Submitted:
23 September 2023
Posted:
26 September 2023
You are already at the latest version
Abstract
ABSTRACTBackground: Crohn's disease (CD) is a chronic inflammatory bowel disorder with limited treatment options. Mitochondrial dysfunction has been implicated in CD pathogenesis, and mitochondrial-based interventions have emerged as a potential therapeutic avenue. This systematic review aimed to assess the efficacy of mitochondrial-based interventions in the management of CD.Methods: A systematic search of multiple databases was conducted to identify relevant studies in accordance with the PRISMA protocol. Inclusion criteria encompassed studies investigating mitochondrial-targeted interventions in CD patients. Methodological quality and risk of bias assessments were performed. Data synthesis involved both quantitative meta-analysis and qualitative narrative synthesis.Results: A total of 23 studies were included in this review, comprising randomized controlled trials, observational studies, and case reports. Mitochondrial-based interventions encompassed nutraceuticals, probiotics, exercise, and dietary modifications. However, the overall quality of evidence was moderate, primarily due to methodological limitations in some studies.Conclusion: This systematic review suggests that mitochondrial-based interventions hold promise as adjunctive therapies for CD management. They appear to contribute to clinical remission and amelioration of disease activity. Nevertheless, the moderate quality of evidence underscores the need for further well-designed clinical trials to substantiate these findings and delineate optimal intervention strategies.
Keywords:
Crohn's disease
; mitochondrial dysfunction
; nutraceuticals
; probiotics
; exercise
; dietary modifications
; systematic review
; meta-analysis
; clinical remission
; disease activity indices
INTRODUCTION
Crohn's disease (CD) is a chronic, relapsing-remitting inflammatory bowel disorder characterized by transmural inflammation, affecting any part of the gastrointestinal tract from the mouth to the anus [1]. Despite extensive research, its etiology remains incompletely understood, but it is believed to result from a complex interplay of genetic, environmental, and immune factors [2]. The current therapeutic options for CD primarily focus on immune modulation and suppression, which may not be curative and are associated with adverse effects and variable responses. Hence, there is a compelling need for innovative therapeutic strategies to enhance the management of CD [3].
One emerging area of interest in CD pathogenesis is mitochondrial dysfunction [3]. Mitochondria are pivotal cellular organelles responsible for energy production, calcium homeostasis, and regulation of apoptosis [4]. Dysfunctional mitochondria can lead to oxidative stress, inflammation, and cell death—all of which are key features of CD. Studies have shown that CD patients often exhibit abnormalities in mitochondrial structure and function within the inflamed mucosal tissue [5]. These mitochondrial disturbances are implicated in amplifying inflammatory cascades and perpetuating intestinal tissue damage.
Inflammatory bowel disease (IBD) represents a highly intricate and multifaceted group of immune-mediated inflammatory disorders predominantly impacting the gastrointestinal tract. The prevalent manifestations of IBD encompass CD and ulcerative colitis (UC), each distinguished by distinct clinical and histopathological characteristics [6]. CD is characterized by a heterogeneous profile, involving the entire gastrointestinal tract, and is characterized by a discontinuous pattern of transmural inflammation, frequently accompanied by the presence of characteristic histological granulomas [7-11]. Conversely, UC predominantly manifests as inflammation restricted to the mucosal layer, typically commencing in the rectum and extending proximally in a contiguous manner along the colon [12].
The global prevalence of IBD is of significant concern, with a rising incidence observed in newly industrialized nations and a stable yet escalating prevalence in regions adopting a westernized lifestyle, such as Europe and North America [13]. Onset most commonly occurs within the age bracket of 15 to 30 years, with approximately 10% of diagnoses occurring during childhood and adolescence [14]. Importantly, IBD imparts lifelong morbidity and challenges both patients and clinicians. Current therapeutic strategies encompass a spectrum of interventions, including biologics, immunomodulators, aminosalicylates, and corticosteroids [15]. However, the marked heterogeneity observed in IBD patients, spanning disease location, progression, and mechanistic underpinnings, poses a formidable obstacle to achieving consistent therapeutic outcomes [16]. For example, while anti-tumor necrosis factor alpha (anti-TNFα) biologics have revolutionized IBD management, they exhibit primary non-response rates of 30% and secondary non-response rates of 50% [17-19]. Furthermore, the efficacy of anti-TNFα therapies in achieving mucosal healing, a pivotal clinical endpoint, is limited, with only approximately 45% of patients demonstrating mucosal healing at 12 and 24 months [20].
In light of this, the concept of mitochondrial-based interventions has gained attention in the management of CD [14-17]. Such interventions encompass a spectrum of approaches, including the use of nutraceuticals, probiotics, exercise, and dietary modifications, all aimed at preserving mitochondrial integrity and function [21-23]. These interventions hold promise not only for alleviating symptoms but also for modifying the course of the disease by addressing a potential underlying driver of CD pathophysiology.
While there is a growing body of evidence exploring the utility of mitochondrial-based interventions in CD, the literature remains scattered, and a comprehensive synthesis of the available data is lacking. Therefore, this systematic review aims to provide a thorough evaluation of the efficacy of mitochondrial-based interventions in CD management. Through a rigorous and systematic analysis of existing studies, we seek to elucidate the potential benefits, limitations, and future prospects of these interventions in improving clinical outcomes and enhancing the quality of life for individuals living with CD.
MATERIALS AND METHODS
Review design and protocol
The systematic review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) protocol [24], ensuring a meticulous and transparent approach in the selection and synthesis of pertinent studies related to interventions targeting mitochondria in the management of Crohn's disease (see Figure 1). The initial phase involved a thorough and systematic search across various electronic databases. The review's study population (P) encompassed individuals diagnosed with Crohn's disease, representing a diverse array of demographic characteristics. The interventions (E) primarily revolved around mitochondrial-focused approaches, including coenzyme Q10 supplementation, exercise regimens targeting mitochondrial function, dietary adjustments aimed at supporting mitochondria, and pharmacological agents known to impact mitochondrial health. These interventions were evaluated for their potential influence on the progression of Crohn's disease. The comparator (C) included control conditions, placebo interventions, or alternative treatments. Lastly, the study's outcome (O) was centered on assessing changes in Crohn's disease-related factors, encompassing parameters such as motor function, cognitive function, quality of life, disease progression, and the occurrence of both motor and non-motor symptoms.
Search strategy
The systematic review's database search methodology employed a thorough and methodical approach to locate pertinent studies from nine distinct databases. The search strategy was thoughtfully constructed by employing a blend of Boolean operators (specifically, AND and OR) and Medical Subject Headings (MeSH) keywords, which are further detailed in Table 1.
Selection protocol
Inclusion criteria:
- Study types: This systematic review considered a wide spectrum of research methodologies eligible for inclusion. These methodologies encompassed randomized controlled trials (RCTs), cohort studies, cross-sectional studies, case-control studies, observational studies, experimental studies, systematic reviews, and meta-analyses.
- Population: The study population of interest included individuals diagnosed with CD or animal models of CD.
- Interventions: Included studies primarily focused on the evaluation or exploration of mitochondrial-based interventions. These interventions comprised various strategies, such as dietary interventions, exercise programs, pharmacological interventions, probiotics, and any approaches targeting mitochondrial function or dynamics.
- Outcomes: Eligible studies were required to report outcomes related to the effectiveness, safety, or influence of mitochondrial interventions on Crohn's disease (CD). The outcomes of interest encompassed alterations in both motor and non-motor symptoms, changes in quality of life, disease progression, biochemical markers, and any pertinent clinical assessments.
- Publication date: No constraints were placed on the publication date of the included studies.
Exclusion criteria:
- Case reports: Case reports were excluded from this systematic review to maintain a higher level of evidence and mitigate potential bias associated with single-case observations.
- Thesis articles: Articles originating from theses and unpublished theses themselves were excluded due to concerns regarding limited peer review and potential shortcomings in methodological rigor.
Data extraction
The data extraction process for this systematic review involved the systematic collection of essential study details, including the title, authors, publication year, and source. The study design was categorized, specifying whether it was an RCT, cohort study, cross-sectional study, case-control study, observational study, experimental study, systematic review, or meta-analysis. Population information encompassed participant numbers, age, gender distribution, and relevant inclusion criteria specific to CD. Details regarding the mitochondrial-based interventions, including type, dosage, duration, and protocol, were documented. Information regarding control groups or comparators, which might involve placebos or alternative treatments, was also recorded. Primary and secondary outcomes, spanning motor and non-motor CD symptoms, quality of life, disease progression indicators, biochemical markers, and clinical assessments, were extracted. Key findings, effect sizes, statistical significance, and adverse events were synthesized, and any employed statistical methods, including tests, models, and software, were documented.
Bias assessment
This investigation’s bias evaluation methodology utilized the Newcastle-Ottawa Scale (NOS) tool [25] to assess the quality and bias risk of the chosen studies (see Figure 2). Studies were allocated stars for comparability when they effectively controlled for these variables. The outcome criteria considered the evaluation of the primary outcome, the duration of follow-up, and the presence of any follow-up data loss.
RESULTS
Initially, an extensive search was conducted across various databases, yielding a total of 459 records. Simultaneously, no records were identified from registers. Before the screening phase, 94 duplicate records were removed, and 78 records were excluded based on ineligibility criteria flagged by automation tools, streamlining the dataset for further evaluation. Following the initial database search, additional records were discovered through alternative sources. Specifically, 124 records were retrieved from websites, and 116 records were identified through citation searching. These records were then subjected to screening, resulting in a total of 287 records that were assessed for eligibility. Remarkably, none of the screened records were excluded at this stage. Continuing with the study selection process, efforts were made to obtain full reports for the 287 records, with 62 reports remaining unretrieved. Consequently, 225 reports were further scrutinized for eligibility, with 71 scoping reviews, 59 studies not conforming to the PECO (Population, Exposure, Comparator, Outcome) protocol, and 72 reports being excluded for reasons such as unavailability of full-text articles. Ultimately, after a comprehensive and meticulous selection process, 23 studies [26-48] were deemed suitable for inclusion in the review.
Table 2 provides a comprehensive overview of selected studies [26-48] aimed at investigating different aspects related to CD and its management, whereas Table 3 provides the overview of findings and assessments focusing on various parameters related to CD and its management. The studies, referenced by citation numbers, cover a wide range of research objectives, study designs, methodologies assessed, and types of interventions investigated. Ananthakrishnan et al [26] conducted a prospective cohort study to explore the association between dietary fat and the risk of CD and ulcerative colitis (UC). They employed Cox proportional hazards models to assess the impact of long-chain n-3 PUFAs and trans-unsaturated fatty acids on these conditions. Bottoms et al [27] performed a randomized feasibility trial to understand the affective and enjoyment responses to high-intensity interval training (HIIT) and moderate-intensity continuous training (MICT) in adults with CD. They utilized various metrics, including heart rate, ratings of perceived exertion (RPE), feeling state (FS), and the Physical Activity Enjoyment Scale (PACES), to assess responses to these exercise protocols. Cosin et al [28] conducted an experimental study aimed at investigating the role of hypoxia in regulating inflammation and autophagy in CD patients and murine colitis models. They employed measurements of inflammatory markers, autophagy, NLRP3 expression, and activation of HIF-1α and mTOR/NLRP3 pathways to assess the role of hypoxia in disease pathogenesis. De Galan et al [29] utilized an experimental mouse model to investigate the impact of environmental hypoxia and immune cell-specific deletion of oxygen sensor prolyl hydroxylase (PHD) 1 on Crohn's-like ileitis. Their assessments included hematological evaluation, distal ileal hypoxia measurement, histological scoring, and gene expression analysis. Gomez et al [30] conducted in vitro and in vivo studies to assess the therapeutic potential of extracellular vesicles (EVs) derived from mesenchymal stromal cells (MSCs) engineered to overexpress hypoxia-inducible factor 1-alpha and telomerase. They performed analyses related to macrophage repolarization, cytokine release, and functional assays, along with testing in a mouse colitis model. Guslandi et al [31] conducted a randomized controlled trial to evaluate the role of Saccharomyces boulardii in the maintenance treatment of CD patients in clinical remission. They compared clinical relapses based on CDAI values between patients receiving mesalamine alone and those receiving mesalamine plus Saccharomyces boulardii. Jones et al [32] conducted a randomized controlled trial to assess the effect of 6 months of combined impact and resistance training on bone mineral density (BMD) and muscle function in adults with CD. Their assessments included BMD measurement, muscle function evaluation, and fatigue severity assessment. Lewis et al [33] conducted a randomized controlled trial to compare the effectiveness of the Specific Carbohydrate Diet (SCD) to the Mediterranean diet (MD) as a treatment for CD with mild to moderate symptoms. Their assessments included the evaluation of symptomatic remission, fecal calprotectin (FC) response, and C-reactive protein (CRP) response. Limketkai et al [34] investigated the efficacy and safety of probiotics for the induction of remission in CD. Their assessments focused on remission induction in CD and the evaluation of adverse events. Negm et al [35] studied the effect of intermittent fasting (IF) during Ramadan on CD patients, assessing its impact on clinical disease activity, quality of life, and depression. They utilized serum CRP and stool calprotectin levels, the Partial Mayo score, the Harvey Bradshaw index, and the Simple IBD questionnaire for evaluation. Ng et al [36] conducted a prospective study to evaluate the effects of low-intensity walking on CD patients' quality of life. They employed various assessments, including the Inflammatory Bowel Disease Questionnaire, Inflammatory Bowel Disease Stress Index, and Harvey-Bradshaw Simple Index. Plein et al [37] performed a randomized, double-blind, placebo-controlled pilot study to investigate the effects of Saccharomyces boulardii on CD patients with diarrhea. Their assessments included the frequency of bowel movements and the BEST Index. Scheffers et al [38] assessed the effects of a 12-week lifestyle intervention in children with IBD through a randomized semi-crossover controlled trial, including physical training and dietary advice. Their assessments covered physical fitness, patient-reported outcomes, clinical disease activity, and nutritional status. Schultz et al [39] conducted a randomized placebo-controlled trial to determine the effect of oral Lactobacillus GG (L. GG) on inducing or maintaining medically induced remission in CD. The study focused on the outcomes related to inducing or maintaining remission in CD. Seeger et al [40] examined and compared the safety, feasibility, and potential beneficial effects of individual moderate endurance and moderate muscle training in patients with CD. Their assessments covered safety, feasibility, disease activity, inflammatory parameters, quality of life, physical activity, and strength. Starz et al [41] reviewed the influence of reduction diets, including low-FODMAP, lactose-free, and gluten-free diets, on the microbiome of CD patients, focusing on their effects on gut microbiota composition and diversity. Steed et al [42] conducted a randomized, double-blind, placebo-controlled trial to investigate the effects of synbiotic consumption (Bifidobacterium longum and Synergy 1) on disease processes in CD patients. Their assessments encompassed clinical outcomes, histological scores, immune marker transcription levels, and mucosal bacterial 16S rRNA gene copy numbers. Su et al [43] conducted a randomized controlled trial to investigate the effect of glucocorticoids combined with probiotics on inflammatory factors and intestinal microflora in the treatment of CD. Their assessments included clinical efficacy, changes in inflammatory factors, incidence of infection, and changes in intestinal flora. Suskind et al. [44] aimed to determine the potential efficacy of three variations of the specific carbohydrate diet (SCD) in managing active Crohn's Disease (CD). They enrolled 18 patients with mild to moderate CD and randomized them into three groups: SCD, modified SCD (MSCD), and a whole foods (WF) diet. The evaluation was carried out at baseline, 2, 4, 8, and 12 weeks, encompassing assessments of Pediatric Crohn's Disease Activity Index (PCDAI), inflammatory biomarkers, and multi-omics evaluations. The primary objective was to assess the impact of these dietary interventions on achieving clinical remission, reducing C-reactive protein (CRP) levels, and altering the composition of the gut microbiome. Takayuki et al. [45] conducted a study to examine the effects of an elemental diet (Elental) on mucosal inflammation in Crohn's disease (CD). They enrolled 28 consecutive patients with active CD and treated them with Elental for a duration of 4 weeks. A control group consisting of 20 patients without inflammation was included for comparison. Mucosal biopsies were obtained before and after treatment. The study aimed to assess the elemental diet's impact on clinical remission, endoscopic healing, histologic healing, and mucosal cytokine concentrations. Tew et al. [46] focused on assessing the feasibility and acceptability of high-intensity interval training (HIIT) and moderate-intensity continuous training (MICT) in adults with Crohn's disease (CD). Participants with either quiescent or mildly-active CD were randomly assigned to one of three groups: HIIT, MICT, or usual care control. The study evaluated various feasibility outcomes, including recruitment, retention, outcome completion, and exercise attendance. Additionally, data were collected on cardiorespiratory fitness, disease activity, and other relevant parameters to determine the feasibility and acceptability of these exercise training regimens in adults with CD. Walters et al. [47] conducted research to develop an optimized methodology for fecal sample processing and to detect changes in the gut microbiota of patients with Crohn's disease (CD) who were receiving specialized diets. Their pilot diet crossover trial compared the effects of the specific carbohydrate diet (SCD) to a low residue diet (LRD) on the composition and resolution of symptoms related to inflammatory bowel disease (IBD). The study assessed gut microbiota using a high-density DNA microarray PhyloChip and aimed to understand the impact of these diets on DNA extraction methods, microbial composition, microbial complexity, and changes in the abundance of Bacteroides fragilis (B. fragilis). Yilmaz et al. [48] conducted a single-center, prospective, open-label randomized controlled trial to investigate the effects of kefir consumption on the fecal microflora and symptoms of patients with inflammatory bowel disease (IBD). In this study, 400 mL/day of kefir was administered to the patients for 4 weeks. Assessment included quantitation of stool Lactobacillus and Lactobacillus kefiri content using real-time quantitative polymerase chain reaction (PCR) and recording symptoms such as abdominal pain, bloating, stool frequency, stool consistency, and feelings of well-being. The primary objective was to evaluate how probiotic consumption in the form of kefir influenced the fecal microflora and the quality of life of patients with IBD.
DISCUSSION
Ananthakrishnan et al. [26] conducted a study to assess the association between dietary fat intake and the risk of CD and ulcerative colitis (UC). Their results indicated no significant association between cumulative energy-adjusted intake of various fats and the risk of CD or UC. However, higher long-term intake of trans-unsaturated fatty acids showed a potential trend towards increased UC incidence, while high intake of long-chain n-3 PUFAs suggested a potential trend towards a lower risk of UC. Bottoms et al. [27] explored the affective and enjoyment responses to high-intensity interval training (HIIT) and moderate-intensity continuous training (MICT) in adults with CD. Their study revealed that HIIT led to higher heart rates and perceived exertion compared to MICT, but both exercise protocols resulted in similar feelings of enjoyment and affect among adults with quiescent or mildly-active CD. Cosin et al. [28] delved into the role of hypoxia in regulating inflammation and autophagy in CD patients and murine colitis models. Their findings indicated that hypoxia could reduce inflammatory markers, increase autophagy, inhibit NF-κB signaling, and downregulate NLRP3 expression. Hypoxia appeared to counteract inflammation by promoting autophagy and inhibiting the mTOR/NLRP3 pathway. Moreover, hypoxia and HIF-1α activation were found to be protective in mouse models of colitis. De Galan et al. [29] investigated the impact of environmental hypoxia and immune cell-specific deletion of the oxygen sensor prolyl hydroxylase (PHD) 1 on Crohn's-like ileitis in mice. Their study indicated that long-term environmental hypoxia or haematopoietic Phd1-deletion did not significantly impact the development of experimental ileitis. However, hypoxia led to various physiological changes, including increased red blood cell count, haemoglobin, and pimonidazole intensity in the ileum. Additionally, hypoxia induced an increase in circulatory monocytes, ileal mononuclear phagocytes, and proinflammatory cytokine expression in WT mice but did not translate into histological or gene expression differences in TNF∆ARE/+ mice.
Gomez et al. [30] assessed the therapeutic potential of extracellular vesicles (EVs) derived from mesenchymal stromal cells (MSCs) engineered to overexpress HIF-1alpha and telomerase. Their results showed that these EVs effectively repolarized monocytes from M1 to an M2-like phenotype with reduced inflammatory cytokine release. Furthermore, the EV-treated M1 cells exhibited immunosuppressive effects similar to M2 cells on activated peripheral blood mononuclear cells (PBMCs), reduced PBMC adhesion to activated endothelium, and prevented myofibroblast differentiation. The administration of these EVs also promoted healing in a mouse colitis model. Guslandi et al. [31] conducted a randomized controlled trial to evaluate the role of Saccharomyces boulardii in the maintenance treatment of Crohn's disease in patients in clinical remission. Their findings indicated that clinical relapses, as assessed by Crohn's Disease Activity Index (CDAI) values, were less frequent in patients treated with mesalamine plus Saccharomyces boulardii compared to those receiving mesalamine alone. This suggested a potential role for Saccharomyces boulardii in the maintenance treatment of Crohn's disease. Jones et al. [32] assessed the effect of exercise intervention on bone mineral density (BMD) and muscle function in adults with CD. Their study demonstrated that a 6-month exercise program significantly improved BMD at the lumbar spine, resulted in superior muscle function outcomes, and lowered fatigue severity among CD patients. Lewis et al. [33] compared the effectiveness of the Specific Carbohydrate Diet (SCD) to the Mediterranean diet (MD) in treating CD with mild to moderate symptoms. The study found no significant differences in symptomatic remission rates between the SCD and MD groups, nor were there significant differences in fecal calprotectin (FC) and C-reactive protein (CRP) responses. Limketkai et al. [34] assessed the efficacy and safety of probiotics for the induction of remission in CD. Their study showed that probiotics did not significantly differ from placebo in inducing remission in Crohn's disease after six months. Negm et al. [35] examined the effect of intermittent fasting (IF) during Ramadan on CD patients' clinical disease activity, quality of life, and depression. Their study revealed no significant change in serum CRP and stool calprotectin levels, but there was a significant rise in the partial Mayo score after fasting. This rise in clinical parameters was more pronounced in older patients and those with higher baseline calprotectin levels. Ng et al. [36] studied the effects of low-intensity walking on CD patients' quality of life. Their findings indicated statistically significant improvements in quality of life based on various questionnaires without detrimental effects on disease activity.
In the study by Plein et al. [37], a significant reduction in the frequency of bowel movements and BEST Index was observed in the group receiving S. boulardii (S.b.), suggesting potential benefits in CD management without any adverse drug events. Scheffers et al. [38] conducted a 12-week lifestyle intervention in pediatric IBD patients, demonstrating improvements in bowel symptoms, quality of life, and fatigue. While peak VO2 did not change significantly, exercise capacity and core stability improved, and the Pediatric Crohn's Disease Activity Index decreased significantly. Schultz et al. [39] evaluated the safety and feasibility of individual moderate endurance and muscle training in CD patients, showing that both forms of exercise can be safely performed and result in strength improvements and enhanced emotional function.
In contrast, Schultz et al. [39] did not find statistically significant changes in disease activity or other outcome parameters, highlighting the complexity of exercise effects on CD. Starz et al. [41] investigated the influence of reduction diets on gut microbiota composition and diversity, revealing that such diets, including low-FODMAP, lactose-free, and gluten-free diets, negatively affected microbial diversity and the abundance of beneficial microbial species. However, the Crohn's disease exclusion diet (CDED) with partial enteral nutrition positively influenced the microbiota and may impact the future course of the disease.
Steed et al. [42] explored the clinical outcomes of synbiotic consumption in CD patients, showing that it improved clinical symptoms, reduced disease activity indices, and histological scores, along with alterations in specific immune markers and an increase in mucosal bifidobacteria. Su et al. [43] investigated the combination of probiotics with glucocorticoids in CD treatment, revealing improved clinical outcomes, reduced inflammatory factors, and positive changes in intestinal flora composition, as well as lower infection rates compared to conventional treatment methods.
Suskind et al. [44] conducted a study involving three different diets (SCD, MSCD, and WF) and found that all participants who completed the study achieved clinical remission, with significant reductions in C-reactive protein (CRP) levels and shifts in microbiome composition. Takayuki et al. [45] examined mucosal cytokine concentrations and reported clinical remission rates along with endoscopic and histologic healing, coupled with changes in mucosal cytokine levels. Tew et al. [46] assessed the feasibility and acceptability of HIIT and MICT exercise training, with both interventions demonstrating high feasibility and acceptability, and HIIT resulting in a greater improvement in peak oxygen uptake.
Walters et al. [47] investigated gut microbiota composition and complexity in IBD patients compared to healthy controls, highlighting lower microbial complexity and an increased abundance of Bacteroides fragilis in IBD patients. They observed changes in the gut microbiome composition and complexity in response to the specialized carbohydrate diet (SCD), which was associated with restructuring of gut microbial communities. Finally, Yilmaz et al. [48] explored the effects of kefir consumption on stool Lactobacillus and Lactobacillus kefiri content, along with clinical parameters. They found significant improvements in erythrocyte sedimentation rate, C-reactive protein, hemoglobin levels, bloating scores, and feeling good scores in CD patients, suggesting a potential short-term improvement in patient quality of life.
The collective findings presented in this review hold significant promise for advancing our understanding and management of CD. These studies span a wide range of parameters, from dietary interventions and exercise regimens to microbiome composition and treatments, providing a holistic view of potential strategies for CD management. One notable implication is the potential role of probiotics and synbiotics in CD treatment. Studies like Plein et al. [37], Steed et al. [42], and Su et al. [43] suggest that these interventions can improve clinical outcomes, reduce disease activity, and modulate immune responses. This opens up avenues for further research into optimizing probiotic formulations and treatment protocols to harness their therapeutic benefits effectively.
Exercise, as highlighted by Scheffers et al. [38] and Tew et al. [46], demonstrates its feasibility and positive impact on CD patients. While exercise may not significantly alter some physiological parameters, it enhances overall well-being, exercise capacity, and core stability. Future studies could delve deeper into tailoring exercise regimens to individual patient needs and assessing their long-term effects on CD management.
Dietary interventions, particularly specialized diets like the Specific Carbohydrate Diet (SCD) examined by Suskind et al. [44], have shown the potential to induce clinical remission and alter microbiome composition. This implies that dietary modifications can play a pivotal role in CD management. Further research should explore the long-term effects of these diets, their mechanisms of action, and their potential as adjunct therapies to conventional CD treatments.
The microbiome's role, as seen in Starz et al. [41] and Walters et al. [47], underscores its importance in CD. Reduction diets negatively impact microbial diversity, while Crohn's disease exclusion diet (CDED) has a positive influence. Understanding the mechanisms behind these changes could lead to more targeted dietary interventions for CD patients. Mucosal cytokine concentrations and histologic healing, as demonstrated by Takayuki et al. [45], offer promise for improved treatment strategies focusing on mucosal inflammation. Investigating the mechanisms underlying these changes could lead to more effective therapies for CD patients.
Much like in the context of UC, recent scientific investigations have unveiled the pivotal role of mitochondrial health in the pathophysiology of CD [49-53]. These emerging studies have uncovered associations between genetic variations related to mitochondrial homeostasis and CD susceptibility or its clinical course. Notable examples include polymorphisms in genes like SLC22A5, encoding OCTN2, IRGM, and UCP2 [17, 21-23]. Notably, the pediatric RISK stratification study, which leveraged RNA sequencing analysis on mucosal biopsies from CD patients, identified a distinct mitochondrial function gene signature in individuals predicted to be at high risk of stricturing complications but who, remarkably, remained complication-free during a 36-month follow-up period [5].
Moreover, in-depth proteomic investigations of pediatric CD patients revealed impaired mitochondrial function, particularly in proteins associated with H2S detoxification. This impairment correlated with increased disease severity [54-56]. Ultrastructural examinations of epithelial cell mitochondria unveiled morphological irregularities characterized by dissolved or irregular mitochondrial cristae, indicative of dysfunctional mitochondria in CD patients [57]. Intriguingly, these mitochondrial alterations appeared to precede other early events in the inflammation progression, such as changes in tight junctions controlling barrier function [58-62].
However, it's crucial to acknowledge the limitations inherent in these investigations, which can affect the generalizability and interpretation of their findings. Firstly, many of the studies exhibit relatively small sample sizes, as seen in studies like Schultz et al. [39] and Seeger et al. [40]. This limitation reduces the statistical power of these investigations and makes it challenging to draw definitive conclusions that can be broadly applied to the CD population. Additionally, the demographic and clinical heterogeneity of CD patients further complicates generalization, as CD can manifest differently in various individuals. Several studies, such as Negm et al. [35] and Scheffers et al. [38], face potential biases related to patient selection and recruitment. For instance, patients willing to participate in exercise interventions or dietary trials may inherently have a more favorable attitude towards these interventions, which could skew the results. Moreover, the use of self-reported measures, such as patient-reported outcomes and questionnaires, introduces the possibility of response bias, as participants may provide socially desirable responses. Another common limitation is the relatively short duration of the studies. Many of the interventions, including dietary modifications and exercise regimens, were implemented for relatively brief periods, which may not capture the long-term effects or sustainability of these approaches in CD management. For a chronic condition like CD, long-term outcomes are of paramount importance. Furthermore, the absence of a standardized or universally accepted definition for clinical remission in CD poses a challenge. Studies like Suskind et al. [44] and Takayuki et al. [45] aimed to achieve clinical remission, but the specific criteria and endpoints for defining remission can vary between studies. This lack of standardized definitions can make it challenging to compare and synthesize results across different investigations. In some cases, the studies in reported dropout rates or loss to follow-up, which can introduce attrition bias and potentially affect the validity of the results. For instance, Schultz et al. [39] noted a higher dropout rate in the endurance exercise group, which can influence the interpretation of the study's findings. Finally, while several studies assessed specific parameters, such as mucosal cytokine concentrations or microbial composition, the underlying mechanisms driving the observed changes are not always fully elucidated. Understanding these mechanisms is critical for developing more targeted and effective interventions.
CONCLUSION
The assessed investigations in this review collectively shed light on various facets of the disease, encompassing dietary interventions, exercise regimens, microbial composition, and immunomodulatory approaches. Dietary modifications emerge as a significant avenue for CD management. Studies suggest that specific dietary regimens, such as the SCD, elemental diet, and synbiotic consumption, hold promise in achieving clinical remission and reducing inflammatory markers. This highlights the potential of personalized nutrition as a non-pharmacological approach to ameliorating CD symptoms. Also, exercise interventions, particularly HIIT and MICT, exhibit feasibility and acceptability among CD patients. These structured exercise programs may enhance cardiovascular fitness and overall well-being, potentially becoming an integral part of CD management. Furthermore, insights into the gut microbiota composition underline the significance of microbial diversity and specific taxa in CD. The microbial changes observed with dietary interventions, including the reduction of microbial diversity with certain diets and the positive influence of the Crohn's disease exclusion diet (CDED), underscore the importance of dietary strategies in modulating the gut microbiome—a pivotal factor in CD pathogenesis. Immunomodulatory approaches, such as synbiotics and probiotics, show promise in improving clinical outcomes, reducing disease activity indices, and modulating immune markers. These findings suggest that targeting the gut microbiota and the immune system may hold the key to more effective CD therapies. However, it's important to acknowledge the limitations of these studies, including small sample sizes and the need for longer-term investigations. Additionally, the heterogeneity of CD poses challenges in generalizing findings across all patient populations.
References
- Colombel, J.F.; Panaccione, R.; Bossuyt, P.; Lukas, M.; Baert, F.; et al. Effect of tight control management on Crohn’s disease (CALM): a multicentre, randomised, controlled phase 3 trial. Lancet 2018, 390, 2779–2789. [Google Scholar] [CrossRef] [PubMed]
- Mancini, N.L.; Rajeev, S.; Jayme, T.S.; Wang, A.; Keita, A.V.; et al. Crohn’s disease pathobiont adherent-invasive E coli disrupts epithelial mitochondrial networks with implications for gut permeability. Cell. Mol. Gastroenterol. Hepatol. 2021, 11, 551–571. [Google Scholar] [CrossRef] [PubMed]
- Franke, A.; McGovern, D.P.; Barrett, J.C.; Wang, K.; Radford-Smith, G.L.; et al. Genome-wide meta-analysis increases to 71 the number of confirmed Crohn’s disease susceptibility loci. Nat. Gen. 2010, 42, 1118–1125. [Google Scholar] [CrossRef] [PubMed]
- Peltekova, V.D.; Wintle, R.F.; Rubin, L.A.; Amos, C.I.; Huang, Q.; et al. Functional variants of OCTN cation transporter genes are associated with Crohn disease. Nat. Genet. 2004, 36, 471–475. [Google Scholar] [CrossRef]
- Parkes, M.; Barrett, J.C.; Prescott, N.J.; Tremelling, M.; Anderson, C.A.; et al. Sequence variants in the autophagy gene IRGM and multiple other replicating loci contribute to Crohn’s disease susceptibility. Nat. Genet. 2007, 39, 830–832. [Google Scholar] [CrossRef]
- Kugathasan, S.; Denson, L.A.; Walters, T.D.; Kim, M.O.; Marigorta, U.M.; et al. Prediction of complicated disease course for children newly diagnosed with Crohn’s disease: a multicentre inception cohort study. Lancet 2017, 389, 1710–1718. [Google Scholar] [CrossRef]
- Mottawea, W.; Chiang, C.K.; Muhlbauer, M.; Starr, A.E.; Butcher, J.; et al. Altered intestinal microbiotahost mitochondria crosstalk in new onset Crohn’s disease. Nat. Commun. 2016, 7, 13419. [Google Scholar] [CrossRef]
- Söderholm, J.D.; Olaison, G.; Peterson, K.H.; Franzén, L.E.; Lindmark, T.; et al. Augmented increase in tight junction permeability by luminal stimuli in the non-inflamed ileum of Crohn’s disease. Gut 2002, 50, 307–313. [Google Scholar] [CrossRef]
- Khaloian, S.; Rath, E.; Hammoudi, N.; Gleisinger, E.; Blutke, A.; et al. Mitochondrial impairment drives intestinal stem cell transition into dysfunctional Paneth cells predicting Crohn’s disease recurrence. Gut 2020, 69, 1939–1951. [Google Scholar] [CrossRef]
- Roy, S.; Esmaeilniakooshkghazi, A.; Patnaik, S.; Wang, Y.; George, S.P.; et al. Villin-1 and gelsolin regulate changes in actin dynamics that affect cell survival signaling pathways and intestinal inflammation. Gastroenterology 2018, 154, 1405–1420.e2. [Google Scholar] [CrossRef]
- Vidrich, A.; Buzan, J.M.; Barnes, S.; Reuter, B.K.; Skaar, K.; et al. Altered epithelial cell lineage allocation and global expansion of the crypt epithelial stem cell population are associated with ileitis in SAMP1/YitFc mice. Am. J. Pathol. 2005, 166, 1055–1067. [Google Scholar] [CrossRef]
- Adolph, T.E.; Tomczak, M.F.; Niederreiter, L.; Ko, H.J.; Bock, J.; et al. Paneth cells as a site of origin for intestinal inflammation. Nature 2013, 503, 272–276. [Google Scholar] [CrossRef]
- Kerr, W.G.; Park, M.Y.; Maubert, M.; Engelman, R.W. SHIP deficiency causes Crohn’s disease-like ileitis. Gut 2011, 60, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Merkwirth, C.; Dargazanli, S.; Tatsuta, T.; Geimer, S.; Lower, B.; et al. Prohibitins control cell proliferation and apoptosis by regulating OPA1-dependent cristae morphogenesis in mitochondria. Genes Dev. 2008, 22, 476–488. [Google Scholar] [CrossRef] [PubMed]
- Nijtmans, L.G.; de Jong, L.; Artal Sanz, M.; Coates, P.J.; Berden, J.A.; et al. Prohibitins act as a membrane-bound chaperone for the stabilization of mitochondrial proteins. EMBO J. 2000, 19, 2444–2451. [Google Scholar] [CrossRef] [PubMed]
- Theiss, A.L.; Idell, R.D.; Srinivasan, S.; Klapproth, J.M.; Jones, D.P.; et al. Prohibitin protects against oxidative stress in intestinal epithelial cells. FASEB J. 2007, 21, 197–206. [Google Scholar] [CrossRef]
- Gunther, C.; Martini, E.; Wittkopf, N.; Amann, K.; Weigmann, B.; et al. Caspase-8 regulates TNF-α-induced epithelial necroptosis and terminal ileitis. Nature 2011, 477, 335–339. [Google Scholar] [CrossRef]
- Yang, E.; Shen, J. The roles and functions of Paneth cells in Crohn’s disease: a critical review. Cell Prolif. 2020, 54, e12958. [Google Scholar] [CrossRef]
- Liu, T.C.; Gao, F.; McGovern, D.P.; Stappenbeck, T.S. Spatial and temporal stability of Paneth cell phenotypes in Crohn’s disease: implications for prognostic cellular biomarker development. Inflamm. Bowel Dis. 2014, 20, 646–651. [Google Scholar] [CrossRef]
- Liu, T.C.; Gurram, B.; Baldridge, M.T.; Head, R.; Lam, V.; et al. Paneth cell defects in Crohn’s disease patients promote dysbiosis. JCI Insight 2016, 1, e86907. [Google Scholar] [CrossRef]
- Liu, T.C.; Kern, J.T.; VanDussen, K.L.; Xiong, S.; Kaiko, G.E.; et al. Interaction between smoking and ATG16L1T300A triggers Paneth cell defects in Crohn’s disease. J. Clin. Investig. 2018, 128, 5110–5122. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.C.; Naito, T.; Liu, Z.; VanDussen, K.L.; Haritunians, T.; et al. LRRK2 but not ATG16L1 is associated with Paneth cell defect in Japanese Crohn’s disease patients. JCI Insight 2017, 2, e91917. [Google Scholar] [CrossRef]
- VanDussen, K.L.; Liu, T.C.; Li, D.; Towfic, F.; Modiano, N.; et al. Genetic variants synthesize to produce Paneth cell phenotypes that define subtypes of Crohn’s disease. Gastroenterology 2014, 146, 200–209. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Lo, C.K.L.; Mertz, D.; Loeb, M. Newcastle-Ottawa Scale: comparing reviewers’ to authors’ assessments. BMC Med Res Methodol 2014, 14, 45. [Google Scholar] [CrossRef]
- Ananthakrishnan, A.N.; Khalili, H.; Konijeti, G.G.; et al. Long-term intake of dietary fat and risk of ulcerative colitis and Crohn's disease. Gut 2014, 63, 776–784. [Google Scholar] [CrossRef] [PubMed]
- Bottoms, L.; Leighton, D.; Carpenter, R.; Anderson, S.; Langmead, L.; Ramage, J.; Faulkner, J.; Coleman, E.; Fairhurst, C.; Seed, M.; et al. Affective and enjoyment responses to 12 weeks of high intensity interval training and moderate continuous training in adults with Crohn's disease. PLoS One. 2019, 14, e0222060. [Google Scholar] [CrossRef] [PubMed]
- Cosin-Roger, J.; Simmen, S.; Melhem, H.; Atrott, K.; Frey-Wagner, I.; Hausmann, M.; de Vallière, C.; Spalinger, M.R.; Spielmann, P.; Wenger, R.H.; et al. Hypoxia ameliorates intestinal inflammation through NLRP3/mTOR downregulation and autophagy activation. Nat Commun. 2017, 8, 98. [Google Scholar] [CrossRef]
- De Galan, C.; De Vos, M.; Hindryckx, P.; Laukens, D.; Van Welden, S. Long-Term Environmental Hypoxia Exposure and Haematopoietic Prolyl Hydroxylase-1 Deletion Do Not Impact Experimental Crohn's Like Ileitis. Biology (Basel). 2021, 10, 887. [Google Scholar] [CrossRef]
- Gómez-Ferrer, M.; Amaro-Prellezo, E.; Dorronsoro, A.; Sánchez-Sánchez, R.; Vicente, Á.; Cosín-Roger, J.; Barrachina, M.D.; Baquero, M.C.; Valencia, J.; Sepúlveda, P. HIF-Overexpression and Pro-Inflammatory Priming in Human Mesenchymal Stromal Cells Improves the Healing Properties of Extracellular Vesicles in Experimental Crohn's Disease. Int J Mol Sci. 2021, 22, 11269. [Google Scholar] [CrossRef]
- Guslandi, M.; Mezzi, G.; Sorghi, M.; Testoni, P.A. Saccharomyces boulardii in maintenance treatment of Crohn's disease. Dig Dis Sci. 2000, 45, 1462–4. [Google Scholar] [CrossRef] [PubMed]
- Jones, K.; Baker, K.; Speight, R.A.; Thompson, N.P.; Tew, G.A. Randomised clinical trial: combined impact and resistance training in adults with stable Crohn's disease. Aliment Pharmacol Ther. 2020, 52, 964–975. [Google Scholar] [CrossRef] [PubMed]
- Lewis, J.D.; Sandler, R.S.; Brotherton, C.; Brensinger, C.; Li, H.; Kappelman, M.D.; Daniel, S.G.; Bittinger, K.; Albenberg, L.; Valentine, J.F.; et al. A Randomized Trial Comparing the Specific Carbohydrate Diet to a Mediterranean Diet in Adults With Crohn's Disease. Gastroenterology. 2021, 161, 837–852.e9. [Google Scholar] [CrossRef]
- Limketkai, B.N.; Akobeng, A.K.; Gordon, M.; Adepoju, A.A. Probiotics for induction of remission in Crohn's disease. Cochrane Database Syst Rev. 2020, 7, CD006634. [Google Scholar] [CrossRef] [PubMed]
- Negm, M.; Bahaa, A.; Farrag, A.; et al. Effect of Ramadan intermittent fasting on inflammatory markers, disease severity, depression, and quality of life in patients with inflammatory bowel diseases: A prospective cohort study. BMC Gastroenterol 2022, 22, 203. [Google Scholar] [CrossRef] [PubMed]
- Ng, V.; Millard, W.; Lebrun, C.; Howard, J. Low-intensity exercise improves quality of life in patients with Crohn's disease. Clin J Sport Med. 2007, 17, 384–388. [Google Scholar] [CrossRef] [PubMed]
- Plein, K.; Hotz, J. Therapeutic effects of Saccharomyces boulardii on mild residual symptoms in a stable phase of Crohn's disease with special respect to chronic diarrhea--a pilot study. Z Gastroenterol. 1993, 31, 129–134. [Google Scholar] [PubMed]
- Scheffers, L.E.; Vos, I.K.; Utens, E.M.W.J.; Dieleman, G.C.; Walet, S.; Escher, J.C.; van den Berg, L.E.M.; Rotterdam Exercise Team. Physical Training and Healthy Diet Improved Bowel Symptoms, Quality of Life, and Fatigue in Children With Inflammatory Bowel Disease. J Pediatr Gastroenterol Nutr. 2023, 77, 214–221. [Google Scholar] [CrossRef]
- Schultz, M.; Timmer, A.; Herfarth, H.H.; Sartor, R.B.; Vanderhoof, J.A.; Rath, H.C. Lactobacillus GG in inducing and maintaining remission of Crohn's disease. BMC Gastroenterol. 2004, 4, 5. [Google Scholar] [CrossRef]
- Seeger, W.A.; Thieringer, J.; Esters, P.; Allmendinger, B.; Stein, J.; Schulze, H.; Dignass, A. Moderate endurance and muscle training is beneficial and safe in patients with quiescent or mildly active Crohn's disease. United European Gastroenterol J. 2020, 8, 804–813. [Google Scholar] [CrossRef]
- Starz, E.; Wzorek, K.; Folwarski, M.; Kaźmierczak-Siedlecka, K.; Stachowska, L.; Przewłócka, K.; Stachowska, E.; Skonieczna-Żydecka, K. The Modification of the Gut Microbiota via Selected Specific Diets in Patients with Crohn’s Disease. Nutrients 2021, 13, 2125. [Google Scholar] [CrossRef] [PubMed]
- Steed, H.; Macfarlane, G.T.; Blackett, K.L.; Bahrami, B.; Reynolds, N.; Walsh, S.V.; Cummings, J.H.; Macfarlane, S. Clinical trial: the microbiological and immunological effects of synbiotic consumption - a randomized double-blind placebo-controlled study in active Crohn's disease. Aliment Pharmacol Ther. 2010, 32, 872–83. [Google Scholar] [CrossRef] [PubMed]
- Su, H.; Kang, Q.; Wang, H.; Yin, H.; Duan, L.; Liu, Y.; Fan, R. Effects of glucocorticoids combined with probiotics in treating Crohn's disease on inflammatory factors and intestinal microflora. Exp Ther Med. 2018, 16, 2999–3003. [Google Scholar] [CrossRef]
- Suskind, D.L.; Lee, D.; Kim, Y.-M.; Wahbeh, G.; Singh, N.; Braly, K.; Nuding, M.; Nicora, C.D.; Purvine, S.O.; Lipton, M.S.; et al. The Specific Carbohydrate Diet and Diet Modification as Induction Therapy for Pediatric Crohn’s Disease: A Randomized Diet Controlled Trial. Nutrients 2020, 12, 3749. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Nakahigashi, M.; Umegae, S.; Kitagawa, T.; Matsumoto, K. Impact of Elemental Diet on Mucosal Inflammation in Patients with Active Crohn's Disease: Cytokine Production and Endoscopic and Histological Findings. Inflammatory Bowel Diseases 2005, 11, 580–588. [Google Scholar] [CrossRef]
- Tew, G.A.; Leighton, D.; Carpenter, R.; Anderson, S.; Langmead, L.; Ramage, J.; Faulkner, J.; Coleman, E.; Fairhurst, C.; Seed, M.; et al. High-intensity interval training and moderate-intensity continuous training in adults with Crohn's disease: a pilot randomised controlled trial. BMC Gastroenterol. 2019, 19, 19. [Google Scholar] [CrossRef]
- Walters, S.S.; Quiros, A.; Rolston, M.; Grishina, I.; Li, J.; Fenton, A.; DeSantis, T.Z.; Thai, A.; Andersen, G.L.; Papathakis, P.; et al. Analysis of Gut Microbiome and Diet Modification in Patients with Crohn's Disease. SOJ Microbiol Infect Dis. 2014, 2, 1–13. [Google Scholar] [CrossRef]
- Yılmaz, İ.; Dolar, M.E.; Özpınar, H. Effect of administering kefir on the changes in fecal microbiota and symptoms of inflammatory bowel disease: A randomized controlled trial. Turk J Gastroenterol. 2019, 30, 242–253. [Google Scholar] [CrossRef]
- Vincent, G.; Novak, E.A.; Siow, V.S.; Cunningham, K.E.; Griffith, B.D.; et al. Nix-mediated mitophagy modulates mitochondrial damage during intestinal inflammation. Antioxid. Redox Signal. 2020, 33, 1–19. [Google Scholar] [CrossRef]
- Natl. Inst. Health. 2020. MARVEL: Mitochondrial Anti-oxidant Therapy to Resolve Inflammation in Ulcerative Colitis (MARVEL). Natl. Inst. Health, Washington, DC. https://clinicaltrials.gov/ct2/show/NCT04276740.
- Gane, E.J.; Weilert, F.; Orr, D.W.; Keogh, G.F.; Gibson, M.; et al. The mitochondria-targeted anti-oxidant mitoquinone decreases liver damage in a phase II study of hepatitis C patients. Liver Int. 2010, 30, 1019–1026. [Google Scholar] [CrossRef]
- Snow, B.J.; Rolfe, F.L.; Lockhart, M.M.; Frampton, C.M.; O’Sullivan, J.D.; et al. A double-blind, placebo-controlled study to assess the mitochondria-targeted antioxidant MitoQ as a disease-modifying therapy in Parkinson’s disease. Mov. Disord. 2010, 25, 1670–1674. [Google Scholar] [CrossRef] [PubMed]
- Nicoletti, V.; Palermo, G.; Del Prete, E.; Mancuso, M.; Ceravolo, R. Understanding the multiple role of mitochondria in Parkinson’s disease and related disorders: lesson from genetics and protein-interaction network. Front. Cell Dev. Biol. 2021, 9, 636506. [Google Scholar] [CrossRef] [PubMed]
- Okuda, M.; Li, K.; Beard, M.R.; Showalter, L.A.; Scholle, F.; et al. Mitochondrial injury, oxidative stress, and antioxidant gene expression are induced by hepatitis C virus core protein. Gastroenterology 2002, 122, 366–375. [Google Scholar] [CrossRef] [PubMed]
- Hofer, A.; Noe, N.; Tischner, C.; Kladt, N.; Lellek, V.; et al. Defining the action spectrum of potential PGC-1α activators on a mitochondrial and cellular level in vivo. Hum. Mol. Genet. 2014, 23, 2400–2415. [Google Scholar] [CrossRef]
- Mancini, N.L.; Goudie, L.; Xu, W.; Sabouny, R.; Rajeev, S.; et al. Perturbed mitochondrial dynamics is a novel feature of colitis that can be targeted to lessen disease. Cell. Mol. Gastroenterol. Hepatol. 2020, 10, 287–307. [Google Scholar] [CrossRef] [PubMed]
- Cadwell, K.; Patel, K.K.; Maloney, N.S.; Liu, T.C.; Ng, A.C.; et al. Virus-plus-susceptibility gene interaction determines Crohn’s disease gene Atg16L1 phenotypes in intestine. Cell 2010, 141, 1135–1145. [Google Scholar] [CrossRef]
- Rogala, A.R.; Schoenborn, A.A.; Fee, B.E.; Cantillana, V.A.; Joyce, M.J.; et al. Environmental factors regulate Paneth cell phenotype and host susceptibility to intestinal inflammation in Irgm1-deficient mice. Dis. Model Mech. 2018, 11, dmm031070. [Google Scholar] [CrossRef]
- Nguyen, H.T.; Lapaquette, P.; Bringer, M.A.; Darfeuille-Michaud, A. Autophagy and Crohn’s disease. J. Innate Immun. 2013, 5, 434–443. [Google Scholar] [CrossRef]
- Kim, S.; Eun, H.S.; Jo, E.K. Roles of autophagy-related genes in the pathogenesis of inflammatory bowel disease. Cells 2019, 8, 77. [Google Scholar] [CrossRef]
- Lu, R.; Zhang, Y.; Xia, Y.; Zhang, J.; Kaser, A.; et al. Paneth cell alertness to pathogens maintained by vitamin D receptors. Gastroenterology 2021, 160, 1269–1283. [Google Scholar] [CrossRef]
- Cadwell, K.; Patel, K.K.; Komatsu, M.; Virgin, H.W.I.V.; Stappenbeck, T.S. A common role for Atg16L1, Atg5 and Atg7 in small intestinal Paneth cells and Crohn disease. Autophagy 2009, 5, 250–252. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
PRISMA protocol representing the study selection process for the review.
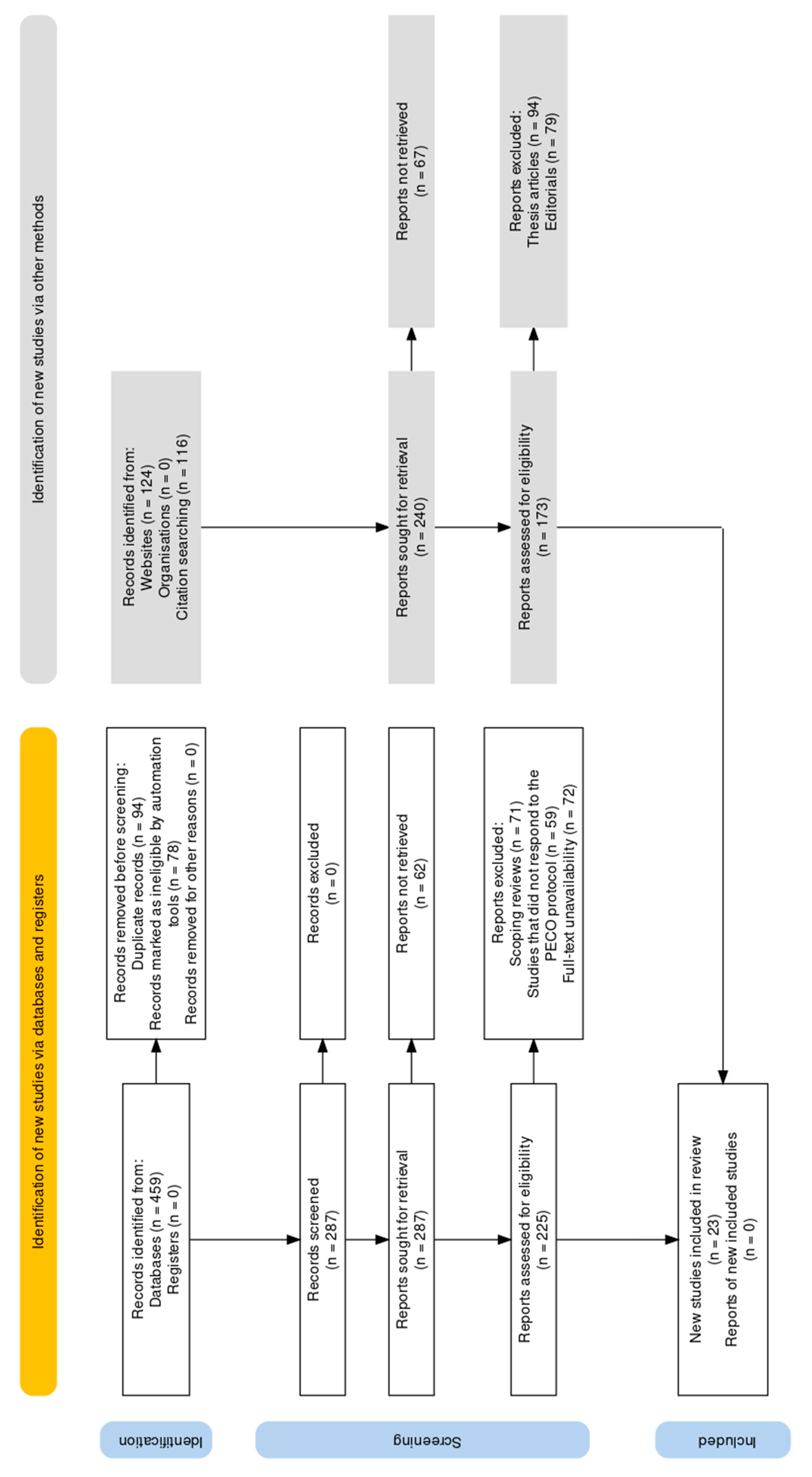
Figure 2.
Evaluation of bias in the selected papers.
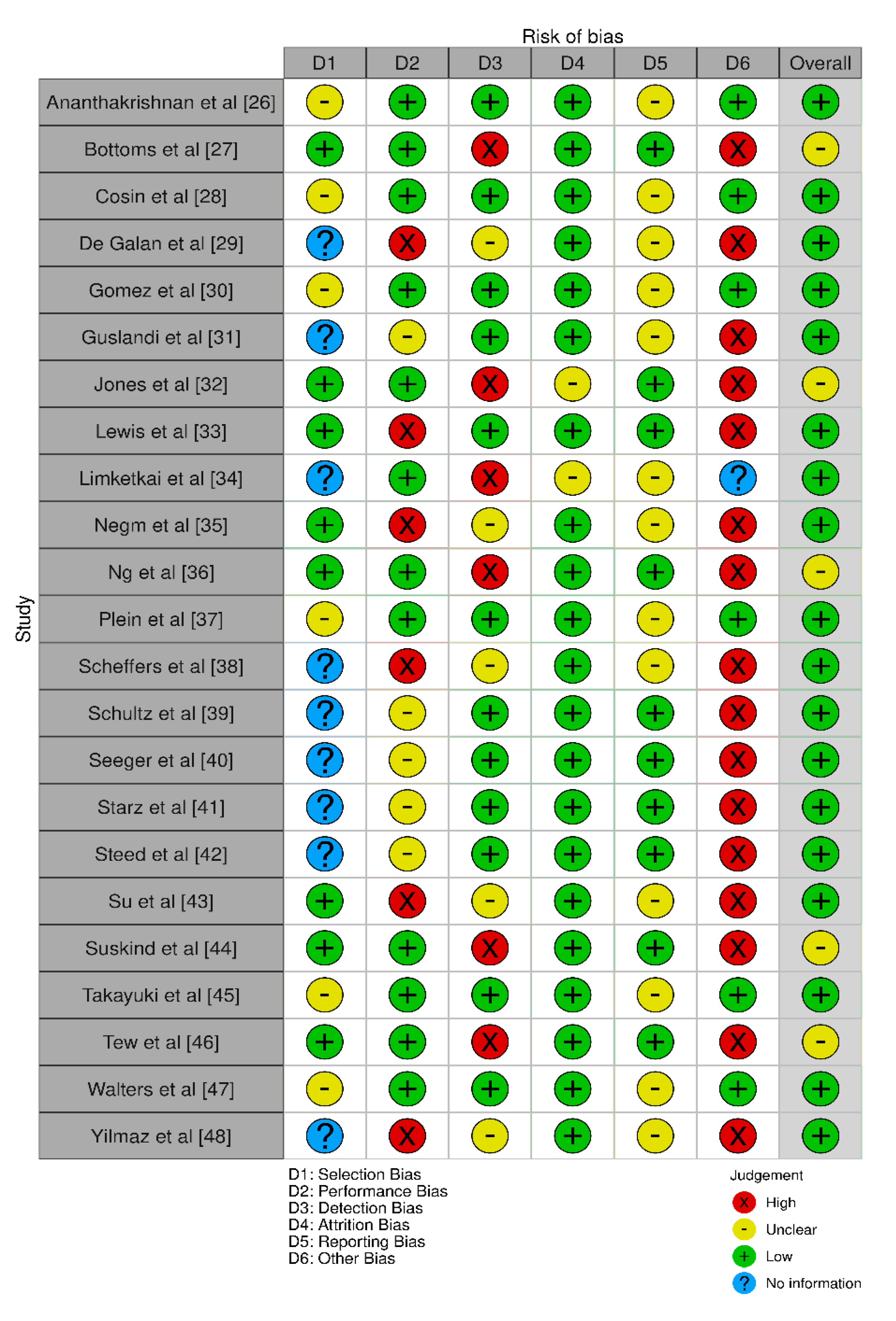

Table 1.
Search strings utilised across the databases.
| Database | Intermittent Cold Exposure | Intermittent Heat Exposure | Evolutionary Based Foods | Intermittent Fasting | Circadian-Based Interventions | Fermented Drinks | Fermented Foods | Intermittent Hypercapnia | Intermittent Hypoxia | Intermittent Exercise |
|---|---|---|---|---|---|---|---|---|---|---|
| PubMed | ("ice bath" OR "cold plunge" OR "whole body cryotherapy" OR "cryochamber") AND ("Crohn’s disease" OR "Crohn’s") | ("sauna" OR "infrared sauna") AND ("Crohn’s disease" OR "Crohn’s") | ("paleo diet" OR "paleolithic diet" OR "ketogenic diet" OR "carnivore diet") AND ("Crohn’s disease" OR "Crohn’s") | ("intermittent fasting" OR "caloric restriction" OR "fasting") AND ("Crohn’s disease" OR "Crohn’s") | ("bluelight therapy" OR "melatonin" OR "bright light therapy" OR "light therapy" OR "blue light blocker") AND ("Crohn’s disease" OR "Crohn’s") | ("probiotic drinks" OR "kefir" OR "kombucha" OR "ayran" OR "buttermilk") AND ("Crohn’s disease" OR "Crohn’s") | ("fermented foods" OR "miso" OR "natto" OR "Tempeh" OR "skyr" OR "strained yoghurt" OR "greek yoghurt") AND ("Crohn’s disease" OR "Crohn’s") | ("breath holding" OR "hypercapnia") AND ("Crohn’s disease" OR "Crohn’s") | ("ihht" OR "altitude training" OR "breath holding") AND ("Crohn’s disease" OR "Crohn’s") | ("hiit" OR "high intensity interval training" OR "tabata" OR "interval training") AND ("Crohn’s disease" OR "Crohn’s") |
| ScienceDirect | ("ice bath" OR "cold plunge" OR "whole body cryotherapy" OR "cryochamber") AND ("Crohn’s disease" OR "Crohn’s") | ("sauna" OR "infrared sauna") AND ("Crohn’s disease" OR "Crohn’s") | ("paleo diet" OR "paleolithic diet" OR "ketogenic diet" OR "carnivore diet") AND ("Crohn’s disease" OR "Crohn’s") | ("intermittent fasting" OR "caloric restriction" OR "fasting") AND ("Crohn’s disease" OR "Crohn’s") | ("bluelight therapy" OR "melatonin" OR "bright light therapy" OR "light therapy" OR "blue light blocker") AND ("Crohn’s disease" OR "Crohn’s") | ("probiotic drinks" OR "kefir" OR "kombucha" OR "ayran" OR "buttermilk") AND ("Crohn’s disease" OR "Crohn’s") | ("fermented foods" OR "miso" OR "natto" OR "Tempeh" OR "skyr" OR "strained yoghurt" OR "greek yoghurt") AND ("Crohn’s disease" OR "Crohn’s") | ("breath holding" OR "hypercapnia") AND ("Crohn’s disease" OR "Crohn’s") | ("ihht" OR "altitude training" OR "breath holding") AND ("Crohn’s disease" OR "Crohn’s") | ("hiit" OR "high intensity interval training" OR "tabata" OR "interval training") AND ("Crohn’s disease" OR "Crohn’s") |
| IEEE Xplore | ("ice bath" OR "cold plunge" OR "whole body cryotherapy" OR "cryochamber") AND ("Crohn’s disease" OR "Crohn’s") | ("sauna" OR "infrared sauna") AND ("Crohn’s disease" OR "Crohn’s") | ("paleo diet" OR "paleolithic diet" OR "ketogenic diet" OR "carnivore diet") AND ("Crohn’s disease" OR "Crohn’s") | ("intermittent fasting" OR "caloric restriction" OR "fasting") AND ("Crohn’s disease" OR "Crohn’s") | ("bluelight therapy" OR "melatonin" OR "bright light therapy" OR "light therapy" OR "blue light blocker") AND ("Crohn’s disease" OR "Crohn’s") | ("probiotic drinks" OR "kefir" OR "kombucha" OR "ayran" OR "buttermilk") AND ("Crohn’s disease" OR "Crohn’s") | ("fermented foods" OR "miso" OR "natto" OR "Tempeh" OR "skyr" OR "strained yoghurt" OR "greek yoghurt") AND ("Crohn’s disease" OR "Crohn’s") | ("breath holding" OR "hypercapnia") AND ("Crohn’s disease" OR "Crohn’s") | ("ihht" OR "altitude training" OR "breath holding") AND ("Crohn’s disease" OR "Crohn’s") | ("hiit" OR "high intensity interval training" OR "tabata" OR "interval training") AND ("Crohn’s disease" OR "Crohn’s") |
| PsycINFO | ("ice bath" OR "cold plunge" OR "whole body cryotherapy" OR "cryochamber") AND ("Crohn’s disease" OR "Crohn’s") | ("sauna" OR "infrared sauna") AND ("Crohn’s disease" OR "Crohn’s") | ("paleo diet" OR "paleolithic diet" OR "ketogenic diet" OR "carnivore diet") AND ("Crohn’s disease" OR "Crohn’s") | ("intermittent fasting" OR "caloric restriction" OR "fasting") AND ("Crohn’s disease" OR "Crohn’s") | ("bluelight therapy" OR "melatonin" OR "bright light therapy" OR "light therapy" OR "blue light blocker") AND ("Crohn’s disease" OR "Crohn’s") | ("probiotic drinks" OR "kefir" OR "kombucha" OR "ayran" OR "buttermilk") AND ("Crohn’s disease" OR "Crohn’s") | ("fermented foods" OR "miso" OR "natto" OR "Tempeh" OR "skyr" OR "strained yoghurt" OR "greek yoghurt") AND ("Crohn’s disease" OR "Crohn’s") | ("breath holding" OR "hypercapnia") AND ("Crohn’s disease" OR "Crohn’s") | ("ihht" OR "altitude training" OR "breath holding") AND ("Crohn’s disease" OR "Crohn’s") | ("hiit" OR "high intensity interval training" OR "tabata" OR "interval training") AND ("Crohn’s disease" OR "Crohn’s") |
| Web of Science | ("ice bath" OR "cold plunge" OR "whole body cryotherapy" OR "cryochamber") AND ("Crohn’s disease" OR "Crohn’s") | ("sauna" OR "infrared sauna") AND ("Crohn’s disease" OR "Crohn’s") | ("paleo diet" OR "paleolithic diet" OR "ketogenic diet" OR "carnivore diet") AND ("Crohn’s disease" OR "Crohn’s") | ("intermittent fasting" OR "caloric restriction" OR "fasting") AND ("Crohn’s disease" OR "Crohn’s") | ("bluelight therapy" OR "melatonin" OR "bright light therapy" OR "light therapy" OR "blue light blocker") AND ("Crohn’s disease" OR "Crohn’s") | ("probiotic drinks" OR "kefir" OR "kombucha" OR "ayran" OR "buttermilk") AND ("Crohn’s disease" OR "Crohn’s") | ("fermented foods" OR "miso" OR "natto" OR "Tempeh" OR "skyr" OR "strained yoghurt" OR "greek yoghurt") AND ("Crohn’s disease" OR "Crohn’s") | ("breath holding" OR "hypercapnia") AND ("Crohn’s disease" OR "Crohn’s") | ("ihht" OR "altitude training" OR "breath holding") AND ("Crohn’s disease" OR "Crohn’s") | ("hiit" OR "high intensity interval training" OR "tabata" OR "interval training") AND ("Crohn’s disease" OR "Crohn’s") |
| Embase | ("ice bath" OR "cold plunge" OR "whole body cryotherapy" OR "cryochamber") AND ("Crohn’s disease" OR "Crohn’s") | ("sauna" OR "infrared sauna") AND ("Crohn’s disease" OR "Crohn’s") | ("paleo diet" OR "paleolithic diet" OR "ketogenic diet" OR "carnivore diet") AND ("Crohn’s disease" OR "Crohn’s") | ("intermittent fasting" OR "caloric restriction" OR "fasting") AND ("Crohn’s disease" OR "Crohn’s") | ("bluelight therapy" OR "melatonin" OR "bright light therapy" OR "light therapy" OR "blue light blocker") AND ("Crohn’s disease" OR "Crohn’s") | ("probiotic drinks" OR "kefir" OR "kombucha" OR "ayran" OR "buttermilk") AND ("Crohn’s disease" OR "Crohn’s") | ("fermented foods" OR "miso" OR "natto" OR "Tempeh" OR "skyr" OR "strained yoghurt" OR "greek yoghurt") AND ("Crohn’s disease" OR "Crohn’s") | ("breath holding" OR "hypercapnia") AND ("Crohn’s disease" OR "Crohn’s") | ("ihht" OR "altitude training" OR "breath holding") AND ("Crohn’s disease" OR "Crohn’s") | ("hiit" OR "high intensity interval training" OR "tabata" OR "interval training") AND ("Crohn’s disease" OR "Crohn’s") |
| CINAHL | ("ice bath" OR "cold plunge" OR "whole body cryotherapy" OR "cryochamber") AND ("Crohn’s disease" OR "Crohn’s") | ("sauna" OR "infrared sauna") AND ("Crohn’s disease" OR "Crohn’s") | ("paleo diet" OR "paleolithic diet" OR "ketogenic diet" OR "carnivore diet") AND ("Crohn’s disease" OR "Crohn’s") | ("intermittent fasting" OR "caloric restriction" OR "fasting") AND ("Crohn’s disease" OR "Crohn’s") | ("bluelight therapy" OR "melatonin" OR "bright light therapy" OR "light therapy" OR "blue light blocker") AND ("Crohn’s disease" OR "Crohn’s") | ("probiotic drinks" OR "kefir" OR "kombucha" OR "ayran" OR "buttermilk") AND ("Crohn’s disease" OR "Crohn’s") | ("fermented foods" OR "miso" OR "natto" OR "Tempeh" OR "skyr" OR "strained yoghurt" OR "greek yoghurt") AND ("Crohn’s disease" OR "Crohn’s") | ("breath holding" OR "hypercapnia") AND ("Crohn’s disease" OR "Crohn’s") | ("ihht" OR "altitude training" OR "breath holding") AND ("Crohn’s disease" OR "Crohn’s") | ("hiit" OR "high intensity interval training" OR "tabata" OR "interval training") AND ("Crohn’s disease" OR "Crohn’s") |
| Scopus | ("ice bath" OR "cold plunge" OR "whole body cryotherapy" OR "cryochamber") AND ("Crohn’s disease" OR "Crohn’s") | ("sauna" OR "infrared sauna") AND ("Crohn’s disease" OR "Crohn’s") | ("paleo diet" OR "paleolithic diet" OR "ketogenic diet" OR "carnivore diet") AND ("Crohn’s disease" OR "Crohn’s") | ("intermittent fasting" OR "caloric restriction" OR "fasting") AND ("Crohn’s disease" OR "Crohn’s") | ("bluelight therapy" OR "melatonin" OR "bright light therapy" OR "light therapy" OR "blue light blocker") AND ("Crohn’s disease" OR "Crohn’s") | ("probiotic drinks" OR "kefir" OR "kombucha" OR "ayran" OR "buttermilk") AND ("Crohn’s disease" OR "Crohn’s") | ("fermented foods" OR "miso" OR "natto" OR "Tempeh" OR "skyr" OR "strained yoghurt" OR "greek yoghurt") AND ("Crohn’s disease" OR "Crohn’s") | ("breath holding" OR "hypercapnia") AND ("Crohn’s disease" OR "Crohn’s") | ("ihht" OR "altitude training" OR "breath holding") AND ("Crohn’s disease" OR "Crohn’s") | ("hiit" OR "high intensity interval training" OR "tabata" OR "interval training") AND ("Crohn’s disease" OR "Crohn’s") |
| Google Scholar | ("ice bath" OR "cold plunge" OR "whole body cryotherapy" OR "cryochamber") AND ("Crohn’s disease" OR "Crohn’s") | ("sauna" OR "infrared sauna") AND ("Crohn’s disease" OR "Crohn’s") | ("paleo diet" OR "paleolithic diet" OR "ketogenic diet" OR "carnivore diet") AND ("Crohn’s disease" OR "Crohn’s") | ("intermittent fasting" OR "caloric restriction" OR "fasting") AND ("Crohn’s disease" OR "Crohn’s") | ("bluelight therapy" OR "melatonin" OR "bright light therapy" OR "light therapy" OR "blue light blocker") AND ("Crohn’s disease" OR "Crohn’s") | ("probiotic drinks" OR "kefir" OR "kombucha" OR "ayran" OR "buttermilk") AND ("Crohn’s disease" OR "Crohn’s") | ("fermented foods" OR "miso" OR "natto" OR "Tempeh" OR "skyr" OR "strained yoghurt" OR "greek yoghurt") AND ("Crohn’s disease" OR "Crohn’s") | ("breath holding" OR "hypercapnia") AND ("Crohn’s disease" OR "Crohn’s") | ("ihht" OR "altitude training" OR "breath holding") AND ("Crohn’s disease" OR "Crohn’s") | ("hiit" OR "high intensity interval training" OR "tabata" OR "interval training") AND ("Crohn’s disease" OR "Crohn’s") |
Table 2.
Demographic characteristics of the included papers.
| Study | Aims | Study design | Methodology assessed | Type of mitochondrial intervention assessed |
|---|---|---|---|---|
| Ananthakrishnan et al [26] | Investigate the association between dietary fat and risk of Crohn's disease (CD) and ulcerative colitis (UC). | Prospective cohort study | Cox proportional hazards models | Long-chain n-3 PUFAs, trans-unsaturated fatty acids |
| Bottoms et al [27] | Explore affective and enjoyment responses to high-intensity interval training (HIIT) and moderate-intensity continuous training (MICT) in adults with Crohn's disease (CD). | Randomized feasibility trial | Heart rate, ratings of perceived exertion (RPE-L and RPE-C), feeling state (FS), Physical Activity Enjoyment Scale (PACES) | HIIT and MICT protocols |
| Cosin et al [28] | Investigate the role of hypoxia in regulating inflammation and autophagy in Crohn's disease patients and murine colitis models. | Experimental study | Measurement of inflammatory markers, autophagy, and NLRP3 expression | Hypoxia, HIF-1α activation, mTOR/NLRP3 pathway, autophagy |
| De Galan et al [29] | - Investigate the impact of environmental hypoxia and immune cell-specific deletion of oxygen sensor prolyl hydroxylase (PHD) 1 on Crohn's-like ileitis in mice. | Experimental mouse model | - Haematological assessment - Evaluation of distal ileal hypoxia via pimonidazole staining - Histological scoring and gene expression analysis - Comparison between TNF∆ARE/+ mice and Phd1-deficient TNF∆ARE/+ mice |
Environmental hypoxia, immune cell-specific Phd1-deletion |
| Gomez et al [30] | - Assess the therapeutic potential of extracellular vesicles (EVs) derived from mesenchymal stromal cells (MSCs) engineered to overexpress hypoxia-inducible factor 1-alpha and telomerase. | Experimental in vitro and in vivo studies | - Analysis of macrophage repolarization, cytokine release, and functional assays - Evaluation of anti-inflammatory effects on endothelium and fibrosis - Testing in a mouse colitis model | EVs derived from MSCs overexpressing HIF-1alpha and telomerase |
| Guslandi et al [31] | - Evaluate the role of Saccharomyces boulardii in the maintenance treatment of Crohn's disease in patients in clinical remission. | Randomized controlled trial | Comparison of clinical relapses based on CDAI values between patients receiving mesalamine alone and those receiving mesalamine plus Saccharomyces boulardii | Saccharomyces boulardii as a probiotic agent |
| Jones et al [32] | To assess the effect of 6 months of combined impact and resistance training on bone mineral density (BMD) and muscle function in adults with CD. | Randomized controlled trial with exercise and control groups. | - Measurement of BMD using dual energy X-ray absorptiometry. - Assessment of muscle function including measures of upper and lower limb strength and endurance. - Evaluation of fatigue severity. |
Combined impact and resistance training program for 6 months. |
| Lewis et al [33] | To compare the effectiveness of the Specific Carbohydrate Diet (SCD) to the Mediterranean diet (MD) as treatment for Crohn's disease (CD) with mild to moderate symptoms. | Randomized controlled trial comparing SCD and MD diets. | - Assessment of symptomatic remission at week 6. - Measurement of fecal calprotectin (FC) response. - Measurement of C-reactive protein (CRP) response. |
Specific Carbohydrate Diet (SCD) and Mediterranean diet (MD). |
| Limketkai et al [34] | To assess the efficacy and safety of probiotics for the induction of remission in CD. | Inclusion of two studies involving probiotics and placebo groups. | - Assessment of remission induction in CD. - Evaluation of adverse events. |
Lactobacillus rhamnosus strain GG and synbiotic treatment. |
| Negm et al [35] | - Effect of IF during Ramadan on CD patients - Impact on clinical disease activity, quality of life, and depression |
Prospective study with IBD patients observing Ramadan fasting | - Serum CRP and stool calprotectin levels - Partial Mayo score - Harvey Bradshaw index - Simple IBD questionnaire |
Intermittent fasting (IF) during Ramadan |
| Ng et al [36] | - Effects of low-intensity walking on Crohn's disease patients' quality of life | Prospective study with exercise and nonexercise groups | - Inflammatory Bowel Disease Questionnaire - Inflammatory Bowel Disease Stress Index - Harvey-Bradshaw Simple Index |
Low-intensity walking program |
| Plein et al [37] | - Effects of Saccharomyces boulardii on Crohn's disease patients with diarrhea | Randomized, double-blind, placebo-controlled pilot study | - Frequency of bowel movements - BEST Index | Saccharomyces boulardii (S.b.) yeast preparation |
| Scheffers et al [38] | Assess the effects of a 12-week lifestyle intervention in children with IBD. | Randomized semi-crossover controlled trial, lifestyle program (physical training + dietary advice) | Physical fitness, patient-reported outcomes, clinical disease activity, nutritional status | Lifestyle intervention (physical training + diet) |
| Schultz et al [39] | Determine the effect of oral Lactobacillus GG (L. GG) on inducing or maintaining medically induced remission in Crohn's disease. | Randomized placebo-controlled trial | Inducing or maintaining remission in Crohn's disease | Oral Lactobacillus GG (L. GG) |
| Seeger et al [40] | Examine and compare the safety, feasibility, and potential beneficial effects of individual moderate endurance and moderate muscle training in patients with Crohn's disease. | Random allocation to control, endurance, or muscle training group | Safety, feasibility, disease activity, inflammatory parameters, quality of life, physical activity, and strength | Moderate endurance and moderate muscle training |
| Starz et al [41] | Investigate the influence of reduction diets, including low-FODMAP diet and others, on the microbiome of patients with CD. | Review article | Effect of reduction diets (e.g., low-FODMAP, lactose-free, gluten-free) on gut microbiota composition and diversity. | Dietary interventions |
| Steed et al [42] | Investigate the effects of synbiotic consumption (Bifidobacterium longum and Synergy 1) on disease processes in patients with Crohn's disease. | Randomized, double-blind placebo-controlled trial | Clinical outcomes, histological scores, immune marker transcription levels, mucosal bacterial 16S rRNA gene copy numbers. | Synbiotic supplementation (Bifidobacterium longum and Synergy 1) |
| Su et al [43] | Investigate the effect of glucocorticoids combined with probiotics on inflammatory factors and intestinal microflora in the treatment of Crohn's disease. | Randomized controlled trial (control group with oral sulfasalazine, treatment group with probiotics and glucocorticoids) | Clinical efficacy, changes in inflammatory factors, incidence of infection, changes in intestinal flora. | Combination of glucocorticoids and probiotics |
| Suskind et al [44] | To determine the potential efficacy of three versions of the specific carbohydrate diet (SCD) in active Crohn’s Disease. | 18 patients with mild/moderate CD were enrolled and randomized to SCD, modified SCD (MSCD), or whole foods (WF) diet. Evaluation at baseline, 2, 4, 8, and 12 weeks included PCDAI, inflammatory labs, and multi-omics evaluations. | Impact of SCD, MSCD, and WF diets on clinical remission, CRP levels, and microbiome composition. | Specific Carbohydrate Diet (SCD), Modified SCD (MSCD), Whole Foods (WF) Diet |
| Takayuki et al [45] | To examine the impact of elemental diet (Elental) on mucosal inflammation in Crohn's disease, mainly by cytokine measurements. | 28 consecutive patients with active CD were treated with Elental for 4 weeks. Mucosal biopsies were obtained before and after treatment. Control group consisted of 20 patients without inflammation. | Effect of elemental diet on clinical remission, endoscopic healing, histologic healing, and mucosal cytokine concentrations. | Elemental Diet (Elental) |
| Tew et al [46] | To assess the feasibility and acceptability of high-intensity interval training (HIIT) and moderate-intensity continuous training (MICT) in adults with Crohn's disease (CD). | Participants with quiescent or mildly-active CD were randomly assigned to HIIT, MICT, or usual care control. Feasibility outcomes included recruitment, retention, outcome completion, exercise attendance. Data collected on cardiorespiratory fitness, disease activity, and more. | Feasibility and acceptability of HIIT and MICT exercise training in adults with CD. | High-Intensity Interval Training (HIIT), Moderate-Intensity Continuous Training (MICT) |
| Walters et al [47] | Develop methodology for fecal sample processing and detect changes in gut microbiota of Crohn’s disease patients receiving specialized diets | Pilot diet crossover trial comparing specific carbohydrate diet (SCD) vs. low residue diet (LRD) on gut microbiota composition and resolution of IBD symptoms. Assessment of gut microbiota using high-density DNA microarray PhyloChip. | DNA extraction using a column-based method, gut microbiota composition, microbial complexity, changes in B. fragilis abundance | Specialized carbohydrate diet (SCD) vs. low residue diet (LRD) |
| Yilmaz et al [48] | Investigate effects of kefir consumption on fecal microflora and symptoms of IBD patients | Single-center, prospective, open-label randomized controlled trial. Administration of 400 mL/day kefir to patients for 4 weeks. Assessment of stool Lactobacillus and Lactobacillus kefiri content by real-time quantitative polymerase chain reaction. | Stool Lactobacillus and Lactobacillus kefiri content, abdominal pain, bloating, stool frequency, stool consistency, feeling good scores | Probiotic consumption |
Table 3.
Characteristics pertaining to CD as observed in the included papers.
| Study | Parameters Assessed | Inferences Observed | Results Observed |
|---|---|---|---|
| Ananthakrishnan et al [26] | - Dietary fat intake (total fat, saturated fats, unsaturated fats, n-6 and n-3 PUFAs, trans-unsaturated fatty acids) - Risk of Crohn's disease (CD) and ulcerative colitis (UC) |
- No association between cumulative energy-adjusted intake of various fats and risk of CD or UC. - High intake of long-chain n-3 PUFAs may be associated with a trend towards lower risk of UC. - High long-term intake of trans-unsaturated fatty acids may be associated with a trend towards an increased incidence of UC. |
- No significant association between various fat intake and CD or UC risk. - Long-chain n-3 PUFAs associated with a potential lower risk of UC. - Trans-unsaturated fatty acids potentially linked to increased UC incidence. |
| Bottoms et al [27] | - Heart rate (HR) - Ratings of perceived exertion for legs (RPE-L) and central (RPE-C) - Feeling state (FS) - Physical Activity Enjoyment Scale (PACES) - Affective and enjoyment responses to high-intensity interval training (HIIT) and moderate-intensity continuous training (MICT) in adults with Crohn's disease (CD) |
- HR, RPE-L, and RPE-C were higher during HIIT compared to MICT. - FS scores were similar between HIIT and MICT. - No significant difference in PACES scores between HIIT and MICT. - Both HIIT and MICT protocols elicited similar enjoyment and affect in adults with quiescent or mildly-active CD. |
- HR during HIIT significantly greater than during MICT. - Higher RPE-L and RPE-C during HIIT compared to MICT. - Similar FS scores between HIIT and MICT. - No significant difference in PACES scores between HIIT and MICT. - HIIT and MICT both resulted in similar enjoyment and affect in CD patients. |
| Cosin et al [28] | - Expression of inflammatory markers (TNF-α, IL-6, NLRP3) - Autophagy modulation - Effects of hypoxia and dimethyloxalylglycine-mediated hydroxylase inhibition on inflammation - Role of mTOR/NLRP3 pathway in inflammation and autophagy regulation |
- Hypoxia reduces inflammatory markers and increases autophagy. - Hypoxia inhibits NF-κB signaling and NLRP3 expression. - Hypoxia counteracts inflammation by downregulating mTOR/NLRP3 pathway and promoting autophagy. - Hypoxia and HIF-1α activation are protective in mouse models of colitis. |
- Reduced expression of TNF-α, IL-6, and NLRP3 in response to hypoxia. - Increased autophagy and reduced NF-κB signaling and NLRP3 expression due to hypoxia. - Dimethyloxalylglycine-mediated hydroxylase inhibition ameliorates colitis and downregulates NLRP3 while promoting autophagy. - Hypoxia and HIF-1α activation are protective against colitis by inhibiting mTOR/NLRP3 pathway and promoting autophagy. |
| De Galan et al [29] | - Impact of environmental hypoxia and immune cell-specific deletion of oxygen sensor prolyl hydroxylase (PHD) 1 on Crohn's-like ileitis in mice. - Systemic inflammation assessed by haematology. - Distal ileal hypoxia evaluated by pimonidazole staining. - Histological scoring and gene expression analysis of ileitis. |
- Long-term environmental hypoxia or haematopoietic Phd1-deletion does not impact experimental ileitis development. - Hypoxia increases red blood cell count, haemoglobin, haematocrit, and pimonidazole intensity in the ileum. - Hypoxia leads to an increase in circulatory monocytes, ileal mononuclear phagocytes, and proinflammatory cytokine expression in WT mice. - No histological or ileal gene expression differences identified between TNF∆ARE/+ mice in hypoxia versus normoxia or between haematopoietic Phd1-deficient TNF∆ARE/+ and WT counterparts. |
- Long-term hypoxia or Phd1-deletion does not affect ileitis development. - Hypoxia-related changes in blood parameters and ileal hypoxia are observed. - Hypoxia induces an increase in circulatory monocytes, ileal mononuclear phagocytes, and proinflammatory cytokine expression in WT mice, but this does not translate into histological or gene expression differences in TNF∆ARE/+ mice. |
| Gomez et al [30] | - Effects of extracellular vesicles (EVs) derived from MSCs engineered to overexpress HIF-1alpha and telomerase on M1 macrophages (Mφ1) repolarization. - Analysis of surface markers, cytokines, and functional assays in co-culture. - Anti-inflammatory effects on activated endothelium and fibrosis. - Therapeutic capacity in a mouse colitis model. |
- EVMSC-T-HIFc induces repolarization of monocytes from Mφ1 to an Mφ2-like phenotype with reduced inflammatory cytokine release. - EVMSC-T-HIFc-treated Mφ1 exhibits immunosuppressive effects similar to Mφ2 on activated PBMCs and reduces PBMC adhesion to activated endothelium. - EVMSC-T-HIFc prevents myofibroblast differentiation in TGF-β-treated fibroblasts. - EVMSC-T-HIFc administration promotes healing in a mouse colitis model. |
- EVMSC-T-HIFc effectively repolarizes Mφ1, reducing inflammatory cytokine release. - Immunomodulatory effects of EVMSC-T-HIFc are similar to Mφ2. - EVMSC-T-HIFc reduces PBMC adhesion to activated endothelium and prevents myofibroblast differentiation. - EVMSC-T-HIFc promotes healing in a mouse colitis model, preserving colon length and altering the Mφ1/Mφ2 ratio. |
| Guslandi et al [31] | - Role of Saccharomyces boulardii in the maintenance treatment of Crohn's disease in patients in clinical remission. - Clinical relapses assessed by CDAI values. |
- Saccharomyces boulardii may represent a useful tool in the maintenance treatment of Crohn's disease, as clinical relapses were less frequent in patients receiving mesalamine plus the probiotic agent. | - Clinical relapses as assessed by CDAI values were less frequent in patients treated with mesalamine plus Saccharomyces boulardii compared to those receiving mesalamine alone, suggesting a potential role for Saccharomyces boulardii in the maintenance treatment of Crohn's disease. |
| Jones et al [32] | - Bone mineral density (BMD) - Muscle function |
- Exercise intervention for 6 months improved BMD at the lumbar spine. - Exercise group had superior muscle function outcomes. - Lower fatigue severity observed in the exercise group. |
- BMD values were significantly higher in the exercise group at the lumbar spine. - Superior muscle function outcomes in the exercise group. - Lower fatigue severity in the exercise group. - Three exercise-related adverse events reported. |
| Lewis et al [33] | - Symptomatic remission - Fecal calprotectin (FC) response - C-reactive protein (CRP) response |
- Specific Carbohydrate Diet (SCD) was not superior to the Mediterranean diet (MD) in achieving symptomatic remission. - No significant differences in FC and CRP responses between SCD and MD groups. |
- Symptomatic remission rates at week 6 were similar between SCD and MD groups. |
| Limketkai et al [34] | - Remission induction in CD - Adverse events |
- Probiotics did not show a significant difference compared to placebo in inducing remission in Crohn's disease (CD) after six months. | - No significant difference in remission induction between probiotics and placebo. - No significant difference in adverse events between probiotics and placebo. |
| Negm et al [35] | - Serum CRP and stool calprotectin levels - Partial Mayo score - Harvey Bradshaw index - Simple IBD questionnaire |
- No significant change in serum CRP and stool calprotectin levels - Significant rise in partial Mayo score after fasting - Older age and higher baseline calprotectin associated with higher Mayo score change |
- Serum CRP (median): 0.53 vs 0.50, P = 0.27 - Calprotectin (median): 163 vs 218, P = 0.62 - Partial Mayo score (median): 1 vs 1, P = 0.02 - Harvey-Bradshaw index (median): 4 vs 5, P = 0.4 - Worsening clinical parameters in UC patients, more pronounced in older patients and those with higher baseline calprotectin levels |
| Ng et al [36] | - Inflammatory Bowel Disease Questionnaire - Inflammatory Bowel Disease Stress Index - Harvey-Bradshaw Simple Index |
- Statistically significant improvement in quality of life in all 3 outcome measurement questionnaires - No detrimental effects on disease activity |
- Exercise group showed significant improvement in quality of life based on the mentioned questionnaires (P < 0.05) |
| Plein et al [37] | - Frequency of bowel movements - BEST Index | - Reduction in the frequency of bowel movements and BEST Index as compared to baseline - S.b. group showed significant reduction in frequency of bowel movements and BEST Index - No adverse drug events observed |
- Frequency of bowel movements (evacuations/day): 5.0 +/- 1.4 vs 4.1 +/- 2.3, p < 0.01 - BEST Index: 193 +/- 32 vs 168 +/- 59, p < 0.05 - S.b. group had reduced frequency of bowel movements and BEST Index in the tenth week (3.3 +/- 1.2 evacuations/day and 107 +/- 85) - Control group did not show this effect; values returned to initial levels |
| Scheffers et al [38] | Physical fitness (maximal and submaximal exercise capacity, strength, core stability), patient-reported outcomes, clinical disease activity, nutritional status | 12-week lifestyle intervention improved bowel symptoms, quality of life, and fatigue in pediatric IBD patients. | - Peak VO2 did not change significantly after the 12-week program. - Exercise capacity measured by 6-minute walking test and core stability improved. - Pediatric Crohn's Disease Activity Index decreased significantly. - Fecal calprotectin decreased significantly. - Quality of life (IMPACT-III) improved on 4 out of 6 domains and total score. - Parents-reported quality of life and total fatigue score also improved significantly. |
| Schultz et al [39] | Effect of oral Lactobacillus GG (L. GG) on inducing or maintaining medically induced remission in Crohn's disease. | L. GG did not demonstrate a benefit in inducing or maintaining medically induced remission in Crohn's disease. | - 5 out of 11 patients finished the study. - Median time to relapse was not significantly different between L. GG and placebo groups. |
| Seeger et al [40] | Safety, feasibility, and potential beneficial effects of individual moderate endurance and moderate muscle training in patients with Crohn's disease. | Both individual moderate endurance and muscle training can be safely performed in patients with mild or quiescent Crohn's disease. | - Higher dropout rate in the endurance group compared to the muscle group. - Maximal and average strength in upper and lower extremities increased significantly in both groups. - Emotional function significantly improved in the endurance group. - No statistically significant changes in disease activity or other outcome parameters in this pilot cohort. |
| Starz et al [41] | Influence of reduction diets (e.g., low-FODMAP, lactose-free, gluten-free) on the gut microbiota composition and diversity. | Reduction diets may lead to decreased abundance of beneficial microbial species (e.g., Bifidobacterium, Faecalibacterium prausnitzii) and reduced microbial diversity. CDED (Crohn’s disease exclusion diet) with partial enteral nutrition has a positive influence on the microbiota. | Reduction diets, including low-FODMAP, lactose-free, and gluten-free diets, negatively affect microbial diversity and the abundance of beneficial microbial species. CDED improves microbiota and may impact the future course of the disease. |
| Steed et al [42] | Clinical outcomes, histological scores, immune marker transcription levels, mucosal bacterial 16S rRNA gene copy numbers. | Synbiotic consumption (Bifidobacterium longum and Synergy 1) improves clinical outcomes, reduces Crohn's disease activity indices, and histological scores. It has a limited effect on certain immune markers (IL-18, INF-gamma, IL-1beta) but reduces TNF-alpha expression at 3 months. Mucosal bifidobacteria increase in synbiotic patients. | Synbiotic consumption (Bifidobacterium longum and Synergy 1) is effective in improving clinical symptoms, reducing disease activity indices, and histological scores in patients with active Crohn's disease. It leads to changes in specific immune markers and an increase in mucosal bifidobacteria. |
| Su et al [43] | Clinical efficacy, changes in inflammatory factors, incidence of infection, changes in intestinal flora. | Combination of probiotics and glucocorticoids in the treatment of Crohn's disease improves clinical curative effect, reduces the secretion of inflammatory factors, and enhances intestinal flora (e.g., increased lactobacillus and reduced yeast, enterococci, and peptococcus). Treatment group exhibits significantly higher treatment efficiency and lower infection rate compared to the control group. | Combining probiotics with glucocorticoids in Crohn's disease treatment results in improved clinical outcomes, reduced inflammatory factors, and positive changes in intestinal flora composition. The treatment group shows better treatment efficiency and lower infection rates compared to conventional treatment methods. |
| Suskind et al [44] | PCDAI, inflammatory labs, multi-omics evaluations | At week 12, all participants (n = 10) who completed the study achieved clinical remission. The C-reactive protein (CRP) levels decreased significantly in all three diet groups (SCD, MSCD, and WF). The microbiome composition shifted in all patients across the study period, with consistent changes in the predicted metabolic mode of organisms. | Clinical remission achieved in all participants. Significant reduction in CRP levels. Shifts in microbiome composition. |
| Takayuki et al [45] | Mucosal cytokine concentrations (IL-1β, IL-1ra, IL-6, IL-8, TNF-α) | Clinical remission achieved in 71% of patients. Endoscopic healing and improvement rates were observed in the terminal ileum and large bowel. Histologic healing and improvement rates were also observed. Changes in mucosal cytokine concentrations, specifically a decrease after treatment. Correction of the IL-1ra/IL-1β ratio. | Clinical remission, endoscopic healing, and histologic healing observed. Reduction in mucosal cytokine levels. Correction of IL-1ra/IL-1β ratio. |
| Tew et al [46] | Feasibility outcomes (recruitment, retention, outcome completion, etc.), cardiorespiratory fitness, disease activity, quality of life, adverse events, intervention acceptability | High attendance and completion rates for both HIIT and MICT groups. Mean increase in peak oxygen uptake was greater following HIIT than MICT. Few non-serious exercise-related adverse events, and some participants experienced disease relapse during follow-up. | High feasibility and acceptability of HIIT and MICT exercise training. Greater improvement in peak oxygen uptake with HIIT. Some adverse events and disease relapses observed. |
| Walters et al [47] | Gut microbiota composition, microbial complexity, abundance of Bacteroides fragilis | Lower gut microbiome complexity in IBD patients compared to healthy controls. Increased abundance of B. fragilis in fecal samples from IBD patients. Changes in gut microbiome composition and complexity in response to specialized carbohydrate diet (SCD). SCD associated with restructuring of gut microbial communities. | - The complexity of the gut microbiome was lower in IBD patients. - Increased abundance of B. fragilis in fecal samples of IBD-positive patients. - Temporal response to SCD resulted in increased microbial diversity. - LRD diet associated with reduced diversity of microbial communities. - Changes in composition and complexity of the gut microbiome observed in response to specialized carbohydrate diet. |
| Yilmaz et al [48] | Stool Lactobacillus, Lactobacillus kefiri content, abdominal symptoms, feeling good scores | Kefir consumption may modulate gut microbiota. Significant decrease in erythrocyte sedimentation rate and C-reactive protein in patients with CD. Increased hemoglobin levels. Bloating scores significantly reduced in the last 2 weeks of the study. Increased feeling good scores. | - Stool Lactobacillus bacterial load in treatment group between 104 and 109 CFU/g. - Significant reductions in erythrocyte sedimentation rate and C-reactive protein in CD patients. - Increased hemoglobin levels. - Reduction in bloating scores during the last 2 weeks. - Improvement in feeling good scores. - Kefir consumption may improve patient's quality of life in the short term. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



