Submitted:
27 September 2023
Posted:
28 September 2023
You are already at the latest version
Abstract
This study presents a case report demonstrating an anomalous origin of the right subclavian artery from the aortic arch, accompanied by proximal dilation and a retro-esophageal course, characteristic of arteria lusoria and Kommerell's diverticulum. The research highlights the clinical significance of this anomaly and discusses its management strategies, emphasizing the importance of precise surgical intervention in addressing this condition.
Keywords:
arteria lusoria
; cardiac surgery
; vascular
; sternotomy
; dysphagia
Case Report
A 44-year-old patient underwent gastric bypass surgery in 2015, resulting in a remarkable weight loss of 30 kilograms. The patient presented with a progressively worsening dysphagia over the past six months. Diagnostic investigations revealed a pulsatile compression of the esophagus, suggestive of dysphagia lusoria. Subsequent computed tomography (CT) imaging confirmed the presence of an arteria lusoria, accompanied by a Kommerell's diverticulum provided (Figure 1). Given the symptomatic nature of the condition and the concurrent presence of Kommerell's diverticulum, surgical intervention was deemed necessary.
The selected surgical approach involved a median sternotomy, enabling a one-stage procedure involving resection of Kommerell's diverticulum and the establishment of a neo-trajectory. This neo-trajectory involved the reinsertion of the right subclavian artery into the ascending aorta, achieved through the interposition of a 10mm Dacron tube. The surgical process commenced with an upper laterotracheal dissection to expose the aberrant right subclavian artery, located retro-esophageally. The origin of the artery was demarcated by the presence of the Kommerell's diverticulum. Following the establishment of cardiopulmonary bypass (CPB) between the ascending aorta and an atrio-caval cannula, the distal portion of the right subclavian artery was clamped at its origin, and the arteria lusoria, along with its dystrophic segment, was excised. Closure of the resection site was meticulously executed through a double suture technique, fortified by the application of two extra-luminal pericardial pledgets.
Temporary lateral aortic clamping, applied anterolaterally, facilitated the successful interposition of a 10mm Dacron prosthesis between the aorta and the right subclavian artery, positioned beneath the innominate vein (Figure 2). Intraoperative assessments affirmed the prosthesis's excellent patency, along with secure anastomotic sealing. Subsequent post-operative follow-up (Figure 3) revealed an uneventful recovery, and she was relieved of dysphagia.
Discussion
The aortic arch and its branches can exhibit anatomical variations that have been described since the first half of the 18th century by anatomists such as Hummel and Hunauld1. These anomalies share a common embryological origin, giving rise to diverse clinical presentations. Some anomalies remain asymptomatic and are discovered incidentally, while others can lead to severe clinical symptoms from birth. The most common anomaly involving the branches of the aortic arch pertains to the right subclavian artery. Instead of arising jointly with the right carotid artery to form the brachiocephalic trunk, it originates directly from the aorta downstream from the left subclavian artery. It then follows an aberrant course to supply the right upper limb. This artery was aptly named Arteria Lusoria, or the "jesting artery," in 17942.
There is no strict indication to operate on an asymptomatic, non-aneurysmal arteria lusoria unless it is associated with adjacent aortic pathology for tactical reasons. Surgical intervention is only warranted when the aberrant artery causes troublesome dysphagia, upper limb ischemia, vertebral-basilar territory ischemia. On the other hand, there is a clear indication to operate on aneurysmal aberrant right subclavian arteries, regardless of symptoms.
There are two technical considerations which arise for the surgeon. Firstly, the choice of the surgical approach, as the lusoria artery is a deep vascular structure located in the mid-posterior mediastinum, oriented from bottom to top and from left to right. This explains the significant variability in the surgical approaches historically used for this artery, including left or right thoracotomy, median sternotomy, low tie-neck cervical incision, and right supraclavicular cervical incision. Secondly, the restoration of arterial continuity in the right upper limb. The selected surgical strategy primarily hinges on whether the aberrant right subclavian artery is aneurysmal or not, as well as the presence of associated lesions in the adjacent aorta6.
For the treatment of non-aneurysmal aberrant right subclavian arteries, the preferred surgical approach remains the isolated cervical route. This technique involves a supraclavicular cervicotomy on the side of the arteria lusoria, providing access to the artery's pre-scalene segment through an inter-jugulo-carotid pathway. The esophagus is carefully repositioned forward after releasing it from fibrous attachments that secure it to the spine. This maneuver facilitates continued dissection towards the artery's aortic origin, allowing for ligature under direct visual control. Left thoracotomy is commonly considered the approach of choice in such cases, as it enables adequate aortic control on both sides of the aneurysm. However, full lateral clamping around the origin of a lusoria aneurysm may not always be feasible, prompting the need for complete aortic clamping to facilitate lesion repair. While a simple closure of the aneurysmal neck with a prosthetic patch may suffice in certain instances, the presence of concomitant aortic lesions may necessitate partial prosthetic replacement of the descending thoracic aorta7.
In complex scenarios or when a more precise control of the artery's origin is required, the possibility of employing median sternotomy presents itself. We advocate for this approach as it provides safety measures and meticulous control facilitated by the extracorporeal circulation machine. It's important to note that while this approach is notably invasive, it generally entails less post-operative discomfort when compared to the left thoracotomy technique.
A comprehensive review of the literature reveals that interventions targeting arteria lusoria aneurysms have historically been associated with mortality rates ranging from 25% to 50%8. With the emergence of less invasive endovascular techniques, alternative strategies have been explored to minimize the necessity for traditional surgeries. However, this treatment still presents some limitations, notably the fact that it does not allow the repair of large aneurysms, nor the replacement of the pathological artery.
However, in our specific case, besides being aneurysmal, the artery's tortuous course along the esophagus caused symptomatic complications, necessitating artery replacement and repositioning. Consequently, we opted for a median sternotomy approach, facilitating both artery replacement and aneurysm repair within a single surgery. Alternatively, the thoracotomy approach was a viable choice, albeit entailing a two-stage procedure.

Table 1.
The different surgical approaches to treat Arteria Lusoria.
| Approach | Pros | Cons | Posibilities |
|---|---|---|---|
| Full median sternotomy |
|
|
|
| Right supraclavicular approach |
|
|
|
| Thoracotomy |
|
|
|
| Supraclavicular cervical incision |
|
|
|
Conclusion
In summary, our experience underscores that while median sternotomy represents a highly invasive procedure, it offers the unique advantage of enabling the concurrent resolution of substantial aneurysmatic lesions and the repositioning of the pathological subclavian artery within a single surgical intervention in a safe and controlled manner.
References
- Rana, M. S., Sizarov, A., Christoffels, V. M. & Moorman, A. F. M. Development of the human aortic arch system captured in an interactive three-dimensional reference model. Am. J. Med. Genet. A. 164A, 1372–1383 (2014). [CrossRef]
- Molz, G. & Burri, B. Aberrant subclavian artery (arteria lusoria): sex differences in the prevalence of various forms of the malformation. Evaluation of 1378 observations. Virchows Arch. A Pathol. Anat. Histol. 380, 303–315 (1978). [CrossRef]
- Tanaka, A., Milner, R. & Ota, T. Kommerell’s diverticulum in the current era: a comprehensive review. Gen. Thorac. Cardiovasc. Surg. 63, 245–259 (2015). [CrossRef]
- Carrizo, G. J. & Marjani, M. A. Dysphagia Lusoria Caused by an Aberrant Right Subclavian Artery. Tex. Heart Inst. J. 31, 168–171 (2004).
- Dueppers, P., Floros, N., Schelzig, H., Wagenhäuser, M. & Duran, M. Contemporary Surgical Management of Aberrant Right Subclavian Arteries (Arteria Lusoria). Ann. Vasc. Surg. 72, 356–364 (2021). [CrossRef]
- Myers PO, Fasel JH, Kalangos A, Gailloud P. Arteria lusoria: developmental anatomy, clinical, radiological and surgical aspects. Ann Cardiol Angeiol (Paris). 2010 Jun;59(3):147-54. Epub 2009 Aug 8. PMID: 19962688. [CrossRef]
- KIEFFER E., BAHNINI A., KOSKAS F. Aberrant subclavian artery: surgical treatment in thirty-three adult patients, J Vasc Surg, 1994, vol. 19, n° 1, 100-109; discussion 110-101. [CrossRef]
- AUSTIN E.H., WOLFE W.G. Aneurysm of aberrant subclavian artery with a review of the literature, J Vasc Surg, 1985, vol. 2, n° 4, 571-577.
- Shennib, H. & Diethrich, E. B. Novel approaches for the treatment of the aberrant right subclavian artery and its aneurysms. J. Vasc. Surg. 47, 1066–1070 (2008). [CrossRef]
Figure 1.
Sagittal and transversal CT scan views revealing an aberrant origin of the right subclavian artery from the aortic arch and a dilated appearance of its proximal segment, with a retro-esophageal course.
Figure 1.
Sagittal and transversal CT scan views revealing an aberrant origin of the right subclavian artery from the aortic arch and a dilated appearance of its proximal segment, with a retro-esophageal course.
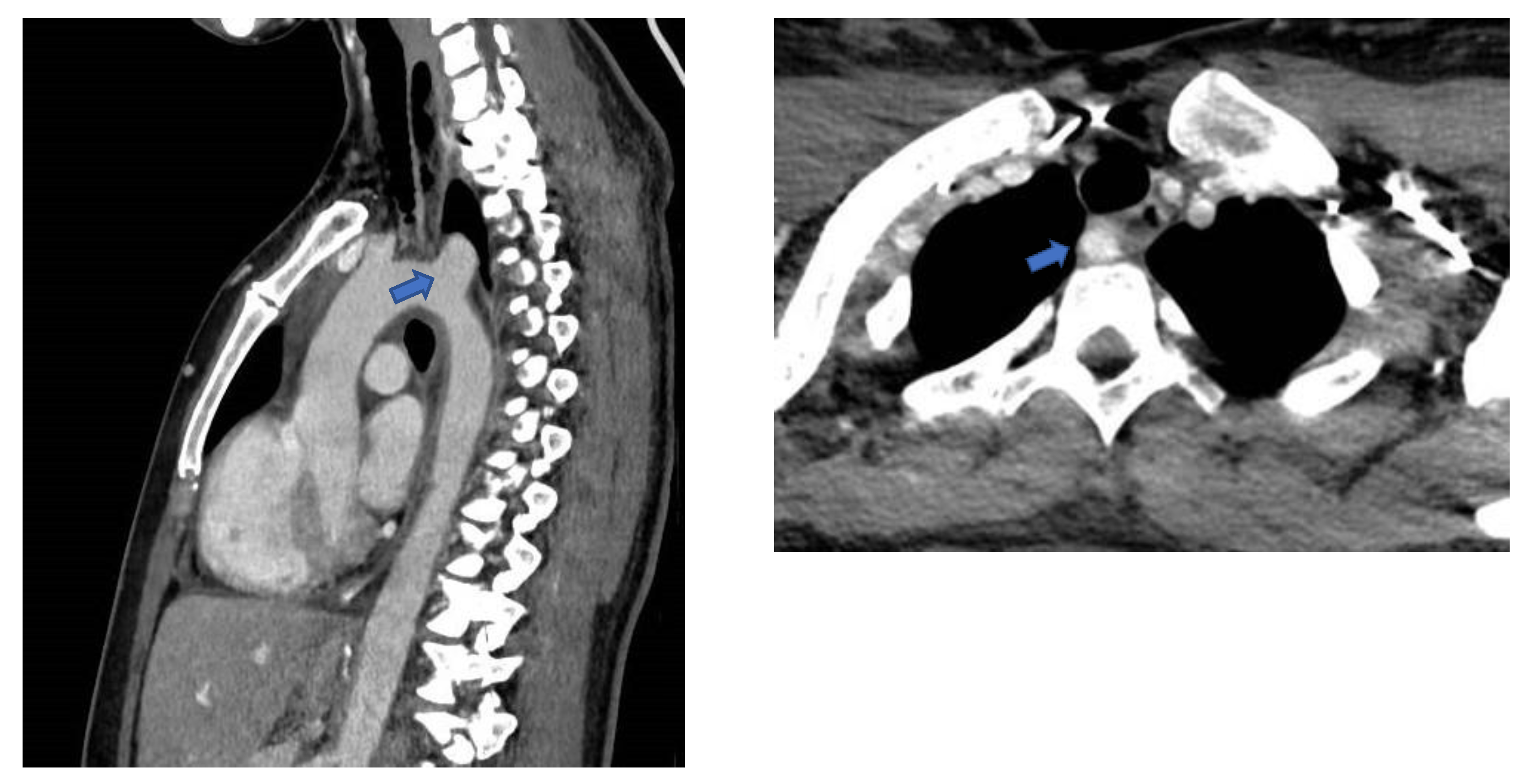
Figure 2.
Operative finding showing the interposition of a Dacron Tube to connect the ascending aorta to the right subclavian artery.
Figure 2.
Operative finding showing the interposition of a Dacron Tube to connect the ascending aorta to the right subclavian artery.
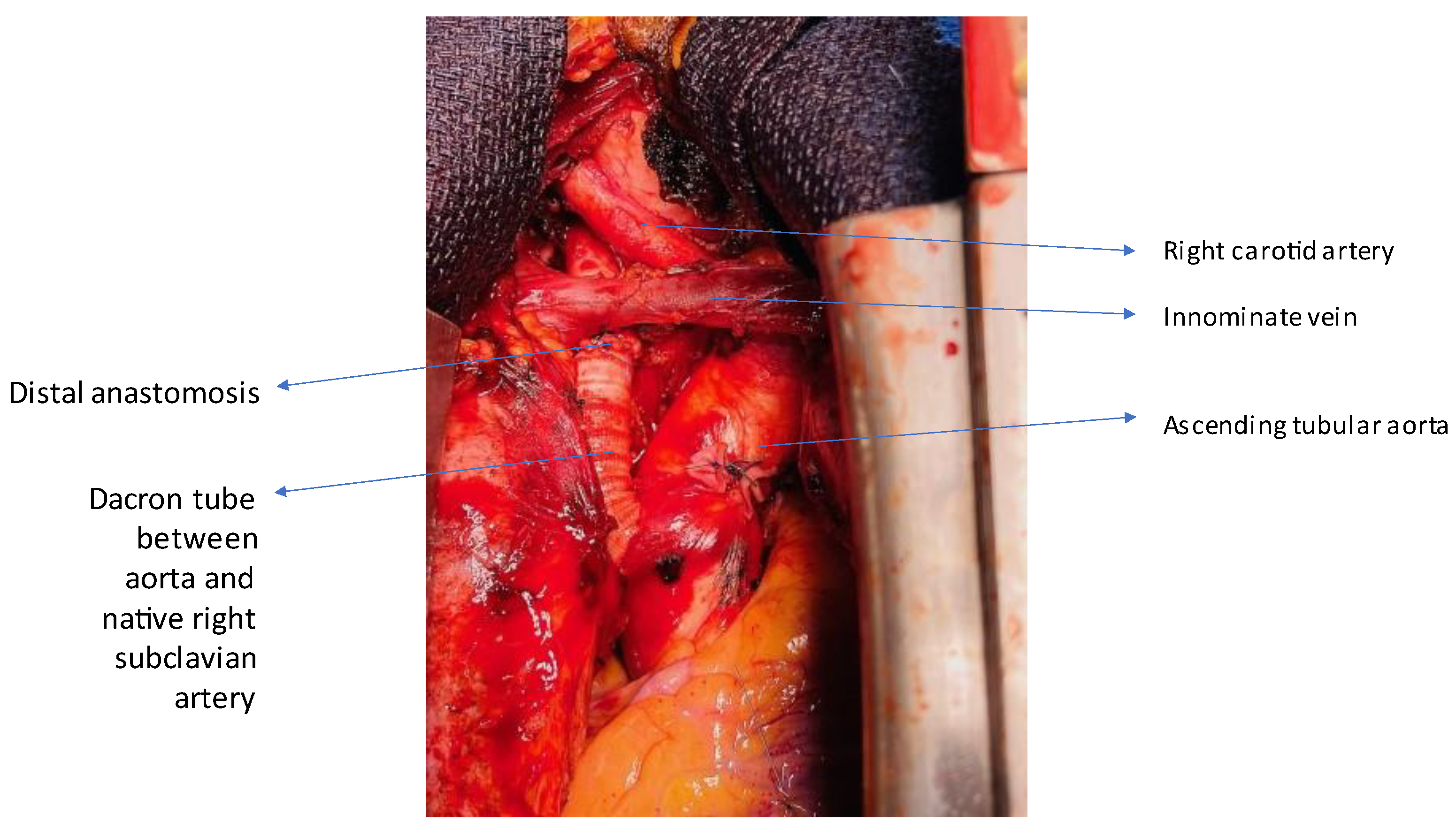
Figure 3.
Post-operative CT scan follow-up.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



