
Submitted:
28 September 2023
Posted:
29 September 2023
You are already at the latest version
Abstract
There is considerable interest in the use of doxycycline post exposure prophylaxis (PEP) to reduce the incidence of bacterial sexually transmitted infections (STIs). An important concern is that this could select for tetracycline resistance in these STIs and other species. We searched PubMed and Google Scholar, (1948–2023) for randomized controlled trials comparing tetracycline PEP with non-tetracycline controls. The primary outcome was antimicrobial resistance (AMR) to tetracyclines in all bacterial species with available data. Our search yielded 140 studies, of which three met the inclusion criteria. Tetracycline PEP had no effect on the prevalence of tetracycline resistance in Neisseria gonorrhoeae in any of the three trials or the pooled estimates. PEP did, however, have a marked effect on the tetracycline MIC distribution in the one study where this was assessed. Prophylactic efficacy was 100% at low MICs and 0% at high MICs. In the one study where this was assessed, PEP resulted in a significant increase in tetracycline resistance in commensal Neisseria species compared to the control group but no significant effect on the prevalence of tetracycline resistance in Staphylococcus aureus. The available evidence suggests that PEP with tetracyclines could be associated with selecting tetracycline resistance in N. gonorrhoeae and commensal Neisseria species.
Keywords:
doxycycline PEP
; tetracycline
; minocycline
; AMR
; PrEP
; gonorrhoea
1. Introduction
Four recently randomized controlled trials (RCTs) have found that doxycycline post exposure prophylaxis (PEP) can reduce the incidence of chlamydia and syphilis in men who have sex with men (MSM) (1-4). Three of these trials found a reduced incidence of gonorrhoea. The median doxycycline consumption in these trials ranged from 8 to 30 defined daily doses (DDD) per month, which raised concerns that doxycycline PEP could induce tetracycline resistance in a range of bacterial species (1, 3, 5). Only two of these RCTs have evaluated the effect of doxycycline on tetracycline resistance in N. gonorrhoeae. Both found no statistically significant effect, but the duration of follow-up was short, and the number of gonococcal isolates tested were small (n=9 (1) and n=47 (3)). In addition, one of these RCTs evaluated the effect of doxycycline PEP on the prevalence of doxycycline resistance in Staphylococcus aureus and commensal Neisseria species (3, 6). They reported no increase in resistance in these species. The authors of these studies have concluded that the risk of antimicrobial resistance (AMR) is small or non-existent (1, 3, 6). These conclusions have, in turn, led to doxycycline PEP being offered to MSM attending certain STI clinics (7).
In contrast, an RCT in women in Africa found that doxycycline PEP had no effect on the incidence of chlamydia, gonorrhoea or syphilis (8). An older RCT from 1979 in men in the US Navy found that although minocycline PEP reduced the incidence of gonorrhoea by 54% overall, this effect was driven by a reduction in the incidence of gonococcal infections with low minocycline MICs (9). Minocycline PEP had no effect on the incidence of infections with higher tetracycline MICs. The authors concluded that minocycline PEP would likely select for gonococcal AMR and was thus not advisable.
These contrasting findings provided the motivation to conduct this systematic review to summarize the available evidence from RCT as to the association between tetracycline PEP and tetracycline resistance in all bacterial species with available data.
2. Materials and methods
This review was performed according to the PRISMA guidelines (10). All the steps were performed independently by two reviewers (CK and TV). The PRISMA checklists are presented in STable 1.
Search strategy
PubMed and Google Scholar were searched for articles and conference abstracts published between 1 March 1948 (first report of tetracyclines in the scientific literature) and 30/4/2023. Reference lists of relevant articles were checked for additional titles for inclusion in the review. Keywords used for the search included “postexposure prophylaxis”, “tetracycline”, “doxycycline”, “minocycline”, “sexually”, and “gonorrhoea.” (STable 2).
Selection process and criteria
The titles and abstracts of all the articles were screened by two independent reviewers (CK and TV). Duplicates were then manually removed.
Studies were included or excluded according to the following predefined criteria:
Inclusion criteria
1. Randomized controlled trial study design
2. Compare the efficacy of tetracycline with either placebo or no treatment for reducing the incidence of bacterial STIs (syphilis/gonorrhoea/chlamydia)
3. Abstracts and full text available
4. Report the prevalence of tetracycline resistance in any bacterial species at baseline and study end
Data extraction and synthesis
Data on study characteristics and outcomes were extracted by two review authors (CK and TV) into the Review Manager software (RevMan, version 5.4.1, Cochrane, London, UK).
Two types of resistance data were extracted:
- Tetracycline MIC distribution of isolates. The tetracycline MIC distribution of isolates per species of the two arms post PEP were compared with the Mann-Whitney test.
- The proportion of isolates resistant to tetracycline. This variable was calculated for each bacterial species as the number of individuals with tetracycline resistant isolates cultured per total number of individuals with this same species cultured. If only MIC distribution was available, we calculated the proportion of tetracycline resistance using the resistance thresholds used in the other studies included this review, in order to allow for comparison (≥ 1 or 2 mg/L). The number of events and the number of participants included in the control and intervention groups of each study were extracted. Data was extracted for all bacterial species with available data.
- Tetracycline MIC distribution of isolates. This data was only available for N. gonorrhoeae from a single study. The tetracycline MIC distribution of gonococcal isolates per species of the two arms for the tetracycline and placebo groups post PEP were compared with the Mann-Whitney test.
The Odds ratio (OR) and the 95% confidence intervals were calculated for the proportion of isolates resistant to tetracycline. Heterogeneity was assessed via the I2 statistics and the p- value of the chi-square statistics. A random-effect model was used to combine the results for the meta-analysis. Publication bias was not assessed as only three studies were assessed. All analyses were conducted in Review Manager software (RevMan, version 5.4.1, Cochrane, London, UK) or STATA v16.1. When necessary, data from figures were digitized using WebPlotDigitizer (https://apps.automeris.io/wpd/).
Risk of bias assessment
The risk of bias was assessed by two independent reviewers (CK and TV) using the Cochrane risk-of-bias tool for randomised trials version 2 (RoB 2). As prescribed by the RoB 2 tool, each study was assessed in six domains: (1) randomisation process, (2) allocation concealment, (3) blinding of participants and personnel, (4) blinding of outcome assessment, (5) incomplete outcome data, and (6) selective reporting. Each domain was assessed as ‘low risk of bias’, ‘some concerns’ or ‘high risk of bias’. The assessment for domains 5 and 6 was based on outcome data for culture and tetracycline susceptibility testing of N. gonorrhoeae since this was an outcome of each included study and a primary objective of our analysis. Assessment of each of the 6 domains led to an overall risk of bias assessment. Any disagreements were resolved by discussion between the two reviewers.
3. Results
Study characteristics
The literature search identified 140 studies (Figure 1). Of these, 49 were excluded due to duplication, 54 were excluded based on title and abstract, and 37 full-text articles were reviewed. Five of these articles met the inclusion criteria and were included in the review (Table 1). These five articles described the findings of three RCTs. All three of these RCTs reported tetracycline resistance in N. gonorrhoeae, one in commensal Neisseria spp., one in Mycoplasma genitalium, and one in Staphylococcus aureus. In one of these RCTs, the authors only reported the MIC distribution of individual isolates, for the two remaining RCTs only the proportion of resistant isolates were reported, without individual MICs (Table 1).
Assessment of risk of bias
The Molina study was an open label study and thus at high risk for bias for allocation concealment and blinding of participants and staff (Figure 2). Both the Molina and Luetkemeyer studies had low culture positivity rates for N. gonorrhoeae. In the Molina study, for example, of the 57 incident gonococcal infections detected, culture was only attempted in 28 and was only successful in 9 infections. Because the Molina study was not blinded, it is possible that there was a selection bias in which infections were subjected to culture. The Luetkemeyer study had considerable attrition of samples at the later study visits (Figure 2; Table 1). The Molina and Luetkemeyer studies were longitudinal studies of cohorts from defined geographical areas. Participants from one arm could have sex with participants from the other arm or partners of these individuals. This could lead to contamination and a bias to the null hypothesis (11). The cross-sectional nature of the Harrison study meant it would not be expected to be affected by such a bias.
Tetracycline resistance in N. gonorrhoeae
- Proportion resistant
There was no statistically significant difference in the prevalence of tetracycline resistance in N. gonorrhoeae between the tetracycline and placebo arms in any of the three trials regardless of whether resistance was defined as ≥ 1 or ≥ 2 mg/L. There was also no significant difference in the pooled estimates (OR 2.3; 95% CI 0.9-5.9; Table 2). This pooled estimate was comprised of the proportion resistant at ≥1 mg/L for the Molina study and ≥2 mg/L for the other two studies (Table 3).
- Effect on MIC distribution
The N. gonorrhoeae tetracycline MICs were significantly higher in the minocycline (median 2mg/L IQR 1.5-2.5 mg/L) than the placebo arm (median 1.5 mg/L IQR 1-2 mg/L; P = 0.0018; Figure 3). None of the gonococcal isolates in the minocycline arm had MICs <1.5mg/L whereas 10/44 (22.7%) of the isolates in the placebo arm had MICs in this range (Figure 3).
Tetracycline resistance in commensal Neisseria species
The prevalence of tetracycline resistance in commensal Neisseria species was higher in the tetracycline than the placebo arm in the Luetkemeyer study - the only study where this was assessed (OR 2.9, 95% CI 1.5-5.4; Table 4).
Tetracycline resistance in Staphylococccus aureus
There was no statistically significant difference in the prevalence of tetracycline resistance in S. aureus between the tetracycline and placebo arms in the only study where this was assessed (Luetkemeyer study; OR 2.1; 95% CI 0.4-12.0; Table 5).
Tetracycline resistance in Mycoplasma genitalium
The number of samples analyzed for 16s rRNA mutations at baseline (n=11) and 6 months (n=5) was very small in the only study where this was assessed (Molina study). At 6 months, there was no statistically significant difference in the prevalence of suspected tetracycline resistance between the tetracycline (1/2) and no tetracycline arms (0/3) (12).
4. Discussion
Our review identified differing results according to how the effect of PEP on tetracycline susceptibility was assessed. When assessed according to the proportion of gonococcal isolates resistant to tetracycline (≥1 or ≥2mg/L), there was no statistically significant difference in the prevalence of tetracycline resistance between the tetracycline and placebo arms in any of the three trials. However, when MIC distribution was used as the outcome, PEP had a pronounced effect. In the Harrison study, which was the only study where MIC distributions were assessed, the calculated efficacy of PEP varied from 100% if the MICs were <1mg to around 50% with intermediate MICs and 0% with MICs >2mg/L (Figure 4). It would be useful to assess if MIC distributions were similarly affected in the other two RCTs. We have requested this MIC distribution data from these RCTs, but the corresponding authors were unable to provide this data in the available time.
An important reason for the difference between these two outcome measures may be that changes in MIC distribution is a more sensitive measure of the impact of an antimicrobial than the proportion of isolates that are resistant where MIC distribution is dichotomized into resistant or susceptible. This process of dichotomization results in a loss of information which, particularly in the setting of small sample sizes, increases the probability of type II errors, and the probability of determining between group differences may be affected by the tetracycline concentration used to define resistance (STable 3) (13). The Harrison study also found that the incubation period of gonorrhoea was longer in the minocycline group than in the placebo group. Furthermore, in the minocycline (but not the placebo) group, the mean incubation period was longer in isolates with MICs ≤ 2 mg/L (2.7 days) versus those with MICs > 2 mg/L (5.6 days) (9). These findings provide further evidence that minocycline was exerting a differential effect according to minocycline susceptibility.
The study with the largest number and proportion of gonococcal isolates assessed for tetracycline susceptibility was the Harrison study. This study found that the prophylactic efficacy of minocycline varied from 0% to 100% in highly versus poorly susceptible isolates (Figure 4). The authors concluded that this differential efficacy would be expected to place significant selection pressure for the emergence of gonococcal resistance to tetracyclines. As a result, they argued against the introduction of minocycline PEP. This conclusion is commensurate with the conclusions derived from other strategies involving the mass use of antimicrobials to reduce the incidence of STIs and related pathogens. A number of placebo controlled trials in the 1940s found that oral penicillin and sulfathiazole PEP reduced the incidence of syphilis, chancroid and gonorrhoea (14, 15). However, as early as 1949, concerns were raised about the effects on antimicrobial resistance (14). Likewise, efforts to control gonorrhoea through the mass administration of penicillin in Greenland in the 1950s resulted in a small, temporary reduction in gonococcal prevalence but at the expense of a large increase in penicillin resistance (16). Mass treatment to reduce meningococcal carriage has similarly been noted to reduce prevalence but at the expense of AMR. As an example, sulfadiazine was used extensively in the US military to prevent meningococcal disease from the 1950s, but this usage was stopped in the 1960s when this programme was implicated in the rapid and extensive emergence of AMR (17). These findings led researchers to urge caution in the widespread use of antimicrobials to reduce the prevalence of these bacteria (9, 16, 17). RCTs of doxycycline versus placebo to prevent travellers’ diarrhoea have come to similar conclusions (18-20). As an example, an RCT found that doxycycline reduced the incidence of travellers’ diarhoea, but at the cost of a higher prevalence of doxycycline resistance – 100% versus 53.3% in the doxycycline and placebo arms, respectively (18). This plus the risk of microbiome disruption and increased probability of acquiring other multidrug resistant bacteria has led guideline committees to recommend against the routine use of antimicrobials to prevent travellers’ diarrhoea (20, 21).
As far as the commensal Neisseria spp., were concerned, the prevalence of tetracycline resistance at the end of the Luetkemeyer study was higher in the doxycycline than in the placebo recipients (6). This finding was in contrast to the lack of difference found in this study in gonococcal tetracycline resistance. One possible explanation is the larger sample size of commensal Neisseria (n=176) compared to N. gonorrhoeae (n=27) isolates evaluated. Of note, the odds ratio point estimate for tetracycline resistance between arms for N. gonorrhoeae (OR 4.4) was similar to that for the commensal Neisseria spp. (OR 2.9; Table 2 and Table 3). Other explanations are, however, possible increase in tetracycline resistance between baseline and month 12 in the doxycycline arm was not statistically significant. The difference in tetracycline resistance between arms at month 12 was driven predominantly by a reduced prevalence of tetracycline resistance in the placebo arm at month 12 (STable 4). The sample sizes at month 12 were roughly one-third of the size as the baseline, meaning that the lower prevalence of tetracycline resistance in the placebo arm at month 12 may represent stochastic variations related to small sample sizes.
Our review only identified three studies for inclusion. For the Molina and Luetkemeyer studies, there was a risk of contamination between arms, the number of isolates of N. gonorrhoeae cultured was very low, and these isolates comprised a small proportion of all incident infections. The problems in these two studies were compounded by them not considering the effect on MIC distributions. These considerations mean that we need to be cautious about the conclusions we draw. A number of other limitations are important. The selected studies span 4 decades, were performed in heterogenous populations, used different methods for the diagnosis of N. gonorrhoeae (urethral culture versus nucleic acid amplification tests of urine/pharyngeal/rectal samples), and the circulating N. gonorrhoeae in the various studies likely had different tetracycline MICs at baseline. In addition to selecting for resistance to tetracyclines, tetracycline PEP could select for resistance to other classes of antimicrobials via bystander selection (22-24). This bystander effect could be in STIs or other bacteria. Antimicrobials have also been shown to select for AMR at both individual and population levels (25, 26). We were unable to evaluate these risks as none of the studies we included in this review evaluated these effects. A different systematic review has, however, noted a number of examples of studies where tetracycline use resulted in reduced susceptibility to tetracyclines in a range of bacterial species (27). Future studies are required to assess the effects of tetracycline PEP on other important parameters, such as bacterial tolerance to antimicrobials and the human associated microbiome (5). By reducing the incidence of gonorrhoea, chlamydia and syphilis, doxycycline PEP could reduce the use of broad-spectrum antimicrobials and thereby prevent the emergence of AMR. We were unable to evaluate this hypothesis in our review. Conversely, doxycycline PEP could select for collateral resistance in other antimicrobials (5). To our knowledge, the only doxycycline PEP study where this has been assessed, was a substudy of the Molina study which found that doxycycline PEP did not have an effect on the prevalence of macrolide and fluoroquinolone resistance in Mycoplasma genitalium (12). However, this substudy was limited by a very small sample size, as only five Mycoplasma genitalium isolates are reported after six months of doxycycline PEP.
We conclude that the available evidence suggests that PEP with tetracyclines such as doxycycline and minocycline is associated with selecting tetracycline resistance in N. gonorrhoeae and commensal Neisseria species.
Author Contributions
CK, TV and SMB conceptualized the study and performed the systematic review. CK was responsible for the statistical analyses and writing the first draft. All authors read and approved the final draft.
Funding
Nil.
Consent for publication
Not applicable.
Acknowledgments
Nil.
Conflicts of Interest
The authors declare that they have no competing interests.
References
- Molina, J.-M.; Charreau, I.; Chidiac, C.; Pialoux, G.; Cua, E.; Delaugerre, C.; Capitant, C.; Rojas-Castro, D.; Fonsart, J.; Bercot, B.; et al. Post-exposure prophylaxis with doxycycline to prevent sexually transmitted infections in men who have sex with men: an open-label randomised substudy of the ANRS IPERGAY trial. Lancet Infect. Dis. 2018, 18, 308–317. [CrossRef]
- Bolan RK, Beymer MR, Weiss RE, et al. Doxycycline prophylaxis to reduce incident syphilis among HIV-infected men who have sex with men who continue to engage in high risk sex: a randomized, controlled pilot study. Sexually transmitted diseases. 2015;42(2):98. [CrossRef]
- Luetkemeyer, A.F.; Donnell, D.; Dombrowski, J.C.; Cohen, S.; Grabow, C.; Brown, C.E.; Malinski, C.; Perkins, R.; Nasser, M.; Lopez, C.; et al. Postexposure Doxycycline to Prevent Bacterial Sexually Transmitted Infections. New Engl. J. Med. 2023, 388, 1296–1306. [CrossRef]
- Jean-Michel Molina BB, Lambert Assoumou, Algarte-Genin Michele, et al,. ANRS 174 DOXYVAC: an open-label randomized trial to prevent STIs in MSM on PrEP. CROI 2023, Seattle, Washington.
- Kong, F.Y.S.; Kenyon, C.; Unemo, M. Important considerations regarding the widespread use of doxycycline chemoprophylaxis against sexually transmitted infections. J. Antimicrob. Chemother. 2023, 78, 1561–1568. [CrossRef]
- Luetkemeyer AF, Donnell D, Dombrowski JC, et al. DoxyPEP and antimicrobial resistance in N. gonorrhoeae, commensal Neisseria and S. aureus. CROI 2023, Seattle, Washington.
- Population Health Division San Francisco Department of Health. Doxycycline Post-Exposure Prophylaxis Reduces Incidence of Sexually Transmitted Infections. 2022.
- Stewart J, Bukusi E, Sesay FA, et al. Doxycycline postexposure prophylaxis for prevention of stis among cisgender women. CROI 2023, Seattle, Washington. 2022;23(1):495. [CrossRef]
- Harrison, W.O.; Hooper, R.R.; Wiesner, P.J.; Campbell, A.F.; Karney, W.W.; Reynolds, G.H.; Jones, O.G.; Holmes, K.K. A Trial of Minocycline Given after Exposure to Prevent Gonorrhea. New Engl. J. Med. 1979, 300, 1074–1078. [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88. [CrossRef]
- Torgerson DJ. Contamination in trials: is cluster randomisation the answer? Bmj. 2001;322(7282):355-7. [CrossRef]
- Berçot, B.; Charreau, I.; Rousseau, C.; Delaugerre, C.; Chidiac, C.; Pialoux, G.; Capitant, C.; Bourgeois-Nicolaos, N.; Raffi, F.; Pereyre, S.; et al. High Prevalence and High Rate of Antibiotic Resistance of Mycoplasma genitalium Infections in Men Who Have Sex With Men: A Substudy of the ANRS IPERGAY Pre-exposure Prophylaxis Trial. Clin. Infect. Dis. 2020, 73, e2127–e2133. [CrossRef]
- Fedorov V, Mannino F, Zhang R. Consequences of dichotomization. Pharmaceutical Statistics: The Journal of Applied Statistics in the Pharmaceutical Industry. 2009;8(1):50-61. [CrossRef]
- Eagle, H.; Gude, A.V.; Beckmann, G.E.; Mast, G.; Sapero, J.J.; Shindledecker, J.B. PREVENTION OF GONORRHEA WITH PENICILLIN TABLETS. JAMA 1949, 140, 940–3. [CrossRef]
- Loveless JA, Denton W. The oral use of sulfathiazole as a prophylaxis for gonorrhea Journal of the American Medical Association. 1943;121(11):827-8. [CrossRef]
- Kenyon, C.; Laumen, J.; Van Dijck, C. Could Intensive Screening for Gonorrhea/Chlamydia in Preexposure Prophylaxis Cohorts Select for Resistance? Historical Lessons From a Mass Treatment Campaign in Greenland. Sex. Transm. Dis. 2019, 47, 24–27. [CrossRef]
- Millar, J.W.; Siess, E.E.; Feldman, H.A.; Silverman, C.; Frank, P. In Vivo and In Vitro Resistance to Sulfadiazine in Strains of Neisseria Meningitidis. JAMA 1963, 186, 139–141. [CrossRef]
- DA S, DC K, Sack R. Prophylactic doxycycline for travelers diarrhea. Results of a prospective double-blind study of Peace Corps volunteers in Kenya. N Engl J Med. 1978;298:758-63. [CrossRef]
- Sack, R.B.; Santosham, M.; Froehlich, J.L.; Medina, C.; Orskov, F.; Orskov, I. Doxycycline Prophylaxis of Travelers' Diarrhea in Honduras, an Area where Resistance to Doxycycline is Common among Enterotoxigenic Escherichia coli *. Am. J. Trop. Med. Hyg. 1984, 33, 460–466. [CrossRef]
- Kantele, A.; Laaveri, T.; Mero, S.; Vilkman, K.; Pakkanen, S.H.; Ollgren, J.; Antikainen, J.; Kirveskari, J. Antimicrobials Increase Travelers' Risk of Colonization by Extended-Spectrum Betalactamase-Producing Enterobacteriaceae. Clin. Infect. Dis. 2015, 60, 837–846. [CrossRef]
- Riddle, M.S.; Connor, B.A.; Beeching, N.J.; DuPont, H.L.; Hamer, D.H.; Kozarsky, P.; Libman, M.; Steffen, R.; Taylor, D.; Tribble, D.R.; et al. Guidelines for the prevention and treatment of travelers’ diarrhea: a graded expert panel report. J. Travel Med. 2017, 24, S63–S80. [CrossRef]
- Sanders CC, Sanders Jr WE, Goering RV, et al. Selection of multiple antibiotic resistance by quinolones, beta-lactams, and aminoglycosides with special reference to cross-resistance between unrelated drug classes. Antimicrobial agents and chemotherapy. 1984;26(6):797-801. [CrossRef]
- Tedijanto, C.; Olesen, S.W.; Grad, Y.H.; Lipsitch, M. Estimating the proportion of bystander selection for antibiotic resistance among potentially pathogenic bacterial flora. Proc. Natl. Acad. Sci. 2018, 115, 201810840–E11995. [CrossRef]
- Vanbaelen T, Manoharan-Basil SS, Kenyon C. Doxycycline Post Exposure Prophylaxis could induce cross-resistance to other classes of antimicrobials in Neisseria gonorrhoeae: an in-silico analysis. Sexually Transmitted Diseases. 2023.
- Kenyon, C.R.; Schwartz, I.S. Effects of Sexual Network Connectivity and Antimicrobial Drug Use on Antimicrobial Resistance inNeisseria gonorrhoeae. Emerg. Infect. Dis. 2018, 24, 1195–1203. [CrossRef]
- Lipsitch, M.; Samore, M.H. Antimicrobial Use and Antimicrobial Resistance: A Population Perspective. Emerg. Infect. Dis. 2002, 8, 347–354. [CrossRef]
- Truong, R.; Tang, V.; Grennan, T.; Tan, D.H.S. A systematic review of the impacts of oral tetracycline class antibiotics on antimicrobial resistance in normal human flora. JAC-Antimicrobial Resist. 2022, 4, dlac009. [CrossRef]
Figure 1.
PRISMA flowchart of study selection.
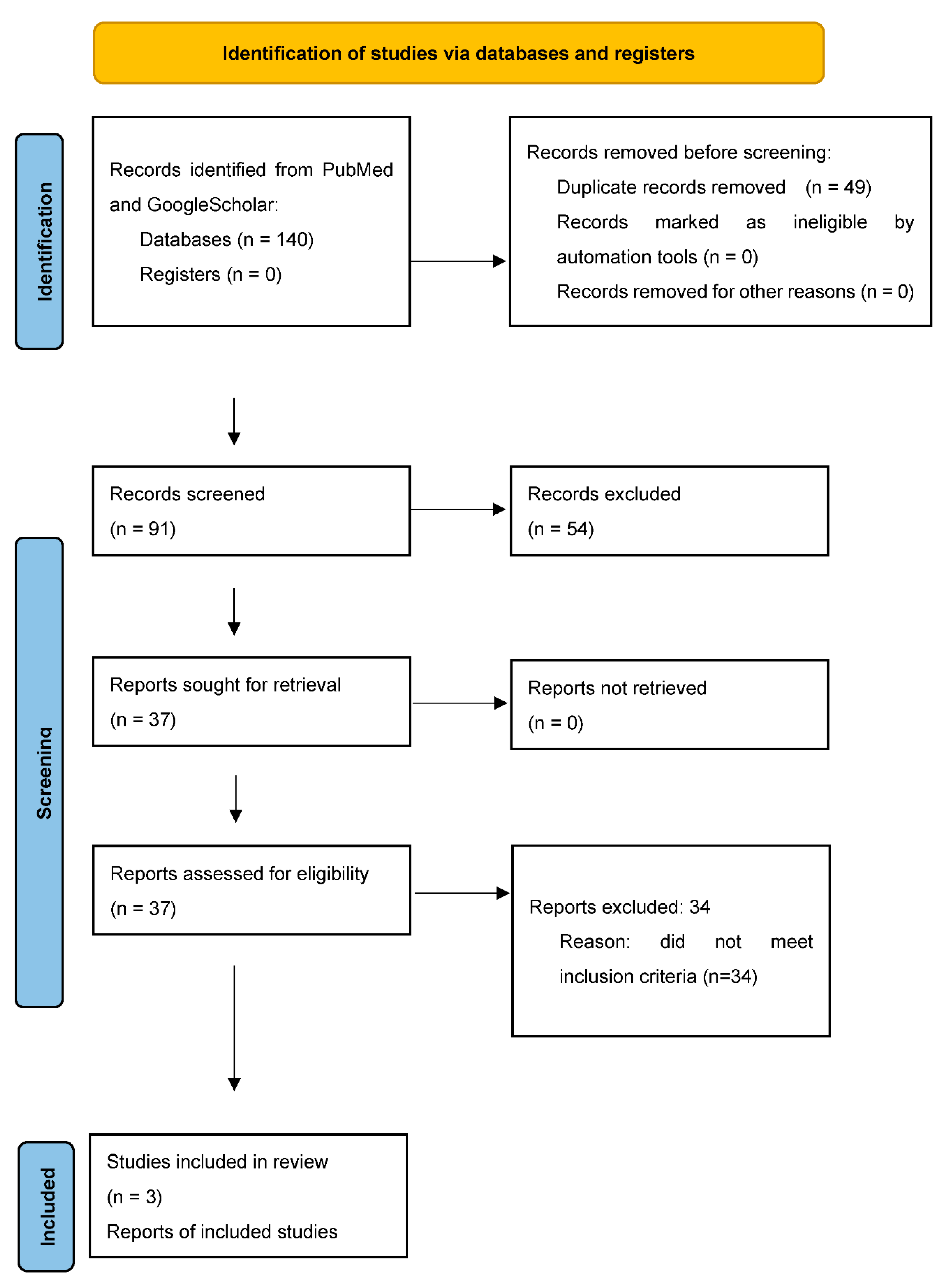
Figure 2.
Risk of bias assessment.
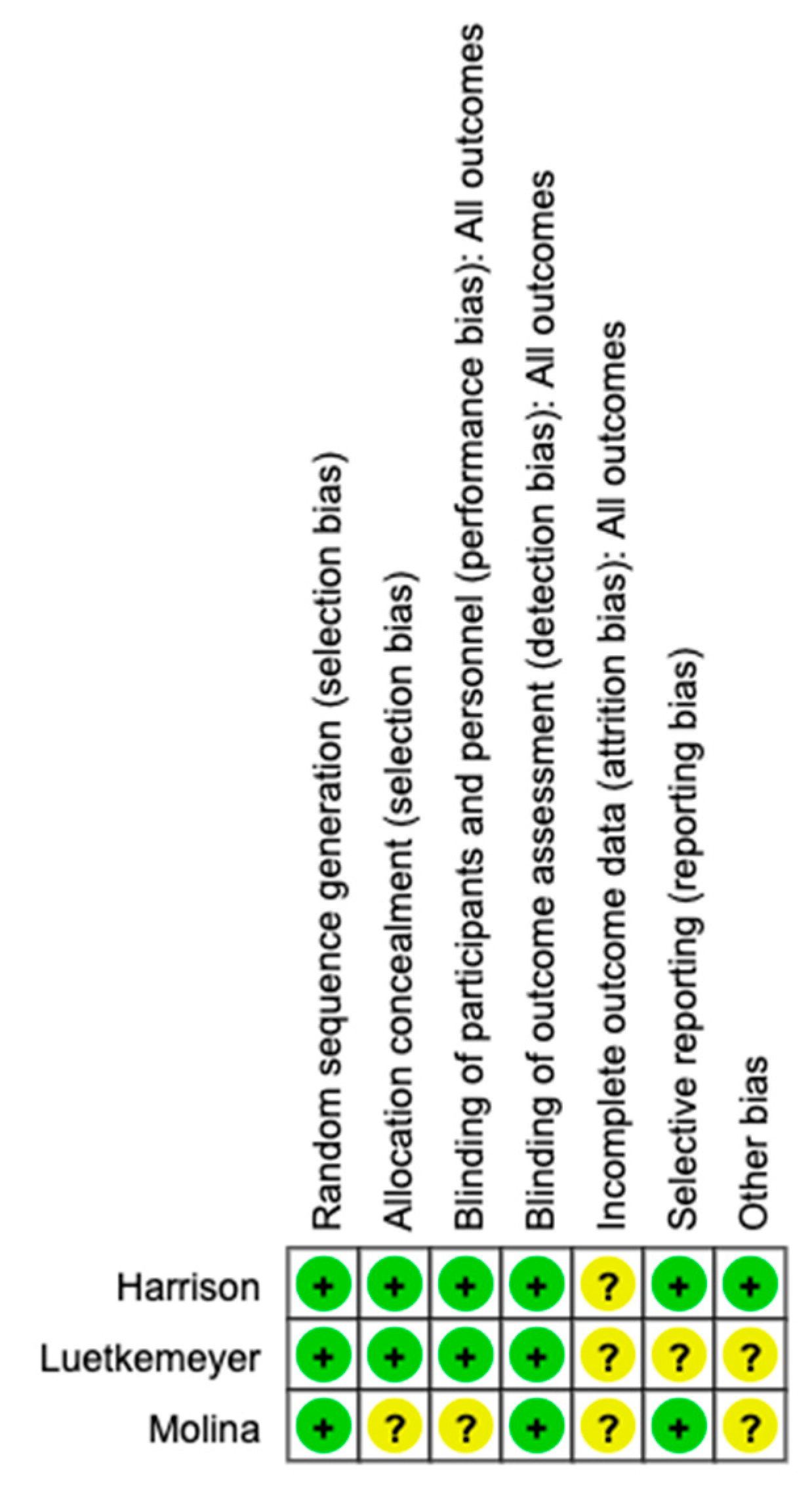
Figure 3.
Histograms of the Neisseria gonorrhoeae tetracycline MIC distributions in the placebo and minocycline PEP arms of the Harrison et al., study (P = 0.0018, Mann Whitney test).
Figure 3.
Histograms of the Neisseria gonorrhoeae tetracycline MIC distributions in the placebo and minocycline PEP arms of the Harrison et al., study (P = 0.0018, Mann Whitney test).
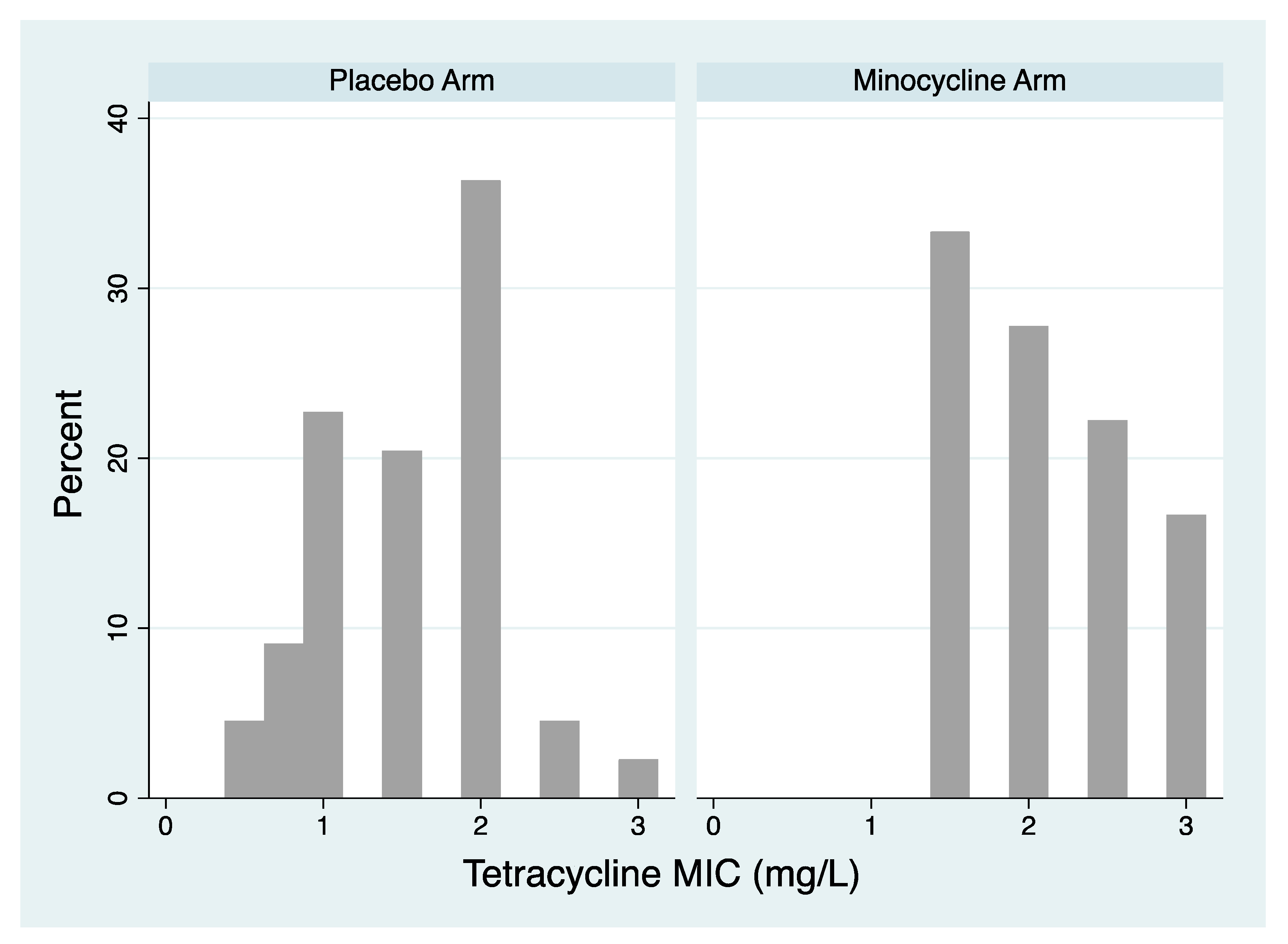
Figure 4.
Illustration of the relationship between gonococcal tetracycline MIC and calculated prophylactic efficacy of minocycline in preventing gonorrhoea in the Harrison study. Prophylactic efficacy is defined as the calculated percent of gonorrhoea cases prevented. (Figure produced by the digitalization of two figures in Harrison et al. (9)).
Figure 4.
Illustration of the relationship between gonococcal tetracycline MIC and calculated prophylactic efficacy of minocycline in preventing gonorrhoea in the Harrison study. Prophylactic efficacy is defined as the calculated percent of gonorrhoea cases prevented. (Figure produced by the digitalization of two figures in Harrison et al. (9)).
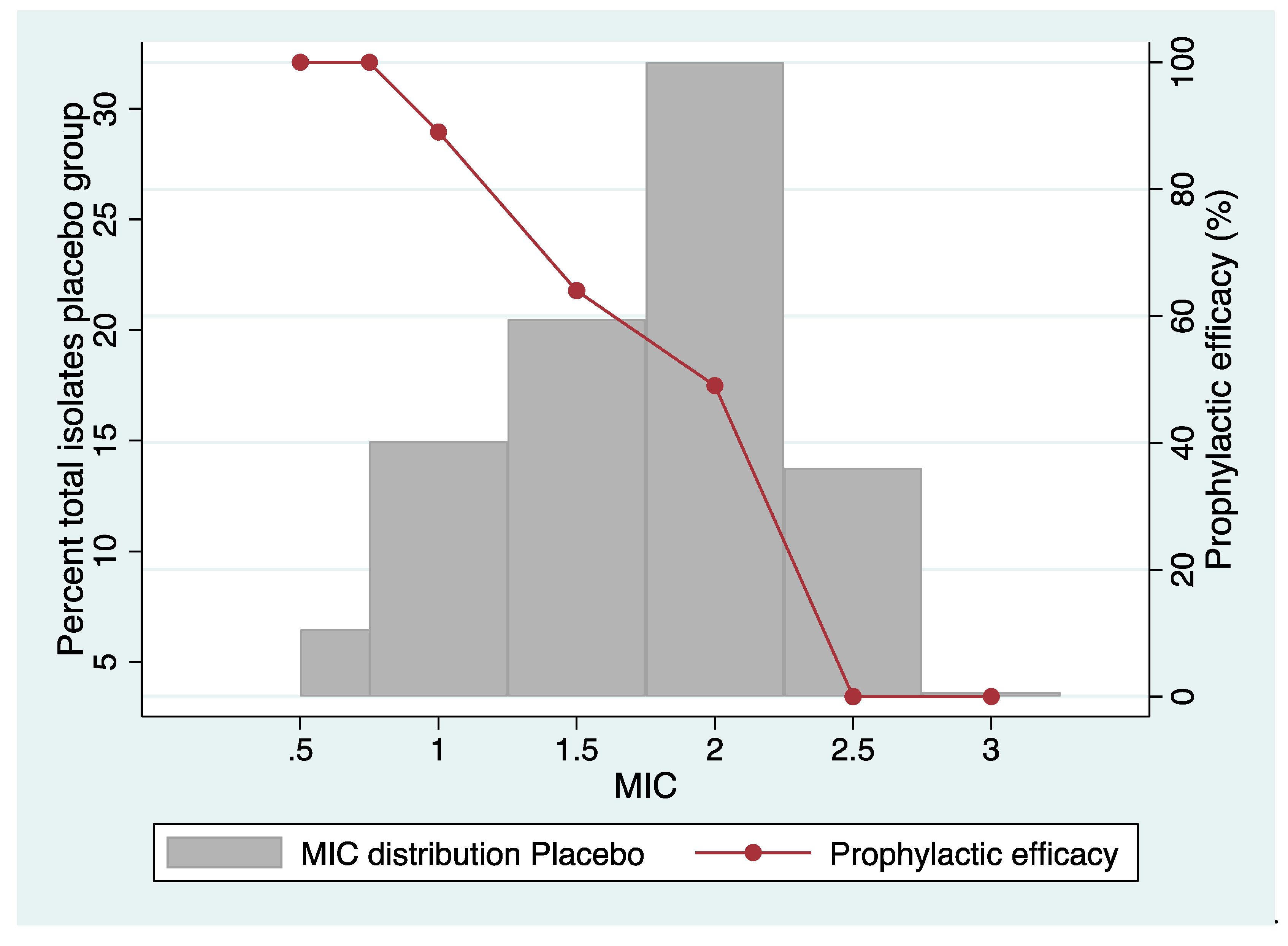

Table 1.
Selected characteristics of the studies included in the systematic review.
| Study, Year of publication, references | Target bacterial species assessed for tetracycline susceptibility | Country | Study Population/method | PEP protocol | MIC testing methodology | Primary outcome |
|---|---|---|---|---|---|---|
| Harrison 1979 (9) |
N. gonorrhoeae | USA | 1080 men from a US Navy ship after sexual exposure during 2 periods of leave in a port in East Asia randomized to either 200mg minocycline or placebo after each sexual exposure, but maximum 200mg per 18 hour period. 815 of these men were reinterviewed and had urethral samples taken at a single time point. MIC results available for 62 isolates of N. gonorrhoeae out of 81 incident N. gonorrhoeae infections. | 200mg minocycline after each sexual exposure (median time between sex and PEP 8 hours, range 30min-36 hours) | Agar dilution with tetracycline. MICs of each isolate reported. Threshold for definition of tetracycline resistance not defined |
Overall, 54% reduction in culture positive urethral gonorrhoea. No effect on infections with elevated minocycline MIC |
| Molina 2018 (1, 12) |
N. gonorrhoeae, M. genitalium | France | 232 MSM randomized 1:1 to doxycycline (200mg) or no prophylaxis within 24 hours post each episode of condomless sex. Follow up was 10 months. NG tested for via quarterly NG PCR of the pharynx/rectum/urine. Primary analysis mITT. The primary outcome was the occurrence of a first STI, defined as first episode of syphilis, chlamydia, or gonorrhoea infection. MIC results were provided for 9 isolates of N. gonorrhoeae out of 57 incident N. gonorrhoeae infections. Culture was only attempted in 28 of the infections. | 200mg doxycycline within 24 hours after condomless sex | Agar dilution with tetracycline. Resistance defined as ≥1mg/L. Only proportion of resistant isolates were reported (MICs of each isolate were not reported) | Occurrence of a first STI was lower in the doxyPEP arm than in the placebo arm (HR 0.53). Doxycycline reduced the occurrence of a first episode of chlamydia (HR 0.3) and syphilis (HR 0.27). The effect on gonorrhoea was not significant. |
| Luetkemeyer 2023 (3, 6) | N. gonorrhoeae, commensal Neisseria species, S. aureus | USA | 501 MSM and transgender women (327 in the PrEP cohort and 174 in the PLWH cohort), with a history of chlamydia, gonorrhoea or syphilis in the past 12 months were randomized 2:1 to doxycycline (200mg) or placebo within 72 hours post each episode of condomless sex. Followed up quarterly for 12 months. NG tested for via quarterly NG PCR of the pharynx/rectum/urine. The primary analysis was mITT. The primary outcome was the incidence of at least one bacterial STI (gonorrhea, chlamydia, syphilis) each quarter. cumulative incidence of each STI over 12 months. Tetracycline susceptibility data available for 29 isolates of N. gonorrhoeae out of 157 incident N. gonorrhoeae infections, for 162 isolates of S. Aureus and for 178 isolates of commensal Neisseria spp. | 200mg doxycycline within 72 hours after condomless sex | Agar dilution with tetracycline. Resistance defined as ≥2mg/L. Only proportion of resistant isolates were reported (MICs of each isolate were not reported) | Doxycycline reduced the incidence of at least one diagnosed STI (RR 0.34 in PrEP cohort and 0.38 PLWHIV), of gonorrhoea (RR 4.5/0.43 respectively), chlamydia (RR 0.12/0.26, respectively) and syphilis (0.13/0.23, respectively) |
Abbreviations: mITT – Modified intention to treat, MSM – men who have sex with men, NG – Neisseria gonorrhoeae, PLWH – People living with HIV, PrEP – preexposure prophylaxis, RR – relative risk, HR – hazard ratio.
Table 2.
Prevalence of tetracycline resistance in N. gonorrhoeae, commensal Neisseria species and S. aureus in the three included studies.
Table 2.
Prevalence of tetracycline resistance in N. gonorrhoeae, commensal Neisseria species and S. aureus in the three included studies.
| Study, Year of publication | Target bacterial species | Tetracycline breakpoint (mg/L) |
Baseline | Month 12 (During follow up for N. gonorrhoeae) | ||
| Tetracycline arm N resistant/N tested (% resistant to tetracycline) | Placebo arm N resistant/N tested (% resistant to tetracycline) | Tetracycline arm N resistant/N tested (% resistant to tetracycline) | Placebo arm N resistant/N tested (% resistant to tetracycline) | |||
| Harrison 1979 | N. gonorrhoeae | ≥1mg/L | NA | NA | 18/18 (100%) | 38/44 (86.4%) |
| Harrison 1979 | N. gonorrhoeae | ≥2mg/L | NA | NA | 12/18 (66.7%) | 19/44 (43.2%) |
| Molina 2018 | N. gonorrhoeae | ≥1mg/L | NA | NA | 0/2 (0%) | 4/6 (66.7%) |
| Luetkemeyer 2023 | N. gonorrhoeae | ≥2mg/L | 2/7 (28.6%) | 2/8 (25%) | 5/13 (38.5%) | 2/16 (12.5%) |
| Commensal Neisseria spp. | ≥2mg/L | 189/302 (62.6%) | 92/153 (60.1%) | 85/122 (69.7%) | 25/56 (44.6%)* | |
| S. aureus | ≥2mg/L | 12/334 (3.6%) | 19/161 (11.8%) | 16/137 (11.7%) | 3/62 (4.8%) | |
* P<0.01.
Table 3.
Forest plot showing individual study and pooled ORs (log scale) for tetracycline resistance in N. gonorrhoeae and exposure to tetracycline PEP. The tetracycline resistance threshold was ≥1 mg/L for the Molina study and ≥2 mg/L for the other two studies.
Table 3.
Forest plot showing individual study and pooled ORs (log scale) for tetracycline resistance in N. gonorrhoeae and exposure to tetracycline PEP. The tetracycline resistance threshold was ≥1 mg/L for the Molina study and ≥2 mg/L for the other two studies.
Table 4.
Forest plot showing individual study ORs (log scale) for tetracycline resistance (≥2 mg/L) in commensal Neisseria species and exposure to tetracycline PEP.
Table 4.
Forest plot showing individual study ORs (log scale) for tetracycline resistance (≥2 mg/L) in commensal Neisseria species and exposure to tetracycline PEP.
Table 5.
Forest plot showing individual study ORs (log scale) for tetracycline resistance (≥2 mg/L) in S. aureus and exposure to tetracycline PEP.
Table 5.
Forest plot showing individual study ORs (log scale) for tetracycline resistance (≥2 mg/L) in S. aureus and exposure to tetracycline PEP.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



