Submitted:
11 August 2023
Posted:
14 August 2023
You are already at the latest version
Abstract
The scope of this paper is to compare different dental sealants and flow materials indicated for sealing pit and fissures considering their chemical formula. The narrative review aims to address the questions: What is the essence of different dental sealants’ activity, how their chemical formula affects their mechanisms of caries prevention and what makes a dental sealant efficient mean of caries prevention. Another vital issue is whether the sealants which contain fluoride, or any other additions have potentially increased antimicrobial properties. Methods: An electronic search of the PubMed, Cochrane, Web of Science and Scopus databases was performed. The following keywords were used: (dental sealants) AND (chemical composition). Additionally, information about composition and indications for clinical use provided by manufacturers were utilized. The review aims are to find crucial elements of sealants’ composition which affect their cariostatic mechanisms.
Keywords:
sealants
; dental
; fluoride
; marginal integrity
; caries prevention
; resin-based sealants
; composition
1. Introduction
According to World Health Organization (WHO), dental caries is a major public health problem globally and is the most widespread Noncommunicable Disease (NCD). Moreover, the WHO states that: “Dental caries can be prevented by avoiding dietary free sugars (…) is largely preventable through simple and cost-effective population-wide and individual interventions, whereas treatment is costly, and is often unavailable in low- and middle-income countries” [1]. To present the scale of the phenomena of untreated caries, the results of systematic review on the global burden of untreated caries can be referenced to. It reported that between 1990 and 2010 caries prevalence worldwide affected 2.4 billion people [2]. Over recent years, methods of prevention of tooth decay are shifting towards minimal intervention dentistry. Tendency to preserve as many natural tooth tissues as possible and nonrestorative approach are promoted [3].
Fluoride is an important factor in caries prevention. It has a proved impact both on cariogenic bacteria and on maintaining balance between the processes of demineralization and remineralization. It may disturb bacteria’s metabolism and adherence to the enamel. Moreover, fluoride ions, when present in saliva in a sufficient amount, delay demineralization and promote enamel remineralization [4]. It is worth mentioning that antibacterial properties of fluoride are as important as the process of remineralization of hard tooth tissues. The mechanism of fluoride's antibacterial action considers diffusion of fluoride ions into the bacterial cell. At acidic pH values, enolase and adenosine triphosphatase enzymes are inactivated. Fluoride is also indicated to block the carbohydrate cycle, nonetheless scientists dispute over the exact antibacterial effect of fluoride [5]. The aforementioned multidirectional activity of fluoride is depicted graphically on Figure 1.
Dental sealants were first introduced in the 1960s, in scope of helping to prevent dental caries, mainly in the pits and fissures of occlusal tooth surfaces [6]. Since their introduction to the market, sealants are frequently mentioned as dental materials serving for caries prevention and managing early caries lesions [4]. Their effectiveness in preventing and detaining pit-and-fissure occlusal carious lesions of primary and permanent molars was concluded in a clinical guideline by the American Dental Association and the American Academy of Paediatric Dentistry [7]. The aim of this narrative review is to summarize the information on fissure sealants with particular emphasis on their composition as well as physicochemical and biological properties.
2. Methods
The review revolves around the following questions: What is the essence of action of different dental sealants and how their composition affects their effectiveness in caries prevention; Do the sealants contain fluoride and by means of what mechanisms they release it to the environment of oral cavity? An electronic search of the PubMed, Cochrane, Web of Science, Google Scholar and Scopus databases was performed. The following keywords were used: (dental sealants) AND (chemical composition) according to MeSH terms. Information about chemical composition of some commonly used dental sealants provided by manufactures were found.
3. Results
3.1. Comparison of Composition of Commercially Used Materials
Commercial sealants differ in the composition of matrix, added fillers or presence of fluoride. Their structure directly influences their properties. Therefore, a literature-based comparison of 19 different commercial sealants was performed. Juxtaposition was executed with respect to product name, abbreviation (for the sake of discussion), manufacturer, composition, presence of fluoride (Table 1). Furthermore, the experimental properties influencing their clinical performance included shear bond strength, hardness and shrinkage. The references include peer-reviewed publications as well as Material Safety Data Sheets of the materials and other data shared by manufacturers. The table is lacking in parameters for few materials which indicate the gap in knowledge for further research on commercial materials.
The shear bond strength of the analyzed sealants ranged from 3.5 ± 0.8 MPa for FT up to 42.6 ± 3.2 for GS. In terms of hardness, HF possesses the lowest value (19.3 HV) and EGF the highest (99.3 ± 4.5 HV). Ultimately, shrinkage of the presented materials is within the range of 1.95 - 7.40% the lowest end being TEC and the highest TF1.
3.2. Modifications in Composition
Biomaterials used in dentistry are constantly evaluated to meet demands of clinical needs. Non-invasive approach and prevention are promoted in modern dentistry. Modifications of materials are performed to enhance their clinical behavior. Among desired traits of materials dedicated for sealing we may list durability, easiness of application or bacteriostatic potential.
In order to decrease biofilm viability on the surface of resin-based sealant its composition can be altered. Study presents that doping a methacrylate monomer matrix with 2.5 wt.% of 1,3,5-triacryloylhexahydro-1,3,5-triazine (TAT) in dental sealant’s structure impacts its cytotoxicity, biofilm formation and physicochemical properties [37]. TAT exhibits antibacterial, antiviral, antifungal, and antiprotozoal activity. The results showed potential enhancement in antibacterial potential of dental sealant. The modified material did not show cytotoxic effect or decrease in any other physicochemical properties.
Another example of structural modification of dental sealant available on the market includes incorporation of methacryloxylethyl cetyl dimethyl ammonium chloride (DMAE-CB) into Helioseal pit and fissure sealant [38]. Since microleakage is claimed to be one of the major causes of secondary caries, authors of this study assumed, that it is crucial to increase it along with antibacterial activity of a sealant. Properties of a doped material including contact angle, degree of conversion, microhardness and microleakage remained similar to the origin material being a control group. A study concluded that the incorporation of small amounts (one percent of weight) of the monomer DMAE-CB into Helioseal may inhibit the growth of Streptococcus mutans and be an effective way of secondary caries prevention.
The antibacterial action of a dental material may be also obtained by an incorporation of acrylated hydroxyazobenzene (AHA) copolymers into a composite-resin matrix [39]. The study was based on samples of bisphenol A-glycidyl methacrylate and triethylene glycol dimethacrylate (bisGMA:TEGDMA) with and without AHA doping. It resulted in the same level of biocompatibility of both materials. Moreover, an inhibitory effect of AHA addiction on Streptococcus mutans biofilm growth was observed [40]. Authors claim, AHA may be incorporated into restorative and sealing materials in order to increase anticaries potential of dental materials.
As we may see in the Table 1. some of the materials for sealing contain fluoride in different forms, whereas others do not have it in their composition at all. Role of fluoride ions in caries prevention is important and was briefly described in the introduction paragraph. The study comparing sealant containing fluoride and without it showed differences in enamel hardness after cariogenic challenge [41]. Experiment was performed on blocks of human third molars and showed no significant differences between materials in aspect of marginal adaptation. However, it concluded that using fluoride sealant is recommended to prevent caries in high-caries-risk patients because of its favorable impact on enamel’s hardness decrease. The chemical structure of aforementioned compounds used for doping sealing materials is depicted on the Figure 2.
3.3. Indications for Use
All of the considered materials defined as dental sealants are described by manufacturers as indicated to seal fissures, pits and foramina caeca of primary and permanent teeth. At the same time allergies or hypersensitivity for any ingredient of the material and inability to keep operative field dry are defined as contraindications. Flow composite indicated as suitable for sealing or releasing fluoride were also took into consideration into this study. Some of the materials are clearly indicated to extended fissure sealing, e.g., TF. Among analysed dental sealants that contain fluoride are HF, EW, FT, SSLF, F7E, GCP, KM, IMAC, USXT, TF, TEC, CS, FFX, DS and TF1.
The review based on several research, concluded that caries may be avoided in 60% of sealed surfaces [42]. At the same time, author notices that the beneficial effect is more significant in population of high caries baseline risk. The article points out that both resin and glass ionomer sealants are indicated as effective method of caries prevention. The time which is indicated as the most appropriate for sealing is a first year after eruption of the first molar and first two to three years regarding the second molar.
On may planes dental sealants are described as materials indicated to prevent caries and manage early carious lesions [4]. Once again, it is concluded that the most beneficial effect of sealing is obtained in the groups, mostly children, characterised by a high caries risk. Among the limitations of optimal sealant application authors list operator’s and cooperation’s dependent factors, such as optimum isolation, cleaning of the tooth surface and etching.
3.4. Microleakage and Adhesion
One of the desired features of restorative material is its durability. It depends on many factors and adhesion is one of them. The criteria considered in number of studies is marginal adaptation and microleakage as a factor describing material’s potential of durability and efficiency. Adhesion depends not only on material itself but also on widely recognized surface preparation. Conditioning of the surface should provoke better retention of the material which is mainly mechanical as the physico-chemical interaction between the resin and etched enamel is small [43]. The essence of its action considering hard dental tissues bases on fulfilling the pores by resin monomers which are polymerised and are interlocked [44]. Etching has an impact on enamel dissolving rods and creating microporosities which can be penetrated by a material [45]. Adhesion which enables junction between dental material and hard tissues of the tooth is also a part of aforementioned non-invasive approach, as it promotes preserving sound dental structures. Producers usually provide user of the sealer with an instruction containing indications for use. Most of them advice to etch the enamel surface prior to applying a material by a 37% phosphoric acid for around 30 seconds (e.g. for 20-40 seconds such as in case of Arkona dental sealant [46]. It is a protocol commonly followed by clinicians which has support in numerous studies and sheets for the users attached to materials for sealing [47,48].
A lot of studies aim to find the best way of conditioning enamel surface so that pit and fissure sealing is most effective, which means has the lowest microleakage or better retention. The comparison of acid-etching, laser or combination of them both was tested in the contest of different sealants [49,50,51,52]. All above mentioned studies concern human teeth and natural enamel tissue. Most of them were performed on extracted teeth apart from one, which was conducted in the oral cavity of patients and controlled for one year [51]. This study concluded that both ways of conditioning – laser and acid-etching are successful in promoting sealant retention and in all cases there was no secondary caries detected. The studies on extracted teeth used an artificial samples ageing by using a thermocycling and water bath. The microleakage was assessed by imaging methods such as stereo-microscope, electron microscopy with energy-dispersive X-ray or SEM. It is worth mentioning that, all the researchers noticed some differences provoked not only by conditioning method but also by a material chosen. Better acid-etching (Effect of acid etching and different Er:YAG laser procedures on microleakage of three different fissure sealants in primary teeth after aging) In the most studies, no differences between acid or laser conditioning was noticed but combination of laser irradiation and acid etching resulted in a lower microleakage [50,52].
The study on twenty bovine incisors concluded that conditioning the surface of enamel provokes a higher bond strength under artificial aging. An ultrasound enamel preparation was compared with classical bur preparation on pit and fissure sealing in context of caries prevention[53]. Fissures of extracted third molars were prepared in different ways and sealed and assessed with SEM. Study shows that conventional bur preparation prior to sealing gives better retention and may be more effective in caries prevention than ultrasound preparation. Another approach is showed in the study which prepared an enamel not only with etching, but also with combinations with the use of the bonding agents or chlorhexidine digluconate [54]. Authors of this 6-month in vitro research claimed that microleakage reduction is most effective in case of conventional acid etching alone or with a one-bottle adhesive, while it is increased by applying of chlorhexidine digluconate. Conventional etching was also compared to self-etch method in a study conducted on third molars and shear bond strength was checked. This study showed superiority of self-etch preparation for applying a sealer in comparison to etching, adding that results depend also on chemical composition of the materials and content of 10-methacryloyloxydecyl dihydrogen phosphate [55]. At that point, it is worth mentioning that in general it is claimed, that self-etch systems require selective-etching by phosphoric acid anyway [56,57,58]. Conditioning enamel surface by acid-etching or no conditioning at all was also studied [59] and concluded that etching the surface promotes adhesion of the sealant and enamel.
Another aspect of adhesion considering composite materials is bonding procedures. Usually considering dental sealants, usage of bonding agent is not recommended by the manufacturer. However, it is regarded to use an adhesive to obtain better retention of composite materials. As mentioned at the beginning of this paragraph, adhesion is obtained by fulfilling the pores in the hard dental tissues by resin monomers which are polymerised and are micromechanically interlocked. Bonding agents penetrates microporosities, which were revealed after etching, by capillary attraction [60]. A clinical trial was performed at group of children aged 5-15, to compare retention of sealants with or without using a bonding agent within 12 months. The study concluded that ethanol-based bonding agent significantly increased the retention of sealants on different surfaces of teeth [61].
Taking all the above-mentioned studies into consideration we may assume, that conditioning the enamel prior to sealing has an impact on quality of sealing. That means, in general, there is significantly lower microleakage and better retention of the material. However, there are many studies promoting different approaches than given by the manufacturers which require further assessment to be commonly accepted. Bonding the enamel surface prior to applying sealant seems to be promising approach.
4. Discussion
Caries is a common disease. Due to difficulties with maintaining proper hygiene and greater susceptibility of milk teeth to caries, children are more exposed to it than adults. It is estimated that nowadays 621 million children in the world suffer from tooth decay. In Europe it affects 20 to 80% of children, depending on the level of development of the country [62]. Fissure sealants are commonly used materials, especially in the paediatric dentistry. Sealing is an effective way to prevent caries in permanent molar and premolar teeth. Lacquers are also utilised in case of minor carious lesions located in the fissures, as well as PRR method. The content of fluoride in the materials enable remineralization of hard tooth tissues and has a bactericidal effect. These are key features for young people who often have poor oral hygiene [63,64,65].
Numerous studies prove the high effectiveness of fissure sealants in prevention of caries formation. According to Fernandez Barrera M.A., the differences between the effectiveness of individual products of different companies are not clinically significant [66]. Considering materials used in the dental office, their price may be regarded as an important economical factor. While dental caries is a very common health problem globally and dental sealants are perceived as accessible mean of caries prevention, the differences in their prices may be significant. Therefore, it is important to choose the optimal material that will have good tissue retention and effectively prevent the caries formation. Multiple researches clearly indicate high effectiveness of fissure sealants in caries prevention [67]. Yet, the chemical formula and mechanical properties of the material are not the only factors that determine its efficacy. The clinical success of sealing pits and fissures lays also in operator’s dependent factors and cooperation with the patient. Furthermore, it is worth to note, that sealing materials are compared to another method of prevention – fluoridation. Nonetheless, the application of fluoride usually considers full dentition present in the oral cavity of the patient instead of selected teeth surfaces. It should be emphasized that properly applied sealing does not have to be repeated regularly so as fluoridation [68].
As the meter of fact, market offers a wide variety of dental materials dedicated for sealing. The multiple studies prove their effectiveness in caries prevention. The beneficial effect of sealing pits and fissures depends both on sealing procedure and material’s choice. Modifying dental sealants striving for increasing their cariostatic potential may be an interesting direction of dental materials’ development. The research should not only be a R&D focus, but also a subject of interest of scientists around the world.
Funding
The authors would like to acknowledge the National Science Centre Poland (NCN) for financial support within the Project “Evaluation of biocompatibility, antibacterial properties, marginal integrity and fluoride release rate of dental sealants doped with nanoparticles of copper and fluoroapatite in in vitro studies” (No. DEC-2022/06/X/NZ7/01317). This article was also co-financed by a subsidy from Wroclaw Medical University, number SUBZ.B180.23.054.
Acknowledgements
Declaration of Interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
- World Health Organization Sugars and Dental Caries. Available online: https://www.who.int/news-room/fact-sheets/detail/sugars-and-dental-caries.
- Kassebaum, N.J.; Bernabé, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.L.; Marcenes, W. Global Burden of Untreated Caries: A Systematic Review and Metaregression. J Dent Res 2015, 94, 650–658. [Google Scholar] [CrossRef] [PubMed]
- Yu, O.Y.; Lam, W.Y.H.; Wong, A.W.Y.; Duangthip, D.; Chu, C.H. Nonrestorative Management of Dental Caries. Dent J (Basel) 2021, 9. [Google Scholar] [CrossRef]
- Naaman, R.; El-Housseiny, A.A.; Alamoudi, N. The Use of Pit and Fissure Sealants-a Literature Review. Dent J (Basel) 2017, 5, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Rošin-Grget, K.; Peroš, K.; Sutej, I.; Bašić, K. The Cariostatic Mechanisms of Fluoride. Acta Med Acad 2013, 42, 179–188. [Google Scholar] [CrossRef]
- Ahovuo-Saloranta, A.; Forss, H.; Walsh, T.; Nordblad, A.; Mäkelä, M.; Worthington, H. V. Pit and Fissure Sealants for Preventing Dental Decay in Permanent Teeth. Cochrane Database of Systematic Reviews 2017, 2017. [Google Scholar] [CrossRef]
- Wright, J.T.; Crall, J.J.; Fontana, M.; Gillette, E.J.; Nový, B.B.; Dhar, V.; Donly, K.; Hewlett, E.R.; Quinonez, R.B.; Chaffin, J.; et al. Evidence-Based Clinical Practice Guideline for the Use of Pit-and-Fissure Sealants: A Report of the American Dental Association and the American Academy of Pediatric Dentistry. Journal of the American Dental Association 2016, 147, 672–682.e12. [Google Scholar] [CrossRef] [PubMed]
- Arumugam, P. Comparative Evaluation of the Effect of Variation in Light-Curing Cycle with a Time Gap and Its Effect on Polymerization Shrinkage and Microhardness of Conventional Hydrophobic Sealants and Moisture-Tolerant Resin-Based Sealants: An in Vitro Study. Indian Journal of Multidisciplinary Dentistry 2018, 8, 13. [Google Scholar] [CrossRef]
- Babaji, P.; Vaid, S.; Deep, S.; Mishra, S.; Srivastava, M.; Manjooran, T. In Vitro Evaluation of Shear Bond Strength and Microleakage of Different Pit and Fissure Sealants. J Int Soc Prev Community Dent 2016, 6, S111. [Google Scholar] [CrossRef]
- Pulpdent Corporation Embrace WetBond Safety Data Sheet. Available online: https://www.pulpdent.com/wp-content/uploads/2021/03/GHS-SDS-EMS.pdf (accessed on 23 July 2023).
- Panigrahi, A. Microtensile Bond Strength of Embrace Wetbond Hydrophilic Sealant in Different Moisture Contamination: An In-Vitro Study. JOURNAL OF CLINICAL AND DIAGNOSTIC RESEARCH 2015, 9, ZC23. [Google Scholar] [CrossRef]
- Kucukyilmaz, E.; Savas, S. Evaluation of Shear Bond Strength, Penetration Ability, Microleakage and Remineralisation Capacity of Glass Ionomer-Based Fissure Sealants. Eur J Paediatr Dent 2016, 17, 17–23. [Google Scholar]
- Arslanoğlu, Z.; Altan, H.; Kale, E.; Bılgıç, F.; Şahin, O. Nanomechanical Behaviour and Surface Roughness of New Generation Dental Fissure Sealants. Acta Phys Pol A 2016, 130, 388–393. [Google Scholar] [CrossRef]
- Muwaffaq Attash, Z.; Sami Gasgoos, Z. Shear Bond Strength of Four Types of Pit and Fissure Sealants (In Vitro Study). Int J Enhanc Res Sci Technol Eng 2018, 7. [Google Scholar]
- Kucukyilmaz, E.; Savas, S.; Sener, Y.; Tosun, G.; Botsali, M. Polymerization Shrinkage of Six Different Fissure Sealants. Journal of Restorative Dentistry 2014, 2, 88. [Google Scholar] [CrossRef]
- Zalizniak, I.; Palamara, J.E.A.; Wong, R.H.K.; Cochrane, N.J.; Burrow, M.F.; Reynolds, E.C. Ion Release and Physical Properties of CPP–ACP Modified GIC in Acid Solutions. J Dent 2013, 41, 449–454. [Google Scholar] [CrossRef] [PubMed]
- Elkwatehy, W.M.A.; Bukhari, O.M. The Efficacy of Different Sealant Modalities for Prevention of Pits and Fissures Caries: A Randomized Clinical Trial. J Int Soc Prev Community Dent 2019, 9, 119. [Google Scholar] [CrossRef] [PubMed]
- Gavic, L.; Gorseta, K.; Borzabadi-Farahani, A.; Tadin, A.; Glavina, D.; van Duinen, R.; Lynch, E. Influence of Thermo-Light Curing with Dental Light-Curing Units on the Microhardness of Glass-Ionomer Cements. Int J Periodontics Restorative Dent 2016, 36, 425–430. [Google Scholar] [CrossRef]
- Murthy, S.S.; Murthy, G.S. Comparative Evaluation of Shear Bond Strength of Three Commercially Available Glass Ionomer Cements in Primary Teeth. J Int Oral Health 2015, 7, 103. [Google Scholar]
- VOCO Ionofil Safety Data Sheet. Available online: https://www.voco.dental/en/portaldata/1/resources/products/safety-data-sheets/gb/voco-ionofil-molar-ac_sds_gb.pdf (accessed on 23 August 2022).
- Shebl, E.A.; Etman, W.M.; Genaid, Th.M.; Shalaby, M.E. Durability of Bond Strength of Glass-Ionomers to Enamel. Tanta Dental Journal 2015, 12, 16–27. [Google Scholar] [CrossRef]
- Ultradent Ultraseal XT Brochure. Available online: https://assets.ctfassets.net/wfptrcrbtkd0/6CDOVq0rW3Ia1bBseRnDYG/5de0b1fac706906d9c3577d36589e1ad/UltraSeal-XT-Sealant-Family-Sales-Sheet-1007280AR03.pdf.
- Ultradent UltraSeal XT plus Safety Data Sheet. Available online: https://optident.co.uk/app/uploads/2018/03/UltraSeal-XT%C2%AE-plus-SDS-English.pdf (accessed on 8 August 2023).
- Hannig, C.; Duong, S.; Becker, K.; Brunner, E.; Kahler, E.; Attin, T. Effect of Bleaching on Subsurface Micro-Hardness of Composite and a Polyacid Modified Composite. Dental Materials 2007, 23, 198–203. [Google Scholar] [CrossRef]
- Ivoclar Vivadent Tetric EvoFlow Satety Data Sheet. Available online: https://us.vwr.com/assetsvc/asset/en_US/id/16490607/contents.
- Oglakci, B.; Arhun, N. The Shear Bond Strength of Repaired High-Viscosity Bulk-Fill Resin Composites with Different Adhesive Systems and Resin Composite Types. 2019, 33, 1584–1597. [Google Scholar] [CrossRef]
- Salem, H.; Hefnawy, S.; Nagi, S. Degree of Conversion and Polymerization Shrinkage of Low Shrinkage Bulk-Fill Resin Composites. Contemp Clin Dent 2019, 10, 465. [Google Scholar] [CrossRef]
- Najafi -Abrandabadi, A.; Najafi -Abrandabadi, S.; Ghasemi, A.; Kotick, P.G. Microshear Bond Strength of Composite Resins to Enamel and Porcelain Substrates Utilizing Unfilled versus Filled Resins. Dent Res J (Isfahan) 2014, 11, 636. [Google Scholar]
- Deb, S.; Di Silvio, L.; MacKler, H.E.; Millar, B.J. Pre-Warming of Dental Composites. Dental Materials 2011, 27, e51–e59. [Google Scholar] [CrossRef] [PubMed]
- Alonso, R.C.B.; Correr, G.M.; Borges, A.F.S.; Kantovitz, K.R.; Rontani, R.M.P. Minimally Invasive Dentistry: Bond Strength of Different Sealant and Filling Materials to Enamel. Oral Health Prev Dent 2005, 3, 87–95. [Google Scholar]
- Kuşgöz, A.; Tüzüner, T.; Ülker, M.; Kemer, B.; Saray, O. Conversion Degree, Microhardness, Microleakage and Fluoride Release of Different Fissure Sealants. J Mech Behav Biomed Mater 2010, 3, 594–599. [Google Scholar] [CrossRef] [PubMed]
- Simsek Derelioglu, S.; Yilmaz, Y.; Celik, P.; Carikcioglu, B.; Keles, S. Bond Strength and Microleakage of Self-Adhesive and Conventional Fissure Sealants. Dent Mater J 2014, 33, 530–538. [Google Scholar] [CrossRef] [PubMed]
- VOCO Grandio Seal Safety Data Sheet. Available online: https://www.voco.dental/us/portaldata/1/resources/products/safety-data-sheets/us/grandio-seal_sds_us.pdf (accessed on 8 August 2023).
- Bayrak, G.D.; Gurdogan-Guler, E.B.; Yildirim, Y.; Ozturk, D.; Selvi-Kuvvetli, S. Assessment of Shear Bond Strength and Microleakage of Fissure Sealant Following Enamel Deproteinization: An in Vitro Study. J Clin Exp Dent 2020, 12, e220. [Google Scholar] [CrossRef]
- VOCO Fissurit FX Safety Data Sheet. Available online: https://www.voco.dental/au/portaldata/1/resources/products/safety-data-sheets/au/fissurit-fx_sds_au.pdf (accessed on 8 August 2023).
- Güngör, özge E.; Erdogan, Y.; Yalçin-Güngör, A.; Alkiş, H. Comparative Evaluation of Shear Bond Strength of Three Flowable Compomers on Enamel of Primary Teeth: An in-Vitro Study. J Clin Exp Dent 2016, 8, e322. [CrossRef]
- Garcia, I.M.; Leitune, V.C.B.; Rücker, V.B.; Nunes, J.; Visioli, F.; Collares, F.M. Physicochemical and Biological Evaluation of a Triazine-Methacrylate Monomer into a Dental Resin. J Dent 2021, 114. [Google Scholar] [CrossRef]
- Li, F.; Li, F.; Wu, D.; Ma, S.; Gao, J.; Li, Y.; Xiao, Y.; Chen, J. The Effect of an Antibacterial Monomer on the Antibacterial Activity and Mechanical Properties of a Pit-and-Fissure Sealant. Journal of the American Dental Association 2011, 142, 184–193. [Google Scholar] [CrossRef]
- Mori, D.I.; Powell, A.; Kehe, G.M.; Schurr, M.J.; Nair, D.P.; Puranik, C.P. Acrylated Hydroxyazobenzene Copolymers in Composite-Resin Matrix Inhibits Streptococcus Mutans Biofilms In Vitro. Pediatr Dent 2021, 43, 484–491. [Google Scholar] [PubMed]
- Mori, D.I.; Schurr, M.J.; Nair, D.P. Selective Inhibition of Streptococci Biofilm Growth via a Hydroxylated Azobenzene Coating. Adv Mater Interfaces 2020, 7, 1902149. [Google Scholar] [CrossRef] [PubMed]
- Kantovitz, K.R.; Pascon, F.M.; Nociti, F.H.; Tabchoury, C.P.M.H.; Puppin-Rontani, R.M. Inhibition of Enamel Mineral Loss by Fissure Sealant: An in Situ Study. J Dent 2013, 41, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Mejàre, I. Indications for Fissure Sealants and Their Role in Children and Adolescents. Dent Update 2011, Dec, 699–703. [Google Scholar] [CrossRef]
- Lupi-Pégurier, L.; Bertrand, M.F.; Genovese, O.; Rocca, J.P.; Muller-Bolla, M. Microleakage of Resin-Based Sealants after Er:YAG Laser Conditioning. Lasers Med Sci 2007, 22, 183–188. [Google Scholar] [CrossRef]
- Summitt, J.B.; Robbins, J.W.; Hilton, T.J.; Schwartz, R.S. Fundamentals of Operative Dentistry A Contemporary Approach; 2006; Vol. 5; ISBN 9781119130536.
- Cardoso, M. V.; De Almeida Neves, A.; Mine, A.; Coutinho, E.; Van Landuyt, K.; De Munck, J.; Van Meerbeek, B. Current Aspects on Bonding Effectiveness and Stability in Adhesive Dentistry. Aust Dent J 2011, 56, 31–44. [Google Scholar] [CrossRef]
- Arkona Arkona Fissure Sealant Brochure. Available online: https://arkonadent.com/wp-content/uploads/2020/10/arkonadent-lak-szczelinowy-kompendium-wiedzy.pdf (accessed on 8 August 2023).
- Ivoclar Vivadent Helioseal F Instruction of Use. Available online: https://www.dentaltix.com/en/sites/default/files/helioseal_1.pdf (accessed on 8 August 2023).
- SDI Conseal F Brochure. Available online: https://www.sdi.com.au/pdfs/brochures/au/conseal%20f_sdi_brochures_au.pdf (accessed on 8 August 2023).
- Unal, M.; Hubbezoglu, I.; Zan, R.; Kapdan, A.; Hurmuzlu, F. Effect of Acid Etching and Different Er:YAG Laser Procedures on Microleakage of Three Different Fissure Sealants in Primary Teeth after Aging. Dent Mater J 2013, 32, 557–563. [Google Scholar] [CrossRef]
- Güçlü, Z.A.; Dönmez, N.; Tüzüner, T.; Odabaş, M.E.; Hurt, A.P.; Coleman, N.J. The Impact of Er:YAG Laser Enamel Conditioning on the Microleakage of a New Hydrophilic Sealant—UltraSeal XT® HydroTM. Lasers Med Sci 2016, 31, 705–711. [Google Scholar] [CrossRef]
- Karaman, E.; Yazici, A.R.; Baseren, M.; Gorucu, J. Comparison of Acid versus Laser Etching on the Clinical Performance of a Fissure Sealant: 24-Month Results. Oper Dent 2013, 38, 151–158. [Google Scholar] [CrossRef]
- Güçlü, Z.A.; Hurt, A.P.; Dönmez, N.; Coleman, N.J. Effect of Er:YAG Laser Enamel Conditioning and Moisture on the Microleakage of a Hydrophilic Sealant. Odontology 2018, 106, 225–231. [Google Scholar] [CrossRef]
- Ferrazzano, G.F.; Ingenito, A.; Alcidi, B.; Sangianantoni, G.; Schiavone, M.G.; Cantile, T. In Vitro Performance of Ultrasound Enamel Preparation Compared with Classical Bur Preparation on Pit and Fissure Sealing. Eur J Paediatr Dent 2017, 18, 263–267. [Google Scholar] [CrossRef] [PubMed]
- Memarpour, M.; Shafiei, F. The Effect of Antibacterial Agents on Fissure Sealant Microleakage: A 6-Month in Vitro Study. Oral Health Prev Dent 2014, 12, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Mézquita-Rodrigo, I.; Scougall-Vilchis, R.J.; Moyaho-Bernal, M.A.; Rodríguez-Vilchis, L.E.; Rubio-Rosas, E.; Contreras-Bulnes, R. Using Self-Etch Adhesive Agents with Pit and Fissure Sealants. In Vitro Analysis of Shear Bond Strength, Adhesive Remnant Index and Enamel Etching Patterns. European Archives of Paediatric Dentistry 2022, 23, 233–241. [Google Scholar] [CrossRef]
- Rotta M, Bresciani P, Moura SK, Grande RH, Hilgert LA, Baratieri LN, Loguercio AD, R.A. Effects of Phosphoric Acid Pretreatment and Substitution of Bonding Resin on Bonding Effectiveness of Self-Etching Systems to Enamel. J Adhes Dent. 2007, 9, 537–545. [CrossRef]
- Tsujimoto, A.; Barkmeier, W.; Takamizawa, T.; Latta, M.; Miyazaki, M. The Effect of Phosphoric Acid Pre-Etching Times on Bonding Performance and Surface Free Energy with Single-Step Self-Etch Adhesives. Oper Dent 2016, 41, 441–449. [Google Scholar] [CrossRef]
- Eltoukhy, R.I.; Elkaffas, A.A.; Ali, A.I.; Mahmoud, S.H. Indirect Resin Composite Inlays Cemented with a Self-Adhesive, Self-Etch or a Conventional Resin Cement Luting Agent: A 5 Years Prospective Clinical Evaluation. J Dent 2021, 112, 103740. [Google Scholar] [CrossRef]
- Yun, X.; Li, W.; Ling, C.; Fok, A. Effect of Artificial Aging on the Bond Durability of Fissure Sealants. J Adhes Dent 2013, 15, 251–258. [Google Scholar] [CrossRef]
- Cardoso, M. V.; De Almeida Neves, A.; Mine, A.; Coutinho, E.; Van Landuyt, K.; De Munck, J.; Van Meerbeek, B. Current Aspects on Bonding Effectiveness and Stability in Adhesive Dentistry. Aust Dent J 2011, 56, 31–44. [Google Scholar] [CrossRef]
- McCafferty, J.; O’Connell, A.C. A Randomised Clinical Trial on the Use of Intermediate Bonding on the Retention of Fissure Sealants in Children. Int J Paediatr Dent 2016, 26, 110–115. [Google Scholar] [CrossRef]
- Colombo, S.; Paglia, L. Dental Sealants Part 1: Prevention First. Eur J Paediatr Dent 2018, 19, 80–82. [Google Scholar] [CrossRef]
- Olczak-Kowalczyk, D.; Szczepańska, J.; Kaczmarek, U. Współczesna Stomatologia Wieku Rozwojowego, 1st ed.; Med Tour Press: Otwock, 2017; ISBN 978-83-87717-26-1. [Google Scholar]
- Lubojanski, A.; Piesiak-Panczyszyn, D.; Zakrzewski, W.; Dobrzynski, W.; Szymonowicz, M.; Rybak, Z.; Mielan, B.; Wiglusz, R.J.; Watras, A.; Dobrzynski, M. The Safety of Fluoride Compounds and Their Effect on the Human Body—A Narrative Review. Materials 2023, 16. [Google Scholar] [CrossRef]
- Wright, J.T.; Tampi, M.P.; Graham, L.; Estrich, C.; Crall, J.J.; Fontana, M.; Gillette, E.J.; Nový, B.B.; Dhar, V.; Donly, K.; et al. Sealants for Preventing and Arresting Pit-and-Fissure Occlusal Caries in Primary and Permanent Molars: A Systematic Review of Randomized Controlled Trials - A Report of the American Dental Association and the American Academy of Pediatric Dentistry. Pediatr Dent 2016, 38, 282–294. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Barrera, M.Á.; De Jesús Saucedo-Molina, T.; Scougall-Vilchis, R.J.; De Lourdes Márquez-Corona, M.; Medina-Solís, C.E.; Maupomé, G. Comparison of Two Types of Pit and Fissure Sealants in Reducing the Incidence of Dental Caries Using a Split-Mouth Design. Acta Stomatol Croat 2021, 55, 137–146. [Google Scholar] [CrossRef]
- Kosior, P.; Dobrzyński, M.; Korczyński, M.; Herman, K.; Czajczyńska-Waszkiewicz, A.; Kowalczyk-Zając, M.; Piesiak-Pańczyszyn, D.; Fita, K.; Janeczek, M. Long-Term Release of Fluoride from Fissure Sealants—In Vitro Study. Journal of Trace Elements in Medicine and Biology 2017, 41, 107–110. [Google Scholar] [CrossRef] [PubMed]
- Horst, J.A.; Tanzer, J.M.; Milgrom, P.M. Fluorides and Other Preventive Strategies for Tooth Decay. Dent Clin North Am 2018, 62, 207–234. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Graphical depiction of fluoride activity in caries prevention.
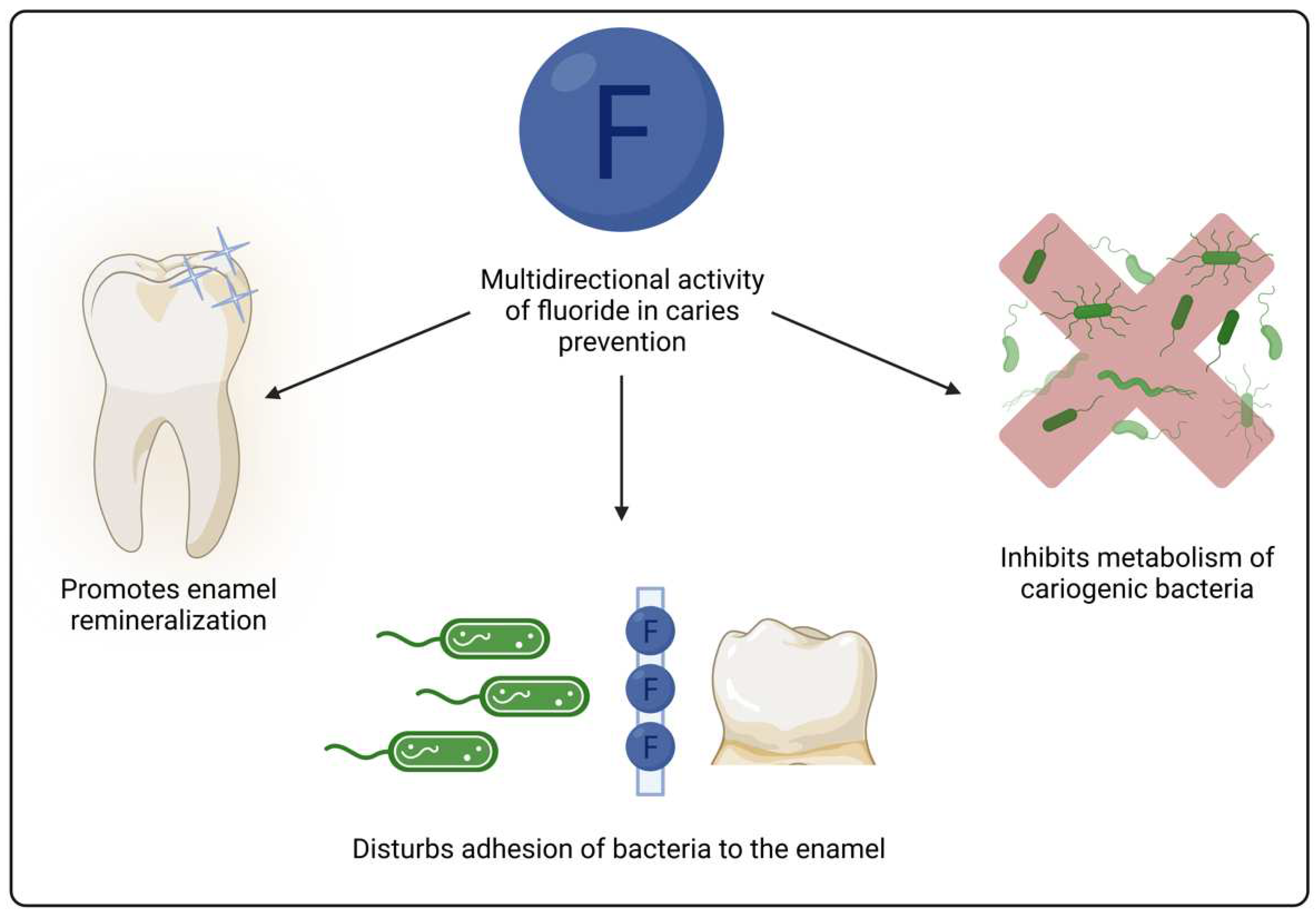
Figure 2.
Exemplary chemical structure of compounds with antimicrobial properties used in dental sealants including 1,3,5-triacryloylhexahydro-1,3,5-triazine (TAT), methacryloxylethyl cetyl dimethyl ammonium chloride (DMAE-CB) and acrylated hydroxyazobenzenes (AHA).
Figure 2.
Exemplary chemical structure of compounds with antimicrobial properties used in dental sealants including 1,3,5-triacryloylhexahydro-1,3,5-triazine (TAT), methacryloxylethyl cetyl dimethyl ammonium chloride (DMAE-CB) and acrylated hydroxyazobenzenes (AHA).
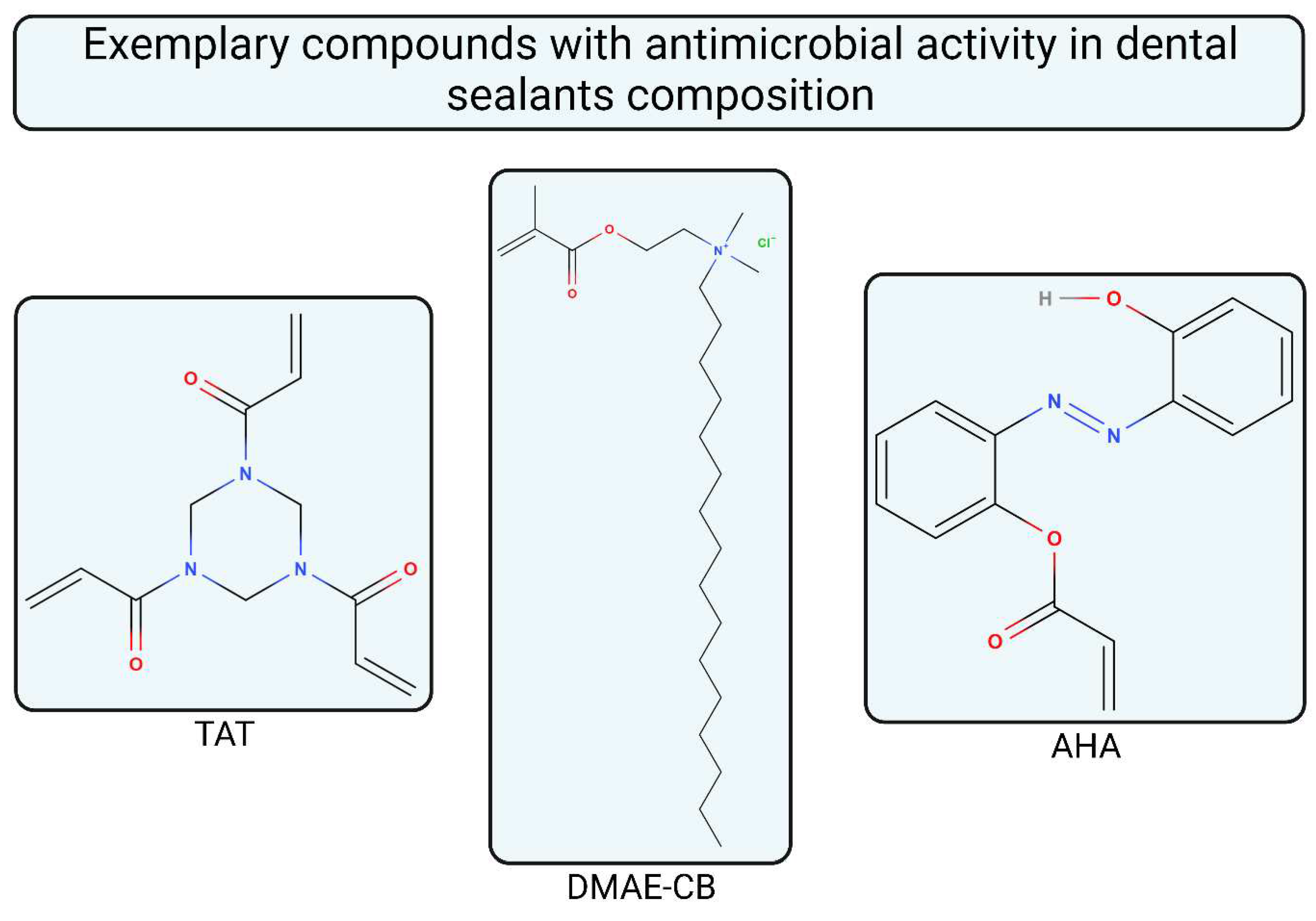

Table 1.
Juxtaposition of commercially used materials dedicated for sealing.
| Product Name | Abbreviation | Manufacturer | Composition | Fluoride Presence | Shear bond Strength [MPa] | Hardness [HK] or [HV] |
Shrinkage [%] | Reference |
|---|---|---|---|---|---|---|---|---|
| Helioseal F | HF | Ivoclar Vivadent, Lichtenstein | Bis-GMA, dimetacrylates fluorosilicate glass, silica, titanium dioxide, initiators and stabilizers | Yes | 13.7 ± 7.0 | 19.3 HV | 3.98 | [8,9] |
| Embrace Wetbond | EW | Pulpdent, United States | Uncured acrylate ester monomers 55-60%, amorphous silica 5 %, sodium fluoride <2% | Yes | 21.7 ± 2.0 | 23.9 HV | 3.45 | [8,10,11] |
| Fuji Triage | FT | GC Cooperation, Japan | Glass-ionomer, aluminofluorosilicate glass, polyacrylic acid, distilled water, polybase carboxylic acid | Yes | 3.5 ± 0.8 | 52.0 ± 1.0 HV* | - | [12,13] |
| Smart Seal loc F | SSLF | Detax, Germany | bis(methacryloxyethyl) hydrogen phosphate,2-propenoic acid, 2-methyl-2-hydroxyethyl ester, phosphate,2-dimethylaminoethyl methacrylate | Yes | 9.5 ± 1.4 | - | 5.06 ± 1.20 | [14,15] |
| Fuji VII EP | F7E | GC Cooperation, Japan | Fluoroaluminosilicate glass, CPP-ACP, pigment, distilled water, polyacrylic acid, polybase carboxylic acid | Yes | 5.0 ± 1.7 | 47.1 ± 6.0 HV | - | [12,16] |
| GCP Glass Seal | GCP | GCP Dental, Netherlands | Nanoparticles glass ionomer-based material | Yes | - | 50.0 ± 1.5 HV | - | [13,17] |
| Ketac Molar | KM | 3M ESPE, Germany | Al-Ca-La fluorosilicate glass, 5% copolimeracid (acrylic and maleic), polyacril enoic acid, tartaric acid, water | Yes | 4.8 ± 1.0 | 89.9 ± 4.2 HV | - | [18,19] |
| Voco Ionofil Molar AC Quick | IMAC | Voco, Germany | Water, pure polyacrid acid, (+)-tartaric acid, aluminofluorosilicate glass and pigments | Yes | 5.3 ± 0.6 | 79.9 ± 2.1 HV | - | [18,20,21] |
| Equia Fil | EQF | GC Cooperation, Japan | Polyacrylic acid, aluminosilicate glass, distilled water | No | - | 99.3 ± 4.5 HV | - | [18] |
| UltraSeal XT plus | USXT | Ultradent, USA | Triethylene glycol dimethacrylate 10-25%, diurethane dimethacrylate 2.5-10%, aluminium oxide 2.5-10%, 2-hydroxyethyl methacrylate < 2.5%, amine methacrylate < 2.5%, organophosphine oxide < 2.5%, sodium monofluorophosphate < 0.1% | Yes | 42.7 | 27.6 HK | 5.98 | [22,23] |
| Conseal F | CF | SDI, Australia | Urethane dimethacrylate base 7% filled with a submicron filler size of 0.04 µm | No | 14.0 ± 0.9 | - | - | [14] |
| Tetric Flow | TF | Vivadent | Bis-GMA (10-25%), urethane dimethacrylate (10-25%), ytterbium trifluoride, 1,10-decandiol dimethacrylate (2.5-10%), diphenyl(2,4,6- trimethylbenzoyl)phosphine oxide (0.1-2.5%), 2-(2-Hydroxy-5-methylphenyl)-benzotriazol; 2-(2H-Benzotriazol-2-yl)-p-kresol (0.1-1.0%) | Yes | 16.8 ± 2.7 | 34.0 HV** | - | [9,24,25] |
| Tetric Evo Ceram | TEC | Vivadent | Dimethacrylate co-monomers (17-18 wt.%), barium glass, ytterbium trifluorid, mixed oxides and prepolymers (82-83 wt.%) | Yes | 20.7 ± 7.2 | 51.0 HV** | 1.95 ± 0.03 | [24,26,27] |
| Wave | WV | SDI, Australia | UDMA, strontium glass | No | 24.6 ± 1.5 | - | 5.00 | [28,29] |
| Clinpro Sealant | CS | 3M ESPE, Germany | TEGDMA, bisphenol A digilycidyl ether dimethacrylate, tetrabuttylammonium tetrafluoroborat, silane-treated silica |
Yes | 12.8 ± 8.3 | 21.5 ± 0.2 HV | 6.60 ± 1.54 | [15,30,31] |
| Grandio Seal | GS | Voco, Germany | Triethylene glycol dimethacrylate (10-25%), fumed silica (5-10%), Bis-GMA (2.5-5%) | No | 42.6 ± 3.2 | 75.1 ± 2.0 HV | - | [31,32,33] |
| Fissurit FX | FFX | Voco, Germany | Triethylene glycol dimethacrylate (15–25%), Bis-GMA (5–10%), sodium fluoride (≤2.5%) | Yes | 6.2 ± 0.7 | - | 4.30 ± 1.15 | [15,34,35] |
| Dyract Seal | DS | Dentsply, Germany | Aminopenta, strontium-aluminium, macromonomer, fl uorosilicate glass, DGDMA, aerosil, initiators, inhibitor | Yes | 8.3 ± 0.3 | - | 5.38 ± 1.30 | [15,36] |
| Teethmate F-1 | TF1 | Kuraray, Japan | 2-hydroxyethyl methacrylate, TEGDMA, 10-methacryloyloxydecyl dihydrogen phosphate, methacryloylfluoride-methyl methacrylate copolymer, hydrophobic aromatic dimethacrylate, dl-camphorquinone, initiators, accelerators, dyes |
Yes | - | 26.7 ± 1.3 HV* | 7.40 ± 1.17 | [13,15] |
* Recalculated from GPa; ** Coverted from HK.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



