Submitted:
09 October 2023
Posted:
09 October 2023
You are already at the latest version
Abstract
Diabetes mellitus (DM) and chronic kidney disease (CKD) are common in middle aged and elderly individuals. DM may accelerate the aging process, and the age-related declines in the estimated Glomerular Filtration Rate (eGFR), can pose a challenge to diagnose diabetic kidney disease (DKD) using standard diagnostic criteria especially with absence of severe albuminuria among the elderly. In the presence of CKD and DM, elderly patients may need multidisciplinary care due to susceptibility to various health issues e.g., cognitive decline, auditory or visual impairment, various comorbidities, complex medical regimens, and increased sensitivity to medication adverse effects. As a result, it can be challenging to apply recent therapeutic advancements for the general population to the elderly. We review the evidence that the benefits from these newer therapies apply equally to elderly and non-elderly patients and propose a framework for the management of DKD by discussing the nonpharmacological measures and pharmacological management with renin angiotensin system inhibitors (RASi), Sodium Glucose Co-Transporter two inhibitors (SGLT2i), non-steroidal mineralocorticoids receptor antagonists (MRAs), and Glucagon Like Peptide 1 Receptor Agonists (GLP1-RAs).
Keywords:
Diabetes
; Chronic Kidney Disease
; Treatment
; Elderly
; Geriatric
; Dialysis
; SGLT2 inhibitors
; GLP1 Receptor Agonists
; Non-steroidal Mineralocorticoid Antagonists
1. Introduction
Diabetes mellitus (DM) and chronic kidney disease (CKD) pose substantial challenges for the elderly patients. Historically known as Diabetic Nephropathy (DN), CKD attributed to DM is often referred to as Diabetic Kidney Disease (DKD) and is the major cause of CKD and end-stage kidney disease (ESKD) in those over 60 years old [1]. Furthermore, a third of new ESKD cases in those over 75 years old are attributed to DKD, often without a histologic diagnosis. For those individuals the more appropriate term is Diabetes in CKD [2], a term that reflects the complex and often multifactorial pathogenesis of CKD in individuals with diabetes. This form of CKD is increasingly not associated with proteinuria [3,4,5,6] and conversely the presence of proteinuria or CKD in an elderly patient with DM is not always due to DN or DKD.
Providing care in elderly individuals with DM and CKD is challenging because of the substantial comorbidity burden, and the co-existence of physical and mental conditions such as dementia [7]. Multidisciplinary medical management may be required due to these concomitant conditions, and the application of emerging evidence based therapies should neither be reflexively applied nor arbitrarily withheld.
While guidelines have incorporated fixed, age-independent referral criteria to nephrology, elderly patients may benefit less from nephrology referral than younger individuals [8], while the likelihood of regression, i.e., a spontaneous improvement in kidney filtration often exceeds the likelihood of progression [9]. This creates challenges in translating interventions which are often tested in populations with some degree of proteinuria to those patients with (near-) normoalbuminuria. However, recent advancements in DKD therapy are applicable to both old and non-elderly patients and confer broad cardiovascular benefits (e.g. on cardiovascular disease or heart failure) that may be particularly applicable to elderly patients with multiple comorbidities. Furthermore, these newer therapies are extremely easy to apply and can be used in a pillars of therapy approach by either primary care providers or specialists, offering unique opportunities to improve the outlook of elderly patients with DM and CKD.
2. Definition, Epidemiology and Burden of Diabetes in Elderly patients with CKD
CKD is defined as either a persistent estimate GFR < 60 ml/min/1.73m2 and/or evidence of kidney damage (most commonly albuminuria). Based on this definition and using NHANES data an estimated 14% of the adult population has CKD, however the prevalence is 33.2% in those 65 years old and older. The epidemiology of CKD seems to vary with age, in that CKD determined by low eGFR alone (< 60) is more common in the elderly than in younger populations. Furthermore, the association of low GFR with mortality and ESKD in the elderly while still present is less pronounced in older individuals[10] . Nevertheless, the implications of CKD on the health of older indviduals remains profound given how commonly it occurs. Among US adults with CKD 35.6% have diabete mellitus
CKD in DM predates the development of ESKD among patients with type II DM [3] and is considered a problem of pandemic dimensions [11], as a result of the increasing rates of DM and obesity. Sequential analyses of the National Health and Nutrition Examination Survey (NHANES analysis: 2003-2004 vs. 2013-2014) showed that the estimated frequency of DM increased by 9 million, affecting 30.2 (13%) million US adults [3]. The 2020 updated National Diabetes Statistics that examined data from 2013-2018 suggests very little improvement in this figure [12]. According to the National Diabetes Statistics report (10), the prevalence of diagnosed and total DM among people over the age of 65 in the United States was 21.4% and 26.8%, respectively. These worrisome trends are not US specific; the International Diabetes Federation Atlas [13] projects an increasing trend of DM up to 2045. The NHANES analyses also showed very little change in the prevalence of CKD as defined by a persistent urine albumin-to-creatinine ratio of ≥30 mg/g, or a persistent estimated Glomerular Filtration Rate [eGFR] of <60 mL/min per 1.73 m2, from 28.4% (1988 to 1994) vs. 26.2% from 2009 to 2014.
The higher rates of DM pose a significant threat to the falling incidence rates of ESKD observed in recent years[14]. While improvements in the overall standards of care could reduce the risk of a single individual to experience worsening of their kidney function to the point they need dialysis or transplant, the overall number of patients needing renal replacement therapy may increase if more patients develop DM. Analyses in NHANES [3] and in non-US cohorts [15] suggest that this epidemiological trend may be particularly relevant for the elderly patients since those older than 65-year-old are 35% more likely to manifest albuminuria than those younger than 65 (32.3% vs 23.9%, NHANES estimate). Prior to the COVID19 pandemic, these trends were expected to lead to a rising prevalence in the ESKD from 2015 to 2030 [16]. African Americans, Hispanic Americans and American Indians [3], may exhibit even higher rates of CKD and DM in CKD[17], and these disparities carried to self-management of DM among elderly Medicare beneficiaries [18].
3. Pathophysiology of CKD in DM among the elderly
The natural aging process in the kidney shares histopathologic findings e.g. sclerosis, mesangial matrix expansion, tubular and glomerular basement thickening and interstitial atrophy and fibrosis [19] with those observed in CKD in DM (Table 1), suggesting shared but not identical pathophysiology.
Hyperfiltration is thought to proceed the functional loss of nephrons in DN, however in “normal aging” this loss [23], is not accompanied by a rise in single nephron GFR [24,25]. Genetic studies have shown that loci linked to albuminuria in aging mice and diabetic people are partially overlapping [26]. Accelerated senescence in tubular cells (primarily) and podocytes (secondarily) has been shown in kidney biopsies from patients with DN and type II DM [27]. Furthermore, these senescent cells secrete a variety of mediators (e.g. proinflammatory cytokines, complement component and pro-fibrotic factors) that drive glomerulosclerosis, podocyte hypertrophy, mesangial changes and tubulointerstitial fibrosis observed in DKD [28]. Advanced Glycosylation End products (AGEs) and the RAGR (cell surface receptor of AGEs) accumulate in both diabetic and senescent kidneys [29], where they promote oxidation and inflammation [30,31], thus increasing the likelihood of age- and diabetic-related CKD [32]. A recent review of the molecular pathways underlying the progression of DKD in the elderly [33] revealed a complex interplay between oxidative stress, inflammation, and hyperglycemia.
The final common pathway linking inflammation and tissue fibrosis in CKD may be mediated through the aberrant activation of the mineralocorticoid receptor, an observation that is more than eighty years old [34]. Mineralocorticoid receptor activation links tissue injury, oxidative stress, inflammation, arterial hypertension, and end organ damage of the heart, blood vessels and the kidneys [35,36,37].
While kidney biopsies are not typically obtained to diagnose DKD or DN, but to exclude other non-diabetic forms of kidney injury, if diabetic lesions are obtained they should be staged in both the Glomerular and the Vascular/Tubulointerstitial Compartments [20]. Due to the shared histology and pathophysiology the cause of the lesions observed in biopsies of patients with DM cannot be unequivocally assigned to the latter. For example renal artery stenosis (RAS) and secondary kidney ischemia [38] may lead to intrarenal arterial hyalinosis [39]. While efferent arteriolar hyalinosis is typically associated with a diabetic kidney lesion, afferent arteriolar hyalinosis may be observed in hypertensive nephropathy. Normoalbuminuric kidney disease in elderly CKD patients with DM, and this clinical phenotype may be associated with non-glomerular lesions [40,41] or the use of inhibitors of the renin angiotensin system [3,42,43,44].
4. Diagnosis of CKD in the elderly patients with DM
The diagnostic criteria for CKD do not vary by change, i.e., either a depressed eGFR or an elevated index of protein excretion in the urine (usually the microalbumin to creatinine ratio) as a marker of kidney damage should be demonstrated for diagnosis and staging of CKD. In caring for individual patients, the potential for an age-related loss of kidney function should also be considered as a potential cause of a reduced eGFR value in the absence of albuminuria. One cohort study was conducted in Canada with a considerable representation of cohorts > 65 years old and compared the implications of age-adapted vs. fixed eGFR on the 5-year risk of renal failure and death. They identified a similar difference in the 5-year absolute risk of kidney failure (0.12%) among individuals 65 years and older who had an eGFR of 45–60 mL/min/1.73 at baseline and no detectable proteinuria compared to non-CKD patients[45]. Proposals for an age-adapted definition of CKD [46], by adopting a threshold of <45 ml/min/1.73m2 instead of the <60 ml/min/1.73m2 have not gained traction and thus the fixed age-independent threshold of 60 ml/min/1.73m2 should be applied initially. Albuminuria is never a manifestation of “normal aging” and its presence signifies an elevated risk for progression of CKD, endothelial dysfunction, need for dialysis and cardiovascular morbidity and mortality [47,48,49]. For the elderly individual with DM, who is at risk for other forms of kidney disease (e.g., vasculitis), the initial diagnostic step is to exclude a non-diabetic kidney lesion. In particular, if the diagnosis of CKD predates the diagnosis of DM or occurs within a short period of time (5-10 years), then the risk for another kidney disorder is particularly high [50].
The initial workup should not differ for elderly and younger patients and includes a urinalysis, Urine Albumin to Creatinine Ratio (UACR), an eGFR, a complete blood count and a basic metabolic profile that incorporates measurements of sodium, potassium, bicarbonate, calcium, and phosphorus. Serological tests as per the guidance of the US National Institute for Diabetes, Digestive and Kidney Diseases include tests for chronic hepatitis B and C, antinuclear antibodies, rheumatoid factor, complement levels (C3/C4), serum and urine protein electrophoresis, a free light chain assay. A kidney ultrasound is also part of the workup and can be used to diagnose bona fide urinary outflow obstruction (e.g., hydronephrosis), or subtler forms of bladder dysfunction (e.g., an elevated postvoid residual urinary volume in the bladder). If a patient with DM has typical and advanced retinopathy [51,52,53,54], albuminuria and a negative serologic evaluation, most clinicians would not proceed to obtain a kidney biopsy. In the elderly patient, vascular disease (e.g. due to atherosclerosis, hypertension, and RAS) [38,55] may also be present, and such conditions may be used to diagnose the patient with cardiovascular disease and target them for high intensity therapy to reduce cardiovascular risk. At the time of this writing, a precise histological diagnosis of DKD is not required to initiate therapies such as inhibitors of the renin angiotensin system or sodium glucose co-transporter two inhibitors, whose spectrum of indications include both diabetic and non-diabetic kidney lesions. However, a missed glomerular diagnosis does not allow the initiation of specific therapy that may preserve kidney function or prevent damage to other organs (e.g., due to vasculitis). Since the histology cannot be predicted from clinical criteria [56] and a definitively higher risk of bleeding is not seen in the elderly [57,58,59], it may be reasonable to apply the same “atypical feature” [60,61,62,63] criteria for pursuing a kidney biopsy as in the young (Table 2).
5. Treatment Considerations
The general approach to treating CKD in DM in the elderly is not different than the one applied to younger individuals, though the elements should be highly individualized in order to account for other medical problems and comorbidities with advancing age. When approaching any patient with CKD, the overarching aim is to control the risks of both cardiovascular disease and kidney disease progression, as most patients are more likely to experience a cardiovascular event than needing dialysis [64,65]. The components of this approach include lifestyle changes (smoking cessation, a healthy lifestyle that includes exercise preferably longer than 150 minutes weekly), reduction in sodium intake (to less than 2 grams every day) and avoiding extreme protein intakes (e.g., 0.8gm/kg/d is a reasonable goal), and active pharmaceutical interventions to control blood pressure, glycemia, atherosclerotic cardiovascular risk and specific antiproteinuric and antifibrotic therapies.
5.1. Non-Pharmaceutical interventions and goals of therapy
5.1.1. Exercise
An individualized, planned and supervised combination of aerobic and resistance training is considered the most effective way to control glycemia [66]. Contraindications to exercise stem from specific comorbidities (e.g. proliferative retinopathy, aneurysms, severe autonomic insufficiency with propensity for hypoglycemia) and are often temporary in nature (e.g. during an acute exacerbation of ischemia, heart failure or hypertensive event and periods of poor glycemic control with propensity to hypoglycemia) [67]. Tailoring the prescription of exercise program to the functional capacity limitations of the individual can be achieved through the Vivifrail multicomponent exercise program [68].
5.1.2. Dietary Considerations
Sodium restriction to less than 2g a day improves hypertension and the efficacy of antihypertensive medications. When dietary intake of fresh vegetables is poor, increasing levels of sodium intake has been associated with increased incidence of diabetic retinal disease [69]. A DASH diet can improve hypertension control, but can lead to hyperkalemic episodes in individuals with hyporeninemic hypoaldosteronism. Current American Diabetes Association (ADA) guidelines suggest limiting protein intake to 0.8-1.0 g/kg/day in those with DM and CKD. Nevertheless, studies on dietary protein restriction have failed to show a clear benefit in reducing the progression of DKD [55,70,71]. One should be aware that this target conflicts with that in the guideline for geriatric adults that recommend a target protein intake of 1-1.2g/kg to prevent malnutrition and sarcopenia in old age [72]. The benefit (progression of CKD) to risk (developing protein – energy wasting) should be carefully balanced to when prescribing low protein diets in elderly adults with advanced CKD. This balancing act should consider the presence of pre-existing malnutrition, rate of progression of CKD, CKD stage and the presence of comorbidities/anticipated life expectancy which would shift the focus towards quality, rather than quantity of life and dialysis avoidance. An approach that attempts to reconcile guidelines and prioritize goals distinguishes between “nutritional-geriatric” priorities (age is the dominant factor) vs. “renal” priority (when the patient’s goal would be to avoid dialysis at any cost, emphasizing that these priorities may shift during periods of critical illness [73]. Implementing nutritional therapies should be done in a stepwise manner: first, a nutritional assessment with a validated tool should take place and if the patient screens positive for protein-energy malnutrition, a formal assessment with the Subjective Global Assessment (SGA), second an on-going evaluation of muscle mass and function during the implementation of dietary restrictions to detect early development of sarcopenia and protein-energy malnutrition that would limit the continuation of such diets [73].
5.1.3. Blood Pressure, Lipid and Glycemia Control in the Elderly with CKD in DM
The ADA standards of care in DM [74] framework considers blood pressure, glycemic control and lipids together and this is integrative, comprehensive approach provides a solid base to approach the elderly individual with CKD in DM. This framework acknowledges that tight glycemic control comes with higher risks [75,76,77,78,79] in such individuals due to a non-robust physiologic response to hypoglycemia and greater hypoglycemia unawareness. That framework progressively de-escalates the aggressiveness of goal directed therapy as the number of pre-existing conditions (those severe enough to require medication or lifestyle management) advance to end-stage chronic illness. The blood pressure targets that the ADA proposes differ from those in the KDIGO guidelines [80] which are heavily influenced by the SPRINT trial [81]. However, even the KDIGO guidelines point out that the benefits of tight blood pressure control is less certain in those with DM, advanced (stages 4 and 5) CKD and the very old (individuals older than 90). Hence for the elderly patients with DM and CKD who find themselves at the intersection of these groups, shared decision making and individualized goal setting that minimizes the side effects of therapy and their effect on quality of life should take precedence over a “one-size-fits-all” blood pressure target.

Table 3.
Targets of anti-hypertensive, glycemic and lipid therapy in the elderly patient with CKD in diabetes.
Table 3.
Targets of anti-hypertensive, glycemic and lipid therapy in the elderly patient with CKD in diabetes.
| Healthy | Complex | Very Complex | |
|---|---|---|---|
| Patient Characteristics Health Status |
Few coexisting chronic illnesses AND intact cognitive and functional status |
At least 3 coexisting chronic illnesses OR 2+ instrumental ADL impairments OR mild-to-moderate cognitive impairment |
Long Term Care facility resident OR end-stage chronic illnesses OR moderate-to-severe cognitive impairment OR 2+ ADL impairments |
| Rationale | Longer remaining life expectancy | Intermediate remaining life expectancy, high treatment burden, hypoglycemia vulnerability, fall risk | Limited remaining life expectancy makes benefit uncertain |
| HbA1c | <7.0–7.5% (53–58 mmol/mol) |
<8.0% (64 mmol/mol) |
Do not rely on HbA1C; glucose control decisions should be based on avoiding hypoglycemia and symptomatic hyperglycemia |
| Fasting/pre-prandial glucose | 80–130 mg/dL (4.4–7.2 mmol/L) |
90–150 mg/dL (5.0–8.3 mmol/L) |
100–180 mg/dL (5.6–10.0 mmol/L) |
| Bedtime glucose | 80–180 mg/dL (4.4–10.0 mmol/L) | 100–180 mg/dL (5.6–10.0 mmol/L) |
110–200 mg/dL (6.1–11.1 mmol/L) |
| Blood Pressure | <140/90 mmHg | <140/90 mmHg | <150/90 mmHg |
| Lipid Target | Statin unless contraindicated, or not tolerated |
Statin unless contraindicated, or not tolerated |
Consider likelihood of benefit with statin |
Coexisting chronic illnesses: arthritis, cancer, heart failure, depression, emphysema, falls, hypertension, incontinence, Stage 3 or worse CKD, myocardial infarction, and stroke. End-stage chronic illness, such as stage 3–4 heart failure or oxygen-dependent lung disease, dialysis dependent ESKD, or uncontrolled metastatic malignancy. ADL: Activities of daily living.
When statins are used for primary and secondary prevention, a benefit can be unequivocally expected for those individuals whose life expectancy exceeds the time frames (2 – 6 years) of the clinical trials [82]. Equivalently, one may use the average time to benefit for a therapy, which for statins was 2.5 years [83] and treat individuals whose expected survival exceeds this time frame. Many advanced age individuals with CKD stage 3a-5 would benefit according to this criterion, and this is the reason the KDIGO clinical practice guidelines [84] recommend the use of a statin or a statin/ezetimibe in patients older than 50 years old. These recommendations are largely based on the SHARP trial [85] that randomized participants with CKD (mean eGFR of 27 ml/min/1.73 m2,, N = 9270) to receive simvastatin 20 mg plus ezetimibe 10 mg daily or placebo. Statin plus ezetimibe therapy reduced the primary outcome of major atherosclerotic event (coronary death, myocardial infarction, need for revascularization, non-hemorrhagic stroke) by 17% (95% CI: 0.06 – 0.26), but without delaying dialysis.
5.2. Pharmaceutical interventions to reduce cardiorenal risk in eldelry patients with CKD in DM
5.2.1. Inhibitors of the Renin Angiotensin System
Inhibitors of the renin angiotensin system (RASi) were established in the treatment of DKD by the pivotal trials IDT [86] and RENAAL [87]. IDT and RENAAL established that benefits of RASi are maximized when the dose is maximized and identified residual albuminuria as marker of increased cardiovascular and kidney disease risk [88,89] and a criterion for adding additional agents and/or enrolling patients in trials of investigational agents to retard the progression of kidney disease. In a recent analysis these agents were underutilized: 17% of patients with DM initiated these agents [90] within 12 months of diagnosis of CKD [91], eventually these agents are only used in ~ 60% of eligible patients, but without any racial disparities in utilization [92]. The British Clinical Diabetologists and the UK renal association guidelines about the management of ACEi and ARBs in patients with DM and CKD [93], which don’t explicitly apply to elderly individuals are summarized below:
- Kidney function and potassium level should be checked within 7 to 10 days after initiation
- Up to 30% of eGFR decline may be tolerated.
- Drops in kidney function more than 30%, should prompt investigation for RAS, sepsis, volume depletion or concomitant medications, e.g., NSAIDs
- If an alternative explanation for a marked decline in renal function cannot be inferred, the dose of the RASi may be reduced.
- Potassium binders (Patiromer and Sodium Zirconium Cyclosilicate) may be used to reduce the serum potassium if it rises over 5 mEq/l and allow the RASi to be continued.
- Combination therapy with ACEi, Direct Renin Inhibitor, and ARBs should not be used since multiple clinical trials have shown greater risks of hypotension, hyperkalemia, and acute renal injury with these combinations [94].
- In advanced (stage 4 and 5) CKD, discontinuation [95] of the RASi was associated with a lower risk for hyperkalemia (HR, 0.65; 95% CI, 0.54-0.79), but higher risk of death (HR, 1.39, 95% CI 1.20 – 1.60), and higher risk of progression to ESKD (HR 1.19, 95% CI: 0.86 – 1.65). The STOP-ACEi [96,97] RCT examined the benefits vs. harm of stopping the RASi in patients with advanced CKD (eGFR was ~18 ml/min/1.73m2 at baseline). There was no difference in the eGFR (primary outcome) at 3 years between participants older than 65 years (- 0.32, 95% CI -2.72 – 2.09 ml/min/1.73m2) and those younger than 65 years (- 0.32, 95%CI -2.92 – 2.28 ml/min/1.73m2). ESKD occurred in 128 patients (62%) among those who discontinued the RASi and in 115 patients (56%) who continued them (HR, 1.28; 95% CI, 0.99 to 1.65). There was a similar number of cardiovascular events (108 vs. 88) and deaths (20 vs. 22) in the two arms.
5.2.2. Sodium Glucose Co-transporter two inhibitors
SGLT2is are small molecules that act on the luminal side in the proximal tubule of the kidney and inhibit the SGLT2 transporter. In meta-analyses of treatment naïve patients and patients treated with metformin SGLT2is reduced HbA1c by -0.81 to -1.02% and by -0.57 to -0.63%, respectively [98]. The glycosuric effect of this category of antidiabetic agents depends on the total GFR and they become less efficacious in reducing HbA1c when eGFR drops below 60mL/min/1.73m [99,100]. Nevertheless, according to Brenner’s hypothesis hyperfiltering nephrons exist at all levels of kidney dysfunction and SGLT2is continue to alleviate kidney hyperfiltration in diabetic patients with low GFRs.
The cardiovascular safety trials for empagliflozin (EMPA-REG OUTCOME) [101,102], canagliflozin (integrated CANVAS program consisting of two clinical trials, CANVAS and CANVAR-R) [103,104,105], dapagliflozin (DECLARE-TIMI-58) and ertugliflozin (VERTIS-CV)[99,103] hinted at the combined cardiorenal benefit of SGLT2i. In these SGLT2i reduced Major Adverse Cardiovascular Events (MACE:cardiovascular death, non-fatal myocardial infarction, or stroke) in the case of the empagliflozin and canagliflozin trials were non-inferior in the dapagliflozin and ertugliflozin trials. All drugs reduced heart failure hospitalizations in these trials. When the composite kidney specific outcome of progression to dialysis dependency/need for kidney transplantation and declines in eGFR was harmonized across the four trials [99], SGLT2is were seen to be associated with renal benefits. Heart failure specific trials have included patients with reduced (dapagliflozin, DAPA-HF [106], empaglifozin EMPEROR-REDUCED[107]) and preserved (dapagliflozin, DELIVER [108] , empagliflozin EMPEROR-PRESERVED [109]) ejection fraction. Trials with primary kidney specific outcomes include the CREDENCE trial (canagliflozin) [110] in DKD, DAPA-CKD (dapagliflozin) [111] and EMPA-KIDNEY (empagliflozin) [112]. The latter two trials included patients with both diabetic and non-diabetic forms of CKD. All SGLT2i kidney outcome trials included patients who manifested residual, moderate to severe albuminuria while on the standard of therapy for kidney disease, i.e. a maximum tolerated dose of an ACEi or an ARB. Across all trials, the SGLT2i have been associated with biphasic effects on the eGFR, with an acute dip of between 2-5 ml/min/1.73m2 during the first month [113,114,115] followed by stabilization thereafter, while the participants in the placebo group experienced a faster decline in kidney function.
A previous random effect meta-analysis that modelled heterogeneity in these trials [116] by one of the authors has demonstrated that the beneficial effects of SGLT2i is a class effect . Other meta-analyses have shown that the benefits of these drugs do not vary by participant age [117,118]. In Figure 1 we summarize the age by subgroup results in the cardiovascular, heart failure and kidney outcomes in the SGLT2i trials to date. Taken as a class the interactions with age are not statistically significant (p=0.294, Wald p-value), i.e. benefit of the SGLT2i do not vary by age. Furthermore, there was no evidence of heterogeneity by drug type (p=0.62, ANOVA test comparing a model adjusting for drug, outcome, age group vs model adjusting for outcome, age group). SGLT2is are in general safe drugs, but reported side effects such as diabetic ketoacidosis, and lower limb amputations appear to be barriers in prescribing them. A meta-analysis [119] has quantified risks and benefits of SGLT2i in patients with and without DM: the Number Needed to Treat to prevent one death (120) or one kidney disease progression event (48) dominated the Number Needed to Harm for the development of one lower limb amputation (309) or diabetic ketoacidosis event (636). For most patients, SGLT2i would accrue a 3-10 fold larger benefit than risk depending on the specific pair of outcomes considered [119]. Of note, Acute Kidney Injury (AKI) is reduced by 23% (RR 0.77, 95% CI 0.70–0.84) under a SGLT2i. A framework for managing the risks of the SGLT2i was put forward in a roundtable discussion involving representatives from cardiology, endocrinology, and nephrology (Table 3).
Table 3.
Adverse events associated with SGLT-2i and proposed preventative measures.
| Adverse Events | Title 2 | At risk |
| Genitourinary Infections | Women, Uncircumcised men |
Adequate perineal hygiene Optimal diabetes care Antifungals Avoid SGLT-2is in patients with history of severe, recurrent infections |
| Diabetic Ketoacidosis | Insulin deficiency, ketogenic diet, alcohol abuse, acute illness, surgery | Maintain insulin; ≤20% reduction in insulin dosage if necessary Discontinue SGLT-2i temporarily in acute illness or surgery Avoid SGLT-2is in patients with history of DKA Discontinue SGLT-2i if patient is not eating or has vomiting and/or diarrhea |
| Acute Kidney Injury | eGFR dip ≥30%, volume depletion | Reassess SGLT-2i regimen Frequently assess renal function, especially in patients with baseline eGFR<60 mL/min/1.73 m2 Discontinue SGLT-2i temporarily in acute illness |
| Volume Depletion | eGFR<60 mL/min/1.73 m2, old age, concomitant diuretic, prior volume depletion, hypotension, SBP<110mm Hg | Reduce diuretic or hypotension-inducing agent use Inform patients to maintain adequate oral hydration Discontinue SGLT-2i temporarily in AKI |
| Hypoglycemia | Concomitant insulin or SU, old age | Reduce insulin ≤20% or SU ≤50% if HbA1c<7.0%-8.0% Discontinue SU if HbA1c <8.0% in older patients Gradually reduce SU if HbA1c <8.0% in younger patients |
| Amputation | History of amputation, peripheral vascular disease, neuropathy, foot ulcers | Monitor at-risk patients for new pain, skin ulcerations, or infections Inform patients about proper foot care |
| Hyperkalemia | No concern |
The data in this table was adapted from Figure 3 from [120] under the Creative Commons Attribution (CC BY) license.
5.2.3. Mineralocorticoid antagonists
The use of Mineralocorticoid receptor antagonism (MRAs) in CKD with DM is predicated on their anti-inflammatory and anti-fibrotic effects on heart, blood vessels and kidneys. The benefits of steroidal MRAs (e.g. eplerenone, spironolactone) were summarized by the Cochrane group[121] and include reductions in systolic blood pressure by ~ 5mmHg (95% CI 1.22 to 1.75 mmHg), protein excretion by 500mg per day (95% CI 0.2 to 0.82 gm/day) but uncertain effects on kidney failure, cardiovascular and total mortality. In this meta-analysis of mostly spironolactone studies, the risk for gynecomastia and hyperkalemia were increased with the use of spironolactone.
Non-steroidal MRAs such as finerenone, esaxerenone and apararenone offer a balanced antagonism in the kidney and the heart, thus reducing the risk of hyperkalemia [37,122]. Phase 2 clinical trials with esaxerenone [123] and apararenone [124] in DKD show that these agents may reduce proteinuria by 40-60% when added on RASi. At the time of this writing the only commercially available non-steroidal MRA for CKD in DM is finerenone. The approval of finerenone was based on two large randomized controlled trials: FIDELIO-DKD [125] and FIGARO-DKD [126] and a pre-specified patient level meta-analysis of these two trials (FIDELITY) [127] which provided the data for the effects of this drug on cardiovascular and kidney specific outcomes. Both these studies followed a similar design, i.e., they enrolled patients with CKD in Type II DM who had some degree of residual albuminuria despite being on a maximum tolerated dose of RASi. FIGARO-DKD recruited patients with better preserved kidney function (UACR > 300 mg/g with eGFR > 60ml/min/1.73m2 or UACR in 30-300 mg/g & eGFR in 25-90 ml/min/1.73m2), while FIDELIO-DKD patients with more advanced CKD (UACR > 300 mg/g and eGFR 25-75 ml/min/1.73m2 or UACR in 30-300 mg/g and eGFR 25-60 ml/min/1.73m2 ). The primary outcome of FIDELIO-DKD was a composite of kidney failure (need of dialysis and transplant), sustained decrease of the eGFR by 40% relative to baseline and death from renal causes). The primary outcome for FIGARO-DKD was a composite of cardiovascular death, non-fatal myocardial infarction and stroke and hospitalization for heart failure (MACE/HHF). The primary outcome of FIGARO-DKD was a secondary outcome of FIDELIO-DKD and vice versa, enabling the joint examination of the effects of finerenone on the cardiorenal risk in patients with DKD in FIDELITY. Finerenone was equally effective in younger (< 65 years old) and older (≥65 years old) patients (Table 4).
Table 4.
Finerenone and Clinical Outcomes in Older vs. Younger Individuals (Hazard Ratio and 95% Confidence Intervals).
Table 4.
Finerenone and Clinical Outcomes in Older vs. Younger Individuals (Hazard Ratio and 95% Confidence Intervals).
| Clinical Trial | Outcome | Effect in younger patients | Effect in older patients |
|---|---|---|---|
| FIGARO-DKD | MACE/HHF2 | 0.90 0.74 – 1.10 |
0.85 0.72 – 1.00 |
| FIGARO-DKD1 | CR3 | 0.72 0.52 – 0.99 |
0.92 0.61-1.38 |
| FIDELIO-DKD | CR | 0.85 0.72 – 1.01 |
0.79 0.67 – 0.94 |
1 the subgroup analysis was presented in a follow-up publication [128] and used a sustained reduction of eGFR>57%, rather than the 40% used in the primary analysis of the FIGARO-DKD study 2, HHF: Hospitalization for Heart Failure, MACE: Major Adverse Cardiovascular Events (composite of cardiovascular death, non-fatal myocardial infarction, or stroke) 3 CR: Composite Renal outcome.
3.2.4. GLP1 and dual GLP1/GIP1 Receptor Agonists
GLP1 and the dual receptor agonists of the GLP1/GIP receptors are a class of antiglycemic agents with broad cardiometabolic effects and emerging benefit for kidney and cardiovascular benefits. These drugs activate the receptors of the endogenous incretins, glucagon-like peptide 1 and glucose-dependent insulinotropic polypeptide (GIP). Similar to SGLT2is, GLP1RAs were initially introduced to reduce glycemia with a minimal risk for hypoglycemia, while also reducing weight. Specific GLP1 RAs (liraglutide and semaglutide) have been approved as anti-obesity medications even in patients without DM. Dual agonists are associated with more pronounced weight loss and an enhanced antiglycemic effect relative to insulin or pure GLP1RAs in the SURPASS clinical trial [129,130,131,132]. Certain GLP1 class (dulaglutide, liraglutide, semaglutide) have been shown to reduce cardiovascular disease, and thus are indicated in the ADA standards of care for DM [133] for the management of patients with atherosclerotic cardiovascular disease (ASCVD), or with high-risk indicators of ASCVD. In a recent meta-analysis [134], GLP-1 receptor agonists in adults older than 65 years old, were associated with a 15.3% (OR 0.85, 95% CI 0.79 to 0.91) reduction in MACE events, similar to the 16% (OR 0.84, 95% CI 0.70 to 1.01) benefit seen in younger adults. Hence, GLP1RAs are equally beneficial in older and younger adults with type II DM for the management of their cardiovascular disease. To date, the clinical benefits of GLP1 and GLP1/GIP RA on kidney outcomes has been limited to surrogate markers of kidney function loss (eGFR slope) and markers of kidney damage (UACR) often examined as explorations of kidney specific outcomes [135,136,137,138] in their cardiovascular safety and primary efficacy trials. A recent meta-analysis [139] examined the effects of GLP1RAs on cardiovascular (MACE) and two kidney outcomes: a kidney composite consisting of development of macroalbuminuria, doubling of serum creatinine or at least a 40% decline in eGFR, kidney replacement therapy, or death due to kidney disease; and worsening of kidney function, defined as either doubling of serum creatinine or at least a 40% decline in eGFR. GLP1RA reduced MACE by 14% (HR 0.86, 95% CI 0.80 – 0.96, p< 0.001), with no evidence of interaction by age (p=0.78 comparing effects in individuals younger than 65 vs. those older than 65). In REWIND [140], one of the few GLP1RA trials to report a kidney specific outcome by age, individuals older than 66 years had a HR of 0.79 (95%CI 0.69 – 0.90) that was not statistically different (p-value for the interaction 0.17) to that of individuals younger than 66 (HR: 0.90, 95% CI: 0.79 – 1.02). In SURPASS-4[136], the placebo corrected difference in the eGFR slope did not differ in older (≥65 years old) and younger individuals: 2.4 (1.5 – 3.3) vs. 2.1 (95% CI 1.2 – 2.9) ml/min/1.73m2/year, p for interaction = 0.67. Finally, the least squares change from baseline over placebo was -38.5% (95% CI: -43.6% to -26.2%) vs. -28.5% (95% CI: -36.4% to -19.7%) p for interaction = 0.80. Hence, similarly to SGLT2i and non-steroidal MRA, the beneficial effects of GLP1 and GLP1/GIP receptor agonists are observed across the adult age span.
6. Conclusions
CKD in the elderly patient with DM is associated with both cardiovascular risk and kidney progression risks. Pathophysiology is complex and the spectrum of CKD is not limited to typical DN, but may also include additional vascular insults superimposed on a senescence molecular phenotype. Care of the elderly patient with CKD in DM requires a multidisciplinary, holistic approach that considers cardiovascular risk, comorbidities, life expectancy in addition to the risk of kidney disease progression. The effects of emerging standard of care pharmaceutical interventions (e.g. SLGT2 inhibitors, MRAs and GLP1RA/dual GLP1/GIP RA antagonists) to reduce the risk of cardiovascular and kidney risk are observed in both younger and older individuals
Author Contributions
“Conceptualization, C.A. and M.E.R.; writing—original draft preparation, C.A, M.E.R.; writing—review and editing, all authors.; visualization, C.A.; project administration, C.A.. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
No new data were generated for this paper.
Conflicts of Interest
CA has received consultant fees from Bayer (manufacturer of finerenone).
References
- Wild, S.; Roglic, G.; Green, A.; Sicree, R.; King, H. Global Prevalence of Diabetes: Estimates for the Year 2000 and Projections for 2030. Diabetes Care 2004, 27, 1047–1053. [Google Scholar] [CrossRef]
- Rossing, P.; Caramori, M.L.; Chan, J.C.N.; Heerspink, H.J.L.; Hurst, C.; Khunti, K.; Liew, A.; Michos, E.D.; Navaneethan, S.D.; Olowu, W.A.; et al. KDIGO 2022 Clinical Practice Guideline for Diabetes Management in Chronic Kidney Disease. Kidney International 2022, 102, S1–S127. [Google Scholar] [CrossRef]
- Afkarian, M.; Zelnick, L.R.; Hall, Y.N.; Heagerty, P.J.; Tuttle, K.; Weiss, N.S.; de Boer, I.H. Clinical Manifestations of Kidney Disease Among US Adults With Diabetes, 1988-2014. JAMA 2016, 316, 602–610. [Google Scholar] [CrossRef]
- Halimi, J.M. The Emerging Concept of Chronic Kidney Disease without Clinical Proteinuria in Diabetic Patients. Diabetes Metab 2012, 38, 291–297. [Google Scholar] [CrossRef]
- Ho, K.; McKnight, A.J. The Changing Landscape of Diabetic Kidney Disease: New Reflections on Phenotype, Classification, and Disease Progression to Influence Future Investigative Studies and Therapeutic Trials. Adv Chronic Kidney Dis 2014, 21, 256–259. [Google Scholar] [CrossRef] [PubMed]
- Robles, N.R.; Villa, J.; Gallego, R.H. Non-Proteinuric Diabetic Nephropathy. J Clin Med 2015, 4, 1761–1773. [Google Scholar] [CrossRef] [PubMed]
- Williams, M.E. Diabetic Kidney Disease in Elderly Individuals. Med Clin North Am 2013, 97, 75–89. [Google Scholar] [CrossRef]
- McClure, M.; Jorna, T.; Wilkinson, L.; Taylor, J. Elderly Patients with Chronic Kidney Disease: Do They Really Need Referral to the Nephrology Clinic? Clin Kidney J 2017, 10, 698–702. [Google Scholar] [CrossRef]
- Liu, P.; Quinn, R.R.; Lam, N.N.; Al-Wahsh, H.; Sood, M.M.; Tangri, N.; Tonelli, M.; Ravani, P. Progression and Regression of Chronic Kidney Disease by Age Among Adults in a Population-Based Cohort in Alberta, Canada. JAMA Netw Open 2021, 4, e2112828. [Google Scholar] [CrossRef]
- Hallan, S.I.; Matsushita, K.; Sang, Y.; Mahmoodi, B.K.; Black, C.; Ishani, A.; Kleefstra, N.; Naimark, D.; Roderick, P.; Tonelli, M.; et al. Age and the Association of Kidney Measures with Mortality and End-Stage Renal Disease. JAMA 2012, 308, 2349–2360. [Google Scholar] [CrossRef] [PubMed]
- Nelson, R.G.; Pavkov, M.E. The Pandemic of Diabetes and Kidney Disease. Kidney News 2020, 12, 7–9. [Google Scholar]
- National Diabetes Statistics Report 2020. Estimates of Diabetes and Its Burden in the United States. 2020, 32.
- Home; Resources; diabetes, L. with; Acknowledgement; FAQs; Contact; Policy, P. IDF Diabetes Atlas | Tenth Edition.
- Johansen, K.L.; Chertow, G.M.; Gilbertson, D.T.; Herzog, C.A.; Ishani, A.; Israni, A.K.; Ku, E.; Li, S.; Li, S.; Liu, J.; et al. US Renal Data System 2021 Annual Data Report: Epidemiology of Kidney Disease in the United States. Am J Kidney Dis 2022, 79, A8–A12. [Google Scholar] [CrossRef]
- Russo, G.T.; De Cosmo, S.; Viazzi, F.; Mirijello, A.; Ceriello, A.; Guida, P.; Giorda, C.; Cucinotta, D.; Pontremoli, R.; Fioretto, P.; et al. Diabetic Kidney Disease in the Elderly: Prevalence and Clinical Correlates. BMC Geriatr 2018, 18, 38. [Google Scholar] [CrossRef]
- McCullough, K.P.; Morgenstern, H.; Saran, R.; Herman, W.H.; Robinson, B.M. Projecting ESRD Incidence and Prevalence in the United States through 2030. J Am Soc Nephrol 2019, 30, 127–135. [Google Scholar] [CrossRef]
- Dias, J.P.; Shardell, M.; Golden, S.H.; Ahima, R.S.; Crews, D.C. Racial/Ethnic Trends in Prevalence of Diabetic Kidney Disease in the United States. Kidney Int Rep 2018, 4, 334–337. [Google Scholar] [CrossRef] [PubMed]
- Center for Medicare & Medical Services, Office of Minority Health Racial and Ethnic Disparities in Diabetes Prevalence, Self-Management, and Health Outcomes among Medicare Beneficiaries; Baltimore, MD, 2017; pp. 1–22;
- Rule, A.D.; Amer, H.; Cornell, L.D.; Taler, S.J.; Cosio, F.G.; Kremers, W.K.; Textor, S.C.; Stegall, M.D. The Association between Age and Nephrosclerosis on Renal Biopsy among Healthy Adults. Ann Intern Med 2010, 152, 561–567. [Google Scholar] [CrossRef] [PubMed]
- Tervaert, T.W.C.; Mooyaart, A.L.; Amann, K.; Cohen, A.H.; Cook, H.T.; Drachenberg, C.B.; Ferrario, F.; Fogo, A.B.; Haas, M.; de Heer, E.; et al. Pathologic Classification of Diabetic Nephropathy. J Am Soc Nephrol 2010, 21, 556–563. [Google Scholar] [CrossRef]
- Alsaad, K.O.; Herzenberg, A.M. Distinguishing Diabetic Nephropathy from Other Causes of Glomerulosclerosis: An Update. J Clin Pathol 2007, 60, 18–26. [Google Scholar] [CrossRef]
- Mauer, S.M.; Steffes, M.W.; Ellis, E.N.; Sutherland, D.E.; Brown, D.M.; Goetz, F.C. Structural-Functional Relationships in Diabetic Nephropathy. J Clin Invest 1984, 74, 1143–1155. [Google Scholar] [CrossRef]
- Denic, A.; Lieske, J.C.; Chakkera, H.A.; Poggio, E.D.; Alexander, M.P.; Singh, P.; Kremers, W.K.; Lerman, L.O.; Rule, A.D. The Substantial Loss of Nephrons in Healthy Human Kidneys with Aging. J Am Soc Nephrol 2017, 28, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Denic, A.; Mathew, J.; Lerman, L.O.; Lieske, J.C.; Larson, J.J.; Alexander, M.P.; Poggio, E.; Glassock, R.J.; Rule, A.D. Single-Nephron Glomerular Filtration Rate in Healthy Adults. N Engl J Med 2017, 376, 2349–2357. [Google Scholar] [CrossRef]
- Tan, J.C.; Busque, S.; Workeneh, B.; Ho, B.; Derby, G.; Blouch, K.L.; Sommer, F.G.; Edwards, B.; Myers, B.D. Effects of Aging on Glomerular Function and Number in Living Kidney Donors. Kidney Int 2010, 78, 686–692. [Google Scholar] [CrossRef] [PubMed]
- Tsaih, S.-W.; Pezzolesi, M.G.; Yuan, R.; Warram, J.H.; Krolewski, A.S.; Korstanje, R. Genetic Analysis of Albuminuria in Aging Mice and Concordance with Loci for Human Diabetic Nephropathy Found in a Genome-Wide Association Scan. Kidney Int 2010, 77, 201–210. [Google Scholar] [CrossRef]
- Verzola, D.; Gandolfo, M.T.; Gaetani, G.; Ferraris, A.; Mangerini, R.; Ferrario, F.; Villaggio, B.; Gianiorio, F.; Tosetti, F.; Weiss, U.; et al. Accelerated Senescence in the Kidneys of Patients with Type 2 Diabetic Nephropathy. American Journal of Physiology-Renal Physiology 2008, 295, F1563–F1573. [Google Scholar] [CrossRef]
- Wiley, C.D. Role of Senescent Renal Cells in Pathophysiology of Diabetic Kidney Disease. Curr Diab Rep 2020, 20, 33. [Google Scholar] [CrossRef] [PubMed]
- Kasper, M.; Funk, R.H. Age-Related Changes in Cells and Tissues Due to Advanced Glycation End Products (AGEs). Arch Gerontol Geriatr 2001, 32, 233–243. [Google Scholar] [CrossRef]
- Mei, C.; Zheng, F. Chronic Inflammation Potentiates Kidney Aging. Semin Nephrol 2009, 29, 555–568. [Google Scholar] [CrossRef]
- Vlassara, H.; Torreggiani, M.; Post, J.B.; Zheng, F.; Uribarri, J.; Striker, G.E. Role of Oxidants/Inflammation in Declining Renal Function in Chronic Kidney Disease and Normal Aging. Kidney Int Suppl 2009, S3–11. [Google Scholar] [CrossRef]
- Vlassara, H.; Uribarri, J.; Ferrucci, L.; Cai, W.; Torreggiani, M.; Post, J.B.; Zheng, F.; Striker, G.E. Identifying Advanced Glycation End Products as a Major Source of Oxidants in Aging: Implications for the Management and/or Prevention of Reduced Renal Function in Elderly Persons. Semin Nephrol 2009, 29, 594–603. [Google Scholar] [CrossRef]
- Guo, J.; Zheng, H.J.; Zhang, W.; Lou, W.; Xia, C.; Han, X.T.; Huang, W.J.; Zhang, F.; Wang, Y.; Liu, W.J. Accelerated Kidney Aging in Diabetes Mellitus. Oxid Med Cell Longev 2020, 2020, 1234059. [Google Scholar] [CrossRef] [PubMed]
- Selye, H.; Hall, C.E.; Rowley, E.M. Malignant Hypertension Produced by Treatment with Desoxycorticosterone Acetate and Sodium Chloride. Can Med Assoc J 1943, 49, 88–92. [Google Scholar] [PubMed]
- Ferreira, N.S.; Tostes, R.C.; Paradis, P.; Schiffrin, E.L. Aldosterone, Inflammation, Immune System, and Hypertension. Am J Hypertens 2021, 34, 15–27. [Google Scholar] [CrossRef] [PubMed]
- Fuller, P.J.; Yang, J.; Young, M.J. 30 YEARS OF THE MINERALOCORTICOID RECEPTOR: Coregulators as Mediators of Mineralocorticoid Receptor Signalling Diversity. J Endocrinol 2017, 234, T23–T34. [Google Scholar] [CrossRef]
- Kawanami, D.; Takashi, Y.; Muta, Y.; Oda, N.; Nagata, D.; Takahashi, H.; Tanabe, M. Mineralocorticoid Receptor Antagonists in Diabetic Kidney Disease. Frontiers in Pharmacology 2021, 12. [Google Scholar] [CrossRef]
- Sawicki, P.T.; Kaiser, S.; Heinemann, L.; Frenzel, H.; Berger, M. Prevalence of Renal Artery Stenosis in Diabetes Mellitus--an Autopsy Study. J Intern Med 1991, 229, 489–492. [Google Scholar] [CrossRef]
- Moriya, T.; Omura, K.; Matsubara, M.; Yoshida, Y.; Hayama, K.; Ouchi, M. Arteriolar Hyalinosis Predicts Increase in Albuminuria and GFR Decline in Normo- and Microalbuminuric Japanese Patients With Type 2 Diabetes. Diabetes Care 2017, 40, 1373–1378. [Google Scholar] [CrossRef]
- Ekinci, E.I.; Jerums, G.; Skene, A.; Crammer, P.; Power, D.; Cheong, K.Y.; Panagiotopoulos, S.; McNeil, K.; Baker, S.T.; Fioretto, P.; et al. Renal Structure in Normoalbuminuric and Albuminuric Patients with Type 2 Diabetes and Impaired Renal Function. Diabetes Care 2013, 36, 3620–3626. [Google Scholar] [CrossRef]
- Shimizu, M.; Furuichi, K.; Yokoyama, H.; Toyama, T.; Iwata, Y.; Sakai, N.; Kaneko, S.; Wada, T. Kidney Lesions in Diabetic Patients with Normoalbuminuric Renal Insufficiency. Clin Exp Nephrol 2014, 18, 305–312. [Google Scholar] [CrossRef]
- Dai, Q.; Chen, N.; Zeng, L.; Lin, X.-J.; Jiang, F.-X.; Zhuang, X.-J.; Lu, Z.-Y. Clinical Features of and Risk Factors for Normoalbuminuric Diabetic Kidney Disease in Hospitalized Patients with Type 2 Diabetes Mellitus: A Retrospective Cross-Sectional Study. BMC Endocr Disord 2021, 21, 104. [Google Scholar] [CrossRef]
- Retnakaran, R.; Cull, C.A.; Thorne, K.I.; Adler, A.I.; Holman, R.R.; UKPDS Study Group Risk Factors for Renal Dysfunction in Type 2 Diabetes: U.K. Prospective Diabetes Study 74. Diabetes 2006, 55, 1832–1839. [Google Scholar] [CrossRef] [PubMed]
- Shi, S.; Ni, L.; Gao, L.; Wu, X. Comparison of Nonalbuminuric and Albuminuric Diabetic Kidney Disease Among Patients With Type 2 Diabetes: A Systematic Review and Meta-Analysis. Front Endocrinol (Lausanne) 2022, 13, 871272. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.; Quinn, R.R.; Lam, N.N.; Elliott, M.J.; Xu, Y.; James, M.T.; Manns, B.; Ravani, P. Accounting for Age in the Definition of Chronic Kidney Disease. JAMA Internal Medicine 2021, 181, 1359–1366. [Google Scholar] [CrossRef] [PubMed]
- Delanaye, P.; Jager, K.J.; Bökenkamp, A.; Christensson, A.; Dubourg, L.; Eriksen, B.O.; Gaillard, F.; Gambaro, G.; van der Giet, M.; Glassock, R.J.; et al. CKD: A Call for an Age-Adapted Definition. J Am Soc Nephrol 2019, 30, 1785–1805. [Google Scholar] [CrossRef] [PubMed]
- de Zeeuw, D.; Parving, H.-H.; Henning, R.H. Microalbuminuria as an Early Marker for Cardiovascular Disease. J Am Soc Nephrol 2006, 17, 2100–2105. [Google Scholar] [CrossRef]
- Stehouwer, C.D.A.; Henry, R.M.A.; Dekker, J.M.; Nijpels, G.; Heine, R.J.; Bouter, L.M. Microalbuminuria Is Associated with Impaired Brachial Artery, Flow-Mediated Vasodilation in Elderly Individuals without and with Diabetes: Further Evidence for a Link between Microalbuminuria and Endothelial Dysfunction--the Hoorn Study. Kidney Int Suppl 2004, S42–44. [Google Scholar] [CrossRef]
- Hwang, S.; Lee, K.; Park, J.; Kim, D.H.; Jeon, J.; Jang, H.R.; Hur, K.Y.; Kim, J.H.; Huh, W.; Kim, Y.-G.; et al. Prognostic Significance of Albuminuria in Elderly of Various Ages with Diabetes. Sci Rep 2023, 13, 7079. [Google Scholar] [CrossRef]
- Anders, H.-J.; Huber, T.B.; Isermann, B.; Schiffer, M. CKD in Diabetes: Diabetic Kidney Disease versus Nondiabetic Kidney Disease. Nat Rev Nephrol 2018, 14, 361–377. [Google Scholar] [CrossRef]
- Iqbal, Z.; Meguira, S.; Friedman, E.A. Geriatric Diabetic Nephropathy: An Analysis of Renal Referral in Patients Age 60 or Older. Am J Kidney Dis 1990, 16, 312–316. [Google Scholar] [CrossRef]
- Marshall, S.M.; Alberti, K.G. Comparison of the Prevalence and Associated Features of Abnormal Albumin Excretion in Insulin-Dependent and Non-Insulin-Dependent Diabetes. Q J Med 1989, 70, 61–71. [Google Scholar]
- Parving, H.H.; Gall, M.A.; Skøtt, P.; Jørgensen, H.E.; Løkkegaard, H.; Jørgensen, F.; Nielsen, B.; Larsen, S. Prevalence and Causes of Albuminuria in Non-Insulin-Dependent Diabetic Patients. Kidney Int 1992, 41, 758–762. [Google Scholar] [CrossRef]
- Torffvit, O.; Agardh, E.; Agardh, C.D. Albuminuria and Associated Medical Risk Factors: A Cross-Sectional Study in 476 Type I (Insulin-Dependent) Diabetic Patients. Part 1. J Diabet Complications 1991, 5, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Joseph, A.J.; Friedman, E.A. Diabetic Nephropathy in the Elderly. Clin Geriatr Med 2009, 25, 373–389. [Google Scholar] [CrossRef] [PubMed]
- Nair, R.; Bell, J.M.; Walker, P.D. Renal Biopsy in Patients Aged 80 Years and Older. Am J Kidney Dis 2004, 44, 618–626. [Google Scholar] [CrossRef]
- Fedi, M.; Bobot, M.; Torrents, J.; Gobert, P.; Magnant, É.; Knefati, Y.; Verhelst, D.; Lebrun, G.; Masson, V.; Giaime, P.; et al. Kidney Biopsy in Very Elderly Patients: Indications, Therapeutic Impact and Complications. BMC Nephrol 2021, 22, 362. [Google Scholar] [CrossRef]
- Kohli, H.S.; Jairam, A.; Bhat, A.; Sud, K.; Jha, V.; Gupta, K.L.; Sakhuja, V. Safety of Kidney Biopsy in Elderly: A Prospective Study. Int Urol Nephrol 2006, 38, 815–820. [Google Scholar] [CrossRef]
- Uezono, S.; Hara, S.; Sato, Y.; Komatsu, H.; Ikeda, N.; Shimao, Y.; Hayashi, T.; Asada, Y.; Fujimoto, S.; Eto, T. Renal Biopsy in Elderly Patients: A Clinicopathological Analysis. Ren Fail 2006, 28, 549–555. [Google Scholar] [CrossRef]
- Blicklé, J.F.; Doucet, J.; Krummel, T.; Hannedouche, T. Diabetic Nephropathy in the Elderly. Diabetes Metab 2007, 33 Suppl 1, S40–55. [Google Scholar] [CrossRef]
- Espinel, E.; Agraz, I.; Ibernon, M.; Ramos, N.; Fort, J.; Serón, D. Renal Biopsy in Type 2 Diabetic Patients. J Clin Med 2015, 4, 998–1009. [Google Scholar] [CrossRef]
- Fiorentino, M.; Bolignano, D.; Tesar, V.; Pisano, A.; Biesen, W.V.; Tripepi, G.; D’Arrigo, G.; Gesualdo, L. ; ERA-EDTA Immunonephrology Working Group Renal Biopsy in Patients with Diabetes: A Pooled Meta-Analysis of 48 Studies. Nephrol Dial Transplant 2017, 32, 97–110. [Google Scholar] [CrossRef] [PubMed]
- Glassock, R.J.; Hirschman, G.H.; Striker, G.E. Workshop on the Use of Renal Biopsy in Research on Diabetic Nephropathy: A Summary Report. Am J Kidney Dis 1991, 18, 589–592. [Google Scholar] [CrossRef]
- Faller, B.; Beuscart, J.-B.; Frimat, L. Competing-Risk Analysis of Death and Dialysis Initiation among Elderly (≥80 Years) Newly Referred to Nephrologists: A French Prospective Study. BMC Nephrol 2013, 14, 103. [Google Scholar] [CrossRef]
- Tuttle, K.R.; Wong, L.; St Peter, W.; Roberts, G.; Rangaswami, J.; Mottl, A.; Kliger, A.S.; Harris, R.C.; Gee, P.O.; Fowler, K.; et al. Moving from Evidence to Implementation of Breakthrough Therapies for Diabetic Kidney Disease. Clin J Am Soc Nephrol 2022, 17, 1092–1103. [Google Scholar] [CrossRef]
- Umpierre, D.; Ribeiro, P.A.B.; Kramer, C.K.; Leitão, C.B.; Zucatti, A.T.N.; Azevedo, M.J.; Gross, J.L.; Ribeiro, J.P.; Schaan, B.D. Physical Activity Advice Only or Structured Exercise Training and Association with HbA1c Levels in Type 2 Diabetes: A Systematic Review and Meta-Analysis. JAMA 2011, 305, 1790–1799. [Google Scholar] [CrossRef]
- Hoffmann, T.C.; Maher, C.G.; Briffa, T.; Sherrington, C.; Bennell, K.; Alison, J.; Singh, M.F.; Glasziou, P.P. Prescribing Exercise Interventions for Patients with Chronic Conditions. CMAJ 2016, 188, 510–518. [Google Scholar] [CrossRef]
- Izquierdo, M.; Rodriguez-Mañas, L.; Sinclair, A.J. Editorial: What Is New in Exercise Regimes for Frail Older People - How Does the Erasmus Vivifrail Project Take Us Forward? J Nutr Health Aging 2016, 20, 736–737. [Google Scholar] [CrossRef]
- Horikawa, C.; Aida, R.; Tanaka, S.; Kamada, C.; Tanaka, S.; Yoshimura, Y.; Kodera, R.; Fujihara, K.; Kawasaki, R.; Moriya, T.; et al. Sodium Intake and Incidence of Diabetes Complications in Elderly Patients with Type 2 Diabetes-Analysis of Data from the Japanese Elderly Diabetes Intervention Study (J-EDIT). Nutrients 2021, 13, 689. [Google Scholar] [CrossRef]
- Klahr, S.; Levey, A.S.; Beck, G.J.; Caggiula, A.W.; Hunsicker, L.; Kusek, J.W.; Striker, G. The Effects of Dietary Protein Restriction and Blood-Pressure Control on the Progression of Chronic Renal Disease. Modification of Diet in Renal Disease Study Group. N Engl J Med 1994, 330, 877–884. [Google Scholar] [CrossRef]
- Pijls, L.T.J.; de Vries, H.; van Eijk, J.T.M.; Donker, A.J.M. Protein Restriction, Glomerular Filtration Rate and Albuminuria in Patients with Type 2 Diabetes Mellitus: A Randomized Trial. Eur J Clin Nutr 2002, 56, 1200–1207. [Google Scholar] [CrossRef]
- Volkert, D.; Beck, A.M.; Cederholm, T.; Cruz-Jentoft, A.; Goisser, S.; Hooper, L.; Kiesswetter, E.; Maggio, M.; Raynaud-Simon, A.; Sieber, C.C.; et al. ESPEN Guideline on Clinical Nutrition and Hydration in Geriatrics. Clinical Nutrition 2019, 38, 10–47. [Google Scholar] [CrossRef]
- Piccoli, G.B.; Cederholm, T.; Avesani, C.M.; Bakker, S.J.L.; Bellizzi, V.; Cuerda, C.; Cupisti, A.; Sabatino, A.; Schneider, S.; Torreggiani, M.; et al. Nutritional Status and the Risk of Malnutrition in Older Adults with Chronic Kidney Disease – Implications for Low Protein Intake and Nutritional Care: A Critical Review Endorsed by ERN-ERA and ESPEN. Clinical Nutrition 2023, 42, 443–457. [Google Scholar] [CrossRef]
- American Diabetes Association Professional Practice Committee; Draznin, B.; Aroda, V.R.; Bakris, G.; Benson, G.; Brown, F.M.; Freeman, R.; Green, J.; Huang, E.; Isaacs, D.; et al. 13. Older Adults: Standards of Medical Care in Diabetes-2022. Diabetes Care 2022, 45, S195–S207. [Google Scholar] [CrossRef]
- Kahn, S.E. Glucose Control in Type 2 Diabetes: Still Worthwhile and Worth Pursuing. JAMA 2009, 301, 1590–1592. [Google Scholar] [CrossRef]
- Shorr, R.I.; Franse, L.V.; Resnick, H.E.; Di Bari, M.; Johnson, K.C.; Pahor, M. Glycemic Control of Older Adults with Type 2 Diabetes: Findings from the Third National Health and Nutrition Examination Survey, 1988-1994. J Am Geriatr Soc 2000, 48, 264–267. [Google Scholar] [CrossRef]
- Whitmer, R.A.; Karter, A.J.; Yaffe, K.; Quesenberry, C.P.; Selby, J.V. Hypoglycemic Episodes and Risk of Dementia in Older Patients with Type 2 Diabetes Mellitus. JAMA 2009, 301, 1565–1572. [Google Scholar] [CrossRef]
- Effect of Intensive Blood-Glucose Control with Metformin on Complications in Overweight Patients with Type 2 Diabetes (UKPDS 34). UK Prospective Diabetes Study (UKPDS) Group. Lancet 1998, 352, 854–865. [CrossRef]
- Intensive Blood-Glucose Control with Sulphonylureas or Insulin Compared with Conventional Treatment and Risk of Complications in Patients with Type 2 Diabetes (UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group. Lancet 1998, 352, 837–853. [CrossRef]
- Cheung, A.K.; Chang, T.I.; Cushman, W.C.; Furth, S.L.; Hou, F.F.; Ix, J.H.; Knoll, G.A.; Muntner, P.; Pecoits-Filho, R.; Sarnak, M.J.; et al. Executive Summary of the KDIGO 2021 Clinical Practice Guideline for the Management of Blood Pressure in Chronic Kidney Disease. Kidney International 2021, 99, 559–569. [Google Scholar] [CrossRef]
- Group, T.S.R. A Randomized Trial of Intensive versus Standard Blood-Pressure Control. New England Journal of Medicine 2015, 373, 2103–2116. [Google Scholar] [CrossRef]
- Gencer, B.; Marston, N.A.; Im, K.; Cannon, C.P.; Sever, P.; Keech, A.; Braunwald, E.; Giugliano, R.P.; Sabatine, M.S. Efficacy and Safety of Lowering LDL Cholesterol in Older Patients: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Lancet 2020, 396, 1637–1643. [Google Scholar] [CrossRef]
- Yourman, L.C.; Cenzer, I.S.; Boscardin, W.J.; Nguyen, B.T.; Smith, A.K.; Schonberg, M.A.; Schoenborn, N.L.; Widera, E.W.; Orkaby, A.; Rodriguez, A.; et al. Evaluation of Time to Benefit of Statins for the Primary Prevention of Cardiovascular Events in Adults Aged 50 to 75 Years: A Meta-Analysis. JAMA Intern Med 2021, 181, 179–185. [Google Scholar] [CrossRef]
- Kidney Disease: Improving Global Outcomes (KDIGO) Blood Pressure Work Group KDIGO 2021 Clinical Practice Guideline for the Management of Blood Pressure in Chronic Kidney Disease. Kidney Int 2021, 99, S1–S87. [CrossRef]
- Baigent, C.; Landray, M.J.; Reith, C.; Emberson, J.; Wheeler, D.C.; Tomson, C.; Wanner, C.; Krane, V.; Cass, A.; Craig, J.; et al. The Effects of Lowering LDL Cholesterol with Simvastatin plus Ezetimibe in Patients with Chronic Kidney Disease (Study of Heart and Renal Protection): A Randomised Placebo-Controlled Trial. Lancet 2011, 377, 2181–2192. [Google Scholar] [CrossRef]
- Lewis, E.J.; Hunsicker, L.G.; Clarke, W.R.; Berl, T.; Pohl, M.A.; Lewis, J.B.; Ritz, E.; Atkins, R.C.; Rohde, R.; Raz, I.; et al. Renoprotective Effect of the Angiotensin-Receptor Antagonist Irbesartan in Patients with Nephropathy Due to Type 2 Diabetes. N Engl J Med 2001, 345, 851–860. [Google Scholar] [CrossRef]
- Brenner, B.M.; Cooper, M.E.; de Zeeuw, D.; Keane, W.F.; Mitch, W.E.; Parving, H.H.; Remuzzi, G.; Snapinn, S.M.; Zhang, Z.; Shahinfar, S.; et al. Effects of Losartan on Renal and Cardiovascular Outcomes in Patients with Type 2 Diabetes and Nephropathy. N Engl J Med 2001, 345, 861–869. [Google Scholar] [CrossRef]
- Lambers Heerspink, H.J.; Gansevoort, R.T.; Brenner, B.M.; Cooper, M.E.; Parving, H.H.; Shahinfar, S.; de Zeeuw, D. Comparison of Different Measures of Urinary Protein Excretion for Prediction of Renal Events. J Am Soc Nephrol 2010, 21, 1355–1360. [Google Scholar] [CrossRef]
- de Zeeuw, D.; Remuzzi, G.; Parving, H.-H.; Keane, W.F.; Zhang, Z.; Shahinfar, S.; Snapinn, S.; Cooper, M.E.; Mitch, W.E.; Brenner, B.M. Proteinuria, a Target for Renoprotection in Patients with Type 2 Diabetic Nephropathy: Lessons from RENAAL. Kidney Int 2004, 65, 2309–2320. [Google Scholar] [CrossRef]
- Fried, L.F.; Petruski-Ivleva, N.; Folkerts, K.; Schmedt, N.; Velentgas, P.; Kovesdy, C.P. ACE Inhibitor or ARB Treatment among Patients with Diabetes and Chronic Kidney Disease. Am J Manag Care 2021, 27, S360–S368. [Google Scholar] [CrossRef]
- Yang, Y.; Thumula, V.; Pace, P.F.; Banahan, B.F.; Wilkin, N.E.; Lobb, W.B. High-Risk Diabetic Patients in Medicare Part D Programs: Are They Getting the Recommended ACEI/ARB Therapy? J Gen Intern Med 2010, 25, 298–304. [Google Scholar] [CrossRef]
- Rosen, A.B.; Karter, A.J.; Liu, J.Y.; Selby, J.V.; Schneider, E.C. Use of Angiotensin-Converting Enzyme Inhibitors and Angiotensin Receptor Blockers in High-Risk Clinical and Ethnic Groups with Diabetes. J Gen Intern Med 2004, 19, 669–675. [Google Scholar] [CrossRef]
- Banerjee, D.; Winocour, P.; Chowdhury, T.A.; De, P.; Wahba, M.; Montero, R.; Fogarty, D.; Frankel, A.H.; Karalliedde, J.; Mark, P.B.; et al. Management of Hypertension and Renin-Angiotensin-Aldosterone System Blockade in Adults with Diabetic Kidney Disease: Association of British Clinical Diabetologists and the Renal Association UK Guideline Update 2021. BMC Nephrol 2022, 23, 9. [Google Scholar] [CrossRef]
- Fried, L.F.; Emanuele, N.; Zhang, J.H.; Brophy, M.; Conner, T.A.; Duckworth, W.; Leehey, D.J.; McCullough, P.A.; O’Connor, T.; Palevsky, P.M.; et al. Combined Angiotensin Inhibition for the Treatment of Diabetic Nephropathy. N Engl J Med 2013, 369, 1892–1903. [Google Scholar] [CrossRef]
- Qiao, Y.; Shin, J.-I.; Chen, T.K.; Inker, L.A.; Coresh, J.; Alexander, G.C.; Jackson, J.W.; Chang, A.R.; Grams, M.E. Association Between Renin-Angiotensin System Blockade Discontinuation and All-Cause Mortality Among Persons With Low Estimated Glomerular Filtration Rate. JAMA Intern Med 2020, 180, 718–726. [Google Scholar] [CrossRef]
- Bhandari, S.; Ives, N.; Brettell, E.A.; Valente, M.; Cockwell, P.; Topham, P.S.; Cleland, J.G.; Khwaja, A.; El Nahas, M. Multicentre Randomized Controlled Trial of Angiotensin-Converting Enzyme Inhibitor/Angiotensin Receptor Blocker Withdrawal in Advanced Renal Disease: The STOP-ACEi Trial. Nephrol Dial Transplant 2016, 31, 255–261. [Google Scholar] [CrossRef]
- Bhandari, S.; Mehta, S.; Khwaja, A.; Cleland, J.G.F.; Ives, N.; Brettell, E.; Chadburn, M.; Cockwell, P. ; STOP ACEi Trial Investigators Renin-Angiotensin System Inhibition in Advanced Chronic Kidney Disease. N Engl J Med 2022, 387, 2021–2032. [Google Scholar] [CrossRef]
- Tsapas, A.; Karagiannis, T.; Avgerinos, I.; Matthews, D.R.; Bekiari, E. Comparative Effectiveness of Glucose-Lowering Drugs for Type 2 Diabetes. Ann Intern Med 2021, 174, 141. [Google Scholar] [CrossRef]
- Cherney, D.Z.I.; Charbonnel, B.; Cosentino, F.; Dagogo-Jack, S.; McGuire, D.K.; Pratley, R.; Shih, W.J.; Frederich, R.; Maldonado, M.; Pong, A.; et al. Effects of Ertugliflozin on Kidney Composite Outcomes, Renal Function and Albuminuria in Patients with Type 2 Diabetes Mellitus: An Analysis from the Randomised VERTIS CV Trial. Diabetologia 2021, 64, 1256–1267. [Google Scholar] [CrossRef]
- Dekkers, C.C.J.; Wheeler, D.C.; Sjöström, C.D.; Stefansson, B.V.; Cain, V.; Heerspink, H.J.L. Effects of the Sodium-Glucose Co-Transporter 2 Inhibitor Dapagliflozin in Patients with Type 2 Diabetes and Stages 3b-4 Chronic Kidney Disease. Nephrol Dial Transplant 2018, 33, 2005–2011. [Google Scholar] [CrossRef]
- Wanner, C.; Inzucchi, S.E.; Lachin, J.M.; Fitchett, D.; von Eynatten, M.; Mattheus, M.; Johansen, O.E.; Woerle, H.J.; Broedl, U.C.; Zinman, B.; et al. Empagliflozin and Progression of Kidney Disease in Type 2 Diabetes. N Engl J Med 2016, 375, 323–334. [Google Scholar] [CrossRef]
- Zinman, B.; Wanner, C.; Lachin, J.M.; Fitchett, D.; Bluhmki, E.; Hantel, S.; Mattheus, M.; Devins, T.; Johansen, O.E.; Woerle, H.J.; et al. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N Engl J Med 2015, 373, 2117–2128. [Google Scholar] [CrossRef]
- Cannon, C.P.; Pratley, R.; Dagogo-Jack, S.; Mancuso, J.; Huyck, S.; Masiukiewicz, U.; Charbonnel, B.; Frederich, R.; Gallo, S.; Cosentino, F.; et al. Cardiovascular Outcomes with Ertugliflozin in Type 2 Diabetes. N Engl J Med 2020, 383, 1425–1435. [Google Scholar] [CrossRef] [PubMed]
- Neal, B.; Perkovic, V.; Matthews, D.R. Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes. N Engl J Med 2017, 377, 2099. [Google Scholar] [CrossRef] [PubMed]
- Wiviott, S.D.; Raz, I.; Bonaca, M.P.; Mosenzon, O.; Kato, E.T.; Cahn, A.; Silverman, M.G.; Zelniker, T.A.; Kuder, J.F.; Murphy, S.A.; et al. Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes. N Engl J Med 2019, 380, 347–357. [Google Scholar] [CrossRef]
- McMurray, J.J.V.; Solomon, S.D.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; Anand, I.S.; Bělohlávek, J.; et al. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. N Engl J Med 2019, 381, 1995–2008. [Google Scholar] [CrossRef] [PubMed]
- Packer, M.; Anker, S.D.; Butler, J.; Filippatos, G.; Pocock, S.J.; Carson, P.; Januzzi, J.; Verma, S.; Tsutsui, H.; Brueckmann, M.; et al. Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure. N Engl J Med 2020, 383, 1413–1424. [Google Scholar] [CrossRef] [PubMed]
- Solomon, S.D.; McMurray, J.J.V.; Claggett, B.; de Boer, R.A.; DeMets, D.; Hernandez, A.F.; Inzucchi, S.E.; Kosiborod, M.N.; Lam, C.S.P.; Martinez, F.; et al. Dapagliflozin in Heart Failure with Mildly Reduced or Preserved Ejection Fraction. N Engl J Med 2022, 387, 1089–1098. [Google Scholar] [CrossRef]
- Anker, S.D.; Butler, J.; Filippatos, G.; Ferreira, J.P.; Bocchi, E.; Böhm, M.; Brunner-La Rocca, H.-P.; Choi, D.-J.; Chopra, V.; Chuquiure-Valenzuela, E.; et al. Empagliflozin in Heart Failure with a Preserved Ejection Fraction. N Engl J Med 2021, 385, 1451–1461. [Google Scholar] [CrossRef]
- Perkovic, V.; Jardine, M.J.; Neal, B.; Bompoint, S.; Heerspink, H.J.L.; Charytan, D.M.; Edwards, R.; Agarwal, R.; Bakris, G.; Bull, S.; et al. Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy. N Engl J Med 2019, 380, 2295–2306. [Google Scholar] [CrossRef]
- Heerspink, H.J.L.; Stefánsson, B.V.; Correa-Rotter, R.; Chertow, G.M.; Greene, T.; Hou, F.-F.; Mann, J.F.E.; McMurray, J.J.V.; Lindberg, M.; Rossing, P.; et al. Dapagliflozin in Patients with Chronic Kidney Disease. N Engl J Med 2020, 383, 1436–1446. [Google Scholar] [CrossRef]
- EMPA-KIDNEY Collaborative Group; Herrington, W.G.; Staplin, N.; Wanner, C.; Green, J.B.; Hauske, S.J.; Emberson, J.R.; Preiss, D.; Judge, P.; Mayne, K.J.; et al. Empagliflozin in Patients with Chronic Kidney Disease. N Engl J Med 2022. [Google Scholar] [CrossRef]
- van Bommel, E.J.M.; Muskiet, M.H.A.; van Baar, M.J.B.; Tonneijck, L.; Smits, M.M.; Emanuel, A.L.; Bozovic, A.; Danser, A.H.J.; Geurts, F.; Hoorn, E.J.; et al. The Renal Hemodynamic Effects of the SGLT2 Inhibitor Dapagliflozin Are Caused by Post-Glomerular Vasodilatation Rather than Pre-Glomerular Vasoconstriction in Metformin-Treated Patients with Type 2 Diabetes in the Randomized, Double-Blind RED Trial. Kidney Int 2020, 97, 202–212. [Google Scholar] [CrossRef]
- Heerspink, H.J.L.; Cherney, D.Z.I. Clinical Implications of an Acute Dip in eGFR after SGLT2 Inhibitor Initiation. Clin J Am Soc Nephrol 2021, 16, 1278–1280. [Google Scholar] [CrossRef] [PubMed]
- Kraus, B.J.; Weir, M.R.; Bakris, G.L.; Mattheus, M.; Cherney, D.Z.I.; Sattar, N.; Heerspink, H.J.L.; Ritter, I.; von Eynatten, M.; Zinman, B.; et al. Characterization and Implications of the Initial Estimated Glomerular Filtration Rate “dip” upon Sodium-Glucose Cotransporter-2 Inhibition with Empagliflozin in the EMPA-REG OUTCOME Trial. Kidney Int 2021, 99, 750–762. [Google Scholar] [CrossRef] [PubMed]
- Johansen, M.E.; Argyropoulos, C. The Cardiovascular Outcomes, Heart Failure and Kidney Disease Trials Tell That the Time to Use Sodium Glucose Cotransporter 2 Inhibitors Is Now. Clin Cardiol 2020, 43, 1376–1387. [Google Scholar] [CrossRef]
- Bhattarai, M.; Salih, M.; Regmi, M.; Al-Akchar, M.; Deshpande, R.; Niaz, Z.; Kulkarni, A.; Siddique, M.; Hegde, S. Association of Sodium-Glucose Cotransporter 2 Inhibitors With Cardiovascular Outcomes in Patients With Type 2 Diabetes and Other Risk Factors for Cardiovascular Disease: A Meta-Analysis. JAMA Netw Open 2022, 5, e2142078. [Google Scholar] [CrossRef]
- Strain, W.D.; Griffiths, J. A Systematic Review and Meta-Analysis of the Impact of GLP-1 Receptor Agonists and SGLT-2 Inhibitors on Cardiovascular Outcomes in Biologically Healthy Older Adults. British Journal of Diabetes 2021, 21, 30–35. [Google Scholar] [CrossRef]
- Nuffield Department of Population Health Renal Studies Group; SGLT2 inhibitor Meta-Analysis Cardio-Renal Trialists’ Consortium Impact of Diabetes on the Effects of Sodium Glucose Co-Transporter-2 Inhibitors on Kidney Outcomes: Collaborative Meta-Analysis of Large Placebo-Controlled Trials. Lancet 2022, 400, 1788–1801. [CrossRef]
- Jabbour, S.A.; Ibrahim, N.E.; Argyropoulos, C.P. Physicians’ Considerations and Practice Recommendations Regarding the Use of Sodium-Glucose Cotransporter-2 Inhibitors. J Clin Med 2022, 11, 6051. [Google Scholar] [CrossRef]
- Chung, E.Y.; Ruospo, M.; Natale, P.; Bolignano, D.; Navaneethan, S.D.; Palmer, S.C.; Strippoli, G.F. Aldosterone Antagonists in Addition to Renin Angiotensin System Antagonists for Preventing the Progression of Chronic Kidney Disease. Cochrane Database Syst Rev 2020, 2020, CD007004. [Google Scholar] [CrossRef]
- Barrera-Chimal, J.; Kolkhof, P.; Lima-Posada, I.; Joachim, A.; Rossignol, P.; Jaisser, F. Differentiation between Emerging Non-Steroidal and Established Steroidal Mineralocorticoid Receptor Antagonists: Head-to-Head Comparisons of Pharmacological and Clinical Characteristics. Expert Opin Investig Drugs 2021, 30, 1141–1157. [Google Scholar] [CrossRef] [PubMed]
- Ito, S.; Kashihara, N.; Shikata, K.; Nangaku, M.; Wada, T.; Okuda, Y.; Sawanobori, T. Esaxerenone (CS-3150) in Patients with Type 2 Diabetes and Microalbuminuria (ESAX-DN): Phase 3 Randomized Controlled Clinical Trial. CJASN 2020, 15, 1715–1727. [Google Scholar] [CrossRef]
- Wada, T.; Inagaki, M.; Yoshinari, T.; Terata, R.; Totsuka, N.; Gotou, M.; Hashimoto, G. Apararenone in Patients with Diabetic Nephropathy: Results of a Randomized, Double-Blind, Placebo-Controlled Phase 2 Dose-Response Study and Open-Label Extension Study. Clin Exp Nephrol 2021, 25, 120–130. [Google Scholar] [CrossRef]
- Bakris, G.L.; Agarwal, R.; Anker, S.D.; Pitt, B.; Ruilope, L.M.; Rossing, P.; Kolkhof, P.; Nowack, C.; Schloemer, P.; Joseph, A.; et al. Effect of Finerenone on Chronic Kidney Disease Outcomes in Type 2 Diabetes. N Engl J Med 2020, 383, 2219–2229. [Google Scholar] [CrossRef]
- Pitt, B.; Filippatos, G.; Agarwal, R.; Anker, S.D.; Bakris, G.L.; Rossing, P.; Joseph, A.; Kolkhof, P.; Nowack, C.; Schloemer, P.; et al. Cardiovascular Events with Finerenone in Kidney Disease and Type 2 Diabetes. N Engl J Med 2021, 385, 2252–2263. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, R.; Filippatos, G.; Pitt, B.; Anker, S.D.; Rossing, P.; Joseph, A.; Kolkhof, P.; Nowack, C.; Gebel, M.; Ruilope, L.M.; et al. Cardiovascular and Kidney Outcomes with Finerenone in Patients with Type 2 Diabetes and Chronic Kidney Disease: The FIDELITY Pooled Analysis. Eur Heart J 2022, 43, 474–484. [Google Scholar] [CrossRef] [PubMed]
- Ruilope, L.M.; Pitt, B.; Anker, S.D.; Rossing, P.; Kovesdy, C.P.; Pecoits-Filho, R.; Pergola, P.; Joseph, A.; Lage, A.; Mentenich, N.; et al. Kidney Outcomes with Finerenone: An Analysis from the FIGARO-DKD Study. Nephrol Dial Transplant 2022, gfac157. [Google Scholar] [CrossRef]
- Del Prato, S.; Kahn, S.E.; Pavo, I.; Weerakkody, G.J.; Yang, Z.; Doupis, J.; Aizenberg, D.; Wynne, A.G.; Riesmeyer, J.S.; Heine, R.J.; et al. Tirzepatide versus Insulin Glargine in Type 2 Diabetes and Increased Cardiovascular Risk (SURPASS-4): A Randomised, Open-Label, Parallel-Group, Multicentre, Phase 3 Trial. Lancet 2021, 398, 1811–1824. [Google Scholar] [CrossRef] [PubMed]
- Frías, J.P.; Davies, M.J.; Rosenstock, J.; Pérez Manghi, F.C.; Fernández Landó, L.; Bergman, B.K.; Liu, B.; Cui, X.; Brown, K. ; SURPASS-2 Investigators Tirzepatide versus Semaglutide Once Weekly in Patients with Type 2 Diabetes. N Engl J Med 2021, 385, 503–515. [Google Scholar] [CrossRef]
- Min, T.; Bain, S.C. The Role of Tirzepatide, Dual GIP and GLP-1 Receptor Agonist, in the Management of Type 2 Diabetes: The SURPASS Clinical Trials. Diabetes Ther 2021, 12, 143–157. [Google Scholar] [CrossRef]
- Rosenstock, J.; Wysham, C.; Frías, J.P.; Kaneko, S.; Lee, C.J.; Fernández Landó, L.; Mao, H.; Cui, X.; Karanikas, C.A.; Thieu, V.T. Efficacy and Safety of a Novel Dual GIP and GLP-1 Receptor Agonist Tirzepatide in Patients with Type 2 Diabetes (SURPASS-1): A Double-Blind, Randomised, Phase 3 Trial. Lancet 2021, 398, 143–155. [Google Scholar] [CrossRef]
- American Diabetes Association Standards of Medical Care in Diabetes-2022 Abridged for Primary Care Providers. Clin Diabetes 2022, 40, 10–38. [CrossRef] [PubMed]
- Strain, W.D.; Griffiths, J. A Systematic Review and Meta-Analysis of the Impact of GLP-1 Receptor Agonists and SGLT-2 Inhibitors on Cardiovascular Outcomes in Biologically Healthy Older Adults. British Journal of Diabetes 2021, 21, 30–35. [Google Scholar] [CrossRef]
- Gerstein, H.C.; Colhoun, H.M.; Dagenais, G.R.; Diaz, R.; Lakshmanan, M.; Pais, P.; Probstfield, J.; Botros, F.T.; Riddle, M.C.; Rydén, L.; et al. Dulaglutide and Renal Outcomes in Type 2 Diabetes: An Exploratory Analysis of the REWIND Randomised, Placebo-Controlled Trial. Lancet 2019, 394, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Heerspink, H.J.L.; Sattar, N.; Pavo, I.; Haupt, A.; Duffin, K.L.; Yang, Z.; Wiese, R.J.; Tuttle, K.R.; Cherney, D.Z.I. Effects of Tirzepatide versus Insulin Glargine on Kidney Outcomes in Type 2 Diabetes in the SURPASS-4 Trial: Post-Hoc Analysis of an Open-Label, Randomised, Phase 3 Trial. Lancet Diabetes Endocrinol 2022, 10, 774–785. [Google Scholar] [CrossRef]
- Mann, J.F.E.; Ørsted, D.D.; Brown-Frandsen, K.; Marso, S.P.; Poulter, N.R.; Rasmussen, S.; Tornøe, K.; Zinman, B.; Buse, J.B. LEADER Steering Committee and Investigators Liraglutide and Renal Outcomes in Type 2 Diabetes. N Engl J Med 2017, 377, 839–848. [Google Scholar] [CrossRef] [PubMed]
- Marso, S.P.; Bain, S.C.; Consoli, A.; Eliaschewitz, F.G.; Jódar, E.; Leiter, L.A.; Lingvay, I.; Rosenstock, J.; Seufert, J.; Warren, M.L.; et al. Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N Engl J Med 2016, 375, 1834–1844. [Google Scholar] [CrossRef]
- Sattar, N.; Lee, M.M.Y.; Kristensen, S.L.; Branch, K.R.H.; Del Prato, S.; Khurmi, N.S.; Lam, C.S.P.; Lopes, R.D.; McMurray, J.J.V.; Pratley, R.E.; et al. Cardiovascular, Mortality, and Kidney Outcomes with GLP-1 Receptor Agonists in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis of Randomised Trials. Lancet Diabetes Endocrinol 2021, 9, 653–662. [Google Scholar] [CrossRef] [PubMed]
- Gerstein, H.C.; Colhoun, H.M.; Dagenais, G.R.; Diaz, R.; Lakshmanan, M.; Pais, P.; Probstfield, J.; Botros, F.T.; Riddle, M.C.; Rydén, L.; et al. Dulaglutide and Renal Outcomes in Type 2 Diabetes: An Exploratory Analysis of the REWIND Randomised, Placebo-Controlled Trial. The Lancet 2019, 394, 131–138. [Google Scholar] [CrossRef]
Figure 1.
SGLT2i and Clinical Outcomes in Older vs. Younger Individuals (Hazard Ratio and 95% Confidence Intervals). CRC: Cardiorenal Composite (CREDENCE: death from renal or cardiovascular causes, doubling of serum creatinine, or kidney failure defined as eGFR< 15 ml/min/1.73m2, need for dialysis or transplant, DAPA-CKD: death from renal or cardiovascular causes, decline of > 50% of the eGFR from baseline and kidney failure, defined as need for dialysis, transplant, or sustained eGFR to less than 15 ml/min/1.73m2, EMPA-KIDNEY: death from cardiovascular cases or progression of kidney disease defined as ESKD, sustained decrease in eGFR < 10 ml/min/1.73m2, decrease of eGFR >40% from baseline, death from kidney renal causes) , HHF: Hospitalization for Heart Failure, MACE: Major Adverse Cardiovascular Events (composite of cardiovascular death, non-fatal myocardial infarction, or stroke). Diamonds show predictions for a random effects model adjusting for drug, outcome and age subgroup, whiskers-boxes show the observed hazard ratios and 95% confidence intervals in the source trial data.
Figure 1.
SGLT2i and Clinical Outcomes in Older vs. Younger Individuals (Hazard Ratio and 95% Confidence Intervals). CRC: Cardiorenal Composite (CREDENCE: death from renal or cardiovascular causes, doubling of serum creatinine, or kidney failure defined as eGFR< 15 ml/min/1.73m2, need for dialysis or transplant, DAPA-CKD: death from renal or cardiovascular causes, decline of > 50% of the eGFR from baseline and kidney failure, defined as need for dialysis, transplant, or sustained eGFR to less than 15 ml/min/1.73m2, EMPA-KIDNEY: death from cardiovascular cases or progression of kidney disease defined as ESKD, sustained decrease in eGFR < 10 ml/min/1.73m2, decrease of eGFR >40% from baseline, death from kidney renal causes) , HHF: Hospitalization for Heart Failure, MACE: Major Adverse Cardiovascular Events (composite of cardiovascular death, non-fatal myocardial infarction, or stroke). Diamonds show predictions for a random effects model adjusting for drug, outcome and age subgroup, whiskers-boxes show the observed hazard ratios and 95% confidence intervals in the source trial data.
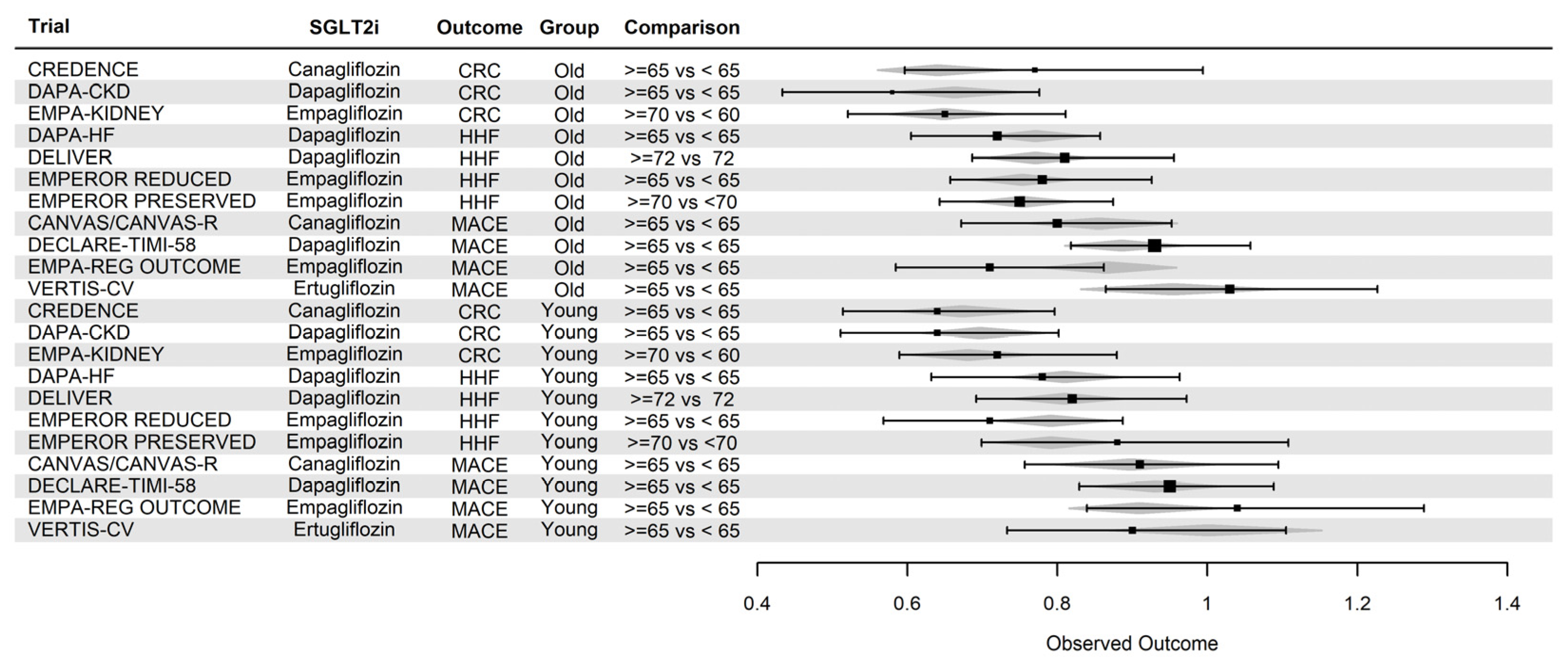
Table 1.
Lesions by Histologic Compartment in the 2010 Pathologic Classification of Diabetic Kidney Disease [20].
Table 1.
Lesions by Histologic Compartment in the 2010 Pathologic Classification of Diabetic Kidney Disease [20].
| Glomerulus | Arterioles | Mesangium2 | Tubulo-interstitium |
|---|---|---|---|
| Diffuse Intra-capillary Glomerulosclerosis |
Subintimal Hyaline Deposits |
Mesangial Matrix Expansion |
Tubular Atrophy / Interstitial Space Expansion |
| Nodular (Kimmelstein Wilson) |
Capillary Walls Bowman Capsules (capsular drops) 1 |
Mesangiolysis |
Tubular Basement Membrane Thickening |
| Glomerulosclerosis | Mesangial CellProliferation | Interstitial Fibrosis | |
Table 2.
Atypical presentation features for Diabetic Kidney Disease.
| Features On Presentation | Features Developing on Presentation or Follow-up |
|---|---|
| Absence of Retinopathy | Rapid Decline in eGFR (> 5ml/min/1.73m2) |
| Albuminuria < 5 years or > 25 years after diagnosis of Type 1 Diabetes |
↓ eGFR by more than 30% after initiation of an Inhibitor of the Renin Angiotensin System |
| Active Urine Sediment or Serologies | Acute Kidney Injury |
| Hematuria/Nephritic Syndrome | Sudden/acute worsening of albuminuria |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



