Submitted:
30 August 2023
Posted:
01 September 2023
You are already at the latest version
Abstract
Objective: Infliximab (IFX) concentrations are a predictive factor (PF) of pharmacokinetic (PK) origin in the treatment of Crohn’s disease (CD). We evaluated clearance, another PF of PK origin, either alone or in combination with concentrations. Methods: PF of PK origin were evaluated from two cohorts, the first received standard dosing (n=37), and the second was designed to proactively target therapeutic IFX concentrations (n=108). Concentrations were measured using homogenous mobility shift assay. Clearance was estimated using nonlinear mixed effects methods with Bayesian priors. C-reactive protein based clinical remission (<3mg/L in the absence of symptoms) was used for the disease control outcome. Longitudinal changes in disease control due to factors including time, IFX concentration, and clearance were analyzed using repeated event analysis. Change in objective function value (∆OFV) was calculated to compare concentration and clearance. Results: Lower baseline clearance and proactive dosing associated with enhanced disease control during induction (p<0.01). Higher IFX concentrations and lower Clearance measured at the second, third and fourth infusion yielded improved disease control during maintenance (p<0.032). During maintenance, the association with disease control was better with clearance than with concentrations (∆OFV= -19.2; p<0.001), and the combination of both further minimized OFV (p<0.001) with markedly improved clinical yield in the presence of both PF of PK origin. Conclusion: PF of PK origin and lower clearance during induction and maintenance yielded enhanced disease control in pediatric CD treated with IFX. The combination of IFX concentration and clearance are better predictors of therapeutic outcome compared to either one alone.
Keywords:
infliximab
; pharmacokinetics
; disease control
; inflammatory bowel disease
1. Introduction
The outcome of Crohn’s disease (CD) treatment with the chimeric Tumor Necrosis Factor-α (TNF-α) neutralizing agent infliximab (IFX) is known to be enhanced with the knowledge of clinical pharmacokinetic (PK) and therapeutic drug monitoring (TDM)[1,2,3] measurements. The incorporation of individualized PK profiles in the dose decision making process and dose intensification strategy (DIS) [4,5] can help achieve the minimal effective concentration that neutralizes the TNF-α pathway and inflammatory burden[6].
For IFX, it is well established that higher circulating IFX concentrations are associated with a higher degree of disease control across multiple immune mediated inflammatory diseases.[2,7] The expert consensus is to implement DIS to achieve adequate exposure during treatment to sustain remission[1]. However, the association between IFX concentration and outcome is modest and additional markers reflecting exposure and effect are needed. Recently, IFX Clearance, or the propensity of the IFX containing volume to be eliminated from the body (expressed as Liters per day), has emerged as a potential predictive factor (PF) of PK origin, both before starting therapy[8,9] and during treatment[10,11]. Accelerated Clearance reflects higher inflammatory burden that significantly decreases the IFX containing volume[12]. This poor outcome of accelerated Clearance and reduced IFX exposure is further worsened in the presence of immunization and formation of antibodies to infliximab (ATI)[10].
High-level inflammatory burden present in CD often precludes achievement of effective concentrations using a standard dosing regimen[13]. It follows that DIS is often implemented, either reactively, in face of the symptomatic patient that receives too little, or proactively, to avoid the “too little and too late” issues arising from suboptimal pharmacokinetics. Several reports including observational and randomized clinical studies have established that proactive personalized dosing based on patient PK profiles associates with improved outcomes for IFX[3,14,15,16]. However, the clinical utility of proactive DIS is still a matter of debate[17,18,19]. At the PK level, another key benefit of proactive dosing is that sustained IFX exposure promotes tolerance and lessens the risk of immunization against IFX antigens, as seen in patients receiving episodic IFX treatment or carriers of HLA DQA1*05 allele[20,21,22].
In this study we evaluated the association between Clearance, either alone or in combination with IFX concentrations, with disease control. Our results show that, in addition to IFX trough concentrations, the presence of low IFX Clearance associates with enhanced disease control, where patients with optimal PK (higher IFX trough concentrations and lower IFX Clearance) are likely to do very well on IFX.
2. Materials and Methods
2.1. Patients
All patients were consented and enrolled from 2 separate cohorts of pediatric patients with CD. Patients in the first cohort (Standard dosing cohort, Cedars Sinai Medical Center, SR) received standard IFX dosing (5 mg/kg given for three consecutive doses at week 0, 2 and 6 followed by maintenance treatment every 8 weeks at the same dose). Patients in the second cohort (Proactive dosing cohort, PRECISION IFX trial [NCT02624037]) received proactive dose intensification using the iDose dashboard (Baysient, LLC, Fort Myers, FL, USA) to target therapeutic concentrations (>17 µg/mL before the third induction infusion and >10 µg/mL during maintenance). All IFX samples were assayed at Prometheus Laboratories (San Diego, CA) and reported to the clinician within 3 days of receipt (after overnight transportation)[14].
2.2. Clinical PK Testing
All specimens were collected in serum separator tubes and shipped overnight to the clinical laboratory for testing (PRECISION trial) or stored at subzero temperature (Standard dosing cohort) for testing. During induction, specimens were collected immediately before (trough) the second, third, and fourth infusion dose (corresponding to week 2, 6, and 14 on a standard dosing schedule or per the clinician’s recommendations on proactive dosing). During maintenance specimens were collected at trough before each infusion. All IFX testing was calibrated against WHO standard (NIBSC code: 16/170) and conducted in the CLIA certified clinical PK laboratory at Prometheus Laboratories (San Diego, CA). IFX and ATI were determined using drug tolerant homogenous mobility shift assay (HMSA)[23]. Albumin and CRP (C-reactive protein) levels were determined using standard immunochemistry techniques. The clinical PK parameters were estimated using a nonlinear mixed-effects modeling with Bayesian priors via Monolix (Lixoft, 2021R2, Paris France) that incorporated amount of IFX given (in mg), weight (in kg), albumin (in g/dL), ATI (positive>3.1 U/mL) and IFX concentration (in µg/mL) as described[24]. Clearance (expressed as L/day), the volume of IFX-containing serum cleared from the patient as a function of time, was calculated at each cycle; a value below 0.294 L/day (the value of the reference population) was defined as low Clearance.
Baseline Clearance (immediately before first infusion dose) for each patient was estimated using the previously reported population PK model[24] using albumin and weight
2.3. Outcome Variables
The outcome variable used was the CRP-based clinical remission status achieved during the induction and maintenance period of therapy. CRP-based clinical remission status was defined as CRP levels below 3 mg/L in the absence of disease activity (remission), as determined using the CRP level immediately before infusion. Disease activity was assessed using either the pediatric Crohn’s disease activity index (pCDAI; below 10 points indicates remission) in the Standard dosing cohort, or the Harvey Bradshaw index (below 5 points indicates remission) in the Proactive dosing cohort. During treatment the longitudinal changes in PF of PK origin (concentration and Clearance) were analyzed as continuous variables. In addition, the combined presence of PF of PK origin corresponding to higher concentration and lower Clearance immediately before first maintenance dose (infusion 4: >10 µg/mL with Clearance <0.294 L/day) and during maintenance (>5 µg/mL with Clearance <0.294 L/day) were calculated.
2.4. Statistical Analysis
Longitudinal changes in disease control (CRP-based clinical remission status as repeated categorical observation) over induction and maintenance were analyzed using non-linear mixed effects modeling with a logistic regression model via Monolix (Lixoft, 2021R2, Paris France). Covariates including baseline Clearance, treatment group (Standard and Proactive dosing), PF of PK origin (either alone as concentration and Clearance or combined) were evaluated for their impact on disease control. The addition of a covariate to the model was considered significant (p=0.05) if it decreased the -2log likelihood [-2LL] by ≥ 3.84 given one degree of freedom (based on the χ2 distribution). Mann-Whitney and Fisher Exact tests were used as appropriate.
Time to CRP-based clinical remission status achieved during treatment was estimated using standard Kaplan-Meier analysis. The Hazard ratio (HR) corresponding to the ratio of the rate of CRP-based clinical remission achieved in the presence or absence of the PF of PK origin where higher HR represented improved rates of remission and thus enhanced disease control. The specific PF of PK origin considered were IFX levels above threshold at the second (>20 µg/mL), third (>15 µg/mL) and fourth (>10 µg/mL) infusion during induction, and above 5 µg/mL during maintenance starting at the fifth dose (week 22 on a standard dosing) either alone or in combination with lower Clearance (<0.294 L/day).
3. Results
3.1. Baseline Clearance
Patient demographics across the two cohorts are reported in Table 1. The association between concentration and Clearance at each of the time points of the induction period and during maintenance is provided in Figure S1. As expected, repeated event analysis over the induction period revealed that disease control increased with time under treatment (log odds: +0.042±0.008 per day) (p<0.001; -2LL: 470.9). Patients from the Proactive dosing cohort had higher baseline Clearance (median 0.271 L/day; IQR: 0.227-0.327 L/day) than those from the Standard dosing cohort (median 0.234 L/day; IQR: 0.179-0.260 L/day) (p<0.01) (Table 1). Accounting for time, treatment group and baseline Clearance, higher baseline Clearance predicted reduced disease control during induction (log odds: -5.77±2.4 per each L per day) (p=0.016), and Proactive dosing treatment resulted in better disease control compared to Standard dosing (log odds: 2.53±0.61, p<0.001)(∆OFV=-25.1; p<0.01). The probability of achieving disease control during induction is presented in Figure 1.
3.2. Pharmacokinetic Parameter during Induction and Outcomes
The impact of IFX concentration and Clearance at each induction time point (immediately before second, third and fourth dose) on disease control achieved during maintenance is presented in Table 2. Higher IFX concentrations measured at the second, third and fourth infusion yielded improved disease control during maintenance (log odds=+0.045±0.021, +0.114±0.027 and +0.136±0.032, per µg/mL, respectively) (p<0.032) with significant decrease in OFV (p≤0.020) compared to the base model (time only). Conversely, higher Clearance measured before the second, third, or fourth infusions predicted worse CRP-based clinical remission during maintenance (log odds=-7.43±2.88, -8.35±2.3 and -11.90±2.79 per each L/day immediately, respectively) (p≤0.001). Analysis with both IFX concentration and Clearance revealed that the combination of concentration and Clearance together further minimized the OFV as compared to the best OFV achieved with either PF of PK origin alone at the second (∆OFV=-4.7 [349.7 vs 355.3]; p=0.030) and fourth infusion (∆OFV=-6.2 [385.5 vs 398.3]; p=0.013).
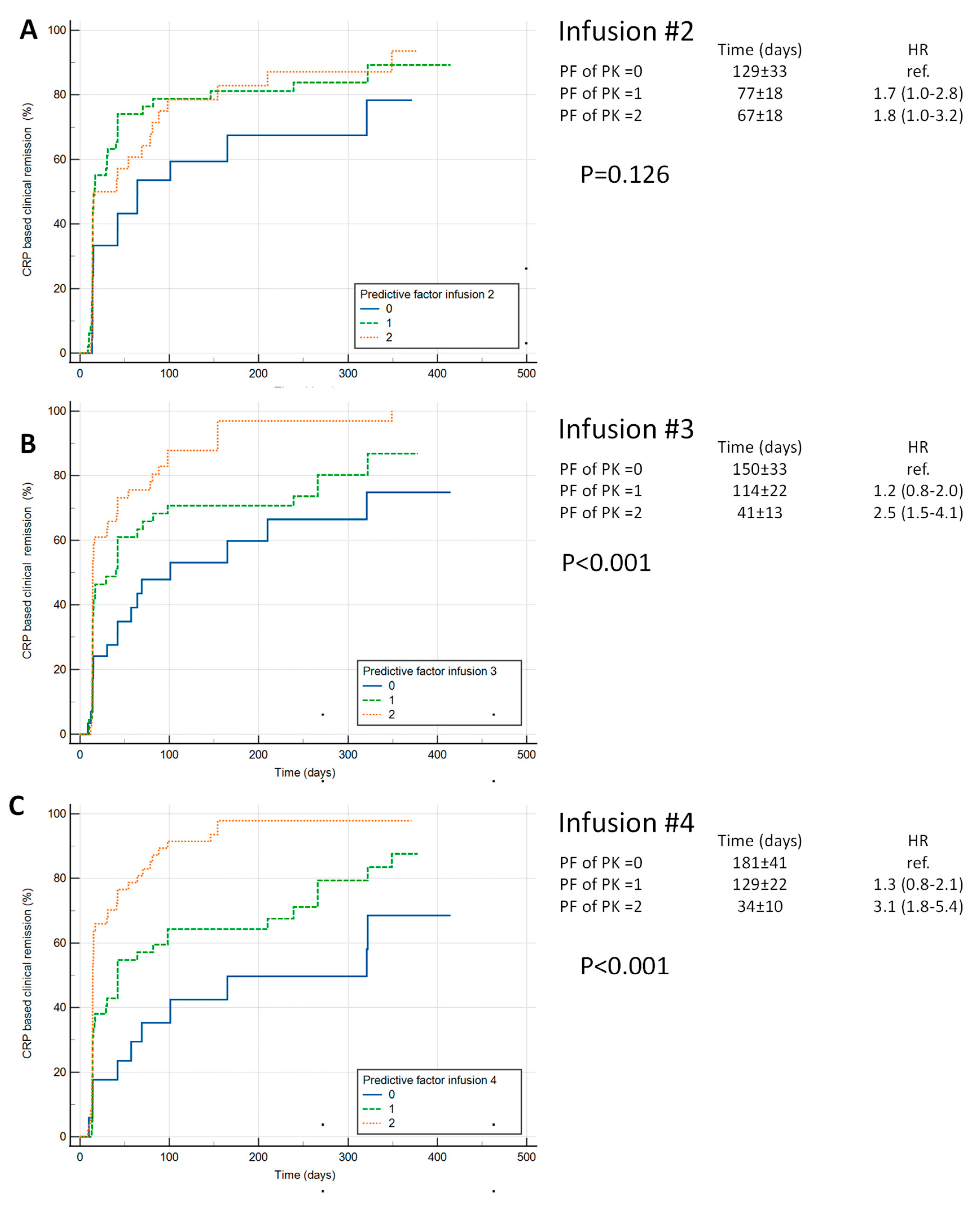
Time to CRP-based clinical remission status generally confirmed these findings with higher rate of remission with lower Clearance and higher concentration (supplementary Table S1 and Figure S2) during induction. The combined PF of PK origin corresponding to lower Clearance (<0.294 L/day) and higher IFX concentrations (above 20 µg/mL, 15 µg/mL and 10 µg/mL at second, third and fourth infusion, respectively) each associated with shorter time to remission. Furthermore, lower IFX Clearance at the second, third and fourth infusion of the induction period all significantly associated with higher likelihood of sustained CRP-based clinical remission status during maintenance (Table 3).
3.3. Pharmacokinetic Parameter during Maintenance and Outcomes
The impact of IFX concentration and Clearance on outcome during maintenance is presented in Table 4. Higher IFX concentration and lower Clearance associated with improved outcome (log odds=+0.12±0.027 per µg/mL and -16.71±2.28 per L/day, respectively (p<0.001) with Clearance having significantly stronger effect than concentration with lower OFV (380.8 vs 400.0; ∆OFV=-19.2; p<0.001). In addition, the combination of IFX concentration and Clearance outperformed either one alone (∆OFV=-19.0 [400 vs 371.0; p<0.001] versus concentration alone and ∆OFV=-10.8 [380.8 vs 371.0; p<0.001] versus Clearance alone).
A total of 419 cycles with clinical status were collected in the group of 135 patients who entered maintenance (>4 infusions). Overall, there was a greater proportion of maintenance cycles with both PF of PK origin (lower Clearance [<0.294 L/day] and higher concentration [>5µg/mL]) in the group of patients enrolled in the Proactive dosing cohort (79%, 236/299) as compared to the Standard dosing cohort (42%, 50/120) (p<0.01). Repeated event analysis during maintenance revealed that the presence of both PF of PK origin (concentration>5 µg/mL with Clearance <0.294 L/day) yielded enhanced disease control (p<0.001) with lower OFV as compared to IFX concentration above 5 µg/mL alone (∆OFV=-12.6 [361.6 vs 349.0]; p<0.001) or Clearance below 0.294 L/day alone (∆OFV=-4.7 [353.7 vs 349.0]; p=0.030). Finally, the presence of both PF of PK origin immediately before the first maintenance infusion (concentration>10 µg/mL with Clearance below 0.294 L/day) further produced additional clinical benefit and minimization of OFV (∆OFV=-10.6; [349.0 vs 338.4]; p<0.001) (Table S2 and Figure 3).
Figure 2.
Predictive factors of Pharmacokinetic origin in association with CRP-based clinical remission status.
Figure 2.
Predictive factors of Pharmacokinetic origin in association with CRP-based clinical remission status.
4. Discussion
This report evaluated predictive factors (PF) of pharmacokinetic (PK) origins, lower Clearance, and higher trough concentrations, either alone or in combination, as indicators of achieving optimal PK and disease control in pediatric patients with CD receiving treatment with IFX. Our rationale was that lower Clearance, and thus improved retention of IFX-containing volume available for the neutralization of inflammatory burden, would associate with improved disease control, simply the opposite of what is typically observed in the presence of active disease that eliminates IFX and worsens in the presence of immunization against IFX [25,26,27].
This was a retrospective exploratory analysis and our data suggest enhanced disease control achieved in the group of patients undergoing Proactive dosing (log odds: 2.53±0.61 vs Standard dosing), thereby adding to the body of evidence that this DIS (by model-informed precision dosing tools coupled with HMSA assay) has strong clinical utility and higher clinical yield as compared to Standard dosing[11,14]. We noticed that baseline Clearance associated with worse outcomes as already reported[9], an impact that was significant after adjusting for the treatment group where the potential negative impact of higher baseline Clearance in the group of patients who received Proactive dosing was minimized. We acknowledge that the absence of a comparator group undergoing reactive DIS and the lack of a randomized control group does not allow us to draw conclusions on the superiority of proactive dosing versus other DIS as seen with other IFX[3,15] and adalimumab[28] reports. Yet, the data suggests that enhanced disease control was achieved in the proactive group from optimal management of dosing and exposure commensurate with inflammatory burden, as reported.[29,30,31,32]
As expected, higher IFX concentrations during induction predicted improved outcomes during maintenance, further adding to the body of evidence that optimal exposure achieved early is important for patient outcomes. Moreover, lower Clearance during induction also predicted better disease control, and these data are consistent with the notion that sufficient neutralization of TNF-α allows greater retention of IFX in the central compartment, the opposite of what is observed in the presence of higher inflammatory burden and tissue inflammation that serves as a sink for IFX with attendant accelerated Clearance, as reported[6].
In combination, lower Clearance and higher drug concentrations during induction yielded improved disease control during maintenance, where the objective function value (OFV) was minimized as compared to concentration and Clearance alone, thus suggesting that the measurement of Clearance might provide additional value in clinical practice, where further clinical improvements can be expected in the presence of higher concentration and lower Clearance. This was also confirmed in maintenance, where Clearance was superior to concentration (lower OFV) and the combination of Clearance and concentration together outperformed either one alone. These data support the assertion that Clearance is as good as concentration, if not better, in associating with clinical outcomes, likely due to an underlying degree of causality with improvements in clinical benefit; this supports the clinical utility of PK measures for patients with IBD[3,14,33]. While it will be important to validate this concept in additional cohorts of patients receiving IFX, this finding of better outcomes in a group of patients with improved IFX retention, as indicated by lower Clearance and higher exposure, is novel. It is, further, tempting to suggest that the combination of these PF of PK origin may also associate with enhanced disease control for other monoclonal antibodies as we anticipate that the lower elimination of other monoclonal antibodies from the central compartment produces optimal PK and thus higher likelihood of disease control, as seen with IFX in this study. We acknowledge that endoscopy was not available in this cohort of pediatric patients with CD, and it will be important to also evaluate the impact of PF of PK origin on endoscopic remission.
Our data show that in the presence of both PF of PK origin, at the end of the induction period and during maintenance, superior disease control is achieved. It follows that optimizing IFX exposure early during induction to reach and then sustain exposure commensurate with the effective neutralization of inflammatory burden is vital to achieving and maintaining remission.
As we enter this new era of precision-guided dosing, DIS can be implemented reactively or proactively with the same goal of remediating underexposure and insufficient control of inflammation. We are not ignoring the fact that these hypotheses-generating data are subject to type 1 error and the rejection of the null hypothesis that benefit PK and Clearance could be happening by chance. While the group of patients presenting with the PF of PK origin and thus with optimal PK appear to be doing very well under IFX, it is also evident that some of these will not respond to IFX, owing to an unsuitable mechanism of action.
Additional cohorts will be important to further evaluate the impact of PF of PK origin on outcome; however, Clearance has been shown to be particularly important in pediatrics, making this data an important contribution to knowledge in pediatric IBD. Importantly, the currently active OPTIMIZE trial[30] (NCT04835506) is exploring the benefit of proactive DIS as compared to standard of care in a randomized controlled trial of patients 16 and older, which will further enhance the knowledge that we have presented herein.
Sustained CRP based clinical remission corresponds to CRP below 3 mg/L in the absence of symptoms at all maintenance cycle post induction
Probability to achieve CRP-based clinical remission status by week (2, 6 and 14) during induction by treatment group (standard and proactive) and baseline IFX Clearance (median, with interquartile range). Estimates are: θpop=2.49±0.78 (p=0.001); θcl=-5.77±2.40 per L/day (p=0.016); θproactive= +2.53±0.61 (p<0.001) ; θtime =+0.042±0.0064 per day (p<0.001)
Panel A: PF of PK origin infusion 2; Panel B: PF of PK origin infusion 3; Panel C: PF of PK origin infusion 4.
Repeated event analysis and probability of CRP-based clinical remission status over the maintenance period (>4 infusions) stratified by the presence or absence of both PF of PK origin determined immediately before the fourth infusion (IFX concentrations above 10 µg/mL with Clearance below 0.294 L/day) and during maintenance (IFX concentrations above 5 µg/mL with Clearance below 0.294 L/day). The probability of remission is given over 32 weeks of maintenance treatment. Week 0 corresponds to the start of maintenance. Estimates: θpop=0.35±0.50 (p=0.012); θtime=0.002±0.001 (p=0.046) per day (p<0.001); θboth PF of PK 4th inf=2.44±0.64 (p<0.001); θboth PF of PK= 2.51±0.73 (p<0.001)
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Figure S1 and Table S1.
Author Contributions
Conceptualization, MD, EP, SR and TD; methodology, MD, EP, SR, AE and TD; software, CP and TD.; validation, TD, AE and CP; formal analysis, CP and TD.; investigation, MD; resources, MD and TD; data curation, AE, TD and CP; writing—original draft preparation, TD; writing—review and editing, all supervision, MD and TD; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of Mount Sinai Medical Center (protocol code #15-1475; date of approval 10/14/2015).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
no data sharing available.
Acknowledgments
We acknowledge Tom Stockfish for data management, and also Judson McFarland, Michael Schwalbe and Patty Hughes from Prometheus Laboratories for management of clinical testing.
Conflicts of Interest
EAS: none. MCD is a consultant for Prometheus Laboratories, Janssen, Abbvie, Takeda, Celgene, Gilead, UCB, Pfizer, Arena, and Eli Lilly as well as co-Founder of Mi Test Health and Trellus Health. SR is a consultant for Prometheus Laboratories. JCP is a consultant for Prometheus laboratories. TD and AE are employees of Prometheus Laboratories.
References
- Cheifetz, A.S.; Abreu, M.T.; Afif, W.; Cross, R.K.; Dubinsky, M.C.; Loftus, E.V.; Osterman, M.T.; Saroufim, A.; Siegel, C.A.; Yarur, A.J.; et al. A Comprehensive Literature Review and Expert Consensus Statement on Therapeutic Drug Monitoring of Biologics in Inflammatory Bowel Disease. Am. J. Gastroenterol. 2021, 116, 2014–2025. [CrossRef]
- Vande Casteele N, Herfarth H, Katz J, et al. American Gastroenterological Association Institute Technical Review on the Role of Therapeutic Drug Monitoring in the Management of Inflammatory Bowel Diseases. Gastroenterology 2017;153:835-857 e6. [CrossRef]
- Strik, A.S.; Löwenberg, M.; Mould, D.R.; Berends, S.E.; Ponsioen, C.I.; Brande, J.M.H.v.D.; Jansen, J.M.; Hoekman, D.R.; Brandse, J.F.; Duijvestein, M.; et al. Efficacy of dashboard driven dosing of infliximab in inflammatory bowel disease patients; a randomized controlled trial. Scand. J. Gastroenterol. 2020, 56, 145–154. [CrossRef]
- Baert F, Noman M, Vermeire S, et al. Influence of immunogenicity on the long-term efficacy of infliximab in Crohn's disease. N Engl J Med 2003;348:601-8. [CrossRef]
- Irving, P.M.; Gecse, K.B. Optimizing Therapies Using Therapeutic Drug Monitoring: Current Strategies and Future Perspectives. Gastroenterology 2022, 162, 1512–1524. [CrossRef]
- Yarur, A.J.; Jain, A.; A Sussman, D.; Barkin, J.S.; A Quintero, M.; Princen, F.; Kirkland, R.; Deshpande, A.R.; Singh, S.; Abreu, M.T. The association of tissue anti-TNF drug levels with serological and endoscopic disease activity in inflammatory bowel disease: the ATLAS study. Gut 2015, 65, 249–255. [CrossRef]
- Krieckaert, C.L.; van Tubergen, A.; Gehin, J.E.; Hernández-Breijo, B.; Le Mélédo, G.; Balsa, A.; Böhm, P.; Cucnik, S.; Elkayam, O.; Goll, G.L.; et al. EULAR points to consider for therapeutic drug monitoring of biopharmaceuticals in inflammatory rheumatic and musculoskeletal diseases. Rheumatology 2022, 82, 65–73. [CrossRef]
- Casteele, N.V.; Jeyarajah, J.; Jairath, V.; Feagan, B.G.; Sandborn, W.J. Infliximab Exposure-Response Relationship and Thresholds Associated With Endoscopic Healing in Patients With Ulcerative Colitis. Clin. Gastroenterol. Hepatol. 2018, 17, 1814–1821.e1. [CrossRef]
- Battat, R.; Hemperly, A.; Truong, S.; Whitmire, N.; Boland, B.S.; Dulai, P.S.; Holmer, A.K.; Nguyen, N.H.; Singh, S.; Casteele, N.V.; et al. Baseline Clearance of Infliximab Is Associated With Requirement for Colectomy in Patients With Acute Severe Ulcerative Colitis. Clin. Gastroenterol. Hepatol. 2020, 19, 511–518.e6. [CrossRef]
- Kevans, D.; Murthy, S.; Mould, D.R.; Silverberg, M.S. Accelerated Clearance of Infliximab is Associated With Treatment Failure in Patients With Corticosteroid-Refractory Acute Ulcerative Colitis. J. Crohn’s Colitis 2018, 12, 662–669. [CrossRef]
- Kantasiripitak, W.; Wang, Z.; Spriet, I.; Ferrante, M.; Dreesen, E. Recent advances in clearance monitoring of monoclonal antibodies in patients with inflammatory bowel diseases. Expert Rev. Clin. Pharmacol. 2021, 14, 1455–1466. [CrossRef]
- Funk, R.S.; Shakhnovich, V.; Cho, Y.K.; Polireddy, K.; Jausurawong, T.; Gress, K.; Becker, M.L. Factors associated with reduced infliximab exposure in the treatment of pediatric autoimmune disorders: a cross-sectional prospective convenience sampling study. Rheumatology 2021, 19, 1–11. [CrossRef]
- Kennedy NA, Heap GA, Green HD, et al. Predictors of anti-TNF treatment failure in anti-TNF-naive patients with active luminal Crohn's disease: a prospective, multicentre, cohort study. Lancet Gastroenterol Hepatol 2019;4:341-353. [CrossRef]
- Dubinsky, M.C.; Mendiolaza, M.L.; Phan, B.L.; Moran, H.R.; Tse, S.S.; Mould, D.R. Dashboard-Driven Accelerated Infliximab Induction Dosing Increases Infliximab Durability and Reduces Immunogenicity. Inflamm. Bowel Dis. 2022, 28, 1375–1385. [CrossRef]
- Syversen, S.W.; Goll, G.L.; Jørgensen, K.K.; Olsen, I.C.; Sandanger, .; E Gehin, J.; Warren, D.J.; Sexton, J.; Mørk, C.; Jahnsen, J.; et al. Therapeutic drug monitoring of infliximab compared to standard clinical treatment with infliximab: study protocol for a randomised, controlled, open, parallel-group, phase IV study (the NOR-DRUM study). Trials 2020, 21, 1–14. [CrossRef]
- Sánchez-Hernández, J.G.; Rebollo, N.; Martin-Suarez, A.; Calvo, M.V.; Muñoz, F. A 3-year prospective study of a multidisciplinary early proactive therapeutic drug monitoring programme of infliximab treatments in inflammatory bowel disease. Br. J. Clin. Pharmacol. 2020, 86, 1165–1175. [CrossRef]
- 17. D'Haens G, Vermeire S, Lambrecht G, et al. Increasing Infliximab Dose Based on Symptoms, Biomarkers, and Serum Drug Concentrations Does Not Increase Clinical, Endoscopic, and Corticosteroid-Free Remission in Patients With Active Luminal Crohn's Disease. Gastroenterology 2018;154:1343-1351 e1. [CrossRef]
- Syversen, S.W.; Bolstad, N.; Haavardsholm, E.A. Therapeutic Drug Monitoring vs Standard Therapy During Infliximab Induction in Patients With Chronic Immune-Mediated Inflammatory Diseases—Reply. JAMA 2021, 326, 1069–1070. [CrossRef]
- Casteele, N.V.; Ferrante, M.; Van Assche, G.; Ballet, V.; Compernolle, G.; Van Steen, K.; Simoens, S.; Rutgeerts, P.; Gils, A.; Vermeire, S. Trough Concentrations of Infliximab Guide Dosing for Patients With Inflammatory Bowel Disease. Gastroenterology 2015, 148, 1320–1329.e3. [CrossRef]
- Pradeu T, Jaeger S, Vivier E. The speed of change: towards a discontinuity theory of immunity? Nat Rev Immunol 2013;13:764-9. [CrossRef]
- Sazonovs, A.; Kennedy, N.A.; Moutsianas, L.; Heap, G.A.; Rice, D.L.; Reppell, M.; Bewshea, C.M.; Chanchlani, N.; Walker, G.J.; Perry, M.H.; et al. HLA-DQA1*05 Carriage Associated With Development of Anti-Drug Antibodies to Infliximab and Adalimumab in Patients With Crohn’s Disease. Gastroenterology 2020, 158, 189–199. [CrossRef]
- Spencer, E.A.; Stachelski, J.; Dervieux, T.; Dubinsky, M.C. Failure to Achieve Target Drug Concentrations During Induction and Not HLA-DQA1∗05 Carriage Is Associated With Antidrug Antibody Formation in Patients With Inflammatory Bowel Disease. Gastroenterology 2022, 162, 1746–1748.e3. [CrossRef]
- Wang, S.-L.; Ohrmund, L.; Hauenstein, S.; Salbato, J.; Reddy, R.; Monk, P.; Lockton, S.; Ling, N.; Singh, S. Development and validation of a homogeneous mobility shift assay for the measurement of infliximab and antibodies-to-infliximab levels in patient serum. J. Immunol. Methods 2012, 382, 177–188. [CrossRef]
- Primas, C.; Reinisch, W.; Panetta, J.C.; Eser, A.; Mould, D.R.; Dervieux, T. Model Informed Precision Dosing Tool Forecasts Trough Infliximab and Associates with Disease Status and Tumor Necrosis Factor-Alpha Levels of Inflammatory Bowel Diseases. J. Clin. Med. 2022, 11, 3316. [CrossRef]
- Whaley, K.G.; Xiong, Y.; Karns, R.; Hyams, J.S.; Kugathasan, S.; Boyle, B.M.; Walters, T.D.; Kelsen, J.; LeLeiko, N.; Shapiro, J.; et al. Multicenter Cohort Study of Infliximab Pharmacokinetics and Therapy Response in Pediatric Acute Severe Ulcerative Colitis. Clin. Gastroenterol. Hepatol. 2023, 21, 1338–1347. [CrossRef]
- Colman, R.J.; Xiong, Y.; Mizuno, T.; Hyams, J.S.; Noe, J.D.; Boyle, B.; D’haens, G.R.; van Limbergen, J.; Chun, K.; Yang, J.; et al. Antibodies-to-infliximab accelerate clearance while dose intensification reverses immunogenicity and recaptures clinical response in paediatric Crohn’s disease. Aliment. Pharmacol. Ther. 2021, 55, 593–603. [CrossRef]
- Petitcollin, A.; Brochard, C.; Siproudhis, L.; Tron, C.; Verdier, M.; Lemaitre, F.; Lucidarme, C.; Bouguen, G.; Bellissant, . Pharmacokinetic Parameters of Infliximab Influence the Rate of Relapse After De-Escalation in Adults With Inflammatory Bowel Diseases. Clin. Pharmacol. Ther. 2019, 106, 605–615. [CrossRef]
- Assa, A.; Matar, M.; Turner, D.; Broide, E.; Weiss, B.; Ledder, O.; Guz-Mark, A.; Rinawi, F.; Cohen, S.; Topf-Olivestone, C.; et al. Proactive Monitoring of Adalimumab Trough Concentration Associated With Increased Clinical Remission in Children With Crohn’s Disease Compared With Reactive Monitoring. Gastroenterology 2019, 157, 985–996.e2. [CrossRef]
- Negoescu, D.M.; A Enns, E.; Swanhorst, B.; Baumgartner, B.; Campbell, J.P.; Osterman, M.T.; Papamichael, K.; Cheifetz, A.S.; Vaughn, B.P. Proactive Vs Reactive Therapeutic Drug Monitoring of Infliximab in Crohn’s Disease: A Cost-Effectiveness Analysis in a Simulated Cohort. Inflamm. Bowel Dis. 2020, 26, 103–111. [CrossRef]
- Papamichael K, Jairath V, Zou G, et al. Proactive infliximab optimisation using a pharmacokinetic dashboard versus standard of care in patients with Crohn's disease: study protocol for a randomised, controlled, multicentre, open-label study (the OPTIMIZE trial). BMJ Open 2022;12:e057656. [CrossRef]
- Papamichael, K.; Vajravelu, R.K.; Vaughn, B.P.; Osterman, M.T.; Cheifetz, A.S. Proactive Infliximab Monitoring Following Reactive Testing is Associated With Better Clinical Outcomes Than Reactive Testing Alone in Patients With Inflammatory Bowel Disease. J. Crohn’s Colitis 2018, 12, 804–810. [CrossRef]
- Fernandes SR, Bernardo S, Simoes C, et al. Proactive Infliximab Drug Monitoring Is Superior to Conventional Management in Inflammatory Bowel Disease. Inflamm Bowel Dis 2020;26:263-270. [CrossRef]
- Dubinsky, M.C.; Phan, B.L.; Singh, N.; Rabizadeh, S.; Mould, D.R. Pharmacokinetic Dashboard-Recommended Dosing Is Different than Standard of Care Dosing in Infliximab-Treated Pediatric IBD Patients. AAPS J. 2016, 19, 215–222, . [CrossRef]
Figure 1.
CRP-based clinical remission during induction by baseline Clearance and treatment.
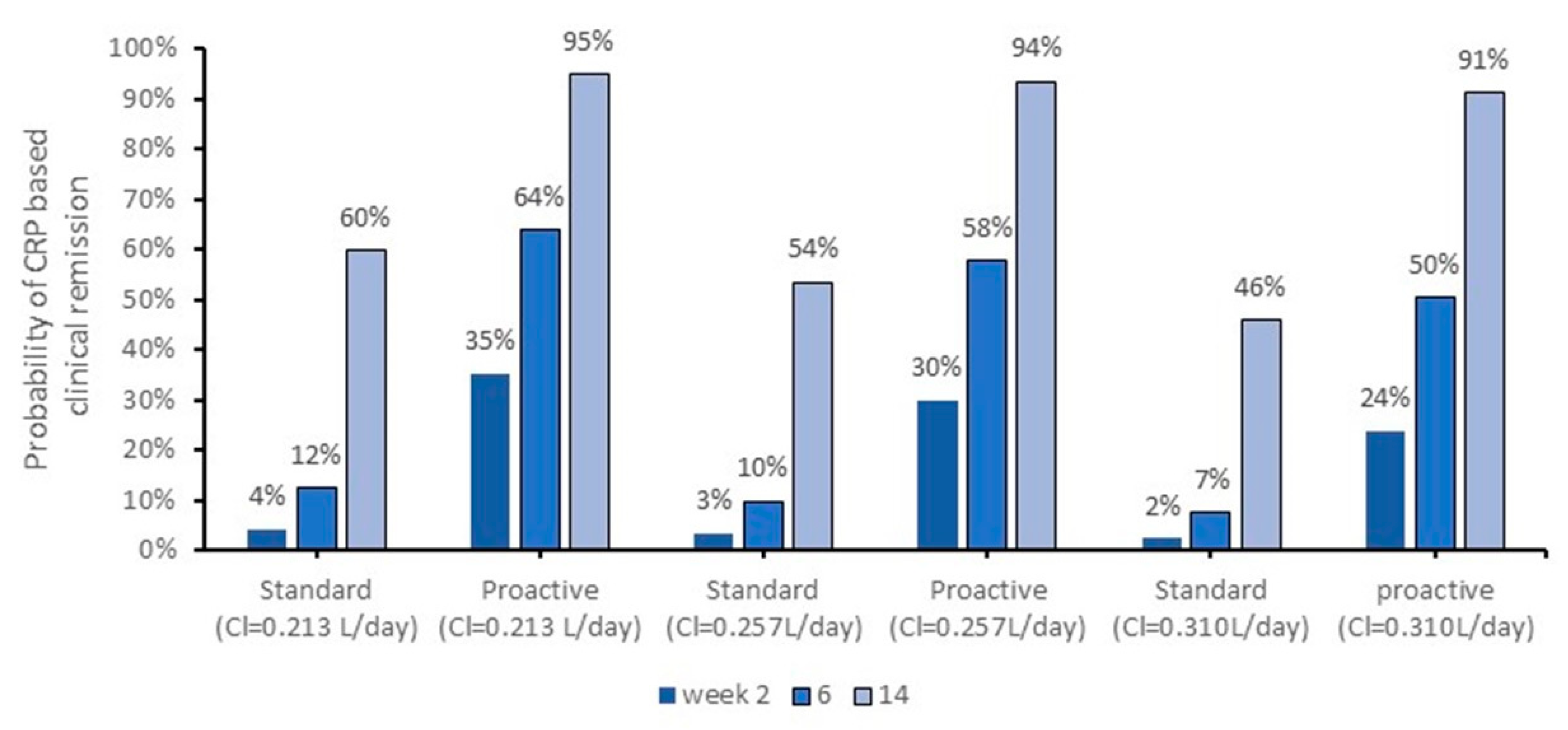
Figure 3.
PF of PK origin during maintenance therapy and CRP-based clinical remission status.
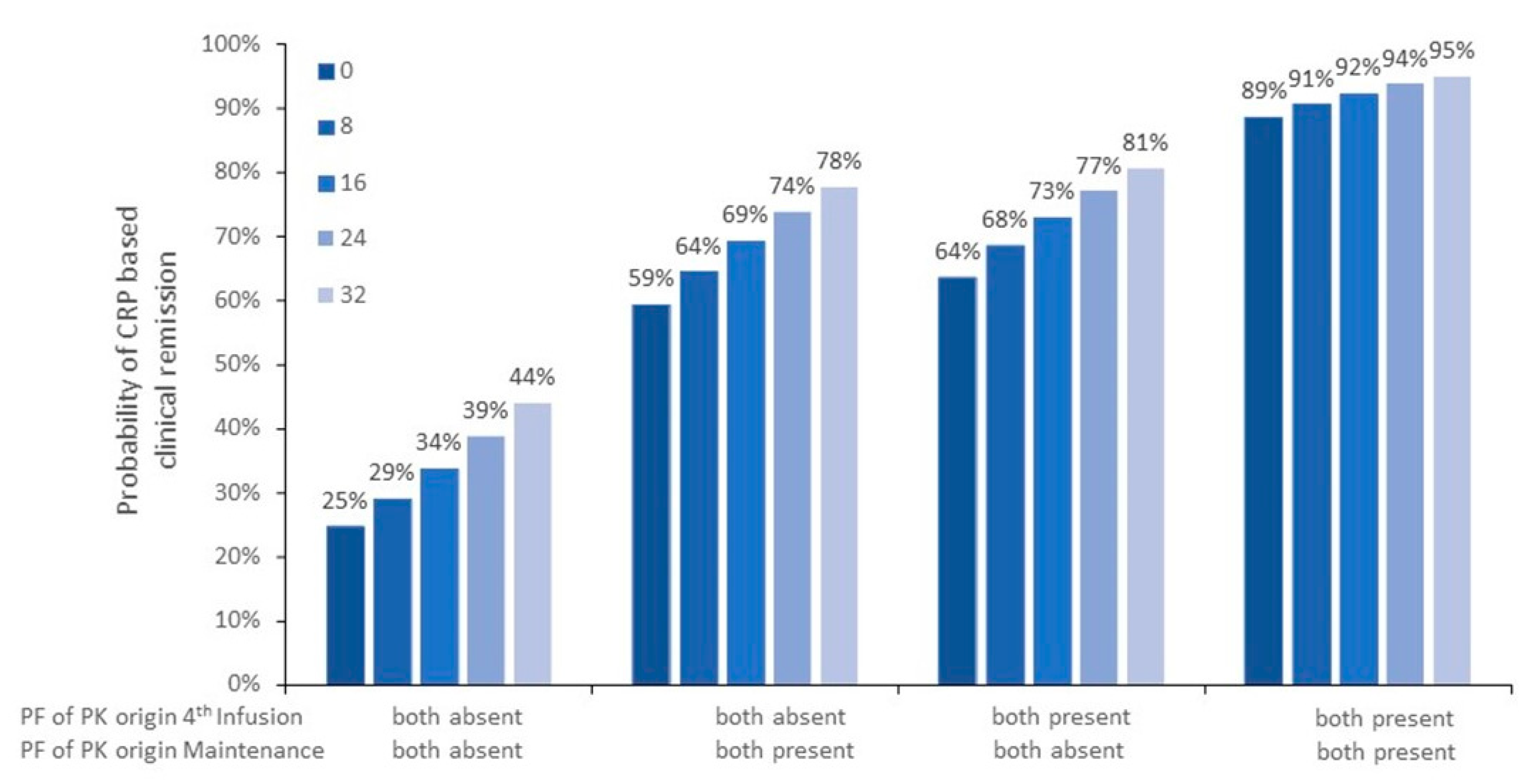

Table 1.
Patient characteristics.
| Standard Dosing | Proactive Dosing | Overall | |
|---|---|---|---|
| Pre-infusion 1 (patient number) | 37 | 108 | 145 |
| Gender (female) | 45.9% (17/37) | 44.4% (48/108) | 44.8% (65/145) |
| Age (years) | 13.0 [10.0-14.0] | 13.5 [11.2-15.2] | 13.3 [11.0-15.1] |
| Immunosuppressants | 21.6% (8/37) | 7.4% (8/108) | 11.0% (16/145) |
| Dose mg/Kg | 5.0 [5.0-5.0] | 5.0 [5.0-10.0] | 5.0 [5.0-5.2] |
| Weight Kg | 39.1 [29.5-52.9] | 41.5 [30.3-53.0] | 41.5 [29.9-52.9] |
| Clearance baseline | 0.234 [0.179-0.260] | 0.271 [0.227-0.327] | 0.258 [0.213-0.310] |
| Albumin (g/dL) | 4.0 [3.5-4.3] | 3.2 [2.8-3.7] | 3.4 [2.9-3.9] |
| CRP based clinical remission | 8.1% (3/37) | 14.8% (16/108) | 13.1% (19/145) |
| Pre-infusion 2 (patient number) | 36 | 105 | 141 |
| Time (days) | 14.0 [14.0-14.0] | 14.0 [13.1-14.2] | 14.0 [13.3-14.0] |
| Dose mg/Kg | 5.0 [5.0-5.0] | 5.1 [5.0-9.9] | 5.0 [5.0-6.0] |
| Weight Kg | 40.1 [30.7-52.9] | 41.3 [31.3-54.0] | 40.8 [31.0-54.0] |
| Albumin (g/dL) | 3.9 [3.7-4.2] | 3.6 [3.3-3.9] | 3.7 [3.4-4.0] |
| Clearance (L/day) | 0.208 [0.194-0.249] | 0.243 [0.200-0.308] | 0.234 [0.196-0.302] |
| IFX (µg/mL) | 16.2 [10.4-27.5] | 22.0 [15.4-32.1] | 20.8 [14.6-30.4] |
| ATI Status | 5.4% (2/37) | 0.0% (0/108) | 1.4% (2/145) |
| CRP-based clinical remission | 33.3% (12/36) | 70.5% (74/105) | 61.0% (86/141) |
| Pre-Infusion 3 (patient number) | 35 | 106 | 141 |
| Time (days) | 42.0 [42.0-42.0] | 38.0 [32.3-42.0] | 42.0 [34.9-42.0] |
| Dose mg/Kg | 5.0 [5.0-5.0] | 5.1 [5.0-10.0] | 5.0 [5.0-9.9] |
| Weight Kg | 41.1 [30.9-54.4] | 42.6 [32.8-54.8] | 42.4 [32.7-54.9] |
| Albumin (g/dL) | 4.1 [3.8-4.4] | 3.9 [3.7-4.1] | 3.9 [3.7-4.2] |
| Clearance (L/day) | 0.213 [0.170-0.405] | 0.212 [0.174-0.300] | 0.212 [0.174-0.324] |
| IFX (µg/mL) | 7.4 [1.3-21.3] | 15.5 [10.8-24.2] | 14.9 [7.9-23.0] |
| ATI Status | 8.3% (3/36) | 6.7% (7/105) | 7.1% (10/141) |
| CRP-based clinical remission | 40.0% (14/35) | 69.8% (74/106) | 62.4% (88/141) |
| Pre-Infusion 4 (patient number) | 32 | 104 | 136 |
| Time (days) | 98.0 [98.0-98.0] | 74.2 [63.0-90.9] | 83.4 [66.1-98.0] |
| Dose mg/Kg | 5.0 [5.0-5.0] | 10.0 [6.9-10.0] | 9.9 [5.0-10.0] |
| Weight Kg | 42.2 [32.0-54.8] | 44.9 [34.0-56.2] | 43.9 [33.5-55.9] |
| Albumin (g/dL) | 4.0 [3.7-4.2] | 4.0 [3.8-4.2] | 4.0 [3.7-4.2] |
| Clearance (L/day) | 0.215 [0.149-0.262] | 0.188 [0.155-0.269] | 0.190 [0.153-0.267] |
| IFX (µg/mL) | 4.5 [1.3-9.2] | 12.2 [7.8-17.7] | 10.4 [5.7-15.0] |
| ATI Status | 28.6% (10/35) | 0.9% (1/106) | 7.8% (11/141) |
| CRP-based clinical remission | 43.8% (14/32) | 74.0% (77/104) | 66.9% (91/136) |
| Continued | |||
| Maintenance (patient number) | 32 | 103 | 135 |
| Number of cycles | 120 | 299 | 419 |
| Dose mg/Kg | 5.0 [5.0-5.0] | 10.0 [9.9-10.0] | 9.9 [5.0-10.0] |
| Weight Kg | 43.4 (34.1-56.5) | 46.0 (34.8-59.5) | 45.5 (34.7-58.6) |
| Albumin (g/dL) | 3.9 (3.7-4.2) | 4.0 (3.9-4.2) | 4.0 (3.8-4.2) |
| Clearance (L/day) | 0.185 (0.134-0.244) | 0.200 (0.160-0.262) | 0.192 (0.154-0.253) |
| IFX (µg/mL) | 4.4 (1.1-6.8) | 12.4 (8.3-17.9) | 10.0 (5.2-15.9) |
| ATI Status | 26.7% (32/120) | 4.7% (14/299) | 11.0% (46/419) |
| CRP based clinical remission | 60% (72/120) | 76.9% (230/299) | 72.0% (302/419) |
Results are reported as median, interquartile range (IQR) or % as appropriate.
Table 2.
CRP based clinical remission status during maintenance with induction PK parameters immediately before the second, third and fourth infusion.
Table 2.
CRP based clinical remission status during maintenance with induction PK parameters immediately before the second, third and fourth infusion.
| Parameter* | Second infusion estimates |
Third infusion estimates |
Fourth infusion estimates |
|
|---|---|---|---|---|
| Time only | θpop θtime -2LL |
0.75±0.45 (p=0.096) 0.004±0.001 (p<0.001) 360.7 |
0.68±0.43 (p=0.114) 0.004±0.002 (p=0.003) 413.7 |
0.35±0.47 (p=0.456) 0.006±0.002 (p=0.003) 412.5 |
| Time and IFX concentration | θpop θconcentration θtime -2LL |
0.185±0.667 (p=0.782) 0.045±0.021 (p=0.032) 0.004±0.001 (p<0.001) 355.3 (∆= -5.4; p=0.020) |
-1.33±0.56 (p=0.0018) 0.114±0.027 (p<0.001) 0.004±0.001 (p<0.001) 389.7 (∆= -24.0; p<0.001) |
-1.02±0.56 (p=0.069) 0.136±0.032 (p<0.001) 0.005±0.001 (p<0.001) 398.3 (∆= -14.2; p<0.001) |
| Time and Clearance | θpop θCL θtime -2LL |
+2.5±0.96 (p=0.009) -7.43±2.88 (p=0.001) +0.005±0.002 (p=0.012) 354.4 (∆= -6.3; p=0.012) |
+2.77±0.80 (p=0.001) -8.35±2.31 (p<0.001) +0.004±0.002 (p=0.012) 399.7 (∆= -14.0; p<0.001) |
+3.11±0.83 (p<0.001) -11.90±2.79 (p<0.001) +0.005±0.002 (p<0.001) 391.7 (∆= -20.8; p<0.001) |
|
Time, concentration and Clearance |
θpop θconcentration θCL θtime -2LL |
-1.48±1.04 (p=0.155) +0.038±0.021 (p=0.074) -6.33±2.74 (p=0.003) +0.046±0.009 (p=0.021) 349.7 (∆= -11.0; p=0.001) |
-0.07±1.08 (p=0.94) +0.092±0.030 (p=0.002) -3.37±2.34 (p=0.015) +0.004±0.002 (p=0.012) 387.4 (∆= -26.3; p<0.001) |
+1.49±0.93 (p=0.109) +0.087±0.029 (p=0.003) -9.14±2.67 (p=0.015) +0.004±0.002 (p=0.001) 385.5 (∆= -27.0; p<0.001) |
*Model: logit(Probability of CRP Based Remission)= θpop+θcovi*covi+….
Table 3.
IFX Clearance and concentrations during induction and sustained CRP-based clinical remission during maintenance.
Table 3.
IFX Clearance and concentrations during induction and sustained CRP-based clinical remission during maintenance.
| Predictive factor, Clearance | Predictive factor, IFX concentrations | |||
|---|---|---|---|---|
| Pre-infusion # | L/day | below cutoff | µg/mL | above cutoff b |
|
Infusion 2 Not sustained Sustained p value |
0.259 [0.205-0.317] 0.221 [0.194-0.266] p=0.032 |
64.8% (35/54) 77.3% (51/66) p=0.156 |
17.0 [12.6-23.1] 26.1 [17.0-34.9] p<0.001 |
35.2% (19/54) 65.2% (43/66) p=0.002 |
|
Infusion 3 Not sustained Sustained p value |
0.241 [0.188-0.399 0.187 [0.154-0.239] p<0.001 |
66.1% (41/62) 83.8% (57/68) p=0.025 |
12.1 [5.0-18.6] 20.7 [12.7-31.1] p<0.001 |
33.9% (21/62) 67.6% (46/68) p<0.001 |
|
Infusion 4 Not sustained Sustained p value |
0.247 [0.167-0.313] 0.175 [0.132-0.214] p<0.001 |
62.5% (41/62) 97.1% (57/68) p<0.001 |
7.8 [2.2-11.9] 13.0 [8.7-18.8] p<0.001 |
37.5% (24/64) 66.2% (45/68) p<0.001 |
a<0.294 L/day; bInfusion 2: >20µg/mL; Infusion 3: >15µg/mL; Infusion 4: >10µg/mL.
Table 4.
CRP-based clinical remission status during maintenance with maintenance PK.
| Parameter* | estimates | |
|---|---|---|
|
Time only (days) |
θpop θtime -2LL |
+0.65±0.46 (p=0.158) +0.0047±0.0014 (p<0.001) 424.8 |
|
Time and Concentrations (µg/mL) |
θpop θtime θconcentration -2LL |
-0.84±0.63 (p=0.312) +0.0055±0.0018 (p<0.001) +0.120±0.027 (p<0.001) 400.0 (∆= -24.8; p<0.001) |
|
Time and Clearance (L/day) |
θpop θtime θCL -2LL |
+4.05±0.57 (p<0.001) +0.0055±0.0017 (p<0.001) -16.71±2.28 (p<0.001) 380.8 (∆= -44.0; p<0.001) |
| Time PF of PK: concentration(µg/mL) and Clearance (L/day) | θpop θtime θconcentration θCL -2LL |
+1.98±0.56 (p<0.001) +0.0058±0.0016 (p<0.001) +0.093±0.025 (p<0.001) -12.84±2.27 (p<0.001) 371.0 (∆= -53.8; p<0.001) |
*Model: logit(Probability of CRP based remission)= θpop+θcovi*covi+….
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



