
Submitted:
22 August 2023
Posted:
23 August 2023
You are already at the latest version
Abstract
With enhanced life expectancy and ageing global populations, the prevalence of multimorbidity continues to increase. However, there is a dearth of evidence linked to multimorbidity diagnoses, treatments and health outcomes which remains a concern for future proofing optimal healthcare services. Generating evidence is critical to managing multimorbidity, promoting public health and minimizing health inequalities via effective healthcare policies that improve quality of life for vulnerable populations. This study assessed meta-epidemiology of multimorbidity to report the gaps in scientific knowledge and clinical practice. A systematic methodology was designed and published in PROSPERO (CRD42022347308) to report meta-epidemiology analyses using databases including PubMed, Web of Science, ScienceDirect, EMBASE, The Cochrane Gynaecology and Fertility Group Specialised Register of Controlled Trials and MEDLINE for studies published between the 1st of January 1980 - 31st December 2022. A random-effects model was used to estimate the pooled proportion of multimorbidity in adults. Forest plots, pooled odds ratios and statistical heterogeneity metrics were used to assess the association between multimorbidity and investigated factors. Funnel plots and Egger’s regression were used to detect and correct for publication bias. Our findings identified women to be 0.32 times more likely to have multimorbidity in comparison to males. In regard to ethnicity, white people were 0.47 times less likely to develop comorbidities than black people. People who identified as a drinker or unmarried were more likely to develop comorbidities than those who are non-drinkers or married, respectively. Regardless of smoking status, people were equally likely to have comorbidity. In terms of environmental influences, people in rural areas were found to be 0.2 times less likely to have comorbidity in comparison to those living in urban areas. Interestingly, people with a higher education level were 0.57 times more likely to develop comorbidities than those with only a high school education. It is evident that multimorbidity has a significant burden globally and impacts the provision of care necessitated across populations given its association with several social determinants of health. Robust research and healthcare policies are required to better manage multimorbidity in patients. An example of such intervention includes employing prevention programs to reduce risk and incidence of multimorbidity within at-risk populations.
Keywords:
Multimorbidity
; Chronic condition
; Health Inequalities
; Global health
; Epidemiology
Background
Multimorbidity is defined as the presence of two or more chronic conditions in a given individual. The rise in ageing populations globally due to improvements in life expectancy elevates risk of chronic health conditions such as diabetes, cancer, human immunodeficiency virus/ acquired immunodeficiency syndrome, mental health and pain conditions1,2. Multimorbidity is common amongst vulnerable populations such as those impacted by socioeconomic inequities that accelerate the process for deprivations. In fact, Link and Phelan have found socioeconomic status and support to be “fundamental causes” of disease outcomes due to these factors enabling access to resources regardless of individual-based interventions.3 On the other hand, younger populations such as adolescents and children with congenital or acquired impairments may suffer from multimorbidity as a result of becoming physically or mentally ill.
Patients with multimorbidity have been found to a be at a higher risk of safety issues due to the use of polypharmacy and complex regimen management prescribed by multidisciplinary healthcare professionals. Given the complexities of combination treatments and competing priorities regarding clinical regimens, communication failure between healthcare professional and patients remains a challenge. Multimorbidity is also highly associated with worsening clinical outcomes, poorer quality of life, and increasing healthcare expenditures[3-6]. At present, multimorbidity trends present a challenge across key stakeholders ranging from medical professions across disciplines to community care, which require extensive specialization for hospitals.
On a macroscale, multimorbidity has been associated with varying demographic factors such as gender and region. For instance, women have been linked with higher multimorbidity in certain countries – a consideration for further research and health policy. [6 7]. Similarly, emerging research includes systematic reviews and meta-analyses exploring multimorbidity in community settings, however, their study designs included fewer chronic conditions and were restricted to a specific geographic region [8 11]. A systematic review study incorporating longitudinal data from 1992 to 2017 concluded that the global pooled prevalence of multimorbidity in community settings was 33.1% [8], however no insights on changes in multimorbidity patterns changed as a function of time or number of conditions were provided.
These multimorbidity patterns were observed by Choudhry and colleagues whilst investigating the prevalence of multimorbidity across WHO geographic regions among adults between 2000 and 2021 [19]. They found that multimorbidity patterns by geographic regions, time, age, and gender suggested noticeable demographic and regional differences in burden of multimorbidity and that the global burden continues at the same pace. Moreover, the authors highlighted the need for effective, integrated interventions to reduce burden of morbidity for older adults in regions with high prevalence such as South America, Europe, and North America. The study also found a low prevalence in Africa suggesting the need for improved screening and diagnosis for chronic illness as underdiagnosis may be underlying these observed discrepancies.
Similarly, mixed findings regarding prevalence of multimorbidity and the most common comorbid diseases have been found in literature. A study by Tacken et al. [12] considering 3 categories of chronic diseases: diabetes, pulmonary and cardiovascular diseases, predicted that multimorbidity among patients over 65 years of age would be over 30%. Whereas, Sousa and colleagues [13] analysed the prevalence trends of multimorbidity among 15 European community-dwelling adults to find large variability in prevalence of multimorbidity in adults aged 50 and older between European countries. In terms of most prevalent co-occuring chronic diseases, systematic reviews on multimorbidity identified depression, hypertension, and diabetes as most prevalent [14 15]. On the other hand, Grain et al. identified cardiovascular and metabolic diseases as the most common diseases, followed by mental health disorders and musculoskeletal conditions [16]. Overall, the main three broad multimorbidity patterns identified by Wallace and co-authors in individuals aged 65 and older are: cardiovascular/metabolic disorders, anxiety/depression disorders, and pain/neuropsychiatric disorders [17 18].
Given the mixed literature in regard to multimorbidity trends, the primary aim of our study was to conduct a comprehensive meta-epidemiology to update the current status and identify trends of multimorbidity globally to address gaps in scientific knowledge and clinical practice, thereby, effectively contributing enhance care for multimorbidity populations. This study considers gender, age, ethnicities, and races as well as, reporting the prevalence of cardiometabolic diseases, musculoskeletal, respiratory, neurodegenerative disorders, and pharmacological treatments used — secondary aims of the study.
Methods
A systematic methodology was developed, peer reviewed and the protocol was published in PROSPERO (CRD42022347308). Data from studies that met the eligibility criteria were extracted.
Aim
This study aimed to report the differences in multimorbidity by gender, age, race, wealth, marital status, smoking, alcohol consumption, geographic location, and education level.
Eligibility criteria
Our search strategy included the use of multiple databases including PubMed, Web of Science, ScienceDirect, EMBASE, The Cochrane Gynaecology and Fertility Group Specialised Register of Controlled Trials and MEDLINE. The search terms used include multimorbidity, cardiometabolic disease, diabetes type I, diabetes type II, stroke, cardiovascular diseases, cardiomyopathy, heart arrhythmias, myocardial infarction, aortic disease, coronary artery disease, pericardial diseases, insulin, hormone replacement treatments and menopause. All studies peer reviewed and published in English and including women between the 30th of April 1980-30th of April 2022 were included. All studies included quantitative measures and designs such as randomised clinical trials, mixed-methods and epidemiology studies. Studies were excluded from the meta-analysis based on their inability to meet this predetermined criterion to ensure consistency and maintain studies with similar methodological rigor within analyses.
Data extraction and management
All participants included within the study experienced multimorbidity. A study specific extraction sheet was designed and employed to include interventions used, tools used and numerical results. The extraction template also included objectives, outcomes and demographics. Studies that included either a sub-analysis linked to a sub-study or an additional analysis were extracted separately if the study duration periods varied. The results of different stages were included as a new row to the data analysis. The extracted, final pooled data was reviewed by two investigators to ensure any disputes were discussed and agreed. The final analysis was reviewed by an independent reviewer prior to submission.
Outcomes
The outcomes included the prevalence of multimorbidity based on biological gender, geographical location and socio-demographical indicators such as ethnicity, smoking, alcohol consumption and economical status.
Statistical analysis plan
Throughout this study, meta-analysis of single proportion has been utilized to synthesize the overall prevalence of selected outcomes of interest. Additionally, a pairwise meta-analysis was used to combine the results of multiple studies containing common denominators and/or outcomes. We used rate and composition ratios to conduct a descriptive analysis of primary demographics and other sociological denominators. Differences were regarded as statistically significant if the p-value was less than 0.05. When the p-value was found to be less than 0.01, the difference was considered to have a higher level of significance. Conducting pairwise meta-analysis allowed us to summarize the overall effect size based on the differences between two interventions. Given that most outcomes of interest in the analysis were dichotomous, meta-analysis with binary data was conducted. Consequently, the pooled odds ratio (OR) with a 95% confidence interval (CI) was employed to assess the effects of the two interventions.
Statistical heterogeneity was evaluated by the commonly used measure with a p-value; if was greater than 50% and the associated p-value was less than 0.01, the dataset being analysed was determined to be heterogeneous. Conversely, an below 50% with a large p-value associated was determined to have weak heterogeneity.
Random effects model is used in meta-analysis when there exists heterogeneity among studies being analysed; instead, fixed effects model was employed if no heterogeneity existed. A statistical approach to dealing with heterogeneity is to stratify the dataset into subgroups based on relevant characteristics. When there exist more than 10 studies, a subgroup analysis was employed to help identify differences between subgroups and relationships that may be obscured by the heterogeneity in the overall dataset.
A chi-squared test would be used to determine if there is a significant difference between subgroups. If the test is significant, there may be publication bias, which means that studies with negative or non-significant results may be less likely to be published than those with positive results. The analysis was performed using R, involving the estimation of treatment effects, subgroup analyses and result presentation. Egger’s test was utilised to detect publication bias in meta-analysis. This is based on the regression of its accuracy on the size of the standardization effect and evaluates whether there is significant asymmetry in the funnel plot included in the studies.
Results
In total, 165 studies reported are associated with the presence of physical health conditions and physical multimorbidity. These multi-national studies offered potentially valuable insights into several hypotheses that may influence multimorbidity prevalence. After evaluating 165 systematically, we identified 84 studies to be eligible for inclusion in the meta-analysis (Table 1). The associations between marital status, gender, age group, race, wealth, region, smoking, drinking, living environment and multimorbidity were analysed. An increase in multimorbidity functioning was associated with being male, being younger, having a high level of education, wealth, marriage, alcohol, being Caucasian and living in rural areas. The most prevalent multimorbidity pattern was among people beyond 50 years of age with lower educational levels (OR = 1.57, 95% CI = 0.80 - 3.08).
Meta-analysis
Prevalence of Multimorbidity Cohort
We explored the prevalence of the multimorbidity cohort to assess the proportion of people with multimorbidity. Meta-analysis of single proportions was applied to 84 studies with a sample of 24,160,411 individuals, resulting in a prevalence of 33% (95% CI = [0.28, 0.38]). Figure 1 shows the forest plot for 84 studies. A high degree of heterogeneity with 100% of (p-value = 0) was seen indicating statistically significant heterogeneity.
To explore the sources of heterogeneity, a subgroup analysis was conducted based on the geographical locations of the studies and demonstrated in a forest plot (Figure 2). Of the 84 studies, 59 studies were from high-income countries (HICs) whereas, were 24 from middle-income countries (MICs). No significant subgroup difference (p-value=0.95 and of 100%) was identified between high-income countries and middle-income countries when considering approximately all age groups, as shown in Figure 2.
A moderate level of heterogeneity was seen across countries when exploring the association between age and multimorbidity. Figure 3 shows a statistically significant difference (p-value<0.05) identified between HICs and MICs when solely considering adults aged 50 and older, where the pooled prevalence was 36% (95% CI = [0.26, 0.49]) and 53% (95% CI = [0.44, 0.64]), respectively. Additionally, heterogeneity remained unchanged in HICs (, p-value = 0) and MICs (, p-value = 0), indicating that the identified heterogeneity was not influenced by geographical location (Figure 3). The value of X-squared was 4.24, indicating the differences between subgroups to be significant. Therefore, people over 50 in middle-income countries were found to be more likely to have multimorbidity than their counterparts in high-income countries.
Gender differences
A total of 34 studies with a sample size of 17,267,458 people reported differences in multimorbidity levels between females and males. The pooled odds ratio (OR) of multimorbidity between females and males was 1.32 (95% CI = [1.21, 1.43]), indicating that females were 0.32-times more likely to have multimorbidity in comparison to males. A high heterogeneity of 99% of (p-value < 0.01) was identified in Figure 4.
Rural-Urban differences
Of the sample, five studies included both, rural and urban populations. It is significant evidence of statistical heterogeneity (of =99%, p-value < 0.01). Figure 5 showed that the pooled OR of 0.8, but (95% CI = [0.60, 1.06]) included 1, which indicates no statistical significance. Based on systematic analyses, our findings indicate that people living in rural areas are 0.2 times less likely to have comorbidity in comparison to those living in urban areas.
Difference between smokers and non-smokers
Figure 6 depicts how eight studies conducted a large-scale survey covering 10 countries (n=619,862) to study the comorbidity responses to smoking versus not smoking. Significant evidence of statistical heterogeneity was found (of =99%, p-value < 0.01). The pooled OR of 1.00 (95% CI = [0.84, 1.19]), which is not statistically significant. Based on systematic analyses, our findings indicate that people were equally likely to have comorbidity whether they smoked or not.
Differences between black and white patients
The factor of ethnicity has been extensively discussed in numerous studies; for example, Caraballo et al[13] and King et al[137] discovered that multimorbidity was common and had been increasing in the United States due to temporal trends in ethnic disparities. By examining the roles of white and black ethnicities in multimorbidity and improving forest plot targeted systematic review, a meta-analysis was conducted with a total sample size of 554,733 people across 4 studies (ref. Figure 7). The pooled odds ratio (OR) was 0.53 (95% CI = [0.20, 1.41]), which is not statistically significant. Based on systematic analyses, our findings indicate that white people were 0.47 times less likely to develop comorbidities than black people. The associated = 99% (p-value < 0.01) shows that the sample has a high degree of heterogeneity.
Differences in educational status
A total of four studies with a sample size of 11,475 people reported differences in comorbidity levels between high school and university settings. The pooled odds ratio (OR) was 1.57 (95% CI = [0.80, 3.08]), which is not statistically significant. Based on systematic analyses, our findings indicate that people with a college education were 0.57 times more likely to develop comorbidities than those with only a high school education. Figure 10 indicates significant evidence of statistical heterogeneity ( = 92%, p-value <0.01).
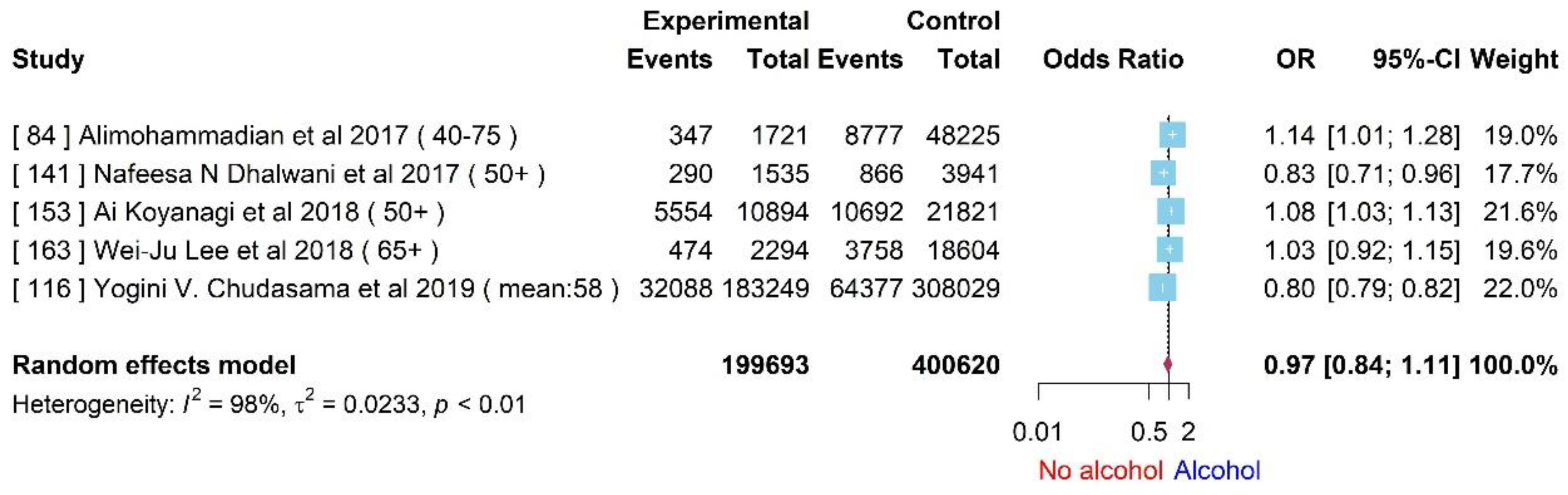
Difference among patients that consume alcohol
We conducted a meta-analysis of five studies with a sample size of 600,313 patients. A high heterogeneity was detected with = 98% and p-value < 0.01. The random effects model reported an odds ratio (OR) of 0.97 (95% CI = [0.84,1.11]), which is not statistically significant. Based on systematic analyses, our findings indicate that people who do not drink were less likely to develop comorbidities than those who drink.
Socioeconomical status
To assess if wealth is a helpful indicator of comorbidity, it is of great significance to study a sample size of 215,766 people across five studies; the results are shown in Figure 10. As indicated in the forest plot, the pooled odds ratio (OR) of multimorbidity between poor people and rich people was found to be 1.34 (95% CI = [0.86,2,07]), which is not statistically significant. Based on systematic analyses, our findings indicate that poor people are 0.34 times more likely to have multimorbidity in comparison to rich people. The value of 100% of (p-value < 0.01) indicates significant statistical heterogeneity.
Figure 9.
Forest plot for the association between multimorbidity and alcohol.
Difference between married and non-married
To explore the association between multimorbidity cohorts in married and non-married people, a meta-analysis was applied to four studies with a total sample size of 63,043 people. Our findings revealed that people see a substantial reduction in their risk of having comorbidities when they got married. Figure 11 showed that the pooled odds ratio (OR) of multimorbidity between married and non-married people was 0.94 (CI 95%=[0.52,1.68]), which is not statistically significant. Figure 11 indicates significant evidence of statistical heterogeneity ( =98%, p-value < 0.01). We observed that, on average, unmarried people were more likely to develop multimorbidity than people who got married.
Publication Bias
Given that results of studies that show statistically significant findings are more likely to be published than those that do not, the true effect size or relationship between variables can be distorted upon analysis. During gender-specific meta-analysis, females were more represented than males in the multimorbidity group. A high heterogeneity was quantified ( = 99%, ), suggesting that the studies included had substantial differences. We used statistical methods, such as funnel plots and Egger’s regression, to detect and correct for publication bias.
The funnel plot illustrated in Figure 12 demonstrated a clear indication of statistically evaluated minimal publication bias, as the distribution of the studies appeared asymmetric. However, the p-value of the Egger’s regression test (Figure 13) for the meta-analysis reporting multimorbidity with gender was 0.8196, indicating a lack of an effect size. As a result of this, significant publication bias cannot exist. These methods have less power if there are only a few studies in the meta-analysis, and they can be influenced by other sources of bias, such as heterogeneity in study quality or reporting biases.
Discussion
This study represents the first meta-epidemiology study to review papers published more than 42 years ago on the increasingly critical condition of multimorbidity. Multimorbidity is considered by WHO to have significant burden on the health of populations globally, with the sole exception of Africa wherein, the challenge of underdiagnosis plagues our understanding of true burden in patient populations.
Our study included 165 papers for systematic review and 84 papers within the meta-analysis out of a total 278 identified publications. Previous literature [12-18] identified a vast spectrum of medical conditions as the most prevalent co-occurring chronic diseases in people with multimorbidity. This spectrum includes depression, hypertension, diabetes, mental health disorders, cardiovascular and metabolic diseases, musculoskeletal conditions, and neuropsychiatric disorders. Despite these conditions being considered as the main broad multimorbidity patterns, limited insights on how multimorbidity patterns evolve over time or based on the number of conditions have been reported. In this study, we assessed the association between multimorbidity and numerous demographic factors including gender, age, ethnicity, geographical location. We also evaluated lifestyle factors such as smoking and alcohol consumption as well as economic indicators including wealth, marriage status, and education level to report comprehensive findings. In doing so, we were able to holistically evaluate the relationships between various social determinants of health and multimorbidity and report effect sizes found via meta-analysis.
In exploring gender and multimorbidity, our results aligned with findings by Zielinski & colleagues, and multimorbidity was found to be highly prevalent among women of all ages which is contrary to the common perception that it is confined to geriatric populations [19]. It is possible these findings are attributable to more realistic reporting as women tend to share more information with healthcare facilities, in comparison to their male counterparts. On the other hand, exposure to common risk factors among women could also be a driving factor for the elevated prevalence of multimorbidity.
Given the significant rise in life expectancy and declining fertility rates, the increase in older populations globally is expected with 1 in 6 people predicted to be over 65 years by 2050 [20]. Countries such as India and China are experiencing major transitions leading to a significant increase in the proportion of older populations, rise in associated medical and biopsychosocial needs and thus, elevated prevalence of multimorbidity.
Similarly to gender and age, ethnicity is one the factors that has been extensively investigated in association with multimorbidity over the last 40 years. Our study found that white people were 0.47 times less likely to develop comorbidities compared to black people. Interestingly, a recent study by Kuan and co-authors [xx] examined multimorbidity patterns stratified by ethnicity and other factors such as race, sex, and age for 308 health conditions (n= 872,451; eligible patients). Their study reported that white individuals (78.7% of 2,666,234) were more likely to be diagnosed with two or more conditions than were black (60.1% of 98,815) or south Asian individuals (60.2% of 155,435). Additionally, they identified that spinal fractures were most strongly non-randomly associated with malignancy in black individuals, but with osteoporosis in white individuals. It was reported that multimorbidity had been increasing in the United Stated due to temporal trends in ethnic disparities [13,137].Taking our findings in conjunction with findings of Kuan et. al regarding differential diagnosis of spinal fractures, highlights the dire need for improved understanding and management of multimorbidity across ethnic groups.
To manage multimorbidity patients, it is also vital to ensure local healthcare systems understand the differences between the rural and urban comorbidities. This is crucial as multimorbidity is also a strong predictor of mortality, disability and poor quality of life [21]. Our findings reported rural populations to be 0.8 times less likely to face multimorbidity in comparison to those in urban areas. From an economic perspective, having knowledge of the difference in prevalence and type of comorbidities found by region may inform improved resource and expenditure allocation in healthcare system. From a clinical perspective, these findings and further research can be a step towards personalized healthcare by improving patient-physician interaction as physicians would be more aware of regional differences in comorbidity to prescrible polypharmacy use or self-management, accordingly.
Lifestyle factors such as smoking and alcohol consumption that are known to have a negative causal impact on health were also evaluated in relation to multimorbidity. There is significant evidence that smoking negatively impacts individual health and worsens comorbidities such as hypertension, cardiac conditions and diabetes [22]. Though our results indicated that women may have had comorbidities regardless of their smoking status, a study conducted by Newson and colleagues indicated smoking cessation in a Canadian cohort reporting the need for behavioural change following cancer, diabetes, cardiac disease and stroke [23].
Similarly, there is sufficient evidence of excessive alcoholic consumption and an increased risk of health issues such as unintentional injuries, depression, brain disorders, violence, liver diseases, cancer as well as reduced health-related quality of life; elevating the likelihood of multimorbidity and mortality. Our results identified that people who do not drink were less likely to develop comorbidities than those who do. A national survey in the United States [25] on Drug Use and Health from 2005 to 2014 examining excessive alcohol consumption and lifetime medical conditions (13 medical conditions and medical multimorbidity of at least 2 diseases) among adults over 50 years old who were either binge drinkers or non-binge drinkers found that multimorbidity was lower among binge drinkers compared to non-binge drinkers; causing significant health risks especially with the concurrent use of other substances.
Provided that socio-economic indicators such as education levels, wealth, and marriage impact access to resources and health outcomes, it is imperative they be assessed in relation to multimorbidity.
Pathirana and colleagues [27] reported, from a review of 24 cross-sectional studies, that low versus high education level and deprivation were consistently associated with increased of risk of multimorbidity, whereas the evidence on association with family income was inconclusive (or mixed). A German cross-sectional study including 19,294 adults with a total of 17 self-reported health conditions along with sociodemographic characteristics [28] indicated that adults aged 40-49 years with lower levels of education were more likely to suffer multimorbidity with a prevalence of 47.4% matching those of highly educated individuals. Our findings indicated that people with higher education level were 0.57 times more likely to develop comorbidities than those with a low level of education.
In regard to the correlation between wealth and multimorbidity, our results indicate no significant difference between high-income countries (n=59) and middle-income countries (n=24) when all age groups were considered, however people over 50 years in middle-income countries were more likely to have multimorbidity compared to high-income countries. In light of such findings, it is key that emphasis in the development of national public health approaches and prevention programs on multimorbidity is placed on supporting adults over the age of 50 especially, in middle income countries as well as individuals with lower levels of education. It is key to note the limitations that underdiagnosis or underreporting in certain countries may place on findings of economic indicators and reported multimorbidities.
On the other hand, we found that prevalence of marriage was inversely associated with multimorbidity and people showed a substantial reduction in risk of having comorbidities when they got married. These findings align with existing evidence that married individuals have better health-related quality of life and wellbeing compared to their unmarried counterparts. A study by Wang and team [29] was conducted using a nationally representative data on 23641 adults aged 50-60 years who participated in four longitudinal studies in the US, UK, Europe, and China. The study reported that individuals who had been married for 21-30 years had a lower multimorbidity rate than those married for less than 10 years. These associations remained robust after adjusting for socioeconomic and lifestyle factors. Though the association of marriage and multimorbidity has not been investigated across all age groups, these results are mainly due to influence of marital partners on reinforcing healthy behaviours and discouraging habits such as smoking and drinking, for example. These findings highlight the protective role that marital relationships may play against multimorbidity by preserving overall health and wellbeing across the life course.
Conclusion
Our findings regarding multimorbidity and its association with demographic, lifestyle and economic factors can support development of evidence-based policies and inform cultural or regional adaptions of clinical management such as polypharmacy to optimise therapeutic benefit for patients with multimorbidity. Some key considerations for clinical management from our findings include identifying women, black people, and unmarried individuals who are drinkers at high risk of multimorbidity. Additionally, the finding that marital status may render protective effects against multimorbidity by encouragement of healthier behaviours alludes to the role socially focused interventions may have in negatively reinforcing lifestyle factors that increase risk of multimorbidity in populations. High prevalence of multimorbidity places significant burden on healthcare systems as well as the global population thus, it is imperative that robust research and healthcare policy be implemented for optimal multimorbidity management. Lastly, earlier stage interventions such as prevention programs to reduce risk of multimorbidity in at-risk populations may support decreased the incidence of cases.
Author Contributions
GD developed the FEINMAN project as part of the ELEMI program. The statistical analysis was developed by GD and JQS. The analysis was performed by GD, GL, XY and JQS. GD and YB wrote the initial draft of the manuscript. All authors read and approved the final manuscript.
Data Availability Statement
All data used within this study has been publicly available. The authors will consider sharing the dataset gathered upon request.
Acknowledgements
The authors acknowledge support from Southern Health NHS Foundation Trust, Southern University of Science and Technology and University of Southampton.
Conflicts of Interest
PP has received research grant from Novo Nordisk, and other, educational from Queen Mary University of London, other from John Wiley & Sons, other from Otsuka, outside the submitted work. SR reports other from Janssen, Lundbeck and Otsuka outside the submitted work. All other authors report no conflict of interest. The views expressed are those of the authors and not necessarily those of the NHS, the National Institute for Health Research, the Department of Health and Social Care or the Academic institutions.
Consent for publication
All authors consented to publish this manuscript. All authors critically appraised and commented on previous versions of the manuscript.
References
- Murray CJL, Barber RM, Foreman KJ, et al. Global, regional, and national disability-adjusted life years (DALYs) for 306 diseases and injuries and healthy life expectancy (HALE) for 188 countries, 1990-2013: quantifying the epidemiological transition. Lancet. 2015, 386, 2145–2191. [Google Scholar] [CrossRef] [PubMed]
- Le Reste JY, Nabbe P, Manceau B, et al. The European general practice research network presents a comprehensive definition of multimorbidity in family medicine and long term care, following a systematic review of relevant literature. J Am Med Dir Assoc. 2013, 14, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Link BG, Phelan J. Social Conditions As Fundamental Causes of Disease. Journal of Health and Social Behavior.
- Sum, G.; Hone, T.; Atun, R.; Millett, C.; Suhrcke, M.; Mahal, A.; Koh, G.C.-H.; Lee, J.T. Multimorbidity and out-of-pocket expenditure on medicines: A systematic review. BMJ Glob. Health 2018, 3, e000505. [Google Scholar]
- Makovski, T.T.; Schmitz, S.; Zeegers, M.P.; Stranges, S.; van den Akker, M. Multimorbidity and quality of life: Systematic literature review and meta-analysis. Ageing Res. Rev. 2019, 53, 100903. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, Q.D.; Wu, C.; Odden, M.C.; Kim, D.H. Multimorbidity Patterns, Frailty, and Survival in Community-Dwelling Older Adults. J. Gerontol. A Biol. Sci. Med. Sci. 2019, 74, 1265–1270. [Google Scholar] [CrossRef] [PubMed]
- Lai FTT, Guthrie B, Wong SY, et al. Sex-specific intergenerational trends in morbidity burden and multimorbidity status in Hong Kong community: an age-period-cohort analysis of repeated population pen. 2019. [CrossRef]
- Uijen A, van de Lisdonk E. Multimorbidity in primary care: prevalence and trend over the last 20 years. Eur J Gen Pract. 2008, 14, 28–32. [Google Scholar] [CrossRef]
- Nguyen H, Manolova G, Daskalopoulou C, Vitoratou S, Prince M, Prina AM. Prevalence of multimorbidity in community settings: a systematic review and meta-analysis of observational studies.
- J Comorb. 2019;9:2235042X1987093. [CrossRef]
- Fortin M, Stewart M, Poitras ME, Almirall J, Maddocks H. A systematic review of prevalence studies on multimorbidity: toward a more uniform methodology. Ann Fam Med. 2012, 10, 142–151. [Google Scholar] [CrossRef]
- Violan C, Foguet-Boreu Q, Flores-Mateo G, et al. Prevalence, determinants and patterns of multimorbidity in primary care: a systematic review of observational studies. PLoS One. 2014, 9, e102149. [Google Scholar] [CrossRef]
- Tacken MAJB, Opstelten W, Vossen I, et al. Increased multimorbidity in patients in general practice in the period 2003–2009. Ned Tijdschr Geneeskd. 2011, 155, A3109. [Google Scholar]
- Souza, D.L.B. , Oliveras-Fabregas, A., Minobes-Molina, E. et al. Trends of multimorbidity in 15 European countries: a population-based study in community-dwelling adults aged 50 and over. BMC Public Health 21, 76 (2021). [CrossRef]
- Zhang X, Padhi A, Wei T, et al. Community prevalence and dyad disease pattern of multimorbidity in China and India: a systematic review. BMJ Glob Health. 2022, 7, e008880. [Google Scholar] [CrossRef]
- Prados-Torres A, Calderón-Larrañaga A, Hancco-Saavedra J, Poblador-Plou B, van den Akker M. Multimorbidity patterns: a systematic review. J Clin Epidemiol. 2014, 67, 254–266 https://doi org/101016/jjclinepi201309021. [Google Scholar] [CrossRef] [PubMed]
- Garin N, Koyanagi A, Chatterji S, et al. Global multimorbidity patterns: a cross-sectional, population-based, multi-country study. J Gerontol A Biol Sci Med Sci. 2016, 71, 205–214. [Google Scholar] [CrossRef] [PubMed]
- Wallace E, Salisbury C, Guthrie B, Lewis C, Fahey T, Smith SM. Managing patients with multimorbidity in primary care. BMJ. [CrossRef]
- Chowdhury SR, Chandra Das D, Sunna TC, Beyene J, Hossain A. Global and regional prevalence of multimorbidity in the adult population in community settings: a systematic review and meta-analysis. EClinicalMedicine. 1018. [CrossRef]
- Zielinski A , Halling A . Association between age, gender and multimorbidity level and receiving home health care: a population-based Swedish study. BMC Res Notes.
- United Nations and Department of Economic and Social Affairs, World population ageing, 2019 highlights, NewYork, 2020.
- Gu J, Chao J, Chen W, et al. Multimorbidity and health-related quality of life among the community-dwelling elderly: a longitudinal study. Arch Gerontol Geriatr 2018, 74, 133–140. [Google Scholar] [CrossRef]
- Shahoumian TA, Phillips BR, Backus LI. Cigarette smoking, reduction and quit attempts: prevalence among veterans with coronary heart disease. Prev Chronic Dis 2016, 13, E41. [Google Scholar]
- Newson JT, Huguet N, Ramage-Morin PL, et al. Health behaviour changes after diagnosis of chronic illness among Canadians aged 50 or older. Health Rep 2012, 23, 49. [Google Scholar]
- Fu Y, Chen M, Si L. Multimorbidity and catastrophic health expenditure among patients with diabetes in China: a nationwide population-based study. BMJ Glob Health. 2022, 7, e007714. [Google Scholar] [CrossRef] [PubMed]
- 26. Han BH, Moore AA, Sherman SE, Palamar JJ. Prevalence and correlates of binge drinking among older adults with multimorbidity. Drug Alcohol Depend. [CrossRef]
- Afshar, S. , Roderick, P.J., Kowal, P. et al. Multimorbidity and the inequalities of global ageing: a cross-sectional study of 28 countries using the World Health Surveys. BMC Public Health 2015, 15, 776. [Google Scholar] [CrossRef] [PubMed]
- Pathirana TI, Jackson CA. Socioeconomic status and multimorbidity: a systematic review and meta-analysis. Aust N Z J Public Health. 2018, 42, 186–194. [Google Scholar] [CrossRef] [PubMed]
- Puth MT, Weckbecker K, Schmid M, Münster E. Prevalence of multimorbidity in Germany: impact of age and educational level in a cross-sectional study on 19,294 adults. BMC Public Health. 2017, 17, 826. [Google Scholar] [CrossRef]
- Wang D, Li D, Mishra SR, Lim C, Dai X, Chen S, Xu X. Association between marital relationship and multimorbidity in middle-aged adults: a longitudinal study across the US, UK, Europe, and China. Maturitas. 2022, 155, 32–39. [Google Scholar] [CrossRef] [PubMed]
- K. N. Anushree, Prem Shankar Mishra,Prevalence of multi-morbidities among older adults in India: Evidence from national Sample Survey organization, 2017–2018, Clinical Epidemiology and Global Health, 2022, 15, 101025, ISSN 2213–3984. [CrossRef]
- Arias-de la Torre J, Vilagut G, Ronaldson A, Serrano-Blanco A, Martín V, Peters M, Valderas JM, Dregan A, Alonso J. Prevalence and variability of current depressive disorder in 27 European countries: a population-based study. Lancet Public Health. 2021, 6, e729–e738. [Google Scholar] [CrossRef] [PubMed]
- Waterhouse P, van der Wielen N, Banda PC, Channon AA. The impact of multi-morbidity on disability among older adults in South Africa: do hypertension and socio-demographic characteristics matter? Int J Equity Health. 2017, 16, 62, PMID: 28388911; PMCID: PMC5385014. [CrossRef]
- Banjare P, Pradhan J. Socio-economic inequalities in the prevalence of multi-morbidity among the rural elderly in Bargarh District of Odisha (India). PLoS One. 2014, 9, e97832, PMID: 24902041; PMCID: PMC4046974. [Google Scholar] [CrossRef]
- Bennett, H. Q. , Kingston, A., Lourida, I., Robinson, L., Corner, L., Brayne, C. E.,... & Jagger, C. The contribution of multiple long-term conditions to widening inequalities in disability-free life expectancy over two decades: Longitudinal analysis of two cohorts using the Cognitive Function and Ageing Studies. EClinicalMedicine, 2021, 39.
- Wolff JL, Starfield B, Anderson G. Prevalence, expenditures, and complications of multiple chronic conditions in the elderly. Arch Intern Med. 2002, 162, 2269–2276. [Google Scholar] [CrossRef] [PubMed]
- Bernardes, G. M. , Saulo, H., Santos, J. L. F., da Cruz Teixeira, D. S., de Oliveira Duarte, Y. A., & de Andrade, F. B. Effect of education and multimorbidity on mortality among older adults: findings from the health, well-being and ageing cohort study (SABE). Public Health 2021, 201, 69–74. [Google Scholar]
- Bisquera A, Gulliford M, Dodhia H, Ledwaba-Chapman L, Durbaba S, Soley-Bori M, Fox-Rushby J, Ashworth M, Wang Y. Identifying longitudinal clusters of multimorbidity in an urban setting: A population-based cross-sectional study. Lancet Reg Health Eur. 1000; PMID: 34557797; PMCID: PMC8454750. [CrossRef]
- Bustos-Vázquez, E. , Fernández-Niño, J. A., & Astudillo-Garcia, C. I. Self-rated health, multimorbidity and depression in Mexican older adults: Proposal and evaluation of a simple conceptual model. Biomedica 2017, 37, 92–103. [Google Scholar]
- Butterworth, J. E. , Hays, R., McDonagh, S. T., Bower, P., Pitchforth, E., Richards, S. H., & Campbell, J. L. Involving older people with multimorbidity in decision-making about their primary healthcare: a Cochrane systematic review of interventions (abridged). Patient Education and Counseling, 2020, 103, 2078–2094. [Google Scholar]
- Caraballo, C. , Herrin, J., Mahajan, S., Massey, D., Lu, Y., Ndumele, C. D.,... & Krumholz, H. M. Temporal trends in racial and ethnic disparities in multimorbidity prevalence in the United States, 1999-2018. The American Journal of Medicine, 2022, 135, 1083–1092. [Google Scholar]
- Carrilero, N. , Dalmau-Bueno, A., & García-Altés, A. (2020). Comorbidity patterns and socioeconomic inequalities in children under 15 with medical complexity: a population-based study. BMC pediatrics, 20, 1-10.
- Charlton, J. , Rudisill, C., Bhattarai, N., & Gulliford, M. Impact of deprivation on occurrence, outcomes and health care costs of people with multiple morbidity. Journal of health services research & policy, 2013, 18, 215–223. [Google Scholar]
- Chauhan, S. , Srivastava, S., Kumar, P., & Patel, R. Decomposing urban-rural differences in multimorbidity among older adults in India: a study based on LASI data. BMC Public Health, 2022, 22, 502. [Google Scholar]
- Chung, G. K. K. , Chan, S. M., Chan, Y. H., Yip, T. C. F., Ma, H. M., Wong, G. L. H.,... & Woo, J. Differential impacts of multimorbidity on COVID-19 severity across the socioeconomic ladder in Hong Kong: a syndemic perspective. International journal of environmental research and public health, 2021, 18, 8168. [Google Scholar] [PubMed]
- Cooper SA, McLean G, Guthrie B, McConnachie A, Mercer S, Sullivan F, Morrison J. Multiple physical and mental health comorbidity in adults with intellectual disabilities: population-based cross-sectional analysis. BMC Fam Pract. PMID: 26310664; PMCID: PMC4551707. [CrossRef]
- Corrao G, Rea F, Carle F, Di Martino M, De Palma R, Francesconi P, Lepore V, Merlino L, Scondotto S, Garau D, Spazzafumo L, Montagano G, Clagnan E, Martini N; working group “Monitoring and assessing care pathways (MAP)” of the Italian Ministry of Health. Measuring multimorbidity inequality across Italy through the multisource comorbidity score: a nationwide study. Eur J Public Health. 2020, 30, 916–921. [Google Scholar] [CrossRef] [PubMed]
- Costa, Â. K. , Bertoldi, A. D., Fontanella, A. T., Ramos, L. R., Arrais, P. S. D., Luiza, V. L.,... & Nunes, B. P. Does socioeconomic inequality occur in the multimorbidity among Brazilian adults? Revista de Saúde Pública, 2020, 54, 138. [Google Scholar] [PubMed]
- Araujo, M. E. A. , Silva, M. T., Galvao, T. F., Nunes, B. P., & Pereira, M. G. Prevalence and patterns of multimorbidity in Amazon Region of Brazil and associated determinants: a cross-sectional study. BMJ open, 2018, 8, e023398. [Google Scholar]
- Diderichsen, F. , Bender, A. M., Lyth, A. C., Andersen, I., Pedersen, J., & Bjørner, J. B. Mediating role of multimorbidity in inequality in mortality: a register study on the Danish population. J Epidemiol Community Health, 2022, 76, 466–470. [Google Scholar]
- González-Chica, D. A. , Hill, C. L., Gill, T. K., Hay, P., Haag, D., & Stocks, N. Individual diseases or clustering of health conditions? Association between multiple chronic diseases and health-related quality of life in adults. Health and quality of life outcomes, 2017, 15, 1–9. [Google Scholar]
- Guimarães, R. M. , & Andrade, F. C. D. Healthy life-expectancy and multimorbidity among older adults: Do inequality and poverty matter? Archives of Gerontology and Geriatrics 2020, 90, 104157. [Google Scholar] [PubMed]
- Halonen, P. , Raitanen, J., Jämsen, E., Enroth, L., & Jylhä, M. Chronic conditions and multimorbidity in population aged 90 years and over: associations with mortality and long-term care admission. Age and Ageing, 2019, 48, 564–570. [Google Scholar]
- Hamiduzzaman, M. , Torres, S., Fletcher, A., Islam, M. R., Siddiquee, N. A., & Greenhill, J. Aging, care and dependency in multimorbidity: how do relationships affect older Bangladeshi women’s use of homecare and health services? Journal of Women & Aging, 2022, 34, 731–744. [Google Scholar]
- Alshamsan, R. , Lee, J. T., Rana, S., Areabi, H., & Millett, C. Comparative health system performance in six middle-income countries: cross-sectional analysis using World Health Organization study of global ageing and health. Journal of the Royal Society of Medicine, 2017, 110, 365–375. [Google Scholar] [PubMed]
- Kuan, V. , Denaxas, S., Patalay, P., Nitsch, D., Mathur, R., Gonzalez-Izquierdo, A.,... & Zwierzyna, M. Identifying and visualising multimorbidity and comorbidity patterns in patients in the English National Health Service: a population-based study. The Lancet Digital Health, 2023, 5, e16–e27. [Google Scholar] [PubMed]
- Siddiqi, N. , Doran, T., Prady, S. L., & Taylor, J. Closing the mortality gap for severe mental illness: are we going in the right direction? The British Journal of Psychiatry, 2017, 211, 130–131. [Google Scholar] [PubMed]
- Drake, R. E. , Essock, S. M., Shaner, A., Carey, K. B., Minkoff, K., Kola, L.,... & Rickards, L. Implementing dual diagnosis services for clients with severe mental illness. Psychiatric services, 2001, 52, 469–476. [Google Scholar]
- Barron, E. , Bakhai, C., Kar, P., Weaver, A., Bradley, D., Ismail, H.,... & Valabhji, J. Associations of type 1 and type 2 diabetes with COVID-19-related mortality in England: a whole-population study. The lancet Diabetes & endocrinology, 2020, 8, 813–822. [Google Scholar]
- Ronaldson, A. , de la Torre, J. A., Prina, M., Armstrong, D., Das-Munshi, J., Hatch, S.,... & Dregan, A. Associations between physical multimorbidity patterns and common mental health disorders in middle-aged adults: A prospective analysis using data from the UK Biobank. The Lancet Regional Health–Europe,.
- Steed, L. , Lankester, J., Barnard, M., Earle, K., Hurel, S., & Newman, S. Evaluation of the UCL diabetes self-management programme (UCL-DSMP): a randomized controlled trial. Journal of health psychology, 2005, 10, 261–276. [Google Scholar]
- Divo, M. J. , Casanova, C., Marin, J. M., Pinto-Plata, V. M., De-Torres, J. P., Zulueta, J. J.,... & Celli, B. R. COPD comorbidities network. European Respiratory Journal, 2015, 46, 640–650. [Google Scholar]
- Wijlaars LPMM, Hardelid P, Guttmann A, Gilbert R. Emergency admissions and long-term conditions during transition from paediatric to adult care: a cross-sectional study using Hospital Episode Statistics data. BMJ Open. 2018, 8, e021015. [Google Scholar] [CrossRef]
- Head, A. , Fleming, K., Kypridemos, C., Pearson-Stuttard, J., & O’Flaherty, M. Multimorbidity: the case for prevention. J Epidemiol Community Health, 2021, 75, 242–244. [Google Scholar] [PubMed]
- Head, A. , Fleming, K., Kypridemos, C., Schofield, P., Pearson-Stuttard, J., & O'Flaherty, M. Inequalities in incident and prevalent multimorbidity in England, 2004–2019: a population-based, descriptive study. The Lancet Healthy Longevity, 2021, 2, e489–e497. [Google Scholar]
- Hussain, M. A. , Huxley, R. R., & Al Mamun, A. Multimorbidity prevalence and pattern in Indonesian adults: an exploratory study using national survey data. BMJ open, 2015, 5, e009810. [Google Scholar]
- Agborsangaya, C.B. , Lau, D., Lahtinen, M. et al. Multimorbidity prevalence and patterns across socioeconomic determinants: a cross-sectional survey. BMC Public Health 12, 201 (2012). [CrossRef]
- Jackson CA, Jones M, Tooth L, Mishra GD, Byles J, Dobson A. Multimorbidity patterns are differentially associated with functional ability and decline in a longitudinal cohort of older women. Age Ageing. 2015, 44, 810–816. [Google Scholar] [CrossRef] [PubMed]
- Jantsch, A. G. , Alves, R. F. S., & Faerstein, E. Educational inequality in Rio de Janeiro and its impact on multimorbidity: evidence from the Pró-Saúde study. A cross-sectional analysis. Sao Paulo Medical Journal, 2018, 136, 51–58. [Google Scholar]
- Jerliu, N. , Toçi, E., Burazeri, G., Ramadani, N., & Brand, H. Prevalence and socioeconomic correlates of chronic morbidity among elderly people in Kosovo: a population-based survey. BMC geriatrics, 2013, 13, 1–9. [Google Scholar]
- Johnston, M. C. , Crilly, M., Black, C., Prescott, G. J., & Mercer, S. W. Defining and measuring multimorbidity: a systematic review of systematic reviews. European journal of public health, 2019, 29, 182–189. [Google Scholar]
- McQueenie, R. , Foster, H. M., Jani, B. D., Katikireddi, S. V., Sattar, N., Pell, J. P.,... & Nicholl, B. I. Multimorbidity, polypharmacy, and COVID-19 infection within the UK Biobank cohort. PloS one, 2020, 15, e0238091. [Google Scholar]
- Keller, T. , Hohmann, C., Standl, M., Wijga, A. H., Gehring, U., Melén, E.,... & Roll, S. The sex-shift in single disease and multimorbid asthma and rhinitis during puberty-a study by MeDALL. Allergy, 2018, 73, 602–614. [Google Scholar]
- Khanolkar, A. R. , Chaturvedi, N., Kuan, V., Davis, D., Hughes, A., Richards, M.,... & Patalay, P. Socioeconomic inequalities in prevalence and development of multimorbidity across adulthood: a longitudinal analysis of the MRC 1946 national survey of health and development in the UK. PLoS medicine, 2021, 18, e1003775. [Google Scholar]
- Knies, G. , & Kumari, M. Multimorbidity is associated with the income, education, employment and health domains of area-level deprivation in adult residents in the UK. Scientific Reports, 2022, 12, 7280. [Google Scholar]
- Kunna, R. , San Sebastian, M., & Stewart Williams, J. Measurement and decomposition of socioeconomic inequality in single and multimorbidity in older adults in China and Ghana: results from the WHO study on global AGEing and adult health (SAGE). International journal for equity in health, 2017, 16, 1–17. [Google Scholar]
- Kuo, R. N. , & Lai, M. S. The influence of socio-economic status and multimorbidity patterns on healthcare costs: a six-year follow-up under a universal healthcare system. International journal for equity in health, 2013, 12, 1–11. [Google Scholar]
- Mondor, L. , Maxwell, C. J., Hogan, D. B., Bronskill, S. E., Gruneir, A., Lane, N. E., & Wodchis, W. P. Multimorbidity and healthcare utilization among home care clients with dementia in Ontario, Canada: a retrospective analysis of a population-based cohort. PLoS medicine, 2017, 14, e1002249. [Google Scholar]
- Lawson, K. D. , Mercer, S. W., Wyke, S., Grieve, E., Guthrie, B., Watt, G., & Fenwick, E. A. Double trouble: the impact of multimorbidity and deprivation on preference-weighted health related quality of life a cross sectional analysis of the Scottish Health Survey. International journal for equity in health, 2013, 12, 1–9. [Google Scholar]
- Lu, J. , Wang, Y., Hou, L., Zuo, Z., Zhang, N., & Wei, A. Multimorbidity patterns in old adults and their associated multi-layered factors: a cross-sectional study. BMC geriatrics, 2021, 21, 372. [Google Scholar]
- McQueenie, R. , Foster, H. M., Jani, B. D., Katikireddi, S. V., Sattar, N., Pell, J. P.,... & Nicholl, B. I. Multimorbidity, polypharmacy, and COVID-19 infection within the UK Biobank cohort. PloS one, 2020, 15, e0238091. [Google Scholar]
- Johnston, M. C. , Crilly, M., Black, C., Prescott, G. J., & Mercer, S. W. Defining and measuring multimorbidity: a systematic review of systematic reviews. European journal of public health, 2019, 29, 182–189. [Google Scholar]
- Mondor, L. , Cohen, D., Khan, A. I., & Wodchis, W. P. Income inequalities in multimorbidity prevalence in Ontario, Canada: a decomposition analysis of linked survey and health administrative data. International journal for equity in health, 2018, 17, 1–13. [Google Scholar]
- Niksic, M. , Redondo-Sanchez, D., Chang, Y. L., Rodriguez-Barranco, M., Exposito-Hernandez, J., Marcos-Gragera, R.,... & Luque-Fernandez, M. A. The role of multimorbidity in short-term mortality of lung cancer patients in Spain: a population-based cohort study. BMC cancer, 2021, 21, 1–12. [Google Scholar]
- Nunes, B. P. , Flores, T. R., Mielke, G. I., Thumé, E., & Facchini, L. A. Multimorbidity and mortality in older adults: a systematic review and meta-analysis. Archives of gerontology and geriatrics, 2016, 67, 130–138. [Google Scholar]
- Zhao, J. , Chhetri, J. K., Chang, Y., Zheng, Z., Ma, L., & Chan, P. Intrinsic capacity vs. multimorbidity: a function-centered construct predicts disability better than a disease-based approach in a community-dwelling older population cohort. Frontiers in medicine, 2021, 8, 753295. [Google Scholar] [PubMed]
- Orueta, J. F. , Nuño-Solinís, R., García-Alvarez, A., & Alonso-Morán, E. Prevalence of multimorbidity according to the deprivation level among the elderly in the Basque Country. BMC Public Health, 2013, 13, 1–11. [Google Scholar]
- Sun, J. J. , Perera, B., Henley, W., Angus-Leppan, H., Sawhney, I., Watkins, L.,... & Shankar, R. Epilepsy related multimorbidity, polypharmacy and risks in adults with intellectual disabilities: a national study. Journal of Neurology, 2022, 269, 2750–2760. [Google Scholar] [PubMed]
- Lee, S. I. , Azcoaga-Lorenzo, A., Agrawal, U., Kennedy, J. I., Fagbamigbe, A. F., Hope, H.,... & McCowan, C. Epidemiology of pre-existing multimorbidity in pregnant women in the UK in 2018: a population-based cross-sectional study. BMC pregnancy and childbirth, 2022, 22, 1–15. [Google Scholar]
- Reis-Santos, B. , Gomes, T. , Macedo, L. R., Horta, B. L., Riley, L. W., & Maciel, E. L. Prevalence and patterns of multimorbidity among tuberculosis patients in Brazil: a cross-sectional study. International journal for equity in health, 2013, 12, 1–8. [Google Scholar]
- ROMANA, G. Q. , KISLAYA, I., SALVADOR, M. R., GONÇALVES, S. C., NUNES, B., & DIAS, C. Multimorbidity in Portugal: Results from The First National Health Examination Survey Multimorbilidade em Portugal: Dados do Primeiro Inquérito Nacional de Saúde com Exame Físico.
- Ryan, B. L. , Bray Jenkyn, K., Shariff, S. Z., Allen, B., Glazier, R. H., Zwarenstein, M.,... & Stewart, M. Beyond the grey tsunami: a cross-sectional population-based study of multimorbidity in Ontario. Canadian Journal of Public Health, 2018, 109, 845–854. [Google Scholar]
- Singer, L. , Green, M., Rowe, F., Ben-Shlomo, Y., & Morrissey, K. Social determinants of multimorbidity and multiple functional limitations among the ageing population of England, 2019, 2002–2015. SSM-population health, 8, 100413.
- Singh-Manoux, A. , Fayosse, A., Sabia, S., Tabak, A., Shipley, M., Dugravot, A., & Kivimäki, M. Clinical, socioeconomic, and behavioural factors at age 50 years and risk of cardiometabolic multimorbidity and mortality: a cohort study. PLoS medicine, 2018, 15, e1002571. [Google Scholar]
- Smith, D. J. , McLean, G., Martin, D., Martin, J. L., Guthrie, B., Gunn, J., & Mercer, S. W. Depression and multimorbidity: a cross-sectional study of 1,751,841 patients in primary care. The Journal of clinical psychiatry, 2014, 75, 4205. [Google Scholar]
- Smith, M. J. , Belot, A. , Quartagno, M., Luque Fernandez, M. A., Bonaventure, A., Gachau, S.,... & Njagi, E. N. Excess mortality by multimorbidity, socioeconomic, and healthcare factors, amongst patients diagnosed with diffuse large B-cell or follicular lymphoma in England. Cancers, 2021, 13, 5805. [Google Scholar] [PubMed]
- Van Zon, S. K. , Reijneveld, S. A., Galaurchi, A., Mendes de Leon, C. F., Almansa, J., & Bültmann, U. Multimorbidity and the transition out of full-time paid employment: a longitudinal analysis of the health and retirement study. The Journals of Gerontology: Series B, 2020, 75, 705–715. [Google Scholar]
- Vasiliadis, H. M. , Gontijo Guerra, S., Berbiche, D., & Pitrou, I. E. (2021). The factors associated with 3-year mortality stratified by physical and mental multimorbidity and area of residence deprivation in primary care community-living older adults. Journal of Aging and Health, 33(7-8), 545-556.
- Violan, C. , Foguet-Boreu, Q., Flores-Mateo, G., Salisbury, C., Blom, J., Freitag, M.,... & Valderas, J. M. Prevalence, determinants and patterns of multimorbidity in primary care: a systematic review of observational studies. PloS one, 2014, 9, e102149. [Google Scholar]
- Lu, H. , Xu, X., Hu, J., Zhao, Z., Si, Z., Wang, X.,... & Li, X. (2023). Association between exposure to Occupational hazard factors and multimorbidity in steelworkers: A Cross-Sectional Study.
- Zhao, Y. , Atun, R., Oldenburg, B., McPake, B., Tang, S., Mercer, S. W.,... & Lee, J. T. Physical multimorbidity, health service use, and catastrophic health expenditure by socioeconomic groups in China: an analysis of population-based panel data. The Lancet Global Health, 2020, 8, e840–e849. [Google Scholar]
- Wang, H. H. , Wang, J. J., Lawson, K. D., Wong, S. Y., Wong, M. C., Li, F. J.,... & Mercer, S. W. Relationships of multimorbidity and income with hospital admissions in 3 health care systems. The Annals of Family Medicine, 2015, 13, 164–167. [Google Scholar]
- Aarts, S. , Van den Akker, M., Hajema, K. J., van Ingen, A. V., Metsemakers, J. F. M., Verhey, F. R. J., & Van Boxtel, M. P. J. Multimorbidity and its relation to subjective memory complaints in a large general population of older adults. International psychogeriatrics, 2011, 23, 616–624. [Google Scholar]
- Aarts, S. , Van den Akker, M., Tan, F. E. S., Verhey, F. R. J., Metsemakers, J. F. M., & Van Boxtel, M. P. J. Influence of multimorbidity on cognition in a normal aging population: a 12-year follow-up in the Maastricht Aging Study. International journal of geriatric psychiatry, 2011, 26, 1046–1053. [Google Scholar]
- Aarts, S. , van den Akker, M. , Bosma, H., Tan, F., Verhey, F., Metsemakers, J., & van Boxtel, M. The effect of multimorbidity on health related functioning: temporary or persistent? Results from a longitudinal cohort study. Journal of psychosomatic research, 2012, 73, 211–217. [Google Scholar]
- Abizanda, P. , Romero, L. , Sanchez-Jurado, P. M., Martinez-Reig, M., Alfonso-Silguero, S. A., & Rodriguez-Manas, L. Age, frailty, disability, institutionalization, multimorbidity or comorbidity. Which are the main targets in older adults?. The journal of nutrition, health & aging, 2014, 18, 622–627. [Google Scholar]
- Agborsangaya, C. B. , Lau, D. , Lahtinen, M., Cooke, T., & Johnson, J. A. Health-related quality of life and healthcare utilization in multimorbidity: results of a cross-sectional survey. Quality of life Research, 2013, 22, 791–799. [Google Scholar] [PubMed]
- Agborsangaya, C. B. , Lau, D. , Lahtinen, M., Cooke, T., & Johnson, J. A. Health-related quality of life and healthcare utilization in multimorbidity: results of a cross-sectional survey. Quality of life Research, 2013, 22, 791–799. [Google Scholar]
- Agborsangaya, C. B. , Ngwakongnwi, E. , Lahtinen, M., Cooke, T., & Johnson, J. A. Multimorbidity prevalence in the general population: the role of obesity in chronic disease clustering. BMC Public Health, 2013, 13, 1–6. [Google Scholar]
- Rizzi, S. , Wensink, M. , Ahrenfeldt, L. J., Christensen, K., & Lindahl-Jacobsen, R. Age-specific cancer rates: a bird's-eye view on progress. Annals of Epidemiology, 2020, 48, 51–54. [Google Scholar]
- Alimohammadian, M. , Majidi, A. , Yaseri, M., Ahmadi, B., Islami, F., Derakhshan, M.,... & Malekzadeh, R. Multimorbidity as an important issue among women: results of a gender difference investigation in a large population-based cross-sectional study in West Asia. BMJ open, 2017, 7, e013548. [Google Scholar]
- Angst, J. , Sellaro, R. , & Ries Merikangas, K. Multimorbidity of psychiatric disorders as an indicator of clinical severity. European Archives of Psychiatry and Clinical Neuroscience, 2002, 252, 147–154. [Google Scholar]
- Rizzi, S. , Wensink, M. , Ahrenfeldt, L. J., Christensen, K., & Lindahl-Jacobsen, R. Age-specific cancer rates: a bird's-eye view on progress. Annals of Epidemiology, 2020, 48, 51–54. [Google Scholar]
- Gausi, B. , Berkowitz, N. , Jacob, N., & Oni, T. Treatment outcomes among adults with HIV/non-communicable disease multimorbidity attending integrated care clubs in Cape Town, South Africa. AIDS research and therapy, 2021, 18, 1–13. [Google Scholar]
- Adams, M. L. Peer Reviewed: Differences Between Younger and Older US Adults With Multiple Chronic Conditions. Preventing Chronic Disease, 2017, 14.
- Amaral, T. L. M. , Amaral, C. D. A., Lima, N. S. D., Herculano, P. V., Prado, P. R. D., & Monteiro, G. T. R. Multimorbidity, depression and quality of life among elderly people assisted in the Family Health Strategy in Senador Guiomard, Acre, Brazil. Ciência & Saúde Coletiva, 2018, 23, 3077–3084. [Google Scholar]
- An, K. O. , & Kim, J. Association of sarcopenia and obesity with multimorbidity in Korean adults: a nationwide cross-sectional study. Journal of the American Medical Directors Association, 2016, 17, 960–e1. [Google Scholar]
- An, K. O. , & Kim, J. Association of sarcopenia and obesity with multimorbidity in Korean adults: a nationwide cross-sectional study. Journal of the American Medical Directors Association, 2016, 17, 960–e1. [Google Scholar]
- Brett, T. , Arnold-Reed, D. E., Popescu, A., Soliman, B., Bulsara, M. K., Fine, H.,... & Moorhead, R. G. Multimorbidity in patients attending 2 Australian primary care practices. The Annals of Family Medicine, 2013, 11, 535–542. [Google Scholar]
- Arokiasamy, P. , Uttamacharya, U., Jain, K., Biritwum, R. B., Yawson, A. E., Wu, F.,... & Kowal, P. The impact of multimorbidity on adult physical and mental health in low-and middle-income countries: what does the study on global ageing and adult health (SAGE) reveal? BMC medicine, 2015, 13, 1–16. [Google Scholar]
- Sinnige, J. , Braspenning, J., Schellevis, F., Stirbu-Wagner, I., Westert, G., & Korevaar, J. The prevalence of disease clusters in older adults with multiple chronic diseases–a systematic literature review. PloS one, 2013, 8, e79641. [Google Scholar]
- Zemedikun, D. T. , Gray, L. J., Khunti, K., Davies, M. J., & Dhalwani, N. N. (2018, July). Patterns of multimorbidity in middle-aged and older adults: an analysis of the UK biobank data. In Mayo Clinic Proceedings (Vol. 93, No. 7, pp. 857–866). Elsevier.
- Mounce, L. T. , Campbell, J. L., Henley, W. E., Arreal, M. C. T., Porter, I., & Valderas, J. M. Predicting incident multimorbidity. The Annals of Family Medicine, 2018, 16, 322–329. [Google Scholar] [PubMed]
- Taylor, A. W. , Price, K. , Gill, T. K., Adams, R., Pilkington, R., Carrangis, N.,... & Wilson, D. Multimorbidity-not just an older person's issue. Results from an Australian biomedical study. BMC public health, 2010, 10, 1–10. [Google Scholar]
- Vancampfort, D. , Koyanagi, A., Ward, P. B., Veronese, N., Carvalho, A. F., Solmi, M.,... & Stubbs, B. Perceived stress and its relationship with chronic medical conditions and multimorbidity among 229,293 community-dwelling adults in 44 low-and middle-income countries. American journal of epidemiology, 2017, 186, 979–989. [Google Scholar]
- Vancampfort, D. , Koyanagi, A., Ward, P. B., Rosenbaum, S., Schuch, F. B., Mugisha, J.,... & Stubbs, B. (2017). Chronic physical conditions, multimorbidity and physical activity across 46 low-and middle-income countries. International Journal of Behavioral Nutrition and Physical Activity, 14, 1-13.
- Aubert, C. E. , Schnipper, J. L., Roumet, M., Marques-Vidal, P., Stirnemann, J., Auerbach, A. D.,... & Donzé, J. Best definitions of multimorbidity to identify patients with high health care resource utilization. Mayo Clinic Proceedings: Innovations, Quality & Outcomes, 2020, 4, 40–49. [Google Scholar]
- Autenrieth, C. S. , Kirchberger, I., Heier, M., Zimmermann, A. K., Peters, A., Döring, A., & Thorand, B. Physical activity is inversely associated with multimorbidity in elderly men: results from the KORA-Age Augsburg Study. Preventive medicine, 2013, 57, 17–19. [Google Scholar]
- Bähler, C. , Huber, C. A., Brüngger, B., & Reich, O. Multimorbidity, health care utilization and costs in an elderly community-dwelling population: a claims data based observational study. BMC health services research, 2015, 15, 1–12. [Google Scholar]
- Vancampfort, D. , Koyanagi, A. , Ward, P. B., Veronese, N., Carvalho, A. F., Solmi, M.,... & Stubbs, B. Perceived stress and its relationship with chronic medical conditions and multimorbidity among 229,293 community-dwelling adults in 44 low-and middle-income countries. American journal of epidemiology, 2017, 186, 979–989. [Google Scholar]
- Bernard, S. , Inderjeeth, C., & Raymond, W. Higher Charlson Comorbidity Index scores do not influence Functional Independence Measure score gains in older rehabilitation patients. Australasian Journal on Ageing, 2016, 35, 236–241. [Google Scholar] [PubMed]
- Biswas, T. , Townsend, N., Islam, M. S., Islam, M. R., Gupta, R. D., Das, S. K., & Al Mamun, A. Association between socioeconomic status and prevalence of non-communicable diseases risk factors and comorbidities in Bangladesh: findings from a nationwide cross-sectional survey. BMJ open, 2019, 9, e025538. [Google Scholar] [PubMed]
- Blakemore, A. , Hann, M., Howells, K., Panagioti, M., Sidaway, M., Reeves, D., & Bower, P. Patient activation in older people with long-term conditions and multimorbidity: correlates and change in a cohort study in the United Kingdom. BMC Health Services Research, 2016, 16, 1–11. [Google Scholar]
- Bowling, C. B. , Deng, L. ( 34, 2390–2396. [PubMed]
- Stewart, M. , Fortin, M., Britt, H. C., Harrison, C. M., & Maddocks, H. L. Comparisons of multi-morbidity in family practice—issues and biases. Family Practice, 2013, 30, 473–480. [Google Scholar] [PubMed]
- Broeiro-Gonçalves, P. , Nogueira, P. , & Aguiar, P. Multimorbidity and disease severity by age groups, in inpatients: cross-sectional study. Portuguese Journal of Public Health, 2019, 37, 1–9. [Google Scholar]
- Uhlig, K. , Leff, B., Kent, D., Dy, S., Brunnhuber, K., Burgers, J. S.,... & Boyd, C. M. A framework for crafting clinical practice guidelines that are relevant to the care and management of people with multimorbidity. Journal of general internal medicine, 2014, 29, 670–679. [Google Scholar]
- Buurman, B. M. , Frenkel, W. J., Abu-Hanna, A., Parlevliet, J. L., & de Rooij, S. E. Acute and chronic diseases as part of multimorbidity in acutely hospitalized older patients. European journal of internal medicine, 2016, 27, 68–75. [Google Scholar]
- Calderón-Larrañaga, A. , Vetrano, D. L., Onder, G., Gimeno-Feliu, L. A., Coscollar-Santaliestra, C., Carfí, A.,... & Fratiglioni, L. Assessing and measuring chronic multimorbidity in the older population: a proposal for its operationalization. Journals of Gerontology Series A: Biomedical Sciences and Medical Sciences, 2017, 72, 1417–1423. [Google Scholar]
- Canevelli, M. , Raganato, R., Remiddi, F., Quarata, F., Valletta, M., Bruno, G., & Cesari, M. Counting deficits or diseases? the agreement between frailty and multimorbidity in subjects with cognitive disturbances. Aging Clinical and Experimental Research, 2020, 32, 179–182. [Google Scholar]
- Chamberlain, A. M. , Sauver, J. L. S., Gerber, Y., Manemann, S. M., Boyd, C. M., Dunlay, S. M.,... & Roger, V. L. Multimorbidity in heart failure: a community perspective. The American journal of medicine, 2015, 128, 38–45. [Google Scholar]
- Chen, H. , Cheng, M., Zhuang, Y., & Broad, J. B. Multimorbidity among middle-aged and older persons in urban China: Prevalence, characteristics and health service utilization. Geriatrics & gerontology international, 2018, 18, 1447–1452. [Google Scholar]
- Ng, N. M. , Ng, Y. S., Chu, T. K., & Lau, P. Factors affecting prescription of sodium-glucose co-transporter 2 inhibitors in patients with type 2 diabetes mellitus with established cardiovascular disease/chronic kidney disease in Hong Kong: a qualitative study. BMC Primary Care, 2022, 23, 317. [Google Scholar]
- Chudasama, Y. V. , Khunti, K. K., Zaccardi, F., Rowlands, A. V., Yates, T., Gillies, C. L.,... & Dhalwani, N. N. Physical activity, multimorbidity, and life expectancy: a UK Biobank longitudinal study. BMC medicine, 2019, 17, 1–13. [Google Scholar]
- Cimarras-Otal, C. , Calderón-Larrañaga, A., Poblador-Plou, B., González-Rubio, F., Gimeno-Feliu, L. A., Arjol-Serrano, J. L., & Prados-Torres, A. Association between physical activity, multimorbidity, self-rated health and functional limitation in the Spanish population. BMC public health, 2014, 14, 1–10. [Google Scholar]
- Chin, W. Y. , Choi, E. P. H., Wan, E. Y. F., & Lam, C. L. K. Health-related quality of life mediates associations between multi-morbidity and depressive symptoms in Chinese primary care patients. Family practice, 2016, 33, 61–68. [Google Scholar] [PubMed]
- Agrawal, S. , & Agrawal, P. K. Association between body mass index and prevalence of multimorbidity in low-and middle-income countries: a cross-sectional study. International journal of medicine and public health, 2016, 6, 73. [Google Scholar]
- Gunn, J. M. , Ayton, D. R., Densley, K., Pallant, J. F., Chondros, P., Herrman, H. E., & Dowrick, C. F. The association between chronic illness, multimorbidity and depressive symptoms in an Australian primary care cohort. Social psychiatry and psychiatric epidemiology, 2012, 47, 175–184. [Google Scholar]
- Koh, H. Y. , Kim, T. H., Sheen, Y. H., Lee, S. W., An, J., Kim, M. A.,... & Yon, D. K. Serum heavy metal levels are associated with asthma, allergic rhinitis, atopic dermatitis, allergic multimorbidity, and airflow obstruction. The Journal of Allergy and Clinical Immunology: In Practice, 2019, 7, 2912–2915. [Google Scholar]
- Hanlon, P. , Nicholl, B. I., Jani, B. D., Lee, D., McQueenie, R., & Mair, F. S. Frailty and pre-frailty in middle-aged and older adults and its association with multimorbidity and mortality: a prospective analysis of 493 737 UK Biobank participants. The Lancet Public Health, 2018, 3, e323–e332. [Google Scholar] [PubMed]
- Jantsch, A. G. , Alves, R. F. S., & Faerstein, E. Educational inequality in Rio de Janeiro and its impact on multimorbidity: evidence from the Pró-Saúde study. A cross-sectional analysis. Sao Paulo Medical Journal, 2018, 136, 51–58. [Google Scholar]
- Jovic, D. , Vukovic, D. , & Marinkovic, J. Prevalence and patterns of multi-morbidity in Serbian adults: a cross-sectional study. PloS one, 2016, 11, e0148646. [Google Scholar]
- Juul-Larsen, H. G. , Christensen, L. D., Bandholm, T., Andersen, O., Kallemose, T., Jørgensen, L. M., & Petersen, J. (2020). Patterns of multimorbidity and differences in healthcare utilization and complexity among acutely hospitalized medical patients (≥ 65 Years)–a latent class approach. Clinical epidemiology, 245-259.
- Juul-Larsen, H. G. , Christensen, L. D., Bandholm, T., Andersen, O., Kallemose, T., Jørgensen, L. M., & Petersen, J. (2020). Patterns of multimorbidity and differences in healthcare utilization and complexity among acutely hospitalized medical patients (≥ 65 Years)–a latent class approach. Clinical epidemiology, 245-259.
- Fortin, M. , Bravo, G. , Hudon, C., Vanasse, A., & Lapointe, L. Prevalence of multimorbidity among adults seen in family practice. The Annals of Family Medicine, 2005, 3, 223–228. [Google Scholar]
- Ie, K. , Felton, M. , Springer, S., Wilson, S. A., & Albert, S. M. Multimorbidity and polypharmacy in family medicine residency practices. Journal of Pharmacy Technology, 2017, 33, 219–224. [Google Scholar]
- Ishizaki, T. , Kobayashi, E. , Fukaya, T., Takahashi, Y., Shinkai, S., & Liang, J. Association of physical performance and self-rated health with multimorbidity among older adults: results from a nationwide survey in Japan. Archives of Gerontology and Geriatrics, 2019, 84, 103904. [Google Scholar] [PubMed]
- Schwartz, A. , de Heer, H. D., & Bea, J. W. Initiating exercise interventions to promote wellness in cancer patients and survivors. Oncology (Williston Park, NY), 2017, 31, 711. [Google Scholar]
- Demirchyan, A. , Khachadourian, V., Armenian, H. K., & Petrosyan, V. (2013). Short and long term determinants of incident multimorbidity in a cohort of 1988 earthquake survivors in Armenia. International journal for equity in health, 12, 1-8.
- Fabbri, E. , Zoli, M. , Gonzalez-Freire, M., Salive, M. E., Studenski, S. A., & Ferrucci, L. Aging and multimorbidity: new tasks, priorities, and frontiers for integrated gerontological and clinical research. Journal of the American Medical Directors Association, 2015, 16, 640–647. [Google Scholar]
- Blay, S. L. , Fillenbaum, G. G., & Peluso, E. T. Differential characteristics of young and midlife adult users of psychotherapy, psychotropic medications, or both: information from a population representative sample in São Paulo, Brazil. BMC psychiatry, 2015, 15, 1–9. [Google Scholar]
- Kang, J. , & Song, Y. M. The association between submarine service and multimorbidity: a cross-sectional study of Korean naval personnel. BMJ open, 2017, 7, e017776. [Google Scholar]
- Harrison, C. , Britt, H. , Miller, G., & Henderson, J. Examining different measures of multimorbidity, using a large prospective cross-sectional study in Australian general practice. BMJ open, 2014, 4, e004694. [Google Scholar]
- Khan, N. , Rahman, M. , Mitra, D., & Afsana, K. Prevalence of multimorbidity among Bangladeshi adult population: a nationwide cross-sectional study. BMJ open, 2019, 9, e030886. [Google Scholar] [PubMed]
- Khanam, M. A. , Streatfield, P. K., Kabir, Z. N., Qiu, C., Cornelius, C., & Wahlin, Å. Prevalence and patterns of multimorbidity among elderly people in rural Bangladesh: a cross-sectional study. Journal of health, population, and nutrition, 2011, 29, 406. [Google Scholar]
- King, D. E. , Xiang, J. , & Pilkerton, C. S. Multimorbidity trends in United States adults, 1988–2014. The Journal of the American Board of Family Medicine, 2018, 31, 503–513. [Google Scholar]
- Gandhi, K. , Lim, E. , Davis, J., & Chen, J. J. Racial-ethnic disparities in self-reported health status among US adults adjusted for sociodemographics and multimorbidities, National Health and Nutrition Examination Survey 2011–2014. Ethnicity & health, 2020, 25, 65–78. [Google Scholar]
- Gaulin, M. , Simard, M. , Candas, B., Lesage, A., & Sirois, C. Combined impacts of multimorbidity and mental disorders on frequent emergency department visits: a retrospective cohort study in Quebec, Canada. CMAJ, 2019, 191, E724–E732. [Google Scholar] [PubMed]
- Calderón-Larrañaga, A. , Vetrano, D. L., Onder, G., Gimeno-Feliu, L. A., Coscollar-Santaliestra, C., Carfí, A.,... & Fratiglioni, L. Assessing and measuring chronic multimorbidity in the older population: a proposal for its operationalization. Journals of Gerontology Series A: Biomedical Sciences and Medical Sciences, 2017, 72, 1417–1423. [Google Scholar]
- Dhalwani, N. N. , Zaccardi, F. , O’Donovan, G., Carter, P., Hamer, M., Yates, T., & Khunti, K. Association between lifestyle factors and the incidence of multimorbidity in an older English population. Journals of Gerontology Series A: Biomedical Sciences and Medical Sciences, 2017, 72, 528–534. [Google Scholar]
- Excoffier, S. , Herzig, L. , N’Goran, A. A., Déruaz-Luyet, A., & Haller, D. M. Prevalence of multimorbidity in general practice: a cross-sectional study within the Swiss Sentinel Surveillance System (Sentinella). BMJ open, 2018, 8, e019616. [Google Scholar] [PubMed]
- Fortin, M. , Bravo, G. , Hudon, C., Vanasse, A., & Lapointe, L. Prevalence of multimorbidity among adults seen in family practice. The Annals of Family Medicine, 2005, 3, 223–228. [Google Scholar] [PubMed]
- Galenkamp, H. , Gagliardi, C. , Principi, A., Golinowska, S., Moreira, A., Schmidt, A. E.,... & Deeg, D. J. Predictors of social leisure activities in older Europeans with and without multimorbidity. European Journal of Ageing, 2016, 13, 129–143. [Google Scholar]
- Gawron, L. M. , Sanders, J. N., Sward, K., Poursaid, A. E., Simmons, R., & Turok, D. K. Multi-morbidity and highly effective contraception in reproductive-age women in the US Intermountain West: a retrospective cohort study. Journal of General Internal Medicine, 2020, 35, 637–642. [Google Scholar]
- Habib, R. R. , Hojeij, S. , Elzein, K., Chaaban, J., & Seyfert, K. Associations between life conditions and multi-morbidity in marginalized populations: the case of Palestinian refugees. The European Journal of Public Health, 2014, 24, 727–733. [Google Scholar] [PubMed]
- Harrison, C. , Britt, H. , Miller, G., & Henderson, J. Examining different measures of multimorbidity, using a large prospective cross-sectional study in Australian general practice. BMJ open, 2014, 4, e004694. [Google Scholar]
- Hayek, S. (2017). Prevalence, correlates, and time trends of multiple chronic conditions among Israeli adults: estimates from the Israeli National Health Interview Survey, 2014–2015. Preventing chronic disease, 14.
- Miller, J. L. , Thylén, I. , Elayi, S. C., Etaee, F., Fleming, S., Czarapata, M. M.,... & Moser, D. K. Multi-morbidity burden, psychological distress, and quality of life in implantable cardioverter defibrillator recipients: results from a nationwide study. Journal of Psychosomatic Research, 2019, 120, 39–45. [Google Scholar] [PubMed]
- Hernández, B. , Reilly, R. B., & Kenny, R. A. Investigation of multimorbidity and prevalent disease combinations in older Irish adults using network analysis and association rules. Scientific reports, 2019, 9, 14567. [Google Scholar]
- Ng, C. Y. H. , Tay, S. H., McIntyre, R. S., Ho, R., Tam, W. W., & Ho, C. S. Elucidating a bidirectional association between rheumatoid arthritis and depression: A systematic review and meta-analysis. Journal of affective disorders, 2022, 311, 407–415. [Google Scholar]
- Kingston, A. , Robinson, L., Booth, H., Knapp, M., Jagger, C., & Modem Project. Projections of multi-morbidity in the older population in England to 2035: estimates from the Population Ageing and Care Simulation (PACSim) model. Age and ageing, 2018, 47, 374–380. [Google Scholar] [PubMed]
- Garin, N. , Koyanagi, A., Chatterji, S., Tyrovolas, S., Olaya, B., Leonardi, M.,... & Haro, J. M. Global multimorbidity patterns: a cross-sectional, population-based, multi-country study. Journals of Gerontology Series A: Biomedical Sciences and Medical Sciences, 2016, 71, 205–214. [Google Scholar]
- Kriegsman, D. M. , Deeg, D. J., & Stalman, W. A. Comorbidity of somatic chronic diseases and decline in physical functioning: the Longitudinal Aging Study Amsterdam. Journal of clinical epidemiology, 2004, 57, 55–65. [Google Scholar]
- Kristensen, K. , König, H. H., & Hajek, A. The association of multimorbidity, loneliness, social exclusion and network size: findings from the population-based German Ageing Survey. BMC Public Health, 2019, 19, 1–10. [Google Scholar]
- Kristensen, K. , König, H. H., & Hajek, A. The longitudinal association of multimorbidity on loneliness and network size: Findings from a population-based study. International journal of geriatric psychiatry, 2019, 34, 1490–1497. [Google Scholar] [PubMed]
- Lai, F. T. , Ma, T. W., & Hou, W. K. Multimorbidity is associated with more subsequent depressive symptoms in three months: a prospective study of community-dwelling adults in Hong Kong. International psychogeriatrics, 2019, 31, 1367–1371. [Google Scholar]
- Lai, F. T. , Wong, S. Y., Yip, B. H., Guthrie, B., Mercer, S. W., Chung, R. Y.,... & Yeoh, E. K. Multimorbidity in middle age predicts more subsequent hospital admissions than in older age: a nine-year retrospective cohort study of 121,188 discharged in-patients. European Journal of Internal Medicine 2019, 61, 103–111. [Google Scholar] [PubMed]
- Laires, P. A. , & Perelman, J. The current and projected burden of multimorbidity: a cross-sectional study in a Southern Europe population. European journal of ageing, 2019, 16, 181–192. [Google Scholar] [PubMed]
- Lang, K. , Alexander, I. M., Simon, J., Sussman, M., Lin, I., Menzin, J.,... & Hsu, M. A. The impact of multimorbidity on quality of life among midlife women: findings from a US nationally representative survey. Journal of Women's Health, 2015, 24, 374–383. [Google Scholar] [PubMed]
- Le Cossec, C. , Perrine, A. L., Beltzer, N., Fuhrman, C., & Carcaillon-Bentata, L. Pre-frailty, frailty, and multimorbidity: prevalences and associated characteristics from two French national surveys. The journal of nutrition, health & aging, 2016, 20, 860–869. [Google Scholar]
- Vogeli, C. , Shields, A. E., Lee, T. A., Gibson, T. B., Marder, W. D., Weiss, K. B., & Blumenthal, D. Multiple chronic conditions: prevalence, health consequences, and implications for quality, care management, and costs. Journal of general internal medicine, 2007, 22, 391–395. [Google Scholar]
- Li, H. W. , Lee, W. J., Lin, M. H., Peng, L. N., Loh, C. H., Chen, L. K., & Lu, C. C. Quality of life among community-dwelling middle-aged and older adults: function matters more than multimorbidity. Archives of gerontology and geriatrics, 2021, 95, 104423. [Google Scholar]
- Lujic, S. , Randall, D. A., Simpson, J. M., Falster, M. O., & Jorm, L. R. Interaction effects of multimorbidity and frailty on adverse health outcomes in elderly hospitalised patients. Scientific reports, 2022, 12, 14139. [Google Scholar]
- Lupiáñez-Villanueva, F. , Anastasiadou, D., Codagnone, C., Nuño-Solinís, R., & Garcia-Zapirain Soto, M. B. Electronic health use in the European Union and the effect of multimorbidity: cross-sectional survey. Journal of medical Internet research, 2018, 20, e165. [Google Scholar] [PubMed]
Figure 1.
Forest plot for the prevalence of multimorbidity cohort across 84 studies.
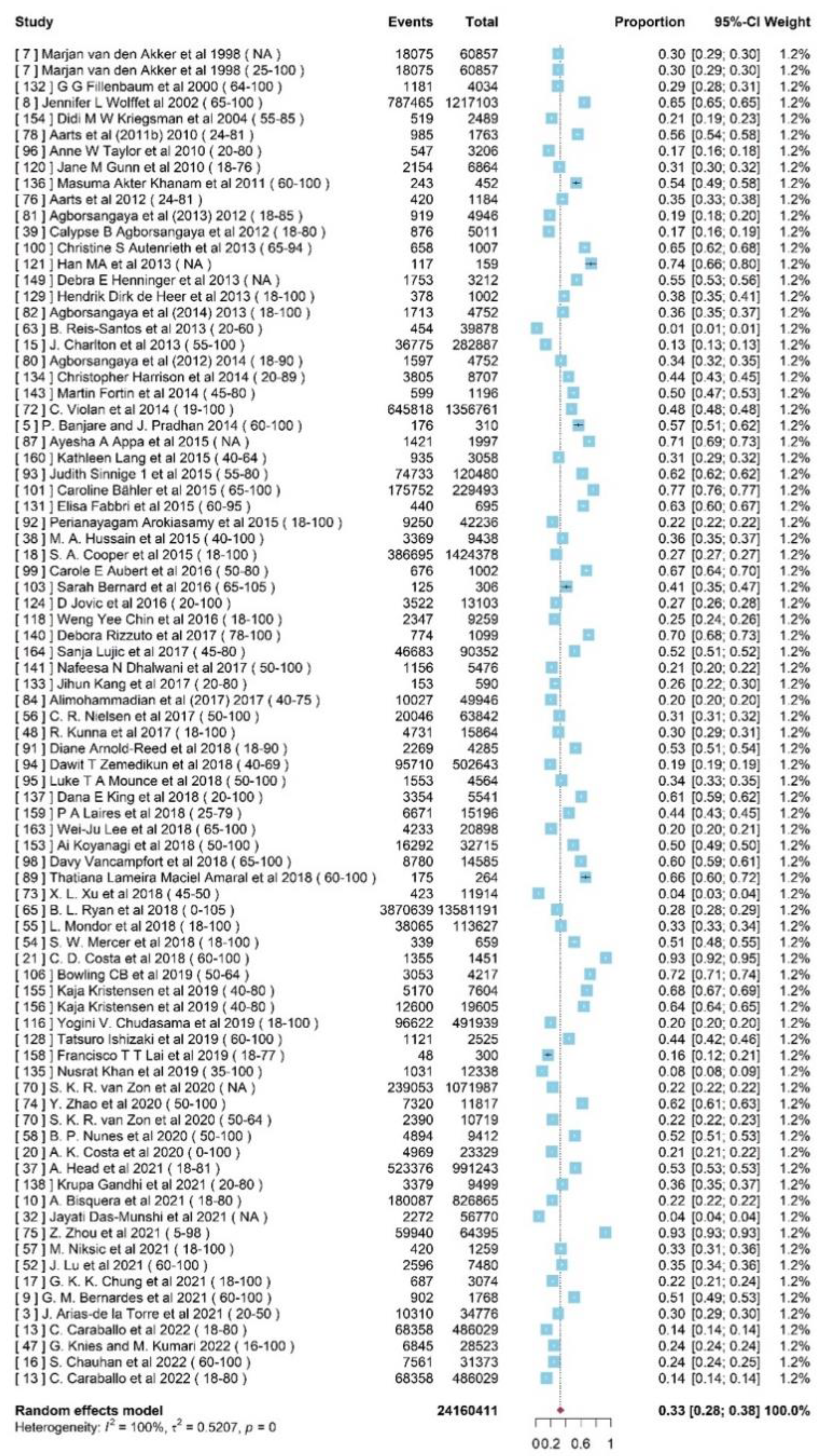
Figure 2.
Forest plot for the prevalence of multimorbidity in MICs and HICs.
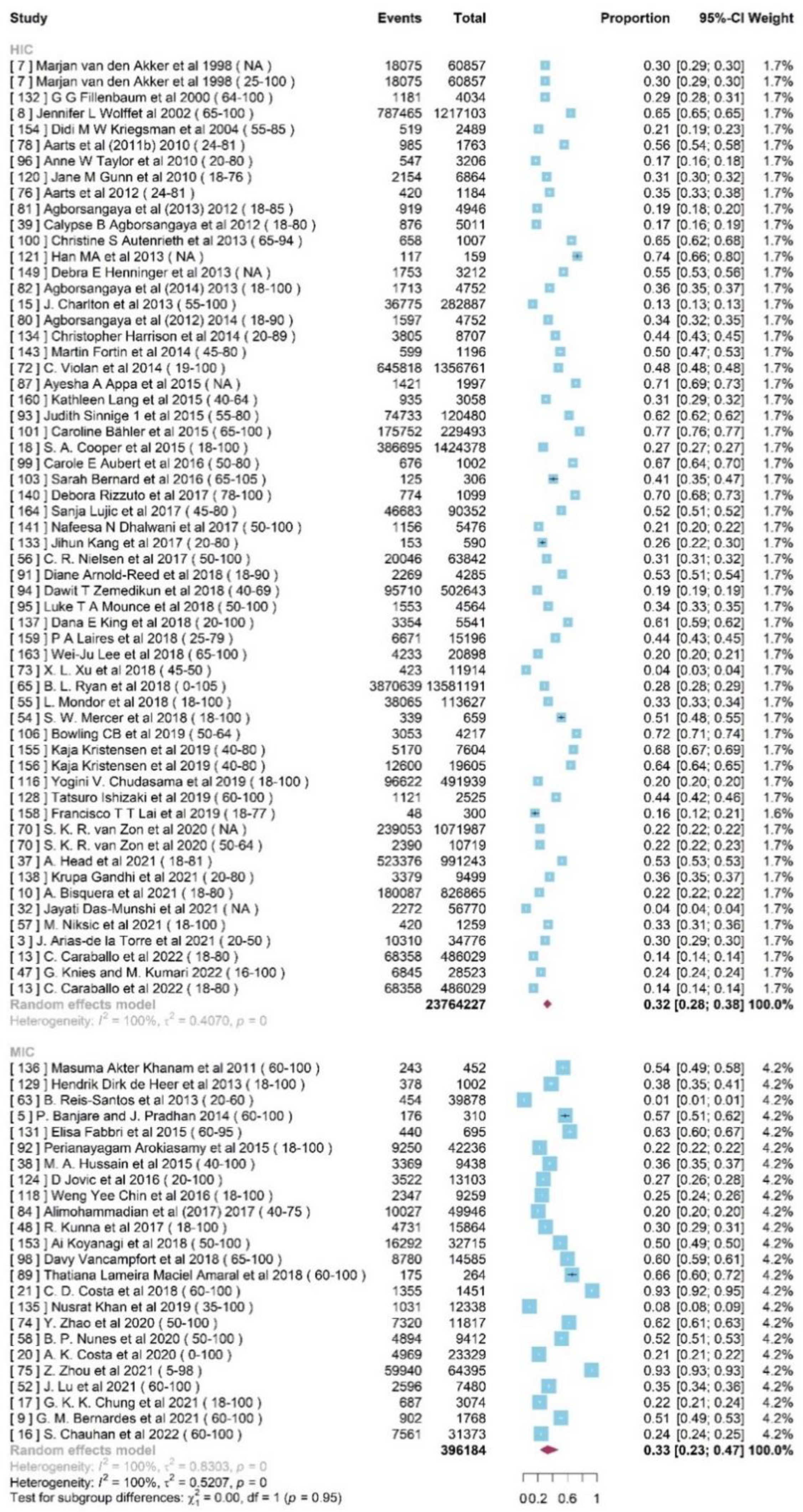
Figure 3.
Forest plot for the prevalence of multimorbidity in MIC and HIC age 50 above.
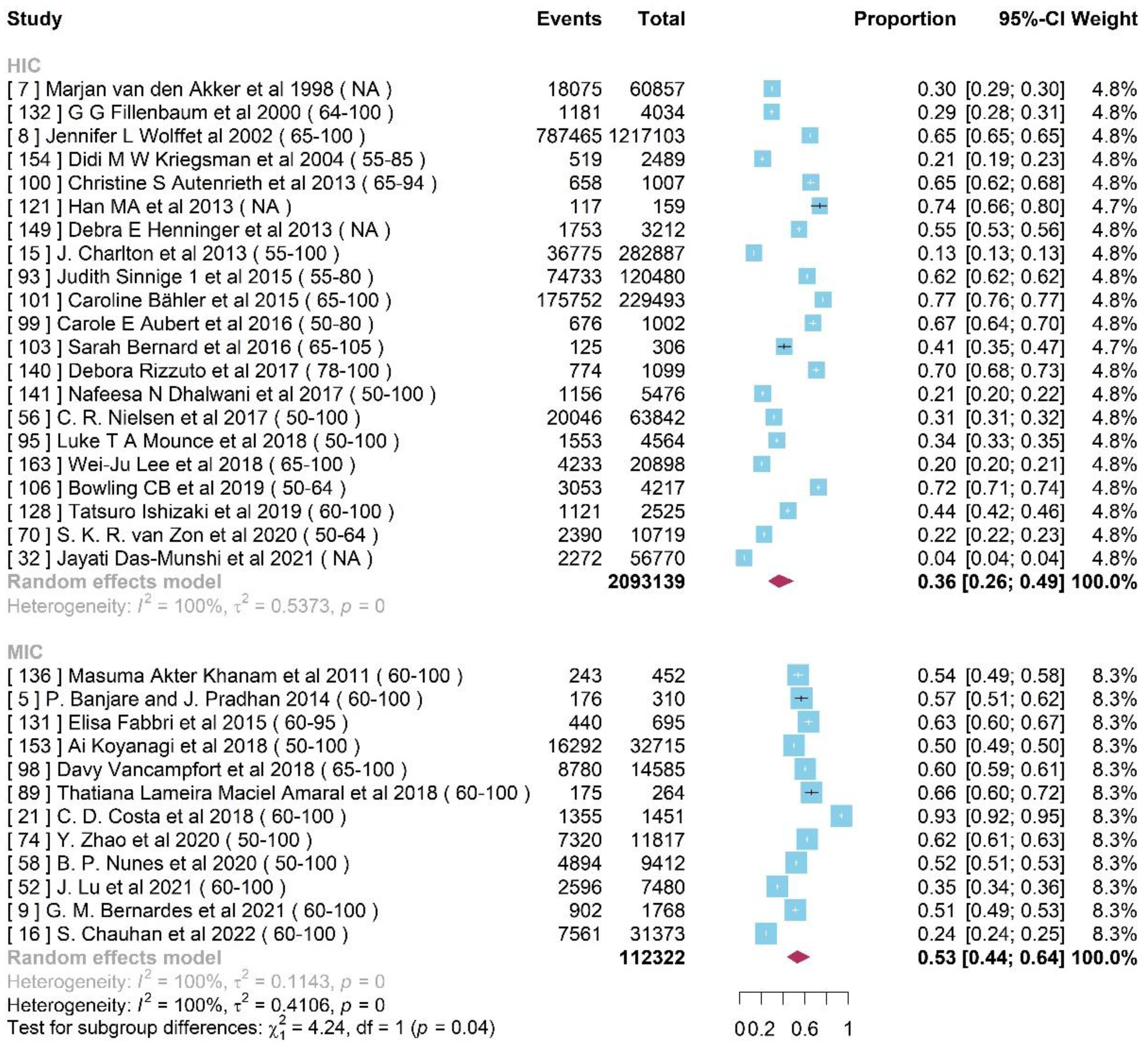
Figure 4.
Forest plot for the association between multimorbidity and gender.
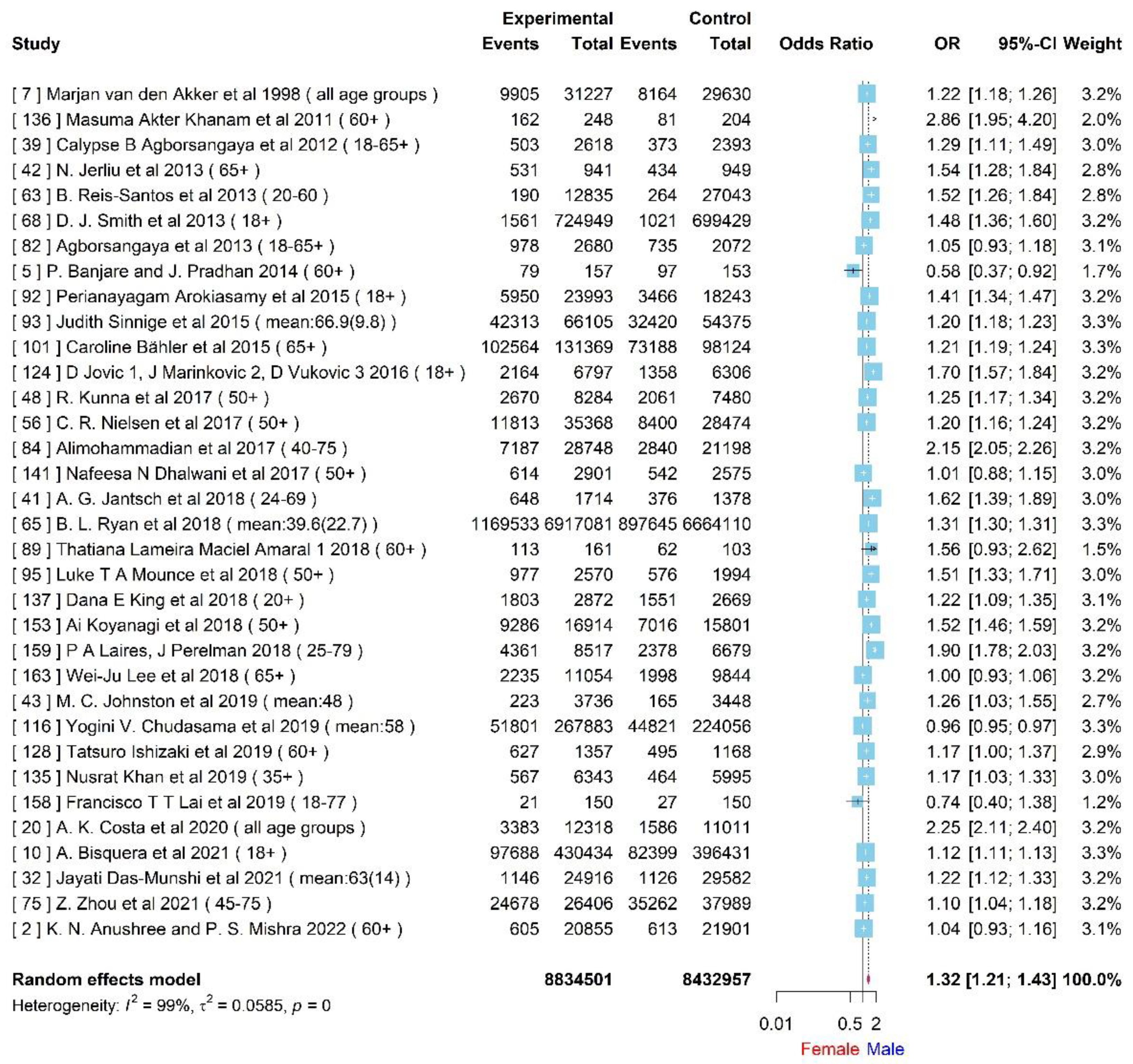
Figure 5.
Forest plot for difference of multimorbidity with rural and urban areas.
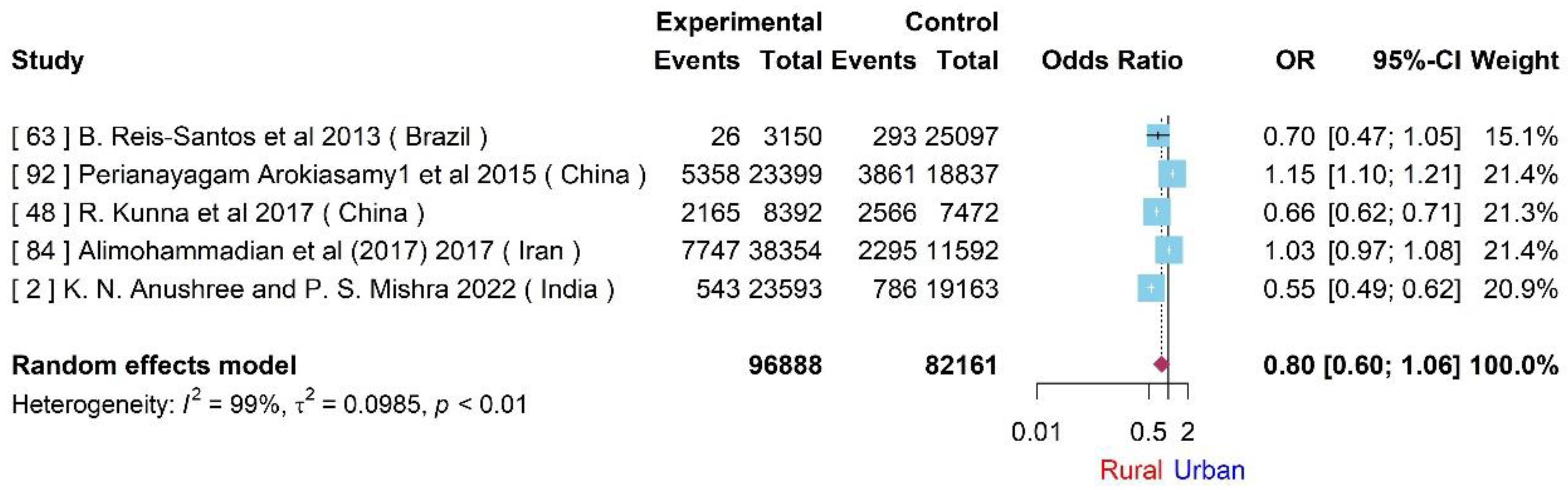
Figure 6.
Forest plot for the association between multimorbidity and smoke.
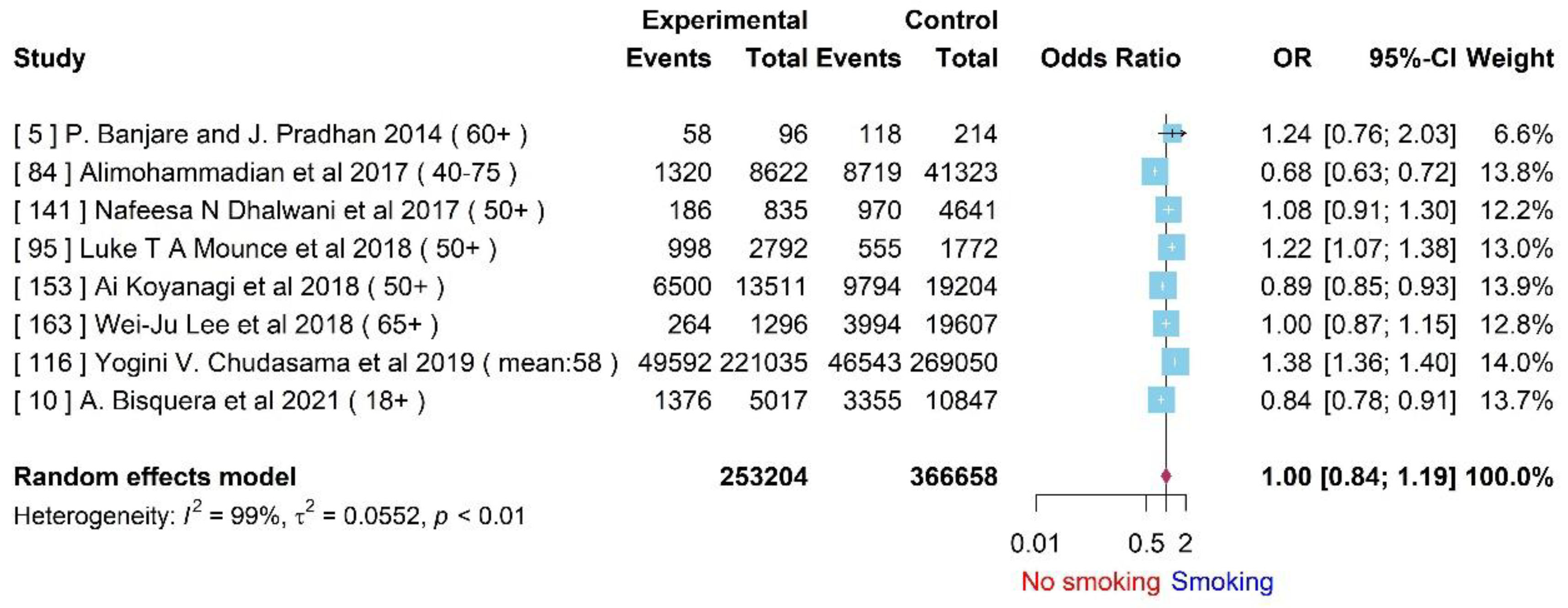
Figure 7.
Forest plot for the association between multimorbidity and ethnicity.
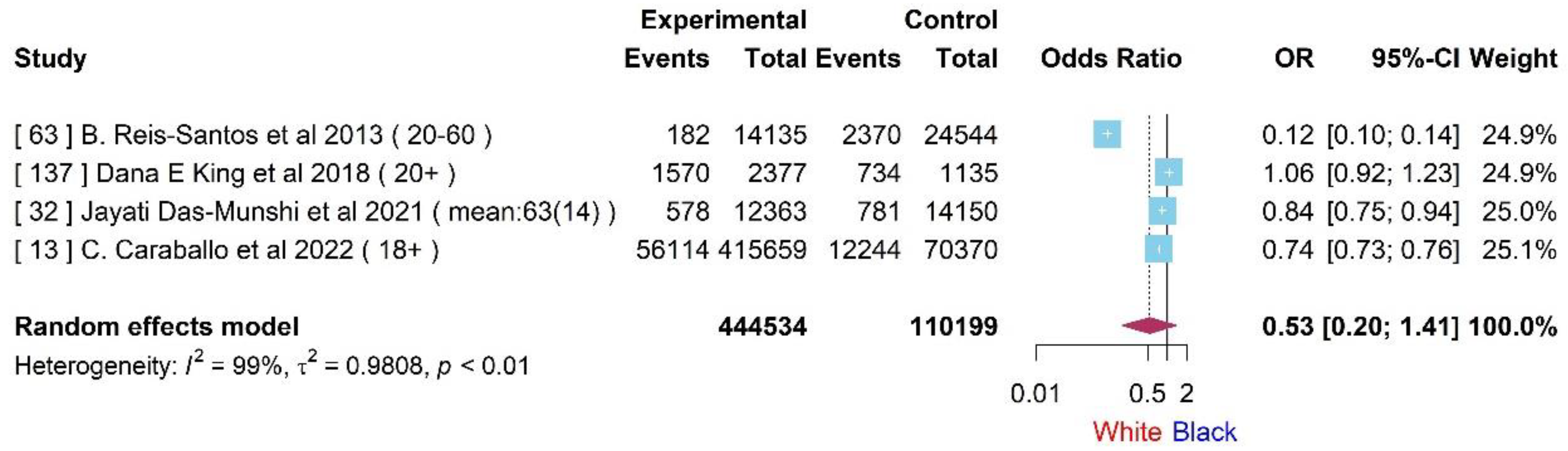
Figure 8.
Forest plot for difference of multimorbidity with high school and university education levels.
Figure 8.
Forest plot for difference of multimorbidity with high school and university education levels.
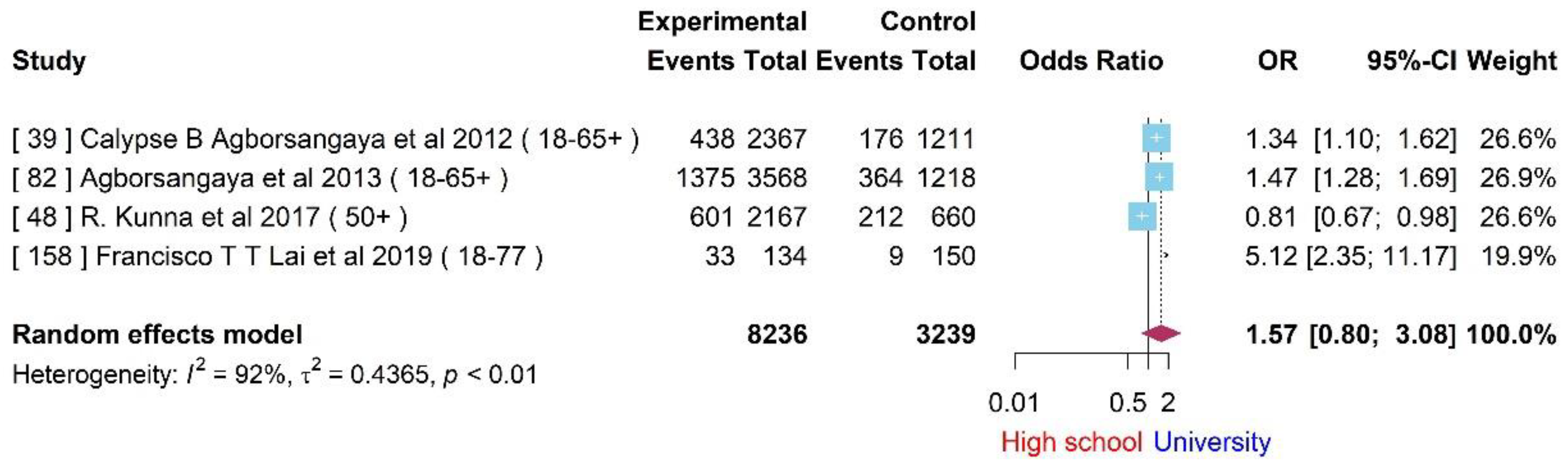
Figure 10.
Forest plot for the Rich-pool difference in multimorbidity cohort.
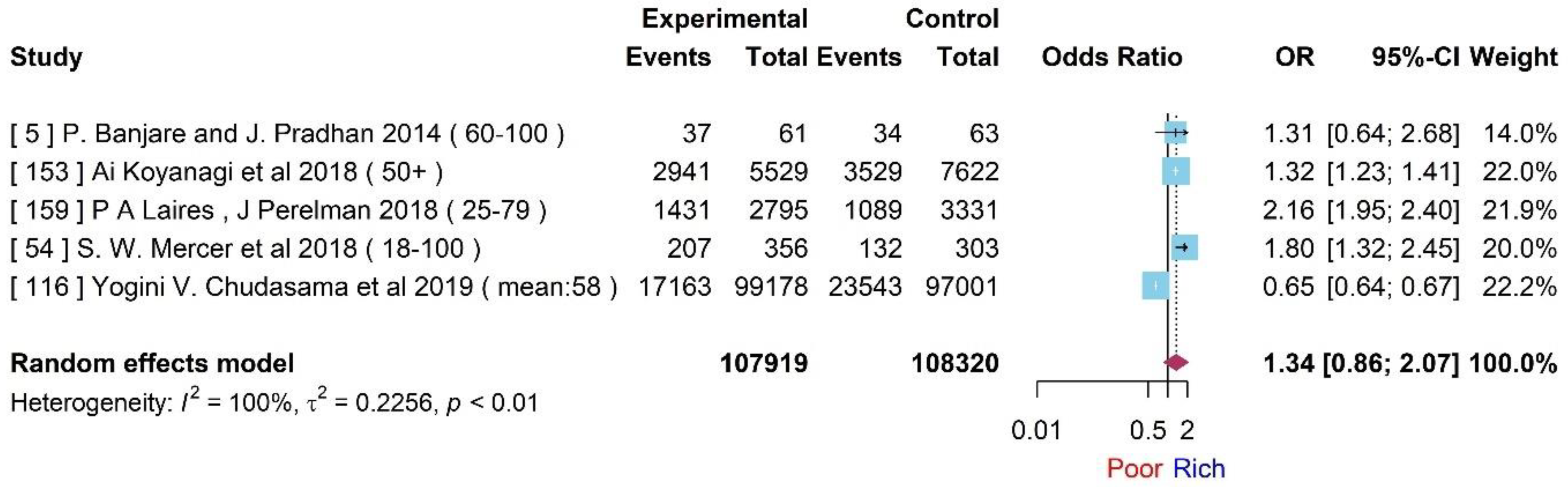
Figure 11.
Forest plot for the association between multimorbidity and marriage.
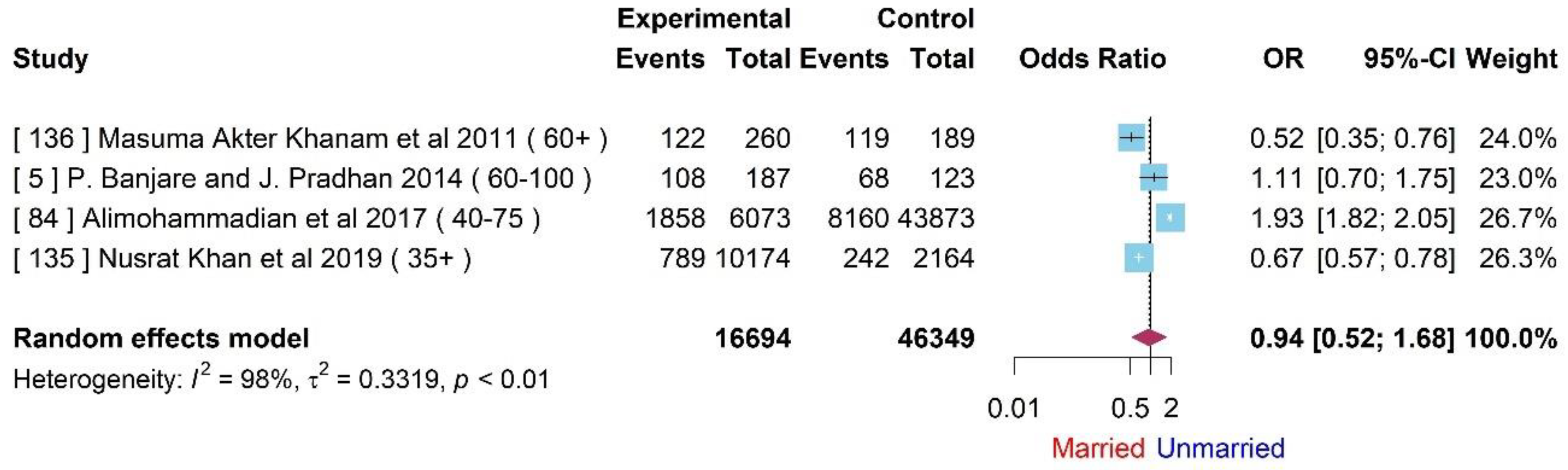
Figure 12.
Funnel plot of studies included in the meta-analysis of multimorbidity with gender effect.
Figure 12.
Funnel plot of studies included in the meta-analysis of multimorbidity with gender effect.
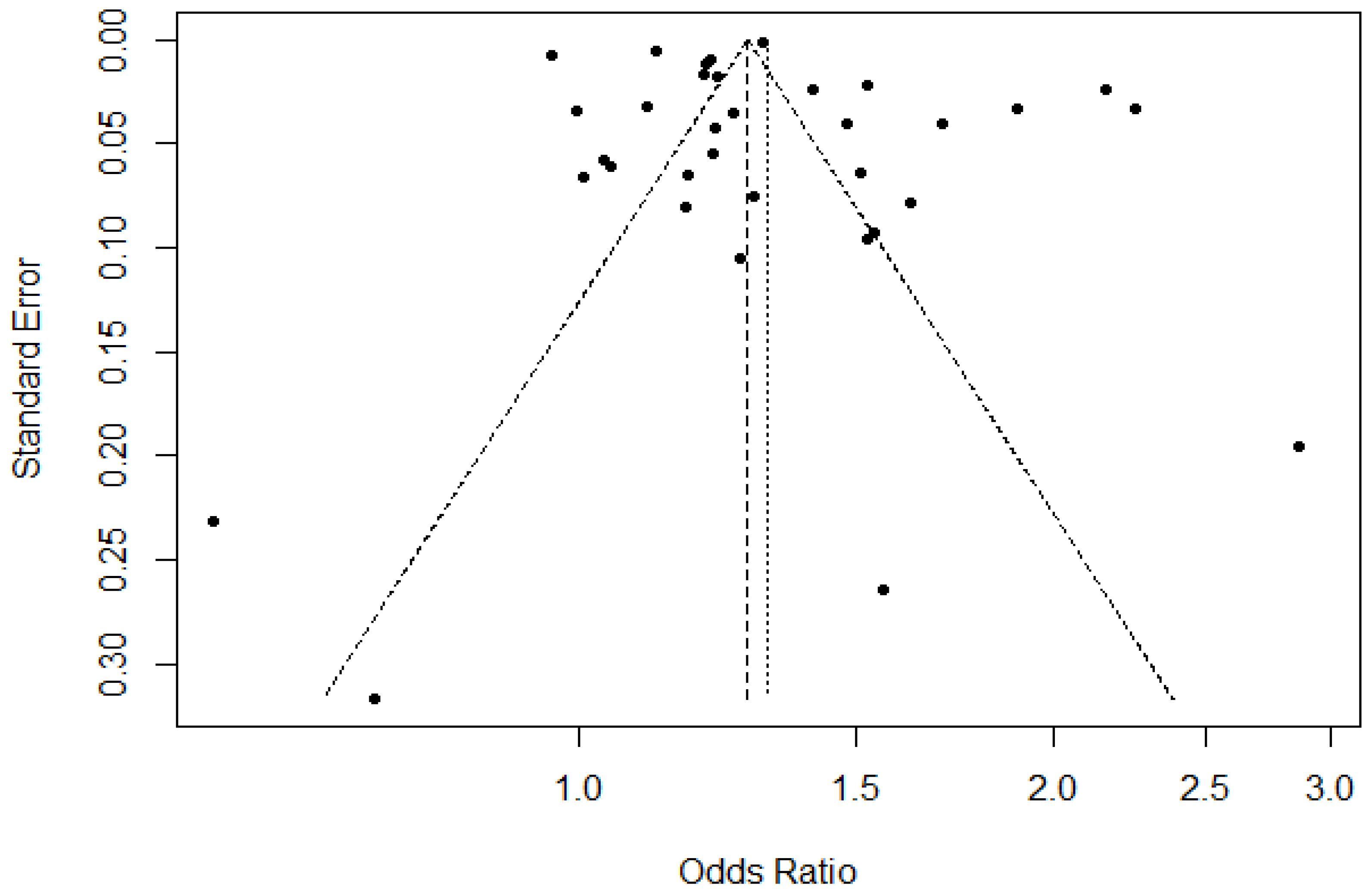
Figure 13.
Egger’s test for the gender effect on multimorbidity.
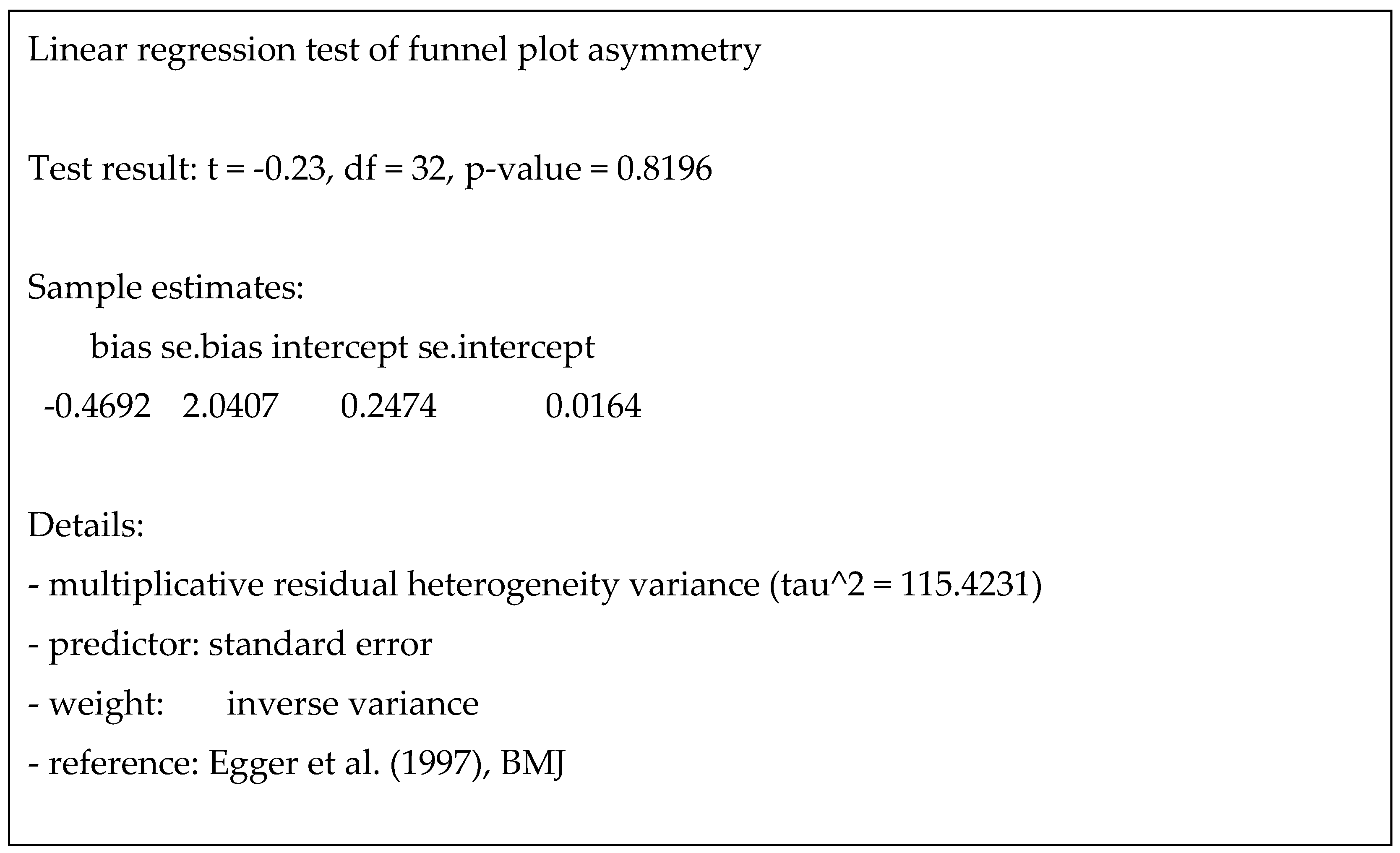

Table 1.
Characteristics of the studies included in systematic review.
| Study ID | Authors | Year | Study Type | Country | Sample Size | Mean Age | Age Range | Meta-analysis Inclusion Y/N |
|---|---|---|---|---|---|---|---|---|
| 1 | S. Afshar et al [34] |
2015 | Cross-sectional |
Myanmar | 125404 | 72 | N | |
| 2 | K. N. Anushree and P. S. Mishra [35] | 2022 | India |
42756 | 60-100 | N | ||
| 3 | J. Arias-de la Torre et al [36] | 2021 | Observational cohort study |
UK | 34776 | 20-50 | Y | |
| 4 | J. E. O. Ataguba [37] | 2013 | South Africa |
26.80 | N | |||
| 5 | P. Banjare and J. Pradhan [38] | 2014 | India |
310 | 60-100 | Y | ||
| 6 | H. Q. Bennett et al [39] | 2021 | UK | 15431 | 75.6 | N | ||
| 7 | Marjan van den Akker et al [40] | 1998 | Longitudinal |
Netherlands |
60857 | 25-100 | Y |
|
| 8 | Jennifer L Wolff et al [41] | 2002 | Cross sectional |
USA | 1 217 103 | 75.4 | 65-100 | Y |
| 9 | G. M. Bernardes et al [42] | 2021 | Cohort study. |
Brazil |
1768 | 67.5 | 60-100 | Y |
| 10 | A. Bisquera et al [43] | 2021 | Retrospective cohort |
UK |
826936 | 42·4 | 18-80 | Y |
| 11 | E. Bustos-Vazquez et al [44] | 2017 | Cross-sectional study |
Mexico |
8874 | 60-100 | N | |
| 12 | J. Butterworth et al [45] | 2020 | Cluster randomized controlled feasibility trial |
N | ||||
| 13 | C. Caraballo et al [46] | 2022 | Cross-sectional |
USA | 596355 | 48.4 | 18-80 | Y |
| 14 | N. Carrilero et al [47] | 2020 | Cross-sectional |
Spain | 1189325 | 0-14 | N | |
| 15 | J. Charlton et al [48] | 2013 | Cohort study |
England. |
282887 | 55-100 | Y | |
| 16 | S. Chauhan et al [49] | 2022 | Cross-sectional |
India |
31 373 | 60-100 | N | |
| 17 | G. K. K. Chung et al[50] | 2021 | China | 3074 | 48.5 | 18-100 | Y | |
| 18 | S. A. Cooper et al [51] | 2015 | Cross-sectional analysis |
Scotland | 1424378 | 43.1 48.0 | 18-100 | Y |
| 19 | G. Corrao et al [52] | 2020 | A nationwide study | Italy | N | |||
| 20 | A. K. Costa et al [53] | 2020 | Cross-sectional |
Brazil |
23329 | 37.9 | 0-100 | Y |
| 21 | C. D. Costa et al [54] | 2018 | Cross-sectional |
Brazil |
1451 | 60-100 | Y | |
| 22 | F. Diderichsen et al [55] | 2021 | N | |||||
| 23 | D. A. González-Chica et al [56] | 2017 | Cross-sectional study |
Australian | 2912 | 48.9 | N | |
| 24 | R. M. Guimaraes et al [57] | 2020 | Cross-sectional |
Brazil | 60-100 | N | ||
| 25 | P. Halonen et al [58] | 2019 | Cross-sectional |
Finland | 2862 | 91 | 90-107 | Y |
| 26 | M. Hamiduzzaman et al [59] | 2021 | Qualitative study |
Bangladesh | 22 | 72 | N | |
| 27 | Riyadh Alshamsan et al [60] | 2011 | Cross-sectional study |
UK | 6690 | N | ||
| 28 | Rohini Mathur et al [61] | 2018 | Observational cohort study |
99648 | 25-85 | N | ||
| 29 | Stephanie L. Prady et al [62] | 2016 | Cross sectional |
UK | 2234 | 26.8 | N | |
| 30 | SARAH A. AFUWAPE et al [63] | 2006 | Retrospective cohort |
UK | 213 | 37 | N | |
| 31 | Emma Barron et al [64] | 2020 | Cross sectional |
UK | 61414470 | 40.9 | N | |
| 32 | Jayati Das-Munshi et al [65] | 2021 | Longitudinal study | England |
56770 | 63 | Y | |
| 33 | Kenneth A. Earle et al[64] | 2001 | Retrospective case note review |
UK | 45 | 66 | N | |
| 34 | Rebecca Pinto et al[65] | 2010 | Cross-sectional study |
England |
1090 | 46.8 | 16-74 | N |
| 35 | Linda Petronella Martina Maria Wijlaars et al [66] | 2018 | Cross-sectional study |
England |
763 199 | 10月24日 | N | |
| 36 | A. Head et al[67] | 2021 | Descriptive epidemiology |
England |
1.000.000 | 46 | N | |
| 37 | A. Head et al[68] | 2021 | Descriptive study |
England |
991 243 | 18-81 | Y | |
| 38 | M. A. Hussain et al[69] | 2015 | Cross-sectional study |
Indonesia |
9438 | 40-100 | Y | |
| 39 | Calypse B Agborsangaya et al [70] | 2012 | Cross-sectional survey | Canada |
5010 | 46.7 | 18-80 | Y |
| 40 | C. A. Jackson et al[71] | 2016 | Longitudinal Study |
Australian |
4896 | 49.5 | N | |
| 41 | A. G. Jantsch et al[72] | 2018 | Cross-sectional | Brazil |
3092 | 41.3 | 24-69 | Y |
| 42 | N. Jerliu et al [73] | 2013 | Cross-sectional | Kosovo |
1890 | 73.4 | 65-100 | Y |
| 43 | M. C. Johnston et al [74] | 2019 | Prospective cohort study | Scotland |
12 150 | 48 | Y |
|
| 44 | S. V. Katikireddi et al [75] | 2017 | Cohort study |
Scotland |
12743 | N | ||
| 45 | T. Keller et al [76] | 2018 | Cohort study |
the Netherlands, , Sweden, Denmark, and German | 19 013 | N | ||
| 46 | A. R. Khanolkar et al[77] | 2021 | Cohort study |
3723 | N | |||
| 47 | G. Knies et al[78] | 2022 | Longitudinal, nationally representative study | UK | 28523 | 16-100 | Y | |
| 48 | R. Kunna et al [79] | 2017 | China and Ghana |
15864 | 18-100 | Y | ||
| 49 | R. N. Kuo et al [80] | 2013 | Longitudinal study |
Taiwan | 959990 | N | ||
| 50 | N. E. Lane et al [81] | 2015 | Retrospective cohort |
Canada | 1518939 | 75.5 | N | |
| 51 | K. D. Lawson et al [82] | 2013 | Cross-sectional |
Scotland | 7054 | N | ||
| 52 | J. Lu et al [83] | 2021 | Cross-sectional |
China | 7480 | 70.79 | 60-100 | Y |
| 53 | R. McQueenie et al [84] | 2019 | National retrospective |
Scotland |
824374 | N | ||
| 54 | S. W. Mercer et al [85] | 2018 | Secondary cross-sectional |
UK | 659 | 51.2 | 18-100 | Y |
| 55 | L. Mondor et al [86] | 2018 | Cross-sectional |
Canada |
113627 | 18-100 | Y | |
| 56 | C. R. Nielsen et al [87] | 2017 | Cross-sectional | Austria, Germany, Sweden,Netherlands, Spain, Italy, France, Denmark, Switzerland,Belgium, Czech Republic, Luxembourg, Slovenia, Estonia andIsrael |
63842 | 50-100 | Y | |
| 57 | M. Niksic et al [88] | 2021 | Cohort study |
Spain | 1259 | 68.4 | 18-100 | Y |
| 58 | B. P. Nunes et al [89] | 2020 | Cross-sectional |
Brazil | 9412 | 50-100 | Y | |
| 59 | Z. Or et al [90] | 2021 | The analysis is based on patient-level linked routine data sources onhealth care |
Australia, Canada, England, France, Germany, New Zealand, Spain, Switzerland, and the United States |
56364 | 65-90 | N | |
| 60 | J. F. Orueta et al [91] | 2013 | Cross-sectional |
Basque Country |
452698 | N | ||
| 61 | B. Perera et al [92] | 2020 | Anecdotal analysis |
UK | N | |||
| 62 | S. Reilly et al [93] | 2015 | Retrospective cohort |
UK | 346 551 | N | ||
| 63 | B. Reis-Santos et al [94] | 2013 | Cross-sectional | Brazil |
39881 | 20-60 | Y | |
| 64 | G. Q. Romana et al [95] | 2020 | Cross-sectional,observational, epidemiological |
Portugal |
4911 | N | ||
| 65 | B. L. Ryan et al [96] | 2018 | Cross-sectional | Canada |
13581191 | 39.6 | 0-105 | Y |
| 66 | L. Singer et al [97] | 2019 | Longitudinal Study |
England |
7,130( | 66(10.9) | 50-100 | N |
| 67 | A. Singh-Manoux et al [98] | 2018 | Cohort study |
UK | 8270 | 50.2 | N | |
| 68 | D. J. Smith et al [99] | 2013 | Cross sectional | UK |
1751841 | 54.5 | Y | |
| 69 | M. J. Smith et al [100] | 2021 | Multilevel cohort study |
England |
45414 | N | ||
| 70 | S. K. R. van Zon et al [101] | 2020 | Longitudinal cohort |
US | 10719 | 53.8 | 50-64 | Y |
| 71 | H. M. Vasiliadis et al [102] | 2021 | Longitudinal cohort |
Canada |
1570 | N | ||
| 72 | C. Violan et al [103] | 2014 | Cross-sectional |
Spain | 1356761 | 47.4 | 19-100 | Y |
| 73 | X. L. Xu et al [104] | 2018 | Cohort study |
Australia |
11914 | 47.7 | 45-50 | Y |
| 74 | Y. Zhao et al [105] | 2020 | Population-based, panel data analysis | China | 11 817 | 62 | 50-100 | Y |
| 75 | Z. Zhou et al [106] | 2021 | A two-stage cluster sampling method | China |
64, 395 | 60 | 5-98 | Y |
| 76 | Aarts et al [107] | 2012 | Cohort study |
Netherlands |
1184 | 55.4 | 24-81 | Y |
| 77 | Aarts et al [108] | 2011 | Cross-sectional |
Netherlands |
15188 | 70 | 55-90 | N |
| 78 | Aarts et al [109] | 2011 | Prospective study |
Netherlands |
1763 | 55.4 | 24-81 | Y |
| 79 | Abizanda et al [110] | 2014 | Cohort study |
Spain | 842 | 78.6 | 70-100 | N |
| 80 | Agborsangaya et al [111] | 2012 | Cross-sectional |
Canada |
4752 | 47.7 | 18-90 | Y |
| 81 | Agborsangaya et al [112] | 2013 | Cross-sectional |
Canada | 4946 | 46.6 | 18-85 | Y |
| 82 | Agborsangaya et al [113] | 2013 | Canada |
4752 | 47.7 | 18-100 | Y |
|
| 83 | Ahrenfeldt et al [114] | 2019 | Cohort Study |
Europe |
49946 | 66.25 | N | |
| 84 | Alimohammadian et al [115] | 2017 | Cohort Study | Iran |
49946 | 40-75 | Y | |
| 85 | Angst et al [116] | 2002 | Prospective cohort |
Switzerland |
591 | N | ||
| 86 | Linda Juel Ahrenfeldt et al [117] | 2019 | Cross-sectional |
Europe |
244258 | 66.25 | N | |
| 87 | Ayesha A Appa et al [118] | 2014 | Multiethnic cross-sectional cohort |
USA | 1997 | 60.2 | Y | |
| 88 | Mary L Adams et al [119] | 2017 | USA | 400000 | N | |||
| 89 | Thatiana Lameira Maciel Amaral 1 [120] | 2018 | Cross-sectional | Brazil |
264 | 60-100 | Y | |
| 90 | Keun Ok An et al [121] | 2016 | Cross-sectional |
South Korea |
10118 | 54.8 | N | |
| 91 | Diane Arnold-Reed et al [122] | 2018 | Retrospective cohort study |
Australia |
4285 | 38.2 | 18-90 | Y |
| 92 | Perianayagam Arokiasamy et al [123] | 2015 | China, Ghana, India, Mexico, Russia, South |
42236 | 18-100 | Y | ||
| 93 | Judith Sinnige et al [124] | 2015 | Netherlands |
120480 | 66.9 | 55-80 | Y | |
| 94 | Dawit T Zemedikun et al [125] | 2018 | Cluster analysis |
UK | 502643 | 58 | 40-69 | Y |
| 95 | Luke T A Mounce et al [126] | 2018 | Cohort | UK |
4564 | 50-100 | Y | |
| 96 | Anne W Taylor et al [127] | 2010 | logistic regression |
Australia |
3206 | 20-80 | Y | |
| 97 | Davy Vancampfort et al [128] | 2019 | Cross-sectional |
Multiple continents |
34129 | 62.4 | N | |
| 98 | Davy Vancampfort et al [129] | 2018 | Cross-sectional study |
Multiple continents |
14585 | 72.6 | 65-100 | Y |
| 99 | Carole E Aubert et al [130] | 2016 | Cross-sectional |
Switzerland |
1002 | 63.5 | 50-80 | Y |
| 100 | Christine S Autenrieth et al [131] | 2013 | Cross-sectional |
Germany |
1007 | 75.7 | 65-94 | Y |
| 101 | Caroline Bähler et al [132] | 2015 | Observational study | Switzerland |
229493 | 74.9 | 65-100 | Y |
| 102 | Davy Vancampfort et al [133] | 2017 | Cross-sectional |
44 low and middle income countries |
194431 | 38.3 | N | |
| 103 | Sarah Bernard et al [134] | 2016 | Prospective cohort |
Australia |
306 | 81.8 | 65-105 | Y |
| 104 | Tuhin Biswas et al [135] | 2019 | Cross-sectional |
Bangladesh |
8763 | 35-100 | N | |
| 105 | Amy Blakemore et al [136] | 2016 | Prospective cohort design |
UK | 4377 | 75 | N | |
| 106 | Bowling C B et al [137] | 2019 | Cross-sectional |
USA | 4217 | 56.7 | 50-64 | Y |
| 107 | Helena C Britt et al [138] | 2021 | Secondary analysis of data from a sub studyof the BEACH (Bettering the Evaluation AndCare of Health) |
Australia |
9156 | N | ||
| 108 | Paula Broeiro-Gonçalves et al [139] | 2019 | Cross-sectional | Portugal | 800376 | 59.8 | N | |
| 109 | Jako S Burgers et al [140] | 2010 | France, Germany, Canada, Australia, Netherlands, New Zealand,UK, USA | 8973 | N | |||
| 110 | Bianca M Buurman et al [141] | 2016 | Prospective cohort | The Netherlands | 639 | 78.2 | N | |
| 111 | Amaia Calderón-Larrañaga et al [142] | 2017 | Sweden | 3363 | 74.6 | N | ||
| 112 | Marco Canevelli et al [143] | 2020 | Italy | 185 | 75.1 | N | ||
| 113 | Alanna M. Chamberlain et al [144] | 2020 | USA | 198941 | N | |||
| 114 | He Chen et al [145] | 2018 | China | 30774 | N | |||
| 115 | Tsun-kit Chu et al [146] | 2018 | Retrospective cross-sectional study | China | 382 | N | ||
| 116 | Yogini V. Chudasama et al [139] | 2019 | Longitudinal study | UK |
491939 | 58 | 18-100 | Y |
| 117 | Cristina Cimarras-Otal et al [147] | 2014 | Cross-sectional | Spain | 22190 | N | ||
| 118 | Weng Yee Chin et al [148] | 2016 | Cross-sectional | China | 9259 | 48 | 18-100 | Y |
| 119 | Sutapa Agrawal et al [149] | 2016 | Cross-sectional | India, China, Russia, Mexico,South Africa, Ghana | 40166 | 57.8 | N | |
| 120 | Jane M Gunn et al [150] | 2012 | Cross-sectional | Australia | 6864 | 50.89 | 18-76 | Y |
| 121 | Han MA et al [151] | 2013 | Cross-sectional | USA | 159 | 76 | Y | |
| 122 | Peter Hanlon et al [152] | 2018 | Prospective, population-based cohort study | UK | 493737 | 37-73 | N | |
| 123 | Adelson Guaraci Jantsch et al [153] | 2018 | Cross-sectional | Brazil | 3092 | 42 | N | |
| 124 | D Jovic 1, J Marinkovic 2, D Vukovic 3 [154] | 2016 | Secondary data analysis | Serbia |
13103 | 49.4 | 20-100 | Y |
| 125 | Helle Gybel Juul-Larsen et al [155] | 2020 | Longitudinal prospective cohort | Denmark | 369 | N | ||
| 126 | Catherine Hudon et al [156] | 2008 | Secondary analysis | Canada | 16782 | N | ||
| 127 | Kenya Ie et al [157] | 2017 | A cross-sectional | USA | 1084 | N | ||
| 128 | Tatsuro Ishizaki et al [158] | 2019 | Japan |
2525 | 76.9 | 60-100 | Y | |
| 129 | Hendrik Dirk de Heer et al [159] | 2013 | A stratified, two-stage, randomized, cross-sectional health survey | Mexico | 1002 | 47.72 | 18-100 | Y |
| 130 | Anahit Demirchyan et al [160] | 2013 | Armenia | 721 | 58.8 | N | ||
| 131 | Elisa Fabbri et al [161] | 2015 | Cross-sectionally | Italy | 695 | 72.3 | 60-95 | Y |
| 132 | G G Fillenbaum et al [162] | 2000 | Longitudinalstudy | USA | 4034 | 73.44 | 64-100 | Y |
| 133 | Jihun Kang et al [163] | 2017 | Cross sectional | South Korea | 590 | 32.2 | 20-80 | Y |
| 134 | Christopher Harrison et al [164] | 2014 | Cross sectional | Australia | 8707 | 20-89 | Y | |
| 135 | Nusrat Khan et al [165] | 2019 | Cross sectional | Bangladesh |
12 338 | 58.6 (SD ±9.2) years | 35-100 | Y |
| 136 | Masuma Akter Khanam et al [166] | 2011 | Cross sectional | Bangladesh |
452 | 60-100 | Y | |
| 137 | Dana E King et al [167] | 2018 | Cross-sectional | USA |
57303 | 20-100 | Y | |
| 138 | Krupa Gandhi et al [168] | 2017 | Cross-sectional | USA | 9499 | 20-80 | Y | |
| 139 | Myles Gaulin et al [169] | 2019 | Retrospective cohort | Canada | 5 316 832 | 51.2 ± 17.93 | N | |
| 140 | Debora Rizzuto et al [170] | 2017 | Population-based cohort study. | Sweden | 1099 | 78-100 | Y | |
| 141 | Nafeesa N Dhalwani et al [171] | 2017 | Longitudinal Study | UK |
5476 | 61 | 50-100 | Y |
| 142 | Sophie Excoffier et al [172] | 2018 | Longitudinal Study | UK | 56.5 (20.5 | N | ||
| 143 | Martin Fortin et al [173] | 2014 | Cross sectional | Canada | 1196 | 57.8 | 45-80 | Y |
| 144 | Henrike Galenkamp et al [174] | 2011 | Longitudinal Study | The Netherlands | 2046 | 69.2 | N | |
| 145 | Lori M Gawron et al [175] | 2020 | Retrospective cohort study | USA | 741612 | N | ||
| 146 | Rima R. Habib et al [176] | 2014 | Cross-sectional | Lebanon | 2501 | 46.6 | N | |
| 147 | Christopher Harrison et al [175] | 2017 | Cross-sectional | Australia | 8707 | N | ||
| 148 | Samah Hayek et al [176] | 2017 | Australia | 8707 | N | |||
| 149 | Debra E Henninger et al [177] | 2012 | Cross-sectional | USA | 3212 | 76 | 68-100 | Y |
| 150 | Belinda Hernández et al [178] | 2019 | Ireland | 6101 | N | |||
| 151 | Cyrus Sh Ho et al [179] | 2014 | Cross-sectional and longitudinal | Singapore | 1844 | 66.15 | N | |
| 152 | Andrew Kingston et al [180] | 2018 | Dynamic microsimulation model | 9723900 | N | |||
| 153 | Ai Koyanagi et al [181] | 2018 | Cross-sectional, | China, Ghana, India, Mexico, Russia, andSouth Africa |
32715 | 62.1 | 50-100 | Y |
| 154 | Didi M W Kriegsman et al [182] | 2004 | Longitudinal design | Netherlands | 2489 | 69.2 | 55-85 | Y |
| 155 | Kaja Kristensen et al [183] | 2019 | Cross-sectional | Germany | 7604 | 64.37 | 40-80 | Y |
| 156 | Kaja Kristensen et al [184] | 2019 | Longitudinal | Germany | 19605 | 63.47 | 40-80 | Y |
| 157 | Francisco T T Lai et al [185] | 2019 | Sex-specific age-period-cohort analysis with repeated cross-sectional surveys. | Hong Kong (SAR of China | 69 636 | N | ||
| 158 | Francisco T T Lai et al [186] | 2019 | Prospective | Hong Kong (SAR of China |
300 | 18-77 | Y | |
| 159 | P A Laires, J Perelman [187] | 2018 | Cross-sectional | Portugal |
15196 | 25-79 | Y | |
| 160 | Kathleen Lang et al [188] | 2015 | Cross-sectional, | USA | 3058 | 53.4 | 40-64 | Y |
| 161 | C Le Cossec et al [189] | 2016 | Cross-sectional | France | 15325 | 70 | N | |
| 162 | Todd A Lee et al [190] | 2007 | Cohort study | USA | 741847 | N | ||
| 163 | Wei-Ju Lee et al [191] | 2018 | Taiwan |
20898 | 65-100 | Y | ||
| 164 | Sanja Lujic et al [192] | 2017 | cohort study | Australia | 90352 | 70.2 | 45-80 | Y |
| 165 | Francisco Lupiáñez-Villanueva et al [193] | 2018 | Cross-sectional | 14 European countries | 14000 | N |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



