
Submitted:
23 October 2023
Posted:
25 October 2023
You are already at the latest version
Abstract
General anesthesia and surgical stress can suppress the immunological response by acting both directly on the immune system and indirectly on the hypothalamic-pituitary-adrenal axis and the sympathetic nervous system. Disturbance of the immune system during the perioperative period can lead to complications such as wound-healing disorders and infections up to sepsis. Effective-ness of acupuncture in regulating the immune function by increasing leukocyte numbers and in-hibiting inflammatory response has been proven.
The aim of this study was to explore the impact of electroacupuncture (EAP) on the dynamic bal-ance of the immune system and immune cell populations in dogs undergoing surgery. For this purpose, twelve healthy bitches scheduled for elective ovariectomy were divided into two groups according to whether (EAP, n=6) or not (CTR, n=6) a peri-operative electroacupuncture treatment was performed. Levels of leukocytes (neutrophils, monocytes, T- and B-cells) and immunoglobu-lins M (IgM) and A (IgA) were measured in blood samples collected before (T0), 1 hour (T1) and 2.5 hours (T2) after anesthesia induction. Leukocytes count decreased from T0 to T1 in both groups and restored within 1.5 hours in EAP group whereas remained significantly lower in CTR group (P<0.02). In particular, neutrophils and monocytes increased in dogs receiving EAP (P<0.01) while T-cells decreased in CTR group (P<0.04) at T2. B-cells and cytotoxic T-cells de-creased in EAP dogs (P<0.04) at T2. No differences in helper T-cells, IgM and IgA levels were recorded between groups and over time. Our results suggest a modulatory effect of EAP on the immune system which is early expressed on neutrophils, monocytes and T-cells.
Keywords:
immunoglobulins
; leukocytes
; lymphocytes
1. Introduction
The innate immunity is the first defense of the organism, it acts immediately after an aggression and involves both cellular and molecular defenses. In particular, phagocytic cells such as neutrophils, monocytes and macrophages play a crucial role, whereas complement, interferon, lysozyme and defensins are some examples of molecules [1]. The innate immunity uses primitive nonspecific recognition systems to bind, neutralize and destroy pathogens [2]. The adaptive or acquired immunity is responsible for a targeted response to antigens through the activation of B- and T-cells and the synthesis of proteins such as antibodies and cytokines [2,3,4]. Adaptive response comprises humoral and cellular components [4]. Humoral immunity is mediated by antibodies (immunoglobulins) secreted by plasma cells. In particular, immunoglobulins M (IgM) are produced in response to the first antigenic stimulation and are soon replaced by immunoglobulins G (IgG) or A (IgA) [1,5]. Cell-mediated immunity involves helper T-cells and cytotoxic T-cells. Helper T-cells play a central role in facilitating and driving the activity of other immune cells through the release of cytokines and chemokines, either improving antibody production or cell-mediated responses depending on the antigen nature and localization. Cytotoxic T-cells act by killing cells expressing non-self antigens, including tumor cells and virus-infected cells [1,2,5]. These cells have been reported to increase during the surgical trauma period [6].
Surgical tissue injury and exposure to anesthetic drugs during the perioperative period can affect the immune system [7]. The first pro-inflammatory response to surgical stress triggers the innate immune system eliciting an increase in monocytes, neutrophils and macrophages [7,8]. Since an excessive reaction may be harmful, a compensatory immunosuppressive response occurs, the extent and duration of which depends on the surgery magnitude [9]. It mainly involves cells of the adaptive immune system and mediators such as cytokines, chemokines and other molecules, leading to a decrease in circulating lymphocytes [7,8,9]. Apparently, T-cells are the most affected, whereas B-cells numbers change little [9]. A progressive suppression of the immune response during the first week after surgical trauma contributes to the development of sepsis and the multiorgan dysfunction syndrome [4].
Evidence suggests that acupuncture can regulate the immune system [10,11]. In humans, electroacupuncture (EAP), an application of electrical current on acupuncture needles, is reported to be effective in enhancing immune function by alleviating immunosuppression of patients during [4] and after surgery [4,11]. Similarly, in laboratory species, EAP resulted in a decrease in lymphocyte apoptosis induced by surgical trauma [12] and in a restoration of suppressed lymphocyte proliferation [4,13]. Electroacupuncture appears to reduce immunosuppression of both humoral and cellular components by contrasting the decrease in IgM and IgA levels as soon as 2 hours after anesthesia [4].
The present study aimed to explore the effect of EAP on the immune system and immune cell populations in healthy dogs undergoing ovariectomy. In particular, leukocytes count (WBC) and neutrophils, monocytes, T- (cytotoxic and helper) and B-cells, and IgM and IgA levels were evaluated at three time points within 2.5 hours from induction of anesthesia in dogs treated with peri-operatively EAP and compared with those of untreated dogs. Furthermore, a complete blood cell count (CBC) was performed at each time, also red cells and platelet parameters were evaluated.
We expected that EAP could restrain the immunosuppression that develops during the perioperative period by harmonizing cellular and humoral immune responses.
2. Materials and Methods
This study was approved by the Institutional Ethical Committee for Animal Care of Università degli Studi di Milano, Italy (OPBA_56_2023). Written consent acquisition by the owner was mandatory to participate to the research.
2.1. Animals
Twelve healthy bitches (ASA status I–II) undergoing elective ovariectomy were randomly (www.randomizer.org) assigned either to the electroacupuncture (EAP, n=6) or to control (CTR, n=6) group. Bitches were both purebred dogs (American Staffordshire n=3; Bouledogue n=1; Hound n=1; Schnauzer n=1) and mongrels (n=6), aged from 9 months to 2 years (1.4±0.4), weighted 7.8 kg to 25 kg (18.2±5.5) and had body condition score (BCS) 2/5 to 3/5 (2.6±0.5).
Dogs with ASA status > II, aged more than 3 years, that underwent previous anesthesia and surgery and that were administered pharmacological therapy within 6 months prior to ovariectomy, or that were otherwise unhealthy were excluded from the present study.
2.2. Anesthetic Protocol
All dogs were fasted for 8 hours, and water was withheld for 2 hours before the beginning of the study. Dogs were premedicated with intramuscular methadone (Semfortan, Dechra Veterinary Products, Italy) at 0.3 mg kg-1. After 20 minutes, an intravenous (IV) catheter was aseptically placed into a cephalic vein and general anesthesia was induced with IV propofol (Proposure; Merial Italia S.p.A., Italy) at 2.5 mg kg-1, in combination with dexmedetomidine (Dexdomitor, Vetoquinol S.r.l., Italy) administered IV at a dose of 2 mcg kg-1, as co-inducer and supplementary analgesic drug. After orotracheal intubation, general anesthesia was maintained with isoflurane (Isoflo, Esteve S.p.A., Italy) in oxygen (100%) titrated to effect in order to obtain a plane of anesthesia that maintained a ventral eye globe position, absence of palpebral reflex and relaxed jaw tone. During anesthesia, IV lactated Ringer’s solution (Ringer Lattato; Fresenius Kabi, Italy) was given at 5 ml kg-1 h-1 and IV cefazolin (Cefazolina, Teva, Italy) 25 mg kg-1 was administered 20 minutes before surgery. During the anesthesiologic and surgical periods, the animals were continuously monitored for respiratory rate, heart rate, electrocardiogram, oxyhemoglobin saturation, end-tidal CO2 concentration and non-invasive arterial blood pressure using a multiparameter monitor (Datex Ohmeda S5, GE Healthcare, Italy). Post-operative pain was further controlled by a non-steroidal anti-inflammatory drug, meloxicam (Metacam; Boehringer Ingelheim, Germany), administered subcutaneously at 0.2 mg kg-1 upon awakening, according to standard practice. Surgical and anesthetic procedures were performed routinely by the same operators and their duration was recorded.
2.3. Electroacupuncture Protocol
In EAP group, acupoints stimulation began 20 minutes after general anesthesia induction, i.e. 15 minutes before the start of surgery, and lasted until the last skin suture was placed. An electronic acupunctoscope (WQ-6F(57–6F), Beijing Haidian, China) was used. Dogs in CTR group were kept inducted as long as those in the EAP group; for both groups surgery started 35 minutes after general anesthesia induction. Selected acupoints were Kong Zui or Lung 6 (LU6), Hegu or Large intestine 4 (LI4), Zusanli or Stomach 36 (ST36), Xuan Zhong or Gall bladder 39 (GB39), Ge Shu or Bladder 17 (BL17), and Shenshu or Bladder 23 (BL23).
Needles (0.30 x 50 mm; Hwato, GMT2000, Laveno, Italy) were inserted at a depth of 15-20 mm. A frequency of 16 Hz and 0.4 V was applied to all acupoints except BL17 and BL23 stimulated with 43 Hz and 0.1 V.
2.4. Sampling and Analysis of Immune Function
Three blood samples were taken in both groups at the time of anesthesia induction (T0), 1 h after T0 (T1), i.e. 40 min from the start of EAP and 25 min after the start of surgery, and 2.5 hours after T0 (T2), i.e. after the end of the surgery. The blood samples were divided into two aliquots of 1.5 mL each: one was put in EDTA-containing tubes for hematological and flow cytometric analysis, the other was centrifugated at 4 °C for 5 min and the serum used for immunoglobulin titration. For each sample, a complete blood cell count (CBC) was performed with an automated hematology analyzer equipped with the veterinary software (Sysmex XN-V, Sysmex corporation, Kobe, Japan) and blood smear was prepared to perform leukocyte differential and platelet estimation. In order to further quantify leukocyte subclasses, flow cytometry (FC) was performed on each sample. All samples were processed according to already published protocols [14], acquired with a Bricyte E6 flow cytometer (Mindray, Shenzhen, China) and analyzed with the specific software MRflow (Mindray) by a single experienced operator (VM). A panel of five antibodies was applied, including anti-CD11b (neutrophils and monocytes), anti-CD5 (T-cells), anti-CD8 (cytotoxic T-cells), anti-CD4 (Helper T-cells), and anti-CD21 (B-cells) [15]. Both CBC and FC were performed within few minutes from sampling.
Serum IgM and IgA levels were determined using specific ELISA kits (BT LAB Bioassay Technology Laboratory, Jiaxing, Zhejiang, China) based on the sandwich approach. Expressed as coefficient of variability (CV), the declared intra-assay precision was <8% and the declared inter-assay precision was <10%.
2.5. Statistical Analysis
Descriptive statistics are expressed as means (± sd). Data were analyzed using a commercial statistical software (IBM SPSS, 28.0) comparing analyzed different parameters in the experimental groups at each time point with non-parametric test U- Mann-Whitney, since data were not normally distributed (Shapiro-Wilk test). The effect of time in treated and control groups on different measured parameters was assessed with a non-parametric Friedman ANOVA test and pairwise comparison. Statistical significance was accepted at P<0.05.
3. Results
All surgeries and recoveries had a regular course. No peri-operative complications occurred in any dog. Dogs in the two groups had similar age (EAP: 1.6±0.5 years; CTR: 1.5±0.3), body weight (EAP: 17.8±3.1 kg; CTR:18.5±7.4) and BCS (EAP: 2.5±0.5; CTR: 2.6±0.5) as well as the same surgical (EAP: 40.8±11.9 min; CTR: 40.8±13.6 min) and anesthetic, i.e. from induction to extubation, (EAP: 86.7±4.5 min; CTR: 84.7±16) times. No statistical differences in these parameters were recorded between the groups.
Hematological parameters concerning erythrocytes (RBC) and platelets (PLT) showed no differences between groups and time points (Appendix A). Conversely, leukocytes count (WBC) was significantly lower in CTR than EAP group at all time points (P≤0.03). They decreased soon after induction (at T1) in both groups but restored at T2 in EAP group while remained significantly lower than T0 in the CTR group (Figure 1; P<0.02).
Myeloid cells (neutrophils and monocytes) increased at T2 compared to T0 in dogs undergoing EAP (P=0.005) but not in CTR group (Figure 2).
On the contrary, 2.5 hours after induction T-cells decreased in CTR group (P<0.04) but not in EAP group (Figure 3).
Cytotoxic T-cells (P=0.03) and B-cells decreased in EAP group (P<0.04) at T2 compared to T0 (Figure 4 and Figure 5). Helper T-cells did not show variations between groups and over time.
No significant differences in IgM and IgA concentrations were recorded between groups and over time. However, a decreasing trend of IgM levels was observed in EAP compared to CTR group (Figure 6).
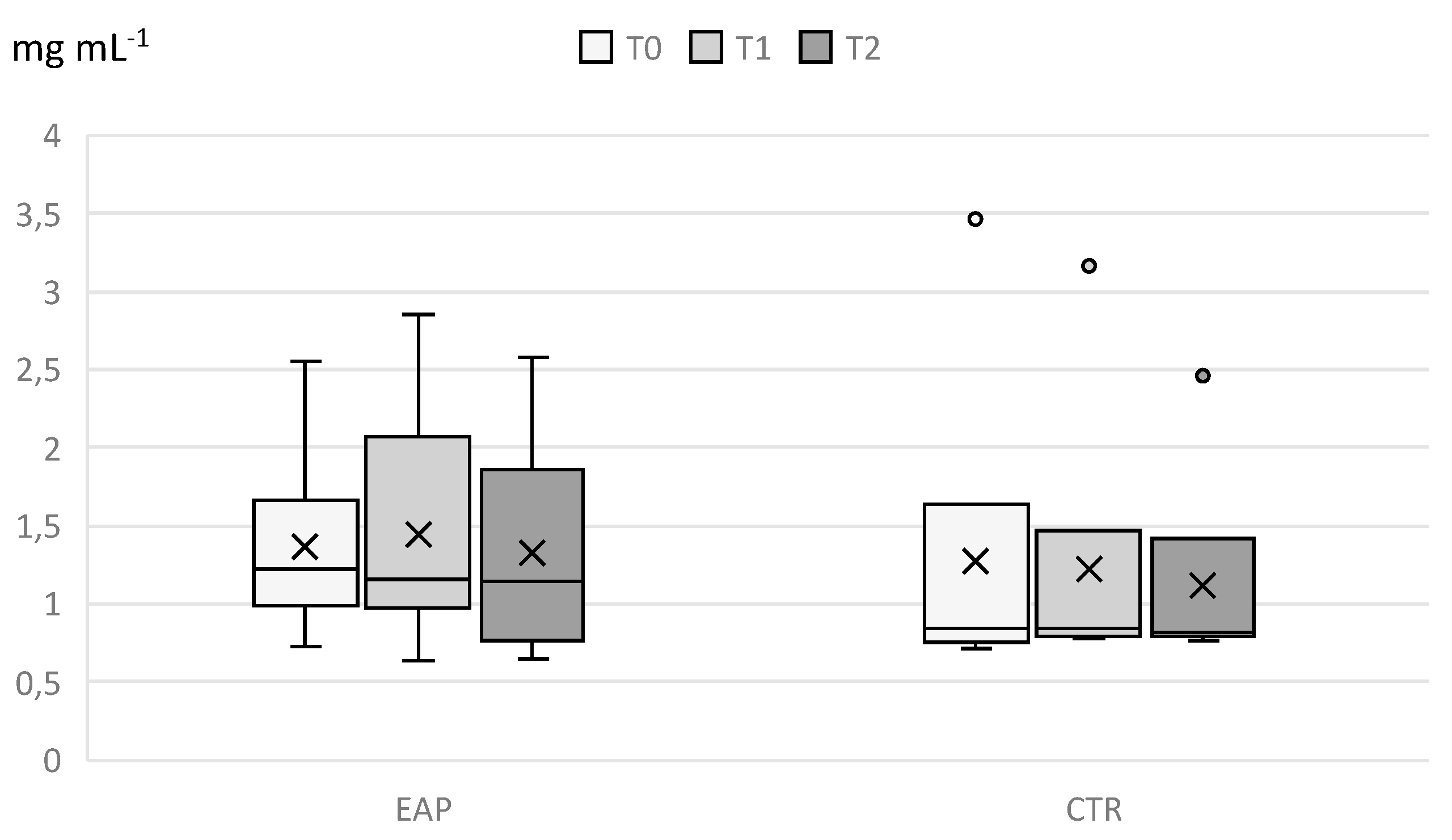
On the contrary, EAP dogs tended to have higher IgA values than CTR dogs even without statistical significance (Figure 7).
4. Discussion
Immunosuppression due to surgery and anesthesia is a current and debated topic with many aspects still unknown in both human and veterinary medicine. Most publications report medium- and long-term effects on the immune system (days, weeks) [8,16,17], while few studies target the very early perioperative period [6,18]. The present study focused precisely on this period which may account for some unexpected results. We only included elective ovariectomy as a routine surgery performed on healthy dogs that allows for standardized clinical trials. In fact, the surgical technique together with its duration and extent are closely related to the degree of immunosuppression [9]. Moreover, inclusion of dogs with different diseases and undergoing different surgical procedures would have biased the results. In our study the two groups (EAP and CTR) were equivalent in terms of surgical and anesthesiologic procedures and exposition besides in size, age, body weight and BCS, making them suitable to compare and evaluate the effects of electroacupuncture.
To date, the detailed mechanisms of action of EAP are still unclear. Acupuncture is reported to be effective in regulating nonspecific immune function [19] as well as cellular and humoral immunity [20,21]. In general, acupuncture immunomodulation acts by stimulating the somatic-autonomic-immune reflexes that include the somatic-sympathetic-splenic reflex, the somatic-sympathetic-adrenal reflex, the somatic-vagal-splenic reflex and the somatic-vagal-adrenal reflex leading to a systemic involvement [22]. Furthermore, the stimulation of peripheral nerve due to the insertion of an acupuncture needle induces a traumatic inflammation also responsible for a local immunomodulation at the acupoint level [23].
The most intriguing aspect of acupuncture recently arose in the literature is its bidirectional effect aimed to maintain the homeostasis by balancing hyper- and hypo-functional states [24,25]. It refers to the ability of acupuncture to act by both activating and inhibiting the same mechanism that relies on the body’s self-healing [22]. This is a unique aspect of acupuncture that no specific drug has achieved so far.
An initial pro-inflammatory effect is reported to occur as a result of surgical stress and tissue damage, which is followed by a compensatory immunosuppressive response aiming to facilitating the resolution of inflammation and protecting against excessive systemic consequences of the primary insult [18,26]. The decreasing trend of WBC observed in both EAP and CTR groups within 1 hour from general anesthesia induction can be interpreted as an early sign of immunosuppression. The latter appeared to persist until the end of monitoring, i.e. 2.5 hours after induction, in CTR (P<0.02) but not in EAP group, with the number of leucocytes significantly lower than pre-surgically. Furthermore, the percentage of neutrophils and monocytes increased in EAP dogs after 1.5 hours (P=0.005) while remained low in CTR dogs. Innate immunity is described to restore early during postoperative recovery taking 2 to 3 days for neutrophils and monocytes, respectively [18]. EAP seems to be able to shorten this time.
In accordance with a suppression of acquired immunity lasting several days postoperatively [18] and characterized by apoptotic reduction in the number of T-cells [26], we recorded a decrease in T-cells in the CTR group (P<0.04). The concentration of T-cells in the EAP group, however, remained unchanged over time, suggesting a possible counteracting action due to EAP treatment. On the other hand, B-cells and cytotoxic T-cells decreased in EAP dogs (P<0.04) but not in CTR group. Since acquired immune cells are reported not to recover until 5 days from surgical insults [18], it is possible that the effect of EAP may be noticeable after such period, not earlier. Moreover, a modulatory action of EAP on the type 1 (Th1) and type 2 (Th2) T helper cells is reported [27,28,29,30]. EAP can both stimulate and downregulate Th1 and Th2, that are responsible for pro-inflammatory and anti-inflammatory responses, respectively [22,30,31,32]. In the present study we have not performed a distinction between Th1 and Th2 T helper cells, therefore it is not possible to argue about them. Finally, EAP stimulation at Zusanli (ST36) acupoint in rats increases lymphocyte proliferation after surgery [13,33,34] while in mice suppresses Th2 cytokine IL-4 [31]. To the authors’ knowledge, to date no studies in dogs have been published on this aspect, and a species-specific modality of EAP can only be speculated.
The few data in the literature on immunoglobulin are conflicting. Some authors reported no differences in IgM and IgA concentrations between groups and over time [35] while a study on the effect of EAP on postoperative immunoinflammatory response in human patients undergoing craniotomy showed that the blood IgA decreased significantly in control group 4 hours after induction of anesthesia and one day after surgery, but no significant differences were noted between control and treated groups [36]. The same research group soon after noted that electroacupuncture was able to alleviate intraoperative immunosuppression in the same type of human patients: in that case, both IgM and IgA decreased significantly in control group compared with treated groups 2 and 4 hours after induction of anesthesia, while no significant differences between groups were noted for IgG [4]. In our study, dogs treated with EAP showed a decreasing trend of IgM levels and an increasing trend of IgA levels compared to the CTR group. It should be noted that all dogs except one in the CTR group resulted below the expected values for IgM in canine species (0.7-2.7 mg/mL) [1]. On the contrary, IgA levels were always within the expected range (0.2-2.5 mg/mL) in both groups [1]. The degree of dogs immunization, and particularly few contacts with new antigens never encountered before (which would have resulted in the production of IgM), could have affected our results, but these are aspects that we did not take into account in this study.
At last, even anesthetic drugs can have an impact on the immune function such as opioids which are mediated indirectly by activation of the HPA axis and sympathetic nervous system, and by a direct effect on many subtypes of immune cells [9]. Recent review studies underlined conflicting conclusions reporting immunosuppressive, immunostimulatory, or dual mechanisms for opioids [37]. Morphine is known to suppress a variety of immune functions including T lymphocytes proliferation [37]. The use of methadone to premedicate dogs in our study can justify the significant decrease in T-cells observed in the CRT group. Conversely in EAP group, endogenous endorphins releasing due to EAP stimulation may have acted as competitive agonists thus reducing the suppressive effect of methadone.
The small sample size of our caseload is a limitation that cannot be neglected before generalizing these findings. In addition, although we included a standardized population in order to avoid biases, it is possible that different anesthetic or surgical procedures might bring to different results. Moreover, we monitored hematological and immune parameters only for 2.5 hours after induction, and effects on longer periods could be quite different.
5. Conclusions
In conclusion, the results of this exploratory study suggest that EAP may influence the immune response in dogs undergoing elective ovariectomy. EAP appears to reduce the immunosuppression through a modulatory effect which is expressed early on neutrophils, monocytes and T-cells. EAP also seems to shorten the time of immune system restoration after surgery. EAP due to a non-pharmacological and non-invasive approach, is an attracting and promising therapy to reduce immunosuppressive perioperative risk in dogs.
In any case, a larger-scale randomized controlled trial also including a longer postoperative period is advisable to confirm these promising results.
Author Contributions
Conceptualization, V.R., F.A.B. and D.G.; methodology, V.R., G.R. and D.G.; formal analysis, V.B., V.M. and P.D.; investigation, A.P. and D.G.; data curation, V.R., V.B., V.M.; writing—original draft preparation, V.R., F.A.B.; and D.G.; writing—review and editing, all authors; supervision, G.R.; project administration, D.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Università degli Studi di Milano (OPBA_56_2023).
Informed Consent Statement
Informed consent was obtained from all dog owners that were involved in the study.
Data Availability Statement
All the data that support the findings of this study are available from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A. Hematological Parameters in EAP and CTR Groups at Each Time Point

|
RBC x106µL-1 |
WBC x103µL-1 |
Hb g dL-1 |
Ht % |
PLT x103µL-1 |
MCH pg |
MCHC g dL-1 |
MCV µ3 |
RDW % |
MPV µ3 |
|||||||||||||||||||||
| ID. | T0 | T1 | T2 | T0 | T1 | T2 | T0 | T1 | T2 | T0 | T1 | T2 | T0 | T1 | T2 | T0 | T1 | T2 | T0 | T1 | T2 | T0 | T1 | T2 | T0 | T1 | T2 | T0 | T1 | T2 |
| EAP1 | 5.8 | 6.4 | 6.8 | 14.8 | 10.4 | 18.5 | 12.9 | 14.2 | 15.2 | 37.6 | 41.9 | 44 | 385 | 243 | 372 | 22.1 | 22.2 | 22.2 | 34.3 | 33.9 | 34.5 | 64.3 | 65.4 | 64.2 | 16.9 | 18.4 | 18.7 | 10.3 | 11.5 | 10.1 |
| EAP 2 | 6.2 | 5.3 | 5.5 | 18.4 | 16.7 | 14.2 | 15.1 | 12.9 | 13.5 | 44.1 | 38.5 | 39.8 | 438 | 462 | 422 | 24.5 | 24.4 | 24.5 | 34.2 | 33.5 | 33.9 | 71.6 | 72.9 | 72.4 | 19 | 16.3 | 17.2 | 10.1 | 11.1 | 9.6 |
| EAP 3 | 7.5 | 6.1 | 6.5 | 13.5 | 13.7 | 12.6 | 18.3 | 14.8 | 15.7 | 50.6 | 44 | 45.6 | 213 | 236 | 233 | 24.4 | 24.1 | 24.1 | 36.2 | 33.6 | 34.4 | 67.4 | 71.8 | 70 | 20.3 | 17.9 | 18.5 | 11.7 | 12.4 | 12 |
| EAP 4 | 7.6 | 5.6 | 7 | 14.8 | 14.5 | 13.4 | 17.5 | 15.6 | 16.4 | 49.4 | 38.8 | 47.8 | 211 | 190 | 237 | 23 | 27.9 | 23.3 | 35.4 | 40.2 | 34.3 | 65 | 69.3 | 67.8 | 19.8 | 15.6 | 18.9 | 10.5 | 9.7 | 11.8 |
| EAP 5 | 7.2 | 6 | 6.1 | 19.5 | 16.2 | 15.2 | 16.4 | 14 | 14.1 | 46.1 | 41.6 | 41.7 | 201 | 192 | 184 | 22.9 | 23.2 | 23 | 35.6 | 33.7 | 33.8 | 64.4 | 68.9 | 68.1 | 20.2 | 18.2 | 18.1 | 11.6 | 11.4 | 11.6 |
| EAP 6 | 7.2 | 5.9 | 7.3 | 15.4 | 13.7 | 12.3 | 16.8 | 13.8 | 16.9 | 41.5 | 40.2 | 49.5 | 164 | 138 | 163 | 23.3 | 23.5 | 23.3 | 35.4 | 34.3 | 34.2 | 66 | 68.6 | 68.2 | 20.9 | 18.2 | 19.9 | 13.5 | 12.6 | 12.4 |
| CTR 1 | 7.9 | 6.9 | 7.7 | 13.1 | 10.2 | 11.9 | 19.6 | 16.9 | 18.8 | 53.5 | 47.9 | 52.4 | 311 | 172 | 278 | 24.6 | 24.6 | 24.5 | 36.6 | 35.3 | 35.9 | 67.1 | 69.7 | 67.3 | 20.1 | 18.7 | 20.1 | 11.3 | 11.9 | 11.3 |
| CTR 2 | 8 | 7 | 7.1 | 13.1 | 11.6 | 10.2 | 19.6 | 17.1 | 17.2 | 54.4 | 47.7 | 46.7 | 170 | 174 | 164 | 24.4 | 24.3 | 24.3 | 36 | 35.8 | 36.8 | 67.7 | 67.8 | 66 | 21.1 | 20.2 | 20.1 | 12.9 | 13 | 13.1 |
| CTR 3 | 6.7 | 5.4 | 5.7 | 11.4 | 8.2 | 8 | 16 | 13.1 | 13.2 | 47.9 | 39.4 | 40.1 | 230 | 212 | 139 | 23.8 | 24.1 | 23.3 | 33.4 | 33.2 | 32.9 | 71.2 | 72.6 | 70.7 | 19.1 | 16.3 | 17.8 | 12.3 | 12.6 | 12.3 |
| CTR 4 | 6.8 | 6.4 | 6.6 | 12.7 | 10.6 | 10.9 | 15.3 | 14.3 | 14.8 | 44 | 42.1 | 41.1 | 276 | 288 | 258 | 22.5 | 22.3 | 22.3 | 34.8 | 34 | 36 | 64.6 | 65.7 | 62 | 20 | 19.6 | 19.6 | 11.6 | 12 | 11.2 |
| CTR 5 | 7.7 | 6.8 | 6.7 | 12.7 | 13 | 10 | 18.3 | 16.2 | 16 | 52.7 | 45.9 | 45.6 | 193 | 192 | 199 | 23.7 | 23.9 | 23.7 | 34.7 | 35.3 | 35.1 | 68.4 | 67.6 | 67.7 | 19.9 | 18.8 | 18.3 | 12.8 | 13 | 13 |
| CTR 6 | 6.8 | 5.7 | 5.6 | 14.5 | 12.1 | 11.4 | 17.2 | 14.4 | 14.1 | 47.8 | 41.6 | 41.3 | 284 | 310 | 287 | 25.4 | 25.4 | 25.3 | 36 | 34.6 | 34.1 | 70.5 | 73.4 | 74.1 | 20.4 | 17.8 | 16.8 | 11.5 | 11.7 | 11.2 |
RBC: total red blood cell count, WBC: total white blood cell count, Hb: hemoglobin, Ht: hematocrit, PLT: platelet count, MCH: mean cell hemoglobin, MCHC: MCH concentration, MCV: mean cell volume, RDW: red cell distribution width, MPV: mean platelet volume. T0: at the time of induction of anesthesia, T1: 30 min after T0, T2: 2 hours after T0.
References
- Tizard, I.R. Veterinary immunology, 10th ed.; Elsevier: St Louis, USA, 2017. [Google Scholar]
- Kurosawa, S.; Kato, M. Anesthetics, immune cells, and immune responses. J Anesth. 2008, 22, 263–77. [Google Scholar] [CrossRef] [PubMed]
- Vivier, E.; Malissen, B. Innate and adaptive immunity: specificities and signaling hierarchies revisited. Nature Immunology 2005, 6, 17–21. [Google Scholar] [CrossRef]
- Li, G.; Li, S.; An, L.; Wang, B. Electroacupuncture alleviates intraoperative immunosuppression in patients undergoing supratentorial craniotomy. Acupuncture Medicine 2013, 31, 51–56. [Google Scholar] [CrossRef]
- Poli, G.; Dall’Ara, P.; Martino, P.A.; Rosati, S. Microbiologia e immunologia veterinaria, 3rd ed.; EDRA: Milano, Italy, 2017. [Google Scholar]
- Navarro, M.; Lozano, R.; Larrad, L.; Román, A.; Suarez, J.; Armijo, J. Variation in T helper cell/T cytotoxic-suppressor cell index during cardiac operations. J Thorac Cardiovasc Surg. 1988, 96, 962–6. [Google Scholar] [CrossRef] [PubMed]
- Cardinale, F.; Chinellato, I.; Caimmi, S.; Peroni, D.G.; Franceschini, F.; Miraglia Del Giudice, M.; Bernardini, R. Perioperative period: immunological modifications. International Journal of Immunopathology and Pharmacology 2011, 24, 3–12. [Google Scholar] [CrossRef]
- Cook, E.J.; Walsh, S.R.; Farooq, N.; Alberts, J.C.; Justin, T.A.; Keeling, NJ. Post-operative neutrophil-lymphocyte ratio predicts complications following colorectal surgery. Int J Surg. 2007, 5, 27–30. [Google Scholar] [CrossRef]
- Hogan, B.V.; Peter, M.B.; Shenoy, H.G.; Horgan, K.; Hughes, T.A. Surgery induced immunosuppression. Surgeon 2011, 9, 38–43. [Google Scholar] [CrossRef]
- Takahashi, T.; Sumino, H.; Kanda, T.; Yamaguchi, N. Acupuncture modifies immune cells. J Exp Clin Med 2009, 1, 17–22. [Google Scholar] [CrossRef]
- Cho, S.Y.; Yang, S.B.; Shin, H.S.; Lee, S.H.; Koh, J.S.; Kwon, S.; Jung, W.S.; Moon, S.K.; Park, J.M.; Ko, C.N.; Park, S.U. Anti-inflammatory and immune regulatory effects of acupuncture after craniotomy: study protocol for a parallel-group randomized controlled trial. Trials 2017, 18, 10. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Wang, Y.Q.; Yu, J.; Cao, X.D.; Wu, G.C. Electroacupuncture suppresses surgical trauma stress-induced lymphocyte apoptosis in rats. Neuroscience Letters 2005, 383, 68–72. [Google Scholar] [CrossRef]
- Cheng, X.D.; Wu, G.C.; He, Q.Z.; Cao, X.D. Effect of continued electroacupuncture on induction of interleukin-2 production of spleen lymphocytes from the injured rats. Acupunct Electrother Res 1997, 22, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.frontiersin.org/articles/10.3389/fvets.2022.868967/full.
- Available online: https://www.frontiersin.org/articles/10.3389/fvets.2022.868967/full.
- Zhou, C.; Wang, Z.; Jiang, B.; Di, J.; Su, X. Monitoring pre- and post-operative immune alterations in patients with locoregional colorectal cancer who underwent laparoscopy by single-cell mass cytometry. Front. Immunol. 2022, 13, 807539. [Google Scholar] [CrossRef]
- Mizutani, Y.; Terachi, T.; Okada, Y.; Yoshida, O. Effect of surgical stress on immune function in patients with urologic cancer. Int J Urol 1996, 3, 426–434. [Google Scholar] [CrossRef]
- Lachmann, G.; von Haefen, C.; Kurth, J.; Yuerek, F.; Spies, C. Innate immunity recovers earlier than acquired immunity during severe postoperative immunosuppression. Int J Med Sci. 2018, 15, 1–9. [Google Scholar] [CrossRef]
- Peng, G. Acupuncture and innate immunity. Acupunct Res 2008, 33, 49–52. [Google Scholar]
- Liu, Y.M.; Liu, X.J.; Bai, S.S.; Mu, L.L.; Kong, Q.F.; Sun, B.; Wang, D.D.; Wang, J.H.; Shu, S.; Wang, G.Y.; Li, H.I. The effect of electroacupuncture on T cell responses in rats with experimental autoimmune encephalitis. J Neuroimmunol 2010, 220, 25–33. [Google Scholar] [CrossRef]
- Matsubara, Y.; Shimizu, K.; Tanimura, Y.; Miyamoto, T.; Akimoto, T.; Kono, I. Effect of acupuncture on salivary immunoglobulin A after a bout of intense exercise. Acupunct Med 2010, 28, 28–32. [Google Scholar] [CrossRef]
- Pan, W.X.; Fan, A.Y.; Chen, S.; Alemi, S.F. Acupuncture modulates immunity in sepsis: Toward a science-based protocol. Auton Neurosci 2021, 232, 102793. [Google Scholar] [CrossRef]
- Cabioğlu, M.T.; Cetin, B.E. Acupuncture and immunomodulation. Am J Chin Med 2008, 36, 25–36. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.Y.; Lee, B.H.; Kim, H.Y.; Yang, C.H. Bidirectional role of acupuncture in the treatment of drug addiction. Neurosci Biobehav Rev 2021, 126, 382–397. [Google Scholar] [CrossRef]
- Pan, W.X. Bidirectional regulation of acupuncture and its plausible mechanisms. Acupunct Res 2019, 44, 843–853. [Google Scholar]
- Alazawi, W.; Pirmadjid, N.; Lahiri, R.; Bhattacharya, S. Inflammatory and immune responses to surgery and their clinical impact. Annals of Surgery 2016, 64, 73–80. [Google Scholar] [CrossRef]
- Yamaguchi, N.; Takahashi, T.; Sakuma, M.; Sugita, T.; Uchikawa, K.; Sakaihara, S.; Kanda, T.; Arai, M.; Kawakita, K. Acupuncture regulates leukocyte subpopulations in human peripheral blood. Evid Based Complement Alternat Med 2007, 4, 447–453. [Google Scholar] [CrossRef] [PubMed]
- Dai, Q.M.; Shang, Y.Q.; Liang, H.; Yan, P.Y.; Wang, M.Q.; Wang, K. Research progress of effect of acupuncture therapy on T cell subsets. J Clin Acupunct 2018, 7, 78–82. [Google Scholar]
- Silvério-Lopes, S.; da Mota, M.P.G. Acupuncture in Modulation of Immunity. IntechOpen 2013. [Google Scholar] [CrossRef]
- Wang, M.; Liu, W.; Ge, J.; Liu, S. The immunomodulatory mechanisms for acupuncture practice. Front Immunol 2023, 14, 1147718. [Google Scholar] [CrossRef] [PubMed]
- Park, M.B.; Koc, E.; Ahnc, C.; Choic, H.; Rhoc, S.; Shinc, M.K.; Hongc, M.C.; Minb, B.I.; Bae, H. Suppression of IgE production and modulation of Th1/Th2 cell response by electroacupuncture in DNP-KLH immunized mice. J Neuroimmunol 2004, 151, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.; Yu, Z.F.; Kang, F.H. Th1/Th2 balance on depression patients by acupuncture treatment combined with antidepressant. J Clin Acupunct Moxibustio 2014, 30, 1–3. [Google Scholar]
- Wang, K.; Wu, H.; Wang, G.; Li, M.; Zhang, Z.; Gu, G. The effects of electroacupuncture on TH1/TH2 cytokine mRNA expression and mitogen-activated protein kinase signaling pathways in the splenic T cells of traumatized rats. Anesth Analg 2009, 109, 1666–1673. [Google Scholar] [CrossRef] [PubMed]
- Cao, X.D. Involvement of orphanin FQ in electroacupuncture modulation on immunosuppression by trauma. Zhen Ci Yan Jiu 2001, 26, 219–220. [Google Scholar]
- Cabioğlu, M.T.; Ergene, N.; Surucu, H.S.; Çelik, H.H.; Findik, D. Serum IgG, IgA, IgM, and IgE levels after electroacupuncture and diet therapy in obese women. The American Journal of Chinese Medicine 2007, 35, 955–965. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Li, S.; Wang, B.; An, L. The effect of electroacupuncture on postoperative immunoinflammatory response in patients undergoing supratentorial craniotomy. Experimental and Therapeutic Medicine 2013, 6, 699–702. [Google Scholar] [CrossRef] [PubMed]
- Liang, X.; Liu, R.; Chen, C.; Ji, F.; Li, T. Opioid System Modulates the Immune Function: A Review. Transl Perioper Pain Med 2016, 1, 5–13. [Google Scholar] [PubMed]
Figure 1.
Leukocytes count in EAP and CTR groups over time. T0 represents the anesthesia induction time, T1 means 1 h after T0; T2 means 2.5 hours after T0. ‘*’: P<0.02.
Figure 1.
Leukocytes count in EAP and CTR groups over time. T0 represents the anesthesia induction time, T1 means 1 h after T0; T2 means 2.5 hours after T0. ‘*’: P<0.02.
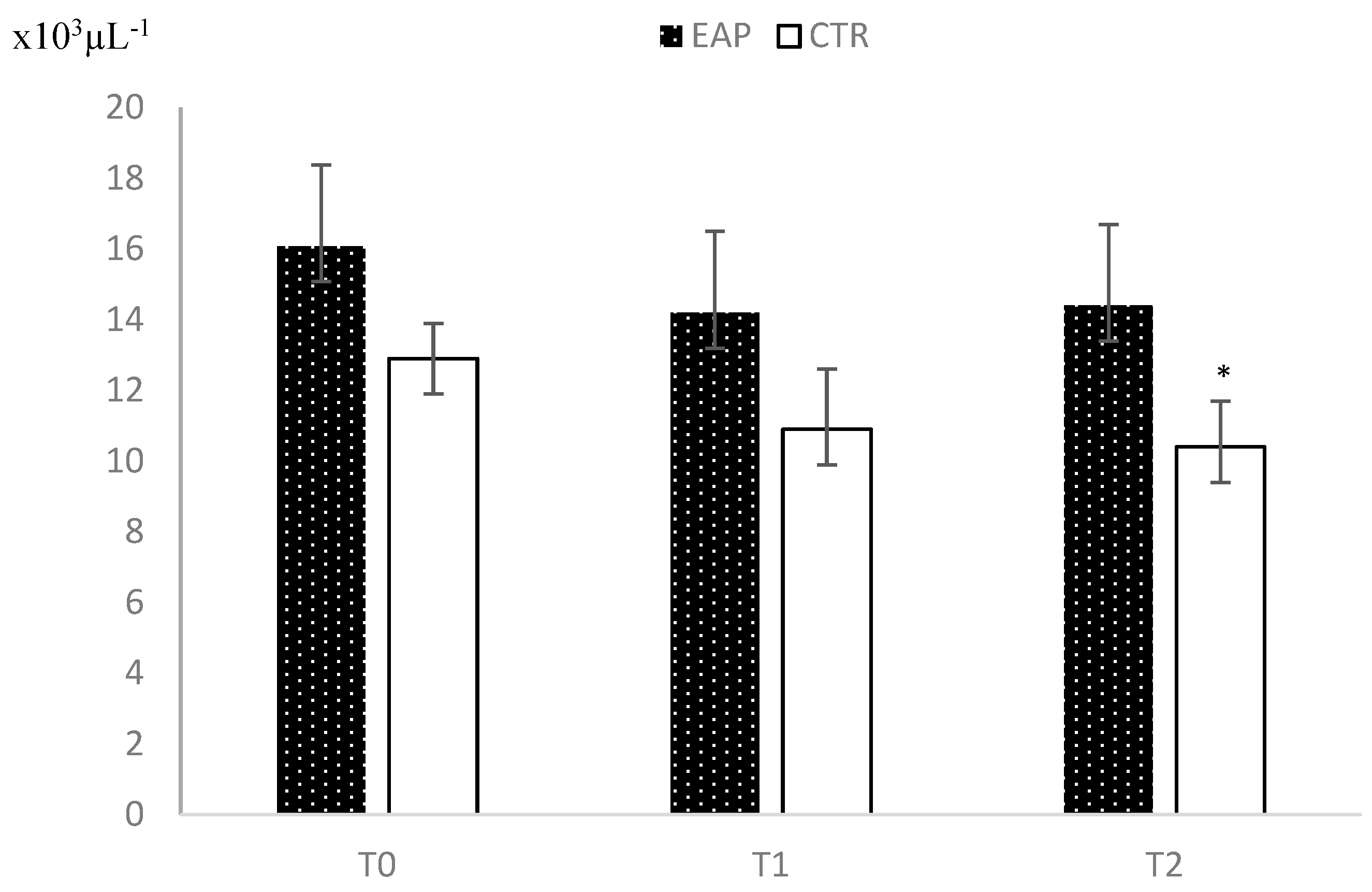
Figure 2.
Percentage of myeloid cells in EAP and CTR groups over time. T0 represents the anesthesia induction time, T1 means 1 h after T0; T2 means 2.5 hours after T0. ‘*’: P=0.005.
Figure 2.
Percentage of myeloid cells in EAP and CTR groups over time. T0 represents the anesthesia induction time, T1 means 1 h after T0; T2 means 2.5 hours after T0. ‘*’: P=0.005.
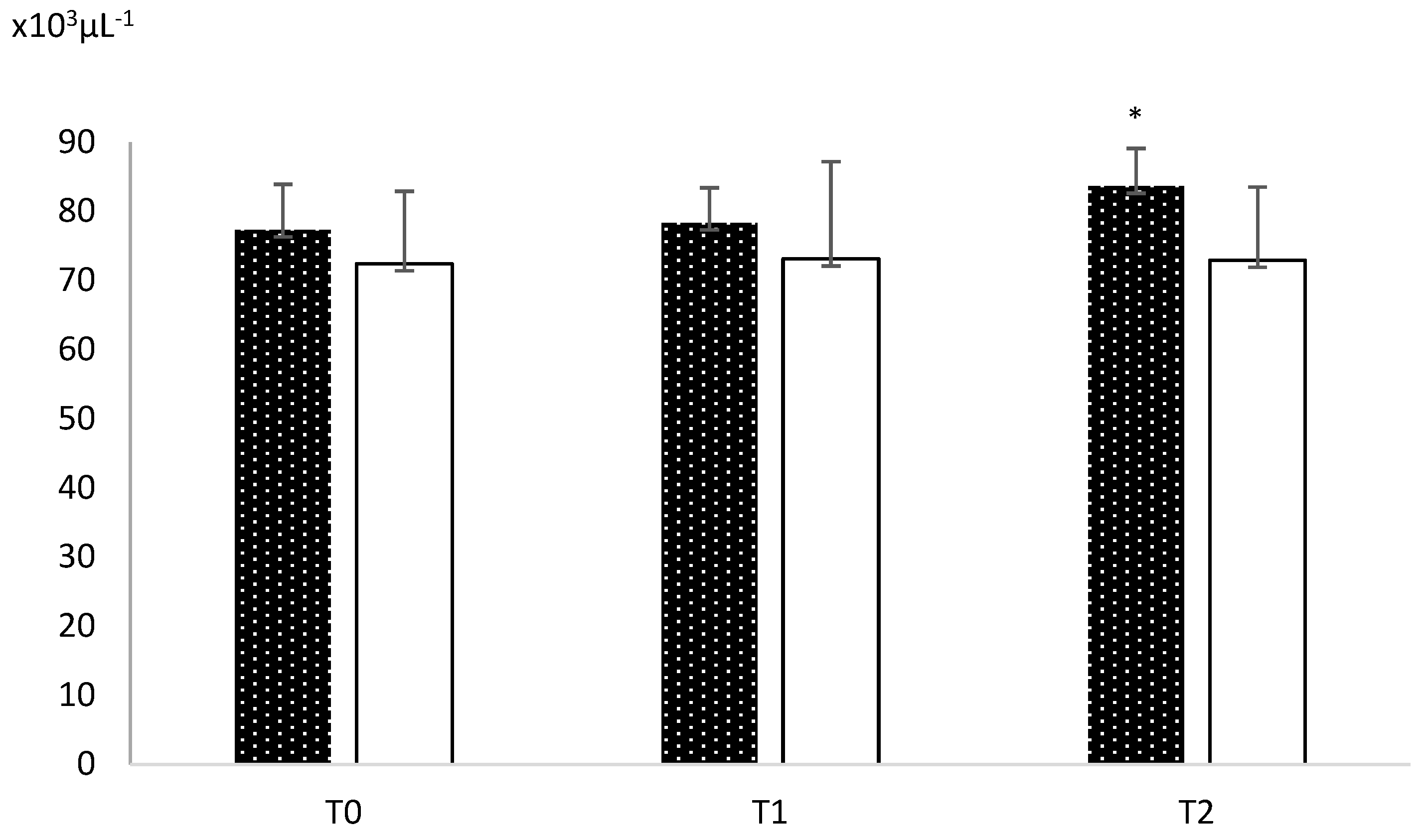
Figure 3.
Concentrations of the T-cells in EAP and CTR groups over time. T0 represents the anesthesia induction time, T1 means 1 h after T0; T2 means 2.5 hours after T0. ‘*’: P=0.038.
Figure 3.
Concentrations of the T-cells in EAP and CTR groups over time. T0 represents the anesthesia induction time, T1 means 1 h after T0; T2 means 2.5 hours after T0. ‘*’: P=0.038.
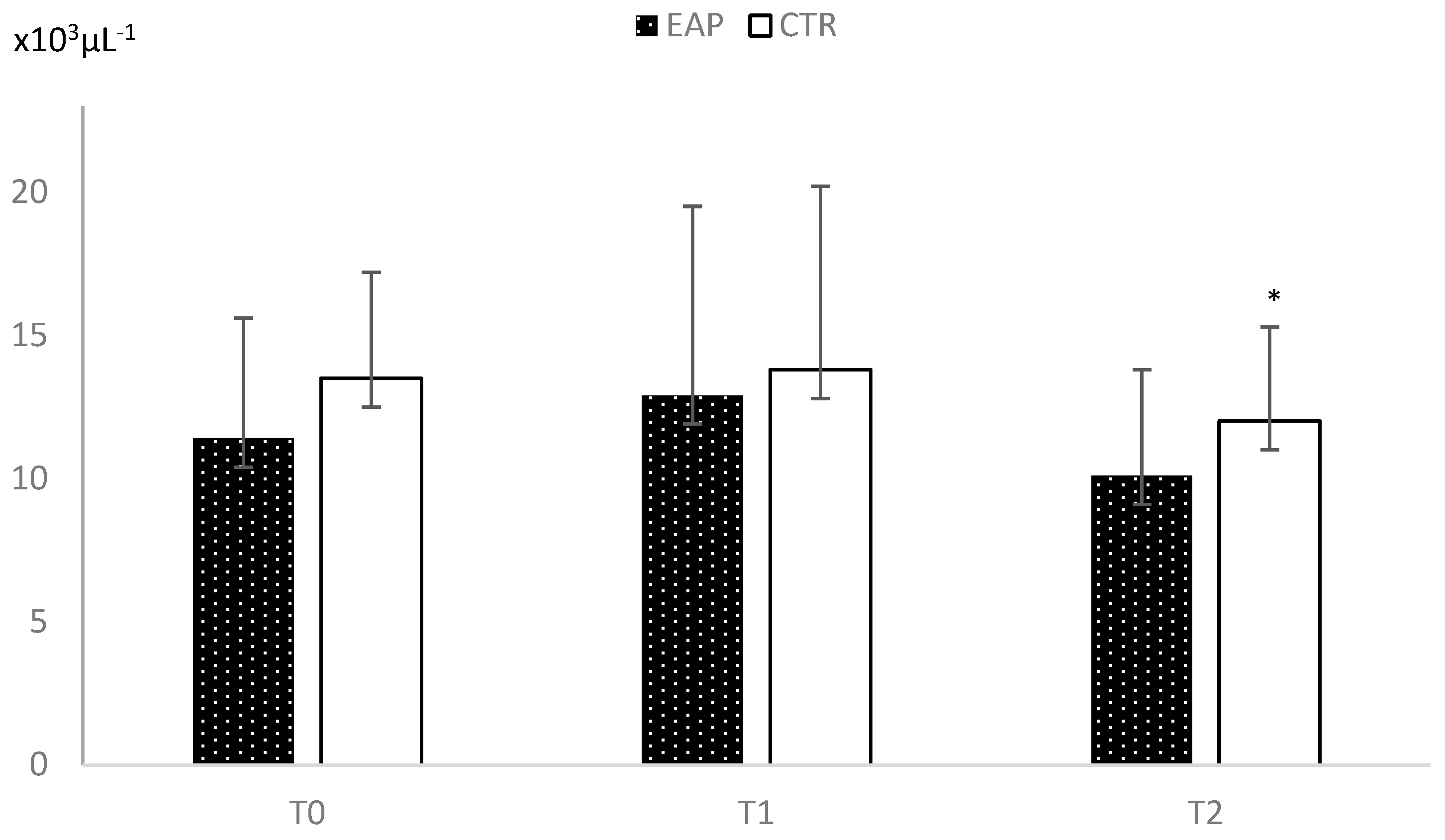
Figure 4.
Concentrations of the cytotoxic T-cells in EAP and CTR groups over time. T0 represents the anesthesia induction time, T1 means 1 h after T0; T2 means 2.5 hours after T0. ‘*’: P=0.03.
Figure 4.
Concentrations of the cytotoxic T-cells in EAP and CTR groups over time. T0 represents the anesthesia induction time, T1 means 1 h after T0; T2 means 2.5 hours after T0. ‘*’: P=0.03.
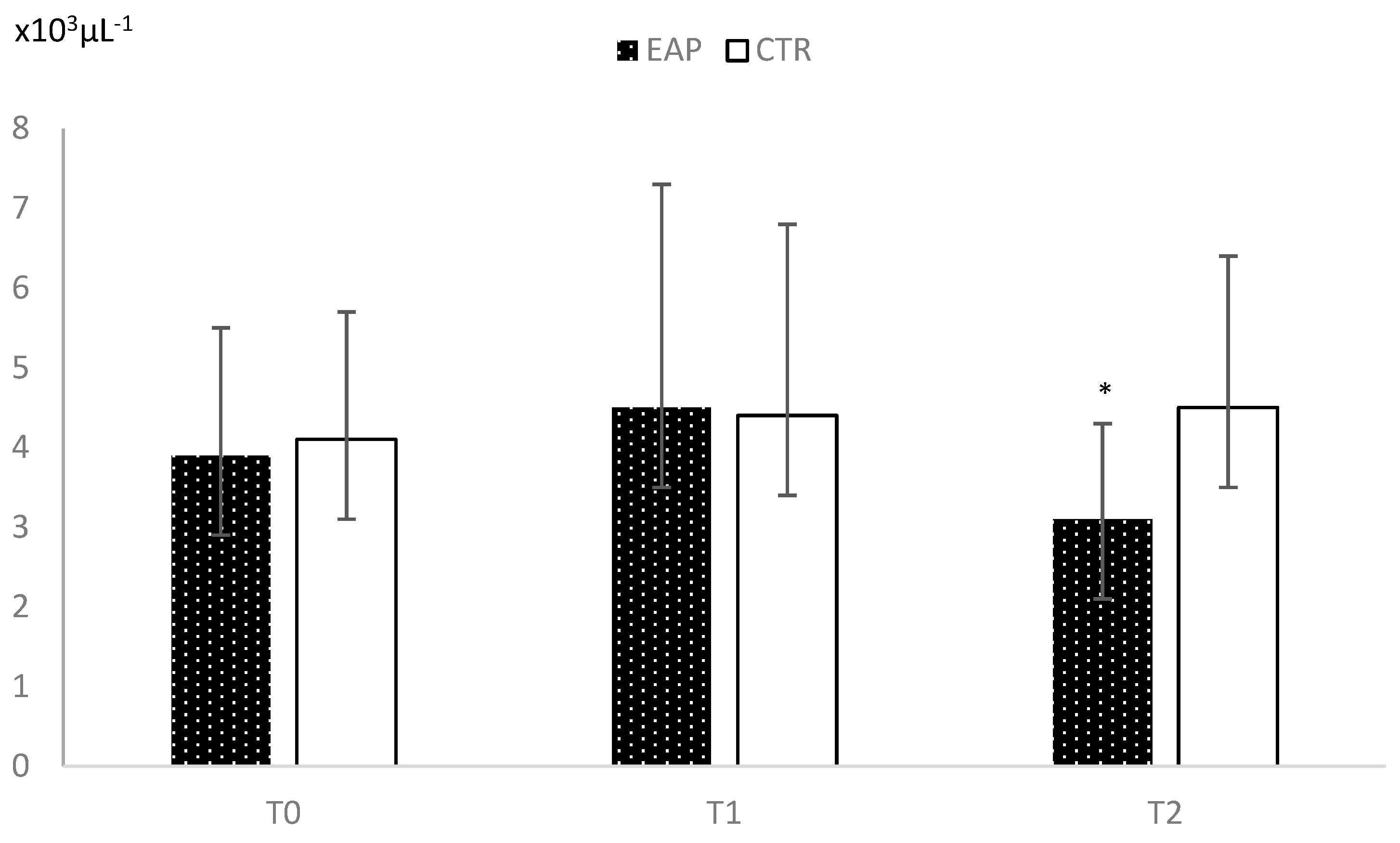
Figure 5.
Concentrations of the B-cells in EAP and CTR groups over time. T0 represents the anesthesia induction time, T1 means 1 h after T0; T2 means 2.5 hours after T0. ‘*’: P=0.036.
Figure 5.
Concentrations of the B-cells in EAP and CTR groups over time. T0 represents the anesthesia induction time, T1 means 1 h after T0; T2 means 2.5 hours after T0. ‘*’: P=0.036.
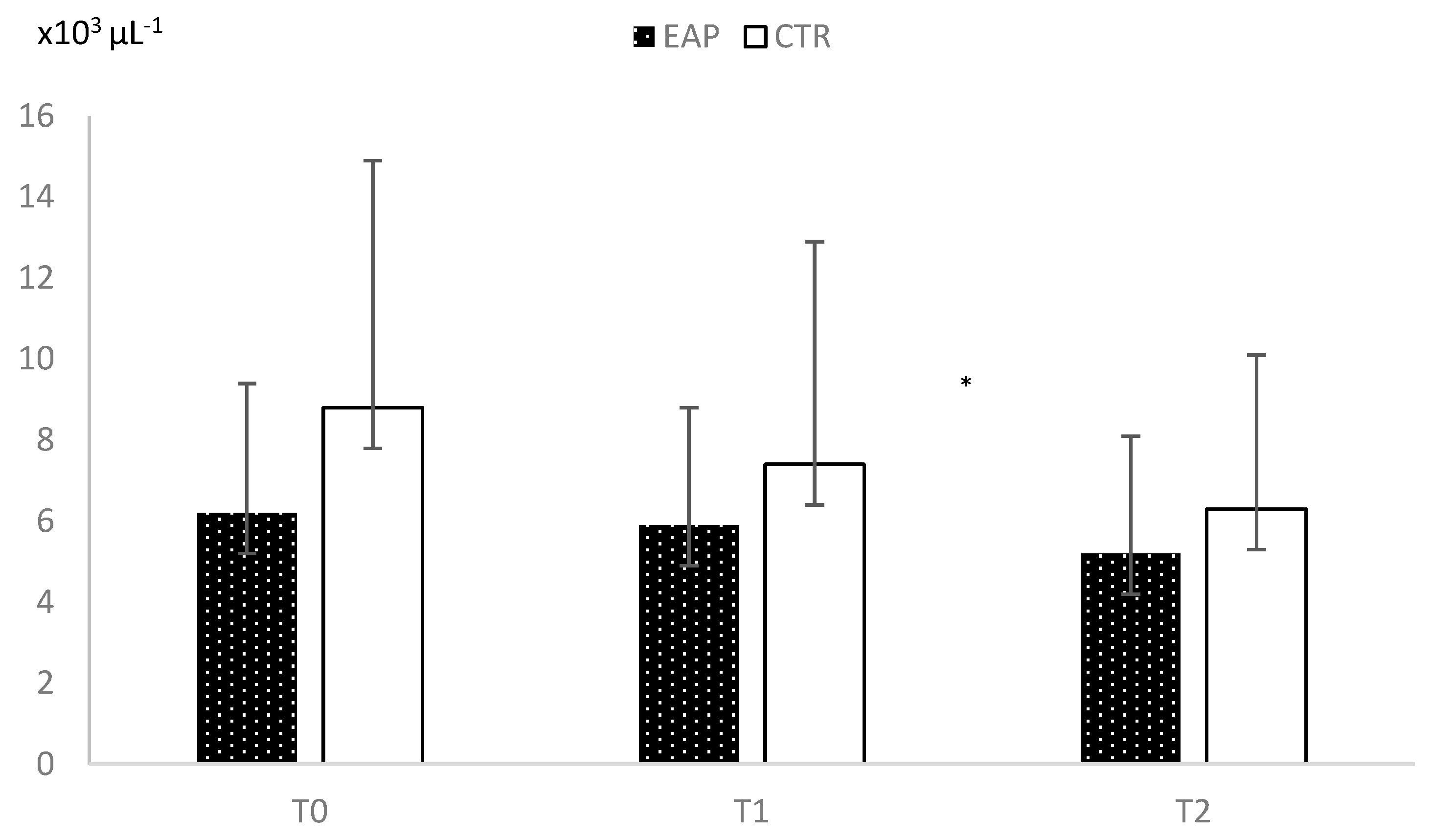
Figure 6.
Concentrations of IgM in EAP and CTR groups over time. T0 represents the anesthesia induction time, T1 means 1 h after T0; T2 means 2.5 hours after T0.
Figure 6.
Concentrations of IgM in EAP and CTR groups over time. T0 represents the anesthesia induction time, T1 means 1 h after T0; T2 means 2.5 hours after T0.
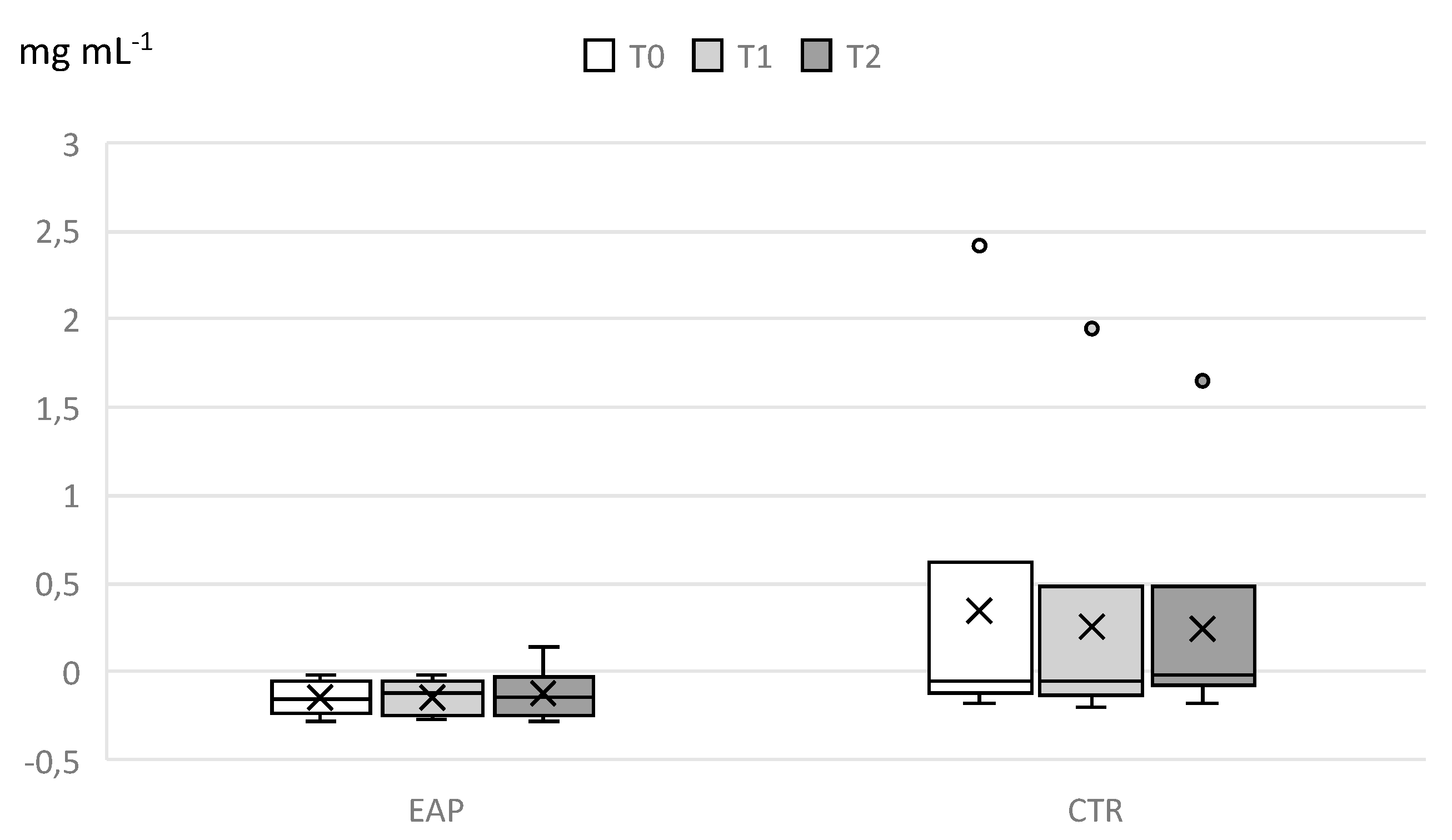
Figure 7.
Concentrations of IgA in EAP and CTR groups over time. T0: time of anesthesia induction, T1: 1 h after T0; T2: 2.5 hours after T0.
Figure 7.
Concentrations of IgA in EAP and CTR groups over time. T0: time of anesthesia induction, T1: 1 h after T0; T2: 2.5 hours after T0.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



