
Submitted:
08 September 2023
Posted:
11 September 2023
You are already at the latest version
Abstract
(1) Background: adnexal masses during pregnancy detection are increased due to the use of first trimester screening and to advanced maternal age. Although the low risk of malignancy, other risks are associated: torsion, rupture or labour obstruction. Correct diagnosis and management are fundamental to guarantee both maternal and fetal safety. Adnexal masses may be troublesome to classify during pregnancy due to the increase in the uterus volume and to pregnancy-related hormonal changes. Management should be based on ultrasound examination to provide the best treatment. (2) Methods: the aim was to describe the ultrasound features of ovarian masses detected during pregnancy. We evaluated patient’s management, perinatal outcomes and follow-up. (3) Results: our study demonstrated that the management should be guided by an accurate ultrasound examination performed by an expert operator according to standardized techniques. Secondly, our results confirm the data present in the literature: the masses are most frequently benign, ultrasound follow-up is the best management strategy and obstetric outcome is not considerably affected. (4) Conclusions: the management of patients with ovarian masses detected during pregnancy should be based on ultrasound examination and a centralization in referral centers for ovarian masses should be considered.
Keywords:
adnexal masses
; pregnancy
; ultrasound
1. Introduction
The incidence of adnexal tumors during pregnancy has increased significantly with the application of routine ultrasound to monitor pregnancy. Most adnexal tumors are discovered incidentally during the first trimester [1].
Despite the management of adnexal masses in pregnancy is still controversial, in recent years there has been an increase of clinical research about adnexal masses in pregnancy, also due to the increased diagnostic ability by experienced sonographers, involving large study population [2].
Adnexal cysts have been reported to be visible on ultrasonography in 4.1–24.9% of pregnant women [3,4], however the majority are benign and typically regress spontaneously or with expectant management; indeed, most ovarian tumors seen during pregnancy seem to disappear in the third trimester, in particular those smaller than 5 cm are at a rate of 71% to 89% [1,5,6]. However, adnexal masses may be challenging to categorize during pregnancy because hormonal changes related to the pregnancy could modify how ovarian masses appear. The most frequent adnexal masses in pregnancy are ovarian cysts, such as follicular cysts and corpus luteal cysts. Follicular cysts grow because of hormonal changes during pregnancy when a follicle that did not ovulate fails to regress on its own. In the early first trimester, progesterone is produced by the corpus luteum to sustain the pregnancy. By the eighth week of pregnancy, when the placenta takes over progesterone secretion, they often regress, but sometimes, they can persist and develop corpus luteal cysts.
Ovarian cysts identified in the early stages of pregnancy are ovarian endometriomas, in about 4-5% of cases; while most adnexal cysts identified after 16 weeks of gestation are mature cystic teratomas. Decidualized endometriomas usually show large intraluminal papillary projections with increased blood flow that resemble malignant ovarian tumors. Papillary projections can make it difficult to distinguish between benign masses like decidualized endometriomas and cystadenofibromas and malignant ones like invasive and borderline tumors [7,8,9,10].
Malignant ovarian tumors (including those of low malignancy) account for about 1-8% of adnexal tumors in pregnancy [11]. If malignancy is suspected, treatment should be decided based on gestational age, stage of disease, and patient preferences. In the early stages, surgery for ovarian cancer can be planned after 16 weeks of pregnancy, and chemotherapy from the second trimester, like non-pregnant patients. In advanced disease, when complete cell reduction is not feasible, neoadjuvant chemotherapy can be used even during pregnancy. The outcome of patients with ovarian cancer diagnosed in pregnancy is similar to non-pregnant patients, and stage of the disease is the most important prognostic factor [12].
Adnexal tumors are often asymptomatic and discovered incidentally. However, some of them are symptomatic due to the size, location, or compression of adjacent structures. Complications such as torsion, hemorrhage, rupture, and obstruction of labour can also occur [13]. The correct approach is a topic of discussion, in order to obtain the right balance between oncological risk, complications and maternal-fetal risks. Currently, ultrasound examination is considered as the first-line imaging method to distinguish between benign and malignant ovarian tumors [14].
Magnetic resonance imaging (MRI) is useful when ultrasound is inconclusive, when there is a high risk of malignancy, or when a more complete definition of histological aspects, such as their relationship to other organs, is needed. This allows for more precise tissue definition and more precise characterization of large masses that are not easily visualized by ultrasound. Recent data indicate that her MRI exposure during pregnancy does not pose any risk to the mother or the newborn. On the contrary, there is no consensus regarding the use of gadolinium during pregnancy. Therefore, use contrast-enhanced MRI only when absolutely necessary [15].
The widespread use of ultrasound has enabled the accurate assessment of incidentally diagnosed ovarian lesions in asymptomatic pregnant women [1,4]. When a pelvic mass is suspected in a pregnant woman, transvaginal ultrasound is currently the first-line imaging method to differentiate adnexal lesions. In cases of larger masses, transabdominal ultrasound is also used. On sonographic examination, size and morphology of the lesions are the main sonographic features used to triage women with adnexal tumors for follow-up management or surgery. Although pattern recognition based on expert subjective assessment of adnexal tumour features remains the best method that can be used to preoperatively distinguish the type of ovarian mass in non-pregnant women [16].
For non-expert sonographers, other prognostic methods are available and include the GI-RADS system, International Ovarian Tumour Analysis (IOTA) group with simple descriptions (SD), logistic regression models 1 and 2 (LR1 and LR2) and Simple Rules (SR) [17]. Simple Description method cannot be used in clinical practice in pregnant women, since one of the necessary conditions for determining the description of malignancy is the patient’s age greater than 50 years [16]. SR uses the presence or absence of specific and selective tumour features such as size, location and presence of solid parts, color Doppler blood flow, and presence of fluid in the pouch of Douglas. In non-pregnant patients, this ultrasonographic method used for characterization of ovarian tumors has a specificity of 78% and a sensitivity of 87% [18]. However, there are important limitations to the use of the original SR scoring system. An adnexal lesion is considered benign when only B (benign) features are seen, and a lesion is classified as malignant when only M (malignant) features are seen on ultrasound. When adnexal tumors do not have B and M features or have both, the tumour should be considered unspecified [19]. However, other scoring systems developed by the IOTA team in recent years can also be used to classify the risk of malignancy in most adnexal tumours. These methods include the evaluation of different NEOplasias in the adneXa (ADNEX) model [20] introduced in 2014 and the Simple Rule Risk (SRR) proposed in 2016 [21].
The traditional treatment for ovarian tumors during pregnancy is surgery in the second trimester due to the risk of possible complications such as torsion, rupture, and late diagnosis of malignancy. Recently, however, conservative management with US follow up has been recommended due to the risks of surgery, including miscarriage, premature contractions, and embolism. Surgery during pregnancy is indicated only if there are acute complications such as torsion, rupture or obstruction or if malignancy is suspected [2].
To our knowledge, studies generally emphasize the importance of a sonographer who can differentiate between benign and malignant adnexal masses; these allows clinicians to conduct the correct management and to prevent surgery in the first trimester, which involves anaesthesia and a materno-fetal risks. In our analysis, the presence of expertise ultra-sonographers with more than 10 years of experience allowed us to change our daily management and predict the proper treatment.
The aim of this study is to describe the ultrasound features of ovarian masses detected during pregnancy and to optimize and to highlight how the presence of an expertise gynaecolostic oncologist sonographer leads us to the personalize and to tailor on patients the correct management.
2. Methods
2.1. Inclusion criteria
This is a retrospective, single-center, cohort study performed at the Gynecology Unit, San Salvatore Hospital, L’Aquila, Italy, and approved by Our Institutional Board (ID 01-2023). All patients had already provided written informed consent for their data to be collected and analyzed for scientific purposes.
We included in the study group all pregnant women with ultrasound diagnosis of adnexal mass during pregnancy, referred to our center between January 2022 and July 2023. Exclusion criteria were: ultrasound examination performed by non-experienced sonographer, ovarian malignancy previously known, twin pregnancies, placenta accreta spectrum (PAS) disorders, in vitro fertilization (IVF) pregnancies with ovarian stimulation. We excluded from the study group patients that not allowed consent to the study.
2.2. Data collection
Clinical and ultrasound features, histological assessment and management (follow-up vs surgery) were retrospectively retrieved from the patients’ medical records. Gestational age at diagnosis, time of surgery, histology, management, and follow-up were documented. Additionally observed were gestational age at delivery, type of delivery, indication of cesarean section, obstetrics, and perinatal outcomes. In cases of bilateral adnexal masses, our analysis focused on the mass with the more complex ultrasonography shape.
Information about follow-up during and after pregnancy were reported, including the number of follow up scans and the time intervals between scans. According to the literature, indications for surgery depended on suspicion of malignancy reported by the examiner according to pattern recognition, symptoms or prevention of complications such as torsion, rupture, or obstacle to normal full-term pregnancy [17,22,23].
All clinical and ultrasound information were collected retrospectively, setting up an Excel database (Microsoft Office Excel 2017, Redmond, WA). Results are shown as absolute frequency (%) for nominal variables and as median (range) for continuous variables.
2.3. Ultrasound evaluation
Transvaginal ultrasound was used to examinate all patients using standardized technique; transabdominal scan was added when necessary. The exams were performed through high-quality ultrasound equipment (Esaote Technos MP, Genova, Italy; Esaote MyLab 70 XVG, Genova, Italy; GE Voluson E8 Medical Systems, Zipf, Austria; Samsung Medison Hera9, Samsung Healthcare, Seoul, Korea) by a Level III ultrasound examiner (M.L.) with more than 15 years of experience in gynecological ultrasound.
The following parameters were assessed: location and size of the lesion (three orthogonal diameters), unilateral or bilateral mass, type of mass (unilocular, unilocular-solid, multilocular, multilocular-solid or solid), presence of papillary projections (defined as any solid protrusion into a cyst cavity with a height ≥3mm), number of papillary projections within the cyst, irregularity of the surface of papillary projections, presence of solid tissue different from papillary projections and presence of septa, ascites and/or fluid in the pouch of Douglas. Color content of the papillary projections and/or other solid tissue were subjectively estimated at power Doppler examination, using a color score (1=no vascularization; 2=minimal vascularization; 3=moderate vascularization; 4=strong vascularization). In case of bilateral masses, the mass with the most complex ultrasound morphology was used. If the masses had similar morphology, the larger mass was used. All masses were described using the International Ovarian Tumor Analysis (IOTA) terminology [24]. The specific diagnosis suggested by the experienced ultrasound examiner in the original report was reported.
According to the protocol outlined by Testa et al. in 2020 [25], the advice of clinicians was mostly based on morphological assessment of the adnexal mass at ultrasound. When a conservative approach with strictly ultrasound surveillance was conducted, ultrasound was performed once a month until the term of pregnancy or till ovaries were not usually visible anymore. A post-partum evaluation when available was also reported.
When surgery was necessary, it was usually performed after the first trimester of pregnancy, during the cesarean section or after delivery. All surgical details were reported.
3. Results
We identified 17 patients with a diagnosis of ovarian mass detected during pregnancy. Clinical characteristics of the study population included are shown in Table 1. Median age at diagnosis was 33 (range 23–39) years and 15 patients were nulliparous (88.2 %). The median gestational age at diagnosis was 10 (range 6-21) weeks. In 5 women (29.4 %) a diagnosis of ovarian mass had been made before pregnancy. At the time of data collection, 6 (35.3 %) pregnancies are ongoing; pregnancy outcome was known for 11 women (64.7%); 9 delivered at term (81.8%), 6 (54.5%) vaginally and 5 (45.5%) by caesarean section and 2 (18.2%) had a preterm delivery. The median gestational age at delivery was 39 (range 27-41) weeks.
All women were managed expectantly and no one required surgery during pregnancy, due to the adnexal mass. Four women who attended for monthly scan had a reduction in the cysts dimension compared to the initial measurement and completely resolution at median 26.5 weeks of gestations (range 14-35). Four (23.5 %) patients are in post-partum ultrasound follow-up, and 4 (23.5 %) women underwent surgery. In 2 (50 %) patients the adnexal mass was removed during caesarean delivery. One patient had surgery during preterm caesarean section at 26 weeks because of feto-maternal complications (preterm prelabour rupture of the membranes-pPROM and breech presentation); the histology report confirmed the benign nature of the lesion. Another patient had surgery during cesarean section due to myoma praevia. The remaining 2 (50 %) women underwent surgery at least 3 months after delivery. Among the 2 patients undergoing surgery after pregnancy a laparoscopic approach was used in all two patients. No surgical complications were described. The histological diagnoses of the ovarian cysts are shown in Table 1. All (100 %) lesions were benign, of which 2 (50%) were teratomas, 1 (25%) was serous cystoadenofibroma and 1 (25 %) was corpus luteum. The ultrasound characteristics of the masses are shown in Table 2.
Only one (5.9%) patient had bilateral masses. The median maximum diameter of the masses was 46 mm (range 18–121). In 9 patients (52.9 %) the masses were described as unilocular, 4 (23.5 %) as unilocular solid, in 3 (17.6 %) as multilocular and 1 (5.9 %) as solid mass. Cysts with ground-glass echogenicity were observed in 3 (17.6%) cases, with mixed echogenicity in 5 (29.4 %). The cyst content was anechoic in 6 (35.3%) patients, low level in 1 (5.9%), haemorrhagic in 1 (5.9 %). Papillary projections were observed in 4 (23.5%) patients. The median height of the largest papillary projection was 7.5 mm (range 3-13). The contour of the papillations was irregular in 1/4 (25%) of the cases, and papillation flow was present in 2/4 (50%) of the cases. The median of maximum diameter of largest solid component was 14 (range 8-38) mm. At color Doppler examination the majority of the cysts (82.3 %) had no vascularization. Acoustic shadows were observed in 3 cases (17.6%). No woman had fluid in the pouch of Douglas or ascites. Table 2 lists the diagnosis recommended by the ultrasound examiner in the original reports.
The operator diagnosed all 17 masses as benign. In five (29.4%) cases were teratomas (Figure 1, Figure S1) In three (17.6%) cases were functional cysts (Figure 2), in one (5.9%) case was cystoadenofibroma (Figure 3) and in two (11.8%) cases were decidualized endometrioma (Figure 4 and Figure 5).
CA 125 results were available for 17 (100%) women, and was negative in all patients, with a median CA 125 concentration of 21 UI/ml.
Among patients undergoing surgery, all four masses (100%) described as being most probably benign on ultrasound examination were confirmed on final histology with correct specific diagnosis (two dermoid cyst and one serous cystoadenofibroma). One case misclassified as endometrioma was a corpus luteum on final histology.
Obstetrics and perinatal outcomes were known for eleven patients and are show in Table 3. All pregnancy was singleton. No patients had miscarriage. Only two patients had preterm delivery. No newborns had Apgar score <7 at 1 minute and 5 minutes and none died. Median fetal weight at delivery was 3280 (range 870-3525) gr. Median volume of blood loss during delivery was 500 (range 150-700) cc.
4. Discussion
The finding of adnexal masses in pregnancy is not frequent; the incidence varies from 0.04% to 1.3% of pregnancies [15]. Furthermore, the correct management has been recently investigated in the literature also because the routine use of first trimester ultrasound increased the diagnosis of adnexal masses in asymptomatic pregnant women [26].
The main goal of the finding consists in the correct ultrasound instrumental diagnostics to allow for the implementation of the most correct management during gestation. Approximately 30% of masses in pregnancy are corpus luteum and follicular or teratoma cyst and usually regress during gestation, many ovarian ultrasound findings are functional cysts, including corpus luteum and follicular cyst. These represent about 30% of pregnancy masses and usually regress spontaneously during the first or early second trimester of gestation.
The percentage of borderline or oncological adnexal masses found is between 1 and 8% [27] and the finding is mainly due to related complications like torsion, hemorrhage, rupture, and labor obstruction. These complications are common in all adnexal masses, although are more severe in malignant ones. [13].
We emphasize that any hospital center can be faced with the management of these masses, even complex cases: management of these lesions and their complications is subject to considerable debate, with different opinions on the best care planning.
Ultrasonography is the most commonly used tool for evaluating ovarian tumors during pregnancy because of its relative safety. The availability of an ultrasound III level center and a sonographer with more than 10 years of experience is a fundamental step in the daily practice of managing these issues.
The conventional first-line imaging study for the assessment of adnexal disease is frequently recognized in clinical practice as a transvaginal ultrasound examination [28,29,30,31]. It has been demonstrated that the operator’s skill improves the accuracy of diagnosis by ultrasonography in discriminating between benign and malignant adnexal tumors [16,32,33]. It is crucial for both the diagnosis of adnexal lesions and the choice of the appropriate management.
In our series we presented 17 pregnant women with ultrasound diagnosis of adnexal mass during pregnancy, from January 2022 and July 2023. We present this limited data numbers, since recently we have the possibility to carry out III level ultrasound scans by the experienced sonographer.
The sonographer reported in our studies all benign masses, thus avoiding unnecessary or ineffective surgeries. The best ultrasound skills and the ability to differentiate benign from malignant in pregnancy allows to reduce surgeries, to personalize the treatment, to choose the appropriate management. These evaluations have also been expressed in other studies [2,25,34] and all agree on identifying the clinical characteristics of the patients and the ultrasound characteristics of the adnexal masses that allow tailoring management.
For sonographers with different experiences, it may be difficult to distinguish between benign and malignant tumors detected in pregnant patients. Depending on the fact that a woman is pregnant, some ovarian lesions may appear differently on sonography. Although most of the several histological adnexal entities in our investigation displayed predicted sonographic features.
In 36 pregnant patients with complex adnexal masses found during ultrasound examination, Czekierdowski et al. documented ultrasonography characteristics, therapy, and outcomes [34]. Even when asymptomatic, persistent lesions with complex morphology identified during an ultrasound scan need to be carefully evaluated to rule out the possibility malignacy.
IOTA, Sassone, and Lerner are three ultrasonographic ovarian mass scoring systems that Lee et al. compare [2] and assess as potential predictors of the risk of cancer in pregnant women. The maximum ovarian mass diameter, the maximum ovarian solid mass diameter, the inner wall structure, the wall thickness, the thickness of the septum, and papillarity were the six ultrasonic characteristics that differed statistically significantly from one another.
Regarding the management, during pregnancy laparoscopic evaluation of the abdomen could be difficult and, in this context, ultrasound could play an important role in tailoring the appropriate management and personalizing the treatment for the patient. A centralization of these pregnant patients in a reference center for ovarian masses should be taken into consideration for the management of patients with ovarian masses discovered during pregnancy.
In 22 pregnant patients with ultrasound-detected malignant ovarian tumors, Moro et al. recently characterized the most significant characteristics of these tumors [35]. They also showed how uncommon ovarian cancer is, with only 22 malignant tumors found during a 17-year span. Malignant ovarian tumors found during pregnancy can be identified by ultrasound using similar morphological characteristics to those seen in patients who are not pregnant.
Furthermore, ultrasound and other testing are utilized to determine whether an otherwise asymptomatic adnexal mass should be handled expectantly or through surgical excision due to the high incidence of spontaneous remission. A thorough examination is crucial to determine the potential of complications including rupture, torsion, and labour obstruction as well as to rule out the likelihood of cancer and probable benign masses.
In previous studies no maternal or neonatal complications were reported for patients operated because of borderline tumors or epithelial ovarian carcinomas [2,34].
Also, a recent investigation of 113 pregnant women with adnexal tumors by Testa et al. [16], showed that patients in the surveillance group, as well as those with benign, borderline, or primary epithelial invasive histology, no obstetric or neonatal problems were noted.
Related to the incidence of malignancy, management, and surveillance, our findings are consistent with those previously published in the literature [2,34]. Pregnancy significantly affects the biological behaviour of ovarian endometriomas masses, according to our study. The majority of cysts are benign or decrease during pregnancy, with corpus luteal cysts, functional cysts, and decidualized endometriomas showing the highest rates of regression (Figure 2 and Figure 5). Considering that we did not discover any malignant masses during our period of observation, the current study demonstrates that malignant ovarian masses in pregnancy represent a rare clinical disease.
The chance of distinguish ovarian masses during pregnancy may help clinicians to decide the appropriate course of treatment for the patient. Making this distinction, for instance, would make it possible to avoid performing unneeded surgeries on adnexal masses during pregnancy. Expectant management appears to be a safe approach for functional cysts, which are likely to regress during pregnancy [36].
We highlight that in cases of small size, sub-specialization and competence in the field of gynecological oncology provide an excellent chance of an early diagnosis, which is necessary for obtaining personalized treatment, according to Di Legge et al. [37,38]. Furthermore, the waiting behavior carried out by the expert sonographer represents a safe and reliable management for the patient. We therefore underline the importance of the diagnosis made by an expert sonographer of a benign mass, the most frequent in pregnancy, which most of the time does not require surgery.
Finally, we also confirm that the presence of ovarian masses in pregnancy does not invalidate the obstetric outcome of the patients.
Our study’s strength is the availability of ultrasound photos or video clips for all cases of ovarian masses found during pregnancy that can be reviewed and eventually used to identify or confirm common imaging findings.
Indeed, the retrospective nature of the analysis and the low incidence of malignant ovarian masses in pregnancy and the single center analysis are the main limitation.
More studies are needed, also prospectively. For example, comparison with MRI may also be useful in determining the optimal imaging technique, particularly for patients with adnexal masses who received an unreliable diagnosis from an US examination. We are currently conducting a study comparison between MRI and US-TV in pregnancy and we are progressively enlarging the study population.
5. Conclusion
Ultrasound evaluation performed by an expert sonographer, who can differentiate between benign and malignant adnexal masses, is crucial because the management of adnexal tumors during pregnancy depends on the nature and type of the tumor and the complications that may arise. Conservative treatment is a good option for women with no symptoms and no signs of malignancy on imaging. In particular our study showed that pregnant patients with ovarian masses should be centralized at a referral III level ultrasound center and that the treatment of these patients should be based on ultrasound examination, performed by an expertized sonographer, that permit to personalize the best management. To support our findings and outline a clinical care of pregnant patients with ovarian lesions, additional significant prospective trials are required.
6. Patents
Supplementary Materials
Figure S1: Grayscale ultrasound images of suspected teratomas.
Author Contributions
MB: Writing- Review & Editing, Visualization and Validation. GC: Software and Resources acquisition and interpretation of data and literature review. VS: Software and Resources acquisition and interpretation of data and literature review. RC: Software and Resources and literature review. ST: Validation. IF: Validation. CDF: Validation. GS: Validation. D’AA: Validation. MG: Supervision. ML: Writing – Review & Editing, Project Administration.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Gynecological and Obstetrics Department Review Board of University of L’Aquila (ID 01/2023).
Informed Consent for Publication Statement: Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Condous, G.; Khalid, A.; Okaro, E.; Bourne, T. Should we be examining the ovaries in pregnancy? Prevalence and natural history of adnexal pathology detected at first-trimester sonography. Ultrasound Obstet. Gynecol. 2004, 24, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Kim, Y.H.; Lee, M.Y.; Ko, H.S.; Oh, S.Y.; Seol, H.J.; Kim, J.W.; Ahn, K.H.; Na, S.; Seong, W.J.; Kim, H.S.; Park, C.W.; Park, J.S.; Jun, J.K.; Won, H.S.; Kim, M.Y.; Hwang, H.S.; Lee, S.M. Ultrasonographic evaluation of ovarian mass for predicting malignancy in pregnant women. Gynecologic Oncology 2021, 163, 385–391. [Google Scholar] [CrossRef]
- Hill, L.M.; Connors-Beatty, D.J.; Nowak, A.; Tush, B. The role of ultrasonography in the detection and management of adnexal masses during the second and third trimesters of pregnancy. Am J Obstet Gynecol 1998, 179, 703–707. [Google Scholar] [CrossRef] [PubMed]
- Yazbek, J.; Salim, R.; Woelfer, B.; Aslam, N.; Lee, C.T.; Jurkovic, D. The value of ultrasound visualization of the ovaries during the routine 11–14 weeks nuchal translucency scan. Eur. J. Obstet. Gynecol. Reprod. Biol. 2007, 132, 154–158. [Google Scholar] [CrossRef] [PubMed]
- Hogston, P.; Lilford, R.J. Ultrasound study of ovarian cysts in pregnancy: prevalence and significance. BJOG: Int. J. Obstet. Gynaecol. 1986, 93, 625–628. [Google Scholar] [CrossRef] [PubMed]
- Bernhard, L.M.; Klebba, P.K.; Gray, D.L.; Mutch, D.G. Predictors of persistence of adnexal masses in pregnancy. Obstet Gynecol 1999, 93, 585–589. [Google Scholar]
- Moro, F.; Poma, C.B.; Zannoni, G.F.; Urbinati, A.V.; Pasciuto, T.; Ludovisi, M.; Moruzzi, M.C.; Carinelli, S.; Franchi, D.; Scambia, G.; et al. Imaging in gynecological disease (12): clinical and ultrasound features of invasive and non-invasive malignant serous ovarian tumors. Ultrasound Obstet. Gynecol. 2017, 50, 788–799. [Google Scholar] [CrossRef]
- Ludovisi, M.; Foo, X.; Mainenti, S.; Testa, A.C.; Arora, R.; Jurkovic, D. Ultrasound diagnosis of serous surface papillary borderline ovarian tumor: A case series with a review of the literature. J. Clin. Ultrasound 2015, 43, 573–577. [Google Scholar] [CrossRef]
- Fagotti, A.; Ludovisi, M.; De Blasis, I.; Virgilio, B.; Di Legge, A.; Mascilini, F.; Moruzzi, M.; Giansiracusa, C.; Fanfani, F.; Tropeano, G.; et al. The sonographic prediction of invasive carcinoma in unilocular-solid ovarian cysts in premenopausal patients: a pilot study. Hum. Reprod. 2012, 27, 2676–2683. [Google Scholar] [CrossRef]
- Valentin, L. Use of morphology to characterize and manage common adnexal masses. Best Pr. Res. Clin. Obstet. Gynaecol. 2004, 18, 71–89. [Google Scholar] [CrossRef]
- Hoover, K.; Jenkins, T.R. Evaluation and management of adnexal mass in pregnancy. American Journal of Obstetrics & Gynecology august 2011, 97–102. [Google Scholar]
- Fruscio, R.; De Daan, J.; Van Calsteren, K.; Verheecke, M.; Mhallem, M.; Amant, F. Ovarian cancer in pregnancy. Best Practice & Research Clinical Obstetrics and Gynaecology 2017, 41, 108–117. [Google Scholar]
- Aggarwal, P.; Kehoe, S. Ovarian tumours in pregnancy: A literature review. Eur J Obstet Gynecol Reprod Biol 2011, 155, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Timmerman, D.; Testa, A.C.; Bourne, T.; Ferrazzi, E.; Ameye, L.; Konstantinovic, M.L.; Van Calster, B.; Collins, W.P.; Vergote, I.; Van Huffel, S.; et al. Logistic Regression Model to Distinguish Between the Benign and Malignant Adnexal Mass Before Surgery: A Multicenter Study by the International Ovarian Tumor Analysis Group. J. Clin. Oncol. 2005, 23, 8794–8801. [Google Scholar] [CrossRef]
- D’ambrosio, V.; Brunelli, R.; Musacchio, L.; Del Negro, V.; Vena, F.; Boccuzzi, G.; Boccherini, C.; Di Donato, V.; Piccioni, M.G.; Panici, P.B.; et al. Adnexal masses in pregnancy: an updated review on diagnosis and treatment. Tumori J. 2020, 107, 12–16. [Google Scholar] [CrossRef]
- Valentin, L. Prospective cross-validation of Doppler ultrasound examination and gray-scale ultrasound imaging for discrimination of benign and malignant pelvic masses. Ultrasound Obstet. Gynecol. 1999, 14, 273–283. [Google Scholar] [CrossRef]
- Froyman, W.; Landolfo, C.; De Cock, B.; Wynants, L.; Sladkevicius, P.; Testa, A.C.; Van Holsbeke, C.; Domali, E.; Fruscio, R.; Epstein, E.; et al. Risk of complications in patients with conservatively managed ovarian tumours (IOTA5): a 2-year interim analysis of a multicentre, prospective, cohort study. Lancet Oncol. 2019, 20, 448–458. [Google Scholar] [CrossRef]
- Timmerman, D.; Ameye, L.; Fischerova, D.; Epstein, E.; Melis, G.B.; Guerriero, S.; Van Holsbeke, C.; Savelli, L.; Fruscio, R.; Lissoni, A.A.; Testa, A.C.; Veldman, J.; Vergote, I.; Van Huffel, S.; Bourne, T.; Valentin, L. Simple ultrasound rules to distinguish between benign and malignant adnexal masses be-fore surgery: Prospective validation by IOTA group. BMJ 2010, 341, c6839. [Google Scholar] [CrossRef]
- Nunes, N.; Ambler, G.; Foo, X.; Naftalin, J.; Widschwendter, M.; Jurkovic, D. Use of IOTA simple rules for diagnosis of ovarian cancer: meta-analysis. Ultrasound Obstet. Gynecol. 2014, 44, 503–514. [Google Scholar] [CrossRef]
- Van Calster, B.; Van Hoorde, K.; Valentin, L.; Testa, A.C.; Fischerova, D.; Van Holsbeke, C.; Savelli, L.; Franchi, D.; Epstein, E.; Kaijser, J.; et al. Evaluating the risk of ovarian cancer before surgery using the ADNEX model to differentiate between benign, borderline, early and advanced stage invasive, and secondary metastatic tumours: prospective multicentre diagnostic study. BMJ 2014, 349, g5920. [Google Scholar] [CrossRef]
- Timmerman, D.; Van Calster, B.; Testa, A.; Savelli, L.; Fischerova, D.; Froyman, W.; Wynants, L.; Van Holsbeke, C.; Epstein, E.; Franchi, D.; et al. Predicting the risk of malignancy in adnexal masses based on the Simple Rules from the International Ovarian Tumor Analysis group. Am. J. Obstet. Gynecol. 2016, 214, 424–437. [Google Scholar] [CrossRef] [PubMed]
- Koo, Y.J.; Kim, T.J.; Lee, J.E.; Kwon, Y.S.; Kim, H.J.; Lee, I.H.; Lim, K.T.; Lee, K.H.; Shim, J.U.; Mok, J.E. Risk of torsion and malignancy by adnexal mass size in pregnant women. Acta Obstet Gynecol Scand 2011, 90, 358–361. [Google Scholar] [CrossRef] [PubMed]
- Mascilini, F.; Moruzzi, C.; Giansiracusa, C.; Guastafierro, F.; Savelli, L.; De Meis, L.; Epstein, E.; Timor-Tritsch I., E.; Mailath-Pokorny, M.; Ercoli, A.; Exacoustos, C.; Benacerraf B., R.; Valentin, L.; Testa, A.C. Imaging in gynecological disease. 10: Clinical and ultrasound characteristics of decidualized endometriomas surgically removed during pregnancy. Ultrasound Obstet Gynecol 2014, 44, 354–360. [Google Scholar] [CrossRef]
- Timmerman, D.; Valentin, L.; Bourne, T.H.; Collins, W.P.; Verrelst, H.; Vergote, I. Terms, definitions and measurements to describe the sonographic features of adnexal tumors: a consensus opinion from the International Ovarian Tumor Analysis (IOTA) group. Ultrasound Obstet. Gynecol. 2000, 16, 500–505. [Google Scholar] [CrossRef] [PubMed]
- Testa, A.C.; Mascilini, F.; Quagliozzi, L.; Moro, F.; Bolomini, G.; Mirandola, M.T.; Moruzzi, M.C.; Scambia, G.; Fagotti, A. Management of ovarian masses in pregnancy: patient selection for interventional treatment. Int. J. Gynecol. Cancer 2020, 31, 899–906. [Google Scholar] [CrossRef]
- Whitecar, P.; Turner, S.; Higby, K. Adnexal masses in pregnancy: A review of 130 cases undergoing surgical management. Am. J. Obstet. Gynecol. 1999, 181, 19–24. [Google Scholar] [CrossRef]
- Giuntoli, R.L.; Vang, R.S.; Bristow, R.E. Evaluation and Management of Adnexal Masses During Pregnancy. Clin. Obstet. Gynecol. 2006, 49, 492–505. [Google Scholar] [CrossRef]
- Kaijser, J.; Vandecaveye, V.; Deroose, C.M.; Rockall, A.; Thomassin-Naggara, I.; Bourne, T.; Timmerman, D. Imaging techniques for the pre-surgical diagnosis of adnexal tumours. Best Pr. Res. Clin. Obstet. Gynaecol. 2014, 28, 683–695. [Google Scholar] [CrossRef]
- Valentin, L.; Hagen, B.; Tingulstad, S.; Eik-Nes, S. Comparison of ‘pattern recognition’ and logistic regression models for discrimination between benign and malignant pelvic masses: a prospective cross validation. Ultrasound Obstet. Gynecol. 2001, 18, 357–365. [Google Scholar] [CrossRef]
- Timmerman, D. The use of mathematical models to evaluate pelvic masses; can they beat an expert operator? Best Pract Res Clin Obstet Gynaecol 2004, 18, 91–104. [Google Scholar] [CrossRef]
- Meys, E.; Kaijser, J.; Kruitwagen, R.; Slangen, B.; Van Calster, B.; Aertgeerts, B.; Verbakel, J.; Timmerman, D.; Van Gorp, T. Subjective assessment versus ultrasound models to diagnose ovarian cancer: A systematic review and meta-analysis. Eur. J. Cancer 2016, 58, 17–29. [Google Scholar] [CrossRef] [PubMed]
- Timmerman, D.; Schwärzler, P.; Collins, W.P.; Claerhout, F.; Coenen, M.; Amant, F.; Vergote, I.; Bourne, T.H. Subjective assessment of adnexal masses with the use of ultrasonography: an analysis of interobserver variability and experience. Ultrasound Obstet. Gynecol. 1999, 13, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Yazbek, J.; Raju, S.K.; Ben-Nagi, J.; Holland, T.K.; Hillaby, K.; Jurkovic, D. Effect of quality of gynaecological ultrasonography on management of patients with suspected ovarian cancer: a randomised controlled trial. Lancet Oncol. 2008, 9, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Czekierdowski, A.; Stachowicz, N.; Smole ´n, A.; Kluz, T.; Łozi ´nski, T.; Miturski, A.; Kraczkowski, J. Sonographic Assessment of Complex Ultrasound Morphology Adnexal Tumors in Pregnant Women with the Use of IOTA Simple Rules Risk and ADNEX Scoring Systems. Diagnostics 2021, 11, 414. [Google Scholar] [CrossRef] [PubMed]
- Moro, F.; Mascilini, F.; Pasciuto, T.; Leombroni, M.; Destri, M.L.; De Blasis, I.; Garofalo, S.; Scambia, G.; Testa, A.C. Ultrasound features and clinical outcome of patients with malignant ovarian masses diagnosed during pregnancy: experience of a gynecological oncology ultrasound center. Int. J. Gynecol. Cancer 2019, 29, 1182–1194. [Google Scholar] [CrossRef]
- Pateman, K.; Moro, F.; Mavrelos, D.; Foo, X.; Hoo, W.L.; Jurkovic, D. Natural history of ovarian endometrioma in pregnancy. BMC Womens Health 2014, 14, 128. [Google Scholar] [CrossRef]
- Di Legge, A.; Pollastri, P.; Mancari, R.; Ludovisi, M.; Mascilini, F.; Franchi, D.; Jurkovic, D.; Coccia M., E.; Timmerman, D.; Scambia, G.; Testa, A.C.; Valentin, L. Clinical and ultrasound characteristics of surgically removed adnexal lesions with largest diameter ≤ 2.5 cm: A pictorial essay. Ultrasound Obstet Gynecol 2017, 50, 648–656. [Google Scholar] [CrossRef]
- Bruno, M.; Capanna, G.; Di Florio, C.; Sollima, L.; Guido, M.; Ludovisi, M. Sonographic characteristics of ovarian Leydig cell tumor. Ultrasound Obstet. Gynecol. 2023, 62, 441–442. [Google Scholar] [CrossRef]
Figure 1.
Ultrasound follow up of the patient n° 10 (a-f): grayscale ultrasound images showing adnexal masses with mixed content suspected for teratomas, as reported by the experienced examiner in the original ultrasound reports.
Figure 1.
Ultrasound follow up of the patient n° 10 (a-f): grayscale ultrasound images showing adnexal masses with mixed content suspected for teratomas, as reported by the experienced examiner in the original ultrasound reports.
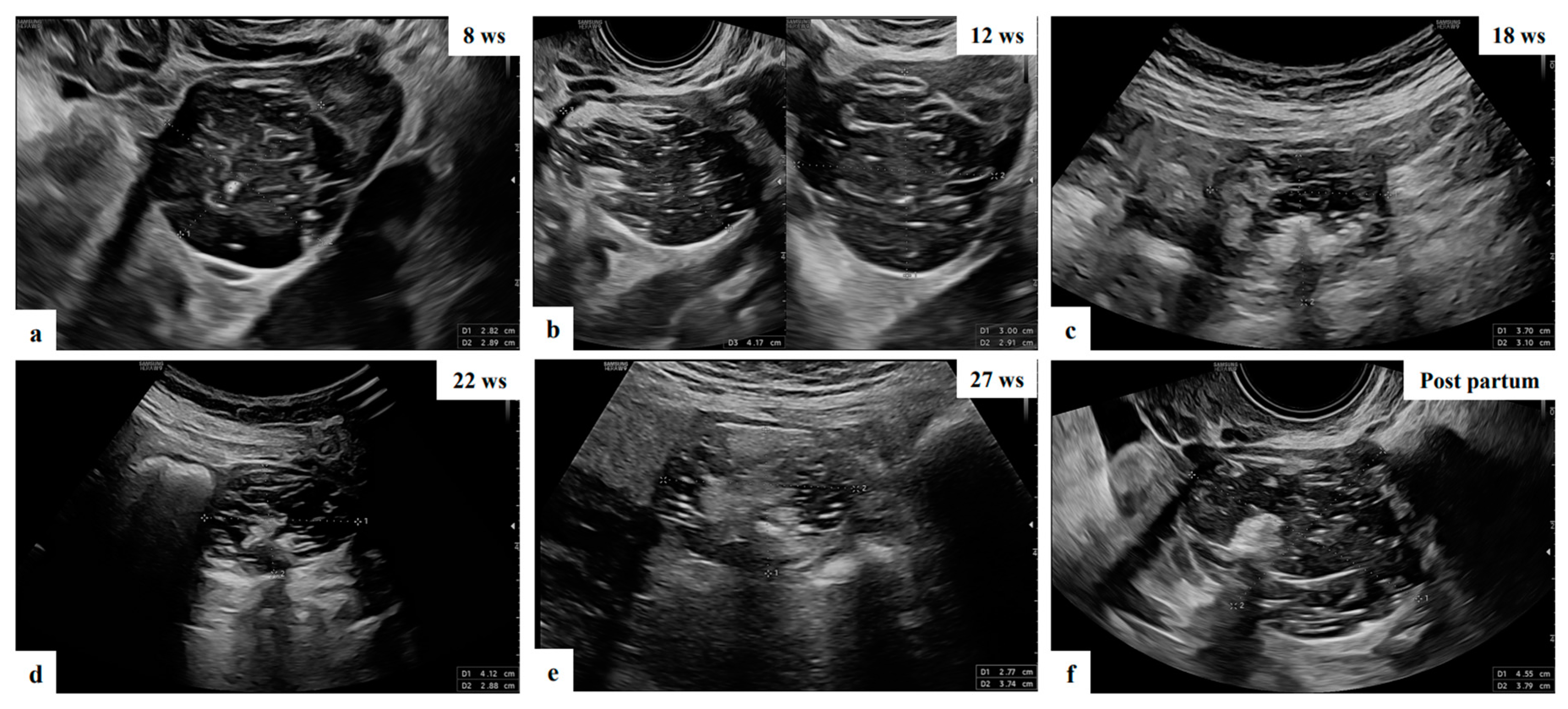
Figure 2.
Grayscale ultrasound images showing adnexal anechoic unilocular mass, suspected of functional cyst of 32 ys old patient in ultrasound managed expectantly during the pregnancy who attended for monthly scan had a reduction in the cysts dimension compared to the initial measurement and completely resolution at median 35 weeks of gestations (a-f).
Figure 2.
Grayscale ultrasound images showing adnexal anechoic unilocular mass, suspected of functional cyst of 32 ys old patient in ultrasound managed expectantly during the pregnancy who attended for monthly scan had a reduction in the cysts dimension compared to the initial measurement and completely resolution at median 35 weeks of gestations (a-f).
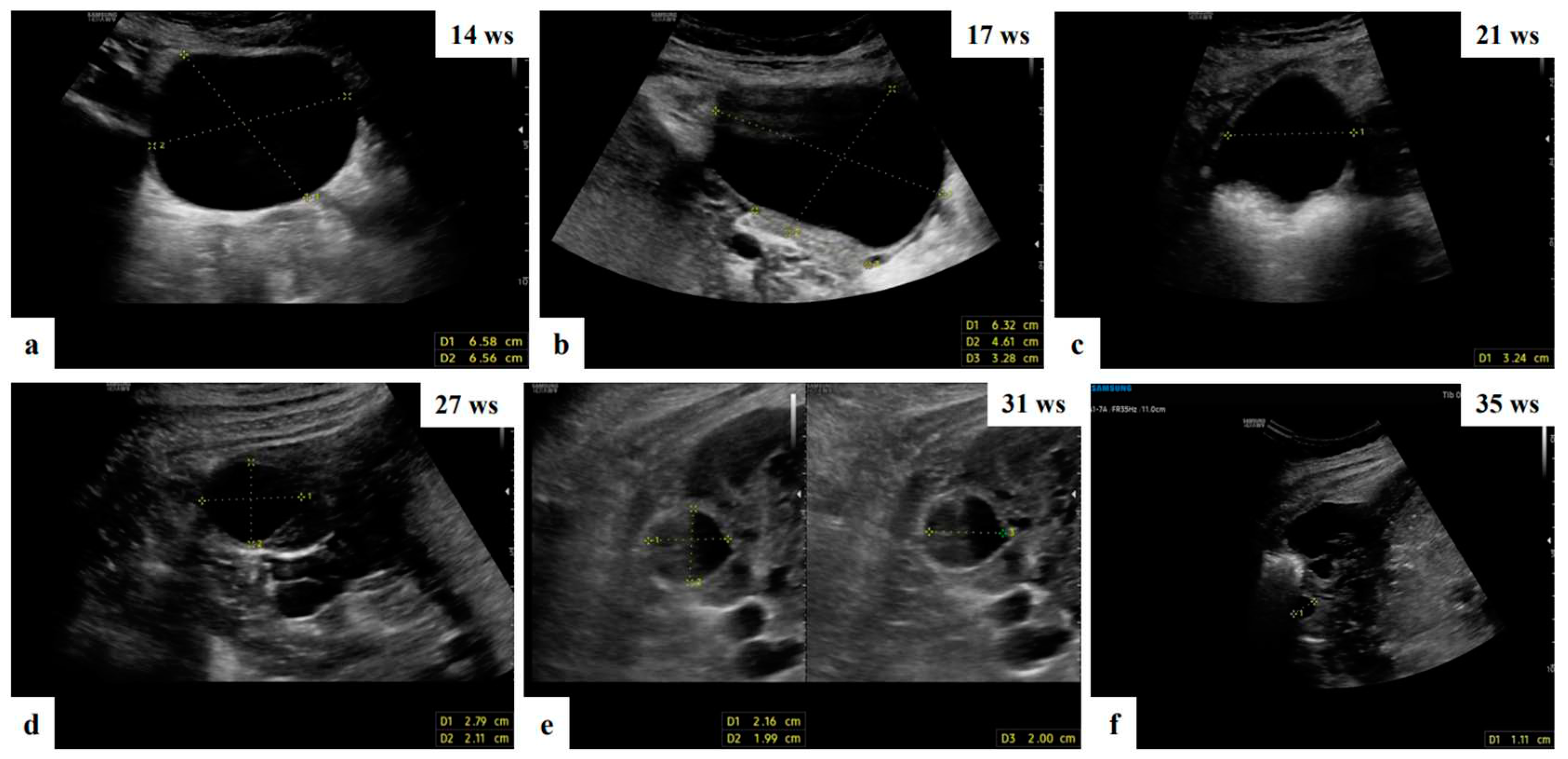
Figure 3.
Grayscale and color Doppler ultrasound (a,b) images showing unilocular solid mass with anechoic content and papillary projection, suspected of serous cystoadenofibroma (patient n° 5).
Figure 3.
Grayscale and color Doppler ultrasound (a,b) images showing unilocular solid mass with anechoic content and papillary projection, suspected of serous cystoadenofibroma (patient n° 5).
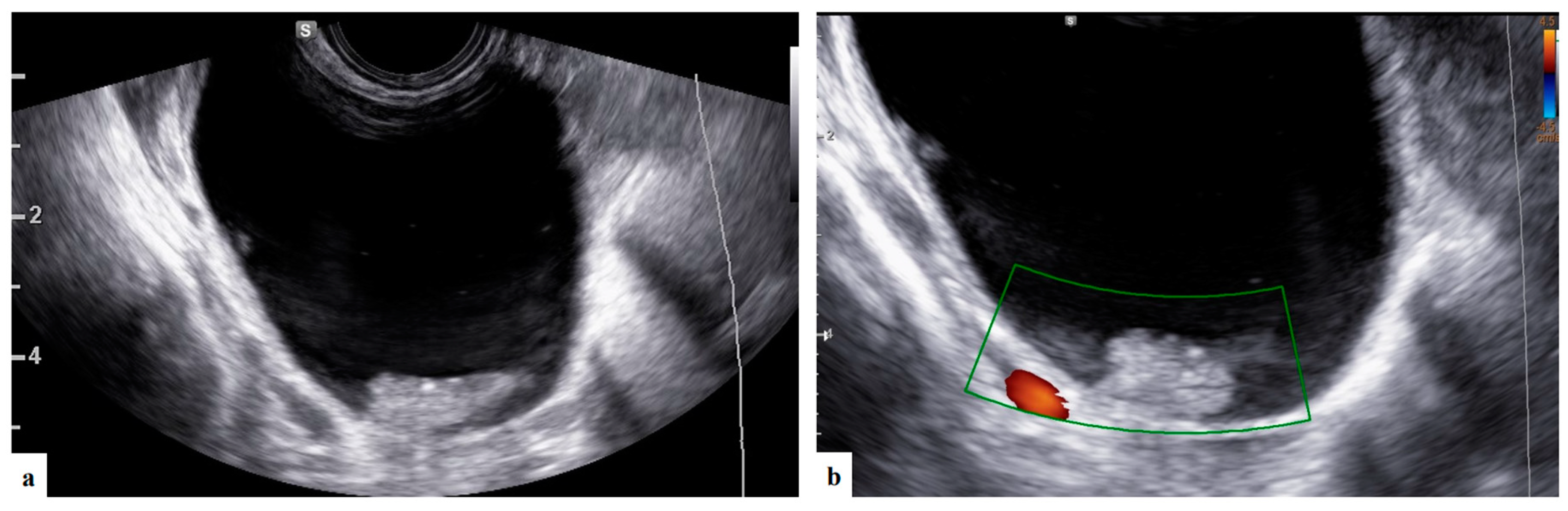
Figure 4.
Grayscale (1a,2a) and color Doppler (1b,2b) ultrasound images of two decidualized endometriomas in our series (patients ongoing): internal cyst wall moderately vascularized rounded papillary projections with smooth contour and cyst content with ground-glass echogenicity.
Figure 4.
Grayscale (1a,2a) and color Doppler (1b,2b) ultrasound images of two decidualized endometriomas in our series (patients ongoing): internal cyst wall moderately vascularized rounded papillary projections with smooth contour and cyst content with ground-glass echogenicity.
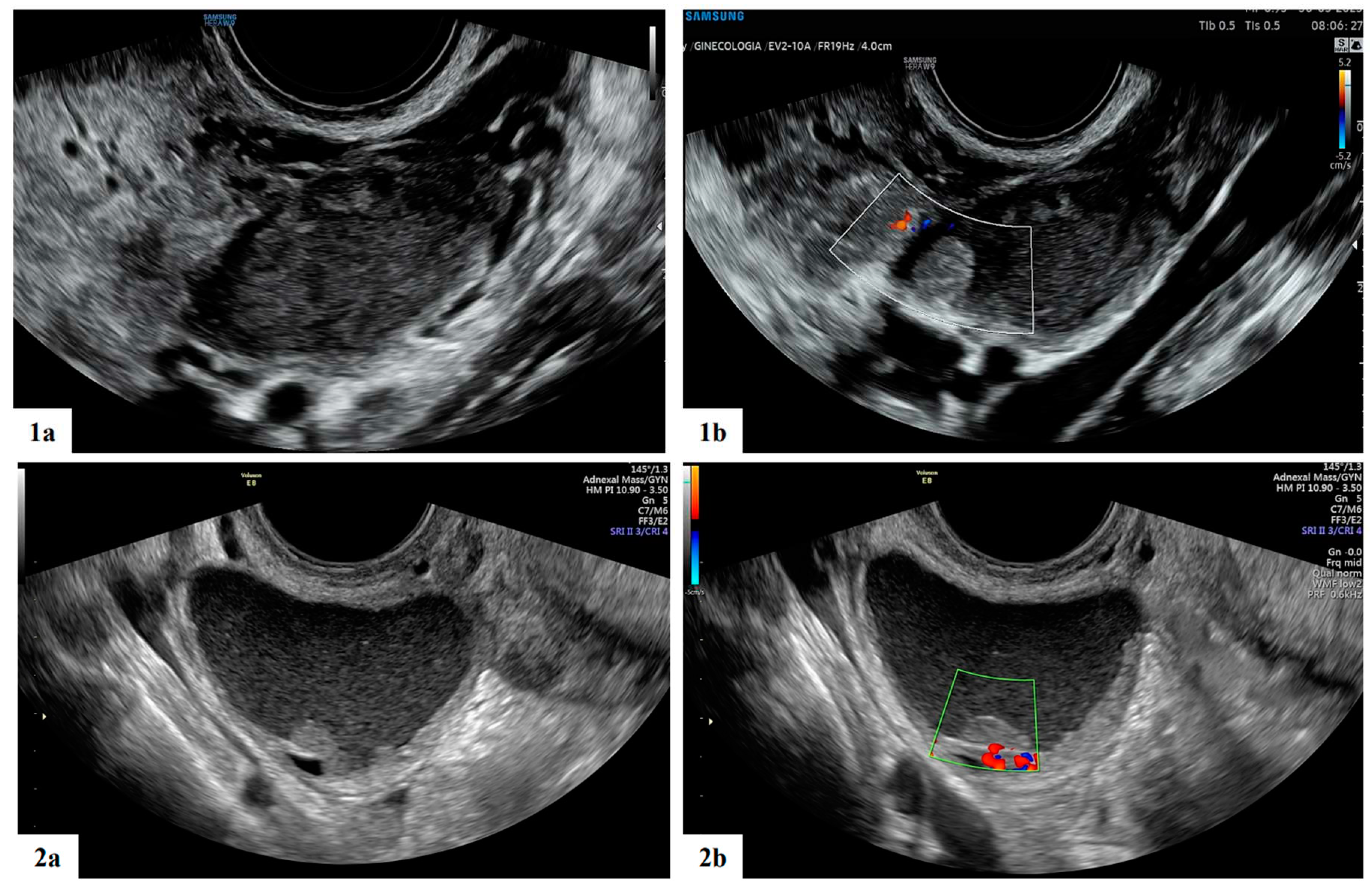
Figure 5.
Ultrasound follow up of the ongoing patient: grayscale (1a,2a,3a) ultrasound images showing unilocular mass with "ground glass" content, suspected for decidualized endometrioma. The mass shows papillary projections with regular smooth contour and moderately vascularization at 15 wks (2a,b) of gestations and reductions in the cyst dimension and number of papillary projection at 19 wks (3a,b).
Figure 5.
Ultrasound follow up of the ongoing patient: grayscale (1a,2a,3a) ultrasound images showing unilocular mass with "ground glass" content, suspected for decidualized endometrioma. The mass shows papillary projections with regular smooth contour and moderately vascularization at 15 wks (2a,b) of gestations and reductions in the cyst dimension and number of papillary projection at 19 wks (3a,b).
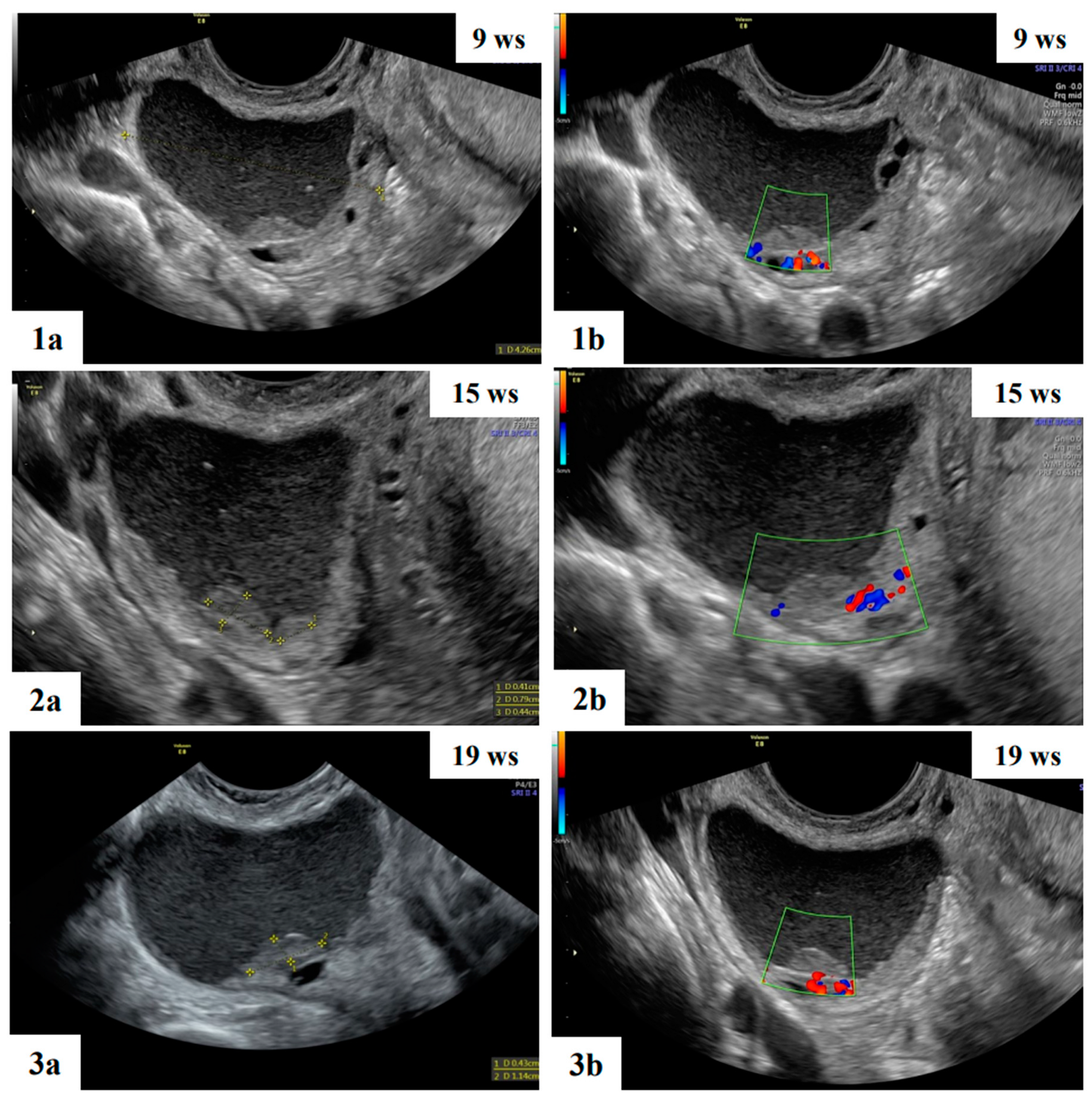

Table 1.
Clinical characteristics of 17 women with ovarian cysts during pregnancy.
| Characteristics | Value |
|---|---|
| Number of cases | 17 |
| Nulliparous | 15 (88.2) |
| Ultrasound diagnosis before pregnancy | 5 (29.4) |
| Age at diagnosis (years) | 33 (23-39) |
| Gestational age at diagnosis (weeks) | 10 (6-21) |
| Gestational age at last ultrasound examination (weeks) | 26 (9-39) |
| Gestational age at delivery* | 39 (27-41) |
| Delivery Spontaneous delivery Cesarean section Ongoing pregnancy |
6 (35.3)5 (29.4)6 (35.3) |
| Management Follow up Surgery after delivery Spontaneous resolution |
9 (52.9)4 (23.5)4 (23.5) |
| Histological diagnosis** Teratoma Serous cystoadenofibroma Corpus luteum |
2 (50)1 (25)1 (25) |
Data are given as median (range) or n (%). *Information available for 11 patients. ** Information available for 4 patients.
Table 2.
Ultrasound characteristics of 17 women with ovarian cysts during pregnancy.
| Ultrasound characteristics | All (n=17) |
|---|---|
| Bilateral mass | 1 |
| Maximum diameter of lesion (mm) (range) | 46 (18-121) |
| Type of tumor Unilocular Unilocular solid Multilocular Multilocular solid Solid |
9 4 3 0 1 |
| Cyst content echogenicity Anechoic Low level Ground glass Mixed Hemorrhagic Not applicable (solid mass) |
6 1 3 5 1 1 |
| Color score 1 2 3 4 |
14 2 1 0 |
| Maximum diameter of largest solid component (mm) (range) | 14 (8-38) |
| Presence of papillary projections | 4 |
| Number of papillary projections 1 2 3 |
1/4 2/4 1/4 |
| Papillation contour Irregular Smooth |
1/4 3/4 |
| Papillation flow Present Absent |
2/4 2/4 |
| Heigh of the largest papillary projection (mm) (range) | 7.5 (3-13) |
| Presence of acoustic shadow | 3 |
| Presence of crescent sign | 13 |
| Diagnosis based on subjective assessment Benign Borderline Malignant |
17 0 0 |
| Specific diagnosis suggested by the original examiner Teratoma Functional cyst Decidualized endometrioma Paraovarian cyst Endometrioma Fibroma Cystoadenofibroma Sactosalpinx Corpus luteum |
5 3 2 2 1 1 1 1 1 |
Data are given as median (range).
Table 3.
Perinatal outcomes.
| Patients | Gestational age at delivery |
Singleton/ twin pregnancy |
Type of delivery |
Indication for cesarean section | Perineal lacerations |
Blood loss during delivery(cc) |
APGAR score | Fetal weight(gr) |
|---|---|---|---|---|---|---|---|---|
| 1 | 27 | Singleton | Caesarean section and cystectomy |
pPROM, breech presentation | - | 500 | 7/8 | 870 |
| 2 | 40 | Singleton | Vaginal delivery |
- | Episiotomy and I grade laceration | 700 | 8/9 | 3500 |
| 3 | 38 | Singleton | Vaginal delivery |
- | - | 150 | 8/9 | 3450 |
| 4 | 41 | Singleton | Caesarian delivery |
Abnormal CTG | - | 500 | 9/10 | 3185 |
| 5 | 38 | Singleton | Vaginal delivery |
- | I gradelaceration | 100 | 8/10 | 3070 |
| 6 | 39 | Singleton | Caesarian delivery |
- | II grade laceration | 300 | 9/9 | 2880 |
| 7 | 40 | Singleton | Vaginal delivery |
Abnormal CTG | - | 300 | 9/10 | 3525 |
| 8 | 40 | Singleton | Caesarian delivery |
- | Episiotomy | 500 | 9/10 | 3300 |
| 9 | 38 | Singleton | Vaginal delivery |
Fetalmalformation | - | 500 | 7/9 | 3280 |
| 10 | 40 | Singleton | Caesarian delivery |
- | Episiotomy | 200 | 9/10 | 3280 |
| 11 | 36 | Singleton | Caesarean section and unilateral salpingo- oophorectomy |
Myomapraevia | - | 600 | 8/9 | 2850 |
Information available for 11 patients.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



