
Submitted:
29 October 2023
Posted:
30 October 2023
You are already at the latest version
Abstract
Proprioceptive deficits accompanied with motor paresis after stroke, namely sensory ataxic motor paresis has a poorer prognosis of recovery than pure motor deficit. We aimed to investigate the effects of repetitive peripheral magnetic stimulation (rPMS) on sensory ataxic upper extremity (UE) paresis at acute stroke. Eighteen stroke participants with sensory ataxic UE paresis were randomized. rPMS group received five sessions of intervention per week, where 20 minutes of rPMS prior to 20 minutes of physical therapy (PT) every other day, alternating with 40 minutes of PT. The control group received five sessions of 40 minutes of PT/week. Outcome measures were Wolf motor function test (WMFT), UE motor section of Fugl-Meyer Motor Assessment Scale (FMA-UE), and Thumb localizing test (TLT). All assessments were compared before and after intervention. rPMS group received mean 6.5 sessions and the control group received 12.8 sessions, showing significantly imbalanced intervention due to different timing of hospital discharge. The imbalance was corrected by calculating gains of motor scores divided by sessions as Progress Rate (PR). Corrected gains (PR) of rPMS group was more significantly enhanced in WMFT and FMA-UE than control groups. rPMS group tended to improve TLT more than control one. rPMS might improve sensory ataxic UE paresis after stroke and proprioceptive deficit.
Keywords:
motor recovery
; neurorehabilitation
; proprioceptive impairment
; position sense
; thumb localizing test
1. Introduction
Proprioceptive information is essential for motor control [1] and motor learning [2]. Proprioceptive deficits of upper extremity impair activities in daily livings, such as skillful movement of hands and manipulating objects. It has been exhibited in healthy older people [3] and poststroke survivors [4].
Proprioceptive deficits following stroke occurred in 27 to 54 % of patients [5,6], but it remains controversial how the disabilities arise. It is correlated with length of hospitalization and mortality rates [4,7,8]. Moreover, proprioceptive deficits accompanied with motor paresis after stroke, namely sensory ataxic motor paresis after stroke has a poorer prognosis of recovery than pure motor deficit. Severity of impaired proprioception can also predict poor prognosis of motor ability, functional ability, and dexterity of the affected UE in chronic phase of stroke [9]. Several reports have suggested the significant association of proprioception dysfunction with motor recovery of paretic UE function after stroke [10,11,12]. Therefore, proprioceptive deficit may be a prognostic factor for the extent of long-term motor recovery after stroke.
Neuromodulators to the periphery, such as neuromuscular electrical stimulation (NMES) and repetitive peripheral magnetic stimulation (rPMS), are expected to become an intervention device facilitating motor recovery after stroke [13,14,15,16]. To date, new findings are being reported that rPMS may facilitate motor recovery of upper extremity (UE) pure paresis in acute phase of stroke [13,17]. rPMS-induced proprioceptive inflows can be finally conveyed to the affected hemisphere, thereby potentially enhancing synaptic connectivity of the neighboring cortex [18]. Therefore, one hypothesis is proposed that rPMS may facilitate motor recovery of UE paresis accompanied with proprioceptive impairments when it was given to paretic muscles of UE with ataxia. The other is that proprioceptive declines themselves might be improved by rPMS, enhancing an augmented somatosensory and proprioceptive input.
Now, we aimed to determine whether rPMS would be beneficial for sensory and motor recovery or not when applied to affected sensory ataxic UE during early acute phase of stroke.
2. Results
2.1. Participants
A CONSORT flow diagram explaining allocation of participants in a randomized manner through the study is shown (Figure 1). 18 subjects met the study criteria and agreed to participate (Table 1 and Table 2). The participants were randomly allocated to two groups in a stratified way (age, sex), the rPMS group and the control one. The demographic characteristics were not significantly different between the two groups (Table 2). Of the 18 participants, 9 patients in rPMS group with UE sensory-motor disability (median 37.9 of FMA-UE function scores; 5 severe proprioception deficit and 4 moderate) received rPMS prior to PT after median 5.6 days from stroke onset, while 9 patients in control group (median 26.0; severe 4, moderate 3 and mild 2) received PT after 5.7 days. The durations of treatment from pretreatment to follow-up estimation (4-25 sessions) were median 6.6 and 12.9 sessions, respectively (Table 2). The findings exhibited significantly shorter sessions of the rPMS group relative to the control group (p = 0.031). Therefore, progress rate was required to justify comparison of restorative gains between two groups.
2.2. Effects of rPMS on motor recovery
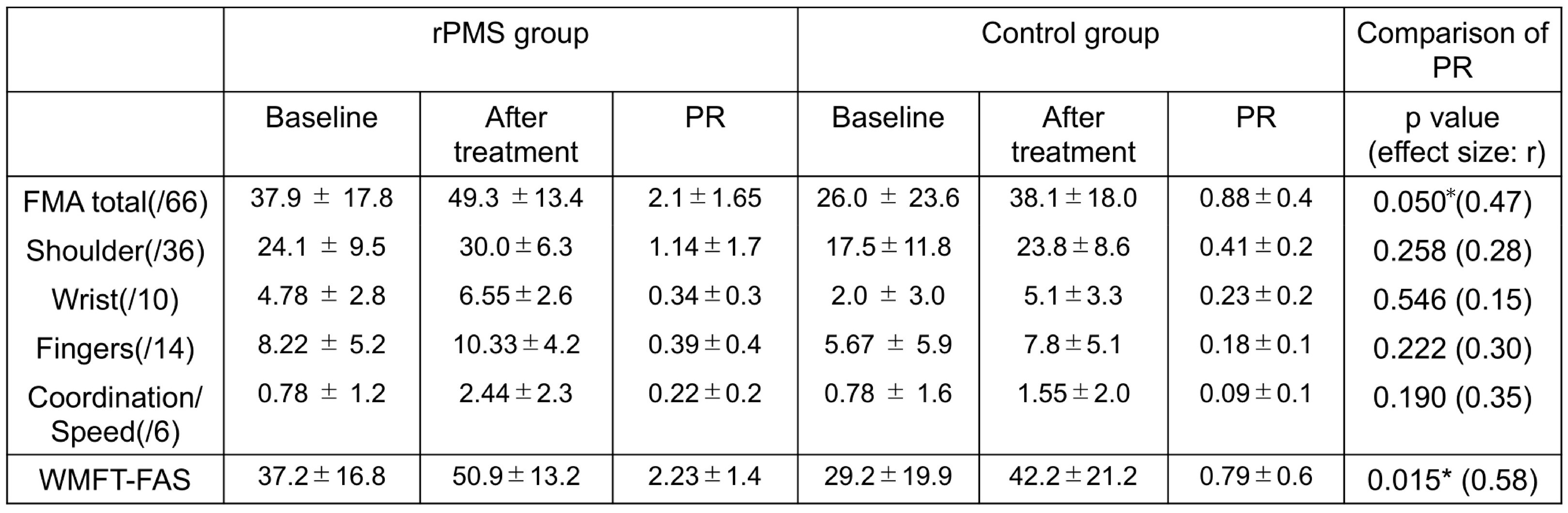
Comparison of WMFT-FAS scores between the groups were not significantly different at pre-and post-treatment. However, the corrected gain (PR) in motor recovery of WMFT-FAS scores was significantly different (U = 61, Z =2.406, p = 0.015). The rPMS group showed large effect size on WMFT-FAS (r = 0.58), suggesting high clinical significance in WMFT-FAS (Figure 2).
Comparison of FMA-UE function between the two groups showed no significant difference at pre- and post-treatment. The corrected gain (PR) of FMA-UE total scores, however, showed significant difference between groups, i.e., 2.10 for rPMS group and 0.88 for control group (U test; U= 63, z = 1.991, p = 0.05). The rPMS group demonstrated medium effect size (r = 0.47) on FMA-UE, suggesting moderate clinical significance in FMA-UE. In sub-analysis of each component of FMA; namely FMA-shoulder, FMA-wrist, FMA-fingers, and FMA-coordination/speed, corrected gains (PRs) of FMA-shoulder, fingers and coordination/speed was not significantly different between two group (Figure 2 and Table 3 and Table 4). However, rPMS group demonstrated medium effect size on FMA-fingers (r = 0.30) and FMA-coordination/speed (r = 0.35), suggesting moderate clinical significance with FMA-fingers and FMA-coordination/speed.
2.3. Effects of rPMS on proprioceptive function
As qualitative analysis, 5 out of 9 patients (44.4%) in rPMS group improved their position sense deficits whereas only two out of 9 patients (22.2%) in control group improved (Table 3). According to the quantitative analysis represented by FMA coordination/speed, the corrected gain (PR) was not significantly higher in rPMS group than those in control one (p = 0.190), but the effect size demonstrated medium (r = 0.35), suggesting moderate clinical significance with FMA coordination/speed (Table 4).
2.4. Others
No adverse events such as pain or discomfort have been observed.
3. Discussion
The present study suggested that rPMS may improve sensory ataxic paresis of UE during early acute phase of stroke. Although only a few reports have suggested the beneficial effect of rPMS on UE pure motor function in acute phase of stroke [13,17], this is the first report supporting the involvement of rPMS in motor recovery of sensory ataxic UE paresis during the early acute phase of stroke. rPMS tended to improve proprioceptive deficits, but the effects were not proven to be significantly beneficial in this study.
Several advantageous points feature in use of rPMS. Especially, it can penetrate deeper without pain, generates higher muscle torque, and is applicable to children. In contrast, the shortcomings are recognized, such as overheating of the coil and a larger area stimulated with increased intensity. So far, rPMS relevant papers used rTMS coil (usually used for stimulating brain over the skull) to convert into peripheral use. In contrast, pathleader, used for this study, was uniquely developed for selective and exclusive stimulation of target muscles with accuracy and could contract target muscles more specifically than above coil (for detail see Figure 3 in methods section).
Proprioceptive declines was affected by aging [3]. This declines were attributable to morphological and physiological changes in both the central [19] and peripheral nervous system [20]. Peripheral nerve abnormalities included capsular thickness [21], decreases in muscle spindle sensitivity [22], and loss of joint mechanoreceptors [20]. Also, morphological and physiological changes in the central nervous system involved decreased gray matter volume in anterior cingulate gyrus, pre- and postcentral gyri, insula, and angular gyri [23], and attenuated activity in proprioceptive regions of the basal ganglia [19]. Accordingly, it is possible that age-related proprioceptive impairments might have already occurred in the enrolled participants (averaged 64 years old and 70 in rPMS and control group, respectively) since before stroke and is plausible that the insult might deteriorate the disability. In addition to age-related proprioceptive declines, the benefits of rPMS to proprioceptive function might be underestimated due to variety of the participants’ age (ranging 44 to 90 years old). The neural mechanisms responsible for proprioceptive deficits affected by stroke have been speculated as to the relevance of damage to the ipsilesional uncrossed descending corticospinal pathways [24] or the disconnection of interhemispheric transcallosal transfer [25]. In addition, we are fully aware of the participants showing a higher progress rate, and inter-subject difference in the magnitude of motor recovery existed not only in the rPMS intervention group but also in the control group. The difference may depend on another factor, such as expression of C-C chemokine receptor 5 (CCR5) in the cortex, affecting motor recovery after stroke [26].
So far, proprioceptive function has been estimated by various measures. TLT has been often used for assessment of position sense [27,28], and several reports have discussed the validation and reliability of TLT and compared TLT with other relevant measures [28,29]. The association between proprioception and UE motor recovery is still unclear because of mixed results among the relevant studies. The difference may in part depend on proprioception measures used [30]. Additionally, we tried to use FMA coordination/speed for estimate position sense. A desirable proprioception measure would be awaited in the future.
Prognosis of sensory deficits after stroke also remains unknown. Our daily clinical observation impressed on us that the sensory disturbances after stroke are often persistent. The impression may be supported by our results, showing that only 20 percent of patients in control group improved their proprioceptive impairment within a month of the insult onset. Several reports have described recovery of sensory function after stroke within the first six months after the onset [6,31]. In contrast, our present results, showing a higher rate of improvement of position sense in rPMS group during shorter duration than control group, would be favorable for the view that rPMS might improve proprioceptive decline. This is supported by a previous study showing a positive effect of rPMS on sensory function, as estimated by a sensation domain of FMA [32]. Another report is also helpful, demonstrating that the improvement of tactile extinction may be induced by a single session of rPMS [33]. Both a direct activation of sensorimotor nerve fibers and an indirect activation of mechanoreceptors could enhance an augmented somatosensory and proprioceptive input. The findings suggested that proprioceptive function may benefit from the application of rPMS.
The rPMS could generate cortical plastic changes in conjunction with motor recovery. The stimulation generates massive proprioceptive flows to the affected hemisphere [34]. A previous PET activation study [35] observed the reorganization of the motor map in the cortex, induced by rPMS. Another study demonstrated that application of rPMS to the peripheral muscles led to an increased motor-evoked potential (MEP) amplitude and decreased MEP latency [34]. Higher MEP amplitudes reflect the recruitment of a larger volume of residual motor pyramidal neurons after a stroke [36]. Shorter MEP latencies can be explained by either better synchronicity of rPMS-derived multiple descending volleys (I-wave) [37], or better recruitment of short-latency corticocortical projections from premotor cortices to primary motor areas [38]. There is increasing evidence supporting the association of motor recovery after stroke with reorganization of damaged brain [39,40]. Specifically, a previous study with monkey ischemic model has been well-known [39]. They revealed that intensive rehabilitative training regained UE paresis and induced an enlargement of the motor map representing the affected forearm. Similarly, many studies have been disclosed the outline of possible neural mechanism underlying UE function recovery mediated by peripheral stimulation, such as NMES [14]. A near-infrared spectroscopy study with chronic patients poststroke suggested that the association of activated ipsilateral sensorimotor cortex with UE motor recovery might be produced by applying NMES to the affected UE [41]. Another neuroimaging study demonstrated that electrical stimulation of the wrist extensor and flexor muscles could activate the contralateral sensorimotor cortex [42]. Given neuroplastic changes associated with motor recovery by virtue of peripheral stimulation, rPMS could improve UE motor function.
This study includes several limitations. A larger sample size with sufficient power is required to obtain definitive statistical results. Further study would be required to find more optimal stimulation parameters and conditions for maximizing the beneficial effects of rPMS on sensory and motor recovery. It remains riddle whether the beneficial effect would be long-lasting. To address this issue, it would be helpful to compare the short-term effects of rTMS on sensory ataxic motor paresis poststroke with the long-term effects.
4. Materials and Methods
4.1. Participants
Subjects were recruited from stroke patients admitted to an academic medical center from March 2020 to February 2021. Inclusion criteria were: (1) medically stable condition; (2) inpatients within two weeks of stroke onset; (3) age 40 – 90 years; (4) intact skin on the affected UE; (5) adequate mental state to participate (well-consciousness); (6) first-ever, UE paresis; 7) proprioceptive impairment. Exclusion criteria were: (1) history of damage from stroke, brain injury or brain tumor; (2) metal implant in head or within stimulation area; (3) aphasia; (4) history of cardiac arrhythmia with hemodynamic instability; (5) comorbidity with neurodegenerative diseases and mental disorders; (6) uncontrolled seizure; (7) impaired consciousness; (8) implanted stimulator (such as cardiac pacemaker and defibrillator).
4.2. Interventional Protocols
We utilized a peripheral magnetic stimulator (Pathleader, IFG, Sendai, Japan) for rPMS treatment. This stimulator is uniquely characterized by generating a selective and exclusive contraction of the target muscle with accuracy. This round coil stimulator generated biphasic 350 μsec with magnetic gradients of up to 15 kT/sec, thus generating repetitive contraction-relaxation cycles that amplify proprioceptive input from target muscles. We adopted an intermittent ON/OFF stimulation protocol consisting of three times 10 consecutive stimulations for each muscle per session, where the duration of each stimulation (ON) was made for 2 sec with a frequency of 30 Hz, a total of 1800 pulses and intensity of 70% MSO (maximal stimulator output: corresponding to 0.65 Tesla) at each stimulation site, and then the stimulation intervals (OFF period) were set at 2 sec. Each of ON period forced each targeted paretic muscle of subjects to contract for 2 sec when stimuli were given to the belly of the muscle of subjects in a sitting position. The stimulator was applied to each of paretic UE muscles in a sequential manner (Figure 3B). The procedure proceeded in the following order: (1) identification of optimal stimulation point (Figure 3A), (2) repeated stimuli (Figure 3B). The target was moved proximal part to distal and the same procedure was continued for each muscle (Figure 3C). We began with identifying such an optimal stimulation point as maximizing the contraction of deltoid. Stimuli were repeated thirty times while keeping the stimulator on optimal point of deltoid muscle. After that, it was followed by biceps brachii, triceps brachii, flexor digitorum superficialis (FDS), and extensor digitorum communis (EDC) & extensor carpi radialis (ECR), respectively (Figure 3C, D). Deltoid, triceps brachii, ECR and EDC were mandatory target muscles applied for rPMS. Optional application of rPMS to flexor muscles (biceps brachii and FDS) was made only to patients with flaccid muscle tone (below 3 in knee-mouth test and/or finger function test of SIAS).
4.3. Intervention protocol
The rPMS group received five sessions of treatment per week, alternating 20 minutes of rPMS and subsequent 20 minutes of physical therapy (PT) with 40 minutes of PT every other day. The control group received five sessions of treatment/week, consisting of a 40 minutes of PT per day (Figure 4). PT included range of motion exercise, affected arm muscle tone normalization, passive and passive-assisted mobilization, progressive neuromuscular facilitation training, and task-oriented training conducted by a trained therapist.
Rehabilitation intervention of acute care hospitals in Japan is often suspended within 2 to 4 weeks of the onset and subsequently followed at restorative rehabilitation care units of other hospitals. Actually, anybody could not anticipate the time of hospital discharge for each subject. This means that the intervention was abruptly ended for both groups. As a result, we can predict that the sessions of intervention attained in the study depend on length of hospitalization.
4.4. Outcome measures
Outcome measures included Wolf motor function test (WMFT) functional ability scale (FAS) [43], and the upper-extremity (UE) motor section of the Fugl-Meyer Motor Assessment Scale (FMA) [44]. These assessment points are set before intervention and after the end of intervention. In WMFT assessment sessions, all tasks are performed as quickly as possible and are truncated at 120 seconds. Tasks 1 - 6 of the WMFT comprise timed joint-segment movements, and tasks 7 - 15 involve timed integrative functional movements. When scoring the FMA motor section (0-66 points), each patient is required to perform 33 movements including shoulder, wrist, fingers, and coordination/speed. Their performance of each movement is scored on a 3-point ordinal scale (0, cannot perform; 1, performs partially; 2, performs fully). As Estimation of coordination/speed, finger-to-nose test was adopted. When subject was sitting with eyes closed, he was instructed to put the tip of his index finger from knee to nose 5 times as fast as possible. The following details are assessed: Tremor: 0 marked tremor; 1: slight tremor; 2: no tremor. Dysmetria: 0: pronounced dysmetria; 1: slight and systematic dysmetria; 2: no dysmetria. Speed: the swiftness of motion is compared relative to unaffected arm. 0: repeated 5 times of finger-to-nose test with the affected arm is at least 6 seconds slower than the unaffected one; 1: 2 to 5 seconds slower than the affected one; 2: less than 2 seconds difference. Three details estimated gave a maximum sum of 6 points.
4.5. Assessment of Proprioceptive function
Proprioception is generally classified into three subtypes: i.e., position, motion, and force senses. Especially, position sense refers to as the ability to perceive the position of a joint or body part. For quantitative assessment of whole-limb position sense, thumb localizing test (TLT) was chosen [27,29,45]. The examiner begins by confirming normal proprioception in the unaffected arm by enabling patients to touch the nose by the unaffected arm with the eyes closed. After the participant’s affected arm is moved passively to four different locations in space, the participant is required to precisely grasp their affected thumb with their unaffected hand in their eyes-closed condition. The scoring is based on the estimated distance that each patient misses their affected thumb in space and discriminates between 4 grades; no difficulty (grade 0: locates the affected thumb accurately and grasps it precisely), mild (grade 1: just misses to grasp the thumb by no more 3 inches and locates correctly it within 5 seconds), moderate (grade 2: is able to find the arm and then uses the arm to find the thumb), or severe proprioception deficits (grade 3: cannot climb up the affected arm to locate his/her thumb). The final TLT score is determined according to the worst performance. As another index of position sense, we shed light on FMA coordination/speed. Because proprioceptive disturbance can cause profound dysregulation of coordinated movements of UE.
4.6. Indices of corrected gains of UE motor recovery
To decide whether rPMS prior to PT would be more effective for motor recovery than conventional PT, restorative gains of improvement in UE function were compared. Because inter-subject differences in sessions as treatment duration depend on the time of hospital discharge, gains should be corrected for comparison between the two groups. Thus, progress rate was defined as corrected gains of motor recovery, namely UE function scores divided by sessions and then the progress rates were comparison between groups.
4.7. Statistical Analysis
Statistical analysis was performed by either Pearson’s chi-square test or Mann-Whitney U test for nonparametric data using SPSS ver. 26. Results were accepted as statistically significant at p ≦ 0.05. p value is likely to be vulnerable for sample size, whereas effect size is more valuable and reliable than p value in case of small sampling size. Accordingly, effect size (r value) of outcome measures for nonparametric data was worked out to measure the magnitude of treatment effect: r = Z/√N, where N is the total number of samples and Z is derived from Mann-Whitney U test. r values of 0.1, 0.3, and 0.5 represent small, moderate, and large effect sizes, respectively.
5. Conclusions
We showed that rPMS might facilitate motor recovery for ataxic hemiparesis at acute phase of stroke patients although it might have only a trend toward proprioceptive improvement. We just hope that our efforts might provide some clue to full recovery of UE sensory ataxic paresis after stroke in the future.
Author Contributions
“Conceptualization, S.O. and R.T.; methodology, S.O., R.T. H.S.; validation, S.O., R.T. and H.S..; formal analysis, K.T.; investigation, R.T. and H.S.; resources, S.O.; data curation, S.O. and R.T.; writing—original draft preparation, S.O.; writing—review and editing, S.O.; visualization, S.O., R.T. and H.S.; supervision, S.O.; project administration, S.O.; funding acquisition, S.O. All authors have read and agreed to the published version of the manuscript.
Funding
This study was partially supported by a Grant-in-Aid for Scientific Research (C; Grant number 22K11425) from the Japan Society for the Promotion of Science.
Institutional Review Board Statement
The study protocol was approved by the ethics committee of Dokkyo Medical University Saitama Medical Center (Registered Number:1902) and was registered at University hospital Medical Information Network Clinical Trials Registry(https://www.umin.ac.jp/ctr/. Unique identifier: UMIN000047323). This study was conducted in accordance with relevant ethical guidelines.
Informed Consent Statement
Participants provided written informed consent before study enrollment.
Data Availability Statement
All data generated or analyzed during this study are included in this published article.
Acknowledgments
The authors thank our co-medical staffs in our acute rehabilitation care unit for their cooperation.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Jeannerod, M. The Neural and Behavioral Organization of Goal-Directed Movements. Oxford University Press. 1988. [Google Scholar]
- Schmidt, R.A.L., T. Motor Control and Learning. 5th Edn. Champaign, IL.: Human Kinetics. 1988.
- Adamo, D.E.; Martin, B.J.; Brown, S.H. Age-related differences in upper limb proprioceptive acuity. Percept Mot Skills 2007, 104, 1297–1309. [Google Scholar] [CrossRef]
- Carey, L.M.; Matyas, T.A.; Oke, L.E. Sensory loss in stroke patients: effective training of tactile and proprioceptive discrimination. Arch Phys Med Rehabil 1993, 74, 602–611. [Google Scholar] [CrossRef]
- Tyson, S.F.; Hanley, M.; Chillala, J.; Selley, A.B.; Tallis, R.C. Sensory loss in hospital-admitted people with stroke: characteristics, associated factors, and relationship with function. Neurorehabil Neural Repair 2008, 22, 166–172. [Google Scholar] [CrossRef] [PubMed]
- Connell, L.A.; Lincoln, N.B.; Radford, K.A. Somatosensory impairment after stroke: frequency of different deficits and their recovery. Clin Rehabil 2008, 22, 758–767. [Google Scholar] [CrossRef]
- Zeman, B.D.; Yiannikas, C. Functional prognosis in stroke: use of somatosensory evoked potentials. J Neurol Neurosurg Psychiatry 1989, 52, 242–247. [Google Scholar] [CrossRef] [PubMed]
- Sommerfeld, D.K.; von Arbin, M.H. The impact of somatosensory function on activity performance and length of hospital stay in geriatric patients with stroke. Clin Rehabil 2004, 18, 149–155. [Google Scholar] [CrossRef]
- Rand, D. , Weiss, P.L., Gottlieb, D. Does Proprioceptive Loss Influence Recovery of the Upper Extremity After Stroke? Neurorehabilitation and Neural Repair 1999, 13, 15–21. [Google Scholar] [CrossRef]
- Kusoffsky, A.; Wadell, I.; Nilsson, B.Y. The relationship between sensory impairment and motor recovery in patients with hemiplegia. Scand J Rehabil Med 1982, 14, 27–32. [Google Scholar] [CrossRef]
- de Weerdt, W.; Lincoln, N.B.; Harrison, M.A. Prediction of arm and hand function recovery in stroke patients. Int J Rehabil Res 1987, 10, 110–112. [Google Scholar] [CrossRef]
- Wade, D.T.; Langton-Hewer, R.; Wood, V.A.; Skilbeck, C.E.; Ismail, H.M. The hemiplegic arm after stroke: measurement and recovery. J Neurol Neurosurg Psychiatry 1983, 46, 521–524. [Google Scholar] [CrossRef] [PubMed]
- Obayashi, S.; Takahashi, R. Repetitive peripheral magnetic stimulation improves severe upper limb paresis in early acute phase stroke survivors. NeuroRehabilitation 2020, 46, 569–575. [Google Scholar] [CrossRef] [PubMed]
- Obayashi, S.; Saito, H. Neuromuscular Stimulation as an Intervention Tool for Recovery from Upper Limb Paresis after Stroke and the Neural Basis. Applied Sciences 2022, 12. [Google Scholar] [CrossRef]
- Obayashi, S.; Takahashi, R.; Onuki, M. Upper limb recovery in early acute phase stroke survivors by coupled EMG-triggered and cyclic neuromuscular electrical stimulation. NeuroRehabilitation 2020, 46, 417–422. [Google Scholar] [CrossRef]
- Francisco, G.; Chae, J.; Chawla, H.; Kirshblum, S.; Zorowitz, R.; Lewis, G.; Pang, S. Electromyogram-triggered neuromuscular stimulation for improving the arm function of acute stroke survivors: a randomized pilot study. Arch Phys Med Rehabil 1998, 79, 570–575. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.F.; Zhang, D.; Zhang, J.; Hai, H.; Zhao, Y.Y.; Ma, Y.W. A Randomized Controlled Trial of Repetitive Peripheral Magnetic Stimulation applied in Early Subacute Stroke: Effects on Severe Upper-limb Impairment. Clin Rehabil 2022, 36, 693–702. [Google Scholar] [CrossRef]
- Beaulieu, L.D.; Schneider, C. Effects of repetitive peripheral magnetic stimulation on normal or impaired motor control. A review. Neurophysiol Clin 2013, 43, 251–260. [Google Scholar] [CrossRef] [PubMed]
- Goble, D.J.; Coxon, J.P.; Van Impe, A.; Geurts, M.; Van Hecke, W.; Sunaert, S.; Wenderoth, N.; Swinnen, S.P. The neural basis of central proprioceptive processing in older versus younger adults: an important sensory role for right putamen. Hum Brain Mapp 2012, 33, 895–908. [Google Scholar] [CrossRef]
- Morisawa, Y. Morphological study of mechanoreceptors on the coracoacromial ligament. J Orthop Sci 1998, 3, 102–110. [Google Scholar] [CrossRef]
- Swash, M.; Fox, K.P. The effect of age on human skeletal muscle. Studies of the morphology and innervation of muscle spindles. J Neurol Sci 1972, 16, 417–432. [Google Scholar] [CrossRef]
- Kim, G.H.; Suzuki, S.; Kanda, K. Age-related physiological and morphological changes of muscle spindles in rats. J Physiol 2007, 582, 525–538. [Google Scholar] [CrossRef] [PubMed]
- Good, C.D.; Johnsrude, I.S.; Ashburner, J.; Henson, R.N.; Friston, K.J.; Frackowiak, R.S. A voxel-based morphometric study of ageing in 465 normal adult human brains. Neuroimage 2001, 14, 21–36. [Google Scholar] [CrossRef] [PubMed]
- Ziemann, U.; Ishii, K.; Borgheresi, A.; Yaseen, Z.; Battaglia, F.; Hallett, M.; Cincotta, M.; Wassermann, E.M. Dissociation of the pathways mediating ipsilateral and contralateral motor-evoked potentials in human hand and arm muscles. J Physiol 1999, 518 Pt 3, 895–906. [Google Scholar] [CrossRef]
- Shimizu, T.; Hosaki, A.; Hino, T.; Sato, M.; Komori, T.; Hirai, S.; Rossini, P.M. Motor cortical disinhibition in the unaffected hemisphere after unilateral cortical stroke. Brain 2002, 125, 1896–1907. [Google Scholar] [CrossRef] [PubMed]
- Joy, M.T.; Ben Assayag, E.; Shabashov-Stone, D.; Liraz-Zaltsman, S.; Mazzitelli, J.; Arenas, M.; Abduljawad, N.; Kliper, E.; Korczyn, A.D.; Thareja, N.S.; et al. CCR5 Is a Therapeutic Target for Recovery after Stroke and Traumatic Brain Injury. Cell 2019, 176, 1143–1157. [Google Scholar] [CrossRef] [PubMed]
- Hirayama, K.; Fukutake, T.; Kawamura, M. 'Thumb localizing test' for detecting a lesion in the posterior column-medial lemniscal system. J Neurol Sci 1999, 167, 45–49. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Chen, Y.; Lou, T.; Shen, X. Correlation Between Proprioceptive Impairment and Motor Deficits After Stroke: A Meta-Analysis Review. Front Neurol 2021, 12, 688616. [Google Scholar] [CrossRef]
- Suda, M.; Kawakami, M.; Okuyama, K.; Ishii, R.; Oshima, O.; Hijikata, N.; Nakamura, T.; Oka, A.; Kondo, K.; Liu, M. Validity and Reliability of the Semmes-Weinstein Monofilament Test and the Thumb Localizing Test in Patients With Stroke. Front Neurol 2020, 11, 625917. [Google Scholar] [CrossRef] [PubMed]
- Hughes, C.M.; Tommasino, P.; Budhota, A.; Campolo, D. Upper extremity proprioception in healthy aging and stroke populations, and the effects of therapist- and robot-based rehabilitation therapies on proprioceptive function. Front Hum Neurosci 2015, 9, 120. [Google Scholar] [CrossRef]
- Winward, C.E.; Halligan, P.W.; Wade, D.T. The Rivermead Assessment of Somatosensory Performance (RASP): standardization and reliability data. Clin Rehabil 2002, 16, 523–533. [Google Scholar] [CrossRef]
- Krewer, C.; Hartl, S.; Muller, F.; Koenig, E. Effects of repetitive peripheral magnetic stimulation on upper-limb spasticity and impairment in patients with spastic hemiparesis: a randomized, double-blind, sham-controlled study. Arch Phys Med Rehabil 2014, 95, 1039–1047. [Google Scholar] [CrossRef] [PubMed]
- Heldmann, B.; Kerkhoff, G.; Struppler, A.; Havel, P.; Jahn, T. Repetitive peripheral magnetic stimulation alleviates tactile extinction. Neuroreport 2000, 11, 3193–3198. [Google Scholar] [CrossRef] [PubMed]
- Flamand, V.H.; Schneider, C. Noninvasive and painless magnetic stimulation of nerves improved brain motor function and mobility in a cerebral palsy case. Arch Phys Med Rehabil 2014, 95, 1984–1990. [Google Scholar] [CrossRef] [PubMed]
- Struppler, A.; Binkofski, F.; Angerer, B.; Bernhardt, M.; Spiegel, S.; Drzezga, A.; Bartenstein, P. A fronto-parietal network is mediating improvement of motor function related to repetitive peripheral magnetic stimulation: A PET-H2O15 study. Neuroimage 2007, 36 Suppl 2, T174–186. [Google Scholar] [CrossRef]
- Rothwell, J.C. Techniques and mechanisms of action of transcranial stimulation of the human motor cortex. J Neurosci Methods 1997, 74, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Amassian, V.E.; Stewart, M.; Quirk, G.J.; Rosenthal, J.L. Physiological basis of motor effects of a transient stimulus to cerebral cortex. Neurosurgery 1987, 20, 74–93. [Google Scholar] [CrossRef] [PubMed]
- Volz, L.J.; Hamada, M.; Rothwell, J.C.; Grefkes, C. What Makes the Muscle Twitch: Motor System Connectivity and TMS-Induced Activity. Cereb Cortex 2015, 25, 2346–2353. [Google Scholar] [CrossRef] [PubMed]
- Nudo, R.J.; Wise, B.M.; SiFuentes, F.; Milliken, G.W. Neural substrates for the effects of rehabilitative training on motor recovery after ischemic infarct. Science 1996, 272, 1791–1794. [Google Scholar] [CrossRef] [PubMed]
- Grefkes, C.; Fink, G.R. Connectivity-based approaches in stroke and recovery of function. Lancet Neurol 2014, 13, 206–216. [Google Scholar] [CrossRef]
- Hara, Y.; Obayashi, S.; Tsujiuchi, K.; Muraoka, Y. The effects of electromyography-controlled functional electrical stimulation on upper extremity function and cortical perfusion in stroke patients. Clin Neurophysiol 2013, 124, 2008–2015. [Google Scholar] [CrossRef]
- Blickenstorfer, A.; Kleiser, R.; Keller, T.; Keisker, B.; Meyer, M.; Riener, R.; Kollias, S. Cortical and subcortical correlates of functional electrical stimulation of wrist extensor and flexor muscles revealed by fMRI. Hum Brain Mapp 2009, 30, 963–975. [Google Scholar] [CrossRef] [PubMed]
- Wolf, S.L.; Catlin, P.A.; Ellis, M.; Archer, A.L.; Morgan, B.; Piacentino, A. Assessing Wolf motor function test as outcome measure for research in patients after stroke. Stroke 2001, 32, 1635–1639. [Google Scholar] [CrossRef] [PubMed]
- Fugl-Meyer, A.R.; Jaasko, L.; Leyman, I.; Olsson, S.; Steglind, S. The post-stroke hemiplegic patient. 1. a method for evaluation of physical performance. Scand J Rehabil Med 1975, 7, 13–31. [Google Scholar] [CrossRef] [PubMed]
- Prescott, R.J.; Garraway, W.M.; Akhtar, A.J. Predicting functional outcome following acute stroke using a standard clinical examination. Stroke 1982, 13, 641–647. [Google Scholar] [CrossRef]
Figure 1.
CONSORT flow diagram.
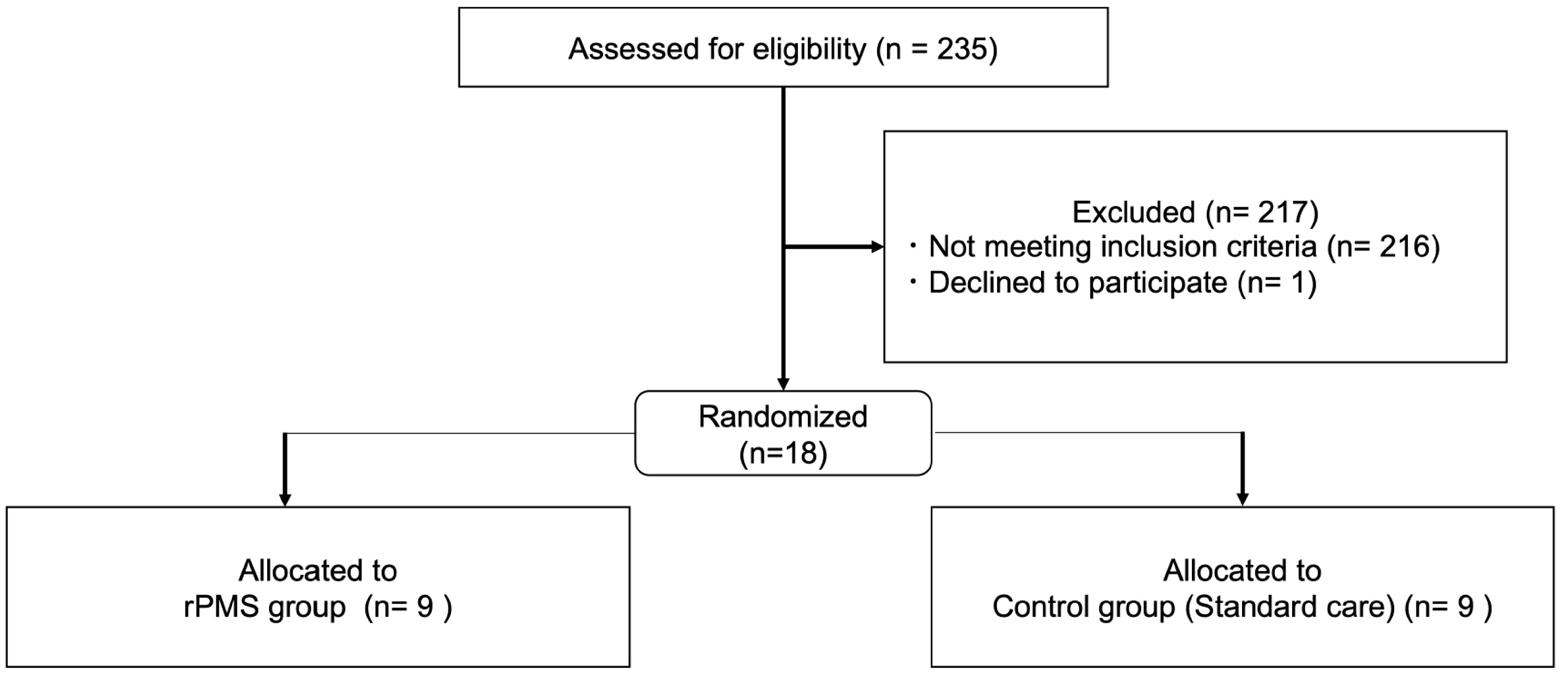
Figure 2.
Corrected gains in motor recovery. A. Corrected gain (PR) of WMFT scores differed significantly between groups. * denotes significant different p value (p ≦ 0.05). Error bar means SEM. AVG: average; G: group. B. Corrected gain (PR) of FMA-UE total scores were significantly different (p ≦ 0.05).
Figure 2.
Corrected gains in motor recovery. A. Corrected gain (PR) of WMFT scores differed significantly between groups. * denotes significant different p value (p ≦ 0.05). Error bar means SEM. AVG: average; G: group. B. Corrected gain (PR) of FMA-UE total scores were significantly different (p ≦ 0.05).
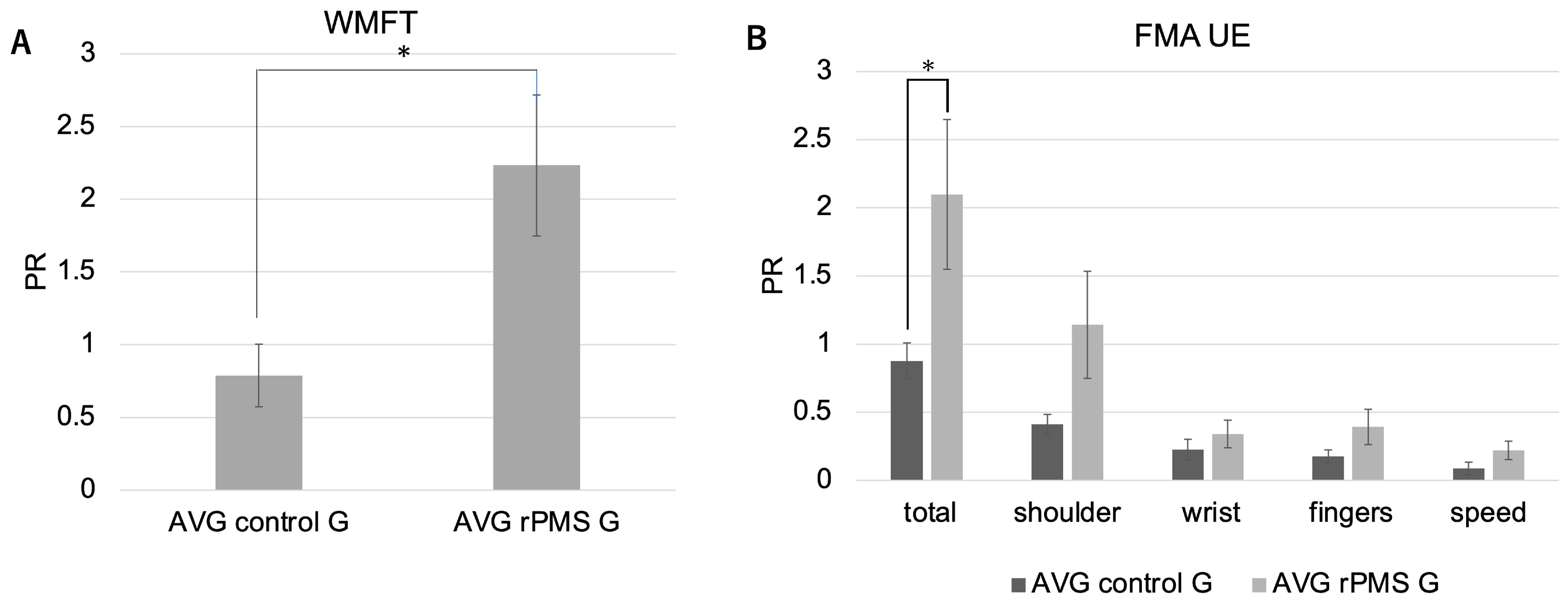
Figure 3.
Stimulation procedure. A) Identification of stimulation point. We began with identifying such an optimal stimulation point as maximizing the contraction of a target muscle. This stimulator is uniquely characterized by generating a selective and exclusive contraction of the target muscle with accuracy. The placement of stimulator for deltoid muscle was illustrated. B) Stimulation setting. S: stimuli; I: interval, C) Stimulation sequence. The daily stimulation was proceeded in numerical order. D) rPMS placement. The placement of stimulator for each muscle was illustrated.
Figure 3.
Stimulation procedure. A) Identification of stimulation point. We began with identifying such an optimal stimulation point as maximizing the contraction of a target muscle. This stimulator is uniquely characterized by generating a selective and exclusive contraction of the target muscle with accuracy. The placement of stimulator for deltoid muscle was illustrated. B) Stimulation setting. S: stimuli; I: interval, C) Stimulation sequence. The daily stimulation was proceeded in numerical order. D) rPMS placement. The placement of stimulator for each muscle was illustrated.
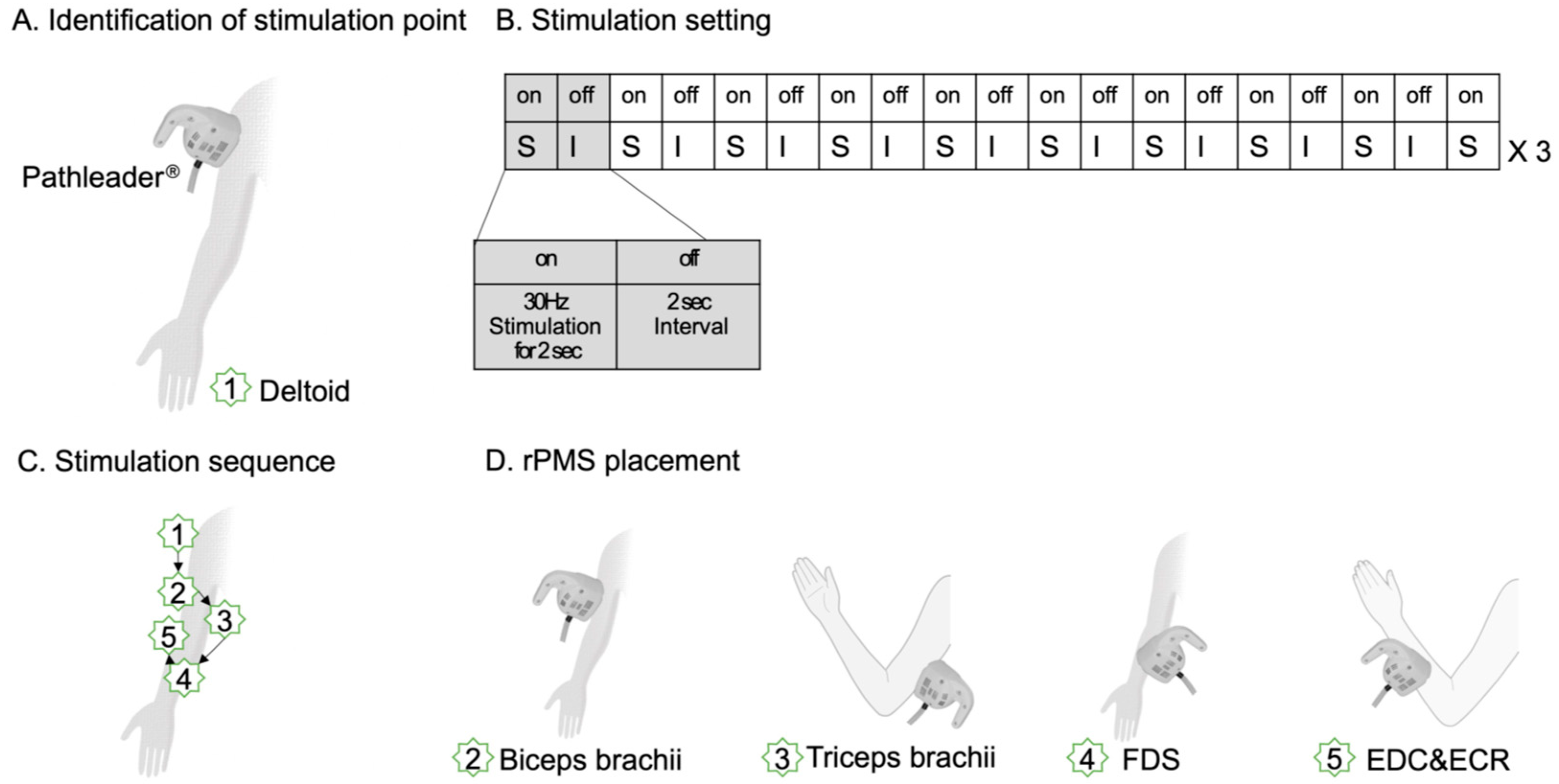
Figure 4.
Intervention protocol. (A) Schedule for rPMS group; (B) Schedule for Control group. Intervention was continued in this sequence since 4 th week.
Figure 4.
Intervention protocol. (A) Schedule for rPMS group; (B) Schedule for Control group. Intervention was continued in this sequence since 4 th week.
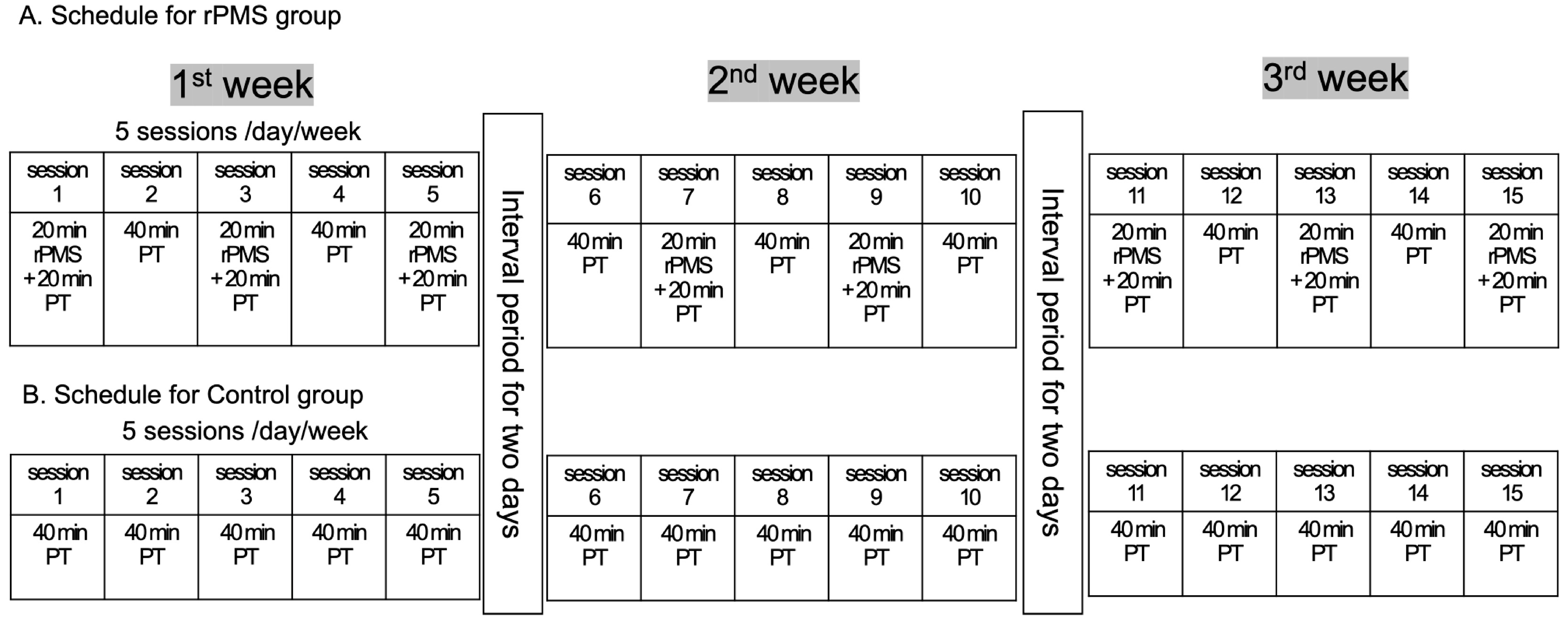

Table 1.
Patient Characteristics. BAD: branch atheromatous disease; Int.: internal; MCA: middle cerebral artery; multiple: multiple cerebral infarcts; M: male; F: female; I: infarct; H: hemorrhage; R: right; L: left.
Table 1.
Patient Characteristics. BAD: branch atheromatous disease; Int.: internal; MCA: middle cerebral artery; multiple: multiple cerebral infarcts; M: male; F: female; I: infarct; H: hemorrhage; R: right; L: left.
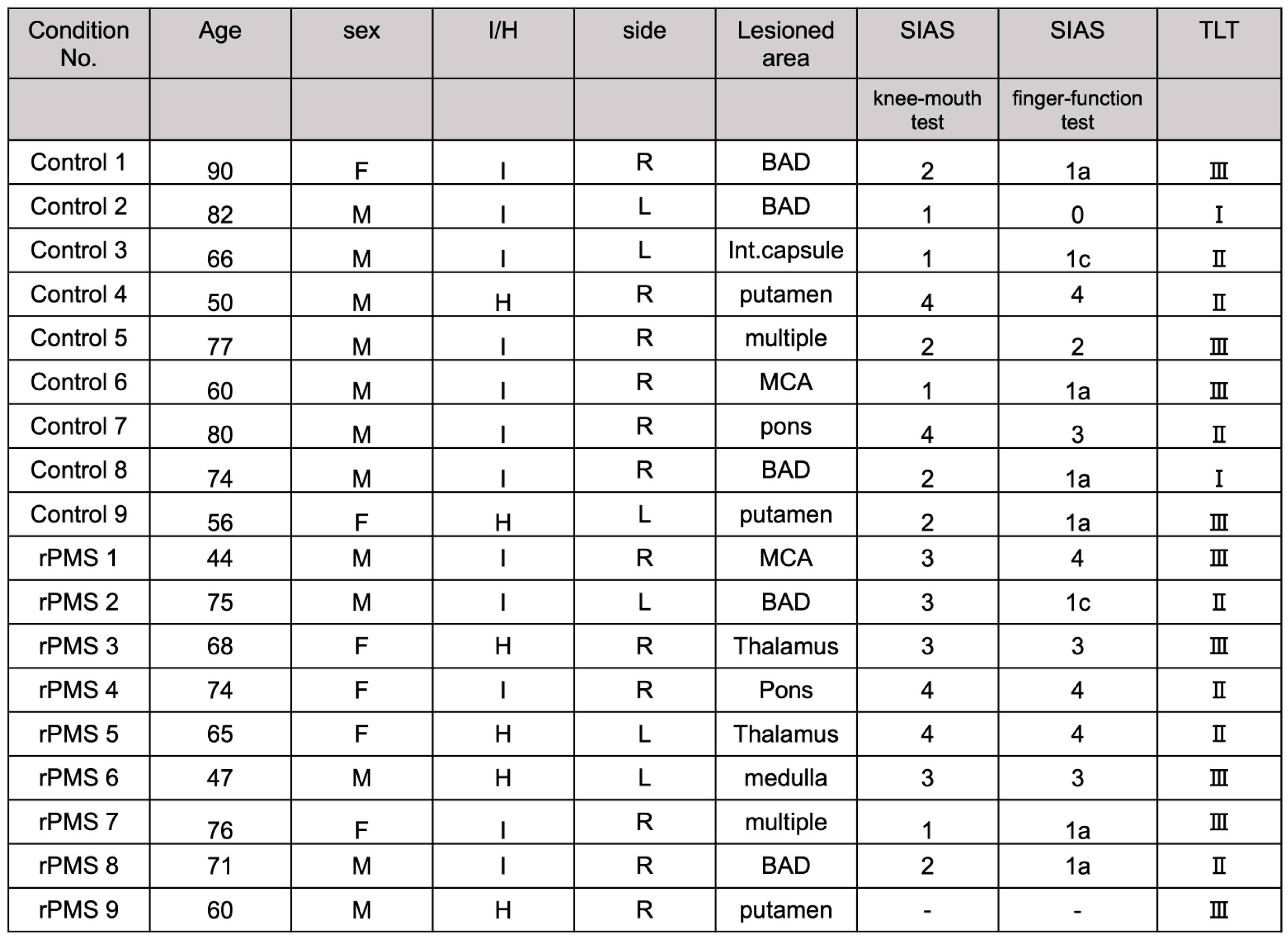 |
Table 2.
Demographic and clinical data. M: male; F: female; y: years; H: hemorrhage; I: infarct; L: left; R: right.
Table 2.
Demographic and clinical data. M: male; F: female; y: years; H: hemorrhage; I: infarct; L: left; R: right.
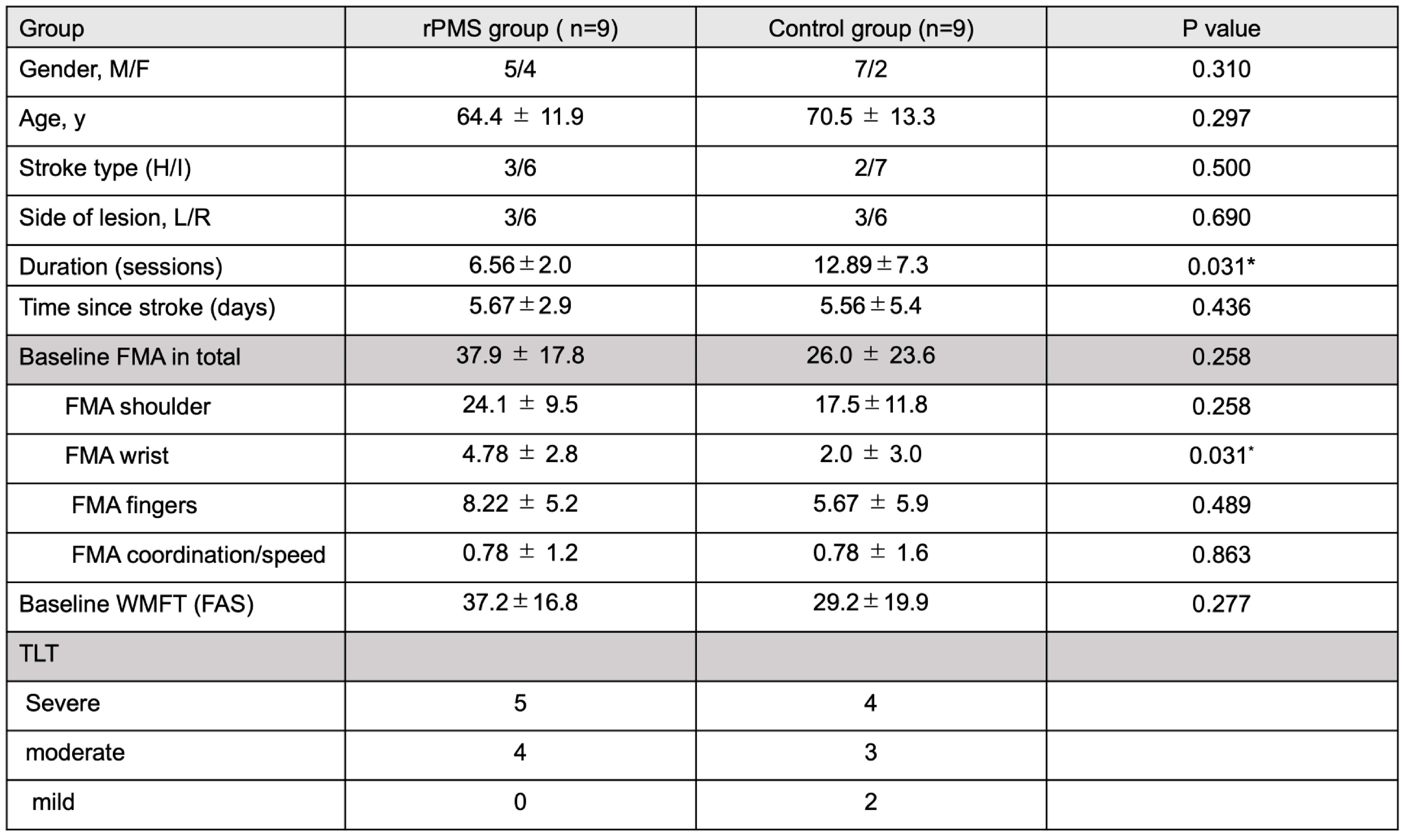 |
Table 3.
Behavioral changes in individual subjects. We could not find any association between age and PR. The recovery speed, represented by PR, seemed to be independent of aging in both groups. Co: coordination; PR: progress rate.
Table 3.
Behavioral changes in individual subjects. We could not find any association between age and PR. The recovery speed, represented by PR, seemed to be independent of aging in both groups. Co: coordination; PR: progress rate.
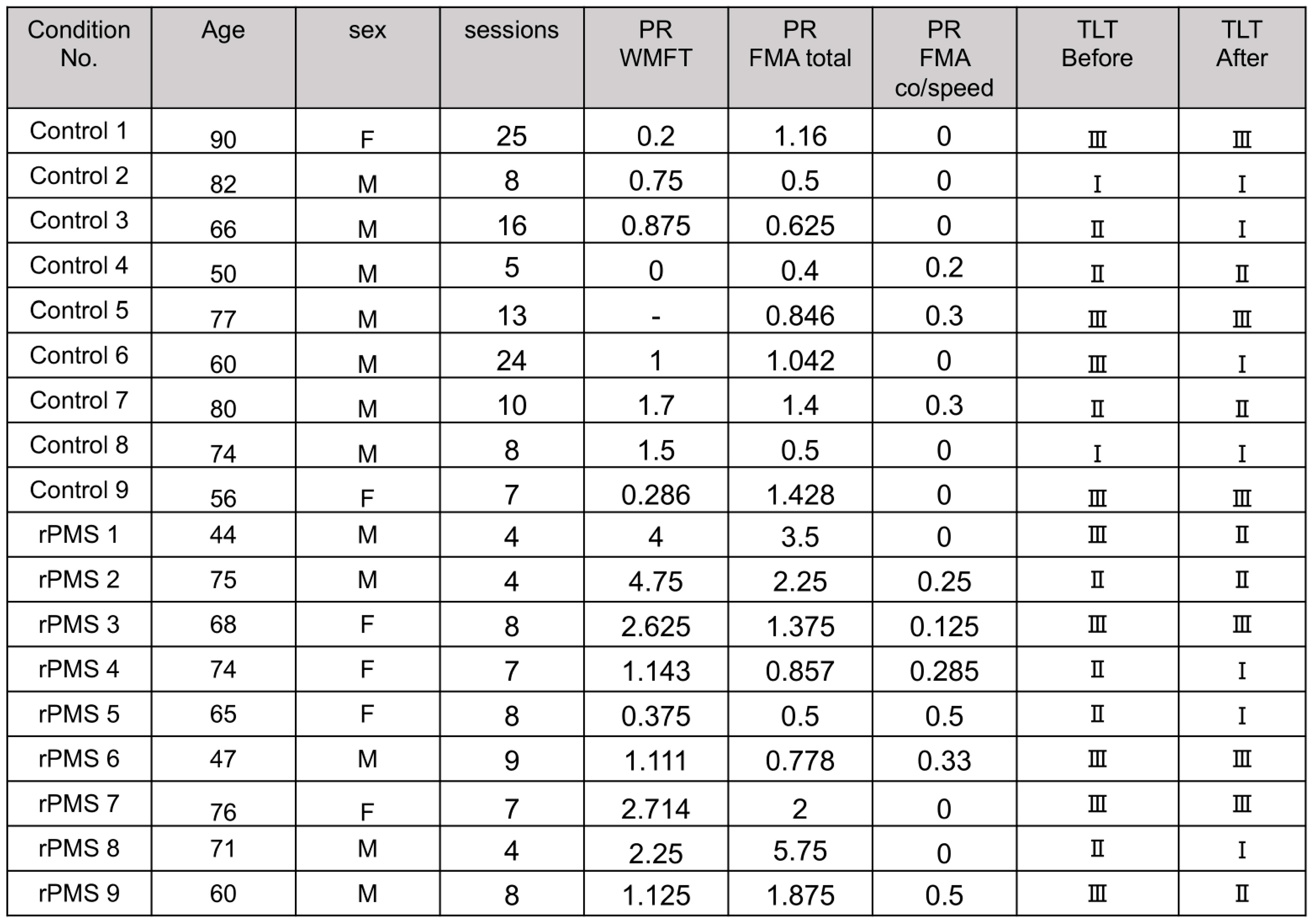 |
Table 4.
Changes in UE functions after intervention. * denotes significant different p value (p ≦ 0.05).
Table 4.
Changes in UE functions after intervention. * denotes significant different p value (p ≦ 0.05).
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



