
Submitted:
12 September 2023
Posted:
13 September 2023
You are already at the latest version
Abstract
Atrial fibrillation (AF) is an increasingly recognized comorbidity in patients with can-cer. Indeed, cancer patients have a significantly higher incidence of AF than that ob-served in the general population. A reciprocal relationship between these two diseases has been observed, as much as some assume AF as a marker for occult cancer screen-ing, especially in older adults. The pathophysiological mechanisms are many and var-ied, including the underlying pro-inflammatory state, specific treatments (chemo and radiotherapy) and surgery. The therapeutic management of patients with cancer and AF involves the same rhythm and frequency control strategies as the general popula-tion; however, the numerous interactions with chemotherapeutics, which lead to a sig-nificant increase in side effects, as well as the extreme fragility of the patient should be considered. Anticoagulant therapy is also a complex challenge to address, as bleeding and stroke risk scores have not been fully assessed in this subpopulation. Furthermore, in large studies establishing the efficacy of direct oral anticoagulants (DOACs), cancer patients have been underrepresented. In this review, we elaborate on mechanisms linking AF to cancer patients with a particular focus on therapeutic challenges in this population.
Keywords:
atrial fibrillation
; management
; cardio-oncology
1. Introduction and Epidemiology: Atrial Fibrillation in Cancer Patients
The improvement in cancer patients’ prognosis and therefore the aging of this population, as well as the introduction of targeted therapies, have exponentially increased the incidence of cardiac arrhythmias seen in oncology and hematology wards (1;2). In particular, AF, a leading cause of thrombotic morbidity and overall cardiovascular (CV) mortality, is the most common sustained arrhythmia in the general population and revealed to be more common in patients with malignancies (1-3), reaching an incidence of 30% in available studies (1-3). In this setting, prevalence seems extremely variable in literature, depending on the age of population examined, pre-existing risk factors, type of primitive cancer, previous oncologic surgery and chemotherapy schemes instituted (4-7). Indeed, the risk of AF is higher in subjects older than 65 years with known CV disease (4-7), as well as in those patients affected by all hematologic malignancies, including lymphoma, leukemia and multiple myeloma rather than solid tumors (8). Moreover, higher cancer stages and grades at diagnosis raise the risk of AF, even suggesting a systemic effect of advanced cancer itself on the heart (7). Of importance, post-operative AF is the most frequent form of sustained arrhythmia in cancer patients. Its prevalence ranges from 16 to 46% for cardiothoracic surgery and 0.4–12% in non-cardiothoracic surgery, increasing post-operative mortality, hospitalization length and intensive care unit admissions (9;10). AF may therefore represent an additional determinant of malignancies’ prognosis and a challenge for the therapeutic management of cancer patients (11;12). The aim of this review is hence to elucidate novel etiological aspects subtending AF occurrence in this population, to give advice on management aspects and shed light on future research scopes in this expanding field of cardio-oncology.
2. Risk factor and pathogenesis of atrial fibrillation in cancer patients
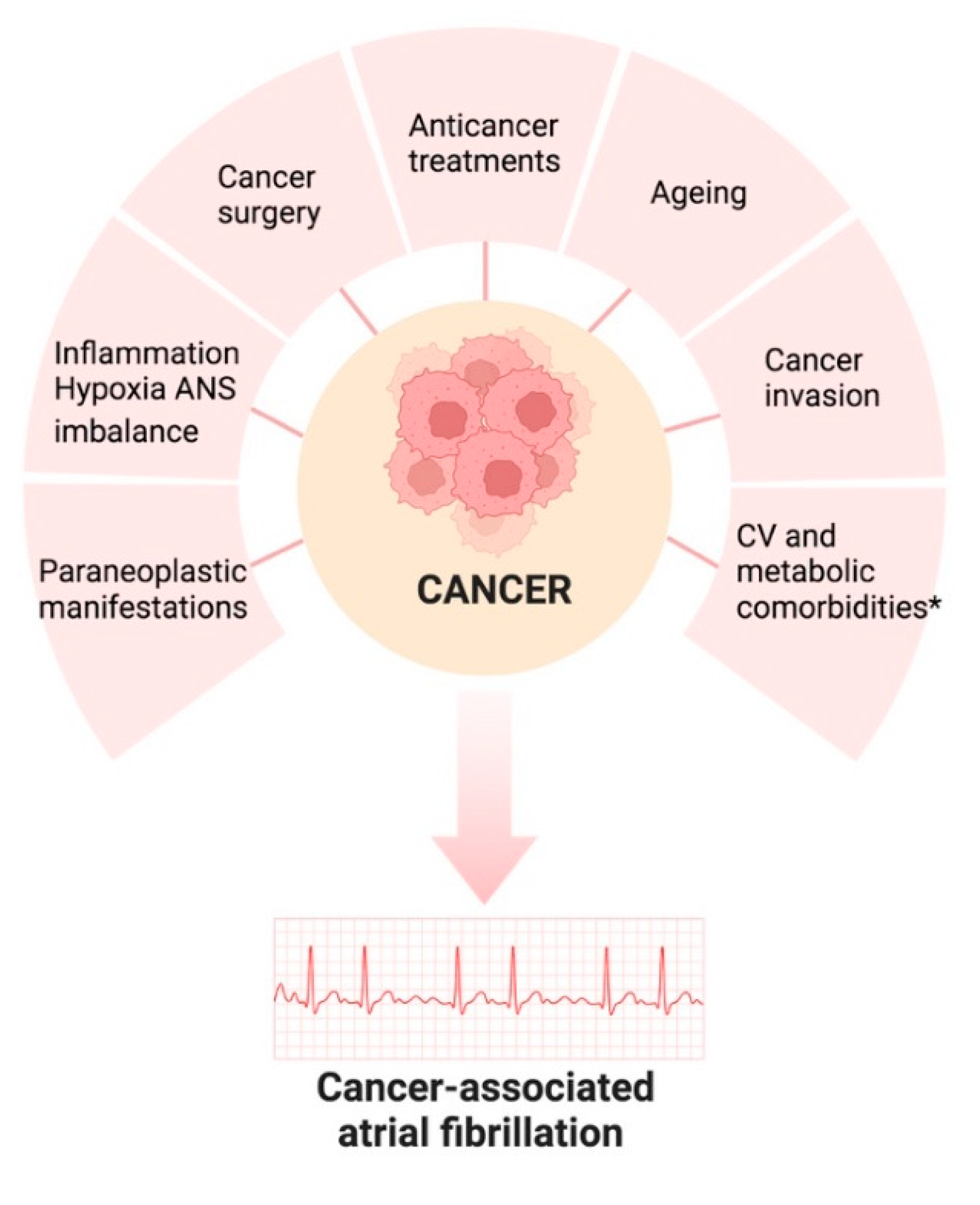
To date, inflammation-related oxidative stress in cancer is believed to cause electrical and anatomical changes that predispose and maintain AF, including through fibrosis. C-reactive protein (CRP), interleukins (IL), in particular IL-2, IL-6 and IL-8, macrophage migration inhibition factor (MIF) and tumour necrosis factor alpha are all elevated in AF and cancer patients (13). Increased inflammatory markers can lead to autonomic dysfunction, electrolyte imbalances, structural alterations of the heart and electrical remodelling. Alterations in calcium haemostasis and connexins can cause a number of atrial conduction abnormalities, including AF (14). A causal role of inflammation in AF has been suggested by studies showing increased activation of the NLRP3 inflammasome ((NACHT, LRR, and PYD domain containing protein 3) in AF (15). NLRP3 inflammasome mediates caspase-1 activation and interleukin-1β release in immune cells, this interleukin is increased in cancer patients also promoting AF onset. The neoplasm-related pro-inflammatory state also includes an increase in reactive oxygen species (ROS), which are a by-product of increased cell metabolism and can promote atrial fibrosis and remodelling of the extracellular matrix of the atrium through activation of metalloproteinases (16,17) In summary, inflammation plays a central role in the development and progression of cancer and thus subsequently in the trigger or maintenance of AF. More research is needed to determine the role of anti-inflammatory therapies in cancer prevention or therapies, as well as AF (18).Many anticancer drugs have been associated with an increased risk of AF both in terms of incident and recurrent AF. Cancer drug- induced AF may occur shortly after treatment (cisplatin or gemcitabine) or weeks or months after starting treatment, as in the case of ibrutinib (10). Tyrosine kinase inhibitors (TKI), immunomodulators like interleukin-2 (IL-2), antimetabolites like 5-fluorouracil and gemcitabine, HER-2/Neu receptor blockers, alkylating agents, anthracyclines and antimicrotubular agents have all been related to the development of new-onset AF. Ibrutinib is a Bruton TKI used to treat a variety of B-cell malignancies. It is the TKI most linked to an increased risk of AF, with up to 16% of patients developing AF after starting therapy (19). Off-target inhibition of other tyrosine kinases in cardiac myocardial cells may be the mechanism underlying the development of AF in patients (20). Ibrutinib, for example, has been shown to inhibit C-terminal Src kinase. A knockout mouse model lacking C-terminal Src kinase was found to induce left atrial enlargement, fibrosis, and inflammation, resulting in increased AF. Furthermore, ibrutinib may cause AF by producing ROS (21). Immune checkpoint inhibitors are also commonly used to treat specific types of cancer and have been linked to cardiotoxicity, myocarditis, and AF caused by altered inflammation. Surgical procedures such as lung resection or other extensive operations are also often followed by peri-operative AF. In a cohort of 13,906 patients undergoing lung resection for lung cancer, perioperative AF occurred in 12.6 % of patients (22). Perioperative AF appears to be more frequent in patients with advanced age and stage of cancer who have cardiovascular comorbidities and who undergo extensive resections (23). Furthermore, high adrenergic states following cancer surgery may induce or worsen AF (14). Infection, anaemia, hypoxia, pleurisy, pericarditis and cardiomyopathy are all potential complications of cancer and cancer treatment and all are potential triggers of AF (24). More rarely, AF may be triggered by metastatic involvement of the heart. (10). The most common neoplasms associated with cardiac metastases are lung cancer, lymphoma, breast cancer, leukaemia, stomach cancer and melanoma (25). Cardiac metastases mostly appear in elderly patients already with disseminated cancer disease. Tumours may reach the heart by lymphatic or intravenous route, or by direct extension, and the sites most affected are the pericardium or epicardium (26). There is a growing understanding of shared risk factors that may be responsible for the development or progression of cancer and AF. Modifiable risk factors for such as hypertension and obesity continue to be underdiagnosed and undertreated in cancer patients (27). To improve long-term outcomes in cancer patients, early diagnosis via standardized risk-based screening and management of these conditions in accordance with general ESC Guidelines is recommended. (28)
Figure 1.
Pathogenesis of atrial fibrillation associated with cancer. ANS, autonomic nervous system. CV, cardiovascular; * Obesity, hypertension, DM, CVDs (HF, VHD, IHD, cardiomyopathies, cardiac amyloidosis), .
Figure 1.
Pathogenesis of atrial fibrillation associated with cancer. ANS, autonomic nervous system. CV, cardiovascular; * Obesity, hypertension, DM, CVDs (HF, VHD, IHD, cardiomyopathies, cardiac amyloidosis), .
4. Management of Atrial Fibrillation in the setting of Cancer
4.1. Rate and Rhythm control
Although the management of AF in patients with cancer should follow the 2020 European Society of Cardiology (ESC) guidelines on AF and the ‘ABC pathway’ approach should be applied there are some exceptions where treatment modifications should be considered (38,39).
Among rate-control drugs, beta-blockers are preferred, especially if the cancer therapies have a potential cardiac dysfunction risk. Calcium channel blocker (diltiazem and verapamil) should be avoided if possible due to drug-drug interactions and negative inotropic effects. The same applies to digoxin, which is to be considered a second choice (11).
The decision to convert AF to sinus rhythm (rhythm control) is made individually for each patient. For older adults, who are especially vulnerable to the side effects of antiarrhythmic medications, there is less emphasis on rhythm control. Rhythm control may be indicated in patients who are significantly symptomatic from AF or whose AF is difficult to rate control (40). To convert AF to sinus rhythm, both electrical and pharmacologic methods can be used. For unstable patients (altered mental status, hypotension, chest pain or hypoxia attributed to arrythmia), emergency electrical cardioversion is the first-line therapy. Flecainide and Propafenone are anti-arrhythmic medications that are frequently used for pharmacologic cardioversion. However, many older adults, including those with cancer, have underlying structural heart disease, which restricts the use of these therapies in this group due to its increased pro-arrhythmic effects (41).
Although amiodarone is effective in maintaining sinus rhythm, it has greater toxicities than other antiarrhythmics used in AF. There is a strong temporal relationship between therapy with taxanes, such as paclitaxel and docetaxel, used for the treatment of many cancers, such as breast and lung cancer, and the development of severe skin and mucosal toxicity due to reduced clearance of taxanes in patients taking amiodarone (42). Amiodarone has also been shown to increase the adverse effects of radiation on the skin and mucous membranes (43). In older adults with a normal QTc interval, sotalol, a class III antiarrhythmic agent, may be a good choice for maintaining sinus rhythm (31). However several anti-cancer treatments, may contribute to QTc prolongation, which can lead to life-threatening ventricular arrhythmias (44). Kinase inhibitors, such as dasatinib and ruxolitnib, used to treat chronic myeloid leukemia and myelofibrosis, may cause QTc interval prolongation. Arsenic trioxide, which is used to treat promyelocytic leukemia, may also cause QTc interval prolongation. Some anti-emetic drugs, such as ondansetron, which is commonly used in cancer patients to prevent and treat nausea, may also contribute to QTc prolongation (45). The possibility of ablation of atrial fibrillation should be discussed in selected patients with heart failure (HF) and uncontrolled symptoms, taking into account cancer status and prognosis (46). In a retrospective study, ablation of AF in patients with cancer in the preceding 5 years or with exposure to anthracyclines and/or thoracic radiation at any time prior to index ablation was analysed in comparison with patients with no history of cancer. The primary outcome was freedom from atrial fibrillation (with or without antiarrhythmic drugs , or the need to repeat catheter ablation at 12 months after first procedure of ablation). Freedom from atrial fibrillation at 12 months was not different in the two comparison groups and the need to repeat ablation was also similar between the groups (20.7% vs 27.5%, p 0.29) (47). In addition, there were no differences in safety endpoints between the groups with regard to the risk of bleeding. However, data on ablation in cancer patients are still limited. Finally, if the above-mentioned strategies fail to control AF, AV node ablation with permanent pacing should be considered to alleviate symptoms and haemodynamic effects of refractory AF (48).
4.2. Anticoagulant treatment:
a) Risk benefit decision about anticoagulation: Ischaemic and bleeding risk
Anticoagulant therapy is a complex challenge, as cancer patients present both a high thrombotic and haemorrhagic risk. According to the ESC guidelines, the therapeutic decision should be based on both the CHA 2 DS 2 -Vasc (Congestive heart failure, Hypertension, Age ≥ 75 years [2 points], Diabetes mellitus, Stroke [2 points]-Vascular disease, Age 65-74 years, Sex category [female]) score and on haemorrhagic risk scores such as HASBLED (Hypertension, Abnormal renal and liver function, Stroke, Bleeding Labile international normalized ratio, Elderly, Drugs or alcohol); although these have not been validated in cancer patients (table 1) (31,32, 49). In a retrospective cohort study including 2,435,541 adults hospitalised with AF the predictive value of the CHA2DS2-VASc score was lower in patients with cancer than in those without . In another retrospective cohort study, patients with AF and cancer and with AF without cancer were compared. Both groups had a CHA2DS2-VASc score of 0 to 2 and were not receiving anticoagulation at the diagnosis of cancer or at the date of inclusion in the study. The primary outcome was the risk of arterial thromboembolism (ischaemic stroke, transient ischaemic attack or systemic arterial thromboembolism) at 12 months. The 12-month cumulative incidence of arterial thromboembolism was 2.13% (95% CI: 1.47-2.99) in 1,411 AF patients with cancer and 0.8% (95% CI: 0.56-1.10) in 4,233 AF patients without cancer (HR: 2.70; 95% CI: 1.65-4.41). The risk was higher in men with CHA2DS2-VASc = 1 and in women with CHA2DS2-VASc = 2 (HR: 6.07; 95% CI: 2.45-15.01) (50). Although cancer is not mentioned in the CHA2DS2-VASc score, the latter is associated with a propensity to thrombosis (51). Regarding the assessment of bleeding risk, the HAS BLED was quite accurate (52) although the HEMORR2HAGES score also includes a history of malignancy and thrombocytopenia in the risk assessment (table 2) (53). The latter is an important finding as it has been shown that platelets < 100,000 × 10 9/L increase the risk of bleeding for cancer patients taking anticoagulants and tumours together with cancer treatments may cause thrombocytopenia (54,18). Farmakis et al proposed an alternative approach for risk stratification including: The acronyms T (thrombotic risk), B (bleeding risk), I (drug interactions), and P (patient access and preferences) (55). This algorithm guides the clinician in adopting an appropriate therapy based on a comprehensive assessment of all aspects of the cancer patient (Figure 2).

Table 1.
HAS BLED score. A score of ≥3 indicates "high risk" and some caution and regular review of the patient is needed. TTR, Time in Therapeutic Range.
Table 1.
HAS BLED score. A score of ≥3 indicates "high risk" and some caution and regular review of the patient is needed. TTR, Time in Therapeutic Range.
| Points | Condition | |
|---|---|---|
| H -Hypertension | 1 | Systolic blood pressure > 160 mmHg |
| A -Abnormal liver or renal function | 1 each | Abnormal renal function: dialysis, creatinine > 2.3 mg/dL,transplantation. Abnormale liver function: chornic hepatitis, cirrhosis, bilirubin > 2 ULN, ALT > 3 ULN |
| S -Stroke | 1 | Previous history, particularly lacunar |
| B - Bleeding | 1 | Recent bleed, anemia, etc |
| L -Labile INR | 1 | Unstable/high INR or TTR < 60% |
| E - Eldery | 1 | Age > 65 year, extreme frailty |
| D -Drugs or Alcohol | 1 each | Prior Alcohol or Drug Usage History (≥ 8 drinks/week) Drugs: concomitant antiplatelet, or NSAID use, etc.. |
Table 2.
HEMORR2HAGES score. Patients with a score of 0 or 1 were classified as low-risk, 2 or 3 intermediate-risk, ≥4 high-risk.
Table 2.
HEMORR2HAGES score. Patients with a score of 0 or 1 were classified as low-risk, 2 or 3 intermediate-risk, ≥4 high-risk.
| Points | ||
|---|---|---|
| H –Hepatic or Renal disease | 1 each | |
| E – Ethanol Abuse | 1 | |
|
M-Malignancy History |
1 | |
|
O-Older (Age > 75) |
1 | |
|
R-Reduced Platelet Count or Function |
1 | Includes aspirin use, any thrombocytopenia or blood dyscrasia, like hemophilia. |
|
R- Rebleeding Risk |
2 | |
|
H- Hypertension (Uncontrolled) |
1 | |
| A-Anemia | 1 | Hgb <13 g/dL for Men; Hgb <12 g/dL for Women |
| G-Genetic Factors | 1 | CYP 2C9 single-nucleotide polymorphisms |
|
E-Excessive Fall Risk |
1 | |
| S-Stroke Hystory | 1 |
- a) Choice of anticoagulant therapy.
Established the need for anticoagulant therapy, it is necessary to evaluate which drug is the most appropriate for the specific patient.Vitamin K antagonists (VKAs) are recognized to be effective in reducing thromboembolic risk in patients with atrial fibrillation and cancer; despite that, compared to cancer-free controls, cancer patients who take warfarin - whether for NVAF or venous thromboembolism (VTE) - have worse anticoagulation management and worse outcomes, including a six-fold increase in bleeding rates. Additionally, a large reduction in the time in the therapeutic range is linked to the development of cancer in those using long-term warfarin, especially within the first six months following cancer diagnosis (56). Furthermore, its use in these patients is complicated by drug-drug interaction with chemotherapy drugs that occur through several mechanisms including induction or inhibition of cytochrome P450 isozymes, displacement of binding from plasma proteins, alterations in vitamin K status. Despite these difficulties, warfarin has long been the drug of choice for NVAF anticoagulation.
Low-molecular-weight heparins (LMWH) have not been proven to be effective in preventing stroke or systemic embolism in AF and cancer, and their use is only justified by their demonstrated efficacy and safety in venous thromboembolism (VTE) (57). Their use often is limited to the perioperative-bridging period for patients on warfarin. It’s debated if data supporting use of LMWH as perioperative-bridging agents could be extended to their long-term use; since chemotherapy regimens last up to many months, so it’s difficult to suppose if long-term daily dose of LMWH could be safe and efficacy.
No specifically designed randomized controlled trial has looked at the use of non-vitamin K antagonist oral anticoagulants (NOACs) for AF in cancer patients. Large observational studies and post-hoc analyses of pivotal trials utilizing NOACs in AF patients indicate that NOACs are safe and at least as effective as VKAs in patients with AF and active cancer.
A minority of patients with a history of cancer (640 out of 14264) have been enrolled in the ROCKET AF trial with the most common types of malignancies being prostate, colorectal, and breast cancer. There were not significant differences between rivaroxaban and warfarin in terms of relative efficacy and safety between patients with and without a history of cancer. The risk of ischemic events was not affected by a history of malignancy, although it did raise the risk of bleeding and non-cardiovascular death (58).
A history of cancer was present in 6.8% of participants only in the ARISTOTLE trial. A history of cancer was not substantially related with major bleeding, mortality, stroke, or systemic embolism. Apixaban was as effective as warfarin in preventing stroke and systemic embolism in patients with and without a history of cancer, and its safety profile was comparable to that of warfarin (59).
A minority (5.5%) of patients in the ENGAGE AF - TIMI 48 study had a new or recurrent cancer diagnosed, with the gastrointestinal tract, the prostate, and the lung being the most common sites. Malignancy per se was associated with a higher risk of overall mortality and severe bleeding, but not for stroke or systemic embolism. In AF patients who develop cancer, edoxaban maintains its efficacy and safety profile, making it a potentially more useful treatment choice (60).
NOACs showed a better safety profile than warfarin in patients with underlying malignancy and AF, according to a large retrospective American database investigation. Warfarin was associated with greater death rates in addition to a higher risk of hemorrhagic stroke (61).
To confirm the security and effectiveness of NOACs in patients with active malignancy and AF, an administrative dataset was examined. NOACs users had decreased or equivalent rates of bleeding, stroke, and incident VTE compared to warfarin users (62).
An additional study of 40,271 individuals with AF and cancer using retrospective data from Medicare and other commercial claims databases revealed that apixaban was associated with a lower risk of stroke/systemic embolism and significant bleeding compared to warfarin, although dabigatran and rivaroxaban exhibited equivalent hazards (63). According to a recent meta-analysis, NOACs were linked to a significantly lower rate of serious bleeding complications and thromboembolic events in patients with cancer and AF compared to VKA (64).
NOACs, with apixaban being the best of those examined, demonstrated a decreased incidence of stroke/systemic embolism, VTE, all-cause death, and significant bleeding in AF patients with cancer than warfarin, according to network meta-analysis (65).
At the MD Anderson Cancer Center, 1133 patients with current malignancy and AF were included in a recent single institution retrospective analysis. The result in terms of cerebrovascular accident, gastrointestinal bleeding, and cerebral hemorrhage of NOAC versus VKA was compared using propensity score matching. The study revealed that patients with active malignancy had equivalent risks for cerebrovascular accident, gastrointestinal bleeding, and cerebral hemorrhage when given NOACs instead of warfarin for AF (66).
According to a Surveillance, Epidemiology, and End Results cancer registry database analysis, similar risks of stroke, systemic embolism, and severe bleeding have been observed in older persons with cancer and AF who were exposed to NOACs or to warfarin. In comparison to warfarin, NOACs use was linked to a decreased risk of death from all causes and a similar risk of cardiovascular death (67).
Although use of NOACs for AF in cancer patients grew from 2010 to 2016, there is still a significant percentage of patients with AF and cancer who are not taking anticoagulation (68).
According to recent ESC guidelines on cardio-oncology, the use of NOACs in cancer patients with AF is broadly accepted in light of previous findings even if a clear prospective evaluation is lacking. NOAC should be considered for stroke prevention instead of LMWH and VKA in patients without significant drug-drug interactions, mechanical heart valves, or moderate-to-severe mitral stenosis (46).
Similarly, The International Society on Thrombosis and Haemostasis already recommended that specific decisions for a patient with cancer and AF be made, taking into account the risk of bleeding and stroke. If there are no substantial interactions with oncological medications in patients who started anticoagulation prior to receiving anti-cancer treatment, therapy shouldn't be changed. If there are no substantial drug-drug interactions, NOACs should be chosen over VKAs or low-molecular-weight heparin in patients with newly diagnosed AF receiving chemotherapy. Patients with gastrointestinal neoplasms or other gastrointestinal tract conditions that increase bleeding risk are the exception (46).
Although several early reports point to the efficacy and safety of NOACs in cancer patients with AF, but RCTs should confirm these results. (69)
However, individuals with active cancer constitute a challenging patient population that requires extra attention. Oral anticoagulant therapy in cancer patients may be hampered by other factors like drug-drug interactions, renal impairment, and thrombocytopenia (70). Drug interaction is not limited to anticancer agents but also supportive care drugs (i.e. antiemetics, opioids, etc) must be taken into consideration (71).
Active cancer patients are likely to benefit from a closer follow-up plan with regular re-evaluations given the rapidly changing clinical scenario. A multidisciplinary management that considers individual bleeding and thrombotic risks, drug-drug interactions, patient preferences, and routine clinical evaluation is necessary to identify the appropriate anticoagulation strategy for cancer patients (72). As previously debated, the algorithm proposed by Pastori et al. (Figure 2), could guide represent a useful guide for the management of this complex category of patients.The safety and efficacy of NOACs for stroke prevention in cancer patients with AF are being supported by accumulating research, making them a viable and patient-centered anticoagulation therapy (Table 3).
5. Conclusion
AF is a very common comorbidity in cancer patients as there are several mechanisms that can trigger it or make it worse. Rate control is frequently preferred over rhythm control strategy in cancer patients due to the higher prevalence of side effects of anti-arrhythmic drugs and the numerous interactions with chemotherapy treatments. Anticoagulation risk-benefit ratio decisions and anticoagulant drug selection remain difficult challenges. This population is predisposed to thromboembolic and haemorrhagic complications. The current risk scores used in the general population have not been validated in this subgroup and do not always provide a true estimate of risk. Although there is substantial evidence in favour of DOACs, they are currently underutilized in favour of more widespread use of LMWH, which should be considered a second choice, and VKAs. Close follow-up remains a key issue, given the rapidly changing clinical scenario.
Conflicts of Interest
none.
References
- Lyon AR, López-Fernández T, Couch LS, Asteggiano R, Aznar MC, Bergler-Klein J, Boriani G, Cardinale D, Cordoba R, Cosyns B, Cutter DJ, de Azambuja E, de Boer RA, Dent SF, Farmakis D, Gevaert SA, Gorog DA, Herrmann J, Lenihan D, Moslehi J, Moura B, Salinger SS, Stephens R, Suter TM, Szmit S, Tamargo J, Thavendiranathan P, Tocchetti CG, van der Meer P, van der Pal HJH; ESC Scientific Document Group. 2022 ESC Guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur Heart J. 2022 Nov 1;43(41):4229-4361. [CrossRef]
- Madnick DL, Fradley MG. Atrial Fibrillation and Cancer Patients: Mechanisms and Management. Curr Cardiol Rep. 2022 Oct;24(10):1517-1527. [CrossRef]
- Boriani G, Menna P, Morgagni R, Minotti G, Vitolo M. Ibrutinib and Bruton's tyrosine kinase inhibitors in chronic lymphocytic leukemia: focus on atrial fibrillation and ventricular tachyarrhythmias/sudden cardiac death. Chemotherapy. 2022 Nov 10. [CrossRef]
- O'Neal WT, Lakoski SG, Qureshi W, Judd SE, Howard G, Howard VJ, Cushman M, Soliman EZ. Relation between cancer and atrial fibrillation (from the REasons for Geographic And Racial Differences in Stroke Study). Am J Cardiol. 2015 Apr 15;115(8):1090-4. [CrossRef]
- Ay C, Grilz E, Nopp S, Moik F, Königsbrügge O, Klimek P, Thurner S, Posch F, Pabinger I. Atrial fibrillation and cancer: prevalence and relative risk from a nationwide study. Res Pract Thromb Haemost. 2022 Dec 23;7(1):100026. [CrossRef]
- Han H, Chen L, Lin Z, Wei X, Guo W, Yu Y, Wu C, Cao Y, He J. Prevalence, trends, and outcomes of atrial fibrillation in hospitalized patients with metastatic cancer: findings from a national sample. Cancer Med. 2021 Aug;10(16):5661-5670. [CrossRef]
- Guha A, Fradley MG, Dent SF, Weintraub NL, Lustberg MB, Alonso A, Addison D. Incidence, risk factors, and mortality of atrial fibrillation in breast cancer: a SEER-Medicare analysis. Eur Heart J. 2022 Jan 31;43(4):300-312. [CrossRef]
- Yun JP, Choi EK, Han KD, Park SH, Jung JH, Park SH, Ahn HJ, Lim JH, Lee SR, Oh S. Risk of Atrial Fibrillation According to Cancer Type: A Nationwide Population-Based Study. JACC CardioOncol. 2021 Jun 15;3(2):221-232. [CrossRef]
- Fabiani I, Colombo A, Bacchiani G, Cipolla CM, Cardinale DM. Incidence, Management, Prevention and Outcome of Post-Operative Atrial Fibrillation in Thoracic Surgical Oncology. J Clin Med. 2019 Dec 23;9(1):37. [CrossRef]
- Farmakis D, Parissis J, Filippatos G. Insights into onco-cardiology: atrial fibrillation in cancer. J Am Coll Cardiol. 2014 Mar 18;63(10):945-53. [CrossRef]
- López-Fernández T, Martín-García A, Roldán Rabadán I, Mitroi C, Mazón Ramos P, Díez-Villanueva P, Escobar Cervantes C, Alonso Martín C, Alonso Salinas GL, Arenas M, Arrarte Esteban VI, Ayala de La Peña F, Castro Fernández A, García Pardo H, García-Sanz R, González Porras JR, López de Sá E, Lozano T, Marco Vera P, Martínez Marín V, Mesa Rubio D, Montero Á, Oristrell G, Pérez de Prado A, Velasco Del Castillo S, Virizuela Echaburu JA, Zatarain-Nicolás E, Anguita Sánchez M, Tamargo Menéndez J; Expert reviewers. Atrial Fibrillation in Active Cancer Patients: Expert Position Paper and Recommendations. Rev Esp Cardiol. 2019 Sep;72(9):749-759. English, Spanish. [CrossRef]
- Buza V, Rajagopalan B, Curtis AB. Cancer Treatment-Induced Arrhythmias: Focus on Chemotherapy and Targeted Therapies. Circ Arrhythm Electrophysiol. 2017 Aug;10(8):e005443. [CrossRef]
- Hu YF, Chen YJ, Lin YJ, Chen SA. Inflammation and the pathogenesis of atrial fibrillation. Nat Rev Cardiol. 2015 Apr;12(4):230-43. [CrossRef]
- Cheng WL, Kao YH, Chen SA, Chen YJ. Pathophysiology of cancer therapy-provoked atrial fibrillation. Int J Cardiol. 2016 Sep 15;219:186-94.
- Yao, C. , Veleva T., Scott L., Jr., et al. Enhanced cardiomyocyte NLRP3 inflammasome signalling promotes atrial fibrillation. Circulation. 2018;138:2227-2242).
- Moloney JN, Cotter TG. ROS signalling in the biology of cancer. Semin Cell Dev Biol. 2018 Aug;80:50-64. Epub 2017 Jun 3. [CrossRef] [PubMed]
- Rudolph V, Andrié RP, Rudolph TK, Friedrichs K, Klinke A, Hirsch-Hoffmann B, Schwoerer AP, Lau D, Fu X, Klingel K, Sydow K, Didié M, Seniuk A, von Leitner EC, Szoecs K, Schrickel JW, Treede H, Wenzel U, Lewalter T, Nickenig G, Zimmermann WH, Meinertz T, Böger RH, Reichenspurner H, Freeman BA, Eschenhagen T, Ehmke H, Hazen SL, Willems S, Baldus S. Myeloperoxidase acts as a profibrotic mediator of atrial fibrillation. Nat Med. 2010 Apr;16(4):470-4.
- Leiva O, AbdelHameid D, Connors JM, Cannon CP, Bhatt DL. Common Pathophysiology in Cancer, Atrial Fibrillation, Atherosclerosis, and Thrombosis: JACC: CardioOncology State-of-the-Art Review. JACC CardioOncol. 2021 Nov 16;3(5):619-634.
- Ganatra S, Sharma A, Shah S, Chaudhry GM, Martin DT, Neilan TG, Mahmood SS, Barac A, Groarke JD, Hayek SS, Dani S, Venesy D, Patten R, Nohria A. Ibrutinib-Associated Atrial Fibrillation. JACC Clin Electrophysiol. 2018 Dec;4(12):1491-1500.
- Yang T, Yang P, Roden DM, Darbar D. Novel KCNA5 mutation implicates tyrosine kinase signaling in human atrial fibrillation. Heart Rhythm. 2010 Sep;7(9):1246-52.
- Yang X, Li X, Yuan M, et al Anticancer therapy-induced atrial fibrillation: electrophysiology and related mechanisms. Front Pharmacol. 2018;9:1058.
- Alexandre, J. , Moslehi, J. J., Bersell, K. R., Funck-Brentano, C., Roden, D. M., & Salem, J. E. (2018). Anticancer drug-induced cardiac rhythm disorders: Current knowledge and basic underlying mechanisms. Pharmacol Ther, 189, 89–103.
- Onaitis M, D'Amico T, Zhao Y, O'Brien S, Harpole D. Risk factors for atrial fibrillation after lung cancer surgery: analysis of the Society of Thoracic Surgeons general thoracic surgery database. Ann Thorac Surg. 2010 Aug;90(2):368-74.
- Kumar M, Lopetegui-Lia N, Malouf CA, Almnajam M, Coll PP, Kim AS. Atrial fibrillation in older adults with cancer. J Geriatr Cardiol. 2022 Jan 28;19(1):1-8.
- 25. Suter TM, Ewer MS Cancer drugs and the heart: importance and management. Eur Heart J. 2013;34:1102–1111. [CrossRef]
- 26. Butany J, Leong SW, Carmichael K, Komeda M. A 30-year analysis of cardiac neoplasms at autopsy. Can J Cardiol.
- Gibson TM, Li Z, Green DM, Armstrong GT, Mulrooney DA, Srivastava D, Bhakta N, Ness KK, Hudson MM, Robison LL. Blood Pressure Status in Adult Survivors of Childhood Cancer: A Report from the St. Jude Lifetime Cohort Study. Cancer Epidemiol Biomarkers Prev. 2017 Dec;26(12):1705-1713.
- Visseren FLJ, Mach F, Smulders YM, Carballo D, Koskinas KC, Bäck M, Benetos A, Biffi A, Boavida JM, Capodanno D, Cosyns B, Crawford C, Davos CH, Desormais I, Di Angelantonio E, Franco OH, Halvorsen S, Hobbs FDR, Hollander M, Jankowska EA, Michal M, Sacco S, Sattar N, Tokgozoglu L, Tonstad S, Tsioufis KP, van Dis I, van Gelder IC, Wanner C, Williams B; ESC National Cardiac Societies; ESC Scientific Document Group. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J. 2021 Sep 7;42(34):3227-3337.
- 29. Bussani R, De-Giorgio F, Abbate A, Silvestri F. Cardiac metastases. J Clin Pathol. 2007;60(1):27-34.
- Tsang, T. S. et al. Left atrial volume: important risk marker of incident atrial fibrillation in 1655 older men and women. Mayo Clin.
- Echocardiographic predictors of nonrheumatic atrial fibrillation. The Framingham Heart Study. S M Vaziri, M G Larson, E J Benjamin and D Levy.
- Seko Y, Kato T, Haruna T, Izumi T, Miyamoto S, Nakane E, Inoko M. Association between atrial fibrillation, atrial enlargement, and left ventricular geometric remodeling. Sci Rep. 2018 Apr 23;8(1):6366. PMID: 29686287; PMCID: PMC5913256. [CrossRef]
- Rosenberg MA, Gottdiener JS, Heckbert SR, Mukamal KJ. Echocardiographic diastolic parameters and risk of atrial fibrillation: the Cardiovascular Health Study. Eur Heart J. 2012 Apr;33(7):904-12. Epub 2011 Oct 11. PMID: 21990265; PMCID: PMC3345546. [CrossRef]
- Left Atrial Strain and the Risk of Atrial Arrhythmias From Extended Ambulatory Cardiac Monitoring: MESA. Matthew P. Huber, MD MS; Jay A. Pandit, MD; Paul N. Jensen, PhD; Kerri L. Wiggins, MS; Ravi B. Patel, MD, MS; Benjamin H. Freed, MD; Alain G. Bertoni, MD, MPH; Sanjiv J. Shah, MD; Susan R. Heckbert , MD, PhD; James S. Floyd, MD, MS.
- Müller P, Weijs B, Bemelmans NMAA, Mügge A, Eckardt L, Crijns HJGM, Bax JJ, Linz D, den Uijl DW. Echocardiography-derived total atrial conduction time (PA-TDI duration): risk stratification and guidance in atrial fibrillation management. Clin Res Cardiol. 2021 Nov;110(11):1734-1742. Epub 2021 Aug 28. PMID: 34453577; PMCID: PMC8563556. [CrossRef]
- 8.Sieweke JT, Hagemus J, Biber S, Berliner D, Grosse GM, Schallhorn S, Pfeffer TJ, Derda AA, Neuser J, Bauersachs J and Bavendiek U (2022) Echocardiographic Parameters to Predict Atrial Fibrillation in Clinical Routine—The EAHsy-AF Risk Score. Front. Cardiovasc. Med. 9:851474. [CrossRef]
- Predictive value of preoperative tissue Doppler echocardiographic analysis for postoperative atrial fibrillation after pulmonary resection for lung cancerTakashi Nojiri, MD,a Hajime Maeda, MD, PhD,a Yukiyasu Takeuchi, MD, PhD,a Yasunobu Funakoshi, MD, PhD,a Ryoji Maekura, MD, PhD,b Kazuhiro Yamamoto, MD, PhD,c and Meinoshin Okumura, MD, PhDd.
- Anile M, Telha V, Diso D, De Giacomo T, Sciomer S, Rendina EA, et al. Left atrial size predicts the onset of atrial fibrillation after major pulmonary resections. Eur J Cardiothorac Surg. 2012;41:1094–7.9.Nojiri T, Maeda H, Takeuchi Y, Funakoshi Y, Maekura R, Yamamoto K, et al. Predictive value of preoperative tissue Doppler echocardiographic analysis for postoperative atrial fibrillation after pulmonary resection for lung cancer. J Thorac Cardiovasc Surg. 2010;140:764–8.
- .
- Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomström-Lundqvist C, Boriani G, Castella M, Dan GA, Dilaveris PE, Fauchier L, Filippatos G, Kalman JM, La Meir M, Lane DA, Lebeau JP, Lettino M, Lip GYH, Pinto FJ, Thomas GN, Valgimigli M, Van Gelder IC, Van Putte BP, Watkins CL; ESC Scientific Document Group. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. 2021 Feb 1;42(5):373-498. Erratum in: Eur Heart J. 2021 Feb 1;42(5):507. Erratum in: Eur Heart J. 2021 Feb 1;42(5):546-547. Erratum in: Eur Heart J. 2021 Oct 21;42(40):4194. [CrossRef]
- Lyon AR, López-Fernández T, Couch LS, Asteggiano R, Aznar MC, Bergler-Klein J, Boriani G, Cardinale D, Cordoba R, Cosyns B, Cutter DJ, de Azambuja E, de Boer RA, Dent SF, Farmakis D, Gevaert SA, Gorog DA, Herrmann J, Lenihan D, Moslehi J, Moura B, Salinger SS, Stephens R, Suter TM, Szmit S, Tamargo J, Thavendiranathan P, Tocchetti CG, van der Meer P, van der Pal HJH; ESC Scientific Document Group. 2022 ESC Guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur Heart J. 2022 Nov 1;43(41):4229-4361.
- Heist EK, Mansour M, Ruskin JN. Rate control in atrial fibrillation: targets, methods, resynchronization considerations. Circulation. 2011 Dec 13;124(24):2746-55.
- Echt DS, Ruskin JN. Use of Flecainide for the Treatment of Atrial Fibrillation. Am J Cardiol. 2020 Apr 1;125(7):1123-1133.
- Hammann F, Gotta V, Conen K, Medinger M, Cesana P, Rochlitz C, Taegtmeyer AB. Pharmacokinetic interaction between taxanes and amiodarone leading to severe toxicity. Br J Clin Pharmacol. 2017 Apr;83(4):927-930.
- Su VY, Hu YW, Chou KT, Ou SM, Lee YC, Lin EY, Chen TJ, Tzeng CH, Liu CJ. Amiodarone and the risk of cancer: a nationwide population-based study. Cancer. 2013 May 1;119(9):1699-705.
- Tamargo J, Caballero R, Delpón E. Cancer chemotherapy and cardiac arrhythmias: a review. Drug Saf. 2015 Feb;38(2):129-52.
- Suter TM, Ewer MS. Cancer drugs and the heart: importance and management. Eur Heart J. 2013 Apr;34(15):1102-11.
- Ganatra S, Abraham S, Kumar A, Parikh R, Patel R, Khadke S, Kumar A, Liu V, Diaz ANR, Neilan TG, Martin D, Hook B, Dani SS, Asnani A, Nohria A. Efficacy and safety of catheter ablation for atrial fibrillation in patients with history of cancer. Cardiooncology. 2023 Apr 5;9(1):19. [CrossRef]
- Kanmanthareddy A, Vallakati A, Reddy Yeruva M, Dixit S, DI Biase L, Mansour M, Boolani H, Gunda S, Bunch TJ, Day JD, Ruskin JN, Buddam A, Koripalli S, Bommana S, Natale A, Lakkireddy D. Pulmonary vein isolation for atrial fibrillation in the postpneumonectomy population: a feasibility, safety, and outcomes study. J Cardiovasc Electrophysiol. 2015 Apr;26(4):385-389.
- Chatterjee NA, Upadhyay GA, Ellenbogen KA, McAlister FA, Choudhry NK, Singh JP. Atrioventricular nodal ablation in atrial fibrillation: a meta-analysis and systematic review. Circ Arrhythm Electrophysiol. 2012 Feb;5(1):68-76.
- Leader A, Mendelson Cohen N, Afek S, Jaschek R, Frajman A, Itzhaki Ben Zadok O, Raanani P, Lishner M, Spectre G. Arterial Thromboembolism in Patients With AF and CHA2DS2-VASc Score 0-2 With and Without Cancer. JACC CardioOncol. 2023 Jan 17;5(2):174-185. [CrossRef]
- Pastori D, Marang A, Bisson A, Menichelli D, Herbert J, Lip GYH, Fauchier L. Thromboembolism, mortality, and bleeding in 2,435,541 atrial fibrillation patients with and without cancer: A nationwide cohort study. Cancer. 2021 Jun 15;127(12):2122-2129. [CrossRef]
- 53. Patell R, Gutierrez A, Rybicki L, Khorana AA Usefulness of CHADS2 and CHA2DS2-VASc scores for stroke prediction in patients with cancer and atrial fibrillation. Am J Cardiol. 2186. [CrossRef]
- O'Neal WT, Claxton JS, Sandesara PB, MacLehose RF, Chen LY, Bengtson LGS, Chamberlain AM, Norby FL, Lutsey PL, Alonso A. Provider Specialty, Anticoagulation, and Stroke Risk in Patients With Atrial Fibrillation and Cancer. J Am Coll Cardiol. 2018 Oct 16;72(16):1913-1922. [CrossRef]
- Apostolakis S, Lane DA, Guo Y, et al. Performance of the HEMORR 2 HAGES, ATRIA, and HAS-BLED bleeding risk-prediction scores in nonwarfarin anticoagulated atrial fibrillation patients. J Am Coll Cardiol 2013;61:386–7.
- Farmakis D, Papakotoulas P, Angelopoulou E, Bischiniotis T, Giannakoulas G, Kliridis P, Richter D, Paraskevaidis I. Anticoagulation for atrial fibrillation in active cancer. Oncol Lett. 2022 Apr;23(4):124. [CrossRef]
- Angelini DE, Radivoyevitch T, McCrae KR, Khorana AA. Bleeding incidence and risk factors among cancer patients treated with anticoagulation. Am J Hematol. 2019 Jul;94(7):780-785. [CrossRef]
- Delluc A, Wang TF, Yap ES, Ay C, Schaefer J, Carrier M, Noble S. Anticoagulation of cancer patients with non-valvular atrial fibrillation receiving chemotherapy: Guidance from the SSC of the ISTH. J Thromb Haemost. 2019 Aug;17(8):1247-1252. [CrossRef]
- Lyon AR, López-Fernández T, Couch LS, Asteggiano R, Aznar MC, Bergler-Klein J, Boriani G, Cardinale D, Cordoba R, Cosyns B, Cutter DJ, de Azambuja E, de Boer RA, Dent SF, Farmakis D, Gevaert SA, Gorog DA, Herrmann J, Lenihan D, Moslehi J, Moura B, Salinger SS, Stephens R, Suter TM, Szmit S, Tamargo J, Thavendiranathan P, Tocchetti CG, van der Meer P, van der Pal HJH; ESC Scientific Document Group. 2022 ESC Guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur Heart J. 2022 Nov 1;43(41):4229-4361. [CrossRef]
- Chen ST, Hellkamp AS, Becker RC, Berkowitz SD, Breithardt G, Fox KAA, Hacke W, Halperin JL, Hankey GJ, Mahaffey KW, Nessel CC, Piccini JP, Singer DE, Patel MR, Melloni C. Efficacy and safety of rivaroxaban vs. warfarin in patients with non-valvular atrial fibrillation and a history of cancer: observations from ROCKET AF. Eur Heart J Qual Care Clin Outcomes. 2019 Apr 1;5(2):145-152. [CrossRef]
- Melloni C, Dunning A, Granger CB, Thomas L, Khouri MG, Garcia DA, Hylek EM, Hanna M, Wallentin L, Gersh BJ, Douglas PS, Alexander JH, Lopes RD. Efficacy and Safety of Apixaban Versus Warfarin in Patients with Atrial Fibrillation and a History of Cancer: Insights from the ARISTOTLE Trial. Am J Med. 2017 Dec;130(12):1440-1448.e1. [CrossRef]
- Fanola CL, Ruff CT, Murphy SA, Jin J, Duggal A, Babilonia NA, Sritara P, Mercuri MF, Kamphuisen PW, Antman EM, Braunwald E, Giugliano RP. Efficacy and Safety of Edoxaban in Patients With Active Malignancy and Atrial Fibrillation: Analysis of the ENGAGE AF - TIMI 48 Trial. J Am Heart Assoc. 2018 Aug 21;7(16):e008987. [CrossRef]
- Sawant AC, Kumar A, Mccray W, Tetewsky S, Parone L, Sridhara S, Prakash MPH, Tse G, Liu T, Kanwar N, Bhardwaj A, Khan S, Manion C, Lahoti A, Pershad A, Elkin P, Corbelli J. Superior safety of direct oral anticoagulants compared to Warfarin in patients with atrial fibrillation and underlying cancer: a national veterans affairs database study. J Geriatr Cardiol. 2019 Sep;16(9):706-709. [CrossRef]
- Shah S, Norby FL, Datta YH, Lutsey PL, MacLehose RF, Chen LY, Alonso A. Comparative effectiveness of direct oral anticoagulants and warfarin in patients with cancer and atrial fibrillation. Blood Adv. 2018 Feb 13;2(3):200-209. [CrossRef]
- Deitelzweig S, Keshishian AV, Zhang Y, Kang A, Dhamane AD, Luo X, Klem C, Ferri M, Jiang J, Yuce H, Lip GYH. Effectiveness and Safety of Oral Anticoagulants Among Nonvalvular Atrial Fibrillation Patients With Active Cancer. JACC CardioOncol. 2021 Sep 21;3(3):411-424. [CrossRef]
- Mariani MV, Magnocavallo M, Straito M, Piro A, Severino P, Iannucci G, Chimenti C, Mancone M, Rocca DGD, Forleo GB, Fedele F, Lavalle C. Direct oral anticoagulants versus vitamin K antagonists in patients with atrial fibrillation and cancer a meta-analysis. J Thromb Thrombolysis. 2021 Feb;51(2):419-429. [CrossRef]
- Yang P, Zhu D, Xu X, Shen W, Wang C, Jiang Y, Xu G, Wu Q. Efficacy and safety of oral anticoagulants in atrial fibrillation patients with cancer-a network meta-analysis. Heart Fail Rev. 2020 Sep;25(5):823-831. [CrossRef]
- Potter AS, Patel A, Khawaja M, Chen C, Zheng H, Kaczmarek J, Gao F, Karimzad K, Song J, Koutroumpakis E, Khalaf S, Iliescu C, Deswal A, Palaskas NL. Outcomes by Class of Anticoagulant Use for Nonvalvular Atrial Fibrillation in Patients With Active Cancer. JACC CardioOncol. 2022 Sep 20;4(3):341-350. [CrossRef]
- Mehta HB, An H, Ardeshirrouhanifard S, Raji MA, Alexander GC, Segal JB. Comparative Effectiveness and Safety of Direct Oral Anticoagulants Versus Warfarin Among Adults With Cancer and Atrial Fibrillation. Circ Cardiovasc Qual Outcomes. 2022 Dec;15(12):e008951. [CrossRef]
- Ardeshirrouhanifard S, An H, Goyal RK, Raji MA, Segal JB, Alexander GC, Mehta HB. Use of oral anticoagulants among individuals with cancer and atrial fibrillation in the United States, 2010-2016. Pharmacotherapy. 2022 May;42(5):375-386. [CrossRef]
- Carbone A, Bottino R, D'Andrea A, Russo V. Direct Oral Anticoagulants for Stroke Prevention in Special Populations: Beyond the Clinical Trials. Biomedicines. 2023 Jan 4;11(1):131. [CrossRef]
- Mosarla RC, Vaduganathan M, Qamar A, Moslehi J, Piazza G, Giugliano RP. Anticoagulation Strategies in Patients With Cancer: JACC Review Topic of the Week. J Am Coll Cardiol. 2019 Mar 26;73(11):1336-1349. [CrossRef]
- Peixoto de Miranda ÉJF, Takahashi T, Iwamoto F, Yamashiro S, Samano E, Macedo AVS, Ramacciotti E. Drug-Drug Interactions of 257 Antineoplastic and Supportive Care Agents With 7 Anticoagulants: A Comprehensive Review of Interactions and Mechanisms. Clin Appl Thromb Hemost. 2020 Jan-Dec;26:1076029620936325. [CrossRef]
- Wu VC, Wang CL, Huang YT, Lan WC, Wu M, Kuo CF, Chen SW, Chu PH, Wen MS, Kuo CC, Chang SH. Novel Oral Anticoagulant versus Warfarin in Cancer Patients with Atrial Fibrillation: An 8-Year Population-Based Cohort Study. J Cancer. 2020 Jan 1;11(1):92-99. PMID: 31892976; PMCID: PMC6930400. [CrossRef]
- Yasui T, Shioyama W, Oboshi M, Oka T, Fujita M. Oral Anticoagulants in Japanese Patients with Atrial Fibrillation and Active Cancer. Intern Med. 2019 Jul 1;58(13):1845-1849. [CrossRef]
- Kim K, Lee YJ, Kim TH, Uhm JS, Pak HN, Lee MH, Joung B. Effect of Non-vitamin K Antagonist Oral Anticoagulants in Atrial Fibrillation Patients with Newly Diagnosed Cancer. Korean Circ J. 2018 May;48(5):406-417. [CrossRef]
- Ording AG, Horváth-Puhó E, Adelborg K, Pedersen L, Prandoni P, Sørensen HT. Thromboembolic and bleeding complications during oral anticoagulation therapy in cancer patients with atrial fibrillation: a Danish nationwide population-based cohort study. Cancer Med. 2017 Jun;6(6):1165-1172. [CrossRef]
- Tran E, Ledbetter LE. A retrospective evaluation of direct oral anticoagulant (DOAC) management strategies in patients with cancer on active chemotherapy. J Thromb Thrombolysis. 2023 May;55(4):721-728. [CrossRef]
- Parrini I, Lucà F, Rao CM, Parise G, Micali LR, Musumeci G, La Meir M, Colivicchi F, Gulizia MM, Gelsomino S. Superiority of Direct Oral Anticoagulants over Vitamin K Antagonists in Oncological Patients with Atrial Fibrillation: Analysis of Efficacy and Safety Outcomes. J Clin Med. 2022 Sep 27;11(19):5712. PMID: 36233581; PMCID: PMC9572823. [CrossRef]
- Liu F, Xu Z, Luo J, Yu P, Ma J, Yuan P, Zhu W. Effectiveness and Safety of DOACs vs. VKAs in AF Patients With Cancer: Evidence From Randomized Clinical Trials and Observational Studies. Front Cardiovasc Med. 2021 Nov 5;8:766377. PMID: 34805320; PMCID: PMC8602680. [CrossRef]
Figure 2.
Structured approach to anticoagulation for atrial fibrillation in patients with cancer. AF, atrial fibrillation; CHA2DS2-VASc, Congestive heart failure, Hypertension, Age ≥ 75 years (2 points), Diabetes mellitus, Stroke (2 points)—Vascular disease, Age 65–74 years, Sex category (female); eGFR, estimated glomerular filtration rate; GI, gastrointestinal; GU, genitourinary; HAS-BLED, Hypertension, Abnormal renal and liver function, Stroke, Bleeding Labile international normalized ratio, Elderly, Drugs or alcohol.
Figure 2.
Structured approach to anticoagulation for atrial fibrillation in patients with cancer. AF, atrial fibrillation; CHA2DS2-VASc, Congestive heart failure, Hypertension, Age ≥ 75 years (2 points), Diabetes mellitus, Stroke (2 points)—Vascular disease, Age 65–74 years, Sex category (female); eGFR, estimated glomerular filtration rate; GI, gastrointestinal; GU, genitourinary; HAS-BLED, Hypertension, Abnormal renal and liver function, Stroke, Bleeding Labile international normalized ratio, Elderly, Drugs or alcohol.
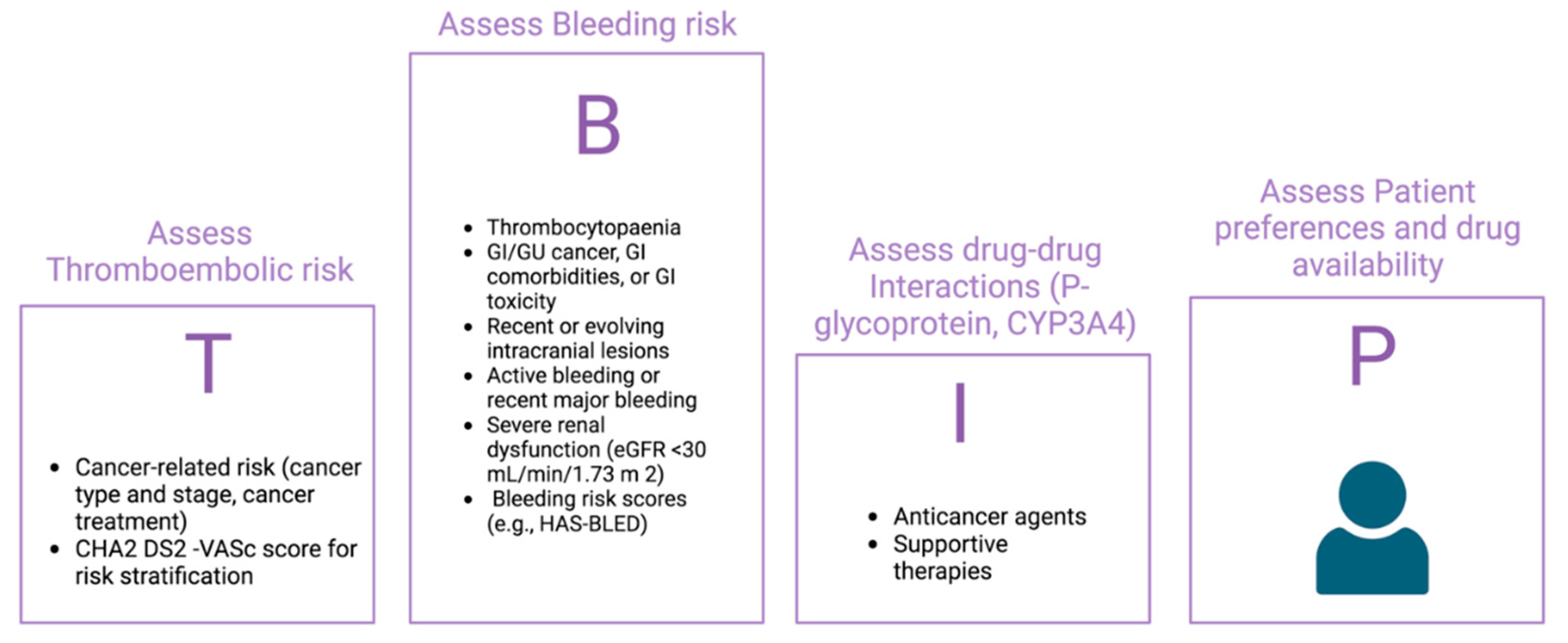
Table 3.
Summary of available evidences on the use of NOAC for AF management in cancer patients.RCT: randomized controlled trial; VTE: venous thromboembolism; IS: ischemic stroke; SE: systemic embolism; GI: gastrointestinal; MI: myocardial infarction; CV: cardiovascular; NMCR: non-major clinically relevant.
Table 3.
Summary of available evidences on the use of NOAC for AF management in cancer patients.RCT: randomized controlled trial; VTE: venous thromboembolism; IS: ischemic stroke; SE: systemic embolism; GI: gastrointestinal; MI: myocardial infarction; CV: cardiovascular; NMCR: non-major clinically relevant.
| Publication year | Trial/reference | Type of evidence | Prospective/retreospective | Number of patients | Drug | Summary of evidences |
|---|---|---|---|---|---|---|
| 2019 | ROCKET-AF (58) | Sub-group analysis of RCT | Prospecitve | 640 | Rivaroxaban | No efficacy and safety differences. Increased risk of bleeding |
| 2017 | ARISTOTLE (59) |
Sub-group analysis of RCT | Prospecitve | 1,236 | Apixaban | Similar efficacy in preventing stroke and systemic embolism. No increase in major bleedings |
| 2018 | ENGAGE AF- TIMI 48 (60) |
Sub-group analysis of RCT | Prospecitve | 1,153 | Edoxaban | Similar efficacy and safety |
| 2018 | Shah S, et al. (63) | Administrative analysis | Retrospective | 16,096 | Various NOACs | lower or similar rates of bleeding and stroke and a lower rate of incident VTE |
| 2022 | Potter AS, et al. (67) | Single-center database analysis | Retrospective | 1,133 | Various NOACs | Similar risks for cerebrovascular accident, gastrointestinal bleeding, and intracranial hemorrhage |
| 2020 | Wu VC, et al. (73) | Administrative analysis | Retrospective | 336 | Various NOACs | reduced IS/SE, major bleeding, and ICH compared to warfarin. |
| 2019 | Yasui T, et al. (74) | Single-center database analysis | Retrospective | 127 | Various NOACs | Similar rates of IS, SE and major bleeding |
| 2018 | Kim K, et al. (75) |
Single-center database analysis | Retrospective | 388 | Various NOACs | NOACs associated with lower incidences of IS/SE, major bleeding and all-cause mortality |
| 2017 | Ording AG, et al. (76) | Administrative analysis | Retrospective | 1809 | Various NOACs | Similar risks of SE or bleeding in patients with and without cancer |
| 2021 | Mariani MV, et al. (65) | Meta-analysis | Prospective/Retrospective | 46,424 | Various NOACs | NOACs associated with reduction of thromboembolic events and major bleeding |
| 2023 | Tran E, et al. (77) | Single-center database analysis | Retrospective | 58 | Various NOACs | Evidence for management issues during chemotherapy |
| 2022 | Parrini I, et al. (78) | Meta-analysis | Prospective/Retrospective | 228,497 | Various NOACs | NOACs showed better efficacy and safety outcomes than warfarin |
| 2021 | Liu F, et al. (79) | Meta-analysis | Prospective/Retrospective | 248,218 | Various NOACs | Reduction in SE, VTE, intracranial and GI bleeding. Same risk of IS, MI, CV death, all-cause death, major bleeding, major or NMCR bleeding. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



