
Submitted:
06 September 2023
Posted:
07 September 2023
You are already at the latest version
Abstract
Syndactyly is the most common congenital malformation of the hand, leading to the fusion of the digits, frequently affecting the ring and middle fingers. The incidence is one out of 2500 children, predominantly occurring in boys and Caucasians. Clinically, the malformation may present as soft tissue or bony fusion, resulting in the union of the fingers characterised as complete or incomplete. This fusion may involve the phalanges but may also extend to the carpal/tarsal bones, even to the metacarpal’s or metatarsal’s level, rarely to the distal end of the forearm and lower leg. Mostly isolated but may occur together with other disorders or malformations such as synostosis, acro-syndactyly, cleft hand, clinodactyly, or polydactyly. Syndromic syndactyly can be observed in cases of Apert Syndrome, Poland’s Syndrome, Pfeiffer Syndrome and many others. A girl born in June of 2019 was diagnosed with congenital malformation of the right hand at birth —affecting the right middle, ring and little fingers, respectively. After X-ray imaging, the fusion of the third and fourth proximal phalanges to a common metacarpal was identified, forming a unique diagnosis of clino-syndactyly with metacarpal aplasia. Surgical intervention was advocated for, including a wedge osteotomy to correct the synchondrosis at the phalangeal base and a dorsal flap to close the interdigital space created during the correction of the III and IV. fingers. A trapezoid flap for the release of the syndactyly of the IV and V. fingers was applied. The paper aims to present the surgical correction and its results regarding an atypical case of syndactyly with clinodactyly and metacarpal aplasia.
Keywords:
Clinodactily
; Syndactyly
; Wedge osteotomy
; Congenital
; Flaps
; Plastic surgery
; Hand surgery
1. Introduction
Syndactyly, derived from the Greek words “syn” (meaning “together”) and “dactyly” (meaning “digits”), ranks among the most prevalent congenital malformations affecting the extremities [1,2,3]. It arises due to a developmental separation failure (webbing) during embryological limb formation, resulting in the fusion of the digits. This condition frequently affects the ring and middle fingers. The incidence of syndactyly is estimated to be approximately one occurrence per 2,500 children, with a higher prevalence among boys and individuals of Caucasian ethnicity. Mothers aged 40 years or older face an increased risk of giving birth to an offspring with congenital limb deformities compared to mothers below 30. Predominantly a genetic disease, however, contributing factors such as maternal smoking, lower nutritional or socio-economic status and increased meat and egg consumption during pregnancy have also been identified [1,2,3,4,5,6].
From a clinical perspective, the malformation may manifest as the fusion of soft tissue or bones, leading to the fusion of the fingers characterised as complete or incomplete. This fusion may encompass the phalanges and may also extend to the carpal/tarsal bones, It could even reach the metacarpal’s or metatarsal’s level, and rarely it may extend to the distal end of the forearm or lower leg [1,2,3]. The malformation can be further categorised as simple, complex and complicated. It can exhibit symmetry or asymmetry and may affect one side (unilateral) or both sides (bilateral), affecting the right, left or both sides and feet, hands, or both. This condition may present as an isolated malformation (non-syndromic) or as a characteristic feature of hundreds of recognised syndromes. The classification system for non-syndromic syndactyly, initially proposed by Temtamy and McKusick is based on the phenotypic appearance. This classification was extended by Malik et al. in 2012. Currently, non-syndromic syndactyly is classified into nine primary types by the Temtamy and McKusick classification, which are further divided into subtypes [2,3,4]. Non-syndromic syndactyly is predominantly isolated, but it can occur together with other disorders or malformations such as synostosis, acro-syndactyly, cleft hand, clinodactyly, synonychia or polydactyly. On the other hand, syndromic syndactyly can be observed in specific conditions like Apert Syndrome, Poland’s Syndrome, Pfeiffer Syndrome and numerous others [1,2,3,4].
Diagnosing the condition relies primarily on patient history and physical examination. Notably, the deformity may be apparent at birth or even detectable on ultrasound images during fetal development. Treatment typically necessitates surgical intervention, as potential benefits outweigh the associated risks. However, surgery is contraindicated in cases of mild syndactyly where functionality is preserved, complex syndactyly with risk of functional deterioration due to surgery, or medical conditions that interfere with the surgical approach. Careful consideration of the specific situation is essential to determine appropriate therapy [1,4,7].
The surgery is ideally performed at around 12 months of age to allow for uninterrupted growth and minimise the risks of postoperative complications. Reconstruction should be concluded before the child reaches school age [1,7,8,9]. The specific surgical approach varies based on the classification of the malformation and its individual features. Careful consideration and comprehensive assessment of the condition will guide the selection of the most appropriate surgical technique. Similar flaps are employed in both simple and complete syndactyly cases, including the use of rectangular, triangular, omega and multilobed flaps. Other methods such as Z-plasty, four-flap Z-plasty, double-opposing Z-plasty, Cronin’s technique, Sharma’s method, or the “open-finger” method can also be utilized[1,7]. However, it is important to note that the “open-finger” method has raised concerns due to the potential for secondary cicatrix formation, scar contracture and hypertrophic scarring, leading to controversies regarding its application [3,7]. Surgical release procedures utilising skin grafting encompass a variety of methods such as the M-V flap, reverse W-M flap, Flatt technique, dorsal omega flap, or the combination of V-Y and rectangular flaps [1,7,8]. Alternatively, operational methods designed to mitigate the need for grafts include trilobed flap, three-square flap, reverse-triangular flap, open finger technique, V-M plasty, end of skin graft, or the modified bell-bottom flap [1,7]. Each technique has its advantages and limitations, with selection based on the case’s specifics and the surgeon’s expertise. In complex cases, surgical planning may involve the utilisation of multiple approaches, potentially necessitating several surgeries and the implementation of multiple flaps, which carry a higher risk for complications. During surgery, a significant emphasis should be placed on meticulously assessing the patient's neurovascular structures. The course of these structures is often unpredictable, unlike the normal anatomical structure. The amount of osseous involvement directly correlates with the extent of neurovascular involvement and the associated risk of injury[1,7]. Simple cases are resolved by surgery with improvement in hand function, resulting in digits that are freely movable. The correction of complex syndactyly often carries the risk of reoperation, contractures and scarring, potentially leading to loss of function. Intraoperative complications, namely neurovascular injury, mandate immediate and diligent care to prevent loss of the affected appendage and minimise any negative functional consequences. Postoperative complications that may arise include infections, graft maceration or failure, wound dehiscence (separation of wound edges), web creep (recurrence of webbing due to growth), scar hypertrophy, nail deformities, and joint contractures [1,7,8,10].
Clinodactily refers to the congenital curvature of a digit beyond the metacarpophalangeal (MCP) joint. When the angular deviation is within physiological limits, typically fewer than 5 to 10 degrees, it is considered a normal variation [11,12]. However, if the coronal angulation exceeds 10 degrees, it is classified as a pathological deformity. This curvature seen in clinodactyly is primarily attributed to the abnormal triangular or trapezoidal shape of one or more phalanges, leading to the misalignment of the interphalangeal joint(s) involved [11,12]. This malformation causes the affected finger to exhibit an asymmetric longitudinal growth, yielding the curved appearance of the finger. Clinodactyly can occur as syndromic, familial (inherited) or sporadic (occurring by chance). Classified by Burke and Flatt into four groups: (1) familial, (2) other congenital anomaly, (3) due to epiphyseal injury (4) due to triphalangeal thumb. This classification is sufficient to diagnose and find the origin of the malformation; however, it is not suitable for choosing the appropriate treatment option [11,13,14]. Cooney’s classification system differentiates between simple and complex clinodactyly and takes into account the curvature (deviation in degrees) and the involvement of surrounding tissues [12,15,16]. The most recent classification, expanded by Ali et al. is based on the severity of angular deviation. Composed of four groups, with the first group involving physiological curvature up to 5 degrees. The second group is mild curvature with a 5-10-degree deviation, while the third group includes 15-30-degree deformities and the fourth group includes patients with severe curvature greater than 30 degrees [11,12,16,17]. It most commonly affects the middle phalanx of the fifth digit, as well as the proximal phalanx of the first and second fingers. The aetiology of this condition is still not fully understood. The condition commonly affects males, frequently bilaterally, and has an occurrence rate ranging from 2-19% [11,12,17,18]. The malformation has been linked to numerous syndromic anomalies, namely, Klinefelter syndrome, Rubinstein-Taybi syndrome, Fanconi anaemia, Cenani-Lenz syndactyly, Turner syndrome, and is found in approximately 25% of children with Down syndrome [11]. The association with multiple syndromes highlights the diverse range of conditions where clinodactyly may be observed as a feature. The abnormal growth is attributed to the peculiar configuration of the proximal portion of the phalanx’s epiphyseal growth plate. This abnormal configuration contributes to the curvature of the finger during growth. In this condition, the epiphyseal plate takes on a C-shaped appearance, yielding incomplete or restricted growth on one side of the phalanx. The presence of a delta phalanx occurs when there is early and complete ossification of the physeal plate, leading to disrupted or restricted growth of the affected digit. In some cases, traumatic injuries of the plate can result in an acquired case of clinodactyly [11,12,17,19].
Diagnosis is based on a comprehensive physical exam and a detailed review of the patient’s history, which helps differentiate between the congenital or traumatic origins of the deformity [17]. A thorough evaluation should encompass range of motion testing to assess and document the impact on grasp and pinch functions. On radiographs, a C-shaped physis might be present along with the delta phalanx formation, providing insights into the underlying structural abnormalities [9,11,12,15,19].
Splinting of the affected digit is generally not recommended and has been shown to be ineffective as a treatment option [12,16,19]. In the majority of cases, conservative management through observation is preferred; surgery for cosmetic purposes is typically discouraged due to the associated complications, such as scarring and reduced joint mobility. Surgical intervention becomes necessary in instances of severe angulation and shortening, especially if the thumb or the radial digits are involved. Such cases could significantly interfere with the hand’s grasp and punch function, justifying the need for surgical correction. The operative technique for clinodactyly is referred to as corrective osteotomy, which is ideally performed at a skeletally mature age to minimise the risk of physeal injury and excessive or inadequate correction [18]. Various methods could be employed, including reverse wedge osteotomy, opening or closing wedge osteotomy, and epiphyseal bracket resection and fat grafting. In open wedge osteotomy, bone grafting is typically performed, enabling the preservation or even an increase of the length of the digit. In contrast, closed wedge osteotomy often results in some degree of shortening [16,20]. Mild soft tissue deficits that are created can be managed with “Z”-plasty. In contrast, severe soft tissue defects might demand advancement or rotational flaps for adequate coverage and optimal wound healing. “Vikcer’s physiolysis”, also known as epiphyseal bracket resection and fat grafting, is an alternative method of treatment that can be employed in patients with open growth plates. During this procedure, the cartilaginous or osseous bracket of the short end of the digit is surgically resected and interposed, and the resulting void is filled with fat tissue [18,21]. Indeed, the process of longitudinal growth over the course of one to two years is expected to correct the angulation. This approach has demonstrated its effectiveness in comparison to osteotomy, particularly when dealing with deformities that are less than 55 degrees [11,18]. Complications include growth arrest, skin deficits, scarring, stiffness, over or under-correction, and the risk of infection [11,18,20].
2. Materials and Methods
2.1. Case Description:
A girl born in June of 2019 was diagnosed with congenital malformation of the right hand at birth — affecting the right middle, ring and little fingers, respectively. Upon physical examination, the III. digit deviates from its origin at the metacarpophalangeal joint (MCP) radially approximately 45 degrees, while the IV. finger deviates to the ulnar side 45 degrees from the MCP joint. Clinodactyly is apparent when looking at the proximal-interphalangeal (PIP) joints of the III and IV. finger, as they are positioned in a close to 90-degree deviation. Between the IV and V., finger webbing was visible, resembling a plate, adding to the syndactyly component of the malformation (Figure 1A). The fingers' PIP and distal interphalangeal (DIP) joints were movable; however, passive flexion and extension were restricted. The passive flexion of the MCP was close to 90 degrees, while extension was limited. Radiological evaluation revealed a common metacarpal of the III and IV. finger (Figure 1B). Altogether, there were only four metacarpal bones in the patient's hand. The common MCP joint was fused with the proximal phalanxes of the middle and ring fingers. The plate acquired a deviated position which led to the angular displacement of the fingers. The PIP joints’ clinodactyly was apparent as the large degree of deviation speaks for itself. In this case, the middle finger’s deviation was a close 90-degree deviation towards the ulnar side, while the ring finger deviated radially approximately 40 degrees with the interdigital webbing of the little and ring fingers (Figure 1C). Functionality was restricted both actively and passively, with some flexion present. Grasp and pinch function was decreased as the child could not hold items in their palm faced down. When grabbing items the child used the index finger and thumb to hold onto the object. These findings formed the diagnosis of clino-syndactyly of the III and IV. finger’s base and PIP joints, with incomplete cutaneous syndactyly of the IV and V. digits, paired with metacarpal aplasia of the IV. metacarpal bone.
Figure 1.
Pre-operative pictures depicting the malformations (A and C). The radiograph shows the degree of deviation and the missing metacarpal (B).
Figure 1.
Pre-operative pictures depicting the malformations (A and C). The radiograph shows the degree of deviation and the missing metacarpal (B).

2.2. Surgical Method:
Surgical intervention was advocated for, which included a wedge osteotomy to correct the synchondrosis at the phalangeal base, and a dorsal flap to close the interdigital space that was created during the correction of the III. and IV. fingers. A trapezoid flap was applied for the release of the syndactyly of the IV and V. fingers. Clinical application of the technique was accepted and permitted by our medical review board, the Hungarian Pediatric Trauma Committee, and the Hungarian Pediatric Surgery Committee. The work was performed in Pécs, at the Surgical Division, Department of Paediatrics, Medical School, University of Pécs, 7 József Attila Street, Pécs, H7623, Hungary.
Prior to undergoing general anaesthesia, the patient received antibiotic prophylaxis. The operation took place in exsanguinated conditions, which totalled 110 minutes, with the patient in a supine position. The patient received postoperative anticoagulant therapy, as is used routinely.
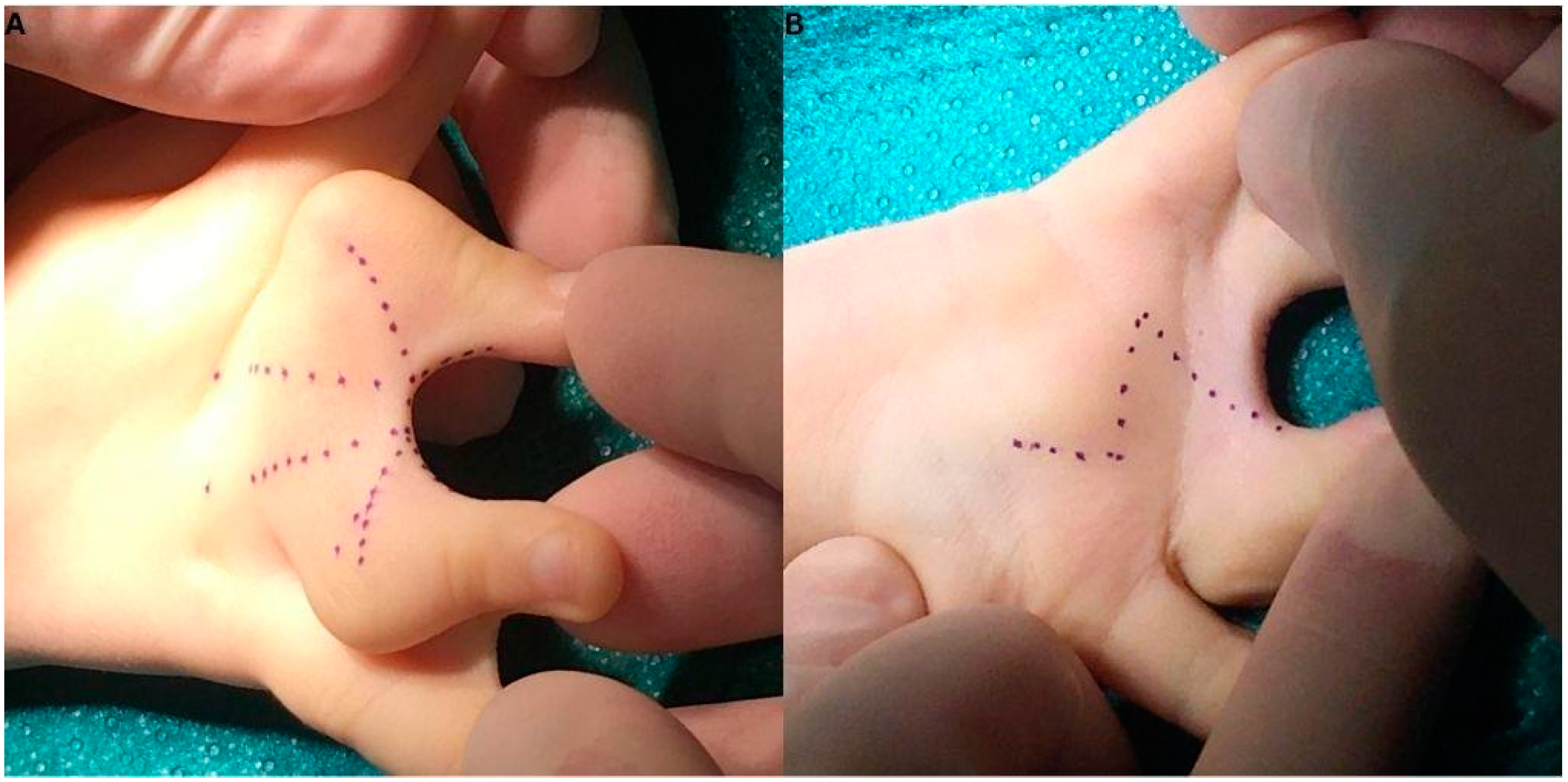
After disinfection and draping, the incision lines on the palmar and dorsal surface of the right hand were marked (Figure 2). As the first step, we aspired to solve the clino-syndactyly of the III. and IV. finger’s base by wedge osteotomy and utilisation of a dorsal flap, after which we focused on the webbing between the IV and V. fingers. The latter was repaired by the application of trapezoidal island flaps.
Figure 2.
Incision lines can be seen in a W-pattern, combining a rectangular flap and a Z-plasty method. Between the III. and IV. fingers dorsal aspect (A) and on the palmar side a Z-pattern (B).
Figure 2.
Incision lines can be seen in a W-pattern, combining a rectangular flap and a Z-plasty method. Between the III. and IV. fingers dorsal aspect (A) and on the palmar side a Z-pattern (B).
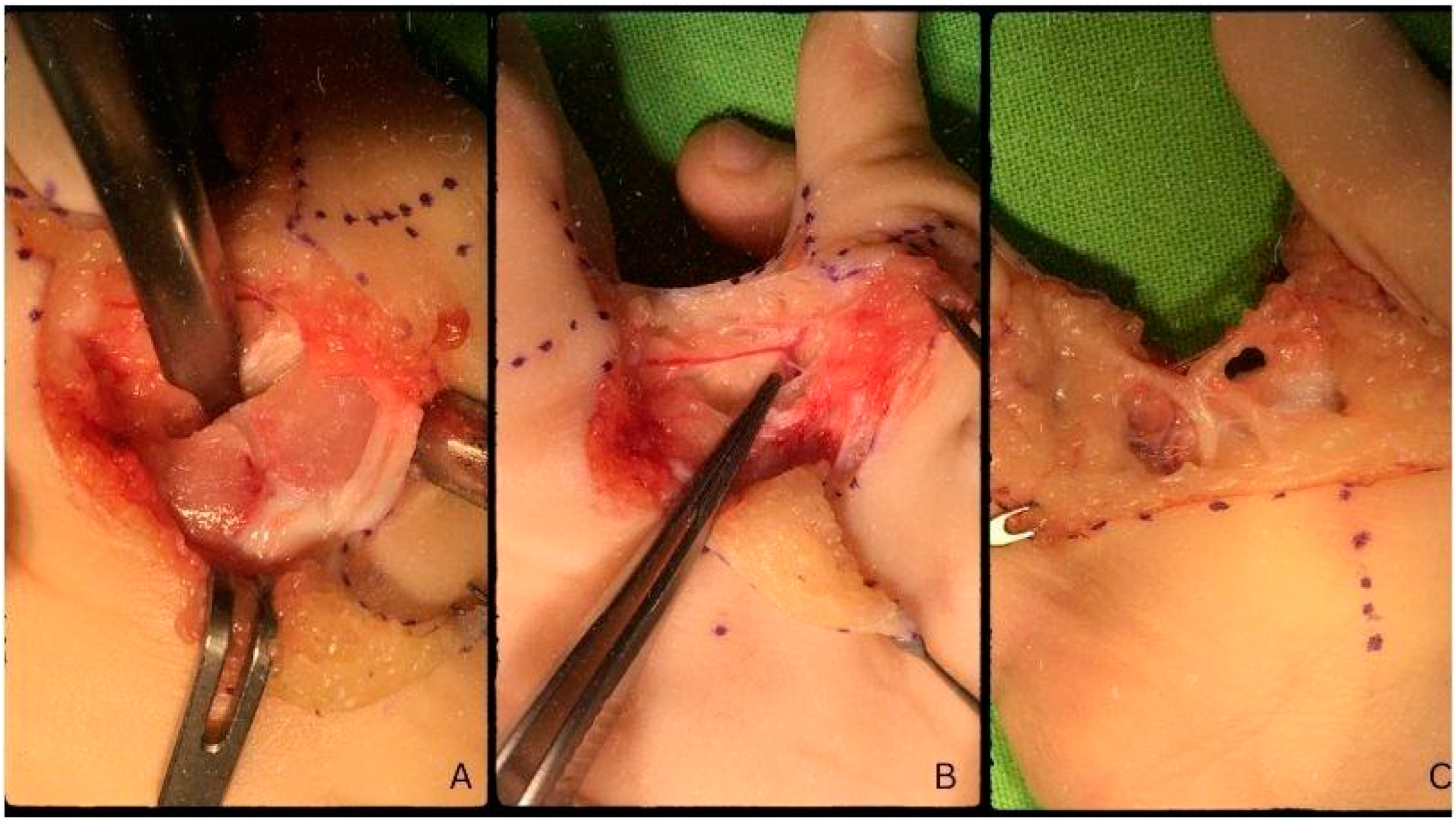
We followed the incision lines based on the designed Dorsal W-Z flap, first dorsally, then palmarly. As a first step, the digital artery and nerve (Figure 3), which was positioned quite distally, were identified. Proximally, at the base of the proximal phalanges, the synchondrosis became visible (Figure 3). After marking the appropriate position of the osteotomy, with the help of an oscillating saw, a part of the synchondrosis together with a small piece of the metaphysis was removed without coming into contact with the growth plates of the proximal phalanges. Thereby performing a closed wedge osteotomy. With the help of a Luer, we deepened the area after which we could rotate the fingers medially, towards each other. Upon volar approach, we noted that the branching of the digital nerve takes place rather distally. With the help of micro-equipment, we separated the common digital nerve so its branching was positioned more proximally in order to aid the turning of the fingers into the ideal position. We lead a strong 2/0 Vicryl® absorbable thread, subperiostally around the bone, in order to bring the III. and IV. radi closer to each other. Before final fixation, we applied the dorsal flap, which was meant to cover the interdigital space between the fingers. Subsequently, we tied the strong 2/0 (Vicryl®)thread so that the two proximal phalanges were positioned parallel to each other. After confirming the adequate position of the fingers, the remaining soft tissue defects were covered by the flaps yielding no deficits of any kind. We sutured the area with 6/0 (Vicryl®) absorbable thread by the application of interrupted and continuous sutures.
Figure 3.
Synchondrosis at the base of the proximal phalanges (A). Digital artery (B). Common digital nerve prior to separation (C).
Figure 3.
Synchondrosis at the base of the proximal phalanges (A). Digital artery (B). Common digital nerve prior to separation (C).
At this point, the process of exsanguination was temporarily halted to check the circulation of the fingers, which was ideal. All surgeons present agreed to correct the IV. and V. fingers interdigital webbing to ease the syndactyly affecting the ring and little fingers as well. To achieve this, incision lines were marked in the shape of two trapezoid flaps, facing each other between the fingers (Figure X). One was marked on the palmar side, while the other was positioned dorsally. This created a soft tissue defect, approximately 2x0.5 cm, over the ring finger’s proximal phalanx which was covered by a full-thickness skin graft obtained from the excess skin of the little finger. After making sure that the interdigital fold was well positioned and acquired a deep enough orientation, the flaps were sutured with a 6/0 thread and continuous suture technique. We applied Bacitracin containing swathing and bandaging, after which the exsanguination was terminated, this time permanently. We checked for capillary reflex and proper microcirculation when we noticed that the ring finger differed in colour from the rest of the fingers. It was whitish, therefore we removed and reapplied new swathing and bandages in a more loose fashion. Following this, the microcirculation of the finger returned to normal and signs of arterial congestion ceased.
2.3. Post-Operative Therapy and Follow-Up:
Post-op antibiotic prophylaxis was given in the form of Augmentin (Amoxicillin + Clavulanic Acid) syrup 3x4 ml for seven days. During the early postoperative period, there were no signs of circulatory anomalies and the microcirculation was continuous. The control radiograph described the post-osteotomy state as the fusion of the proximal phalanges’ proximal epiphyses, forming a Y-shape from a common metacarpal (Figure C). One day after surgery, during rebandaging, proper capillary reflex and microcirculation were noted, with non-reactive scarring (Figure 4). On the 3rd day after surgery, the patient was emitted to their home for recovery. On control examination, ten days after surgery, circulation was adequate with proper capillary reflex. On the dorsal surface of the hand, a slight hematoma was visible, with mild swelling and non-reactive scars. Rebandaging and Bacitracin-containing swathing were applied. Three days later, the bandaging was removed and the wound was left to heal on its own two weeks after surgery. Further control examinations on days 21 and 35, corresponding to weeks three and five, noted the proper depth of the IV. interdigital space and adequate circulation of the fingers. The scars remained non-reactive and continued to heal while the swelling went down (Figure 5). The fingers were straight; however, functionality could not be tested yet.
Figure 4.
Post-operative images one day after surgery, dorsal side (A) and palmar side (C). Radiograph describes the postoperative state … weeks after the surgery (B).
Figure 4.
Post-operative images one day after surgery, dorsal side (A) and palmar side (C). Radiograph describes the postoperative state … weeks after the surgery (B).
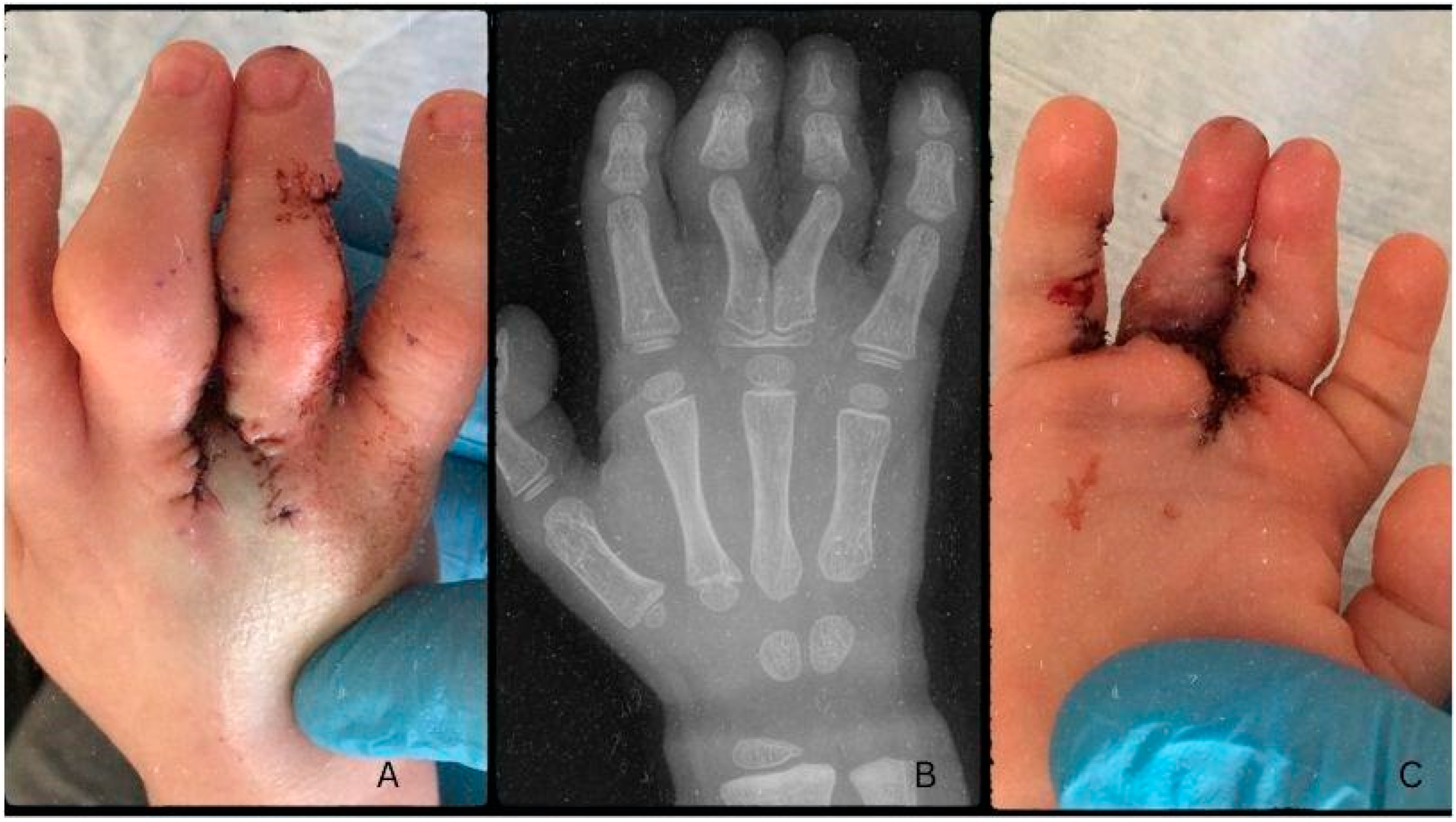
Figure 5.
Images taken five weeks after surgery (A and B). The healing is almost complete eight weeks post-op (C and D). Long-term follow-up images at 24 weeks (E and F).
Figure 5.
Images taken five weeks after surgery (A and B). The healing is almost complete eight weeks post-op (C and D). Long-term follow-up images at 24 weeks (E and F).

During the late postoperative period, the patient underwent physiotherapeutic training and daily exercise to better the functionality of the fingers. During the control examination on week 8, it was noted that the wound remained non-reactive, and the swelling had completely disappeared (Figure 5). After six months (24 weeks), there was no recurrence of deformity and the wound healed with minimal scarring (Figure 5). The enhanced functionality of the fingers was described by the parents. Upon examination, the grasp and pinch functions were identical to the other side and were not lacking in strength, coordination or range of motion. The PIP joints of the III. and IV. fingers were still restricted in motion, however, their orientation was now ideal to allow for proper grasp.
3. Discussion
Numerous flap designs have been employed in the correction of cutaneous syndactyly, either with or without the use of skin grafts. Methods without skin grafting, such as the three-square flap, trilobed flap, reverse triangular V-Y flap, dorsal V-Y metacarpal flap, dancing-girl flap, open finger technique, V-M plasty, end-of-skin graft, or the modified bell-bottom flap is advised in cases of incomplete and simple syndactyly [1,7,10].
Surgical correction of more complex cases includes the Flatt technique, the dorsal omega flap, the M-V flap, the reverse W-M flap, and the combination of the V-Y and rectangular flap with full-thickness grafts. These can be obtained from various areas, such as the groin (frequently at the region of the anterior superior iliac spine), the dorsal or lateral thigh, the medial upper arm, the distal wrist, or the dorsal metacarpal region [1,7]. In our case, we applied an individually made dorsal flap design to correct the III and IV. fingers syndactyly. This approach entailed a palmar incision line resembling that of a Z-plasty and a dorsal flap, composed of two bilobed triangular flaps on each side with a dorsal rectangular flap in the middle, collectively forming a shape resembling a W (Figure X). For the correction of the component responsible for the IV and V. finger’s involvement, two trapezoid flaps were used, which were also individually tailored for this patient during surgical planning. These approaches enabled the surgeons to operate without the need for skin grafting from additional donor sites.
Complications of surgical correction include web creep, graft failure or maceration, infection, joint contractures and scar hypertrophy [1]. Factors that play a role in the formation of web creep after surgery include complex syndactyly, wound dehiscence, secondary healing due to graft failure, the use of split-thickness skin graft, and poor flap design. Graft failure or maceration is often associated with active children and improper immobilisation and, if substantial, requires a secondary grafting procedure. Joint contractures which are due to contracture of scars on the palmar aspect of the interphalangeal joints can be corrected by Z-plasty or skin grafting[1,7,8].
Clinodactyly, as mentioned, can be corrected by open or closed wedge osteotomy, reverse wedge osteotomy, and by Vicker’s physiolysis [11,12,18]. All methods have their advantages and disadvantages; however, in this case, we applied closed wedge osteotomy. This is due to the fact that the base of the fingers was fused forming a synchondrosis. As there was a single metacarpal connecting to both proximal phalanges, the removal of a wedge was necessary for achieving proper positioning. Both reverse wedge and open wedge methods were unfit for this particular case as the open wedge technique would have required a more aggressive operative approach, while reverse wedge osteotomy was deemed unfit as it would have required two wedges in order to turn both fingers appropriately. These would've required more extensive open surgery and hence, would've led to more scar formation. Complications include loss of motion, recurrence of deformity, infection, nonunion, or joint stiffness [11,16,17].
The osteotomy was performed at the phalangeal base; the synchondrosis was released, deepened and rotated to achieve the proper positioning of the fingers. The unlikely location of the curvature called for a unique approach to preserve the functionality of the III. and IV. finger. As the base of the digits fused, forming a synchondrosis on top of a common metacarpal, their orientation at the joint mandated careful repositioning to avoid loss of function or loss in the range of motion. By removing the wedge-shaped fragment from the fused joints, encompassing a bit of the metaphysis, we enable the rotation of the base of the digits into the appropriate position. The digits were fixed following the osteotomy with 2/0 absorbable (Vicryl®) thread in their final position. This was achieved by threading the suture line around the bone subperiosteally and utilising it to turn and fixate the fingers in an ideal position. The dorsal flaps were closed on the interdigital space for adequate coverage after repositioning. Interrupted and continuous intercutaneous sutures were applied for wound closure with 6/0 absorbable (Vicryl®) thread for best results. We cut and realigned the base of the fingers so that the growth plates were not affected to preserve the lengthening of the fingers during the growth period.
The patient was aged three at the time of the surgery and two years post-op; the child presents good functionality without complications or scarring. The growth of the fingers is symmetrical, and the deformity did not reoccur during growth. There were no signs of web creep affecting either the III. and IV. or the IV. and V. interdigital space.
Figure X:
The syndactyly affecting the ring and little finger was released by designing an island flap in the form of two trapezoid shapes. The release was successful and besides the soft tissue deficit, that was created during the first incisions which formed the flaps, the operation was unremarkable. The approximately 2x0.5 cm defect was closed by the use of a skin graft which was obtained from the excess skin of the V. finger’s flap. We decided on the local graft instead of a rotational flap as the turning of the lobe would’ve placed the skin under tension in a way not suitable for healing. To avoid this, we utilised the excess skin and grafted a piece onto the IV. finger’s inner side, facing the interdigital space.
Figure Y:
4. Conclusions
Firstly, we wanted to show that even after age one, in a complicated case, syndactyly could be corrected. The patient was aged three at the time of the surgery, with two subsequent malformations affecting the right hand. Regardless, the surgery was successful, and even though one metacarpal was amiss, we managed to correct the curvature of the fingers while salvaging vital arteries and nerves and bettering the functionality of the affected hand.
The malformation formed a rare orientation at the MCP joint, which was challenging to correct as it required pre-op planning and careful execution during surgery. We hope to contribute with this report to the correction of inborn hand deformities. Furthermore, the surgical, therapeutical, and post-operative treatment descriptions could be of high value to those who meet a similar case, to them, we dedicate this report.
Author Contributions
Conceptualization, J.G. and N.H.; methodology, J.G.; software, N.H and A.L.; validation, J.G., N.H. and A.L.; formal analysis, N.H. and A.L.; investigation, N.H.; resources, J.G.; data curation, J.G.; writing—original draft preparation, N.H.; writing—review and editing, N.H. and A.L.; visualization, J.G., V.M., and K.T.; supervision, J.G.; project administration, J.G.; funding acquisition, J.G. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported, in part, by the …..(grant number) and by the Medical School, University of Pécs. The funders had no role in study design, data collection and analysis, the decision to publish, or manuscript preparation. The APC was funded by ……
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of the Surgical Division, Department of Paediatrics, Medical School, University of Pécs (protocol code XXX and date of approval) for studies involving humans.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient’s guardians to publish this paper.
Data Availability Statement
The data is contained within this article.
Acknowledgements
The authors would like to extend thanks to Daniel Frank M.D. and Lee Chan Young for reviewing the article for better intellectual content.
Conflicts of Interest
The authors declare no conflict of interest.
Ethical statement
Clinical application of the technique was accepted and permitted in 2010 by our medical review board, the Hungarian Pediatric Trauma Committee, and the Hungarian Pediatric Surgery Committee. The work was performed in Pécs and Budapest at the Surgical Division, Department of Paediatrics, Medical School, University of Pécs, 7 József Attila Street, Pécs, H7623, Hungary and at the Department of Paediatric Traumatology, Péterfy Hospital, Manninger Jenő National Trauma Center, 1081, 17 Fiumei Street, Budapest, Hungary.
References
- Mahindroo, S.; Tabaie, S. Syndactyly in the Pediatric Population: A Review of the Literature. Cureus 2023, 15. [Google Scholar] [CrossRef] [PubMed]
- Malik, S. Syndactyly: Phenotypes, Genetics and Current Classification. Eur. J. Hum. Genet. 2012, 20, 817–824. [Google Scholar] [CrossRef] [PubMed]
- Zaib, T.; Rashid, H.; Khan, H.; Zhou, X.; Sun, P. Recent Advances in Syndactyly: Basis, Current Status and Future Perspectives. Genes 2022, 13, 771. [Google Scholar] [CrossRef] [PubMed]
- Cassim, A.; Hettiarachchi, D.; Dissanayake, V.H.W. Genetic Determinants of Syndactyly: Perspectives on Pathogenesis and Diagnosis. Orphanet J. Rare Dis. 2022, 17, 198. [Google Scholar] [CrossRef]
- Luo, J.; Fu, C.; Yao, K.; Hu, R.; Du, Q.; Liu, Z. [A case-control study on genetic and environmental factors regarding polydactyly and syndactyly]. Zhonghua Liu Xing Bing Xue Za Zhi Zhonghua Liuxingbingxue Zazhi 2009, 30, 903–906. [Google Scholar]
- Man, L.-X.; Chang, B. Maternal Cigarette Smoking during Pregnancy Increases the Risk of Having a Child with a Congenital Digital Anomaly. Plast. Reconstr. Surg. 2006, 117, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Braun, T.L.; Trost, J.G.; Pederson, W.C. Syndactyly Release. Semin. Plast. Surg. 2016, 30, 162–170. [Google Scholar] [CrossRef] [PubMed]
- McGarry, K.; Martin, S.; McBride, M.; Beswick, W.; Lewis, H. The Operative Incidence of Syndactyly in Northern Ireland. A 10-Year Review. Ulster Med. J. 2021, 90, 3. [Google Scholar]
- VICKERS, D. Clinodactyly of the Little Finger: A Simple Operative Technique for Reversal of the Growth Abnormality. J. Hand Surg. 1987, 12, 335–342. [Google Scholar] [CrossRef] [PubMed]
- Chouairi, F.; Mercier, M.R.; Persing, J.S.; Gabrick, K.S.; Clune, J.; Alperovich, M. National Patterns in Surgical Management of Syndactyly: A Review of 956 Cases. Hand N. Y. N 2020, 15, 666. [Google Scholar] [CrossRef] [PubMed]
- Burke, F.; Flatt, A. Clinodactyly. A Review of a Series of Cases. The Hand 1979, 11, 269–280. [Google Scholar] [CrossRef] [PubMed]
- Tse, R.; Ljungquist, K. Camptodactyly and Clinodactyly. In Congenital Anomalies of the Upper Extremity: Etiology and Management; Laub Jr., D.R., Ed.; Springer US: Boston, MA, 2015; pp. 209–217. ISBN 978-1-4899-7504-1. [Google Scholar]
- Flatt, A.E. The Troubles with Pinkies. Proc. Bayl. Univ. Med. Cent. 2005, 18, 341–344. [Google Scholar] [CrossRef] [PubMed]
- Smith, P.J.; Grobbelaar, A.O. Camptodactyly: A Unifying Theory and Approach to Surgical Treatment. J. Hand Surg. 1998, 23, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Foucher, G.; Loréa, P.; Khouri, R.K.; Medina, J.; Pivato, G. Camptodactyly as a Spectrum of Congenital Deficiencies: A Treatment Algorithm Based on Clinical Examination. Plast. Reconstr. Surg. 2006, 117, 1897–1905. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.; Jackson, T.; Rayan, G.M. Closing Wedge Osteotomy of Abnormal Middle Phalanx for Clinodactyly. J. Hand Surg. 2009, 34, 914–918. [Google Scholar] [CrossRef] [PubMed]
- Matošević, M.; Lamot, L.; Antičević, D. CAMPTODACTYLY AND CLINODACTYLY – NEW UNDERSTANDING OF KNOWN DEFORMITIES. Acta Clin. Croat. 2021, 60, 525–531. [Google Scholar] [CrossRef] [PubMed]
- Gillis, J.A.; Nicoson, M.C.; Floccari, L.; Khouri, J.S.; Moran, S.L. Comparison of Vickers’ Physiolysis With Osteotomy for Primary Correction of Clinodactyly. Hand N. Y. N 2020, 15, 472–479. [Google Scholar] [CrossRef] [PubMed]
- Kaempf, R.; Brunelli, J.P.F.; Aita, M.A.; Delgado, P.J.; Soldado, F.; Vergara, E. Bilobed Flap in Hand Clinodactyly Reconstruction: Technique Description and Result Appraisal. Rev. Bras. Ortop. 2021, 57, 642–648. [Google Scholar] [CrossRef]
- Piper, S.L.; Goldfarb, C.A.; Wall, L.B. Outcomes of Opening Wedge Osteotomy to Correct Angular Deformity in Small Finger Clinodactyly. J. Hand Surg. 2015, 40, 908–913. [Google Scholar] [CrossRef] [PubMed]
- Vickers, D. Clinodactyly of the Little Finger: A Simple Operative Technique for Reversal of the Growth Abnormality. J. Hand Surg. Edinb. Scotl. 1987, 12, 335–342. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



