large-for-gestational age newborns. | High | |
| 49 | Prospective cohort study | 12970 healthy adults | <20g/day up to >50g/day in food | 9 years | Chilli intake was inversely associated with risk of hypertension in Chinese adults | ||
| 48 | Prospective cohort study | 12970 healthy adults | <20g/day up to >50g/day in food | 9 years | There was a positive association between chilli intake and energy intake, however, chilli consumption was inversely associated with incidence of overweight/obesity | ||
| 41 | Cross-over clinical trial | 12 healthy adults | 5g in capsules | Single dose | When 5g of chilli was administered in a capsule after a glucose challenge, plasma glucose levels were sig lower after 30 and 45 mins than those in the placebo group. Insulin levels in the chilli group were sig higher than in the placebo group at 1 and 2 hours after glucose challenge. | Low | |
| 43 | Single-blind, randomized, cross-over trial | 14 healthy volunteers | 3.09g/day in food | 36 hours | Chilli increased fat oxidation and prevented reductions in sleeping metabolic rate, diet-induced thermogenesis or resting energy expenditure that were caused by restricting food intake. This indicates a potential beneficial effect in dieting individuals. There was no effect of chilli on BP | Low | |
| 44 | Single-blinded, randomized, cross-over design | 15 healthy adults | 3.09g/day in food | 36 hours | Chilli significantly decreased the desire to eat and increased satiety and fullness, particularly when participants under-ate. | Low | |
| Cinnamon | 59 | Single-blind randomized cross-over study | 8 sedentary, healthy males | 3g/day in capsules | 2 weeks | Cinnamon reduced glucose response to a glucose challenge and improved insulin sensitivity, but effects were not long-lasting once cinnamon consumption ceases. | High |
| 74 | Double-blind RCT | 25 post-menopausal women with type 2 diabetes | 1.5g/day in capsules | 7 weeks | Cinnamon did not improve fasting plasma glucose or insulin concentrations, whole-body oral glucose tolerance, or blood lipid profiles | Low | |
| 58 | Randomized cross-over study | 7 lean, healthy adults | 5g in capsules | Single dose | Cinnamon reduced plasma glucose responses to glucose tolerance tests and improved insulin sensitivity | Low | |
| 53 | Randomized cross-over study | 15 healthy adults | 1 or 3g/day in food | Single dose | Ingestion of 3 g cinnamon reduced postprandial serum insulin and increased GLP-1 concentrations without significantly affecting blood glucose, GIP, the ghrelin concentration, satiety, or GER in healthy subjects. 1g did not have an effect | High | |
| 55 | Single-blind randomized cross-over study | 9 healthy young adults | 3g in capsules | Single dose | 3 g cinnamon did not alter the postprandial response to a high-fat test meal. No change in gastric emptying, glucose response, arterial function, oxidative stress or appetite. | High | |
| 87 | Double-blind cross-over RCT | 10 individuals with impaired glucose tolerance | 6g in capsules | Single dose | No sig differences in glucose or insulin responses compared with placebo | High | |
| 88 | Double-blind cross-over RCT | 10 young, sedentary obese women | 5g in capsules | Single dose | Peak blood glucose was lower in the cinnamon group, but blood insulin and insulin sensitivity/resistance were not affected. | High | |
| 71 | Double-blind RCT | 26 pts with type 2 diabetes | 1g/day in capsules | 12 weeks | Cinnamon sig reduced FBG by 6 weeks that this was maintained for the whole 12 weeks of the study. The decrease in HbA1c was not significant. Serum glutathione and superoxide dismutase were sig increased by cinnamon at 12 weeks, while MDA was sig reduced, indicating an overall antioxidant effect. | Low | |
| 54 | Randomized cross-over study | 30 healthy obese or normal weight individuals | 6g powder in food | Single dose | Cinnamon sig reduced blood glucose in obese and healthy weight individuals | Low | |
| 51 | Randomized clinical trial | 30 healthy adults | 100ml cinnamon tea | Single dose | Cinnamon sig decreased postprandial maximal glucose level | Low | |
| 52 | Crossover clinical study | 14 healthy individuals | 6g powder in food | Single dose | Cinnamon sig reduced the postprandial glucose response and the gastric emptying rate. | Low | |
| 50 | Randomized crossover study | 10 healthy individuals | 6g in food | Single dose | Cassia cinnamon, but not Ceylon cinnamon, reduced postprandial insulin and glucose responses | Low | |
| 83 | Double-blind RCT | 45 women with PCOS | 1.5g/day in capsules | 24 weeks | Menstrual cyclicity improved for women taking cinnamon with no effect on insulin resistance or serum androgens | High | |
| 64 | Single-blind RCT | 109 adults with diabetes | 1g/day in capsules | 12 weeks | Cinnamon lowered HbA1c | High | |
| 72 | Single-blind RCT | 60 patients with type 2 diabetes | 1.5g/day | 12 weeks | Cinnamon had no impact on fasting plasma glucose, HbA1c, or serum lipids | ||
| 63 | Double-blind RCT | 43 individuals with diabetes | 1g/day in capsules | 12 weeks | Cinnamon produced no significant change in fasting glucose, lipid, A1C, or insulin levels | High | |
| 86 | Double-blind RCT | 50 pts with NAFLD | 1.5g/day in capsules | 12 weeks | significant decreases in HOMA index, fasting blood glucose, total cholesterol, triglyceride, ALT, AST, GGT, and high-sensitivity CRP with cinnamon | High | |
| 73 | Double-blind RCT | 39 adults with diabetes | 3g/day in capsules | 8 weeks | Cinnamon had no effect on glycaemic and inflammatory markers | High | |
| 69 | Double-blind RCT | 44 adults with diabetes | 3g/day in capsules | 8 weeks | Cinnamon had no effect on soluble vascular adhesion molecules | High | |
| 84 | Single-blind RCT | 40 women with PCOS | 1.5g of Ceylon cinnamon in capsules | 8 weeks | Sig improvement in cyclicity with cinnamon, which was equivalent to metformin. No change in fasting blood glucose or serum progesterone or androgen levels. | High | |
| 65 | Double-blind RCT | 39 adults with diabetes | 3g/day in capsules | 8 weeks | Cinnamon had no effect on inflammatory markers | High | |
| 61 | Double-blind RCT | 57 adolescents with diabetes | 1g/day in capsules | 12 weeks | Cinnamon had no effect on A1c or insulin sensitivity | High | |
| 60 | Double-blind RCT | 58 patients with type 2 diabetes | 2g/day in capsules | 12 weeks | Intake of 2g of cinnamon significantly reduced the HbA1c, SBP and DBP among poorly controlled type 2 diabetes patients | High | |
| 75 | Double-blind RCT | 59 adults with type 2 diabetes | 1.2g/day in capsules | 12 weeks | There was no significant change in SBP from baseline when cinnamon was compared with placebo | High | |
| 76 | Double-blind RCT | 136 individuals with type 2 diabetes | 1.5g/day in capsules | 90 days | HbA1c was sig reduced by cinnamon, but there was no effect on FBG. | High | |
| 77 | Double-blind RCT | 61 pts with type 2 diabetes | 2g/day in capsules | 8 weeks | Cinnamon did not sig improve FBG, HbA1c, blood lipids | High | |
| 79 | Double-blind RCT | 84 overweight individuals with PCOS | 1.5g/day in capsules | 8 weeks | Cinnamon increased serum antioxidant capacity, and improved total cholesterol, LDL and HDL | High | |
| 80 | Double-blind RCT | 84 overweight individuals with PCOS | 1.5g in capsules | 8 weeks | Cinnamon significantly decreased serum FBG, insulin, homeostatic model assessment for insulin resistance, total cholesterol and LDL-cholesterol and weight and increased HDL-cholesterol compared with placebo | High | |
| 68 | Triple-blinde RCT | 105 pts with type 2 diabetes | 1g/day in capsules | 12 weeks | Cinnamon sig improved glucose control and reduced BMI | High | |
| 70 | Double-blind RCT | 115 pts with type 2 diabetes | 0.5g/day in capsules | 12 weeks | Cinnamon sig reduced FBG, HbA1c and hepatic enzymes. Probiotics were also effective. | High | |
| 66 | Double-blind RCT | 60 people with type 2 diabetes | 1, 3, or 6g/day in capsules | 40 days | Intake of 1, 3, or 6g of cinnamon per day reduces serum glucose, triglyceride, LDL-cholesterol, and total cholesterol inpeople with type 2 diabetes | High | |
| 85 | Double-blind RCT | 116 Asian Indians with metabolic syndrome | 3g/day | 16 weeks | FBG, HbA1c, waist circumference, and BMI were significantly reduced by cinnamon. Waist-hip ratio, BP, serum total cholesterol, LDL-cholesterol, serum triglycerides, and HDL-cholesterol were also sig improved. | High | |
| 67 | Triple-blind RCT | 160 people with type 2 diabetes | 3g/day | 12 weeks | Cinnamon reduced HbA1c and blood glucose | High | |
| 78 | Triple-blind RCT | 140 patients with diabetes | 1g/day | 12 weeks | Cinnamon supplementation led to improvement of all anthropometric (BMI, body fat, and visceral fat), glycemic (FBG, 2hpp, HbA1C, fasting insulin, and insulin resistance), and lipids (cholesterol, LDL-c and HDL-c) outcomes (except for triglycerides) | High | |
| 82 | Double-blind RCT | 59 women with PCOS | 1.5g/day | 12 weeks | fasting insulin, HOMA-IR, LDL and HDL were sig reduced in the cinnamon group. Changes in blood sugar, serum androgen levels and anthropometric measures were not significant. | High | |
| 57 | Open, randomized, cross-over clinical trial | 21 healthy volunteers | 2g in 200ml hot water | Single dose | No sig difference in energy expenditure, dietary-induced thermogenesis, hunger fullness and desire to eat. However, cinnamon tea decreased satiety and increased food intake in the subsequent meal. | Low | |
| 56 | Randomized cross-over study | 18 healthy adults | 4g | Single dose | Cinnamon decreased blood glucose and satiety 15 min after test meal, but didn't decrease blood sugar overall. | Low | |
| Cinnamon and ginger | 81 | Double-blind RCT | 83 women with PCOS | 1.5g of cinnamon or ginger | 8 weeks | Cinnamon and ginger both sig decreased weight and BMI. Insulin resistance decreased, but only in the cinnamon group. FSH and LH sig decreased in the ginger group, while testosterone was sig reduced in the cinnamon group. | High |
| Cinnamon, cardamom, saffron, ginger | 62 | Single-blind RCT | 208 pts with type 2 diabetes | 3g | 8 weeks | No significant difference in BP, serum soluble (s)ICAM-1 concentrations and anthropometric measures | High |
| Cumin | 92 | Randomized clinical trial | 88 overweight/obese women | 6g/day | 12 weeks | Cumin powder reduced serum levels of fasting cholesterol, triglyceride, and LDL and increased HDL. Weight, BMI, waist circumference, fat mass and its percentage significantly reduced | High |
| Cumin and cinnamon | 89 | Double-blind RCT | 99 women with dyslipidemia | 3g/day | 8 weeks | Cumin and cinnamon both sig reduced total cholesterol compared with placebo. Differences in triglycerides, HDL and LDL were not significant. | High |
| Fennel and fenugreek | 93 | Single-blinded cross-over trial | 9 healthy women | 2g fennel infused in 250ml of water and strained. 24g of fenugreek, infused in 250ml of water and strained. | Single dose (with 1-week washout between each arm of the study) | Both fennel and fenugreek increased feelings of fullness and decreased desire to eat food, however, there were no changes in amount of food consumed after drinking either tea compared with placebo tea. | Low |
| Fenugreek | 112 | Clinical trial | 20 adults with hypercholesterolemia | 12.5-18g/day | 4 weeks | Total cholesterol and LDL cholesterol sig decreased at both doses. | Low |
| 108 | Clinical trial | pts with type 1 diabetes | 100g/day | 10 days | Fenugreek sig reduced fasting blood sugar, improved glucose tolerance, and reduced LDL, total cholesterol and triglycerides | ||
| 104 | Clinical trial | Type 2 diabetics | 15g | Single dose | Postprandial glucose was sig decreased, but there was no impact on insulin or lipids | ||
| 95 | Double-blind RCT | 13 healthy volunteers | 3g/day | 10 days | Fenugreek improved glucose tolerance and insulin sensitivity (as shown by reduction in melanin-concentrating hormone) | High | |
| 94 | Double-blind cross-over RCT | 10 healthy volunteers and 6 pts with type 2 diabetes | Bread with 10% fenugreek | Single dose | Adding fenugreek (1 part to 9 parts of wheat flour) reduced the glycaemic response and GI of bread in both healthy volunteers and diabetics | Low | |
| 102 | Clinical trial | 18 pts with type 2 diabetes | 10g/day | 8 weeks | FBS, TG and VLDL-C decreased significantly (25 %, 30 % and 30.6 % respectively) after taking fenugreek seed soaked in hot water whereas there were no significantly changes in lab parameters in cases who consumed it mixed with yoghurt | Low | |
| 103 | Double-blind RCT | 8 pts with diabetes | 5.6g in bread | Single dose | Blood glucose was not changed, but total insulin concentration decreased | High | |
| 96 | Randomized cross-over study | 10 healthy adults | Bread with 10% fenugreek | Single dose | Adding fenugreek reduced the glycaemic response and GI of bread | Low | |
| 105 | Randomized clinical trial | 12 pts with uncontrolled diabetes | 2g/day | 12 weeks | Blood glucose was not changed, but fasting insulin level increased significantly. The ratio of HDL:LDL sig decreased | Low | |
| 110 | Parallel randomized study | 48 pts with type 2 diabetes | 15g/day fenugreek powder | 8 weeks | Fenugreek sig decreased CRP and increased superoxide dismutase. There was no effect on glutathione peroxidase activity, total antioxidant capacity, IL-6 or TNFα | High | |
| 109 | Clinical trial | 60 type 2 diabetics | 25g/day | 24 weeks | Serum cholesterol and triglyceride were sig reduced | Low | |
| 97 | Cross-sectional observational study | 25 patients with type 2 diabetes | 5g/day | 12 weeks | Fasting blood glucose was decreased significantly by month 2. Postprandial blood glucose level was sig lower by month 3. | ||
| 99 | Parallel randomized study | 50 pts with type 2 diabetes | 15g/day fenugreek powder | 8 weeks | Fenugreek sig decreased fasting blood glucose, and liver enzymes, serum ALT and alkaline phosphatase, compared with baseline. Compared with control group, SBP, AST and irisin (a marker of metabolic health) were decreased. | High | |
| 98 | RCT | 114 pts with type 2 diabetes | 50g/day | 4 weeks | Fenugreek improved lipid metabolism | Low | |
| 113 | Double-blind RCT | 56 adults with borderline hyperlipidemia | 8g/day | 8 weeks | TG, LDL, total cholesterol and FBG were sig decreased by fenugreek | High | |
| 106 | Triple-blind RCT | 88 pts with type 2 diabetes | 10g/day | 8 weeks | Fenugreek seeds significantly decreased FBG and HbA1c, serum levels of insulin, HOMA-IR, total cholesterol and TG and increased serum levels of adiponectin | High | |
| 100 | Double-blind RCT | 125 pts with type 2 diabetes | 10g/day | 8 weeks | Fenugreek alone and fenugreek combined with nutrition training sig decreased FBG, HbA1c, BMI and waist circumference compared with placebo. | High | |
| 101 | Double-blind RCT | 62 pts with type 2 diabetes | 10g/day fenugreek powder | 8 weeks | Fenugreek sig improved mean FBG, HgA1C, BMI, waist circumference, DBP, and quality of life | High | |
| 107 | Randomized cross-over study | 8 healthy individuals | 25g | single dose | Fenugreek seeds sig reduced the rise in blood glucose and insulin caused by a meal. | Low | |
| Garlic | 117 | Clinical trial | 40 patients with metabolic syndrome | 100mg/kg bodyweight crushed garlic | 4 weeks | Raw crushed garlic significantly reduced waist circumference, SBP and DBP, TG, FBG and significantly increased serum HDL cholesterol. There was no significant difference found in BMI | Low |
| 120 | Clinical trial | 4 healthy adults | 40g fresh garlic | 1 week | Garlic sig reduced the serum cholesterol and triglycerides when consumed with a high-fat diet | Low | |
| 121 | Clinical trial | 20 healthy individuals | 3g/day | 90 days | Garlic sig reduced total cholesterol and LDL, but had no impact on toal bacterial faecal count | ||
| 119 | Single-blind randomized cross-over study | 18 healthy volunteers | 4.2g | 1 week | Baseline values of platelet function were within normal range in all volunteers. Platelet function was not impaired by single and repeated oral consumption of Greek tsatsiki containing raw garlic | Low | |
| 116 | Randomized clinical trial | 112 hyperlipidemic patients | 20g/day | 8 weeks | Garlic and a combination of garlic and lemon sig reduced blood lipids (total cholesterol, TG and LDL) and BP, while increasing HDL. | Low | |
| 114 | Retrospective cohort study | 101 healthy adults | There was a significant association between people who eat higher levels of garlic in the diet and those with lower SBP. 232g garlic/month = <100mmHg vs 148g garlic/month = >120mmHg | ||||
| 118 | Double-blind RCT | 90 overweight smokers | 2.1g/day | 12 weeks | Garlic had no significant effect on inflammatory biomarkers, endothelial function, or lipid profile in normolipidemic subjects with risk factors for CVD | High | |
| 125 | Double-blind RCT | 90 pts with NAFLD | 1.6g/day | 12 weeks | Garlic decreased hepatic steatosis, liver enzymes and blood lipids (total cholesterol, TG, HDL and LDL) | High | |
| 124 | Double-blind RCT | 90 pts with NAFLD | 1.6g/day | 12 weeks | Waist circumference, body fat, FBG, insulin and insulin resistance sig improved. Skeletal muscle mass increased and antioxidant capacity increased. | High | |
| 123 | Double-blind RCT | 90 pts with metabolic syndrome | 1.6g/day | 12 weeks | Garlic increased HDL. Sig decreases in waist circumference, BP, TG, insulin and appetite. | High | |
| 115 | Cross-sectional cohort study | 22812 adults | Raw garlic | There was an inverse association between higher garlic intake and prehypertension | |||
| Garlic and coriander seed | 91 | Single-blind RCT | 80 pts with hyperlipidemia | 2g/day | 40 days | Garlic and coriander improved BMI, total cholesterol, HDL and LDL. Garlic powder was more effective than coriander | Low |
| Ginger | 143 | Double-blind RCT | 160 obese children with NAFLD | 1g/day | 12 weeks | Serum FBG and CRP, BMI, waist circumference, AST, hepatic steatosis, total cholesterol and LDL sig decreased with ginger. | High |
| 127 | Placebo-controlled study | 23 healthy male volunteers | 1g | Single dose | Ginger had no effect on thermoregulatory function, but increased fat utilisation in the morning | High | |
| 126 | Randomized cross-over study | 18 healthy volunteers | 15g raw ginger or 40g cooked ginger | 2 weeks | Ginger did not affect thromboxane production | High | |
| 128 | Randomised cross-over study | 10 healthy men | 2 g | 2 days | Ginger significantly enhanced thermogenesis and reduced hunger and food intake. | Low | |
| 139 | Double-blind RCT | 20 60-year-old patients with diabetes | 3 g | 12 weeks | Significant improvements found in blood glucose, insulin resistance, inflammatory and oxidative markers (CRP and MDA). | High | |
| 140 | Double-blind RCT | 45 diabetic patients | 2g/day | 10 weeks | Ginger supplementation decreased ADMA serum levels (although this change wasn't sig different to placebo), but had no effect on sICAM-1. | High | |
| 144 | Double-blind RCT | 50 pts with NAFLD | 1.5g/day of ginger | 12 weeks | No sig difference between ginger and placebo for anthropometric measurements or liver markers. However, FBG and insulin resistance were sig improved by ginger. Serum lipids (total cholesterol and LDL) and CRP sig decreased in the ginger group. | High | |
| 141 | Double-blind RCT | 45 diabetic patients | 2g/day | 10 weeks | No effect of ginger on anthropometric measurements or NFκB | High | |
| 135 | Double-blind RCT | 64 pts with type 2 diabetes | 2g/day | 8 weeks | TNFα and hs-CRP were sig reduced by ginger. IL-6 was reduced by ginger compared with baseline, but not sig compared with placebo | High | |
| 134 | Double-blind RCT | 64 pts with diabetes | 2g/day | 8 weeks | Ginger supplementation significantly lowered the levels of insulin, LDL-cholesterol, TG and the HOMA index and increased the QUICKI index, but had no effect on FBG, total cholesterol, HDL-C and HbA1c. | High | |
| 138 | Double-blind RCT | 88 diabetics | 3g/day | 8 weeks | Ginger improved fasting blood glucose, insulin levels and insulin sensitivity | High | |
| 129 | Double-blind RCT | 80 healthy obese women | 2g/day | 12 weeks | Ginger decreased anthropometric measurements and appetite | High | |
| 137 | Double-blind RCT | 70 women with gestational diabetes | 1.5g/day | 6 weeks | Ginger treatment significantly reduced the levels of FBS, serum insulin and HOMA index, but did not affect postprandial blood sugar | High | |
| 131 | Double-blind RCT | 70 Obese women | 2g/day | 12 weeks | Ginger sig reduced blood glucose, total cholesterol, TG and LDL/HDL, while increasing MDA and HDL. Body weight, waist circumference and BMI were also sig reduced without any difference in energy and macronutrient intake between groups. | High | |
| 145 | Pilot double-blind RCT | 60 hypothyroid patients with normal serum TSH | 1g/day | 30 days | Ginger sig reduced the thyroid symptom score. Additionally, weight gain, cold intolerance, constipation, dry skin, appetite, memory loss, concentration disturbance, and feeling giddy or dizzy domains also sig improved. Ginger supplementation also led to a significant decrease in body weight, BMI, waist circumference, serum TSH, FBG, TG, and total cholesterol levels compared to the placebo. | High | |
| 136 | Double-blind RCT | 70 pts with type 2 diabetes | 1.6 g | 12 weeks | Ginger sig reduced multiple markers of metabolic health (blood glucose, insulin, insulin resistance, cholesterol) and inflammation (CRP and prostaglandin). | High | |
| 130 | Double-blind RCT | 80 Obese women | 2g | 12 weeks | Statistically significant reduction in BMI, serum insulin and HOMA-IR. | High | |
| 132 | Double-blind RCT | 103 pts with diabetes | 1.2g/day | 12 weeks | Ginger sig reduced fasting blood glucose and total cholesterol | High | |
| 133 | Double-blind RCT | 41 pts with type 2 diabetes | 2g/day | 12 weeks | Ginger supplementation significantly reduced the levels of fasting blood sugar, HbA1c, apolipoprotein B, apolipoprotein B/apolipoprotein A-I and MDA in ginger group in comparison to baseline, as well as control group, while it increased the level of apolipoprotein A-I | High | |
| 142 | Double-blind RCT | 85 pts with hyperlipidemia | 3g/day | 45 days | TG and cholesterol levels were sig lower in the ginger group than placebo. Changes in LDL and HDL were not significant between the two groups | High | |
| Ginger and fenugreek | 111 | Placebo-controlled study | 30 patients with coronary artery disease and 30 healthy individuals | 4g/day or 10g one-off dose of ginger. 5g/day fenugreek | 12 weeks | Ginger did not affect platelet aggregation when given at 4g/day, but 10g single dose reduced platelet aggregation. Ginger had no effect on blood sugar or blood lipids. Fenugreek had no effect on cholesterol, TG or blood sugar in healthy individuals, but reduced cholesterol and triglycerides in pts with coronary artery disease and diabetes | Low |
| Mustard, black pepper, ginger, horseradish | 27 | Single-blind cross-over trial | 22 young, healthy males | 20g ginger or 1.3g of black pepper | Single dose | Ginger and black pepper had no effect on appetite, energy intake or diet-induced thermogenesis | High |
| Nigella seeds | 153 | Double-blind cross-over RCT | 51 pts with metabolic syndrome | 3g/day | 8 weeks | Nigella had no sig effect on BP, weight, waist circumference, FBG and BMI | High |
| 152 | Double-blind cross-over RCT | 51 pts with metabolic syndrome | 3g/day | 8 weeks | No sig effect of Nigella on blood lipids, apolipoproteins and inflammatory factor | High | |
| 146 | Double-blind RCT | 30 healthy male volunteers | 1g/day | 4 weeks | Nigella seeds had no effect on glycaemia or insulin. Total cholesterol and LDL-cholesterol were decreased with no effect on triglycerides or HDL-cholesterol. | Low | |
| 160 | Clinical trial | 94 pts with type 2 diabetes | 1, 2 or 3g/day | 12 weeks | Sig reductions in FBG, postprandial glucose, HbA1c and insulin resistance from 2g/day. No effect on serum C-peptide or body weight. | Low | |
| 151 | Placebo-controlled study | 35 menopausal women with metabolic syndrome | 1g/day | 8 weeks | No sig change in body weight. Nigella sig reduced FBG. Total cholesterol, TG and LDL were sig reduced. HDL change wasn't sig. | Low | |
| 155 | Randomized controlled trial | 37 menopausal women with moderate risk of hyperlipidemia | 1g/day | 8 weeks | Sig decrease in hyperlipidemia from Nigella | Low | |
| 158 | Single-blind, non-randomized trial | 114 pts with type 2 diabetes | 2g/day | one year | N sativa group had a significant decline in TC, LDL-cholesterol, total cholesterol/HDL-C and LDL/HDL ratios, as well as DBP, mean arterial pressure and heart rate. | High | |
| 156 | Double-blind RCT | 73 adults with hyperlipidemia | 2g/day | 6 weeks | No significant effects were seen for blood sugar or lipids | High | |
| 149 | Double-blind RCT | 40 pts with Hashimoto's thyroiditis | 2g/day | 8 weeks | Nigella sativa supplementation significantly reduced anthropometric variables including weight, BMI, and waist circumference. Serum TSH and anti-TPO concentrations reduced while serum T3 increased in Nigella sativa treated group. VEGF also decreased significantly in Nigella group. | High | |
| 161 | Double-blind RCT | 50 pts with NAFLD | 2g/day | 12 weeks | Levels of CRP and NFκB were sig decreased by Nigella. No sig change in hepatic steatosis or TNFα. | High | |
| 162 | Double-blind RCT | 50 pts with NAFLD | 2g/day | 12 weeks | Sig reduction in glucose, insulin and insulin resistance, but no change to lipid profile. Percentage of hepatic steatosis also decreased | High | |
| 150 | Double-blind RCT | 40 pts with Hashimoto's thyroiditis | 2g/day | 8 weeks | Nigella seeds sig decreased TG, LDL, weight and BMI, and increased SOD and total antioxidant capacity. | High | |
| 159 | Double-blind RCT | 114 pts with type 2 diabetes | 2g/day | one year | No change to BMI. Nigella led to a decrease in FBG, HbA1c and insulin resistance | High | |
| 154 | Double-blind RCT | 140 menopausal women with metabolic syndrome | 500mg/day | 8 weeks | LDL-cholesterol, TG, total cholesterol and FBG decreased significantly | High | |
| 148 | Double-blind RCT | 39 men with obesity | 3g/day | 12 weeks | There was no change in serum free testosterone, FBG, TG and inflammatory markers. However, body weight, waist circumference and BP did improve. | High | |
| 157 | Randomized, placebo-controlled trial | 74 individuals with hypercholesterolemia | 2g/day | 4 weeks | Nigella seed sig lowered triglycerides, LDL and cholesterol compared with baseline, but had no effect on blood glucose or HDL. | High | |
| Rosemary | 163 | Double-blind RCT | 110 pts with NAFLD | 4g/day | 8 weeks | There were no sig effects on liver enzymes, anthropometric measurements, FBG, insulin, insulin resistance and blood lipids from rosemary when compared with placebo. | High |
| Sage | 164 | Non-randomized cross-over trial | 6 healthy female volunteers | 600ml sage tea/day | 4 weeks | No effects on blood glucose, but LDL and total cholesterol decreased, while HDL increased. Lymphocyte hsp70 expression also increased | Low |
| Turmeric | 166 | Single-blinded RCT | 42 women with type 2 diabetes and hyperlipidemia | 2.1g/day | 8 weeks | There was a sig improvement in body composition, lipid profile and glycemic status in the turmeric group and the aerobic training or the aerobic training plus turmeric groups compared with control group. The combined group also had sig lower blood lipids, blood glucose and insulin than turmeric alone group. | High |
| 170 | Randomized cross-over study | 14 healthy volunteers | 6g | Single dose | Turmeric increased postprandial insulin without affecting plasma glucose | High | |
| 165 | Open-label, randomized clinical trial | 60 diabetic pts on metformin | 2g/day | 4 weeks | Turmeric sig reduced fasting plasma glucose, but had no effect on post-prandial glucose. Turmeric also increased glutathione, MDA and CRP compared with baseline. LDL cholesterol was sig decreased compared with baseline. | High | |
| 174 | Double-blind RCT | 46 pts with NAFLD | 3g/day | 12 weeks | Turmeric consumption decreased serum levels of glucose, insulin, HOMA-IR and leptin. Changes in weight, BMI and liver enzymes were not significant | High | |
| 167 | Randomized, single-blinded placebo-controlled trial | 42 hyperlipidemic pts with type 2 diabetes | 2.1g/day | 8 weeks | Turmeric alone and turmeric plus aerobic training sig decreased waist circumference, FBG, TG and BP, while HDL cholesterol increased. Metabolic syndrome Z score and inflammatory markers significantly improved in both turmeric groups. | High | |
| 168 | Double-blind RCT | 80 type 2 diabetes mellitus patients (30-70 years old) | 2.1g turmeric powder | 8 weeks | Turmeric was found to significantly decrease body weight, TG and total cholesterol. | High | |
| 173 | Double-blind RCT | 64 pts with NAFLD | 2g/day | 8 weeks | Turmeric sig reduced liver enzymes AST, ALT and GGT compared with placebo. Triglycerides, LDL, HDL and MDA sig decreased from baseline, but weren't sig different from placebo. | High | |
| 169 | Double-blind RCT | 114 pts with type 2 diabetes | 1.2g/day | 12 weeks | Turmeric sig reduced arterial stiffness. No change was found in markers of endothelial function. | High | |
| Turmeric and Nigella seed | 147 | Double-blind RCT | 250 healthy men with metabolic syndrome | 1.5g/day Nigella, 2.4g/day turmeric | 8 weeks | Nigella seed led to sig improvement in triglycerides, total cholesterol, LDL and HDL, but no change to anthropometric measures, blood glucose, BP or inflammation. Turmeric sig improved cholesterol, LDL and inflammation, but not TG, HDL, anthropometric measures, BP or blood glucose. | High |
| Turmeric and cinnamon | 90 | Double-blind RCT | 48 people >60 years with prediabetes | 1g turmeric or 2g of cinnamon | Single dose | Co-ingestion of turmeric with white bread increases working memory independent of body fatness, glycaemia, insulin, or AD biomarkers. Cinnamon had no impact on working memory. Use of turmeric or cinnamon regularly had no impact on glycaemia or insulin responses to breakfast | High |
| Turmeric and red pepper spice | 171 | Double-blind cross-over RCT | 98 overweight or obese women | 2.8g turmeric/day | 4 weeks | Turmeric does not alter oxidative stress or inflammation in overweight/obese females with systemic inflammation, or cause a significant shift in the global metabolic profile | High |
AD: Alzheimer’s disease, ADMA: asymmetric dimethylarginine, ALT: alanine transaminase, AST: aspartate aminotransferase, BMI: body mass index, BP: blood pressure, CRP: c-reactive protein, CVD: cardiovascular disease, DBP: diastolic blood pressure, FBG: fasting blood glucose, FSH: follicle stimulating hormone, GER: gastric emptying rate, GGT: γ-glutamine transpeptidase, GI: glycaemic index, GIP: glucose-dependent insulinotropic polypeptide, GLP: glucagon-like peptide, HbA1c: glycated haemoglobin, HDL: high-density lipoprotein, HOMA-IR: homeostasis model assessment of insulin resistance, 2hpp: 2-hour postprandial, hsp: heat shock protein, IL: interleukin, LDL: low-density lipoprotein, LH: leutenising hormone, MDA: malondialdehyde, MMP: matrix metalloproteinase, NAFLD: non-alcoholic fatty liver disease, NFκB: nuclear factor κB, NO: nitric oxide, PCOS: polycystic ovarian syndrome, pt: patient, QUICKi index: quantitative insulin sensitivity check index, RCT: randomised-controlled trial, SBP: systolic blood pressure, sICAM: soluble intercellular adhesion molecule, Sirt: sirtuin, SOD: superoxide dismutase, TG: triglycerides, TNF: tumor necrosis factor, TPO: thyroid peroxidase, TSH: thyroid-stimulating hormone, VCAM: vascular cell adhesion protein, VEGF: vascular endothelial growth factor.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



