Submitted:
12 September 2023
Posted:
13 September 2023
You are already at the latest version
Abstract
Malignant neoplasms arising from the gastrointestinal (GI) tract are among the most common cancer types with a high mortality rate. Despite advances in treatment in a small subgroup harboring targetable mutations, the outcome remains poor, accounting for one in three cancer-related deaths observed globally. As a promising therapeutic option in various tumor types, immunotherapy with immune checkpoint inhibitors has also been evaluated in GI cancer, albeit with limited efficacy except for a small subgroup expressing microsatellite instability. In the quest for more effective treatment options, energetic efforts have been placed to evaluate the role of several immunotherapy approaches comprising of cancer vaccines, adoptive cell therapies and immune checkpoint inhibitors. In this review, we report our experience with personalized dendritic cell cancer vaccine and cytokine-induced killer cell therapy in three patients with GI cancers and summarize current clinical data on combined immunotherapy strategies.
Keywords:
gastrointestinal cancer
; immunotherapy
; cancer vaccines
; dendritic cell vaccine
; adoptive cell treatment
; cytokine-induced killer cells
; immune checkpoint inhibitors
; angiogenesis inhibition
Introductıon
Despite improvements in screening and treatment, gastrointestinal (GI) tract cancers are a major contributor to the global cancer burden. According to the Globocan statistics, with 3,574,000 new cases, the incidence of esophageal, gastric and colorectal cancers (CRC) represents 19.7% of all cancers diagnosed in 2020, leading to 22.5% of all cancer-related deaths (1). In the US, with 213000 new cases and 85000 deaths projected for 2023, GI cancers rank 3rd in incidence and mortality among all sites diagnosed with cancer. Although 5-year survival rates have been improved for all stages combined in both colorectal (CRC) and gastric cancers, with mortality rates steadily decreasing over the last decade; but need to be improved for both tumor types as GI-related cancer deaths comprise about 13.7% of all cancer deaths and an annual rise in mortality by 1% is noted among young adults with CRC (2,3).
With the advent of modern immunotherapy, a new era of cancer therapy has been initialized. Markedly improved survival rates have been achieved with immune checkpoint inhibitors for several cancer types, which had otherwise been considered the most lethal of all cancer types. Programmed-death ligand-1 (PD-1) inhibitors, namely nivolumab and pembrolizumab have been approved for the upfront treatment of advanced esophagogastric cancers combined with chemotherapy based on the significantly improved survival rates with hazard ratios (HR) ranging between 0.71 and 0.74 (4,5). Furthermore, monotherapy with immune checkpoint inhibitors has yielded favorable response rates and prolonged survival rates in microsatellite instable /mismatch repair deficient cancers as compared to standard chemotherapy, earning a rightful designation of “the game-changer treatment” even in heavily pretreated groups. (6-10). Nevertheless, accumulating data have shown that the majority of patients still succumb to their disease, indicating a requirement for novel approaches to overcome resistance.
Immunosuppressive microenvironment (TME), inadequate effector immune response and function of cancer-specific cytolytic CD8 (+) T cells, inefficient antigen presentation as well as epigenetic modifications that control immune regulation are major mechanisms that are implicated in acquired resistance to immune-mediated cell killing (11). Addressing some of these tumor-escape pathways, cancer vaccines and adoptive transfer of T cells combined with chemotherapy, anti-angiogenic agents and radiotherapy have been established as complementary methods to induce an effective anti-cancer immune response (12).
In this review, we will discuss the role of immunotherapy in GI tract cancers based on our experience with combined strategies and place this in context with emerging evidence from clinical trials. We hope that this overview will provide insight into comprehensive immunotherapy approaches not only for GI cancers, but for all cancer types where immune-associated cell killing is warranted.
II. Cancer immunology and immunotherapy
The immune system is comprised of myeloid cells such as lymphocytes and macrophages that are differentiated to generate an immune response when encountered with foreign appearing structures in the host, including cancerous cells. When tumor cells are identified by the innate immune system, cellular fragments or foreign antigens from these cells are internalized by the antigen-presenting cells (APC), such as dendritic cells or macrophages, which are the main components of the immune system that are responsible for antigen cross-presentation to prime specific B and T cell responses (13).
Dendritic cells are the most potent antigen-presenting cells in the human immune system. Dendritic cells, which can activate naive T cells against various host attacks, including cancer, belong to the mononuclear phagocyte system and are professional antigen-presenting cells (14). First discovered by Paul Langerhans in 1868, dendritic cells were named after cells that exhibited long cytoplasmic processes in the mouse spleen in 1973. Various subsets of dendritic cells originate from a unique hematopoietic lineage in the bone marrow (15,16). In addition to the activation of innate immunity, it plays an important role in the stimulation of cytotoxic T lymphocyte-mediated acquired immunity. Immature forms of dendritic cells circulate widely in the blood and peripheral tissues, where they contain pathogen-infected or tumor cell-derived antigens. After antigen uptake, immature dendritic cells undergo phenotypic and functional maturation. They migrate to secondary lymphoid organs and tissues, such as lymph nodes, presenting processed antigens and activating cytotoxic T lymphocytes (15-17). Thus, mature dendritic cells trigger an antigen-specific immune response to eliminate the antigen-expressing target cells. In addition, mature dendritic cells can increase the cytotoxic activity of NK cells, which, like immature dendritic cells, act as innate immune effector cells to destroy pathogen-infected or tumor cells (18).
Like other leukocytes, dendritic cells develop from bone marrow-derived hematopoietic stem cells (CD34 + active) and differentiate from common myeloid progenitors. However, a small fraction of dendritic cells may arise from common lymphoid progenitor cells (19). In the downregulation of common myeloid progenitors, macrophage/dendritic cell progenitor cells serve to provide the host with a constant source of monocytes, macrophages, and classical dendritic cells. Specifically for dendritic cell development, macrophage/dendritic cell progenitors give rise to common dendritic cell progenitor cells that expand into progenitor dendritic cells. These cells migrate to lymphoid and non-lymphoid organs to mature further into functional dendritic cell subtypes based on intrinsic and/or extrinsic factors (20, 21). When dendritic cells are found in peripheral tissues, they represent the surrounding environment via receptor-mediated phagocytosis or macro-pinocytosis (21, 22). Following antigen uptake, dendritic cells respond to the chemokines CCL19 secreted by mature dendritic cells or CCL21 as lymphatic vessel-derived endothelial cells and migrate to draining lymph nodes, via upregulation of CCR7 (23, 24). During antigenic transfer, dendritic cells assume a phenotype of mature antigen-presenting cells marked by increased expression of surface molecules, such as major tissue compatibility complex class II (MHC-II) and CD80/CD86. The dendritic cells then bind and present the transduced antigen to the T cells in the lymph node paracortex via the MHC. This provides the necessary co-stimulation and cytokine support for T-cell activation and proliferation (18, 23).
Once antigens are processed and loaded onto MHC I and II molecules, APC’s interact with the microenvironment to present the neoantigen to cytotoxic T cells and B cells, respectively, which are subsequently activated to develop an antigen-specific immune response [13,25]. Nevertheless, during tumor progression, the anti-cancer immunologic activity may be restricted by the upregulation of various checkpoints and immune-suppressive elements of the host immune system, which is inherently programmed to balance any excessive immune activity against the host. It has been shown that recently identified inhibitory immune checkpoints such as LAG-3, TIGIT and IDO control immune activity by suppressing tumor-specific T and B lymphocytes, resulting in a shift towards generation of an immune-suppressive stroma comprised of regulatory T cells (Treg), immature dendritic cells, M2 macrophages and myeloid-derived suppressor cells (MDSC) [26]. It has been shown that cancer cells interact with the host immune system to overcome anti-tumor immunity by switching the tumor microenvironment to an immuno-suppressive or immune-cold phenotype mediated by several cytokines and molecules [26-28].
Immunotherapy refers to various treatment strategies that aim to restore a dysregulated immune function or to modulate the host immune system to generate an adequate immune-mediated anti-tumor response. The current immunotherapy approaches address several mechanisms that hamper generation of a sufficient immune response for immune-mediated cell killing. Immune checkpoint inhibitors are monoclonal antibodies that aim to release the brakes on immune cells by blockade of PD-1, PD-L1 or CTLA receptors. As mentioned above, nivolumab and pembrolizumab are PD-1 inhibitors that have been approved for the treatment of gastric and CRC for various indications. Other investigational approaches for immunotherapy target the immune system to generate a cancer-specific response by cancer vaccines or to administer ex-vivo activated autologous or allogeneic immune cells that target cancer cells, such as tumor-associated lymphocytes (TIL), CAR-T cells or engineered NK cells, otherwise referred to as adoptive cell therapy [29-34]. Detailed information on these strategies will be provided in context with current evidence in GI immunotherapy in the corresponding sections below.
III. Immunotherapy in GI cancers: Cellular treatment systems
a. Cancer vaccines: rationale, limitations and potential combinations
The history of immunization for cancer therapy dates back to 1890, when Sir William Coley treated cancer patients with streptococcal bacterial cultures and reported tumor regressions (35). Since then, enormous efforts have been placed to design an efficient system, which would stimulate the host immune system to elicit an adequate and specific immune response against cancer cells. Biologic systems that aim to prime T and B lymphocytes by introducing tumor neoantigens via distinct delivery systems are called cancer vaccines. The neoantigens are provided as inactivated whole tumor cells or components of cells that convey specific characteristics, such as nucleic acids or peptides, which lead to the recognition of the cancer cells by effector lymphocytes of the host immune system. These antigens are delivered through several systems including dendritic cells, viral particles, exosomes, or synthetic systems such as lipid and polymer-based nanoparticles. As an active immunotherapy strategy, the goal of treatment with cancer vaccines is not only to induce a cancer-specific response, but also to establish immunologic memory for a sustained and prolonged immune-mediated cell-killing effect (36-38). Despite the enthusiasm generated over immunotherapy in the past century, the clinical efficacy of cancer vaccines has been underwhelming except for Spileucel-T, an autologous tumor cell-based vaccine, which was approved for routine clinical use based on overall survival advantage for patients with castration-resistant prostate cancer and Talimogene Laherperepvec for malignant melanoma based on efficacy to elicit durable tumor responses in remote lesions (39-41).
Dendritic cell vaccines
Human dendritic cell subsets loaded with tumor-associated antigens, referred to as dendritic cell vaccines have emerged as a promising immunotherapeutic tool for the treatment of many cancer types, including colorectal cancer, breast cancer, and hepatocellular carcinoma (42-44). The mainstay of designing dendritic cell vaccines is the development of an effective and durable cytotoxic T-lymphocyte immune response by inducing both humoral and cellular immune responses that, together with the immune capacities of dendritic cells, induce the clonal expansion of T cells (45). Once activated, dendritic cells have the capability to migrate to the nearest lymph nodes, which is required to initiate immunologic mechanisms leading to the generation of humoral and cellular immune responses against tumors (46, 47). Generally, vaccine production involves isolation of immature dendritic cells or precursors from the blood, followed by ex vivo maturation and activation through co-culturing with cytokine cocktails. The generated mature dendritic cells are then pulsed with autologous tumor cells or neoantigens to form dendritic vaccines which are administered back to the patient (48). Encouraging preclinical data on the anti-tumor efficacy of dendritic cells packed with tumor lysates led to intensive clinical evaluation of dendritic vaccines by the end of the last century (49). Subsequent clinical trials utilizing antigen-specific dendritic cells showed partial responses coupled with anti-tumor immune responses in several tumor types including B-cell lymphoma, melanoma and hepatocellular carcinoma (50-53).
Cancer vaccines and combined strategies to improve immunogenic activity in GI cancers
Nevertheless, cancer vaccines against pre-identified tumor neoantigens in CRC have shown limited efficacy, as the “cold” tumor microenvironment (TME) has precluded the generation of an adequate specific cytotoxic T cell response. Therefore, energetic efforts are being placed to overcome the immunosuppressive TME and turn “cold” tumors into “hot” tumors, where an effective immune-mediated response can be triggered through activation of CD8 (+) T cells, Th1 B cells as well as inhibition of Tregs, tumor-associated macrophages (TAM’s) and proinflammatory signals such as TNF-alpha. Among many strategies, activating cytokine adjuvants used along with vaccines have shown enhanced tumor-specific immune responses. In a murine model with CRC, GM-CSF and IL-2 combination with a vaccine targeting WNT as a neoantigen, has yielded an augmented T cell response which translated into an effective tumor cell killing (54). Despite discrepant effects of interleukins in the ability to induce both pro-inflammatory and anti-inflammatory responses in the TME, pretreatment with IL-2 has also been shown to improve the efficacy of chemotherapy in a group of metastatic CRC patients by increasing lymphocyte proliferation (55). Interferon-alpha is another cytokine that plays an important role in generating an immune stimulatory response through upregulating MHC-I molecules on the surface of dendritic cells and in turn improving neoantigen presentation. Furthermore, the anti-angiogenic effect of IFN-alpha helps overcome a significant resistance mechanism by converting a cold TME into an immune-friendly stroma (56, 57).
As mentioned above, immune checkpoint inhibitors have not shown clinical efficacy in microsatellite stable (MSS) GI tumors through mechanisms that involve increased T cell exhaustion and activation of co-inhibitory signals such as TIM3 and Lag3 (58-60). In fact, combined inhibition of PD-1 and TIM-3 pathways have resulted in enhanced cytotoxic T cell responses to autologous dendritic cell vaccination in CRC patients, addressing an unmet need in this patient population (61). Chemotherapy has also been shown to activate the immune system by modifying the TME and may have a potential role in converting “cold” into a “hot” TME with a high TIL infiltration (62). As hypothesized, chemotherapy and CEA vaccine combinations have yielded increased antigen-specific T cell responses and improved clinical responses in earlier clinical trials, providing a strong rationale for integrating cytotoxic agents in vaccination protocols (63, 64).
Angiogenesis, which plays a significant role in escape mechanisms by supplying nutrients to a growing tumor tissue, is a relevant target in carcinogenesis (65). Further evidence suggests a possible interplay with angiogenesis and the TME that interferes with immune cell adhesions and migration across the vascular-endothelial junctions, thus preventing infiltration of immune effector cells within the tumor tissue (66). The hypoxic tumor environment mediated through activation of VEGF and angiopoietin pathways provides an unfriendly stroma not only by inactivation of cytotoxic T cells, but also by promoting expansion of inhibitory components of the immune system including Tregs and TAMs (67). Earlier observations that have shown inhibition of Tregs with bevacizumab and activation of mature dendritic cell and T cell proliferation lend support to the potential role of anti-angiogenic therapy in generating an immune-friendly TME (68, 69).
Cancer vaccines for esophageal and gastric cancer: clinical evidence
Earlier clinical trials evaluating the role of dendritic vaccines pulsed with peptides including Her-2 and MAGE have shown the feasibility of this approach with a low toxicity profile and tumor-specific T cell responses which translated into minor tumor regressions (70-72). More recent trials focused on combination strategies aiming to improve immune responses as well as clinical efficacy. A peptide vaccine combining URLC10 peptide, a neoantigen frequently expressed in gastric cancer and VEGFR1, an anti-angiogenic epitope was evaluated in a cohort of refractory metastatic gastric cancer patients. Although specific cytotoxic T cell responses were detected in 65% of patients, 30% had disease stabilization as the best response and a poor outcome with a median survival of 3.6 months (73). In a phase Ib trial, 14 patients with Her-2 overexpressing metastatic gastric cancer were treated with a Her-2 peptide vaccine selected for B cell epitopes combined with a non-toxic form of diphtheria toxin, which is not only intended to prime specific memory T cell responses, but also blocks cellular proliferation through targeting heparin-binding receptors on tumor cells. Out of 11 patients eligible for response assessment, the overall response rate was reported as 54.5%, with one patient who achieved a complete response (74).
Several trials evaluated the efficacy of vaccines combined with chemotherapy in the advanced setting and as part of adjuvant chemotherapy in patients who underwent surgery for localized gastric cancer. The GC4 was a multicenter trial that enrolled advanced gastric and gastroesophageal cancer patients investigating the role of chemotherapy and a peptide vaccine from the gastrin sequence conjugated with diphtheria toxin. Previously untreated 96 patients received standard treatment with cisplatin and fluorouracil in combination with the vaccine administered intramuscularly in weeks 1, 5, 9 and 25, yielding a confirmed ORR of 30% in evaluable patients. The median TTP and OS were estimated as 5.4 and 9.2 months, respectively; with a significant improvement in immune-responders as compared to those who failed to generate circulating anti-G17 antibody titers (75). A similar approach of dendritic cell vaccination pulsed with WNT and MUC1 peptide given in combination with salvage chemotherapy was evaluated in 20 patients with gastric cancer. The treatment was feasible and a trend for prolonged survival was observed in patients in whom a higher percentage of effector T cells could be induced (76). As an adjuvant strategy, a multi-epitope vaccine combining neoantigens with angiogenic peptides was evaluated in 14 patients who received adjuvant chemotherapy for stage III resected gastric cancer. The combined approach was found feasible, but outcomes were not reported (77).
Immune checkpoint inhibitors revolutionized immunotherapy for the treatment of numerous cancer types. From a mechanistic point of view, these agents are hypothesized to boost cancer-specific cytotoxic T cell responses by releasing the brakes on the immune system. This strategy was explored in a patient with metastatic gastric cancer as part of an ongoing clinical trial investigating a dendritic cell vaccine pulsed with eight tumor-associated neoantigens. The patient received four vaccines after lymphodepletion with cyclophosphamide followed by boosters given in combination with nivolumab every two weeks starting from day 65, leading to a rapid tumor response despite progression over the first two months of single-agent vaccine therapy. The patient displayed a complete response which was ongoing after 25 months (78). Ongoing and completed clinical trials with vaccines in upper GI malignancies are listed in Table 1.
Cancer vaccines for colorectal cancer: clinical evidence
As a universal biomarker, carcinoembryonic antigen (CEA) is a frequently utilized tumor antigen in CRC vaccine trials. Early phase I trials evaluating the role of DC vaccines pulsed with CEA have demonstrated potent T cell responses in a small cohort of CRC patients with liver metastases. Correlations with outcomes could not be analyzed due to the small sample size (79). Another study investigating the role of an engineered adenovirus construct encoding a modified HLA-restricted CEA included 32 patients with CRC who had progressed following a median of three previous lines of standard chemotherapy. These patients who received three subcutaneous injections every three weeks were found to generate polyfunctional CD 8 (+) cytotoxic T cells and exhibited an encouraging 12-month survival rate of 48% (80). Similarly, a MUC-1 peptide vaccine given as three subcutaneous injections with a booster dose at week 52 was shown to generate weakly increased memory cell immune responses in a cohort of 37 patients with CR adenomas, suggesting possible efficacy as a preventive strategy (81). A recombinant vaccinia virus-based vaccine encoding multiple neoantigens including CEA, MUC-1, ICAM and LFA was evaluated in a randomized study including CRC patients who had undergone resections for liver or lung metastases. Seventy-six patients were enrolled in the trial, which aimed to investigate the role of two different vaccine constructs in a minimal residual disease setting. Translational analysis showed a high ratio of CEA-specific T cell responses. Although there was no difference between the two groups, the median RFS and OS rates reported as 25.7 and 44.1 months, respectively, were higher than contemporary unvaccinated controls (82). A recent study evaluated the role of an immunomodulatory vaccination with arginase-I (ARG-I) peptide, which targets the immunosuppressive tumor microenvironment (TME) in a small cohort with multiple tumor types including CRC. Nevertheless, despite generation of a specific T and B cell immune response, there were no objective responses attained with the new approach (83).
Further clinical trials integrated innovative immunostimulatory strategies in vaccination schedules to improve response rates. One of these, which included 53 advanced cancer patients comprising 38 patients with CRC evaluated the efficacy of a Ras-peptide vaccine. Patients received 3 doses of the vaccine every 3-5 weeks with GM-CSF or IL-2 as immunostimulatory adjuvants. The study demonstrated that almost all patients who received GM-CSF developed an immune response by the ELISPOT assay. An unplanned subgroup analysis of CRC patients revealed an encouraging OS of 14.2 months, which compared favorably to historical controls who had a median OS of 12.9 months, despite the shorter median PFS of 3.5 months in the vaccinated cohort. This interesting observation lends support to the generally accepted notion that response to immunotherapy and overall survival are not correlated (84).
Numerous clinical studies have utilized chemotherapy as an immune modulatory approach to improve efficacy of cancer vaccines. Barve et al (85) have reported two cases who had been treated with an autologous tumor vaccine given in conjunction with the FOLFOX regimen following resection of liver metastases. The vaccine consisted of surgically resected autologous tumor samples electroporated with a plasmid encoding GM-CSF and a bifunctional siRNA targeting immunosuppressant cytokines. Patients received subcutaneous two injections every two weeks followed by maintenance every four weeks until the product was exhausted along with six cycles of chemotherapy, which resulted in a disease-free survival extending beyond eight years. A similar approach was evaluated in a phase I trial that evaluated the role of a peptide vaccine containing seven tumor neoantigens combined with chemotherapy as an add-on maintenance strategy in the minimal residual disease setting. In addition to sustained tumor-specific T cell responses, a confirmed ORR of 27.5% and a clinical benefit rate of 63.6% was achieved with the combination in a cohort of 11 patients with metastatic CRC (86).
Emerging clinical evidence suggests a possible role for immune checkpoint inhibitors in priming T cell responses in an otherwise immune-suppressed TME, such as microsatellite stable CRC. A phase II clinical trial evaluated the role of GVAX, an allogeneic, whole-cell cancer vaccine given in combination with pembrolizumab and low-dose cyclophosphamide in patients who had progressed after at least two prior lines of chemotherapy for mismatch repair proficient metastatic CRC. Unfortunately, the trial was terminated due to futility after enrolment of 17 patients, in whom no objective responses were observed despite a substantial biochemical response (87). Similarly, a combination of avelumab and an autologous dendritic cell vaccine yielded no objective responses in a small phase II study comprising of a heavily pretreated cohort with metastatic CRC (88). Nevertheless, a phase I trial investigating the role of a combined viral-based multiepitope vaccine comprising of a chimpanzee adenovirus and Venezuelan equine encephalitis virus-based vectors has been shown to elicit long-term memory immune responses in 14 patients comprising of 7 MSS metastatic CRC and 8 patients with metastatic GC. In the expanded phase 9 patients (3 GC, 6 CRC) received subcutaneous low-dose anti-CTLA monoclonal antibody (ipilimumab) or PD-1 therapy with nivolumab along with vaccination. In this cohort, 1 patient with GC had a complete response and was alive after 470 days. In the whole cohort, the majority of patients had a stable response. For patients with MSS-CRC, 3 of 7 patients remained alive with an OS of 42% at 12 months, suggesting that some patients may derive durable clinical benefit despite the lack of a radiologic response by imaging (89).
Angiogenic inhibition with bevacizumab has recently been explored as a distinct approach to overcome the immune suppressive environment in a phase II randomized trial. Patients with untreated MSS metastatic CRC were randomized to FOLFOX plus bevacizumab as standard treatment or the same regimen combined with avelumab and an adenovirus-based vaccine encoding CEA. The trial was terminated early after an unplanned futility analysis conducted with eight patients, showing no difference in PFS (90).
Despite the capability to generate robust cancer-specific T cell responses, the inadequate clinical efficacy of cancer vaccines combined with several immunomodulatory strategies highlights the requirement for the identification of subgroups who benefit from these therapies, as well as innovative approaches that would boost immunogenic anti-cancer responses. Ongoing and completed clinical trials with vaccines in CRC are listed in Table 2.
b. Adoptive cell therapy: cytokine-induced killer cells as an immunotherapy approach in GI cancers
Adoptive cell therapy (ACT) is a type of personalized cellular immunotherapy, that involves isolation of immune cells from the blood and re-administration following ex-vivo expansion. Initial evidence regarding the efficacy of ACT has been generated from earlier melanoma trials, which have demonstrated response rates ranging between 49-72%, and long-term survival achieved in a fraction of patients (91). Cytokine-induced killer cells (CIK) represent a fraction of expanded lymphocytes that are comprised of CD3+CD56+ natural killer cells (NK), which are capable of MHC-unrestricted immune cell killing, as well as CD3+CD56-T cells. Although NK cells are the major effector cells, the anti-tumor efficacy of CIK cells is enhanced through the induction of cytokines that upregulate Th1 type immune response and promote migration to the tumor site following infusion. The main advantage of CIK cells is their potential efficacy against a wide array of tumors, MHC-unrestricted activity and less demanding technical requirements, which have led to the widespread use of this promising strategy as an adoptive immunotherapy tool in several tumor types (92, 93).
Numerous clinical trials have evaluated the feasibility and efficacy of CIK cell therapy in GI cancers. One of the earlier studies randomized 60 patients with metastatic CRC to standard chemotherapy versus 1-4 cycles of CIK cycles in combination with 6 cycles of FOLFOX chemotherapy. The majority of these patients had undergone surgical resection of metastatic sites. The investigators reported a significant improvement in PFS (25.8 vs. 12 months; p:0.01) and OS (41.3 vs. 30.8 months; p:0.037) in the combined treatment group (94). A phase II clinical study including 33 patients with stage IV GI cancers evaluated the role of combined CIK and CAPOX chemotherapy in the first-line setting. Two CIK infusions were administered on days 14 and 16 in the first couple of chemotherapy cycles in the first group, whereas the second group of 17 patients received chemotherapy only. Numerically longer PFS and OS rates were achieved with the combination despite failure to show a significant difference (PFS: 5.6 vs 3.8 months, p:0.06; OS: 13.9 vs 11 months in combined versus chemotherapy arms respectively). Although the CD8 (+) ratio was not different, patients in the combined arm showed an improved humoral immune response with increased NK, and CD4 (+) helper T cells (95). In a prospective phase II trial by Zhao et al (96) 122 patients were randomized to autologous CIK cells combined with chemotherapy or to chemotherapy alone. The chemotherapy arm consisted of the FOLFOX regimen given for 12 cycles every two weeks and CIK cells were administered on days 15 and 16 of each cycle. As often encountered in immunotherapy trials, with the combined treatment a significant OS (36 vs. 16 months, p<0.001) was achieved, despite a numerically longer PFS not reaching significance levels (16 vs. 10 months, p:0.07).
The impact of CIK cell-based immunotherapy was also investigated by several trials in the adjuvant setting following resection for early-stage CRC. In a retrospective analysis comprised of 96 patients who received at least one CIK infusion during adjuvant chemotherapy, a significant improvement in DFS was achieved with a HR:0.28 (p:0.034) (97). A small prospective randomized phase II study enrolling 46 patients reported improved quality of life and longer OS with the combined CIK and adjuvant FOLFOX regimen (41.9 months) as compared to those who received only chemotherapy (33.8 months) (98). A retrospective study evaluated the role of combined CIK treatment and chemotherapy in a cohort of 60 patients with a control arm comprising of 62 patients who received chemotherapy. Despite a higher ratio of stage III patients in the CIK arm, a significantly higher 5-year DFS (70.7 % vs. 48.3%, p: 0.0024) and OS rate (88.7% vs. 72.4%; p:0.008) were achieved with the combination arm as compared to controls (99).
The encouraging efficacy of adoptive immunotherapy with CIK cells in CRC, either given as a single treatment or in combination with DC was confirmed in a meta-analysis, which included data from 70 studies involving 6743 patients with all stages, of whom 66.7% had stage IV disease. Twenty-five studies included CIK as the only investigational procedure. A substantial difference in PFS (HR:0.63, p<0.00001) and OS (HR:0.57, p<0.00001) was observed with CIK cell immunotherapy as compared to non-immunotherapy treatment (100).
c. Combined immunotherapy approaches: Rationale and preclinical evidence
Favorable outcomes achieved with CIK cell therapy led to increased efforts to improve efficacy with combined approaches. There exists strong preclinical evidence on the synergistic efficacy of pro-inflammatory cytokines such as interleukins (101-104) and interferon (105) as well as cytotoxic agents (106), novel small molecule inhibitors (107-109), immune checkpoint inhibitors (110-112), monoclonal antibodies (113, 114) and dendritic cell (115-117) or viral-based vaccines (118-120) combined with adoptive cell therapy. Several stromal or intracellular mechanisms implicated in the synergistic activity have been identified. As mentioned above cytokines and cytotoxic agents improve immune-mediated cell killing through TME modulation not only by decreasing the ratio of Tregs, but also by induction of a memory effector cell response (102, 104) or direct anti-tumor effect by blockade of cytokine-receptors (105). Co-incubation with dendritic cells has yielded a higher percentage of CD3, CD4 (+) helper T and CD8 (+) T cell accumulation in cell cultures, resulting in improved anti-proliferative and cytotoxic effects not only through induction of immune-mediated cell killing, but also direct activation of CIK cells through CCR5 signaling (115, 116). Small molecule inhibitors that interfere with immunosuppressive pathways such as angiogenesis or beta-catenin-mediated CXCR3 chemokines have also been shown to enhance effector T and NK cell infiltration within the tumor stroma, thus inducing a friendly T-cell inflamed TME (107, 109). As a complementary strategy, immune checkpoint inhibitors augment the anti-tumor efficacy of CIK cells by neutralizing PD-1 and PD-L1 signalling upregulated on both tumor and CIK cells upon engagement (110). Recent advances in technology have led to the development of novel gene therapies delivered through viral constructs which directly target cancer cells and exert cytolytic activity (118-120).
d. Clinical applications of combined cellular immunotherapy in GI cancer: Dendritic cell vaccines and cytokine-induced killer cells
Based on preclinical evidence showing synergistic interaction between dendritic and CIK cells, numerous trials have investigated the role of combined immunotherapy with DC vaccines and CIK cells. In general, these trials have confirmed preclinical observations for GI cancers with enhanced humoral immune responses translating into significantly improved ORR and survival rates (121-126). A recent meta-analysis including 70 trials has reported significant PFS (HR: 0.55, p<0.00001) and OS (HR:0.61, p<0.00001) advantage with DC/CIK therapy in CRC for all stages. Although direct comparison with single CIK therapy is not given, benefit rates in outcomes are numerically higher for the DC/CIK combination, providing clinical evidence of the synergistic activity (100).
IV. Case reports
Case 1
The sixty-six-year-old male patient was admitted to the clinic with epigastric pain, fatigue and exertional dyspnea. Laboratory findings revealed iron deficiency anemia, for which he was referred to the endoscopy unit for further evaluation. A subsequent gastroscopy showed an erosive mass measuring 3x4 cm. located in the antrum, whereas a colonoscopy denied any pathologic findings. A biopsy obtained from the antral mass confirmed the diagnosis as poorly cohesive adenocarcinoma, consistent with gastric primary. Following the completion of imaging workup which showed multiple regional enlarged lymph nodes without any systemic metastatic involvement, he was recommended to undergo perioperative platin-based chemotherapy followed by surgery. Nevertheless, he refused chemotherapy and opted for upfront surgery. Subsequently, he underwent distal subtotal gastrectomy on August 21, 2017. Pathologic evaluation revealed a poorly cohesive, signet-cell ring adenocarcinoma in the antral region which invaded the serosa as well as the lesser omentum and 32 out of 75 lymph nodes involved, consistent with T4N3M0 gastric cancer. Further analysis by FISH revealed Her2 amplification. At that stage, we discussed the risks and benefits of adjuvant chemotherapy, which he refused and opted for personalized cellular immunotherapy. Following regulatory approval based on encouraging evidence from a phase II prospective study combining adjuvant chemotherapy with a cancer vaccine and cytokine-induced killer cells in patients undergoing surgery with gastric cancer, he underwent a combined immunotherapy program consisting of dendritic cells pulsed with autologous tumor cells and cytokine-induced killer cell infusions intercalated with PD-1 inhibition, and metronomic oral cyclophosphamide for 6 months. The adoptive cell therapy was supported with an in-vivo cellular expansion protocol including rh-interleukin-2 and interferon-alpha injections. The detailed treatment protocol is depicted in Fig 1.
He received four DC/CIK infusions between Oct 10, 2017 and Feb 20, 2018, which was lower than the planned schedule due to side effects related to IL-2 injections and limited cellular product yield. In vivo expansion was generally provided by IFN-alpha as IL-2 had to be discontinued due to severe fever, chills, and arthralgias. Starting from the initiation of the treatment protocol, he was routinely screened with imaging studies every twelve weeks and remained disease-free until November 2018, when he started complaining of weight loss. A subsequent endoscopic evaluation revealed recurrent tumoral lesions at the distal anastomosis level extending throughout the colonic mucosa. Following confirmation of Her2 overexpressing adenocarcinoma consistent with relapsed gastric cancer, systemic chemotherapy with trastuzumab was initiated. Unfortunately, failing several lines of chemotherapy combined with Her-2 inhibition, he was deceased on November 2019 with leptomeningeal involvement.
Figure 1.
Detailed treatment protocol.
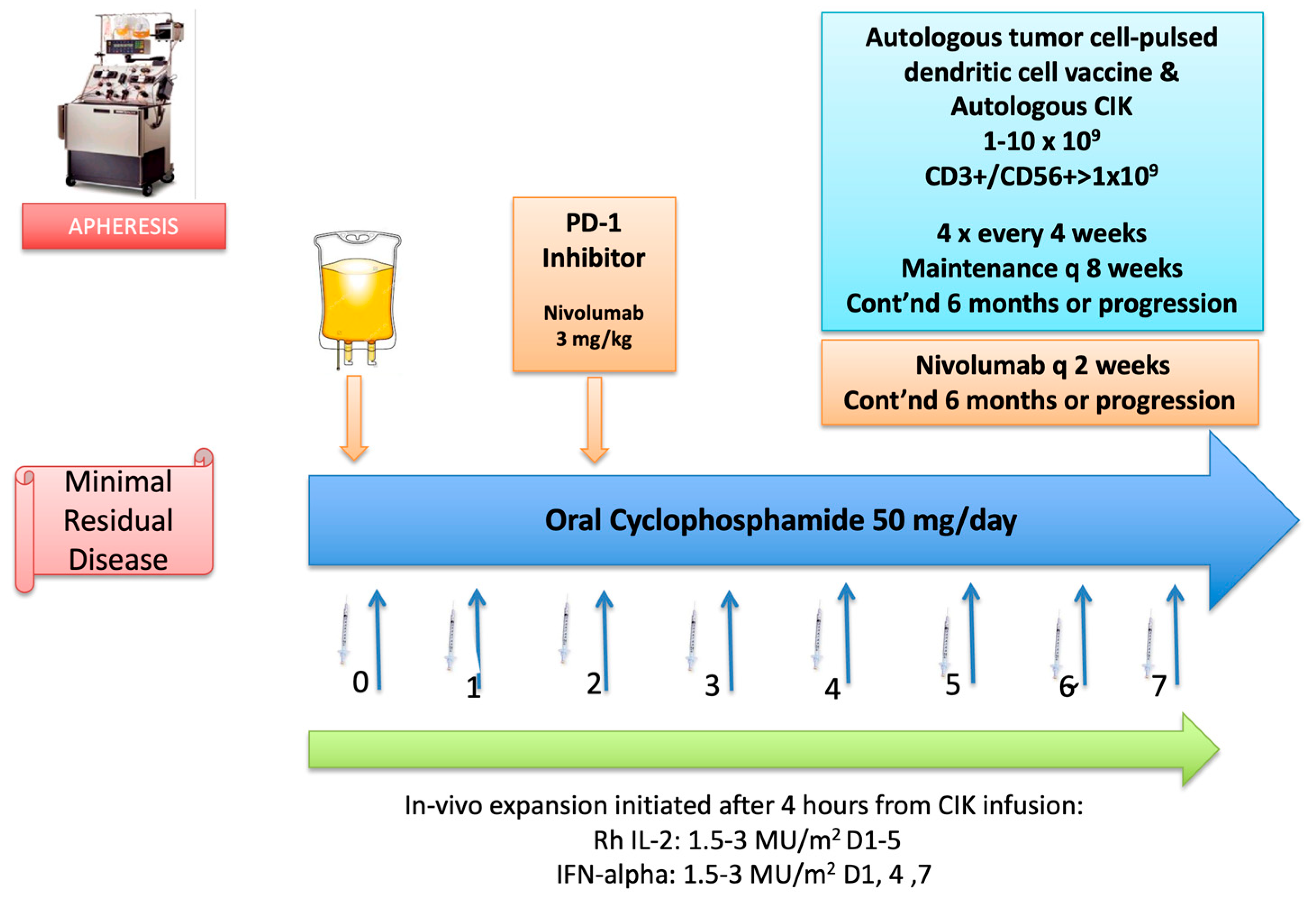
The protocol was initiated following 7 days of conditioning with metronomic oral cyclophosphamide 50 mg daily. Cellular therapy was initiated on day zero (0) with DC injections and CIK infusion. DC/CIK therapy was planned to be given weekly for 4 cycles, followed by maintenance infusions every 8 weeks. Four hours after completion of the infusion, an in-vivo expansion protocol with subcutaneous injections of rh-interleukin-2 (IL-2) at 3 mU/m2 and rh-IFN alpha (IFN-a) at 3 MU/m2 was initiated. IL-2 was planned to be given daily for 5 consecutive days (Days 0-4), whereas IFN-a was administered every other day as a single daily dose for 3 days (Days 0, 2, 4) after DC/CIK infusions. On day +2, nivolumab was started at a dose of 3 mg/kg given as an IV infusion over 60 minutes, followed by 30 minute-infusions at subsequent doses every 2 weeks. The initial plan was to continue the whole protocol for 6 months, and continue with maintenance DC/CIK boosters every 3 months for up to 2 years or progression; whichever occurs first. (Abbreviations: Cont’nd: continued; Rh: recombinant human)
Case 2
A 39-year-old male patient was admitted to our clinic in February 2019 with progressive metastatic right colon cancer. His diagnosis dated back to March 2017, when he underwent a right hemicolectomy for a tumor in the caecum. The pathologic evaluation was consistent with a T3N1M0 KRAS mutant, grade 2 mucinous adenocarcinoma. Following adjuvant chemotherapy with the FOLFOX regimen for 3 months, he was followed up until August 2017, when recurrence in the abdominal cavity and liver metastases were noted. He then underwent several cycles of perioperative chemotherapy consisting of oxaliplatin and capecitabine, followed by cytoreductive surgery with HIPEC, as well as radioablative treatment (RFA) to the liver metastases until November 2017. In January 2018 progression in the liver lesions was identified and he received combination chemotherapy with oxaliplatin-irinotecan-flurouracil and bevacizumab with consolidative RFA that was completed in March 2018. Nevertheless, due to rapid and subsequent recurrences, he underwent a second cytoreductive surgery with HIPEC in May 2018 and a colon resection in January 2019. He was then referred to our clinic for a second opinion on personalized immunotherapy strategies. Imaging studies obtained after his admission failed to show any recurrent lesions, consistent with minimal residual disease. After a thorough discussion of further treatment options, he decided to pursue a combined immunotherapy approach consisting of a personalized DC vaccine, CIK adoptive cell therapy, PD-1 inhibition and bevacizumab based on favorable responses reported by several phase II clinical trials. Following regulatory approval, he underwent apheresis by which cellular products were manufactured under GMP conditions. A detailed treatment plan is provided in Figure 2. He received this protocol between May 15, 2019 and Aug 22, 2019. On the day of the first DC/CIK administration, he experienced a grade 3 infusion reaction with fever, chills and hypotension which required hospitalization. The incident was managed with hydration as well as intravenous medications and did not recur on subsequent therapies. He generally tolerated the protocol well with minimal temporary fatigue throughout the treatment. Unfortunately, an abdominal MRI obtained in September 2019 revealed two implants consistent with peritoneal recurrence. He then went back to his primary treating center for continuation of systemic therapy. In February 2020, he reported being enrolled in a clinical trial with investigational agents which proved to be unresponsive and had been under evaluation for additional systemic therapy. He is still alive with disease progression as of July 2023.
Figure 2.
Detailed treatment protocol.

The protocol was initiated on day (-7) with a conditioning regimen consisting of intravenous cyclophosphamide given as a single IV infusion at 1 gr/m2, followed by subcutaneous GM-SCF injections at a dose of 75 mcg/day starting on day (-1) and continued for 5 days until day 3. Cellular therapy was initiated on day zero (0) with DC injections and CIK infusion. DC/CIK therapy was planned to be given twice every 2 weeks, followed by 4 cycles given every 4 weeks and maintenance infusions every 8 weeks thereafter for up to 2 years or progression; whichever occurs first. On day 7, nivolumab was started at a dose of 3 mg/kg given as an IV infusion over 60 minutes, followed by 30 minute-infusions at subsequent doses every 2 weeks in addition to bevacizumab at a dose of 5 mg/kg given every 2 weeks throughout the immunotherapy period. (Abbreviations: GM-CSF: granulocyte-macrophage-colony stimulating factor; CTX: cyclophosphamide)
Case 3
A 47-year-old patient was referred to our clinic for a second opinion on personalized immunotherapy options as consolidation treatment after induction chemotherapy and surgery for left-sided colon cancer in addition to chemoembolization for liver metastases. His initial diagnosis dated back to March 2018, when a tumor located in the rectosigmoid colon with synchronous multiple liver metastases was detected. After a stable response to three months of systemic chemotherapy with oxaliplatin, irinotecan and fluorouracil combined with cetuximab, he underwent radiofrequency ablation to several liver metastases on May 29, 2018, followed by a low anterior resection procedure with resection of residual liver metastases on June 25, 2018. The pathologic evaluation revealed a grade 2 adenocarcinoma with minimal response to cytotoxic chemotherapy. With no proven evidence for further chemotherapy, we discussed the potential benefits of a combination regimen with DC/CIK infusions administered in conjunction with programmed death-1 (PD-1) and vascular endothelial growth factor (VEGF) inhibitors, based on encouraging outcomes with personalized cellular immunotherapy strategies in the minimal residual disease setting. Following regulatory approval, he underwent apheresis by which cellular products were manufactured under GMP conditions. A detailed treatment plan is provided in Figure 3.
He received this protocol between Feb 15, 2019 and Apr 30, 2019, followed by nine booster DC/CIK infusions until Jan 13, 2021. He generally tolerated the protocol well, with no major toxicity throughout the treatment. Follow-up imaging studies failed to show any recurrence until July 4, 2022, when a nodular lesion in the right thoracic wall and an FDG-avid lymph node in the right hilar station were detected in a PET-CT scan. He then underwent resection of the thoracic lesion, which confirmed the diagnosis as metastatic adenocarcinoma, consistent with colorectal primary. A comprehensive genomic evaluation revealed pathogenic mutations in NRAS, TP-53, SMAD4, APC and ZFHX3 genes, and no PD-L1 expression. The tumor was microsatellite stable and had a low tumor mutation burden of 3.7 m/MB. He then underwent 6 cycles of systemic chemotherapy with the FOLFOX and bevacizumab combination between June and December 2022, which resulted in a partial regression of the hilar lymph node and no residual disease elsewhere. At this stage, we discussed further therapy options and based on his favorable experience with previous consolidative immunotherapy resulting in a sustained progression-free interval, we decided to pursue a similar immunotherapy strategy following irradiation of the residual lymph node basin. Based on the previous protocol, we initiated the treatment with the conditioning regimen on April 4, 2023, and he received this protocol until the last bevacizumab infusion which was administered on July 12, 2023. There were no major side effects encountered during the immunotherapy period except a prolonged grade 1 diarrhea accounted for by pembrolizumab and managed by symptomatic medications. Response assessment by a PET-CT scan obtained on July 24, 2023 failed to show any foci of active lesions suspicious of residual disease. He is planned to receive booster vaccinations every 2-3 months until the vaccine product is exhausted. Please refer to Fig 3 for details on the final immunotherapy protocol.
The protocol was initiated on day (-7) with a conditioning regimen consisting of intravenous cyclophosphamide given as a single IV infusion at 1 gr/m2, followed by subcutaneous GM-SCF injections at a dose of 75 mcg/day starting on day (-1) and continued for 5 days until day 3. Cellular therapy was initiated on day zero (0) with DC injections and CIK infusion. DC/CIK therapy was planned to be given every 2 weeks for 4 cycles, followed by 4 cycles given every 4 weeks and maintenance infusions every 8 weeks thereafter for up to 2 years or progression; whichever occurs first. On day 7, pembrolizumab was started at a fixed dose of 200 mg given as an IV infusion over 60 minutes, followed by 30 minute-infusions at subsequent doses every 2 weeks in addition to bevacizumab at a dose of 7.5 mg/kg given every 3 weeks throughout the immunotherapy period. Starting from the 3rd week after IV cyclophosphamide, oral metronomic cyclophosphamide at 50 mg daily was started and continued throughout. The second immunotherapy protocol was similar to the original protocol except that DC/CIK infusions were administered every 10 days (twice in a 3-week cycle), with omission for some DC vaccine injections and continued for 6 weeks after switching to every 3-week schedule for 6 more weeks due to limitations in cellular content obtained by apheresis. (Abbreviations: GM-CSF: granulocyte macrophage colony stimulating factor; CTX: cyclophosphamide)
Methods
All cellular therapy products were produced under GMP conditions in an approved facility. Dendritic cells and CIK cells were generated from peripheral blood mononuclear cells expanded ex vivo via incubation with cytokines including IL-1, IFN-alpha, TNF-alpha, and IFN-gamma. Activated mature dendritic cells were further incubated with autologous cancer cells to produce a personalized DC vaccine for each patient. Generally, seven days of culture was sufficent to produce the vaccine, whereas 3-4 weeks were required to produce a sufficient amount of CD3+/CD56+ CIK cells to ensure optimal activity. Although the number of viable cells differed for each apheresis procedure, the ultimate aim was to administer 1-10 x 109 cells at each administration. Dendritic cell vaccine pulsed with autologous tumor cells was split in aliquotes and administered subcutanously in all four limbs. Frozen CD3+/CD56+ CIK cells cells suspended in isotonic saline solution was thawed and administered as an IV infusion over 10-20 minutes.
All subjects gave their informed consent for inclusion before they participated in the study. The investigational study was conducted in accordance with the Declaration of Helsinki, and individual approvals were obtained by the Ethics Committee of Gayrettepe Florence Nightingale Hospital, Istanbul, Turkey and subsequently from the Ministry of Health, Health Services General Directorate, Department of Tissue, Organ Transplant and Dialysis (ID codes: 02.11.2017/56733164/203; 27.03.2019; no:216/56733164/203; 19.01.2023/E-56733164-203-210725859).
V. Future prospects and conclusion
Accumulating evidence suggests a possible beneficial role for active immunotherapy with cancer vaccines and adoptive cell therapy with CIK cells in combination with several immunomodulatory agents for GI cancers. Nevertheless, most of the trials evaluating these strategies suffer from a lack of standardization and imbalances in patient characteristics, which limit our ability to reach a definite conclusion on the optimal clinical use of cellular immunotherapy. Furthermore, both tumor and patient-related factors cause temporal immunologic plasticity over the evolution of disease progression through aberrant genomic signaling and TME modulation; which complicate the process even further. Given these constraints, our preliminary experience with cellular immunotherapy showing a lack of efficacy in two out of three patients despite the addition of VEGF and PD-1 inhibiton is in line with previous reports highlighting the difficulties in achieving an immune-mediated response in an otherwise “cold” tumor microenvironment seen in GI cancers. Nevertheless, in the patient with de novo metastatic CRC who had been refractory to initial chemotherapy, the progression-free interval of 18 months after completion of immunotherapy is encouraging and may be considered as a signal of activity. However, a limitation in our protocol that should be mentioned is the lack of laboratory analysis to monitor the humoral immunologic response generated throughout the treatment and follow-up period.
Cancer immunotherapy is a rapidly evolving field. Advances in technology have led to the development of engineered cellular systems or synthetic nanotechnology-based materials that tap into the immune system to activate cytotoxic and memory-effector response against cancer cells. Innovative delivery systems such as non-replicating viral particles, nanoliposomes, exosomes or polymeric nanoparticles loaded with immune checkpoint inhibitors, siRNA, or tumor antigens have been shown to hold great potential as immunotherapeutics by inducing potent anti-tumor response as well as modulating an immunologically “cold” TME as demonstrated by preclinical studies (89, 127-130). Furthermore, engineered dendritic cells expressing CD40 bispecific antibodies showing anti-cancer activity through enhanced DC and T cell activity, hold promise as vaccines against several cancers (131).
Oncolytic viruses which are specifically designed to selectively replicate in cancer cells, possess a potential for dual anti-tumor action by a direct cytolytic effect as well as activation of the stroma to induce an immunologic effector cell response. Engineered oncolytic constructs derived from herpes, adeno, vaccinia, pox or reoviruses have been evaluated in several phase I trials, showing feasibility of this approach with manageable side effects as well as humoral and genomic evidence cancer-specific immune activity such as cytotoxic CD8 (+) and CD4 (+) Th1 cell infiltration; decreased VEGF and tumor-promoting miRNA levels in tumor samples and upregulated IFN-gamma and IL 12 in blood samples (132-134). However, a phase II randomized trial including 103 patients with metastatic CRC failed to show a benefit of the oncolytic Pelareorep, a reovirus construct, when combined with the standard FOLFOX and bevacizumab regimen, with a shorter PFS in the investigational arm (9 vs 7 months, HR: 1.59, p: 0.046), despite a higher ORR (HR: 2.52; p: 0.03) (135). Recently, a phase II study investigating a more contemporary approach with dual PD-1 and CTLA blockade in combination with a vaccinia virus-based oncolytic immunotherapy (Pexastimogene devacirepvec) targeting aberrant EGFR/RAS pathway was reported. The study cohort comprising 34 patients with refractory MSS metastatic CRC was split into two groups receiving single or dual checkpoint inhibition. Although there was no significant difference noted between the two regimens, there was evidence of increased peripheral cytotoxic T cell activity (136). Similarly, Enadenotucirev, an adenovirus-based oncolytic construct was investigated in combination with nivolumab in 51 patients with refractory tumors, 35 of whom had metastatic CRC. Despite the failure to achieve a meaningful objective response, an encouraging survival rate coupled with increased intra-tumoral CD8 (+) T cell activity was observed (137). Further improved activity was reported in a preclinical study investigating the role of herpes simplex-based oncolytic virus combined with PD-1 blockade and trametinib, a novel agent targeting the MAPK-KRAS signaling pathway in a murine model with KRAS or BRAF mutant tumors (138). The results of ongoing trials with engineered constructs encoding multiple tumor- and immune cell-related epitopes in combination with immunomodulatory strategies are awaited with enthusiasm.
Chimeric antigen receptor T cells (CAR-T) have revolutionized adoptive immunotherapy by sustained complete remissions achieved in patients with leukemias (139). There exists encouraging evidence from preclinical and early phase I clinical trials evaluating the role of CAR-T or NK cells engineered to express specific immunomodulatory molecules to overcome resistance in hematologic malignancies (140-142). Nevertheless, the promise of CAR-T’s has not been realized for solid tumors and several hurdles remain to be faced until meaningful clinical utility can be established. Spatial and temporal heterogeneity in tumor antigen expression, as well as obstacles to infiltrating tumor masses protected from immunologic cell kill through abnormal vasculature and a hostile TME are the major factors that pose barriers to an efficacious CAR-T cell therapy (143). Energetic efforts have been placed to improve CAR-T activity in solid tumors by building novel cellular constructs engineered to express immunostimulatory checkpoints including CD28 and OX-40 (144), specific tumor antigens (145-147) or effector cytokines such as IL-12, IL-18 (148). These strategies have yielded promising efficacy in murine models engrafted with several tumors like melanoma, mesothelioma, neuroendocrine tumors as well as CRC (149). However, there exists evidence from phase I clinical trials showing limited activity with short-acting stable disease as the best response, highlighting the challenges that need to be addressed by future research (150). The Keynote B79 trial, which is an ongoing study evaluating the role of an allogeneic CAR-T cell expressing an NKG2D receptor targeting both tumor cells and the TME presents a valuable example of where the field is directed. Based on previous experience suggesting preliminary efficacy with this engineered construct aiming to induce an MHC-I unrestricted immune-mediated cell kill and to antagonize immune suppressive components of the TME, the trial combines complementary immunomodulating strategies including a chemotherapy backbone with FOLFOX and pembrolizumab to drive a deeper and sustained response in a cohort of patients with refractory CRC (151).
Advances in the field of immunotherapy have led to the accumulation of an expanding pool of information on the complexity of anti-cancer immunity. Despite encouraging results investigating combinations of innovative strategies as outlined above, clinical outcomes in GI cancers have proved to pose challenges with regards to immunotherapy. In fact, preclinical and translational analyses have led to the identification of a substantial number of biomarkers, which have been implicated to play crucial roles in the generation of the immunosuppressant stroma, an inherent characteristic encountered in most GI cancers. Future studies focusing on the identification of the genomic characteristics underlying the hostile “cold” TME, as well as mechanisms elucidating the intricate interactions between effector and suppressor cell components of the tumor stroma will help to define patients who would derive benefit from these approaches. These ongoing efforts will undoubtedly deepen our understanding of the immunologic landscape and provide unprecedented insight into optimizing personalized immunotherapy for patients with GI cancers.
Author Contributions
Conceptualization, Methodology, Formal Analysis, Investigation, Resources, Data Curation: Y.E. and U.A; Writing – Original Draft Preparation; Writing – Review & Editing; Visualization, Supervision, Funding Acquisition: Y.E.
Conflicts of Interest
The authors declare no conflict of interest relevant to this work.
Informed Consent; Institutional and Central Review Board Approval
All subjects gave their informed consent for inclusion before they participated in the study. The investigational study was conducted in accordance with the Declaration of Helsinki, and individual approvals were obtained by the Ethics Committee of Gayrettepe Florence Nightingale Hospital, Istanbul, Turkey and subsequently from the Ministry of Health, Health Services General Directorate, Department of Tissue, Organ Transplant and Dialysis (ID codes: 02.11.2017/56733164/203; 27.03.2019; no:216/56733164/203; 19.01.2023/E-56733164-203-210725859).
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef] [PubMed]
- Arnold, M.; Abnet, C.C.; Neale, R.E.; Vignat, J.; Giovannucci, E.L.; McGlynn, K.A.; Bray, F. Global Burden of 5 Major Types of Gastrointestinal Cancer. Gastroenterology 2020, 159, 335–349. [Google Scholar] [CrossRef] [PubMed]
- Janjigian, Y.Y.; Shitara, K.; Moehler, M.; Garrido, M.; Salman, P.; Shen, L.; Wyrwicz, L.; Yamaguchi, K.; Skoczylas, T.; Bragagnoli, A.C.; et al. First-line nivolumab plus chemotherapy versus chemotherapy alone for advanced gastric, gastro-oesophageal junction, and oesophageal adenocarcinoma (CheckMate 649): a randomised, open-label, phase 3 trial. Lancet 2021, 3, 27–40. [Google Scholar] [CrossRef]
- Rha, S.Y.; Wyrwicz, L.S.; Weber, P.E.Y.; Bai, Y.; Ryu, M.H.; Lee, J.; Rivera, F.; Alves, G.V.; Garrido, M.; Shiu, K.K.; et al. VP1-2023: Pembrolizumab (pembro) plus chemotherapy (chemo) as first-line therapy for advanced HER2-negative gastric or gastroesophageal junction (G/GEJ) cancer: Phase III KEYNOTE-859 study. Annals of Oncology 2023, 34, 319–320. [Google Scholar] [CrossRef]
- Pietrantonio, F.; Randon, G.; Di Bartolomeo, M.; Luciani, A.; Chao, J.; Smyth, E.; Petrelli, F. Predictive role of microsatellite instability for PD-1 blockade in patients with advanced gastric cancer: a meta-analysis of randomized clinical trials. ESMO Open 2021, 6, 100036. [Google Scholar] [CrossRef]
- Marcus, L.; Lemery, S.J.; Keegan, P.; Pazdur, R. FDA Approval Summary: Pembrolizumab for the Treatment of Microsatellite Instability-High Solid Tumors. Clin. Cancer Res. 2019, 25, 3753–3758. [Google Scholar] [CrossRef]
- Marabelle, A.; Le, D.T.; Ascierto, P.A.; Di Giacomo, A.M.; De Jesus-Acosta, A.; Delord, J.-P.; Geva, R.; Gottfried, M.; Penel, N.; Hansen, A.R.; et al. Efficacy of Pembrolizumab in Patients With Noncolorectal High Microsatellite Instability/Mismatch Repair–Deficient Cancer: Results From the Phase II KEYNOTE-158 Study. J. Clin. Oncol. 2020, 38, 1–10. [Google Scholar] [CrossRef]
- Le, D.T.; Kim, T.W.; Van Cutsem, E.; Geva, R.; Jager, D.; Hara, H.; Burge, M.; O’Neil, B.; Kavan, P.; Yoshino, T.; et al. Phase II Open-Label Study of Pembrolizumab in Treatment-Refractory, Microsatellite Instability-High/Mismatch Repair-Deficient Metastatic Colorectal Cancer: KEYNOTE-164. J. Clin. Oncol. 2020, 38, 11–19. [Google Scholar] [CrossRef]
- A Diaz, L.; Shiu, K.-K.; Kim, T.-W.; Jensen, B.V.; Jensen, L.H.; Punt, C.; Smith, D.; Garcia-Carbonero, R.; Benavides, M.; Gibbs, P.; et al. Pembrolizumab versus chemotherapy for microsatellite instability-high or mismatch repair-deficient metastatic colorectal cancer (KEYNOTE-177): final analysis of a randomised, open-label, phase 3 study. Lancet Oncol. 2022, 23, 659–670. [Google Scholar] [CrossRef]
- Taefehshokr, S.; Parhizkar, A.; Hayati, S.; Mousapour, M.; Mahmoudpour, A.; Eleid, L.; Rahmanpour, D.; Fattahi, S.; Shabani, H.; Taefehshokr, N. Cancer immunotherapy: Challenges and limitations. Pathol. - Res. Pr. 2022, 229, 153723. [Google Scholar] [CrossRef] [PubMed]
- Gerard, C.; Delyon, J.; Wicky, A.; Homicsko, K.; Cuendet, M.A.; Michielin, O. Turning tumors from cold to inflamed to improve immunotherapy response. Cancer Treat. Rev. 2021, 101, 102227. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.Y.; Jeon, J.W.; Sievers, C.; Allen, C.T. Antigen processing and presentation in cancer immunotherapy. J Immunother Cancer. 2020, 8, e001111. [Google Scholar] [CrossRef]
- O’keeffe, M.; Mok, W.H.; Radford, K.J. Human dendritic cell subsets and function in health and disease. Cell. Mol. Life Sci. 2015, 72, 4309–4325. [Google Scholar] [CrossRef] [PubMed]
- Banchereau, J.; Briere, F.; Caux, C.; Davoust, J.; Lebecque, S.; Liu, Y.-J.; Pulendran, B.; Palucka, K. Immunobiology of Dendritic Cells. Annu. Rev. Immunol. 2000, 18, 767–811. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.; Nussenzweig, M.C. Origin and development of dendritic cells. Immunol. Rev. 2010, 234, 45–54. [Google Scholar] [CrossRef]
- Peterson, E.E.; Barry, K.C. The Natural Killer–Dendritic Cell Immune Axis in Anti-Cancer Immunity and Immunotherapy. Front. Immunol. 2021, 11, 621254. [Google Scholar] [CrossRef] [PubMed]
- Constantino, J.; Gomes, C.; Falcão, A.; Neves, B.M.; Cruz, M.T. Dendritic cell-based immunotherapy: a basic review and recent advances. Immunol. Res. 2017, 65, 798–810. [Google Scholar] [CrossRef]
- van de Laar, L.; Buitenhuis, M.; Wensveen, F.M.; Janssen, H.L.; Coffer, P.J.; Woltman, A.M. Human CD34-Derived Myeloid Dendritic Cell Development Requires Intact Phosphatidylinositol 3-Kinase–Protein Kinase B–Mammalian Target of Rapamycin Signaling. J. Immunol. 2010, 184, 6600–6611. [Google Scholar] [CrossRef]
- Lee, J.; Breton, G.; Oliveira, T.Y.K.; Zhou, Y.J.; Aljoufi, A.; Puhr, S.; Cameron, M.J.; Sékaly, R.-P.; Nussenzweig, M.C.; Liu, K. Restricted dendritic cell and monocyte progenitors in human cord blood and bone marrow. J. Exp. Med. 2015, 212, 385–399. [Google Scholar] [CrossRef]
- Naik, S.H.; Sathe, P.; Park, H.-Y.; Metcalf, D.; I Proietto, A.; Dakic, A.; Carotta, S.; O'Keeffe, M.; Bahlo, M.; Papenfuss, A.; et al. Development of plasmacytoid and conventional dendritic cell subtypes from single precursor cells derived in vitro and in vivo. Nat. Immunol. 2007, 8, 1217–1226. [Google Scholar] [CrossRef] [PubMed]
- Laursen, M.F.; Kofod-Olsen, E.; Agger, R. Activation of dendritic cells by targeted DNA: a potential addition to the armamentarium for anti-cancer immunotherapy. Cancer Immunol. Immunother. 2019, 68, 1875–1880. [Google Scholar] [CrossRef] [PubMed]
- Saban, D.R. The Chemokine Receptor CCR7 Expressed by Dendritic Cells: A Key Player in Corneal and Ocular Surface Inflammation. Ocul. Surf. 2014, 12, 87–99. [Google Scholar] [CrossRef]
- Yan, Y.; Chen, R.; Wang, X.; Hu, K.; Huang, L.; Lu, M.; HU, Q. CCL19 and CCR7 Expression, Signaling Pathways, and Adjuvant Functions in Viral Infection and Prevention. Front Cell Dev Biol 2019, 7, 212. [Google Scholar] [CrossRef] [PubMed]
- Anari, F.; Ramamurthy, C.; Zibelman, M. Impact of tumor microenvironment composition on therapeutic responses and clinical outcomes in cancer. Futur. Oncol. 2018, 14, 1409–1421. [Google Scholar] [CrossRef]
- Khalaf, K.; Hana, D.; Chou, J.T.-T.; Singh, C.; Mackiewicz, A.; Kaczmarek, M. Aspects of the Tumor Microenvironment Involved in Immune Resistance and Drug Resistance. Front. Immunol. 2021, 12, 656364. [Google Scholar] [CrossRef]
- Li, J.; Byrne, K.T.; Yan, F.; Yamazoe, T.; Chen, Z.; Baslan, T.; Richman, L.P.; Lin, J.H.; Sun, Y.H.; Rech, A.J.; et al. Tumor Cell-Intrinsic Factors Underlie Heterogeneity of Immune Cell Infiltration and Response to Immunotherapy. Immunity. 2018, 49, 178–193. [Google Scholar] [CrossRef]
- Gerard, C.; Delyon, J.; Wicky, A.; Homicsko, K.; Cuendet, M.A.; Michielin, O. Turning tumors from cold to inflamed to improve immunotherapy response. Cancer Treat. Rev. 2021, 101, 102227. [Google Scholar] [CrossRef]
- Ito, F.; Chang, A.E. Cancer immunotherapy: current status and future directions. Surg Oncol Clin N Am. 2013, 22, 765–83. [Google Scholar] [CrossRef]
- Ayana, R.; Kumar, A.R.; Devan, A.R.; Nair, B.; Vinod, B.S.; Nath, L.R. Harnessing the immune system against cancer: current immunotherapy approaches and therapeutic targets. Molecular Biology Reports 2021, 48, 8075–8095. [Google Scholar]
- Stephan, K.; Matthias, I.; Sebastian, K. Advances in cancer immunotherapy 2019 – latest trends. Exp Clin Cancer Res 2019, 38, 1–11. [Google Scholar]
- Marshall, H.T.; Djamgoz, M.B.A. Immuno-Oncology: Emerging targets and combination therapies. Front Oncol. 2018, 8, 315. [Google Scholar] [CrossRef] [PubMed]
- Khalil, D.N.; Smith, E.L.; Brentjens, R.J.; Wolchok, J.D. The future of cancer treatment: immunomodulation, CARs and combination immunotherapy. Nat Rev Clin Oncol. 2016, 13, 273–90. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Cao, Y.J. Adoptive Cell Therapy Targeting Neoantigens: A Frontier for Cancer Research. Front Immunol. 2020, 11, 176. [Google Scholar] [CrossRef]
- Coley, W.B. The treatment of malignant tumors by repeated inoculations of erysipelas: with a report of ten original cases. Am. J. Med. Sci. 1893, 105, 487–511. [Google Scholar] [CrossRef]
- Parish, C.R. Cancer immunotherapy: the past, the present and the future. Immunol Cell Biol 2003, 81, 106–13. [Google Scholar] [CrossRef]
- Fritah, H.G.; Rovelli, R.; Chiang, C.L.-L.; Kandalaft, L.E. The current clinical landscape of personalized cancer vaccines. Cancer Treat. Rev. 2022, 106, 102383. [Google Scholar] [CrossRef]
- Lin, M.J.; Svensson-Arvelund, J.; Lubitz, G.S.; Marabelle, A.; Melero, I.; Brown, B.D.; Brody, J.D. Cancer vaccines: the next immunotherapy frontier. Nat. Cancer 2022, 3, 911–926. [Google Scholar] [CrossRef]
- Kantoff, P.W.; Higano, C.S.; Shore, N.D.; Berger, E.R.; Small, E.J.; Penson, D.F.; Redfern, C.H.; Ferrari, A.C.; Dreicer, R.; Sims, R.B.; et al. Sipuleucel-T Immunotherapy for Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2010, 363, 411–422. [Google Scholar] [CrossRef]
- Andtbacka, R.H.; Kaufman, H.L.; Collichio, F.; Amatruda, T.; Senzer, N.; Chesney, J.; et al. Faculty Opinions recommendation of Talimogene laherparepvec improves durable response rate in patients with advanced melanoma. Journal of clinical oncology 2015, 33, 2780–2788. [Google Scholar] [CrossRef]
- Fritsch, E.F.; Burkhardt, U.E.; Hacohen, N.; Wu, C.J. Personal Neoantigen Cancer Vaccines: A Road Not Fully Paved. Cancer Immunol. Res. 2020, 8, 1465–1469. [Google Scholar] [CrossRef] [PubMed]
- Palucka, K.; Banchereau, J. Cancer immunotherapy via dendritic cells. Nat. Rev. Cancer 2012, 12, 265–277. [Google Scholar] [CrossRef] [PubMed]
- Constantino, J.; Gomes, C.; Falcão, A.; Cruz, M.T.; Neves, B.M. Antitumor dendritic cell–based vaccines: lessons from 20 years of clinical trials and future perspectives. Transl. Res. 2016, 168, 74–95. [Google Scholar] [CrossRef]
- Chudnovskiy, A.; Pasqual, G.; Victora, G.D. Studying interactions between dendritic cells and T cells in vivo. Curr. Opin. Immunol. 2019, 58, 24–30. [Google Scholar] [CrossRef]
- Zanna, M.Y.; Yasmin, A.R.; Omar, A.R.; Arshad, S.S.; Mariatulqabtiah, A.R.; Nur-Fazila, S.H.; Mahiza, I.N. Review of Dendritic Cells, Their Role in Clinical Immunology, and Distribution in Various Animal Species. Int. J. Mol. Sci. 2021, 22, 8044. [Google Scholar] [CrossRef] [PubMed]
- Allan, R.S.; Waithman, J.; Bedoui, S.; Jones, C.M.; Villadangos, J.A.; Zhan, Y.; Lew, A.M.; Shortman, K.; Heath, W.R.; Carbone, F.R. Migratory Dendritic Cells Transfer Antigen to a Lymph Node-Resident Dendritic Cell Population for Efficient CTL Priming. Immunity 2006, 25, 153–162. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Sánchez, N.; Riol-Blanco, L.; Rodríguez-Fernández, J.L. The Multiple Personalities of the Chemokine Receptor CCR7 in Dendritic Cells. J. Immunol. 2006, 176, 5153–5159. [Google Scholar] [CrossRef]
- Filin, I.Y.; Kitaeva, K.V.; Rutland, C.S.; Rizvanov, A.A.; Solovyeva, V.V. Recent Advances in Experimental Dendritic Cell Vaccines for Cancer. Front. Oncol. 2021, 11, 730824. [Google Scholar] [CrossRef]
- Gardner, A.; Ruffell, B. Dendritic Cells and Cancer Immunity. Trends Immunol. 2016, 37, 855–865. [Google Scholar] [CrossRef]
- Hsu, F.J.; Benike, C.; Fagnoni, F.; Liles, T.M.; Czerwinski, D.; Taidi, B.; Engleman, E.G.; Levy, R. Vaccination of patients with B–cell lymphoma using autologous antigen–pulsed dendritic cells. Nat. Med. 1996, 2, 52–58. [Google Scholar] [CrossRef]
- Dashti, A.; Ebrahimi, M.; Hadjati, J.; Memarnejadian, A.; Moazzeni, S.M. Dendritic cell based immunotherapy using tumor stem cells mediates potent antitumor immune responses. Cancer Lett. 2016, 374, 175–185. [Google Scholar] [CrossRef] [PubMed]
- Carreno, B.M.; Magrini, V.; Becker-Hapak, M.; Kaabinejadian, S.; Hundal, J.; Petti, A.A.; Ly, A.; Lie, W.R.; Hildebrand, W.H.; Mardis, E.R.; Linette, G.P. Cancer immunotherapy. A dendritic cell vaccine increases the breadth and diversity of melanoma neoantigen-specific T cells. Science 2015, 348, 803–808. [Google Scholar] [CrossRef]
- Jeng, L.B.; Liao, L.Y.; Shih, F.Y.; Teng, CF. Dendritic-Cell-Vaccine-Based Immunotherapy for Hepatocellular Carcinoma: Clinical Trials and Recent Preclinical Studies. Cancers (Basel) 2022, 14, 4380. [Google Scholar] [CrossRef]
- Ju, H.; Xing, W.; Yang, J.; Zheng, Y.; Jia, X.; Zhang, B.; Ren, H. An effective cytokine adjuvant vaccine induces autologous T-cell response against colon cancer in an animal model. BMC Immunol. 2016, 17, 31. [Google Scholar] [CrossRef] [PubMed]
- Lissoni, P.; Brivio, F.; Fumagalli, L.; Di Fede, G.; Brera, G. Enhancement of the efficacy of chemotherapy with oxaliplatin plus 5-fluorouracil by pretreatment with IL-2 subcutaneous immunotherapy in metastatic colorectal cancer patients with lymphocytopenia prior to therapy. Vivo 2005, 19, 1077–80. [Google Scholar]
- Borden, E.C. Interferons α and β in cancer: therapeutic opportunities from new insights. Nat Rev Drug Discov. 2019, 18, 219–234. [Google Scholar] [CrossRef]
- Spaapen, R.M.; Leung, M.Y.K.; Fuertes, M.B.; Kline, J.P.; Zhang, L.; Zheng, Y.; Fu, Y.-X.; Luo, X.; Cohen, K.S.; Gajewski, T.F. Therapeutic Activity of High-Dose Intratumoral IFN-β Requires Direct Effect on the Tumor Vasculature. J. Immunol. 2014, 193, 4254–4260. [Google Scholar] [CrossRef]
- Anderson, A.C. Tim-3: An Emerging Target in the Cancer Immunotherapy Landscape. Cancer Immunol. Res. 2014, 2, 393–398. [Google Scholar] [CrossRef]
- Shen, R.; Postow, M.A.; Adamow, M.; Arora, A.; Hannum, M.; Maher, C.; Wong, P.; Curran, M.A.; Hollmann, T.J.; Jia, L.; et al. LAG-3 expression on peripheral blood cells identifies patients with poorer outcomes after immune checkpoint blockade. Sci. Transl. Med. 2021, 13, eabf5107. [Google Scholar] [CrossRef]
- Liu, L.; Chen, J.; Zhang, H.; Ye, J.; Moore, C.; Lu, C.; Fang, Y.; Fu, Y.X.; Li, B. Concurrent delivery of immune checkpoint blockade modulates T cell dynamics to enhance neoantigen vaccine-generated antitumor immunity. Nat Cancer. 2022, 3, 437–452. [Google Scholar] [CrossRef]
- Liu, J.; Zhang, S.; Hu, Y.; Yang, Z.; Li, J.; Liu, X.; Deng, L.; Wang, Y.; Zhang, X.; Jiang, T.; Lu, X. Targeting PD-1 and Tim-3 Pathways to Reverse CD8 T-Cell Exhaustion and Enhance Ex Vivo T-Cell Responses to Autologous Dendritic/Tumor Vaccines. J Immunother. 2016, 39, 171–80. [Google Scholar] [CrossRef]
- Vanmeerbeek, I.; Sprooten, J.; De Ruysscher, D.; Tejpar, S.; Vandenberghe, P.; Fucikova, J.; Spisek, R.; Zitvogel, L.; Kroemer, G.; Galluzzi, L.; et al. Trial watch: chemotherapy-induced immunogenic cell death in immuno-oncology. OncoImmunology 2020, 9, 1703449. [Google Scholar] [CrossRef]
- Kaufman, H.L.; Lenz, H.J.; Marshall, J.; Singh, D.; Garett, C.; Cripps, C.; Moore, M.; von Mehren, M.; Dalfen, R.; Heim, W.J.; et al. Combination chemotherapy and ALVAC-CEA/B7.1 vaccine in patients with metastatic colorectal cancer. Clin Cancer Res. 2008, 14, 4843–4849. [Google Scholar] [CrossRef]
- Weihrauch, M.R.; Ansén, S.; Jurkiewicz, E.; Geisen, C.; Xia, Z.; Anderson, K.S.; Gracien, E.; Schmidt, M.; Wittig, B.; Diehl, V.; et al. Phase I/II combined chemoimmunotherapy with carcinoembryonic antigen-derived HLA-A2-restricted CAP-1 peptide and irinotecan, 5-fluorouracil, and leucovorin in patients with primary metastatic colorectal cancer. Clin Cancer Res. 2005, 11, 5993–6001. [Google Scholar] [CrossRef]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: the next generation. Cell. 2011, 144, 646–674. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Ji, Y.R.; Le, Y.M. Crosstalk between angiogenesis and immune regulation in the tumor microenvironment. Arch. Pharm. Res. 2022, 45, 401–416. [Google Scholar] [CrossRef] [PubMed]
- Rahma, O.E.; Hodi, F.S. The Intersection between Tumor Angiogenesis and Immune Suppression. Clin Cancer Res. 2019, 25, 5449–5457. [Google Scholar] [CrossRef] [PubMed]
- Osada, T.; Chong, G.; Tansik, R.; Hong, T.; Spector, N.; Kumar, R.; Hurwitz, H.I.; Dev, I.; Nixon, A.B.; Lyerly, H.K.; et al. The effect of anti-VEGF therapy on immature myeloid cell and dendritic cells in cancer patients. Cancer Immunol. Immunother. 2008, 57, 1115–1124. [Google Scholar] [CrossRef] [PubMed]
- Terme, M.; Pernot, S.; Marcheteau, E.; Sandoval, F.; Benhamouda, N.; Colussi, O.; Dubreuil, O.; Carpentier, A.F.; Tartour, E.; Taieb, J. VEGFA-VEGFR pathway blockade inhibits tumor-induced regulatory T-cell proliferation in colorectal cancer. Cancer Res. 2013, 73, 539–549. [Google Scholar] [CrossRef] [PubMed]
- Sadanaga, N.; Nagashima, H.; Mashino, K.; Tahara, K.; Yamaguchi, H.; Ohta, M.; Fujie, T.; Tanaka, F.; Inoue, H.; Takesako, K.; et al. Dendritic cell vaccination with MAGE peptide is a novel therapeutic approach for gastrointestinal carcinomas. Clin. Cancer Res. 2001, 7, 2277–2284. [Google Scholar]
- Galetto, A.; Contarini, M.; Sapino, A.; Cassoni, P.; Consalvo, E.; Forno, S.; Pezzi, C.; Barnaba, V.; Mussa, A.; Matera, L. Ex Vivo Host Response to Gastrointestinal Cancer Cells Presented by Autologous Dendritic Cells. J. Surg. Res. 2001, 100, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Kono, K.; Takahashi, A.; Sugai, H.; Fujii, H.; Choudhury, A.R.; Kiessling, R.; Matsumoto, Y. Dendritic cells pulsed with HER-2/neu-derived peptides can induce specific T-cell responses in patients with gastric cancer. Clin Cancer Res. 2002, 8, 3394–400. [Google Scholar] [PubMed]
- Higashihara, Y.; Kato, J.; Nagahara, A.; Izumi, K.; Konishi, M.; Kodani, T.; Serizawa, N.; Osada, T.; Watanabe, S. Phase I clinical trial of peptide vaccination with URLC10 and VEGFR1 epitope peptides in patients with advanced gastric cancer. Int J Oncol. 2014, 44, 662–668. [Google Scholar] [CrossRef] [PubMed]
- Wiedermann, U.; Garner-Spitzer, E.; Chao, Y.; Maglakelidze, M.; Bulat, I.; Dechaphunkul, A.; Arpornwirat, W.; Charoentum, C.; Yen, C.J.; Yau, T.C.; et al. Clinical and Immunologic Responses to a B-Cell Epitope Vaccine in Patients with HER2/neu-Overexpressing Advanced Gastric Cancer-Results from Phase Ib Trial IMU.ACS.001. Clin Cancer Res. 2021, 27, 3649–3660. [Google Scholar] [CrossRef]
- Ajani, J.A.; Hecht, J.R.; Ho, L.; Baker, J.; Oortgiesen, M.; Eduljee, A.; Michaeli, D. An open-label, multinational, multicenter study of G17DT vaccination combined with cisplatin and 5-fluorouracil in patients with untreated, advanced gastric or gastroesophageal cancer : The GC4 study. Cancer 2006, 106, 1908–1916. [Google Scholar] [CrossRef]
- Ogasawara, M. Dendritic cell vaccine-based immunotherapy in combination with salvage chemotherapy for patients with advanced or relapsed gastric cancer. Ann. Oncol. 2018, 29, P075. [Google Scholar] [CrossRef]
- Fujiwara, Y.; Sugimura, K.; Miyata, H.; Omori, T.; Nakano, H.; Mochizuki, C.; Shimizu, K.; Saito, H.; Ashida, K.; Honjyo, S.; Nakamura, Y.; Yano, M. A Pilot Study of Post-Operative Adjuvant Vaccine for Advanced Gastric Cancer. Yonago Acta Med. 2017, 60, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Guo, Z.; Yuan, Y.; Chen, C.; Lin, J.; Ma, Q.; Liu, G.; Gao, Y.; Huang, Y.; Chen, L.; Chen, L.Z.; et al. Durable complete response to neoantigen-loaded dendritic-cell vaccine following anti-PD-1 therapy in metastatic gastric cancer. NPJ Precis Oncol. 2022, 6, 34. [Google Scholar] [CrossRef]
- Lesterhuis, W.J.; de Vries, I.J.M.; Schuurhuis, D.H.; Boullart, A.C.I.; Jacobs, J.F.M.; de Boer, A.J.; Scharenborg, N.M.; Brouwer, H.M.H.; van de Rakt, M.W.M.M.; Figdor, C.G.; et al. Vaccination of colorectal cancer patients with CEA-loaded dendritic cells: antigen-specific T cell responses in DTH skin tests. Ann. Oncol. 2006, 17, 974–980. [Google Scholar] [CrossRef]
- Morse, M.A.; Chaudhry, A.; Gabitzsch, E.S.; Hobeika, A.C.; Osada, T.; Clay, T.M.; Amalfitano, A.; Burnett, B.K.; Devi, G.R.; Hsu, D.S.; et al. Novel adenoviral vector induces T-cell responses despite anti-adenoviral neutralizing antibodies in colorectal cancer patients. Cancer Immunol. Immunother. 2013, 62, 1293–1301. [Google Scholar] [CrossRef]
- Kimura, T.; McKolanis, J.R.; Dzubinski, L.A.; Islam, K.; Potter, D.M.; Salazar, A.M.; Schoen, R.E.; Finn, O.J. MUC1 Vaccine for Individuals with Advanced Adenoma of the Colon: A Cancer Immunoprevention Feasibility Study. Cancer Prev. Res. 2013, 6, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Morse, M.A.; Niedzwiecki, D.; Marshall, J.L.; Garrett, C.; Chang, D.Z.; Aklilu, M.; Crocenzi, T.S.; Cole, D.J.; Dessureault, S.; Hobeika, A.C.; et al. A randomized phase II study of immunization with dendritic cells modified with pox vectors encoding CEA and MUC1 compared with the same pox vectors plus GM-CSF for resected metastatic colorectal cancer. Ann Surg. 2013, 258, 879–86. [Google Scholar] [CrossRef] [PubMed]
- Lorentzen, C.L.; Martinenaite, E.; Kjeldsen, J.W.; Holmstroem, R.B.; Mørk, S.K.; Pedersen, A.W.; Ehrnrooth, E.; Andersen, M.H.; Svane, I.M. Arginase-1 targeting peptide vaccine in patients with metastatic solid tumors – A phase I trial. Front. Immunol. 2022, 13, 1023023. [Google Scholar] [CrossRef]
- E Rahma, O.; Hamilton, J.M.; Wojtowicz, M.; Dakheel, O.; Bernstein, S.; Liewehr, D.J.; Steinberg, S.M.; Khleif, S.N. The immunological and clinical effects of mutated ras peptide vaccine in combination with IL-2, GM-CSF, or both in patients with solid tumors. J. Transl. Med. 2014, 12, 55–55. [Google Scholar] [CrossRef]
- Barve, V.; Adams, N.; Stanbery, L.; Manning, L.; Horvath, S.; Wallraven, G.; Bognar, E.; Barve, M.; Nemunaitis, J. Case Report: Marked Survival Advantage of Two Colorectal Cancer Patients with Liver Metastases Treated with Vigil and FOLFOX-6. Vaccines 2021, 9, 1201. [Google Scholar] [CrossRef]
- Hubbard, J.M.; Tőke, E.R.; Moretto, R.; Graham, R.P.; Youssoufian, H.; Lőrincz, O.; Molnár, L.; Csiszovszki, Z.; Mitchell, J.L.; Wessling, J.; et al. Safety and Activity of PolyPEPI1018 Combined with Maintenance Therapy in Metastatic Colorectal Cancer: an Open-Label, Multicenter, Phase Ib Study. Clin Cancer Res. 2022, 28, 2818–2829. [Google Scholar] [CrossRef]
- Yarchoan, M.; Huang, C.Y.; Zhu, Q.; Ferguson, A.K.; Durham, J.N.; Anders, R.A.; Thompson, E.D.; Rozich, N.S.; Thomas, D.L., 2nd; Nauroth, J.M.; et al. A phase 2 study of GVAX colon vaccine with cyclophosphamide and pembrolizumab in patients with mismatch repair proficient advanced colorectal cancer. Cancer Med. 2020, 9, 1485–1494. [Google Scholar] [CrossRef]
- Español-Rego, M.; Fernández-Martos, C.; Elez, E.; Foguet, C.; Pedrosa, L.; Rodríguez, N.; Ruiz-Casado, A.; Pineda, E.; Cid, J.; Cabezón, R.; et al. A Phase I-II multicenter trial with Avelumab plus autologous dendritic cell vaccine in pre-treated mismatch repair-proficient (MSS) metastatic colorectal cancer patients; GEMCAD 1602 study. Cancer Immunol. Immunother. 2023, 72, 827–840. [Google Scholar] [CrossRef]
- Palmer, C.D.; Rappaport, A.R.; Davis, M.J.; Hart, M.G.; Scallan, C.D.; Hong, S.-J.; Gitlin, L.; Kraemer, L.D.; Kounlavouth, S.; Yang, A.; et al. Individualized, heterologous chimpanzee adenovirus and self-amplifying mRNA neoantigen vaccine for advanced metastatic solid tumors: phase 1 trial interim results. Nat. Med. 2022, 28, 1619–1629. [Google Scholar] [CrossRef]
- Redman, J.M.; Tsai, Y.-T.; A Weinberg, B.; Donahue, R.N.; Gandhy, S.; E Gatti-Mays, M.; Sater, H.A.; Bilusic, M.; Cordes, L.M.; Steinberg, S.M.; et al. A Randomized Phase II Trial of mFOLFOX6 + Bevacizumab Alone or with AdCEA Vaccine + Avelumab Immunotherapy for Untreated Metastatic Colorectal Cancer. Oncol. 2022, 27, 198–209. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, S.A.; Yang, J.C.; Sherry, R.M.; Kammula, U.S.; Hughes, M.S.; Phan, G.Q.; Citrin, D.E.; Restifo, N.P.; Robbins, P.F.; Wunderlich, J.R.; et al. Durable complete responses in heavily pretreated patients with metastatic melanoma using T-cell transfer immunotherapy. Clin Cancer Res. 2011, 17, 4550–4557. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Mi, Y.; Guo, N.; Xu, H.; Xu, L.; Gou, X.; Jin, W. Cytokine-Induced Killer Cells As Pharmacological Tools for Cancer Immunotherapy. Front Immunol. 2017, 8, 774. [Google Scholar] [CrossRef] [PubMed]
- Meng, Y.; Yu, Z.; Wu, Y.; Du, T.; Chen, S.; Meng, F.; Su, N.; Ma, Y.; Li, X.; Sun, S.; Zhang, G. Cell-based immunotherapy with cytokine-induced killer (CIK) cells: From preparation and testing to clinical application. Hum Vaccin Immunother. 2017, 13, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zhu, L.; Zhang, Q.; He, X.; Yin, Y.; Gu, Y.; Guo, R.; Lu, K.; Liu, L.; Liu, P.; Shu, Y. Effects of cytokine-induced killer cell treatment in colorectal cancer patients: a retrospective study. Biomed Pharmacother. 2014, 68, 715–720. [Google Scholar] [CrossRef]
- Xu, Y.C.; Xu, Q.; Li, J.J.; Gu, X.F.; Lin, X.L.; Sun, L.; Lu, H.M.; Tang, L.; Ma, Y.; Lu, Z.; Wang, H.X. Chemotherapy with or without autologous cytokine-induced killer cell transfusion as the first-line treatment for stage IV gastrointestinal cancer: a phase II clinical trial. J Cancer Res Clin Oncol. 2016, 142, 1315–1323. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Wang, Y.; Yu, J.; Wei, F.; Cao, S.; Zhang, X.; Dong, N.; Li, H.; Ren, X. Autologous Cytokine-Induced Killer Cells Improves Overall Survival of Metastatic Colorectal Cancer Patients: Results From a Phase II Clinical Trial. Clin Colorectal Cancer. 2016, 15, 228–235. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Zhang, H.; Li, Y.; Bai, J.; Liu, L.; Liu, Y.; Qu, Y.; Qu, X. Efficacy of postoperative adjuvant transfusion of cytokine-induced killer cells combined with chemotherapy in patients with colorectal cancer. Cancer Immunol Immunother. 2013, 62, 1629–1635. [Google Scholar] [CrossRef] [PubMed]
- Peng, H.; Yao, M.; Fan, H.; Song, L.; Sun, J.; Zhou, Z.; Du, Y.; Lu, K.; Li, T.; Yin, A.; Xu, J.; Wei, S. Effects of Autologous Cytokine-Induced Killer Cells Infusion in Colorectal Cancer Patients: A Prospective Study. Cancer Biother Radiopharm. 2017, 32, 221–226. [Google Scholar] [CrossRef]
- Pan, Q.Z.; Zhao, J.J.; Yang, C.P.; Zhou, Y.Q.; Lin, J.Z.; Tang, Y.; Gu, J.M.; Wang, Q.J.; Li, Y.Q.; He, J.; et al. Efficacy of adjuvant cytokine-induced killer cell immunotherapy in patients with colorectal cancer after radical resection. Oncoimmunology 2020, 9, 1752563. [Google Scholar] [CrossRef]
- Li, C.M.Y.; Tomita, Y.; Dhakal, B.; Li, R.; Li, J.; Drew, P.; Price, T.; Smith, E.; Maddern, G.J.; Fenix, K.A. Use of cytokine-induced killer cell therapy in patients with colorectal cancer: a systematic review and meta-analysis. J. Immunother. Cancer 2023, 11, e006764. [Google Scholar] [CrossRef]
- Rettinger, E.; Kuçi, S.; Naumann, I.; Becker, P.; Kreyenberg, H.; Anzaghe, M.; Willasch, A.; Koehl, U.; Bug, G.; Ruthardt, M.; et al. The cytotoxic potential of interleukin-15-stimulated cytokine-induced killer cells against leukemia cells. Cytotherapy 2012, 14, 91–103. [Google Scholar] [CrossRef] [PubMed]
- Lin, G.; Wang, J.; Lao, X.; Wang, J.; Li, L.; Li, S.; Zhang, J.; Dong, Y.; Chang, A.E.; Li, Q.; Li, S. Interleukin-6 inhibits regulatory T cells and improves the proliferation and cytotoxic activity of cytokine-induced killer cells. J Immunother. 2012, 35, 337–343. [Google Scholar] [CrossRef]
- Yang, Z.; Zhang, Q.; Xu, K.; Shan, J.; Shen, J.; Liu, L.; Xu, Y.; Xia, F.; Bie, P.; Zhang, X.; et al. Combined therapy with cytokine-induced killer cells and oncolytic adenovirus expressing IL-12 induce enhanced antitumor activity in liver tumor model. PLoS One. 2012, 7, e44802. [Google Scholar] [CrossRef] [PubMed]
- Peng, Z.; Liang, W.; Li, Z.; Xu, Y.; Chen, L. Interleukin-15-transferred cytokine-induced killer cells elevated anti-tumor activity in a gastric tumor-bearing nude mice model. Cell Biol Int. 2016, 40, 204–13. [Google Scholar] [CrossRef] [PubMed]
- Fiorino, E.; Merlini, A.; D'Ambrosio, L.; Cerviere, I.; Berrino, E.; Marchiò, C.; Giraudo, L.; Basiricò, M.; Massa, A.; Donini, C.; et al. Integrated Antitumor Activities of Cellular Immunotherapy with CIK Lymphocytes and Interferons against KIT/PDGFRA Wild Type GIST. Int J Mol Sci. 2022, 23, 10368. [Google Scholar] [CrossRef]
- Tanaka, Y.; Nakazawa, T.; Nakamura, M.; Nishimura, F.; Matsuda, R.; Omoto, K.; Shida, Y.; Murakami, T.; Nakagawa, I.; Motoyama, Y.; et al. Ex vivo-expanded highly purified natural killer cells in combination with temozolomide induce antitumor effects in human glioblastoma cells in vitro. PLOS ONE 2019, 14, e0212455. [Google Scholar] [CrossRef]
- Yang, Y.; Lin, H.; Zhao, L.; Song, Y.; Gao, Q. Combination of sorafenib and cytokine-induced killer cells in metastatic renal cell carcinoma: a potential regimen. Immunotherapy. 2017, 9, 629–635. [Google Scholar] [CrossRef]
- Capellero, S.; Erriquez, J.; Melano, C.; Mesiano, G.; Genta, S.; Pisacane, A.; Mittica, G.; Ghisoni, E.; Olivero, M.; Di Renzo, M.F.; et al. Preclinical immunotherapy with Cytokine-Induced Killer lymphocytes against epithelial ovarian cancer. Sci. Rep. 2020, 10, 6478. [Google Scholar] [CrossRef]
- Wang, C.; Yan, J.; Yin, P.; Gui, L.; Ji, L.; Ma, B.; Gao, W.Q. β-Catenin inhibition shapes tumor immunity and synergizes with immunotherapy in colorectal cancer. Oncoimmunology. 2020, 9, 1809947. [Google Scholar] [CrossRef]
- Dai, C.; Lin, F.; Geng, R.; Ge, X.; Tang, W.; Chang, J.; Wu, Z.; Liu, X.; Lin, Y.; Zhang, Z.; Li, J. Implication of combined PD-L1/PD-1 blockade with cytokine-induced killer cells as a synergistic immunotherapy for gastrointestinal cancer. Oncotarget 2016, 7, 10332–10344. [Google Scholar] [CrossRef]
- Chen, J.; Chen, Y.; Feng, F.; Chen, C.; Zeng, H.; Wen, S.; Xu, X.; He, J.; Li, J. Programmed cell death protein-1/programmed death-ligand 1 blockade enhances the antitumor efficacy of adoptive cell therapy against non-small cell lung cancer. J Thorac Dis. 2018, 10, 6711–6721. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Sharma, A.; Wu, X.; Weiher, H.; Skowasch, D.; Essler, M.; Schmidt-Wolf, I.G.H. A Combination of Cytokine-Induced Killer Cells With PD-1 Blockade and ALK Inhibitor Showed Substantial Intrinsic Variability Across Non-Small Cell Lung Cancer Cell Lines. Front Oncol. 2022, 12, 713476. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.K.; Hamilton, C.A.; Cheung, M.K.; Karimi, M.; Baker, J.; Gall, J.M.; Schulz, S.; Thorne, S.H.; Teng, N.N.; Contag, C.H.; et al. Enhanced Killing of Primary Ovarian Cancer by Retargeting Autologous Cytokine-Induced Killer Cells with Bispecific Antibodies: A Preclinical Study. Clin. Cancer Res. 2006, 12, 1859–1867. [Google Scholar] [CrossRef] [PubMed]
- Kujawski, M.; Li, L.; Li, H.; Yazaki, P.J.; Swiderski, P.; Shively, J.E. T-cell surface generation of dual bivalent, bispecific T-cell engaging, RNA duplex cross-linked antibodies (dbBiTERs) for re-directed tumor cell lysis. Biotechnol. J. 2022, 17, e2100389. [Google Scholar] [CrossRef]
- Lee, H.K.; Kim, Y.G.; Kim, J.S.; Park, E.J.; Kim, B.; Park, K.H.; Kang, J.S.; Hong, J.T.; Kim, Y.; Han, S.B. Cytokine-induced killer cells interact with tumor lysate-pulsed dendritic cells via CCR5 signaling. Cancer Lett. 2016, 378, 142–149. [Google Scholar] [CrossRef]
- Cao, J.; Chen, C.; Wang, Y.; Chen, X.; Chen, Z.; Luo, X. Influence of autologous dendritic cells on cytokine-induced killer cell proliferation, cell phenotype and antitumor activity in vitro. Oncol Lett. 2016, 12, 2033–2037. [Google Scholar] [CrossRef]
- Jung, N.C.; Lee, J.H.; Choi, H.J.; Hwang, S.U.; Song, J.Y.; Seo, H.G.; Choi, J.; Jung, S.Y.; Han, S.G.; Lim, D.S. Dendritic Cell Immunotherapy Combined with Cytokine-Induced Killer Cells Effectively Suppresses Established Hepatocellular Carcinomas in Mice. Immunol Invest. 2016, 45, 553–565. [Google Scholar] [CrossRef]
- Yan, Y.; Xu, Y.; Zhao, Y.; Li, L.; Sun, P.; Liu, H.; Fan, Q.; Liang, K.; Liang, W.; Sun, H.; Du, X.; Li, R. Combination of E2F-1 promoter-regulated oncolytic adenovirus and cytokine-induced killer cells enhances the antitumor effects in an orthotopic rectal cancer model. Tumour Biol. 2014, 35, 1113–1122. [Google Scholar] [CrossRef]
- Liu, F.R.; Bai, S.; Feng, Q.; Pan, X.Y.; Song, S.L.; Fang, H. Anti-colorectal cancer effects of anti-p21Ras scFv delivered by the recombinant adenovirus KGHV500 and cytokine-induced killer cells. BMC Cancer. 2018, 18, 1087. [Google Scholar] [CrossRef]
- Dai, F.; Zhang, P.B.; Feng, Q.; Pan, X.Y.; Song, S.L.; Cui, J.; Yang, J.L. Cytokine-induced killer cells carrying recombinant oncolytic adenovirus expressing p21Ras scFv inhibited liver cancer. J Cancer. 2021, 12, 2768–2776. [Google Scholar] [CrossRef]
- Niu, J.; Ren, Y.; Zhang, T.; Yang, X.; Zhu, W.; Zhu, H.; Li, J.; Li, J.; Pang, Y. Retrospective comparative study of the effects of dendritic cell vaccine and cytokine-induced killer cell immunotherapy with that of chemotherapy alone and in combination for colorectal cancer. Biomed Res Int. 2014, 2014, 214727. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Yang, X.; Li, J.; Ren, Y.; Zhang, T.; Zhang, C.; Zhang, J.; Li, J.; Pang, Y. Immune response, safety, and survival and quality of life outcomes for advanced colorectal cancer patients treated with dendritic cell vaccine and cytokine-induced killer cell therapy. Biomed Res Int. 2014, 2014, 603871. [Google Scholar] [CrossRef] [PubMed]
- Gao, D.; Li, C.; Xie, X.; Zhao, P.; Wei, X.; Sun, W.; Liu, H.C.; Alexandrou, A.T.; Jones, J.; Zhao, R.; Li, J.J. Autologous tumor lysate-pulsed dendritic cell immunotherapy with cytokine-induced killer cells improves survival in gastric and colorectal cancer patients. PLoS One. 2014, 9, e93886. [Google Scholar] [CrossRef] [PubMed]
- Lin, T.; Song, C.; Chuo, D.Y.; Zhang, H.; Zhao, J. Clinical effects of autologous dendritic cells combined with cytokine-induced killer cells followed by chemotherapy in treating patients with advanced colorectal cancer: a prospective study. Tumour Biol. 2016, 37, 4367–4372. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Huang, L.; Chen, L.; Lin, X.; Chen, L.; Zheng, Q. Effect of dendritic cell-cytokine-induced killer cells in patients with advanced colorectal cancer combined with first-line treatment. World J. Surg. Oncol. 2017, 15, 209. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Qin, W.; Feng, H.; Song, D.; Yang, X.; Zhang, J. Analysis of the Clinical Efficacy of Dendritic Cell -cytokine Induced Killer Cell-based Adoptive Immunotherapy for Colorectal Cancer. Immunol Invest. 2021, 50, 622–633. [Google Scholar] [CrossRef] [PubMed]
- Dai, D.; Yin, Y.; Hu, Y.; Lu, Y.; Zou, H.; Lu, G.; Wang, Q.; Lian, J.; Gao, J.; Shen, X. Tumor RNA-loaded nanoliposomes increases the anti-tumor immune response in colorectal cancer. Drug Deliv. 2021, 28, 1548–1561. [Google Scholar] [CrossRef]
- Zhang, H.; Wang, S.; Sun, M.; Cui, Y.; Xing, J.; Teng, L.; Xi, Z.; Yang, Z. Exosomes as smart drug delivery vehicles for cancer immunotherapy. Front Immunol. 2023, 13, 1093607. [Google Scholar] [CrossRef]
- Xu, Y.; Ma, S.; Zhao, J.; Chen, H.; Si, X.; Huang, Z.; Yu, Z.; Song, W.; Tang, Z.; Chen, X. Mannan-decorated pathogen-like polymeric nanoparticles as nanovaccine carriers for eliciting superior anticancer immunity. Biomaterials. 2022, 284, 121489. [Google Scholar] [CrossRef]
- Gabel, M.; Knauss, A.; Fischer, D.; Neurath, M.F.; Weigmann, B. Surface Design Options in Polymer- and Lipid-Based siRNA Nanoparticles Using Antibodies. Int. J. Mol. Sci. 2022, 23, 13929. [Google Scholar] [CrossRef]
- Salomon, R.; Rotem, H.; Katzenelenbogen, Y.; Weiner, A.; Cohen Saban, N.; Feferman, T.; Amit, I.; Dahan, R. Bispecific antibodies increase the therapeutic window of CD40 agonists through selective dendritic cell targeting. Nat Cancer. 2022, 3, 287–302. [Google Scholar] [CrossRef] [PubMed]
- Park, S.H.; Breitbach, C.J.; Lee, J.; Park, J.O.; Lim, H.Y.; Kang, W.K.; Moon, A.; Mun, J.H.; Sommermann, E.M.; Maruri Avidal, L.; Patt, R.; Pelusio, A.; Burke, J.; Hwang, T.H.; Kirn, D.; Park, Y.S. Phase 1b Trial of Biweekly Intravenous Pexa-Vec (JX-594), an Oncolytic and Immunotherapeutic Vaccinia Virus in Colorectal Cancer. Mol Ther. 2015, 23, 1532–40. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Carbonero, R.; Salazar, R.; Duran, I.; Osman-Garcia, I.; Paz-Ares, L.; Bozada, J.M.; Boni, V.; Blanc, C.; Seymour, L.; Beadle, J.; et al. Phase 1 study of intravenous administration of the chimeric adenovirus enadenotucirev in patients undergoing primary tumor resection. J. Immunother. Cancer 2017, 5, 71. [Google Scholar] [CrossRef]
- Parakrama, R.; Fogel, E.; Chandy, C.; Augustine, T.; Coffey, M.; Tesfa, L.; Goel, S.; Maitra, R. Immune characterization of metastatic colorectal cancer patients post reovirus administration. BMC Cancer 2020, 20, 569. [Google Scholar] [CrossRef]
- Jonker, D.J.; Tang, P.A.; Kennecke, H.; Welch, S.A.; Cripps, M.C.; Asmis, T.; Chalchal, H.; Tomiak, A.; Lim, H.; Ko, Y.J.; Chen, E.X.; Alcindor, T.; Goffin, J.R.; Korpanty, G.J.; Feilotter, H.; Tsao, M.S.; Theis, A.; Tu, D.; Seymour, L. A Randomized Phase II Study of FOLFOX6/Bevacizumab With or Without Pelareorep in Patients With Metastatic Colorectal Cancer: IND 210, a Canadian Cancer Trials Group Trial. Clin Colorectal Cancer. 2018, 17, 231–239.e7. [Google Scholar] [CrossRef] [PubMed]
- Monge, C.; Xie, C.; Myojin, Y.; Coffman, K.; Hrones, D.M.; Wang, S.; Hernandez, J.M.; Wood, B.J.; Levy, E.B.; Juburi, I.; Hewitt, S.M.; Kleiner, D.E.; Steinberg, S.M.; Figg, W.D.; Redd, B.; Homan, P.; Cam, M.; Ruf, B.; Duffy, A.G.; Greten, TF. Phase I/II study of PexaVec in combination with immune checkpoint inhibition in refractory metastatic colorectal cancer. J Immunother Cancer. 2023, 11, e005640. [Google Scholar] [CrossRef]
- Fakih, M.; Harb, W.; Mahadevan, D.; Babiker, H.; Berlin, J.; Lillie, T.; Krige, D.; Carter, J.; Cox, C.; Patel, M.; et al. Safety and efficacy of the tumor-selective adenovirus enadenotucirev, in combination with nivolumab, in patients with advanced/metastatic epithelial cancer: a phase I clinical trial (SPICE). J. Immunother. Cancer 2023, 11, e006561. [Google Scholar] [CrossRef]
- Zhou, X.; Zhao, J.; Zhang, J.V.; Wu, Y.; Wang, L.; Chen, X.; Ji, D.; Zhou, G.G. Enhancing Therapeutic Efficacy of Oncolytic Herpes Simplex Virus with MEK Inhibitor Trametinib in Some BRAF or KRAS-Mutated Colorectal or Lung Carcinoma Models. Viruses. 2021, 13, 1758. [Google Scholar] [CrossRef]
- Maus, M.V. A decade of CAR T cell evolution. Nat Cancer. 2022, 3, 270–271. [Google Scholar] [CrossRef]
- Zhao, X.Y.; Jiang, Q.; Jiang, H.; Hu, L.J.; Zhao, T.; Yu, X.X.; Huang, X.J. Expanded clinical-grade membrane-bound IL-21/4-1BBL NK cell products exhibit activity against acute myeloid leukemia in vivo. Eur J Immunol. 2020, 50, 1374–1385. [Google Scholar] [CrossRef]
- Mani, R.; Rajgolikar, G.; Nunes, J.; Zapolnik, K.; Wasmuth, R.; Mo, X.; Byrd, J.C.; Lee, D.A.; Muthusamy, N.; Vasu, S. Fc-engineered anti-CD33 monoclonal antibody potentiates cytotoxicity of membrane-bound interleukin-21 expanded natural killer cells in acute myeloid leukemia. Cytotherapy. 2020, 22, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Mailankody, S.; Devlin, S.M.; Landa, J.; Nath, K.; Diamonte, C.; Carstens, E.J.; Russo, D.; Auclair, R.; Fitzgerald, L.; Cadzin, B.; et al. GPRC5D-Targeted CAR T Cells for Myeloma. New Engl. J. Med. 2022, 387, 1196–1206. [Google Scholar] [CrossRef] [PubMed]
- Guzman, G.; Reed, M.R.; Bielamowicz, K.; Koss, B.; Rodriguez, A. CAR-T Therapies in Solid Tumors: Opportunities and Challenges. Curr. Oncol. Rep. 2023, 25, 479–489. [Google Scholar] [CrossRef] [PubMed]
- Chmielewski, M.; Abken, H. TRUCKs: the fourth generation of CARs. Expert Opin. Biol. Ther. 2015, 15, 1145–1154. [Google Scholar] [CrossRef]
- Feng, Z.; He, X.; Zhang, X.; Wu, Y.; Xing, B.; Knowles, A.; Shan, Q.; Miller, S.; Hojnacki, T.; Ma, J.; Katona, B.W.; Gade, T.P.F.; Schrader, J.; Metz, D.C.; June, C.H.; Hua, X. Potent suppression of neuroendocrine tumors and gastrointestinal cancers by CDH17CAR T cells without toxicity to normal tissues. Nat Cancer. 2022, 3, 581–594. [Google Scholar] [CrossRef]
- Magee, M.S.; Abraham, T.S.; Baybutt, T.R.; Flickinger, J.C. Jr; Ridge, N.A.; Marszalowicz, G.P.; Prajapati, P.; Hersperger, A.R.; Waldman, S.A.; Snook, A.E. Human GUCY2C-Targeted Chimeric Antigen Receptor (CAR)-Expressing T Cells Eliminate Colorectal Cancer Metastases. Cancer Immunol Res. 2018, 6, 509–516. [Google Scholar] [CrossRef]
- Sureban, S.M.; Berahovich, R.; Zhou, H.; Xu, S.; Wu, L.; Ding, K.; May, R.; Qu, D.; Bannerman-Menson, E.; Golubovskaya, V.; Houchen, C.W. DCLK1 Monoclonal Antibody-Based CAR-T Cells as a Novel Treatment Strategy against Human Colorectal Cancers. Cancers (Basel). 2019, 12, 54. [Google Scholar] [CrossRef]
- Olivera, I.; Bolaños, E.; Gonzalez-Gomariz, J.; Hervas-Stubbs, S.; Mariño, K.V.; Luri-Rey, C.; Etxeberria, I.; Cirella, A.; Egea, J.; Glez-Vaz, J.; Garasa, S.; Alvarez, M.; Eguren-Santamaria, I.; Guedan, S.; Sanmamed, M.F.; Berraondo, P.; Rabinovich, G.A.; Teijeira, A.; Melero, I. mRNAs encoding IL-12 and a decoy-resistant variant of IL-18 synergize to engineer T cells for efficacious intratumoral adoptive immunotherapy. Cell Rep Med. 2023, 4, 100978. [Google Scholar] [CrossRef]
- Milone, M.C.; Xu, J.; Chen, S.J.; Collins, M.A.; Zhou, J.; Powell, D.J. Jr; Melenhorst, J.J. Engineering enhanced CAR T-cells for improved cancer therapy. Nat Cancer. 2021, 2, 780–793. [Google Scholar] [CrossRef]
- Drougkas, K.; Karampinos, K.; Karavolias, I.; Koumprentziotis, I.A.; Ploumaki, I.; Triantafyllou, E.; Trontzas, I.; Kotteas, E. Comprehensive clinical evaluation of CAR-T cell immunotherapy for solid tumors: a path moving forward or a dead end? J Cancer Res Clin Oncol. 2023, 149, 2709–2734. [Google Scholar] [CrossRef]
- Kim, R.D.; Prenen, H.; Rottey, S.; Kim, D.W.; Flament, A.; Lehmann, F.; Van Cutsem, E. KEYNOTE-B79 phase 1b trial to evaluate the allogeneic CAR T-cells CYAD-101 and pembrolizumab in refractory metastatic colorectal cancer patients. J. Clin. Oncol. 2022, 40, TPS227–TPS227. [Google Scholar] [CrossRef]
Figure 3.
Detailed treatment protocol.
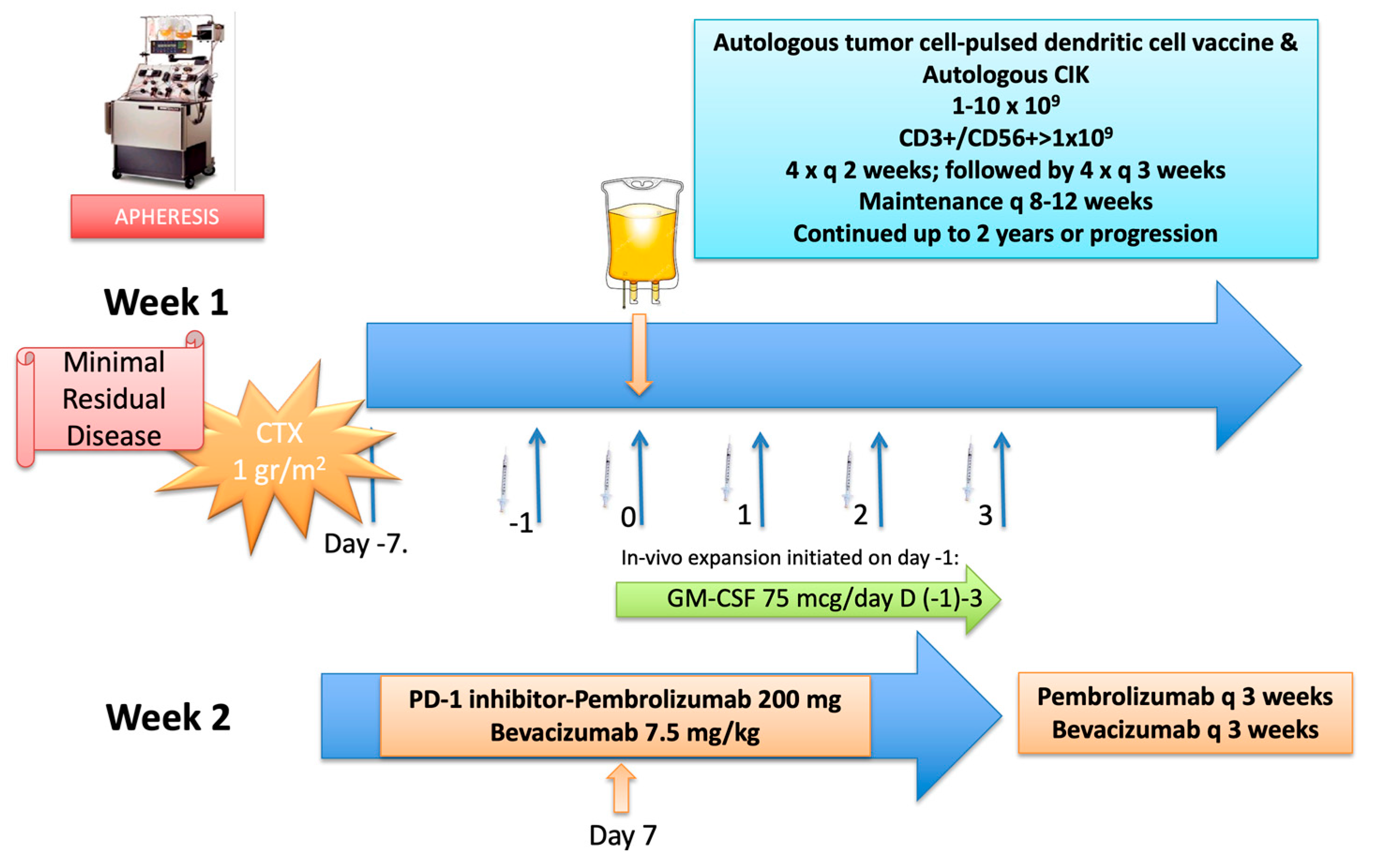

Table 1.
Selected clinical trials with cancer vaccines in gastric and esophageal cancers.
| Vaccine type | Intervention/ neoantigen | Adjuvant / Combined Tx | Stage | Design | Outome measures | Status | Phase | Reference |
|---|---|---|---|---|---|---|---|---|
| B-cell & Monocyte | BVAC-B (Her-2) |
none | IV | Her2 (+) GC, 0,4,8, 12 wks | Establish MTD, AE | completed | Ib | NCT03425773 Cellid Co, Ltd. |
| Allogeneic | K562-GM | Cyclophosphamide Celecoxib |
NED/MRD Primary site |
Esophagus & Mediastinal after standard Tx;6 vaccines q4 wks | AE, humoral immune response | Terminated (futility) | Ib | NCT01143545 NCI |
| mRNA | personalized | none | IV | Esophageal, GC, CRC; 4 vaccines SC |
AE, DCR, PFS, TTP, OS | Unknown | Ib | NCT03468244 Chanhai Hospital, China |
| B-cell epitope | Her-2 | CT (Cisplatin-FU/Capecitabine) |
IV | Her2 (+) GC/GE D1,14,28 vaccine vs CT + vaccine |
AE, ORR, humoral immune response | Ongoing | Ib | NCT05315830 Bengbu Med College, China |
| MVB-BN non-replicating viral |
TAEK-VAC-Herby encoding Her-2, CD40L, TF Brachyury |
Trastuzumab Pertuzumab |
IV | Her2 (+) GC/GE, Breast, Chordoma 3 vaccines q3 wks |
DLT | Ongoing | Ib/II | NCT04246671 Bavarian Nordic |
| T-cell receptor | KK-LC1 neoantigen HLA-A-01:01 restricted |
2 x prior CT & IL-2 4 days & Cyclophosphamide (D-6, -5) + Fludarabine (D-6—2) |
IV | KK-LC1 (+) GC, breast, lung cancer 1 vaccine infusion |
DLT | Ongoing | I | NCT05035407 NCI |
| mRNA | PGV-002 Personalized mRNA |
PD-1/PD-L1 (expansion phase) | IV | GC, esophageal, liver cancer refractory to standard CT | AE, ORR, MTD, PFS | Ongoing | I | NCT05192460 Chinese Academy of MMS NeoCura |
| Peptide | Personalized | Pembrolizumab, Cyclophosphamide (D-3), GM-CSF (D 1,4,8, 15) q 3 wks | III -IV | GC/GEJ, breast, NSCLC, HCC, Merkel, GU | AE, ORR, feasibility, humoral immune response | Ongoing | I | NCT05269381 Mayo Clinic |
| Peptide (Da VINci) |
OTSGC-A24 Multiple epitope |
Nivolumab, Ipilimumab | IV | GC; refractory | AE, ORR, humoral immune response | Ongoing | Ib | NCT03784040 Natl. Uni Hospital, Singapore |
| Peptide | iNEO-Vac-P01 Personalized |
GM-CSF | II-III maintenance |
Esophageal, resectable, after resection & (neo)/adj CT+PD-1 7 vaccines D1-82 |
AE, RFS, OS, QoL | Ongoing | I | ZheJiang Uni; Hangzhou Neoantigen Ther Co, Ltd |
| mRNA | Personalized | none | IIIC -IV | Esophageal ca; NSCLC Failure of standard Tx |
AE, ORR, TTP, PFS | Ongoing | NA | NCT03908671 Zhengzhou Uni; Stemirna Ther |
| Adenoviral Self-replicating mRNA |
GRT-C901 & R902 (predicted multiple epitopes) |
Nivolumab Ipilimumab |
IV | GE/G ≤ 1 prior CT |
AE, ORR, dose finding | Ongoing | Ib | NCT03639714 Gritstone Bio, Inc |
(Abbreviations: HLA: human leucocyte antigen; Tx: treatment; CT: chemotherapy; GM-CSF: granulocyte macrophage colony stimulating factor; FU: 5-fluorouracil; NED: no evidence of disease; MRD: minimal residual disease; D: day; wks: weeks; GC: gastric cancer; CRC: colorectal cancer; NSCLC: non-small cell lung cancer; HCC: hepatocellular carcinoma; GU; genitourinary carcinoma; SC: subcutaneous; neo/adj CT: neoadjuvant / adjuvant chemotherapy; PD-1; programmed death-1; MTD: maximal toxic dose; AE: adverse effects; DCR: disease control rate; PFS: progression-free survival; RFS: relapse-free survival; TTP: time to progression; OS: overall survival; ORR; overall response rate; DLT: dose limiting toxicity; QoL: quality of life).
Table 2.
Selected clinical trials with cancer vaccines in colorectal cancer.
| Vaccine type | Intervention/ neoantigen | Adjuvant / Combined Tx | Stage | Design | Outome measures | Status | Phase | Reference |
|---|---|---|---|---|---|---|---|---|
| Adenoviral Self-replicating mRNA |
GRT-C901 & R902 (predicted multiple epitopes) |
Nivolumab Ipilimumab |
IV | CRC-MSS; GC/GEJ; NSCLC; GU1 prior CT | AE, ORR, dose finding, Humoral immune response |
Completed | Ib/II | NCT03639714 Gritstone Bio, Inc |
| Adenoviral Self-replicating mRNA |
GRT-C901 & R902 (predicted multiple epitopes) |
Atezolizumab Ipilimumab |
II-III; MRD (ctDNA (+)) | CRC-MSS; Resected, after adj CT; 6 x vaccine 2x Ipilimumab; 13x Atezolizumab q4 wks |
AE, ORR (ctDNA); RFS, OS) | Terminated; reprioritization | II | NCT05456165 Gritstone Bio, Inc |
| Dendritic cell | Personalized Antigen pulsed DC |
mFOLFOX6 | IV | Untreated mCRC; CT vs CT+vac Vaccination in cycles 1-3; 7-9 |
PFS, OS, ORR | Unknown | III | NCT02503150 Second MMU, China |
| Adenovirus | QUILT-2.004 Ad-CEA |
Avelumab CT (FOLFOX) Bevacizumab |
IV | Untreated mCRC-MSS; CT (FOLFOX+Bevacizumab) vs CT+ Avelumab + vaccine x 12 | PFS | Terminated; Futility on interim analysis |
II | NCT03050814 NCI |
| Viral (modified vaccinia Ankara- Bavarian Nordic) | CV 301 MVA-BN CEA/MUC1 & Fowlpox booster |
Bifunctional fusion protein composed of IgG1 PD-L1 & TGF-beta; IL-15 fusion protein IL-12 |
IV | mCRC; small bowel ca. Triple vs quadruple Tx (± IL12) |
AE, ORR; PFS; OS | Completed | II | NCT04491955 NCI |
| Autologous | Cryovax; Personalized autologous tumor |
Bioengineered allogenic immunecells (AlloStim) | IV | >2 previous lines of CT; Vaccine x6 over 10 wks |
DLT, QoL, Humoral immune response; ORR |
Completed | II | NCT02380443 Immunovative Therapies Ltd. |
| Allogenic engineered | GVAX whole tumor cell engineered to secrete GM-CSF | Cyc Guadecitabine |
IV | mCRC; stable on 1-2nd Line CT; Vaccine x 1 q 4 wks |
AE; TIL; PFS | Completed | I | NCT01966289 Sydney Kimmel Cancer Center |
| Peptide | PolyPEPI1018 Six sythetic CTA neoantigens |
TAS 102 | IV | mCRC-MSS; prior CTVaccine q2 weeks x 7 doses | AE, PFS, ORR; OS | Completed | I | NCT05130060 Mayo clinic |
| mRNA | mRNA 5671/V941-001 | Pembrolizumab | IV | mCRC- KRASm-MSS; NSCLC; Pancreas Vaccine q 3 wks 9 doses vs Vaccine + Pembrolizumab |
AE, DLT | Completed | I | NCT03948763 Merck Sharp & Dohme LLC |
| Synthetic peptide | Her-2 & CEA HLA A2 / A3 restricted |
GM-CSF Tetanus toxioid Montanide ISA 51 |
II-IV | CRC | AE; T cell response in lymph node | Terminated Slow accrual |
I | NCT00091286 University of Virginia |
| Alphavirus replicon particles | AVX 701 CEA |
none | III | CRC; After adjuvant CT Vaccine x4 q 3 wks |
AE; Humoral immune response | Completed | I | NCT01890213 Duke University |
| Inactivated virus | Influenza vaccine | none | Early, operable | CRC; intratumoral injection x 1 | AE, local immune responses | Completed | II | NCT04591379 Zealand University |
| Plasmid DNA | MYPHISMO Tet-MYB |
BGB-A317 (Anti-PD-1 IgG4 mab) | IV | mCRC, ACC; refractory; Vaccine x 6 q 7d |
AE, ORR; CBR, PFS | Completed | I | NCT03287427 Peter Mc Callum Cancer Centre, Au |
| Adenoviral Self-replicating mRNA |
GRANITE-GRT-C901 & R902 (predicted multiple epitopes) |
Atezolizumab Ipilimumab 5-FU Bevacizumab |
IV | mCRC; maintenace following 1st L CT (FOLFOX-Bevacizumab) | Molecular response; PFS |
Ongoing | II/III | NCT05141721 Gritstone Bio; Inc |
| Liposomal | StimVax; MUC-1 |
AlloStim; Allogenic immune cells |
IV | mCRC-MSS; >2 previous lines of CT; Vaccine 3 cycles (x 5/wk q 6 wks) |
AE, OS | Ongoing | IIb | NCT04444622 Immunovative Ther, LTD |
| Dendritic cell | Personalized neoantigen | Nivolumab | IV; MRD | mCRC; resected liver met; HCC Vaccine x 10 doses q 2wks |
RFS, Humoral immune response | Ongoing | II | NCT04912765 Natl Cancer Centre, Singapore |
| Peptide | Personalized synthetic neoantigen | Pembrolizumab Imoquimod Sotigolimab |
mCRC; any line; Pancreas ca; Vaccine x 7-11 dose q 2 wks |
AE, Feasibility, ORR; PFS; OS | Ongoing | I | NCT02600949 MD Anderson Cancer Center |
|
| Chimeric recombinant protein; Recombinant viral |
KISIMA-01; ATP-128-Three neoantigens+ TLR agonist; VSV-GP128-booster |
Ezabenlimab (anti-PD-1) | IV | mCRC-MSS; 1st Line CT; refractory; liver-only |
AE, PFS; ORR; MTD; RFS |
Ongoing | I/II | NCT04046445 Amal Ther. |
| Peptide | KRAS peptide | Nivolumab Ipilimumab |
IV | mCRC; pancreas; >2 previous lines of CT; Vaccine x 3 q 7 d; x 5 boosters q 8 wks |
AE; humoral immune response; DFS; ORR; PFS; OS | Ongoing | I/II | NCT04117087 Sydney Kimmel Cancer Center |
| Peptide | PolyPEPI1018 7 peptide noeantigens; Montanide |
Atezolizumab | IV | mCRC-MSS >2 previous lines of CT; |
AE, ORR; PFS; OS; Humoral immune response |
Ongoing | II | NCT05243862 Treos Bio Ltd. |
| Yeast cell particles |
PalloV-CRC; Allogenic tumor cells delivered on yeast cell particles |
none | I-IV | CRC prior to surgery Vaccine x 4 q 4 wks |
AE; humoral immune response | Ongoing | I | NCT03827967 Cancer Insight, LLC |
| Dendritic cell | COREVAX-1; Dendritic cells pulsed with autologous tumor cells |
IL-2 (D3-7) | IV; MRD | mCRC; Following resection | AE; humoral immune response; RFS; OS |
Ongoing | II | NCT02919644 Instituto Scientifico Romagnolo per lo Studio e la cura dei Tumori |
| Peptide | CLAUDE; EO2040; TAA-CD8 / CD4 T cell epitopes |
Montanide Nivolumab |
II-IV; MRD (ct-DNA (+) | mCRC; Following resection & standard Tx | ORR at 6 months; AE; DFS; OS | Ongoing | II | NCT05350501 Enterome |
| Lipid conjugated oligonucleotide & peptide | ELI-002; KRAS / NRAS |
none | MRD; ct-DNA (+) | mCRC; pancreatic; NSCLC; Vaccine x 4 q 7 d; x 8 boosters/4 wks |
Ct-DNA clearance; RFS; OS | Ongoing | I/II | NCT05726864 Elicio Ther |
| Adenovirus | Tri-AD5 Trivalent CEA/MUC-1/Brachyury | nogapendekin alfa inbakicept (IL-15 agonist-fusion protein) | Prevention | Lynch Syndrome; colon adenomas & CRC NED; Vaccine x 4 (wks 0,4,8,52) |
Cumulative incidence of adenomas; extracolonic carcinomas; humoral immune responses | Ongoing | IIb | NCT05419011 NCI |
| Adenovirus | Nous-209; Gad-209-FSP priming; MVA-209-FSP booster |
None | Prevention | gLynch Syndrome; NED after non-sporadic MMRd malignant tumors; Vaccine D1 / booster wk 8 |
AE; humoral immune responses; response in colorectal adenomas; incidence of Lynch-associated carcinomas | Ongoing | I/II | NCT05078866 NCI |
(Abbreviations: DC: dendritic cell; CEA: carcinoembryonic antigen; MUC: mucin; KRAS: kirsten rat sarcoma virus; NRAS: neuroblastoma ras viral oncogene homolog; Tx: treatment; CT: chemotherapy; GM-CSF: granulocyte macrophage colony stimulating factor; FOLFOX: oxaliplatin-5-fluorouracil infusion-leucovorin; wk: week; d: days; IL: interleukin; NED: no evidence of disease; MRD: minimal residual disease; ct-DNA (+): circulating tumor DNA; wks: weeks; GC: gastric cancer; GEJ: cancer involving distal osephageal; cardia; proximal gastric areas; CRC: colorectal cancer; mCRC : metastatic CRC; CRC-MSS: microsatellite stable CRC; NSCLC: non-small cell lung cancer; HCC: hepatocellular carcinoma; GU; genitourinary carcinoma; gLynch: germline Lynch; MMRd: mismatch repair deficient; SC: subcutaneous; neo/adj CT: neoadjuvant / adjuvant chemotherapy; PD-L1; programmed death ligand-1; MTD: maximal toxic dose; AE: adverse effects; CBR: clinical benefit rate; DCR: disease control rate; PFS: progression-free survival; RFS: relapse-free survival; TTP: time to progression; OS: overall survival; ORR; overall response rate; DLT: dose limiting toxicity; QoL: quality of life).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



