
Submitted:
15 September 2023
Posted:
20 September 2023
You are already at the latest version
Abstract
Introduction
The climate crisis is essentially a public health crisis. Response is imperative to prevent economic and social crises associated with the growing burden of climate impacts on human health and the health care sector.
Green Podiatry Pillars
By adopting the three pillars of Exercise, Evidence, and Everyday changes, podiatrists can contribute to more sustainable health and health care.
Discussion
Educating our patients to use their feet for low carbon active transport, eliminating interventions not supported by evidence, and reducing fossil fuel driven supply chains and energy use, are three impactful measures that all podiatrists, and indeed, all health and medical personnel, need to adopt.
The avoidable suffering, enormous and costly use of resources for diabetic foot disease, is a scourge that must realise its preventable potential. It is too late, too costly, too polluting, and too sad, to continue to direct health care and research efforts and budgets, to an expensive modifiable diabetes disease process, potentiated by poor food and physical inactivity. Affected patients require skilled support, to avert such chronic disease processes, often not of their making.
Conclusions
Healthcare contributes 5 to 8% of green house gases (GHG), and non-communicable diseases (NCD) are increasing, so healthcare must lead on primary health. As citizens and health professionals, we must advocate for better community health, and educate our patients.
Future Directions
All health and medical personnel need to consider planetary health and sustainable healthcare within their daily work. Healthcare must act to address climate change, and realise benefits for people and planet.
Keywords:
green podiatry
; health
; climate emergency
; climate change
; healthcare
; greenhouse gases
; sustainability
; environment
1. Introduction
A recent Editorial, entitled ‘Climate risks laid bare’1, began with the headline statement from the latest Intergovernmental Panel on Climate Change (IPCC) report:
“It is unequivocal that human influence has warmed the atmosphere, ocean and land. Widespread and rapid changes in the atmosphere, ocean, cryosphere and biosphere have occurred.”
The IPCC places explicit emphasis on the interconnections between people, nature, and climate, viz. species extinctions, reducing tree canopy, ocean degradation, threatened biodiversity. The United Nations have called these findings, ‘a Code Red for humanity’, noting that climate change is widespread, rapid, and intensifying, and some trends are now irreversible. In 2019, atmospheric CO2 concentrations were assessed as greater than any time in the previous 2 million years, and concentrations of CH4 and N2O were higher than at any time in the last 800,000 years.
The IPCC report is grim reading, yet does provide hope, indicating that strong and sustained reductions of greenhouse gases, may improve air quality, and stabilise global temperatures within two or three decades.
We must all act, especially those who live in wealthy, high emission countries, and whose ‘industry’ is a large contributor to global emissions 2–4. Healthcare is a significant polluter, estimated to contribute 5% of carbon emissions globally5. This is surpassed in Australia5,6 and the US, where healthcare emissions are over 7%. In contrast, the UK’s NHS is on track to reduce healthcare emissions to net zero by 2040 for the emissions the NHS controls directly, and net zero by 2045 for the emissions the NHS can influence.
The Greenhouse Gas Protocol 7, provides the most widely recognised accounting standards for GHG emissions, and categorises GHG emissions into three ‘scopes’. Scope 1 covers direct emissions from controlled sources. Scope 2 covers indirect emissions from the purchase and use of energy as electricity, heating and cooling, hence there is responsibility for associated GHG emissions. Scope 3 includes all other indirect emissions that occur in the upstream and downstream activities (largely supply chains) of an organisation (Figure 1 and Figure 2). Healthcare’s footprint, can be identified within these scopes: direct in-clinic emissions, indirect in-clinic emissions, and external supply chains.
Clearly, action is urgent, and governments, all industry sectors, communities and individual citizens must act, if the Paris target to limit temperature rise to 1.5 °C is to be realised. All governments, and especially those of biggest emitter countries, need to strengthen Nationally Determined Contributions (NDCs) to reduce emissions. The Glasgow Climate Pact called on all countries to align with the Paris Agreement temperature goal.
Whilst a small group, podiatric medicine is a part of healthcare and contributes to GHG emissions through practice-associated activities, and has great opportunity to contribute positively in the ‘green healthcare’ space, as is already available4,8.
2. Green podiatry pillars
2.1. Exercise
The World Health Organisation global report on physical activity finds that regular physical activity promotes both mental and
physical health. Exercise and physical activity benefits everyone, regardless of age, ability, and sedentary lifestyle. The report found that 81% of adolescents and 27.5% of adults do not meet recommended levels of physical activity. The effects in insufficient physical activity are costly across an individual life span, costly for health services, and for the community. WHO’s Global Action Plan on Physical Activity 2018–2030 (GAPPA) aims for a 15% reduction in physical inactivity by 2030, and requires implementation by
governments.
The basic community health message is that ‘every move counts’, and WHO has produced recommended physical activity fact sheets for all ages9 (Table 1).
The national health priorities of Australia, and many countries, include all age groups, and prevalent conditions, eg cardiovascular disease, cancer, stroke, diabetes, arthritis, depression, musculoskeletal pain, obesity.
Sedentary time is an important and modifiable determinant of health, and a predictor of healthy ageing 10. Managing sedentary time is important for preventing both disease and disability and for managing existing conditions. Too much sitting is consequential for older adults, who are generally the least physically active of any age group, with some accumulating 10 hours sedentary time each day 10. The association with decreased physical activity, and costly falls, is well established in older people11. In the US, it has been reported that 1 in 5 falls causes a serious injury (fractures, head injury), with a cost estimate greater than $50 billion in 201512.
Walking is affordable, practical, and other than good feet, requires minimal equipment. Cycling moves people further and faster, and can transport bulkier items (panniers are great for shopping, children can ride in carriers), but requires more kit and cost. Active travel will involve (more) footwear, which takes 1000 years to breakdown at end of use. To avert old shoes from landfill, recycling plants adopt a circular economy, eg Treadlightly, Etiko. Whilst nowhere near the quantum of footwear, worn out foot orthoses are another landfill waste. A novel ‘green foot orthoses project’ is exploring options to recycle.
There is also a need to improve diet and physical activity habits to enhance mental and physical health outcomes in young people 13. Both diet and physical activity are frequently deficient in young people, yet regular physical activity is shown to improve mental health, by changing both the structure and neurobiological composition of the brain13. Ultra processed foods (UPF) are prevalent, addictive, and fuel diet-related diseases, including obesity, and related sequelae 1.
Lack of physical activity is a risk factor for premature death, along with smoking, and a poor diet 14. It is recommended that young adults engage in at least 60 minutes of moderate physical activity daily (or 150 minutes of vigorous physical activity weekly) 9. However, globally, approximately 30% of adults and 80% of adolescents have a lifestyle of physical inactivity and sedentary behaviour, especially in developed countries14.
2.2. Evidence
It has been established that overdiagnosis contributes a significant amount of clinical care that of is low value, wasteful, or harmful15. In essence, overdiagnosis is the detection of harmless conditions that could be safely left undiagnosed and untreated16,17.
Globally, the figures of overdiagnosis are startling, as every year: 500,000 people are overdiagnosed with thyroid cancer, 70,000 women in the US, and 4,000 in Australia may be overdiagnosed with breast cancer, and 8,000 Australian men are overdiagnosed with prostate cancer18. Diabetes is a systemic condition, with podiatric implications. ‘Pre-diabetes’ is usually diagnosed on the basis of an HbA1c level of 42–47 mmol/mol. Estimates show that 5 to10% of pre-diabetic patients have overt diabetes within a year, yet a similar percentage revert to normoglycaemia. Those with positive family history, certain ethnic groups, women with polycystic ovarian disease or prior gestational diabetes, have increased risk of frank diabetes 19. Similarly, prevailing views on the management of inflammatory rheumatic diseases may relate to overdiagnosis and overtreatment 20.
By definition, overdiagnosis generates carbon emissions without improving health18. Overdiagnosis also directs unnecessary testing and treatment. Given the health emergency caused by climate change, people will be needing healthcare for conditions related to air pollution, vector-borne diseases, and the increasing extreme weather effects of heat, floods, droughts, and food scarcities. Hence, together, overdiagnosis and climate change health needs, are a threat to sustainable healthcare provision everywhere.
Using evidence can reduce overdiagnosis and unnecessary treatments, and can help to cut healthcare’s carbon emissions, and simultaneously protect from the harms of too much medicine21,22. A further benefit will be cost reductions in healthcare budgets 18.
Examples of overdiagnosis in podiatry and general musculoskeletal areas include:
-customized/bespoke foot orthoses in children with flexible, asymptomatic flat feet23
-x-rays imaging for children with calcaneal apophysitis 24
-customized/bespoke foot orthoses for heel pain in adults 25
-arthroscopy for knee osteoarthritis 26
-spinal fusion surgery 27.
Given both the health consumer and planet perspectives, healthcare that is not evidence-based, and not necessary, results in avoidable emissions, that is of low value. All health and medical clinicians need to cease low and no value healthcare, and end this aspect of unnecessary and harmful healthcare emissions.
2.3. Everyday action
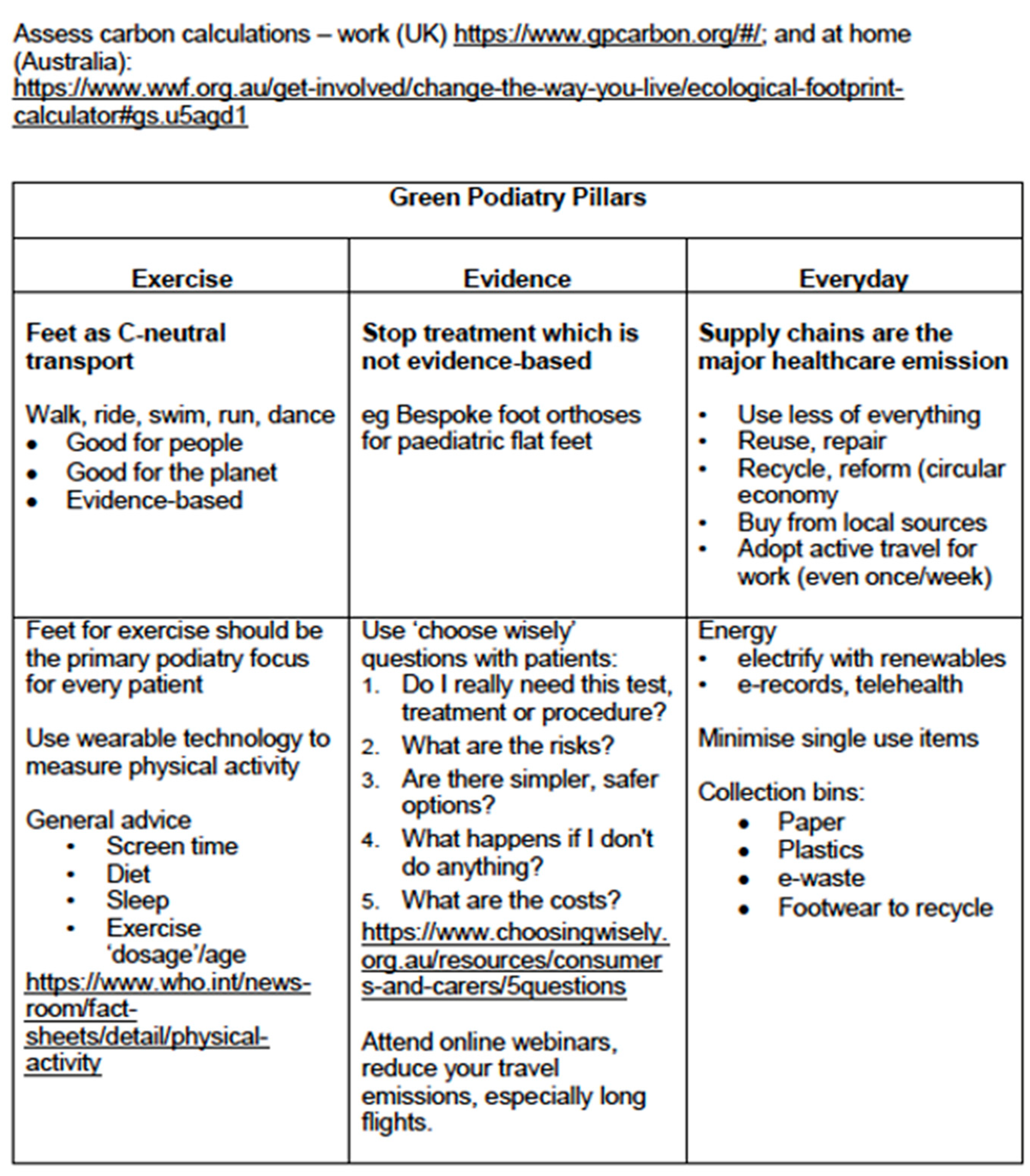
We need to act as citizens as well as health professionals. Table 2 summarises the three Green Podiatry pillars. Our everyday actions can contribute to environmental and social sustainability4,8,28.
Assessment of our own, and our workplace carbon footprint provides a relevant baseline. A free, publicly available Health Care Emissions Impact Calculator has been designed specifically for health care. Developed in line with the GHG Protocol, it enables health care organizations to develop a GHG inventory at the facility or system level for all scope 1, 2, and 3 emissions.
There are many easy checks that you can make, at work and at home. Green Podiatry – in the clinic
- Educate yourself – RCPSG course (https://rcpsg.ac.uk/ )
- Promote exercise, which is low carbon, good for health; healthy feet are basic for walking
- Use the evidence, and stop unnecessary intervention
- Use telehealth, especially for initial consultation interviews, progress reviews
- Talk about health and climate change with your patients (Supplementary file)
- Address supply chains – use less, buy locally
- Review energy – use less, use renewable energy
- Footwear – consider what is ethical, sustainably produced; consider repairing, recycling old shoes, stay abreast of possible recycling of foot orthoses (green foot orthoses)
Living Green - outside the clinic
- Use less of everything
- Electrify everything, turn off gas as soon as you can
- Read labels to avoid ultra-processed food (UPF), adopt a plant-based diet (even partially, and grow what you can)
- Divest from fossil fuel companies (check your superannuation)
- Increase your active transport (walk, cycle), plan for electric car
- Vote ‘green’
3. Discussion
As health professionals we are mandated to prevent and relieve illness and disease, yet as a sector, ’health’ makes a significant contribution to the climate emergency, with at least 5% of global greenhouse gas emissions derived from the healthcare sector.
Emissions are generated from service delivery to the natural resources and products consumed by health care systems, to the substantial waste generated. At the heart, are fossil fuel driven supply chains and energy production (coal, oil, gas), which drive climate change, chemical contamination, resource depletion, loss of biodiversity, poor air and water quality.
Given health is a contributor to the climate emergency, health care providers need to be conscientious about contributing to a solution.
The World Health Organisation’s strategic document, identifies nine main actions on environmental sustainability specific to health systems.
- Adopting: Adopting a national environmental sustainability policy for health systems
- Minimising: Minimising and adequately managing waste and hazardous chemicals
- Promoting: Promoting an efficient management of resources and sustainable procurement
- Reducing: Reducing health systems’ emissions of greenhouse gases and air pollution
- Prioritising: Prioritising disease prevention, health promotion and public health services
- Engaging: Engaging the allied health workforce as an agent of sustainability
- Increasing: Increasing community resilience and promoting local assets
- Creating: Creating incentives for change
- Promoting: Promoting innovative models of care.
The UK’s NHS Green Plan (Greener NHS (england.nhs.uk)) commenced in 2020, with the NHS becoming the first health service globally, to commit to carbon net zero, in response to the threat to health from climate change.
Delivering a Net Zero Health Service is a very ambitious report which aims to build a greener NHS. The Public Sector Decarbonisation Scheme( gov.uk website ) funds public sector organisations, including NHS hospitals, to invest in low-carbon heating and energy innovations viz. heat pumps, LED lighting, building fabric improvements, and renewable energy sources. The aim is to achieve the UK’s carbon reduction targets, while reducing energy costs and supporting energy resilience.
3.1. Putting health before healthcare to prevent diabetes
As podiatrists, we need to return the ‘horse to the front of the cart’, regarding the increasing scourge of diabetic foot disease. Diabetic foot ulcers (DFU) are a costly and preventable complication in adults with longstanding and poorly managed diabetes. The epidemiology is staggering. World figures approximate 540 million people with diabetes, of whom, 19% to 34% will suffer a DFU. Further, 20% of those with a DFU require lower-extremity amputation, and 10% die within one year of initial DFU. Estimates find an overall increase in amputations by up to 50% in some regions 29.
Yet, diabetes is reportedly preventable, by addressing obesity and physically inactive lifestyle. A clear public health message from Harvard’s TH Chan School of Public Health, expounds a straight forward and simple approach:
“Keeping weight in check, being active, and eating a healthy diet can help prevent most cases of type 2 diabetes.”
Given the preventable nature of diabetes, why do we, as health providers, seemingly bypass the public health message of prevention to spend enormous time and resources to address avoidable and costly complications, and inestimable suffering. Diabetes, like the climate crisis, is a public health crisis.
The traditional complications associated with diabetes mellitus have included: macrovascular conditions (eg coronary heart disease, stroke, peripheral arterial disease), microvascular conditions (eg diabetic kidney disease, retinopathy) and peripheral neuropathy 30.
Due to improved management of diabetes mellitus, rates of traditional complications have declined. However, as people (with diabetes mellitus) live to greater age, they are found susceptible to other complications. Cancer has become the main cause of death in people with diabetes mellitus in some regions and deaths due to dementia has also risen. In England, traditional complications directed 50% of hospitalizations in people with diabetes mellitus in 2003, but in 2018 just 30% 30.
3.2. Averting costly diabetic feet
Diabetes increases the incidence of foot ulcer admissions by 11-times, accounting for more than 80% of all amputations and increasing hospital costs more than 10-times 31. The majority of costs are related to the treatment of infected foot ulcers 31. Further, diabetes accounted for 83% of major and 96% of minor amputations related to a foot ulcer, significantly increasing cost of care (DM: $1.38 vs. non-DM: $0.13 billion/year). Hospital costs per foot ulcer admission were significantly higher for patients with infection compared with all other causes ($11,290 vs. $8,145). Education initiatives and early prevention strategies targeted at high-risk populations are essential to preventing further increases in an already substantial economic burden 31.
Five-year mortality for DFU, and amputations were 30%, 46% to 56%, respectively. This is compared to 9% for breast cancer and 80% for lung cancer. Same period mortality for all cancer was 31%. Direct costs of general care for diabetes was US$237 billion in 2017. This is compared to US$80 billion for cancer in 2015. It is notable, that one-third of costs for diabetes can be attributed to the leg and foot32. Diabetic lower extremity complications are extremely burdensome. Most notably, foot ulcers and leg/foot amputations appear to be risk factors for premature death. While advances continue to improve outcomes of care for people with foot ulcers and amputation, efforts should be directed at primary prevention32.
4. Conclusions
Given that healthcare contributes 5 - 8% of GHGs, and that NCD like diabetes are increasing, healthcare must re-focus and lead on primary health.
As citizens as well as health professionals, we must advocate for better community health. We can take a ‘green L.E.A.P.’28 to educate ourselves and our patients about ‘big picture’ health. This is especially important for younger colleagues, to allay eco-anxiety33
- Green prescribing34 doses exercise and time in the natural world, is low cost and essential for primary health.
- In the clinic, push back on single use instruments35, adopt renewable and lower energy usage, ‘choose wisely’ and stop unnecessary treatment which drops supply chain emissions.
- Be active yourself, reduce your screen use, avoid UPF foods, and sleep well.
- Partner with existing organisations like Parkrun, advocate for free coffee for regular participants.
- Stop advertising junk foods to children. Australia’s Climate Council has encouraged organisations to remove fossil fuel sponsoring from sports and arts events.
- Avail all housing access to gardens, solar power, rainwater tanks, insulation, electrify everything, and turn off the gas (methane is 25 times more potent than CO2).
- Cycling lanes that are separate and safe – we need political will, rewards, and champions
4.1. Future Directions
All health and medical personnel need to consider planetary health and sustainable healthcare within their daily work. We cannot lead healthy human lives if we live on a sick planet. The healthcare sector must act to help address climate change, and realise the benefits for both people and planet health.
Curriculums to educate undergraduate health and medical students in training are essential (https://rcpsg.ac.uk/ ), and professional development requires a climate lens, as does patient education. We need to ask every patient about their daily physical activity and sedentary behaviours9, promote active travel for health, and patient reviews with telehealth.
At the heart of the climate emergency is fossil fuel dependence, which not only undermines planet health through increased climate change impacts, but also affects human health and wellbeing directly, through unpredictable fossil fuel markets, weak supply chains, and rising geopolitical conflict 36.
Imagine a world, cleaner, greener, and probably leaner, which is poised for sustaining biodiversity of all life for our youngest and future global citizens.
Clear and strategic use, of diverse knowledge and skills, must be cooperative to minimize the threats and maximize the health opportunities of climate action, and navigate a hopeful way forward.
Supplementary Materials
Included as ‘Supplementary File’
- Initiated ‘Green Podiatry’ and has associated publications
- Member of the Sustainability Steering Group - RCPS Glasgow
- Authored Teaching and Learning modules for ‘Green Podiatric Medicine’ – RCPS Glasgow, 2023
- Chair, Sustainability Panel – APodA conference, 2021
- Green foot orthoses project – UNSW SM@RT, APodA collaboration
Author Contributions
AE conceived, drafted, checked final copy, and submitted this manuscript.
Funding
None received.
Acknowledgments
Disclaimer: I am not a climate change expert, but an engaged earth-dweller, envisaging a podiatry (and whole of health care) community which can act to avert climate change, to better the health of our planet, and ourselves.
Conflicts of Interest
| 1 | Chris van Tulleken, Ultra-processed people, Why we all eat stuff that isn’t food…and why we can’t stop? Cornerstone Press, 27 May, 2023. ISBN-13 978-1529900057. |
References
- Health TLP. Climate risks laid bare. Lancet Planet Heal 2022, 6, e292. [Google Scholar] [CrossRef] [PubMed]
- Spruell T, Webb H, Steley Z, Chan J, Robertson A. Environmentally sustainable emergency medicine. Emerg Med J 2021, 38, 315–318. [Google Scholar] [CrossRef] [PubMed]
- Allwright E, Abbott RA. Environmentally sustainable dermatology. Clin Exp Dermatol 2021, 46, 807–813. [Google Scholar] [CrossRef] [PubMed]
- Evans, AM. Sustainable healthcare – Time for ‘Green Podiatry. ’ J Foot Ankle Res 2021, 14, 45. [Google Scholar] [CrossRef]
- Lenzen M, Malik A, Li M, Fry J, Weisz H, Pichler P-P et al. The environmental footprint of health care: a global assessment. Lancet Planet Heal 2020, 4, e271–e279. [Google Scholar] [CrossRef]
- Malik A, Lenzen M, McAlister S, McGain F. The carbon footprint of Australian health care. Lancet Planet Heal 2018, 2, e27–e35. [Google Scholar] [CrossRef]
- Awanthi MGG, Navaratne CM. Carbon Footprint of an Organization: a Tool for Monitoring Impacts on Global Warming. Procedia Eng 2018, 212, 729–735. [Google Scholar] [CrossRef]
- Evans, AM. ‘Green podiatry’ - reducing our carbon footprints. Lessons from a sustainability panel. J Foot Ankle Res 2021, 14, 59. [Google Scholar] [CrossRef]
- Bull FC, Al-Ansari SS, Biddle S, Borodulin K, Buman MP, Cardon G et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Brit J Sport Med 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Dogra S, Ashe MC, Biddle SJH, Brown WJ, Buman MP, Chastin S et al. Sedentary time in older men and women: an international consensus statement and research priorities. Brit J Sport Med 2017, 51, 1526–1532. [Google Scholar] [CrossRef]
- Gameren M van, Hoogendijk EO, Schoor NM van, Bossen D, Visser B, Bosmans JE et al. Physical activity as a risk or protective factor for falls and fall-related fractures in non-frail and frail older adults: a longitudinal study. Bmc Geriatr 2022, 22, 695. [Google Scholar]
- Park C, Atique MMU, Mishra R, Najafi B. Association between Fall History and Gait, Balance, Physical Activity, Depression, Fear of Falling, and Motor Capacity: A 6-Month Follow-Up Study. Int J Environ Res Pu 2022, 19, 10785. [Google Scholar] [CrossRef] [PubMed]
- Mawer T, Kent K, Williams AD, McGowan CJ, Murray S, Bird M-L et al. The knowledge, barriers and opportunities to improve nutrition and physical activity amongst young people attending an Australian youth mental health service: a mixed-methods study. Bmc Health Serv Res 2022, 22, 789. [Google Scholar]
- Granero-Jiménez J, López-Rodríguez MM, Dobarrio-Sanz I, Cortés-Rodríguez AE. Influence of Physical Exercise on Psychological Well-Being of Young Adults: A Quantitative Study. Int J Environ Res Pu 2022, 19, 4282. [Google Scholar] [CrossRef]
- Moynihan R, Doust J, Henry D. Preventing overdiagnosis: how to stop harming the healthy. BMJ 2012, 344, e3502–e3502. [Google Scholar] [CrossRef]
- Hofmann, B. Back to Basics: Overdiagnosis Is About Unwarranted Diagnosis. Am J Epidemiol 2019, 188, 1812–1817. [Google Scholar] [CrossRef]
- Kale MS, Korenstein D. Overdiagnosis in primary care: framing the problem and finding solutions. Bmj Clin Res Ed 2018, 362, k2820. [Google Scholar]
- Barratt A, McGain F. Overdiagnosis is increasing the carbon footprint of healthcare. Bmj 2021, 375, n2407. [Google Scholar]
- Twohig H, Hodges V, Mitchell C. Pre-diabetes: opportunity or overdiagnosis? Br J Gen Pr 2018, 68, 172–173. [Google Scholar] [CrossRef]
- Landewé RBM. Overdiagnosis and overtreatment in rheumatology: a little caution is in order. Ann Rheum Dis 2018, 77, 1394. [Google Scholar] [CrossRef]
- Abbasi, K. A system reset for the campaign against too much medicine. Bmj 2022, o1466. [Google Scholar] [CrossRef]
- Pathirana T, Clark J, Moynihan R. Mapping the drivers of overdiagnosis to potential solutions. Bmj 2017, 358, j3879. [Google Scholar]
- Evans AM, Rome K, Carroll M, Hawke F. Foot orthoses for treating paediatric flat feet. Cochrane Db Syst Rev 2022, 2022, 2022, CD006311. [Google Scholar]
- Launay, F. Sports-related overuse injuries in children. Orthopaedics & traumatology, surgery & research : OTSR 2015, 101, S139–S147. [Google Scholar]
- Redmond AC, Landorf KB, Keenan A-M. Contoured, prefabricated foot orthoses demonstrate comparable mechanical properties to contoured, customised foot orthoses: a plantar pressure study. Journal of foot and ankle research 2009, 2, 20. [Google Scholar] [CrossRef] [PubMed]
- Brignardello-Petersen R, Guyatt GH, Buchbinder R, Poolman RW, Schandelmaier S, Chang Y et al. Knee arthroscopy versus conservative management in patients with degenerative knee disease: a systematic review. Bmj Open 2017, 7, e016114. [Google Scholar] [CrossRef]
- Maher CG, O’Keeffe M, Buchbinder R, Harris IA. Musculoskeletal healthcare: Have we over-egged the pudding? Int J Rheum Dis 2019, 22, 1957–1960. [Google Scholar] [CrossRef] [PubMed]
- Evans, AM. Incorporating ‘Green Podiatry’ into your clinic, and into your life. J Foot Ankle Res 2022, 15, 87. [Google Scholar] [CrossRef] [PubMed]
- McDermott K, Fang M, Boulton AJM, Selvin E, Hicks CW. Etiology, Epidemiology, and Disparities in the Burden of Diabetic Foot Ulcers. Diabetes Care 2022, 46, 209–221. [Google Scholar]
- Tomic D, Shaw JE, Magliano DJ. The burden and risks of emerging complications of diabetes mellitus. Nat Rev Endocrinol 2022, 18, 525–539. [Google Scholar] [CrossRef]
- Hicks CW, Selvarajah S, Mathioudakis N, Sherman RL, Hines KF, Black JH et al. Burden of Infected Diabetic Foot Ulcers on Hospital Admissions and Costs. Ann Vasc Surg 2016, 33, 149–158. [Google Scholar] [CrossRef] [PubMed]
- Armstrong DG, Swerdlow MA, Armstrong AA, Conte MS, Padula WV, Bus SA. Five year mortality and direct costs of care for people with diabetic foot complications are comparable to cancer. J Foot Ankle Res 2020, 13, 16. [Google Scholar] [CrossRef] [PubMed]
- Gunasiri H, Wang Y, Watkins E-M, Capetola T, Henderson-Wilson C, Patrick R. Hope, Coping and Eco-Anxiety: Young People’s Mental Health in a Climate-Impacted Australia. Int J Environ Res Pu 2022, 19, 5528. [Google Scholar] [CrossRef] [PubMed]
- Robinson JM, Jorgensen A, Cameron R, Brindley P. Let Nature Be Thy Medicine: A Socioecological Exploration of Green Prescribing in the UK. Int J Environ Res Public Heal 2020, 17, 3460. [Google Scholar] [CrossRef] [PubMed]
- Pegna V, McNally SA. Are single use items the biggest scam of the century? Bulletin Royal Coll Surg Engl 2021, 103, 233–235. [Google Scholar] [CrossRef]
- Romanello M, Napoli CD, Drummond P, Green C, Kennard H, Lampard P et al. The 2022 report of the Lancet Countdown on health and climate change: health at the mercy of fossil fuels. Lancet 2022, 400, 1619–1654. [Google Scholar] [CrossRef]
Figure 1.
GHG emissions are identified within 3 scopes, generally, and for healthcare.
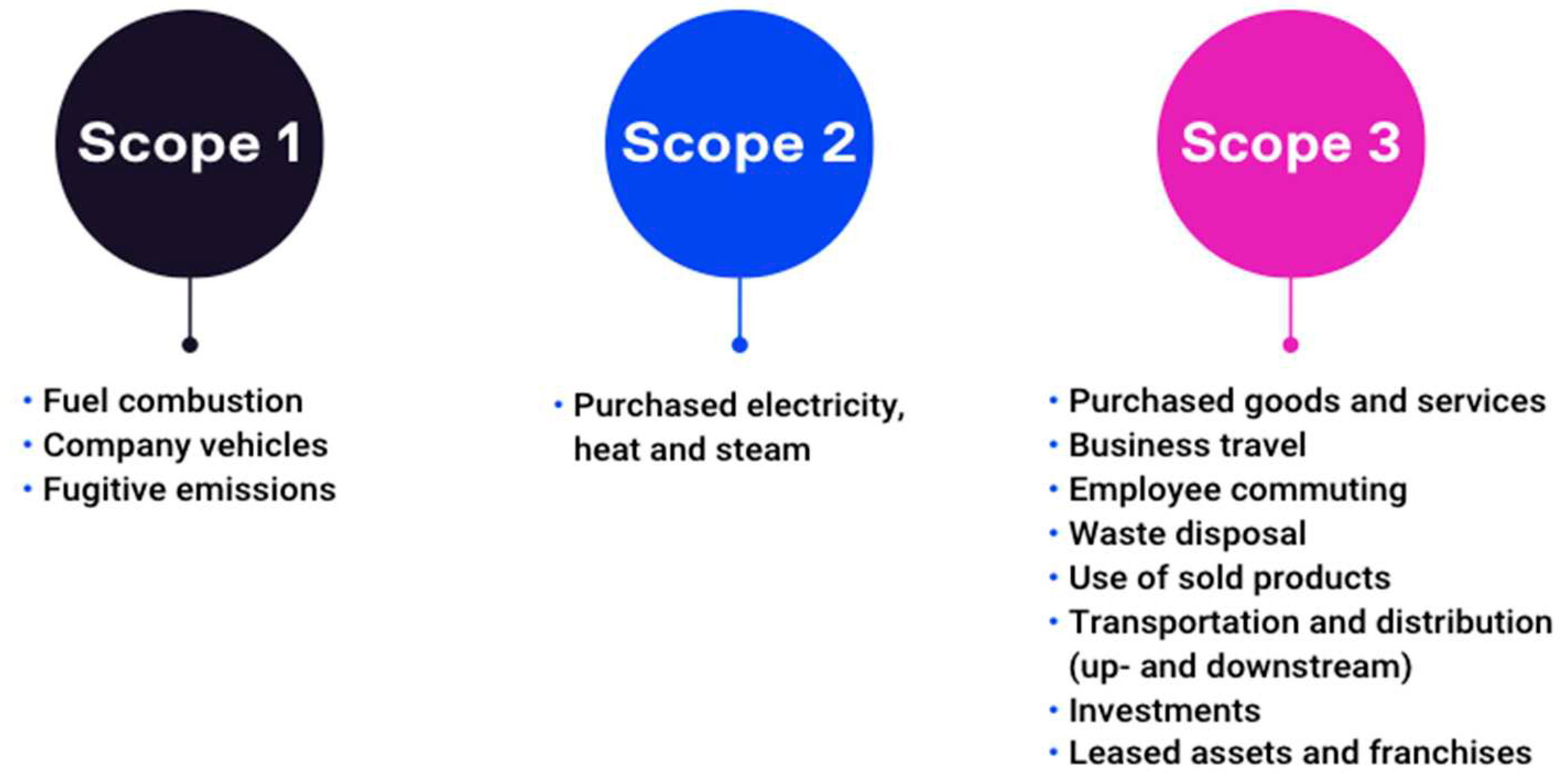
Figure 2.
The global health care footprint split according to GHGP Scopes. Scope 1: emissions directly from health care facilities; Scope 2: indirect emissions from purchasing energy supplies; Scope 3: fossil fuel driven supply chains used to stock clinics (production, transport, use, and disposal of goods and services that health care facility consumes). Note that across the three scopes, more than 50% of the health sector footprint is energy use (mainly electricity, gas, steam, air conditioning, combined with other operational emissions).
Figure 2.
The global health care footprint split according to GHGP Scopes. Scope 1: emissions directly from health care facilities; Scope 2: indirect emissions from purchasing energy supplies; Scope 3: fossil fuel driven supply chains used to stock clinics (production, transport, use, and disposal of goods and services that health care facility consumes). Note that across the three scopes, more than 50% of the health sector footprint is energy use (mainly electricity, gas, steam, air conditioning, combined with other operational emissions).
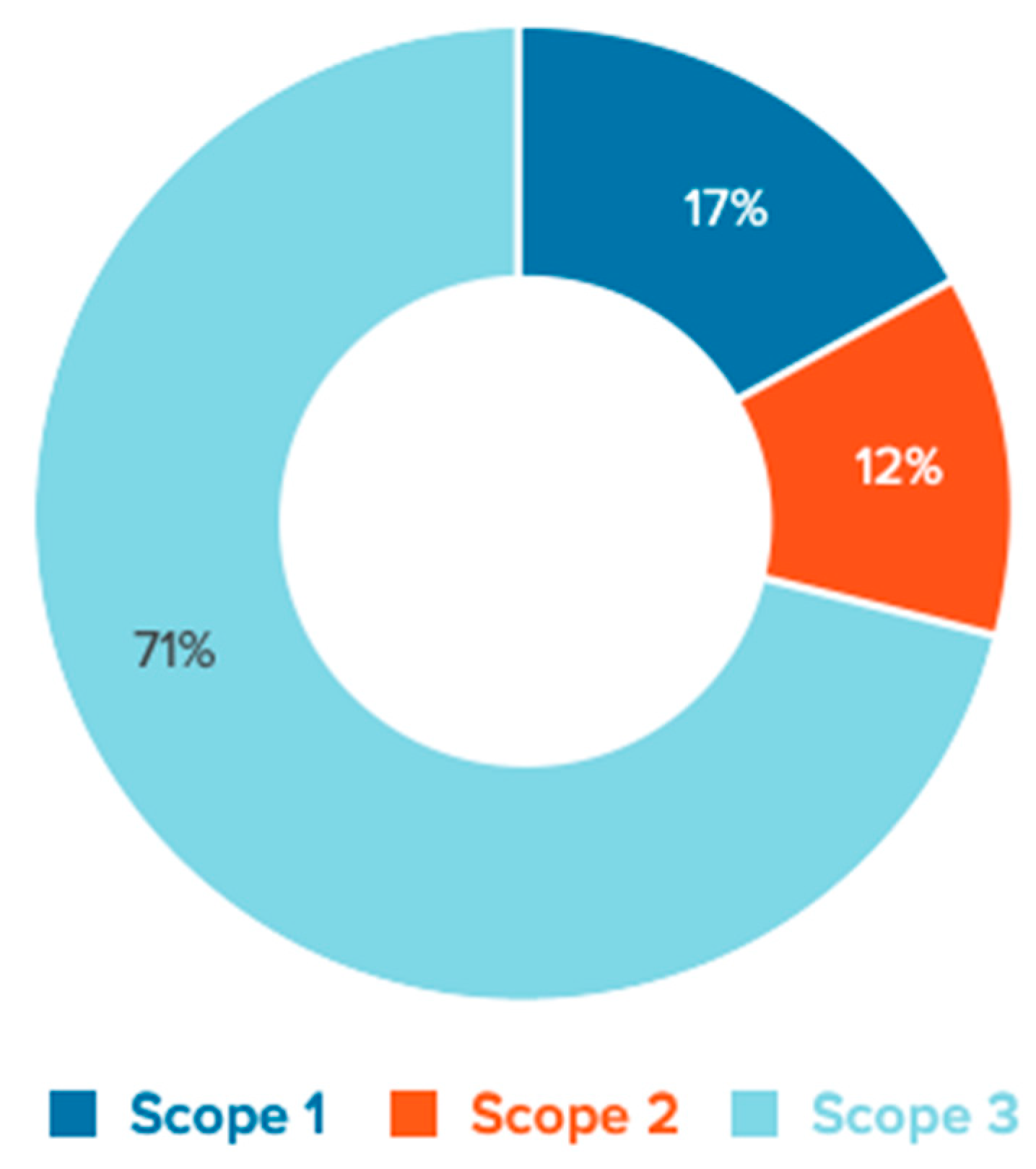

Table 1.
Summary of WHO guidelines and recommendations for physical activity.
| Age (years) | Baseline | Intensity | Sedentary | Screen time | Sleep hours (age) ** |
|---|---|---|---|---|---|
| Recommended physical activity/ 24 hours | |||||
| < 1 | Floor play several times daily | Include 30 minutes tummy time across the day | Restrained in car seat etc, less than 1 hour at a time | No screens; interactive reading and play | 14 to 17 (<3 mths), 2 to 16 (4 to 11 mths) of good quality sleep, including naps. |
| 1 to 2 | at least 180 minutes of varied PA across the day; more is better | Include some moderate- to vigorous-intensity PA | Restrained in car seat etc, less than 1 hour at a time; limit extended sitting | Age 1 year, sedentary screens not recommended. age 2 years, maximum 1 hour; less is better |
11 to 14 of good quality sleep, including naps; regular sleep times. |
| 3 to 4 | at least 180 minutes of varied PA across the day; more is better | at least 60 minutes is moderate- to vigorous-intensity | Restrained less than 1 hour at a time; limit extended sitting | Sedentary screen time of no more than 1 hour; less is better. | 10 to 13h of good quality sleep; may include a nap; regular sleep times. |
| 5 to 17 | at least 60 minutes of moderate-to-vigorous intensity, mostly aerobic PA | Include vigorous aerobic PA; add strengthening for muscle and bone, at least 3/week | limit | limit | |
| Recommended PA per week | |||||
| 18 to 64 | at least 150–300 minutes moderate-intensity aerobic PA |
OR at least 75–150 minutes vigorous-intensity aerobic PA |
Limit; Twice or more muscle-strengthening activities at moderate or greater intensity |
limit | |
| > 65 | As for younger adults; older adults should do varied multicomponent physical activity that emphasizes functional balance and strength training at moderate or greater intensity, on 3 or more days a week, to enhance functional capacity and to prevent falls. |
||||
| Pregnant, postpartum (without contraindication) |
at least 150 minutes of moderate-intensity aerobic PA | include aerobic and muscle-strengthening PA | limit | ||
| Chronic NCD * | at least 150–300 minutes of moderate-intensity | at least 75–150 minutes of vigorous-intensity aerobic PA | Limit; Twice or more muscle-strengthening at moderate or greater intensity |
||
| People with disability | |||||
| Children and adolescents | at least an average of 60 minutes per day of moderate-to-vigorous intensity PA | vigorous-intensity aerobic PA, as well as those that strengthen muscle and bone, at least 3 days a week | limit | limit | |
| Adults | at least 150–300 minutes of moderate-intensity aerobic PA | OR at least 75–150 minutes of vigorous-intensity aerobic PA |
Limit; Twice or more muscle-strengthening at moderate or greater intensity |
Limit; replace with light intensity PA | |
*NCD – noncommunicable disease, eg obesity, hypertension, type 2 diabetes, HIV, cancer survivor; **Sleep, sedentary behaviour guidelines applicable to children up to age 5 years.
Table 2.
The three pillars of Green Podiatry for clinicians2..8.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



