
Submitted:
22 August 2023
Posted:
23 August 2023
You are already at the latest version
Abstract
(1) Background: The aim of this study was to identify predictors of the unmet health care needs during the financial and recent health crisis in Greece. (2) Methods: Time series analysis was performed for the years 2008 through 2022 using the Eurostat database. The dependent variable was the percentage of people who reported unmet need for medical care. Demographic, socioeconomic and health data as well as health expenditures were used as independent variables. Correlation analysis and simple linear regression models were conducted to analyze the results. (3) Results: Unmet health needs in Greece increased from the start of the crisis until 2016, as a gradual de-escalation of the crisis is observed. However, in 2019 the country recorded the second highest level of unmet needs for medical care before the health crisis. People with limitations in usual activities, those who report bad/very bad health status, unemployed and with low-income increased the likelihood of unmet needs. Health expenditures (public or private) were also significant determinants of unmet healthcare needs. (4) Conclusions: The increased unmet health needs widen inequalities in health and healthcare access. Therefore, health policy should eliminate barriers which restrict the access to health and enhance healthcare services, developing conditions for citizens' well-being.
Keywords:
healthcare
; unmet healthcare needs
; economic crisis
; health crisis
; Greece
1. Introduction
Social needs contain the concept of health requirements, however, these needs cannot be identified objectively, either they are subjective requirements of every person, or the collective needs of society that emerge based on objective standards of prioritizing and assessment. The coverage of social requirements is balanced between the necessity for the long-term viability of social systems and the social costs, resulting from the non-satisfaction of social demands and taking into consideration the restrictions of the resources and budget [1,2].
Bradshaw divided need into several different categories after taking these limitations and assessment challenges into account: "normative need" as "desired standard" or "objective," whereas "felt need" is synonymous with desire and "expressed need" is associated with demand [3]. Moreover, according to European Union (EU) the unmet health needs are defined as the percentage of people that require healthcare but have reported a delay in receiving it in the twelve months prior to the incident. The EU claims that the following elements are contributing to unmet health needs: a) high costs for services; b) geographic distance and transportation issues; and c) slow system responses and waiting lists. The limitations on access to health services offered by the State include all of the above factors. However, the demand for health care persists and does not go away, which has the effect of either manifesting later as a major sickness or forcing the person to pay for it privately [4]. The examination and the evaluation of health needs are important as they constitute the basis for figuring out how health services are offered, and they basically constitute market research for the development of services as a public benefit that will be accessible to all individuals without social exclusion [5].
The health systems in Europe were greatly strained by the pandemic, with resources being redirected to manage the crisis and people being advised to stay home to prevent the spread of the virus. As a result, many health services were impacted during the early stages of the pandemic and during its most severe periods [6]. Thus, this disruption of health services led to the increase of unmet healthcare needs.
Most of the population in EU countries reported that they had no unmet medical care needs for financial reasons, geographic reasons or waiting times in 2018 or 2019, based on EU-SILC [7]. The extent of unmet health care needs has been dramatic, although it has differed across various types of care throughout the pandemic's duration. Approximately 20% of people across EU countries stated that forgone medical care during the first wave of the pandemic, and nearly a fifth of respondents (18%) reported having a medical issue for which they had not yet received examination or treatment in spring 2022. Regarding the access to hospital or specialist care half of the EU population in 2020 and more than two fifths in 2021 reported obstacles. Overall, unmet medical care needs remained high in 2021 and 2022 [8].
As far as dental care is concerned, during the pandemic, there was a disturbance in obtaining dental care, and more than 25% people in the EU experienced unmet needs in 2021 and 2022. An explanation may be that dental care is not fully covered in public health schemes in several countries, necessitating out-of-pocket expenses or the of private health insurance [9].
The pandemic has led to growing unmet needs for mental health care, even though there was a rapid adaptation to new service formats such as online therapy and several measures which were taken by EU countries to increase mental health support. The percentage of Europeans adults who reported some unmet needs for mental care increase from 20% in 2021 to 23% in 2022 [8]. Worries arise for young Europeans people, as 53% reported unmet needs for mental health care in 2021, with a slightly decrease in 2022 (49%). However, the situation was exacerbated during the pandemic, as a large proportion of people seeking mental health care reported difficulties obtaining it in the previous years [10].
Greece presents a unique setting in which to analyse inequalities in access to health care services. The repercussions of a financial and recent health crisis have been a challenge for country to handle [11]. GDP per capita was estimated at €18.310 in 2011, decreased at €16.270 in 2014 and in 2022 was €19.670 [12]. Public health expenditures are one area being contained as part of fiscal sustainability measures. More specifically, public expenditures were estimated at €12.3 billion in 2011, which decreased at €8.1 billion in 2014 and reached to €9.7 billion in 2020 (latest data) due to the needs by the pandemic [13]. A steady increase in public health expenditures has been observed beginning to the year 2015. Private expenditures were estimated at €6.4 billion in 2011, which decreased slightly at €5.9 billion in 2014 and remained approximately €6 billion in 2020 accordingly [13]. Private health care expenditures are still expensive, up to 30% over the average across Europe.
The purpose of this research was to present the unmet medical needs during the financial and recent health crisis in Greece by income quintile, region (NUTS 2), occupational status compared with European Union 27, and to identify predictors of the unmet health care needs within the population of the country.
The selection of predictors of the unmet health care needs was based on the international literature. More specifically, females [14], younger people [14], people with chronic conditions [15], and people with bad health status [16] have been shown to be more likely to self-report unmet healthcare needs. Empirical evidence indicates that people with low income have greater healthcare needs [17-19]. Additionally, several studies have provided significant evidence regarding economic activity status related inequalities in unmet healthcare needs. Unemployed or self-employed people were more likely to report unmet healthcare needs in comparison with employees [20,21]. Finally, political circumstances and economic crises were shown to affect unmet healthcare needs of population [22,23].
2. Materials and Methods
This research was a cross-sectional study and represented a secondary analysis of data obtained from Eurostat database [24]. The analysis used time series from 2008 to 2022 and the following indicators were processed, as shown in Table 1.
2.1. Statistical Analysis
The examination of the directional relationship between the unmet medical needs and the above-mentioned indicators, a correlation analysis was conducted using the Pearson correlation coefficient. Indicators which were corelated with unmet medical needs, were used as the independent variables in the simple linear regression models. Eight linear regressions models were performed. The results were considered statistically significant when the p value was ≤0.05. The analysis was performed using the Statistical Package for Social Sciences (SPSS) version 25.
3. Results
3.1. Unmet medical health needs in Greece versus EU27
EU Member States increased access to healthcare significantly between 2005 and 2009. Specifically, the number of those indicating an unmet need for healthcare due to cost, travel distance, or length of wait declined steadily from 24 million in 2005 to 15 million in 2009. This increasing tendency has changed since 2009, showing an evident indication of the destruction caused by the financial and economic crisis. In 2013, 18.6 million individuals (4% of the EU's population) expressed unmet healthcare needs. Regarding Greece's unmet health needs in 2010, there was little distinction compared to those of the EU27; however, during the country's economic crisis, the gap sharply grew from 2011 to 2016. Greece exhibited triple the total number of inadequate needs compared to the EU27 nations. The proportions in Greece have been gradually declining since 2017, though they remain very high when compared to the other EU27 countries (Figure 1).
According to Eurostat (2021) [25], the main reason given for unmet health needs in EU27 are financial reasons, distance or transportation, waiting list (25.5%), following by waiting list (19.4%), financial reasons (13%) and distance or transportation (4%). The Greek data are not differ; financial reasons, distance or transportation, waiting list (19.7%), financial reasons (14.4%), waiting list (12.5%) and distance or transportation (5%).
3.2. Unmet dental health needs
Until the year 2015, about 5% of the EU27 population experienced unmet dental care needs, however the percentage decreased to only 3% in 2019 (latest data). This percentage is comparatively large in Greece during economic and health crisis, reaching 14.9% in 2014 and 12.1% in 2022 (Figure 2).
3.3. Greece's unmet medical health needs, by region
Throughout Eastern Macedonia & Thrace region, approximately 10% of the population stated that they experienced unmet health needs. High percentages are shown for the Northern Aegean, Northern Greece, and Central Macedonia. Τhe percentage of unmet needs in Attica is interesting (6.6%), knowing that the majority of secondary and tertiary hospitals have are located in this region. The regions with the lowest percentages of unmet needs (<5%) are Ionian islands, Crete, Western Macedonia, Thessalia and Western Greece (Figure 3).
3.4. Unmet medical health needs in Greece versus EU27, by income quintile
The percentage of unmet needs declines as an individual's income rises in the upper quartile. The first and second quartiles tend to have the greater percentages of unmet needs in comparison with the rest quartiles. Approximately 27% of Greek population in the first and second quartiles stated unmet medical needs comparatively with the 6.5% of EU27 population (Figure 4).
3.5. Greece's unmet medical health needs, by occupational status
Regarding the distinction between employed and unemployment rates, it is important to mention that the rate of unemployment in Greece was approximately double in comparison to the other EU27 countries. However, it appears that in Greece, during the recession and health crisis, approximately 12.5% of the unemployed people and just 5% of employed stated that they had unmet medical needs, in relation to EU27, where about 4.6% of the unemployed and only 1.7% of employed people experienced unmet needs (Figure 5).
3.6. Comparative effect sizes of key variables predictive of unmet needs
The analysis results, based on Eurostat database, showed that there is a significant positive correlation between unmet medical needs and bad/very bad self-perceived health (r = 0.786), some/severe self-perceived long-standing limitations in usual activities due to health problem (r = 0.681) and unemployment rate (r = 0.599), showing that an increase of bad/very bad health status, some/severe limitations and unemployment corresponds to a simultaneous increase in unmet medical needs (Table 2). On the contrary, unmet needs correlated negatively with private health expenditures (r=-0.682), public health expenditures (r=-0.765), very good/good health status (r=-0.793), real GDP per capita (r=-0.632) and employment rate (r=-0.615), showing that an increase of private and public health expenditures, very good/good health status, GDP per capita and employment corresponds to a simultaneous decrease in unmet medical needs (Table 2).
In the Table 3 is presented the linear regression models regarding the predicted factors of unmet medical needs.
4. Discussion
To our knowledge, the present study is a first attempt to identify factors associated with self-perceived unmet needs during the economic and health crisis in Greece. The study, that records unmet needs in the health sector, is an essential indicator of how effectively the system has reached the wider social strata in terms of access to quality health services and in capturing the gap between the range of services required to satisfy different people's needs and the services that are actually provided.
Our analysis indicated that approximately 1 out of 10 citizens of Greece had unmet health care needs in the last decade, which are much higher in comparison to the other 27 European countries. During the economic crisis in Greece, it is observed that twice as many people experienced unmet health needs until 2016, when the Law 4368/2016 provided the possibility for all people (regardless of insurance or not) to receive free of charge public health services, with the same copayment in the cost of medical care or drugs [26]. However, this reduction did not last long, as due to the pandemic the country mobilised health care resources to respond this urgent situation.
When it concerns unmet health needs, dental care is one of the most serious ones. More than 10% of people in Greece reported unmet needs for dental care in last decade, mainly for financial reasons. Public coverage for dental care costs is far more limited, due to restricted service packages and high levels of cost-sharing [27,28]. On average, only one-third of total costs are borne by government schemes or compulsory insurance. In Greece the level of compulsory coverage is very low so consumers must pay significant out-of-pocket costs for dental care services, that are not part of the healthcare bundle [28].
Regional inequality of access to basic health services is significantly present in Greece. People living in remote regions and isolated islands encounter difficulties in reaching specialized medical practitioners and specialized laboratories [29]. As a result, citizens, particularly those facing health issues, are compelled to relocate to urban areas where suitable healthcare services are accessible. Consequently, the availability of healthcare depends on the individual's place of residence and their proximity to appropriate facilities. This is consistent with our analysis that the region of Eastern Macedonia & Thrace had the highest frequency of unmet health care needs, as well as the islands of the Aegean. Surprisingly, in spite of the region of Attica's extensive concentration of hospitals, it is also observed that there are still considerable unmet health needs. This also seems to be in line with the literature's assertion that unmet health needs in home chronic care are affected by the lack of individualized flexible health services and caregiver networks. Private providers and the one-dimensional perception of the patient's treatment with medicine and prescription only leading in rising private health expenditures, fill the gap in primary health care services. A component of the Greek experience throughout the crisis appears to be linked to the literature's conclusion.
Plethora of international studies has proven that the burden of unmet needs for health care fall mostly on people from low-income households [30-32]. This is in accordance with our results, that in Greece more than 13% in the low income quintiles reported going without some medical care when they needed it in 2022 compared with only 1% among the high income quintiles. Cost was the main reason for these unmet needs. Moreover, our analysis showed that increasing disposable income decreased the likelihood of unmet health care needs, which has been well documented in other countries with universal health care coverage [19, 33,34]. In another similar study, it is mentioned that funding reduction in periods of crisis has a negative impact on access to healthcare, due to the increasing demand for services affecting waiting times, co-payments and informal payments [35].
Furthermore, our analysis displays that unemployment is a major risk factor of unmet medical needs. Although unemployed people in Greece have free access to healthcare services, problems regarding the use of health care have not been overcome [36,37]. Corresponding European studies agree with these results and point out that vulnerable groups, such as the unemployed, are more at risk of reduced access to health services, resulting in an increase in unmet needs and health inequalities [38,39]. It is a fact that health inequalities are associated with increased income inequality, which is a consequence of a political-economic process, such as unemployment [40]. During crisis, health inequalities widened, with multiplying negative consequences for the unemployed population [41,42]. In line with previous studies, our model found that the probability of experiencing unmet healthcare needs is significantly increased for unemployed people.
Concerning health expenditures, after a period of low growth following the global financial crisis, annual per capita health expenditure growth picked up and reached 3% on average across EU member states between 2013 and 2019. However, in Greece the growth rate was less than 1% and the share of health spending financed through households’ out-of-pocket payments accounted for at least one-third of all health spending [6]. Our analysis indicated that an increase in public and private health expenditures lead to a reduction of population’ unmet health needs. Austerity measures in Greece led to a prolonged decline in the availability of healthcare services and financial security, as evidenced by a rise in unmet healthcare needs and significant expenses incurred due to health crises. According to WHO report, low levels of public spending on health are associated with weak financial protection and high levels of unmet need for health services [43]. Additionally, people with low incomes in Greece cannot afford to pay private health expenditures to fulfill their health needs, which are not covered by the public system, so out-of-pocket payments create a financial barrier to access, resulting in unmet need for health care.
Finally, our results confirmed the claims from the previous studies that the deterioration of the health status and the existence of functional limitations increase the likelihood of unmet needs. This finding coincides with the results of previous studies demonstrated that people claiming to be in good or very good health were less likely to perceive any unmet medical need [44-46]. Moreover, patients suffering from long-term health conditions have frequently stated that their health care needs remain unaddressed, and this situation has worsened as the prevalence of chronic diseases has risen [15, 45]. However, it is worth mentioning the endogeneity between health status and unmet health needs. By focusing on contemporaneous values for unmet needs and health, it is difficult to evaluate the direction of causality between these two dimensions. Existing evidence suggests that unmet health needs in the past, cause a worsening in health status in the present [46-49]. Also, individuals who choose to forgo medical care may later encounter a decline in their overall health condition. Therefore, their health is likely to be severely affected if they do not receive timely and sufficient needed healthcare services and even worse, they are more likely to need expensive inpatient care (such as hospitalization), which will frailer their health. Because of this, associations between aforementioned dimensions cannot be inferred to be causal, but a two-way causality direction.
Limitations of the Study
There are some limitations that merit consideration. All data on unmet health care needs, health status and limitations in usual activities due to health problem is based on self-perception, and therefore they are influenced, to some degree, by the respondents' subjective perceptions and their social and cultural backgrounds. An additional limitation is that data obtained from EU-SILC, which do not cover the institutionalised population (individuals residing in health and social care institutions). This group tends to have poorer health status compared to those living in private households. Consequently, it is probable that both data sources somewhat underestimate the proportion of the population with health issues. However, exclusion of these persons, who receive continuously health care services, might result in an overestimation of unmet healthcare needs.
5. Conclusions
The study's statistics has proven that Greece's unmet health needs rose from the start of the crisis until 2016, extending the country's gap with the average throughout Europe. Moreover, the odds of facing unmet health needs are higher for people with limitations in usual activities, those who report bad/very bad health status, unemployed and people with low-income. The low health expenditures (public or private) consist of significant predicted factor increasing the likelihood of unmet needs. If there are no public health services, preventative care, or flexible primary care services that are focused on the needs of the user, the situation is more severe and destructive.
Data for the Greek reality from Eurostat-EUSILC indicates that improving access to health care is a difficulty challenge. The increase in accessibility depends upon a variety of variables, including the socioeconomic status of the population, the kind of illness, and the availability and flexibility of the service. The various areas of action for preventive treatment and medical services must thus be integrated and ready to work together. By integrating all organizations—public and private—under the common goal of strategic planning, this may be achieved. The aim is to enhance people access to health services and strengthen the basis of society's well-being through the health system being proactive and helpful in their daily lives. Comparative analysis of unmet health needs and documentation of the social and economic characteristics of the population with the greatest unmet social needs lead to new insights and well-supported recommendations for assessing the success of social policies and developing conditions for citizens' well-being.
Author Contributions
Conceptualization, G.P.; A.G. and D.L; Methodology, G.P.; A.G. and D.L; Software, G.P. and D.L; Formal analysis, G.P.; A.G. and D.L; Investigation, G.P.; A.G. and D.L; Resources, G.P. and D.L; Data curation, G.P.; A.G. and D.L; Writing—Original Draft Preparation, G.P.; A.G. and D.L; Writing—Review and Editing, G.P.; A.G. and D.L; Visualization, D.L.; Supervision, G.P. and A.G. Project administration, G.P. and A.G. All authors read and approved the final version of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable
Informed Consent Statement
Not applicable
Data Availability Statement
Not applicable
Acknowledgments
This study was supported by the Postgraduate Health and Social Care Management Programme of the University of West Attica.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Rodriguez, S.; Mason, A.; Gutacker, N.; Kasteridis, P.; Santos, R.; Rice, N. Need, demand, supply in health care: working definitions, and their implications for defining access. Health. Econ. Policy Law. 2023, 18, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Asadi-Lari, M.; Packham, C.; Gray, D. Need for redefining needs. Health Qual. Life Outcomes. 2003, 21, 1–34. [Google Scholar] [CrossRef]
- Bradshaw, J. Taxonomy of Social Need; in: McLachlan, Gordon, (ed.) Problems and progress in medical care : essays on current research, 7th series. Oxford University Press: London, 1972; pp. 71–82. [Google Scholar]
- European Union. Expert Panel on effective ways of investing in Health (EXPH). Report on Access to Health Services in the European Union. Brussels: European Commission, 2016, Available online: https://health.ec.europa.eu/system/files/2019-11/015_access_healthservices_en_0.pdf.
- Eurostat. Methodological issues in the analysis of the socioeconomic determinants of health using EU-SILC data, in Eurostat Methodologies and Working Papers; Publications Office of the European Union: Luxembourg, 2010. [Google Scholar]
- OECD/European Union. Health at a Glance: Europe 2022: State of Health in the EU Cycle. OECD Publishing, Paris, 2022, Available online: https://doi.org/10.1787/507433b0-en.
- OECD/European Union. Health at a Glance: Europe 2022: State of Health in the EU Cycle. Accessibility: Affordability, availability and use of services - Figure 7.1. Unmet needs for medical examination due to financial, geographic or waiting time reasons, 2020. OECD Publishing, Paris, 2022; Available online: https://stat.link/63hqkl.
- Eurofound. Ahrendt, D.; Consolini, M.; Mascherini, M.; et al. Fifth round of the living, working and COVID-19 e-survey: living in a new era of uncertainty. Publications Office of the European Union, 2022. Available online: https://data.europa.eu/doi/10.2806/190361.
- OECD/European Union. Health at a Glance: Europe 2022: State of Health in the EU Cycle. Accessibility: Affordability, availability and use of services - Figure 7.2. Unmet needs for dental examination due to financial, geographic or waiting time reasons, 2020. OECD Publishing, Paris, 2022. Available online: https://stat.link/5k7zg0.
- OECD. A New Benchmark for Mental Health Systems: Tackling the Social and Economic Costs of Mental Ill-Health; OECD Health Policy Studies, OECD Publishing: Paris, 2021; Available online: https://doi.org/10.1787/4ed890f6-en. [Google Scholar]
- Kentikelenis, A. Structural adjustment and health: A conceptual framework and evidence on pathways. Soc Sci Med. 2017, 187, 296–305. [Google Scholar] [CrossRef]
- Eurostat. Main GDP aggregates per capita. 2023. Available online: NAMA_10_PC (accessed on 21 June 2023).
- Eurostat. Health care expenditure by financing scheme. 2023. Available online: HLTH_SHA11_HF (accessed on 21 June 2023).
- Kim, J.; Kim, T.H.; Park, E.C.; Cho, W.H. Factors influencing unmet need for health care services in Korea. Asia Pac. J. Public Health. 2015, 27, NP2555–NP2569. [Google Scholar] [CrossRef]
- Ronksley, P.E.; Sanmartin, C.; Quan, H.; Ravani, P.; Tonelli, M.; Manns, B.; Hemmelgarn, B.R. Association between chronic conditions and perceived unmet health care needs. Open Med. 2012, 6, e48, PMCID: PMC3659214. [Google Scholar]
- Song, H.Y.; Choi, J.W.; Park, E.C. The effect of economic participatory change on unmet needs of health care among Korean adults. Health Policy Manag. 2015, 25, 11–21. [Google Scholar] [CrossRef]
- Lahelma, E.; Martikainen, P.; Laaksonen, M.; Aittomäki, A. Pathways between socioeconomic determinants of health. J. Epidemiol. Community Health. 2004, 58, 327–332. [Google Scholar] [CrossRef]
- Allin, S.; Masseria, C. Unmet need as an indicator of health care access. Eurohealth. 2009, 15, 7. [Google Scholar]
- Mielck, A.; Kiess, R.; von dem Knesebeck, O.; Stirbu, I.; Kunst, A.E. Association between forgone care and household income among the elderly in fiveWestern European countries–analyses based on survey data from the SHARE-study. BMC Health Serv. Res. 2009, 9, 52. [Google Scholar] [CrossRef]
- Baert, K.; De Norre, B. Perception of Health and Access to Health Care in the EU-25 in 2007. Eurostat Statistics in Focus 24/2009. Office for Official Publications of the European Communities: Luxembourg, 2009, p. 1–12. Available online: https://ec.europa.eu/eurostat/documents/3433488/5280869/KS-SF-09-024-EN.PDF.pdf/f4f4f956-eafb-49f6-a52a-4a22d602433c.
- Hernández-Quevedo, C.; Masseria, C.; Mossialos, E. Methodological Issues in the Analysis of the Socioeconomic Determinants of Health Using EU-SILC Data. Office for Official Publications of the European Communities: Luxembourg, 2010, ISBN 978-92-79-16753-3.
- Reeves, A.; McKee, M.; Stuckler, D. The attack on universal health coverage in Europe: Recession, austerity and unmet needs. Eur. J. Public Health. 2015, 25, 364–365. [Google Scholar] [CrossRef]
- Rodrigues, R.; Zolyomi, E.; Kalavrezou, N.; Matsaganis, M. The Impact of the Financial Crisis on Unmet Needs for Healthcare. European Centre for Social Welfare Policy and Research: Brussels, Belgium, 2013.
- Eurostat Database. 2023. Available online: https://ec.europa.eu/eurostat/web/main/data/database.
- Eurostat Database. Self-reported unmet needs for health care by sex, age, specific reasons and educational attainment level. 2021. Available online: hlth_ehis_un1e.
- Law 4368/2016. Measures to speed up government work and other provisions. Government Gazette 21/A/21.2.2016 (chapter Ε1, paper 33).
- Damaskinos, P.; Economou, C. Systems for the provision of oral health care in the black sea countries part 10: Greece. Oral Health Dent Manag. 2012, 11, 3–10. [Google Scholar]
- Damaskinos, P.; Koletsi-Kounari, H.; Economou, C.; Eaton, K.A.; Widström, E. The healthcare system and provision of oral healthcare in European Union member states. Part 4: Greece. Br Dent J. 2016, 220, 253–260. [Google Scholar] [CrossRef]
- Gogos, C.; Papadopoulou, E.; Doukas, I.; Tsolaki, M. Regional Distribution Disparities of Healthcare Resources in Greece. EMSJ. 2022, 6, 4. [Google Scholar]
- Mackenbach, JP.; Stirbu, I.; Roskam, AJR. ; Schaap, MM.; Menvielle, G.; Leinsalu, M.; Kunst, AE. Socioeconomic inequalities in health in 22 European countries. N Engl J Med. 2008, 358, 2468–2481. [Google Scholar] [CrossRef] [PubMed]
- Eikemo, TA.; Huisman, M.; Bambra, C.; Kunst, AE. Health inequalities according to educational level in different welfare regimes: a comparison of 23 European countries. Sociol Health Illn. 2008, 30, 565–582. [Google Scholar] [CrossRef]
- Hu, Y.; van Lenthe, FJ.; Borsboom, GJ. , Looman, C.; Bopp, M.; Burström, B. et al. Trends in socioeconomic inequalities in self-assessed health in 17 European countries between 1990 and 2010. J Epidemiol Community Health. 2016, 0, 1–9. [Google Scholar] [CrossRef]
- Sibley, L.; Glazier, R. Reasons for Self-Reported Unmet Healthcare Needs in Canada: A Population-Based Provincial Comparison. Healthc Policy. 2009, 5, 87–101. [Google Scholar] [CrossRef]
- Levesque, J-F. ; Pineault, R.; Hamel, M.; Roberge, D.; Kapetanakis, C.; Simard, B. et al. Emerging organizational models of primary healthcare and unmet needs for care: insights from a population-based survey in Quebec province. BMC Family Practice. 2012, 13, 66. [Google Scholar] [CrossRef]
- Morgan, D. Astolfi, R. Health Spending Continues to Stagnate in Many OECD Countries. OECD Health Working Papers, No. 68, OECD Publishing, Paris. 2014. https://doi.org/10.1787/5jz5sq5qnwf5-en.
- Altanis, P.; Economou, C.; Geitona, M.; Gregory, S.; Mestheneos, E.; Triantafillou, J. et al. Quality in and Equality of Access to Healthcare Services. Country Report for Greece. European Communities. 2008.
- Minogiannis, P. Tomorrow’s public hospital in Greece: Managing health care in the post crisis era. Social Cohesion and Development. 2016, 7, 7,69–80. [Google Scholar] [CrossRef]
- Maruthappu, M.; Watson, Ra.; Watkins, J.; Williams, C.; Zeltner, T.; Faiz, O. et al. Unemployment, public-sector healthcare expenditure and colorectal cancer mortality in the European Union: 1990–2009. Int J Public Health. 2016, 61, 119–130. [Google Scholar] [CrossRef]
- Lima, J.; Reeves, A.; Stuckler, D. Unmet health need and unemployment during recession in Europe. Eur J Public Health. 2015, 25, 260–261. [Google Scholar] [CrossRef]
- Brydsten, A.; Hammarström, A.; San Sebastian, M. Health inequalities between employed and unemployed in northern Sweden: A decomposition analysis of social determinants for mental health. Int J Equity Health. 2018, 17, 59. [Google Scholar] [CrossRef]
- Latsou, D.; Pierrakos, G.; Geitona, M. (2021). Health and unmet health needs of the unemployed in Greece. Arch. Hell. Med. 2021, 38, 642–650. [Google Scholar]
- Latsou, D.; Geitona, M. Predictors of physical and mental health among unemployed people in Greece. J Health Soc Sci. 2020, 5, 115–126. [Google Scholar]
- WHO Regional Office for Europe Can people afford to pay for health care? New evidence on financial protection in Europe. Copenhagen: WHO Regional Office for Europe. 2019. Available online: https://apps.who.int/iris/handle/10665/311654. 1066.
- Cavalieri, M. Geographical variation of unmet medical needs in Italy: a multivariate logistic regression analysis. Int J Health Geogr. 2013, 12, 27. [Google Scholar] [CrossRef]
- Popovic, N.; Terzic-Supic, Z.; Simic, S.; Mladenovic, B. Predictors of unmet health care needs in Serbia; analysis based on EU-SILC data. PLoS One. 2017, 12, 11–e0187866. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Liu, Q.; Fu, R.; Ma, J. Unmet healthcare needs, health outcomes, and health inequalities among older people in China. Front. Public Health. 2023, 11. [Google Scholar] [CrossRef] [PubMed]
- Aragon, MJA; Chalkley, M. Goddard, M. Defining and Measuring Unmet Need to Guide Healthcare Funding: Identifying and Filling the Gaps. Working Papers. New York, Centre for Health Economics, University of York, 2017.
- Gibson, G.; Grignon, M.; Hurley, J.; Wang, L. Here comes the SUN: Self-assessed unmet need, worsening health outcomes, and health care inequity. Health Econ. 2019, 28, 727–735. [Google Scholar] [CrossRef]
- Ko, H. Unmet healthcare needs and health status: panel evidence from Korea. Health Policy. 2016, 120, 646–653. [Google Scholar] [CrossRef]
Figure 1.
Unmet health needs for medical care in Greece & EU27. Source: Eurostat: 2022 (HLTH_SILC_08).
Figure 1.
Unmet health needs for medical care in Greece & EU27. Source: Eurostat: 2022 (HLTH_SILC_08).
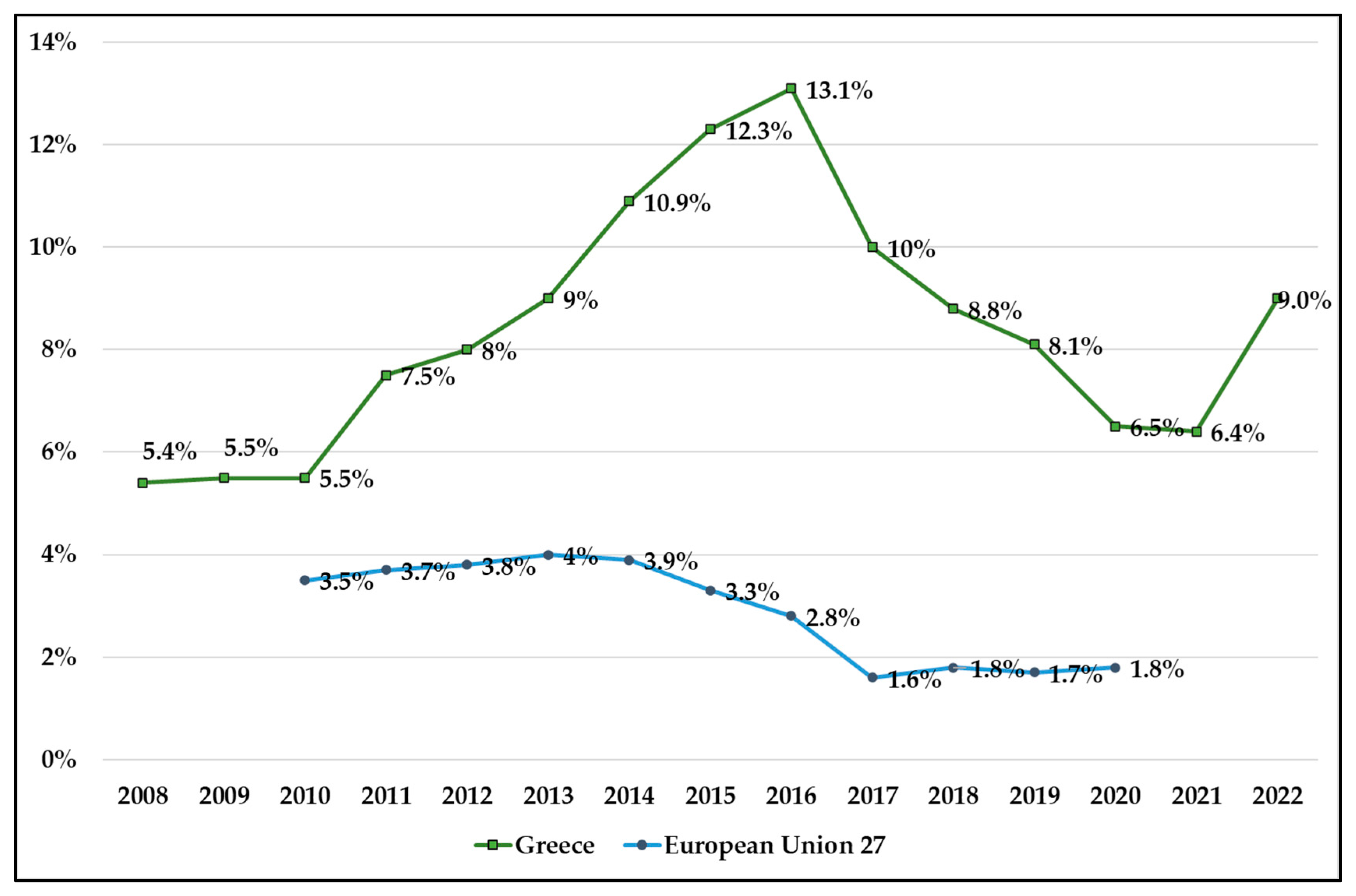
Figure 2.
Unmet dental health needs in Greece & EU27. Source: Eurostat 2022, HLTH_SILC_09.
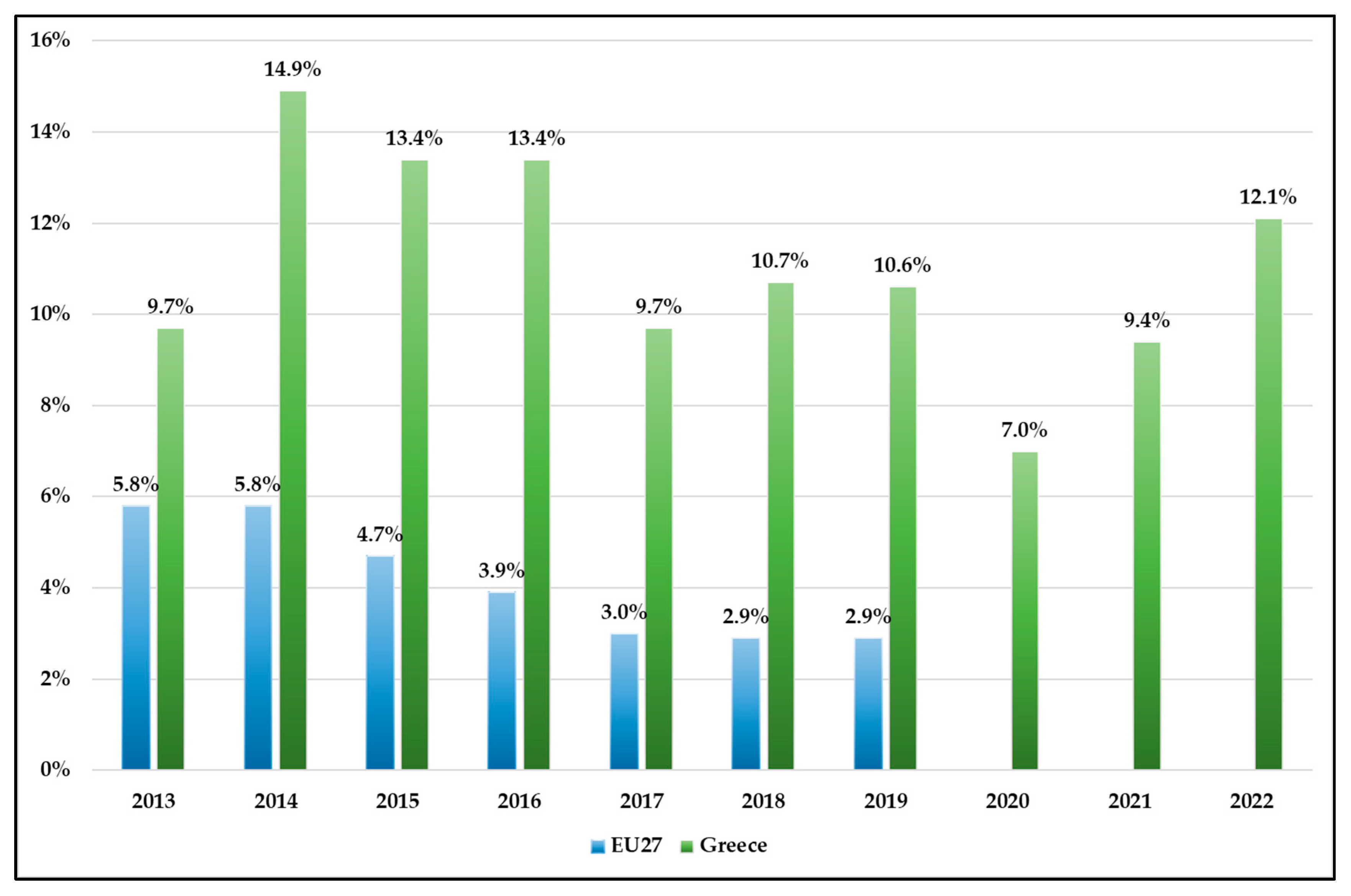
Figure 3.
Unmet medical health needs by region for the year 2020 – Greece. Source: Eurostat 2022 (HLTH_SILC_08_R).
Figure 3.
Unmet medical health needs by region for the year 2020 – Greece. Source: Eurostat 2022 (HLTH_SILC_08_R).
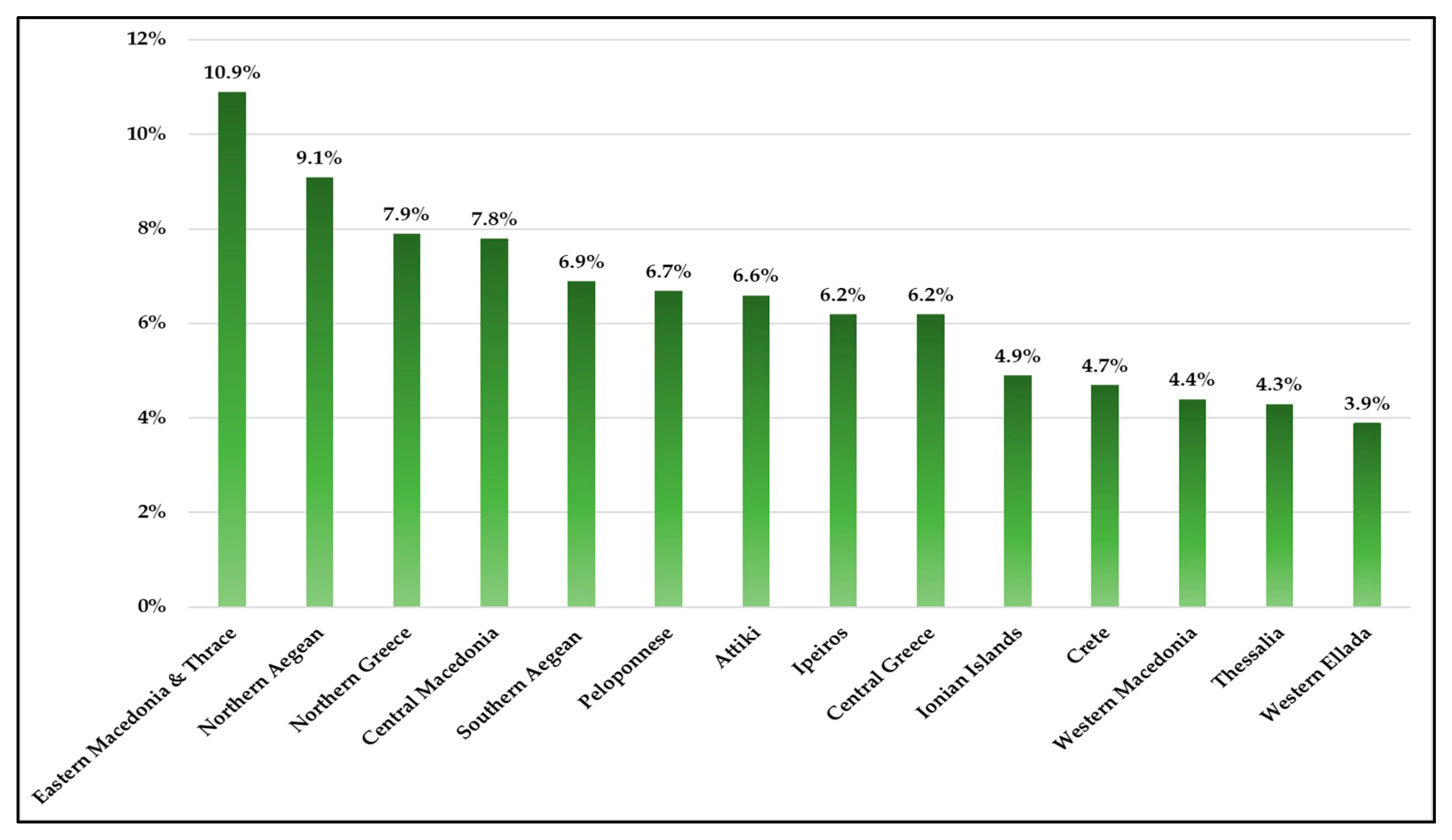
Figure 4.
Unmet health needs for medical care by income quintile in Greece & EU27 (2022). Source: Eurostat: 2023, HLTH_SILC_08.
Figure 4.
Unmet health needs for medical care by income quintile in Greece & EU27 (2022). Source: Eurostat: 2023, HLTH_SILC_08.
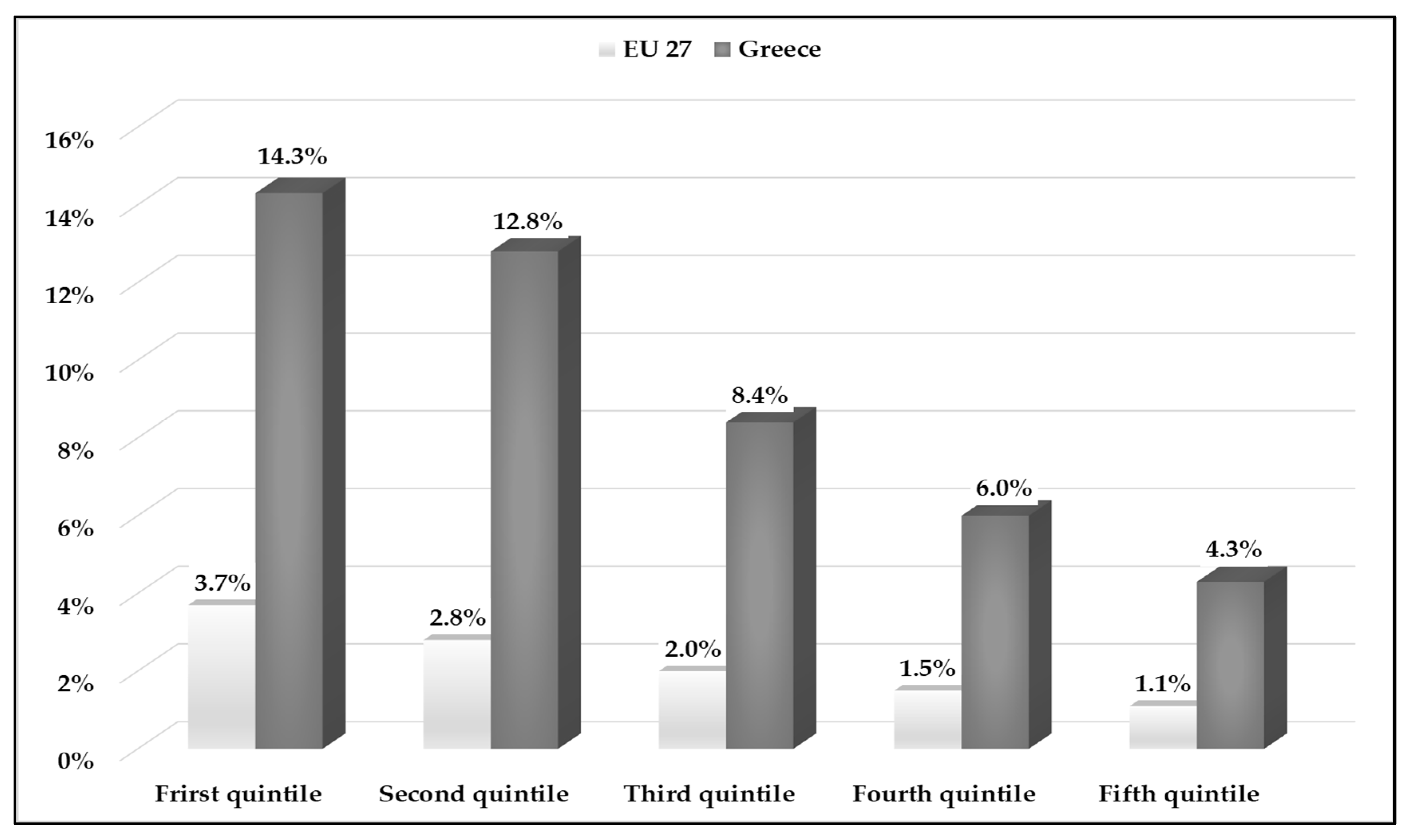
Figure 5.
Employed and unemployed inhabitants's unmet health needs in Greece & EU27. Source: Eurostat: 2022, HLTH_SILC_13.
Figure 5.
Employed and unemployed inhabitants's unmet health needs in Greece & EU27. Source: Eurostat: 2022, HLTH_SILC_13.
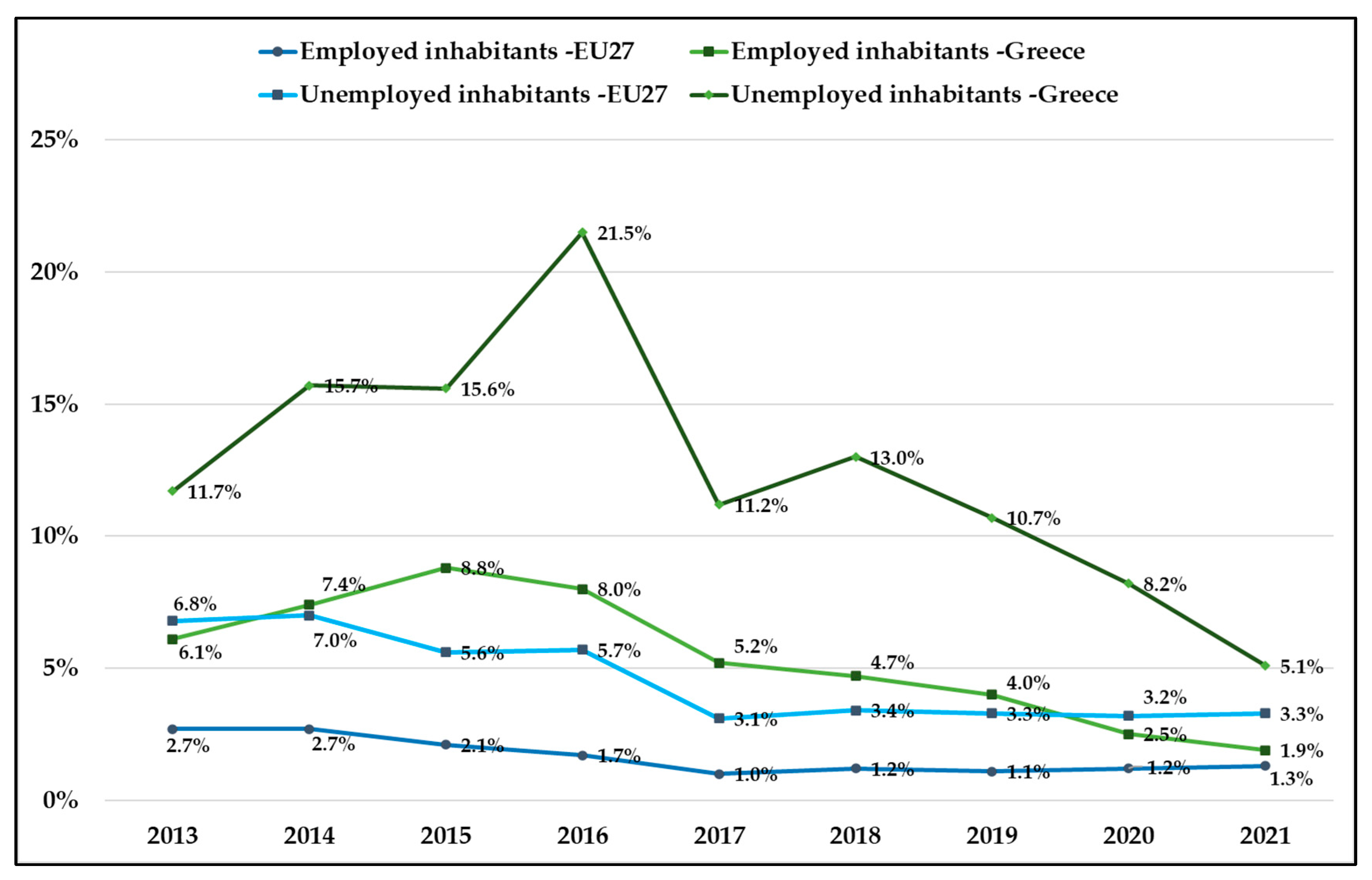

Table 1.
Description of indicators.
| Indicators | Unit | Year | Reference |
|---|---|---|---|
| Self-reported unmet need for medical care (Too expensive or too far to travel or waiting list) | Percentage | 2008-2022 | TESPM110 |
| Gender (Female) | Number | 2013-2022 | DEMO_PJAN__custom_6646580 |
| Gender (Male) | Number | 2013-2022 | DEMO_PJAN__custom_6646561 |
| Household out-of-pocket payment (Private health expenditures) | Million euro | 2012-2021 | HLTH_SHA11_HPHF__custom_6647166 |
| Government schemes and compulsory contributory health care financing schemes (Public health expenditures) | Million euro | 2012-2021 | HLTH_SHA11_HPHF__custom_6647089 |
| Self-perceived health | Percentage | 2013-2022 | |
| (Very good or good) | HLTH_SILC_01__custom_6646803 | ||
| (Fair) | HLTH_SILC_01__custom_6646814 | ||
| (Bad or very bad) | HLTH_SILC_01__custom_6646825 | ||
| People having a long-standing illness or health problem | Percentage | 2013-2022 | HLTH_SILC_04__custom_6647218 |
| Self-perceived long-standing limitations in usual activities due to health problem (Some or severe) | Percentage | 2013-2022 | HLTH_SILC_12$DEFAULTVIEW |
| Real GDP per capita in euro | Number | 2008-2022 | SDG_08_10 |
| Employment rate | Percentage | 2009-2022 | TESEM010 |
| Unemployment rate | Percentage | 2011-2022 | TPS00203 |
Table 2.
Correlation analysis among unmet medical needs and predictors factors.
| Unmet medical needs | ||
| r | p value | |
| Female | 0.418 | 0.229 |
| Male | 0.280 | 0.433 |
| Private health expenditures | -0.682* | 0.014 |
| Public health expenditures | -0.765** | 0.004 |
| Self-perceived health:fair | 0.530 | 0.115 |
| Self-perceived health:bad/very bad | 0.786** | 0.007 |
| Self-perceived health:very good/good | -0.793** | 0.006 |
| Self-perceived long-standing limitations in usual activities due to health problem:some/severe | 0.681* | 0.030 |
| Real GDP per capita | -0.632* | 0.012 |
| Employment rate | -0.615* | 0.019 |
| Unemployment rate | 0.599* | 0.040 |
**. Correlation is significant at the 0.01 level (2-tailed). *. Correlation is significant at the 0.05 level (2-tailed).
Table 3.
Simple Linear Regression Models for unmet medical needs.
| Adjusted R2 | Predicted factors | Dependent variable | Unstandardized Coefficients | t | P value | 95,0% Confidence Interval for B | ||
|---|---|---|---|---|---|---|---|---|
| B | Std. Error | Lower Bound | Upper Bound | |||||
| 41.2% | Private health expenditures | (Constant) | 31.921 | 7.860 | 4.061 | 0.002 | 14.408 | 49.435 |
| Unmet medical needs | -3.832 | 1.298 | -2.953 | 0.014 | -6.724 | -0.941 | ||
| 54.4% | Public health expenditures | (Constant) | 16.580 | 2.134 | 7.771 | 0.001 | 11.826 | 21.334 |
| Unmet medical needs | -0.754 | 0.201 | -3.758 | 0.004 | -1.201 | -0.307 | ||
| 39.6% | Self-perceived long-standing limitations in usual activities due to health problem: some/severe | (Constant) | -34.598 | 16.760 | -2.064 | 0.073 | -73.247 | 4.050 |
| Unmet medical needs | 1.859 | 0.708 | 2.627 | 0.030 | 0.227 | 3.491 | ||
| 57% | Self-perceived health: bad/very bad | (Constant) | 0.833 | 2.430 | .343 | 0.741 | -4.770 | 6.436 |
| Unmet medical needs | 0.966 | 0.269 | 3.596 | 0.007 | 0.346 | 1.585 | ||
| 58.3% | Self-perceived health: very good/good | (Constant) | 70.672 | 16.640 | 4.247 | 0.003 | 32.300 | 109.044 |
| Unmet medical needs | -0.807 | 0.219 | -3.683 | 0.006 | -1.313 | -0.302 | ||
| 35.3% | Real GDP per capita | (Constant) | 23.469 | 5.151 | 4.556 | 0.001 | 12.340 | 34.597 |
| Unmet medical needs | -0.001 | 0.000 | -2.939 | 0.012 | -0.001 | 0.001 | ||
| 32.6% | Employment rate | (Constant) | 27.704 | 7.084 | 3.911 | 0.002 | 12.268 | 43.139 |
| Unmet medical needs | -0.325 | 0.120 | -2.702 | 0.019 | -0.586 | -0.063 | ||
| 29.5% | Unemployment rate | (Constant) | 3.720 | 2.345 | 1.586 | 0.144 | -1.506 | 8.946 |
| Unmet medical needs | 0.439 | 0.186 | 2.365 | 0.040 | 0.025 | 0.853 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



