
Submitted:
25 October 2023
Posted:
26 October 2023
You are already at the latest version
Abstract
The aim of this report is to evaluate the segmental rib index (RI) from T1-T12 spinal level in mild and moderate idiopathic scoliosis (IS) curves of thoracic, thoracolumbar and lumbar type by gender. The relationship of segmental RI to the frontal plane radiological deformity presented as the Cobb angle and to the posterior truncal surface deformity presented as the scoliometric readings of Angle of Trunk Rotation (ATR) in these patients is also assessed. Any statistical significant rela-tionship of these parameters would be very important for biomechanical relations of the rib cage (RC) deformity presented as the rib hump deformity (RHD) and the deformity in the spine and it would thus provide valuable information about scoliogeny. The segmental rib index (RI) is presented in 83 boys and girls with mild and moderate IS. The measurements include the scoliometric readings for truncal asymmetry (TA), the Cobb angle assessment and the segmental RI from T1-T12. The statistical package SPSS 23 was used for statistical analysis. The TA is documented and the Cobb angle is presented by gender and curve type. The segmental RI of thoracic, thoracolumbar and lumbar curves are presented for the first time. The correlations of the segmental RI to surface deformity presented as the rib hump deformity (RHD) in all IS patients and particularly in thoracic curves, to Cobb angle by gender and age and the comparison of the segmental RI index of asymmetric but not scoliotic children to the scoliotic peers by curve (in thoracic, thoracolumbar, lumbar curves) in boys and girls are presented. The findings emphasize the significant protagonistic role of the thoracic asymmetry in relation to the spinal deformity mainly in girls for the thoracic and in boys for the thoracolumbar curves. The cut-off point of age of the examined scoliotics is 14 years, that is when the RI shows stronger correlation with the spinal deformity, namely when the thoracic deformity is decisively effective to the developing thoracic spinal deformity, in terms of Cobb angle. In summary, the results of this study provide aetiological implications for IS, as far as the role of thorax is con-cerned.
Keywords:
Idiopathic scoliosis
; double rib contour sign
; rib index
; rib cage
; Cobb angle
; segmental rib index
; rib hump deformity
; Adams test
; lateral standing radiographs
; angle of trunk rotation
; scoliometer
1. Introduction
The existence of truncal asymmetry (TA) presented as rib hump deformity (RHD) in the Adams bending test during the school scoliosis screening (SSS) programs, is a finding which defines the number of children who will be referred to the scoliosis outpatient departments of hospitals and it is a dominant predictor of scoliosis, [1,2,3].
The rib index (RI) method was introduced as a radiological measurement for the assessment of the RHD which essentially represents the rib cage (RC) deformity in transverse plane. It was originally presented to assess the RHD of IS at the more prominent point of the double rib contour sign (DRCS) on the lateral standing radiographs (LSR) of their RC, [4].
The RI is used for the documentation of the rib-cage initial deformity on the transverse plane before any treatment, for the assessment of the benefits of physiotherapeutic scoliosis specific exercises on RC deformity, [5], for the assessment of bracing on RC deformity, [6], and for the pre- and post-operative assessment of the rib-cage deformity and its correction, [7,8].
Studying the lateral spinal profile (LSR) of the IS patients radiographically, we recognized that the thoracic level of the most prominent point of the DRCS differs in the various types of IS curves. This observation motivated us to study the RI segmentally at all the vertebral levels (T1-T12) on the DRC at the radiographs of thoracic, thoracolumbar and lumbar curves. We also investigated if there was any correlation between segmental RI thoracic levels to the degree of the Cobb angle, respectively when and how the existing surface deformity correlates to mild and moderate spinal deformity.
For idiopathic scoliosis (IS) the word aetiology strictly means the factor(s) causing the AIS, pathogenesis the mode of origin of the morbid process, and pathomechanism / pathobiomechanics the sequence of events in the evolution of its structural and functional changes that result from the pathological process [9]. Prof RG Burwell of Nottingham, suggested the word scoliogeny as the collective noun to include aetiology, pathogenesis and pathomechanism/pathobiomechanics [10]. However, when scoliogeny is used in this study, we will only referrer to the pathogenesis and the pathobiomechanics of this condition.
In summary, the aim of this report was to evaluate the segmental RI from T1-T12 spinal level in mild and moderate IS thoracic, thoracolumbar and lumbar curves by gender and to assess the relationship of segmental RI to the frontal plane radiological deformity and to the scoliometer readings of posterior truncal surface deformity presented by the Angle of Trunk Rotation (ATR). Any significant relationship of these parameters would be very important for the biomechanical relations of the RC (RHD) with the spine deformity and may thus provide information about scoliogeny.
2. Material and Methods
Study design: This is a retrospective statistical study on cross-sectional data collected in Greece, Bosnia and Herzegovina and Serbia.
The examined subjects. Eighty-three children and adolescents, 20 boys and 63 girls with juvenile and adolescent IS were included in the study, with a mean age 12.3±2.7 (range 7 to 17 years), and a mean Cobb angle of 23.8 (15.5-38.7) degrees. 25 patients (19 girls, 6 boys) had primary thoracic, 33 (27 girls, 6 boys) thoracolumbar and 25 (17 girls, 8 boys) lumbar curves respectively. 27 asymmetric children who were referred for further radiological assessment due to the presence of RHD at the Adams test with a radiological curve less than 10 degrees or with a straight spine were also included. The data of scoliotics were collected before any treatment. Any non-idiopathic scoliotic case was excluded from the study.
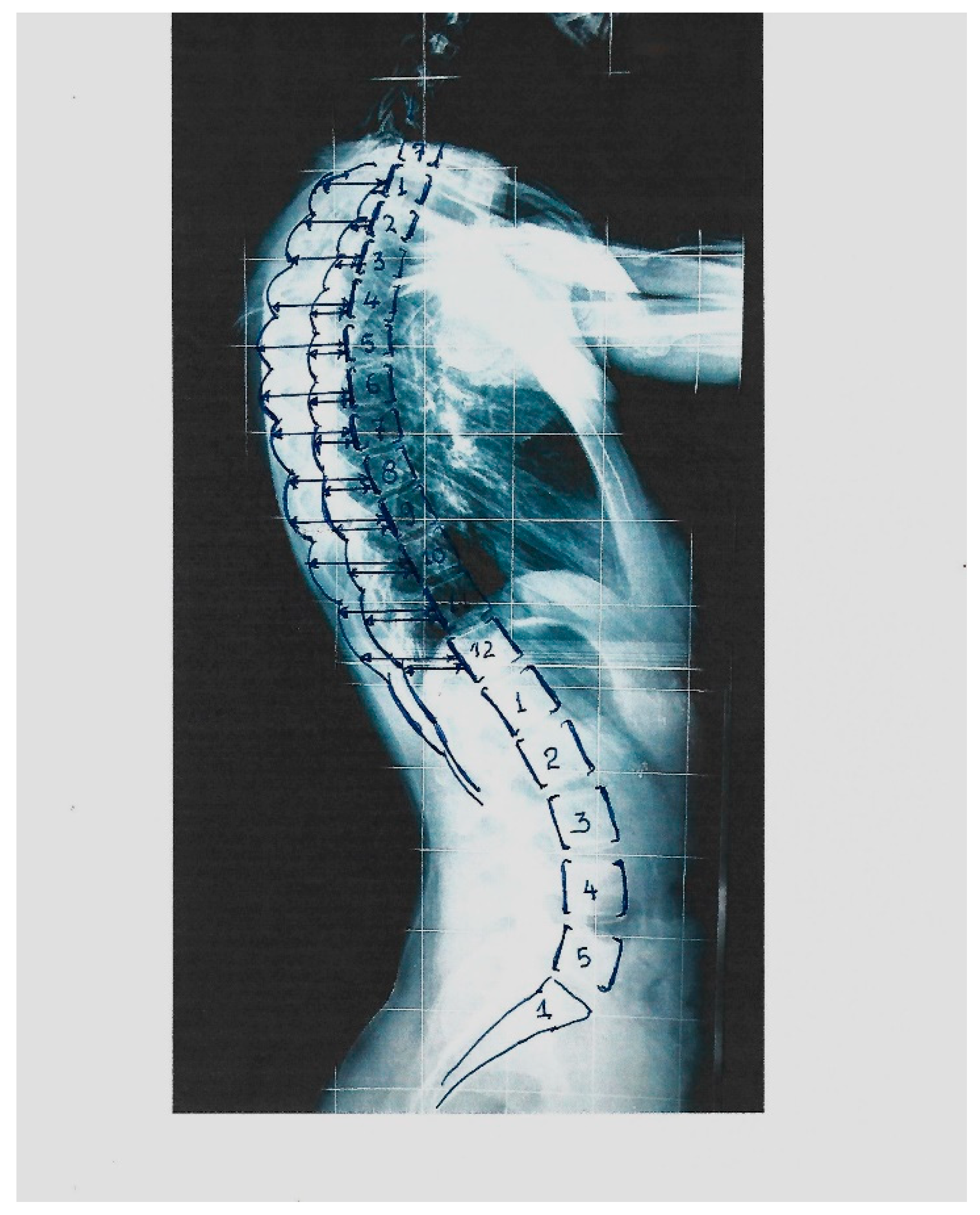
The measurements. The Cobb angle was assessed according to the classical method described by Cobb 1948, [11]. Scoliosis is considered if the Cobb angle is ≥ 10°, according to SRS. The segmental rib index was measured as follows: Initially, for the determination of the DRC and the calculation of the RI we determine in the LSRs: a) at the most extending rib contour (convex) the most extended rib point, which is the contact point of a vertical line tangential to this most extended point and we draw this vertical line passing from this point. b) at the least extending rib contour (concave) we determine the most projected rib point which is the contact point of a vertical line tangential to this most extended point and we draw this vertical line passing from this point. We determine the posterior margin line of the body of the corresponding vertebra of these two previous noted points and we measure their distances from the posterior margin line of the corresponding vertebra. These two distances are named d1 and d2. The quotient of d1/d2 is the rib index for the vertebral level of the corresponding vertebra, see Figure 1, [4]. The RΙ is likewise assessed in all the above and below vertebral levels of the initial RI measurement. Thus, the segmental RIs from T1-T12 are calculated, Figure 2.
Figure 1.
The way the RI is assessed on the standing lateral spinal radiographs, (from Grivas 2014, [4]).
Figure 1.
The way the RI is assessed on the standing lateral spinal radiographs, (from Grivas 2014, [4]).
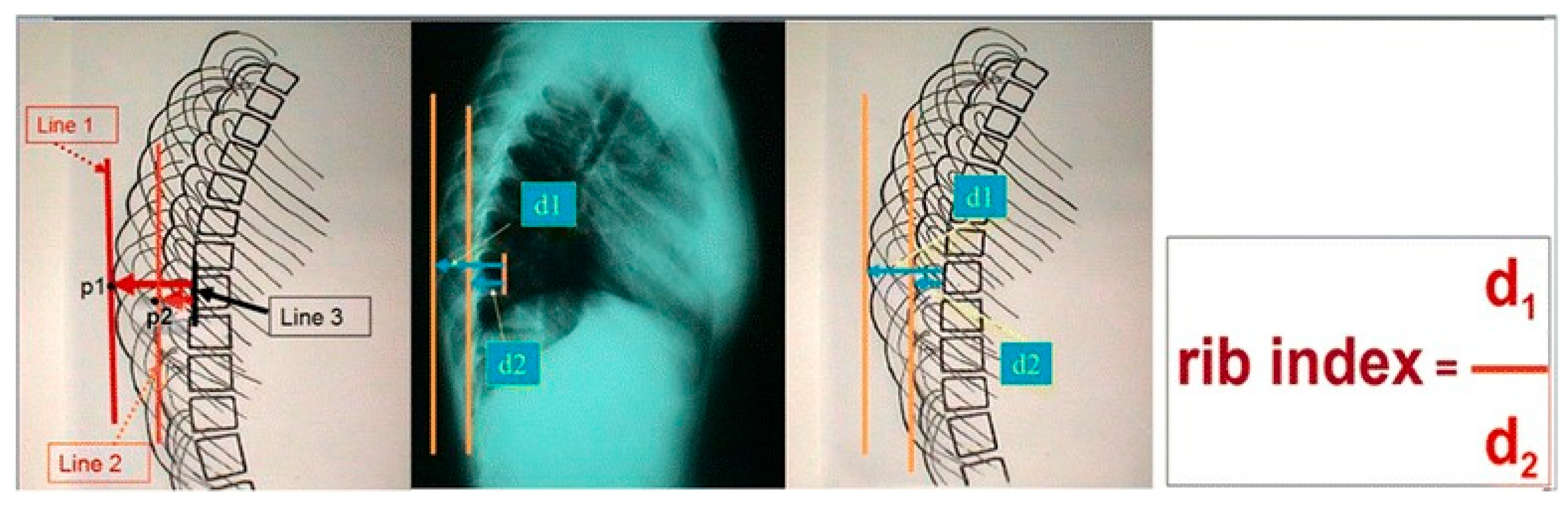
Figure 2.
The way the segmental RI (SRI) is assessed on the standing lateral spinal radiographs.
Truncal asymmetry (TA) assessment. The RHD was measured using the scoliometer. We previously reported the reliability study for the rib index method [4] and for the scoliometer readings [12].
The measurements for the segmental rib index were done by one of the co-authors, (DL), while the scoliometric measurements were done by TBG, SP, and NJ.
Statistical analysis. The statistical analysis was performed using the SPSS 23.0 (SPSS Inc., Chicago, IL). The results were presented as frequency (percent), mean and standard deviation (SD), median and interquartile range (IQR). Kruskal-Wallis test and t-test were used to compare the groups. Mann-Whitney test was used as a post hoc test, if there were significant differences between groups. Bonferroni correction was used to adjust the p-value for multiple comparisons between sub-groups. Pearson correlation coefficient was used to measure the strength of the relationship between Cobb angle and rib index in the sample, the groups by curve type, by sex and by age. All p values less than 0.05 were considered significant.
3. Results
The mean age and the Risser stage in the 83 included patients in the study scoliotics are presented in Table 1.
The Cobb angle by gender and curve type at the 83 scoliotic patients of the study is presented in Table 1 and Table 2. It is evident that the IS mild or moderate, and the sample suitable to draw conclusions on the developing deformity.
The basic characteristics for the 83 studied subjects, total and by gender are shown in Table 1. The average age is similar in both groups by gender. Risser stage was significantly higher in the Female group. A slightly higher Cobb angle and ATR were found in Female group, but without statistical significance.

Table 1.
Basic characteristics of patients.
| Total | Female | Male | p value | |
| N | 83 | 63 (75,9%) | 20 (24.1%) | |
| Age (years) | 12.3 ± 2.7 | 12.5 ± 2.5 | 11.5 ± 3.5 | 0.241a |
| Risser stage | 2 (4) | 2 (4) | 0 (2.8) | 0.023b |
| Cobb angle | 26.3±10.8 | 27.7±11.2 | 22.7±7.8 | 0.068a |
| ATR | 7.6±4.3 | 8.0±4.4 | 7.3±4.6 | 0.514a |
Results are shown as frequency (%), mean ± standard deviation, or median (IQR).a T test b Mann-Whitney test
The Cobb angle by gender and curve type at the 83 scoliotic patients of the study is presented in Table 2.
Table 2.
Cobb angle by curve type and sex .
| Gender | Curve type | n | Mean ± SD |
| Male | Thoracic | 6 (7.2%) | 25.4 ± 8.1 |
| Thoracolumbar | 6 (7.2%) | 22.0 ± 10.4 | |
| Lumbar | 8 (9.6%) | 21.1 ± 5.6 | |
| Female | Thoracic | 19 (22.9%) | 29.0 ± 12.2 |
| Thoracolumbar | 26 (31.3%) | 27.7 ± 9.8 | |
| Lumbar | 18 (21.7%) | 26.2 ± 12.5 |
Results are shown as n (%) and mean ± standard deviation.
The truncal asymmetry (TA): The mean of scoliometer readings was 7.7 ± 4.5 degrees (range: 2 to 13).
Segmental Rib Index and surface deformity (RHD) correlations.
In all 83 cases with IS, the measured Cobb angle was significantly correlated to the RI at the T6, T7 and T8 levels, Table 3.
Table 3.
Segmental Rib Index and surface deformity (RHD) correlations in all the cases.
| n=83 | Pearson correlation | p value |
|---|---|---|
| T6 | 0.292 | 0.007* |
| T7 | 0.220 | 0.046* |
| T8 | 0.240 | 0.029* |
* correlation is statistically significant at the 0.05 level (2-tailed.
In the 25 thoracic IS curves in both genders the Pearson Correlation coefficient was significant for the T6-T12 levels, yet it wasn’t significant at any level of the thoracolumbar and lumbar curves.
Table 4.
Segmental Rib Index and surface deformity (RHD) correlations at the 25 scoliosis patients with a thoracic curve.
Table 4.
Segmental Rib Index and surface deformity (RHD) correlations at the 25 scoliosis patients with a thoracic curve.
| n=25 | Pearson correlation | p value |
|---|---|---|
| T6 | 0.432 | 0.031* |
| T7 | 0.419 | 0.037* |
| T8 | 0.520 | 0.008* |
| T9 | 0.424 | 0.034* |
| T10 | 0.491 | 0.013* |
| T11 | 0.556 | 0.004* |
| T12 | 0.485 | 0.014* |
* correlation is statistically significant at the 0.05 level (2-tailed).
Segmental Rib Index and Cobb angle correlations
The segmental rib index by curve type and gender among all the three curve types - thoracic, thoracolumbar, and lumbar - at girls and boys together, Table 5 and Table 6. No significant correlation was found among the three groups.
The same analysis at females showed significant differences only between groups at T8, T9 and T12 vertebral level. The post hoc analysis showed significant differences between thoracic and thoracolumbar curves at T9 and between thoracolumbar and lumbar curves at T12, Table 5. The same analysis at males showed no significant difference between groups, Table 6.
Table 5.
The segmental rib index by curve type among all three curve types - thoracic, thoracolumbar, and lumbar - at females.
Table 5.
The segmental rib index by curve type among all three curve types - thoracic, thoracolumbar, and lumbar - at females.
| Female |
Thoracic n=19 |
Thoracolumbar n=26 |
Lumbar n=18 |
p value |
| T1 | 1.30 (0.48) | 1.20 (0.43) | 1.15 (0.50) | 0.444a |
| T2 | 1.40 (0.54) | 1.67 (0.72) | 1.24 (0.71) | 0.310a |
| T3 | 1.51 (0.51) | 1.57 (0.59) | 1.38 (0.64) | 0.233a |
| T4 | 1.59 (0.58) | 1.57 (0.40) | 1.38 (0.51) | 0.201a |
| T5 | 1.67 (0.95) | 1.46 (0.35) | 1.45 (0.48) | 0.404a |
| T6 | 1.60 (0.60) | 1.42 (0.40) | 1.40 (0.42) | 0.322a |
| T7 | 1.54 (0.51) | 1.40 (0.29) | 1.39 (0.47) | 0.133a |
| T8 | 1.60 (0.50) | 1.39 (0.30) | 1.34 (0.45) | 0.054a |
| T9 | 1.73 (0.52)TL | 1.38 (0.33) | 1.42 (0.41) | 0.018a |
| T10 | 1.75 (0.57) | 1.42 (0.55) | 1.20 (0.66) | 0.052a |
| T11 | 1.43 (0.70) | 1.49 (0.50) | 1.20 (0.54) | 0.091a |
| T12 | 1.22 (0.67) | 1.41 (0.50)L | 1.11 (0.32) | 0.021a |
Results are presented as median (IQR) a Kruskal-Wallis test, post hoc Mann-Whitney U test TL – Significant difference between examined group and Thoracolumbar group L – Significant difference between examined group and Lumbar group * correlation is statistically significant at the 0.05 level (2-tailed).
| female | Thoracic vs thoracolumbar |
Thoracic vs lumbar |
Thoracolumbar vs lumbar | |
| T9 | 0.011* | - | - | |
| T12 | - | - | 0.005* |
* p value is statistically significant with Bonferroni correction at the 0.017
Table 6.
The segmental rib index by curve type among all three curve types - thoracic, thoracolumbar, and lumbar - at males.
Table 6.
The segmental rib index by curve type among all three curve types - thoracic, thoracolumbar, and lumbar - at males.
| Male | Thoracic (n=6) |
TL (n=6) |
Lumbar (n=8) |
p value |
|---|---|---|---|---|
| T1 | 1.11 (0.20) | 1.18 (0.39) | 1.21 (0.49) | 0.487a |
| T2 | 1.13 (0.51) | 1.29 (0.42) | 1.32 (0.63) | 0.768a |
| T3 | 1.26 (0.58) | 1.52 (1.17) | 1.36 (0.47) | 0.691a |
| T4 | 1.26 (0.66) | 1.50 (1.13) | 1.44 (0.51) | 0.372a |
| T5 | 1.22 (0.88) | 1.50 (1.02) | 1.36 (0.62) | 0.215a |
| T6 | 1.52 (0.59) | 1.39 (0.88) | 1.26 (0.58) | 0.352a |
| T7 | 1.43 (0.35) | 1.58 (0.82) | 1.32 (0.60) | 0.331a |
| T8 | 1.47 (0.28) | 1.61 (1.01) | 1.39 (0.66) | 0.411a |
| T9 | 1.50 (0.17) | 1.61 (0.97) | 1.40 (0.59) | 0.371a |
| T10 | 1.53 (0.41) | 1.70 (0.95) | 1.41 (0.34) | 0.300a |
| T11 | 1.43 (0.66) | 1.59 (0.54) | 1.29 (0.33) | 0.219a |
| T12 | 1.19 (0.38) | 1.63 (0.90) | 1.38 (0.43) | 0.274a |
Results are presented as median [The interquartile range (IQR)]. a Kruskal-Wallis test. * correlation is statistically significant at the 0.05 level (2-tailed).
In order to investigate further the effect of growth on the relationship of RC with the spinal deformity in terms of the Cobb angle, we analyzed the segmentally measured RI from T1-T12. For this purpose, the studied scoliotics were split into two age cohorts, namely a) scoliotics less than 13 and over 13 years of age, and b) scoliotics less than 14 and over 14 years of age. It was thus possible to recognize accurately the cut-off age of the examined scoliotics at which the segmental RI starts correlating or shows stronger correlation to the spinal deformity, specifically when the thoracic deformity starts to dictate the development of spinal deformity, in terms of Cobb angle.
The comparison analysis of the segmental RI for girls only in all types of curves in the 4 age groups showed the following results:
In both cohorts of these age groups together, using the Kruskal Wallis test, a significant difference is observed only at the older girls over 13 years of age at T10 level (p=0.007), and at the group over 14-years (p=0.006).
Comparing the segmental RI index to the Cobb angle by type of curve at all ages for boys and girls, the Pearson Correlation coefficient was significant at T10-T12 for thoracic, T4 for thoracolumbar and T9 for the lumbar curves, see Table 7.
Splitting the ages of the scoliotics in two groups, namely younger and older and using the Pearson correlation coefficient to compare the RI index to Cobb angle by curve type at younger and older boys and girls, it was found that:
Comparing the segmental RI index to the Cobb angle by type of curve at boys and girls less than 13 years of age, the Pearson Correlation coefficient was significant at T4 for thoracolumbar and T1-T2 for the lumbar curves.
Comparing the segmental RI index to the Cobb angle by type of curve at boys and girls over 13-year of age, the Pearson Correlation coefficient was significant at T11-T12 for thoracic, T6-T9 for thoracolumbar and T8, T9 and T11 for the lumbar curves.
Comparing the segmental RI index to the Cobb angle by type of curve at boys and girls less than 14 years of age, the Pearson Correlation coefficient was significant at T4 for thoracolumbar and T8 for the lumbar curves.
Comparing the segmental RI index to the Cobb angle by type of curve at boys and girls over 14-year of age, the Pearson Correlation coefficient was significant at T8-T11 for thoracic and T1 for thoracolumbar curves, (see Table 7).
Comparing the segmental RI index of the asymmetric but not scoliotic children to the scoliotic peers by curve type at boys and girls, interestingly no significant difference between groups (non-scoliotic – thoracic, non-scoliotic – thoracolumbar, non-scoliotic – lumbar) was found.
Table 7.
Comparison of the segmental RI index to the Cobb angle at all ages of boys and girls.
| All patients | Age<13 | Age>13 | Age<14 | Age>14 | |
| r (p value) | r (p value) | r (p value) | r (p value) | r (p value) | |
| Thoracic curve | n=25 | n=13 | n=12 | n=14 | n=11 |
| T8 | - | - | - | - | 0.703 (0.016) |
| T9 | - | - | - | - | 0.679 (0.022) |
| T10 | 0.462 (0.020) | - | - | - | 0.703 (0.016) |
| T11 | 0.465 (0.019) | - | 0.587 (0.045) | - | 0.745 (0.009) |
| T12 | 0.547 (0.005) | - | 0.591 (0.043) | - | - |
| Thoracolumbar curve | n=32 | n=15 | n=17 | n=19 | n=10 |
| T1 | - | - | - | - | 0.642 (0.046) |
| T4 | -0.388 (0.031) | -0.571 (0.026) | - | -0.623 (0.004) | - |
| T6 | - | - | -0.503 (0.039) | - | - |
| T7 | - | - | -0.527 (0.030) | - | - |
| T8 | - | - | -0.582 (0.014) | - | - |
| T9 | - | - | -0.561 (0.019) | - | - |
| Lumbar curve | n=26 | n=10 | n=16 | n=10 | n=16 |
| T1 | - | -0.835 (0.010) | - | - | - |
| T2 | - | -0.938 (0.001) | - | - | - |
| T8 | - | - | 0.527 (0.036) | 0.613 (0.020) | - |
| T9 | 0.394 (0.046) | - | 0.662 (0.005) | - | - |
| T11 | - | - | 0.507 (0.045) | - | - |
Results are presented as Pearson correlation coefficient = r (p value) * correlation is statistically significant at the 0.05 level (2-tailed).
4. Discussion and conclusions
To our best knowledge (reviewing the literature), the segmental RI is presented for the first time in a sample of thoracic, thoracolumbar and lumbar mild and moderate IS patients, Table 4 and Table 5.
No full agreement exists on the definition of mild and moderate idiopathic scoliosis. Mild idiopathic scoliosis is characterized in different reports by a Cobb angle of more than 10 and less than 30 degrees, [13], of more than 10 to 25 degrees, [14], and of more than 10 to 20 degrees, [15]. Moderate IS is characterized by a Cobb angle of 25 to 40 degrees, which is indicated for non-operative treatment, [16,17], and a Cobb from 21 to 35 degrees, [15]. We consider as mild curves those with a Cobb angle from 10 but less than 20 degrees and as moderate those with a Cobb angle from 20 to 35–40 degrees. In these curves, especially in the mild ones, the rotation of the apical vertebrae is only a few degrees, [18]. This morphology is very important for the measurements in the frontal and sagittal plane which is minimally affected. This fact results in more reliable contacted measurements, and it is very important for our study.
The degrees of Cobb angle presented in Table 1 and Table 2, by gender and curve type at the 83 scoliotics of this study showed that the sample is suitable to enable us to draw conclusions on mild and moderate IS.
The segmental RI (a radiological measurement in the sagittal plane) and the RHD in terms of the measured ATR, (a scoliometry/surface topography measurement) at all 83 cases with IS were significantly correlated to the segmental RI at only three levels, namely T6, T7 and T8, presented in Table 3. However, at the 25 scoliotics with a thoracic curve the significance of the correlation was not only stronger but it was also found at seven vertebral levels, namely T6, T7, T8, T9, T10, T11 and T12, presented in Table 4. For the thoracolumbar and lumbar curves this correlation wasn’t significant at any level. This implies the leading role of the RC especially for the development of the thoracic spinal deformity.
In mild and moderate IS curves, the vertebral rotation is minimal. Thus the rib cage deformity can be generally attributed to the asymmetric rib growth and to their deformation and not to the vertebral rotation, as the rotation at this stage is minimal. Therefore, at any level from T1-T12 a value of segmental RI equal or more than 1,45 - 1,50 mainly reflects a significantly asymmetrical DRC, a fact indicating a remarkable asymmetrical growth of pair of ribs on this spinal level. Therefore, this value of RI represents an increasing and progressive rib cage deformity.
The term “pattern of segmental RI asymmetry” is used to indicate the number of rib levels, from T1-T12, with the above coined severe asymmetry, namely equal or more than 1.45 – 1.50.
The comparison of the three types of curve groups in females, using the Kruskal-Wallis test, showed significant differences between groups at T8, T9 and T12 vertebral level. The post hoc analysis showed significant differences between thoracic and lumbar curves at T8, between thoracic and thoracolumbar curves at T9 and between thoracolumbar and lumbar curves at T12, presented in Table 5.
In females with thoracic curves, presented in Table 5, the pattern of segmental RI asymmetry is present in 8 levels from T3-T10 (RI=1.59-1.75), in thoracolumbar curves the pattern of segmental RI asymmetry is present in 4 levels from T2-T5 (RI= 1.46-1.67), while in lumbar curves the RI does not exceed the value of 1.45 in all T1-T12 levels, Table 5.
In males with thoracic curves (Table 6) the pattern of segmental RI asymmetry is present in 6 levels from T6 -T11 (RI=1.51-1.75), i.e. in lower thoracic levels compared to the female pattern of RI asymmetry in thoracic curves. The pattern of segmental RI asymmetry with thoracolumbar curves is present totally in 9 levels from T3-T5 (1.50-1.52) and T7-T12 (1.58-1.70), i.e. in a much lower and more extended number of rib-pair levels compared to the RI pattern levels of asymmetry in females. In lumbar curves the RI in males does not exceed the value of 1.44. These finding validate the role of rib cage deformity for the development of idiopathic scoliosis.
In males, the comparison of the RI at the three curve type groups, using the Kruskal-Wallis test, showed no significant difference between them, Table 6.
The lumbar curves both in females and males are minimally or not at all influenced by the RC deformity, but in contrast the RC deformity has a great impact on the development of the thoracic curves in females and inexpectantly on the thoracolumbar curves in males.
The further analysis of the segmental RI and Cobb angle correlations showed the following interesting findings:
The segmental RI by curve type and gender among all the three curve types - thoracic, thoracolumbar, and lumbar - in girls and boys together, using the non-parametric test of Kruskal-Wallis test [results are presented as median (IQR)], showed no significant differences, [the correlation is significant at the 0.05 level (2-tailed)], among the three groups.
The same analysis at scoliotic females only, [using the Kruskal-Wallis test, post hoc Mann-Whitney U test], showed significant differences between groups at T8, T9 and T12 vertebral levels. The post hoc analysis showed significant differences between thoracic and thoracolumbar at T9 and at T12 between thoracolumbar and lumbar at T12, Table 3.
The same analysis at scoliotic males only showed no significant differences between groups, Table 5.
These findings are emphasizing the importance of the role of the RC asymmetry in relation to the spinal deformity mainly in the girls.
Published articles of previous decades sporadically reported that children could have surface deformity in terms of RHD without deformity in their spine, [19,20]. Nissinen et al 1989, [21,22], stated that “hump size was found to be the most powerful predictor of scoliosis. Large humps were more prevalent among non-scoliotic children that subsequently developed IS. Additionally, Nissinen et al 1993, [21,22], stated that the asymmetric children with a hump deformity but without radiographical diagnosed scoliosis, during FU will develop IS with an odds ratio 1.72 in boys and 1.55 in girls.
The effect of growth was found to play a key role to the correlation between the thoracic and the spinal deformity in girls with IS, [2]. Younger girls may be asymmetric in terms of the RHD without having a spinal deformity, (scoliosis). In older girls a statistical significant correlation of thoracic and spinal deformity does exist, but this is not the case in younger girls. These findings implicate the important role of the RC in IS, because they show that RHD deformity precedes the spinal one in scoliogenesis of mild and moderate IS. This correlation was demonstrated studying the RI at the most extended point of the most extending rib contour (convex) at the SLRs, [4]. This finding inspired us to further investigate the role of RI at all rib-vertebral levels, that is to assess the RI segmentally from T1-T12 in RC, and to examine the relation that these segmental RIs may have to the scoliogenesis of IS.
The findings of this study are in line with those reported by prof. Sevastik research work pertinent to scoliosis aetiology, emphasizing the important role of rib cage on scoliosis development. Therefore, the benefit of this study is that its findings shed more light to the theory of asymmetric function of the ANS, reported by prof. Sevastik and his team, [23,24,25,26,27,28,29,30,31,32,33,34,35], and they also support the physiological approach to the surgical treatment of progressive early IS, [36].
Investigating further the effect of growth on the relationship of RC with the spinal deformity in terms of the Cobb angle, we analyzed the segmentally measured RI from T1-T12. For this purpose, the scoliotics were split into two age cohorts, namely a) scoliotics less than 13 and more than 13 years of age, and b) scoliotics less than 14 and more than 14 years of age, presented in Table 7. It was thus feasible to recognize accurately the cut-off age (of the examined scoliotics) at which the segmental RI starts correlating or shows stronger correlation to the spinal deformity, namely when the thoracic deformity starts to dictate the development of spinal deformity, in terms of Cobb angle.
Before any splitting of the ages, the significant correlation of Cobb angle with the segmental RI (Table 7) exists in thoracic curves at T10,11,12 (p = 0.462, 0.465, 0.547) respectively, in thoracolumbar curves it correlates negatively at T4 only, (p = 0,031) and in lumbar curves at T9 only (p = 0.046), Table 7.
After splitting the scoliotic boys and girls in two cohorts by age, namely over and less than 13 years, it was found that, Table 7:
In scoliotics with thoracic curves over 13-years of age the Pearson Correlation coefficient was significant at T11 and T12 (p = 0.045, 0.043),
In scoliotics with thoracic curves less than 13-years of age the Pearson Correlation coefficient was not significant.
In scoliotics with thoracolumbar curve less than 13 years of age the correlation was significant at T4 (p = 0.026), over 13-years of age at T6-9, (p = 0.039, 0.030, 0.014, 0.019) respectively, and
In scoliotics with lumbar curve less than 13 years of age at T1 and T2, (p = 0.010 and 0,001), and over 13-years of age at T8, 9, and T11 (p = 0.036, 0.005, 0.045), respectively.
Similarly splitting the ages of scoliotics at over and less than 14 years of age it was found that, Table 7:
In thoracic curves over 14-years of age the Pearson Correlation coefficient was significant at T8-11, (p = 0.016, 0.022, 0.016, 0.009),
In thoracolumbar curves at less than 14 years of age at T4, Pearson Corr. Coeff. was negatively correlated (p = 0.004) and over 14-years of age at T1 (p = 0.046), respectively.
Finally, in lumbar curves at less than 14 years of age, at T8 (p = 0.020).
From this analysis it is evident that the cut-off point of ages of the examined scoliotics is this of 14 years, when the segmental RI shows stronger correlation to the spinal deformity, namely when the thoracic deformity correlates to the developing thoracic spinal deformity, in terms of Cobb angle. This is in accordance with what was earlier found, [26].
The RC asymmetry described in this study of segmental RI is also in accordance with the Nottingham concept of IS pathogenesis. The RC deformity is mainly due to the asymmetric rib growth and its deformation affects the rotation defending system of the thorax of the “flag pole dinner plate” concept of this theory, leading to scoliosis, [37].
The results of the comparison of the segmental RI of the asymmetric but non scoliotic children to the RI of scoliotics by curve (thoracic, thoracolumbar, lumbar) in boys and girls, interestingly showed that there is no significant difference between groups (non scoliotic – thoracic, non scoliotic – thoracolumbar, non scoliotic – lumbar). However, considering the fact that a good number of these asymmetric referred children will develop IS, [21,22], our recommendation is not to discharge them from the scoliosis outpatient department but to follow them up for a longer period of time. This recommendation is also one of the benefits of this segmental rib index study.
A limitation of this report is the small number of the curve types of the studied scoliotic children and adolescents. Yet, the results of the analysis are in line with those of a previous publication, see [2], where the included female sample was larger. Additionally, the results are based on a two dimensional radiography. Currently three-dimensional analysis is more frequently used as a procedure to study the morphology of scoliotic curvatures, [38,39,40,41,42], because any study based exclusively on coronal or sagittal plane has its limitations. However, the most important and frequently used radiological parameters are designed and measured on A-P and lateral radiographs (i.e. Cobb, Mehta RVAs, Perdriolle angles).
The benefits of using the RI and segmental RI method are described above. RI can also be used as a surrogate for scoliometry, [7]. RI is a radiographic measurement of asymmetry in the standing position, while the scoliometer measures clinically truncal asymmetry in flexion. It was found that a change from a flexed position to a standing position resulted in a reduction in trunk asymmetry [43]. If patients had RI asymmetry measured on their standing radiographs, the flexion scoliometry reading would have been greater. Therefore, segmental RI can safely be used as a strong substitute for scoliometric measurement and can estimate the severity of thoracic deformity, [43].
One other benefit of using the RI and segmental RI is that the plain chest radiographs of children and adolescents, being easily available at medical archives, can effectively serve the segmental RI method, without the need for any other special radiographs and exposure to additional radiation. One additional benefit of segmental RI method is its implementation not only in prospective but also in retrospective studies on non-operative and operative treatment of IS, using the existing initially obtained chest or spinal radiographs of IS patients, provided that the radiography is performed in a standard way.
The operation named costoplasty or thoracolpasty or pleuroplasty is the one that has been introduced to correct the deformity of the ribs in the chest, of the AIS patients, [44,45,46,47]. In operable cases of IS with excessive hump, in addition to spinal surgery, costoplasty is sometimes performed. The results of costoplasty are not always satisfactory, as it is mentioned in the literature, [48] because in some patients there is a persistent or remaining rib deformity. As a result, the patients and family are not satisfied with the operation. The explanation of this phenomenon is provided by Erkula et al 2003. As ribs slope obliquely downwards, it is difficult to predict which vertebral levels one is making measurements for. This anatomy makes the exact levels of the maximum rib deformity in patients with a severe hump hard to recognize the corresponding vertebral level. They recommend to perform a scanogram or a 3D reconstruction of the spine and ribs which will help to define the exact level of the rib deformity that corresponds to a certain vertebral level, [48]. Their findings are very much in line with what it was trigger us to introduce the segments RI method. The maximum segmental RI value in the above described pattern of increased RI values, see Table 5 and Table 6, could replace the scanogram or the 3D reconstruction and help the recognition of the exact level or levels of the rib deformity/ies that correspond to the certain vertebral level which must be costoplasted. Thus the patients have less exposure to radiation, and this is considered one important benefit of using the new segmental RI method, [43].
In conclusion, this is the first report presenting the segmental rib index according to the location of the curves - in the thoracic, thoracolumbar and lumbar IS. Additionally, the above study presented results from data collected retrospectively from scoliotics, suffering mild and moderate IS. The reported correlations of the surface deformity, in terms of scoliometry, and radiological deformity, in terms of radiography, of the scoliotics in this report show the significant impact of the RC on spine. RC seems to plays a protagonistic role in the scoliogeny of IS in mild and moderate thoracic and thoracolumbar IS.
Author Contributions
Conceptualization: TBG; Data curation: TBG, SP, DL, Statistical analysis: FC, Literature Investigation: TBG, EV; Project administration: TBG, SP, NJ; Writing—original draft: TBG; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
N/A, this study is a statistical retrospective study
Informed Consent Statement
N/A, this study is a statistical retrospective study
Data Availability Statement
Data are available on demand.
Conflicts of Interest
The authors declare that they have no conflict of interest concerning this article.
Abbreviations
AIS = Adolescent Idiopathic Scoliosis
ANS =Autonomic Nerve System
ATR = Angle of Trunk Rotation
ATI = Angle of Trunk Inclination
CNS = Central Nervous System
DRCI = Double Rib Contour Sign
EOS = Early Onset Scoliosis (EOS)
IS = Idiopathic Scoliosis
LSP = Lateral Spinal Profile
LSR = lateral standing radiographs
RC = Rib Cage
RH = Rib Hump
RHD = Rib Hump Deformity
RI = Rib Index
RVA = Rib Vertebra Angle
SRI = Segmental Rib Index
SSS = School Scoliosis Screening
TA = Truncal Asymmetry
References
- Nissinen M, Heliovaara M, Tallroth K, Poussa M. Trunk asymmetry and scoliosis. Anthropometric measurements in prepubertal school children. Acta Paediatr Scand. 1989, 78, 747–753. [Google Scholar] [CrossRef] [PubMed]
- Grivas, T.B. Thorax and the idiopathic Scoliosis. Int. J. Adv. Res. 2023, 11, 1252–1290. [Google Scholar] [CrossRef] [PubMed]
- Labelle H, Richards SB, De Kleuver M, Grivas TB, Luk KD, Wong HK, Thometz J, Beauséjour M, Turgeon I, Fong DY. Screening for adolescent idiopathic scoliosis: an information statement by the scoliosis research society international task force. Scoliosis. 2013, 8:17. [CrossRef] [PubMed]
- Grivas TB. Rib index. Scoliosis. 2014, 9: 20. [CrossRef] [PubMed]
- Lebel, A., Lebel, V. Rib index, an objective measure to document changes of the rib hump deformity in a Risser 4 progressive AIS patient treated with the Schroth method. Scoliosis 9 (Suppl 1), O18, 2014. [CrossRef]
- Grivas TB. Radiological appraisal of thoracic deformity - improvement or deterioration using the convex/concave rib-hump index (‘double rib contour sign’) in curves Lenke Type 1, 3, 5 and 6. In book: Scoliosis Research Society. Half-Day Courses, Chapter: Radiological appraisal of thoracic deformity - improvement or deterioration using the convex/concave rib-hump index (‘double rib contour sign’) in curves Lenke Type 1, 3, 5 and 6., Publisher: Scoliosis Research Society, Editors: SRS 2012-2013 Education Committee, 2013, 29-30.
- Haber LL, Adams TM, Briski DC, Celestre PC, Robbins DJ, Waldron SR. Long-term Results of Spine Stapling for AIS to Skeletal Maturity and Beyond J Pediatr Orthop. 2020, 40(1): e37-e41. [CrossRef] [PubMed]
- Tsirikos AI and McMillan TE. All Pedicle Screw versus Hybrid Hook–Screw Instrumentation in the Treatment of Thoracic Adolescent Idiopathic Scoliosis (AIS): A Prospective Comparative Cohort Study Healthcare 2022, 10, 1455. [CrossRef]
- Sevastik J., Burwell R. G., Dangerfield P. H. A new concept for the etiopathogenesis of the thoracospinal deformity of idiopathic scoliosis: summary of an electronic focus group debate of the IBSE. Eur Spine J (2003) 12: 440–450. [CrossRef]
- Burwell RG, Dangerfield PH, Moulton A, Grivas TB, Cheng JC. Whither the etiopathogenesis (and scoliogeny) of adolescent idiopathic scoliosis? Incorporating presentations on scoliogeny at the 2012 IRSSD and SRS meetings. Scoliosis. 2013 Feb 28;8(1) :4. [CrossRef]
- Cobb, J. Outline for the study of scoliosis. Instr Course Lect. 1948, 5, 261–275. [Google Scholar]
- Grivas TB, Vasiliadis ES, Kouropoulos G, Segos D, Triantafyllopoulos G, Mouzakis V. 2006. Study of trunk asymmetry in normal children and adolescents. Scoliosis. 2006, 1:19. [CrossRef]
- Cheung M-C, Yip J, Lai JSK. Biofeedback Posture Training for Adolescents with Mild Scoliosis. BioMed Res. Int. 2022, 2022, 1–8. [Google Scholar]
- Monticone M, Ambrosini E, Cazzaniga D, Rocca B, Ferrante S. Active self-correction and task-oriented exercises reduce spinal deformity and improve quality of life in subjects with mild adolescent idiopathic scoliosis. Results of a randomized controlled trial. Eur. Spine J. 2014, 23, 1204–1214. [Google Scholar] [CrossRef] [PubMed]
- Negrini S, Donzelli S, Aulisa AG, Czaprowski D, Schreiber S, De Mauroy JC, Diers H, Grivas TB, Knott P, Kotwicki T, et al. 2016 SOSORT guidelines: Orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis Spinal Disord. 2018, 13, 3. [Google Scholar] [CrossRef] [PubMed]
- Weinstein SL, Dolan LA, Wright JG, Dobbs MB. Effects of bracing in adolescents with idiopathic. N. Engl. J. Med. 2013, 369, 1512–1521. [Google Scholar] [CrossRef] [PubMed]
- Kuznia AL, Hernandez AK. Lee LU. Adolescent Idiopathic Scoliosis: Common Questions and Answers. Am. Fam. Physician 2020, 101, 19–23. [Google Scholar]
- Courvoisier A, Drevelle X, Dubousset J, Skalli W. Transverse plane 3D analysis of mild scoliosis. Eur. Spine J. 2013, 22, 2427–243. [Google Scholar] [CrossRef]
- Pruijs JE, W Keessen, R van der Meer, J C van Wieringen, M A Hageman. School screening for scoliosis: methodologic considerations. Part 1: External measurements Spine. 1992, 17, 431–436. [Google Scholar]
- Pruijs JE, W Keessen, R van der Meer, J C van Wieringen. School screening for scoliosis: the value of quantitative measurement. Eur Spine J. 1995. 4(4):226-30. [CrossRef]
- Nissinen M, Heliovaara M, Tallroth K, Poussa M. Trunk asymmetry and scoliosis. Anthropometric measurements in prepubertal school children. Acta Paediatr Scand 1989, 78, 747–753. [Google Scholar] [CrossRef] [PubMed]
- Nissinen M, Heliovaara M, Seltsamo J, Poussa M. Trunk Asymmetry, Posture, Growth, and Risk of Scoliosis. A Three-Year Follow-Up of Finnish Prepubertal School Children. Spine 1993, 18, 1, 99. [Google Scholar]
- Sevastik JA, Aaro S, Normelli H. Scoliosis. Experimental and clinical studies. Clin Orthop Relat Res. 1984, 191, 27–34. [Google Scholar]
- Normelli H, Sevastik J, Wallberg H. The thermal emission from the skin and the vascularity of the breasts in normal and scoliotic girls. Spine 1986, 11(5):405-8. [CrossRef]
- Sevastik JA, Aaro S, Lindholm ST, Dalhborn M. Experimental scoliosis in growing rabbits by operations on the rib cage. Clinical Orthopaedics. 1987, 136, 282–86. [Google Scholar]
- Agadir M, Sevastik B, Sevastik JA, Persson A, Isberg B. Induction of scoliosis in the growing rabbit by unilateral rib-growth stimulation. Spine. 1988, 13, 1065–1069. [Google Scholar] [CrossRef]
- Normelli H, Sevastik JA, Ljung, G, Jönsson-Söderström AM. The symmetry of the breasts in normal and scoliotic girls. Spine (Phila Pa 1976). 1986, 11(7):749-52. [CrossRef]
- Sevastik J, Agadir M, Sevastik B 1990. Effects of rib elongation on the spine: I. Distortion of the vertebral alignment in the rabbit. Spine. 1990, 15: 822-825. [CrossRef]
- Sevastik J, Agadir M, Sevastik B. 1990. Effects of rib elongation on the spine: II. Correction of scoliosis in the rabbit. Spine. 1990, 15: 826-829. [CrossRef] [PubMed]
- Agadir M, Sevastik B, Reinholt FP, Perbeck L, Sevastik J. Vascular Changes in the Chest Wall After Unilateral Resection of the Intercostal Nerves in the Growing Rabbit. Journal of Orthopaedic Research 1990, 8, 283–290. [Google Scholar] [CrossRef]
- Sevastik B, Xiong B, Lundberg A, Sevastik JA. In vitro opto-electronic analysis of 3-D segmental vertebral movements during gradual rib lengthening in the pig. Acta Orthop Belg. 1995, 61, 218–25 PMID: 8525819. [Google Scholar] [PubMed]
- Gréalou L, Aubin CE, Sevastik JA, Labelle H Simulations of rib cage surgery for the management of scoliotic deformities. Stud Health Technol Inform. 2002, 88, 345–9 PMID: 15456059. [PubMed]
- Sevastik JA Dysfunction of the autonomic nerve system (ANS) in the aetiopathogenesis of adolescent idiopathic scoliosis. Stud Health Technol Inform. 2002, 88, 20–3 PMID: 15455999. [PubMed]
- Sevastik JA, Burwell RG, Dangerfild PH. A new concept for the etiopathogenesis of the thoracospinal deformity of idiopathic scoliosis: summary of an electronic focus group debate of the IBSE. Eur Spine J. 2003. 12: 440–450. [CrossRef]
- Sevastik, JA. Right convex thoracic female adolescent scoliosis in the light of the thoracospinal concept. Stud Health Technol Inform. 2006, 123, 552–8 PMID: 17108486. [Google Scholar] [PubMed]
- Xiong B, Sevastik JA. A physiological approach to surgical treatment of progressive early idiopathic scoliosis. Eur Spine J. 1998, 7(6):505-8. [CrossRef] [PubMed]
- Βurwell RG, Cole AA, Cook TA, Grivas TB, Kiel AW, Moulton A, Thirlwall AS, Upadhyay SS, Webb JK, Wemyss-Holden SA, Whitwell DJ, Wojcik AS, Wythers DJ. 1991-1992. Pathogenesis of Idiopathic Scoliosis. The Nottingham Concept. Acta Orthop Belgica 1992, 58 Suppl. 1, 33–58.
- Dansereau J, Stokes IAF. Measurements of three-dimensional shape of the rib cage. J Biomech 1988, 21, 893–901. [Google Scholar] [CrossRef] [PubMed]
- Hierholzer E, Hackenberg L. Three-dimensional shape analysis of the scoliotic spine using MR tomography and rasterstereography. Stud Health Technol Inform. 2002, 91, 184–9, PMID: 15457720. [PubMed]
- Sangole AP, Aubin CE, Labelle H, Stokes IA, Lenke LG, Jackson R, Newton P. Three-dimensional classification of thoracic scoliotic curves. Spine 2009, 1;34(1):91-9. [CrossRef] [PubMed]
- Donzelli S, Poma S, Balzarini L, Borboni A, Respizzi S, Villafane JH, Zaina F, Negrini S. State of the art of current 3-D scoliosis classifications: a systematic review from a clinical perspective. J Neuroeng Rehabil. 2015, 16; 12:91. [CrossRef] [PubMed]
- Dansereau J, Stokes IAF, Moreland MS. Radiographic reconstruction of 3D human rib cage. In Surface Topography and Spinal Deformity Edited by: Stokes IAF, Pekelsky JR, Moreland MS. Stuttgart: Gustav Fischer 33, 67–76.
- Grivas, T.B.; Jevtic, N.; Ljubojevic, D.; Pjanic, P.; Golic, F.; Vasiliadis, E. Segmental Rib Index and Spinal Deformity: Aetiological Implications to Idiopathic Scoliosis. 2023. Međunarodni Kongres, se Održava na Zlatiboru u Kongresnom Centru “Hotel Mona” od 21–24 Septembra 2023, Godine Pod Nazivom: “Nove Perspektive u Razvoju Fizikalne i Rehabilitation Medicine”. Available online: https://fizijatri.org/ (accessed on 10 September 2023).
- Barrett DS, MacLean JGB, Bettany J, Ransford AO, Edgar MA. Costoplasty in adolescent idiopathic scoliosis. Objective results in 55 patients. J Bone Joint Surg Br, 1993, 75, 881–885.
- Harvey Jr. CJ, Betz RR, Clements DH, Huss GK, Clancy M. Are there indications for partial rib resection in patients with adolescent idiopathic scoliosis treated with Cotrel-Dubousset instrumentation? Spine 1593, 18, 1593–1598.
- Shufflebarger HL, Smiley K, Roth HJ. Internal thoracoplasties. A new procedure. Spine 1994, 19, 840–842. [Google Scholar]
- Steel, HH. Rib resection and spine fusion in correction of convex deformity in scoliosis. J Bone Joint Surg Am. 1983, 65, 920–92. [Google Scholar] [CrossRef]
- Erkula G, Sponseller PD, Kiter AE. Rib deformity in scoliosis. Eur Spine J. 2003, 12(3):281-7. [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



