Submitted:
21 October 2023
Posted:
24 October 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Like all RNA viruses, SARS-CoV-2 shows high mutation rate, which has led to the emergence of new variants. Among them, Gamma and Delta developed at the turn of 2020-2021 in Amazonas and India, two ecoregions characterized by hot-humid weather, very similar to that of the summer season due to climate change in Italy, the first Western country to have been hit hard by COVID-19 and to experience lockdown restrictions in a democratic framework of 58,85 million people. Methods: during the state of national health emergency and the Draghi government, the Civil Defense Department daily released the aggregate data coming from the Ministry of Health, the Higher Institute of Health, the Independent Provinces and the Italian Regions, in order to inform about the pandemic situation in Italy. Among these data there were the number of deaths, hospitalizations in intensive care units (ICU), non-ICU patients, contagions, and performed swabs. By means of a team effort, we have collected and elaborated all these data, comparing COVID-19 pandemic in Italy during the summers 2020 (following the nationwide lockdown), 2021 and 2022. Results: from summer 2020 (before mass vaccination) to summers 2021 (after primary mass vaccination) and 2022 (after booster mass vaccination) all pandemic trend indicators have showed a sharp worsening in Italy. COVID-19 deaths increased by ≈298% and ≈834%, ICU hospitalizations by ≈386% and ≈310%, non-ICU hospitalizations by ≈224% and ≈600%, contagions by ≈627% and ≈6.850% (i.e. ≈68,50 times), swabs by ≈354% and ≈370%, and the mean positivity rate passed from ≈1% to ≈2% and ≈20%, respectively. Conclusions: SARS-CoV-2 can be transmitted in any climate, including areas with hot and humid weather, and the emergence of variants adapted to hot-humid climate may result in summer COVID-19 outbreaks, even in neither tropical nor subtropical countries. Although COVID-19 vaccines can confer cross-protection against newly emerging variants, this cross-immunity is obviously not absolute but limited, also taking into account that vaccine protection wanes considerably after 6 months. It follows that a subject vaccinated at the beginning of winter will not be completely covered in the height of summer, without forgetting the unvaccinated. As a final remark, the long nationwide lockdown made it possible to flatten SARS-CoV-2 circulation and, therefore, its negative impact on Italy during summer 2020.
Keywords:
COVID-19
; SARS-CoV-2
; SARS-CoV-2 Gamma variant
; SARS-CoV-2 Delta variant
; variant of concern (VOC)
; tropical and subtropical moist broadleaf forests (TSMF)
; vaccination
; booster dose
; lockdown
; Italy
1. Introduction
First identified at the end of 2019 in the city of Wuhan (Hubei, China), the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is a positive-sense single-stranded ribonucleic acid (RNA) virus, responsible for the ongoing coronavirus disease 2019 (COVID-19) pandemic. Like all RNA viruses, it shows high mutation rate compared to deoxyribonucleic acid (DNA) viruses, because viral RNA polymerase lack the proofreading ability of DNA polymerase [1]. This genetic instability of RNA viruses make difficult to produce long-lasting effective vaccines against them.
Since its discovery, many variants of SARS-CoV-2 have been emerged around the world as expected. The term ‘variant of concern’ (VOC) refers to any variant of the virus where mutations in the receptor-binding domain of the spike protein substantially increase the binding affinity with the human angiotensin-converting enzyme 2 (hACE2) receptors, such as to favor its rapid spread [2]. Before being allocated to this category, an emerging variant may have been labeled a ‘variant of interest’ (VOI) or, alternately as synonyms, ‘variant under investigation’ (VUI) or else ‘variant under monitoring’ (VUM) [3].
To date, five VOC have been detected and designated by the World Health Organization (WHO) following the order of the Greek-letters: Alpha, Beta, Gamma, Delta and Omicron [3]. As of September 2023, only Omicron is a circulating VOC according to the aforementioned WHO [3]. Among them, Gamma and Delta developed at the turn of 2020-2021 in Amazonas and India, hence the nicknames of “Brazilian” and “Indian” variants, respectively. These two ecoregions are characterized by hot-humid weather (Figure 1), very similar to that of the summer season due to climate change in Italy, the first Western country to have been hit hard by COVID-19 and to experience lockdown restrictions in a democratic framework of 58,85 million people [4].
2. Materials and Methods
During the state of national health emergency and the Draghi government (dissolved on 22 October 2022), the Civil Defense Department daily released the aggregate data coming from the Ministry of Health, the Higher Institute of Health, the Independent Provinces (Bolzano and Trento) and the Italian Regions (Abruzzo, Basilicata, Calabria, Campania, Emilia-Romagna, Friuli-Venezia Giulia, Lazio, Liguria, Lombardia, Marche, Molise, Piemonte, Puglia, Sardegna, Sicilia, Toscana, Umbria, Valle d’Aosta, and Veneto), in order to inform the population about the pandemic situation in Italy. Among these data, on a daily basis, there were the number of deaths, hospitalizations in intensive care units (ICU), non-ICU patients, contagions, and performed swabs.
By means of a team effort, we have collected all these data and elaborated the respective graphs, comparing the COVID-19 pandemic in Italy during summers 2020 (before mass vaccination), 2021 (after primary mass vaccination) and 2022 (after booster mass vaccination).
3. Results
3.1. COVID-19 deaths
In summers 2020 (20 June 2020–22 September 2020), 2021 (21 June 2021–22 September 2021) and 2022 (21 June 2022–23 September 2022) there were 1.085, 3.236 and 9.044 deaths due to COVID-19, respectively (Figure 2). This means that in summers 2021 and 2022 there were 2.151 and 7.959 more deaths than in summer 2020, which is equivalent to ≈2,98 and ≈8,34 times higher; in practice, from summer 2020 (before mass vaccination) to summers 2021 (after primary mass vaccination) and 2022 (after booster mass vaccination) there was an increase in deaths of ≈298% and ≈834%, respectively. The peak of deaths in summer 2020 (n. 49) occurred on 20 June 2020, while in summers 2021 (n. 75) and 2022 (n. 253) on 31 August 2021 and 26 July 2022 (Figure 2).
3.2. COVID-19 ICU hospitalizations
In summer 2020 the daily ICU hospitalizations due to COVID-19 averaged 91, with a peak of 239 ICU patients on 22 September 2020, while in summers 2021 and 2022 the daily ICU hospitalizations averaged 351 and 282, with a peak of 572 ICU patients on 5 September 2021 and of 434 ICU patients on 26 July 2022 (Figure 3). This means that in summers 2021 and 2022 the daily ICU hospitalization rate was ≈3,86 and ≈3,10 times higher than for summer 2020; in practice, from summer 2020 (before mass vaccination) to summers 2021 (after primary mass vaccination) and 2022 (after booster mass vaccination) the daily ICU hospitalization rate increased by ≈386% and ≈310%, respectively.
3.3. COVID-19 non-ICU hospitalizations
In summer 2020 the daily non-ICU hospitalizations due to COVID-19 averaged 1.198, with a peak of 2.604 non-ICU patients on 22 September 2020, while in summers 2021 and 2022 the daily non-ICU hospitalizations averaged 2.685 and 7.192, with a peak of 4.307 non-ICU patients on 7 September 2021 and of 11.124 non-ICU patients on 26 July 2022 (Figure 4). This means that in summers 2021 and 2022 the daily non-ICU hospitalization rate was ≈2,24 and ≈6,00 times higher than for summer 2020; in practice, from summer 2020 (before mass vaccination) to summers 2021 (after primary mass vaccination) and 2022 (after booster mass vaccination) the daily non-ICU hospitalization increased by ≈224% and ≈600%, respectively.
3.4. COVID-19 contagions
In summers 2020, 2021 and 2022 COVID-19 contagions were 62.540, 392.322 and 4.283.835 (Figure 5). This means that from summer 2020 (before mass vaccination) to summers 2021 (after primary mass vaccination) and 2022 (after booster mass vaccination) COVID-19 contagions increased by 329.782 and 4.221.295 subjects, an increase of ≈6,27 and ≈68,50 times equal to ≈627% and ≈6.850%, respectively. The peak of contagions in summer 2020 (n. 1.907) occurred on 18 September 2020, while in summers 2021 (n. 7.826) and 2022 (n. 142.967) on 27 August 2021 and 12 July 2022 (Figure 5).
3.5. COVID-19 swab tests
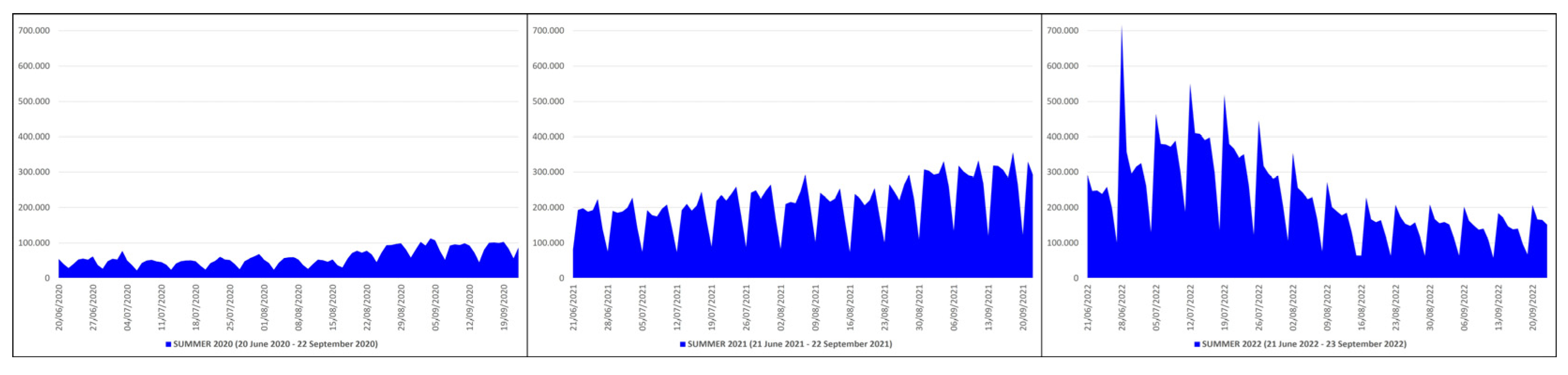
In summers 2020, 2021 and 2022 the swabs performed to detect COVID-19 were 5.717.867, 20.250.565 and 21.713.992 (Figure 6). This means that from summer 2020 (before mass vaccination) to summers 2021 (after primary mass vaccination) and 2022 (after booster mass vaccination) the swab tests increased by 14.532.698 and 15.996.125 units, an increase of ≈3,54 and ≈3,70 times equal to ≈354% and ≈370% more, respectively. The peak of performed tests in summer 2020 (n. 113.085) occurred on 4 September 2020, while in summers 2021 (n. 355.933) and 2022 (n. 717.400) on 18 September 2021 and 28 June 2022 (Figure 6).
4. Discussion
The spread of COVID-19 in Italy was first documented on 31 January 2020, when two Chinese tourists in Rome were found positive for the virus; one week later an Italian man, repatriated to Italy from Wuhan, was tested and hospitalized as the third case. From that day the situation worsened seriously, and the Italian government faced the sanitary emergency with a nationwide lockdown from 9 March 2020 to 3 May 2020 (included) [5]. Thanks to a record-breaking research network, new generation vaccines based on the Wuhan strain had been released at the beginning of 2021 [6], and health policies had been adopted to strongly encourage free mass vaccination. To date, almost 150 million doses have been administered in Italy, where a 90,25% and a 84,89% coverage of the population over 12 has been achieved with regards to the primary vaccination cycle (two doses) and to the booster dose (three doses), respectively [7].
The undoubtful efficacy of primary or booster COVID-19 vaccination in significantly reducing deaths and ICU/non-ICU hospitalizations in adults has been well demonstrated [8,9,10,11,12]. However, from summer 2020 (before mass vaccination) to summers 2021 (after primary mass vaccination) and 2022 (after booster mass vaccination) all pandemic trend indicators have showed a sharp worsening in Italy: COVID-19 deaths increased by ≈298% and ≈834%, ICU hospitalizations by ≈386% and ≈310%, non-ICU hospitalizations by ≈224% and ≈600%, contagions by ≈627% and ≈6.850% (i.e., ≈68,50 times), swabs by ≈354% and ≈370%, and the mean positivity rate passed from ≈1% to ≈2% and ≈20%, respectively.
A first explanation for these results certainly lies in the long nationwide lockdown that preceded summer 2020 but not summers 2021 and 2022, allowing the circulation of SARS-CoV-2 to be flattened during summer 2020; in fact, thanks to the advent of specific vaccines this drastic political measure was no longer adopted. Therefore, lockdown remains the most effective measure of health policy to stop the contagions, when specific or updated vaccines are not yet available, together with wearing mask indoors (preferably filtering face piece), practicing hand hygiene (with soap or hydroalcoholic solution), and keeping interpersonal social distancing (at least 1m).
Secondly, VOC suitable for hot-humid weather, very similar to that of summer season due to climate change in Italy, in particular around the Po basin, emerged from summer 2020 to summers 2021 and 2022, such as Gamma and Delta variants [3]. COVID-19 virulence has been found maximum <10 °C and <40 kJ/m2 or >60% humidity (≈70%) [13,14,15]. This behavior towards environmental temperature, solar ultraviolet radiation or relative humidity explains the reason why SARS-CoV-2 can be transmitted in any climate, including areas with hot and humid weather as stated by the WHO [16], and it is quite similar to that of other respiratory virosis, in primis influenza [17,18]. In Italy, these conditions are typical of autumn-winter (<10 °C and <40 kJ/m2) or summer (>60% humidity); therefore, summer outbreaks should not come as a surprise even in neither tropical nor subtropical countries, especially in front of VOC adapted to hot-humid climate.
Thirdly, the mass vaccination campaign in Italy was implemented with vaccines based on the Wuhan strain; although vaccines developed with an antigen from a non-predominant ancestral strain can confer cross-protection against newly emerging variants of the coronavirus and vice versa [19,20], this cross-immunity is obviously not absolute but limited [21,22]. Moreover, vaccine efficacy or effectiveness against SARS-CoV-2 infection decreases from 1 month to 6 months after full vaccination by 21,0% on average (95% CI: 13,9-29,8) among people of all ages, and by 20,7% (95% CI: 10,2-36,6) among older people (at least 50 years old), until to wane considerably after 6 months [23,24]. It follows that a subject vaccinated at the beginning of winter will not be completely covered in the height of summer. Unfortunately, the available data do not allow us to know in what proportion the surge in the number of deaths, ICU/non-ICU hospitalizations and contagions from summer 2020 to summers 2021 and 2022 affected the 90,25% and the 84,89% of the population over 12 vaccinated with two or three doses, and the remaining 9,75% and 15,11%, nor do they allow us to evaluate any differences among subjects vaccinated with different types of vaccines (mRNA, subunit, viral vector).
5. Conclusion
In the future, it is possible that similar summer outbreaks will be repeated even if with numbers that are unlikely to reach those of the autumn-winter season, and such as to send the healthcare system into a tailspin.
Author Contributions
Conceptualization, L.R.; methodology, L.R.; software, L.R., G.B. and C.G.; validation, S.C.; formal analysis, L.R., G.B. and C.G.; investigation, L.R., G.B. and C.G.; resources, G.B. and C.G.; data curation, L.R.; writing—original draft preparation, L.R.; writing—review and editing, L.R.; visualization, S.C.; supervision, L.R. and S.C.; project administration, L.R. and S.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Publicly available datasets were analyzed in this study; further requests for data should be addressed to the corresponding author.
Acknowledgments
The authors thank the Civil Defense Department of the Italian Republic, the Ministry of Health, the Higher Institute of Health, the National Institute of Statistics, the Independent Provinces (Bolzano and Trento) and all the Italian Regions (Abruzzo, Basilicata, Calabria, Campania, Emilia-Romagna, Friuli-Venezia Giulia, Lazio, Liguria, Lombardia, Marche, Molise, Piemonte, Puglia, Sardegna, Sicilia, Toscana, Umbria, Valle d’Aosta, and Veneto) for data sharing and press releases.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Markov, P.V.; Ghafari, M.; Beer, M.; Lythgoe, K.; Simmonds, P.; Stilianakis, N.I.; Katzourakis, A. The evolution of SARS-CoV-2. Nat Rev Microbiol 2023, 21, 361-379. [CrossRef]
- Shahhosseini, N.; Babuadze, G.G.; Wong, G.; Kobinger, G.P. Mutation signatures and in silico docking of novel SARS-CoV-2 variants of concern. Microorganisms 2021, 9, 926. [CrossRef]
- World Health Organization. Tracking SARS-CoV-2 variants. Available online: https://www.who.int/en/activities/tracking-SARS-CoV-2-variants/(accessed on 30 September 2023).
- Italian Institute of Statistics. Demographic indicators ‒ year 2022. Available online: https://www.istat.it/it/files//2023/04/indicatori-anno-2022.pdf (accessed on 7 April 2023).
- Official Gazette of the Italian Republic. Special edition (year 161st ‒ number 62). Available online: https://www.gazzettaufficiale.it/eli/gu/2020/03/09/62/sg/pdf (accessed on 9 March 2020).
- Roncati, L.; Corsi, L. Nucleoside-modified messenger RNA COVID-19 vaccine platform. J Med Virol 2021, 93, 4054-4057. [CrossRef]
- Italian Government. Anti COVID-19 vaccines report. Available online: https://www.governo.it/it/cscovid19/report-vaccini/(accessed on 30 September 2023).
- Havers, F.P.; Pham, H.; Taylor, C.A.; Whitaker, M.; Patel, K.; Anglin, O.; Kambhampati, A.K.; Milucky, J.; Zell, E.; Moline, H.L.; Chai, S.J.; Kirley, P.D.; Alden, N.B.; Armistead, I.; Yousey-Hindes, K.; Meek, J.; Openo, K.P.: Anderson, E.J.; Reeg, L.; Kohrman, A.; Lynfield, R.; Como-Sabetti, K.; Davis, E.M.; Cline, C.; Muse, A.; Barney, G.; Bushey, S.; Felsen, C.B.; Billing, L.M.; Shiltz, E.; Sutton, M.; Abdullah, N.; Talbot, H.K.; Schaffner, W.; Hill, M.; George, A.; Hall, A.J.; Bialek, S.R.; Murthy, N.C.; Murthy, B.P.; McMorrow, M. COVID-19-associated hospitalizations among vaccinated and unvaccinated adults 18 years or older in 13 US states, January 2021 to April 2022. JAMA Intern Med 2022, 182, 1071-1081. [CrossRef]
- Thomas, S.J.; Moreira, E.D. Jr; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Polack, F.P.; Zerbini, C.; Bailey, R.; Swanson, K.A.; Xu, X.; Roychoudhury, S.; Koury, K.; Bouguermouh, S.; Kalina, W.V.; Cooper, D.; Frenck, R.W. Jr; Hammitt, L.L.; Türeci, Ö.; Nell, H.; Schaefer, A.; Ünal, S.; Yang, Q.; Liberator, P.; Tresnan, D.B.; Mather, S.; Dormitzer, P.R.; Şahin, U.; Gruber, W.C.; Jansen, K.U. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine through 6 months. N Engl J Med 2021, 385, 1761-1773. [CrossRef]
- Moreira, E.D. Jr; Kitchin, N.; Xu, X.; Dychter, S.S.; Lockhart, S.; Gurtman, A.; Perez, J.L.; Zerbini, C.; Dever, M.E.; Jennings, T.W.; Brandon, D.M.; Cannon, K.D.; Koren, M.J.; Denham, D.S.; Berhe, M.; Fitz-Patrick, D.; Hammitt, L.L.; Klein, N.P.; Nell, H.; Keep, G.; Wang, X.; Koury, K.; Swanson, K.A.; Cooper, D.; Lu, C.; Türeci, Ö.; Lagkadinou, E.; Tresnan, D.B.; Dormitzer, P.R.; Şahin, U.; Gruber, W.C.; Jansen, K.U. Safety and efficacy of a third dose of BNT162b2 Covid-19 vaccine. N Engl J Med 2022, 386, 1910-1921. [CrossRef]
- Arbel, R.; Hammerman, A.; Sergienko, R.; Friger, M.; Peretz, A.; Netzer, D.; Yaron, S. BNT162b2 vaccine booster and mortality due to Covid-19. N Engl J Med 2021, 385, 2413-2420. [CrossRef]
- Tartof, S.Y.; Slezak, J.M.; Fischer, H.; Hong, V.; Ackerson, B.K.; Ranasinghe, O.N.; Frankland, T.B.; Ogun, O.A.; Zamparo, J.M.; Gray, S.; Valluri, S.R.; Pan, K.; Angulo, F.J.; Jodar, L.; McLaughlin, J.M. Effectiveness of mRNA BNT162b2 COVID-19 vaccine up to 6 months in a large integrated health system in the USA: a retrospective cohort study. Lancet 2021, 398, 1407-1416. [CrossRef]
- Ma, Y.; Pei, S.; Shaman, J.; Dubrow, R.; Chen, K. Role of meteorological factors in the transmission of SARS-CoV-2 in the United States. Nat Commun 2021, 12, 3602. [CrossRef]
- Balboni, E.; Filippini, T.; Rothman, K.J.; Costanzini, S.; Bellino, S.; Pezzotti, P.; Brusaferro, S.; Ferrari, F.; Orsini, N.; Teggi, S.; Vinceti, M. The influence of meteorological factors on COVID-19 spread in Italy during the first and second wave. Environ Res 2023, 228, 115796. [CrossRef]
- Verheyen, C.A.; Bourouiba, L. Associations between indoor relative humidity and global COVID-19 outcomes. J R Soc Interface 2022, 19, 20210865. [CrossRef]
- World Health Organization. Coronavirus disease (COVID-19) advice for the public: myth busters. Available online: https://www.who.int/images/default-source/health-topics/coronavirus/myth-busters/52.png?sfvrsn=862374e_12 (accessed on 19 January 2022).
- Park, J.E.; Son, W.S.; Ryu, Y.; Choi, S.B.; Kwon, O.; Ahn, I. Effects of temperature, humidity, and diurnal temperature range on influenza incidence in a temperate region. Influenza Other Respir Viruses 2020, 14, 11-18. [CrossRef]
- Neumann, G.; Kawaoka, Y. Seasonality of influenza and other respiratory viruses. EMBO Mol Med 2022, 14, e15352. [CrossRef]
- Dangi, T.; Palacio, N.; Sanchez, S.; Park, M.; Class, J.; Visvabharathy, L.; Ciucci, T.; Koralnik, I.J.; Richner, J.M.; Penaloza-MacMaster, P. Cross-protective immunity following coronavirus vaccination and coronavirus infection. J Clin Invest 2021, 131, e151969. [CrossRef]
- Shen, K.Y.; Yang, C.H.; Chen, C.T.; Ho, H.M.; Chiu, F.F.; Huang, C.Y.; Liao, H.C.; Hsu, C.W.; Yu, G.Y.; Liao, C.L.; Chen, H.W.; Huang, M.H.; Liu, S.J. Omicron-specific mRNA vaccine induced cross-protective immunity against ancestral SARS-CoV-2 infection with low neutralizing antibodies. J Med Virol 2023, 95, e28370. [CrossRef]
- Suryawanshi, R.K.; Chen, I.P.; Ma, T.; Syed, A.M.; Brazer, N.; Saldhi, P.; Simoneau, C.R.; Ciling, A.; Khalid, M.M.; Sreekumar, B.; Chen, P.Y.; Kumar, G.R.; Montano, M.; Gascon, R.; Tsou, C.L.; Garcia-Knight, M.A.; Sotomayor-Gonzalez, A.; Servellita, V.; Gliwa, A.; Nguyen, J.; Silva, I.; Milbes, B.; Kojima, N.; Hess, V.; Shacreaw, M.; Lopez, L.; Brobeck, M.; Turner, F.; Soveg, F.W.; George, A.F.; Fang, X.; Maishan, M.; Matthay, M.; Morris, M.K.; Wadford, D.; Hanson, C.; Greene, W.C.; Andino, R.; Spraggon, L.; Roan, N.R.; Chiu, C.Y.; Doudna, J.A.; Ott, M. Limited cross-variant immunity from SARS-CoV-2 Omicron without vaccination. Nature 2022, 607, 351-355. [CrossRef]
- Bruxvoort, K.J.; Sy, L.S.; Qian, L.; Ackerson, B.K.; Luo, Y.; Lee, G.S.; Tian, Y.; Florea, A.; Aragones, M.; Tubert, J.E.; Takhar, H.S.; Ku, J.H.; Paila, Y.D.; Talarico, C.A.; Tseng, H.F. Effectiveness of mRNA-1273 against delta, mu, and other emerging variants of SARS-CoV-2: test negative case-control study. BMJ 2021, 375, e068848. [CrossRef]
- Feikin, D.R.; Higdon, M.M.; Abu-Raddad, L.J.; Andrews, N.; Araos, R.; Goldberg, Y.; Groome, M.J.; Huppert, A.; O’Brien, K.L.; Smith, P.G.; Wilder-Smith, A.; Zeger, S.; Deloria Knoll, M.; Patel, M.K. Duration of effectiveness of vaccines against SARS-CoV-2 infection and COVID-19 disease: results of a systematic review and meta-regression. Lancet 2022, 399, 924-944. [CrossRef]
- Hall, V.; Foulkes, S.; Insalata, F.; Kirwan, P.; Saei, A.; Atti, A.; Wellington, E.; Khawam, J.; Munro, K.; Cole, M.; Tranquillini, C.; Taylor-Kerr, A.; Hettiarachchi, N.; Calbraith, D.; Sajedi, N.; Milligan, I.; Themistocleous, Y.; Corrigan, D.; Cromey, L.; Price, L.; Stewart, S.; de Lacy, E.; Norman, C.; Linley, E.; Otter, A.D.; Semper, A.; Hewson, J.; D’Arcangelo, S.; Chand, M.; Brown, C.S.; Brooks, T.; Islam, J.; Charlett, A.; Hopkins, S. Protection against SARS-CoV-2 after Covid-19 vaccination and previous infection. N Engl J Med 2022, 386, 1207-1220. [CrossRef]
Figure 1.
World map of tropical and subtropical moist broadleaf forests (TSMF) ecoregions (dark green), particularly present around the Amazon basin and Congo basin, in the Caribbean and Madagascar, and in the Southeast Asia and Indian subcontinent.
Figure 1.
World map of tropical and subtropical moist broadleaf forests (TSMF) ecoregions (dark green), particularly present around the Amazon basin and Congo basin, in the Caribbean and Madagascar, and in the Southeast Asia and Indian subcontinent.
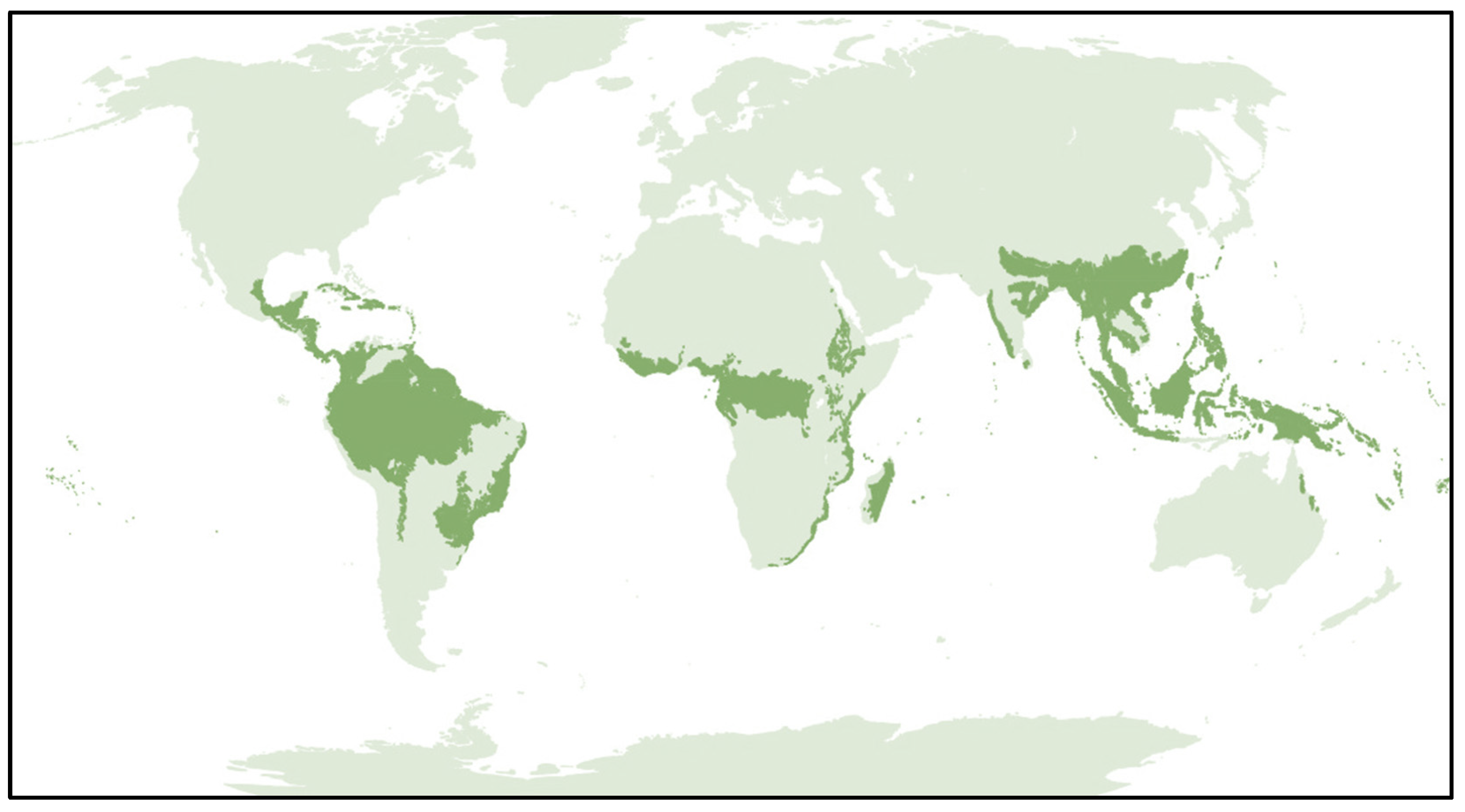
Figure 2.
COVID-19 deaths in Italy during summers 2020 (20 June 2020–22 September 2020), 2021 (21 June 2021–22 September 2021) and 2022 (21 June 2022–23 September 2022) [X axis: days; Y axis: number of deaths].
Figure 2.
COVID-19 deaths in Italy during summers 2020 (20 June 2020–22 September 2020), 2021 (21 June 2021–22 September 2021) and 2022 (21 June 2022–23 September 2022) [X axis: days; Y axis: number of deaths].
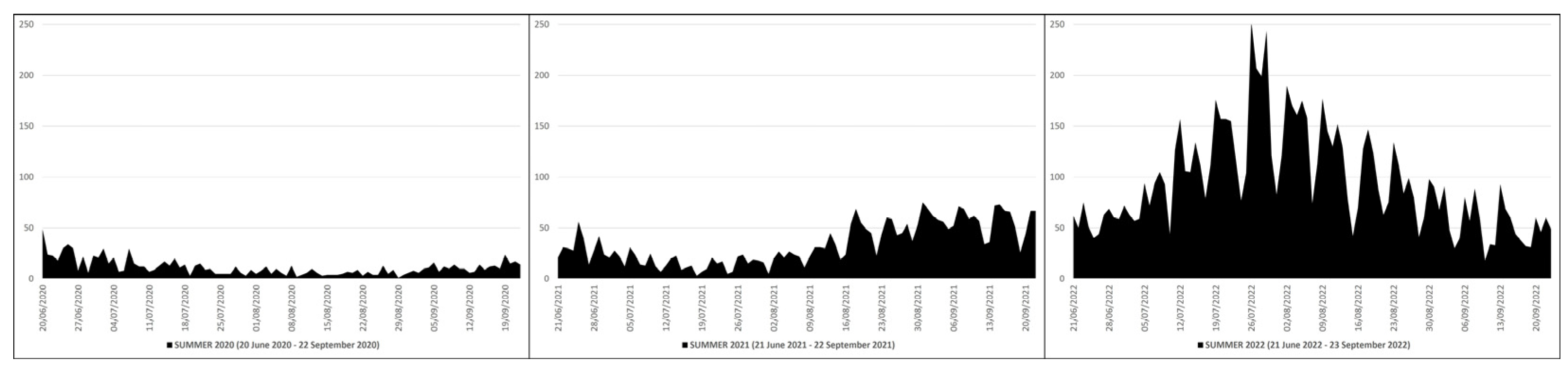
Figure 3.
COVID-19 ICU hospitalizations in Italy during summers 2020 (20 June 2020–22 September 2020), 2021 (21 June 2021–22 September 2021) and 2022 (21 June 2022–23 September 2022) [X axis: days; Y axis: number of ICU hospitalizations].
Figure 3.
COVID-19 ICU hospitalizations in Italy during summers 2020 (20 June 2020–22 September 2020), 2021 (21 June 2021–22 September 2021) and 2022 (21 June 2022–23 September 2022) [X axis: days; Y axis: number of ICU hospitalizations].
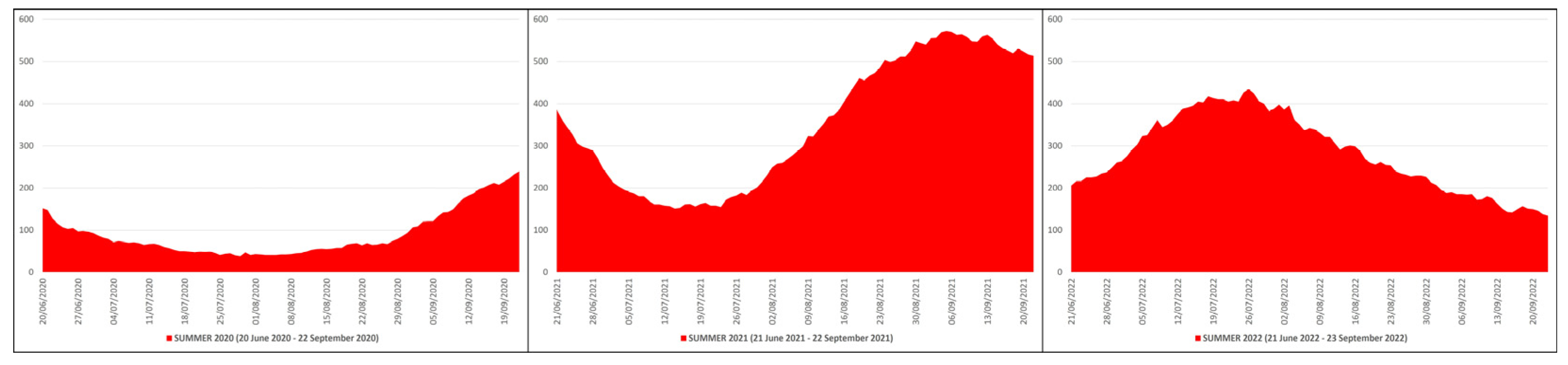
Figure 4.
COVID-19 non-ICU hospitalizations in Italy during summers 2020 (20 June 2020–22 September 2020), 2021 (21 June 2021–22 September 2021) and 2022 (21 June 2022–23 September 2022) [X axis: days; Y axis: number of non-ICU hospitalizations].
Figure 4.
COVID-19 non-ICU hospitalizations in Italy during summers 2020 (20 June 2020–22 September 2020), 2021 (21 June 2021–22 September 2021) and 2022 (21 June 2022–23 September 2022) [X axis: days; Y axis: number of non-ICU hospitalizations].
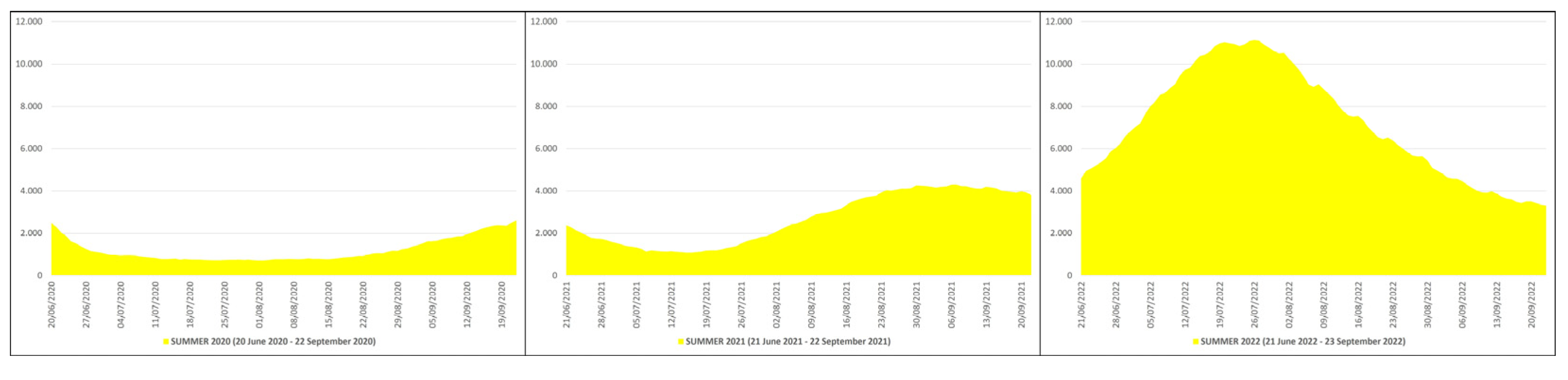
Figure 5.
COVID-19 contagions in Italy during summers 2020 (20 June 2020–22 September 2020), 2021 (21 June 2021–22 September 2021) and 2022 (21 June 2022–23 September 2022) [X axis: days; Y axis: number of contagions].
Figure 5.
COVID-19 contagions in Italy during summers 2020 (20 June 2020–22 September 2020), 2021 (21 June 2021–22 September 2021) and 2022 (21 June 2022–23 September 2022) [X axis: days; Y axis: number of contagions].
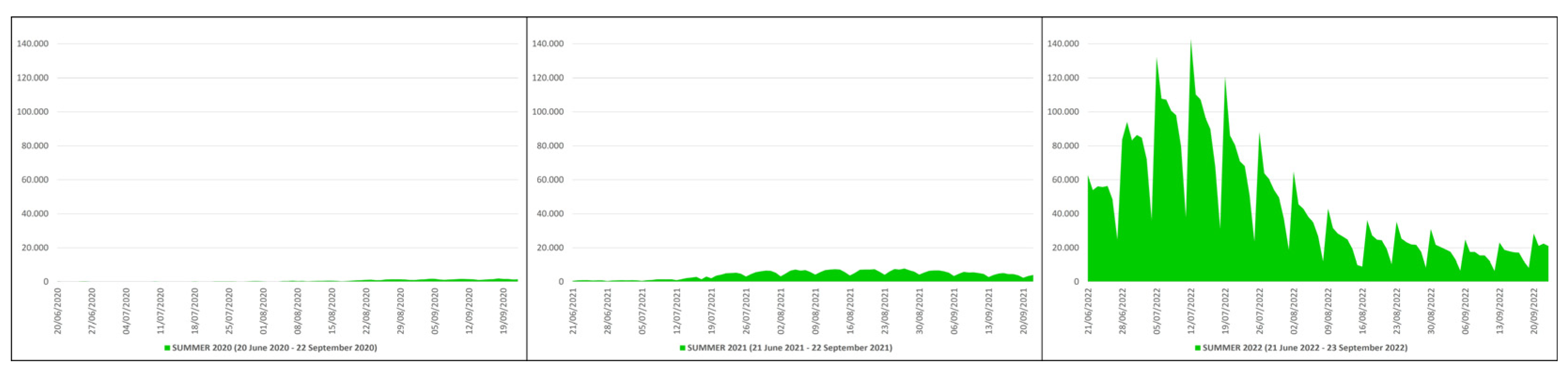
Figure 6.
COVID-19 swab tests in Italy during summers 2020 (20 June 2020–22 September 2020), 2021 (21 June 2021–22 September 2021) and 2022 (21 June 2022–23 September 2022) [X axis: days; Y axis: number of swabs].
Figure 6.
COVID-19 swab tests in Italy during summers 2020 (20 June 2020–22 September 2020), 2021 (21 June 2021–22 September 2021) and 2022 (21 June 2022–23 September 2022) [X axis: days; Y axis: number of swabs].
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



