
Submitted:
02 October 2023
Posted:
03 October 2023
You are already at the latest version
Abstract
The complex interplay between dietary factors, inflammation, and macrophage polarization is pivotal in the pathogenesis and progression of chronic liver diseases (CLDs). Omega-3 fatty acids (FAs) have been attracted attention due to their potential to modulate inflammation and exert protective effects in various pathological conditions. This review explores the emerging role of omega-3 FAs and their specialized pro-resolving mediators (SPMs) in the context of macrophage polarization, with a focus on chronic liver diseases. Omega-3, eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) have promising effects in mitigating inflammation and enhancing the resolution of inflammatory responses. They influence the M1/M2 macrophage phenotype balance, promoting a shift towards the M2 anti-inflammatory phenotype. SPMs, such as resolvins (Rvs), protectins (PDs), and maresins (MaRs), have emerged as potent regulators of inflammation and macrophage polarization. They show anti-inflammatory and pro-resolving properties. These mediators modulate the expression of cytokines, facilitate the phagocytosis of apoptotic cells, and promote tissue repair. MaR1, in particular, has demonstrated significant hepatoprotective effects by promoting M2 macrophage polarization, reducing oxidative stress, and inhibiting key inflammatory pathways such as NF-κB. In the context of CLD, such as nonalcoholic fatty liver disease (NAFLD) and cirrhosis, omega-3 and their SPMs have shown promise in attenuating liver injury, promoting tissue regeneration, and modulating macrophage phenotypes. However, the mechanisms underlying their effects and their interactions with other cell types within the liver microenvironment require further investigation. Understanding the intricate relationship among SPM and macrophage polarization holds unlimited potential for the development of novel therapeutic strategies for chronic liver diseases.
Keywords:
chronic liver disease
; specialized pro-resolving mediators
; inflammation
; macrophage polarization
; inmunometabolism
1. Introduction
Historically, high fat consumption in humans has been associated with metabolic problems, metabolic disease deterioration, overweight and cardiovascular disease. However, since 1960, there has been a growing up evidence of the health benefits and protective effects of omega-3 fatty acids (FAs) [1,2]. This has led to physiological resolution of inflammation and could have a therapeutic role in a wide range of pathologies, both acute and chronic, among the latter being chronic liver diseases (CLDs) [2,3]. According to the global burden of liver disease: 2023 update, CLD was the 11th cause of mortality and the 15th cause of disability-associated life-years worldwide [4,5]. In the context of CLD associated with metabolic disorders, the nonalcoholic fatty liver disease (NAFLD) has increased in the last years, the overall prevalence of NAFLD worldwide is 32.4%, and may appear in absence if obesity or metabolic syndrome clinical criteria’s, and may coexist with insulin resistance or cardiovascular risk [4]. According to the Center for Disease Control and Prevention Analysis (CDC), the NAFLD cases in man are expected to increase by 21% in the US for the 2015-2030 period, pattern that will be followed by other occidental countries [6]. These records justify the search for new non-invasive treatments with a better cost/effectiveness ratio. In this context are the recently discovered specialized proresolving mediators (SPMs), among which are lipoxins from omega-6 polyunsaturated FAs (PUFAs) and resolvins, protectins and maresins from omega-3 PUFAs, synthesized by polymorphonuclear leukocytes (PMNs) [7]. SPMs are able to reduce inflammatory infiltration, promote phagocytosis of cellular debris and tissue regeneration, in addition of having analgesic and anti-inflammatory effects [7]. Due to their role in anti-inflammation, SPMs could be associated with a positive action over the resident macrophages of the liver, the Kupffer cells (KCs), and circulating monocyte-derived macrophages (MoMFs) in murine models [8]. KCs are crucial in maintaining an inflammatory microenvironment, characteristic of the development of cirrhosis. According to these antecedents, the aim of this review article was to examine the influence of n-3 PUFAs and their SPM derivates in the transformation of KCs expressing the proinflammatory phenotype M1 towards the pro-resolving or immune-modulating phenotype M2, which regulates late repair processes, resolution of inflammation and induction of immune tolerance, necessary steps at the beginning of tissue regeneration [9,10].
2. Chronic liver disease
CLD is any long-standing condition that prevents the normal functioning of the liver [11]. Cirrhosis can be a consequence of different causes, such as obesity, NAFLD, high alcohol consumption, hepatitis B or C virus infection, among others. Cirrhosis is an irreversible and diffuse process of liver damage developed after a long period of inflammation that results in replacement of the healthy liver parenchyma by fibrotic tissue and regenerative nodules, with collapse and distortion of liver structures [12,13].
3. Liver inflammation
Hepatocytes are cells that are highly resistant to variations in their environment, but they can undergo a series of reversible changes, among which are the accumulation of fat or steatosis, and that of bilirubin or cholestasis. Furthermore, when the damage exceeds the homeostatic mechanisms of the hepatocyte, cell death ensues, which may occur due to necrosis, apoptosis [11] or ferroptosis [12]. When a considerable amount of tissue becomes necrotic, the space where there should be the hepatocytes is replaced by cellular debris. The inflammatory cytokines derived from this process attract PMNs and activate hepatic stellated cells (HSCs), making them acquire a myofibroblast phenotype that increases their proliferation and fibrogenesis [13]. Under normal conditions, the extracellular matrix (ECM) of Disse’s space is composed of type I, III and IV collagens, fibronectin, laminin, heparan sulfate and dermatan sulfate. As the noxious stimulus is prolonged, the production of HSCs will alter their proportions, increasing the total amount of ECM by three to five times. This alteration favors tissue dysfunction, since under normal conditions, the ECM components interact with neighboring cells, regulating their shape, motility, survival, differentiation and gene expression [13,14]. The excessive production of ECM evolves into fibrous septa. In CLD these septa surround clusters of regenerating hepatocytes forming diffuse scarring or cirrhosis. Thus, fibrosis can be considered as an indicator of the extent of chronic damage. It is important to note that under experimental conditions of hepatic fibrosis, the liver can return to a normal state upon removal of the harmful stimuli, a process known as fibrosis resolution (reversion of HSCs activation) [14,15,16].
4. Liver macrophages
Macrophages are immune cells described by Metchnikoff and that received their name thanks to Aschoff’s studies, as part of the reticule-endothelial system [17]. It is now recognized that murine macrophages originate from monocyte recruitment dependent and independent mechanisms, originated and established during embryonic development) [18]. The origin of macrophages dates back to the early stages of pregnancy, where primitive hematopoiesis occurs in the extra-embryonic yolk sac, which has as its exclusive product red blood cells and macrophages, without a monocytic progenitor. In parallel, hematopoietic stem cells arise from the mesoderm, which during embryogenesis migrate to the fetal liver where temporary hematopoiesis occurs [8,19].
Liver-resident macrophages derive from colonies of erythromyeloid yolk sac, which migrate to the liver in early stages of murine gestation, subsequently being capable of self-renewal without the need to depend on bone marrow progenitors [20], but the latter being able to differentiate into fully functional KCs, if necessary, progenitors from the, as occurs in inflammatory processes. KCs are the largest reserves of resident macrophages, with 20% of non-parenchymal cells in the liver being located in the lumen of hepatic sinusoids, a location that favors their phagocytic function to support liver homeostasis [21,22]. Faced with chronic inflammatory stimuli, KCs change their tolerogenic phenotype towards an activated phenotype where, focusing their functions towards the development of an inflammatory state that, added to the decrease in homeostatic functions, contribute to the development of hepatic pathological states [22]. Both KCs and circulating murine monocytes are characterized by express the cell surface glycoprotein F4/80+, recognized as a distinctive marker of murine macrophages [23]. In addition, the resident KCs mainly express the cluster of differentiation CD68+ but CD11b+ poorly, and have a strong phagocytic and bactericidal activity, in contrast to the macrophages derived from bone marrow expression high CD11b+, which mainly produce cytokines (tumor necrosis factor-α (TNF-α), interleukin-12 (IL-12)), and that during inflammation accumulate and activate in the affected areas [23,24].
5. Macrophage phenotypes M1 and M2
Under milieu stimuli, the macrophages are activated through two common described polarization ways, depending on the specific gene transcription cascade, namely, the classical pathway exhibiting the pro-inflammatory phenotype (M1 or relative to CD4+ T helper (Th1)), and the alternative immune-modulatory pathway (M2 or relative to CD4+ Th2) also denominated anti-inflammatory phenotype [25,26]. M2 macrophages are divided into M2a, M2b, M2c and M2d subclasses, differing by their surface markers, cytokines secreted and immune functions. The production of M1-derived pro-inflammatory cytokines initially regulates the processes of early repair and response to pathogens, while M2-derived cytokines such as IL-4, IL-10 and IL-13, among others, stimulate the late repair process, immunity resolution, and tolerance [27]. It is important to remark that this model of macrophage polarization is not exempted from controversy. The functions that traditionally are attributed to certain pathways or molecular patterns are limited, and there is a lack of tightly defined criteria to score phenotypes due to the complexity of the regulation. [10,28].
Among the most common stimulus for M1 phenotype is the interferon- γ (INF-γ) induced by Th-1, natural killer cells (NKs) and macrophages. The activation of INF-γ receptor (IFNGR 1 and 2) by INF-γ controls specific gene expression programs involving cytokine receptors (including IL-15 receptor α [RA], IL-2RA and IL-6R); cell activation markers (CD36, CD38, CD69, and CD97); and a number of cell adhesion molecules (intercellular adhesion molecule 1 [ICAM1], integrin alpha L [ITGAL], mucin 1 [MUC1], and ST6 beta-galactosamide, among others) related to Th-1 response [29,30]. Others activators of M1 are the pathogen associated molecular patterns (PAMPs) such as lipopolysaccharide (LPS) and granulocyte-macrophage colony-stimulating factor (GM-CSF), all of them favoring antigen presentation, phagocytosis, chemotaxis, adhesion and pro-inflammatory cytokine production [26,29]. Otherwise, one of the inducers of M2 (particularly M2a) is IL-4. The human and murine IL-4 favors the Krüppel-like factor 4 (KLF4) and the peroxisome pathway [31]. The interaction with the IL-4 receptor-1 (IL-4Rα) induces Bcl-2-like protein-1 (BCL2L1) and B-cell lymphoma-extra-large (BCLXL), leading to diminution of apoptosis, fusion of macrophages, promotion of transforming growth factor-β1 (TGF-β1) and production of transglutimase-2 (TGM2) as a co-receptor of peroxisome proliferator-activated receptor-γ (PPARγ). PPARγ appears in the late stages of polarization, regulating progressive and/or reinforcing macrophage polarization [29,32]. In the case of M2c, the glucocorticoid receptor (GCR) induces the formation of IL-1R2, IL-10 and CD163 and accelerates the autophosphorylation of IL-10R inhibiting the production of pro-inflammatory cytokines and the stimulation of chemoattractant factors such as CXC motif chemokine ligand 13 (CXCL-13) and CXCL4 [29]. Due to the M1/M2 equilibrium playing a role in inflammation, proliferation and remodeling, the proportion of the phenotypes has been studied in various models of chronic diseases [33]. Of interest is the relation between inflammatory versus regeneration phenomena, and CLD has been associated with a misbalance in M1/M2 response [33].
6. Omega-3 fatty acids and their role on M1/M2 macrophage polarization
The study of omega-3s dates back to the early 1960s. Danish researchers Bang and Dyerberg observed that Alaska Natives with a diet high in omega-3s, derived from eating seal meat and fish, had a lower incidence of heart disease [1,34]. This study began a series of investigations in which the importance and benefits of this type of fat in the diet were studied. Omega-3s are found in three main forms, namely, α-linolenic acid (ALA, 18C:3 n-3), eicosapentaenoic acid (EPA, 20C:5 n-3) and docosahexaenoic acid (DHA, 22C:6 n-3). In food, EPA and DHA are found in fish such as salmon, tuna or algae, while vegetable oils, chia and nuts are the main foods with a high content of ALA [35]. ALA is a precursor of EPA and DHA, and the synthesis of both fatty acids occurs through desaturation and elongation reactions mainly in the liver, and in brain, testicle, and kidney, [36]. Also, EPA and DHA synthesis is directly related with nutritional status and oxidative stress [37]. Several studies show the importance of maintaining omega-6/omega-3 consumption in a ratio between 1/1 and 4/1. It should be considered that the average Western diet, heavily based on the consumption of meat and animal fats, has an approximate ratio of 16/1 in what the consumption of omega-6 and omega-3 refers to [38]. It has been observed that this results in increased metabolism of omega-6 polyunsaturated fatty acids (PUFAs), generating a greater number of metabolic mediators that, as mentioned above, have proinflammatory and neoplastic properties [39].
EPA and DHA (at 100 mM) have been shown to reduce oxidative damage to endothelial cell DNA, reducing the concentration of H2O2 and other reactive oxygen species (ROS) at the intracellular level in a model of human aortic endothelial cells (HAECs). These findings suggest that omega-3s have protective effects at the genetic level through mechanisms that reduce damage to genetic material without promoting its repair [40]. Based on the above, it was reported that the consumption of omega-3 is related to an improvement in endothelial function associated with an increase in nitric oxide (NO) in human endothelial cells [41,42]. In addition, it has been observed that the administration of omega-3 has protective functions in the development of some relevant pathologies (see Figure 1). In different animals, clinical trials and cellular models, the treatment with DHA and/or EPA promotes beneficial effects through the activation of immune cells such as PMNs or monocytes, decreasing inflammation [3,43,44,45,46,47,48,49]. For example, the addition of 2.4 g/d to type two diabetes (T2DM) patients for 8 weeks, may modulate the activity of PPARγ nuclear receptors, protecting by this way the cardiovascular system against atherosclerotic lesion formation and exerting an anti-inflammatory role [46]. Following the same line, the administration of EPA+DHA at 2 g/d (for six months) can lower c-reactive protein (as marker of cardiovascular disease) in patients with end-stage renal disease, and 4 g/d (for one month in healthy volunteers) can ameliorates acute and chronic vascular inflammation, with a decrease of C–C motif chemokine ligand 2 (CCL2), a chemokine that enhances macrophage responses to pro-inflammatory stimuli [47,48]. In all the cases previously explained the central positive actions of omega-3 is related to their ability to modify the inflammatory status.
Moreover, the direct effect of these fatty acids can be seen on the different tissues, such as cardiac tissue (chosen due to its high relevance) where EPA has been reported to reduce heartbeat through a decrease in membrane potential [50]. In the other hand, in cardiac fibroblast the combination of EPA and DHA (added to c57bl/6 mice for 8 weeks as 1% of total dietary energy) inhibit TGF-β pathways decreasing fibrosis [51], and in humans the addition of 4g/d of omega-3 ethyl esters (Omega-Remodell clinical trial) showed a significant reduction of left ventricular end-systolic volume index, and high dose of omega-3 is associated with significant reduction of inflammation and myocardial fibrosis in patients during convalescent phase of acute infarct healing [43,52]. Also, it was found, in clinical trial analysis, that EPA plus DHA can decrease lipogenesis and liver steatosis [53,54]. Additionally, EPA and DHA being both preventive and therapeutic protective factors related to immunity and particularly macrophages anti-inflammatory balances, as shown in Table 1 [55,56,57,58,59,60,61,62,63,64,65,66,67]. The Table 1 presents a comprehensive summary of the effects of EPA/DHA on different mechanisms and models (clinical trials and animal studies). In clinical trials, EPA/DHA supplementation demonstrated promising results, such as reducing T helper 2/T helper 1 chemokines in newborns from mothers with pregnancy-related depression, improving various metabolic parameters in T2DM, and modulating inflammatory pathways in obese individuals. Moreover, it enhanced specific macrophage markers and promoted anti-inflammatory cytokine production in children with low DHA intake, and it contributed to improved atherosclerotic plaque morphology in patients awaiting carotid endarterectomy. In animal models, EPA/DHA exhibited a range of effects, including attenuating atherosclerotic plaque development and suppressing atherogenesis, reducing aneurysm formation and macrophage infiltration, modulating skin inflammation in a psoriasis model, and influencing various signaling pathways. These findings underscore the potential health benefits of EPA/DHA in diverse contexts, from cardiovascular health to inflammation modulation.
The importance of reviewing data from both human and animal trials in Table 1 allows us to make a critical comparison between the effects of EPA/DHA, where human clinical trials provide direct insights into the effects of EPA/DHA in human populations. The clinical trials focus on health conditions directly relevant to humans, such as pregnancy-related depression, T2DM and atherosclerosis in patients awaiting carotid endarterectomy. This relevance ensures that the observed effects have immediate implications for human health with high ethical standards to protect the rights and well-being of human participants. The wide range of health parameters studied, including chemokine levels, triglycerides, waist measurements, and atherosclerotic plaque morphology, underscores the potential multi-faceted benefits of EPA/DHA in human health. The phenomena observed in the clinical trial enable readily interpretations for medical practice and treatment strategies. For example, the reduction in triglyceride levels in T2DM patients suggests a potential therapeutic opportunity. Also, the results allow to understand that EPA/DHA can decrease inflammatory pathways mostly related to macrophages activity and infiltration, and T-cell cytokine production. Animal models, on the other hand, offer controlled environments for mechanistic studies and initial insights, but require cautious interpretation and translation to human health due to species differences in physiology and metabolism, however, preclinical studies let to elucidate underlying mechanisms of action, providing a deeper understanding of how EPA/DHA exert their effects at the cellular and molecular levels. For example, the Apolipoprotein E-deficient (Ap-oe-/-) mice model helps elucidate the role of EPA/DHA in atherosclerosis development and the induction of Nrf2 to promote the cytokines switch from pro- to anti-inflammatory response, offering valuable mechanistic insights into how EPA/DHA affects pathways, cellular processes, and disease development. For instance, the K14-Rac1V12 mouse model sheds light on EPA/DHA’s effects on psoriasis, due to an increase in the SPM in the skin. These findings serve as a starting point for further research in humans. Combining both types of research can yield a more comprehensive understanding of EPA/DHA’s effects, from basic mechanisms to clinical applications.
The effects of EPA and DHA are of great interest in the scientific community, both in the field of chronic diseases and in the polarization of the M1 and M2 macrophage phenotypes. In this sense, there are multiple studies on EPA and DHA that show their participation in the reduction of arachidonic acid (ARA)-derived lipid mediators and the modulation of inflammation. According to Allam-Ndoul et al. [68], a combination of 75 μM of each EPA-DHA in a 1:1 ratio modulates inflammation (dose-dependently) inhibiting polarization towards M1, in a human monocytic THP-1 cell line. EPA, seems to have larger effects where inflammation is already established that it has resolving effects, while DHA and the EPA/DHA mixture presented higher effectiveness when administered at the same time as the proinflammatory inducer (LPS) [68]. Also, they found that DHA is more potent than EPA. In the same line, Kawano et al. [56], studied the effect of DHA on macrophage polarization, in cells of human monocytic lineage (U937 and THP-1). They showed a polarization towards M2 (CD23, CD206), with secretion of anti-inflammatory cytokines such as TGF-β and IL-10. DHA acts on a p38 MAPK-dependent pathway, a route that participates in the polarization and production of cytokines, and increase the transcription factor KLF4, an inhibitor of NF-κB activity [69]. In the context of metabolic disease, there are a few studies related to the role of omega-3 in macrophage polarization. Song et al. [70], found that macrophage infiltration into the liver and adipose tissue is diminished in a model of fat-1 high-fat diet (HFD)-induced obesity mice, where fat-1 is a gene modification able to convert omega-6 to omega-3 PUFAs in vivo. These investigators found that omega-3 suppresses proinflammatory M1, enhancing M2 polarization in adipose tissue macrophages, and causes anti-inflammatory and insulin-sensitizing effects {70]. More recently, Ontoria-OIviedo et al. reported that the administration of a commercial nutritional preparation of omega-3 (LIPINOVA®) could promote wound closure in a db/db model in the context of diabetes mellitus type-2 (DM2)-related ulcers [71]. The resolution of the wound was directly related to a decrease in the ratio M1/M2 in the area of the noxa, measured by the ratio F4/80+CD274+ (M1) /F4/80+/CD206+ (M2) [58]. Going further, Carpino et al. evaluated the macrophage polarization in 32 children with biopsy-proven NAFLD, 20 of whom received 250 mg/day DHA for 18 months [72]. DHA-treatment determined a significant reduction of liver steatosis, hepatocyte ballooning, and the number of portal CD68+ and total S100A9+ macrophages, concomitantly with the enhancement of the anti-inflammatories CD206+ and CD163+/Arginase1+ lobular macrophages. Also, DHA treatment caused an increased number of apoptotic macrophages [73]. Despite the slight information that exists at the hepatic level, there is clear evidence of factors that would be key in the modulation of the polarization of macrophages by omega-3s, and given their importance, the derivatives of these fatty acids will be described below.
7. Omega-3 lipid mediators
Studies in the last 15 years show the existence of specialized pro-resolving mediators (SPMs) derived from omega-3s with resolving and protecting properties in inflammatory processes, known as resolvins (Rvs), protectins (PDs/NPDs), and maresins (MaRs) [10,73,74]. These molecules were isolated for the first time from inflammatory exudates of murine models and are the product of a series of enzymatic reactions, where EPA and DHA are metabolized by the same enzymes, cyclooxygenase-2 (COX-2) and 15-lipoxygenase (15-LOX), that also participate in ARA metabolism. It should be noted that these enzymes have a higher affinity for ARA than omega-3s, which is why high concentrations of intracellular EPA and DHA are required for clinical benefits [75,76]. Among the Rvs, it is possible to find the E-series including RvE1 and RvE2. Their synthesis is initiated in the presence of aspirin (acetylsalicylic acid) which acetylates COX-2 that produces prostaglandins (PG) [77,78]. SPMs can also be generated independently of aspirin via cytochrome P450 mono-oxygenases that convert n-3 PUFAs into epoxy and hydroxy fatty acids [79]. These lipid mediators have powerful bioactive actions at low doses, for example only 100 ng per mouse of RvE1 is capable of breaking off inflammatory infiltration by over 50% in a murine model of acute inflammation, promoting PMN macrophage ingestion, reducing inflammatory pain and regulating the activity of leukocytes and platelets [80]. The D-series of Rvs include RvD1/RvD2/RvD3/RvD4/RvD5/RvD6, and they can have or not forms derived from aspirin. RvD1 is capable of reducing the migration through the endothelium of PMNs in a dose-dependent manner, also induce the phagocytosis of zymosan and apoptotic PMNs thought ALX/FPR2 lipoxin receptor [81]. All of them, reduce the PMN infiltration, neutrophil counts and proinflammatory cytokines, chemoattractants and other proinflammatory lipid mediators [82,83,84,85,86].
In relation to PD1 or Neuroprotectin (NPD1), their names change depending on where their biosynthesis occurs; the “neuro” suffix for NPD1 is added when it occurs in neural cells/neural ectoderm, while PD1 is mainly synthesized in immune cells [73,74]. Like Rvs, PD1 has anti-inflammatory properties related to the reduction of PMN and leukocyte infiltration into the inflammatory exudate, and also limits the expression of cytokines of this type, such as IL-6. In addition, PD1 decreases cell damage and, in turn, promotes tissue recovery [77,80]. In particular, PD1 has been related to a decrease in leukocyte infiltration in murine models of the immune, cardiovascular and renal systems, whereas NPD1 has been studied in models of stroke-mediated brain damage, which is defined as brain lesions associated with an interruption of blood supply to this organ, and ocular damage where it has a powerful protective action on the retina and the brain, giving its neuro-protective character [80].
Maresin-1 and 2 were the last discovered SPMs. They are generated by the 12-LOX catalyzed epoxidation and enzymatic hydrolysis in macrophages and platelets [87,88,89]. In the in vivo and in vitro administration, a very low concentration of MaR1 was able to decrease PMN infiltration and increase phagocytosis of apoptotic PMNs (efferocytosis) and zymosan [88,90]. These actions would be related to a shortening of the resolution phase of inflammation and restoration of homeostasis, which also protects the remaining cells, that are less exposed to oxidative stress and, therefore, are able to maintain homeostasis. In recent years, MaR1 has been studied in different tissues and organs, describing its resolution actions in inflammatory pathologies in rodent and human brain [91,92], heart [93,94], kidney [95,96] and liver [97,98,99]. The effects of MaR1 would even exceed, in some cases, those produced by other pro-resolving molecules whose effects have already been proven, such as RvD1. This opens up the discussion of its efficacy in more complex and exhaustive models and its possible role, in the long term, as treatment of inflammatory diseases [90].
8. The SPMs in relationship to the M1/M2 macrophage phenotype in chronic liver diseases
The evidence indicates that EPA and DHA participate directly or not in the polarization of the macrophage phenotype [68,70,71]. Historically, SPMs have been characterized as molecules with anti-inflammatory and resolving characteristics through mechanisms such as reduced inflammatory infiltration, decreased trans-epithelial migration of PMNs, decreased expression of proinflammatory cytokines and increased efferocytosis. This has been related to an improvement in the resolution phase of inflammatory processes and restoration of general homeostasis, thus SPMs likely act on the inflammatory environment by promoting macrophage polarization towards the M2 phenotype [88,90].
Research in recent years indicates that lipid mediators with proinflammatory (eicosanoids) or anti-inflammatory (SPMs) characteristics are synthesized in compliance with the M1 and M2 macrophage phenotypes respectively M1 [10,88,89,100] (see Figure 2). M2 macrophages produce MaR1 and lower levels of LTB4 and PG than M1 [89,100]. In the study of Sehan and Dalli [100], they observed that macrophages in efferocytosis feedback promoting the production of RvD3 and RvE1. It was also observed, in recent studies of lung inflammation induced by nanomaterials in a murine model, that there is a temporal correlation between the endogenous RvD1 and RvE1 peaks and the polarization towards an M2 macrophage phenotype [100] Studies carried out in 2011 by Titos et al. demonstrated that RvD1, in addition of being produced by macrophages of obese mice after high-fat diet feeding, increases the attenuated expression of IFNγ/LPS-induced Th1 cytokines (TNF-α and IL-6), while upregulating arginase 1 expression in a concentration-dependent manner [101]. Additionally, the authors found that RvD1 administration increased phagocytic activity, attenuating ROS production, a process typically associated with the M1 phenotype [102]. Related to the last discovered SPM, MaRs, Dalli et al. (2013) observed not only that MaR1 is produced by human macrophages, but it also shifted macrophage phenotype from a CD54+CD80+ to a CD163+CD206+ M2 phenotype [102]. These data are in agreement with that reported by Han et al., where MaR1 acts as an autoregulatory circuit through retinoid orphan receptor-α (RORα)/2-Lox activation [103]. In concordance with these findings, MaR1 inhibited an CD38+CD80+CD86+iNOS+ M1 macrophage differentiation promoting a CD36+CD163+CD206+Arg-1+ M2 in LPS-induced cardiac injury, with inhibition of the release of pro-inflammatory factors IL-1β, IL-6, TNF-α, MCP-1, IL-17 and IFN-γ after treatment with MaR [104]. In the context of protectin, it was not possible to find assays related to macrophage polarization activity, although Ma et al. demonstrated that protectin1 inhibits inflammatory cell death or piroptosis in macrophages, improving survival in LPS-induced sepsis inflammatory model [105]. In the context of inflammatory pain, NPD1 increases phagocytic activity [106].
Regarding the participation of SPMs in macrophage polarization and their role in chronic liver disease, Kang et al., in a murine model of hepatic inflammation induced by ischemia-reperfusion, where an M1 polarization of the KCs is favored, demonstrated the pro-resolving and anti-inflammatory effects of RvD1 through the activation of ALX/FPR2 pathways [107]. Particularly, RvD1 (15 μg/Kg) promotes both M2 polarization (Arg1, Cd206, and Mst1r) and spherocytosis performed by KCs at 24 h of reperfusion. In addition, the administration of RvD1 modified the inflammatory infiltrate, decreasing the population of neutrophils present in the area after 24 h of reperfusion [108]. In the same line, RvD1 and RvD2 has in vitro positive effects on hepatocellular carcinoma cells and/or tumor associated macrophages, connected with M2d polarization [109,110]. Taken together, these results suggest that RvD1 stimulates the pro-resolving functions of the M2 phenotype and inhibits the proinflammatory character of the macrophage M1 phenotype, in models of ischemia-reperfusion and hepatocarcinoma, respectively. Based on the aforementioned studies, it is also possible to highlight the relevance of KCs in the development and resolution of liver diseases, since these are the main agents of PMN phagocytosis and their depletion suppresses the beneficial effects generated by RvD1 [107]. In the case of RvE1, at liver level, data reported are not enough conclusive and there is no information in respect to the role of this Rv over macrophage polarization. For example, Pohl et al. did not find any positive results when RvE1 was administrated in a Non-Alcoholic SteatoHepatitis (NASH) rodent model [110]. The hepatic expression of the macrophage marker F4/80 and the inflammatory mediators TNF-α and CCL2 were not altered at doses of 1.2 ng/g body weight [110]. But according to Kuang et al., 10 μg/kg of RvE1 prevent concanavalin A-induced liver injury and the progression of hepatitis to liver cancer in mice through inhibition of inflammatory cytokine secretion and NF-κB/AP-1 activity [111]. Contrarily, in the study of Rodriguez et al., the administration of 100 ng/kg of RvE1 to rats was not enough to induce NF-κB nuclear activity in a fibrosis liver model (diethylnitrosamine induction) [112]. Also, Qiu et al., found that RvE1 at 100 ng/animal decreased the levels of TNF-α in a Schistosoma japonicum-liver fibrosis induction [113]. Although most of the studies inform that RvE1 could have hepatoprotective activities (depending on the doses), there is not enough information to indicate that these benefits are due to macrophage polarization.
From most of all SPMs, MaR1 appears to have the most potent activity against liver injury even at very small doses. It has been shown that the administration of MaR1 can induce cell division, promoting cell cycle and proliferation, undertaking the characteristics of macrophage M2 [97]. For example, in an ischemia-reperfusion liver injury model in rats, the administration of MaR1 at 4 ng/g body weight demonstrated positive effects on the modulation of primary M1 cytokines (such as TNF-α and IL-6), which are generated by KCs during reperfusion, stimulating liver tissue regeneration [96] In other acute liver injury model, Zhang et al. (2020) showed that MaR1 at 50 or 100 ng/kg reverts inflammatory signs of liver noxa induced by concavalin-A (ConA). The authors revealed that MaR1 reduced mortality caused by ConA due to a reduction in ROS levels and NF-κB activity in liver macrophages, which would indicate an inhibition of the M1 polarization pathways [114]. The authors also re-assayed in macrophage RAW264.7 cells, where MaR1 promoted its apoptosis and the M2 phenotype, with the limitation that the cell line used would only reflect the behavior of the macrophages and not necessarily emulated the Kupffer cell activity over CLD.
As mentioned above, the effects of MaR1 in liver tissue would occur through the stimulation of RORα, a ligand-dependent transcription factor that regulates lipid metabolism and inflammation [96]. Its activation, induced by MaR1, leads to the polarization towards M2 in liver macrophages and improved NASH symptoms, also generating positive feedback on MaR1 biosynthesis by inducing 12-LOX [96]. In Han et al. studies, MaR1 induced M2 switch in liver macrophages, by increasing the CD206+/CD80+ ratio and enhancing the expression of Klf4, Arg1 and Cd163 as M2 markers, all of that under time and dose dependency [104]. Reinforcing the above findings, Yang et al. demonstrated that MaR1 does not promote macrophage polarization in a galactosamine model of acute-liver injury, however, it can suppress the activation of NF-κB and the signaling of the inflammasome NLR family pirin domain containing 3 (NLRP3), which is the signaling via of piroptosis [115]. Besides, the M2 protective effects could be related to nuclear factor erythroid 2-related factor 2 (Nrf2) upregulation [115]. The fact that the resolutive and hepatoprotective effects of MaR1 are determined from two important factors (i) the M1 to M2 polarization related to a decrease in NF-κB activation in liver macrophages but also in the parenchyma; and (ii) the antioxidant response activated via Nrf2 [74,104,115], conclusively support the contention that MaR1 is a potent regulator of the molecular machinery in KCs. It is still necessary to understand the role of this SPM in the hepatocytes and how MaR1 connects the machinery related to the crosstalk among the most important type of cells in the liver (hepatocytes, KCs, HSCs and others), not only to put an end to the damage in chronic liver diseases, if not to use it as a potential regenerative molecule. At present time, however, (i) the complex etiological factors for CLD and the large heterogeneity of KCs challenge the transfer of the current knowledge into the development of macrophage-targeted therapies for CLD; (ii) most of the previous studies on the roles and mechanisms of hepatic macrophages in CLD were carried out in rodent models, thus the applicability of these findings to humans will need future research; and (iii) considering that the precise functions and control mechanisms of liver macrophage subclasses in humans are limited, it is a major concern to just focus on the study of pathogenic phenotypes rather than the physiological and resolutive macrophages. [116,117,118,119]
9. Conclusions
In conclusion, this comprehensive text discusses the intricate relationship between chronic liver diseases, macrophage polarization, and the role of omega-3 fatty acids and their specialized pro-resolving mediators (SPMs). CLD such as cirrhosis and non-alcoholic fatty liver disease (NAFLD), are characterized by inflammation and fibrosis, where macrophages play a crucial role. The M1 and M2 macrophage phenotypes represent pro-inflammatory and anti-inflammatory states, respectively, and their balance is crucial in the progression and resolution of liver diseases. The shift towards the anti-inflammatory M2 phenotype is associated with improved resolution of inflammation, tissue repair, and reduction in oxidative stress, which are all critical factors in chronic liver diseases. SPMs such as resolvins (Rvs), protectins (PDs), and especially maresins (MaRs), play a pivotal role in regulating macrophage polarization and inflammation resolution. RvR1, RvR3, PD1 and MaR1 promote the M2 phenotype while inhibiting the M1 phenotype, contributing to tissue repair and resolution of inflammation in various inflammatory diseases, including CLD. The evidence suggests that they could be a promise as therapeutic interventions to modulate macrophage polarization and resolve inflammation but further studies are needed to fully elucidate the molecular mechanisms underlying the interactions between omega-3 fatty acids, SPMs, and macrophage polarization, and to explore their clinical potential in managing CLD.
Author Contributions
Conceptualization: J.Z.H; Investigation; L.A.V; R.V; A.d.C.; and J.Z.H.; Writing—original draft, J.Z-H.; Writing—review & editing: L.A.V; R.V; A.d.C.; and J.Z.H. All authors have read and agreed to the published version of the manuscript.
Funding
Chilean National Fund for Scientific and Technological Development Fondecyt Iniciación Grant No 11200258 (JZH).
Acknowledgments
we want to thank to Dr. Rodrigo Troncoso for his contribution on Figure 1.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Dyerberg, J.; Bang, H.O.; Stoffersen, E.; Mondaca, S.; Vane, J.R. Eicosaenoic acid and prevention of thrombosis and atherosclerosis? Lancet 1978, 2, 117–119. [Google Scholar] [CrossRef] [PubMed]
- Valenzuela, R.; Ortiz, M.; Hernández-Rodas, M.C.; Echeverría, F.; Videla, L.A. Targeting n-3 Polyunsaturated Fatty Acids in Non-Alcoholic Fatty Liver Disease. Curr. Med. Chem. 2020, 27, 5250–5272. [Google Scholar] [CrossRef] [PubMed]
- Vielma, F.H.; Valenzuela, R.; Videla, L.A.; Zúñiga-Hernández, J. N-3 Polyunsaturated Fatty Acids and Their Lipid Mediators as A Potential Immune–Nutritional Intervention: A Molecular and Clinical View in Hepatic Disease and Other Non-Communicable Illnesses. Nutrients 2021, 13, 3384. [Google Scholar] [CrossRef] [PubMed]
- Devarbhavi, H.; Asrani, S.K.; Arab, J.P.; Nartey, Y.A.; Pose, E.; Kamath, P.S. Global burden of liver disease: 2023 update. J. Hepatol. 2023, 79, 516–537. [Google Scholar] [CrossRef]
- Cheemerla, S.; Balakrishnan, M. Global Epidemiology of Chronic Liver Disease. Clin. Liver Dis. 2021, 17, 365–370. [Google Scholar] [CrossRef]
- Estes, C.; Razavi, H.; Loomba, R.; Younossi, Z.; Sanyal, A.J. Modeling the epidemic of nonalcoholic fatty liver disease demonstrates an exponential increase in burden of disease. Hepatology 2018, 67, 123–133. [Google Scholar] [CrossRef]
- Serhan, C.N.; Levy, B.D. Resolvins in inflammation: emergence of the pro-resolving superfamily of mediators. J. Clin. Investig. 2018, 128, 2657–2669. [Google Scholar] [CrossRef]
- Li, H.; Zhou, Y.; Wang, H.; Zhang, M.; Qiu, P.; Zhang, M.; Zhang, R.; Zhao, Q.; Liu, J. Crosstalk Between Liver Macrophages and Surrounding Cells in Nonalcoholic Steatohepatitis. Front. Immunol. 2020, 11, 1169. [Google Scholar] [CrossRef]
- Chistiakov, D.A.; Myasoedova, V.A.; Revin, V.V.; Orekhov, A.N.; Bobryshev, Y.V. The impact of interferon-regulatory factors to macrophage differentiation and polarization into M1 and M2. Immunobiology 2018, 223, 101–111. [Google Scholar] [CrossRef]
- Mariqueo, T.; Zúñiga-Hernández, J. Omega-3 derivatives, specialized pro-resolving mediators: Promising therapeutic tools for the treatment of pain in chronic liver disease. Prostaglandins, Leukot. Essent. Fat. Acids 2020, 158, 102095. [Google Scholar] [CrossRef]
- Huang, Y.; Chen, Y.; Zhu, H.; Li, W.; Ge, Y.; Huang, X.; He, J. A liver fibrosis staging method using cross-contrast network. Expert Syst. Appl. 2019, 130, 124–131. [Google Scholar] [CrossRef]
- Capelletti, M.M.; Manceau, H.; Puy, H.; Peoc’h, K. Ferroptosis in Liver Diseases: An Overview. Int. J. Mol. Sci. 2020, 21, 4908. [Google Scholar] [CrossRef] [PubMed]
- Aydin, M.M.; Akcali, K.C. Liver fibrosis. Turkish J. Gastroenterol. 2018. 29, 14–21. [CrossRef]
- Senoo, H.; Mezaki, Y.; Fujiwara, M. The stellate cell system (vitamin A-storing cell system). Anat. Sci. Int. 2017, 92, 387–455. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Serna-Salas, S.; Damba, T.; Borghesan, M.; Demaria, M.; Moshage, H. Hepatic stellate cell senescence in liver fibrosis: Characteristics, mechanisms and perspectives. Mech. Ageing Dev. 2021, 199, 111572. [Google Scholar] [CrossRef]
- Troeger, J.S.; Mederacke, I.; Gwak, GY.; Dapito, D.H.; Mu, X.; Hsu, C.C.; Pradere, J.P.; Friedman, R.A.; Schwabe, R.F. Deactivation of hepatic stellate cells during liver fibrosis resolution in mice. Gastroenterology 2012, 143, 1073–1083. [Google Scholar] [CrossRef]
- Munro, D.A.D.; Hughes, J. The Origins and Functions of Tissue-Resident Macrophages in Kidney Development. Front. Physiol. 2017, 8, 837. [Google Scholar] [CrossRef]
- Wynn, T.A.; Chawla, A.; Pollard, J.W. Macrophage biology in development, homeostasis and disease. Nature 2013, 496, 445–455. [Google Scholar] [CrossRef]
- Wynn, T.A.; Vannella, K.M. Macrophages in Tissue Repair, Regeneration, and Fibrosis. Immunity 2016, 44, 450–462. [Google Scholar] [CrossRef]
- Röszer, T. Understanding the Biology of Self-Renewing Macrophages. Cells 2018, 7, 103. [Google Scholar] [CrossRef]
- Luo, W.; Xu, Q.; Wang, Q.; Wu, H.; Hua, J. Effect of modulation of PPAR-γ activity on Kupffer cells M1/M2 polarization in the development of non-alcoholic fatty liver disease. Sci. Rep. 2017, 7, 44612. [Google Scholar] [CrossRef] [PubMed]
- Dixon, L.J.; Barnes, M.; Tang, H.; Pritchard, M.T.; Nagy, L.E. Kupffer cells in the liver. Compr. Physiol. 2013, 3, 785–797. [Google Scholar] [PubMed]
- Nishiyama, K.; Nakashima, H.; Ikarashi, M.; Kinoshita, M.; Nakashima, M.; Aosasa, S.; Seki, S.; Yamamoto, J. Mouse CD11b+Kupffer Cells Recruited from Bone Marrow Accelerate Liver Regeneration after Partial Hepatectomy. PLOS ONE 2015, 10, e0136774. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, M.; Uchida, T.; Sato, A.; Nakashima, M.; Nakashima, H.; Shono, S.; Habu, Y.; Miyazaki, H.; Hiroi, S.; Seki, S. Characterization of two F4/80-positive Kupffer cell subsets by their function and phenotype in mice. J. Hepatol. 2010, 53, 903–910. [Google Scholar] [CrossRef] [PubMed]
- Nasser, M.; Zhu, S.; Huang, H.; Zhao, M.; Wang, B.; Ping, H.; Geng, Q.; Zhu, P. Macrophages: First guards in the prevention of cardiovascular diseases. Life Sci. 2020, 250, 117559. [Google Scholar] [CrossRef]
- Yunna, C.; Mengru, H.; Lei, W.; Weidong, C. Macrophage M1/M2 polarization. Eur. J. Pharmacol. 2020, 877, 173090. [Google Scholar] [CrossRef] [PubMed]
- Murray, P.J. Macrophage polarization. Annu. Rev. Physiol. 2017, 79, 541–566. [Google Scholar] [CrossRef]
- Riis, S.; Murray, J.B.; O’connor, R. IGF-1 Signalling Regulates Mitochondria Dynamics and Turnover through a Conserved GSK-3β–Nrf2–BNIP3 Pathway. Cells 2020, 9, 147. [Google Scholar] [CrossRef]
- Martinez, F.O.; Gordon, S. The M1 and M2 paradigm of macrophage activation: Time for reassessment. F1000Prime Rep. 2014, 6, 13. [Google Scholar] [CrossRef]
- Szondy, Z.; Korponay-Szabó, I.; Király, R.; Sarang, Z.; Tsay, G.J. Transglutaminase 2 in human diseases. BioMedicine 2017, 7, 15. [Google Scholar] [CrossRef]
- Fernando, M.R.; Reyes, J.L.; Iannuzzi, J.; Leung, G.; McKay, D.M. The Pro-Inflammatory Cytokine, Interleukin-6, Enhances the Polarization of Alternatively Activated Macrophages. PLOS ONE 2014, 9, e94188. [Google Scholar] [CrossRef] [PubMed]
- Daniel, B.; Nagy, G.; Czimmerer, Z.; Horvath, A.; Hammers, D.W.; Cuaranta-Monroy, I.; Poliska, S.; Tzerpos, P.; Kolostyak, Z.; Hays, T.T.; et al. The Nuclear Receptor PPARγ Controls Progressive Macrophage Polarization as a Ligand-Insensitive Epigenomic Ratchet of Transcriptional Memory. Immunity 2018, 49, 615–626. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Ma, C.; Gong, L.; Guo, Y.; Fu, K.; Zhang, Y.; Zhou, H.; Li, Y. Macrophage Polarization and Its Role in Liver Disease. Front. Immunol. 2021, 12, 803037. [Google Scholar] [CrossRef]
- Bang, H.; Dyerberg, J.; Sinclair, H.M. The composition of the Eskimo food in north western Greenland. Am. J. Clin. Nutr. 1980, 33, 2657–2661. [Google Scholar] [CrossRef] [PubMed]
- Tur, J.A.; Bibiloni, M.M.; Sureda, A.; Pons, A. Dietary sources of omega 3 fatty acids: public health risks and benefits. Br. J. Nutr. 2012, 107, S23–S52. [Google Scholar] [CrossRef]
- Valenzuela, R.; Metherel, A.H.; Cisbani, G.; Smith, M.E.; Chouinard-Watkins, R.; Klievik, B.J.; Videla, L.A.; Bazinet, R.P. Protein concentrations and activities of fatty acid desaturase and elongase enzymes in liver, brain, testicle, and kidney from mice: Substrate dependency. BioFactors 2023. [Google Scholar] [CrossRef]
- Videla, L.A.; Hernandez-Rodas, M.C.; Metherel, A.H.; Valenzuela, R. Influence of the nutritional status and oxidative stress in the desaturation and elongation of n-3 and n-6 polyunsaturated fatty acids: Impact on non-alcoholic fatty liver disease. Prostaglandins, Leukot. Essent. Fat. Acids 2022, 181, 102441. [Google Scholar] [CrossRef]
- Dinicolantonio, J.J.; O’Keefe, J.H. Importance of maintaining a low omega-6/omega-3 ratio for reducing inflammation. Open Heart 2018, 5(2), e000946. [Google Scholar] [CrossRef]
- Johnson, A.M.; Kleczko, E.K.; Nemenoff, R.A. Eicosanoids in Cancer: New Roles in Immunoregulation. Front. Pharmacol. 2020, 11, 595498. [Google Scholar] [CrossRef]
- Sakai, C.; Ishida, M.; Ohba, H.; Yamashita, H.; Uchida, H.; Yoshizumi, M.; Ishida, T. Fish oil omega-3 polyunsaturated fatty acids attenuate oxidative stress-induced DNA damage in vascular endothelial cells. PLOS ONE 2017, 12, e0187934. [Google Scholar] [CrossRef]
- Zehr, K.R.; Walker, M.K. Omega-3 polyunsaturated fatty acids improve endothelial function in humans at risk for atherosclerosis: A review. Prostaglandins Other Lipid Mediat. 2018, 134, 131–140. [Google Scholar] [CrossRef] [PubMed]
- Colussi, G.; Catena, C.; Novello, M.; Bertin, N.; Sechi, L. Impact of omega-3 polyunsaturated fatty acids on vascular function and blood pressure: Relevance for cardiovascular outcomes. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 191–200. [Google Scholar] [CrossRef] [PubMed]
- Fujikura, K.; Heydari, B.; Ge, Y.; Kaneko, K.; Abdullah, S.; Harris, W.S.; Jerosch-Herold, M.; Kwong, R.Y. Insulin Resistance Modifies the Effects of Omega-3 Acid Ethyl Esters on Left Ventricular Remodeling After Acute Myocardial Infarction (from the OMEGA-REMODEL Randomized Clinical Trial). Am. J. Cardiol. 2020, 125, 678–684. [Google Scholar] [CrossRef] [PubMed]
- Zúñiga-Hernández, J.; Sambra, V.; Echeverría, F.; Videla, L.A.; Valenzuela, R. N-3 PUFAs and their specialized pro-resolving lipid mediators on airway inflammatory response: beneficial effects in the prevention and treatment of respiratory diseases. Food Funct. 2022, 13, 4260–4272. [Google Scholar] [CrossRef]
- Watanabe, Y.; Tatsuno, I. Prevention of Cardiovascular Events with Omega-3 Polyunsaturated Fatty Acids and the Mechanism Involved. J. Atheroscler. Thromb. 2020, 27, 183–198. [Google Scholar] [CrossRef] [PubMed]
- Naeini, Z.; Toupchian, O.; Vatannejad, A.; Sotoudeh, G.; Teimouri, M.; Ghorbani, M.; et al. Effects of DHA-enriched fish oil on gene expression levels of p53 and NF-kappa B and PPAR-gamma activity in PBMCs of patients with T2DM: A randomized, double-blind, clinical trial. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 441–447. [Google Scholar] [CrossRef]
- Bowden, R.G.; Wilson, R.L.; Deike, E.; Gentile, M. Fish Oil Supplementation Lowers C-Reactive Protein Levels Independent of Triglyceride Reduction in Patients With End-Stage Renal Disease. Nutr. Clin. Pr. 2009, 24, 508–512. [Google Scholar] [CrossRef]
- 48. Pisaniello, A.D.; Psaltis, P.J.; King, P.M.; Liu, G.; Gibson, R.A.; Tan, J.T.; et al. Omega-3 fatty acids ameliorate vascular inflammation: A rationale f2or their atheroprotective effects. Atherosclerosis 2021, 324, 27–37. [Google Scholar] [CrossRef]
- Lee, J.Y.; Plakidas, A.; Lee, W.H.; Heikkinen, A.; Chanmugam, P.; Bray, G.; et al. Differential modulation of Toll-like receptors by fatty acids: preferential inhibition by n-3 polyunsaturated fatty acids. Journal of Lipid Research 2003, 44, 479–86. [Google Scholar] [CrossRef]
- Leaf A; Kang J.X; Xiao Y.F; Billman G.E. Clinical prevention of sudden cardiac death by n-3 polyunsaturated fatty acids and mechanism of prevention of arrhythmias by n-3 fish oils. Circulation 2003, 107, 2646–52.
- Chen, J.; Shearer, G.C.; Chen, Q.; Healy, C.L.; Beyer, A.J.; Nareddy, V.B.; Gerdes, A.M.; Harris, W.S.; O’Connell, T.D.; Wang, D.; et al. Omega-3 Fatty Acids Prevent Pressure Overload–Induced Cardiac Fibrosis Through Activation of Cyclic GMP/Protein Kinase G Signaling in Cardiac Fibroblasts. Circulation 2011, 123, 584–593. [Google Scholar] [CrossRef] [PubMed]
- Heydari, B.; Abdullah, S.; Pottala, J.V.; Shah, R.; Abbasi, S.; Mandry, D.; et al. Effect of Omega-3 Acid Ethyl Esters on Left Ventricular Remodeling After Acute Myocardial Infarction: The OMEGA-REMODEL Randomized Clinical Trial. Circulation 2016, 134, 378–91. [Google Scholar] [CrossRef] [PubMed]
- Okada, L.S.D.R.R.; Oliveira, C.P.; Stefano, J.T.; Nogueira, M.A.; da Silva, I.D.C.G.D.; Cordeiro, F.B.; Alves, V.A.F.; Torrinhas, R.S.; Carrilho, F.J.; Puri, P.; et al. Omega-3 PUFA modulate lipogenesis, ER stress, and mitochondrial dysfunction markers in NASH - Proteomic and lipidomic insight. Clin. Nutr. 2018, 37, 1474–1484. [Google Scholar] [CrossRef] [PubMed]
- Song, L.; Zhao, X.G.; Ouyang, P.L.; Guan, Q.; Yang, L.; Peng, F.; Du, H.; Yin, F.; Yan, W.; Yu, W.J.; et al. Combined effect of n-3 fatty acids and phytosterol esters on alleviating hepatic steatosis in non-alcoholic fatty liver disease subjects: a double-blind placebo-controlled clinical trial. Br. J. Nutr. 2020, 123, 1148–1158. [Google Scholar] [CrossRef]
- Romero, V.C.; Somers, E.C.; Stolberg, V.; Clinton, C.; Chensue, S.; Djuric, Z.; Berman, D.R.; Treadwell, M.C.; Vahratian, A.M.; Mozurkewich, E. Developmental programming for allergy: a secondary analysis of the Mothers, Omega-3, and Mental Health Study. Am. J. Obstet. Gynecol. 2013, 208, 316.e1–316.e6. [Google Scholar] [CrossRef]
- Toupchian, O.; Sotoudeh, G.; Mansoori, A.; Nasli-Esfahani, E.; Djalali, M.; Keshavarz, S.A.; Koohdani, F. Effects of DHA-enriched fish oil on monocyte/macrophage activation marker sCD163, asymmetric dimethyl arginine, and insulin resistance in type 2 diabetic patients. J. Clin. Lipidol. 2016, 10, 798–807. [Google Scholar] [CrossRef]
- Fisk, H.L.; Childs, C.E.; Miles, E.A.; Ayres, R.; Noakes, P.S.; Paras-Chavez, C.; Antoun, E.; Lillycrop, K.A.; Calder, P.C. Dysregulation of Subcutaneous White Adipose Tissue Inflammatory Environment Modelling in Non-Insulin Resistant Obesity and Responses to Omega-3 Fatty Acids – A Double Blind, Randomised Clinical Trial. Front. Immunol. 2022, 13, 922654. [Google Scholar] [CrossRef]
- Mazurak V.C; Lien V; Field C.J; Goruk S.D; Pramuk K; Clandinin M.T. Long-chain polyunsaturated fat supplementation in children with low docosahexaenoic acid intakes alters immune phenotypes compared with placebo. J Pediatr Gastroenterol Nutr. 2008, 46, 570–579.
- Thies, F.; MC Garry, J.; Yaqoob, P.; Rerkasem, K.; Williams, J.; Shearman, C.P.; Gallagher, P.J.; Calder, P.C.; Grimble, R.F. Association of n-3 polyunsaturated fatty acids with stability of atherosclerotic plaques: a randomised controlled trial. Lancet 2003, 361, 477–485. [Google Scholar] [CrossRef]
- Takashima, A.; Fukuda, D.; Tanaka, K.; Higashikuni, Y.; Hirata, Y.; Nishimoto, S.; Yagi, S.; Yamada, H.; Soeki, T.; Wakatsuki, T.; et al. Combination of n-3 polyunsaturated fatty acids reduces atherogenesis in apolipoprotein E-deficient mice by inhibiting macrophage activation. Atherosclerosis 2016, 254, 142–150. [Google Scholar] [CrossRef]
- Yoshihara, T.; Shimada, K.; Fukao, K.; Sai, E.; Sato-Okabayashi, Y.; Matsumori, R.; Shiozawa, T.; Alshahi, H.; Miyazaki, T.; Tada, N.; et al. Omega 3 Polyunsaturated Fatty Acids Suppress the Development of Aortic Aneurysms Through the Inhibition of Macrophage-Mediated Inflammation. Circ. J. 2015, 79, 1470–1478. [Google Scholar] [CrossRef] [PubMed]
- Sorokin, A.V.; Arnardottir, H.; Svirydava, M.; Ng, Q.; Baumer, Y.; Berg, A.; Pantoja, C.J.; Florida, E.M.; Teague, H.L.; Yang, Z.-H.; et al. Comparison of the dietary omega-3 fatty acids impact on murine psoriasis-like skin inflammation and associated lipid dysfunction. J. Nutr. Biochem. 2023, 117, 109348. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Khor, T.O.; Saw, C.L.L.; Lin, W.; Wu, T.; Huang, Y.; Kong, A.-N.T. Role of Nrf2 in Suppressing LPS-Induced Inflammation in Mouse Peritoneal Macrophages by Polyunsaturated Fatty Acids Docosahexaenoic Acid and Eicosapentaenoic Acid. Mol. Pharm. 2010, 7, 2185–2193. [Google Scholar] [CrossRef] [PubMed]
- Takase, O.; Hishikawa, K.; Kamiura, N.; Nakakuki, M.; Kawano, H.; Mizuguchi, K.; Fujita, T. Eicosapentaenoic acid regulates IκBα and prevents tubulointerstitial injury in kidney. Eur. J. Pharmacol. 2011, 669, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Elsayed, H.R.H.; Anbar, H.S.; Rabei, M.R.; Adel, M.; El-Gamal, R. Eicosapentaenoic and docosahexaenoic acids attenuate methotrexate-induced apoptosis and suppression of splenic T, B-Lymphocytes and macrophages with modulation of expression of CD3, CD20 and CD68. Tissue Cell 2021, 72, 101533. [Google Scholar] [CrossRef] [PubMed]
- Ontoria-Oviedo, I.; Amaro-Prellezo, E.; Castellano, D.; Venegas-Venegas, E.; González-Santos, F.; Ruiz-Saurí, A.; Pelacho, B.; Prósper, F.; del Caz, M.D.P.; Sepúlveda, P. Topical Administration of a Marine Oil Rich in Pro-Resolving Lipid Mediators Accelerates Wound Healing in Diabetic db/db Mice through Angiogenesis and Macrophage Polarization. Int. J. Mol. Sci. 2022, 23, 9918. [Google Scholar] [CrossRef]
- Chadli, F.K.; Andre, A.; Prieur, X.; Loirand, G.; Meynier, A.; Krempf, M.; Nguyen, P.; Ouguerram, K. n-3 PUFA prevent metabolic disturbances associated with obesity and improve endothelial function in golden Syrian hamsters fed with a high-fat diet. Br. J. Nutr. 2011, 107, 1305–1315. [Google Scholar] [CrossRef]
- Allam-Ndoul, B.; Guénard, F.; Barbier, O.; Vohl, M.-C. Effect of different concentrations of omega-3 fatty acids on stimulated THP-1 macrophages. Genes Nutr. 2017, 12, 7. [Google Scholar] [CrossRef]
- Kawano, A.; Ariyoshi, W.; Yoshioka, Y.; Hikiji, H.; Nishihara, T.; Okinaga, T. Docosahexaenoic acid enhances M2 macrophage polarization via the p38 signaling pathway and autophagy. J. Cell. Biochem. 2019, 120, 12604–12617. [Google Scholar] [CrossRef]
- Song, M.; Wang, J.; Lee, Y.; Lee, J.; Kwon, K.; Bae, E.J.; Park, B. Enhanced M2 macrophage polarization in high n-3 polyunsaturated fatty acid transgenic mice fed a high-fat diet. Mol. Nutr. Food Res. 2016, 60, 2481–2492. [Google Scholar] [CrossRef]
- Ontoria-Oviedo, I.; Amaro-Prellezo, E.; Castellano, D.; Venegas-Venegas, E.; González-Santos, F.; Ruiz-Saurí, A.; Pelacho, B.; Prósper, F.; del Caz, M.D.P.; Sepúlveda, P. Topical Administration of a Marine Oil Rich in Pro-Resolving Lipid Mediators Accelerates Wound Healing in Diabetic db/db Mice through Angiogenesis and Macrophage Polarization. Int. J. Mol. Sci. 2022, 23, 9918. [Google Scholar] [CrossRef] [PubMed]
- Carpino, G.; Nobili, V.; Renzi, A.; De Stefanis, C.; Stronati, L.; Franchitto, A.; Alisi, A.; Onori, P.; De Vito, R.; Alpini, G.; et al. Macrophage activation in pediatric nonalcoholic fatty liver disease (NAFLD) correlates with hepatic progenitor cell response via wnt3a pathway. PLoS One 2016, 11, e0157246. [Google Scholar] [CrossRef] [PubMed]
- Innes, J.K.; Calder, P.C. Omega-6 fatty acids and inflammation. Prostaglandins, Leukot. Essent. Fat. Acids 2018, 132, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Serhan, C.N.; Krishnamoorthy, S.; Recchiuti, A.; Chiang, N. Novel proresolving aspirin-triggered DHA pathway. Chem. Biol. 2011, 18, 629–647. [Google Scholar] [CrossRef]
- Dyall, S.C.; Balas, L.; Bazan, N.G.; Brenna, J.T.; Chiang, N.; Souza, F.d.C.; Dalli, J.; Durand, T.; Galano, J.-M.; Lein, P.J.; et al. Polyunsaturated fatty acids and fatty acid-derived lipid mediators: Recent advances in the understanding of their biosynthesis, structures, and functions. Prog. Lipid Res. 2022, 86, 101165–101165. [Google Scholar] [CrossRef]
- Cabo-Garcia, L.; Achon-Tunon, M.; Gonzalez-Gonzalez, M.P. The influence of the polyunsaturated fatty acids in the prevention and promotion of cancer. Nutr. Hosp. 2015, 32, 41–49. [Google Scholar]
- Sommer, C.; Birklein, F. Resolvins and inflammatory pain. F1000 Med. Rep. 2011, 3, 19. [Google Scholar] [CrossRef]
- Kwon, Y. Immuno-resolving ability of resolvins, protectins, and maresins derived from omega-3 fatty acids in metabolic syndrome. Mol. Nutr. Food Res. 2020, 64, e1900824. [Google Scholar] [CrossRef]
- Divanovic, S.; Dalli, J.; Jorge-Nebert, L.F.; Flick, L.M.; Gálvez-Peralta, M.; Boespflug, N.D.; Stankiewicz, T.E.; Fitzgerald, J.M.; Somarathna, M.; Karp, C.L.; et al. Contributions of the Three CYP1 Monooxygenases to Pro-Inflammatory and Inflammation-Resolution Lipid Mediator Pathways. J. Immunol. 2013, 191, 3347–3357. [Google Scholar] [CrossRef]
- Serhan, C.N.; Petasis, N.A. Resolvins and Protectins in Inflammation Resolution. Chem. Rev. 2011, 111, 5922–5943. [Google Scholar] [CrossRef]
- Serhan, C.N.; Dalli, J.; Colas, R.A.; Winkler, J.W.; Chiang, N. Protectins and maresins: New pro-resolving families of mediators in acute inflammation and resolution bioactive metabolome. Biochim. Biophys. Acta 2015, 1851, 397–413. [Google Scholar] [CrossRef] [PubMed]
- Norris, P.C.; Arnardottir, H.; Sanger, J.M.; Fichtner, D.; Keyes, G.S.; Serhan, C.N. Resolvin D3 multi-level proresolving actions are host protective during infection. Prostaglandins, Leukot. Essent. Fat. Acids 2016, 138, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Winkler, J.; Orr, S.; Dalli, J.; Chiang, N.; Petasis, N.; Serhan, C. Resolvin D4 Potent Antiiinflammatory Proresolving Actions Confirmed via Total Synthesis. FASEB J. 2015, 29, 285–10. [Google Scholar] [CrossRef]
- Gobbetti, T.; Dalli, J.; Colas, R.A.; Canova, D.F.; Aursnes, M.; Bonnet, D.; Alric, L.; Vergnolle, N.; Deraison, C.; Hansen, T.V.; et al. Protectin D1n-3 DPA and resolvin D5n-3 DPA are effectors of intestinal protection. Proc. Natl. Acad. Sci. USA. 2017, 114, 3963–3968. [Google Scholar] [CrossRef] [PubMed]
- Pham, T.L.; Kakazu, A.H.; He, J.; Jun, B.; Bazan, N.G.; Bazan, H.E.P. Novel RvD6 stereoisomer induces corneal nerve regeneration and wound healing post-injury by modulating trigeminal transcriptomic signature. Sci. Rep. 2020, 10, 4582. [Google Scholar] [CrossRef]
- Marcheselli, V.L.; Mukherjee, P.K.; Arita, M.; Hong, S.; Antony, R.; Kristopher Sheets, K.; Winkler, J.W.; Petasis, N.A.; Serhan, C.N.; Bazan, N.G. Neuroprotectin D1/protectin D1 stereoselective and specific binding with human retinal pigment epithelial cells and neutrophils. Prostaglandins Leukot. Essent. Fatty Acids 2010, 82, 27–34. [Google Scholar] [CrossRef]
- Serhan, C.N.; Yang, R.; Martinod, K.; Kasuga, K.; Pillai, P.S.; Porter, T.F.; Oh, S.F.; Spite, M. Maresins: novel macrophage mediators with potent antiinflammatory and proresolving actions. J. Exp. Med. 2009, 206, 15–23. [Google Scholar] [CrossRef]
- Panigrahy, D.; Gilligan, M.M.; Serhan, C.N.; Kashfi, K. Resolution of inflammation: An organizing principle in biology and medicine. Pharmacol. Ther. 2021, 227, 107879. [Google Scholar] [CrossRef]
- Serhan, C.N.; Dalli, J.; Karamnov, S.; Choi, A.; Park, C.-K.; Xu, Z.-Z.; Ji, R.-R.; Zhu, M.; Petasis, N.A. Macrophage proresolving mediator maresin 1 stimulates tissue regeneration and controls pain. FASEB J. 2012, 26, 1755–1765. [Google Scholar] [CrossRef]
- Sánchez-Fernández, A.; Zandee, S.; Mastrogiovanni, M.; Charabati, M.; Rubbo, H.; Prat, A.; López-Vales, R. Administration of Maresin-1 ameliorates the physiopathology of experimental autoimmune encephalomyelitis. J. Neuroinflammation 2022, 19, 27. [Google Scholar] [CrossRef]
- Xian, W.; Li, T.; Li, L.; Hu, L.; Cao, J. Maresin 1 attenuates the inflammatory response and mitochondrial damage in mice with cerebral ischemia/reperfusion in a SIRT1-dependent manner. Brain Res. 2019, 1711, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Wahyuni, T.; Kobayashi, A.; Tanaka, S.; Miyake, Y.; Yamamoto, A.; Bahtiar, A.; Mori, S.; Kametani, Y.; Tomimatsu, M.; Matsumoto, K.; et al. Maresin-1 induces cardiomyocyte hypertrophy through IGF-1 paracrine pathway. Am. J. Physiol. Cell Physiol. 2021, 321, C82–C93. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Li, X.-Y.; Li, L.-C.; Xiao, J.; Zhu, Y.-M.; Tian, Y.; Sheng, Y.-M.; Chen, Y.; Wang, J.-G.; Jin, S.-W. γδ T/Interleukin-17A Contributes to the Effect of Maresin Conjugates in Tissue Regeneration 1 on Lipopolysaccharide-Induced Cardiac Injury. Front. Immunol. 2021, 12, 674542. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Zhang, Z.; Wang, L.; Jiang, L.; Qin, Z.; Yuliang Zhao, Y.; Su, B. Maresin 1 attenuates lipopolysaccharide-induced acute kidney injury via inhibiting NOX4/ROS/NF-κB pathway. Front. Pharmacol. 2021, 12, 782660. [Google Scholar] [CrossRef]
- Li, X.; Xu, B.; Wu, J.; Pu, Y.; Wan, S.; Zeng, Y.; Wang, M.; Luo, L.; Zhang, F.; Jiang, Z.; et al. Maresin 1 alleviates diabetic kidney disease via LGR6-mediated cAMP-SOD2-ROS pathway. Oxid. Med. Cell. Longev. 2022, 2022, 7177889. [Google Scholar] [CrossRef]
- Soto, G.; Rodríguez, M.J.; Fuentealba, R.; Treuer, A.V.; Castillo, I.; González, D.R.; Zúñiga-Hernández, J. Maresin 1, a Proresolving Lipid Mediator, Ameliorates Liver Ischemia-Reperfusion Injury and Stimulates Hepatocyte Proliferation in Sprague-Dawley Rats. Int. J. Mol. Sci. 2020, 21, 540. [Google Scholar] [CrossRef]
- Rodríguez, M.J.; Sabaj, M.; Tolosa, G.; Herrera Vielma, F.; Zúñiga, M.J.; González, D.R.; Zúñiga-Hernández, J. Maresin-1 prevents liver fibrosis by targeting Nrf2 and NF-κB, reducing oxidative stress and inflammation. Cells 2021, 10, 3406. [Google Scholar] [CrossRef]
- Tang, D.; Fu, G.; Li, W.; Sun, P.; Loughran, P.A.; Deng, M.; Scott, M.J.; Billiar, T.R. Maresin 1 protects the liver against ischemia/reperfusion injury via the ALXR/Akt signaling pathway. Mol. Med. 2021, 27, 18. [Google Scholar] [CrossRef]
- Dalli, J.; Serhan, C.N. Specific lipid mediator signatures of human phagocytes: microparticles stimulate macrophage efferocytosis and pro-resolving mediators. Blood 2012, 120, e60–e72. [Google Scholar] [CrossRef]
- Lim, C.S.; Porter, D.W.; Orandle, M.S.; Green, B.J.; Barnes, M.; Croston, T.L.; Wolfarth, M.G.; Battelli, L.A.; Andrew, M.E.; Beezhold, D.H.; et al. Resolution of pulmonary inflammation induced by carbon nanotubes and fullerenes in mice: Role of macrophage polarization. Front. Immunol. 2020, 11, 1186. [Google Scholar] [CrossRef]
- Titos, E.; Rius, B.; González-Périz, A.; López-Vicario, C.; Morán-Salvador, E.; Martínez-Clemente, M.; Arroyo, V.; Clària, J. Resolvin D1 and Its Precursor Docosahexaenoic Acid Promote Resolution of Adipose Tissue Inflammation by Eliciting Macrophage Polarization toward an M2-Like Phenotype. J. Immunol. 2011, 187, 5408–5418. [Google Scholar] [CrossRef] [PubMed]
- Dalli, J.; Zhu, M.; Vlasenko, N.A.; Deng, B.; Haeggström, J.Z.; Petasis, N.A.; Serhan, C.N. The novel 13S,14S-epoxy-maresinis converted by human macrophages to maresin 1 (MaR1), inhibits leukotriene A4 hydrolase (LTA4H), and shifts macrophage phenotype. FASEB J. 2013, 27, 2573–2583. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.-H.; Shin, K.-O.; Kim, J.-Y.; Khadka, D.B.; Kim, H.-J.; Lee, Y.-M.; Cho, W.-J.; Cha, J.-Y.; Lee, B.-J.; Lee, M.-O. A maresin 1/RORα/12-lipoxygenase autoregulatory circuit prevents inflammation and progression of nonalcoholic steatohepatitis. J. Clin. Investig. 2019, 129, 1684–1698. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Wang, M.; Ye, J.; Zhang, J.; Xu, Y.; Wang, Z.; Zhao, M.; Ye, D.; Wan, J. Maresin 1 alleviates the inflammatory response, reduces oxidative stress and protects against cardiac injury in LPS-induced mice. Life Sci. 2021, 277, 119467. [Google Scholar] [CrossRef] [PubMed]
- 105. Ma, M.Q.; Zheng, S.S.; Chen, H.L.; Xu, H.B.; Zhang, D.L.; Zhang, Y.A.; Xiang, S.Y.; Cheng, B.H.; Jin, S.W.; Fu, P.H. Protectin conjugates in tissue regeneration 1 inhibits macrophage pyroptosis by restricting NLRP3 inflammasome assembly to mitigate sepsis via the cAMP-PKA pathway. Lab. Invest. 2023, 103, 100028. [Google Scholar] [CrossRef] [PubMed]
- Bang, S.; Xie, Y.-K.; Zhang, Z.-J.; Wang, Z.; Xu, Z.-Z.; Ji, R.-R. GPR37 regulates macrophage phagocytosis and resolution of inflammatory pain. J. Clin. Investig. 2018, 128, 3568–3582. [Google Scholar] [CrossRef]
- Kang, J.-W.; Lee, S.-M. Resolvin D1 protects the liver from ischemia/reperfusion injury by enhancing M2 macrophage polarization and efferocytosis. Biochim. et Biophys. Acta (BBA) - Mol. Cell Biol. Lipids 2016, 1861, 1025–1035. [Google Scholar] [CrossRef]
- Shan, K.; Feng, N.; Cui, J.; Wang, S.; Qu, H.; Fu, G.; Li, J.; Chen, H.; Wang, X.; Wang, R.; et al. Resolvin D1 and D2 inhibit tumour growth and inflammation via modulating macrophage polarization. J. Cell. Mol. Med. 2020, 24, 8045–8056. [Google Scholar] [CrossRef]
- Lu, Y.; Xu, Q.; Yin, G.; Xu, W.; Jiang, H. Resolvin D1 inhibits the proliferation of lipopolysaccharide-treated HepG2 hepatoblastoma and PLC/PRF/5 hepatocellular carcinoma cells by targeting the MAPK pathway. Exp. Ther. Med. 2018, 16, 3603–3610. [Google Scholar] [CrossRef]
- Pohl, R.; Rein-Fischboeck, L.; Meier, E.M.; Eisinger, K.; Krautbauer, S.; Buechler, C. Resolvin E1 and chemerin C15 peptide do not improve rodent non-alcoholic steatohepatitis. Exp. Mol. Pathol. 2015, 98, 295–299. [Google Scholar] [CrossRef]
- Kuang, H.; Hua, X.; Zhou, J.; Yang, R. Resolvin D1 and E1 alleviate the progress of hepatitis toward liver cancer in long-term concanavalin A-induced mice through inhibition of NF-κB activity. Oncol. Rep. 2016, 35, 307–317. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez, M.J.; Herrera, F.; Donoso, W.; Castillo, I.; Orrego, R.; González, D.R.; Zúñiga-Hernández, J. Pro-Resolving Lipid Mediator Resolvin E1 Mitigates the Progress of Diethylnitrosamine-Induced Liver Fibrosis in Sprague-Dawley Rats by Attenuating Fibrogenesis and Restricting Proliferation. Int. J. Mol. Sci. 2020, 21, 8827. [Google Scholar] [CrossRef] [PubMed]
- Qiu, W.; Guo, K.; Yi, L.; Gong, Y.; Huang, L.; Zhong, W. Resolvin E1 reduces hepatic fibrosis in mice with Schistosoma japonicum infection. Exp. Ther. Med. 2014, 7, 1481–1485. [Google Scholar] [CrossRef]
- Zhang, P.; Yin, Y.; Wang, T.; Li, W.; Li, C.; Zeng, X.; Yang, W.; i Zhang, R.; Tang, Y.; Shi, L.; et al. Maresin 1 mitigates concanavalin A-induced acute liver injury in mice by inhibiting ROS-mediated activation of NF-κB signaling. Free Radic. Biol. Med. 2020, 147, 23–36. [Google Scholar] [CrossRef]
- Yang, W.; Tao, K.; Zhang, P.; Chen, X.; Sun, X.; Li, R. Maresin 1 protects against lipopolysaccharide/d-galactosamine-induced acute liver injury by inhibiting macrophage pyroptosis and inflammatory response. Biochem. Pharmacol. 2022, 195, 114863. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Du, K.; Jin, N.; Tang, B.; Zhang, W. Macrophage in liver Fibrosis: Identities and mechanisms. Int. Immunopharmacol. 2023, 120, 110357. [Google Scholar] [CrossRef] [PubMed]
- Koncz, G.; Jenei, V.; Tóth, M.; Váradi, E.; Kardos, B.; Bácsi, A.; Mázló, A. Damage-mediated macrophage polarization in sterile inflammation. Front. Immunol. 2023, 14, 1169560. [Google Scholar] [CrossRef]
- Peng, Y.; Zhou, M.; Yang, H.; et al. Regulatory mechanism of M1/M2 macrophage polarization in the development of autoimmune diseases. Mediators Inflamm. 2023, 2023, 8821610. [Google Scholar] [CrossRef]
- Liang, W.; Huang, X.; Shi, J. Macrophages Serve as Bidirectional Regulators and Potential Therapeutic Targets for Liver Fibrosis. Cell Biochem. Biophys. 2023, 81, 659–671. [Google Scholar] [CrossRef]
Figure 1.
Beneficial effects of EPA/DHA on immune and cardiac models. A) DHA treatment in PMN cells promotes PPAR-γ activation with a decrease in the inflammatory response. B) In murine monocytes DHA inhibit TLR4 signaling also translating this to a decrease in inflammation. C) in macrophages DHA through PPAR-γ promotes an hepatoprotector effect decreasing inflammation, steatosis and fibrosis, related to a decrease in plasma triglycerides. EGFR, endothelial growth factor receptor; EPA, eicosapentaenoic acid; DHA, docosahexaenoic acid; LPS, lipopolyssacharide; PMN, polymorphonuclear leukocytes; PPAR, peroxisome proliferator-activated receptors; TLR4, toll-like receptor-4; TRIF, TIR-domain-containing adapter-inducing interferon-β; IFN, interferon; STAT, signal transducer and activator of transcription; TGF-β, Transforming growth factor beta; VEGF, Vascular endothelial growth factor.
Figure 1.
Beneficial effects of EPA/DHA on immune and cardiac models. A) DHA treatment in PMN cells promotes PPAR-γ activation with a decrease in the inflammatory response. B) In murine monocytes DHA inhibit TLR4 signaling also translating this to a decrease in inflammation. C) in macrophages DHA through PPAR-γ promotes an hepatoprotector effect decreasing inflammation, steatosis and fibrosis, related to a decrease in plasma triglycerides. EGFR, endothelial growth factor receptor; EPA, eicosapentaenoic acid; DHA, docosahexaenoic acid; LPS, lipopolyssacharide; PMN, polymorphonuclear leukocytes; PPAR, peroxisome proliferator-activated receptors; TLR4, toll-like receptor-4; TRIF, TIR-domain-containing adapter-inducing interferon-β; IFN, interferon; STAT, signal transducer and activator of transcription; TGF-β, Transforming growth factor beta; VEGF, Vascular endothelial growth factor.
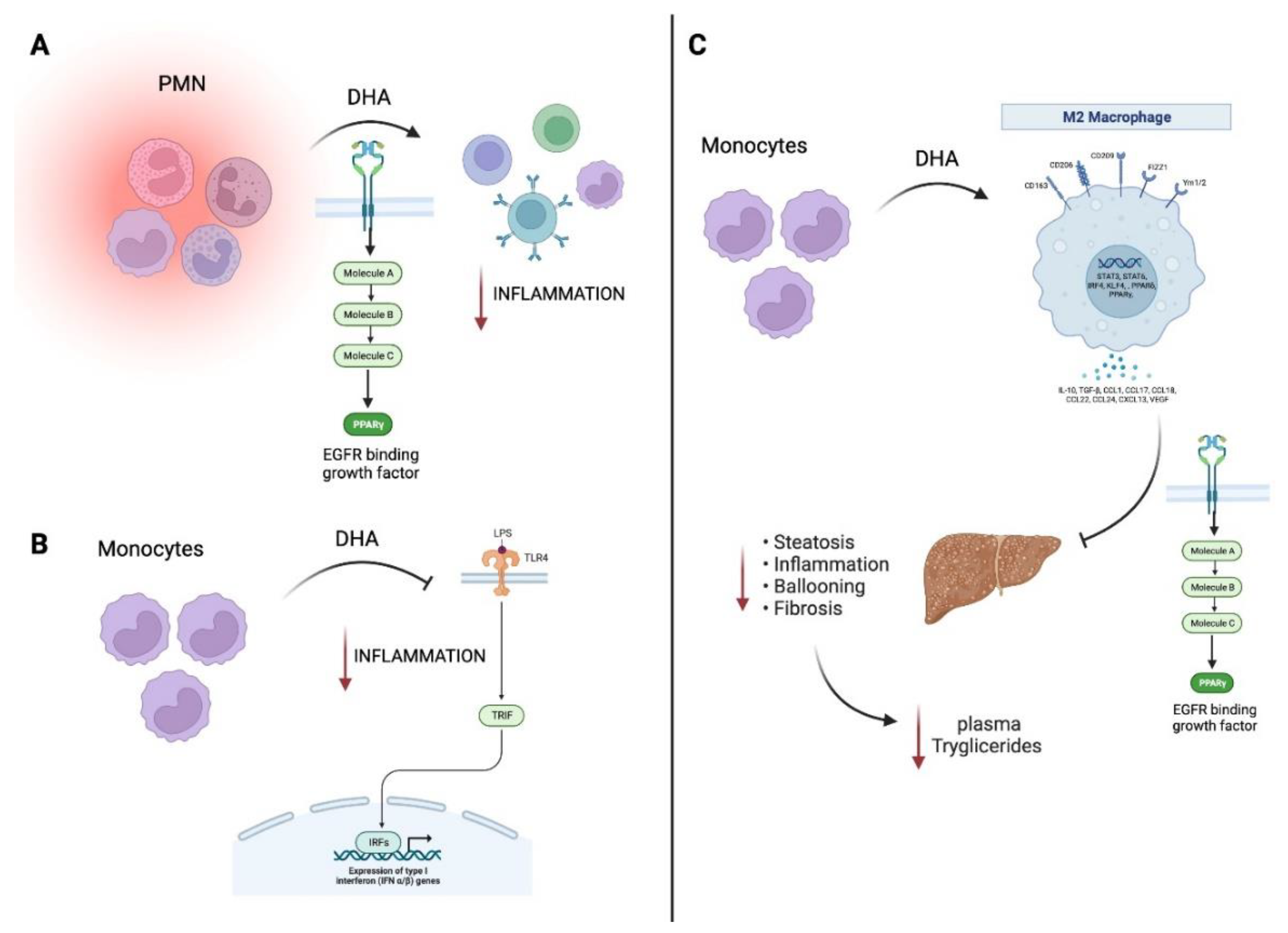
Figure 2.
Specialized pro-resolving mediators (SPM): biosynthetic pathways and macrophage polarization activities. E-series resolvins, D-series resolvins, protectins and maresins are illustrated. ALA, alfa-linoleic acid; EPA, eicosapentaenoic acid; DHA, docosahexaenoic acid; LOX, lipoxygenase; COX, cyclooxygenase; PMN, polymorphonuclear cells.
Figure 2.
Specialized pro-resolving mediators (SPM): biosynthetic pathways and macrophage polarization activities. E-series resolvins, D-series resolvins, protectins and maresins are illustrated. ALA, alfa-linoleic acid; EPA, eicosapentaenoic acid; DHA, docosahexaenoic acid; LOX, lipoxygenase; COX, cyclooxygenase; PMN, polymorphonuclear cells.
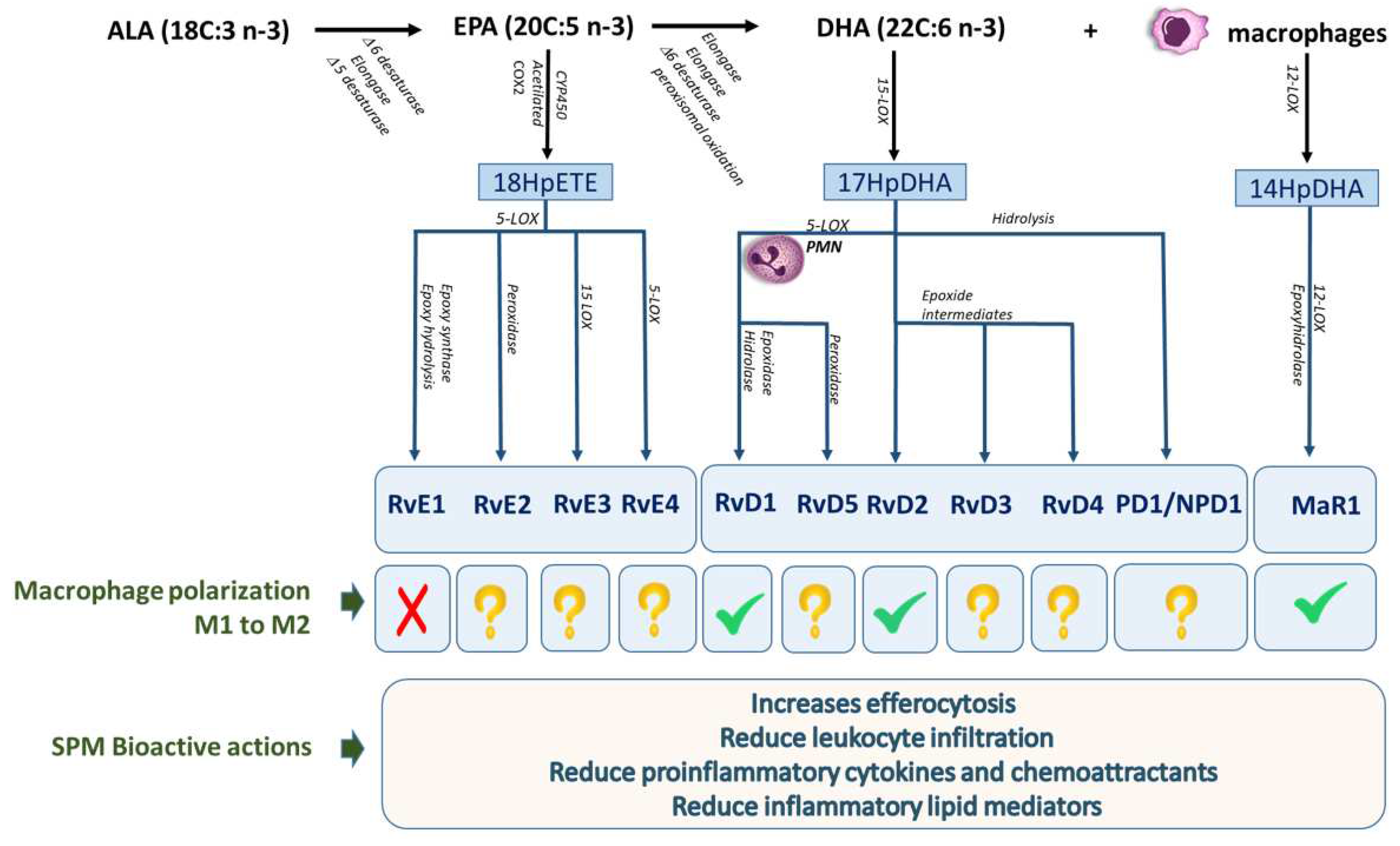

Table 1.
Protective functions of omega-3 related to inflammatory and macrophage modulation.
| Omega-3 | Mechanism | Effect | Model |
|---|---|---|---|
| Clinical trials analysis (A : | EPA+DHA) | ||
| A | Decrease of T helper 2/T helper 1 chemokines | Lower macrophage-derived chemokine/interferon-inducible protein | Cord plasma from newborns from pregnancy-related depressive mothers (prenatal supplementation55 |
| A | Decrease levels of sCD63* | Decrease of triglycerides, waist to height ratio and waist circumference | Type 2 diabetic patients 56 |
| A | Modulation of Wnt/beta-catenine pathways**. | White adipose tissue downregulation of inflammatory pathways with less macrophage infiltration | Obese subjects57 |
| A | Enhance of CD54 macrophages*** | Less T CD8+/T CD4+ after immune challenger and greater production of IL-10 (an anti-inflammatory cytokine) | Children, (ages 5-7 years) who had low intakes of DHA58 |
| A | Less macrophage in atherosclerotic plaques | Improvement of atherosclerotic plaque morphology (tin fibrous cap) | Patients awaiting carotid endartectomy59 |
| Animals model | (A: EPA+DHA) (B: EPA) | (C. EPA or DHA) | |
| A | Attenuated the development and destabilization of atherosclerotic plaques and reduction of TLR4 | Suppressed atherogenesis | Apolipoprotein E-deficient (Apoe-/-) mice60 |
| A | Decreased of TNF-α, MCP-1, TGF β. And arginase 2, this last one is a marker of pro-inflammatory macrophages | Reduction of aneurism formation and macrophage infiltration | Abdominal aortic aneurysm (AAA) animal model61 |
| C | increased levels of resolvin D5, protectin DX and maresin 2 in the mouse skin | Decrease proinflammatory cytokines altered psoriasis macrophage phenotypes and lipid oxidation, modulating psoriasis skin inflammation | K14-Rac1V12 mouse model62 |
| A | Induction of Nrf2 signaling | Decrease proinflammatory cytokines, iNOS and COX-2 | Nrf2 knockout (-/-; KO) mice63 |
| B | Down-regulation of NF-κB activation and regulated genes | Inhibited tubule-interstitial injury and the infiltration of macrophages into tubule-interstitial lesions | Thy-1 nephritis model64 |
| A | Reduce TNFα, caspase-3 and could increasing splenic GSH Bcl-2.Restorating macrophages, B- and T- lymphocytes. | Decrease the Methotrexate-induced histopathological injury. | Methotrexato-induced splenic suppression on Sprague-Dawley rats65 |
| A | Reduced pro-inflammatory macrophages | Promoted wound closure by accelerating the resolution of inflammation | Wound healing in db/db mice 66 |
| A | Reduction of hepatic SREBP-1c and enhancement of PPARγ nuclear receptor | Lower concentration on plasma lipids, triglycerides and liver lipid content. Enhance of endothelial function | HFD in hamsters67 |
* Macrophages activation marker; ** Pathway related to genes involved in adipogenesis; *** Co-stimulatory molecule on antigen-presenting cells that facilitates MHC-restricted immune response. EPA, eicosapentaenoic acid; DHA, docosahexaenoic acid; TLR4, TLR4, toll-like receptor-4; TNF-α, Tumour necrosis factor alpha; MCP-1, Monocyte chemoattractant protein-1; TGF-β, Transforming growth factor beta; Nrf2, nuclear factor erythroid 2-related factor 2; NF-κB, nuclear factor-kappa B; GSH, glutathione; SREBP, sterol regulatory element binding proteins; PPAR, peroxisome proliferator-activated receptors; iNOS, inducible nitric oxide synthase; COX-2, cyclooxygenase-2; HFD, high fat diet.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



