
Submitted:
26 October 2023
Posted:
30 October 2023
You are already at the latest version
Abstract
Musculoskeletal disorders are increasingly prevalent worldwide, causing significant socioeconomic burdens and diminished quality of life. Notably, patellar chondropathy (PC) is among the most widespread conditions affecting the joint structures, resulting in profound pain and disability. Hyaluronic acid (HA) and platelet-rich plasma (PRP) have emerged as reliable, effective, and minimally invasive alternatives. Continuous research spanning from laboratory settings to clinical applications demonstrate the numerous advantages of both products. These encompass lubrication, anti-inflammation, and stimulation of cellular behaviors linked to proliferation, differentiation, migration, and the release of essential growth factors. Cumulatively, these benefits support the rejuvenation of bone and cartilaginous tissues, which are otherwise compromised due to the prevailing degenerative and inflammatory responses characteristic of tissue damage. While existing literature delves into the physical, mechanical, and biological facets of these products, as well as their commercial variants and distinct clinical uses, there is limited discussion on their interconnected roles.
We explore basic science concepts, product variations, and clinical strategies. This comprehensive examination provides physicians with an alternative insight into the pathophysiology of PC as well as biological mechanisms stimulated by both HA and PRP that contribute to tissue restoration.
Keywords:
hyaluronic acid
; platelet-rich plasma
; patellar chondropathy
; regenerative medicine
; orthopedics.
1. Introduction
Patellar chondropathy (PC), also referred to informally as “runner’s knee”, is an orthopedic condition characterized by visible radiological alterations in patellar cartilage and pain in the anterior aspect of the knee [1]. This condition commonly affects younger individuals and the initial changes include swelling, edema and cartilage softening (Figure 1). Notorious factors that contribute to PC are trauma, patellofemoral instability, bony anatomic variations, cartilage vulnerability and abnormal patellar kinematics, or occupational hazards [1].
Although sometimes reversible [1,2], depending on disease stage (Table 1), PC may progress into patellofemoral osteoarthritis (OA) if left untreated [1]. Significant complications associated with PC include medial meniscus injury in association with impaired knee biomechanics and degenerative alterations (Figure 1), which is highly prevalent in affected patients [3]. Although there is no medical consensus regarding a “gold standard” approach, conservative treatments are usually restricted to rest, immobilization, patella stabilization (braces), orthotics, administration of non-steroidal anti-inflammatory drugs (NSAIDs) and physical rehabilitation exercises [4]. However, physicians should always run a thorough evaluation and consider radiological exams and other clinical findings before making a decision. This is of particular importance as failure of conservative strategies in advanced stages of PC may eventually make surgical alternatives required. This typically includes patellar cartilage excision, shaving, drilling, and distal bony patellar realignment procedures [1].
In end stage PC and eventual progression into patellofemoral osteoarthritis, patients may require total knee arthroplasty (TKA), which can generate additional problems. On the one hand, TKA mitigates pain and restores gain in range of motion; on the other hand, it may also contribute to quadriceps weakness and reduced functional capacity, propagating physical limitation after TKA procedures [5]. A recent systematic review [6] revealed that patients receiving TKA presented considerable quadriceps weakness, which remained detectable up to 3 months postoperatively.
The emergence of novel treatments employing the use of orthobiologics have provided physicians feasible alternatives for the management of numerous orthopedic conditions, especially PC [1]. By definition, orthobiologics are organic or synthetic materials that promote enhanced healing of musculoskeletal disorders [7]. Many orthobiologic products have been discussed in the literature, including acellular solutions like hyaluronic acid (HA); and cellular alternatives such as platelet-rich plasma (PRP), injectable platelet-rich fibrin (i-PRF), bone marrow aspirate/bone marrow aspirate concentrate (BMA/BMAC) and adipose tissue derivatives [8,9,10,11,12]. These products can have autologous or allogeneic origins and are known to contain a rich secretome and a wide variety of cells with potent stimulatory effects [16]. These components have shown a satisfactory capacity to modulate the pathophysiology of many disease processes beyond orthopedic conditions, increasing optimism and interest in the field of regenerative medicine [13].
HA and PRP (as well as its derivatives), however, have been extensively investigated in the literature for the treatment of musculoskeletal conditions of the knee, especially in terms of degenerative joint diseases [14,15]. Numerous studies [16,17,18,19,20,21,22,23,24,25,26,27] have demonstrated satisfactory outcomes associated with the application of both PRP and HA, although sometimes PRP may or may not prove to be slightly superior to HA. The effects elicited by PRP include cell recruitment, proliferation, differentiation, neovascularization, cytokine secretion and inflammatory modulation [28]. Similarly, HA attenuates inflammation and induces lubrication, improved biomechanics, cell proliferation, differentiation, migration, and favors anabolic reactions [11]. Collectively, these responses contribute to pain relief and the regeneration of damaged musculoskeletal structures, including bone, tendon and cartilage.
The objective of this manuscript is to present the potential applications of PRP and HA as viable orthobiologic tools for the management of PC.
2. Pathophysiology
Patellar chondropathy is also sometimes referred to as “chondromalacia patellae”, which originates from the Greek language and is broken down into two words: “chrondros”, which means cartilage; and “malakia”, meaning softening [1]. Although complex, there are many factors that contribute to progression of this disease, including direct trauma, patellofemoral instability, bony anatomic variations, cartilage vulnerability and abnormal patellar kinematics, subluxation or occupational hazards [1]. It is worth noting that lifestyle habits may also significantly contribute to general musculoskeletal pathologies affecting locomotor structures, especially in patients with metabolic syndrome (MS) [29,30]. In many ways, PC is quite similar to OA (Figure 1). In fact, it may also be interpreted as a “pre-osteoarthritic” condition, considering the fact that late stage PC ultimately leads to the onset of additional complications, such as patellofemoral OA [1,25].
At the anatomical level, many patients suffering from PC usually present a lower lateral patellar tilt angle, lower trochlear depth, and higher sulcus angle due to pathological dysmorphology [3]. The increased trochlear sulcus angle/trochlear depth ratio is therefore a helpful tool for physicians as a significant predictor of PC [3]. Another significant indicator of PC is subcutaneous knee fat thickness. According to a study published by Kok et al. [31], the subcutaneous knee fat thickness in obese patients with PC was far greater in comparison to the normal group, therefore establishing a significant correlation between subcutaneous knee fat thickness and grade of PC. Furthermore, female patients analyzed in this study displayed thicker subcutaneous knee fat and more severe grades of PC.
Cartilage damage may occur from either noxious biochemical stimuli or direct mechanical forces [29], promoting alterations (Figure 1) that affect both cartilage and the subchondral bone. The alterations that take place beneath the articular cartilage at the osteochondral junction play a role in pain and structural progression of the disease, which may affect additional structures and aggravate pathology [32]. When osteochondral integrity is weakened, the boundary between intra-articular and subchondral compartments is lost, thus exposing the subchondral bone and nerves to noxious biochemical and biomechanical stimuli. The diminishing distinction between bone and articular cartilage, coupled with the unavoidable merging of tissue zones at the interface, correlates with the incursion of blood vessels and sensory nerves into the articular cartilage and the forward progression of endochondral ossification [32]. Increased subchondral bone turnover is also intimately connected to these changes at the osteochondral interface [32]; ongoing biomechanical and biochemical strain on articular cartilage further aggravates chondropathy, subsequently generating additional complications such as microfractures, which, in turn, intensify pain [32]. Researchers believe that the various cytokines and growth factors produced in the early stages of the disease may interact with and harm articular cartilage, which also impairs matrix biosynthesis. This process elicits a positive feedback loop mechanism due to repetitive unsuccessful attempts to repair cartilage and bone, eventually progressing into OA [32,33]. In fact, microfractures can serve as channels for the transport of numerous biomolecules [34,35], including inflammatory cytokines. These inflammatory mediators in turn may attack vital structures in the joint compartment [36]. A previous animal study [37] outlined the interaction between the subchondral bone and articular cartilage in murine knee joints. After measuring matrix permeability, blood vessel invasion and joint structure in both surgically-induced and age-related OA, the researchers compared observations with the control group. No major alterations in tissue matrix permeability appeared to be connected to the disease in either scenario. However, the pathology provoked significant thinning of the subchondral bone and a rise in blood vessel penetration, which breached the calcified cartilage in both cases. This indicates an increased likelihood of cellular interactions between the subchondral bone and articular cartilage in degenerative pathologies stemming from alterations in the overall joint structure.
3. PRP
PRP is a well-known biologic material obtained via the centrifugation of peripheral blood with a concentration 2–5 times above the basal value [14,38,39,40]. It can be prepared either manually or using commercial kits. However, due to the multitude of protocols mentioned in studies, there is no consensus regarding a “gold standard” for PRP preparation. This leads to inconsistencies in the composition of PRP products, resulting in the use of diverse terminologies [28,41,42].
Numerous protocols detail the preparation of platelet-rich plasma. Some of them may require two centrifugation steps (Figure 2) with precise time and centrifugal force (G) specifications [43]. PRP can be produced by means of density gradients of the cell constituents in blood. Following the initial centrifugation, the densest particles (erythrocytes) are separated from the plasma and settle at the bottom layer of the mixture. Right above the erythrocytes, a thin layer rich in leukocytes (and platelets) forms, making up less than 1% of the total blood; this layer is known as the "buffy coat". The uppermost layers of this mix also contain platelets and growth factors, being situated immediately above the buffy coat. Plasma (either including or excluding the buffy coat) is then harvested and subjected to a second, final centrifugation to amplify the concentration of platelets [44].
The final concentration of constituents in a PRP product can differ based on the commercial kits used or the proficiency of the manual technique, especially if automated processes are not the method of choice [43]. Additionally, the end product can be influenced by individual patient factors. Examples of these factors are age, underlying health conditions, use of certain medications and blood circulation [45].
Platelet granules possess numerous bioactive compounds. When activated, these compounds are discharged and subsequently trigger the body's natural healing process [28,46]. Delta granules house substances like magnesium, calcium, adenosine, serotonin, and histamine, which promote clot formation [47]. Alpha granules play a key role in important biological activities like inflammation, blood clotting, immune defense, cell attachment, and cellular proliferation [47]. On the other hand, lambda granules are commonly likened to lysosomes because, just like these organelles, they contain enzymes that break down proteins, lipids, and carbohydrates. As a result, they play a key role in clearing debris and pathogens from damaged tissues [48].
PRP injections can promote rapid neovascularization, enhancing the blood flow and providing essential nutrients to adjacent cells. This is vital for cell rejuvenation and mending of injured tissues [49]. Furthermore, PRP can stimulate many cellular events, including recruitment, division and differentiation of certain cells, therefore ameliorating the healing of complex wounds and injuries [50]. Indeed, numerous research articles have historically highlighted the advantages of PRP therapy in treating a variety of musculoskeletal conditions, with a particular emphasis on knee pathologies. Recent randomized clinical trials (RCTs), meta-analyses and systematic reviews [51,52,53,54,55] have reaffirmed that both leukocyte-poor and leukocyte-rich PRP outperform traditional treatments like HA and NSAIDs. In most of these studies, PRP consistently demonstrated more pronounced benefits in reducing pain and enhancing function for those suffering from symptomatic knee OA, while ensuring safety and efficacy. Only in one of the most recent RCTs [56] a singular intra-articular injection of leukocyte-poor PRP combined with HA (Artz or HYAJOINT Plus) proved to be effective and safe for osteoarthritic knees over a 6-month duration. Notable enhancements were observed in measurements like the visual analogue scale (VAS) for pain, Western Ontario and McMaster Universities Osteoarthritis (WOMAC) scores, Lequesne indices, and Single Leg Stance (SLS) tests at intervals of 1, 3, and 6 months post-treatment.
Robust studies have been conducted in attempts to decipher the regenerative capacities of platelet concentrates. Historically, the advantages of PRP therapy were largely credited to the rich presence of growth factors and their individual biological impacts. Yet, subsequent investigations revealed that PRP also induced remarkable secondary responses, such as the modulation of inflammation [38,57,58,59,60], pro-anabolic stimuli [61], regulation of normal autophagy [62,63], cytokine balance [64,65,66], and anti-catabolic effects [67,68,69]. Moreover, it also plays a direct role in fibrinolytic activities, which are essential for the healing of tissue damage [70]. This holds significant biological importance since the entire fibrinolytic system is vital for attracting mesenchymal stem cells (MSCs), which are crucial for tissue regeneration and repair [28,71]. Finally, an additional positive outcome linked with PRP therapy is the attraction of mononuclear cells. Substances like thrombin and platelet factor 4 (PF4), which are released by platelets, facilitate the gathering of monocytes and drive their transformation into macrophages [72,73,74].
The role of macrophages, in particular, has been much appreciated by researchers due to their adaptability and versatility. Macrophages possess the unique capability to change phenotypes (known as polarization) and even transform into different cell types, such as endothelial cells. This allows them to exhibit varied functions based on the biological signals present in the wound setting [75,76,77]. Macrophages primarily exhibit two main phenotypes: M1 and M2. The M1 phenotype is triggered by microbial elements, taking on a more proinflammatory stance linked with wound cleaning or debridement. Conversely, the M2 phenotype typically arises from type II reactions, expressing anti-inflammatory attributes. This is evident through the increased expression of cytokines like IL-4, IL-5, IL-9, and IL-13 [76]. The polarization of macrophages is largely influenced by the concluding phases of wound healing. M1 macrophages induce neutrophil apoptosis, which drives the clearance process [78]. After the phagocytosis of neutrophils, the production of proinflammatory cytokines is halted, allowing macrophages to undergo polarization and release TGF-β1. This molecule is fundamental in controlling myofibroblast differentiation, which is essential for wound contraction and closure. Consequently, this facilitates the subsiding of inflammation and initiates the proliferative stage of healing [70].
It is important to mention that while PRP offers numerous advantages, it can also lead to negative outcomes in certain situations. This includes potential risks like infections, possibility of neurovascular injury, and discomfort at the injection site. These outcomes might be influenced by the expertise (or lack thereof) of the practitioner administering the treatment and the overall health of the patient. Immunocompromised patients or those more susceptible to specific diseases are at a heightened risk of contracting infections at the treated site [79,80]. Therefore, due to variability in the composition among PRP products and the plethora of other orthobiologic products on the market, PRP might not always stand out as the best option for every patient and every musculoskeletal condition [81,82].
4. Hyaluronic Acid
Hyaluronic acid is a negatively-charged, nonsulfated glycosaminoglycan that is prevalent in various organ systems [83]. HA products with greater molecular weights typically exhibit anti-inflammatory properties as they control the recruitment of immune cells. Lower molecular weights are known to encourage angiogenesis and tissue restructuring during wound healing, however, they might also show increased pro-inflammatory effects in certain cell types, especially in chondrocytes [84,85]. Low-molecular weight (LMW) HA, ranging from 500,000 to 730,000 Daltons, has a less efficient binding to cell surface receptors. This leads to subdued HA synthesis. In reality, this type of formulation is not very advantageous and is more often linked with inflammation. Tanimoto and colleagues [86] evaluated the impact of the pro-inflammatory cytokines tumor necrosis factor alpha (TNF-α) and interleukin 1 beta (IL-1β) on rabbit HA-synthetase (HAS) mRNA expression. Under inflammatory conditions these cytokines elevate HAS mRNA expression, increasing the breakdown and excessive buildup of HA. This therefore negatively affects cell activity. Conversely, medium-molecular weight (MMW) HA seems to be the most convenient strategy as it has been shown to facilitate more robust binding. This activates a greater quantity of HA receptors, which in turn boosts the production of endogenous HA. It is also important to highlight that the large molecules typically found in high-molecular weight (HMW) HA products, for example, might not always display favorable results [87]. While these large molecules still connect to HA receptors, their expansive domains may restrict the availability of unoccupied binding sites on the cell surface. This suggests a potentially reduced efficiency in stimulating HA synthesis [87]. Interestingly, however, one study [88] revealed that HMW HA (>1,250 kDa) inhibits pro-inflammatory responses in lipopolysaccharide-mediated macrophage activation. Additionally, it promotes anti-inflammatory responses according to concentration, especially via the expression of genes associated with the M2 macrophage phenotype [88]. Another study [89] showed that intermediate-sized hyaluronan fragments may also play an immunomodulatory role as they interact with Toll-like receptor 4 (TLR4) and orchestrate macrophage polarization to an M2-like phenotype (Figure 3).
In any case, HA is still a critical component of articular cartilage, where it forms a protective layer around chondrocytes. It serves as a lubricant for tendons and joints, diminishing extracellular matrix (ECM) breakdown by inhibiting the synthesis of matrix metalloproteinase (MMP). Its anti-inflammatory properties reduce the effects of TNF-α and interleukin-1 (IL-1), both primary pro-inflammatory agents. As an independent entity, HA proves to be a powerful tool in managing degenerative conditions of the knee, in particular. In fact, its advantages in orthopedic scenarios have been widely recognized in academic circles for years. More recent systematic reviews reaffirm that intra-articular (IA) uses of HA are not only safe but also cost-effective. They reduce pain and enhance knee functionality when assessed against conventional treatments like NSAIDs, corticosteroids, and other painkillers, in general [90,91].
Intra-articular hyaluronic acid (IA-HA) is viewed as a minimally invasive therapeutic approach, and there have been no major systemic side effects documented [92]. This method has demonstrated positive outcomes in laboratory settings. Not only has IA-HA been found to decrease chondrocyte cell death, but it also boosts their growth [93]. For human use, it is best to rely on formulations of medium- (800,000–2,000,000 Daltons) to high-molecular weight HA, as this closely mirrors the conditions and biological attributes of HA naturally generated in the body. Additionally, it is crucial to employ HA sourced from biological synthesis to prevent unwanted adverse reactions [94].
The molecular mechanism at play is associated to the innate ability of HA to bind to cluster of differentiation 44 (CD44) receptors. By doing so, it inhibits the expression of IL-1β, leading to a decreased production of MMPs 1, 2, 3, 9, and 13 [95,96,97], circumventing the action of degradative enzymes in the musculoskeletal framework [98]. Upon connecting to its receptor, HA activates internal signaling routes related to its own proliferation, differentiation, migration, and breakdown [99]. CD44 is the most extensively researched HA receptor due to its presence in almost all human cell types. The affinity between CD44 and HA is vital, determining HA's capacity as a signaling molecule. Nonetheless, this relationship also hinges on factors such as HA concentration and molecular weight, along with the glycosylation of external domains and serine phosphorylation [100]. CD44 aggregates with HMW HA polymers, facilitating interactions with growth factors, ECM proteins, MMPs, and cytokines [101]. The other notable HA surface receptor is CD168. It is present in various cells and governs migration through its interaction with skeletal proteins, even more so during the healing process [100].
HA conveys its protective benefits through two clear phases. The initial phase, referred to as the mechanical stage, sees the synovial fluid being replaced with denser concentrations of HA, resulting in increased viscosity [15]. Furthermore, this facilitates the enhancement and recovery of the lubrication and shock-absorbing attributes of the synovial fluid. It also forms a protective layer around pain receptors, diminishing pain signals [102]. The subsequent and concluding phase is commonly termed the pharmacological stage. In this phase, the biosynthesis of native HA and ECM components occurs [103]. This decreases the depletion of proteoglycans in the cartilage and wards off chondrocyte cell death [104]. Additionally, it reduces the activity of inflammatory cells, thereby minimizing HA breakdown and the generation of pain-inducing agents [15].
5. Discussion
In clinical trials, Synvisc and Hyalgan were the most commonly utilized HA products because of their safety, effectiveness, and enduring benefits, even though they require intra-articular injections [100,105]. Specifically, Hyalgan has demonstrated its ability to boost the survival and growth of human chondrocytes when subjected to reactive oxygen species (ROS) [106]. In recent times, a novel product composed of a blend of HA and lactose-modified chitosan (Chitlac®) has demonstrated encouraging outcomes in amplifying the anti-inflammatory response and therapeutic efficacy of HA for knee pathologies. Both in vitro and in vivo research has indicated a notable enhancement in cartilage regeneration following the application of this derivative in experimentally-triggered knee OA, for example [107,108]. A recent 2021 study further illuminated its benefits. The combination of HA and Chitlac® notably reduces the cytotoxicity of the triamcinolone acetonide-hydroxypropyl-β-cyclodextrin (TA-CD) drug in human chondrocyte cultures. It also maintains its anti-inflammatory properties, underscoring once more the chondroprotective function of HA in the management of inflammatory knee conditions [109]. However, in the face of more advanced and severe stages of joint degeneration, HA by itself might not be enough, creating the need for further treatments like autologous chondrocyte implantation or even PRP injections. Three-dimensional scaffolds made from biodegradable and biocompatible HA-based polymers, like Hyaff-11®, have been effectively used in the past for cultivating human chondrocyte cultures [110]. After the chondrocytes are implanted, the newly regenerated tissue matures and becomes hyaline tissue, as opposed to forming fibrous cartilage [110].
An RCT [111] evaluated the clinical outcomes of PRP and HA both individually and in combination for treating mild to moderate knee OA in 105 patients. The participants were randomly assigned to HA, PRP, or a combination of HA+PRP groups. They underwent 3 intra-articular knee injections of their designated substance, with 2-week gaps between each injection. The clinical results were assessed using the Western Ontario and McMaster Universities Arthritis Index (WOMAC) and the Visual Analogue Scale (VAS) questionnaires at the start and after intervals of 1, 3, 6, and 12 months. The combination of HA and leukocyte-rich PRP was determined to have a significant positive impact on clinical outcomes, with noticeable improvements in physical function and pain reduction observed within the first 30 days post-treatment. These findings might be linked to the ability of HA in offering a functional matrix that possesses supportive scaffold properties, which can enhance cartilage biomechanics and promote tissue repair [112]. A recent study published by Lana et al. [10] offers a detailed description of the “platelet-rich plasma power mix gel”, a robust orthobiologic product that combines PRP, PRF and HA for enhanced effects.
There are a quite few factors that must be taken in consideration before designing a specific treatment strategy for patients. First and foremost, a practitioner must consider safety, efficacy and practicality of orthobiologic preparation, no matter what they are. For example, there are certain processing hurdles associated with viable PRP processing methods. If the manual alternative is chosen, the orthopedic practitioner will need an adequate room, time, equipment and qualified personnel in order to adequately collect and process blood to avoid sample contamination [113], therefore raising costs. The patient’s lifestyle (i.e. diet, drug consumption, stress) and overall metabolic health status are also important because these individual factors influence PRP efficacy and treatment outcome [29,114]. Commercially available PRP kits are not faring any better [115], as quality and quantity may also differ, for various reasons. Moreover, they are also comparably expensive and therefore limit their widespread use across a broader population [116]. HA application on the other hand is faster and does not require any sort of processing as the vials are readily available for easy aspiration and injection.
In regards to cost-effectiveness and comparison with other known treatments for orthopedic conditions, a recently published study has compared IA administration of HA versus PRP for the treatment of symptomatic knee osteoarthritis [117]. In their research, Samuelson and team reported that the cost per quality-adjusted life-year (QALY) for a series of PRP injections stood at $8,635.23/QALY, in contrast to HA injections which cost $5,331.75/QALY. PRP, however, demonstrated a significantly higher effectiveness at the one-year mark. Rosen et al. [118] sought to compare IA-HA with conservative interventions such as physical therapy, orthosis, NSAIDs and other painkillers for early to mid-stage knee OA. In this specific scenario, their findings indicated that HMW HA surpassed LMW HA and physical therapy, offering a more cost-efficient solution while delivering better results. When compared to orthosis and NSAIDs/analgesics, HMW HA proved to be cost-effective.
6. Author’s Note
It is once again important to emphasize that a precise control over the patient’s metabolic health is of great value. Individuals affected by MS are known to have complications regarding tissue repair [29,119]. MS is a cluster of metabolic dysregulations which lead to a state of chronic low-grade systemic inflammation (meta-inflammation) [120]. These dysregulations are commonly referred to as “The Deadly Quartet”, encompassing insulin resistance, dyslipidemia, visceral obesity, and hypertension [29]. In the context of PC, MS itself does not significantly influence cartilage regeneration, however, it does push cartilage homeostasis towards deterioration. Of the various factors associated with metabolic dysregulation, hypertriglyceridemia notably exerts a distinct impact on cartilage metabolism [119]. The state of chronic low-grade systemic inflammation affects many organs and anatomical structures. The exact metabolic pathways exact metabolic pathways through which obesity, in particular, contributes to structural damage of joints do not seem to be fully elucidated. However, it is believed that the elevated adipokine expression from adipose tissue elicits direct and downstream effects which lead to the destruction and remodelling of the joint as whole [121].
Perhaps the most simple and cost-effective approach to mitigate PC progression is to simply adjust lifestyle habits. This is especially relevant since many risk factors associated with MS are amendable. For example, avoiding diets high in saturated fats and refined carbohydrates, combined with regular moderate exercise in order to reduce weight and the biomechanical burden on the knee can reduce the detrimental impacts brought on by MS. However, it is important to note that with weight reduction there may also be relative loss of muscle mass and strength over time as a result of protein deficiency in these patients, which may lead to the recurrence of PC symptoms [122]. Physicians should manage musculoskeletal diseases using both conservative therapies and surgical options on a case-by-case basis, as patients may experience similar conditions but respond differently to treatments. Rather than focusing solely on orthobiologic therapy, practitioners must be even more attentive to a patient’s metabolic health status. Previous studies have depicted a positive correlation between fat tissue volume and PC, including degree of severity [123,124]. Overall, the association of HA and PRP (Figure 3) may promote better clinical outcomes during the early stages of the disease, such as grade I or II (table 1), where the pathological alterations are moderate and still amendable with less invasive techniques [1].
7. Conclusion
Hyaluronic acid is a crucial biological compound naturally present in many tissues. It plays key physiological roles in supporting musculoskeletal integrity, especially in regards to debilitating orthopedic diseases like patellar chondropathy. Intra-articular injections of hyaluronic acid represent a minimally invasive approach with proven efficacy and safety. This treatment option offers numerous improvements that target inflammation, lubrication, biomechanics, cell growth, differentiation, migration and protein biosynthesis.
PRP products obtained by whole blood centrifugation are another viable orthobiologic tool aiming at an increased concentration of platelets, surpassing the baseline level. This tool fosters rapid growth in bone and soft tissues with minimal adverse reactions. Autologous PRP therapy has consistently demonstrated promising clinical outcomes in stimulating and augmenting the healing of various tissue injuries, just like hyaluronic acid. The effectiveness of this alternative treatment is attributed to the release of a diverse set of bioactive molecules and its capacity to modulate the inflammatory cascade, which reinforce tissue regeneration.
While both of these orthobiologic tools have their own fair share of advantages and drawbacks, they still promote similar positive effects in degenerative joint conditions like patellar chondropathy. Success rates may be higher in the early stages of disease where the pathological alterations are moderate. Also, the management of other comorbidities such as metabolic syndrome is also a wise strategy that may improve clinical outcomes. Although there is an increasing array of new orthobiologic products intended for degenerative joint conditions affecting the patella, further research is still needed in order to better understand the factors that contribute to musculoskeletal tissue restoration.
Author Contributions
Conceptualization, F.C and GSS; Project administration, J.F.L.; Writing – original draft, J.F.L. and GSS; Supervision, MSS., RM and CC; Writing – review and editing, PH., MBS and GSS; Validation, ZM; Investigation, J.F.L and G.A; Visualization, LP; Data curation, G.A, L.P. and GSS; Methodology, J.F.L and F.C.
Funding
This research received no external funding.
Institutional Review Board Statement
N/A.
Informed Consent Statement
N/A.
Data Availability Statement
N/A.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Zheng, W.; Li, H.; Hu, K.; Li, L.; Bei, M. Chondromalacia Patellae: Current Options and Emerging Cell Therapies. Stem Cell Res Ther 2021, 12, 412. [Google Scholar] [CrossRef]
- Hauser, R.A.; Sprague, I.S. Outcomes of Prolotherapy in Chondromalacia Patella Patients: Improvements in Pain Level and Function. Clin Med Insights Arthritis Musculoskelet Disord 2014, 7, 13–20. [Google Scholar] [CrossRef]
- Resorlu, H.; Zateri, C.; Nusran, G.; Goksel, F.; Aylanc, N. The Relation between Chondromalacia Patella and Meniscal Tear and the Sulcus Angle/ Trochlear Depth Ratio as a Powerful Predictor. J Back Musculoskelet Rehabil 2017, 30, 603–608. [Google Scholar] [CrossRef]
- Petersen, W.; Ellermann, A.; Rembitzki, I.V.; Scheffler, S.; Herbort, M.; Brüggemann, G.P.; Best, R.; Zantop, T.; Liebau, C. Evaluating the Potential Synergistic Benefit of a Realignment Brace on Patients Receiving Exercise Therapy for Patellofemoral Pain Syndrome: A Randomized Clinical Trial. Arch Orthop Trauma Surg 2016, 136, 975–982. [Google Scholar] [CrossRef]
- Mizner, R.L.; Petterson, S.C.; Stevens, J.E.; Vandenborne, K.; Snyder-Mackler, L. Early Quadriceps Strength Loss After Total Knee Arthroplasty. J Bone Joint Surg Am 2005, 87, 1047–1053. [Google Scholar] [CrossRef]
- Paravlic, A.H.; Kovač, S.; Pisot, R.; Marusic, U. Neurostructural Correlates of Strength Decrease Following Total Knee Arthroplasty: A Systematic Review of the Literature with Meta-Analysis. Bosn J Basic Med Sci 2020, 20, 1–12. [Google Scholar] [CrossRef]
- Moreno-Garcia, A.; Rodriguez-Merchan, E.C. Orthobiologics: Current Role in Orthopedic Surgery and Traumatology. Arch Bone Jt Surg 2022, 10, 536–542. [Google Scholar] [CrossRef]
- Dhillon, M.S.; Behera, P.; Patel, S.; Shetty, V. Orthobiologics and Platelet Rich Plasma. Indian J Orthop 2014, 48, 1–9. [Google Scholar] [CrossRef]
- Purita, J.; Lana, J.F.S.D.; Kolber, M.; Rodrigues, B.L.; Mosaner, T.; Santos, G.S.; Caliari-Oliveira, C.; Huber, S.C. Bone Marrow-Derived Products: A Classification Proposal – Bone Marrow Aspirate, Bone Marrow Aspirate Concentrate or Hybrid? WJSC 2020, 12, 241–250. [Google Scholar] [CrossRef] [PubMed]
- Lana, J.F.; Purita, J.; Everts, P.A.; De Mendonça Neto, P.A.T.; de Moraes Ferreira Jorge, D.; Mosaner, T.; Huber, S.C.; Azzini, G.O.M.; da Fonseca, L.F.; Jeyaraman, M.; et al. Platelet-Rich Plasma Power-Mix Gel (Ppm)-An Orthobiologic Optimization Protocol Rich in Growth Factors and Fibrin. Gels 2023, 9, 553. [Google Scholar] [CrossRef] [PubMed]
- Costa, F.R.; Costa Marques, M.R.; Costa, V.C.; Santos, G.S.; Martins, R.A.; Santos, M. da S.; Santana, M.H.A.; Nallakumarasamy, A.; Jeyaraman, M.; Lana, J.V.B.; et al. Intra-Articular Hyaluronic Acid in Osteoarthritis and Tendinopathies: Molecular and Clinical Approaches. Biomedicines 2023, 11, 1061. [Google Scholar] [CrossRef]
- Lana, J.F.S.D.; Lana, A.V.S.D.; da Fonseca, L.F.; Coelho, M.A.; Marques, G.G.; Mosaner, T.; Ribeiro, L.L.; Azzini, G.O.M.; Santos, G.S.; Fonseca, E.; et al. Stromal Vascular Fraction for Knee Osteoarthritis - An Update. J Stem Cells Regen Med 2022, 18, 11–20. [Google Scholar] [CrossRef]
- Huddleston, H.P.; Maheshwer, B.; Wong, S.E.; Chahla, J.; Cole, B.J.; Yanke, A.B. An Update on the Use of Orthobiologics: Use of Biologics for Osteoarthritis. Operative Techniques in Sports Medicine 2020. [Google Scholar] [CrossRef]
- Alves, R.; Grimalt, R. A Review of Platelet-Rich Plasma: History, Biology, Mechanism of Action, and Classification. Skin Appendage Disorders 2018. [Google Scholar] [CrossRef]
- Ghosh, P.; Guidolin, D. Potential Mechanism of Action of Intra-Articular Hyaluronan Therapy in Osteoarthritis: Are the Effects Molecular Weight Dependent? Seminars in Arthritis and Rheumatism 2002. [Google Scholar] [CrossRef]
- Örsçelik, A.; Akpancar, S.; Seven, M.M.; Erdem, Y.; Koca, K. The Efficacy of Platelet Rich Plasma and Prolotherapy in Chondromalacia Patella Treatment. Spor Hekimliği Dergisi 2020, 55, 028–037. [Google Scholar] [CrossRef]
- Chang, K.-V.; Hung, C.-Y.; Aliwarga, F.; Wang, T.-G.; Han, D.-S.; Chen, W.-S. Comparative Effectiveness of Platelet-Rich Plasma Injections for Treating Knee Joint Cartilage Degenerative Pathology: A Systematic Review and Meta-Analysis. Arch Phys Med Rehabil 2014, 95, 562–575. [Google Scholar] [CrossRef]
- Subasi, V. Effectiveness of Platelet-Rich Plasma Treatment in Chondromalacia Patellae. JAREM 2017, 7, 36–38. [Google Scholar] [CrossRef]
- Laver, L.; Marom, N.; Dnyanesh, L.; Mei-Dan, O.; Espregueira-Mendes, J.; Gobbi, A. PRP for Degenerative Cartilage Disease: A Systematic Review of Clinical Studies. CARTILAGE 2017, 8, 341–364. [Google Scholar] [CrossRef] [PubMed]
- Sánchez, M.; Jorquera, C.; de Dicastillo, L.L.; Fiz, N.; Knörr, J.; Beitia, M.; Aizpurua, B.; Azofra, J.; Delgado, D. Real-World Evidence to Assess the Effectiveness of Platelet-Rich Plasma in the Treatment of Knee Degenerative Pathology: A Prospective Observational Study. Therapeutic Advances in Musculoskeletal 2022, 14, 1759720X221100304. [Google Scholar] [CrossRef] [PubMed]
- Hart, R.; Safi, A.; Komzák, M.; Jajtner, P.; Puskeiler, M.; Hartová, P. Platelet-Rich Plasma in Patients with Tibiofemoral Cartilage Degeneration. Arch Orthop Trauma Surg 2013, 133, 1295–1301. [Google Scholar] [CrossRef] [PubMed]
- El-Desouky, I.I. Effectiveness of Intra-Articular Injection of Platelet-Rich Plasma in Isolated Patellofemoral Arthritis. The Egyptian Orthopaedic Journal 2022, 57, 152. [Google Scholar] [CrossRef]
- Hart, J.M.; Kuenze, C.; Bodkin, S.; Hart, J.; Denny, C.; Diduch, D.R. Prospective, Randomized, Double Blind Evaluation of the Efficacy of a Single Dose Hyaluronic Acid for the Treatment of Patellofemoral Chondromalacia. Orthop J Sports Med 2018, 6, 2325967118S00118. [Google Scholar] [CrossRef]
- Zhang, S.; Jia, M.; Luo, Y.; Wang, X.; Shi, Z.; Xiao, J. [Hyaluronate acid for treatment of chondromalacia patellae: a 52-week follow-up study]. Nan Fang Yi Ke Da Xue Xue Bao 2019, 39, 791–796. [Google Scholar] [CrossRef] [PubMed]
- da Costa, S.R.; da Mota e Albuquerque, R.F.; Helito, C.P.; Camanho, G.L. The Role of Viscosupplementation in Patellar Chondropathy. Ther Adv Musculoskelet Dis 2021, 13, 1759720X211015005. [Google Scholar] [CrossRef] [PubMed]
- Astur, D.C.; Angelini, F.B.; Santos, M.A.; Arliani, G.G.; Belangero, P.S.; Cohen, M. Use of Exogenous Hyaluronic Acid for the Treatment of Patellar Chondropathy– A Six-Month Randomized Controlled Trial. Rev Bras Ortop (Sao Paulo) 2019, 54, 549–555. [Google Scholar] [CrossRef] [PubMed]
- Cole, B.J.; Karas, V.; Hussey, K.; Merkow, D.B.; Pilz, K.; Fortier, L.A. Hyaluronic Acid Versus Platelet-Rich Plasma: A Prospective, Double-Blind Randomized Controlled Trial Comparing Clinical Outcomes and Effects on Intra-Articular Biology for the Treatment of Knee Osteoarthritis. The American Journal of Sports Medicine 2017. [Google Scholar] [CrossRef] [PubMed]
- dos Santos, R.G.; Santos, G.S.; Alkass, N.; Chiesa, T.L.; Azzini, G.O.; da Fonseca, L.F.; dos Santos, A.F.; Rodrigues, B.L.; Mosaner, T.; Lana, J.F. The Regenerative Mechanisms of Platelet-Rich Plasma: A Review. Cytokine 2021. [Google Scholar] [CrossRef] [PubMed]
- Azzini, G.O.M.; Santos, G.S.; Visoni, S.B.C.; Azzini, V.O.M.; Santos, R.G. dos; Huber, S.C.; Lana, J.F. Metabolic Syndrome and Subchondral Bone Alterations: The Rise of Osteoarthritis – A Review. Journal of Clinical Orthopaedics and Trauma 2020. [Google Scholar] [CrossRef]
- Hafsi, K.; McKay, J.; Li, J.; Lana, J.F.; Macedo, A.; Santos, G.S.; Murrell, W.D. Nutritional, Metabolic and Genetic Considerations to Optimise Regenerative Medicine Outcome for Knee Osteoarthritis. Journal of Clinical Orthopaedics and Trauma 2019, 10. [Google Scholar] [CrossRef]
- Kok, H.K.; Donnellan, J.; Ryan, D.; Torreggiani, W.C. Correlation between Subcutaneous Knee Fat Thickness and Chondromalacia Patellae on Magnetic Resonance Imaging of the Knee. Can Assoc Radiol J 2013, 64, 182–186. [Google Scholar] [CrossRef] [PubMed]
- Karsdal, M.A.; Bay-Jensen, A.C.; Lories, R.J.; Abramson, S.; Spector, T.; Pastoureau, P.; Christiansen, C.; Attur, M.; Henriksen, K.; Goldring, S.R.; et al. The Coupling of Bone and Cartilage Turnover in Osteoarthritis: Opportunities for Bone Antiresorptives and Anabolics as Potential Treatments? Annals of the Rheumatic Diseases 2014. [CrossRef] [PubMed]
- Kadri, A.; Ea, H.K.; Bazille, C.; Hannouche, D.; Lioté, F.; Cohen-Solal, M.E. Osteoprotegerin Inhibits Cartilage Degradation through an Effect on Trabecular Bone in Murine Experimental Osteoarthritis. Arthritis and Rheumatism 2008. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, C.; Deberg, M.A.; Piccardi, N.; Msika, P.; Reginster, J.Y.L.; Henrotin, Y.E. Subchondral Bone Osteoblasts Induce Phenotypic Changes in Human Osteoarthritic Chondrocytes. Osteoarthritis and Cartilage 2005. [Google Scholar] [CrossRef] [PubMed]
- Lajeunesse, D. The Role of Bone in the Treatment of Osteoarthritis. Osteoarthritis and Cartilage 2004. [Google Scholar] [CrossRef] [PubMed]
- Miller, R.E.; Miller, R.J.; Malfait, A.-M. OSTEOARTHRITIS JOINT PAIN: THE CYTOKINE CONNECTION. Cytokine 2014, 70, 185–193. [Google Scholar] [CrossRef]
- Pan, J.; Wang, B.; Li, W.; Zhou, X.; Scherr, T.; Yang, Y.; Price, C.; Wang, L. Elevated Cross-Talk between Subchondral Bone and Cartilage in Osteoarthritic Joints. Bone 2012. [Google Scholar] [CrossRef] [PubMed]
- Parrish, W.R.; Roides, B. Musculoskeletal Regeneration. Musculoskeletal Regeneration 2017. [Google Scholar] [CrossRef]
- Marx, R.E. Platelet-Rich Plasma: Evidence to Support Its Use. Journal of Oral and Maxillofacial Surgery 2004. [Google Scholar] [CrossRef]
- Rui, S.; Yuan, Y.; Du, C.; Song, P.; Chen, Y.; Wang, H.; Fan, Y.; Armstrong, D.G.; Deng, W.; Li, L. Comparison and Investigation of Exosomes Derived from Platelet-Rich Plasma Activated by Different Agonists. Cell Transplant 2021, 30, 9636897211017833. [Google Scholar] [CrossRef]
- Dohan Ehrenfest, D.M.; Andia, I.; Zumstein, M.A.; Zhang, C.Q.; Pinto, N.R.; Bielecki, T. Classification of Platelet Concentrates (Platelet-Rich Plasma-PRP, Platelet-Rich Fibrin-PRF) for Topical and Infiltrative Use in Orthopedic and Sports Medicine: Current Consensus, Clinical Implications and Perspectives. Muscles, Ligaments and Tendons Journal. [CrossRef]
- Dohan Ehrenfest, D.M.; Rasmusson, L.; Albrektsson, T. Classification of Platelet Concentrates: From Pure Platelet-Rich Plasma (P-PRP) to Leucocyte- and Platelet-Rich Fibrin (L-PRF). Trends Biotechnol 2009, 27, 158–167. [Google Scholar] [CrossRef] [PubMed]
- Lana, J.F.S.D.; Purita, J.; Paulus, C.; Huber, S.C.; Rodrigues, B.L.; Rodrigues, A.A.; Santana, M.H.; Madureira, J.L.; Malheiros Luzo, Â.C.; Belangero, W.D.; et al. Contributions for Classification of Platelet Rich Plasma - Proposal of a New Classification: MARSPILL. Regenerative Medicine 2017, 12, 565–574. [Google Scholar] [CrossRef]
- Boswell, S.G.; Cole, B.J.; Sundman, E.A.; Karas, V.; Fortier, L.A. Platelet-Rich Plasma: A Milieu of Bioactive Factors. Arthroscopy - Journal of Arthroscopic and Related Surgery. [CrossRef]
- Pavlovic, V.; Ciric, M.; Jovanovic, V.; Stojanovic, P. Platelet Rich Plasma: A Short Overview of Certain Bioactive Components. Open Medicine (Poland) 2016. [CrossRef]
- Parrish, W.R.; Roides, B.; Hwang, J.; Mafilios, M.; Story, B.; Bhattacharyya, S. Normal Platelet Function in Platelet Concentrates Requires Non-Platelet Cells: A Comparative in Vitro Evaluation of Leucocyte-Rich (Type 1a) and Leucocyte-Poor (Type 3b) Platelet Concentrates. BMJ Open Sport Exerc Med 2016, 2, e000071. [Google Scholar] [CrossRef]
- Pavlovic, V.; Ciric, M.; Jovanovic, V.; Stojanovic, P. Platelet Rich Plasma: A Short Overview of Certain Bioactive Components. Open Medicine (Poland) 2016. [Google Scholar] [CrossRef] [PubMed]
- Boswell, S.G.; Cole, B.J.; Sundman, E.A.; Karas, V.; Fortier, L.A. Platelet-Rich Plasma: A Milieu of Bioactive Factors. Arthroscopy - Journal of Arthroscopic and Related Surgery. [CrossRef]
- Ganguly, P.; Fiz, N.; Beitia, M.; Owston, H.E.; Delgado, D.; Jones, E.; Sánchez, M. Effect of Combined Intraosseous and Intraarticular Infiltrations of Autologous Platelet-Rich Plasma on Subchondral Bone Marrow Mesenchymal Stromal Cells from Patients with Hip Osteoarthritis. J Clin Med 2022, 11, 3891. [Google Scholar] [CrossRef]
- Foster, T.E.; Puskas, B.L.; Mandelbaum, B.R.; Gerhardt, M.B.; Rodeo, S.A. Platelet-Rich Plasma: From Basic Science to Clinical Applications. American Journal of Sports Medicine 2009. [CrossRef] [PubMed]
- Meheux, C.J.; McCulloch, P.C.; Lintner, D.M.; Varner, K.E.; Harris, J.D. Efficacy of Intra-Articular Platelet-Rich Plasma Injections in Knee Osteoarthritis: A Systematic Review. Arthroscopy 2016, 32, 495–505. [Google Scholar] [CrossRef]
- Belk, J.W.; Kraeutler, M.J.; Houck, D.A.; Goodrich, J.A.; Dragoo, J.L.; McCarty, E.C. Platelet-Rich Plasma Versus Hyaluronic Acid for Knee Osteoarthritis: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Am J Sports Med 2021, 49, 249–260. [Google Scholar] [CrossRef]
- Hong, M.; Cheng, C.; Sun, X.; Yan, Y.; Zhang, Q.; Wang, W.; Guo, W. Efficacy and Safety of Intra-Articular Platelet-Rich Plasma in Osteoarthritis Knee: A Systematic Review and Meta-Analysis. Biomed Res Int 2021, 2021, 2191926. [Google Scholar] [CrossRef]
- Park, Y.-B.; Kim, J.-H.; Ha, C.-W.; Lee, D.-H. Clinical Efficacy of Platelet-Rich Plasma Injection and Its Association With Growth Factors in the Treatment of Mild to Moderate Knee Osteoarthritis: A Randomized Double-Blind Controlled Clinical Trial As Compared With Hyaluronic Acid. Am J Sports Med 2021, 49, 487–496. [Google Scholar] [CrossRef] [PubMed]
- Nie, L.-Y.; Zhao, K.; Ruan, J.; Xue, J. Effectiveness of Platelet-Rich Plasma in the Treatment of Knee Osteoarthritis: A Meta-Analysis of Randomized Controlled Clinical Trials. Orthop J Sports Med 2021, 9, 2325967120973284. [Google Scholar] [CrossRef]
- Huang, H.-Y.; Hsu, C.-W.; Lin, G.-C.; Lin, H.-S.; Chou, Y.-J.; Liou, I.-H.; Sun, S.-F. Comparing Efficacy of a Single Intraarticular Injection of Platelet-Rich Plasma (PRP) Combined with Different Hyaluronans for Knee Osteoarthritis: A Randomized-Controlled Clinical Trial. BMC Musculoskelet Disord 2022, 23, 954. [Google Scholar] [CrossRef] [PubMed]
- Xie, X.; Wang, Y.; Zhao, C.; Guo, S.; Liu, S.; Jia, W.; Tuan, R.S.; Zhang, C. Comparative Evaluation of MSCs from Bone Marrow and Adipose Tissue Seeded in PRP-Derived Scaffold for Cartilage Regeneration. Biomaterials 2012. [Google Scholar] [CrossRef]
- Van Buul, G.M.; Koevoet, W.L.M.; Kops, N.; Bos, P.K.; Verhaar, J.A.N.; Weinans, H.; Bernsen, M.R.; Van Osch, G.J.V.M. Platelet-Rich Plasma Releasate Inhibits Inflammatory Processes in Osteoarthritic Chondrocytes. American Journal of Sports Medicine 2011. [Google Scholar] [CrossRef] [PubMed]
- Giannopoulou, M.; Dai, C.; Tan, X.; Wen, X.; Michalopoulos, G.K.; Liu, Y. Hepatocyte Growth Factor Exerts Its Anti-Inflammatory Action by Disrupting Nuclear Factor-κB Signaling. American Journal of Pathology 2008. [Google Scholar] [CrossRef]
- Marathe, A.; Patel, S.J.; Song, B.; Sliepka, J.M.; Shybut, T.S.; Lee, B.H.; Jayaram, P. Double-Spin Leukocyte-Rich Platelet-Rich Plasma Is Predominantly Lymphocyte Rich With Notable Concentrations of Other White Blood Cell Subtypes. Arthrosc Sports Med Rehabil 2022, 4, e335–e341. [Google Scholar] [CrossRef]
- Kennedy, M.I.; Whitney, K.; Evans, T.; LaPrade, R.F. Platelet-Rich Plasma and Cartilage Repair. Current Reviews in Musculoskeletal Medicine 2018. [CrossRef]
- Moussa, M.; Lajeunesse, D.; Hilal, G.; El Atat, O.; Haykal, G.; Serhal, R.; Chalhoub, A.; Khalil, C.; Alaaeddine, N. Platelet Rich Plasma (PRP) Induces Chondroprotection via Increasing Autophagy, Anti-Inflammatory Markers, and Decreasing Apoptosis in Human Osteoarthritic Cartilage. Experimental Cell Research 2017. [Google Scholar] [CrossRef]
- García-Prat, L.; Martínez-Vicente, M.; Perdiguero, E.; Ortet, L.; Rodríguez-Ubreva, J.; Rebollo, E.; Ruiz-Bonilla, V.; Gutarra, S.; Ballestar, E.; Serrano, A.L.; et al. Autophagy Maintains Stemness by Preventing Senescence. Nature 2016. [Google Scholar] [CrossRef]
- Saxena, A.; Khosraviani, S.; Noel, S.; Mohan, D.; Donner, T.; Hamad, A.R.A. Interleukin-10 Paradox: A Potent Immunoregulatory Cytokine That Has Been Difficult to Harness for Immunotherapy. Cytokine 2015. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.M.; An, J. Cytokines, Inflammation, and Pain. International Anesthesiology Clinics 2007. [CrossRef]
- Kendall, R.T.; Feghali-Bostwick, C.A. Fibroblasts in Fibrosis: Novel Roles and Mediators. Frontiers in Pharmacology 2014. [CrossRef]
- Werner, S.; Grose, R. Regulation of Wound Healing by Growth Factors and Cytokines. Physiological Reviews 2003. [CrossRef]
- Cavallo, C.; Filardo, G.; Mariani, E.; Kon, E.; Marcacci, M.; Pereira Ruiz, M.T.; Facchini, A.; Grigolo, B. Comparison of Platelet-Rich Plasma Formulations for Cartilage Healing: An in Vitro Study. Journal of Bone and Joint Surgery - Series A. [CrossRef]
- Sánchez, M.; Anitua, E.; Azofra, J.; Aguirre, J.J.; Andia, I. Intra-Articular Injection of an Autologous Preparation Rich in Growth Factors for the Treatment of Knee OA: A Retrospective Cohort Study. Clin Exp Rheumatol 2008, 26, 910–913. [Google Scholar]
- Opneja, A.; Kapoor, S.; Stavrou, E.X. Contribution of Platelets, the Coagulation and Fibrinolytic Systems to Cutaneous Wound Healing. Thrombosis Research 2019. [CrossRef]
- Nurden, A.T.; Nurden, P.; Sanchez, M.; Andia, I.; Anitua, E. Platelets and Wound Healing. Front Biosci 2008, 13, 3532–3548. [Google Scholar] [CrossRef] [PubMed]
- Von Hundelshausen, P.; Koenen, R.R.; Sack, M.; Mause, S.F.; Adriaens, W.; Proudfoot, A.E.I.; Hackeng, T.M.; Weber, C. Heterophilic Interactions of Platelet Factor 4 and RANTES Promote Monocyte Arrest on Endothelium. Blood 2005. [Google Scholar] [CrossRef]
- Xia, C.Q.; Kao, K.J. Effect of CXC Chemokine Platelet Factor 4 on Differentiation and Function of Monocyte-Derived Dendritic Cells. International Immunology 2003. [Google Scholar] [CrossRef]
- Scheuerer, B.; Ernst, M.; Dürrbaum-Landmann, I.; Fleischer, J.; Grage-Griebenow, E.; Brandt, E.; Flad, H.D.; Petersen, F. The CXC-Chemokine Platelet Factor 4 Promotes Monocyte Survival and Induces Monocyte Differentiation into Macrophages. Blood 2000. [Google Scholar] [CrossRef]
- Gratchev, A.; Kzhyshkowska, J.; Köthe, K.; Muller-Molinet, I.; Kannookadan, S.; Utikal, J.; Goerdt, S. Mφ1 and Mφ2 Can Be Re-Polarized by Th2 or Th1 Cytokines, Respectively, and Respond to Exogenous Danger Signals. Immunobiology 2006. [Google Scholar] [CrossRef]
- Das, A.; Sinha, M.; Datta, S.; Abas, M.; Chaffee, S.; Sen, C.K.; Roy, S. Monocyte and Macrophage Plasticity in Tissue Repair and Regeneration. American Journal of Pathology 2015. [CrossRef]
- Lana, J.F.; Huber, S.C.; Purita, J.; Tambeli, C.H.; Santos, G.S.; Paulus, C.; Annichino-Bizzacchi, J.M. Leukocyte-Rich PRP versus Leukocyte-Poor PRP - The Role of Monocyte/Macrophage Function in the Healing Cascade. Journal of Clinical Orthopaedics and Trauma 2019. [Google Scholar] [CrossRef] [PubMed]
- Meszaros, A.J.; Reichner, J.S.; Albina, J.E. Macrophage-Induced Neutrophil Apoptosis. The Journal of Immunology 2000. [Google Scholar] [CrossRef] [PubMed]
- Ramaswamy Reddy, S.H.; Reddy, R.; Babu, N.C.; Ashok, G.N. Stem-Cell Therapy and Platelet-Rich Plasma in Regenerative Medicines: A Review on Pros and Cons of the Technologies. J Oral Maxillofac Pathol 2018, 22, 367–374. [Google Scholar] [CrossRef] [PubMed]
- Latalski, M.; Walczyk, A.; Fatyga, M.; Rutz, E.; Szponder, T.; Bielecki, T.; Danielewicz, A. Allergic Reaction to Platelet-Rich Plasma (PRP). Medicine (Baltimore) 2019, 98, e14702. [Google Scholar] [CrossRef]
- Cömert Kiliç, S.; Güngörmüş, M. Is Arthrocentesis plus Platelet-Rich Plasma Superior to Arthrocentesis plus Hyaluronic Acid for the Treatment of Temporomandibular Joint Osteoarthritis: A Randomized Clinical Trial. Int J Oral Maxillofac Surg 2016, 45, 1538–1544. [Google Scholar] [CrossRef]
- Dai, W.; Yan, W.; Leng, X.; Wang, J.; Hu, X.; Cheng, J.; Ao, Y. Efficacy of Platelet-Rich Plasma Versus Placebo in the Treatment of Tendinopathy: A Meta-Analysis of Randomized Controlled Trials. Clin J Sport Med 2023, 33, 69–77. [Google Scholar] [CrossRef]
- Lisignoli, G.; Cristino, S.; Piacentini, A.; Cavallo, C.; Caplan, A.I.; Facchini, A. Hyaluronan-Based Polymer Scaffold Modulates the Expression of Inflammatory and Degradative Factors in Mesenchymal Stem Cells: Involvement of Cd44 and Cd54. Journal of Cellular Physiology 2006. [Google Scholar] [CrossRef]
- Campo, G.M.; Avenoso, A.; Campo, S.; D’Ascola, A.; Traina, P.; Rugolo, C.A.; Calatroni, A. Differential Effect of Molecular Mass Hyaluronan on Lipopolysaccharide-Induced Damage in Chondrocytes. Innate Immun 2010, 16, 48–63. [Google Scholar] [CrossRef]
- Day, A.J.; de la Motte, C.A. Hyaluronan Cross-Linking: A Protective Mechanism in Inflammation? Trends Immunol 2005, 26, 637–643. [Google Scholar] [CrossRef]
- Tanimoto, K.; Ohno, S.; Fujimoto, K.; Honda, K.; Ijuin, C.; Tanaka, N.; Doi, T.; Nakahara, M.; Tanne, K. Proinflammatory Cytokines Regulate the Gene Expression of Hyaluronic Acid Synthetase in Cultured Rabbit Synovial Membrane Cells. Connect Tissue Res 2001, 42, 187–195. [Google Scholar] [CrossRef] [PubMed]
- Maheu, E.; Rannou, F.; Reginster, J.Y. Efficacy and Safety of Hyaluronic Acid in the Management of Osteoarthritis: Evidence from Real-Life Setting Trials and Surveys. Seminars in Arthritis and Rheumatism 2016. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.M.; Park, S.J.; Noh, I.; Kim, C.-H. The Effects of the Molecular Weights of Hyaluronic Acid on the Immune Responses. Biomater Res 2021, 25, 27. [Google Scholar] [CrossRef]
- Zhang, B.; Du, Y.; He, Y.; Liu, Y.; Zhang, G.; Yang, C.; Gao, F. INT-HA Induces M2-like Macrophage Differentiation of Human Monocytes via TLR4-miR-935 Pathway. Cancer Immunol Immunother 2019, 68, 189–200. [Google Scholar] [CrossRef] [PubMed]
- Altman, R.; Hackel, J.; Niazi, F.; Shaw, P.; Nicholls, M. Efficacy and Safety of Repeated Courses of Hyaluronic Acid Injections for Knee Osteoarthritis: A Systematic Review. Semin Arthritis Rheum 2018, 48, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Mordin, M.; Parrish, W.; Masaquel, C.; Bisson, B.; Copley-Merriman, C. Intra-Articular Hyaluronic Acid for Osteoarthritis of the Knee in the United States: A Systematic Review of Economic Evaluations. Clin Med Insights Arthritis Musculoskelet Disord 2021, 14, 11795441211047284. [Google Scholar] [CrossRef] [PubMed]
- Bruyère, O.; Cooper, C.; Pelletier, J.P.; Branco, J.; Luisa Brandi, M.; Guillemin, F.; Hochberg, M.C.; Kanis, J.A.; Kvien, T.K.; Martel-Pelletier, J.; et al. An Algorithm Recommendation for the Management of Knee Osteoarthritis in Europe and Internationally: A Report from a Task Force of the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO). Seminars in Arthritis and Rheumatism 2014, 44, 253–263. [Google Scholar] [CrossRef]
- Brun, P.; Zavan, B.; Vindigni, V.; Schiavinato, A.; Pozzuoli, A.; Iacobellis, C.; Abatangelo, G. In Vitro Response of Osteoarthritic Chondrocytes and Fibroblast-like Synoviocytes to a 500-730 kDa Hyaluronan Amide Derivative. Journal of Biomedical Materials Research Part B: Applied Biomaterials 2012, 100B, 2073–2081. [Google Scholar] [CrossRef] [PubMed]
- Kruel, A.V.S.; Ribeiro, L.L.; Gusmão, P.D.; Huber, S.C.; Lana, J.F.S.D. Orthobiologics in the Treatment of Hip Disorders. World J Stem Cells 2021, 13, 304–316. [Google Scholar] [CrossRef]
- Julovi, S.M.; Yasuda, T.; Shimizu, M.; Hiramitsu, T.; Nakamura, T. Inhibition of Interleukin-1β-Stimulated Production of Matrix Metalloproteinases by Hyaluronan via CD44 in Human Articular Cartilage. Arthritis and Rheumatism 2004, 50, 516–525. [Google Scholar] [CrossRef] [PubMed]
- Kalaci, A.; Yilmaz, R.H.; Aslan, B.; Sög̈üt, S.; Yanat, A.N.; Uz, E. Effects of Hyaluronan on Nitric Oxide Levels and Superoxide Dismutase Activities in Synovial Fluid in Knee Osteoarthritis. Clinical Rheumatology 2007, 26, 1306–1311. [Google Scholar] [CrossRef] [PubMed]
- Karna, E.; Miltyk, W.; Surażyński, A.; Pałka, J.A. Protective Effect of Hyaluronic Acid on Interleukin-1-Induced Deregulation of Βeta 1 -Integrin and Insulin-like Growth Factor-I Receptor Signaling and Collagen Biosynthesis in Cultured Human Chondrocytes. Molecular and Cellular Biochemistry 2008, 308, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Abate, M.; Pelotti, P.; De Amicis, D.; Di Iorio, A.; Galletti, S.; Salini, V. Viscosupplementation with Hyaluronic Acid in Hip Osteoarthritis (a Review). Upsala Journal of Medical Sciences 2008, 113, 261–278. [Google Scholar] [CrossRef] [PubMed]
- Dicker, K.T.; Gurski, L.A.; Pradhan-Bhatt, S.; Witt, R.L.; Farach-Carson, M.C.; Jia, X. Hyaluronan: A Simple Polysaccharide with Diverse Biological Functions. Acta Biomater 2014, 10, 1558–1570. [Google Scholar] [CrossRef] [PubMed]
- Abatangelo, G.; Vindigni, V.; Avruscio, G.; Pandis, L.; Brun, P. Hyaluronic Acid: Redefining Its Role. Cells 2020, 9, 1743. [Google Scholar] [CrossRef] [PubMed]
- Vigetti, D.; Karousou, E.; Viola, M.; Deleonibus, S.; De Luca, G.; Passi, A. Hyaluronan: Biosynthesis and Signaling. Biochim Biophys Acta 2014, 1840, 2452–2459. [Google Scholar] [CrossRef]
- Gomis, A.; Miralles, A.; Schmidt, R.F.; Belmonte, C. Intra-Articular Injections of Hyaluronan Solutions of Different Elastoviscosity Reduce Nociceptive Nerve Activity in a Model of Osteoarthritic Knee Joint of the Guinea Pig. Osteoarthritis and Cartilage 2009, 17, 798–804. [Google Scholar] [CrossRef]
- Kuroki, K.; Cook, J.L.; Kreeger, J.M. Mechanisms of Action and Potential Uses of Hyaluronan in Dogs with Osteoarthritis. J Am Vet Med Assoc 2002, 221, 944–950. [Google Scholar] [CrossRef]
- Díaz-Gallego, L.; Prieto, J.G.; Coronel, P.; Gamazo, L.E.; Gimeno, M.; Alvarez, A.I. Apoptosis and Nitric Oxide in an Experimental Model of Osteoarthritis in Rabbit after Hyaluronic Acid Treatment. J Orthop Res 2005, 23, 1370–1376. [Google Scholar] [CrossRef]
- Altman, R.D.; Moskowitz, R. Intraarticular Sodium Hyaluronate (Hyalgan) in the Treatment of Patients with Osteoarthritis of the Knee: A Randomized Clinical Trial. Hyalgan Study Group. J Rheumatol 1998, 25, 2203–2212. [Google Scholar]
- Kolarz, G.; Kotz, R.; Hochmayer, I. Long-Term Benefits and Repeated Treatment Cycles of Intra-Articular Sodium Hyaluronate (Hyalgan) in Patients with Osteoarthritis of the Knee. Semin Arthritis Rheum 2003, 32, 310–319. [Google Scholar] [CrossRef] [PubMed]
- Salamanna, F.; Giavaresi, G.; Parrilli, A.; Martini, L.; Nicoli Aldini, N.; Abatangelo, G.; Frizziero, A.; Fini, M. Effects of Intra-Articular Hyaluronic Acid Associated to Chitlac (Arty-Duo®) in a Rat Knee Osteoarthritis Model. J Orthop Res 2019, 37, 867–876. [Google Scholar] [CrossRef]
- Tarricone, E.; Mattiuzzo, E.; Belluzzi, E.; Elia, R.; Benetti, A.; Venerando, R.; Vindigni, V.; Ruggieri, P.; Brun, P. Anti-Inflammatory Performance of Lactose-Modified Chitosan and Hyaluronic Acid Mixtures in an In Vitro Macrophage-Mediated Inflammation Osteoarthritis Model. Cells 2020, 9, E1328. [Google Scholar] [CrossRef] [PubMed]
- Tarricone, E.; Elia, R.; Mattiuzzo, E.; Faggian, A.; Pozzuoli, A.; Ruggieri, P.; Brun, P. The Viability and Anti-Inflammatory Effects of Hyaluronic Acid-Chitlac-Tracimolone Acetonide- β-Cyclodextrin Complex on Human Chondrocytes. Cartilage 2021, 13, 920S–924S. [Google Scholar] [CrossRef]
- Hollander, A.P.; Dickinson, S.C.; Sims, T.J.; Brun, P.; Cortivo, R.; Kon, E.; Marcacci, M.; Zanasi, S.; Borrione, A.; De Luca, C.; et al. Maturation of Tissue Engineered Cartilage Implanted in Injured and Osteoarthritic Human Knees. Tissue Eng 2006, 12, 1787–1798. [Google Scholar] [CrossRef] [PubMed]
- Lana, J.F.S.D.; Weglein, A.; Sampson, S.E.; Vicente, E.F.; Huber, S.C.; Souza, C.V.; Ambach, M.A.; Vincent, H.; Urban-Paffaro, A.; Onodera, C.M.K.; et al. Randomized Controlled Trial Comparing Hyaluronic Acid, Platelet-Rich Plasma and the Combination of Both in the Treatment of Mild and Moderate Osteoarthritis of the Knee. J Stem Cells Regen Med 2016, 12, 69–78. [Google Scholar] [PubMed]
- Levett, P.A.; Hutmacher, D.W.; Malda, J.; Klein, T.J. Hyaluronic Acid Enhances the Mechanical Properties of Tissue-Engineered Cartilage Constructs. PLoS One 2014, 9, e113216. [Google Scholar] [CrossRef]
- Sebbagh, P.; Cannone, A.; Gremion, G.; Gremeaux, V.; Raffoul, W.; Hirt-Burri, N.; Michetti, M.; Abdel-Sayed, P.; Laurent, A.; Wardé, N.; et al. Current Status of PRP Manufacturing Requirements & European Regulatory Frameworks: Practical Tools for the Appropriate Implementation of PRP Therapies in Musculoskeletal Regenerative Medicine. Bioengineering (Basel) 2023, 10, 292. [Google Scholar] [CrossRef]
- Kuffler, D.P. Variables Affecting the Potential Efficacy of PRP in Providing Chronic Pain Relief. J Pain Res 2018, 12, 109–116. [Google Scholar] [CrossRef]
- Gupta, V.; Parihar, A.S.; Pathak, M.; Sharma, V.K. Comparison of Platelet-Rich Plasma Prepared Using Two Methods: Manual Double Spin Method versus a Commercially Available Automated Device. Indian Dermatol Online J 2020, 11, 575–579. [Google Scholar] [CrossRef] [PubMed]
- Dhurat, R.; Sukesh, M. Principles and Methods of Preparation of Platelet-Rich Plasma: A Review and Author’s Perspective. J Cutan Aesthet Surg 2014, 7, 189–197. [Google Scholar] [CrossRef] [PubMed]
- Samuelson, E.M.; Ebel, J.A.; Reynolds, S.B.; Arnold, R.M.; Brown, D.E. The Cost-Effectiveness of Platelet-Rich Plasma Compared With Hyaluronic Acid Injections for the Treatment of Knee Osteoarthritis. Arthroscopy: The Journal of Arthroscopic & Related Surgery 2020, 36, 3072–3078. [Google Scholar] [CrossRef]
- Rosen, J.; Niazi, F.; Dysart, S. Cost-Effectiveness of Treating Early to Moderate Stage Knee Osteoarthritis with Intra-Articular Hyaluronic Acid Compared to Conservative Interventions. Adv Ther 2020, 37, 344–352. [Google Scholar] [CrossRef] [PubMed]
- Onkarappa, R.S.; Chauhan, D.K.; Saikia, B.; Karim, A.; Kanojia, R.K. Metabolic Syndrome and Its Effects on Cartilage Degeneration vs Regeneration: A Pilot Study Using Osteoarthritis Biomarkers. Indian J Orthop 2020, 54, 20–24. [Google Scholar] [CrossRef] [PubMed]
- Russo, S.; Kwiatkowski, M.; Govorukhina, N.; Bischoff, R.; Melgert, B.N. Meta-Inflammation and Metabolic Reprogramming of Macrophages in Diabetes and Obesity: The Importance of Metabolites. Front Immunol 2021, 12, 746151. [Google Scholar] [CrossRef] [PubMed]
- Toussirot, E. Mini-Review: The Contribution of Adipokines to Joint Inflammation in Inflammatory Rheumatic Diseases. Front Endocrinol (Lausanne) 2020, 11, 606560. [Google Scholar] [CrossRef] [PubMed]
- Bliddal, H.; Leeds, A.R.; Christensen, R. Osteoarthritis, Obesity and Weight Loss: Evidence, Hypotheses and Horizons - a Scoping Review. Obes Rev 2014, 15, 578–586. [Google Scholar] [CrossRef] [PubMed]
- KURT, M.; ÖNER, A.Y.; UÇAR, M.; ALADAĞ KURT, S. The Relationship between Patellofemoral Arthritis and Fat Tissue Volume, Body Mass Index and Popliteal Artery Intima-Media Thickness through 3T Knee MRI. Turk J Med Sci 2019, 49, 844–853. [Google Scholar] [CrossRef]
- Kızılgöz, V.; Kantarci, M.; Aydın, S. Association between the Subcutaneous Fat Thickness of the Knee and Chondromalacia Patella: A Magnetic Resonance Imaging-Based Study. J Int Med Res 2023, 51, 3000605231183581. [Google Scholar] [CrossRef]
Figure 1.
Patellar chondropathy.
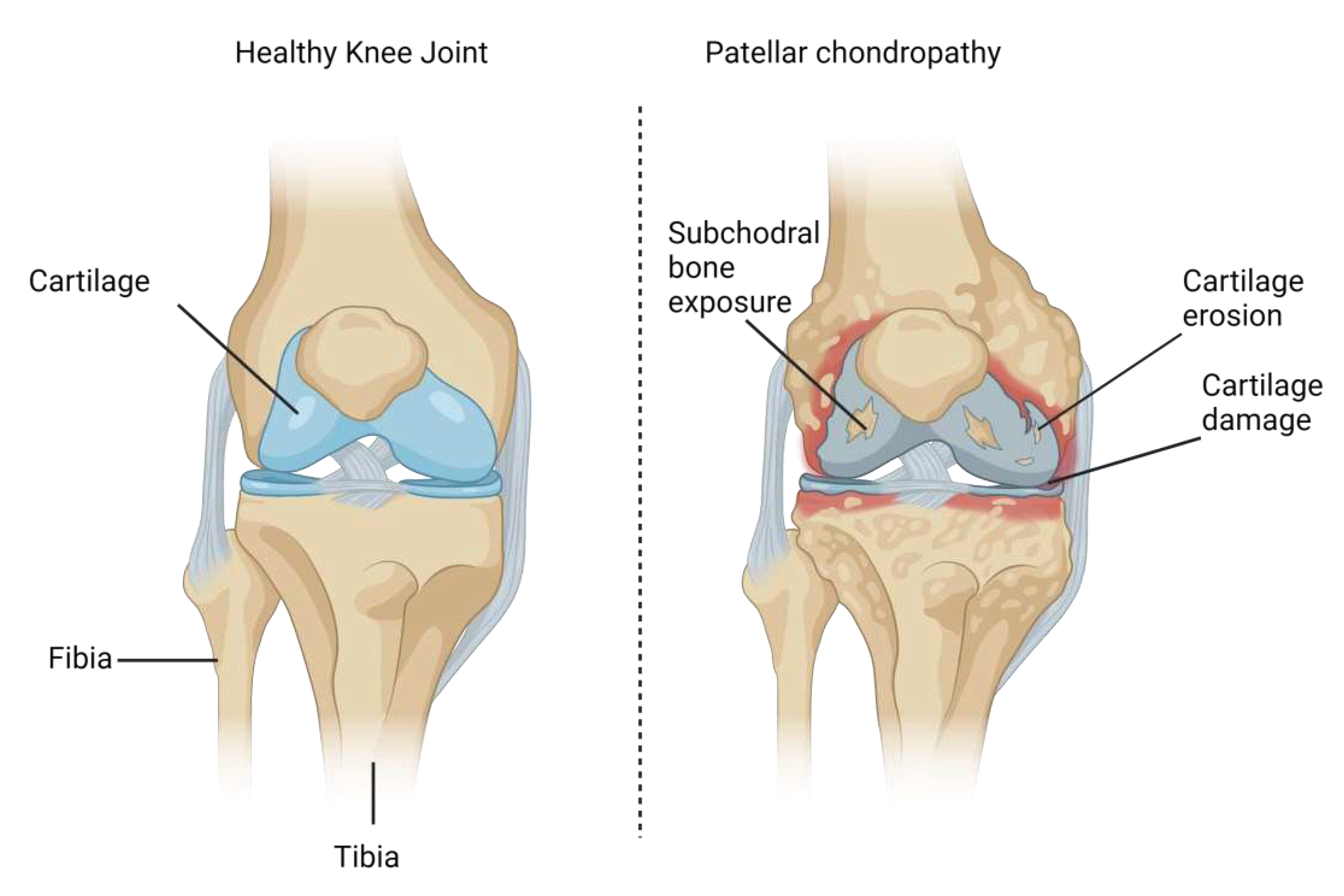
Figure 2.
Platelet-rich plasma flowchart. A) collection of the peripheral blood sample using 3.6 mL of the ACD (acid citrate dextrose) anticoagulant; B) adding blood to sterile falcon tubes; C) separation of blood components after first centrifugation (300 x g for 5 minutes); D) Resuspended pellets (plasma + buffy coat) without platelet poor plasma give rise to L-PRP (Leukocyte-rich PRP) after second centrifugation (700 x g for 17 minutes).
Figure 2.
Platelet-rich plasma flowchart. A) collection of the peripheral blood sample using 3.6 mL of the ACD (acid citrate dextrose) anticoagulant; B) adding blood to sterile falcon tubes; C) separation of blood components after first centrifugation (300 x g for 5 minutes); D) Resuspended pellets (plasma + buffy coat) without platelet poor plasma give rise to L-PRP (Leukocyte-rich PRP) after second centrifugation (700 x g for 17 minutes).
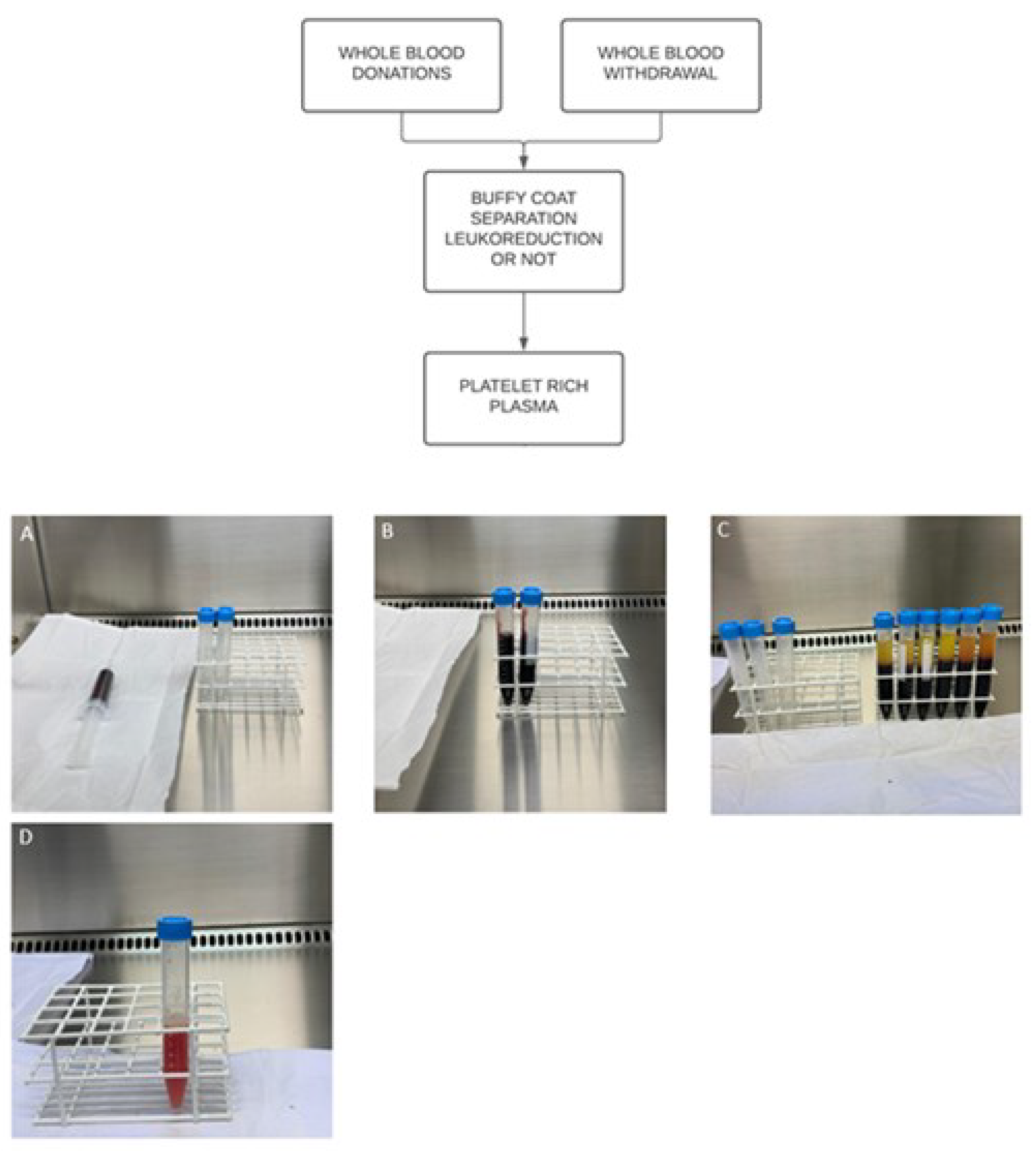
Figure 3.
Intra articular orthobiologic therapy. Intra-articular administration of HA either alone or in combination with PRP attenuates exacerbated pro-inflammatory status in patellar chondropathy.
Figure 3.
Intra articular orthobiologic therapy. Intra-articular administration of HA either alone or in combination with PRP attenuates exacerbated pro-inflammatory status in patellar chondropathy.
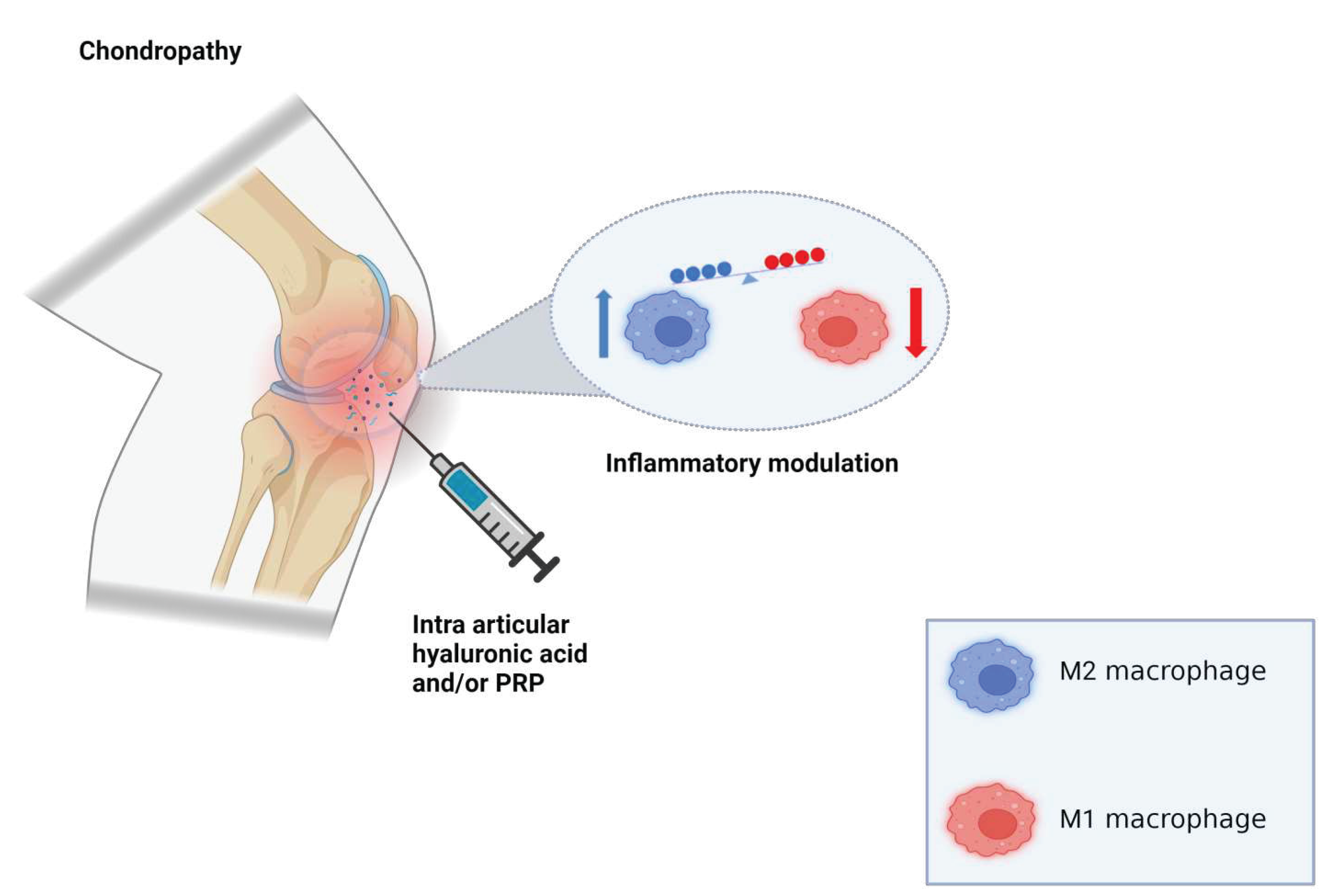

Table 1.
Outerbridge classification scale for patellar chondropathy.
| Grade | Radiological Observations |
|---|---|
| Grade 0 (normal) | No radiological findings |
| Grade I | Softening and swelling, edema |
| Grade II | Fragmentation and fissuring in an area of about 1.27cm2 (half an inch) in diameter |
| Grade III | Acute fragmentation and fissuring in an area of greater than 1.27cm2 (half an inch) in diameter |
| Grade IV | Severe cartilage denudation and erosion down to the subchondral bone compartment |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



