
Submitted:
29 August 2023
Posted:
31 August 2023
You are already at the latest version
Abstract
Diabetic kidney disease (DKD) is one of the leading causes of end-stage renal disease worldwide and significantly increases the risk of premature death due to cardiovascular diseases. Elevated urinary albumin levels are an important clinical feature of DKD. Effective control of albuminuria not only delays glomerular filtration rate (GFR) decline but also markedly reduces cardiovascular disease risk and all-cause mortality. New drugs for treating DKD proteinuria, including sodium-glucose cotransporter 2 inhibitors (SGLT2i), mineralocorticoid receptor antagonists (MRAs), and endothelin receptor antagonists (REAs), have shown significant efficacy. Auxiliary treatment with proprietary Chinese medicine has also yielded promising results; however, it also faces a broader scope for development. The mechanisms by which these drugs treat albuminuria in patients with DKD should be described more thoroughly. The positive effects of combination therapy with two or more drugs in reducing albuminuria and protecting the kidneys warrant further investigation. Therefore, this review explores the pathophysiological mechanism of albuminuria in patients with DKD, the value of clinical diagnosis and prognosis, new progress and mechanisms of treatment, and multidrug therapy in patients who have type 2 diabetic kidney disease (T2DKD), providing a new perspective on the clinical diagnosis and treatment of DKD.
Keywords:
diabetic kidney disease
; proteinuria
; pathophysiological mechanism
; drug therapy
1. Introduction
Diabetic kidney disease (DKD) is one of the leading chronic microvascular complications in patients who have diabetes. The clinical manifestations include persistently increased urinary albumin levels and/or GFR progressively declining. DKD is the leading cause of end-stage kidney disease worldwide, and 30%–50% of end-stage renal disease (ESRD) cases globally are caused by DKD [1]; approximately 50% of patients with DKD in the United States undergo dialysis or kidney transplantation [2]. DKD also significantly increases the risk of cardiovascular disease in patients with diabetes and is an important risk factor for premature death [3].
Proteinuria in patients with DKD is primarily albuminuria, which has long been considered an important clinical feature of DKD. Notably, new therapeutic drugs for albuminuria in DKD are being developed and are widely used. Normoalbuminuric diabetic kidney disease (NADKD) is also gradually being recognized, and the timing of albuminuria control in patients with DKD has become more challenging; therefore, albuminuria in patients with DKD should be re-examined. This paper summarizes the pathophysiological mechanism of albuminuria in patients with DKD, the value of clinical diagnosis and prognosis, new progress and mechanisms of treatment, and multidrug therapy in patients with T2DKD, providing a new perspective on the clinical diagnosis and treatment of DKD.
2. Pathophysiological mechanism of albuminuria in DKD
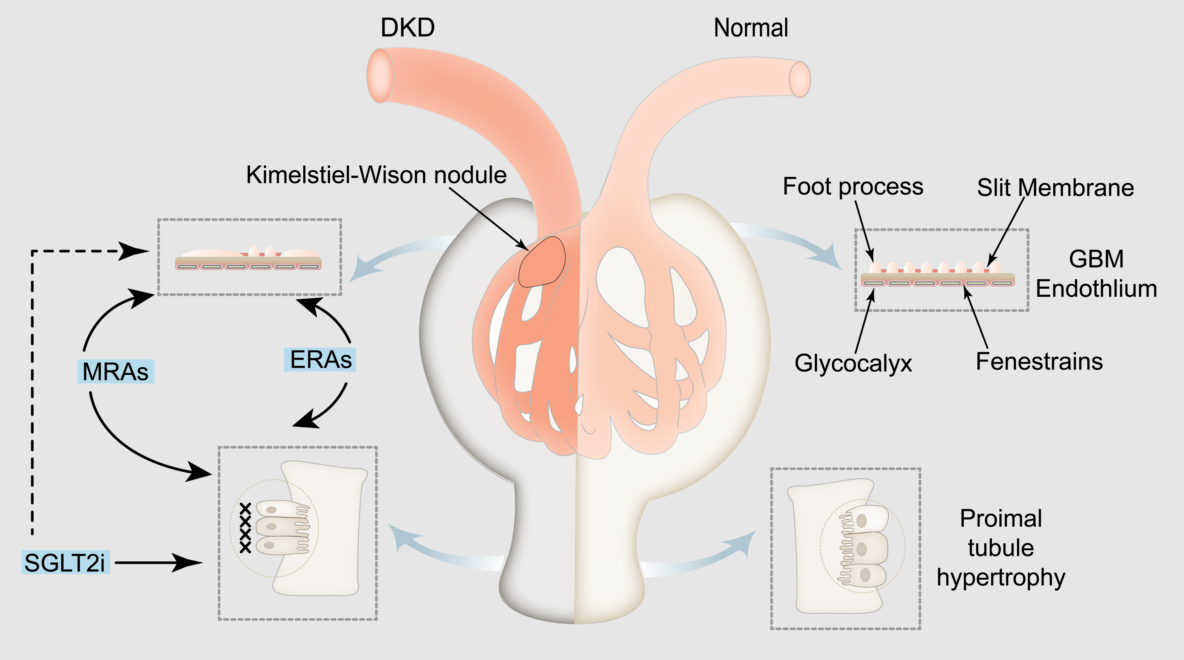
Albuminuria is a prominent feature of DKD, which not only reflects damage to the glomerular filtration barrier but is also affected by glomerular hyperfiltration and renal tubular reabsorption. On the glomerular scale, hyperfiltration, endothelial dysfunction, basement membrane thickening, podocyte foot process fusion or detachment, glomerulosclerosis, and arteriolar hyalinization may lead to proteinuria [4]. Recent studies have demonstrated that both podocyte DNA double-strand breaks and glomerular DNA methylation are associated with the severity of albuminuria [5].
In the renal tubules, cubilin/megalin downregulation, tubular inflammation, atrophy, and reduced reabsorption of amino acids and proteins by the proximal tubules play a role in the development of DKD caused by proteinuria [4,6]. The mechanism underlying renal tubular proteinuria is primarily related to damage to the structure and function of the proximal tubules. Renal tubular epithelial cells (PCT) are located in chronic high-glucose or hypoxia-ischemic environments and exhibit abnormal metabolism and hemodynamics. Additionally, they express advanced glycation end-products (AGEs), reactive oxygen species, and other metabolites. Through a series of kinase cascades, they lead to extracellular matrix accumulation or macrophage infiltration to induce inflammation, eventually resulting in renal tubulointerstitial fibrosis and tubular injury, affecting renal tubular reabsorption function. This leads to renal tubular proteinuria development.
Ion channels and transporters play important roles in the pathogenesis of proteinuria [7]. Regarding ion channels, blocking the epithelial Na+ ion channels located in the epithelial cells of the distal convoluting tubules and collecting ducts can prevent Na+ reabsorption and decrease Na+ retention, thereby reducing proteinuria [8,9]. Blocking the P/Q-, N-, T-, and L-type voltage-gated Ca+ channels located in the arterioles of glomeruli can significantly restore the expression of podocyte-related proteins such as nephrin and podocin, protect podocytes, and reduce glomerular proteinuria [10]. Moreover, TRPC5 [11] and TRPC6 [12] ion channels located in podocytes protect the podocyte cytoskeletal hub structure, actin cytoskeleton, and glomerular proteinuria. Blocking Ca+ -activated K+ channels located in glomeruli and some renal tubules, as well as inhibiting Inflammatory factor-related signaling pathways such as growth factor-beta 1 (TGF-β1) signaling pathway and the expression of inflammatory markers, can reduce glomerular proteinuria and renal tubular proteins [13]. The activation of TRPV4 in proximal tubular epithelial cells can stimulate albumin endocytosis of tubular epithelial cells and reduce tubular proteinuria [14]. This activation also protects the expression of ClC-5, protects the proximal tubule from protein reabsorption, and reduces renal tubular proteinuria [15]. Furthermore, TRPV4 activation stimulates ATP-sensitive K+ channels located in the mitochondrial membrane of podocytes, inhibits the production of reactive oxygen species and podocyte injury, and reduces glomerular proteinuria [16]. Regarding ion transporters, the upregulation of Na+/K+/2Cl-cotransporters in the brush border membrane of the proximal tubule alleviates proteinuria [17]. The deeper the pathophysiological mechanism of DKD, the more precise the treatment for DKD.
Overall, this study summarizes the pathophysiological mechanisms underlying albuminuria in patients with DKD (Figure 1).
3. Role of albuminuria in the diagnosis and prognosis of DKD
According to the degree of proteinuria in patients with DKD, they are categorized into microalbuminuria (urinary albumin-to-creatinine ratio (UACR) 30–299 mg/g) and macroalbuminuria (UACR ≥300 mg/g). Microalbuminuria is used to indicate the possibility of chronic kidney disease (CKD) in patients [18]. Proteinuria is an important risk factor for renal prognosis and is not the only diagnostic criterion for DKD. An artificial intelligence system for detecting urinary microalbuminuria is expected to monitor the progression of diabetic nephropathy (DN) based on laboratory examinations [19]. Studies have confirmed that in patients with diabetes with any level of eGFR, the presence of proteinuria is associated with the risk of cardiovascular disease, CKD progression, and death [20,21]. Therefore, for patients with diabetes with macroalbuminuria, the treatment goal is to reduce urinary albumin by ≥30% to delay CKD progression. For patients with diabetes with microalbuminuria, the risk of progressin to macroalbuminuria should be reduced [22].
According to the concept of proteinuria defined by the National Kidney Foundation and the US Food and Drug Administration in 2009 [23], NADKD (UACR <30 mg/g) should be further refined to UACR <10 mg/g and UACR 10–29 mg/g groups. A UACR of <10 mg/g is the normal urine albumin content, and a UACR in the range of 10–29 mg/g exceeds the normal value [24]. However, a better understanding of NADKD may facilitate its early diagnosis.
4. Timing of control of albuminuria in patients with DKD
Some studies have found that some patients already have ESRD without proteinuria [25], and the specific underlying mechanism remains unclear, which may be related to hypertension, unrecovered acute kidney injury , and renal vascular disease. Data from an autopsy study of 105 community patients with normoalbuminuric diabetes in Japan, published in 2021, showed that advanced DN diagnosed using pathological analysis accounted for approximately 50% of cases. This suggests that the absence of detectable albuminuria does not rule out the presence of DKD. A Spanish autopsy study in 2022 with a small sample of 21 patients reached similar conclusions [26]. The time at which DKD develops in patients with type 2 diabetes remains unknown; however, these findings may lead to a breakthrough in future clinical practice regarding whether early treatment with renin-angiotensin-aldosterone system inhibitors (RAASI) or SGLT2i should be initiated before microalbuminuria develops in patients with diabetes. Future noninvasive diagnostic techniques may help identify patients with cryptic DKD who may benefit from early treatment [27,28]. Therefore, more randomized controlled trials (RCTs) and real-world studies are needed to help clinicians determine the appropriate time to control albuminuria in patients who suffer DKD.
5. Treatment progress and mechanism of albuminuria in patients with DKD
The RENAAL study, a previous large RCT, confirmed the renoprotective effect of reducing proteinuria in patients with type 2 diabetes [29]. Patients receiving losartan showed a 26% decrease in proteinuria within 3 months, a further decrease of more than 40% within 3 years, and a significant improvement in renal survival. The other RAASI were equally effective in reducing the progression of proteinuria and renal insufficiency. As the first landmark drug for DKD treatment, it has been used in clinical practice for more than 20 years. Both the 2023 American Diabetes Association (ADA) guidelines [30] and the 2022 Kidney Disease: Improving Global Outcome (KDIGO) guidelines [31] recommend the use of RAASI in treating microalbuminuria and macroalbuminuria in patients with DKD; however, insufficient evidence still exists to support the use of RAASI for the primary prevention of DKD in patients with diabetes with normal blood pressure and urinary protein.
5.1. SGLT2 i
Recently, the introduction of SGLT2i has revolutionized the clinical management of type 2 diabetes, not only effectively improving the cardiovascular outcomes of patients [32] but also having a renoprotective effect in patients with and without diabetes with moderate and severe renal insufficiency, significantly reducing proteinuria and becoming the second landmark drug for treating DKD [33,34,35,36,37,38]. Therefore, SGLT2i is recommended to delay CKD progression and reduce the risk of cardiovascular events in patients with CKD with type 2 diabetes and large albuminuria in recent guidelines. Compared with SGLT2i drugs, DPP4 inhibitors and GLP1 agonists have been shown to reduce proteinuria but have not been demonstrated to alleviate the deterioration of renal function [39,40]. Encouraging results were expected from the FLOW trial [41] using semaglutide.
The primary mechanism of SGLT2i in treating albuminuria in patients with DKD is to improve hemodynamics [33,42]. Since the mechanism of action of SGLT2i is independent of insulin, it is still functional in patients with T1DKD [43,44,45]. SGLT2i, which is located in the distal convoluted tubules in the macula densa and feels the higher concentration of sodium ions and signal transmission to the juxtaglomerular cell, plays a role in the adjustment of the “feedback” by blocking SGLT2 to sodium and reabsorption of glucose in PCT [46]. SGLT2i induces the production of adenosine, activates the adenosine A1 receptor, increases cytosolic Ca+, and restores glomerulotubular balance, thereby achieving the contraction of afferent arterioles [47]. In patients with type 2 diabetes receiving RAS blockers, SGLT2i causes dilation of the efferent arterioles upon RAS blockade by increasing adenosine and prostaglandin production [47]. SGLT2i has a renoprotective effect in reducing albuminuria by constricting and dilating afferent and efferent arterioles, respectively, during RAS blockade, lowering intraglomerular pressure and improving glomerular hyperfiltration. Because SGLT2 co-localizes with sodium-hydrogen exchanger 3 (NHE3) in PCT, SGLT2i blocks NHE3, which makes the natriuretic effect more significant [48]. In clinical and animal experiments, SGLT2i has been shown to increase podocyte autophagy, lower podocyte lipid content, protect podocytes, and reduce proteinuria [2,49,50]. Recent studies have demonstrated that dapagliflozin can delay renal tubulointerstitial fibrosis by inhibiting YAP/TAZ activation [51], and block CYP4A/20-HETE signaling to reduce reactive oxygen species and inflammation, thereby decreasing glomerulosclerosis and renal tubulointerstitial fibrosis [52]. SGLT2i provides novel perspectives for treating glomerular and tubular proteinuria.
5.2. MRAs
Finerenone, which is a nonsteroidal mineralocorticoid antagonist, is the only nonsteroidal MRA clinically proven to have renal and cardiovascular benefits [53]. It can rapidly reduce proteinuria and provide long-term renal protection in patients with diabetes treated with RAASI [54,55]. Additionally, the 2020 KDIGO guidelines [56] recommend a combination of ACEI/ARB and MRAs to reduce urinary protein levels in patients with T2DKD. The use of MRAs in treating patients with diabetes with CKD was further improved according to the 2022 KDIGO [31] and 2023 ADA guidelines [30].
The renal protective mechanism of finerenone in patients with DKD is mainly due to its anti-inflammatory and anti-fibrosis effects [57,58], and it may also achieve anti-albuminuria by improving hemodynamics [58]. In patients with DKD, aldosterone activity is increased in the kidney, and MRs are overactivated, leading to the overexpression of MR-mediated proinflammatory and pro-fibrotic genes in various somatic cells in the kidney, including distal tubular epithelial cells, macula densa, endothelial cells, mesangial cells, podocytes, macrophages, fibroblasts, and other cells, driving renal inflammation and fibrosis [59,60,61,62]. MR over-activation leads to a series of renal pathological changes, including glomerular basement membrane thickening, podocyte injury, mesangial cell proliferation and apoptosis, mesangial expansion, macrophage infiltration, collagen deposition, glomerulosclerosis, renal tubular epithelial cell atrophy and renal interstitial fibrosis, renal tubular inflammation, endothelial dysfunction, and arteriosclerosis [60,63,64]. These histopathological changes are important mechanisms that lead to albuminuria in patients with DKD. In the cytoplasm, finerenone binds to MR instead of aldosterone, resulting in a conformational change of MR. The MR-finerenone is translocated to the nucleus and binds to the hormone response element, where it cannot transcribe target genes due to the lack of transcription cofactors, leading to the down-regulation of proinflammatory and pro-fibrotic genes, such as NF-κB and AP-1, and ultimately reducing renal inflammation and fibrosis [63,65]. Furthermore, it alleviates the pathological changes in glomerular and renal tubular damage and improves albuminuria. Regarding hemodynamics, finerenone may improve glomerular hyperfiltration by preventing aldosterone-mediated contraction of efferent arterioles over afferent arterioles, reducing intraglomerular pressure, and achieving anti-albuminuria [58]. However, a multicenter, multiracial RCT involving 823 patients with type 2 diabetes and albuminuria treated with RAS blockade showed no significant association between dose-dependent reductions in UACR with finerenone and reductions in blood pressure or eGFR [66], which may indicate that the mechanism by which finerenone reduces albuminuria is hemokinesis-independent [67].
5.3. ERAs
Low-dose, short-term treatment with the selective endothelin A (ETA) receptor antagonist atrasentan has a positive therapeutic effect in reducing albuminuria and improving renal prognosis in some patients with T2DKD without causing significant sodium retention [68,69,70], and its clinical application still has broad development prospects. However, the results of the SONAR study showed that the use of atrasentan did not provide cardiovascular protection [71]; therefore, it is necessary to be alert to the occurrence of cardiovascular adverse events during its clinical application. Additionally, the SONAR trial was conducted to ensure safety and introduce strict inclusion and exclusion criteria, excluding patients who were unresponsive to atrasentan (proteinuria reduction ≤30%) or intolerant (history of heart failure or peripheral edema). Therefore, it generalizing these results for clinical applications is difficult. Furthermore, unresolved scientific questions remain, such as whether patients with T2DKD who do not respond to atrasentan benefit from SGLT2i-, finerenone-, or insulin-based therapies [33]. However, whether early albuminuria reduction with atrasentan treatment can predict long-term renoprotective effects remains unknown [72]. Therefore, the clinical value of selective ETA receptor antagonists in patients with T2DKD still needs substantial medical-based evidence.
The expression of endothelin-1 (ET-1) is increased in the kidney of patients with DKD [73,74,75]. ET-1 binds to the ETA receptor to produce pathological effects through various stimulation of kidney histopathological changes, such as damage to the endothelial cell glycocalyx and actin cytoskeleton of podocytes, causing dysfunction of the podocyte membrane, changing the basement membrane, causing mesangial matrix deposition, damaging renal blood vessels, enhancing vascular reactivity and coagulation, leading to renal tubulointerstitial fibrosis, and promoting inflammatory cell infiltration [69,75,76]. ERA antagonists increase endothelial glycocalyx, reduce glomerular heparanase, protect podocyte actin cytoskeleton and slit diaphragm function, and reduce inflammation, interstitial fibrosis, and extracellular matrix hyperplasia through various mechanisms [77,78]. Animal experiments have shown that blocking ETA can reverse the glomerular hyperosmolar state and reduce glomerular albuminuria caused by glomerular injury [79]. Therefore, ETA antagonists can be used to treat glomerular albuminuria by protecting the glomerular filtration barrier and reversing glomerular hyperfiltration. Additionally, they protect renal tubular epithelial cells, reduce renal tubulointerstitial fibrosis, and treat renal tubular proteinuria.
5.4. Chinese patent medicine
5.4.1. Keluoxin capsule
Keluoxin capsules are composed of Astragali radix, Pseudostellariae radix, Ligustri lucidi fructus, Lycii fructus, Rhei radix et rhizome, and Hirudo. It was the first Chinese patented medicine approved for the treatment of DKD. It can maintain kidney function, reduce the level of urinary protein, delay DKD development, and alleviate related symptoms [80,81,82]. Keluoxin capsules have been recommended to control proteinuria in patients with DKD according to several guidelines, such as the Guidelines for Diagnosis and Management of Diabetic Kidney Disease with Integrated Traditional Chinese and Western Medicine [83] and the Guidelines for the Prevention and Treatment of Type 2 Diabetes Mellitus in China [84]. A double-blind RCT suggested that keluoxin capsules can prominently reduce the ACR level in patients with early DKD and the ratio of those with deteriorated proteinuria, whose ACR levels continue to rise by 30% [85]. According to the study, Keluoxin capsules can also alleviate clinical symptoms, such as fatigue, dry mouth and throat, limb numbness, and pain, aggravated at night, to improve the life quality of patients. The latest meta-analysis, involving 20 studies and 1500 participants, has suggested that a combination of Keluoxin capsules and Western medicine presents better efficiency than a single use of Western medicine in treating DKD, including improving eGFR and reducing the level of microalbuminuria, urinary albumin excretion rate (UAER), 24-hour urine protein, serum creatinine (Scr), blood urea nitrogen, fasting blood glucose, total cholesterol, triglyceride (TG), and low-density lipoprotein [86]. Regarding safety, no statistically significant differences were found in adverse drug events between the two groups. Pharmacoeconomic research has shown that the combined use of keluoxin capsules and chemical medicine is more economical than chemical medicine alone, considering its current price level [87].
Traditional Chinese medicine involves multiple targets and pathways and can regulate the overall situation of disease treatment. Clinical studies and animal trials have suggested that keluoxin capsules can delay or treat DKD by improving glycolipid metabolism and microcirculation, enhancing histiocyte function, and alleviating renal damage [88]. Keluoxin capsules can improve glycolipid metabolism, regulate tubuloglomerular feedback to reduce kidney tubule injury and renal hypertrophy, and alleviate kidney hyperfiltration [89]. Additionally, Keluoxin capsules lower endothelin, thromboxane B2, atrial natriuretic peptide, and angiotensin [90]. Meanwhile, they can also enhance the level of 6-keto-prostaglandin1α, regulate the dynamic balance of the renin-prostacyclin system, and improve hemodynamics and hemorheology and renal microcirculation [90]. Simultaneously, Keluoxin capsules can decrease the level of oxidative stress and inflammatory cytokines, probably because they can regulate the JAK/STAT, MAPK, and NF-κB signaling pathways [91,92,93,94]. Moreover, Keluoxin capsules can regulate podocyte autophagy, alleviate renal damage, and protect the kidney [95]. Research on the mechanism of action of keluoxin capsules is ongoing. We expect that the mechanism of action will be interpreted more comprehensively.
5.4.2. Huangkui capsule
Evidence from the real world shows that Huangkui capsules are widely used to treat proteinuria in patients with DKD, with sufficient evidence of clinical efficacy and high frequency of use [96,97]. For example, a multicenter RCT study involving 413 patients with DKD demonstrated that after 24 weeks of treatment, Huangkui capsules combined with irbesartan had significantly greater reductions in UACR, 24-hour proteinuria, and UPCR (urinary protein creatinine ratio) than irbesartan alone (P<0.001, P=0.001, and P=0.001, respectively); the overall incidence of adverse events was low and largely similar between treatment groups, with no serious adverse events of reduced liver or renal function [98]. A recent meta-analysis of 13 RCTs has shown that Huangkui capsules can effectively reduce 24-hour urinary protein content in patients with CKD. The effectiveness of Huangkui capsules in DKD subgroups should be further clarified; therefore, larger sample sizes and high-quality RCTs in multiple countries are needed to confirm this [99].
A recent animal study has demonstrated that the Huangkui capsule can protect podocytes from doxorubicin (DOX)-induced proteinuria by inhibiting the JAK2/STAT3 and PI3K/Akt pathways and increasing the expression of Nephrin and Podocin in DOX-exposed podocytes [100]. Thus, proteinuria was alleviated. Another animal experiment confirmed the advantages of the Huangkui capsule in treating DN from a different perspective, such as regulating the intestinal microbiota and improving metabolite levels in DN [101]. In terms of reducing renal interstitial fibrosis, animal experiments have demonstrated that Huangkui capsule combined with metformin can effectively improve DN by inhibiting the expression of renal fibrosis-related proteins and blocking Klotho/TGF-β1/p38MAPK signaling pathway in DN rats [102]. Huangkui capsule inhibited NLRP3 inflammasome activation and TLR4/NF-κB signaling pathway and alleviated epithelial to mesenchymal transition of renal tubules [103].
5.4.3. Tripterygium glycosides
In China, T. wilfordii, combined with Western medicine, is widely used in patients with DKD. Many clinical RCTs have shown that T. wilfordii combined with Western medicine can effectively reduce 24-hour urinary protein levels and UAERs [104,105,106]. However, its clinical application is limited due to the presence of minor side effects that mainly focus on abnormal liver function [106]. Therefore, to explore its clinical safety, a meta-analysis involving 31 RCTs suggested that the duration of TG-mediated DN treatment should be less than 3 consecutive months [107]. Therefore, because of the generally low-quality evidence provided by systematic reviews and meta-analyses of Tripterygium for the adjuvant treatment of clinical DKD, it still needs to be treated cautiously [108]. Serious side effects should be carefully monitored, even in courses that are generally considered safe. Large-scale and long-term multicenter studies of T. wilfordii combined with Western medicine are expected. However, the mechanism of action of T. wilfordii in treating DN has not been fully elucidated. Untargeted metabolomic analysis using ultra-high performance liquid chromatography-quadrupole time-of-flight mass spectrometry revealed that Tripterygium improved impaired renal function mainly by promoting TG catabolism in DN mice [109].
5.4.4. Other Chinese patent medicine
Niaoduqing granules can be used to effectively treat proteinuria in patients with DKD. Through network pharmacology, it has been found that the mechanism of Niaoduqing granules in treating DN proteinuria is to inhibit the activity of the AGE/RAGE pathway and the overexpression of VEGF-A, ICAM-2, PTGS-5, and ACE in MPC1 cells to prevent podocyte injury in DN [110]. However, evidence of adverse drug reactions remains unclear [111]. An ESRD rat model confirmed that Niaoduqing granules improved renal fibrosis and urinary protein excretion by regulating the p38 MAPK/NF-κB signaling pathway [112].
Yishen Huashi granules are widely used to treat proteinuria in patients with DKD, and their therapeutic mechanism is related to the improvement in podocyte injury induced by macrophage-derived exosomes [113]. Recent animal experiments have shown that Yishenhuashi granules can improve the pathological mechanism of DKD by regulating the “gut-kidney axis” of intestinal flora and serum metabolites and improving the mRNA expression of the kidney [114].
Cordyceps sinensis preparations have been used in the adjuvant treatment of clinical DKD, and their combination with conventional treatment is better than conventional treatment alone in terms of protecting renal function and reducing the clinical efficacy of proteinuria, which has been clinically confirmed [115,116,117]. A meta-analysis of 38 RCT studies involving 3167 patients with DKD showed that Cordyceps sinensis preparations combined with ACEI/ARB significantly reduced 24-hour urinary protein compared with the ACEI/ARB alone group [standardized mean difference (SMD) = -1.99, 95% confidence interval [CI] (-2.68, P<0.05; -1.31, P<0.01], urinary microalbumin [mean difference (MD) = -37.41, 95% CI (-44.76, -30.06), P<0.01], UAER [MD= -24.11, 95% CI (-30.54, P<0.01), -17.68), P<0.01], and ACR [SMD =1.01, 95% CI (-1.73, -0.29), P<0.01], and no significant difference was found in adverse events between the two groups [118]. Cordyceps sinensis preparation can reduce renal TG accumulation in DN rats by regulating the PPARα pathway, thereby reducing glomerulosclerosis, renal tubulointerstitial injury, and renal fibrosis, as well as glomerular proteinuria and renal tubular proteinuria [119]. Based on the comprehensive metabolomics and pattern recognition technology of ultra-performance liquid chromatography-mass spectrometry, it was found that Cordyceps sinensis preparations may play a role in treating DN by searching abnormal metabolic pathways [120]. From the perspective of the Chinese healthcare system, Cordyceps sinensis preparations may be a cost-effective treatment option for DN in the Chinese population [121].
Therefore, Shenshuaining [122], Fufang Xueshuantong [123], Shenyan Kangfu tablets [124,125], and Liuwei Dihuang decoction [126], which are also combined with Western medicine for the treatment of DKD and effective reduction of proteinuria, should be further confirmed by real-world research and more high-quality, large-scale, and multicenter RCT studies. Chinese patent medicine has broad development potential and an upward space for treating DKD proteinuria [127,128,129].
Overall, this review summarizes the pharmacological mechanisms underlying albuminuria in patients with DKD (Table 1).
5.5. Targeted precision therapy
Although these drugs have shown encouraging efficacy in treating DKD proteinuria, some patients continue to experience uremia. Increasing evidence has shown that targeted drug delivery strategies, such as macromolecular carriers, nanoparticles, and liposomes, can improve drug efficacy and reduce adverse side effects, which may become a new milestone in treating DKD [130]. HDAC4 is involved in podocyte injury in DKD, and HDAC4 siRNA shows good therapeutic prospects for DKD. DTsiANp/HDAC4 can deliver HDAC4 siRNA to the podocytes of DKD rats, and a 4-week intervention can significantly reduce UAER and glomerulosclerosis [131]. Targeted renal delivery of gold nanoparticles with a diameter of 50 nm can reduce UAER, glomerular basement membrane thickness, and foot process width in DKD rats [132]. As an antioxidant, Coenzyme Q10 may be a promising treatment option for early-stage DKD. However, its low water solubility and nonspecific distribution limit its clinical application. Therefore, liposomes containing CoQ10 combined with ultrasound microbubbles were injected into DKD rats to target the kidneys and improve proteinuria and oxidative stress markers [133]. The above studies are still in the preclinical stage; however, as the research on the pathogenesis of DKD advances, targeted precision therapy will be explored for clinical applications.
6. Polydrug therapy for proteinuria in patients with T2DKD
A long history of care has discouraged the use of polypharmacy (more than five different drugs) in patients with diabetes because of the risk of adverse drug–drug interactions [134]. However, patients with diabetes mellitus frequently experience various complications and comorbidities. Multidrug treatment for lowering blood glucose, blood pressure, and lipids has been widely accepted because its efficacy has been confirmed, and the doses used are lower than a single drug dose, with fewer side effects.
Many clinical studies have shown that controlling proteinuria in patients with DKD can delay the progression of cardiovascular disease and CKD and reduce the risk of death. ACEI or ARB are recommended as the first treatment choice for patients with T2DKD, regardless of whether they are complicated with microalbuminuria or macroalbuminuria [53,135]. However, a combination of ACEI and ARB is not recommended, and ACEI/ARB is not recommended for the primary prevention of DKD in patients with diabetes with normal blood pressure and proteinuria [136]. Conversely, the Scr level at which RAS should be contraindicated remains controversial [137]. Non-dihydropyridine calcium channel blockers, such as verapamil, can stabilize or even reduce the level of urinary protein [138] and can be used as the first combination of ACEI/ARB drugs when blood pressure is not well controlled [139]. If a beta-blocker is combined, a vasodilator beta-blocker, including Carvedilol or Nebivolol, may be preferred because non-vasodilator beta-blockers accelerate albuminuria progression [140,141].
In patients with DKD, SGLT2i or mineralocorticoid-receptor antagonists can be added when the target urinary albumin levels are not achieved with RAS blockade [140]. SGLT2i can effectively reduce urinary protein levels in both micro-and macroalbuminuria [142]. Finerenone combined with an ACRI/ARB is effective in reducing urinary protein levels in patients with T2DKD [66], and no clear evidence of an increased risk of hyperkalemia or AKI exists. The FIDELIO-DKD and CREDENCE trials showed similar cardiorenal benefits [143]. Therefore, triple oral therapy with a RAS blocker, an SGLT2i, and an MRA should be considered if the urinary albumin level remains high. To date, no conclusive evidence exists that triple therapy is effective in treating DKD; however, a retrospective report from a prospective study showed that the addition of finerenone can further reduce proteinuria and delay the decline in renal function in patients with DKD who have already received RAS inhibitors, and a small number of individuals in this group also received SGLT2i [144]. Patients with advanced DKD should consider the risk of undertreatment. Therefore, whether triple therapy can be used in patients with diabetes with micro-and macroalbuminuria in the future requires further high-quality, medical-based evidence.
In clinical practice, there has been no experience with the combination of these drugs and ERAs. Theoretically, SGLT2i can reduce sodium and water retention in ERAs by constricting afferent arterioles. ERA dilates efferent arterioles and synergistically reduces glomerular hyperfiltration while complementing SGLT2i. However, an experiment in male db/db mice without kidney resection showed no significant differences in urinary albumin excretion, and histopathological changes were observed in the SGLT2i and ET-A antagonist groups compared with the SGLT2 inhibitor group alone [145].
7. Conclusion and prospect
DKD is a heterogeneous disease characterized by multiple factors and complex phenotypes. Pathophysiological differences among patients can lead to individual differences in drug responses. Therefore, large-scale prospective trials based on individual drug responses and phenotypic characteristics are required to guide precise treatments. Optimal combinations of new therapies can further delay DKD progression. Real-world studies can clarify which combination is beneficial for cardiac and renal outcomes in patients with T2DKD while being well tolerated, safe, easy to manage, and cost-effective. Simultaneously, to better understand the mechanism of DKD, particularly T2DKD, basic research should be intensified, especially based on the metabolic pathways and metabolites of renal cells in chronic high-glucose environments, and focus on the metabolic and hemodynamic pathways in the DKD environment. Furthermore, targeting the AGE-AGE receptor axis involves focusing on new targets for renoprotective intervention, such as AGE inhibitors pyridoxamine and glyoxalase-1, an enzyme that degrades the AGE precursor methylglyoxaldehyde [146]. Therefore, attention should be paid to the kinase cascade initiated by metabolite reactive oxygen species and the transcription factors involved in the reaction. Finally, the targeted drug delivery strategy for DKD is still in its early stages, and there are limitations regarding safety, stability, and clinical efficacy. The selection of the best kidney-targeting strategy is expected to provide a new treatment approach for DKD.
Author Contributions
Conceptualization, Zheyi Dong and Xiangmei Chen; methodology, Zheyi Dong; writing—original draft preparation, Ruimin Zhang and Qian Wang; writing—review and editing, Ruimin Zhang, Qian Wang, Xuefeng Zhou, Qihu Li, Zheyi Dong and Xiangmei Chen; visualization, Ruimin Zhang and Qihu Li; supervision, Qian Wang; funding acquisition, Xiangmei Chen, Zheyi Dong and Qian Wang. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by National Natural Science Foundation of China (No. 62250001 and 81700629), Beijing Natural Science Foundation (No. L222133), Science & Technology Project of Beijing, China (No. Z221100007422121).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
Thanks to the joint efforts of all the authors.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Lin, Y. C.; Chang, Y. H.; Yang, S. Y.; Wu, K. D.; Chu, T. S. Update of pathophysiology and management of diabetic kidney disease. J Formos Med Assoc 2018, 117, 662–675. [Google Scholar] [CrossRef] [PubMed]
- DeFronzo, R. A.; Reeves, W. B.; Awad, A. S. Pathophysiology of diabetic kidney disease: impact of SGLT2 inhibitors. Nat Rev Nephrol 2021, 17, 319–334. [Google Scholar] [CrossRef] [PubMed]
- Johansen, K. L.; Garimella, P. S.; Hicks, C. W.; Kalra, P. A.; Kelly, D. M.; Martens, S.; Matsushita, K.; Sarafidis, P.; Sood, M. M.; Herzog, C. A.; Cheung, M.; Jadoul, M.; Winkelmayer, W. C.; Reinecke, H. Central and peripheral arterial diseases in chronic kidney disease: conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int 2021, 100, 35–48. [Google Scholar] [CrossRef] [PubMed]
- Heyman, S. N.; Raz, I.; Dwyer, J. P.; Weinberg Sibony, R.; Lewis, J. B.; Abassi, Z. Diabetic Proteinuria Revisited: Updated Physiologic Perspectives. Cells 2022, 11. [Google Scholar] [CrossRef]
- Yoshimoto, N.; Hayashi, K.; Hishikawa, A.; Hashiguchi, A.; Nakamichi, R.; Sugita-Nishimura, E.; Yoshida-Hama, E.; Azegami, T.; Nakayama, T.; Itoh, H. Significance of podocyte DNA damage and glomerular DNA methylation in CKD patients with proteinuria. Hypertens Res 2023, 46, 1000–1008. [Google Scholar] [CrossRef]
- Li, H.; Dai, W.; Liu, Z.; He, L. Renal Proximal Tubular Cells: A New Site for Targeted Delivery Therapy of Diabetic Kidney Disease. Pharmaceuticals (Basel) 2022, 15. [Google Scholar] [CrossRef]
- Liu, J.; Li, X.; Xu, N.; Han, H.; Li, X. Role of ion channels in the mechanism of proteinuria (Review). Exp Ther Med 2023, 25, 27. [Google Scholar] [CrossRef]
- Xiao, M.; Bohnert, B. N.; Grahammer, F.; Artunc, F. Rodent models to study sodium retention in experimental nephrotic syndrome. Acta Physiol (Oxf) 2022, 235, e13844. [Google Scholar] [CrossRef]
- Shen, W.; Alshehri, M.; Desale, S.; Wilcox, C. The Effect of Amiloride on Proteinuria in Patients with Proteinuric Kidney Disease. Am J Nephrol 2021, 52, 368–377. [Google Scholar] [CrossRef]
- Tamargo, J.; Ruilope, L. M. Investigational calcium channel blockers for the treatment of hypertension. Expert Opin Investig Drugs 2016, 25, 1295–1309. [Google Scholar] [CrossRef]
- Zhou, Y.; Castonguay, P.; Sidhom, E. H.; Clark, A. R.; Dvela-Levitt, M.; Kim, S.; Sieber, J.; Wieder, N.; Jung, J. Y.; Andreeva, S.; Reichardt, J.; Dubois, F.; Hoffmann, S. C.; Basgen, J. M.; Montesinos, M. S.; Weins, A.; Johnson, A. C.; Lander, E. S.; Garrett, M. R.; Hopkins, C. R.; Greka, A. A small-molecule inhibitor of TRPC5 ion channels suppresses progressive kidney disease in animal models. Science 2017, 358, 1332–1336. [Google Scholar] [CrossRef] [PubMed]
- Hall, G.; Wang, L.; Spurney, R. F. TRPC Channels in Proteinuric Kidney Diseases. Cells 2019, 9. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Zhang, L.; Shi, Y.; Yi, H.; Zhao, Y.; Chen, J.; Pollock, C. A.; Chen, X. M. The KCa3.1 blocker TRAM34 reverses renal damage in a mouse model of established diabetic nephropathy. PLoS One 2018, 13, e0192800. [Google Scholar] [CrossRef] [PubMed]
- Gualdani, R.; Seghers, F.; Yerna, X.; Schakman, O.; Tajeddine, N.; Achouri, Y.; Tissir, F.; Devuyst, O.; Gailly, P. Mechanical activation of TRPV4 channels controls albumin reabsorption by proximal tubule cells. Sci Signal 2020, 13. [Google Scholar] [CrossRef]
- Jentsch, T. J.; Pusch, M. CLC Chloride Channels and Transporters: Structure, Function, Physiology, and Disease. Physiol Rev 2018, 98, 1493–1590. [Google Scholar] [CrossRef]
- Tinker, A.; Aziz, Q.; Li, Y.; Specterman, M. ATP-Sensitive Potassium Channels and Their Physiological and Pathophysiological Roles. Compr Physiol 2018, 8, 1463–1511. [Google Scholar]
- Shimizu, M. H.; Volpini, R. A.; de Bragança, A. C.; Campos, R.; Canale, D.; Sanches, T. R.; Andrade, L.; Seguro, A. C. N-acetylcysteine attenuates renal alterations induced by senescence in the rat. Exp Gerontol 2013, 48, 298–303. [Google Scholar] [CrossRef]
- Andrassy, K. M. Comments on 'KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease'. Kidney Int 2013, 84, 622–3. [Google Scholar] [CrossRef]
- Lin, X.; Xiao, Y.; Tian, Y.; Cheng, B.; Jiao, X.; Yang, X.; Wang, Y.; Xiong, W.; Guo, W.; Wu, Q.; Zhang, Q. Can the Artificial Intelligence System for Urine Microalbuminuria Detection Monitor the Progression of Diabetic Kidney Disease in the Clinical Laboratory? Diabetes Care 2022, 45, e136–e138. [Google Scholar] [CrossRef]
- Kovesdy, C. P.; Lott, E. H.; Lu, J. L.; Malakauskas, S. M.; Ma, J. Z.; Molnar, M. Z.; Kalantar-Zadeh, K. Outcomes associated with microalbuminuria: effect modification by chronic kidney disease. J Am Coll Cardiol 2013, 61, 1626–33. [Google Scholar] [CrossRef]
- van der Velde, M.; Matsushita, K.; Coresh, J.; Astor, B. C.; Woodward, M.; Levey, A.; de Jong, P.; Gansevoort, R. T.; van der Velde, M.; Matsushita, K.; Coresh, J.; Astor, B. C.; Woodward, M.; Levey, A. S.; de Jong, P. E.; Gansevoort, R. T.; Levey, A.; El-Nahas, M.; Eckardt, K. U.; Kasiske, B. L.; Ninomiya, T.; Chalmers, J.; Macmahon, S.; Tonelli, M.; Hemmelgarn, B.; Sacks, F.; Curhan, G.; Collins, A. J.; Li, S.; Chen, S. C.; Hawaii Cohort, K. P.; Lee, B. J.; Ishani, A.; Neaton, J.; Svendsen, K.; Mann, J. F.; Yusuf, S.; Teo, K. K.; Gao, P.; Nelson, R. G.; Knowler, W. C.; Bilo, H. J.; Joosten, H.; Kleefstra, N.; Groenier, K. H.; Auguste, P.; Veldhuis, K.; Wang, Y.; Camarata, L.; Thomas, B.; Manley, T. Lower estimated glomerular filtration rate and higher albuminuria are associated with all-cause and cardiovascular mortality. A collaborative meta-analysis of high-risk population cohorts. Kidney Int 2011, 79, 1341-52. [Google Scholar] [CrossRef] [PubMed]
- Addendum. 11. Chronic Kidney Disease and Risk Management: Standards of Medical Care in Diabetes-2022. Diabetes Care 2022;45(Suppl. 1): S175-S184. Diabetes Care 2022, 45, 2182-2184.
- Levey, A. S.; Cattran, D.; Friedman, A.; Miller, W. G.; Sedor, J.; Tuttle, K.; Kasiske, B.; Hostetter, T. Proteinuria as a surrogate outcome in CKD: report of a scientific workshop sponsored by the National Kidney Foundation and the US Food and Drug Administration. Am J Kidney Dis 2009, 54, 205–26. [Google Scholar] [CrossRef] [PubMed]
- An, N.; Wu, B. T.; Yang, Y. W.; Huang, Z. H.; Feng, J. F. Re-understanding and focusing on normoalbuminuric diabetic kidney disease. Front Endocrinol (Lausanne) 2022, 13, 1077929. [Google Scholar] [CrossRef]
- Oshima, M.; Shimizu, M.; Yamanouchi, M.; Toyama, T.; Hara, A.; Furuichi, K.; Wada, T. Trajectories of kidney function in diabetes: a clinicopathological update. Nat Rev Nephrol 2021, 17, 740–750. [Google Scholar] [CrossRef] [PubMed]
- D'Marco, L.; Puchades, M. J.; Escudero-Saiz, V.; Giménez-Civera, E.; Terradez, L.; Moscardó, A.; Carbonell-Asins, J. A.; Pérez-Bernat, E.; Torregrosa, I.; Moncho, F.; Navarro, J.; Górriz, J. L. Renal Histologic Findings in Necropsies of Type 2 Diabetes Mellitus Patients. J Diabetes Res 2022, 2022, 3893853. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Liu, X.; Qu, X.; Zhu, P.; Wo, F.; Xu, X.; Jin, J.; He, Q.; Wu, J. Integration of metabolomics and peptidomics reveals distinct molecular landscape of human diabetic kidney disease. Theranostics 2023, 13, 3188–3203. [Google Scholar] [CrossRef]
- Smith, D. A.; Simpson, K.; Lo Cicero, M.; Newbury, L. J.; Nicholas, P.; Fraser, D. J.; Caiger, N.; Redman, J. E.; Bowen, T. Detection of urinary microRNA biomarkers using diazo sulfonamide-modified screen printed carbon electrodes. RSC Adv 2021, 11, 18832–18839. [Google Scholar] [CrossRef]
- Brenner, B. M.; Cooper, M. E.; de Zeeuw, D.; Keane, W. F.; Mitch, W. E.; Parving, H. H.; Remuzzi, G.; Snapinn, S. M.; Zhang, Z.; Shahinfar, S. Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N Engl J Med 2001, 345, 861–9. [Google Scholar] [CrossRef]
- ElSayed, N. A.; Aleppo, G.; Aroda, V. R.; Bannuru, R. R.; Brown, F. M.; Bruemmer, D.; Collins, B. S.; Hilliard, M. E.; Isaacs, D.; Johnson, E. L.; Kahan, S.; Khunti, K.; Leon, J.; Lyons, S. K.; Perry, M. L.; Prahalad, P.; Pratley, R. E.; Seley, J. J.; Stanton, R. C.; Gabbay, R. A.; on behalf of the American Diabetes, A., 11. Chronic Kidney Disease and Risk Management: Standards of Care in Diabetes-2023. Diabetes Care 2023, 46 (Suppl 1), S191-s202.
- KDIGO 2022 Clinical Practice Guideline for Diabetes Management in Chronic Kidney Disease. Kidney Int 2022, 102, S1–s127. [CrossRef]
- Caruso, I.; Giorgino, F. SGLT-2 inhibitors as cardio-renal protective agents. Metabolism 2022, 127, 154937. [Google Scholar] [CrossRef]
- Muskiet, M. H. A.; Wheeler, D. C.; Heerspink, H. J. L. New pharmacological strategies for protecting kidney function in type 2 diabetes. Lancet Diabetes Endocrinol 2019, 7, 397–412. [Google Scholar] [CrossRef] [PubMed]
- Kaze, A. D.; Zhuo, M.; Kim, S. C.; Patorno, E.; Paik, J. M. Association of SGLT2 inhibitors with cardiovascular, kidney, and safety outcomes among patients with diabetic kidney disease: a meta-analysis. Cardiovasc Diabetol 2022, 21, 47. [Google Scholar] [CrossRef] [PubMed]
- Forst, T.; Mathieu, C.; Giorgino, F.; Wheeler, D. C.; Papanas, N.; Schmieder, R. E.; Halabi, A.; Schnell, O.; Streckbein, M.; Tuttle, K. R. New strategies to improve clinical outcomes for diabetic kidney disease. BMC Med 2022, 20, 337. [Google Scholar] [CrossRef] [PubMed]
- Luo, X.; Xu, J.; Zhou, S.; Xue, C.; Chen, Z.; Mao, Z. Influence of SGLT2i and RAASi and Their Combination on Risk of Hyperkalemia in DKD: A Network Meta-Analysis. Clin J Am Soc Nephrol 2023, 18, 1019–1030. [Google Scholar] [CrossRef] [PubMed]
- Górriz, J. L.; Navarro-González, J. F.; Ortiz, A.; Vergara, A.; Nuñez, J.; Jacobs-Cachá, C.; Martínez-Castelao, A.; Soler, M. J. Sodium-glucose cotransporter 2 inhibition: towards an indication to treat diabetic kidney disease. Nephrol Dial Transplant 2020, 35 (Suppl 1), i13–i23. [Google Scholar] [CrossRef]
- Palmer, S. C.; Tendal, B.; Mustafa, R. A.; Vandvik, P. O.; Li, S.; Hao, Q.; Tunnicliffe, D.; Ruospo, M.; Natale, P.; Saglimbene, V.; Nicolucci, A.; Johnson, D. W.; Tonelli, M.; Rossi, M. C.; Badve, S. V.; Cho, Y.; Nadeau-Fredette, A. C.; Burke, M.; Faruque, L. I.; Lloyd, A.; Ahmad, N.; Liu, Y.; Tiv, S.; Millard, T.; Gagliardi, L.; Kolanu, N.; Barmanray, R. D.; McMorrow, R.; Raygoza Cortez, A. K.; White, H.; Chen, X.; Zhou, X.; Liu, J.; Rodríguez, A. F.; González-Colmenero, A. D.; Wang, Y.; Li, L.; Sutanto, S.; Solis, R. C.; Díaz González-Colmenero, F.; Rodriguez-Gutierrez, R.; Walsh, M.; Guyatt, G.; Strippoli, G. F. M. Sodium-glucose cotransporter protein-2 (SGLT-2) inhibitors and glucagon-like peptide-1 (GLP-1) receptor agonists for type 2 diabetes: systematic review and network meta-analysis of randomised controlled trials. Bmj 2021, 372, m4573. [Google Scholar] [CrossRef]
- Michos, E. D.; Bakris, G. L.; Rodbard, H. W.; Tuttle, K. R. Glucagon-like peptide-1 receptor agonists in diabetic kidney disease: A review of their kidney and heart protection. Am J Prev Cardiol 2023, 14, 100502. [Google Scholar] [CrossRef]
- Nicotera, R.; Casarella, A.; Longhitano, E.; Bolignano, D.; Andreucci, M.; De Sarro, G.; Cernaro, V.; Russo, E.; Coppolino, G. Antiproteinuric effect of DPP-IV inhibitors in diabetic and non-diabetic kidney diseases. Pharmacol Res 2020, 159, 105019. [Google Scholar] [CrossRef]
- Rossing, P.; Baeres, F. M. M.; Bakris, G.; Bosch-Traberg, H.; Gislum, M.; Gough, S. C. L.; Idorn, T.; Lawson, J.; Mahaffey, K. W.; Mann, J. F. E.; Mersebach, H.; Perkovic, V.; Tuttle, K.; Pratley, R. The rationale, design and baseline data of FLOW, a kidney outcomes trial with once-weekly semaglutide in people with type 2 diabetes and chronic kidney disease. Nephrol Dial Transplant 2023. [Google Scholar] [CrossRef]
- González-Albarrán, O.; Morales, C.; Pérez-Maraver, M.; Aparicio-Sánchez, J. J.; Simó, R. Review of SGLT2i for the Treatment of Renal Complications: Experience in Patients with and Without T2D. Diabetes Ther 2022, 13 (Suppl 1), 35–49. [Google Scholar] [CrossRef]
- Wang, J.; Xiang, H.; Lu, Y.; Wu, T.; Ji, G. New progress in drugs treatment of diabetic kidney disease. Biomed Pharmacother 2021, 141, 111918. [Google Scholar] [CrossRef] [PubMed]
- Hartman, R. E.; Rao, P. S. S.; Churchwell, M. D.; Lewis, S. J. Novel therapeutic agents for the treatment of diabetic kidney disease. Expert Opin Investig Drugs 2020, 29, 1277–1293. [Google Scholar] [CrossRef] [PubMed]
- Warren, A. M.; Knudsen, S. T.; Cooper, M. E. Diabetic nephropathy: an insight into molecular mechanisms and emerging therapies. Expert Opin Ther Targets 2019, 23, 579–591. [Google Scholar] [CrossRef]
- Kogot-Levin, A.; Hinden, L.; Riahi, Y.; Israeli, T.; Tirosh, B.; Cerasi, E.; Mizrachi, E. B.; Tam, J.; Mosenzon, O.; Leibowitz, G. Proximal Tubule mTORC1 Is a Central Player in the Pathophysiology of Diabetic Nephropathy and Its Correction by SGLT2 Inhibitors. Cell Rep 2020, 32, 107954. [Google Scholar] [CrossRef]
- Kim, N. H.; Kim, N. H. Renoprotective Mechanism of Sodium-Glucose Cotransporter 2 Inhibitors: Focusing on Renal Hemodynamics. Diabetes Metab J 2022, 46, 543–551. [Google Scholar] [CrossRef] [PubMed]
- Salvatore, T.; Galiero, R.; Caturano, A.; Rinaldi, L.; Di Martino, A.; Albanese, G.; Di Salvo, J.; Epifani, R.; Marfella, R.; Docimo, G.; Lettieri, M.; Sardu, C.; Sasso, F. C. An Overview of the Cardiorenal Protective Mechanisms of SGLT2 Inhibitors. Int J Mol Sci 2022, 23. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Wang, J.; Lin, Y.; Liu, Y.; Zhou, T. Signaling Pathways of Podocyte Injury in Diabetic Kidney Disease and the Effect of Sodium-Glucose Cotransporter 2 Inhibitors. Cells 2022, 11. [Google Scholar] [CrossRef]
- Durcan, E.; Ozkan, S.; Saygi, H. I.; Dincer, M. T.; Korkmaz, O. P.; Sahin, S.; Karaca, C.; Sulu, C.; Bakir, A.; Ozkaya, H. M.; Trabulus, S.; Guzel, E.; Seyahi, N.; Gonen, M. S. Effects of SGLT2 inhibitors on patients with diabetic kidney disease: A preliminary study on the basis of podocyturia. J Diabetes 2022, 14, 236–246. [Google Scholar] [CrossRef]
- Feng, L.; Chen, Y.; Li, N.; Yang, X.; Zhou, L.; Li, H.; Wang, T.; Xie, M.; Liu, H. Dapagliflozin delays renal fibrosis in diabetic kidney disease by inhibiting YAP/TAZ activation. Life Sci 2023, 322, 121671. [Google Scholar] [CrossRef]
- Dia, B.; Alkhansa, S.; Njeim, R.; Al Moussawi, S.; Farhat, T.; Haddad, A.; Riachi, M. E.; Nawfal, R.; Azar, W. S.; Eid, A. A. SGLT2 Inhibitor-Dapagliflozin Attenuates Diabetes-Induced Renal Injury by Regulating Inflammation through a CYP4A/20-HETE Signaling Mechanism. Pharmaceutics 2023, 15. [Google Scholar] [CrossRef]
- Rossing, P.; Caramori, M. L.; Chan, J. C. N.; Heerspink, H. J. L.; Hurst, C.; Khunti, K.; Liew, A.; Michos, E. D.; Navaneethan, S. D.; Olowu, W. A.; Sadusky, T.; Tandon, N.; Tuttle, K. R.; Wanner, C.; Wilkens, K. G.; Zoungas, S.; Craig, J. C.; Tunnicliffe, D. J.; Tonelli, M. A.; Cheung, M.; Earley, A.; de Boer, I. H. Executive summary of the KDIGO 2022 Clinical Practice Guideline for Diabetes Management in Chronic Kidney Disease: an update based on rapidly emerging new evidence. Kidney Int 2022, 102, 990–999. [Google Scholar] [CrossRef]
- Rossing, P.; Filippatos, G.; Agarwal, R.; Anker, S. D.; Pitt, B.; Ruilope, L. M.; Chan, J. C. N.; Kooy, A.; McCafferty, K.; Schernthaner, G.; Wanner, C.; Joseph, A.; Scheerer, M. F.; Scott, C.; Bakris, G. L. Finerenone in Predominantly Advanced CKD and Type 2 Diabetes With or Without Sodium-Glucose Cotransporter-2 Inhibitor Therapy. Kidney Int Rep 2022, 7, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Raj, R. Finerenone: a new mineralocorticoid receptor antagonist to beat chronic kidney disease. Curr Opin Nephrol Hypertens 2022, 31, 265–271. [Google Scholar] [CrossRef] [PubMed]
- KDIGO 2020 Clinical Practice Guideline for Diabetes Management in Chronic Kidney Disease. Kidney Int 2020, 98, S1–s115. [CrossRef] [PubMed]
- Agarwal, R.; Kolkhof, P.; Bakris, G.; Bauersachs, J.; Haller, H.; Wada, T.; Zannad, F. Steroidal and non-steroidal mineralocorticoid receptor antagonists in cardiorenal medicine. Eur Heart J 2021, 42, 152–161. [Google Scholar] [CrossRef] [PubMed]
- Barrera-Chimal, J.; Jaisser, F.; Anders, H. J. The mineralocorticoid receptor in chronic kidney disease. Br J Pharmacol 2022, 179, 3152–3164. [Google Scholar] [CrossRef]
- Barrera-Chimal, J.; Lima-Posada, I.; Bakris, G. L.; Jaisser, F. Mineralocorticoid receptor antagonists in diabetic kidney disease - mechanistic and therapeutic effects. Nat Rev Nephrol 2022, 18, 56–70. [Google Scholar] [CrossRef]
- González-Juanatey, J. R.; Górriz, J. L.; Ortiz, A.; Valle, A.; Soler, M. J.; Facila, L. Cardiorenal benefits of finerenone: protecting kidney and heart. Ann Med 2023, 55, 502–513. [Google Scholar] [CrossRef]
- Chaudhuri, A.; Ghanim, H.; Arora, P. Improving the residual risk of renal and cardiovascular outcomes in diabetic kidney disease: A review of pathophysiology, mechanisms, and evidence from recent trials. Diabetes Obes Metab 2022, 24, 365–376. [Google Scholar] [CrossRef]
- Yao, L.; Liang, X.; Wang, P. Therapeutic perspective: evolving evidence of nonsteroidal mineralocorticoid receptor antagonists in diabetic kidney disease. Am J Physiol Endocrinol Metab 2023, 324, E531–e541. [Google Scholar] [CrossRef]
- Kim, D. L.; Lee, S. E.; Kim, N. H. Renal Protection of Mineralocorticoid Receptor Antagonist, Finerenone, in Diabetic Kidney Disease. Endocrinol Metab (Seoul) 2023, 38, 43–55. [Google Scholar] [CrossRef] [PubMed]
- Lv, R.; Xu, L.; Che, L.; Liu, S.; Wang, Y.; Dong, B. Cardiovascular-renal protective effect and molecular mechanism of finerenone in type 2 diabetic mellitus. Front Endocrinol (Lausanne) 2023, 14, 1125693. [Google Scholar] [CrossRef]
- Ortiz, A.; Ferro, C. J.; Balafa, O.; Burnier, M.; Ekart, R.; Halimi, J. M.; Kreutz, R.; Mark, P. B.; Persu, A.; Rossignol, P.; Ruilope, L. M.; Schmieder, R. E.; Valdivielso, J. M.; Del Vecchio, L.; Zoccali, C.; Mallamaci, F.; Sarafidis, P. Mineralocorticoid receptor antagonists for nephroprotection and cardioprotection in patients with diabetes mellitus and chronic kidney disease. Nephrol Dial Transplant 2023, 38, 10–25. [Google Scholar] [CrossRef]
- Bakris, G. L.; Agarwal, R.; Chan, J. C.; Cooper, M. E.; Gansevoort, R. T.; Haller, H.; Remuzzi, G.; Rossing, P.; Schmieder, R. E.; Nowack, C.; Kolkhof, P.; Joseph, A.; Pieper, A.; Kimmeskamp-Kirschbaum, N.; Ruilope, L. M. Effect of Finerenone on Albuminuria in Patients With Diabetic Nephropathy: A Randomized Clinical Trial. Jama 2015, 314, 884–94. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, R.; Anker, S. D.; Bakris, G.; Filippatos, G.; Pitt, B.; Rossing, P.; Ruilope, L.; Gebel, M.; Kolkhof, P.; Nowack, C.; Joseph, A. Investigating new treatment opportunities for patients with chronic kidney disease in type 2 diabetes: the role of finerenone. Nephrol Dial Transplant 2022, 37, 1014–1023. [Google Scholar] [CrossRef] [PubMed]
- Heerspink, H. J. L.; Jongs, N.; Neuen, B. L.; Schloemer, P.; Vaduganathan, M.; Inker, L. A.; Fletcher, R. A.; Wheeler, D. C.; Bakris, G.; Greene, T.; Chertow, G. M.; Perkovic, V. Effects of newer kidney protective agents on kidney endpoints provide implications for future clinical trials. Kidney Int 2023, 104, 181–188. [Google Scholar] [CrossRef]
- Heerspink, H. J. L.; Parving, H. H.; Andress, D. L.; Bakris, G.; Correa-Rotter, R.; Hou, F. F.; Kitzman, D. W.; Kohan, D.; Makino, H.; McMurray, J. J. V.; Melnick, J. Z.; Miller, M. G.; Pergola, P. E.; Perkovic, V.; Tobe, S.; Yi, T.; Wigderson, M.; de Zeeuw, D. Atrasentan and renal events in patients with type 2 diabetes and chronic kidney disease (SONAR): a double-blind, randomised, placebo-controlled trial. Lancet 2019, 393, 1937–1947. [Google Scholar] [CrossRef]
- de Zeeuw, D.; Coll, B.; Andress, D.; Brennan, J. J.; Tang, H.; Houser, M.; Correa-Rotter, R.; Kohan, D.; Lambers Heerspink, H. J.; Makino, H.; Perkovic, V.; Pritchett, Y.; Remuzzi, G.; Tobe, S. W.; Toto, R.; Viberti, G.; Parving, H. H. The endothelin antagonist atrasentan lowers residual albuminuria in patients with type 2 diabetic nephropathy. J Am Soc Nephrol 2014, 25, 1083–93. [Google Scholar] [CrossRef]
- Fernandez-Fernandez, B.; Fernandez-Prado, R.; Górriz, J. L.; Martinez-Castelao, A.; Navarro-González, J. F.; Porrini, E.; Soler, M. J.; Ortiz, A. Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation and Study of Diabetic Nephropathy with Atrasentan: what was learned about the treatment of diabetic kidney disease with canagliflozin and atrasentan? Clin Kidney J 2019, 12, 313–321. [Google Scholar] [CrossRef]
- Heerspink, H. J. L.; Xie, D.; Bakris, G.; Correa-Rotter, R.; Hou, F. F.; Kitzman, D. W.; Kohan, D.; Makino, H.; McMurray, J. J. V.; Perkovic, V.; Rossing, P.; Parving, H. H.; de Zeeuw, D. Early Response in Albuminuria and Long-Term Kidney Protection during Treatment with an Endothelin Receptor Antagonist: A Prespecified Analysis from the SONAR Trial. J Am Soc Nephrol 2021, 32, 2900–2911. [Google Scholar] [CrossRef]
- Zhang, S.; Li, X.; Liu, S.; Zhang, W.; Li, M.; Qiao, C. Research progress on the role of ET-1 in diabetic kidney disease. J Cell Physiol 2023, 238, 1183–1192. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Díaz, I.; Martos, N.; Llorens-Cebrià, C.; Álvarez, F. J.; Bedard, P. W.; Vergara, A.; Jacobs-Cachá, C.; Soler, M. J. Endothelin Receptor Antagonists in Kidney Disease. Int J Mol Sci 2023, 24. [Google Scholar] [CrossRef] [PubMed]
- Kohan, D. E.; Barton, M. Endothelin and endothelin antagonists in chronic kidney disease. Kidney Int 2014, 86, 896–904. [Google Scholar] [CrossRef] [PubMed]
- Smeijer, J. D.; Kohan, D. E.; Webb, D. J.; Dhaun, N.; Heerspink, H. J. L. Endothelin receptor antagonists for the treatment of diabetic and nondiabetic chronic kidney disease. Curr Opin Nephrol Hypertens 2021, 30, 456–465. [Google Scholar] [CrossRef] [PubMed]
- Garsen, M.; Lenoir, O.; Rops, A. L.; Dijkman, H. B.; Willemsen, B.; van Kuppevelt, T. H.; Rabelink, T. J.; Berden, J. H.; Tharaux, P. L.; van der Vlag, J. Endothelin-1 Induces Proteinuria by Heparanase-Mediated Disruption of the Glomerular Glycocalyx. J Am Soc Nephrol 2016, 27, 3545–3551. [Google Scholar] [CrossRef] [PubMed]
- Allison, S. J. Diabetic nephropathy: Atrasentan stabilizes the endothelial glycocalyx. Nat Rev Nephrol 2016, 12, 315. [Google Scholar] [CrossRef]
- Dolinina, J.; Rippe, A.; Öberg, C. M. Sustained, delayed, and small increments in glomerular permeability to macromolecules during systemic ET-1 infusion mediated via the ETA receptor. Am. J. Physiol. Renal Physiol. 2019, 316, F1173–f1179. [Google Scholar] [CrossRef]
- Shanshan, C.; Huiru, C.; Hanbing, Y.; Xiaoxiao, L. Clinical study on Keluoxin Capsules combined with benazepril in treatment of diabetic nephropathy. Drugs & Clinic 2020, 35, 1763–1766. [Google Scholar]
- Xianhong, H.; Lei, L.; Xiaoya, C.; Yang, H. Protective effect of Keluoxin capsule on the renal tubules in patients with early diabetic kidney disease. J Clin Nephrol 2014, 14, 101–103. [Google Scholar]
- Qianqin, C.; Tao, H. Effect of keluoxin capsule combined with losartan potassium on elderly diabetic nephropathy and its effect on proteinuria. International Journal of Urology and Nephrology 2022, 42, 691–694. [Google Scholar]
- Medicine, C. A. o. I.; Medicine, C. A. o. C.; Association, C. M., Guidelines for Diagnosis and Management of Diabetic Kidney Disease with Integrated Traditional Chinese and Western Medicine https://www.cacm.org.cn/2023/05/31/23420/Preprint. In 2023.
- Society, C. D. Guideline for the prevention and treatment of type 2 diabetes mellitus in China (2020 edition). Chin J Diabetes Mellitus 2021, 13, 315–409. [Google Scholar]
- Serra, A.; Romero, R.; Bayés, B.; Lopez, D.; Bonet, J. Is there a need for changes in renal biopsy criteria in proteinuria in type 2 diabetes? Diabetes Res Clin Pract 2002, 58, 149–53. [Google Scholar] [CrossRef]
- Wenhua, Z. Efficacy and safety of Keluoxin capsule in combination with Western medicine for diabetic kidney disease: A systematic review and meta-analysis. Frontiers in pharmacology 2022, 13, 1052852. [Google Scholar]
- Chang, L.; Libo, T.; Hao, L.; Housheng, K.; Wei, L.; Yin, L.; Yanming, X.; Xin, C. Pharmacoeconomic evaluation of Keluoxin capsule combined with chemical medicine in the treatment of diabetic kidney disease. China Pharmacy 2022, 33, 2124–2128. [Google Scholar]
- E, P., The impact of hyperfiltration on the diabetic kidney. Diabetes & metabolism 2015, 41, 5-17.
- Chunxue, Z.; Tianshu, G.; Fengnuan, Z.; Yiwen, L. Effect of Keluoxin Capsule on Early Hyperfiltration in Diabetic Kidney Disease Rats Based on Tubuloglomerular Feedback Mechanism. Chinese Journal of Integrated Traditional and Western Medicine 2023, 43, 822–830. [Google Scholar]
- L, L.; Q, N.; XM, L.; al, e. Study on Mechanism of Protection of Renal Structure and Function by Tangweikang Capsule in Diabetic Rats. Chinese Journal of Experimental Traditional Medical Formulae 2000, 6, 49–50. [Google Scholar]
- Deng, L.; Wang, S.; Leng, X.; Yao, P.; Li, C.; Zheng, Y. Combining network pharmacology and in vitro and in vivo experiments to study the mechanism of Keluoxin in the treatment of radiation nephropathy†. J Radiat Res 2023. [Google Scholar] [CrossRef]
- Kong, L.; Sun, Y.; Sun, H.; Zhang, A. H.; Zhang, B.; Ge, N.; Wang, X. J. Chinmedomics Strategy for Elucidating the Pharmacological Effects and Discovering Bioactive Compounds From Keluoxin Against Diabetic Retinopathy. Front Pharmacol 2022, 13, 728256. [Google Scholar] [CrossRef]
- Huimin, Z.; Jiahui, X.; Qingguang, C.; Hao, L. Study on active ingredients and molecular mechanism of keluoxin in treatment of diabetic kidney disease based on network pharmacology and molecular docking. World Clinical Drugs 2023, 44, 468–476. [Google Scholar]
- XM, Y.; Q, Z.; XK, H.; Y, G.; Q, C., Effect of Keluoxin on Oxidative Stress and Inflammatory Response in the Kidney of Type 2 Diabetic Nephropathy Rats Model. World Science and Technology-Modernization of Traditional Chinese Medicine 2023, 25, 1177-1185.
- Yang, X.; Han, X.; Wen, Q.; Qiu, X.; Deng, H.; Chen, Q. Protective Effect of Keluoxin against Diabetic Nephropathy in Type 2 Diabetic Mellitus Models. Evid Based Complement Alternat Med 2021, 2021, 8455709. [Google Scholar] [CrossRef]
- Shao, M.; Ye, C.; Bayliss, G.; Zhuang, S. New Insights Into the Effects of Individual Chinese Herbal Medicines on Chronic Kidney Disease. Front Pharmacol 2021, 12, 774414. [Google Scholar] [CrossRef] [PubMed]
- Tan, Y.; Li, R.; Zhou, P.; Li, N.; Xu, W.; Zhou, X.; Yan, Q.; Yu, J. Huobahuagen tablet improves renal function in diabetic kidney disease: a real-world retrospective cohort study. Front Endocrinol (Lausanne) 2023, 14, 1166880. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Tostivint, I.; Xu, L.; Huang, J.; Gambotti, L.; Boffa, J. J.; Yang, M.; Wang, L.; Sun, Z.; Chen, X.; Liou-Schischmanoff, A.; Baumelou, A.; Ma, T.; Lu, G.; Li, L.; Chen, D.; Piéroni, L.; Liu, B.; Qin, X.; He, W.; Wang, Y.; Gu, H. F.; Sun, W. Efficacy of Combined Abelmoschus manihot and Irbesartan for Reduction of Albuminuria in Patients With Type 2 Diabetes and Diabetic Kidney Disease: A Multicenter Randomized Double-Blind Parallel Controlled Clinical Trial. Diabetes Care 2022, 45, e113–e115. [Google Scholar] [CrossRef] [PubMed]
- Wei, L. I.; Ping, X.; Wei, S.; Jing, Z.; Qiong, L.; Lianyi, G.; Yao, Z.; Kun, G. Effects of the Huangkui capsule on chronic kidney disease: a systematic review and Meta-analysis. J Tradit Chin Med 2023, 43, 6–13. [Google Scholar]
- Zhao, L.; Han, S.; Chai, C. Huangkui capsule alleviates doxorubicin-induced proteinuria via protecting against podocyte damage and inhibiting JAK/STAT signaling. J Ethnopharmacol 2023, 306, 116150. [Google Scholar] [CrossRef]
- Shi, R.; Tao, Y.; Tang, H.; Wu, C.; Fei, J.; Ge, H.; Gu, H. F.; Wu, J. Abelmoschus Manihot ameliorates the levels of circulating metabolites in diabetic nephropathy by modulating gut microbiota in non-obese diabetes mice. Microb Biotechnol 2023, 16, 813–826. [Google Scholar] [CrossRef]
- Gu, L. Y.; Yun, S.; Tang, H. T.; Xu, Z. X. Huangkui capsule in combination with metformin ameliorates diabetic nephropathy via the Klotho/TGF-β1/p38MAPK signaling pathway. J Ethnopharmacol 2021, 281, 113548. [Google Scholar] [CrossRef]
- Han, W.; Ma, Q.; Liu, Y.; Wu, W.; Tu, Y.; Huang, L.; Long, Y.; Wang, W.; Yee, H.; Wan, Z.; Tang, R.; Tang, H.; Wan, Y. Huangkui capsule alleviates renal tubular epithelial-mesenchymal transition in diabetic nephropathy via inhibiting NLRP3 inflammasome activation and TLR4/NF-κB signaling. Phytomedicine 2019, 57, 203–214. [Google Scholar] [CrossRef]
- Ma, C. E.; Yu, P.; Wei, W.; Chen, X. Q. Efficacy of combined angiotensin II receptor blocker with tripterygium glycosides on diabetic nephropathy: A protocol for meta-analysis. Medicine (Baltimore) 2021, 100, e25991. [Google Scholar] [CrossRef]
- Wu, X.; Huang, Y.; Zhang, Y.; He, C.; Zhao, Y. Wang, L.; Gao, J., Efficacy of tripterygium glycosides combined with ARB on diabetic nephropathy: a meta-analysis. Biosci Rep 2020, 40. [Google Scholar] [CrossRef]
- Xie, D.; Li, K.; Ma, T.; Jiang, H.; Wang, F.; Huang, M.; Sheng, Z.; Xie, Y., Therapeutic Effect and Safety of Tripterygium Glycosides Combined With Western Medicine on Type 2 Diabetic Kidney Disease: A Meta-Analysis. Clin Ther 2022, 44, 246-256.e10.
- Li, Y.; Miao, R.; Liu, Y.; Zhang, J.; Dou, Z.; Zhao, L.; Zhang, Y.; Huang, Z.; Xia, Y.; Han, D. Efficacy and Safety of Tripterygium Glycoside in the Treatment of Diabetic Nephropathy: A Systematic Review and Meta-Analysis Based on the Duration of Medication. Front Endocrinol (Lausanne) 2021, 12, 656621. [Google Scholar] [CrossRef] [PubMed]
- Shi, H.; Deng, P.; Dong, C.; Lu, R.; Si, G.; Yang, T. Quality of Evidence Supporting the Role of Tripterygium Glycosides for the Treatment of Diabetic Kidney Disease: An Overview of Systematic Reviews and Meta-Analyses. Drug Des. Devel. Ther. 2022, 16, 1647–1665. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Li, S. L.; Lin, W.; Pan, R. H.; Dai, Y.; Xia, Y. F. Tripterygium glycoside tablet attenuates renal function impairment in diabetic nephropathy mice by regulating triglyceride metabolism. J Pharm Biomed Anal 2022, 221, 115028. [Google Scholar] [CrossRef] [PubMed]
- Fang, Y.; Zhang, Y.; Jia, C.; Ren, C.; Zhao, X.; Zhang, X. Niaoduqing alleviates podocyte injury in high glucose model via regulating multiple targets and AGE/RAGE pathway: Network pharmacology and experimental validation. Front Pharmacol 2023, 14, 1047184. [Google Scholar] [CrossRef]
- Fu, B.; Shang, Z.; Song, S.; Xu, Y.; Wei, L.; Li, G.; Yang, H. Adverse reactions of Niaoduqing granules: A systematic review and meta-analysis. Phytomedicine 2023, 109, 154535. [Google Scholar] [CrossRef]
- Li, X.; Zheng, J.; Wang, J.; Tang, X.; Zhang, F.; Liu, S.; Liao, Y.; Chen, X.; Xie, W.; Tang, Y. Effects of Uremic Clearance Granules on p38 MAPK/NF-κB Signaling Pathway, Microbial and Metabolic Profiles in End-Stage Renal Disease Rats Receiving Peritoneal Dialysis. Drug Des. Devel. Ther. 2022, 16, 2529–2544. [Google Scholar] [CrossRef] [PubMed]
- Liang, M.; Zhu, X.; Zhang, D.; He, W.; Zhang, J.; Yuan, S.; He, Q.; Jin, J. Yi-Shen-Hua-Shi granules inhibit diabetic nephropathy by ameliorating podocyte injury induced by macrophage-derived exosomes. Front Pharmacol 2022, 13, 962606. [Google Scholar] [CrossRef] [PubMed]
- Han, C.; Shen, Z.; Cui, T.; Ai, S. S.; Gao, R. R.; Liu, Y.; Sui, G. Y.; Hu, H. Z.; Li, W. Yi-Shen-Hua-Shi granule ameliorates diabetic kidney disease by the "gut-kidney axis". J Ethnopharmacol 2023, 307, 116257. [Google Scholar] [CrossRef]
- Li, Y.; Xu, G. Clinical Efficacy and Safety of Jinshuibao Combined With ACEI/ARB in the Treatment of Diabetic Kidney Disease: A Meta-Analysis of Randomized Controlled Trials. J Ren Nutr 2020, 30, 92–100. [Google Scholar] [CrossRef]
- Zhang, H.; Yuan, C.; Sun, C.; Zhang, Q. Efficacy of Jinshuibao as an adjuvant treatment for chronic renal failure in China: A meta-analysis. Medicine (Baltimore) 2023, 102, e34575. [Google Scholar] [CrossRef]
- Yu, X.; Yan, D.; Lan, Q.; Fang, J.; Ding, Z.; Guan, Y.; Zhu, W.; Yan, L.; Nie, H. Efficacy and Safety of Jinshuibao Capsule in Diabetic Nephropathy: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Comput Math Methods Med 2022, 2022, 9671768. [Google Scholar] [CrossRef] [PubMed]
- Yan, G.; Chang, T.; Zhao, Y.; Yu, M.; Mi, J.; Wang, G.; Wang, X.; Liao, X. The effects of Ophiocordyceps sinensis combined with ACEI/ARB on diabetic kidney disease: A systematic review and meta-analysis. Phytomedicine 2023, 108, 154531. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Xiao, X.; Li, M.; Yu, M.; Ping, F. Bailing capsule (Cordyceps sinensis) ameliorates renal triglyceride accumulation through the PPARα pathway in diabetic rats. Front Pharmacol 2022, 13, 915592. [Google Scholar] [CrossRef]
- Xu, J.; Yuan, Q.; Wu, K.; Li, X.; Zhao, Y.; Li, X. Effects of Bailing capsule on diabetic nephropathy based on UPLC-MS urine metabolomics. RSC Adv 2019, 9, 35969–35975. [Google Scholar] [CrossRef]
- He, Y.; Li, W.; Zhu, H.; Han, S. Economic evaluation of bailing capsules for patients with diabetic nephropathy in China. Front Pharmacol 2023, 14, 1175310. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Ma, J.; Leng, T.; Yuan, Z.; Hu, T.; Liu, Q.; Shen, T. Advances in oxidative stress in pathogenesis of diabetic kidney disease and efficacy of TCM intervention. Ren Fail 2023, 45, 2146512. [Google Scholar] [CrossRef] [PubMed]
- Tang, X.; Huang, M.; Jiang, J.; Liang, X.; Li, X.; Meng, R.; Chen, L.; Li, Y. Panax notoginseng preparations as adjuvant therapy for diabetic kidney disease: a systematic review and meta-analysis. Pharm Biol 2020, 58, 138–145. [Google Scholar] [CrossRef]
- Wang, X.; He, Q.; Chen, Q.; Xue, B.; Wang, J.; Wang, T.; Liu, H.; Chen, X. Network pharmacology combined with metabolomics to study the mechanism of Shenyan Kangfu Tablets in the treatment of diabetic nephropathy. J Ethnopharmacol 2021, 270, 113817. [Google Scholar] [CrossRef]
- Chen, Q.; Ren, D.; Wu, J.; Yu, H.; Chen, X.; Wang, J.; Zhang, Y.; Liu, M.; Wang, T. Shenyan Kangfu tablet alleviates diabetic kidney disease through attenuating inflammation and modulating the gut microbiota. J Nat Med 2021, 75, 84–98. [Google Scholar] [CrossRef]
- Liao, T.; Zhao, K.; Huang, Q.; Tang, S.; Chen, K.; Xie, C.; Zhang, C.; Gan, W. A randomized controlled clinical trial study protocol of Liuwei Dihuang pills in the adjuvant treatment of diabetic kidney disease. Medicine (Baltimore) 2020, 99, e21137. [Google Scholar] [CrossRef]
- Huang, X.; Gao, L.; Deng, R.; Peng, Y.; Wu, S.; Lu, J.; Liu, X. Huangqi-Danshen decoction reshapes renal glucose metabolism profiles that delays chronic kidney disease progression. Biomed Pharmacother 2023, 164, 114989. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Wang, C.; Bai, D.; Chen, N.; Hu, J.; Zhang, J. Perspectives of international multi-center clinical trials on traditional Chinese herbal medicine. Front Pharmacol 2023, 14, 1195364. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Miao, R.; Yu, T.; Wei, R.; Tian, F.; Huang, Y.; Tong, X.; Zhao, L. Comparative effectiveness of traditional Chinese medicine and angiotensin converting enzyme inhibitors, angiotensin receptor blockers, and sodium glucose cotransporter inhibitors in patients with diabetic kidney disease: A systematic review and network meta-analysis. Pharmacol Res 2022, 177, 106111. [Google Scholar] [PubMed]
- Chen, X.; Dai, W.; Li, H.; Yan, Z.; Liu, Z.; He, L. Targeted drug delivery strategy: a bridge to the therapy of diabetic kidney disease. Drug Deliv 2023, 30, 2160518. [Google Scholar] [CrossRef] [PubMed]
- Raval, N.; Jogi, H.; Gondaliya, P.; Kalia, K.; Tekade, R. K. Method and its Composition for encapsulation, stabilization, and delivery of siRNA in Anionic polymeric nanoplex: An In vitro- In vivo Assessment. Sci Rep 2019, 9, 16047. [Google Scholar] [CrossRef]
- Alomari, G.; Al-Trad, B.; Hamdan, S.; Aljabali, A.; Al-Zoubi, M.; Bataineh, N.; Qar, J.; Tambuwala, M. M. Gold nanoparticles attenuate albuminuria by inhibiting podocyte injury in a rat model of diabetic nephropathy. Drug Deliv Transl Res 2020, 10, 216–226. [Google Scholar] [CrossRef]
- Yue, T.; Xu, H. L.; Chen, P. P.; Zheng, L.; Huang, Q.; Sheng, W. S.; Zhuang, Y. D.; Jiao, L. Z.; Chi, T. T.; ZhuGe, D. L.; Liu, J. J.; Zhao, Y. Z.; Lan, L. Combination of coenzyme Q10-loaded liposomes with ultrasound targeted microbubbles destruction (UTMD) for early theranostics of diabetic nephropathy. Int J Pharm 2017, 528, 664–674. [Google Scholar] [CrossRef]
- Guillot, J.; Maumus-Robert, S.; Bezin, J. Polypharmacy: A general review of definitions, descriptions and determinants. Therapie 2020, 75, 407–416. [Google Scholar] [CrossRef]
- Standards of medical care in diabetes--2014. Diabetes Care 2014, 37 (Suppl 1), S14–80. [CrossRef]
- de Boer, I. H.; Khunti, K.; Sadusky, T.; Tuttle, K. R.; Neumiller, J. J.; Rhee, C. M.; Rosas, S. E.; Rossing, P.; Bakris, G. Diabetes management in chronic kidney disease: a consensus report by the American Diabetes Association (ADA) and Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int 2022, 102, 974–989. [Google Scholar] [CrossRef]
- KDOQI Clinical Practice Guideline for Diabetes and CKD: 2012 Update. Am J Kidney Dis 2012, 60, 850–86. [CrossRef] [PubMed]
- Steuber, T. D.; Lee, J.; Holloway, A.; Andrus, M. R. Nondihydropyridine Calcium Channel Blockers for the Treatment of Proteinuria: A Review of the Literature. Ann Pharmacother 2019, 53, 1050–1059. [Google Scholar] [CrossRef] [PubMed]
- Weber, M. A.; Bakris, G. L.; Jamerson, K.; Weir, M.; Kjeldsen, S. E.; Devereux, R. B.; Velazquez, E. J.; Dahlöf, B.; Kelly, R. Y.; Hua, T. A.; Hester, A.; Pitt, B. Cardiovascular events during differing hypertension therapies in patients with diabetes. J Am Coll Cardiol 2010, 56, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Bell, D. S. H. Combine and Conquer: With Type 2 Diabetes Polypharmacy Is Essential Not Only to Achieve Glycemic Control but Also to Treat the Comorbidities and Stabilize or Slow the Advancement of Diabetic Nephropathy. J Diabetes Res 2022, 2022, 7787732. [Google Scholar] [CrossRef]
- Bell, D. S. H.; Goncalves, E. Diabetogenic effects of cardioprotective drugs. Diabetes Obes Metab 2021, 23, 877–885. [Google Scholar] [CrossRef]
- Piperidou, A.; Sarafidis, P.; Boutou, A.; Thomopoulos, C.; Loutradis, C.; Alexandrou, M. E.; Tsapas, A.; Karagiannis, A. The effect of SGLT-2 inhibitors on albuminuria and proteinuria in diabetes mellitus: a systematic review and meta-analysis of randomized controlled trials. J Hypertens 2019, 37, 1334–1343. [Google Scholar] [CrossRef]
- Agarwal, R.; Anker, S. D.; Filippatos, G.; Pitt, B.; Rossing, P.; Ruilope, L. M.; Boletis, J.; Toto, R.; Umpierrez, G. E.; Wanner, C.; Wada, T.; Scott, C.; Joseph, A.; Ogbaa, I.; Roberts, L.; Scheerer, M. F.; Bakris, G. L. Effects of canagliflozin versus finerenone on cardiorenal outcomes: exploratory post hoc analyses from FIDELIO-DKD compared to reported CREDENCE results. Nephrol Dial Transplant 2022, 37, 1261–1269. [Google Scholar] [CrossRef]
- McGill, J. In A new approach to kidney protection in patients with type 2 diabetes, EASD Meeting, Munich, Germany, 2021; Munich, Germany, 2021.
- Stuart, D.; Peterson, C. S.; Hu, C.; Revelo, M. P.; Huang, Y.; Kohan, D. E.; Ramkumar, N. Lack of renoprotective effects of targeting the endothelin A receptor and (or) sodium glucose transporter 2 in a mouse model of Type 2 diabetic kidney disease. Can J Physiol Pharmacol 2022, 100, 763–771. [Google Scholar] [CrossRef]
- Batu Demir, D.; Cooper, M. E. New strategies to tackle diabetic kidney disease. Curr Opin Nephrol Hypertens 2016, 25, 348–54. [Google Scholar] [CrossRef]
Figure 1.
Pathophysiological mechanisms underlying albuminuria in patients with DKD and related drugs. SGLT2i, SGLT-2 inhibitors; MRAs, nonsteroidal mineralocorticoid receptor antagonists; ERAs, endothelin receptor antagonists. The left panel shows pathological glomerular filtration membranes, atrophic renal tubular epithelial cells and interstitial fibrosis and the mechanism of drug action. The right panel shows the physiological mechanism of the kidney in a normal person.
Figure 1.
Pathophysiological mechanisms underlying albuminuria in patients with DKD and related drugs. SGLT2i, SGLT-2 inhibitors; MRAs, nonsteroidal mineralocorticoid receptor antagonists; ERAs, endothelin receptor antagonists. The left panel shows pathological glomerular filtration membranes, atrophic renal tubular epithelial cells and interstitial fibrosis and the mechanism of drug action. The right panel shows the physiological mechanism of the kidney in a normal person.
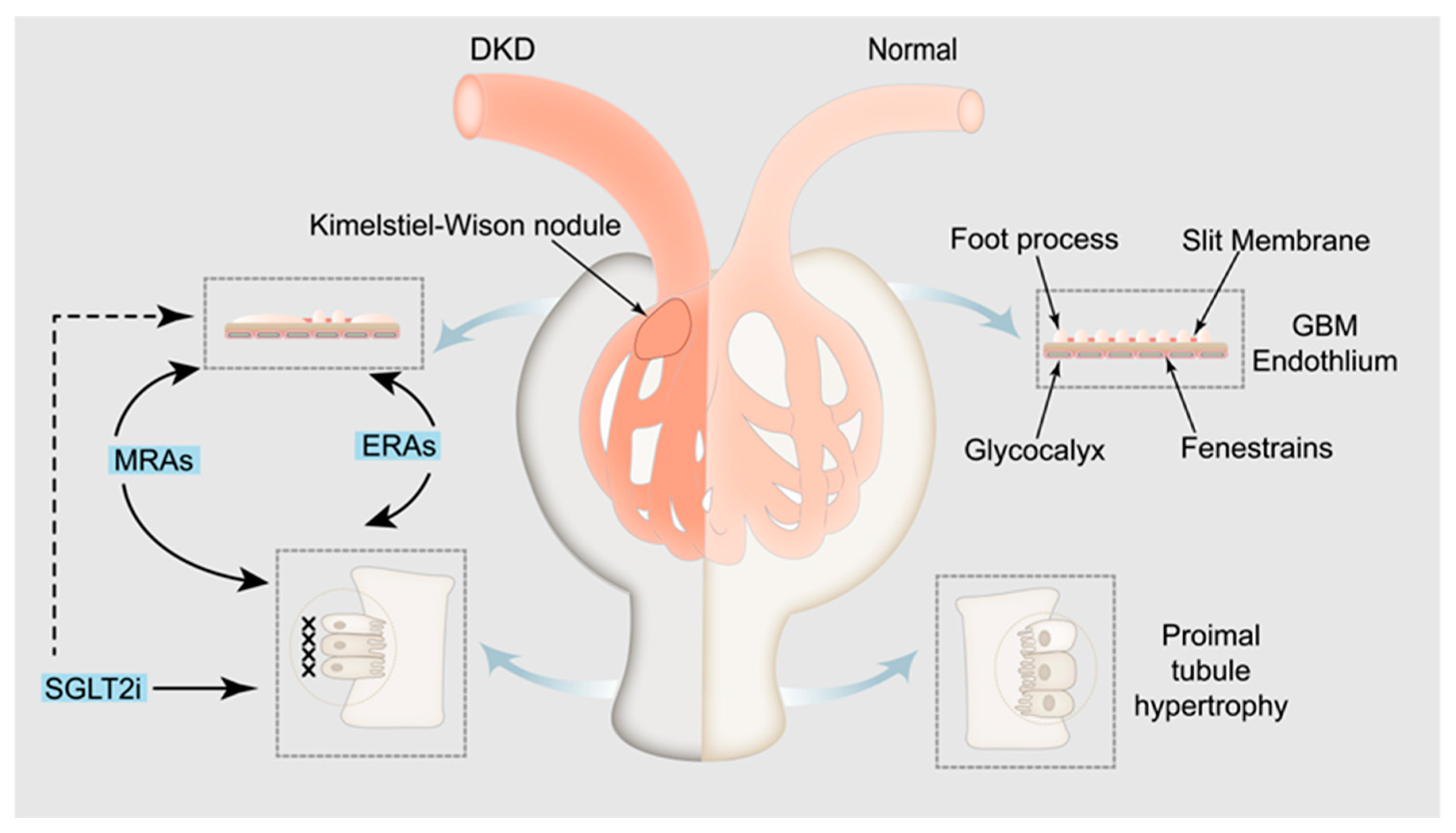

Table 1.
Mechanisms of pharmacologic treatment of albuminuria in DKD.
| Drugs | Therapeutic Mechanisms for Albuminuria in DKD | Reference |
|---|---|---|
| SGLT-2 Inhibitors |
|
1. [33,42,43,44,45,46,47,48] 2. [2,49,50] 3. [51,52] |
| Nonsteroidal Mineralocorticoid Receptor Antagonists | Instead of aldosterone and MR, leading to a proinflammatory and fibrosis of gene expression. | [57,58,59,60,61,62,63,64,65] |
| Endothelin Receptor Antagonists | It binds to ET-1 to protect the glomerular filtration barrier and reverse glomerular hyperfiltration ang improve renal fibrosis. | [77,78,79] |
| Keluoxin Capsule |
|
1. [88,89,90] 2. [91,92,93,94] 3. [95] |
| Huangkui Capsule |
|
1. [100] 2. [101] 3. [102,103] |
| Tripterygium Glycosides | It can promote the decomposition of renal triglyceride and improve the damaged renal function. | [109] |
| Niaoduqing granule |
|
1. [110] 2. [112] |
| Yishen Huashi granule |
|
1. [113] 2. [114] |
| Cordyceps sinensis preparation |
|
1. [119] 2. [120] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



