Submitted:
16 August 2023
Posted:
17 August 2023
You are already at the latest version
Abstract
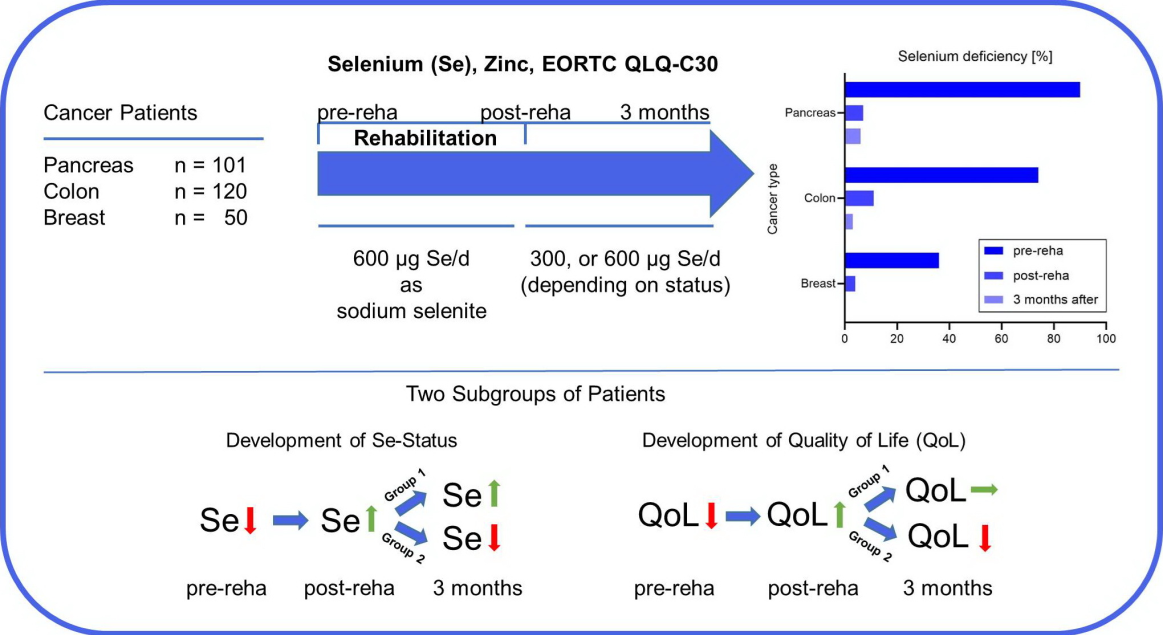
Background: Micronutrient deficiencies are common at the time of cancer diagnosis and are associated with worse prognosis. Little is known about them in cancer rehabilitation. Methods: Data from routine health related quality of life (HRQOL) were analyzed at an inpatient cancer rehabilitation center. Rehabilitation patients completed the EORTC QLQ-C30 questionnaire before and after multidisciplinary rehabilitation treatment, and three month after discharge. Selenium and zinc status was measured in whole blood at these three time points. In case of selenium deficiency up to 600 µg selenium per day as sodium selenite was supplemented. Results: A total of 271 patients (breast, colon, and pancreatic cancer) were included in the analysis. There was clinically meaningful improvement in many domains of the EORTC QLQ-C30 during rehabilitation. However, effect often waned in the three months after. Prevalence for selenium deficiency varied between 34 to 90 percent depending on cancer type (breast < colon < pancreas). In contrast, zinc deficiency was rare. Daily selenium supplementation of 600 µg was more efficient to correct selenium deficiency compared to 300 µg selenium per day. Rehabilitation and increasing selenium status after rehabilitation were associated with improved global quality of life, physical and emotional functioning, and fatigue. In cancer patients with decreasing selenium status, values of global quality of life, physical and emotional functioning, and fatigue were back to the values at the beginning of rehabilitation. Conclusions: Selenium deficiency is common in cancer patients admitted to a cancer rehabilitation clinic. Selenium supplementation during rehabilitation effectively corrected selenium deficiency in most cases. The positive effects of rehabilitation persisted longer, when selenium status did not decrease after rehabilitation.
Keywords:
selenium
; zinc
; micronutrient dietary intake
; cancer
; rehabilitation
; health-related quality of life (HRQOL)
1. Introduction
Rehabilitation is defined as “a process to restore mental and/or physical abilities lost to injury or disease, in order to function in a normal or near-normal way” [1]. As cancer has increasingly become a chronic disease, cancer patients can benefit from rehabilitation before, during, and after treatment [1]. A recent systematic review showed, that 71% of the included trials reported statistically significant results after cancer rehabilitation for at least one functional outcome [2].
Many patients experience unwanted weight loss even before cancer diagnosis, which indicates malnutrition, as weight loss is its hallmark [3]. Side effects of cancer therapy such as emesis, nausea, pain, and gastrointestinal disorders can lead to a reduced food intake [3]. Also, metabolic changes contribute to cancer-associated malnutrition [4]. Malnutrition at the time of diagnosis affects survival [5]. A weight loss of 5 – 10% during radiotherapy had a significant negative impact on 5-year overall survival and disease-specific survival [5].
Pressoir et al. showed that one in three cancer patients are malnourished [6]. Prevalence of malnutrition was lowest in breast cancer patients, followed by patients with colon cancer [6]. In upper digestive cancer, such as pancreatic cancer, prevalence of malnutrition was highest.
Malnutrition is characterized by insufficient energy and macronutrient intake [3]. However, reduced food intake can also lead to micronutrient deficiencies, so-called hidden hunger [7]. In addition, micronutrient deficiencies can also occur without a deficit in energy intake [7].
Selenium is an essential trace element associated with the incidence of certain types of cancer [8,9]. Insufficient selenium intake has been estimated to affect up to 1 billion people worldwide [10]. Selenium deficiency increases the risk for thyroid and cardiovascular diseases [11,12,13,14,15]. Selenium plays an important role in antioxidant defense [16,17] and its deficiency impairs the immune system, increasing the risk for infections [18].
As fellow trace element and antioxidant, zinc is part of over 300 enzymes [19]. Zinc deficiency is estimated to affect up to 2 billion people worldwide, and can result in cell-mediated immune dysfunction, and cognitive impairment [19]. Many epidemiological studies have shown a relationship between zinc content in the diet and cancer risk [20,21].
In cancer patients, micronutrient deficiencies, such as selenium or zinc, can already be present at time of diagnosis [22,23]. For zinc deficiency the results of previous studies are conflicting [21,24,25]. Selenium deficiency at time of diagnosis, however, is associated with worse overall survival [22,26,27]. Selenium status can further decrease during radiotherapy, especially after prior chemotherapy [28,29]. Low selenium levels have been shown in breast, colorectal, and pancreatic cancer patients [30,31,32,33].
The aim of this observational study was to determine the prevalence of selenium and zinc deficiency in patients with breast, colon, and pancreatic cancer at the beginning of rehabilitation and the effect of routine selenium supplementation on selenium status at the end and three months after, in a cancer rehabilitation center in Germany. In addition, global routine health related quality of life (HRQOL) was analyzed at the beginning and the end of rehabilitation, as well as three months after.
2.1. Study Design
An ethics committee vote was not necessary, as only clinic intern register data were used for this retrospective cross-sectional study. The data were routinely collected in patient care. Written informed consents for the data analysis of patient data were obtained from all participating patients in accordance with the Declaration of Helsinki. The clinical data were recorded in a clinic specialized in cancer rehabilitation (Inselsberg Klinik Bad Tabarz, Germany). The data of patients treated for breast cancer, pancreatic cancer, or colon cancer, in which selenium and zinc status were determined as part of their treatment, were anonymized in a period from 2016 to 2022. The anonymized data included age, sex, diagnosis, therapy, prior supplementation, and selenium or zinc supplementation. Selenium and zinc concentrations in whole blood were measured at three time points: admission, discharge (after three weeks), and three months after discharge.
2.2. Measurement of Whole Blood Selenium and Zinc
Whole blood selenium samples were obtained at the beginning and the end of the rehabilitation stay at the Inselsberg Clinic Bad Tabarz, as well as after three months using tubes for trace elements/metal analytic. Blood samples were sent to a certified laboratory (biosyn Arzneimittel GmbH, Fellbach, Germany). Selenium and zinc levels were measured by microwave digestion and flameless atomic absorption spectrometry, according to the method of Winnefeld et al. [34]. Selenium-status in whole blood < 100 µg/l was defined as deficient, using the reference range defined by German authorities [34]. Reference range for zinc was 4.0 – 7.5 mg/l.
Selenium was supplemented in form of sodium selenite (tablets containing 300 µg selenium, selenase, biosyn Arzneimittel GmbH, Fellbach). At the beginning of the analyzed time in 2016, 300 µg selenium per day was supplemented. From 2017 – 2022 the daily selenium supplementation was increased to 600 µg selenium.
2.3. European Organization for Research and Treatment of Cancer (EORTC) Quality of Life Questionnaire Core-30 (EORTC QLQ-C30)
Data from routine HRQOL at an inpatient cancer rehabilitation center was analyzed. Patients completed the European Organization for Research and Treatment of Cancer (EORTC) Quality of Life Questionnaire Core-30 (EORTC QLQ-C30) at the beginning, the end, and three months after the multidisciplinary rehabilitation treatment. Missing values in filled out questionnaires were 1.5%. All included patients completed a EORTC QLQ-30 questionnaire at the beginning of rehabilitation (Pre-Reha). At discharge (Post-Reha) in total 5 EORTC QLQ-30 questionnaires were missing, all from pancreatic cancer patients. Return rate for EORTC QLQ-30 questionnaires three months after rehabilitation was 35% (27% breast cancer; 37% colon cancer; 36% pancreatic cancer).
2.4. Statistical Analysis
All data were stored and analyzed using GraphPad 9.1. All continuous data are presented as means ± standard deviation (SD), and the differences were assessed by one-way analysis of variance (normal distribution) or Kruskal–Wallis H test (non-normal distribution). All categorical data are presented as percentages; the differences were assessed by Pearson chi-square test. Differences between whole blood selenium concentrations in continuous variables were analyzed by Student’s t test (normal distribution) and Mann–Whitney test (non-normal distribution) for independent samples. One-way ANOVA was used to compare three or more groups (p trend). The size of change at admission, discharge, and three months after discharge was evaluated using Cohens’ d. Effect sizes (ES) were considered as small (d = 0.2), medium (d = 0.5) or large (d = 0.8) [35]. All p values were 2-sided statistical tests and were considered statistically significant if < 0.05.
3. Results
3.1. Patients Characteristics
The study included 271 cancer patients in rehabilitation. Age, sex, and therapy varied depending on tumor location (Table 1). There were no age- or sex-dependent effects on baseline whole blood selenium or zinc concentration (data not shown). Selenium and zinc status was not associated with tumor size, grading, chemo- or radiotherapy (data not shown).
3.1. High Prevalence of Selenium Deficiency depending on Tumor Localization
While selenium deficiency was prevalent with high incidence in cancer patients in rehabilitation (73%), zinc deficiency was rare (1%). Selenium deficiency was associated with tumor localization (Table 2). Prevalence of selenium deficiency was 90% in patients with pancreatic cancer, 74% of the patients with colon cancer and 36% in breast cancer patients. Thirteen of fifty breast cancer patients supplemented various dosages of selenium before rehabilitation. Selenium deficiency was less prevalent in this group (23% vs. 41%), but the difference was not significant (p = 0.2591).
3.2. Selenium supplementation during rehabilitation corrects selenium deficiency
Selenium supplementation during rehabilitation significantly improved the selenium status in all patients (p < 0.0001). Initially, breast and colon cancer patients were supplemented with 300 µg selenium per day. Then, supplementation was increased to 600 µg selenium per day. Due to their low selenium status, all pancreatic cancer patients were supplemented with 600 µg selenium per day from the beginning.
There was no significant difference in selenium status at admission between patients with colon cancer receiving 300 µg or 600 µg selenium per day (Figure 1). At the end of rehabilitation, selenium status was significantly higher in breast and colon cancer patients, which received 600 µg selenium per day compared to patients only receiving 300 µg (breast cancer: 141.2 ± 17.1 µg/l vs.127.1 ± 18.8 µg/l , p = 0.0076; colon cancer 126.2 ± 17.5 µg/l vs. 116.5 ± 18.6 µg/l, p = 0.0239). In colon cancer patients the proportion of patients with selenium deficiency was significantly lower at the end of rehabilitation when receiving 600 µg selenium per day (5.9% vs. 24.2%; p = 0.0042) (Figure 1).
3.3. Different development of whole blood selenium concentration
When looking at the individual values of the cancer patients, from whom three measured values were available, there were two different groups. In the first group, the selenium status continued to increase three months after rehabilitation or remained on a comparable level. In the second group, the selenium status decreased three months after rehabilitation. This different development in selenium status was significant in all three tumor types, while the selenium values at the beginning of rehabilitation (pre-rehab) were not significantly different (Figure 2). The values at the end of rehabilitation (post-rehab) in the second group were significantly higher for colon and pancreas cancer patients.
Mean age values were comparable in both groups (67.8 ± 11.2 vs. 66.8 ± 11.7). In addition, ongoing chemotherapy during rehabilitation as well as planned chemotherapy thereafter were not associated with selenium status development.
3.4. Differences in EORTC QLQ-C30 Results depending on Tumor Localization
Overall, rehabilitation improved functional scales and quality of life (Table 3, Table 4 and Table 5). Baseline values were worst in pancreatic cancer patients and best in breast cancer patients.
The four key domains of the EORTC QLQ-C30: physical functioning, emotional functioning, fatigue and pain all improved significantly during rehabilitation (Table 3, Table 4 and Table 5). Assuming a change of ≥ 10 points for a clinical significant improvement, this was only partially achieved in the four key domains and global quality of life during rehabilitation.
Global quality of life improved more than 10 points during rehabilitation in breast, colon, and pancreatic cancer. However, qlobal quality of life values decreased 1.5 to 4.3 points in all three cancer types. The effect size was large at the end of rehabilitation in breast cancer patients (d = 0.820), but was ony moderate three months after discharge (d = 0.535). In pancreatic cancer patients, the effect size was only barely moderate (p = 0.511) during rehabilitation. Effect size further decreased after rehabilitation till only a small effect remained (d = 0.389). In colon cancer patients, effect size of global quality of life was moderate during and after rehabilitation (d = 0.632, respectively d = 0.516.)
In breast cancer, the key domains fatigue and pain improved 10.4 points and 10.9 points, respectively during rehabilitation. A mean value better than the thresholds for clinical importance, as defined by Giesinger et al., was only achieved for fatigue (value below 39 points) [36]. However, both values were worse three months after discharge. The key domain, physical functioning, still improved three months after discharge with a medium effect size (d = 0.588). Emotional functioning improved 17.6 points during rehabilitation. Three months after discharge mean value decreased 17.1 points, displaying no effect (d = 0.027) compared to a medium effect size at discharge (d = 0.739). Global quality of life was the only value, which showed a large effect size (d = 0.820), at the end of rehabilitation.
In colon cancer the mean values in physical functioning and emotional functioning showed a comparable development as in breast cancer (Table 4). Physical functioning improved 9.9 points three month after discharge. Emotional functioning improved 11.5 points during rehabilitation and declined 7.9 points three month after discharge. Fatigue improved 12.9 points during rehabilitation. Mean value worsened slightly but stayed below the threshold of 39 points [36]. In contrast to breast cancer, mean values for pain improved till three month after discharge with 16.2 points, which is below the threshold of 25 points, and showed a medium effect size (d = 0.518) [36]. In colon cancer the symptom diarrhea improved significantly by decreasing 10.3 points during rehabilitation. However, the mean value increased 6.3 points again at three month after discharge. Global quality of life was the only value, which showed a medium effect size (d = 0.632), at the end of rehabilitation, and three motnth after discharge (d = 0.516).
In pancreatic cancer the key domain fatigue improved 11.8 points during rehabilitation and remained stable till three month after discharge. The mean values stayed far above the threshold of 39 [36]. Mean values for pain improved till three month after discharge (10.1 points) and remained above the threshold of 25 [36]. Physical and emotional functioning improved 8.9 and 9.3 points, respectively during rehabilitation. The mean value remained almost 20 points below the threshold of 83 for physical functioning [36]. In pancreatic cancer appetite loss was a major burden compared to breast or colon cancer (47.3 vs. 9.8 vs. 18.3). Appetite loss improved 20.4 points till three months after discharge with a medium effect size (d = 0.541). Also, constipation and diarrhea displayed significant changes during rehabilitation and three months after discharge. While diarrhea improved 15.9 points during rehabilitation, constipation worsened 19.9 points in the same time frame. In contrast, constipation was improved by 28.3 points three months after discharge, while diarrhea worsened 12.8 points.
3.5. Differences in EORTC QLQ-C30 Results depending on selenium status
The four key domains of the EORTC QLQ-C30 and global quality of life were further analyzed in colon and pancreas cancer patients, regarding differences between the two selenium status development groups. Sample size for breast cancer patients was too small for this sub-analysis (n = 14).
In colon cancer patients, global quality of life was significantly higher in group 1 at discharge (p < 0.0001) and three months after rehabilitation compared to the beginning of rehabilitation (p = 0.0002) (Figure 3 (a)). In contrast, while initially global quality of life significantly increased at the end of rehabilitation in group 2 (p = 0.0039), it decreased again significantly till three months after rehabilitation (p = 0.0134). At three month, no significant difference was observed compared to the start of rehabilitation in group 2. The improvement of global quality of life during rehabilitation was also significant in pancreatic cancer patients in both groups (Figure 3b). As in colon cancer, after three month scores decreased in the second group. In addition, global quality of life was significantly better in group 1, with increasing selenium status, three months after rehabilitation, compared to group 2, with decreasing selenium levels (Figure 3 (b)).
In pancreatic cancer, values for physical functioning were significantly higher in group 1 three months after rehabilitation compared to group 2 (p = 0.0245). At the beginning of rehabilitation, values for physical functioning were not significantly different. Developments in physical functioning were comparable between both groups (Data not shown).
Emotional functioning values worsened significantly in group 2 of colon cancer patients, while remaining stable in group 1 (p = 0.0059) three months after rehabilitation (Figure 3 (c)). Values for emotional functioning in group 2 also decreased in pancreatic cancer patients after three months. However, the change was not significant (Figure 3 (d)).
Scores for fatigue improved significantly at the end of rehabilitation and three months after discharge in group 1 of colon cancer patients (Figure 3 (e)). In contrast, fatigue significantly improved only during rehabilitation in group 2 and returned to almost baseline three months after rehabilitation. In pancreatic cancer, only the first group significantly improved fatigue scores during rehabilitation, while there was no change in group 2 (Figure 3 (f)).
In colon cancer patients, pain scores improved significantly at the end of rehabilitation and three months after in group 1 (p = 0.0005 and p = 0.0413, respectively). In group 2 there was no significant change in pain scores (Data not shown). In contrast, in pancreatic cancer pain scores significantly decreased at the end of rehabilitation and three months after in group 2 (p = 0.0176, respectively p = 0.0349). In group 1, with increasing selenium values, there was no significant change in pain scores.
4. Discussion
Cancer patients beginning rehabilitation display a high prevalence of selenium deficiency depending on tumor localization (pancreas > colon > breast). In contrast, zinc deficiency was rare. Daily selenium supplementation of 600 µg was more efficient to correct selenium deficiency compared to 300 µg selenium per day. Rehabilitation and increasing selenium status were associated with improved global quality of life, physical and emotional functioning, and fatigue.
4.1. Selenium deficiency in cancer patients in rehabilitation
Selenium deficiency was common in cancer patients at the beginning of rehabilitation in a German rehabilitation clinic. In contrast, zinc deficiency was rare. With 90%, prevalence of selenium deficiency was highest in pancreatic cancer patients. In colon cancer, prevalence of selenium deficiency was also high with 73%, while breast cancer patients were only deficient in 36%.
To our knowledge, this is the first analysis of micronutrient status of cancer patients in rehabilitation. So far, selenium and zinc levels were determined at the time of cancer diagnosis [22,23]. Selenium levels were found to be lower in cancers of the pancreas, gastric tract and breast, compared to cancer of prostate, throat, or lung [30,31,38,39,40]. This is in accordance with the results for colon and pancreatic cancer in this study. Interestingly, the selenium levels in breast cancer patients were higher, but while the prevalence was much lower, still one-third of the patients were selenium deficient.
Selenium supplementation before rehabilitation was more frequent in breast cancer patients compared with colon cancer and pancreatic cancer patients (28%, 8% and 1%, respectively). Selenium deficiency was less prevalent in breast cancer patients, supplementing selenium before rehabilitation (23% vs. 41%), but the difference was not significant. An online survey with breast cancer patients in Germany showed that selenium was the most frequent used complementary therapy with more than 50% [41]. In an Italian multicenter survey, breast cancer patients were more likely to use complementary therapy compared to patients with colon or pancreatic cancer [42]. In addition, disease severity could have been lower in breast cancer patients, as disease severity has been negatively associated with selenium levels [27,33,43]. Radiotherapy can also cause a decrease in selenium status, especially with prior chemotherapy [28,29]. However, three-quarter of the breast cancer patients had received radiotherapy and one-third also chemotherapy before rehabilitation.
4.2. Selenium supplementation corrects selenium deficiency
Selenium supplementation was standard of care in the rehabilitation center during the analyzed period. At the beginning, breast and colon cancer patients were supplemented with 300 µg selenium per day. Follow-up measurements at the end of rehabilitation indicated that the selenium dosage was not sufficient to reliably correct selenium deficiency in those cancer patients. Therefore, selenium supplementation was increased to 600 µg selenium per day. Due to their low selenium status, all pancreatic cancer patients were supplemented with 600 µg selenium per day from the beginning.
Retrospective analysis in this study confirmed that a selenium supplementation with 600 µg per day decreased the proportion of patients with selenium deficiency more efficiently compared to 300 µg selenium. Only six percent were still selenium deficient with the higher selenium dosage compared to almost one quarter, when receiving 300 µg selenium per day.
Interestingly, when looking at the selenium status in each patient after supplementation, they divided into two groups irrespectively of tumor localization. At the beginning of rehabilitation selenium status was comparable. The first group showed an increasing selenium concentration in whole blood during selenium supplementation at the end of rehabilitation and three months after. In the second group, selenium status was significantly higher post rehabilitation but then markedly decreased three months after rehabilitation compared to the first group.
Differences in the discharge-to-three-month follow-up period might be a reason for this different development in selenium status. Selenium supplementation was standard of care during rehabilitation and further selenium supplementation was recommended to the resident physician. Recommended selenium dosage depended on the selenium status of the patient. Target value was 150 µg/l selenium in whole blood. The recommendation for cancer patients with selenium deficiency (< 100 µg/l) was 600 µg selenium per day and 300 µg selenium per day for everyone else.
However, selenium dosages above 70 µg per day need a prescription in Germany. Thus, ongoing selenium supplementation depended on many different physicians and might have occurred at lower dosages, or been discontinued after discharge. In addition, statutory health insurances pay for selenium supplementation, in form of prescription drugs, only if selenium deficiency is proven beforehand. Physicians might have tended to use private prescriptions. Therefore, for some patients, the additional financial burden might have affected adherence to continuous supplementation.
Another aspect that should be considered regarding the observed differences in the development of selenium levels in these two groups is a changed selenium requirement after rehabilitation. A considerable proportion of the cancer patients had a planned chemotherapy after rehabilitation, which might decrease selenium values [28,29]. However, ongoing chemotherapy during rehabilitation and planned chemotherapy thereafter were not associated with selenium status development.
4.3. Effect of rehabilitation and selenium supplementation on quality of life
Overall, global quality of life improved during rehabilitation more than ten points in all three cancer types. Snyder et al. showed that a 10-point EORTC-QLQC30 score change represent changes in supportive care needs [44]. This indicates that rehabilitation equally improved quality of life in breast, colon, and pancreatic cancer. Long-term effect was determined measuring EORTC-QLQC30 scores again three months after rehabilitation.
Global quality of life values decreased between 2 – 4 points. This result is in accordance with the data from Lamprecht et al., who also measured global quality of life at the beginning, the end and three months after rehabilitation [45]. Starting values for global quality life values were comparable and development was almost identical in breast and colon cancer patients. In contrast, mean values of global quality life was more than 10 points lower in pancreatic cancer patients compared to EORTC QLQ-C30 reference values for metastatic pancreatic cancer [46]. On the other hand, development of global quality of life was comparable to breast and colon cancer patients. This is in contrast to the results of Singer et al. [47]. EORTC-QLQC30 scores were assessed at admission and 4 months after rehabilitation in cancer patients older than 69 years. Global quality of life improved more than 25 points for gastrointestinal tumors, while in breast cancer patients the improvement was only in the range of five points [47].
Interestingly, global quality of life values developed differently three month after rehabilitation depending on selenium status in pancreatic an colon cancer. Global quality of life only decreased in the group of cancer patients, which displayed decreasing selenium values after rehabilitation. In pancreatic cancer, global quality of life was significantly lower in this group compared to the group with increasing or stable selenium status. To our knowledge, this is the first description of a clinically significant effect of selenium status on global quality of life in cancer patients. In elderly healthy volunteers, selenium supplementation did not appear to benefit mood or quality of life [48].
4.4. Effect of rehabilitation and selenium supplementation on key domains
The long-term effects of rehabilitation varied in the key domains physical and emotional function, fatigue, and pain. Colon cancer patients estimated their physical functioning at the start of rehabilitation more poorly than breast cancer patients, which is in line with previous results [45]. In contrast, EORTC QLQ-C30 reference value for physical functioning in metastatic pancreatic cancer was more than 20 points better compared to the starting value in this study (78.2 vs. 54.5 points) [46]. Physical functioning improved further or remained stable in the three month after rehabilitation. As for global quality life, values for physical functioning displayed comparable starting values and development for breast and colon cancer patients as Lamprecht et al. [45]. Change of approximately 10 points was also consistent with previous results [47]. Pancreatic cancer patients displayed lower physical functioning values three months after rehabilitatation, when their selenium status decreased in this timeframe.
Breast and pancreatic cancer patients at the start of rehabilitation and 3 months thereafter rated emotional functioning significantly more poorly compared to colon cancer patients. Lamprecht et al. also showed this in breast cancer [45]. In contrast, emotional functioning value was more than 10 points lower in this earlier study. Results for emotional functioning are conflicting, as another study had lower initial value in gastrointestinal cancer compared to breast cancer [47]. Emotional functioning improved during rehabilitation significantly, especially in breast and colon cancer patients. However, this improvement did not last. While this was already shown before [49], in previous trials there was still a significant improvement [45,47]. Here, initial emotional functioning values were not significantly different compared to those three months after rehabilitation. When taking only those patients with all three selenium status measurements in consideration, improvement of emotional functioning remained in colon cancer patients with increasing or stable selenium levels after rehabilitation.
During rehabilitation, fatigue scores improved most compared to all other symptom scales. While this applied for all tumor types, the initial fatigue score was significantly worse in pancreatic cancer patients. It was also 15 points higher compared to the EORTC QLQ-C30 reference value in metastatic pancreatic cancer [46]. Fatigue scores worsened again 3 months after the end of rehabilitation, but were still significantly better compared to initial values. Similar results were shown by Lamprecht et al., while fatigue score was worse four months after rehabilitation in breast cancer in another trial [45,47]. In colon cancer, patients with increasing or stable selenium levels after rehabilitation, the positive effect of rehabilitation on fatigue persisted longer compared to those with decreasing selenium status.
A possible positive effect of selenium especially on fatigue was shown in a clinical trial with children and adolescents with cancer [50]. After one year supplementation with selenium, fatigue scores decreased in patients with solid tumors and hematological cancer [50]. In a recent trial, selenium biomarkers , such as plasma selenium, glutathione peroxidase, and selenoprotein P, showed linear correlations in patients with chronic fatigue syndrome without reaching saturation, indicative of Se deficiency [51].
As colorectal cancer survivors are more likely to report fatigue [52,53], and often display selenium deficiency, the results indicate that they could benefit, when selenium status is assessed and selenium deficiency corrected. A long-term selenium supplementation seems to be necessary to maintain an adequate selenium status in cancer patients, so the positive effects of rehabilitation persist longer. Symptom burden and prevalence of selenium deficiency was highest in pancreatic cancer patients in this trial. Therefore, the conclusion for colorectal cancer patients could also apply to patients with pancreatic cancer.
4.5. Strengths and Limitations
This study has a number of limitations, including a retrospective single-center design, inherent heterogeneity of cancer patients, lack of a control group (patients’ not undergoing rehabilitation) and low number of patient data three month after discharge regarding selenium and zinc status, and returned EORTC QLQ-30 forms. Another important factor could have been the refusal of further prescription of selenium medication, as selenium dosages over 70 µg per day are prescription only in Germany. After rehabilitation, most often the family doctor takes over further treatment and necessary prescriptions. Therefore, the patient is dependent on the attending physician. The results of our study imply that there might be reservations in Germany to treat selenium deficiency continuously.
The strength of this study is the inclusion of three different cancer types and the numbers of patients in rehabilitation, which received comparable treatment including assessment of selenium and zinc status, and selenium supplementation as standard of care.
5. Conclusions
Selenium deficiency is common in cancer patients starting rehabilitation. Prevalence of selenium deficiency ranged between 36 to 90 percent depending on tumor location. Selenium supplementation with 600 µg was highly efficient to correct selenium deficiency. In cancer patients with decreasing selenium status three months after rehabilitation, values of global quality of life, physical and emotional functioning, and fatigue were back to the values at the beginning of rehabilitation. This indicates that the positive effects of rehabilitation persist longer, when selenium status did not decrease after rehabilitation.
Author Contributions
Conceptualization and methodology, all authors; formal analysis, C.P.; investigation and resources J.S.; data curation, J.S.; writing—original draft preparation, C.P.; writing—review and editing, C.P.; visualization, C.P.; supervision and project administration, J.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy restrictions.
Conflicts of Interest
Christina Pfister is employed by biosyn Arzneimittel GmbH. Selenium measurements were performed in the laboratory of biosyn Arzneimittel GmbH. Joerg Schoenemann did not receive any direct financial support or funding.
References
- Mayer, R.S.; Engle, J. Rehabilitation of Individuals With Cancer. Ann Rehabil Med 2022, 46, 60–70. [Google Scholar] [CrossRef]
- Sleight, A.; Gerber, L.H.; Marshall, T.F.; Livinski, A.; Alfano, C.M.; Harrington, S.; Flores, A.M.; Virani, A.; Hu, X.; Mitchell, S.A.; et al. Systematic Review of Functional Outcomes in Cancer Rehabilitation. Arch Phys Med Rehabil 2022, 103, 1807–1826. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, T.; Süß, P.; Schulte, D.M.; Letsch, A.; Jensen, W. Supportive Care in Oncology-From Physical Activity to Nutrition. Nutrients 2022, 14, 1149. [Google Scholar] [CrossRef]
- Fan, Y.; Yao, Q.; Liu, Y.; Jia, T.; Zhang, J.; Jiang, E. Underlying Causes and Co-Existence of Malnutrition and Infections: An Exceedingly Common Death Risk in Cancer. Front Nutr 2022, 9, 814095. [Google Scholar] [CrossRef] [PubMed]
- Langius, J.A.E.; Bakker, S.; Rietveld, D.H.F.; Kruizenga, H.M.; Langendijk, J.A.; Weijs, P.J.M.; Leemans, C.R. Critical Weight Loss Is a Major Prognostic Indicator for Disease-Specific Survival in Patients with Head and Neck Cancer Receiving Radiotherapy. British Journal of Cancer 2013, 109, 1093–1099. [Google Scholar] [CrossRef] [PubMed]
- Pressoir, M.; Desné, S.; Berchery, D.; Rossignol, G.; Poiree, B.; Meslier, M.; Traversier, S.; Vittot, M.; Simon, M.; Gekiere, J.P.; et al. Prevalence, Risk Factors and Clinical Implications of Malnutrition in French Comprehensive Cancer Centres. British Journal of Cancer 2010, 102, 966–971. [Google Scholar] [CrossRef]
- Lowe, N.M. The Global Challenge of Hidden Hunger: Perspectives from the Field. Proc Nutr Soc 2021, 80, 283–289. [Google Scholar] [CrossRef]
- Schrauzer, G.N.; White, D.A.; Schneider, C.J. Cancer Mortality Correlation Studies--III: Statistical Associations with Dietary Selenium Intakes. Bioinorg Chem 1977, 7, 23–31. [Google Scholar] [CrossRef]
- Cai, X.; Wang, C.; Yu, W.; Fan, W.; Wang, S.; Shen, N.; Wu, P.; Li, X.; Wang, F. Selenium Exposure and Cancer Risk: An Updated Meta-Analysis and Meta-Regression. Scientific Reports 2016, 6, 19213. [Google Scholar] [CrossRef]
- Jones, G.D.; Droz, B.; Greve, P.; Gottschalk, P.; Poffet, D.; McGrath, S.P.; Seneviratne, S.I.; Smith, P.; Winkel, L.H.E. Selenium Deficiency Risk Predicted to Increase under Future Climate Change. Proc Natl Acad Sci U S A 2017, 114, 2848–2853. [Google Scholar] [CrossRef]
- Wu, Q.; Rayman, M.P.; Lv, H.; Schomburg, L.; Cui, B.; Gao, C.; Chen, P.; Zhuang, G.; Zhang, Z.; Peng, X.; et al. Low Population Selenium Status Is Associated With Increased Prevalence of Thyroid Disease. J. Clin. Endocrinol. Metab. 2015, 100, 4037–4047. [Google Scholar] [CrossRef]
- Wu, Q.; Wang, Y.; Chen, P.; Wei, J.; Lv, H.; Wang, S.; Wu, Y.; Zhao, X.; Peng, X.; Rijntjes, E.; et al. Increased Incidence of Hashimoto’s Thyroiditis in Selenium Deficiency: A Prospective Six-Year Cohort Study. The Journal of Clinical Endocrinology & Metabolism. [CrossRef]
- Benstoem, C.; Goetzenich, A.; Kraemer, S.; Borosch, S.; Manzanares, W.; Hardy, G.; Stoppe, C. Selenium and Its Supplementation in Cardiovascular Disease—What Do We Know? Nutrients 2015, 7, 3094–3118. [Google Scholar] [CrossRef]
- Alehagen, U.; Johansson, P.; Björnstedt, M.; Rosén, A.; Post, C.; Aaseth, J. Relatively High Mortality Risk in Elderly Swedish Subjects with Low Selenium Status. European Journal of Clinical Nutrition 2016, 70, 91–96. [Google Scholar] [CrossRef]
- Bomer, N.; Grote Beverborg, N.; Hoes, M.F.; Streng, K.W.; Vermeer, M.; Dokter, M.M.; IJmker, J.; Anker, S.D.; Cleland, J.G.F.; Hillege, H.L.; et al. Selenium and Outcome in Heart Failure. Eur J Heart Fail, 1644. [Google Scholar] [CrossRef]
- Tapiero, H.; Townsend, D.M.; Tew, K.D. The Antioxidant Role of Selenium and Seleno-Compounds. Biomed Pharmacother 2003, 57, 134–144. [Google Scholar] [CrossRef]
- Tinggi, U. Selenium: Its Role as Antioxidant in Human Health. Environmental Health and Preventive Medicine 2008, 13, 102–108. [Google Scholar] [CrossRef]
- Huang, Z.; Rose, A.H.; Hoffmann, P.R. The Role of Selenium in Inflammation and Immunity: From Molecular Mechanisms to Therapeutic Opportunities. Antioxid. Redox Signal. 2012, 16, 705–743. [Google Scholar] [CrossRef] [PubMed]
- Prasad, A.S. Discovery of Human Zinc Deficiency: Its Impact on Human Health and Disease. Advances in Nutrition: An International Review Journal 2013, 4, 176–190. [Google Scholar] [CrossRef]
- Skrajnowska, D.; Bobrowska-Korczak, B. Role of Zinc in Immune System and Anti-Cancer Defense Mechanisms. Nutrients 2019, 11, 2273. [Google Scholar] [CrossRef] [PubMed]
- Bengtsson, Y.; Demircan, K.; Rosendahl, A.H.; Borgquist, S.; Sandsveden, M.; Manjer, J. Zinc and Breast Cancer Survival: A Prospective Cohort Study of Dietary Intake and Serum Levels. Nutrients 2022, 14, 2575. [Google Scholar] [CrossRef] [PubMed]
- Demircan, K.; Bengtsson, Y.; Sun, Q.; Brange, A.; Vallon-Christersson, J.; Rijntjes, E.; Malmberg, M.; Saal, L.H.; Rydén, L.; Borg, Å.; et al. Serum Selenium, Selenoprotein P and Glutathione Peroxidase 3 as Predictors of Mortality and Recurrence Following Breast Cancer Diagnosis: A Multicentre Cohort Study. Redox Biol 2021, 47, 102145. [Google Scholar] [CrossRef]
- Namikawa, T.; Utsunomiya, M.; Yokota, K.; Munekage, M.; Uemura, S.; Maeda, H.; Kitagawa, H.; Kobayashi, M.; Hanazaki, K. Association between Serum Zinc Levels and Clinicopathological Characteristics in Patients with Gastric Cancer. Gastrointest Tumors 2023, 10, 6–13. [Google Scholar] [CrossRef]
- Wu, T.; Sempos, C.T.; Freudenheim, J.L.; Muti, P.; Smit, E. Serum Iron, Copper and Zinc Concentrations and Risk of Cancer Mortality in US Adults. Ann Epidemiol 2004, 14, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Shi, Z.; Chu, A.; Zhen, S.; Taylor, A.W.; Dai, Y.; Riley, M.; Samman, S. Association between Dietary Zinc Intake and Mortality among Chinese Adults: Findings from 10-Year Follow-up in the Jiangsu Nutrition Study. Eur J Nutr 2018, 57, 2839–2846. [Google Scholar] [CrossRef]
- Sandsveden, M.; Nilsssson, E.; Borgquist, S.; Rosendahl, A.H.; Manjer, J. Pre-Diagnostic Serum Selenium Levels in Relation to Breast Cancer Survival and Tumor Characteristics. Int. J. Cancer 2020. [Google Scholar] [CrossRef] [PubMed]
- Lubinski, J.; Marciniak, W.; Muszynska, M.; Huzarski, T.; Gronwald, J.; Cybulski, C.; Jakubowska, A.; Debniak, T.; Falco, M.; Kladny, J.; et al. Serum Selenium Levels Predict Survival after Breast Cancer. Breast Cancer Res. Treat. 2017. [Google Scholar] [CrossRef] [PubMed]
- Franca, C. a. S.; Nogueira, C.R.; Ramalho, A.; Carvalho, A.C.P.; Vieira, S.L.; Penna, A.B.R.C. Serum Levels of Selenium in Patients with Breast Cancer before and after Treatment of External Beam Radiotherapy. Ann. Oncol. 2011, 22, 1109–1112. [Google Scholar] [CrossRef]
- Zeng, Y.C.; Xue, M.; Chi, F.; Xu, Z.G.; Fan, G.L.; Fan, Y.C.; Zheng, M.H.; Zhong, W.Z.; Wang, S.L.; Zhang, Z.Y.; et al. Serum Levels of Selenium in Patients with Brain Metastases from Non-Small Cell Lung Cancer before and after Radiotherapy. Cancer/Radiothérapie 2012, 16, 179–182. [Google Scholar] [CrossRef]
- Charalabopoulos, K.; Kotsalos, A.; Batistatou, A.; Charalabopoulos, A.; Vezyraki, P.; Peschos, D.; Kalfakakou, V.; Evangelou, A. Selenium in Serum and Neoplastic Tissue in Breast Cancer: Correlation with CEA. British Journal of Cancer 2006, 95, 674–676. [Google Scholar] [CrossRef]
- Lener, M.R.; Scott, R.J.; Wiechowska-Kozłowska, A.; Serrano-Fernández, P.; Baszuk, P.; Jaworska-Bieniek, K.; Sukiennicki, G.; Marciniak, W.; Muszyńska, M.; Kładny, J.; et al. Serum Concentrations of Selenium and Copper in Patients Diagnosed with Pancreatic Cancer. Cancer Res Treat 2016, 48, 1056–1064. [Google Scholar] [CrossRef]
- Mikac-Dević, M.; Vukelić, N.; Kljaić, K. Serum Selenium Level in Patients with Colorectal Cancer. Biol Trace Elem Res 1992, 33, 87–94. [Google Scholar] [CrossRef]
- Psathakis, D.; Wedemeyer, N.; Oevermann, E.; Krug, F.; Siegers, C.P.; Bruch, H.P. Blood Selenium and Glutathione Peroxidase Status in Patients with Colorectal Cancer. Dis Colon Rectum 1998, 41, 328–335. [Google Scholar] [CrossRef] [PubMed]
- Winnefeld, K.; Dawczynski, H.; Schirrmeister, W.; Adam, G.; Friedrich, U.; Hein, S. Selenium in Serum and Whole Blood in Patients with Surgical Interventions. Biol Trace Elem Res 1995, 50, 149–155. [Google Scholar] [CrossRef]
- Ellis, P.D. The Essential Guide to Effect Sizes: Statistical Power, Meta-Analysis, and the Interpretation of Research Results; 1st ed.; Cambridge University Press, 2010; ISBN 978-0-521-19423-5.
- Giesinger, J.M.; Kuijpers, W.; Young, T.; Tomaszewski, K.A.; Friend, E.; Zabernigg, A.; Holzner, B.; Aaronson, N.K. Thresholds for Clinical Importance for Four Key Domains of the EORTC QLQ-C30: Physical Functioning, Emotional Functioning, Fatigue and Pain. Health Qual Life Outcomes 2016, 14, 87. [Google Scholar] [CrossRef] [PubMed]
- Waldmann, A.; Schubert, D.; Katalinic, A. Normative Data of the EORTC QLQ-C30 For the German Population: A Population-Based Survey. PLoS ONE 2013, 8, e74149. [Google Scholar] [CrossRef] [PubMed]
- Charalabopoulos, K.; Kotsalos, A.; Batistatou, A.; Charalabopoulos, A.; Peschos, D.; Vezyraki, P.; Kalfakakou, V.; Metsios, A.; Charalampopoulos, A.; Macheras, A.; et al. Serum and Tissue Selenium Levels in Gastric Cancer Patients and Correlation with CEA. Anticancer research 2009, 29, 3465–3467. [Google Scholar]
- Muecke, R.; Klotz, T.; Giedl, J.; Buentzel, J.; Kundt, G.; Kisters, K.; Prott, F.-J.; Micke, O. Whole Blood Selenium Levels (WBSL) in Patients with Prostate Cancer (PC), Benign Prostatic Hyperplasia (BPH) and Healthy Male Inhabitants (HMI) and Prostatic Tissue Selenium Levels (PTSL) in Patients with PC and BPH. Acta Oncologica 2009, 48, 452–456. [Google Scholar] [CrossRef]
- Jaworska, K.; Gupta, S.; Durda, K.; Muszyńska, M.; Sukiennicki, G.; Jaworowska, E.; Grodzki, T.; Sulikowski, M.; Waloszczyk, P.; Woloszczyk, P.; et al. A Low Selenium Level Is Associated with Lung and Laryngeal Cancers. PLoS ONE 2013, 8, e59051. [Google Scholar] [CrossRef]
- Huebner, J.; Muenstedt, K.; Prott, F.J.; Stoll, C.; Micke, O.; Buentzel, J.; Muecke, R.; Senf, B. Online Survey of Patients with Breast Cancer on Complementary and Alternative Medicine. Breast Care (Basel) 2014, 9, 60–63. [Google Scholar] [CrossRef]
- Berretta, M.; Della Pepa, C.; Tralongo, P.; Fulvi, A.; Martellotta, F.; Lleshi, A.; Nasti, G.; Fisichella, R.; Romano, C.; De Divitiis, C.; et al. Use of Complementary and Alternative Medicine (CAM) in Cancer Patients: An Italian Multicenter Survey. Oncotarget 2016. [Google Scholar] [CrossRef]
- Stevens, J.; Waters, R.; Sieniawska, C.; Kassam, S.; Montoto, S.; Fitzgibbon, J.; Rohatiner, A.; Lister, A.; Joel, S. Serum Selenium Concentration at Diagnosis and Outcome in Patients with Haematological Malignancies. Br. J. Haematol. 2011, 154, 448–456. [Google Scholar] [CrossRef]
- Snyder, C.F.; Blackford, A.L.; Sussman, J.; Bainbridge, D.; Howell, D.; Seow, H.Y.; Carducci, M.A.; Wu, A.W. Identifying Changes in Scores on the EORTC-QLQ-C30 Representing a Change in Patients’ Supportive Care Needs. Quality of Life Research 2015, 24, 1207–1216. [Google Scholar] [CrossRef]
- Lamprecht, J.; Thyrolf, A.; Mau, W. Health-Related Quality of Life in Rehabilitants with Different Cancer Entities. Eur J Cancer Care (Engl) 2017, 26. [Google Scholar] [CrossRef]
- Amin, S.; Joo, S.; Nolte, S.; Yoo, H.K.; Patel, N.; Byrnes, H.F.; Costa-Cabral, S.; Johnson, C.D. Health-Related Quality of Life Scores of Metastatic Pancreatic Cancer Patients Responsive to First Line Chemotherapy Compared to Newly Derived EORTC QLQ-C30 Reference Values. BMC Cancer 2022, 22, 563. [Google Scholar] [CrossRef] [PubMed]
- Singer, S.; Schulte, T. [Quality of life in elderly cancer patients--need for and benefit of inpatient rehabilitation]. Dtsch Med Wochenschr 2009, 134, 121–126. [Google Scholar] [CrossRef]
- Rayman, M.; Thompson, A.; Warren-Perry, M.; Galassini, R.; Catterick, J.; Hall, E.; Lawrence, D.; Bliss, J. Impact of Selenium on Mood and Quality of Life: A Randomized, Controlled Trial. Biological Psychiatry 2006, 59, 147–154. [Google Scholar] [CrossRef]
- Scherer, S.; Jansen, L.; Boakye, D.; Hoffmeister, M.; Brenner, H. Changes in Health-Related Outcomes among Colorectal Cancer Patients Undergoing Inpatient Rehabilitation Therapy: A Systematic Review of Observational and Interventional Studies. Acta Oncol 2021, 60, 124–134. [Google Scholar] [CrossRef]
- Vieira, M.L.D.S.; Fonseca, F.L.A.; Costa, L.G.; Beltrame, R.L.; Chaves, C.M. de S.; Cartum, J.; Alves, S.I.P.M. do N.; Azzalis, L.A.; Junqueira, V.B.C.; Pereria, E.C.; et al. Supplementation with Selenium Can Influence Nausea, Fatigue, Physical, Renal, and Liver Function of Children and Adolescents with Cancer. J Med Food 2015, 18, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Sun, Q.; Oltra, E.; Dijck-Brouwer, D.A.J.; Chillon, T.S.; Seemann, P.; Asaad, S.; Demircan, K.; Espejo-Oltra, J.A.; Sánchez-Fito, T.; Martín-Martínez, E.; et al. Autoantibodies to Selenoprotein P in Chronic Fatigue Syndrome Suggest Selenium Transport Impairment and Acquired Resistance to Thyroid Hormone. Redox Biol 2023, 65, 102796. [Google Scholar] [CrossRef]
- Arndt, V.; Merx, H.; Stegmaier, C.; Ziegler, H.; Brenner, H. Quality of Life in Patients with Colorectal Cancer 1 Year after Diagnosis Compared with the General Population: A Population-Based Study. J Clin Oncol 2004, 22, 4829–4836. [Google Scholar] [CrossRef] [PubMed]
- Thong, M.S.Y.; Koch-Gallenkamp, L.; Jansen, L.; Bertram, H.; Eberle, A.; Holleczek, B.; Waldeyer-Sauerland, M.; Waldmann, A.; Zeissig, S.R.; Brenner, H.; et al. Age-Specific Health-Related Quality of Life in Long-Term and Very Long-Term Colorectal Cancer Survivors versus Population Controls - a Population-Based Study. Acta Oncol 2019, 58, 801–810. [Google Scholar] [CrossRef]
Figure 1.
Selenium deficiency in colon cancer patients after supplementation with 300 µg or 600 µg selenium per day. ** p < 0.01.
Figure 1.
Selenium deficiency in colon cancer patients after supplementation with 300 µg or 600 µg selenium per day. ** p < 0.01.
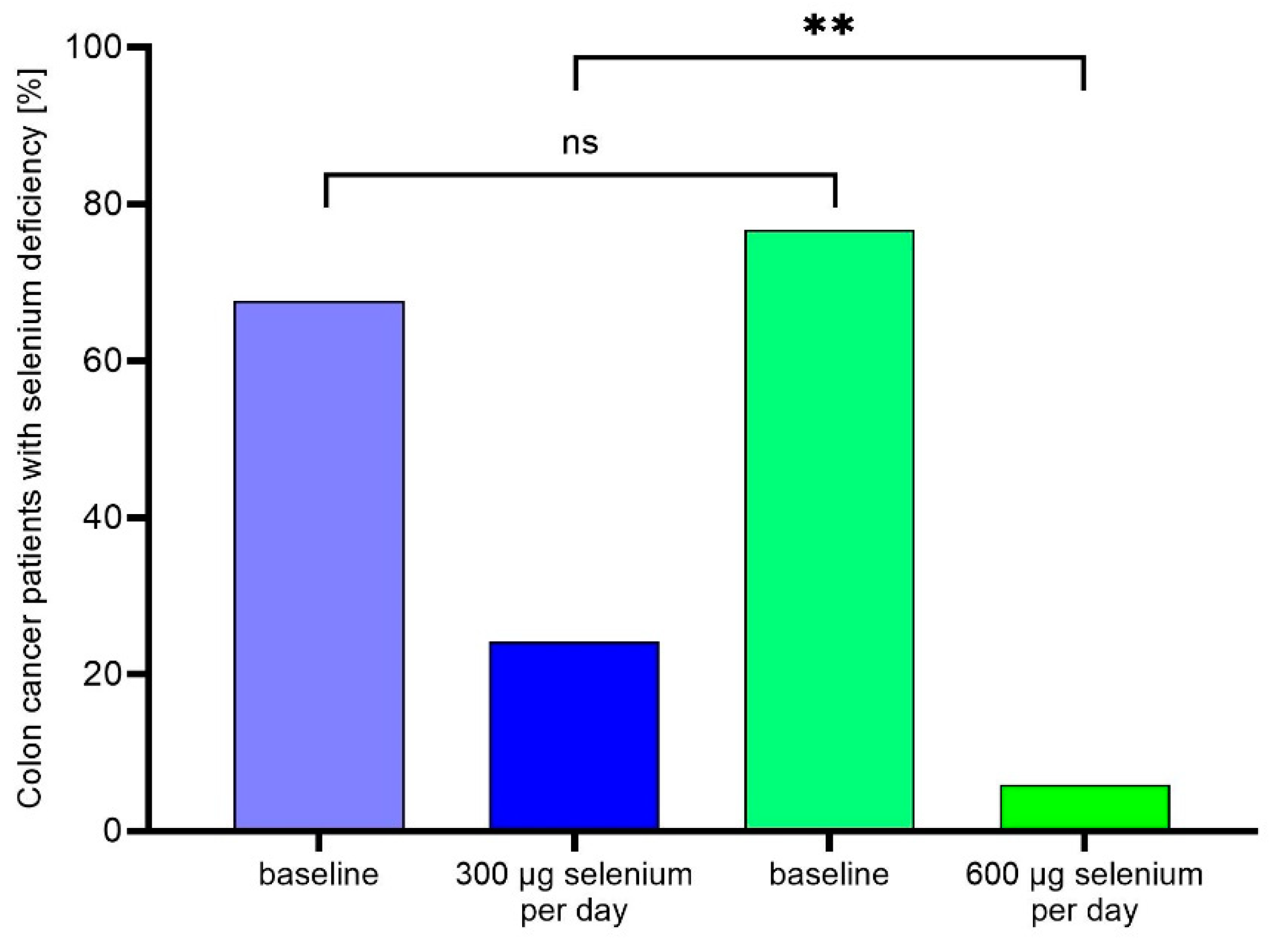
Figure 2.
Median whole blood selenium concentration (95% CI) with individual values in (a) colon (blue n = 34; red n = 28), (b) pancreas (blue n = 27; red n = 25), (C) breast cancer patients (blue n = 6; red n = 8), and (d) all cancer patients with three measurements. Blue Values: Increasing selenium status 3 months after rehabilitation; Violet values: Decreasing selenium status 3 months after rehabilitation. Green lines indicate the German reference range for whole blood selenium concentration. * p < 0.05; ** p < 0.01; **** p < 0.0001.
Figure 2.
Median whole blood selenium concentration (95% CI) with individual values in (a) colon (blue n = 34; red n = 28), (b) pancreas (blue n = 27; red n = 25), (C) breast cancer patients (blue n = 6; red n = 8), and (d) all cancer patients with three measurements. Blue Values: Increasing selenium status 3 months after rehabilitation; Violet values: Decreasing selenium status 3 months after rehabilitation. Green lines indicate the German reference range for whole blood selenium concentration. * p < 0.05; ** p < 0.01; **** p < 0.0001.
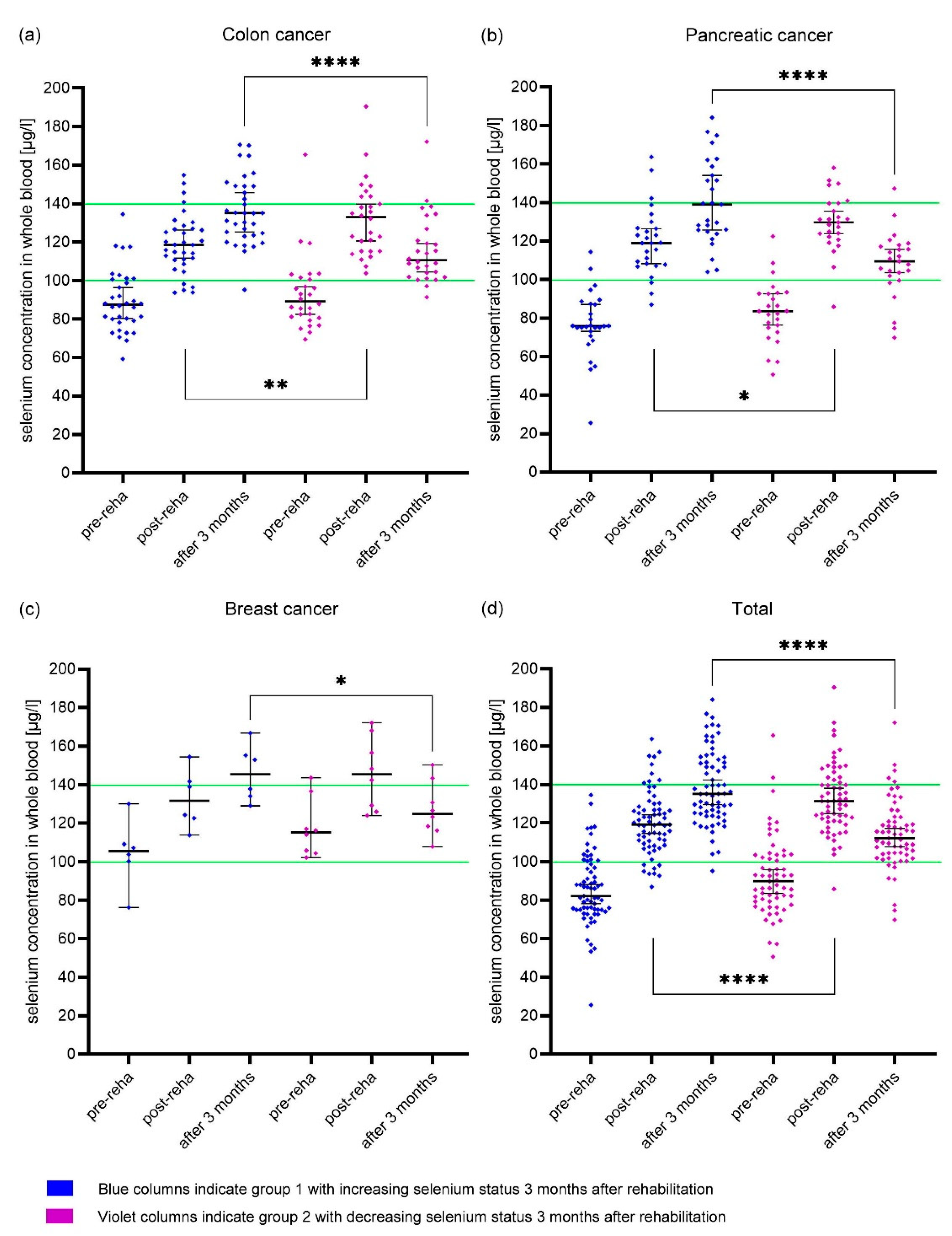
Figure 3.
Median EORTC QLQ-C30 values (95 % CI) at the beginning (pre-reha) and the end (post-reha) of rehabilitation, and after 3 months. (a) + (c) + (e) colon cancer patients; (b) + (d) + (f) pancreatic cancer patients. Blue Values: Increasing selenium status 3 months after rehabilitation; Violet values: Decreasing selenium status 3 months after rehabilitation. Scale from 0 to 100 with 100 reflecting the best possible score for functioning scales and the worst score for symptom scales. [37] * p < 0.05; ** p < 0.01; *** p < 0.001; **** p < 0.0001.
Figure 3.
Median EORTC QLQ-C30 values (95 % CI) at the beginning (pre-reha) and the end (post-reha) of rehabilitation, and after 3 months. (a) + (c) + (e) colon cancer patients; (b) + (d) + (f) pancreatic cancer patients. Blue Values: Increasing selenium status 3 months after rehabilitation; Violet values: Decreasing selenium status 3 months after rehabilitation. Scale from 0 to 100 with 100 reflecting the best possible score for functioning scales and the worst score for symptom scales. [37] * p < 0.05; ** p < 0.01; *** p < 0.001; **** p < 0.0001.
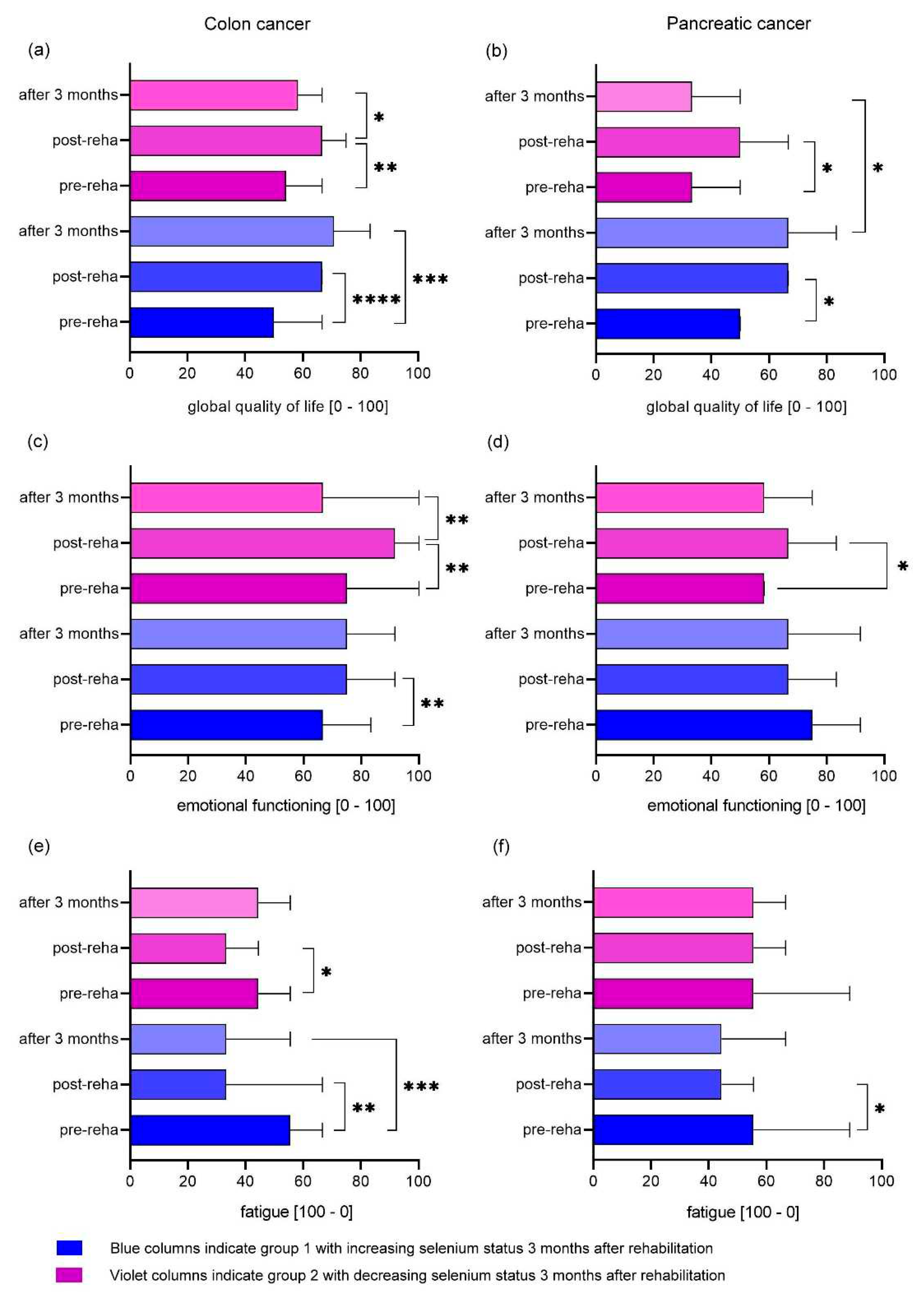

Table 1.
Descriptive characteristics of patients.
| Characteristic | Breast cancer | Pancreatic cancer | Colon cancer |
|---|---|---|---|
| Sample, n | 50 | 101 | 120 |
| Sex (f/m) | 98% / 2% | 64% / 36% | 53% / 47 % |
| Age, years, mean ± SD | 62 ± 10 | 71 ± 11 | 69 ± 11 |
| Operation | 100% | 87% | 97% |
| Chemotherapy | |||
| Planned | 26% | 40% | 7% |
| ongoing | 0% | 20% | 6% |
| after | 34% | 28% | 41% |
| none | 40% | 11% | 47% |
| Radiotherapy | 76% | 4% | 21% |
| Hormone therapy | 78% | - | - |
| Selenium status †, µg/l, mean± SD | 107.2 ± 18.4 | 80.5 ± 15.5 | 90.0 ± 17.6 |
| Prior selenium supplementation | 28% | 1% | 8% |
| Zinc status §, mg/l, mean ± SD | 5.9 ± 0.8 | 6.0 ± 0.8 | 6.0 ± 0.9 |
| Prior zinc supplementation | 0% | 0% | 2% |
† Selenium concentration in whole blood; § Zinc concentration in whole blood.
Table 2.
Selenium and zinc deficiency in cancer patients.
| Characteristic | Breast cancer | Pancreatic cancer | Colon cancer |
|---|---|---|---|
| Sample, n | 50 | 101 | 120 |
| Selenium deficiency † | |||
| Begin rehabilitation | 36% | 90% | 74% |
| End rehabilitation | 4% | 7% | 11% |
| 3 month after rehabilitation | 0% | 6% | 3% |
| Zinc deficiency § | |||
| Begin rehabilitation | 0% | 0% | 1% |
| End rehabilitation | 0% | 0% | 1% |
| 3 month after rehabilitation | 0% | 0% | 1% |
† Selenium concentration in whole blood; § Zinc concentration in whole blood.
Table 3.
EORTC QLQ-30 mean scores (SD) of breast cancer patients at begin and end of rehabilitation, and three month thereafter.
Table 3.
EORTC QLQ-30 mean scores (SD) of breast cancer patients at begin and end of rehabilitation, and three month thereafter.
| pre-reha | post-reha | 3 month after rehabilitation | p-trend | |
|---|---|---|---|---|
| Functional scales and global QoL | ||||
| Physical functioning | 73.6 (16.5) | 80.0 (16.7) | 83.1 (14.6) | 0.0012 |
| Role functioning | 56.1 (26.5) | 68.7 (26.1) | 62.8 (26.5) | 0.0253 |
| Emotional functioning | 57.6 (27.3) | 75.4 (20.3) | 58.3 (21.0) | < 0.0001 |
| Cognitive functioning | 67.7 (29.5) | 76.9 (24.5) | 61.6 (26.7) | 0.0752 |
| Social functioning | 64.2 (27.5) | 74.8 (24.1) | 74.4 (26.0) | 0.0191 |
| Global QoL | 55.6 (15.9) | 68.4 (15.3) | 64.1 (15.7) | < 0.0001 |
| Symptom Scales | ||||
| Fatigue | 48.6 (27.6) | 38.2 (22.7) | 45.3 (20.0) | 0.0030 |
| Nausea/Vomiting | 5.5 (11.5) | 2.7 (9.2) | 2.6 (6.3) | 0.0324 |
| Pain | 39.8 (32.2) | 28.9 (27.4) | 32.1 (26.8) | 0.0329 |
| Dyspnea | 29.9 (33.9) | 26.5 (28.9) | 25.6 (20.0) | 0.3564 |
| Sleep disturbance | 54.4 (31.7) | 44.2 (36.3) | 51.3 (37.6) | 0.0395 |
| Appetite loss | 10.4 (24.0) | 7.5 (20.7) | 10.3 (16.0) | 0.3470 |
| Constipation | 14.6 (25.6) | 10.4 (21.9) | 10.3 (28.5) | 0.2214 |
| Diarrhea | 6.1 (16.2) | 8.2 (21.0) | 7.7 (14.6) | 0.4660 |
| Financial problems | 19.1 (28.4) | 15.0 (27.3) | 7.7 (14.6) | 0.1754 |
Table 4.
EORTC QLQ-30 mean scores (SD) of pancreatic cancer patients at begin and end of rehabilitation, and three month thereafter.
Table 4.
EORTC QLQ-30 mean scores (SD) of pancreatic cancer patients at begin and end of rehabilitation, and three month thereafter.
| pre-reha | post-reha | 3 month after rehabilitation | p-trend | |
|---|---|---|---|---|
| Functional scales and global QoL | ||||
| Physical functioning | 54.5 (24.6) | 63.4 (22.6) | 63.2 (19.6) | < 0.0001 |
| Role functioning | 41.5 (33.4) | 54.5 (30.4) | 52.9 (29.6) | 0.0004 |
| Emotional functioning | 58.3 (28.5) | 67.6 (25.6) | 60.6 (28.1) | 0.0041 |
| Cognitive functioning | 70.3 (27.4) | 76.8 (23.6) | 72.7 (26.2) | 0.0653 |
| Social functioning | 51.7 (33.6) | 62.0 (33.1) | 57.9 (34.8) | 0.0136 |
| Global QoL | 42.9 (23.1) | 54.1 (20.8) | 51.7 (21.3) | < 0.0001 |
| Symptom Scales | ||||
| Fatigue | 60.9 (29.6) | 49.1 (25.7) | 49.4 (23.1) | < 0.0001 |
| Nausea/Vomiting | 17.0 (26.2) | 11.0 (20.4) | 9.7 (13.4) | 0.2027 |
| Pain | 41.1 (34.1) | 32.3 (28.3) | 31.0 (27.1) | 0.0162 |
| Dyspnea | 31.6 (32.4) | 31.9 (29.5) | 27.8 (28.2) | 0.4334 |
| Sleep disturbance | 44.6 (34.8) | 36.9 (33.0) | 38.9 (31.4) | 0.0782 |
| Appetite loss | 47.3 (40.3) | 37.6 (36.5) | 26.9 (29.6) | 0.0016 |
| Constipation | 17.7 (30.2) | 37.6 (36.5) | 9.3 (2.5) | < 0.0001 |
| Diarrhea | 33.7 (35.8) | 17.8 (30.2) | 30.6 (33.2) | 0.0007 |
| Financial problems | 18.9 (27.2) | 16.9 (24.0) | 24.1 (31.5) | 0.3145 |
Table 5.
EORTC QLQ-30 mean scores (SD) of colon cancer patients at begin and end of rehabilitation, and three month thereafter.
Table 5.
EORTC QLQ-30 mean scores (SD) of colon cancer patients at begin and end of rehabilitation, and three month thereafter.
| pre-reha | post-reha | 3 month after rehabilitation | p-trend | |
|---|---|---|---|---|
| Functional scales and global QoL | ||||
| Physical functioning | 66.1 (21.5) | 73.1 (20.4) | 76.0 (19.3) | < 0.0001 |
| Role functioning | 51.8 (33.4) | 65.8 (28.2) | 64.0 (27.8) | < 0.0001 |
| Emotional functioning | 65.7 (24.5) | 77.2 (22.6) | 69.3 (27.7) | < 0.0001 |
| Cognitive functioning | 81.7 (27.3) | 82.7 (23.1) | 72.0 (28.3) | 0.0244 |
| Social functioning | 65.7 (31.8) | 76.0 (27.4) | 74.2 (28.0) | 0.0257 |
| Global QoL | 51.9 (22.2) | 64.4 (16.8) | 62.9 (18.7) | < 0.0001 |
| Symptom Scales | ||||
| Fatigue | 48.6 (27.6) | 35.7 (26.1) | 37.0 (27.1) | < 0.0001 |
| Nausea/Vomiting | 6.4 (14.8) | 5.4 (15.0) | 4.2 (16.1) | 0.2520 |
| Pain | 36.3 (32.9) | 25.3 (27.5) | 20.1 (26.1) | < 0.0001 |
| Dyspnea | 23.8 (30.7) | 26.8 (29.6) | 16.7 (26.4) | 0.0871 |
| Sleep disturbance | 43.5 (35.0) | 38.0 (32.4) | 34.9 (28.7) | 0.0868 |
| Appetite loss | 18.3 (28.9) | 12.3 (20.9) | 11.4 (22.7) | 0.2797 |
| Constipation | 17.1 (28.9) | 11.1 (22.9) | 12.4 (20.6) | 0.3007 |
| Diarrhea | 27.7 (32.7) | 16.4 (25.2) | 22.7 (25.7) | 0.0004 |
| Financial problems | 19.1 (29.3) | 18.8 (30.3) | 13.6 (28.1) | 0.3350 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



